DEVELOPMENT OF THE ORAL FACIAL REGION
After reading this chapter the student will be able to:
• discuss the development of the oral pharynx, the pharyngeal arches including the pharyngeal pouches, the neural, vascular muscular components
• describe the skeletal components and the development of the tissues of the face
Ethmosphenoid and sphenoccipital articulations
Facial bones: zygomatic, maxillary, frontal, and temporal
Facial suture types: simple, serrated/interdigitating, squamosal
Facial sutures: zygomaticomaxillary, frontomaxillary, and zygomaticotemporal
Frontal, parietal, and squamous portions
Hyoid: superior hyoid, inferior hyoid
Masseter, medial, and lateral pterygoid and temporalis muscles
Meckel’s cartilage bar, Meckel’s cartilages
Pharyngeal arch/mandibular arch
Premaxillary, maxillary, zygomatic, and petrous portions
OVERVIEW
This chapter concerns development and orientation of the tissues that form the human face and neck. During the fourth week of development, the human embryo consists of a flat disk that bends down at its anterior extremity as the overlying brain expands and enlarges. This action pushes the heart beneath the brain. A pit develops in the midline between the brain and the heart and becomes the oral cavity or stomodeum (see Fig. 3-2). Beneath this pit the first pharyngeal arch, termed the mandibular arch, forms. The maxillary tissues that form the cheeks grow from this first arch. Below the mandibular arch four other pharyngeal arches or bars appear during the fourth to seventh prenatal week. The second arch is called the hyoid (see Fig. 3-2). These parallel arches are important in the development of the face and neck, and each contains blood vessels, muscles, nerves, and skeletal elements. Aortic arch blood vessels, which course through each pharyngeal arch from the heart below to the brain above, are important to craniofacial development.
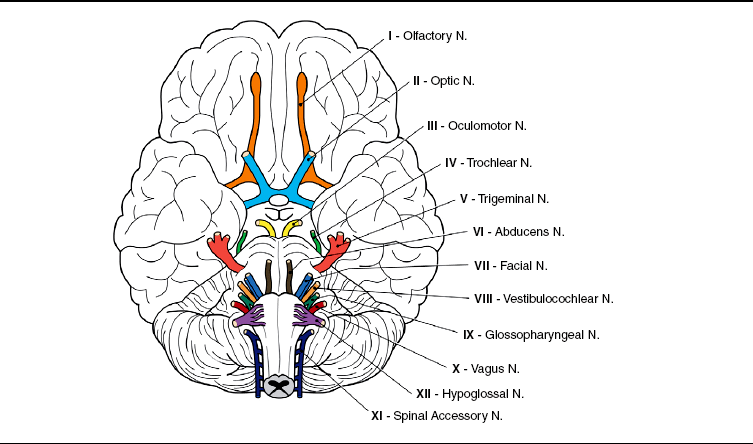
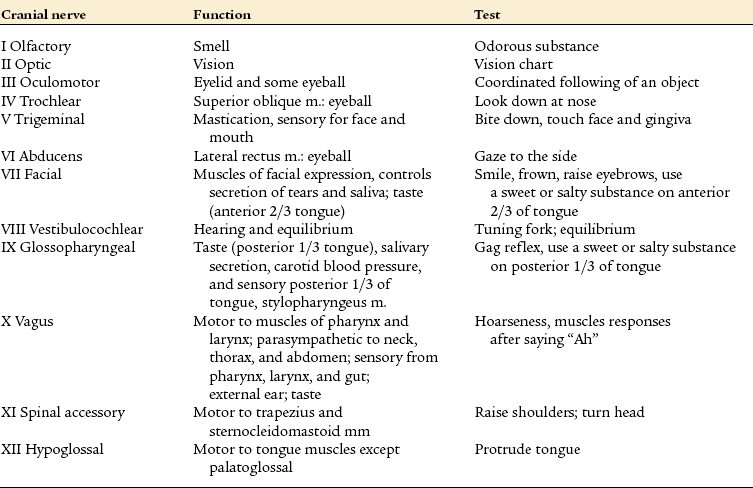
The first, second, and fifth of these vessels soon disappear. The third arch vessel quickly assumes the role of supplying nutrients to the tissues of the first and second arches. This third arch vessel also shifts the blood supply to the face from the internal carotid vessels to the external carotid. Muscles arise in each of the pharyngeal arches: the mandibular arch muscles become the masticatory muscles; the second arch muscles become the facial expression muscles; and the muscles of the third and fourth arches become the constrictor muscles of the throat. Cranial nerves enter each of these muscle masses as they arise. The fifth nerve enters the mandibular arch to innervate the muscles of mastication. The seventh innervates the second arch muscle mass, and other cranial nerves innervate the muscles of the neck. Cartilage also appears in each arch: Meckel’s cartilage bar in the first, the superior hyoid in the second, the inferior hyoid in the third, and the laryngeal cartilages in the fourth. The cranial base cartilages arise to support the brain and from them come the auditory and olfactory sense capsules. All the creative events described in this chapter take place from the fourth to seventh prenatal weeks, the short time required for facial organization. Functions and tests for cranial nerves are discussed in Table 3-1.
DEVELOPMENT OF THE OROPHARYNX
The oropharynx is composed of the primitive oral cavity and the area of foregut called the pharynx. The oral pit first appears in the fourth week of development, when the neural plate bends ventrally as the neural folds develop to form the forebrain. This cephalocaudal bend pushes the heart ventrally, and the yolk sac becomes enclosed to form an elongating tube known as the foregut (Fig. 3-1).
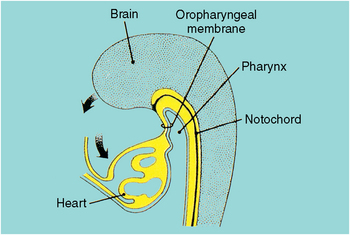
Fig. 3-1 The embryo head bends anteriorly with the growth and expansion to the head. This pushes the heart ventrally and the oral pit (stomodeum, see Fig. 3-2) develops between the brain and the heart.
The deepening oral pocket then appears between the forebrain and the heart and eventually becomes the oral cavity (Fig. 3-2). At its deepest extent is the oropharyngeal membrane, which ruptures in the fifth week, opens the oral cavity to the tubular foregut, and soon becomes the oropharynx (Figs. 3-3 and 3-4). The mandibular arch will grow laterally to the oral pit, developing the maxillary process, which forms the cheeks.
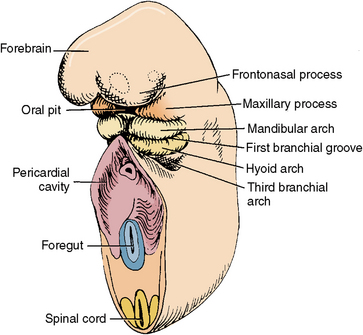
Fig. 3-2 Internal view of the oral pit at 3½ weeks. The oropharyngeal membrane separated the oral pit (stomodeum) and the pharyngeal cavities. The membranes will then rupture, allowing the two cavities to join.
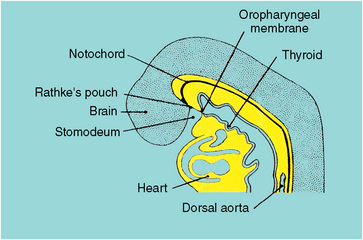
Fig. 3-3 Facial development in the fourth prenatal week. The oral pit is surrounded by the facial primordia, which are the frontonasal processes, the maxillary processes and the mandibular arch. The pharyngeal arches are defined by grooves between each arch. The heart develops in the thorax, which is in the pericardial cavity.
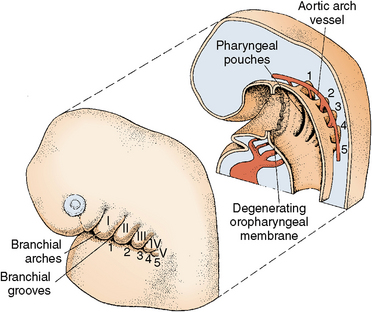
Fig. 3-4 Sagittal view of pharyngeal arches with corresponding groove between each arch. The pharyngeal arches are seen in the wall of the pharynx. The aortic arch vasculature leads from the heart through these arches to the face.
The enlarging heart now becomes positioned below the mandibular arch in the thorax and begins beating at the end of the fourth week (see Fig. 3-2). Blood is forced through the vessels in the pharyngeal arches supplying the face, neck, and brain. The forming face now grows away from the forebrain and presses against the chest and heart.
DEVELOPMENT OF THE PHARYNGEAL ARCHES
 CLINICAL COMMENT
CLINICAL COMMENTFrom the initial development, each pharyngeal arch has a specific cranial nerve associated with it. The nerves and the musculature of each arch emerge together and follow defined pathways to their functional positions. These events are closely regulated genetically during development, and few errors occur.
The pharyngeal arches are so termed because they bend around the sides of the pharynx as bars of tissue. Each arch is separated by vertical grooves on the lateral sides of the neck at the fifth week. Within the pharynx, grooves called pharyngeal pouches separate each arch. These pouches match the pharyngeal clefts on the external aspects of the neck (see Fig. 3-4).
 Consider the Patient
Consider the PatientA patient appears with a swelling in the lateral area of the neck and states that the swelling subsides from time to time but then resumes. He asks you what you think the cause may be.
The five arches with their clefts resemble the embryonic gill slits of fish and amphibians. This is one of many similarities between human embryos and other embryos during early development. The first arch is termed the mandibular arch because it will later form the bony mandible and the associated muscles of mastication, nerves, and blood supply. The second, or hyoid, arch forms the facial muscles, vessels, and hyoid bone. The third, fourth, and fifth arches consist of paired right and left bars that are divided before they reach the midline by the presence of the bulging heart (see Fig. 3-2). The arches become progressively smaller anterior to posterior. The outer surface of each arch is covered with ectoderm as are the inner surface of the first arch and the covering of the anterior surface of the second. This ectoderm is the epithelial lining of the oral cavity. The pharyngeal surface of the remaining four arches is, however, lined by endoderm, which is the same as the lining of the gastrointestinal tract (see Fig. 3-4). The cores of the arches—the blood vessels, muscles, nerves, cartilages, and bones—will differentiate and are important in the development of the adult human face.
The face develops during the short span from the fourth to seventh prenatal weeks. Environmental factors can cause a facial or pharyngeal arch defect, which would probably affect these tissues before the fourth week. This is the time to be especially careful of irradiation and chemical, hormonal, dietary, or stress-related factors.
Pharyngeal Grooves and Pharyngeal Pouches
The first pharyngeal groove deepens to become the external auditory canal leading to the middle ear. The membrane at the depth of this tube becomes the tympanic membrane. The middle ear and eustachian tube develop from the corresponding first pharyngeal pouch. After the fifth week, no other pharyngeal grooves are seen externally as the tissues of the second and fifth arch grow over the other arches and grooves and make contact with each other (Fig. 3-5, A). This overgrowth obscures the tissue of both the arches and the grooves externally, although their internal structures are unaffected and provide an important role in facial and body development (Fig. 3-5, A and B).
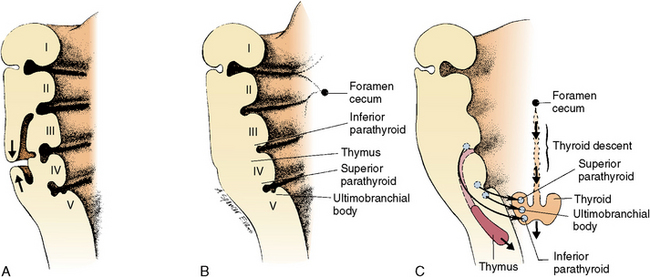
Fig. 3-5 Cross section of the pharyngeal arches. A, Tissues of pharyngeal arches 2 and 5 overgrow together, which results in disappearance of arches 2 to 5 and external smoothing of the neck. B, Resulting external appearance follows overgrowth. C, Contribution of the pharyngeal pouches.
The endodermal lining of the pharyngeal pouches differentiates into several important organs. The second pharyngeal pouch becomes the palatine tonsils; the third becomes the inferior parathyroids and thymus; the fourth becomes the superior parathyroids; and the fifth becomes the ultimobranchial body (Fig. 3-5, C).
The palatine tonsils function in the development of lymphocytes, which are important in the immunology of the body. The parathyroid glands regulate calcium balance throughout life. The thymus, located behind the sternum and between the lungs, is large at birth and continues to grow until puberty, during which it begins to atrophy but continues to function. Although its full importance is unknown, the thymus produces T cells that destroy invading microbes and are therefore important to the body’s immune system. The ultimobranchial body fuses with the thyroid and contributes parafollicular cells to the thyroid. The function of the ultimobranchial body remains unknown (Fig. 3-5, B and C).
Vascular Development
Each of the five pharyngeal arches contains a right and a left aortic arch vessel that leads from the heart through the arches to the face, brain, and posterior regions of the body (see Fig. 3-4). Not all of these paired aortic arches are present at the same time, however. The first and second begin to develop in the fourth week and disappear in the fifth week (Fig. 3-6). The third arch vessels then become prominent, taking over the facial area of the first two. As the fourth and fifth arch vessels arise, the fourth becomes prominent and the fifth disappears (Fig. 3-7). Next, the sixth arch vessels appear and become dominant along with those of the third and fourth.
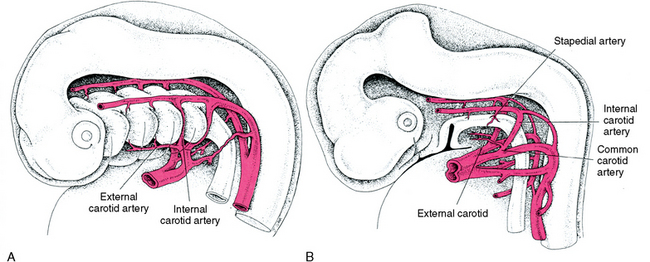
Fig. 3-6 Aortic arch development. A, At 4 weeks, the anterior aortic arch vessels have passed through the pharyngeal arch tissue and then disappear. The pharyngeal arch pouches project laterally between each arch. B, At 5 weeks, the third pharyngeal arch vessels become the right and left common carotid, which supplies the face by means of the internal carotid and stapedial arteries.
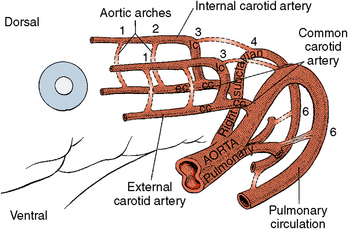
Fig. 3-7 Details of aortic arch changes during early development of 3 to 5 prenatal weeks. Aortic arch vessels numbers 1, 2, and 5 disappear as the arches modify. Arch 3 becomes the common carotid and arch 4 becomes the dorsal aorta. The dorsal aorta then enlarges so that the common carotid arises from the dorsal aorta.
The third arch vessels become the common carotid arteries, which supply the neck, face, and brain. The fourth arch vessels become the dorsal aorta, which supplies blood to the remainder of the body, and the vessels of the sixth arch supply the lungs with pulmonary circulation (Fig. 3-7).
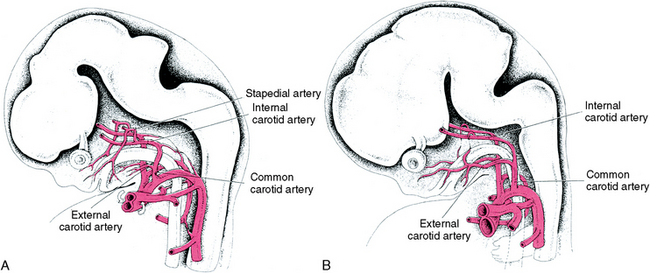
An important feature of the common carotid arteries is the supply of blood to the face, neck, and brain from the internal carotid artery. However, after 7 weeks, the circulation to the face and neck shifts from the internal to the external carotid (Fig. 3-8). The internal carotid continues to supply the growing brain.
Muscular and Neural Development
Muscle cells in the first arch become apparent during the fifth week and begin to spread within the mandibular arch into each muscle site’s origin in the sixth and seventh week (Fig. 3-9). By the tenth week, the muscles of the second arch have formed a thin sheet that extends over the face and posterior to the ear (Fig. 3-10). As these muscles grow over the face, they develop into the various groups of muscles that attach to the newly ossifying bones of the facial skeleton. The muscle masses of the mandibular arch, on the other hand, remain in the first arch and become easily recognized muscles of mastication (Fig. 3-9, A). These are the masseter, medial, and lateral pterygoid, and temporalis muscles. They all relate to the developing mandible (Fig. 3-11).
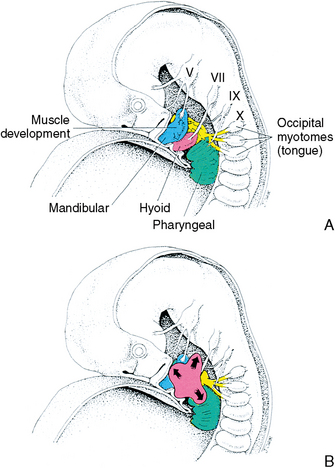
Fig. 3-9 Development of the muscles and nerves of the pharyngeal arches. A, Mandibular muscle mass expands to form the muscles of mastication. B, At 7 weeks, the muscles of the second arch grow upward to form the muscles of the face.
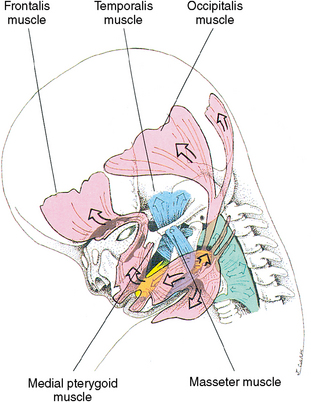
Fig. 3-10 The facial muscles grow from the second arch to cover the face, the scalp, and muscles posterior to the ear. These all become muscles of facial expression.
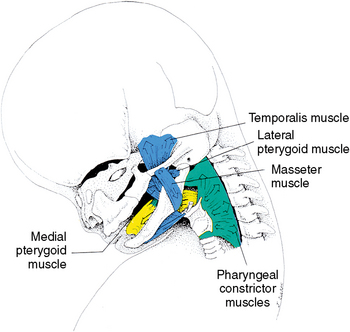
Fig. 3-11 Masticatory muscles of the mandibular arch. The medial pterygoid and masseter muscles attach as a sling at the angle of the mandible. The temporalis muscle grows from the coronoid process into the temporal fossa, and the lateral pterygoid muscle extends from the condyle anteriorly to the sphenoid bone and the pterygoid bone in the temporal fossa.
The masseter and medial pterygoid form a vertical sling that inserts into the angle of the mandible. The temporalis muscle spreads into the infratemporal fossa that inserts into the developing coronoid process of the mandible. The lateral pterygoid extends horizontally from the neck of the condyle, and some fibers insert into the temporomandibular disk (see Chapter 13). The pharyngeal constrictor muscles in the fourth arch have differentiated in the neck and function to enclose the pharynx (see Fig. 3-11).
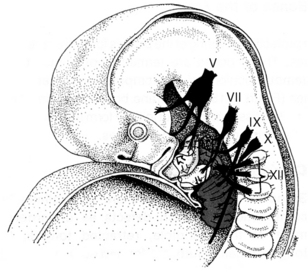
Nerves develop in conjunction with the developing muscle fibers. By the end of the seventh week, the fibers of the fifth nerve have entered the mandibular muscle mass, as has the seventh nerve in the facial muscle mass in the second arch (Fig. 3-12). As these muscle masses develop, the nerves are present and follow or lead them as they migrate to their position of differentiation, maturation, and function. The seventh nerve supplies the stylohyoid and stapedius muscles and the posterior belly of the digastric muscle. The ninth (glossopharyngeal) nerve enters the third arch and supplies the stylopharyngeal and upper pharyngeal constrictor muscles. The tenth (vagus) nerve innervates muscles of the fourth arch, which are the inferior constrictors and laryngeal muscles. The tongue, which is primarily muscle, relates to the branches of the ninth nerve, which carries the sensory modality of taste from the taste buds located in the posterior one third of the tongue and to the seventh nerve, which carries the modality of taste from the taste buds on the anterior two thirds of the tongue. The fifth nerve is the sensory nerve to the same area of the anterior tongue (see Fig. 3-12). The tongue is a good example of muscle cell migration because it originates in the occipital myotome and migrates anteriorly into the floor of the mouth. During migration, the nerves mentioned enter the muscle mass and later carry out their functions (Fig. 3-13).
Cartilaginous Skeletal Development
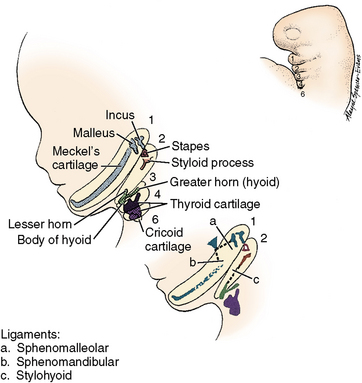
The initial skeleton of the pharyngeal arches develops as cartilaginous bars. In the first arch, Meckel’s cartilages appear bilaterally (see Fig. 3-13). The anterior aspects of these two cartilages approach each other near the midline but do not coalesce. Posteriorly, each terminates in an enlarged bulbous structure called the malleus. The malleus lies adjacent to a small cartilage called the incus. Farther posterior is a third body of cartilage, the stapes (see Fig. 3-13). These three bilateral cartilages later transform into bone and function in the middle ear as hearing bones.
Substantial evidence shows that the contact point of the malleus and incus is the articulation of the lower jaw for the first 20 weeks of prenatal life. Then the second temporomandibular joint, which is the articulation of the condyle and the temporal fossae, becomes functional (Fig. 3-14). Chapter 13 has further information about the temporomandibular joint.
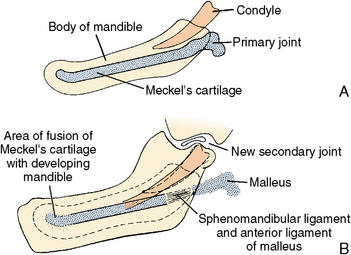
Fig. 3-14 Relationship between the primary and secondary temporomandibular joints. A, Meckel’s cartilage with its posterior malleus-incus joint, which functions in jaw movements during the first 4 months of prenatal life. B, A shift to the condylar-temporal articulation that occurs after that time both prenatally and postnatally.
The rod-shaped cartilage of the second or hyoid arch is known as Reichert’s cartilage. The stapes, styloid process, lesser horn, and upper body of the hyoid arise from this arch (see Fig. 3-13). The third arch cartilage forms the greater horn and the lower part of the hyoid body. The fourth arch contributes to the hyoid cartilage, which then supports the gland. The fifth arch has no adult cartilage derivatives, and the sixth arch cartilage forms the laryngeal cartilage (see Fig. 3-13).
DEVELOPMENT OF THE CRANIOFACIAL SKELETON
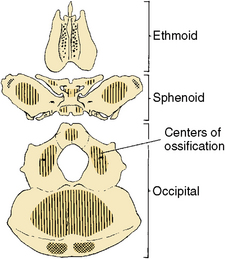
The earliest formed skeletal elements in the craniofacial area are the cartilaginous nasal capsule (ethmoid), the sphenoid, the auditory capsules, and the basioccipital cartilages. All these cartilages initially arise as a single cartilaginous continuum in the midline underlying the brain (Fig. 3-15). Anteriorly, the nasal capsule contains the organ of smell. Laterally, the auditory capsules protect the organs of hearing (see Fig. 3-15). The sphenoid cartilage is posterior to the ethmoid. It later forms wings of bone that spread out under the brain laterally (Fig. 3-16). Behind the sphenoid is the occipital cartilage. Although the ethmoid capsule, sphenoid, and basioccipital cartilages are formed as a single cartilaginous unit initially, they separate later to form individual bones. These cartilages underlie and support the brain and are known as the cranial base. The cranial base is determined by drawing a line from the nasal bone (nasion) to the sella turcica of the sphenoid to the basion, as seen in Figure 3-17. These cartilages are transformed into bone by endochondral bone formation.
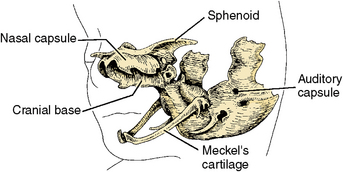
Fig. 3-15 The cartilages of the face and skull. Observe how the cranial base cartilage supports the maxillary and mandibular cartilages of the face. The locations of the nasal and auditory capsules and sphenoid are shown. All central skeletal elements arise in cartilage and later are transformed into bone.

Bones of the Face
The protective covering of the brain is formed by membrane bones. These bones are termed frontal, parietal, and squamous portions of the temporal and interoccipital bones (Fig. 3-18). Membrane bones form directly from connective tissue and do not initially form from cartilage.
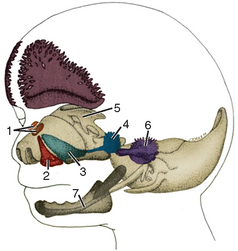
Fig. 3-18 Relationship of cranial cartilages to the membrane bones of the face at 8 weeks. The membrane bones are numbered: 1, nasal; 2, premaxillary; 3, maxillary; 4, zygomatic; 5, sphenoid; 6, temporal; 7, mandible.
Pharyngeal arch syndromes are seen clinically as combinations of such defects as underdevelopment of the mandible, retracted tongue, large tongue, small mouth, malformed ears, and cleft palate. A rare disorder, Treacher Collins syndrome, is directly attributable to pharyngeal arch deficiencies.
The facial bones, which also form in membrane bone, complete the facial skeleton. They develop overlying the nasal capsule and are called the premaxillary, maxillary, zygomatic, and petrous portions of the temporal bone (see Fig. 3-18). These bones initially appear as tiny ossification centers in the face and then increase in diameter, spreading anteriorly, posteriorly, and upward into the tissues surrounding the orbit (Fig. 3-19).
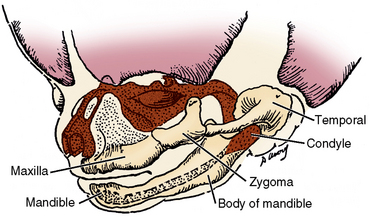
Fig. 3-19 The facial skeleton at the twelfth prenatal week. This figure illustrates the relationship of the maxillary, zygomatic, and temporal bones and their articulations. The membrane bone of the body and the cartilaginous condyle of the mandible are also shown.
The maxillary bones also grow medially into the palate to support the palatine shelf tissue (Fig. 3-20). The bones of the maxilla grow as the facial tissues continue to develop. The height of the maxilla is due partially to the growth in length of the roots of the teeth.
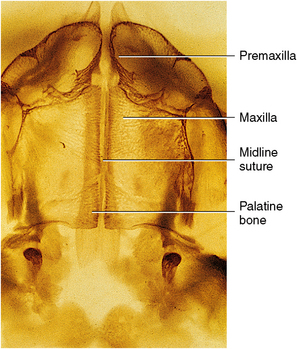
Fig. 3-20 Cleared human palate at 8 months. Sutures are seen in the midline and between the premaxillary and maxillary bones and between the maxillary and the palatine bones in the posterior palate.
The bony mandible grows laterally to the first arch cartilage as well as posteriorly to join the bony body with the cartilaginous condyle. Together, the body of the mandible and the cartilaginous condyle replace Meckel’s cartilage (see Fig. 3-19).
The mandible develops as several units: a condylar unit forms the articulation, allowing movement of the mandible; the body is the center of all growth and function of the mandible; the angular process responds to the lateral pterygoid and masseter masticatory muscles; the coronoid process responds to the temporalis muscle development and attachment; the alveolar process responds to development of the teeth (Fig. 3-21). This development produces the mature mandible (Fig. 3-22).
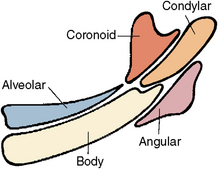
Fig. 3-21 Developing areas of the mandible and their responses to stimuli. The mandible develops from several parts, the condyle in cartilage is the articulation site, the coronoid develops in response to the temporalis muscle, the angular area is in response to the medial pterygoid and the masseter muscle, the mandible in membrane bone is the unifying structure fusing with all parts, and the alveolar process develops in response to the developing teeth.
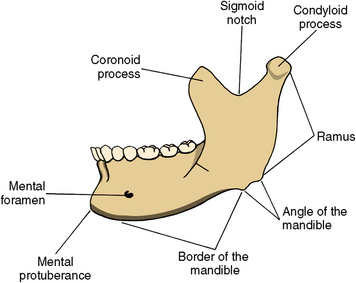
Fig. 3-22 Appearance of the adult mandible. Compare the difference of this adult mandible with the developing one in Figure 3-21. Observe in the adult mandible all parts have fused together to develop a strong, erect single bone.
Many facial defects result from a lack of transformation of the pharyngeal arches to their adult derivatives. Pharyngeal cysts and fistulas may appear along the sides of the neck because the epithelial-lined pockets remain as a result of the overgrowth of the arches. These defects may also open in the pharynx. Cysts and fistulas may result in swelling or draining of mucus from an opening on the side of the neck.
Sutures of the Face
A system of articulations develops between each of the major bones of the face to facilitate growth. These articulations are positioned in the direction of facial growth, which is forward, away from the brain, and downward to facilitate lengthening of the face. The articulations are termed sutures and are defined as fibrous joints in which the opposing surfaces are closely united. A suture develops between the zygomatic, maxillary, frontal, and temporal facial bones. Sutures are named for the two or more bones with which they articulate. Facial sutures are named zygomaticomaxillary, frontomaxillary, and zygomaticotemporal (see Fig. 3-22).
These articulations are growth sites that allow the associated bones to expand and to maintain orientation at their junctions by means of the fibrous attachment that controls their relationship with the adjacent bones. Such articulations may consist of a band of connective tissue termed syndesmosis (Fig. 3-23). In the center of this band are osteogenic cells, which along the periphery provide for new bone growth. The sutures of the face are of three types: simple, which is an uncomplicated band of tissue between bony fronts (see Fig. 3-23); serrated, which is an interdigitating type of suture (Fig. 3-24); and squamosal, which has a beveled or overlapping type junction (Fig. 3-25). Each connective tissue suture consists of a central zone of proliferating connective tissue cells with osteogenic cells along the peripheral bony fronts. Each suture is surrounded by a fibrous connective tissue (see Figs. 3-23 to 3-25). When the position of these sutures in the fetal skull is compared with the position of the sutures in the adult skull, the relationship of these articulations appears similar, although adult bones are larger (compare Figs. 3-26 and 3-27). When facial growth is complete, all of these sutures will become inactive, although the interface of the opposing bones remains and defines the boundary of the facial bones.

Fig. 3-23 Histology of a simple suture. Observe the opposing bony fronts with connective tissue and blood vessels between them. Osteoblasts appear along the opposing bony fronts and form bone to provide growth of this suture.
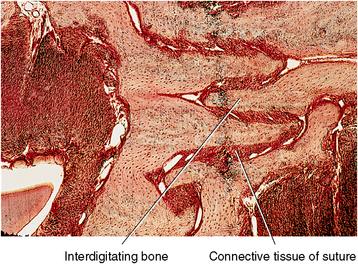
Fig. 3-24 Histology of a serrated suture of the skull. Observe the interdigitating extensions of bone from both adjacent surfaces. Connective tissue appears between these bony fronts. This is a strong suture.
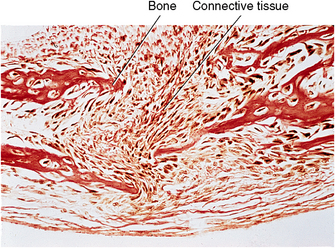
Fig. 3-25 Histology of a developing squamous suture. These are overlapping sutures, and connective tissue and blood vessels appear between the bony fronts. For example, one squamous suture is between the parietal and temporal bones on the sides of the head.
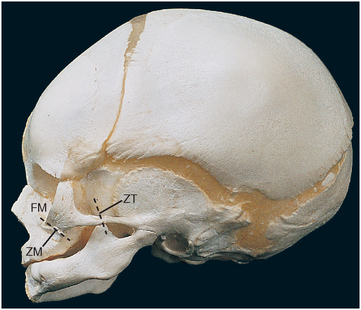
Fig. 3-26 Sutures of the developing skull of the newborn. FM, frontomaxillary; ZM, zygomaticomaxillary; ZT, zygomaticotemporal. The pterygopalatine suture is not present in the newborn but is present in the adult (see Fig. 3-27).
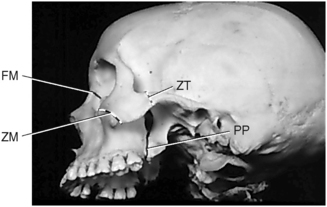
Fig. 3-27 Sutures of the adult human skull. FM, frontomaxillary; ZM, zygomaticomaxillary; ZT, zygomaticotemporal; and PP, pterygopalatine. Observe the difference in location of the sutures in the adult from those in the newborn.
In contrast to the sutures of the external face, the articulations in the midline have interposing bands of cartilage. This type of articulation is termed synchondrosis and is located in the midline (Fig. 3-28). Synchondrosis articulations grow by forming new cartilage in the center of the suture as the cartilage is transformed into bone at the periphery of the cartilage. These cartilage articulations are of only one type and exist between the ethmoid and sphenoid and the occipital bones in the midline during the period of craniofacial growth. These are known as the ethmosphenoid and sphenoccipital articulations. Table 3-2 presents a summary of all structures that develop from the pharyngeal arches, pharyngeal grooves, and pharyngeal pouches.
TABLE 3-2
SUMMARY OF STRUCTURES THAT DEVELOP FROM PHARYNGEAL ARCHES, PHARYNGEAL GROOVES, AND PHARYNGEAL POUCHES
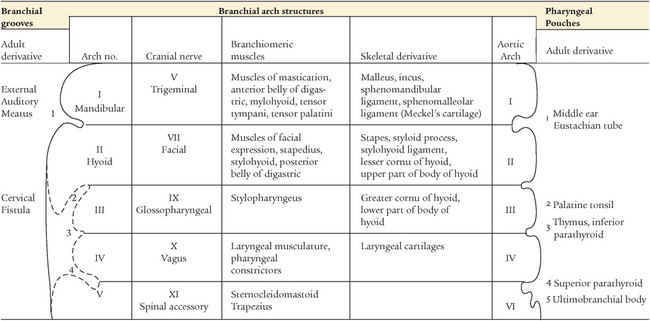
Fig. 3-28 Histology of a cartilage suture located in the midline of the base of the skull. We can observe a band of cartilage with cartilage cells differentiating in the center of it. As they migrate peripherally, the cells become osteoblasts and form bone at the peripheral surfaces of the cartilage, as seen. Bony growth thus occurs in this suture. This suture is between the ethmoid and sphenoid bone.
SELF-EVALUATION QUESTIONS
1. What structures are derived from pharyngeal arch I?
2. What is the importance of Meckel’s cartilage?
3. Identify the structures derived from pharyngeal arch II.
4. Rapid palatal expansion can be used by the orthodontist to increase the width of the hard palate. Why and when can the midpalatal suture be used to effect changes in the hard palate?
5. What are the contributions of pharyngeal pouches number 1, 2, 3, and 4?
6. Describe the origin and growth of the muscles of mastication.
7. Discuss the origin, descent, and function of the thyroid gland.
8. Discuss the origin and time of the shift in the facial blood supply.
9. Describe the cartilages of the early facial skeleton and the bones that replace them.
10. Name, locate, and describe the connective tissue sutures of the face.