PERIODONTIUM: ALVEOLAR PROCESS AND CEMENTUM
After reading this chapter the student will be able to:
• describe the nature of alveolar bone proper and supporting bone
• explain how cementum serves in tooth support
• describe the condition of physiologic tooth movement and the effects of the various types of orthodontic tooth moving devices on the hard tissues of the periodontium
• understand the effects of aging on the tooth supporting structures and the condition of edentulous jaws
OVERVIEW
This chapter discusses the hard tissues of the periodontium, which are cementum and alveolar bone. The alveolar process is the bony part of the maxilla and mandible that has the primary function of supporting the teeth. Alveolar bone is composed of alveolar bone proper, which is attached to the fibers embedded in the roots of the teeth. Supporting bone is the bone covering the mandible, and it serves as cortical plates that give support to the alveolar bone proper. This alveolar bone is in the process of continuous turnover, which enables the tissue to be responsive to manipulation, such as tooth movement resulting from normal physiologic function or orthodontic treatment. Cementum functions as the means of fiber attachment to the tooth roots. These fibers have the ability to form and resorb, which are necessary for support during tooth movement. If teeth are moving in a straight line or rotating, all parts of the suspensory apparatus must change simultaneously. This phenomenon first took place during tooth eruption and continues to function for both the primary and secondary dentition. Tooth function is a prerequisite for the maintenance of the alveolar bone and cementum. Bone loss occurs during aging or periods of inactivity, resulting in possible tooth mobilization. With loss of alveolar bone, loss of periodontal fibers occurs as well. Periodontal disease can cause these conditions with possible tooth loss that could result in an edentulous jaw (Box 12-1).
ALVEOLAR PROCESS
The alveolar process is the part of the maxilla and mandible that supports the roots of teeth and is composed of alveolar bone proper and supporting bone (Fig. 12-1). Alveolar bone proper is the bone lining the tooth socket. In clinical radiographic terms, it is defined as the lamina dura. Dense bone serves as the attachment bone that surrounds the roots of the teeth. Supporting bone is, as the name implies, the bone that serves as a dense cortical plate to sustain the alveolar bone proper. This cortical plate covers the surface of the maxilla and mandible and supports the alveolar bone proper. The supporting cancellous bone underlies and supports the dense cortical bone (see Figs. 12-1 and 12-2). The existence of alveolar bone is entirely dependent on the presence of teeth. Alveolar bone develops initially as a protection for the soft developing teeth and later, as the roots develop, as a support to the teeth. Finally, as the teeth are lost, the alveolar bone resorbs. Teeth are responsible not only for the development but also for the maintenance of the alveolar process of the mandible (see Fig. 3-21). The coronal border of the alveolar process is known as the alveolar crest (see Fig. 12-2). This crest is normally located approximately 1.2 to 1.5 mm below the dentinoenamel junction of the teeth. It is rounded on the anterior region and nearly flat in the molar area. When teeth are in buccolingual version, the alveolar crest may be thin or missing. The area of bone loss where an apical root penetrates the cortical bone is known as a fenestration, and bone loss in the coronal area of the root is termed a dehiscence (Fig. 12-3).
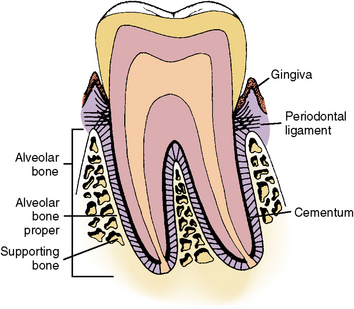
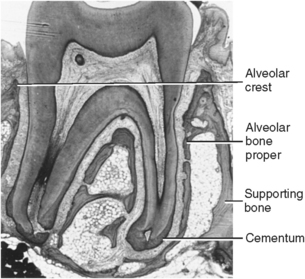
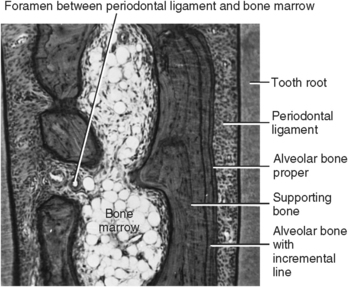
Fig. 12-2 Histology of tooth and its supportive tissues showing relationships among alveolar bone proper, supporting bone, and cementum covering roots.
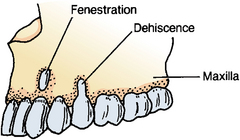
Fig. 12-3 Loss of alveolar bone adjacent to tooth. Loss near root apices is termed fenestration, whereas bone loss in region of cervical root is termed dehiscence.
 CLINICAL COMMENT
CLINICAL COMMENTThe lamina dura is an important diagnostic landmark in determining the health of the periapical tissues. Loss of density usually means infection, inflammation, and resorption of this bony socket lining.
Alveolar Bone Proper
The compact or dense bone that lines the tooth socket is of two types when viewed microscopically. This bone either contains perforating fibers from the periodontal ligament or is similar to compact bone found elsewhere in the body. Perforating fibers or Sharpey’s fibers are bundles of collagen fibers embedded in the alveolar bone proper. These fibers are at right angles or oblique to the surface of the alveolar bone proper and along the root of the tooth (see Fig. 12-1). The fiber bundles inserting in the bone are regularly spaced and appear similar to those that insert into the root surface cementum (Figs. 12-4 and 12-5). These perforating fibers are not limited to periodontal bone. They also appear in the body where ligaments or tendons attach to cartilage or bone.
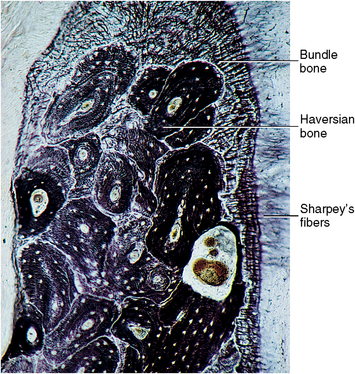
Fig. 12-4 Histology of alveolar crest area from an older individual illustrating bundle bone with penetrating (Sharpey’s) fibers and haversian-type supporting bone.
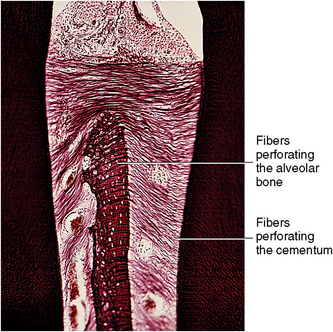
Fig. 12-5 Histology of perforating fiber bundles (Sharpey’s). Uniformity of position of numerous fibers in cemental and bony surfaces is shown. Fiber bundles of bone are larger and less numerous than fibers entering cemental surface.
Because bone of the alveolar process is regularly penetrated by collagen fiber bundles, it can be appropriately termed bundle bone. Bundle bone, being synonymous with alveolar bone proper or lamina dura, appears more dense radiographically than the adjacent supportive bone (Fig. 12-6). This density is probably the result of the mineral content or orientation of the bone crystals surrounding the fiber bundles. Blood vessels and nerves penetrate the lamina dura through small foramina. Because the mineral density is sufficient, this bone appears opaque in radiographs (see Fig. 12-6). Tension on the perforating fibers during mastication is believed to stimulate this bone and is considered important in its maintenance.
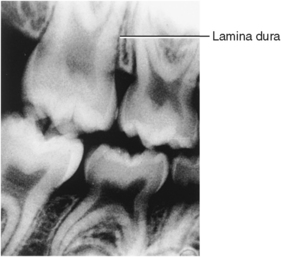
Fig. 12-6 Radiograph of alveolar bone illustrating lamina dura, the radiographically dense bone lining tooth sockets.
Not all alveolar bone proper appears as bundle bone because the bone lining the socket is constantly being remodeled for adaptation to the stresses of occlusal impact. Newly formed bone does not have perforating fibers (Fig. 12-7). Teeth are constantly moving (drifting) within their sockets, resulting in loss of some fibers. Other fibers continually form and initially attach to the bone’s surface and later become embedded.
Supporting Compact Bone
Supporting compact bone of the alveolar process is similar to haversian bone found elsewhere in the body (Fig. 12-8). Compact bone of the alveolar process extends over the lingual surface of the mandible and maxilla beside the tongue. Compact bone also covers the buccal surface of the mandible or maxilla adjacent to the lining of the cheek. Compact or cortical bone contains osteons with radiating lamellae accentuated by lacunae, which contain the osteocytes in living bone (Fig. 12-9). Haversian and Volkmann’s canals form a continuous system of nutrient canals that radiate throughout the bone. The haversian canals extend through the long axis of the bone, and Volkmann’s canals enter haversian canals at right angles. These canals form a nutrient network throughout bone. Bone cells or osteocytes are present in many of the lacunae and provide the maintenance and viability of the bone (see Fig. 12-9).
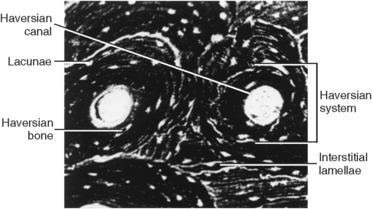
Fig. 12-8 Micrograph of alveolar bone showing a concentric haversian system, interstitial lamellae, and lacunae.
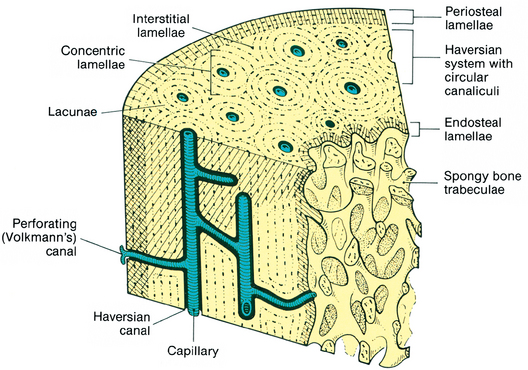
Fig. 12-9 Diagram of haversian systems of compact bone similar to compact bone throughout body. Periosteal lamellae cover the surface of the mandible and numerous haversian systems contain blood vessels interconnected by Volkmann’s canals. Lacunae containing osteocytes surround the haversian canals.
Supporting Cancellous Bone
The cancellous or spongy bone supporting the alveolar bone proper of the alveolar process is composed generally of heavy trabeculae or plates of bone with bone marrow spaces between them. Bone marrow contains blood-forming elements, osteogenic cells, and adipose tissues (see Fig. 12-7). The supporting bone of the maxilla in particular is filled with marrow tissue, which contains immature red blood cells and leukocytes, especially in the molar region posterior to the maxillary sinus. Bone marrow, found in bones throughout the body, is one of the largest organs in the body and represents approximately 4.5% of body weight.
CEMENTAL SUPPORT
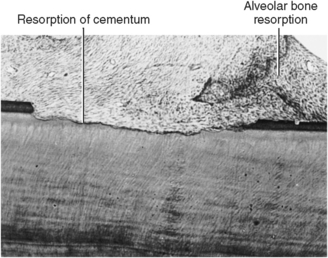
Cementum functions as a support by attaching to perforating fibers of the periodontal ligament at the root surface. The surface of cementum functions like bundle bone because the perforating fibers cover the entire surface of the roots (see Fig. 12-5). Some areas of the cementum are inactive, with the absence of fiber bundles, or they undergo surface resorption (Fig. 12-10). The collagen fiber bundles of cementum are smaller in size but more numerous than the bundles of alveolar bone proper (see Fig. 12-5). The principal fiber bundle system of the periodontal ligament is balanced in function, although distributed differently on the two surfaces.
Characteristic of the two surfaces, bone and cementum, are their ability to resorb and later to rebuild hard tissue. Cementum is more resistant to resorption than bone, hence the ability to move teeth through bone without the loss of the tooth surface. Some investigators claim that an autoinvasive factor in cementum contributes to this resistance. Other investigators believe that the absence of a blood supply in cementum, unlike bone, is important to this resistance. The distribution of penetrating fibers over the surface of the cementum could also relate to resorption. Cementum will resorb, as will dentin, in cases of stress caused by traumatic occlusion or of tooth movement resulting from drift or orthodontic treatment (Box 12-2). During exfoliation of primary teeth, root loss is considered a normal process. This process of normal physiologic root and cemental resorption is the result of permanent tooth eruption.
TOOTH MOVEMENT
The eruptive process involves major remodeling of the alveolar process to compensate for root growth and changes in positional relations of the primary and permanent teeth. Repositioning of teeth occurs, for example, during facial growth. Movement occurs in facial and buccal directions as the arches increase in dimension (Fig. 12-11). The height of the alveolus changes in relation to root growth as part of the facial growth process. Accommodation is made for increased dimension of the permanent teeth. In one situation, leeway space (Fig. 12-12) is created in the arches by the replacement of larger primary molars by smaller permanent premolars. This important situation helps compensate for the incisor liability factor, which is the replacement of the smaller primary incisors with larger permanent ones (Fig. 12-13). Part of this increase is compensated by the inclination of the permanent incisors (Fig. 12-13, B). Also important is mesial drift, a significant occurrence during the mixed dentition period. When the teeth are clenched during normal masticatory function, an anterior force is exerted on the teeth because most cusps are inclined anteriorly and their occlusal inclined planes therefore produce an anterior force. This is in part the result of proximal wear. Summation of these forces defines the principle of mesial drift of the teeth. The alveolar process compensates for tooth-related factors, such as increased arch size, as well as effects of occlusal function. The effect of tooth loss or hypereruption is mesial drift, which can result in disruption of normal occlusal function.
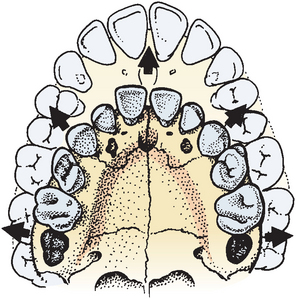
Fig. 12-11 Growth of the face results in migration of teeth laterally and anteriorly. This accompanies an increasing dimension of arch posteriorly as permanent molars develop and erupt.
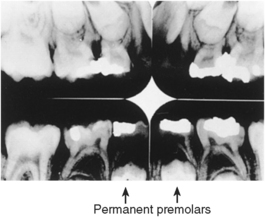
Fig. 12-12 Radiograph of permanent premolars replacing primary molars. A smaller premolar produces a leeway space in the arch.
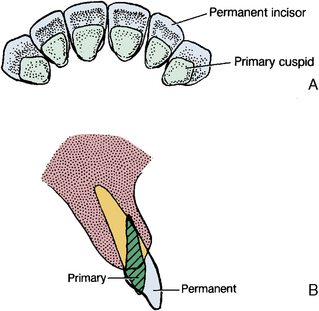
Fig. 12-13 A, Comparison of interdental spacing of primary and permanent incisor teeth. B, Inclination comparison of anterior primary and permanent teeth.
 Consider the Patient
Consider the PatientOrthodontic Movement
Tooth movement by orthodontics is possible only if bone resorption takes place in the direction in which the tooth is being moved. Such movement causes pressure on the surface of the alveolar bone in the direction of tooth movement. Tooth movement also causes tension on the periodontal ligament on the opposite surface of the root. These stresses cause activation of cells and changes in the vascular and neural tissue along the bone and cemental surfaces that are mediated through the periodontal ligament (Fig. 12-14). The alveolar bone and cementum show remarkable ability to be modified. As bone resorption occurs on one surface of the lamina dura, or bone lining the socket, the tooth is allowed to move in that direction and bone consequently forms on the opposite side of the socket. This stabilizes the tooth in a new position.
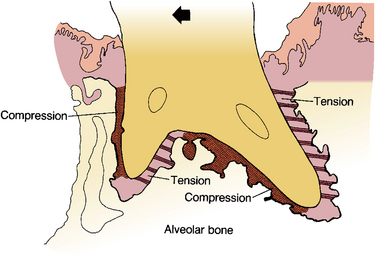
Fig. 12-14 Tooth movement to left with zones of compression along the advancing root surface and tension along the trailing root surface.
For example, if a tooth is tipped, as in Figure 12-15, A, several areas of the periodontium are compressed and several exhibit tension. The tipping movement is necessary to accomplish the change in occlusion desired. Pressure applied on a specific point on the tooth causes compression in a limited area between the root and the bone. However, a tooth may need to be moved by bodily movement, in which case the root is moved in the same direction, affecting the entire surface of the socket. Compression changes occur in the ligament along the advancing root surface, and tension changes occur in the ligament fibers, bone, and cementum along the opposite surface (Fig. 12-15, B). The situation is the same whether a single-rooted tooth or a multiple-rooted tooth is involved. In the multiple-rooted tooth, movement is complicated by the bifurcation bone, which has the additional bony surface related to pressure and tension (see Fig. 12-4).
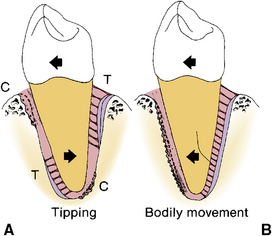
Fig. 12-15 A, Tipping of the tooth crown to the left causes the root to compress the ligament at the upper left and lower right. Tension then occurs at upper right and lower left (T). Bodily movement (B) of the crown and root to the left causes compression on the ligament (C), bone resorption along the entire surface of the advancing root, and formation of a tension surface of bone and cement on the right.
When compression is too great or too rapid, it causes hyalinization of the ligament. The vascularity is excluded, and the ligament appears colorless or “hyalinized.” Tooth movement is limited by the rate of resorption, meaning that cells that respond to the needs of compression and tension must be mobilized. On the compression surface, bone removal is requisite, so the osteoclasts must become organized. These cells originate from monocytes in the bloodstream. The osteoclasts organize rapidly, appearing within a few hours after tooth movement begins (Fig. 12-16).
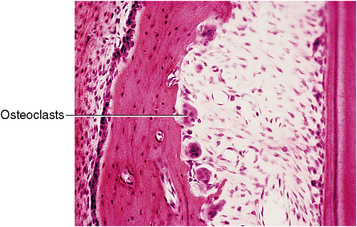
Fig. 12-16 Histology of compression zone of periodontal ligament. Osteoclasts remove bone to relieve compression.
Bone loss may occur on the bony surface of the socket, the cementum of the root surface, or both. This action may be reversed by deposition of bone or cementum in the area of resorption. The process of deposition in a resorption zone is known as an area of reversal. The area where deposition begins, in this site, is termed a reversal line.
On the tension side of the root, collagen fibers appear stretched and the cells become oriented in the direction of the tension (Fig. 12-17). As this occurs, the force of tension is transmitted into a biologic force characterized by the appearance of cells that are responsive to these needs. Fibroblasts, osteoclasts, and cementoblasts arise from mesenchymal cells in this area and begin to function. Many fibroblasts are present that function in collagen renewal. Osteoblasts, in turn, synthesize bone proteins necessary for producing osteoid. These osteoblasts also mineralize the bone matrix. As tension continues, bone develops along the alveolar bone and cemental surfaces around the stretched perforating fibers (Fig. 12-18).

Fig. 12-17 Histology of tension zone of periodontal ligament. Stretched fibers and a number of osteoblasts and cementoblasts are along surface of hard tissue.
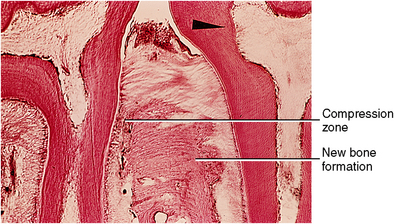
Fig. 12-18 Interproximal zone of two molar teeth. Both teeth moving to the right (arrowhead) cause compression of the ligament on the left and tension on the right. Bone formation appears along the alveolar bone on the right as a result.
Other types of tooth movement include rotation and a combination of tipping and rotation. In addition, intrusion or extrusion of a tooth may be necessary. Figure 12-19 illustrates a case of tooth movement over the long term. Fingerlike projections of bone follow the path of tooth movement. This bone growth is a result of tension. The principles of compression and tension are similar in all cases. The plasticity of the alveolar process is remarkable.
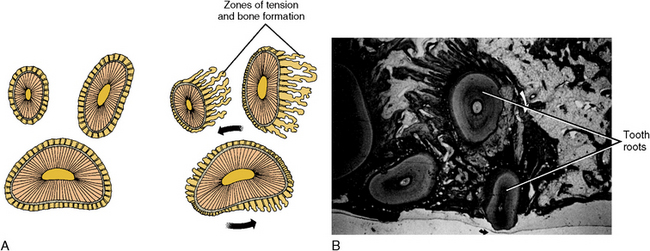
Fig. 12-19 Rotation of a maxillary molar. A, Large lower root moves less than upper two roots. Bone forms along trailing root surfaces, and resorption occurs on the advancing bony surface. B, Histology of rotation of a maxillary molar illustrating loss of bone along the advancing surfaces and bone formation along the tension (trailing) surfaces. In addition to rotation, the tooth is moving away from the zone of tension.
AGING OF ALVEOLAR BONE AND CEMENTUM
A comparison of young and old alveolar bone reveals a shift with age from dense bone and smooth-walled sockets to osteoporotic bone and sockets with rough, jagged walls. Aging brings bone loss with fewer fiber bundles inserted in the bone and cementum. Hard tissue then forms around the fibers in support of these bundles, thus creating a scalloped surface (Fig. 12-20). During aging, fewer viable cells are in the lacunae, and the marrow spaces become infiltrated with fat cells. Osteoporosis then becomes more apparent, and the support of the teeth is further diminished.
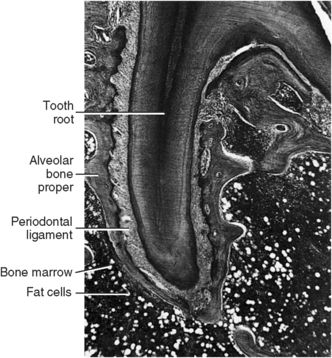
Fig. 12-20 Histology of aging alveolar bone illustrating scalloping of alveolar bone proper and infiltration of fat cells in marrow spaces.
EDENTULOUS JAWS
Several facts are known about the loss of teeth, although much remains to be learned about changes in the bony alveolar process after tooth loss. First, it is recognized that alveolar bone volume decreases. This is evident from the general loss of the alveolar process with tooth extraction. Next, some loss of the internal structure of the bone occurs, resulting in open spaces and fewer trabeculae in the cancellous supporting bone (Fig. 12-21). Osteoporosis may then become more evident. Little change occurs in the location of blood vessels, nerves, glands, and fatty zone in the aging edentulous jaws or in dense compact bone of the mandible beneath the alveolar bone (see Fig. 12-21).
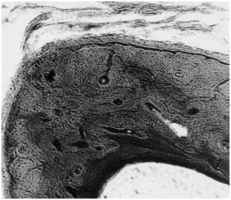
Fig. 12-21 Histology of an edentulous ridge after loss of tooth-bearing alveolar bone. The compact bone of the mandible is dense. This bone shows little evidence of osteoporosis.
Tooth movement can be monitored through radiographic examination, and changes in the interproximal bone density or dimension can also be evaluated. The orthodontist depends on this type of information to follow bone formation and resorption. Radiographs of the hard tissues are also useful in evaluating aging changes. Recognizing changes in the color of the gingival and alveolar mucosa is another valuable index of tissue health.
SELF-EVALUATION QUESTIONS
1. The cortical plates are described as what type of bone?
2. What is the origin of osteoclasts and osteoblasts, and how rapidly can they be mobilized?
3. Define mesial drift and describe some consequences of its occurrence.
4. What is a reversal line, and how is it evidenced?
5. Describe an aging periodontium, and list the features seen.
6. Describe the difference in tipping and bodily movement.
7. Supporting bone comprises what parts of the mandible?
8. Describe the cells that function in compression and tension.
9. What is the life span of the alveolar bone?
10. In what manner do masticatory stress forces placed on bundle bone differ from those placed on haversian bone?