Gait
BACKGROUND
Always examine the patient's gait. It is a coordinated action requiring integration of sensory and motor functions. The gait may be the only abnormality on examination, or it may lead you to seek appropriate clinical associations on the rest of the examination. The most commonly seen are: hemiplegic, parkinsonian, marche à petits pas, ataxic and unsteady gaits.
Romberg's test is conveniently performed after examining the gait. This is a simple test primarily of joint position sense.
WHAT TO DO AND WHAT YOU FIND
Ask the patient to walk.
Is the gait symmetrical?
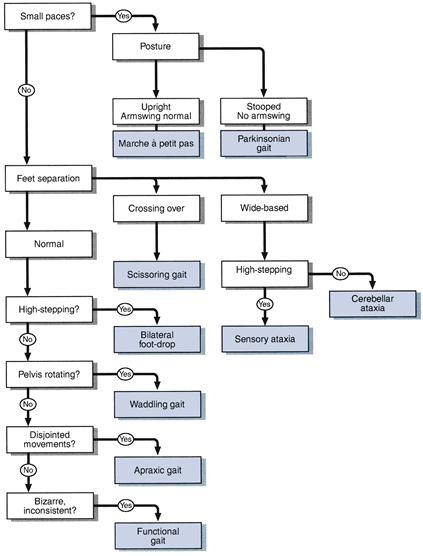
(Gaits can usually be divided into symmetrical and asymmetrical even though the symmetry is not perfect.)
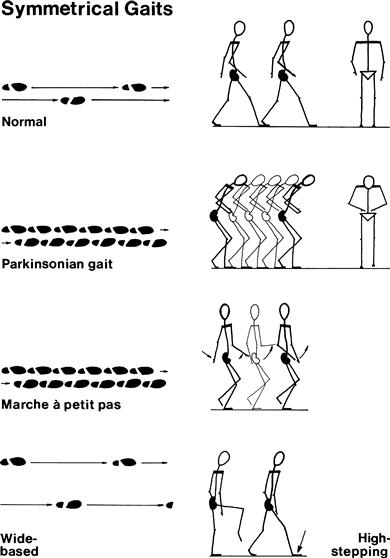
If symmetrical
Look at the size of paces:
If small paces:
Look at the posture and arm-swing:
FURTHER TESTS
Ask the patient to walk as if on a tight-rope (demonstrate).
Ask the patient to walk on his heels (demonstrate).
Ask the patient to walk on his toes (demonstrate).
WHAT IT MEANS
• Parkinsonian: indicates basal ganglion dysfunction. Common causes: Parkinson's disease, major tranquillisers.
• Marche à petits pas: indicates bilateral diffuse cortical dysfunction. Common cause: diffuse cerebrovascular disease ‘lacunar state’.
• Scissoring: indicates spastic paraparesis. Common causes: cerebral palsy, multiple sclerosis, cord compression.
• Sensory ataxia: indicates loss of joint position sense (Romberg's positive). Common causes: peripheral neuropathy, posterior column loss (see below).
• Cerebellar ataxia: veers towards side of lesion. Common causes: drugs (e.g. phenytoin), alcohol, multiple sclerosis, cerebrovascular disease.
• Waddling gait: indicates weak or ineffective proximal muscles. Common causes: proximal myopathies, bilateral congenital dislocation of the hip.
• Apraxic gait: indicates that cortical integration of the movement is abnormal, usually with frontal lobe pathology. Common causes: normal pressure hydrocephalus, cerebrovascular disease.
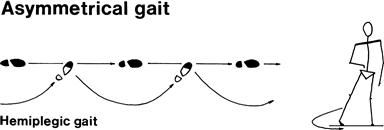
• Hemiplegic: unilateral upper motor neurone lesion. Common causes: stroke, multiple sclerosis.
• Foot drop: Common causes: unilateral—common peroneal palsy, pyramidal lesion, L5 radiculopathy; bilateral—peripheral neuropathy.
• Functional gait: variable, may be inconsistent with rest of examination, worse when watched. May be mistaken for the gait in chorea (especially Huntington's disease), which is shuffling, twitching and spasmodic and has associated findings on examination (see Chapter 24).
Romberg's test
What to do
Ask the patient to stand with his feet together.
Tell the patient you are ready to catch him if he falls (make sure you are).
If not:
Ask the patient to close his eyes.
What you find and what it means
• Stands with eyes open; stands with eyes closed = Romberg's test is negative: normal.
• Stands with eyes open; falls with eyes closed = Romberg's test is positive: loss of joint position sense. This can occur with:
– Posterior column lesion in the spinal cord: Common causes: cord compression (e.g. cervical spondylosis, tumour). Rarer causes: tabes dorsalis, vitamin B12 deficiency, degenerative spinal cord disease.
– Peripheral neuropathy: Common causes: see Chapter 20.
• Unable to stand with eyes open and feet together = severe unsteadiness. Common causes: cerebellar syndromes and both central and peripheral vestibular syndromes.
• Stands with eyes open; rocks backwards and forwards with eyes closed: suggests a cerebellar syndrome.