Abnormal Movements
BACKGROUND
Abnormal movements are best appreciated by seeing affected patients. If you are armed with the right vocabulary, most common abnormal movements can be described. However, many experts will describe the same movements in different ways—so journals about movement disorders come with video clips to illustrate the movements!
In most patients with movement disorder, the diagnosis depends on an accurate description of the clinical phenomenon.
There is frequently a considerable overlap between syndromes, and several types of abnormal movement are often seen in the same patient—for example, tremor and dystonia in a parkinsonian patient on treatment.
The anatomy of the basal ganglia is complicated and wiring diagrams illustrating the connections between the various structures become more complicated as more research is done. Neuro-anatomical correlations are of limited clinical value as most movement disorders are classified as syndromes rather than on anatomical grounds. Correlations of significance include unilateral parkinsonism due to lesions of contralateral substantia nigra and unilateral hemiballismus due to lesions of the contralateral subthalamic nucleus or its connections.
In evaluating movement disorders, there are three aspects to the examination:
– the abnormal positions maintained
– the additional movements seen.
– the abnormal phenomena that can be revealed using various manœuvres (e.g. rigidity on testing tone and the abnormal postures brought on by writing in writer's cramp).
– the inability to do things: for example, a slowness in initiating actions (bradykinesia).
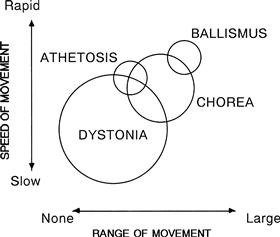
Terms used in movement disorders (Fig. 24.1)
Akathisia: motor restlessness where the patient constantly shifts, crossing and uncrossing his legs and walking on the spot.
Athetosis: slower, writhing, irregular movements predominantly in the hands and wrist (used less frequently now).
Chorea: non-rhythmical movements of a rapid, jerky nature which frequently appear pseudo-purposeful. They may be voluntarily controlled for a short time.
Dyskinesia: a term used to describe movements associated with neuroleptic drugs; particularly used to describe movements of mouth and face (orofacial dyskinesia).
Dystonia: co-contraction of agonist and antagonist which may lead to an intermittent or persistent maintenance of abnormal posture. Position maintained is usually at an extreme of extension or flexion.
Hemiballismus: violent and flinging movements which are irregular, affecting one side. There is no clear distinction from severe chorea.
Myoclonic jerk: an extremely brief contraction of a muscle group leading to involuntary purposeless jerk of the affected limb.
Negative myoclonus: irregular sudden brief loss of muscle tone when a limb is held outstretched. The most common form is asterixis.
Tic: a stereotyped and irresistible repetitive action, normally a repeated purposeful action.
WHAT TO DO
Look at the patient's face.
Look at the patient's head position.
Look at the arms and the legs.
Ask the patient to:
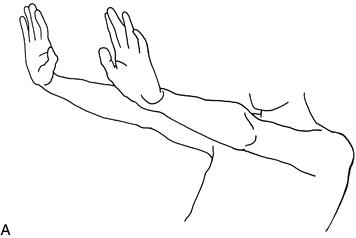
• hold his hands out in front of him with his wrists cocked back (Fig. 24.2A)
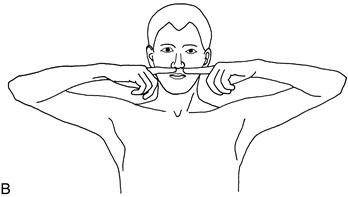
• lift his elbows out sideways and point his index fingers at one another in front of his nose (Fig. 24.2B)
• perform the finger–nose test (as in Chapter 23).
If there is a tremor, note the frequency, the degree of the excursion (fine, moderate, large) and the body parts affected. Look for a tongue tremor (see Chapter 13).
Test eye movements (Chapter 9).
Test tone (Chapter 16).
• When testing tone in one arm, it is sometimes useful to ask the patient to lift the other arm up and down.
Test fast repeating movements.
– bring thumb and index finger rapidly together (demonstrate)
– touch the thumb with each finger rapidly in turn (demonstrate)
– tap his toe as if listening to fast music.
Observe the speed of the movements and whether they break up; compare right with left.
Test gait (Chapter 4).
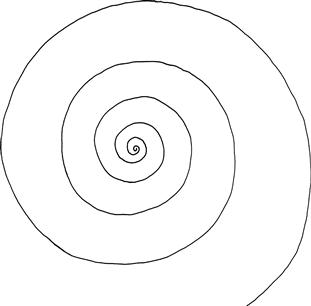
Test writing.
– draw an Archimedes spiral (Fig. 24.3).
Ask the patient to perform any manœuvre that he reports may trigger the abnormal movement.
WHAT YOU FIND
Face
Arms and legs
Positive phenomena
Tremor
• Present when limb (particularly hand) is at rest: rest tremor.
• Present when limb is maintained in a position (especially as in Fig. 24.2): postural tremor.
• Present during an action (e.g. finger–nose testing): action tremor.
• Present and increasing as the finger reaches its target: intention tremor.
 TIP
TIP
Commonly more than one type of tremor coexists.
Asterixis
• Irregular jerky movements of the hands, seen especially in the position illustrated in Figure 24.2. This is actually a sudden loss of tone—negative myoclonus.
Position
• Limb maintained, often only transiently, in abnormal position with contraction of both agonists and antagonists: dystonic posturing. Commonly the arm is abducted at the shoulder, extended at the elbow, and pronated to an extreme position with the fingers extended. The leg is usually extended at the hip and knee and inverted at the ankle with the toes flexed.
TIP
Try to put yourself into these positions to realise what they look like (and why patients find them uncomfortable).
Additional movements (as described above). Describe which part of the movements are seen to be affected:
Latent phenomena
On walking, the following may occur or increase:
Finger–nose testing may reveal:
and exacerbate:
Negative phenomena
• Rigidity: lead pipe or cogwheel.
• Bradykinesia: slowness in initiating movements.
• Reduced arm-swing on walking (see Chapter 4).
WHAT IT MEANS
Akinetic–rigid syndromes (parkinsonism) (common)
• Key features: rigidity, bradykinesia and tremor. Features include reduced facial expression (mask-like), rest tremor, stooped posture with reduced arm-swing and increased tremor on walking. Gait may be festinant (see Chapter 4). Bradykinesia on fast repeating movements and walking. Extrapyramidal dysarthria (see Chapter 2). There may be limitation of convergence.
• Common causes: Parkinson's disease, antipsychotic drugs, particularly the older agents (e.g. chlorpromazine, haloperidol).
• Rare causes: Steele–Richardson syndrome or progressive supranuclear palsy (PSP) (akinetic–rigid syndrome associated with progressive supranuclear palsy), multiple systems atrophy (akinetic–rigid syndrome associated with autonomic failure, pyramidal signs and cerebellar syndrome), Wilson's disease.
Tremors (common)
• Rest tremor: feature of akinetic rigid syndrome (see above).
• Postural and action tremor: Common causes: essential tremor (also called familial tremor if there is a family history), exaggerated physiological tremor (may be caused by hyperthyroidism, beta-agonists). Rarer causes: liver failure, renal failure, alcohol withdrawal.
• Intention tremor: indicates cerebellar disease (see Chapter 23).
Chorea (uncommon)
Common cause:
Rare causes:
Dystonia (uncommon)
Affects only one part of the body during a particular action: task-specific dystonia
Affects only one part of the body: focal dystonia
Affecting two or more adjacent parts of the body: segmental dystonia. For example:
Affects parts of the body that are not adjacent:
Common causes:
• Focal and segmental dystonia: idiopathic, antipsychotic drugs, treated Parkinson's disease on excessive therapy.
Rare cause: dystonia musculorum deformans.
Tic (uncommon)
Usually an isolated finding which may be associated with coprolalia (muttering of obscenities); then referred to as Gilles de la Tourette syndrome.
Myoclonic jerk (rare)
May be seen as part of other movement disorders where chorea or dystonia is predominant.
Associated with a number of metabolic encephalopathies, myoclonic epilepsies—seen in rare neurological diseases such as Creutzfeldt–Jakob disease and postanoxic encephalopathy.
Others
• Orofacial dyskinesia: usually a late reaction to major tranquilliser. May also occur as part of the syndromes listed under chorea.
• Akathisia: late reaction to major tranquilliser.
• Hemifacial spasm: compression of facial nerve by ectopic vessels.
• Facial myokymia: usually benign, possibly exacerbated by tiredness, caffeine. Rarely: indicative of brainstem lesion.
• Asterixis: occurs in metabolic encephalopathy, particularly in liver failure.