Motor System
Tone
BACKGROUND
Testing muscle tone is a very important indicator of the presence and site of pathology. It can be surprisingly difficult to evaluate.
WHAT TO DO
Ensure the patient is relaxed, or at least distracted by conversation. Repeat each movement at different speeds.
Arms
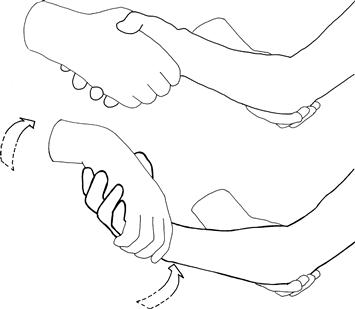
Take the hand as if to shake it and hold the forearm. First pronate and supinate the forearm. Then roll the hand round at the wrist (Fig. 16.1).
Hold the forearm and the elbow and move the arm through the full range of flexion and extension at the elbow.
Legs
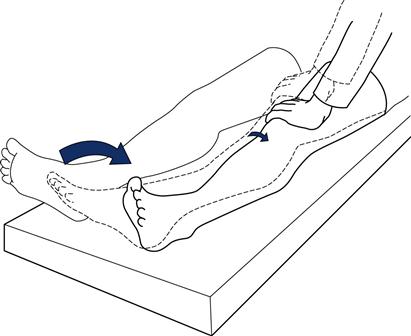
Tone at the hip
The patient is lying with straight legs. Roll the knee from side to side (Fig. 16.2).
WHAT YOU FIND
• Normal: slight resistance through whole range of movements. Heel will lift minimally off the bed.
• Decreased tone: loss of resistance through movement. Heel does not lift off the bed when the knee is lifted quickly. Marked loss of tone = flaccid.
– Resistance increases suddenly (‘the catch’); the heel easily leaves the bed when the knee is lifted quickly: spasticity.
– Increased through whole range, as if bending a lead pipe: lead pipe rigidity. Regular intermittent break in tone through whole range: cogwheel rigidity.
– Patient apparently opposes your attempts to move his limb: Gegenhalten or paratonia.
Special situations
• Myotonia: slow relaxation following action. Demonstrated by asking the patient to make a fist and then release it suddenly. In myotonia the hand will only unfold slowly.
• Dystonia: patient maintains posture at extreme of movement with contraction of agonist and antagonist (see Chapter 24).
• Percussion myotonia: may be demonstrated when a muscle dimples following percussion with a patella hammer. Most commonly sought in abductor pollicis brevis and the tongue.
WHAT IT MEANS
• Flaccidity or reduced tone. Common causes: lower motor neurone or cerebellar lesion. Rare causes: myopathies, ‘spinal shock’ (e.g. early after a stroke), chorea.
• Spasticity: upper motor lesion. This usually takes some time to develop.
• Rigidity and cogwheel rigidity: extrapyramidal syndromes. Common causes: Parkinson's disease, phenothiazines.
• Gegenhalten or paratonia: bilateral frontal lobe damage. Common causes: cerebrovascular disease, dementia.
• Myotonia (rare). Causes: myotonic dystrophy (associated with frontal balding, ptosis, cataracts and cardiac conduction defects) and myotonia congenita. Percussion myotonia may be found in both conditions.