Thorax
Many structures of the chest are in constant motion. Although physiologic motion can make imaging difficult, a thorough knowledge of chest anatomy and physiology can improve diagnostic imaging of this area. (Figure 6.1) This chapter demonstrates sectional anatomy of the following structures:
BONY THORAX
The bony thorax functions to protect the organs of the thorax and to aid in respiration. It consists of the thoracic vertebrae, sternum, ribs, and costal cartilages (Figure 6.2). The 12 thoracic vertebrae make up the posterior boundary of the thoracic cage. The anterior boundary is created by the sternum, located midline. The sternum has three components: manubrium, body, and xiphoid process (Figures 6.3 and 6.4). The triangular-shaped manubrium is the most superior portion and articulates with the first two pairs of ribs and the clavicles. It articulates with the clavicle at the clavicular notch to form the sternoclavicular joints (Figure 6.5). A common landmark, the jugular notch, is located on the superior border of the manubrium at approximately the level of T2-T3. The manubrium and body of the sternum come together at an angle to form a ridge known as the sternal angle, which is located at approximately the level of T4-T5. The slender body of the sternum has several indentations along its sides where it articulates with the cartilage of the third through seventh ribs (Figures 6.6 and 6.7). The small xiphoid process is located on the inferior border of the sternum and is a site for muscle attachments (Figure 6.8).
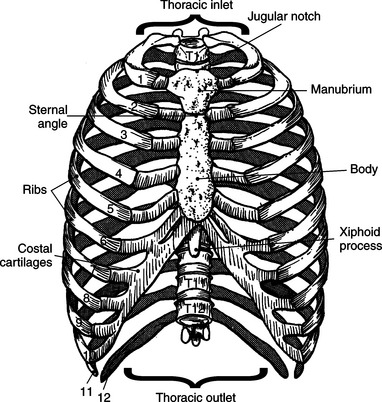

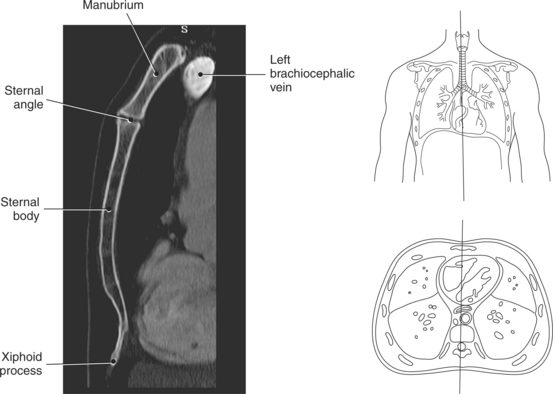
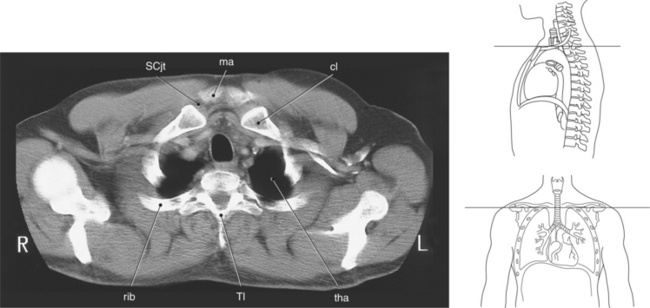
Figure 6.5 Axial CT scan of thoracic inlet.
Key: ma, Manubrium; sta, sternal angle; b, body; tho, thoracic outlet; SCjt, sternoclavicular joint; cl, clavicle; tha, thoracic aperture; T1, first thoracic vertebra; rib, first rib.
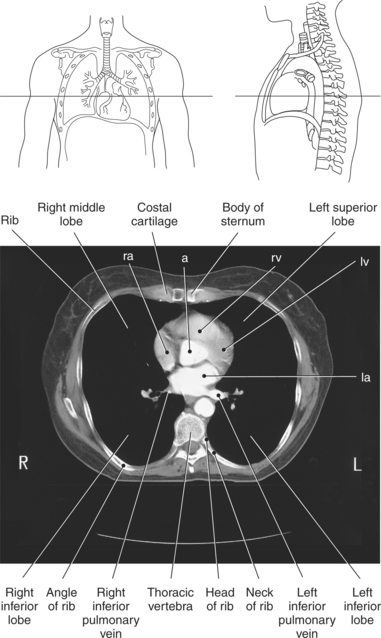
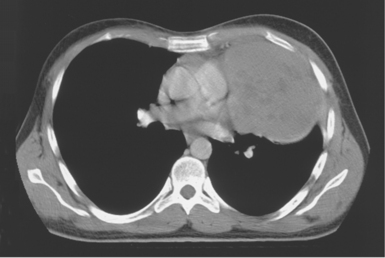
Figure 6.6 Axial CT scan of sternum.
Key: ra, Right atrium; a, aorta; rv, right ventricle; la, left atrium; xi, xiphoid process.
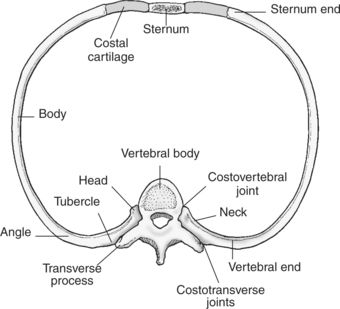
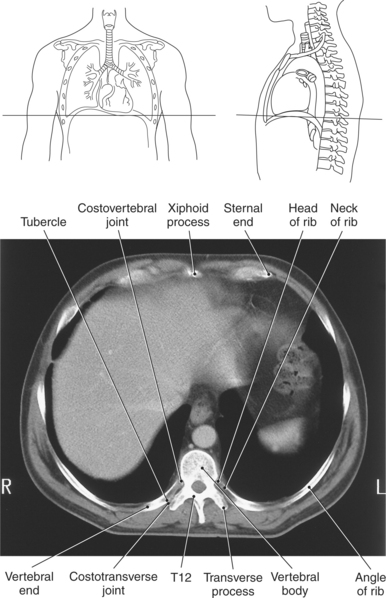
Forming the lateral borders of the thoracic cage are the 12 pairs of ribs. The spaces between adjacent ribs are referred to as the intercostal spaces. All 12 pairs of ribs articulate posteriorly with the thoracic spine. The ribs consist of a head, neck, tubercle, and body (Figures 6.7 and 6.8). The facets of the head of the rib articulate with the vertebral bodies at the costovertebral joints, whereas the facets of the tubercles articulate with the transverse processes of the vertebrae to form the costotransverse joints. The first 7 pairs of ribs (true ribs) articulate anteriorly with the sternum by costal cartilage. The lower 5 pairs of ribs are considered false ribs because they do not attach directly to the sternum. The costal cartilage of the eighth, ninth, and tenth ribs attach to the costal cartilage of the seventh rib. The eleventh and twelfth ribs are considered floating because they attach only to the thoracic vertebrae and contain no neck or tubercle, just vertebral and sternal ends (Figure 6.2).
Thoracic Apertures
There are two openings, or apertures, associated with the bony thorax. The superior aperture is formed by the first thoracic vertebra, first pair of ribs and their costal cartilages, and manubrium. This aperture, known as the thoracic inlet, allows for the passage of nerves, vessels, and viscera from the neck into the thoracic cavity. The inferior aperture is much larger and is made up of the twelfth thoracic vertebra, twelfth pair of ribs and costal margins, and xiphoid sternal junction. This aperture is known as the thoracic outlet (Figures 6.2, 6.5, and 6.8).
LUNGS
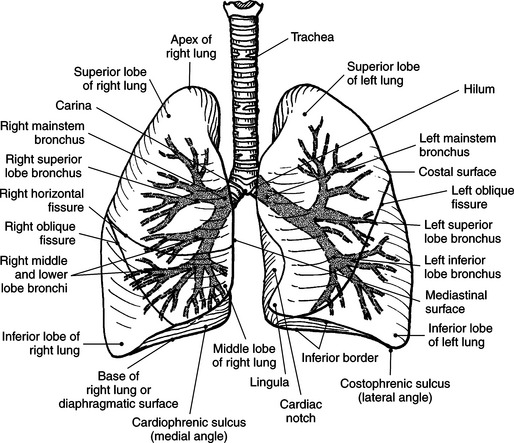
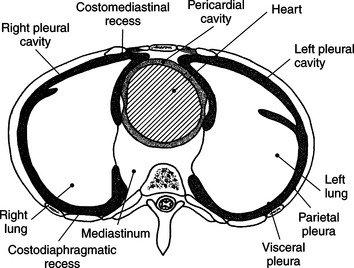
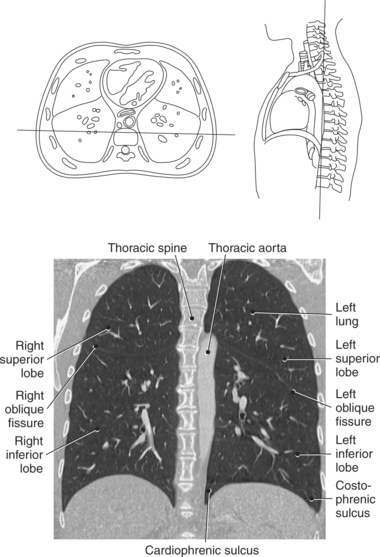
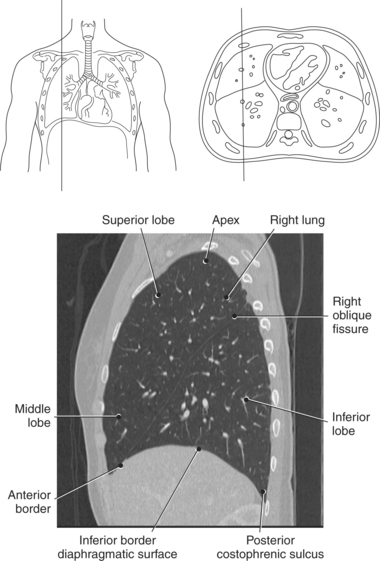
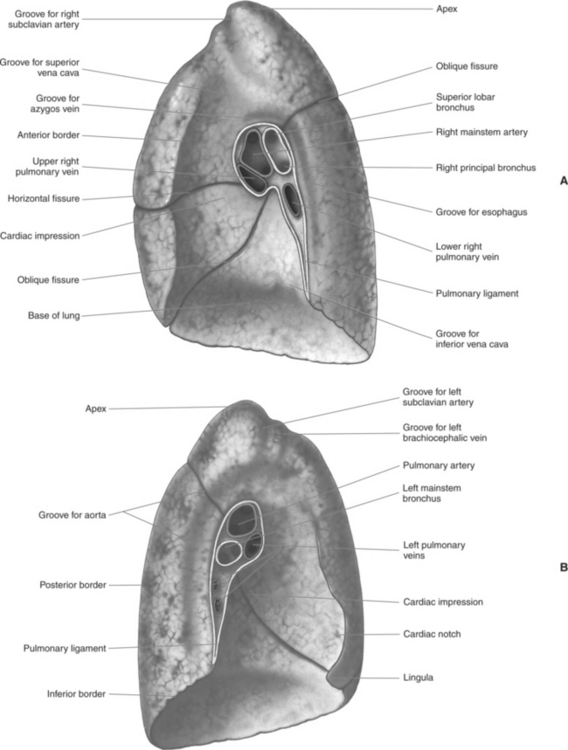
The lungs are the organs of respiration, where gaseous exchange occurs between the respiratory air and blood. They are composed of a spongelike material, the parenchyma, and surrounded by a layer of serous membrane. The large conical-shaped lungs extend up to or slightly above the level of the first rib at their apex and down to the dome of the diaphragm at their wide concave-shaped bases or diaphragmatic surfaces (Figure 6.9). Each lung has a mediastinal or medial surface that is apposed to the mediastinum, and a costal surface that is apposed to the inner surface of the rib cage. Each lung also has an inferior, anterior, and posterior border. The inferior border extends into the costodiaphragmatic recess of the pleural cavity, and the anterior border of each lung extends into the costomediastinal recess of the pleural cavity (Figure 6.10). Two prominent angles can be identified at the medial and lateral edges of the lung bases. The medial angle is termed the cardiophrenic sulcus, and the lateral angle is termed the costophrenic sulcus (Figure 6.11 and 6.12). The lungs are divided into lobes by fissures that are lined by pleura and may extend as far as the hilum (Figure 6.13). The right lung has three lobes (superior [upper], middle, and inferior [lower]), whereas the left lung has just superior (upper) and inferior (lower) lobes (Figures 6.6 and 6.11 through 6.13). The inferior lobe of the right lung is separated from the middle and superior lobes by the oblique fissure, termed oblique because of its posterosuperior to anteroinferior course. Separating the middle lobe from the superior lobe is the horizontal fissure (Figures 6.9 and 6.14, A). An oblique fissure also separates the superior and inferior lobes of the left lung (Figure 6.11). The left lung has a large notch on the medial surface of its superior lobe called the cardiac notch and a tonguelike projection off its inferoanterior surface termed the lingula. Each lung has an opening on the medial surface termed the hilum (Figures 6.14 through 6.16). This opening acts as a passage for mainstem bronchi, blood vessels, lymph vessels, and nerves to enter or leave the lung and is commonly referred to as the root of the lung.
PLEURAL CAVITIES
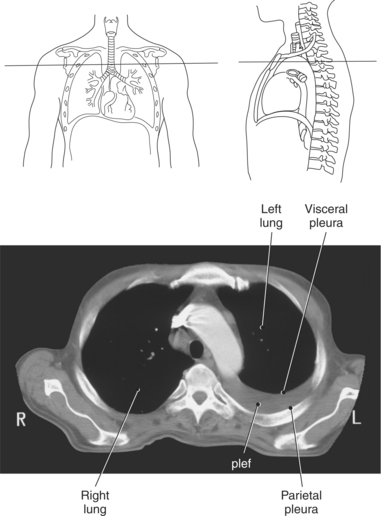
Each lung lies within a single pleural cavity that is lined by a serous membrane, or pleura. The pleura can be divided into two layers. The parietal pleura, the outer layer, is continuous with the thoracic wall and diaphragm and moves with these structures during respiration. The visceral pleura is the inner layer that closely covers the outer surface of the lung and continues into the fissures to cover the individual lobes as well. Both membranes secrete a small amount of pleural fluid that provides lubrication between the surfaces during breathing. Deep pockets or recesses of the pleural cavities are the costomediastinal and costodiaphragmatic recesses. The costomediastinal recesses are located at the point where the mediastinum and costal cartilages meet anteriorly, and the costodiaphragmatic recesses are located where the diaphragm and ribs connect inferiorly. These recesses serve as expansions to provide additional pleural space where parts of the lung can glide during inspiration (Figure 6.10 and 6.17).
BRONCHI
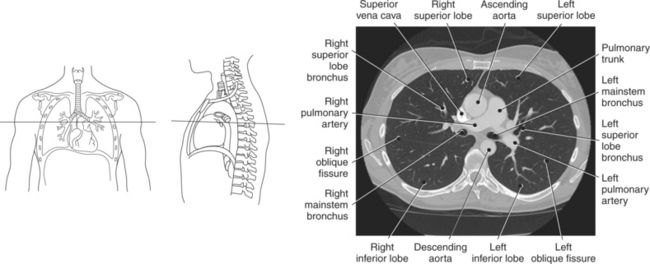
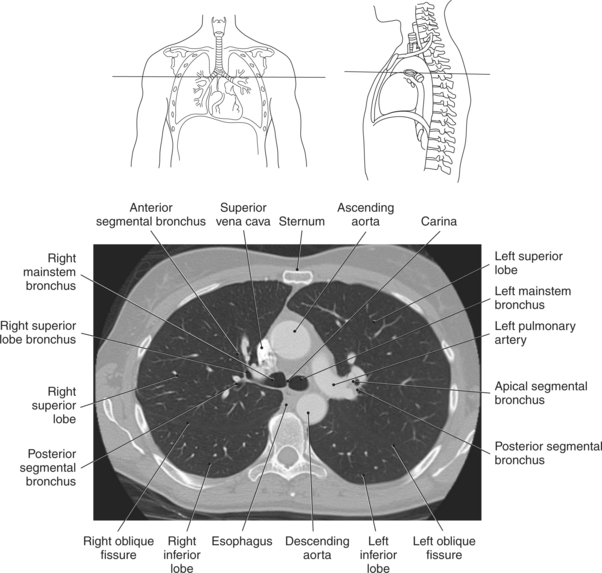
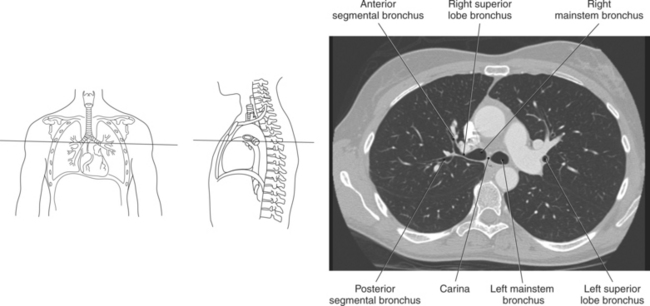
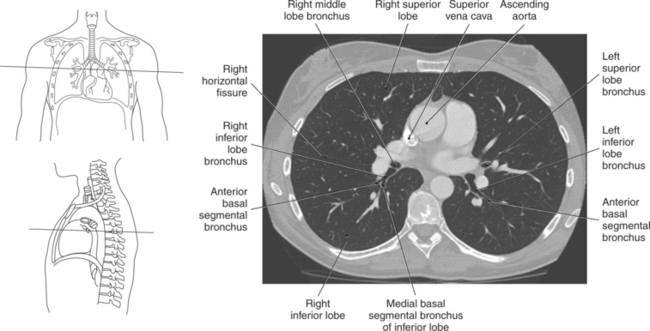
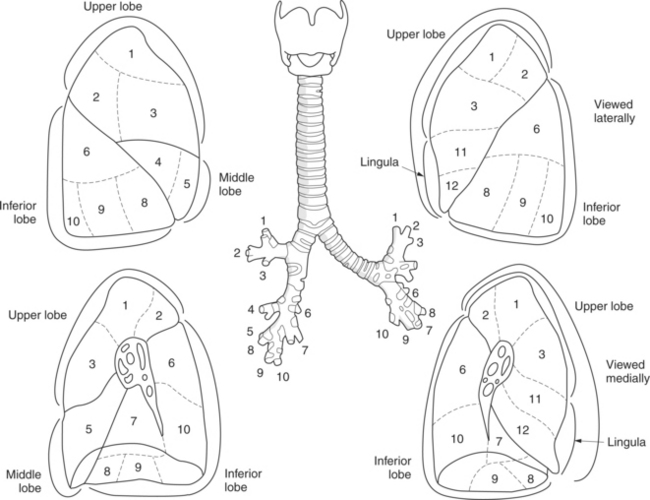
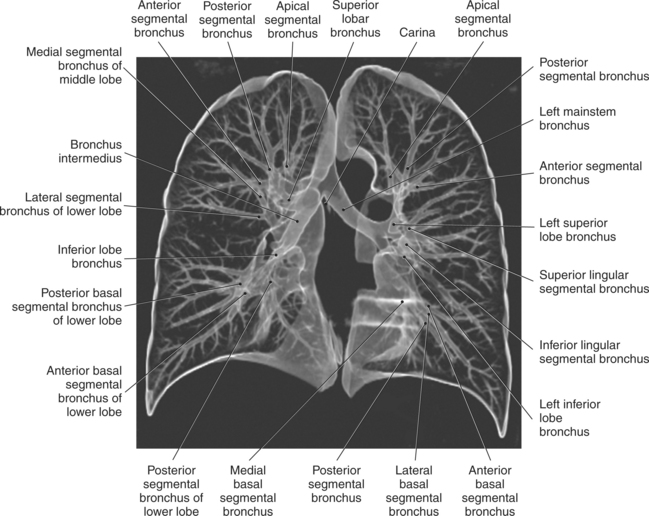
The trachea bifurcates into the left and right mainstem (primary) bronchi at approximately the level of T5. This location is commonly referred to as the carina (Figure 6.9). The right main bronchus is wider, shorter, and more vertical in orientation then the left. At the hilum the mainstem bronchi enter the lung and divide into secondary or lobar bronchi. Secondary bronchi correspond to the lobes of the lungs, thus with three divisions on the right (superior, middle, inferior) and two divisions on the left (superior and inferior) (Figure 6.9, and 6.18 through 6.20). There is further division of the secondary bronchi into tertiary or segmental bronchi that extend into each segment of the lobes (bronchopulmonary segments) (Figure 6.21 and Table 6.1). There are typically 10 segments within each lung. Each bronchopulmonary segment is functionally independent and can be individually removed surgically. The bronchial tree continues to divide many times into smaller bronchi, then into bronchioles (Figure 6.22). Each bronchiole continues to divide until it reaches the terminal end as alveoli, which are the functional units of the respiratory system. Gaseous exchange between alveolar air and capillary blood occurs through the wall of the alveoli.
TABLE 6-1
| LOBE | RIGHT LUNG | LEFT LUNG |
| Superior lobe | Apical segment Posterior segment Anterior segment |
Apical segment Posterior segment Anterior segment Superior lingular segment Inferior lingular segment |
| Middle lobe | Lateral segment Medial segment |
|
| Inferior lobe | Superior segment Medial basal segment Anterior basal segment Lateral basal segment Posterior basal segment |
Superior (apical) segment Medial basal segment Anterior basal segment Lateral basal segment Posterior basal segment |
MEDIASTINUM
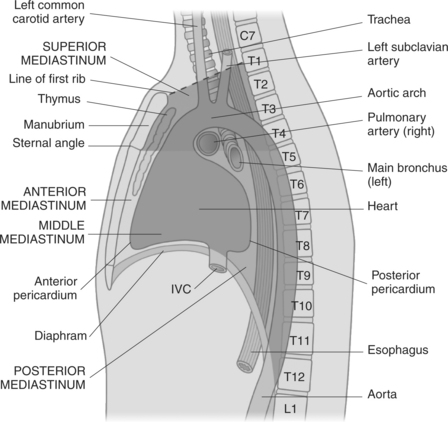
The mediastinum is the midline region of the thoracic cavity located between the two pleural cavities of the lungs. It extends from the superior thoracic aperture to the diaphragm and is bordered anteriorly by the sternum and posteriorly by thoracic vertebrae. The mediastinum can be subdivided into compartments for descriptive purposes. The superior and inferior compartments are made by drawing an imaginary line between the sternal angle and the intervertebral disk of T4-T5. The superior compartment constitutes the upper portion of the mediastinum. It contains the thymus gland and acts as a conduit for structures as they enter and leave the thoracic cavity. The inferior compartment can be further divided into anterior, middle, and posterior compartments (Figure 6.23). The anterior compartment is located anterior to the pericardial sac and posterior to the sternum. The middle compartment is the area that contains the pericardial sac, heart, and roots of the great vessels. The posterior compartment is the area lying posterior to the pericardium and anterior to the inferior eight thoracic vertebrae. Structures located within the mediastinum include the thymus gland, trachea, esophagus, lymph nodes, thoracic duct, heart and great vessels, and various nerves.
Thymus Gland
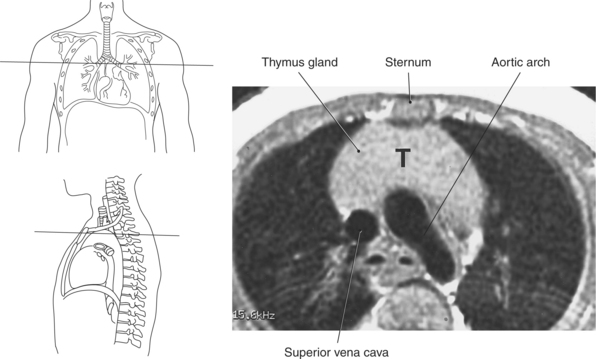
The thymus gland is a triangular-shaped bilobed gland of lymph tissue, located in the superior portion of the mediastinum just behind the manubrium (Figures 6.24 through 6.26). It is considered the primary lymphatic organ responsible for the development of cellular immunity. T-lymphocytes within the blood reach the thymus as stem cells, where they are stored while they undergo T-cell differentiation and maturation. The thymus gland produces a hormone, thymosin, that is responsible for the development and maturation of lymphocytes. The thymus gland reaches its maximum size during puberty and gradually diminishes in size in the adult.
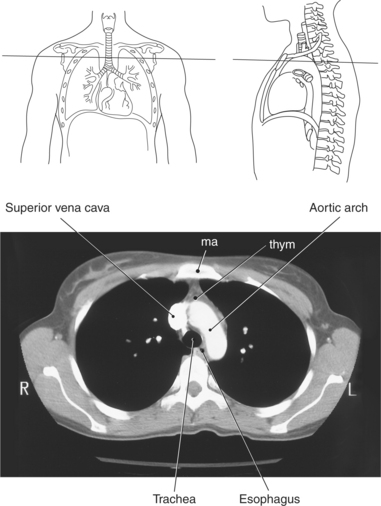
Trachea and Esophagus
Throughout its course in the mediastinum, the trachea runs anterior to the esophagus. In cross section, the trachea appears as a round air-filled structure to the point at which it bifurcates at the carina (Figures 6.9 and 6.18). The esophagus appears as an oval-shaped structure that descends through the diaphragm to enter the stomach at the gastroesophageal junction (Figures 6.27 and 6.28).
LYMPHATIC SYSTEM
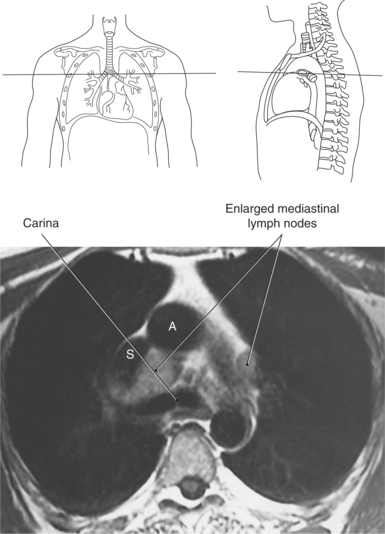
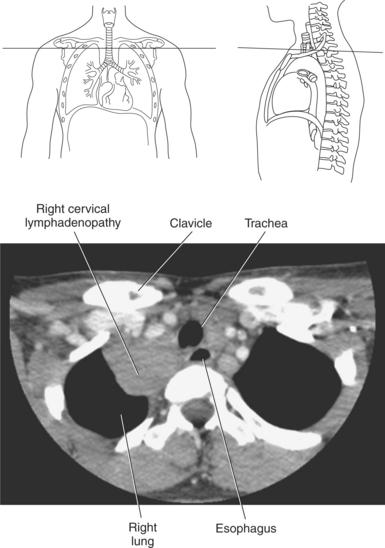
Lymph nodes in the mediastinum are generally clustered around the great vessels, esophagus, bronchi, and carina. Mediastinal lymph nodes are classified according to their location and are grouped into 14 regional nodal stations for use in lung cancer staging (Figure 6.29 and Table 6.2). Lymph vessels and nodes can be difficult to visualize in cross section unless they are enlarged as a result of an abnormality (Figures 6.30 and 6.31).
TABLE 6-2
Regional Nodal Stations for Staging Lung Cancer
| NODES | LOCATION |
| N2 Nodes | |
| Superior Mediastinal Nodes | |
| 2R Right upper paratracheal nodes | Between intersection of caudal margin of innominate artery with trachea and the apex of the lung (suprainnominate nodes) |
| 2L Upper left paratracheal nodes | Between top of aortic arch and apex of the lung (supraaortic nodes) |
| 4R Right lower paratracheal nodes | Between intersection of caudal margin of innominate artery with trachea and cephalic border of azygos vein |
| 4L Left lower paratracheal nodes | Between top of aortic arch and carinamedial to ligamentum arteriosum |
| 10R Right tracheobronchial angle nodes | From cephalic border of azygos vein to origin of right upper lobe bronchus |
| 10L Left tracheobronchial angle nodes | Between carina and left upper lobe—medial to ligamentum arteriosum |
| Aortic Nodes | |
| 5 Aortopulmonary nodes | Subaortic and paraaortic nodes lateral to the ligamentum arteriosumproximal to first branch of left pulmonary artery |
| 6 Anterior mediastinal nodes | Anterior to ligamentum arteriosum |
| Inferior Mediastinal Nodes | |
| 7 Subcarinal nodes | Caudal to the carina |
| 8 Paraesophageal nodes | Dorsal to the posterior wall of the trachea and to the right or left of the midline of the esophagus |
| 9 Pulmonary ligament nodes | Nodes within the pulmonary ligament |
| N3 Nodes | |
| 13 Interlobar nodes | |
| 12 Lobar nodes | |
| 13 Segmental nodes | |
| 14 Subsegmental nodes |
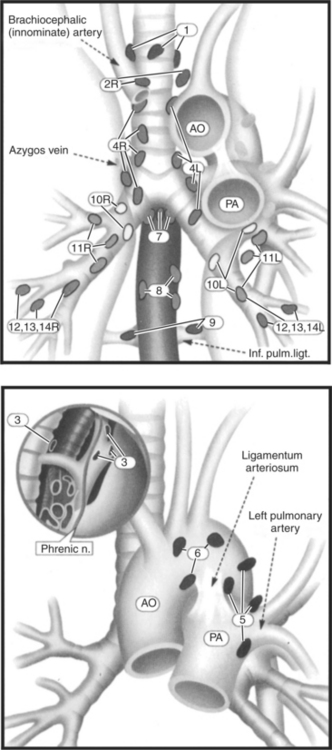
Figure 6.29 Coronal view with distribution of mediastinal lymph nodes.
L, Left; R, right; 1, highest mediastinal nodes; 2, upper paratracheal nodes; 3, prevascular and retrotracheal nodes; 4, lower paratracheal (including azygos) nodes; 5, subaortic nodes; 6, paraaortic nodes; 7, subcarinal; 8, paraesophageal nodes; 9, pulmonary ligament; 10, hilar nodes; 11, interlobar nodes; 12, lobar nodes; 13, segmental nodes; 14, segmental nodes.
Key: AO, aorta; PA, pulmonary artery; Inf. pulm. ligt., inferior pulmonary ligament; Phrenic n., phrenic nerve; S, superior vena cava; A, aorta.
Lymph Vessels
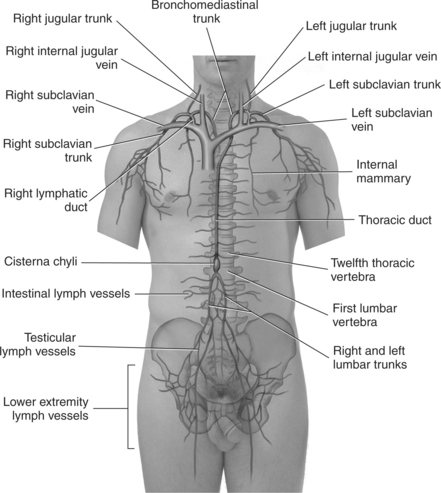
The lymphatic system consists of a network of lymphatic vessels that carry lymph fluid (excess interstitial fluid) away from the tissue and into the venous circulation. Small lymph vessels (capillaries) can be found accompanying the arteries and veins throughout the body. The tiny lymph vessels increase in size until they reach their terminal collecting vessels; the thoracic duct and the right lymphatic duct. The thoracic duct is the main vessel of the lymph system, draining all of the lymph fluid from tissues below the diaphragm and from the left side of the body above the diaphragm. It begins inferior to the diaphragm at the level of L2 and passes from the abdominal cavity into the thorax through the aortic hiatus of the diaphragm. It ascends the thorax, between the azygos vein and the descending aorta, and empties into the left subclavian vein at the level of the clavicle. The smaller right lymphatic duct collects lymph from the right upper side of the body and is formed by the merging of various lymphatic trunks near the right clavicle. This duct empties into the right subclavian vein (Figure 6.32).
HEART AND VASCULATURE
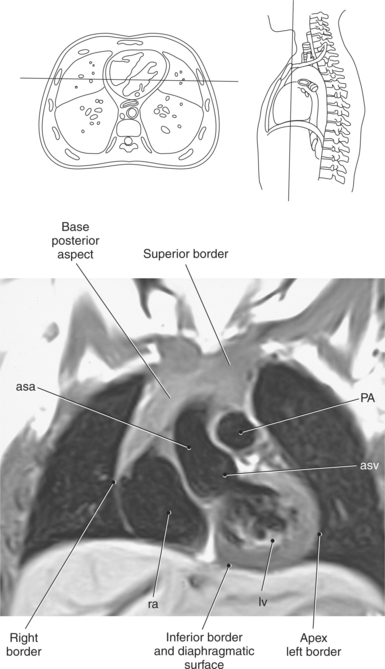
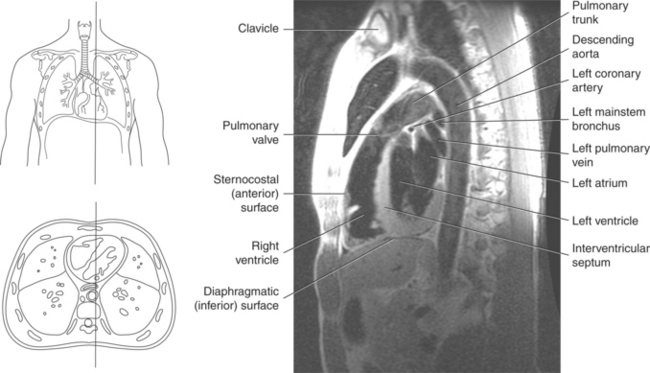
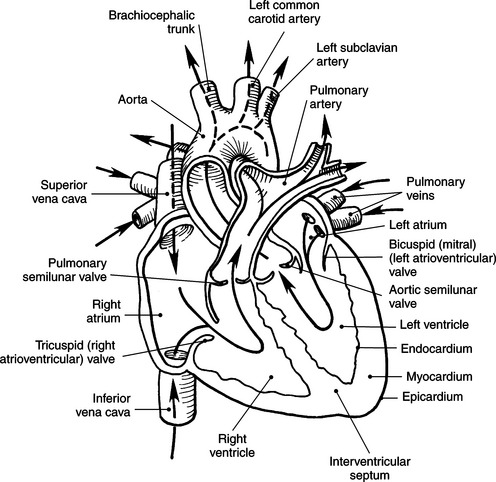
The heart is a hollow, four-chambered muscular organ located within the middle mediastinum. It is approximately the size of a large clenched fist and is situated obliquely in the chest with one third of its mass lying to the right of the median plane and two thirds to the left. The heart can be described as being roughly trapezoid shaped (Figure 6.33). The superficial relationships of the heart include the base, apex, three surfaces (sternocostal, diaphragmatic, pulmonary), and four borders (right, inferior, left, and superior). The broad base (posterior aspect) is the most superior and posterior portion of the heart. It is formed by both atria, primarily the left atrium, and gives rise to the great vessels. The apex is formed by the left ventricle and points inferiorly, anteriorly, and to the left. It is located at the level of the fifth intercostal space, just medial to the midclavicular line. The sternocostal (anterior surface) is formed primarily by the right atrium and right ventricle with a small contribution from the left ventricle. The diaphragmatic (inferior surface) rests on the central tendon of the diaphragm and is formed by both ventricles and a small portion of the right atrium. The pulmonary (left surface) is formed mainly by the left ventricle and fills the cardiac notch of the left lung. The borders of the heart represent the external surfaces of the cardiovascular silhouette in radiographic profile. The borders include the right border, formed by the right atrium and located between the superior and inferior venae cavae; the left border, formed by the apex of the heart or the left ventricle; the superior border, formed by the right and left atria; and the inferior border, which is formed primarily by the right ventricle with a small contribution from the left ventricle (Figures 6.33 through 6.35).
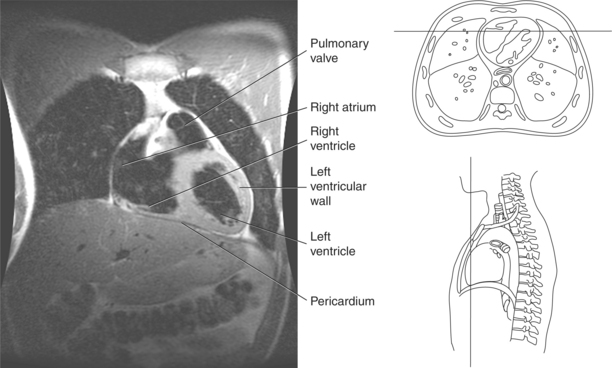
Pericardium
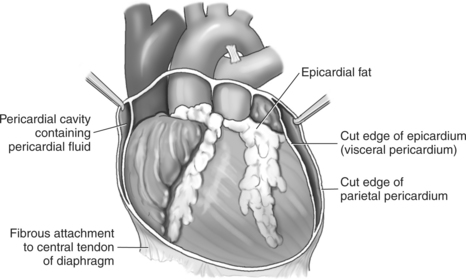
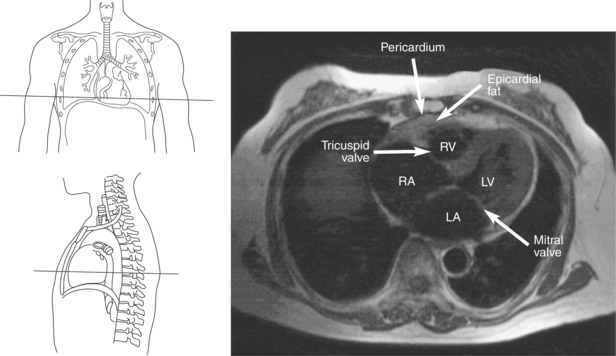
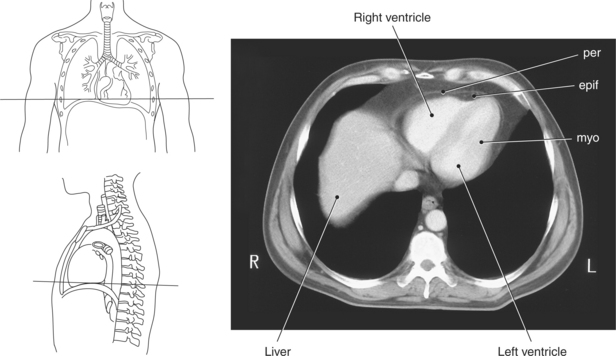
The heart is enclosed in a pericardial sac that surrounds the heart and the proximal portions of the great vessels entering and leaving the heart. The fibrous pericardium is attached to the central tendon of the diaphragm and is pierced by the inferior vena cava. The inner surface of the fibrous pericardium consists of a double-layered serous membrane termed the serous pericardium. The serous pericardial layers are the parietal layer that lines the inner surface of the fibrous pericardium and the visceral layer (epicardium) that covers the outer surface of the heart and the roots of the great vessels. Located between the two layers is a potential space (pericardial cavity) containing a thin film of serous fluid that acts as a lubricant to reduce friction to the tissues caused by heart movement. Located between the pericardium and the heart wall is a layer of epicardial fat that is typically more prominent near the venous inflow and arterial outflow of the heart (Figures 6.36 through 6.38).
Heart Wall
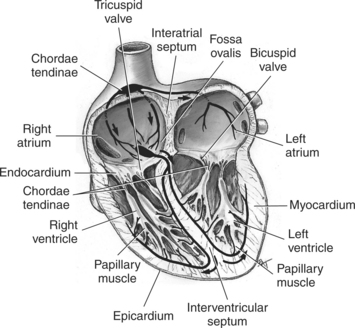
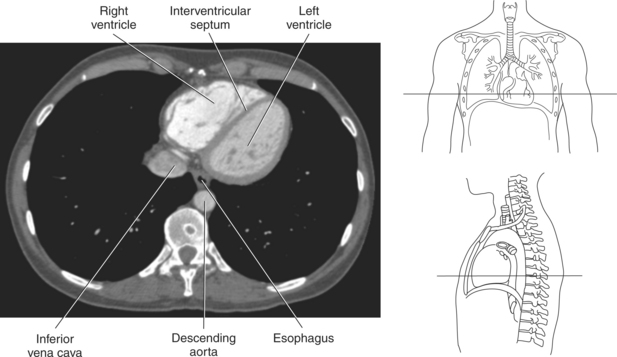
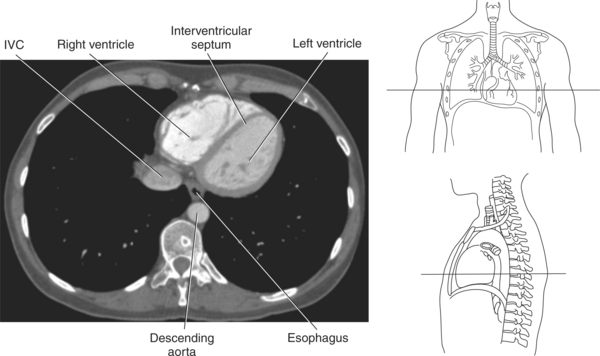
The walls of the heart consist of three layers: (1) epicardium, the thin outer layer that is in contact with the pericardium; (2) myocardium, the thick middle layer consisting of strong cardiac muscle; and (3) endocardium, the thin, endothelial layer lining the inner surface. The endothelial layer also lines the valves of the heart and is continuous with the inner lining of the blood vessels. The heart is divided into four chambers: the right and left atria and the right and left ventricles. The two superior collecting chambers called atria are divided by the interatrial septum. During embryonic development an oval opening exists within the interatrial septum called the foramen ovale. This opening allows blood flow between the right and left atria during fetal lung development. At birth, the foramen ovale closes, leaving a small depression in the septal wall called the fossa ovalis in the adult heart. The two inferior pumping chambers called ventricles are divided by the interventricular septum (Figure 6.39).
Chambers
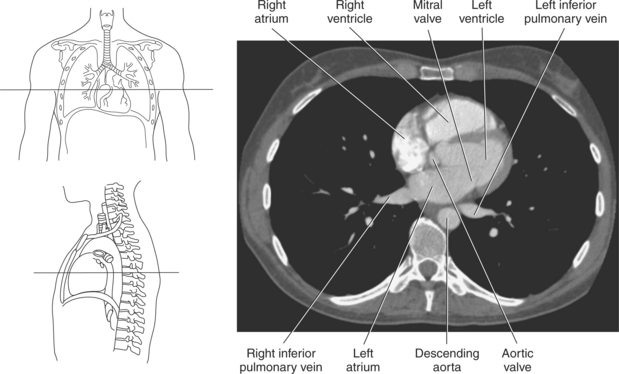
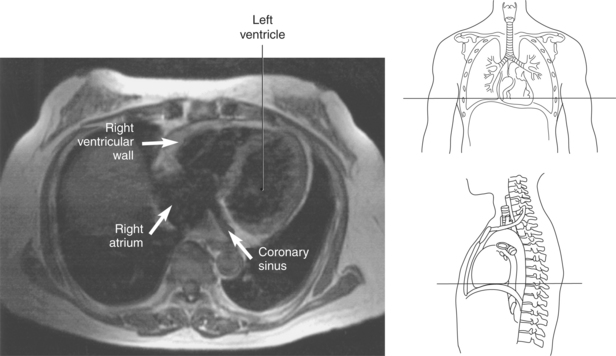
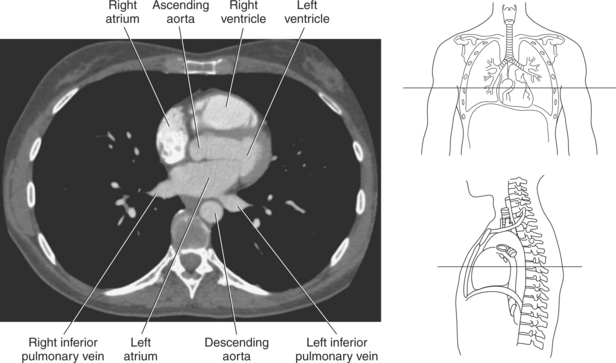
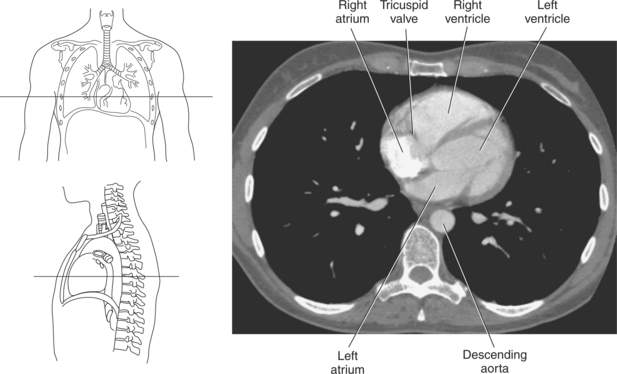
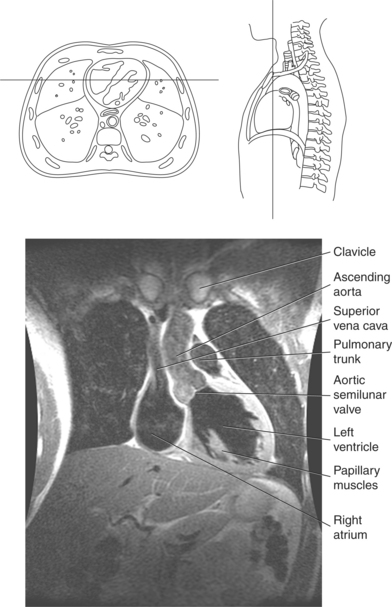
The right atrium forms the right border of the heart and receives deoxygenated blood from the body via the superior and inferior venae cavae and from the coronary sinus and cardiac veins that drain the myocardium. A small muscular embryonic appendage, the right auricle, projects upward and toward the left from the right atrium, covering the root of the aorta (Figure 6.40). The right ventricle lies on the diaphragm and comprises the largest portion of the anterior surface of the heart. It receives deoxygenated blood from the right atrium and forces it into the pulmonary trunk for conveyance to the lungs. Projecting off the inferior surface of the ventricular walls are conical-shaped projections of cardiac muscle called papillary muscles that anchor the cusps of the tricuspid valve to the right ventricle (Figure 6.39). The left atrium lies posterior to the right atrium and is the most posterior surface of the heart. It also has an embryonic appendage, the left auricle, that projects to the left of the pulmonary trunk over the superior surface of the heart. The left atrium receives oxygenated blood directly from the lungs via the four pulmonary veins (two on each side). The left ventricle forms the apex, left border, and most of the inferior surface of the heart. It receives oxygenated blood from the left atrium and pumps it into the aorta for distribution throughout the systemic circuit. The myocardium of the left ventricle is normally three times thicker than that of the right ventricle, reflecting the force necessary to pump blood to the distant sites of the systemic circulation (Figures 6.41 through 6.52). Two papillary muscles project from the ventricular walls to anchor the bicuspid valve to the ventricle (Figures 6.39 and 6.47).
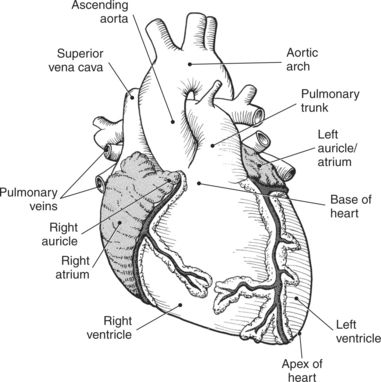
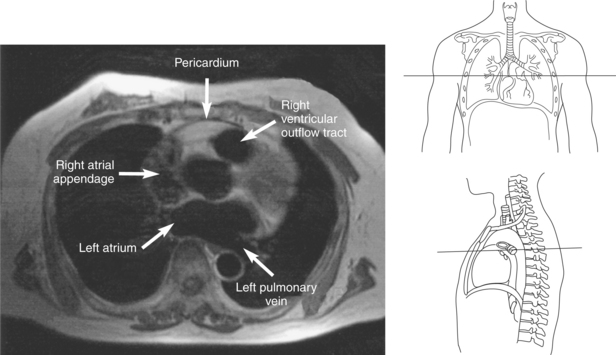
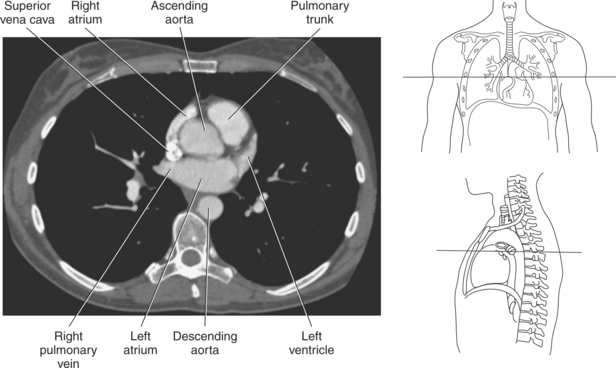
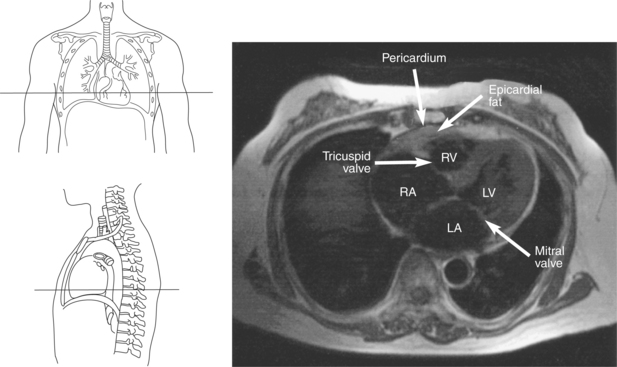
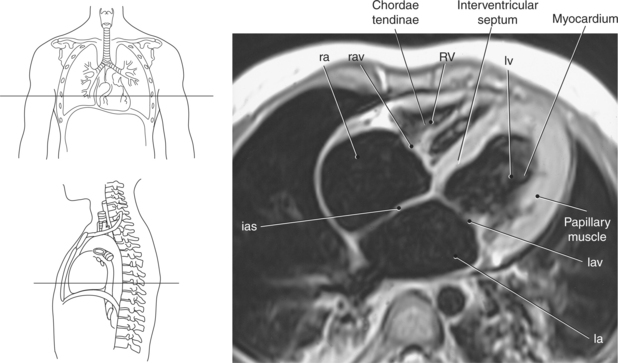
Figure 6.43 Axial, T1-weighted MR scan of left atrium.
Key: RV, Right ventricle; LV, left ventricle; LA, left atrium; RA, right atrium.
Cardiac Valves
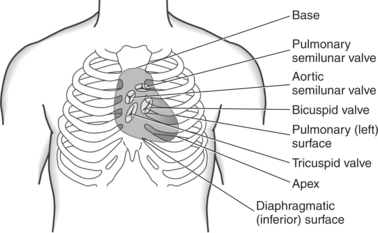
Four valves are located in the heart that function to maintain one-way directional blood flow throughout the heart. The valves can be divided into two groups: atrioventricular and semilunar (Figure 6.51).
Atrioventricular Valves
The two atrioventricular valves are found at the entrances to both ventricles and function to prevent backflow of blood between the atria and ventricles during ventricular contraction. These valves have leaflets that are attached to the papillary muscles by thin cords of fibrous tissue called chordae tendineae. The right atrioventricular valve, with three leaflets, is called the tricuspid valve, and the left atrioventricular valve, with two leaflets, is called the bicuspid (mitral) valve (Figures 6.39, 6.43, 6.44, 6.47, and 6.48).
Semilunar Valves
The semilunar valves are located at the junction where the ventricles meet the great vessels, separating the ventricles from the circulatory system. These valves are called semilunar because of their three crescent-shaped cusps and function to prevent the flow of blood back into the ventricles during ventricular relaxation. The pulmonary semilunar valve is located at the juncture of the right ventricle and pulmonary artery, and the aortic semilunar valve lies between the left ventricle and ascending aorta (Figure 6.51 through 6.53).
GREAT VESSELS
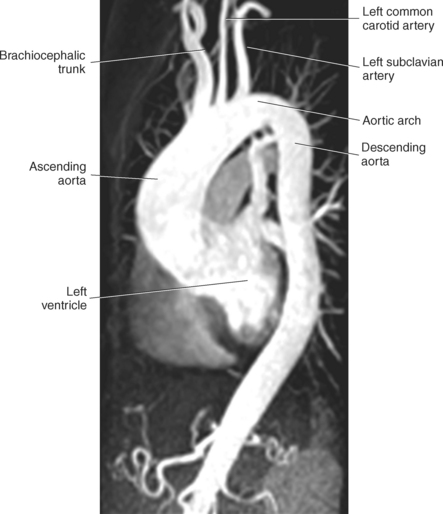
Blood travels to and from the heart through the great vessels, which include the aorta, pulmonary arteries and veins, and superior and inferior venae cavae (Figures 6.54 and 6.55). The aorta is the largest artery of the body and can be divided into the ascending aorta, aortic arch, and descending aorta. The ascending aorta begins at the base of the left ventricle at the level of the sternal angle, then curves superiorly and posteriorly as the aortic arch over the root of the left lung. The top of the aortic arch is approximately at T3 (Figures 6.56 and 6.57). The arch continues as the descending aorta posterior to the left bronchus and pulmonary trunk, on the left side of the vertebral body of T4 (Figures 6.58 and 6.59). The descending aorta passes slightly anterior and to the left of the vertebral column as it descends through the thoracic and abdominal cavities (Figure 6.60). While in the thoracic cavity, the descending aorta is commonly called the thoracic aorta, and while in the abdominal cavity, it is called the abdominal aorta. The pulmonary trunk is the origin of the right and left pulmonary arteries and lies entirely within the pericardial sac. It arises from the right ventricle and ascends in front of the ascending aorta, courses posteriorly and to the left, where it bifurcates at the level of the sternal angle (T4) into the right and left pulmonary arteries (Figures 6.61 through 6.63). The pulmonary trunk is attached to the aortic arch by a fibrous cord called the ligamentum arteriosum, the remnant of an important fetal blood vessel (ductus arteriosus) that links the pulmonary and systemic circuits during fetal development (Figures 6.54 and 6.61). The right pulmonary artery courses laterally, posterior to the ascending aorta and superior vena cava, and anterior to the esophagus and right mainstem bronchus, to the hilum of the right lung. At the root of the right lung, the right pulmonary artery divides into two branches, with the lower branch supplying the middle and inferior lobes and the upper branch supplying the superior lobe (Figures 6.61 through 6.64). The left pulmonary artery, shorter and smaller than the right, is also the most superior of the pulmonary vessels. It travels horizontally, arching over the left mainstem bronchus, and enters the hilum of the left lung just superior to the left mainstem bronchus (Figures 6.61 through 6.64). Within the lungs, each pulmonary artery descends posterolateral to the main bronchus and divides into lobar and segmental arteries, continuing to branch out and to follow along with the smallest divisions of the bronchial tree (Figures 6.61 and 6.64). Located inferior to the pulmonary arteries are the four pulmonary veins, two each (superior and inferior) extending from each lung to enter the left atrium (Figures 6.54, 6.55, 6.61, and 6.64 through 6.68). They commence in a capillary network along the walls of the alveoli, where they are continuous with the capillaries of the pulmonary arteries. The venous capillaries merge to form small vessels that unite successively to eventually form a single trunk for each lobe: three for the right and two for the left lung. Frequently the trunk from the middle lobe of the right lung unites with the trunk from the upper lobe, forming just two trunks on the right side prior to entering the left atrium. The right superior pulmonary vein collects blood from the upper lobe segments of the right lung and passes anterior and inferior to the right pulmonary artery, behind the superior vena cava. The right inferior pulmonary vein receives blood from the right lower lobes of the lung and crosses behind the right atrium to the left atrium (Figures 6.61 and 6.69 through 6.71). The left superior pulmonary vein receives blood from the left upper lobe of the left lung and courses anterior and inferior to the left main bronchus as it enters the left atrium. The left inferior pulmonary vein drains the inferior lobe of the left lung and passes toward the left atrium anterior to the bronchi (Figures 6.61 and 6.72 through 6.74). The pulmonary veins course more horizontally than the pulmonary arteries and are ultimately oriented toward the left atrium. At the root of the lungs, the pulmonary veins are anterior to the pulmonary arteries, which are anterior to the bronchus. While within the lungs, the branches of the pulmonary arteries are anterior to the bronchi, which are anterior to the pulmonary veins. The superior and inferior venae cavae are the largest veins of the body. The superior vena cava is formed by the junction of the brachiocephalic veins, posterior to the right first costal cartilage, and carries blood from the thorax, upper limbs, head, and neck (Figure 6.24). As it travels inferiorly, it is located posterior and lateral to the ascending aorta before entering the upper portion of the right atrium (Figures 6.54 through 6.59). The inferior vena cava is formed by the junction of the common iliac veins in the pelvis and ascends the abdomen to the right of the abdominal aorta and anterior to the vertebral column. It passes through the caval hiatus of the diaphragm and almost immediately enters the inferior portion of the right atrium (Figures 6.75 and 6.76).
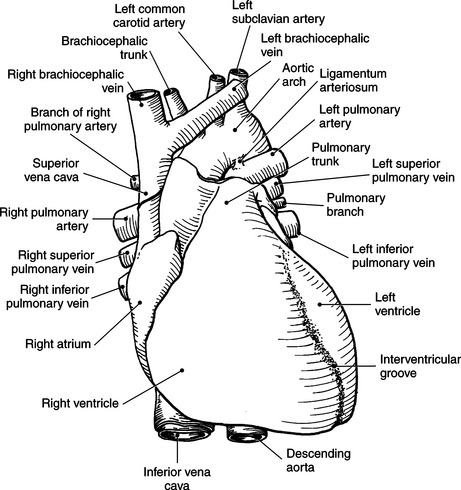
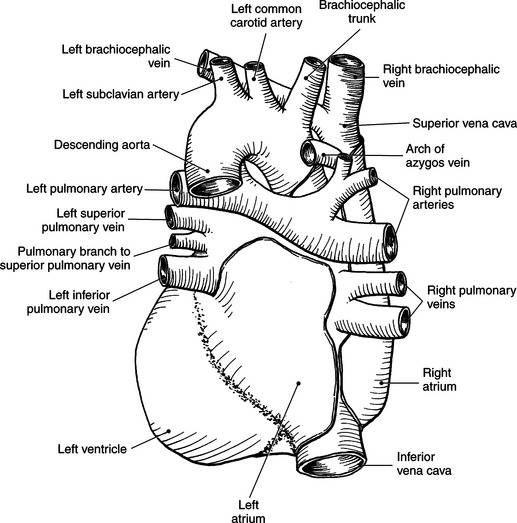
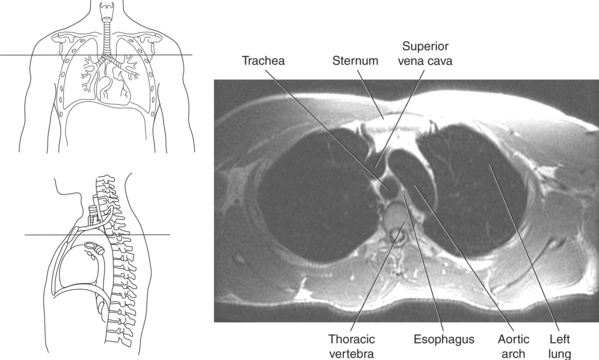
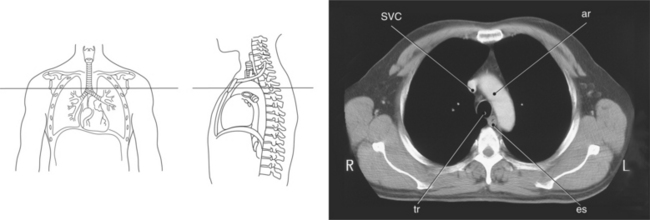
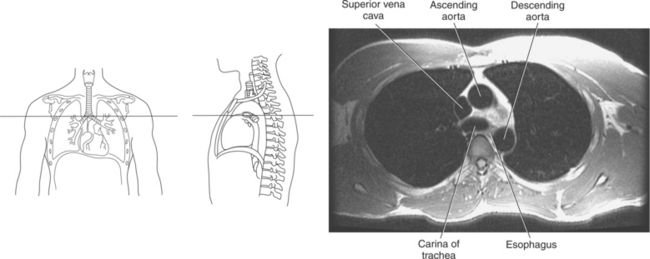
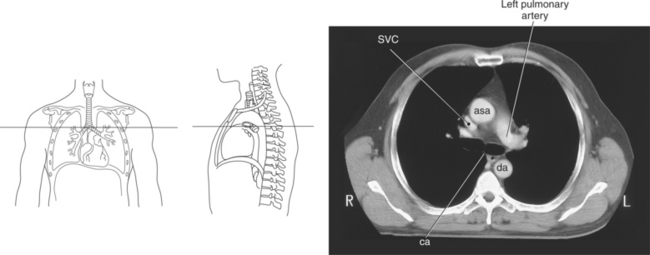
Figure 6.59 Axial CT scan of chest with ascending and descending aorta.
Key: SVC, Superior vena cava; asa, ascending aorta; da, descending aorta; ca, carina;
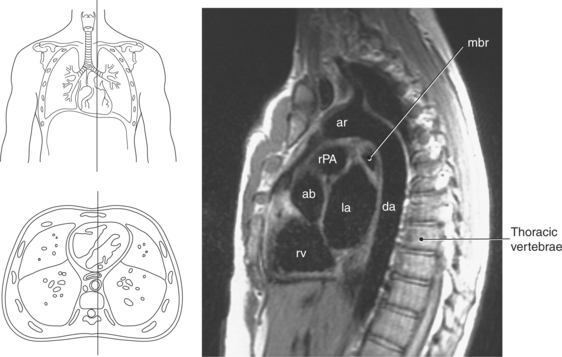
Figure 6.60 Sagittal, T1-weighted MR scan with aortic arch and descending aorta.
Key: ar, aortic arch; da, descending aorta; mbr, mainstem bronchi; rPA, right pulmonary artery; ab, aortic bulb; la, left atrium; rv, right ventricle.
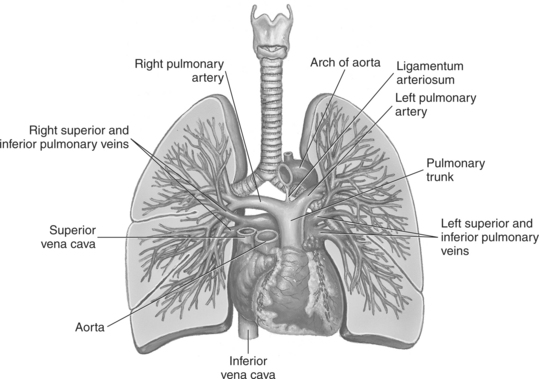
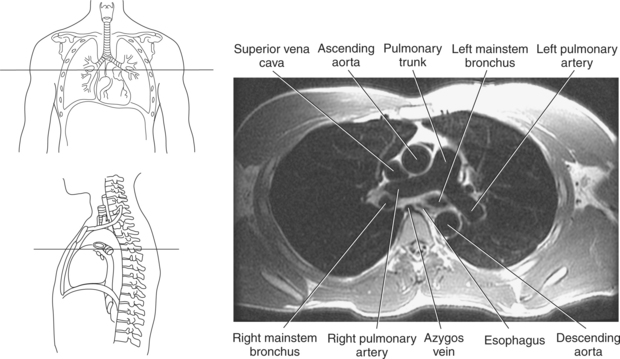
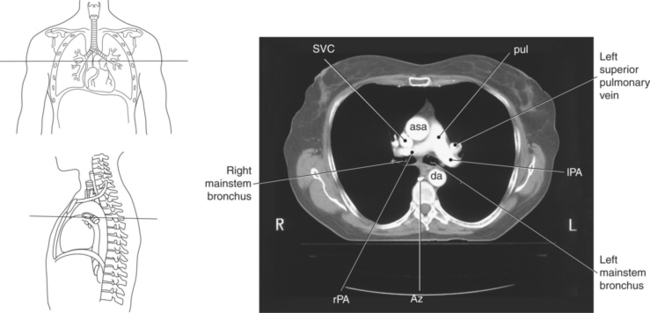
Figure 6.63 Axial CT scan of chest with pulmonary trunk.
Key: SVC, Superior vena cava; pul, pulmonary trunk; asa, ascending aorta; da, descending aorta; rPA, right pulmonary artery; Az, azygous vein; lPA, left pulmonary artery.
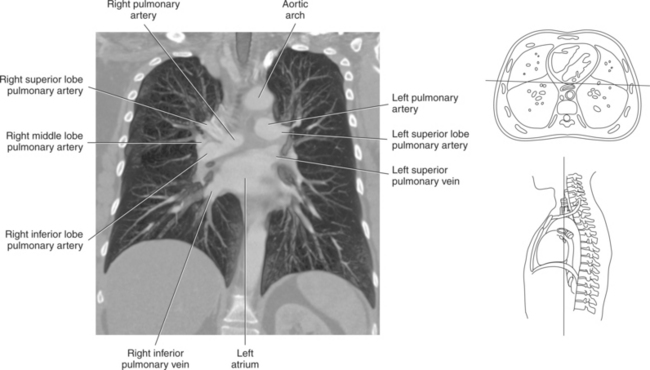
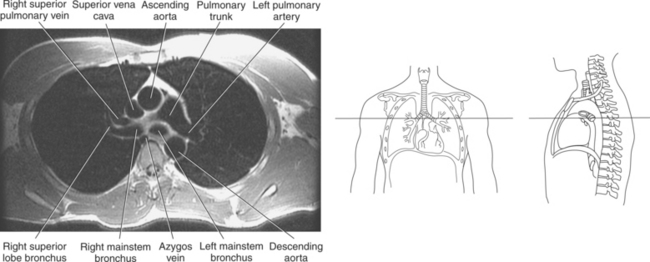
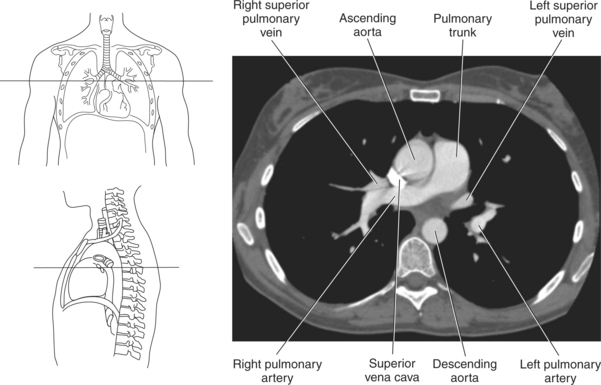
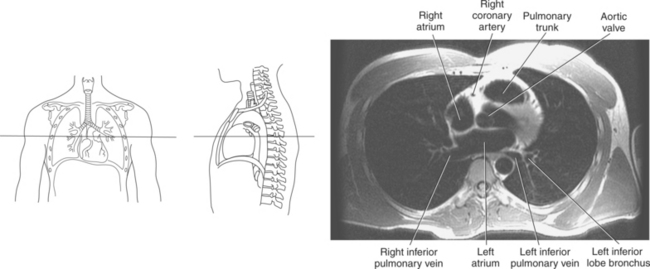
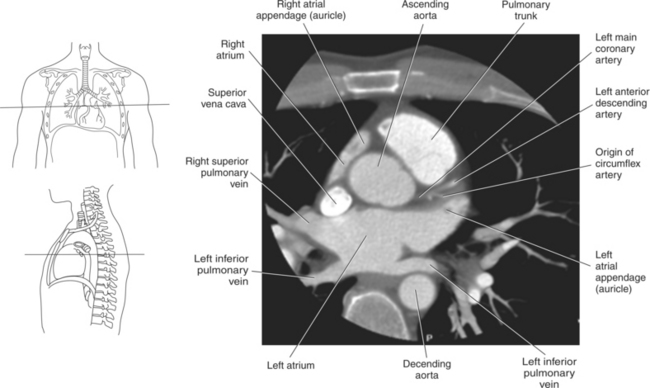
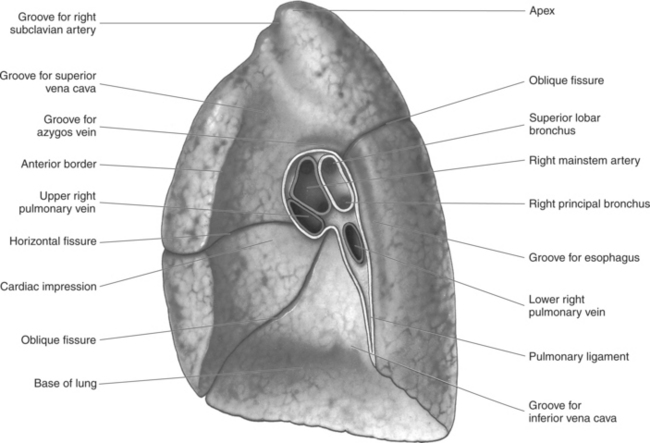
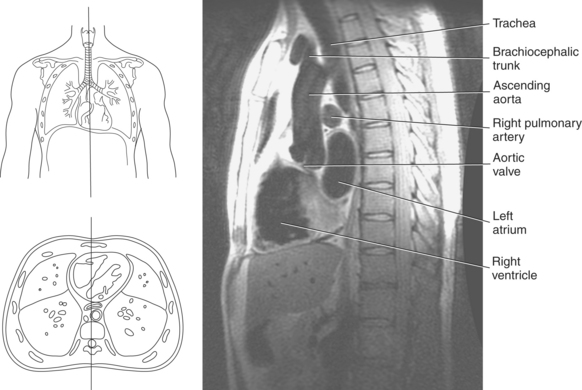
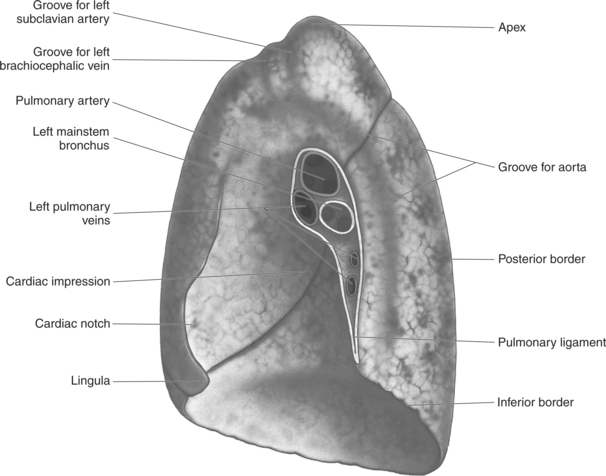
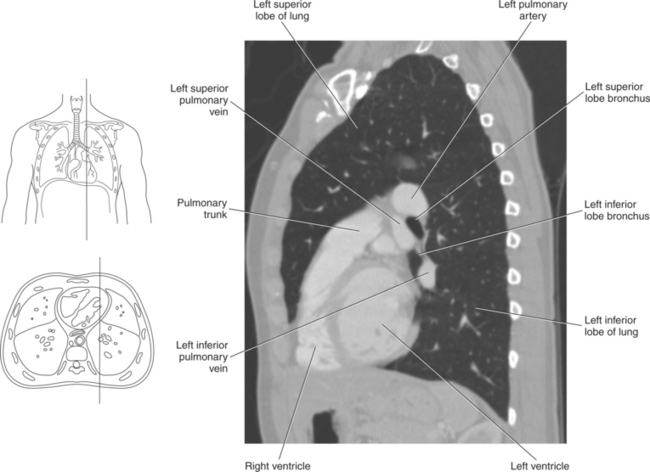
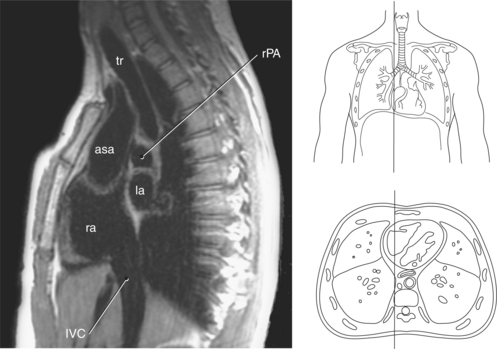
Figure 6.75 Sagittal, T1-weighted MR scan of inferior vena cava.
Key: tr, Trachea; rPA, right pulmonary artery; asa, ascending aorta; la, left atrium; ra, right atrium; IVC, inferior vena cava.
Circulation of Blood through the Heart
Deoxygenated blood is brought to the right atrium from the peripheral tissues by the inferior and superior venae cavae. The right atrium contracts, forcing blood through the tricuspid (right atrioventricular) valve into the right ventricle. The right ventricle pumps blood through the pulmonary semilunar valve to the pulmonary arteries, which enter into the lungs. Oxygenated blood returns to the heart via the pulmonary veins, which enter the left atrium. The left atrium forces blood through the bicuspid (mitral) valve into the left ventricle, where it is then pumped through the aortic semilunar valve to the aorta (Figure 6.51).
Off-Axis Cardiac Imaging
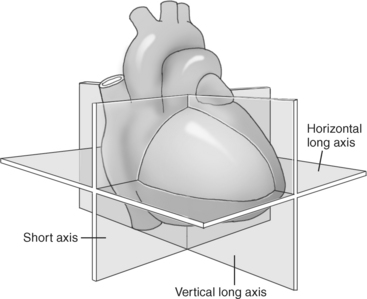
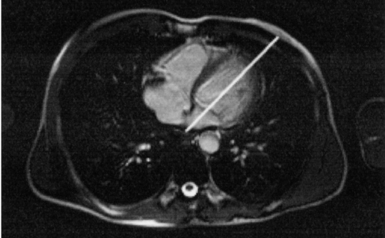
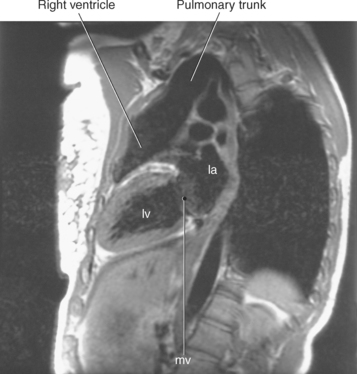
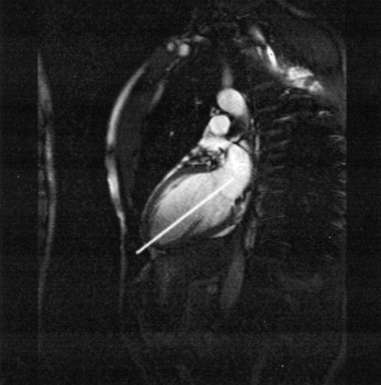
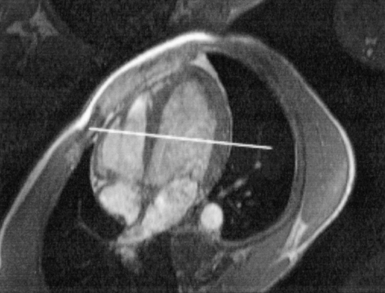
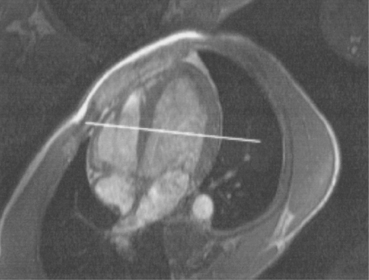
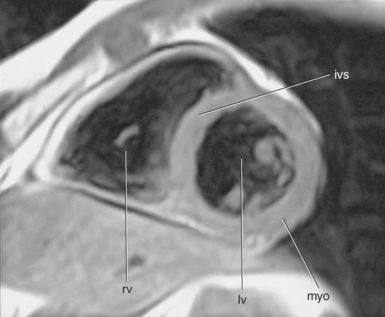
In an effort to standardize nomenclature for tomographic imaging of the heart, the Cardiac Imaging Committee of the Council on Clinical Cardiology of the American Heart Association published a statement recommending that all cardiac imaging modalities use the same nomenclature for defining tomographic imaging planes. Their recommendation stated that “all cardiac imaging modalities should define, orient, and display the heart using the long axis of the left ventricle and selected planes oriented at 90-degree angles relative to the long axis.” Their second recommendation stated, “The names for the 90-degree oriented cardiac planes used in all imaging modalities should be short axis, vertical long axis, and horizontal long axis. These correspond to the short-axis, apical two-chamber, and apical four-chamber planes traditionally used in 2D echocardiography” (Figure 6.77). We will follow these recommendations for labeling cardiac images throughout this text. In magnetic resonance (MR) imaging, each successive acquisition provides the landmarks for planning the next acquisition (view) and provides a logical method to obtain 90-degree viewing of the heart according to its intrinsic short and long axes. Several different methods can be used to obtain views of the cardiac planes during an examination, of which we provide an example of one method. To obtain the vertical long axis (VLA) view, an oblique coronal image can be positioned parallel to the interventricular septum, directly through the left atrium and ventricle (Figures 6.78 and 6.79). This plane closely approximates the right anterior oblique projection used in cineangiography and the two-chamber view used in echocardiography. The horizontal long axis (HLA) view can be obtained by angling an oblique coronal image to bisect the left ventricle, mitral valve, and left atrium (Figures 6.80 and 6.81). The HLA view demonstrates the four cardiac chambers and is comparable with the four-chamber plane used in echocardiography. The short axis (SA) view can be obtained by using the HLA image to prescribe an oblique plane through the right and left ventricles, oriented perpendicular to the interventricular septum (Figures 6.82 and 6.83).
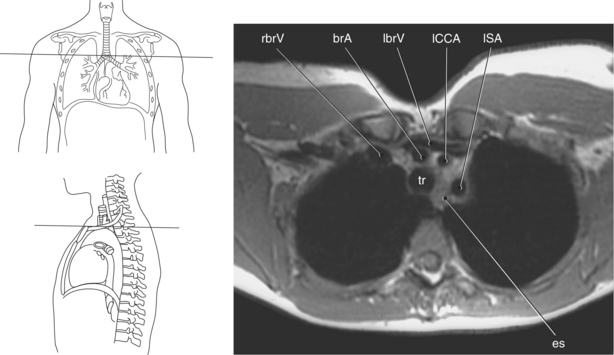
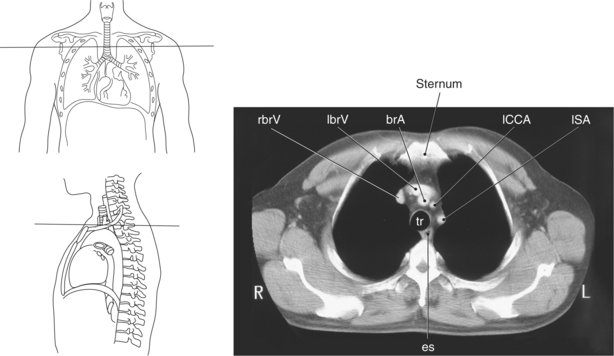
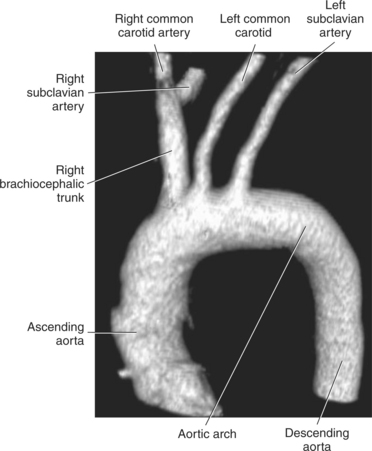
Branches of the Aortic Arch
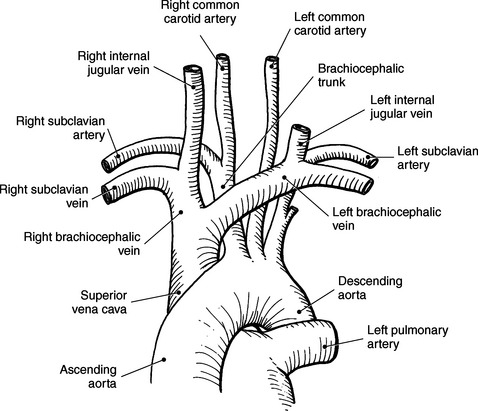
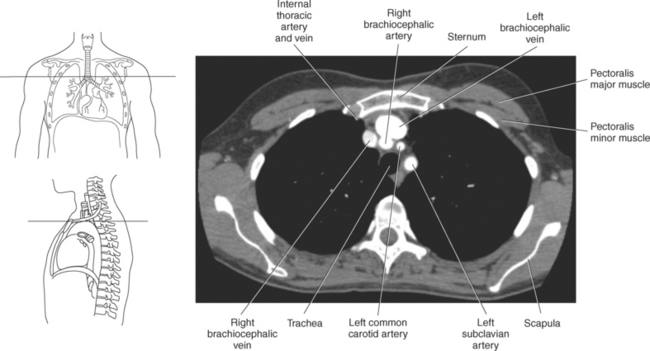
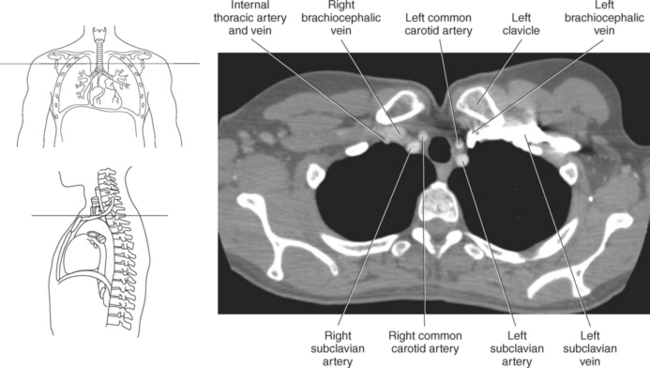
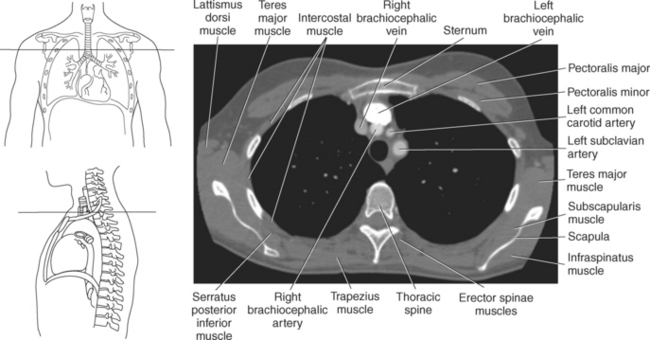
The three main branches of the aortic arch are the brachiocephalic trunk, left common carotid artery, and left subclavian artery (Figure 6.84). The brachiocephalic (innominate) trunk is the first major vessel and the largest branch arising from the aortic arch. It ascends obliquely to the upper border of the right sternoclavicular joint, where it divides into the right common carotid and right subclavian arteries (Figures 6.85 and 6.86). The right common carotid artery ascends the neck lateral to the trachea to the level of C4, where it divides into the right external and internal carotid arteries. The right subclavian artery curves posterior to the clavicle into the axillary region, where it becomes the right axillary artery. The left common carotid artery is the second vessel to branch from the aortic arch. It arises just behind the left sternoclavicular joint and ascends into the neck along the left side of the trachea to the level of C4, where it bifurcates into the left external and internal carotid arteries. The left subclavian artery arises from the aortic arch posterior to the left common carotid artery and arches laterally toward the axilla in a manner similar to that of the right subclavian artery, where it continues as the left axillary artery (Figures 6.85 through 6.88). The right and left internal thoracic arteries arise from the respective subclavian artery at the base of the neck. They run deep to the ribs, just lateral to the sternum, to supply blood to the anterior portion of the thorax (Figure 6.89). The common carotid arteries supply blood to the head and neck, whereas the subclavian arteries supply blood to the upper extremities.
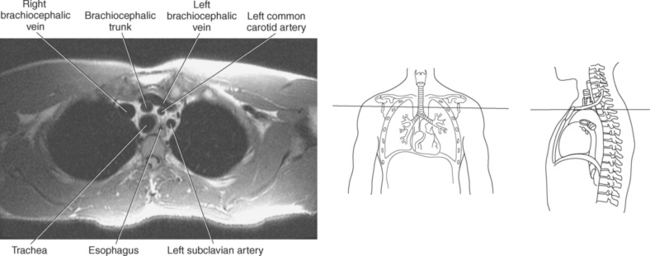
Tributaries of the Superior Vena Cava
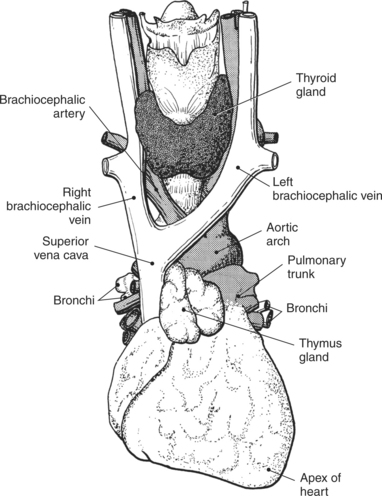
The superior vena cava receives blood from the head and neck via the internal and external jugular veins and from the upper extremities via the subclavian veins (Figures 6.84 and 6.90). The subclavian veins arise from the axillary veins and course posterior to the clavicles. They receive blood from the external jugular veins before uniting with the internal jugular veins behind the sternoclavicular joints, where they continue as the brachiocephalic veins. The left brachiocephalic vein courses across the midline, anterior to the branches of the aorta, to unite with the right brachiocephalic vein just posterior to the costal cartilage of the right first rib. The union of the two brachiocephalic veins forms the superior vena cava, which empties into the right atrium of the heart (Figures 6.75 and 6.76).

CORONARY CIRCULATION
The cardiac muscle requires a continuous supply of oxygen and nutrients, which is supplied by the coronary circulation. The coronary circulation consists of arteries that supply blood to the heart and the cardiac veins that provide venous drainage. The vessels of the coronary circulation frequently vary in their development and distribution of blood to the heart.
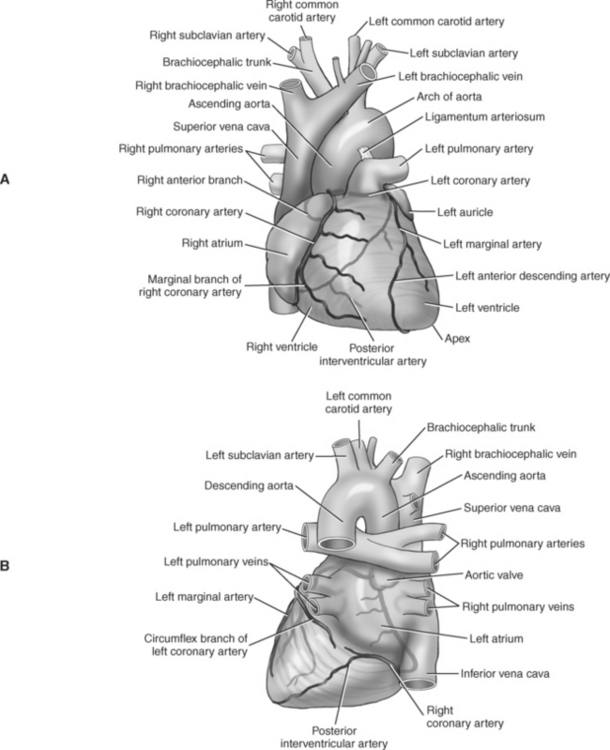
Coronary Arteries
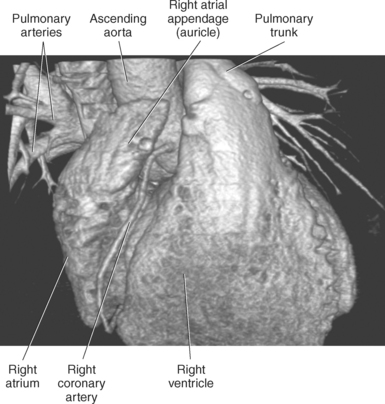
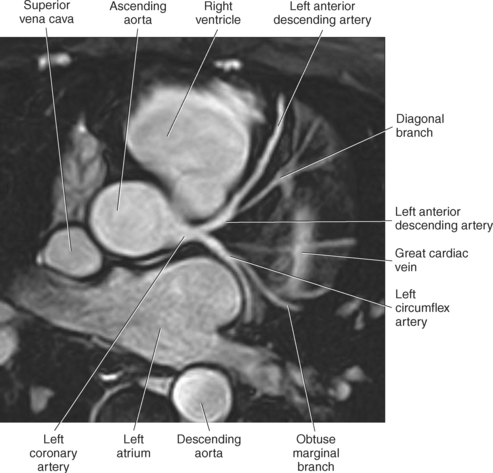
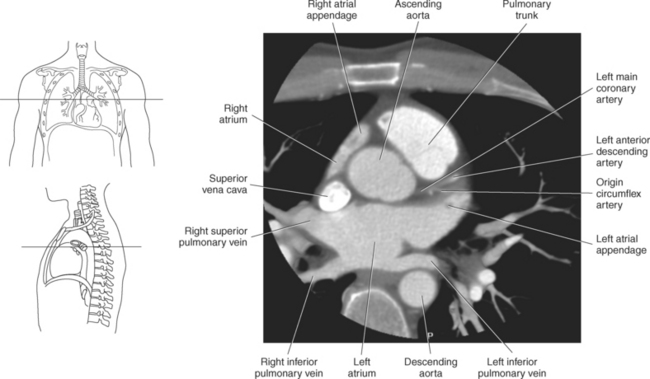
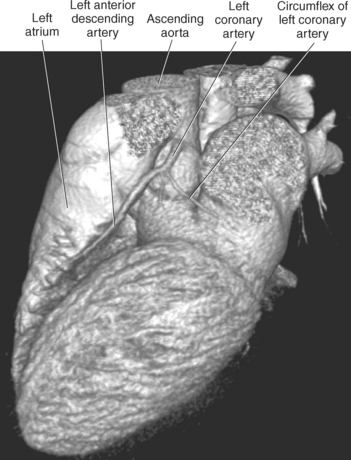
The two main coronary arteries are the first vessels to branch off the ascending aorta (Figures 6.91 and 6.92). The right coronary artery arises from the base or root of the aorta (right aortic sinus) and passes anteriorly between the pulmonary trunk and right atrium to descend in the coronary (atrioventricular) groove. As it reaches the diaphragmatic surface, it gives off a right marginal branch that runs toward the apex of the heart. The right coronary artery then turns to the left and enters the posterior interventricular groove, where it gives off the posterior interventricular branch (posterior descending artery). The posterior interventricular branch continues to descend along the interventricular groove toward the apex, where it anastomoses with the left anterior descending artery of the left coronary artery. The right coronary artery and its branches supply the right atrium, right ventricle, interventricular septum, and the sinoatrial (SA) and atrioventricular (AV) nodes. It also supplies a portion of the left atrium and ventricle (Figures 6.92 through 6.96). The left coronary artery arises from the left aortic sinus and passes to the left between the pulmonary trunk and left atrium to reach the coronary groove (Figures 6.91 and 6.92). Soon after reaching the coronary groove, the left coronary artery divides into the circumflex and left anterior descending (interventricular) arteries. The circumflex artery winds around the left border of the heart to the posterior surface, where it gives off the left marginal artery. The left anterior descending artery (LAD) descends in the anterior interventricular groove toward the apex of the heart, where it reaches the diaphragmatic surface to anastomose with the posterior descending artery. The left coronary artery and its branches supply the interventricular septum, including the AV bundles, and most of the left ventricle and atrium (Figures 6.97 through 6.99).

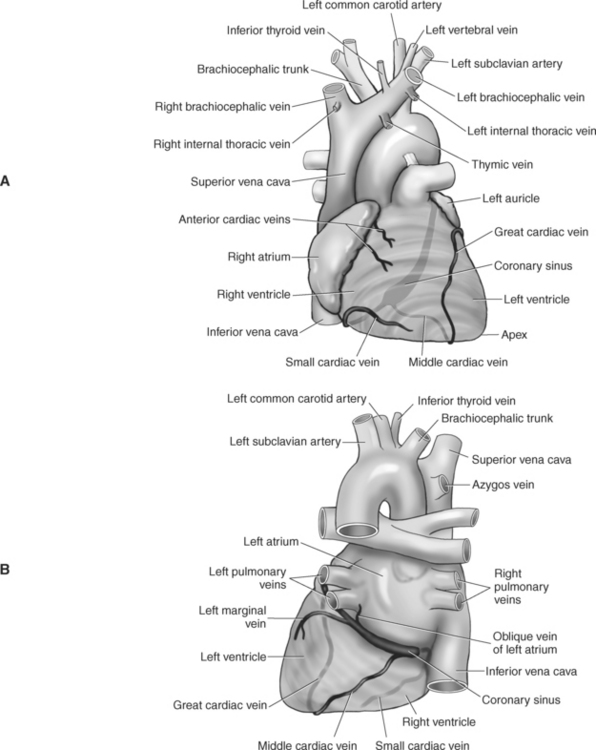
Cardiac Veins
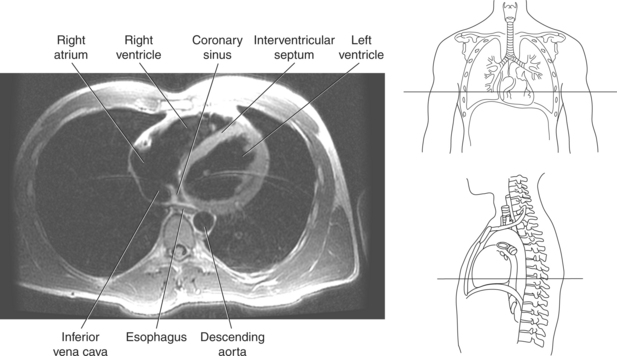
Most of the venous return from the heart is carried by the coronary sinus as it runs along the posterior section of the coronary sulcus and terminates in the right atrium immediately to the left of the inferior vena cava. The coronary sinus is a wide venous channel situated in the posterior part of the coronary sulcus and is the main vein of the heart (Figures 6.100 through 6.102). Its tributaries include the great, small, and middle cardiac veins; the left posterior ventricular vein; and the oblique vein of the left atrium. The great cardiac vein, the main tributary of the coronary sinus, arises near the apex of the heart and ascends in the anterior interventricular groove along with the anterior interventricular artery to the base of the ventricles. It receives blood from the left posterior ventricular vein and the left marginal vein before emptying into the coronary sinus. The small (right) cardiac vein runs in the coronary sulcus between the right atrium and ventricle and joins the coronary sinus from the right side. It receives blood from the right atrium and ventricle. The middle (posterior) cardiac vein commences at the apex of the heart and ascends along the posterior interventricular groove to the base of the heart, where it drains into the coronary sinus near the drainage site of the small cardiac vein. It receives blood from the posterior surface of both ventricles. The left posterior ventricular vein carries blood from the posterior wall of the left ventricle as it runs along the diaphragmatic surface of the left ventricle to drain into either the great cardiac vein or the coronary sinus. The oblique vein of the left atrium, a small vessel, descends obliquely over the posterior wall of the left atrium and enters the left end of the coronary sinus. Two small anterior cardiac veins drain directly into the right atrium (Figure 6.100).
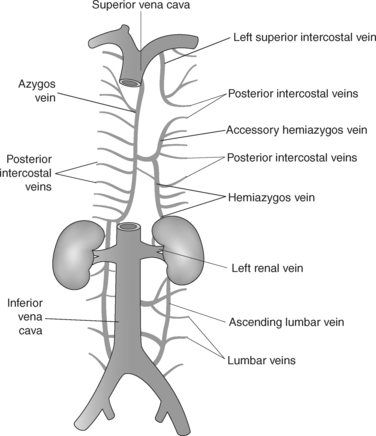
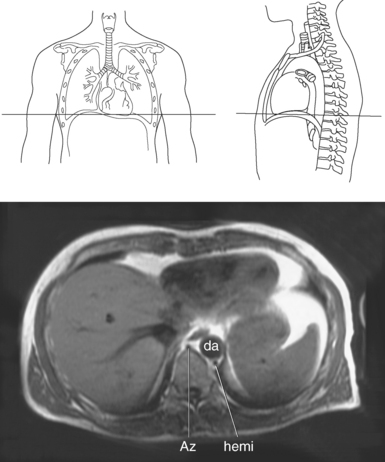
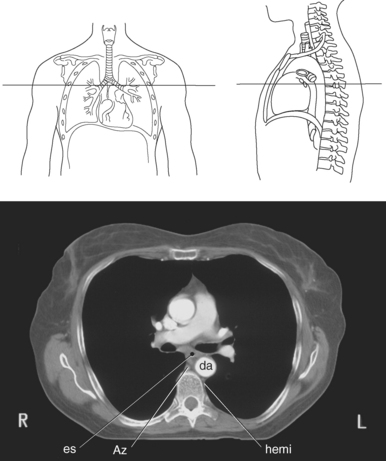
AZYGOS VENOUS SYSTEM
The azygos venous system, which provides collateral circulation between the inferior and superior venae cavae, can be divided into the azygos and hemiazygos veins (Figure 6.103). Together, they drain blood from most of the posterior thoracic wall and from the bronchi, pericardium, and esophagus. The azygos vein ascends along the right side of the vertebral column, whereas the hemiazygos vein ascends along the left side. The hemiazygos vein crosses to the right behind the aorta to join the azygos vein at approximately T7-T9. The azygos vein then arches over the hilum of the right lung to empty into the posterior superior vena cava (Figures 6.104 and 6.105).
MUSCLES
Muscles associated with respiration are the intercostal, serratus posterior superior, serratus posterior inferior, and the diaphragm (Table 6.3). The spaces between the ribs, or the intercostal spaces, are filled with three layers of intercostal muscles (external, internal, and innermost layer) (Figures 6.106 through 6.108). These muscles act together to elevate the ribs and expand the thoracic cavity, as well as keep the intercostal spaces somewhat rigid. The serratus posterior superior muscle spans from C7-T2 to ribs 2 to 5 and acts to assist forced inspiration, whereas the serratus posterior inferior muscle spans from T11-L2 to ribs 9 to 12 and acts to assist forced expiration (Figures 6.109 through 6.110). The diaphragm is a large dome-shaped muscle that spans the entire thoracic outlet and separates the thoracic cavity from the abdominal cavity (Figure 6.111). It is the chief muscle of inspiration because it enlarges the thoracic cavity vertically as the domes move inferiorly and flatten. The muscle fibers of the diaphragm converge to be inserted into a central tendon, which is situated near the center of the diaphragm immediately below the pericardium, with which it is partially blended. The diaphragm is attached to the lumbar spine via two tendinous structures termed crura (Figures 6.111 through 6.113). The right crus arises from the anterior surfaces of L1-L3, whereas the left crus arises from the corresponding parts of L1-L2 only. The left and right crura join together across the ventral aspect of the abdominal aorta to form the medial arcuate ligament. Three major openings, or hiatuses, of the diaphragm allow for the passage of vessels and organs from the thorax to the abdomen. The aortic hiatus allows for the passage of the descending aorta, azygos vein, and thoracic duct. The caval hiatus allows for the passage of the inferior vena cava and the right phrenic nerve. The esophageal hiatus allows for the passage of the esophagus and the vagus nerve.
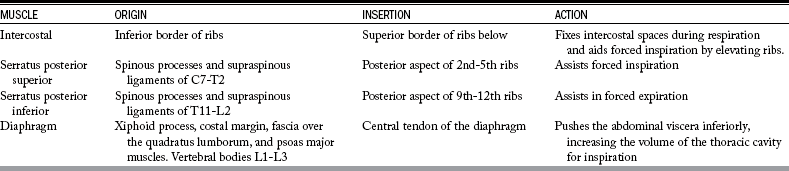
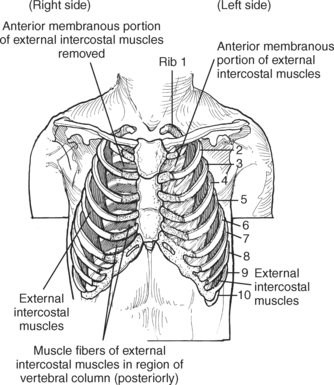
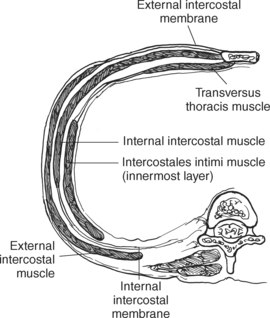
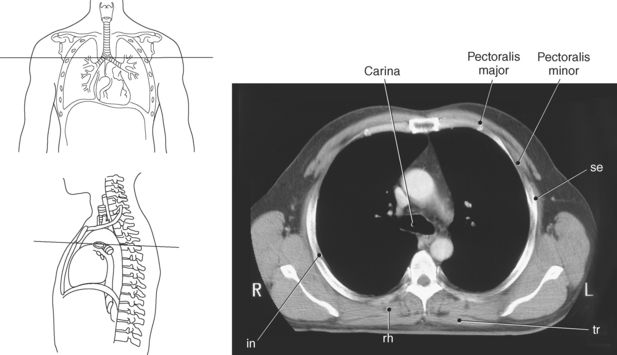
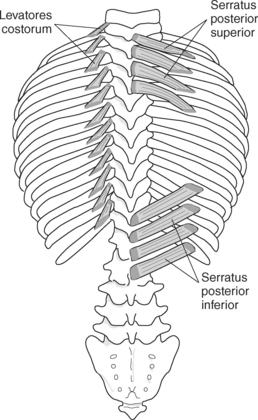

Figure 6.110 Axial CT scan of chest with serratus posterior superior muscle.
Key: se, Serratus posterior superior; tr, trachea; rh, rhomboid muscle; in, intercostals; ts, transversospinal muscles; tra, trapezius muscle.
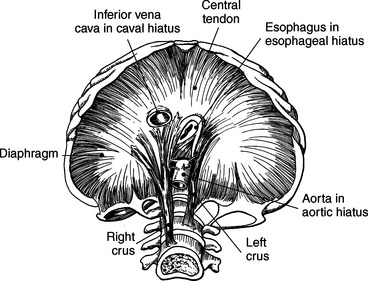
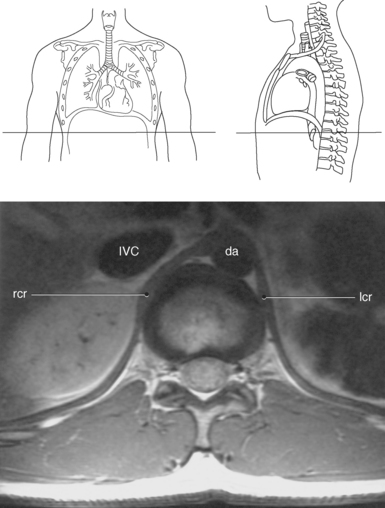
Figure 6.112 Axial, T1-weighted MR scan of abdomen with crura.
Key: rcr, Right crus; IVC, inferior vena cava; da, descending aorta; lcr, left crus.
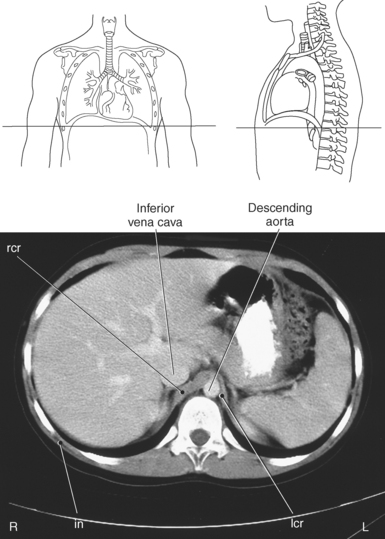
Figure 6.113 Axial CT scan of chest with crura.
Key: rcr, Right crus; lcr, left crus; in, intercostals.
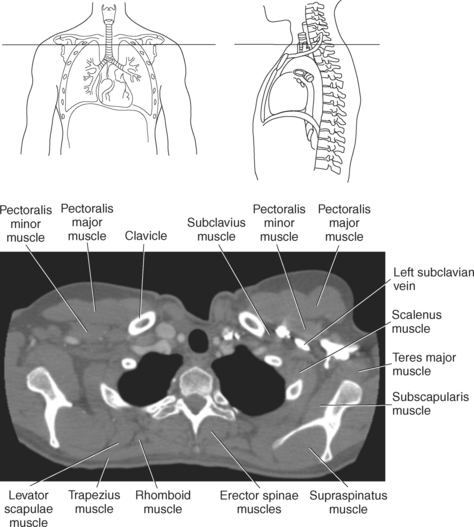
Muscles Connecting the Upper Extremity to the Anterior and Lateral Thoracic Walls
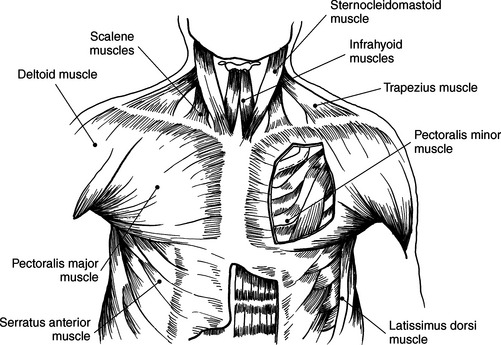
Muscles of the anterior and lateral thoracic region are pectoralis major, subclavius, pectoralis minor, and serratus anterior. Muscles associated with the movement of the upper extremity such as the pectoralis, subclavius, and serratus anterior can also function as accessory muscles for respiration (Figure 6.114 and Table 6.4). For example, the pectoralis muscles (major and minor), located on the anterior surface of the chest, primarily aid in the movement of the upper limb, but the pectoralis major muscle can also act to expand the thoracic cavity on deep inspiration (Figures 6.115 and 6.116). The subclavius, a small triangular-shaped muscle located between the clavicle and first rib acts alone to stabilize the clavicle and depress the shoulder. However, conjointly with the pectoralis muscles, the subclavius muscles act to raise the ribs, drawing them upward and expanding the chest, thus becoming important agents in forced inspiration. Additionally, the serratus anterior muscles aid in respiration. The serratus (sawlike) anterior muscle is visualized on the lateral border of the thorax. It extends from the medial border of the scapula to the lateral surface of the first rib through eighth ribs. The primary action of the serratus anterior muscle is to laterally rotate and protract the scapula. It can, however assist in raising the ribs for inspiration (Figure 6.114; see also Chapter 9).

BREAST
The female breast, or mammary gland, lies within the subcutaneous tissue overlying the pectoralis major muscle. Typically the breast extends laterally from the sternum to the axilla and inferiorly from the second to the seventh ribs. For examination purposes, the breast can be divided into four quadrants (upper inner, upper outer, lower outer, lower inner) and the tail of Spence (Figure 6.117). The breast consists of three layers of tissue: subcutaneous layer, mammary layer, and retromammary layer (Figure 6.118). The subcutaneous layer contains the skin and all of the subcutaneous fat. The mammary layer consists of glandular tissue, excretory (lactiferous) ducts, and connective tissues. The glandular tissue consists of 15 to 20 lobes arranged radially around a centrally located nipple. The glandular lobes are embedded in connective tissue and fat, which give the breast its size and shape. Excretory (lactiferous) ducts extend from each lobe to the nipple, where they terminate as small openings. Cords of connective tissue coursing throughout the mammary layer, from the dermis to the thoracic fascia, are known as the suspensory ligaments of the breast or Cooper’s ligaments. These ligaments provide support for the breasts. The retromammary layer contains muscle, deep connective tissue, and retromammary fat (Figures 6.119 and 6.120).
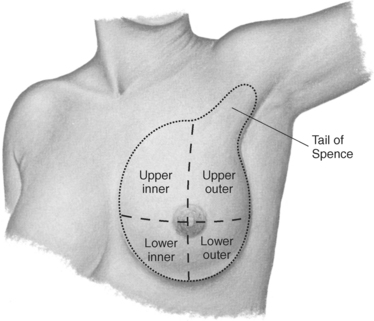
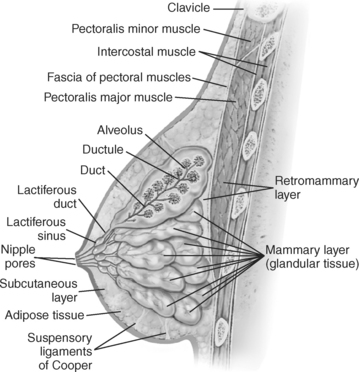
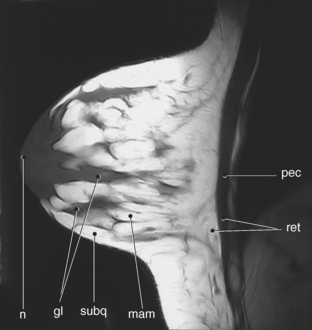
Figure 6.119 Sagittal, T1-weighted MR scan of female breast.
Key: pec, Pectoralis major muscle; ret, retromammary layer; mam, mammary layer; subq, subcutaneous layer; gl, glandular; n, nipple.
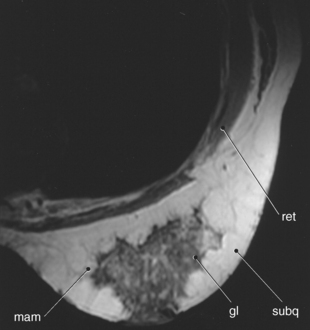
Figure 6.120 Axial, T1-weighted MR scan of female breast.
Key: ret, retromammary layer; mam, mammary layer; subq, subcutaneous layer; gl, glandular.
Axillary lymph nodes drain the lymphatics from the breast, arm, and integument of the back. They are frequently clustered around the axillary vessels, the lower border of the pectoralis major muscle, and the lower margin of the posterior wall.
Agur, AM. Grant’s atlas of anatomy. Baltimore: Williams & Wilkins, 1996.
Applegate, E. The anatomy and physiology learning system, ed 2. Philadelphia: Saunders, 2000.
Applegate, E. The sectional anatomy learning system, ed 2. Philadelphia: Saunders, 2002.
Ballinger, PW. Merrill’s atlas of radiographic positions and radiologic procedures, ed 10. St. Louis: Mosby, 2003.
Blackwell, GG, Cranney, GB, Pohost, GM, et al. MRI: cardiovascular system. New York: Gower Medical Publishing, 1992.
Cerqueira, MD, Weissman, NJ, Dilsizian, V, et al. Standardized myocardial segmentation and nomenclature for tomographic imaging of the heart: a statement for healthcare professionals from the Cardiac Imaging Committee of the Council on Clinical Cardiology of the American Heart Association. Circulation. 2002;105:539.
English, AW. Wolf-Heidegger’s atlas of human anatomy, ed 5. Basel, Switzerland: Karger, 2000.
Gray, H. Gray’s anatomy, ed 38. Philadelphia: Churchill Livingstone, 1995.
Sandring, S. Gray’s anatomy, ed 39. Philadelphia: Churchill Livingstone, 2005.
Haaga, JR, Lanzieri, CF, Gilkeson, RC, et al. CT and MR imaging of the whole body, ed 4. Philadelphia: Mosby, 2003.
Harnsberger, HR. Handbook of head and neck imaging, ed 2. St. Louis: Mosby, 1995.
Jacob, S. Atlas of human anatomy. Philadelphia: Churchill Livingstone, 2002.
Larsen, WJ. Anatomy: development function clinical correlations. Philadelphia: Saunders, 2002.
Manning, WJ, Pennel, DJ. Cardiovascular magnetic resonance. Philadelphia: Churchill Livingstone, 2002.
Martini, FH. Fundamentals of anatomy and physiology, ed 3. Englewood Cliffs, NJ: Prentice-Hall, 1995.
Miller, SW. Cardiac radiology: the requisites. St. Louis: Mosby, 1996.
Mosby’s medical, nursing, and allied health dictionary, ed 6. Mosby: St. Louis, 2002.
Palastanga, N, Field, D, Soames, R, et al. Anatomy and human movement, ed 4. Philadelphia: Butterworth-Heinemann, 2002.
Seidel, HM, Ball, JW, Dains, JE, et al. Mosby’s guide to physical examination, ed 4. St. Louis: Mosby, 1999.
Som, PM, Curtin, HD. Head and neck imaging, ed 3. St. Louis: Mosby, 1996.
Stark, DD, Bradley, WG. Magnetic resonance imaging, ed 3. St. Louis: Mosby, 1999.