Upper Extremity
The intricate anatomy of the musculoskeletal system can make identification of the joint anatomy challenging (Figure 9.1). A basic knowledge of the anatomy and kinesiology of these areas increases the ability to identify pathology or injury that may occur.

SHOULDER
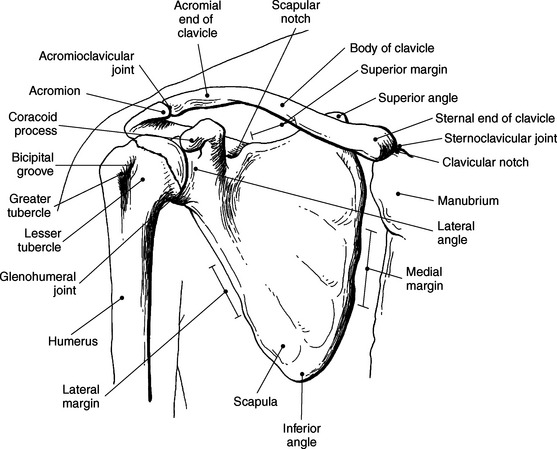
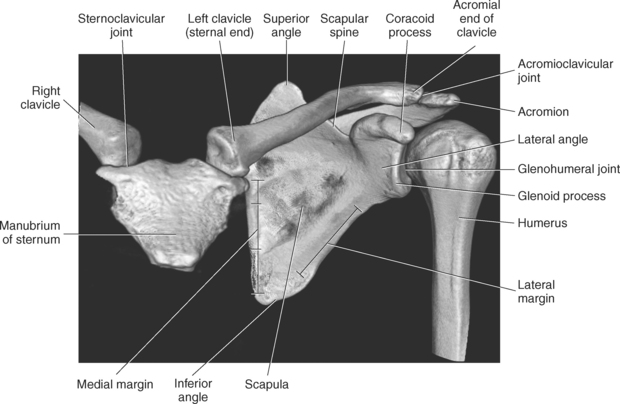
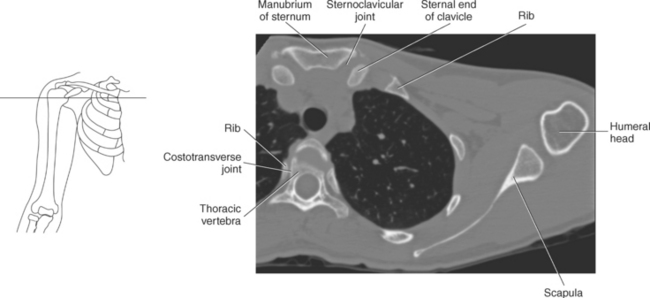
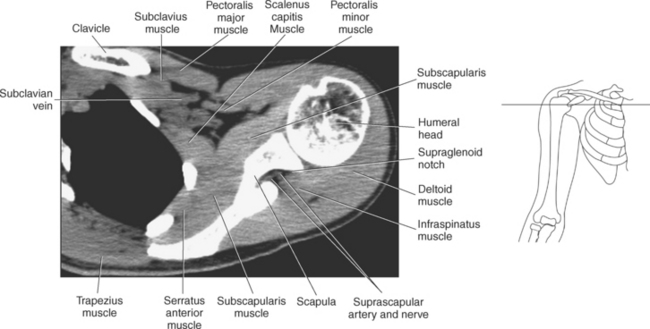
The bony anatomy that comprises the shoulder girdle includes the clavicle, scapula, and humerus (Figures 9.2 and 9.3).
Clavicle
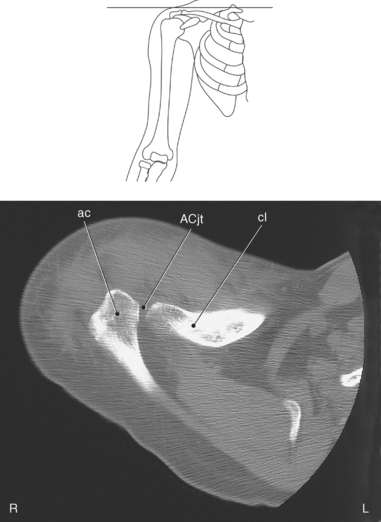
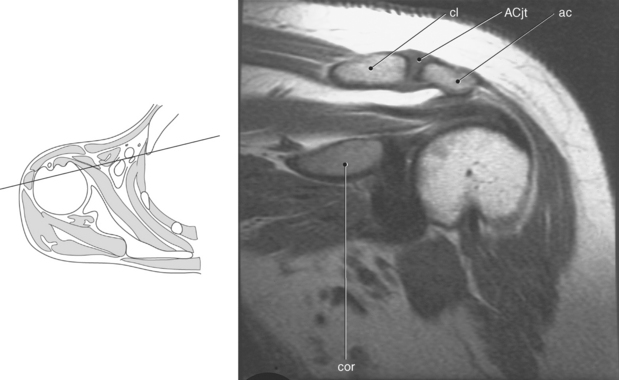
The clavicle connects the upper limb to the trunk of the body and provides attachments for several muscles and ligaments. The clavicle is a long, slender S-shaped bone located anteriorly that extends transversely from the sternum to the acromion of the scapula. The widened sternal end of the clavicle articulates with the clavicular notch of the sternal manubrium to form the sternoclavicular (SC) joint, and its flattened acromial end articulates with the acromial process of the scapula to form the acromioclavicular (AC) joint. The medial two thirds of the body of the clavicle are convex anteriorly, whereas the lateral one third is flattened and concave anteriorly (Figures 9.2 through 9.6).
Scapula
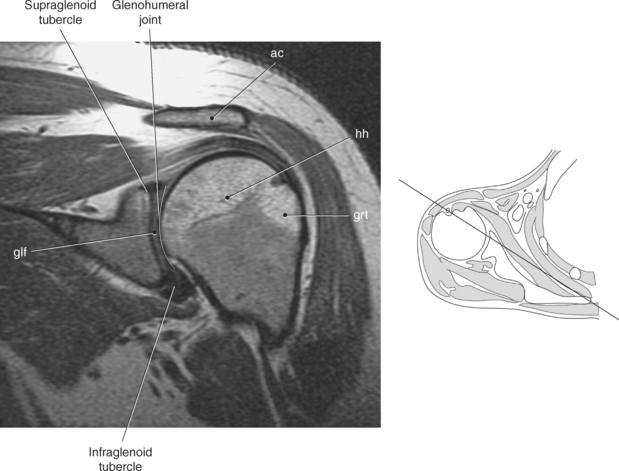
The scapula is a triangular-shaped flat bone that forms the posterior portion of the shoulder girdle. It has a medial margin, a lateral margin, and a superior margin. The margins are separated by the superior, inferior, and lateral angles (Figures 9.2 and 9.3). The anterior surface of the scapula, subscapular fossa, is flat and slightly concave. The posterior surface of the scapula is divided by the scapular spine into a smaller supraspinous fossa, and a larger infraspinous fossa (Figure 9.7). Four projections of the scapula provide attachment sites for the muscles and ligaments contributing to the shoulder girdle. These include the scapular spine, acromion, coracoid process, and glenoid process (Figures 9.7 through 9.10). The scapular spine arises from the upper third of the posterior surface of the scapula and extends obliquely and laterally to give rise to a flattened process termed the acromion. Located on the anterolateral surface of the scapula is a beaklike process termed the coracoid process, which arises just medial to the glenoid process and functions to protect the shoulder joint, which lies beneath it. The coracoid process is an attachment site for the pectoralis minor, short head of the biceps brachii, and the coracobrachialis muscles. The scapular notch is located just medial to the coracoid process, on the superior margin of the scapula and allows for the passage of the suprascapular nerve (Figure 9.2). The glenoid process, the largest of the projections, forms the lateral angle of the scapula and ends in a depression called the glenoid fossa (glenoid cavity) (Figures 9.7 through 9.9). There are two tubercles associated with the glenoid fossa, an upper supraglenoid tubercle and a lower infraglenoid tubercle, which serve as attachment sites for the biceps brachii and triceps brachii (Figure 9.8). The shallow articular surface of the glenoid fossa joins with the relatively large articular surface of the humeral head to create the freely moving glenohumeral joint (Figures 9.2, 9.3, 9.11, and 9.12).
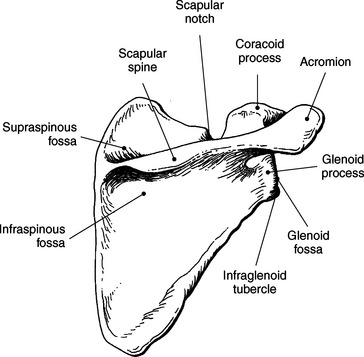
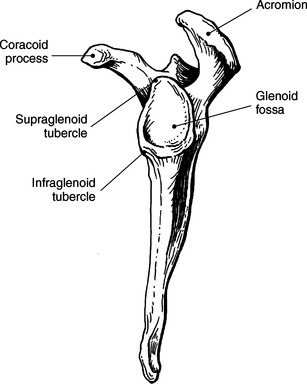
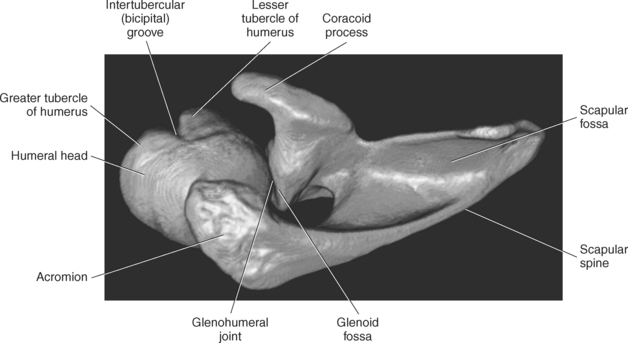
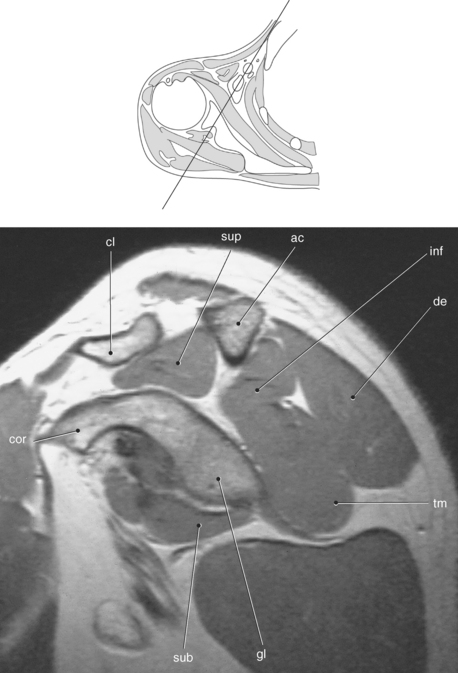
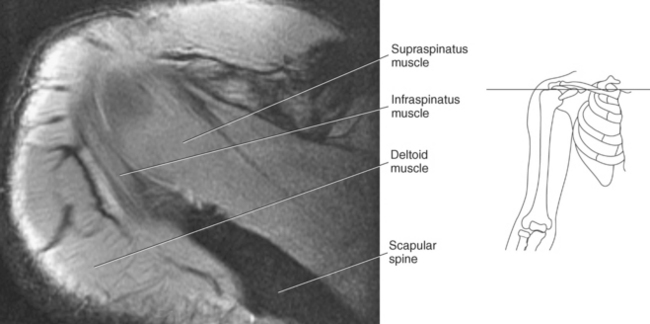
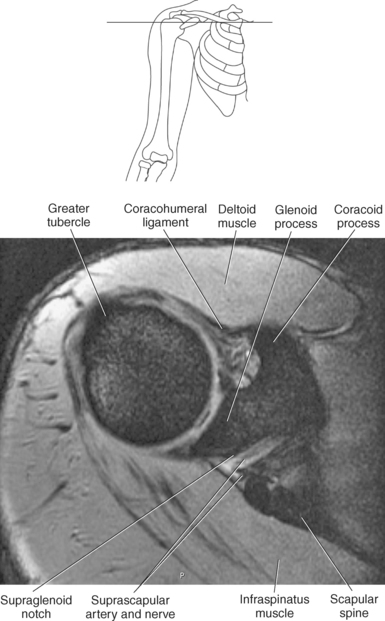
Figure 9.10 Sagittal oblique, T1-weighted MR scan of shoulder.
Key: cor, Coracoid process; cl, clavicle; sup, supraspinatus; ac, acromion; inf, infraspinatus; de, deltoid; tm, teres minor; gl, glenoid; sub, subscapularis; h, humerus; grt, greater tubercle; sc, scapula; glf, glenoid fossa; hh, humeral head.
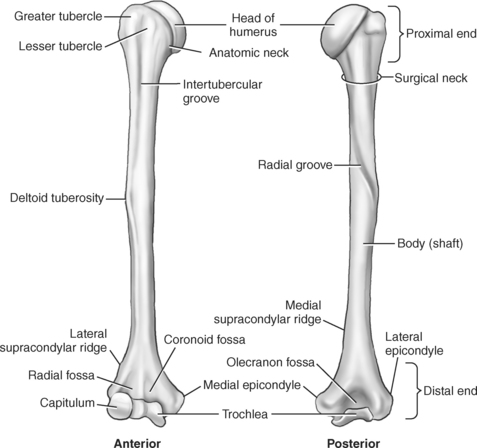
Humerus
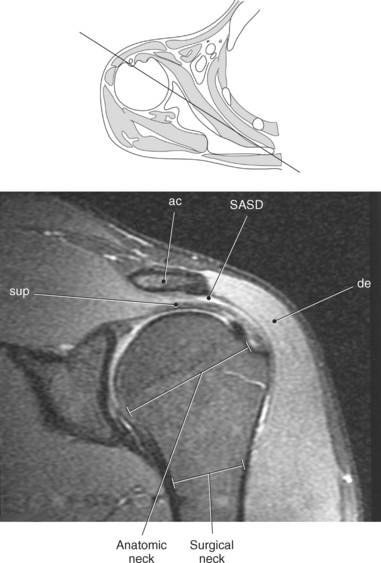
The humerus is a long bone that articulates with the scapula superiorly and the radius and ulna inferiorly. It consists of a body or shaft, a lower end (distal end), and an upper (proximal) end (Figure 9.13). The proximal end is formed by the head of the humerus. Two tubercles project from the humeral head to provide attachment sites for tendons and ligaments. The lesser tubercle is located on the anterior surface of the humeral head, whereas the greater tubercle is located on the lateral surface of the humeral head (Figures 9.12 through 9.15). The tubercles are separated by the intertubercular (bicipital) groove, which is bounded by the crests of the lesser and greater tubercles as it descends the humerus (Figures 9.9 and 9.13 through 9.15). The humerus has two necks, the more proximal anatomic neck and the surgical neck, located inferior to the tubercles just distal to the humeral head (Figures 9.13 and 9.16). In the middle of the body or shaft of the humerus, on the anterior surface, is the roughened area of the deltoid tuberosity that gives attachment for the deltoid muscle (Figure 9.13).
Labrum and Ligaments
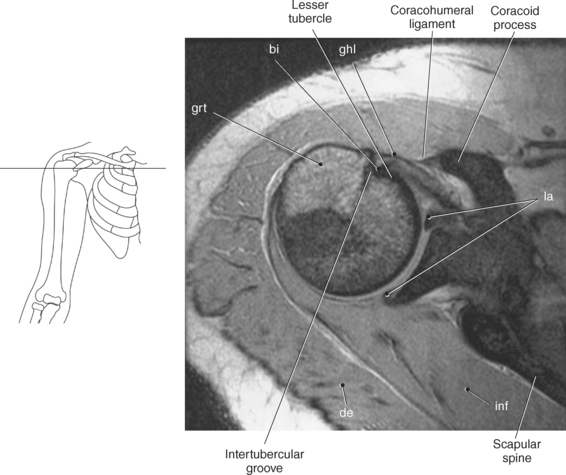
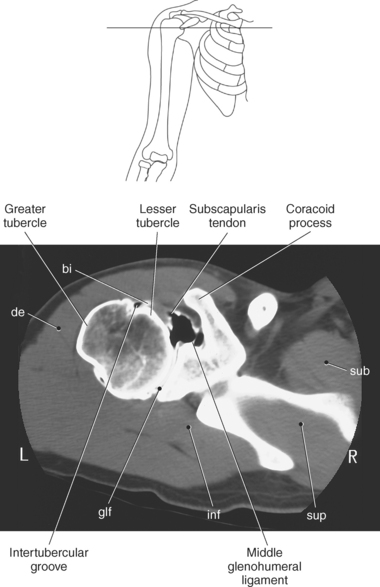
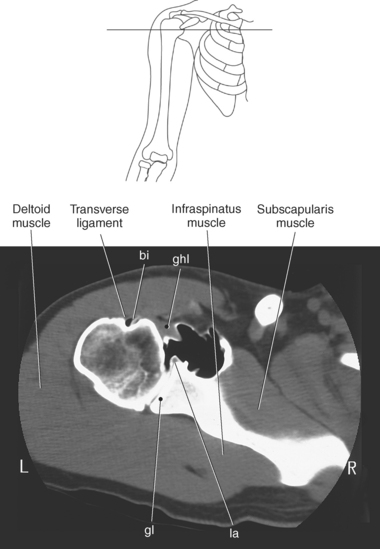
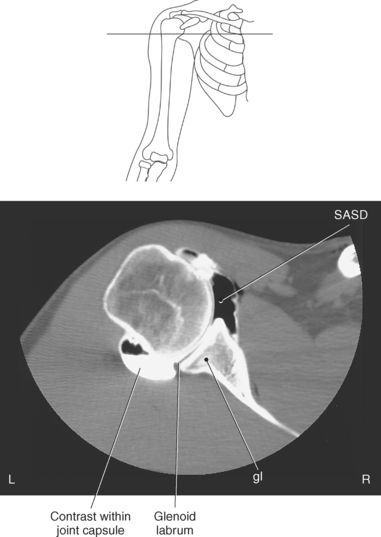
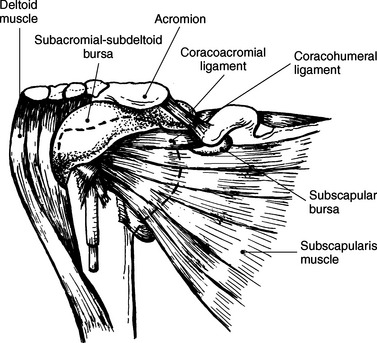
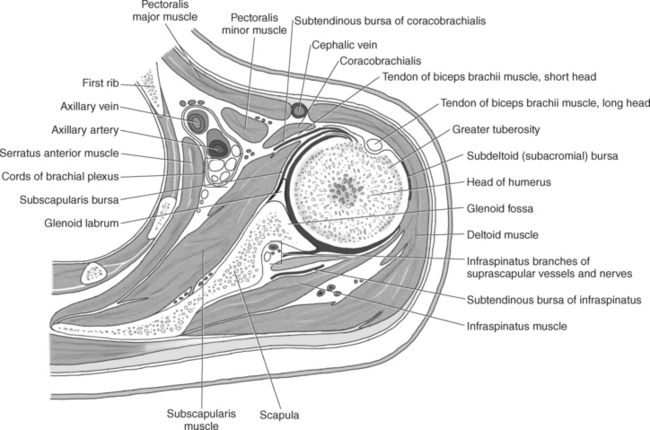
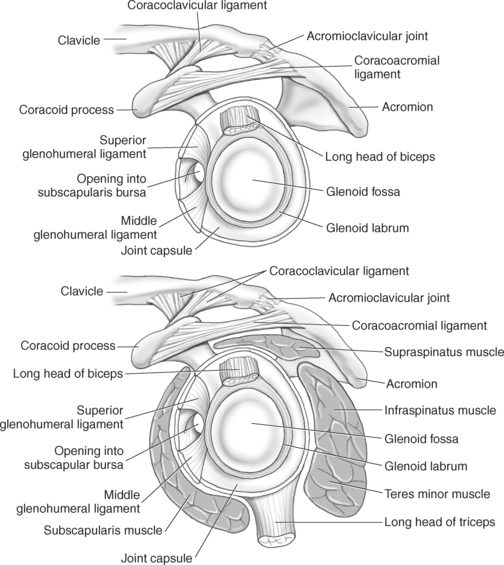
The edge of the glenoid fossa is surrounded by a fibrocartilaginous ring termed the glenoid labrum (glenoid lip) (Figure 9.17). The glenoid labrum is a fold of the articular capsule, which functions to deepen the articular surface of the glenoid fossa. Superiorly, the labrum blends with the long head of the biceps brachii muscle. In cross section it appears triangular (Figure 9.18). The three glenohumeral ligaments (superior middle, and inferior) are thickenings of the fibrous capsule that surrounds the shoulder joint; they contributes to the formation of the glenoid labrum (Figures 9.17 and 9.19). They extend from the supraglenoid tubercle of the scapula to the lesser tubercle of the humerus. Also aiding in strengthening the fibrous capsule is the coracohumeral ligament that passes from the lateral side of the coracoid process of the scapula to the anatomic neck of the humerus (Figure 9.19). The coracoacromial ligament is another important ligament located on the anterior portion of the shoulder. As this ligament joins the coracoid process and acromion, it forms a strong bridge, termed the coracoacromial arch, which protects the humeral head and rotator cuff tendons from direct trauma and prevents displacement of the humeral head superiorly (Figures 9.17 and 9.19). The coracoclavicular ligaments help to maintain the position of the clavicle, in relation to the acromion, by spanning the distance between the clavicle and coracoid process of the scapula (Figure 9.19). The acromioclavicular ligament, at the acromioclavicular joint, provides support for the superior surface of the shoulder (Figures 9.17 and 9.19). The transverse humeral ligament is a broad band of connective tissue passing from the greater tubercle to the lesser tubercle of the humerus, forming a bridge over the intertubercular groove for protection of the long head of the biceps tendon (Figure 9.19). The ligaments of the shoulder are demonstrated in Figures 9.20 through 9.30.
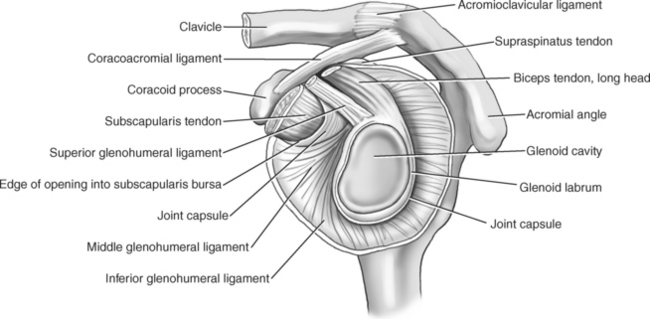
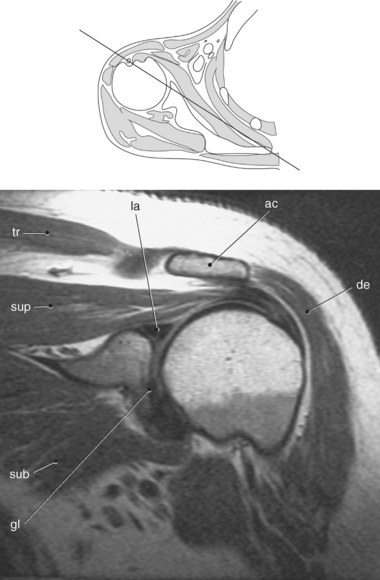
Figure 9.18 Coronal oblique, T1-weighted MR scan of shoulder with glenoid labrum.
Key: tr, Trapezius; la, labrum; ac, acromion; de, deltoid; gl, glenoid; sub, subscapularis; sup, supraspinatus.
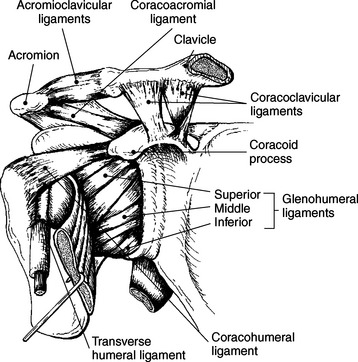
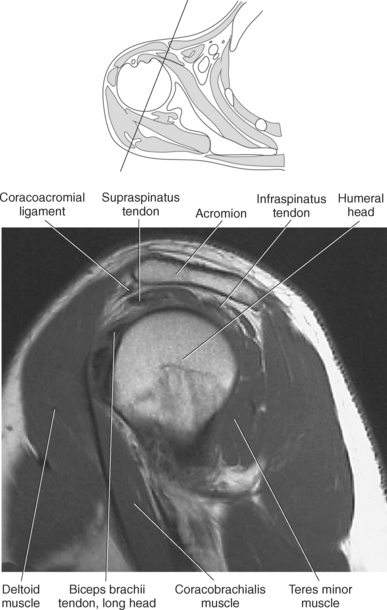
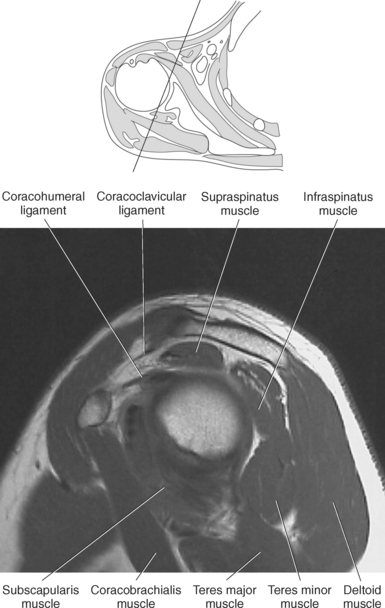
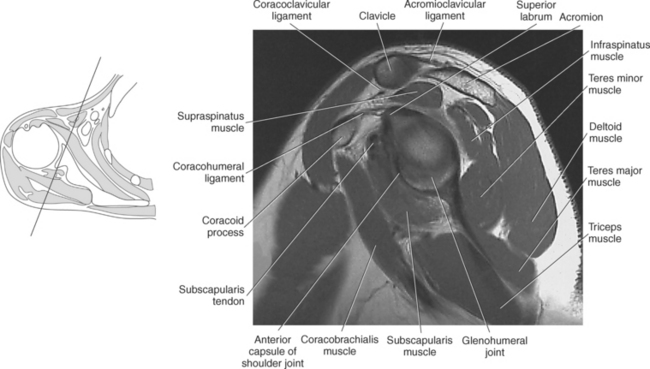
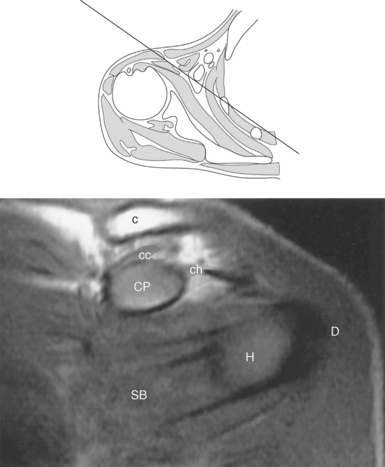
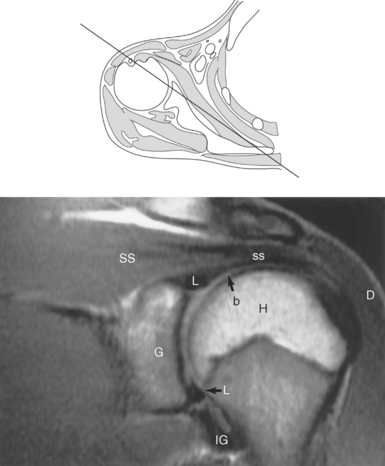
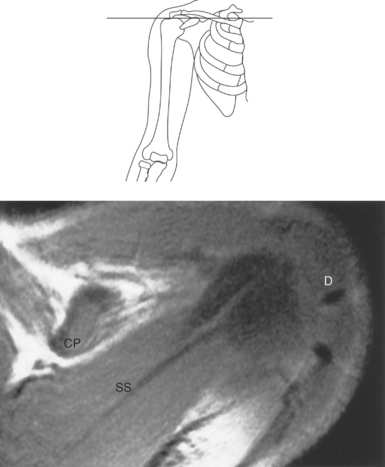
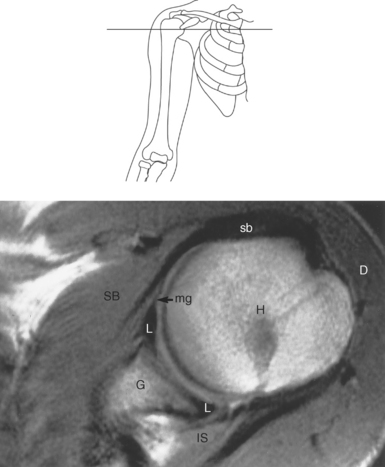
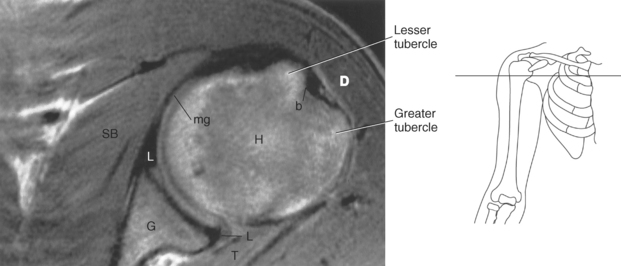
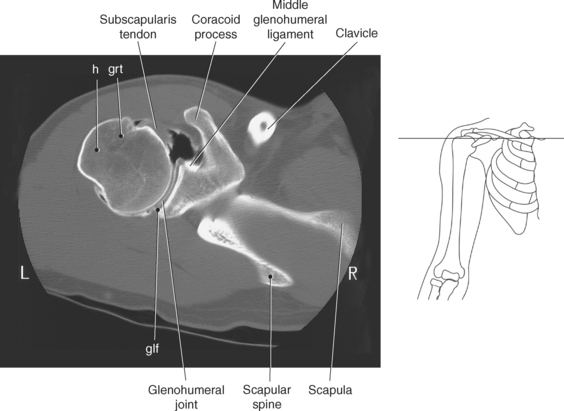
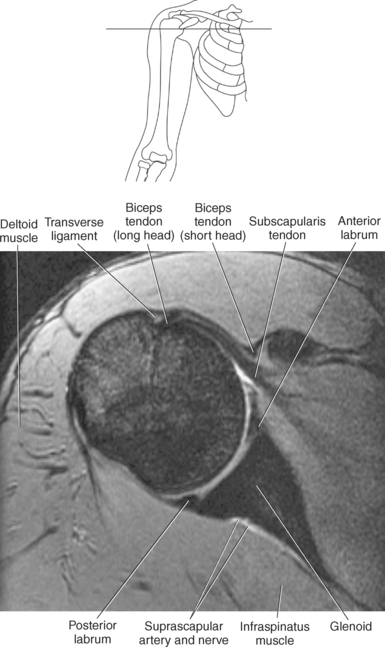
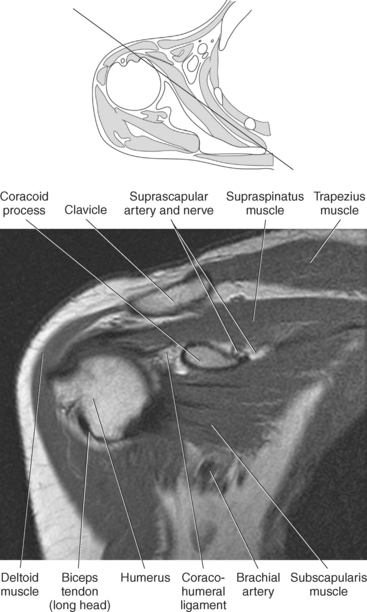
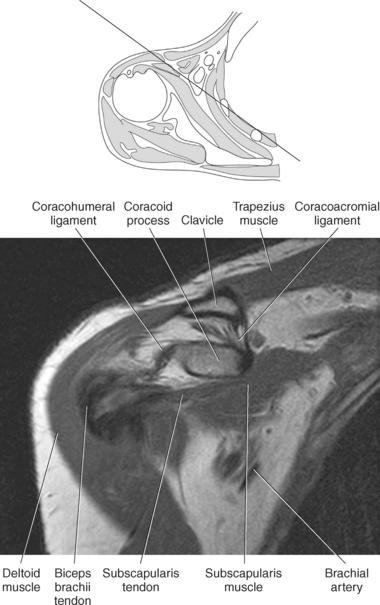
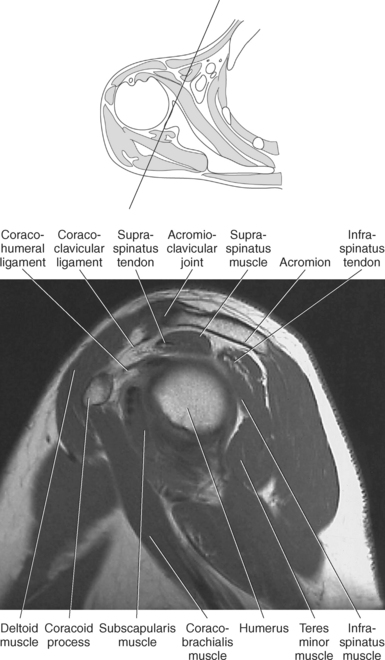
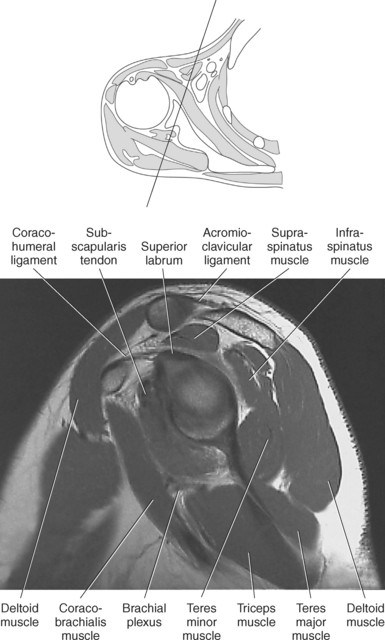
Figure 9.27 Axial, T1-weighted MR scan of shoulder.
Key: c, Clavicle; cc, coracoclavicular ligament; CP, coracoid process; ch, coracohumeral ligament; D, deltoid muscle; H, humeral head; SB, subscapularis muscle; SS, supraspinatus muscle; G, glenoid fossa; L, labrum; ss, supraspinatus tendon; b, tendon of long head of biceps muscle; IG, inferior glenohumeral ligament; mg, middle glenohumeral ligament; sb, subscapularis tendon; T, teres minor muscle.
Articular Joint Capsule
The articular joint capsule completely encloses the shoulder joint and is quite thin and loose to allow for extreme freedom of movement. When the arm is adducted, the capsule sags to form a pouchlike area termed the axillary recess (Figure 9.31). The capsule is attached medially to the glenoid fossa of the scapula and laterally to the anatomic neck of the humerus. The capsule is strengthened by several muscles and ligaments, including the rotator cuff muscles and the long head of the triceps brachii muscle, as well as the glenohumeral and coracohumeral ligaments. There are two openings of the joint capsule. The first is to allow for the transition of the long head of the biceps brachii and the second establishes a communication between the joint and the subscapularis bursa. A synovial membrane lines the fibrous capsule and extends from it onto the glenoid labrum and neck of the humerus. The synovial membrane provides a sheath for the tendon of the long head of the biceps brachii muscle, where it passes into the joint cavity through the intertubercular groove, extending as far as the surgical neck of the humerus (Figure 9.31).
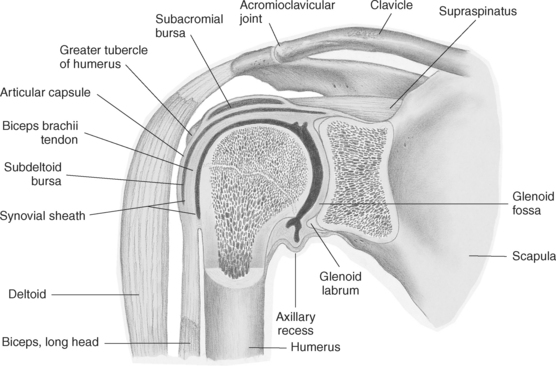
Bursae
The tendons and ligaments of the shoulder joint are cushioned by several fluid-filled bursae. Bursae, within the shoulder, reduce friction where large muscles and tendons pass across the joint capsule. Two prominent shoulder bursae include the subacromial-subdeltoid and subscapular bursae (Figure 9.32). The subacromial-subdeltoid bursa is the main bursa of the shoulder and the largest bursa within the body. Beginning at the coracoid process, the bursa extends laterally over the superior surface of the supraspinatus and infraspinatus tendon, extends beyond the acromion, and continues beneath the deltoid muscle to the greater tubercle of the humerus. This bursa cushions the rotator cuff muscles and coracoacromial arch (Figure 9.16). The subscapular bursa is located between the subscapularis tendon and the scapula and communicates with the synovial cavity through an opening in the joint capsule. This bursa protects the subscapularis tendon where it passes inferior to the coracoid process and over the neck of the scapula (Figure 9.32).
Muscles and Tendons
Numerous muscles and their tendons provide stability for the shoulder joint and movement of the upper arm. These can be separated into four muscle groups: (1) muscles that connect the upper limb to the vertebral column, (2) muscles of the scapula, (3) muscles that connect the upper limb to the anterior thoracic wall, and (4) the muscles of the upper arm.
Muscles Connecting the Upper Limb to the Vertebral Column
Muscles connecting the upper limb to the vertebral column include the following:
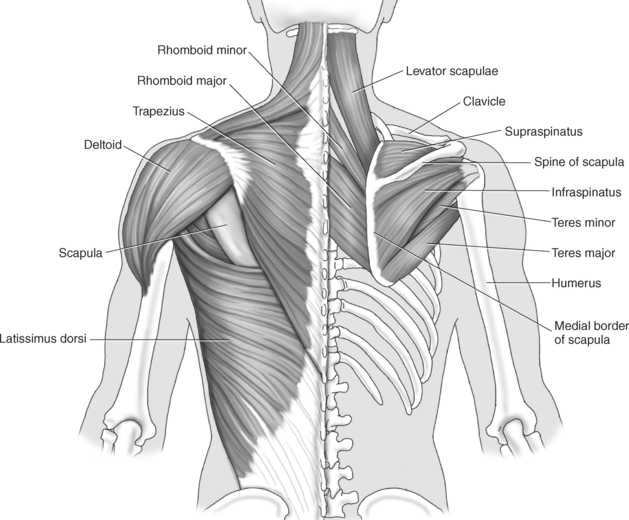
Muscles connecting the upper limb to the vertebral column are demonstrated in Figures 9.33 through 9.47 and are described in Table 9.1. The large triangular trapezius muscle covers the posterior aspect of the neck and superior half of the trunk (Figure 9.33). It connects the upper limb to the cranium via the external occipital protuberance and to the vertebral column via the spinous processes of C7-T12. The trapezius muscle functions to stabilize the scapula as well as elevate, retract, and depress the scapula. The levator scapulae muscle lies deep in the neck and functions to elevate and rotate the scapula. It extends from the transverse processes of C1-C4 to the superior angle and medial border of the scapula above its spine (Figure 9.33). The latissimus dorsi muscle covers the inferior portion of the back as it extends from the spinous processes of the inferior six thoracic vertebrae, iliac crest, and inferior three or four ribs to the distal end of the intertubercular groove of the humerus. The latissimus dorsi medially rotates, extends, and adducts the humerus. The rhomboid muscles, major and minor, lie deep to the trapezius muscle. The rhomboid major is wider than the rhomboid minor. They parallel each other as they span from the ligamentum nuchae and spinous processes of C7-T5 to the medial border of the scapula. They function to retract the scapula and fix the scapula to the thoracic wall (Figures 9.33 through 9.47).
Muscles of the Scapula
Muscles of the scapula include the following:
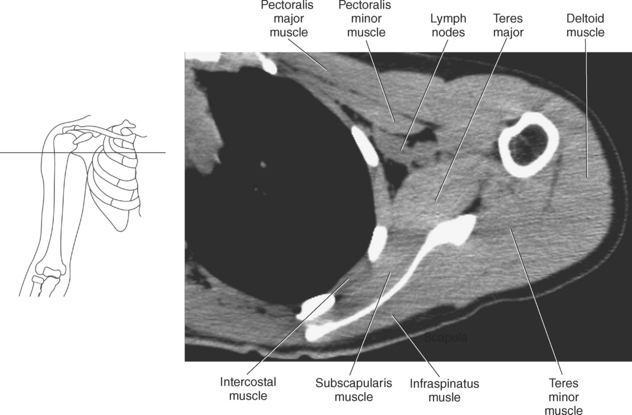
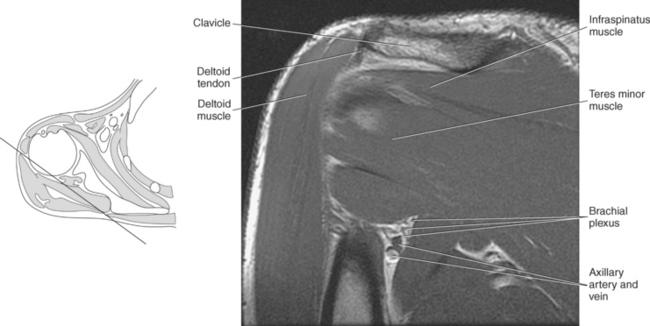
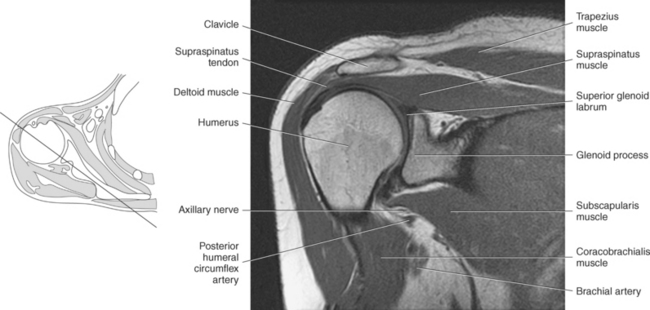
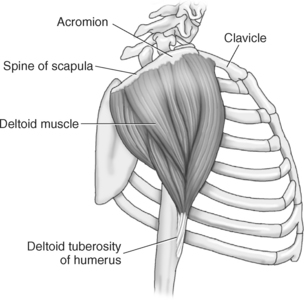
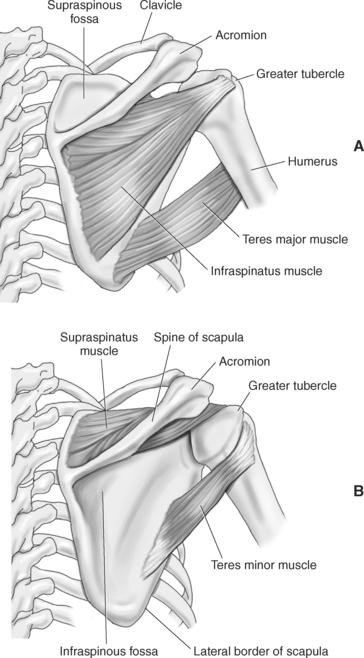
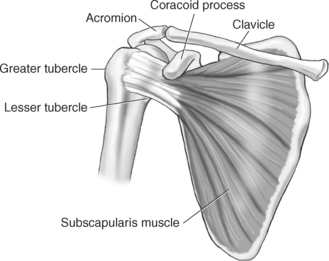
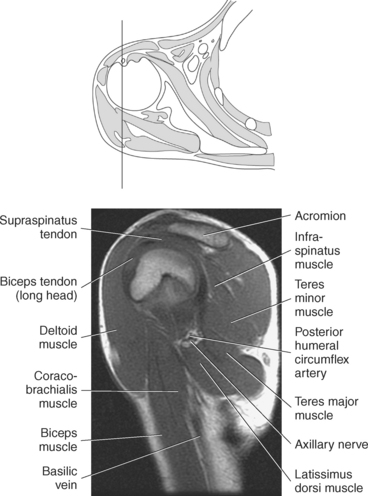
Muscles of the scapula are described in Table 9.2 and demonstrated in Figures 9.34 through 9.52. The large deltoid muscle originates on the clavicle, acromion, and scapular spine to blanket the shoulder joint as it extends to insert on the deltoid tuberosity of the humerus. This powerful muscle forms the rounded contour of the shoulder and functions primarily to abduct the arm (Figure 9.48). The teres major muscle is a flat rectangular muscle that adducts and medially rotates the arm. It extends from the inferior angle of the scapula to the medial aspect or lip of the intertubercular groove of the humerus (Figure 9.49, A). The four remaining muscles, supraspinatus, infraspinatus, teres minor, and subscapularis, closely surround the scapula and compose the rotator cuff (Figures 9.49 through 9.52). The rotator cuff provides dynamic stability to the shoulder joint and allows for adduction, abduction, and rotation of the humerus. The supraspinatus, infraspinatus, and teres minor muscles are located on the posterior aspect of the scapula. The tendons of these muscles insert on the greater tubercle of the humerus. The supraspinatus muscle lies in the supraspinous fossa of the scapula and helps to abduct the arm. The tendon of the supraspinatus muscle is the most frequently injured tendon of the rotator cuff because of possible impingement as it extends under the acromioclavicular joint and continues over the humeral head (Figure 9.49, B). The infraspinatus muscle is a triangular muscle that lies below the scapular spine in the infraspinous fossa. It acts to laterally rotate the arm (Figure 9.49, A). Lying along the inferior border of the infraspinatus muscle is the elongated teres minor muscle, which also acts to laterally rotate the arm (Figure 9.49, B). The subscapularis muscle is the only muscle of the rotator cuff located on the anterior surface of the scapula; its tendon inserts on the lesser tubercle of the humerus (Figures 9.50 through 9.52). The subscapularis muscle acts to medially rotate the humerus. See sequential images through the shoulder (Figures 9.34 through 9.47).

Muscles Connecting the Upper Extremity to the Anterior and Lateral Thoracic Walls
Muscles connecting the upper extremity to the anterior and lateral thoracic walls include the following:
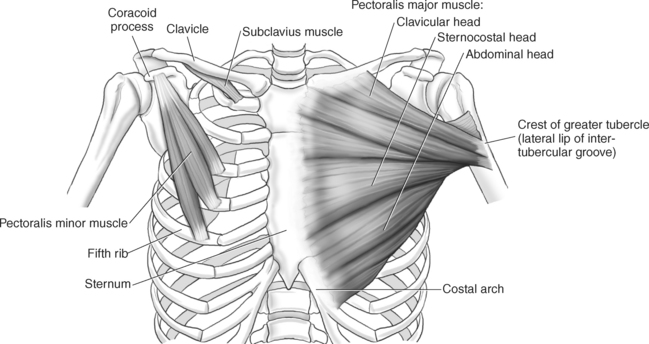
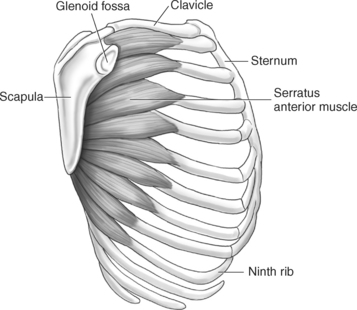
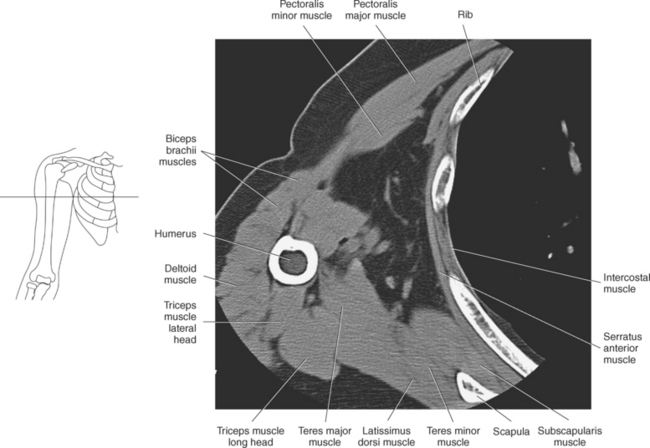
Muscles connecting the upper extremity to the anterior and lateral thoracic walls are demonstrated in Figures 9.34 through 9.47, 9.53, and 9.54 and described in Table 9.3. The pectoralis muscles (major and minor), located on the anterior surface of the chest, primarily aid in the movement of the upper limb (Figure 9.53). The large fan-shaped pectoralis major muscle covers the superior part of the thorax as it spans from the sternum, clavicle, and cartilaginous attachments of the upper six ribs to the lateral aspect or lip of the intertubercular groove of the humerus. Its primary functions are to adduct, medially rotate, flex, and extend the humerus and to assist in forced inspiration. The smaller triangular-shaped pectoralis minor lies beneath the pectoralis major muscle and acts to depress the scapula and assist the serratus anterior muscle in pulling the scapula forward (Figure 9.53). The serratus (sawlike) anterior muscle is visualized on the lateral border of the thorax. It extends from the first rib through eighth rib to the medial border of the scapula. The primary action of the serratus anterior muscle is to protract and stabilize the scapula (Figure 9.54). The subclavius, a small triangular-shaped muscle that spans between the first rib and clavicle, acts to stabilize the clavicle and depress the shoulder (Figure 9.53).

Muscles of the Upper Arm
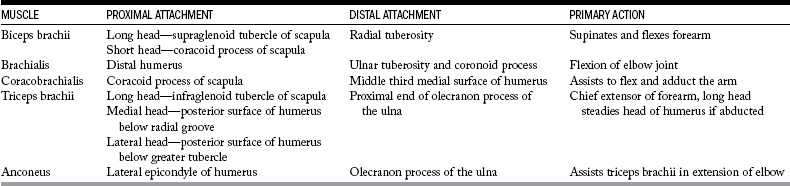
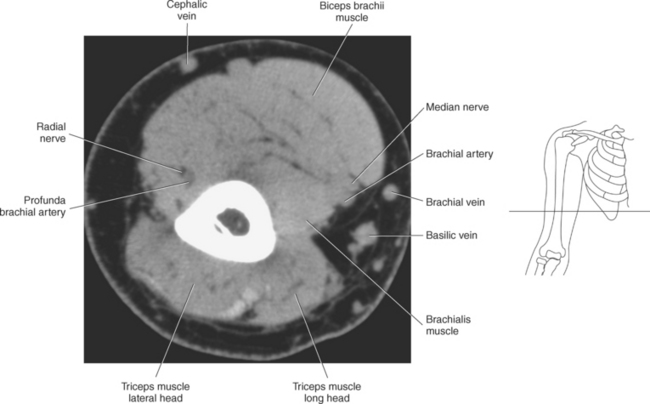
The muscles of the upper arm can be divided into ventral and dorsal groups according to their position. The ventral group contains the biceps brachii, brachialis, and coracobrachialis muscle, and the dorsal group consists of the triceps brachii and anconeus muscles. These muscles are demonstrated in Figures 9.55 through 9.69 and described in Table 9.4.
Ventral Group
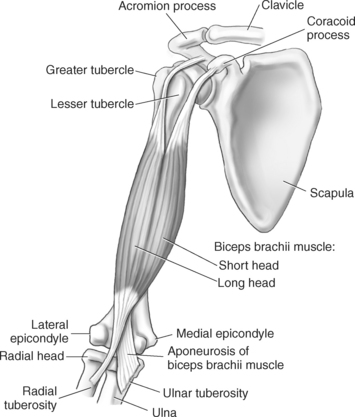
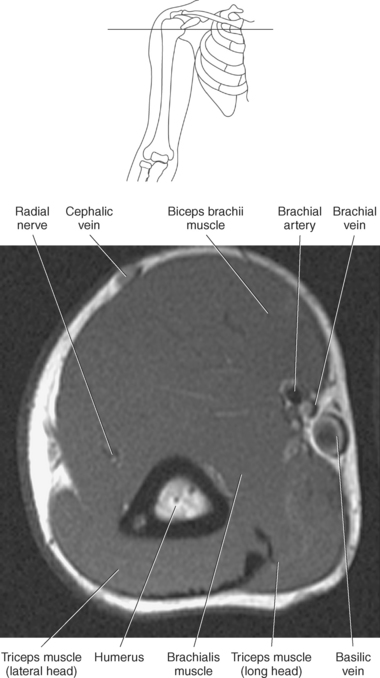
The biceps brachii muscle is located on the anterior surface of the humerus and acts as a strong flexor of the forearm. The biceps brachii muscle is so named “biceps” because of its two expanded heads of proximal attachment (long and short). The tendon of the long head arises from the supraglenoid tubercle and courses through the intertubercular (bicipital) groove to merge with the tendon from the short head. The short head of the biceps brachii muscle originates from the coracoid process and joins with the long head to create the biceps brachii muscle, which terminates in two tendons. The stronger tendon inserts on the radial tuberosity, and the other tendon creates the bicipital aponeurosis, which radiates into the fascia of the forearm (Figure 9.55).
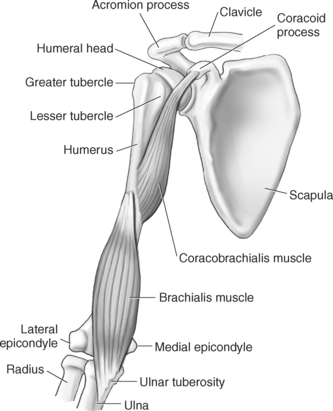
The brachialis muscle originates from the anterior surface of the distal humerus and covers the anterior surface of the elbow joint before inserting on a roughened area of the proximal and anterior surface of the ulna termed the ulnar tuberosity and the coronoid process. The brachialis muscle is considered to be the most important flexor muscle of the elbow joint (Figure 9.56). The coracobrachialis is a long, narrow muscle located in the superomedial aspect of the arm. It arises from the coracoid process along with the short head of the biceps brachii and extends to insert on the medial surface of the humerus. The primary action of the coracobrachialis muscle is to assist with flexion and adduction of the arm, but it also helps hold the head of the humerus within the joint capsule (Figures 9.56 through 9.67).
Dorsal Group
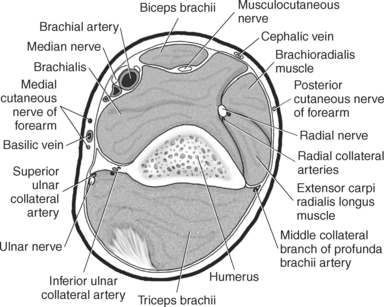
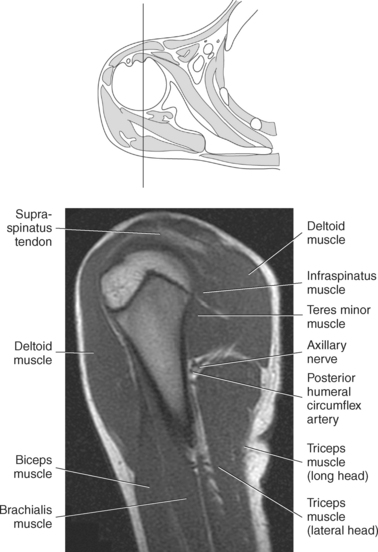
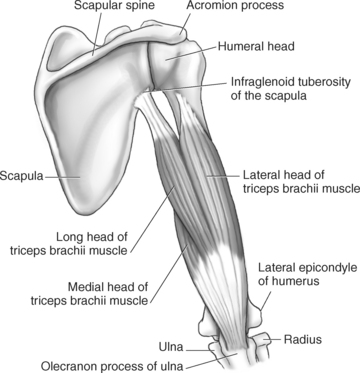
The triceps brachii muscle is located on the posterior surface of the humerus and is the main extensor of the forearm. Its name triceps is associated with three heads of proximal attachment (long, lateral, and medial). The long head of the triceps originates from the infraglenoid tubercle of the scapula, the medial head originates from the entire dorsal surface of the humerus distal to the radial groove, and the lateral head arises from the dorsal surface and lateral intermuscular septum of the humerus. All three heads join in a common tendon that inserts on the olecranon process of the ulna and the posterior joint capsule (Figure 9.68). The small, triangular anconeus muscle originates on the lateral epicondyle and crosses obliquely to insert on the dorsal surface of the olecranon process, close to the tendon of the triceps brachii (Figure 9.69). It assists the triceps brachii in extension and also provides dynamic joint stability to the lateral joint capsule. For images of the upper arm, see Figures 9.57 through 9.67.
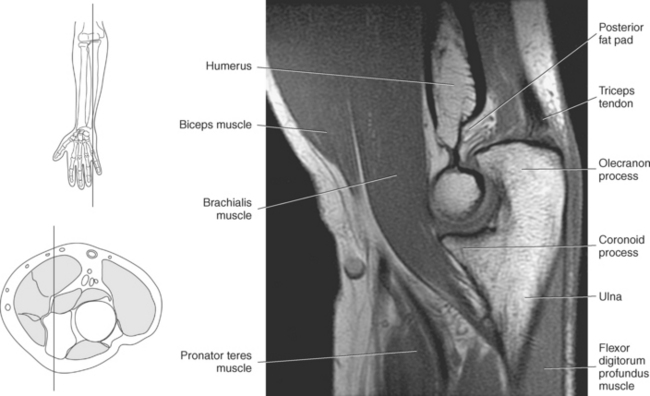
ELBOW
The elbow is a complex hinge-pivot joint created by the articulations of the humerus, radius, and ulna. All three articulations communicate with each other within a single joint capsule. The radius and ulna are the bones of the forearm, with the radius located on the lateral side. The radioulnar and radiohumeral articulations create the pivot joint that aids in supination and pronation of the elbow. The radiohumeral and ulnohumeral articulations form the hinge joint that allows for flexion and extension (Figures 9.70 through 9.73).
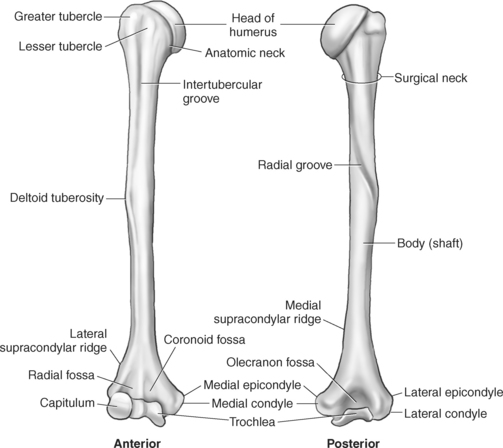
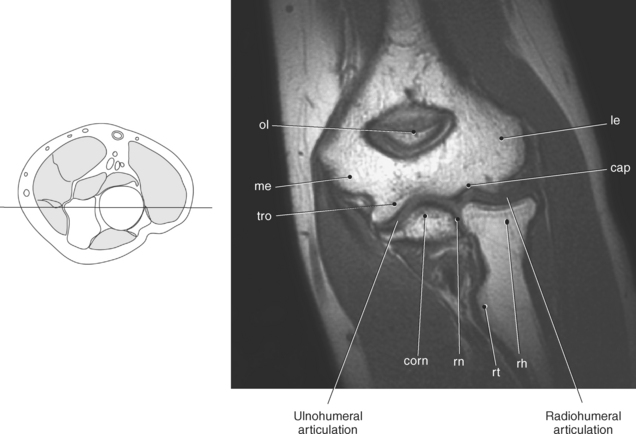
Figure 9.71 Coronal T1-weighted MR scan of elbow.
Key: ol, Olecranon fossa; me, medial epicondyle; tro, trochlea; le, lateral epicondyle; cap, capitellum; rh, radial head; rt, radial tuberosity; rn, radial notch; corn, coronoid process.
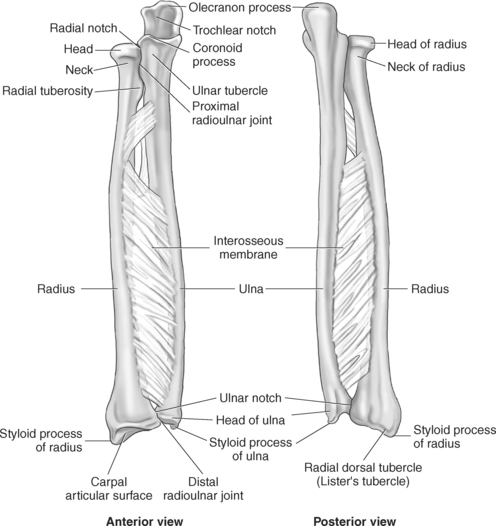
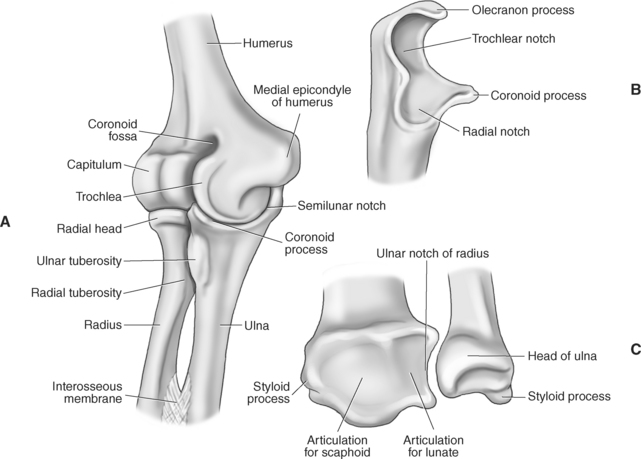
Figure 9.73 Anatomy of the elbow and distal forearm. A, Elbow in medial view. B, Proximal ulna in lateral view. C, Distal radius and ulna.
Bony Anatomy
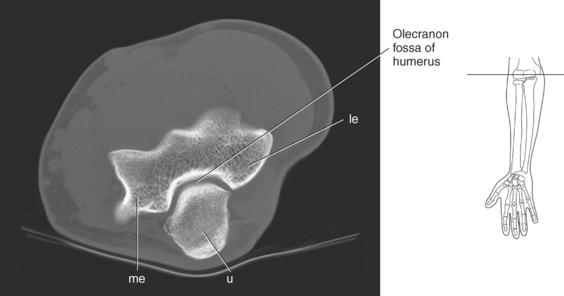
The distal portion of the humerus has two distinct prominences termed the medial and lateral condyles, with associated epicondyles, that provide attachment sites for tendons and ligaments (Figure 9.70). The medial epicondyle serves as the site of origin for the common flexor tendon, pronator teres muscle, and medial collateral ligament, whereas the lateral epicondyle serves as the attachment site for the common extensor tendon, supinator muscle, and lateral collateral ligament. Just lateral to the medial epicondyle along its posterior surface is a shallow groove containing the ulnar nerve. Two depressions located on the distal humerus are the anterior coronoid fossa and the deep posterior olecranon fossa. These depressions accommodate the coronoid and olecranon processes of the proximal ulna (Figures 9.70, 9.71, and 9.73). The distal humerus has two cartilage-covered articular surfaces—the capitellum and the trochlea for articulation with the radius and ulna (Figure 9.71). The lateral of the two surfaces is the capitellum, a rounded projection that articulates with the concave surface of the radial head. The trochlea is more medial and has the appearance of an hourglass if viewed in the horizontal plane. The shape of the trochlea helps keep the ulna in position during flexion between the distal humerus and proximal radius (Figure 9.73).
Radius: Proximal Radius
The radius is a long, slender bone with a proximal portion that consists of the radial head, neck, and tuberosity. The radial head has a flat cartilage-covered depression or fossa (fovea of the radius) that articulates with the capitellum of the humerus. In addition, the articular circumference of the radial head articulates against the radial notch of the ulna during supination and pronation. The radial head is attached to the body of the radius by the narrow radial neck. Located at the distal portion of the neck on the medial side of the radius is a roughened projection termed the radial tuberosity. The radial tuberosity serves as the attachment point for the biceps brachii muscle (Figures 9.72 through 9.74).
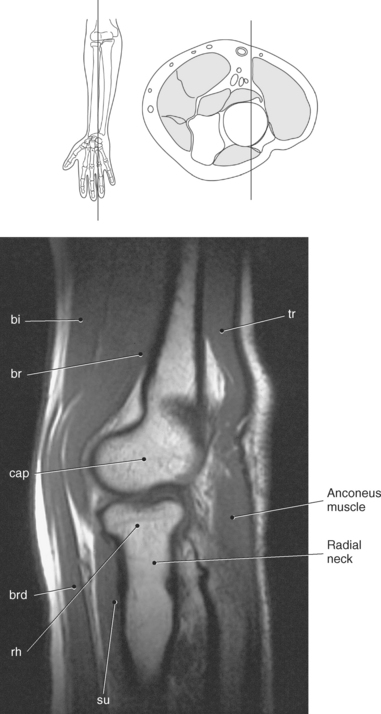
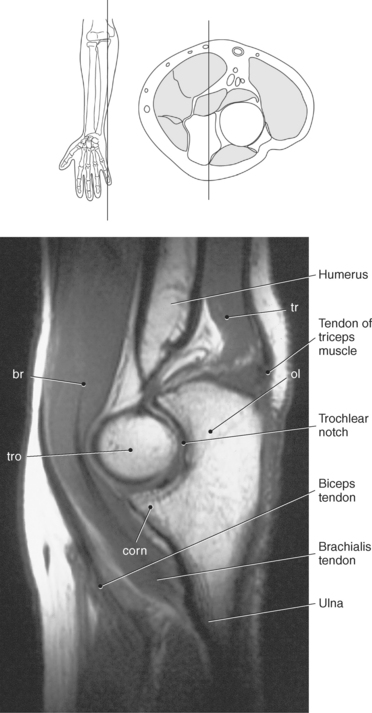
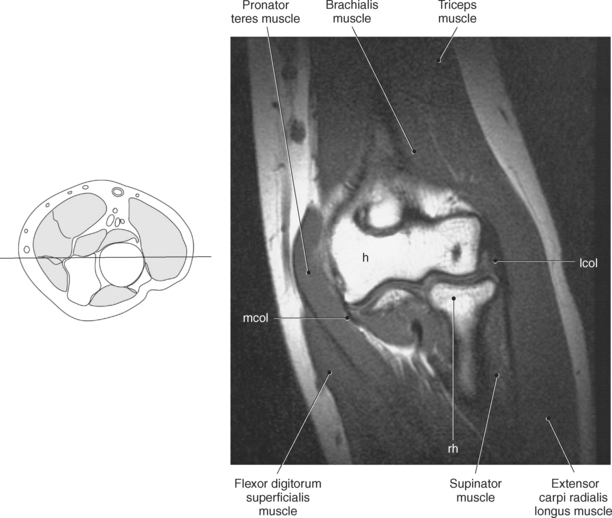
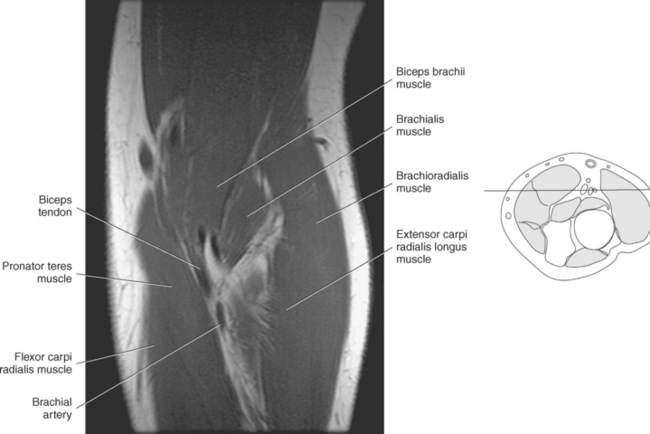
Figure 9.74 Sagittal, T1-weighted MR scan of elbow with proximal radius.
Key: bi, Biceps; br, brachialis; cap, capitellum; brd, brachioradialis; rh, radial head; su, supinator; tr, triceps; ol, olecranon fossa; tro, trochlea; corn, coronoid process; le, lateral epicondyle; u, ulna; me, medial epicondyle.
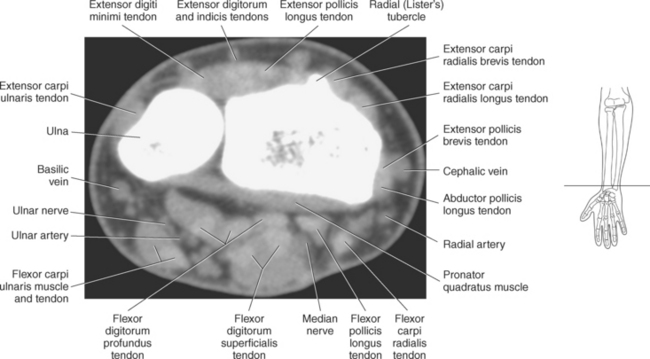
Distal Radius
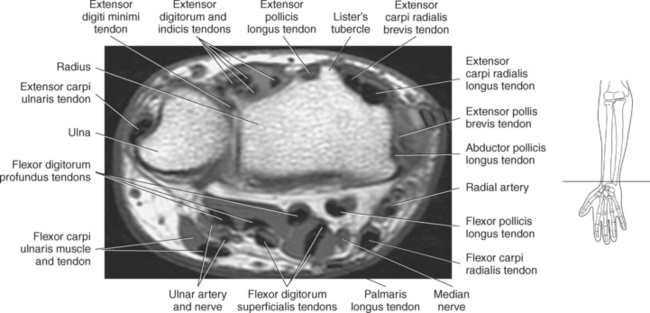
The broadened distal end of the radius includes the cartilage-covered carpal articular surface, the ulnar notch, and the radial styloid process. The carpal articular surface articulates with the scaphoid and lunate bones of the wrist. The ulnar notch articulates with the ulna, and the styloid process serves as an attachment site for the extensor pollicis longus and extensor carpi radialis tendons. The dorsal surface of the radius contains several grooves that serve as passages for the extensor tendons. Along with the grooves, a prominent ridge is located on the dorsal surface termed the radial dorsal tubercle, or Lister’s tubercle, a common site for the formation of bony spurs (Figure 9.72).
Ulna: Proximal Ulna
The ulna is located medial within the forearm. The proximal ulna consists of the olecranon and coronoid processes and the trochlear and radial notches. The superficial dorsal surface is formed by the hook-shaped olecranon process, which is the attachment site for the triceps brachii. The trochlear notch is a half-moon-shaped concave articular surface that curves around the trochlea of the humerus. This articulation allows for flexion and extension of the elbow. Located on the anterior portion of the distal end of the trochlear notch is a small beaklike process called the coronoid process. Just distal and lateral to the coronoid process is a flattened depression called the radial notch. It is covered by articular cartilage for articulation with the radial head. Immediately distal to the coronoid process is a roughened bony surface termed the ulnar tuberosity. The tendon of the brachialis muscle inserts on both the coronoid process and the ulnar tuberosity (Figures 9.72, 9.73, 9.75, and 9.76).
Ulna: Distal Ulna
The smaller, distal end of the ulna has two prominent projections. The larger, rounded projection is an articular eminence termed the head of the ulna. It articulates with the ulnar notch of the radius and the triangular fibrocartilage complex. The small conical projection on the medial surface is called the ulnar styloid process, which serves as the attachment site for the ulnar collateral ligament of the wrist. Another structure that is important in stabilizing and strengthening the connection between the radius and ulna is the interosseous membrane, a strong fibrous sheath stretching between the interosseous borders of both bones (Figure 9.72, A and B).
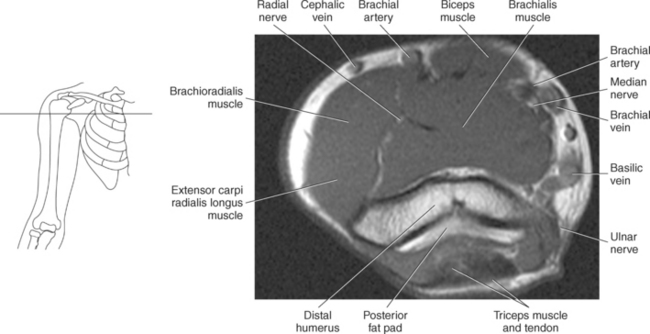
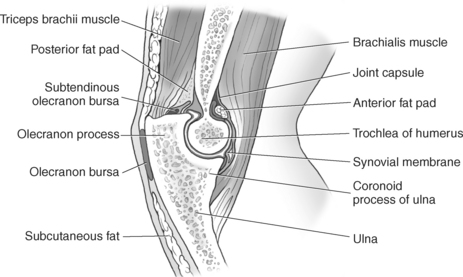
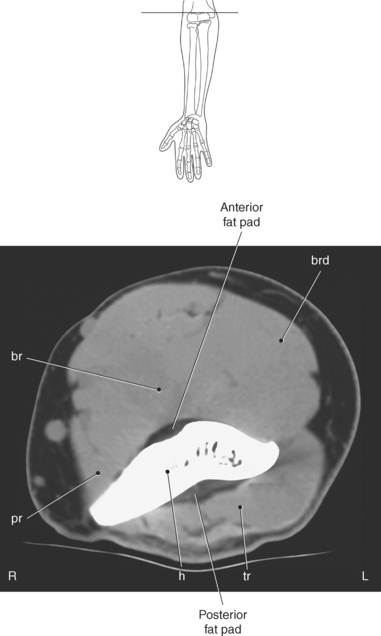
Joint Capsule and Fat Pads
The entire elbow joint is surrounded by a relatively loose joint capsule that allows for the movements of flexion and extension. The joint capsule is weaker anteriorly and posteriorly but is reinforced medially and laterally by the strong radial and ulnar collateral ligaments (discussed in the next section). Located within the olecranon and coronoid fossas are fat pads that fill the space between the synovial membrane and joint capsule (Figures 9.77 and 9.78). The fat pads help cushion the area where the olecranon and coronoid processes move during flexion and extension of the elbow. There are two clinically important bursae located in the elbow: the olecranon bursa and the distal bicipitoradial bursa. The olecranon bursa is located within the subcutaneous tissue overlying the olecranon process (Figure 9.77). The distal bicipitoradial bursa lies between the insertion of the biceps tendon and the humerus.
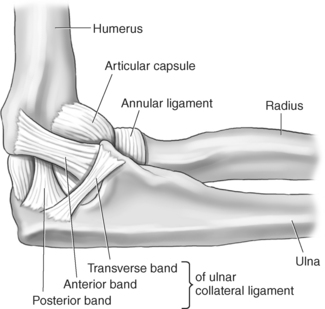
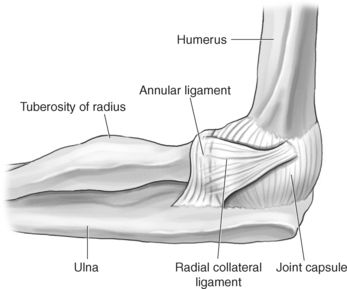
Ligaments
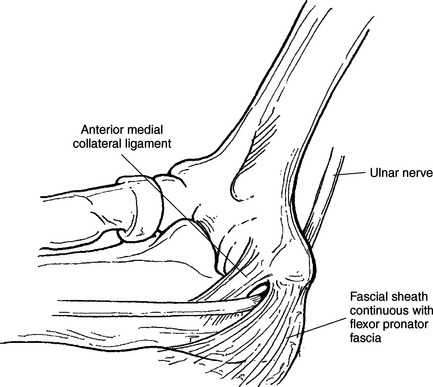
The stability of the elbow joint primarily depends on the collateral ligaments that are woven into the lateral portions of the joint capsule. The ulnar collateral ligament (medial collateral ligament) consists of three components: an anterior band, a posterior band, and a transverse band (ligament of Cooper) (Figures 9.79 through 9.82). The anterior band, which is the strongest, extends from the medial epicondyle of the humerus to the medial aspect of the coronoid process. The posterior band originates along with the anterior band from the medial epicondyle of the humerus and inserts on the medial aspect of the olecranon process, forming a triangular plate. The weaker transverse band stretches between the medial surfaces of the coronoid and olecranon processes to unite the anterior and posterior bands. Reinforcing the lateral side is the triangular radial collateral ligament (lateral collateral ligament). The radial collateral ligament originates from the lateral epicondyle of the humerus, adjacent to and beneath the common extensor tendons, and spreads distally to insert on the annular ligament and the anterior and posterior margins of the radial notch of the ulna (Figures 9.81 and 9.83). The annular ligament forms a fibrous ring that encircles the radial head, with a narrow portion that tightens around the radial neck to prevent inferior displacement of the radius (Figures 9.79 and 9.83 through 9.85). The annular ligament is considered a key structure in the proximal radioulnar joint, allowing the head of the radius to rotate freely. Just distal to the annular ligament is the quadrate ligament, a small band of tissue that passes from the radial notch of the ulna to the neck of the radius to provide stability to the joint during supination and pronation.
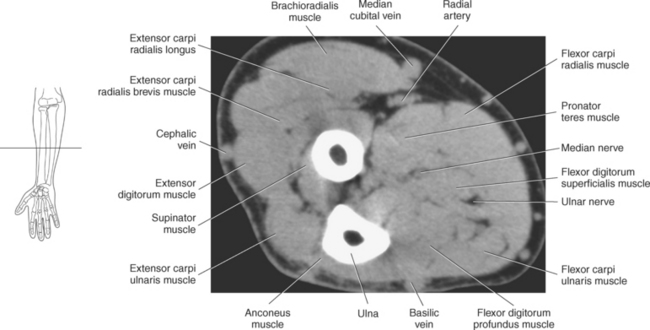
Muscles of the Forearm
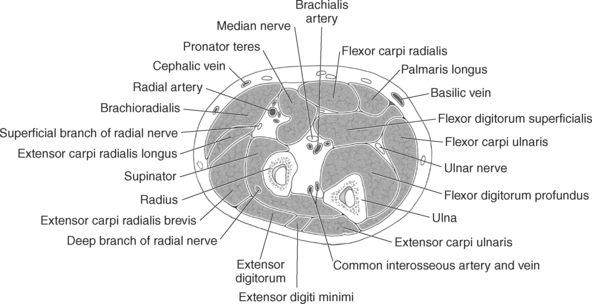
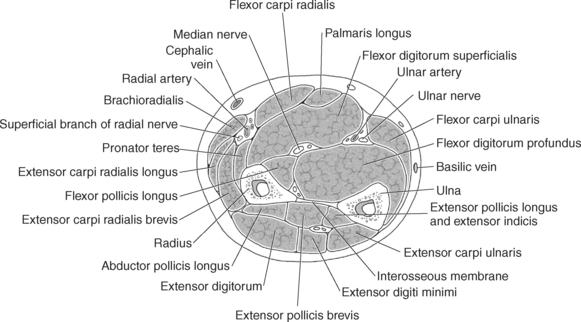
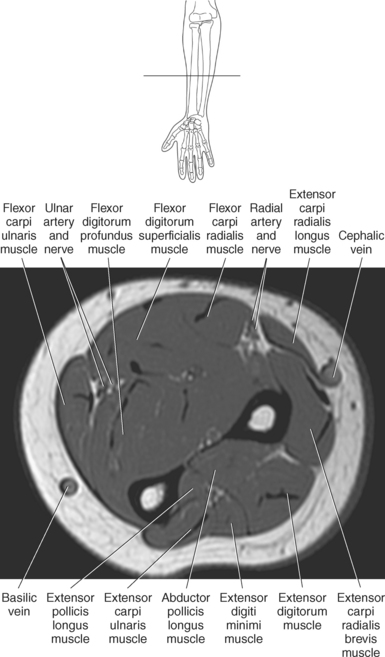
One method to classify the muscles of the forearm is to use the radius, ulna, and interosseous membrane to divide them into a ventral group (the flexors) and a dorsal group (the extensors). The two groups can be further divided into superficial and deep muscles. The muscles of the forearm are described in Table 9.5.
Ventral Group—Superficial Muscles
All five of the superficial muscles in the ventral group have an origin from the common flexor tendon off the medial epicondyle of the humerus. These muscles are demonstrated in Figures 9.86 through 9.98.
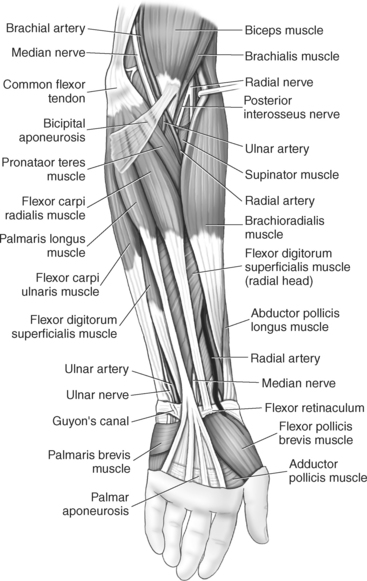
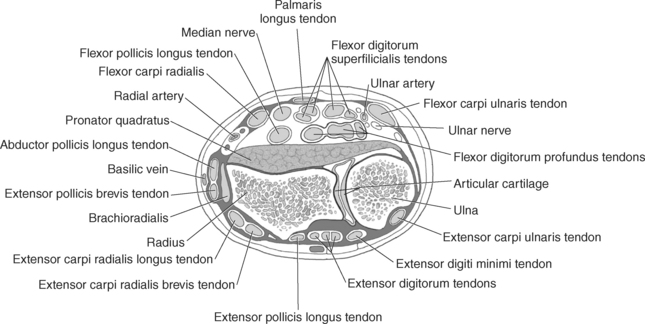
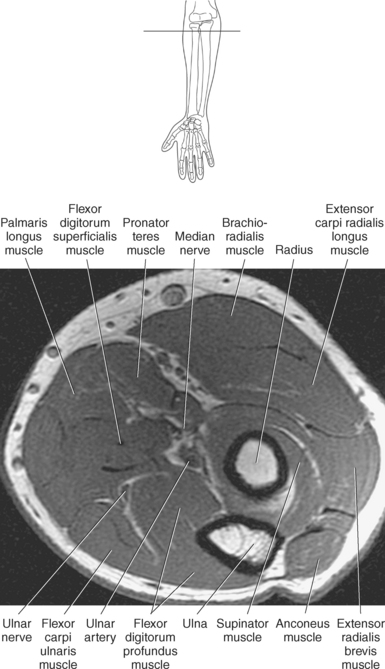
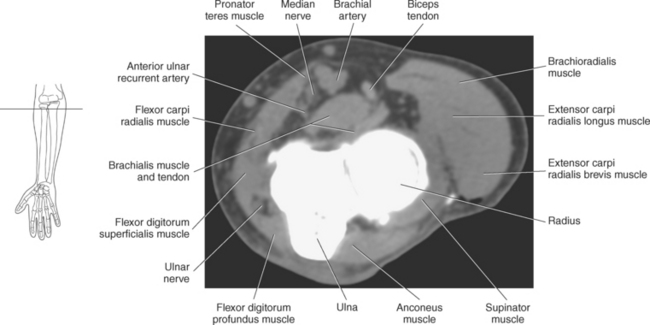
The pronator teres muscle has two heads of origin. Its humeral head originates from the common flexor tendon, whereas the ulnar head originates near the coronoid process of the ulna. The pronator teres muscle courses obliquely before inserting on the lateral surface of the radius at midshaft. It works in conjunction with the pronator quadratus muscle to pronate the forearm (Figure 9.86).
The flexor carpi radialis muscle originates from the common flexor tendon and is located medial to the pronator teres. Its tendon passes through the carpal tunnel before inserting on the palmar surface of the base of the second metacarpal. Its actions include flexion and radial deviation of the hand at the wrist joint (Figure 9.86).
The palmaris longus muscle originates from the common flexor tendon and passes superficial to the flexor retinaculum to merge with the palmar aponeurosis. It acts to flex the hand and tighten the palmar aponeurosis (Figure 9.86).
The flexor carpi ulnaris muscle is the most medial of the superficial muscles located in the anterior compartment of the forearm. It has two heads: The humeral head originates from the common flexor tendon, and the ulnar head originates from the olecranon process. It inserts onto the pisiform, hook of the hamate, and fifth metacarpal and acts to flex and adduct (ulnar deviation) the hand at the wrist joint (Figure 9.86).
The flexor digitorum superficialis muscle is the largest muscle of the superficial muscles in the forearm. It arises from three heads: the humeral head from the common flexor tendon, the ulnar head from the coronoid process, and the radial head from the anterior surface of the proximal half of the radius. Just before reaching the flexor retinaculum, the muscle divides into four tendons that share a common synovial sheath through the carpal tunnel. After passing under the flexor retinaculum, the tendons insert on the lateral sides of the middle phalanges of the second to fifth digits. The flexor digitorum superficialis is a strong flexor of the middle and proximal phalanges of the second through fifth digits (Figure 9.86).
Ventral Group—Deep Muscles
The muscles of the ventral group are demonstrated on Figures 9.97 through 9.99. The flexor digitorum profundus muscle is a long, thick muscle responsible for flexing the distal interphalangeal joints of the fingers. It originates from the anterior surface of the proximal ulna and extends medially to the interosseous membrane. Similar to the flexor digitorum superficialis, the flexor digitorum profundus divides into four tendons before reaching the flexor retinaculum. The four tendons pass deep in the carpal tunnel and continue distally to insert on the distal phalanges, where they pair up with the flexor digitorum superficialis to provide flexion of the middle and proximal phalanges of the second through fifth digits (Figure 9.99, B).
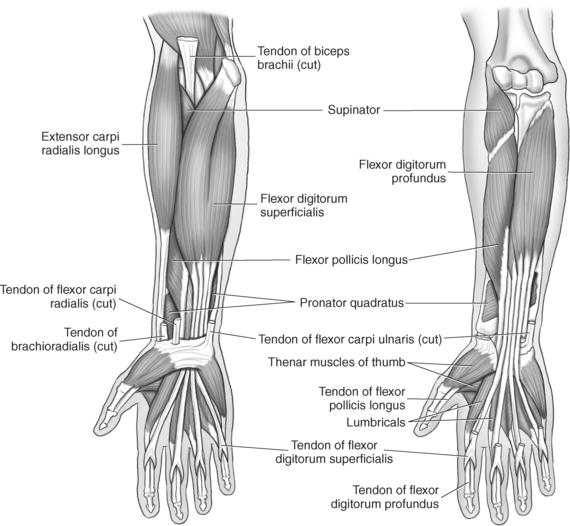
The flexor pollicis longus muscle arises from the anterior surface of the radius and adjacent interosseous membrane and runs lateral to the flexor digitorum profundus to cover the anterior aspect of the radius. After passing through the carpal tunnel, the flexor pollicis longus tendon runs between the flexor pollicis brevis and adductor pollicis brevis muscles to insert on the base of the first distal phalanx (Figure 9.99, A and B).
The pronator quadratus, a quadrangular muscle, is the deepest muscle in the anterior aspect of the forearm. It arises from the anterior and radial aspect of the distal ulna and passes transversely to insert on the anterior surface of the distal radius. The deep fibers of this muscle help bind the radius and ulna together along with the interosseous membrane. The pronator quadratus is the prime mover in pronation of the forearm (Figure 9.99).
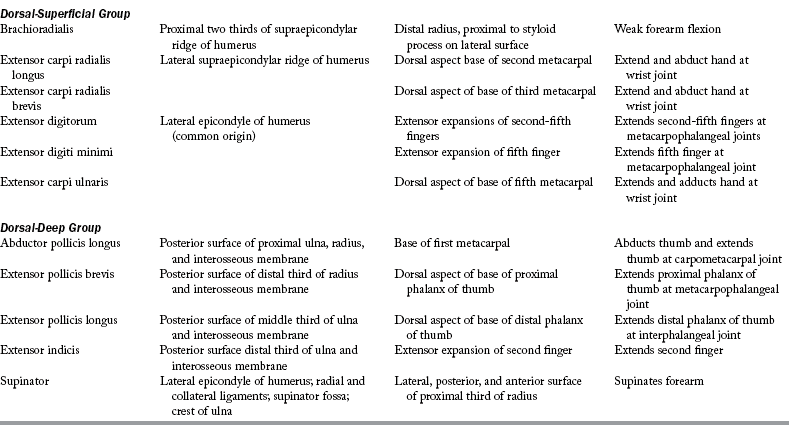
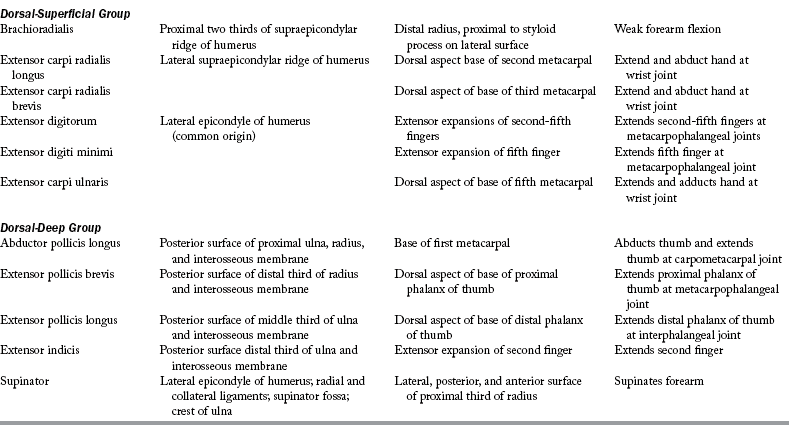
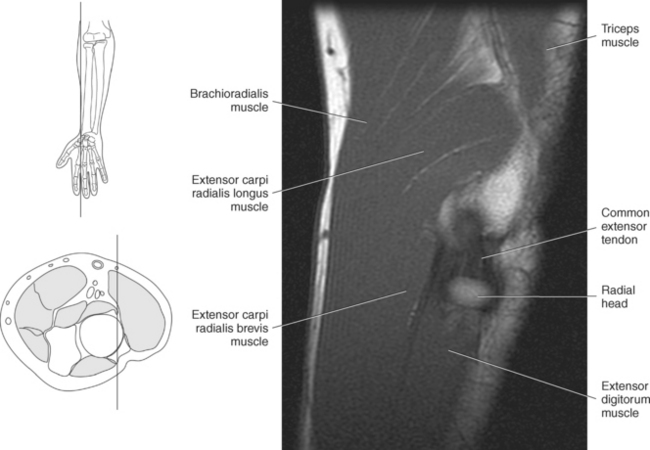
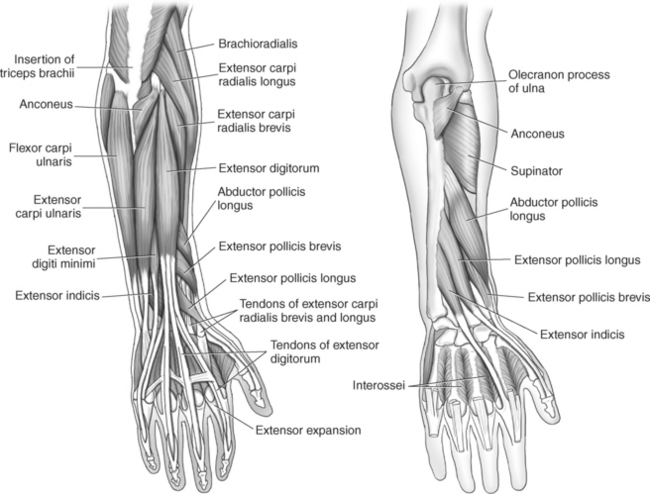
Dorsal Group—Superficial Muscles
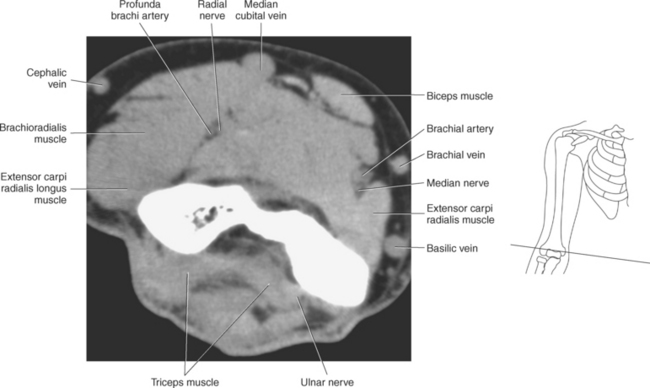
The muscles of the superficial dorsal group are demonstrated in Figures 9.87 through 9.98 and 9.100. The brachioradialis is an extensor muscle lying along the lateral border of the forearm. This large muscle arises from the upper two thirds of the supracondylar ridge of the humerus and attaches distally to the radial styloid process. The brachioradialis flexes the forearm at the elbow and assists with pronation and supination (Figure 9.100).
The extensor carpi radialis longus muscle arises just distal to the brachioradialis on the lower third of the supracondylar ridge of the humerus. It runs posterior and deep to the brachioradialis to insert on the base of the second metacarpal. It acts as an extensor and abductor of the hand at the wrist joint (Figure 9.100).
The other superficial muscles (extensor carpi radialis brevis, extensor carpi ulnaris, extensor digitorum, extensor digiti minimi) arise from a common extensor tendon attached to the lateral epicondyle of the humerus. At the level of the elbow they appear as one structure but become more distinct distally as they insert on various structures about the wrist and hand.
The extensor carpi radialis brevis has components that arise from the radial collateral and annular ligaments as well as the common extensor tendon. It runs along the dorsal surface of the wrist to insert on the base of the third metacarpal and acts to extend and abduct the hand at the wrist joint (Figure 9.100).
The extensor digitorum muscle is the main extensor of the second to fifth digits and occupies much of the posterior surface of the forearm. It arises from the common extensor tendon and divides into four individual tendinous slips just proximal to the wrist. The four tendons run in a single synovial sheath as they pass under the extensor retinaculum. The tendons insert into the extensor expansions of the second through fifth digits, helping to form the extensor hoods (see the section on ligaments of the finger). In addition, small slips of the tendon spread out and run to the bases of the proximal phalanges and to the capsules of the metacarpophalangeal joints (Figure 9.100). The extensor digitorum muscle extends and spreads the fingers and extends the hand at the wrist joint. The extensor digiti minimi muscle arises from the common extensor tendon and passes under the extensor retinaculum in its own synovial compartment. It then divides into two tendinous slips that insert on the proximal phalanx of the fifth digit to help with extension of the little finger (Figure 9.100).
The extensor carpi ulnaris is a long, slender muscle that arises from the common extensor tendon and runs along the medial and dorsal side of the ulna to insert on the base of the fifth metacarpal. Its main actions include extension of the hand at the wrist joint and adduction of the hand, resulting in ulnar deviation (Figure 9.100).
Dorsal Group—Deep Muscles
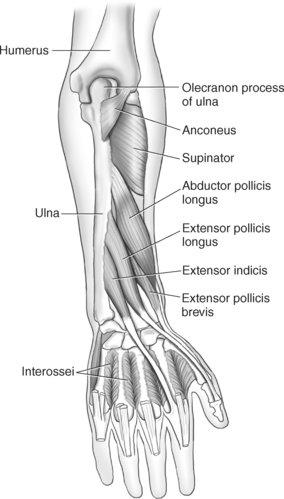
The deep muscles of the dorsal group consists of four extensors that act on either the first or second digit and includes the supinator muscle. These muscles are demonstrated in Figures 9.87 through 9.98 and 9.100.
The three deep extensors that act on the first digit are the abductor pollicis longus, extensor pollicis brevis, and the extensor pollicis longus muscles. The long, slender abductor pollicis longus muscle arises from the dorsal surfaces of the ulna and radius and from the interosseous membrane. It inserts on the base of the first metacarpal to abduct and extend the thumb (Figure 9.100).
The short extensor pollicis brevis muscle arises from the dorsal surfaces of the ulna and radius and from the interosseous membrane just distal to the abductor pollicis longus muscle. It inserts on the base of the proximal phalanx of the first digit and works together with the abductor pollicis longus to extend and abduct the thumb (Figure 9.100).
The extensor pollicis longus muscle arises from the dorsal surface of the ulna and interosseous membrane just distal to the abductor pollicis longus muscle. After passing through the extensor retinaculum, it crosses over the extensor carpi radialis longus and brevis to insert on the base of the distal phalanx of the first digit. Its main action is to extend the distal phalanx of the first digit, but it can also abduct the hand (Figure 9.100).
The extensor indicis muscle arises from the distal third of the dorsal ulna and the interosseous membrane and runs with the extensor digitorum muscle through the extensor retinaculum to insert on the dorsal aponeurosis of the second digit. It functions with the extensor digitorum muscle to extend the index finger, as if pointing (Figure 9.100).
The supinator muscle originates from two heads: oblique and transverse. The oblique head originates from the lateral epicondyle and collateral ligament, whereas the transverse head originates from the supinator crest of the ulna. Both heads wrap laterally around the proximal radius to insert on the posterolateral and anterior surfaces of the proximal radius to supinate the forearm (Figure 9.100).
WRIST AND HAND
The complex anatomy of the wrist and hand provides for a multitude of movements unmatched by any other joints of the body.
Bony Anatomy
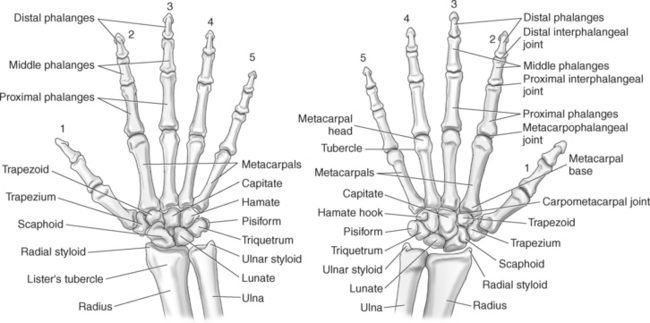
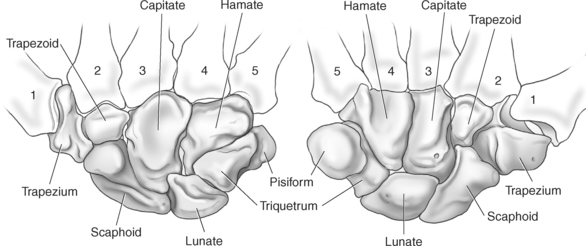
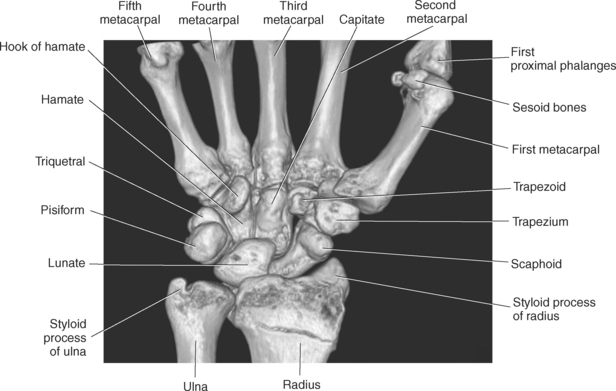
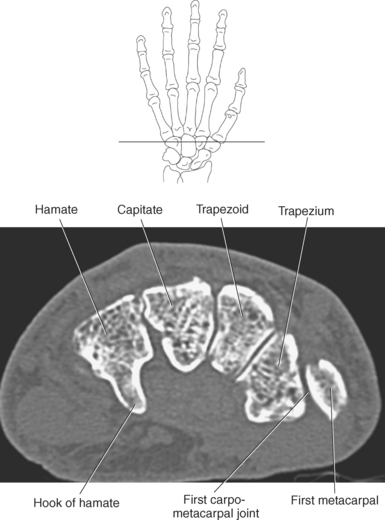
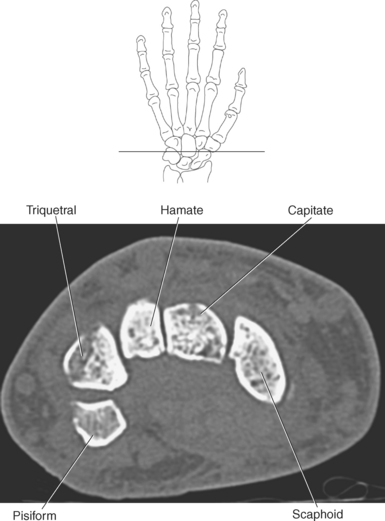
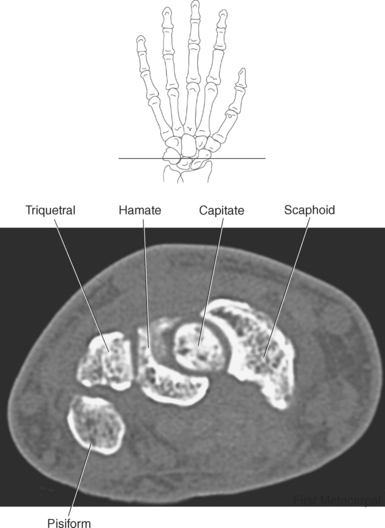
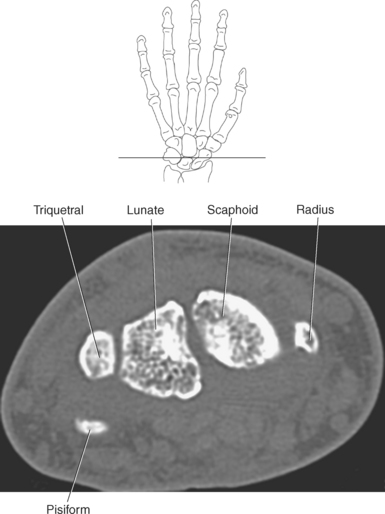
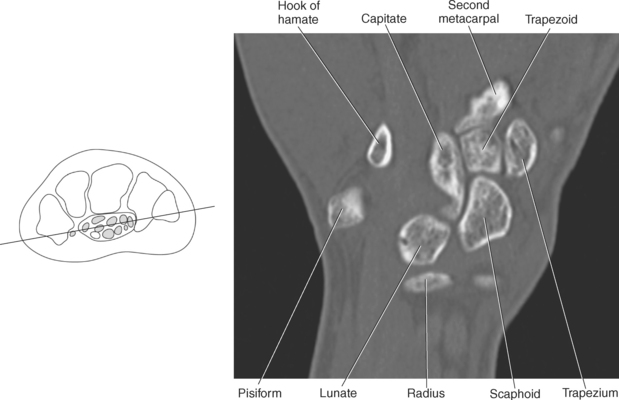
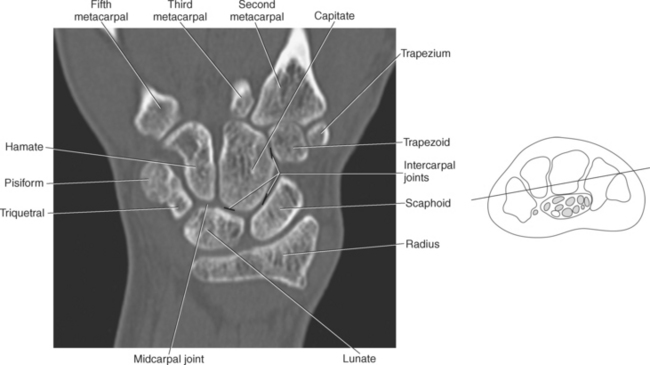
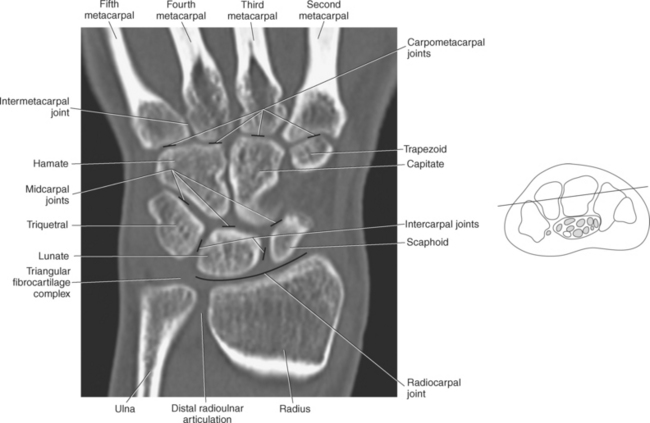
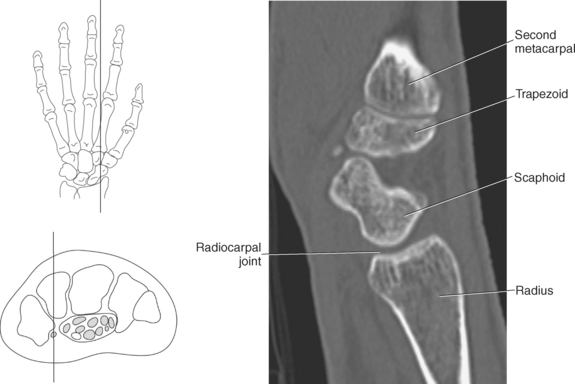
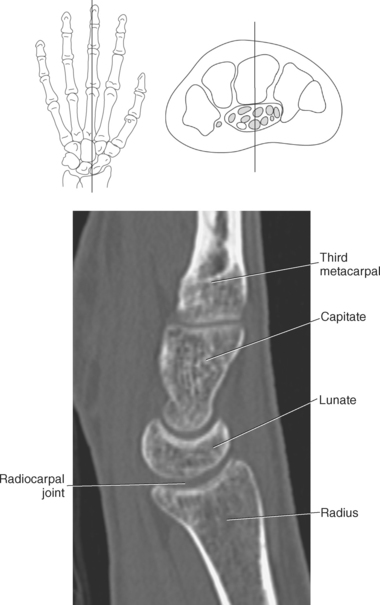
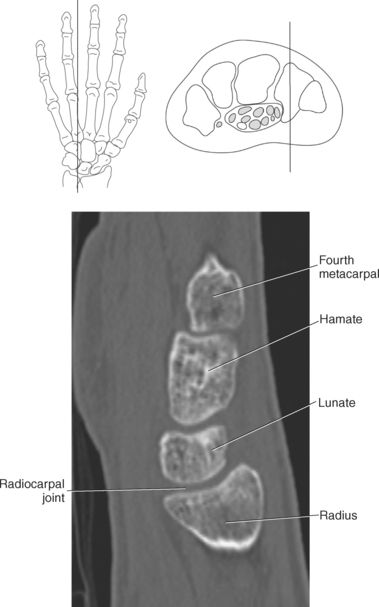
The bony anatomy of the wrist and hand consists of the distal radius and ulna, 8 carpal bones, 5 metacarpals, and 14 phalanges (Figure 9.101). Both the distal radius and ulna have a conical styloid process that acts as an attachment site for ligaments. The radial styloid process is located on the lateral surface of the radius, whereas the ulnar styloid process is located on the posteromedial side of the ulna. The carpal bones are arranged in proximal and distal rows. Located in the proximal row of carpal bones are the scaphoid (navicular), lunate (semilunar), triquetral (triquetrum), and pisiform bones. The pisiform is considered a sesamoid bone that is embedded in the tendon of the flexor carpi ulnaris. The distal row consists of the trapezium (greater multangular), trapezoid (lesser multangular), capitate (os magnum), and hamate (unciform) bones (Figures 9.102 through 9.114). The five metacarpals are small tubular bones with a proximal end (base), distal end (head), and shaft (body). The 14 phalanges that make up the fingers are short tubular bones. Like the metacarpals, each phalanx consists of a proximal (base), middle (body or diaphysis), and distal (head) portion. Each digit consists of 3 phalanges (proximal, middle, and distal), except for the thumb (first digit), which has only 2 phalanges (proximal and distal). The articulation of the phalanges of the second through fifth digits creates three interphalangeal joints: the metacarpophalangeal (MCP) joints classified as condyloid joints, proximal interphalangeal (PIP), and distal interphalangeal (DIP). The proximal and distal interphalangeal joints are classified as hinge joints (Figure 9.101). The first digit, which consists of 2 phalanges, has just two joints: the MCP joint, classified as a saddle joint, and an interphalangeal joint, classified as a hinge joint (Figure 9.101).
Joints
The joints of the wrist and hand are quite complex and consist of the following: distal radioulnar articulation, radiocarpal articulation (proximal joint of hand), midcarpal articulation (distal joint of hand), intercarpal articulations (articulations between proximal and distal carpals), carpometacarpal articulations (between carpals and metacarpals), the intermetacarpal articulations (between bases of metacarpals two through five) and the interphalangeal joints (between phalanges of each digit) (Figures 9.111 and 9.115). The distal radioulnar articulation, also called the distal radioulnar joint (DRUJ), is created when the ulnar notch of the radius moves around the articular circumference of the ulna, providing the movements of supination and pronation. The main stabilizing element of the DRUJ is an articular disk called the triangular fibrocartilage complex (TFCC). The TFCC is a fan-shaped band of fibrous tissue that originates on the medial surface of the distal radius and traverses horizontally to insert on the ulnar styloid process (Figures 9.115 and 9.116). It rotates against the distal surface of the ulnar head during pronation and supination and separates the ulna from the carpal bones. The proximal surface of the radiocarpal articulation is formed by the articular carpal surface of the radius and the TFCC, whereas the distal surface is formed by the articular surfaces of the scaphoid, lunate, and triquetrum and the interosseous ligaments connecting them (Figures 9.111 through 9.115). The midcarpal joint is formed by the articulations between the proximal and distal carpal rows (Figures 9.110 and 9.115). The articulation between the carpals within each row creates the intercarpal joints (Figures 9.111 and 9.115). The carpometacarpal joints are formed by the articulations between the carpus and the five metacarpals (Figure 9.111 and 9.115). The carpometacarpal joint of the thumb is an independent joint formed by the articular surfaces of the trapezium and first metacarpal, creating a pure saddle joint. The carpometacarpal articulations of the two to five digits are amphiarthrotic joints with little mobility (Figures 9.105 and 9.115). The intermetacarpal articulation exists between the base of the metacarpals and is joined by the palmar and dorsal metacarpal ligaments (Figure 9.115).
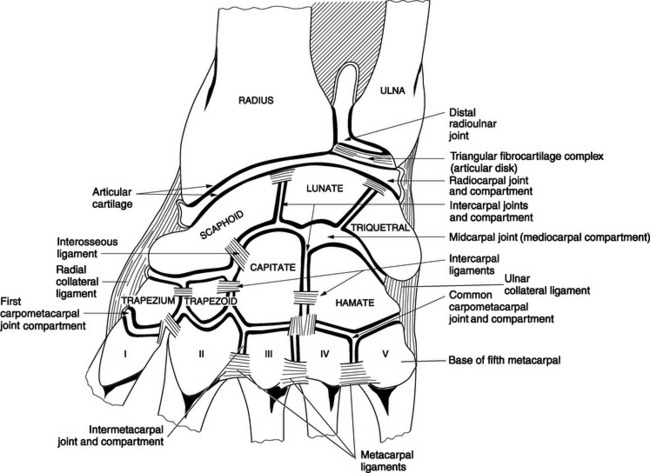
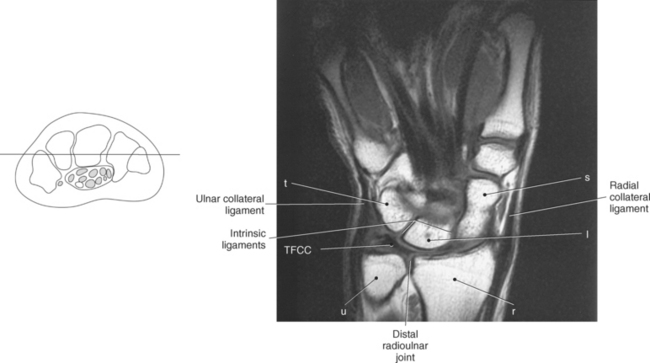
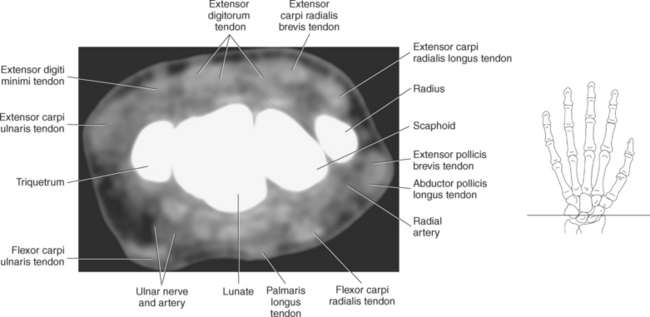
Figure 9.116 Coronal, T1-weighted MR scan of wrist with triangular fibrocartilage complex.
Key: t, Triquetrum; TFCC, triangular fibrocartilage complex; u, ulna; r, radius; s, scaphoid; l, lunate; H, hamate; C, capitate; Td, trapezoid; Tm, trapezium; P, pisiform; L, lunate; S, scaphoid; LT, Lister’s tubercle.
Ligaments and Fascia
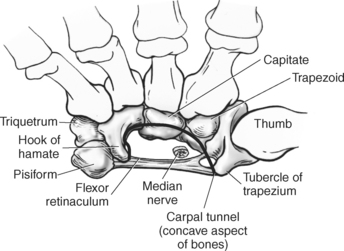
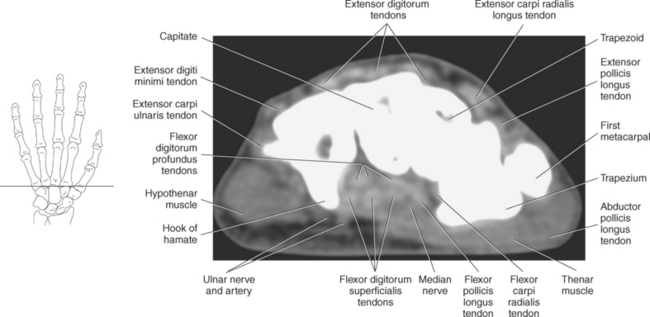
Numerous ligaments provide additional stability to the wrist. The extrinsic ligaments reinforce the joint cavity surrounding the carpal region and include palmar and dorsal radial carpal ligaments, the radial and ulnar collateral ligaments, and the TFCC (Figures 9.115 through 9.117). The many articulations between the carpal bones are supported by the intercarpal ligaments or intrinsic ligaments that connect the carpal bones to each other (Figure 9.115). The configuration of the intrinsic ligaments, metacarpal ligaments, and triangular fibrocartilage complex creates five different joint compartments that can be demonstrated at arthrography: (1) compartment of the first carpometacarpal articulation, (2) common carpometacarpal compartment, (3) mediocarpal compartment, (4) intermetacarpal compartment, and (5) radiocarpal compartment (Figure 9.115). The carpal tunnel is created by the concave arrangement of the carpal bones (Figure 9.103). A thick ligamentous band called the flexor retinaculum (transverse carpal ligament) stretches across the carpal tunnel to create an enclosure for the passage of tendons and the median nerve (Figures 9.118 through 9.120). The flexor retinaculum inserts medially on the pisiform and hook of the hamate and spans the wrist to insert laterally on the scaphoid and trapezium. In addition to the carpal tunnel, another tunnel called Guyon’s canal is formed where the ulnar extension of the flexor retinaculum continues over the pisiform and hamate. This creates a potential site for compression of the ulnar nerve (Figures 9.118, top, and 9.119). The extensor retinaculum (dorsal carpal ligament), located dorsally, is much thinner. It attaches medially to the ulnar styloid process, triquetrum, and pisiform and laterally to the lateral margin of the radius (Figure 9.120, left). Along its course it forms six fibroosseous tunnels for the passage of the synovial sheaths containing the extensor tendons (Figure 9.118, bottom).
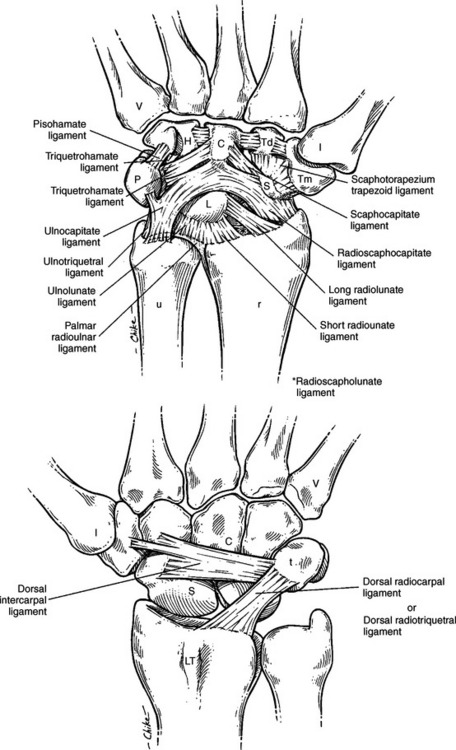
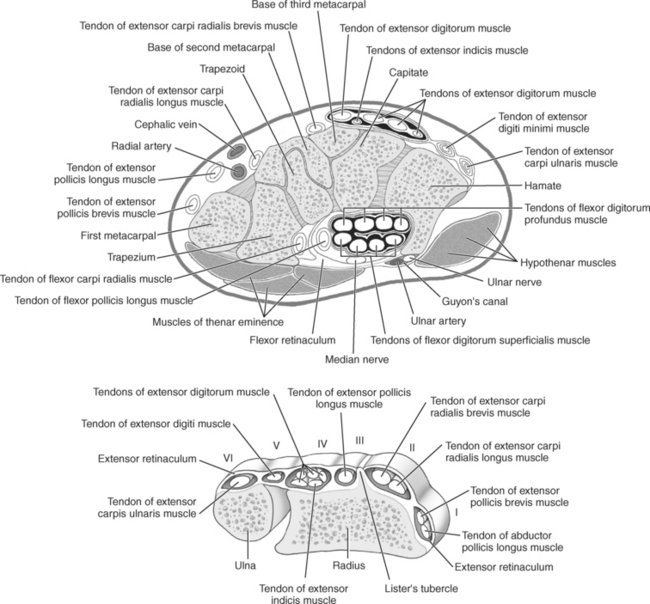
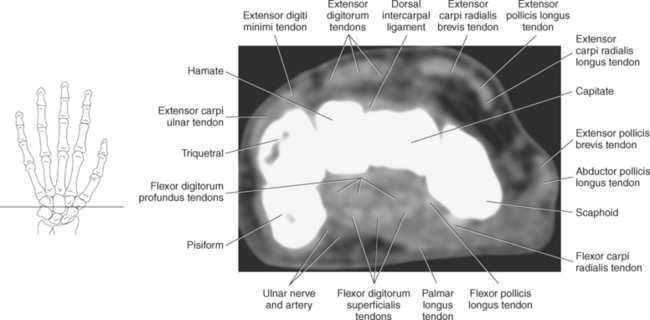
Figure 9.118 Axial view of carpal tunnel and flexor tendons. Top, Extensor tendons. Bottom, Compartments.
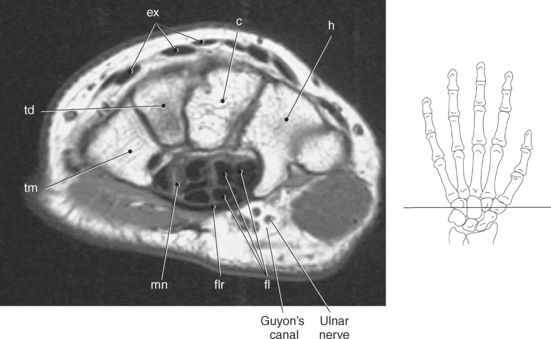
Figure 9.119 Axial, T1-weighted MR scan of wrist with flexor and extensor tendons.
Key: ex, Extensor tendons; c, capitate; h, hamate; fl, flexor tendons; flr, flexor retinaculum; mn, median nerve; tm, trapezium; td, trapezoid.
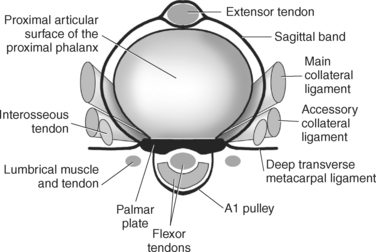
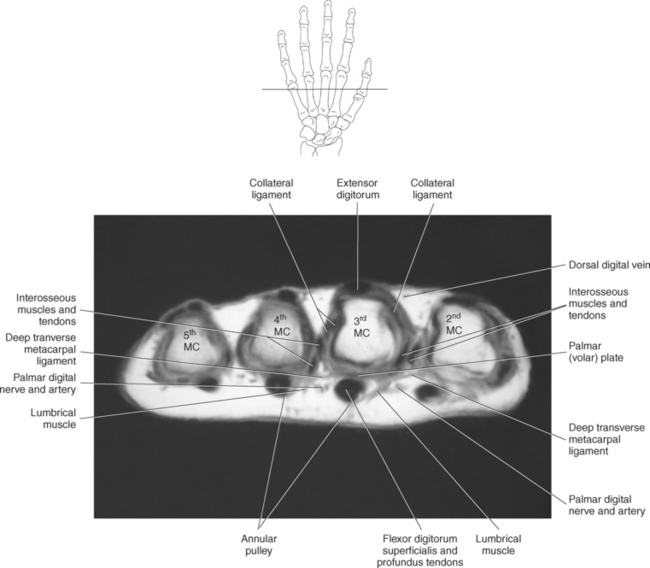
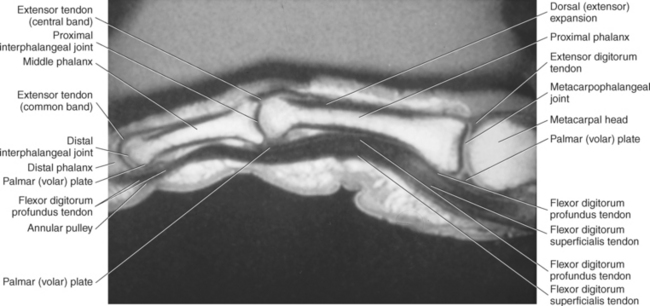
Ligaments of the Fingers
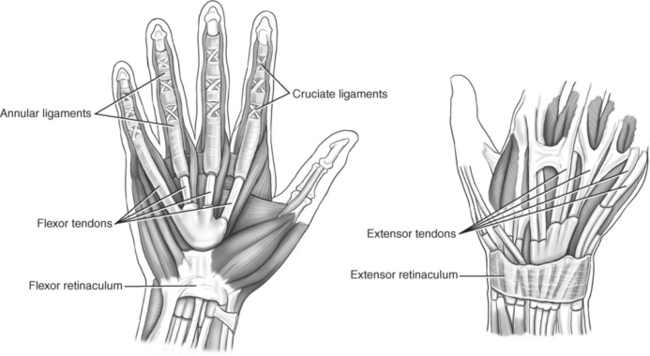
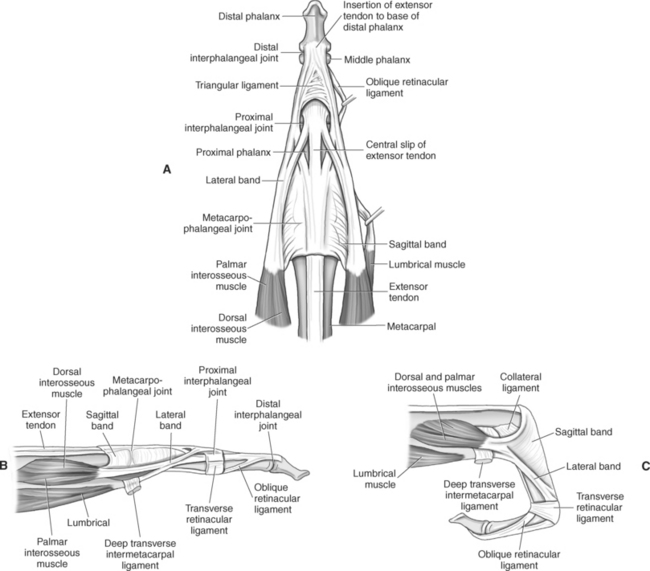
The MCP and interphalangeal joints each have a palmar ligament and two collateral ligaments. The palmar (volar) ligament is a thick, dense fibrocartilaginous tissue that covers the palmar surface of the joints. The palmar ligaments run between and are connected to the collateral ligaments, creating the floor of the interphalangeal and MCP joints. The deep transverse metacarpal ligament (DTML) consists of a series of short ligaments that connect the palmar ligaments of the metacarpal heads (Figure 9.123). The DTML prevents separation of the metacarpals. Along the palmar surface of the fingers, the ligamentous structures of the radial and ulnar collateral ligaments, radial and ulnar accessory collateral ligaments, and palmar plates provide stability for the MCP and interphalangeal joints (Figure 9.121). There is a fibroosseous tunnel along the palmar aspect of each finger for the passage of the flexor tendons. The tunnel is created by well-defined areas of thickening of the tendon sheath and is called the annular pulley system. It is composed of five annular pulleys and three cruciate pulleys, which are important structures that prevent the displacement of the tendons during flexion of the fingers (Figure 9.122). The dorsal surface of the hand and fingers contains the extensor mechanism or extensor hood (Figures 9.123 through 9.126). The extensor hood consists of the digital extensor tendon, extensor hood proper, and insertions of the lumbricals and interossei muscles and serves to maintain the integrity of the extensor tendons along the path of the MCP and interphalangeal joints.
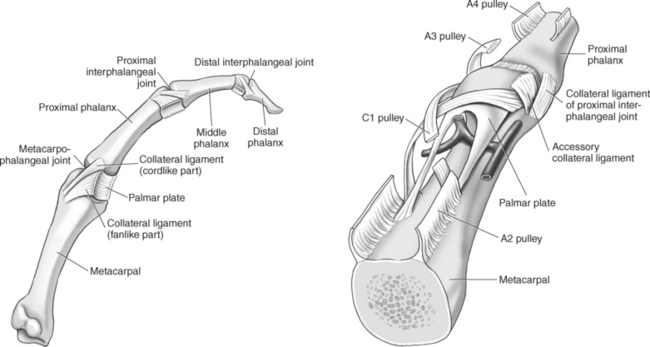
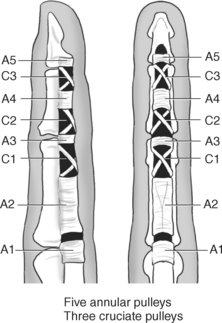
Figure 9.122 Annular pulley system. Left, Sagittal view. Right, Palmar view.
Key: A, Annular pulley; C, cruciate pulley. A B C
Muscles and Tendons
The numerous muscles of the forearm become tendinous just before the wrist joint. The many tendons located in the wrist can be divided into palmar and dorsal tendon groups (Figures 9.120, A and B and 9.127). The palmar tendon group collectively flexes the fingers and wrist. As this group courses through the carpal tunnel, the tendons appear to be arranged in two discrete rows (Figures 9.118, A and 9.119). The tendons of the dorsal tendon group, spanning the superficial surface of the wrist, are considered the extensors of the fingers and wrist (Figures 9.128 through 9.140).

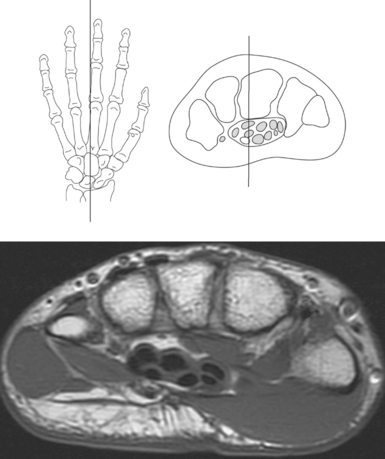
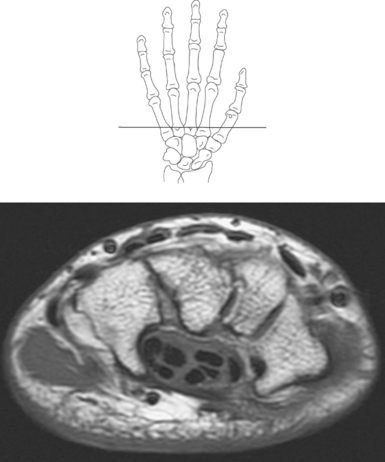
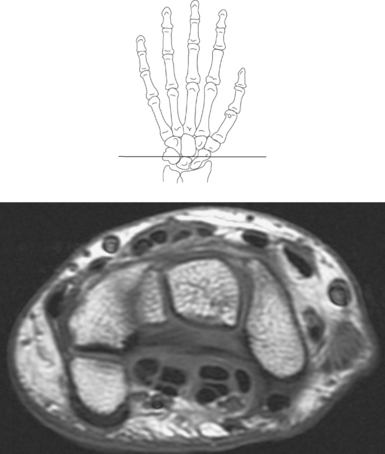
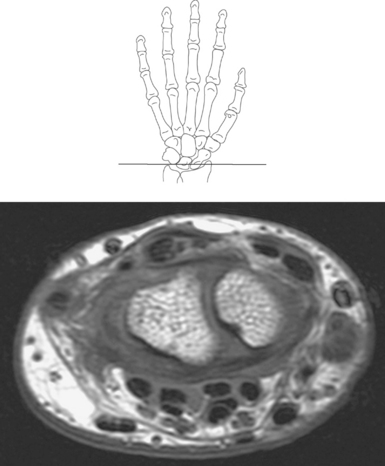
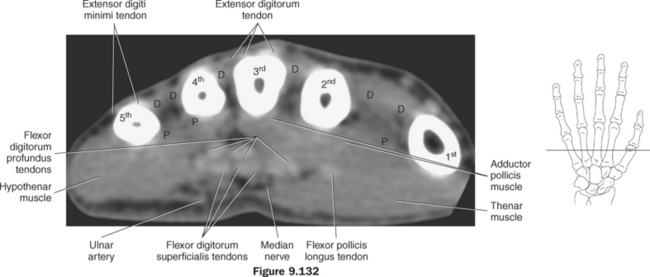
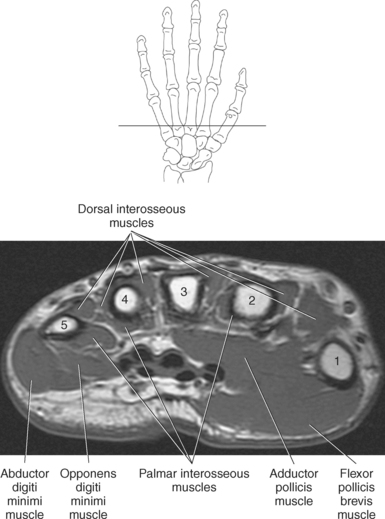
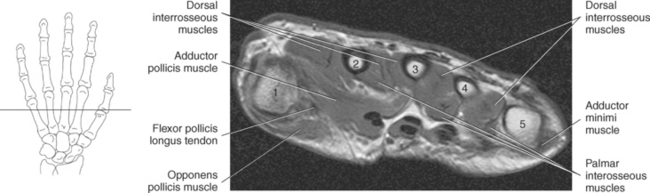
Figure 9.132 Axial CT scan through fingers.
Key: fl, Flexors; c, capitate; ex, extensor tendons; r, radius; l, lunate; D, dorsal interosseus muscles; P, palmar interosseus muscles.
The muscles of the hand can be divided into three groups: (1) metacarpal group (muscles of the metacarpals considered to be the central muscles of the hand), (2) thenar group (muscles involving the thumb and creating the thenar eminence on the radial side), (3) hypothenar group (muscles involving the fifth digit and creating the hypothenar eminence on the ulnar side). These muscles are demonstrated in Figures 9.128 through 9.143.
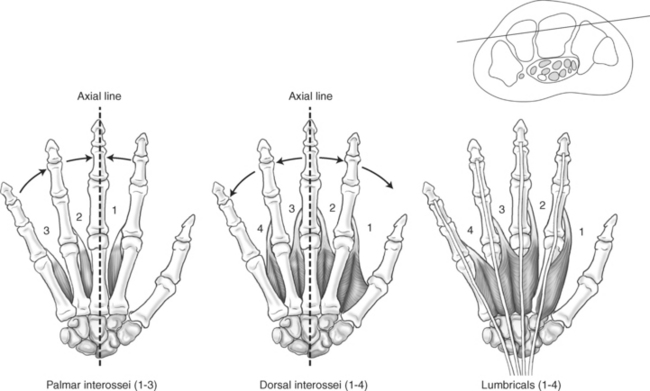
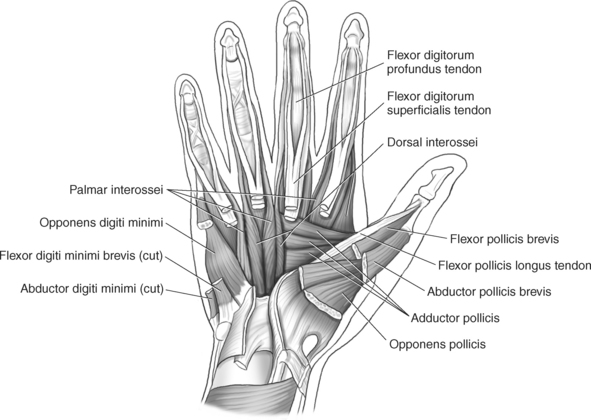
Figure 9.141 Left, Palmar view of interosseous muscles. Center, Dorsal view of interosseous muscles. Right, Lumbrical muscles.
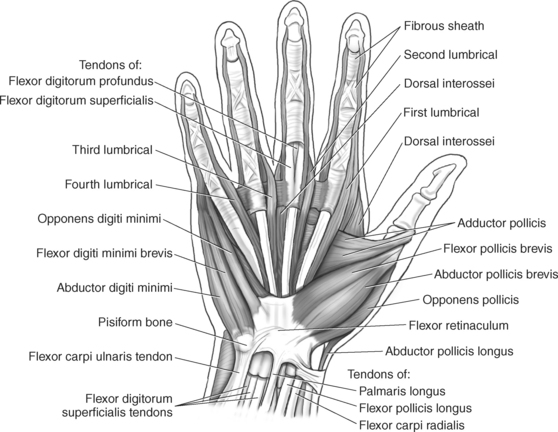
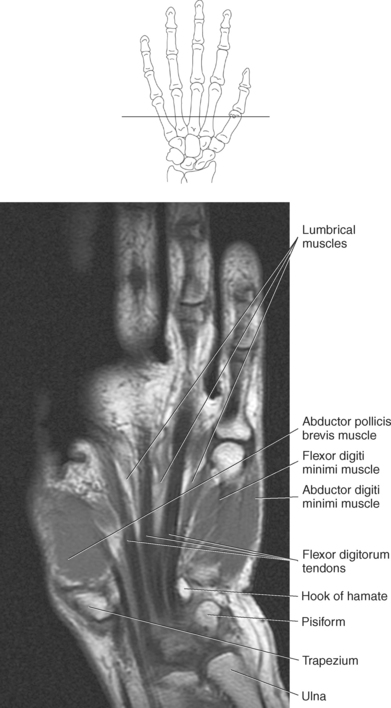
Figure 9.142 Palmar view of flexor pollicis brevis, flexor digiti minimi, abductor pollicis brevis, opponens pollicis, and abdutor digiti minimi muscles.
Metacarpal Group
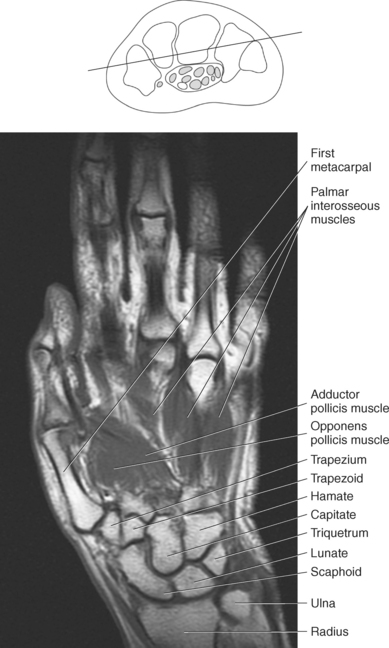
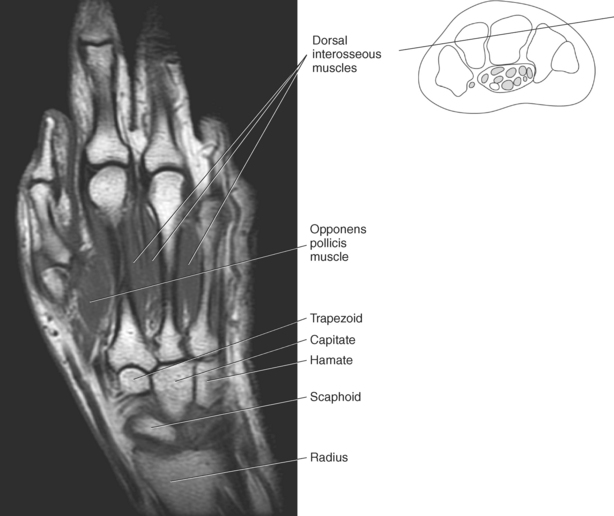
The metacarpal muscle group includes the interossei and lumbrical muscles. There are seven short interossei muscles in the metacarpal muscle group: three single-headed muscles located on the palmar surface and four double-headed muscles located on the dorsal surface (Figure 9.141, A and B). The four palmar interossei muscles arise from the first, second, fourth, and fifth metacarpals and insert on the corresponding proximal phalanges, frequently radiating into the corresponding tendons of the dorsal aponeurosis. These muscles are responsible for flexion at the MCP joints and extension at the interphalangeal joints. The dorsal interossei arise by two heads from the sides of the five metacarpal bones to insert on the proximal phalanges and radiate onto the dorsal aponeurosis. Like their palmar counterparts, the dorsal interossei flex at the MCP joints and extend at the interphalangeal joints. The four small lumbrical muscles arise from the tendons of the flexor digitorum profundus and pass to the radial side of the corresponding finger to insert on the extensor expansion covering the dorsal surface of the finger (Figure 9.142). The lumbricals flex the first phalanges at the MCP joints and extend the second and third phalanges at the interphalangeal joints.
Thenar Group
The four muscles of the thenar group are the abductor pollicis brevis, flexor pollicis brevis, adductor pollicis, and opponens pollicis. The abductor pollicis brevis is a thin, flat superficial muscle arising from the transverse carpal ligament, navicular, and trapezium (Figure 9.143). It runs inferiorly and laterally to insert on the base of the first phalanx of the thumb to abduct the thumb. The flexor pollicis brevis has two heads: The superficial or lateral head arises from the flexor retinaculum, and the deep or medial head arises from the trapezium, trapezoid, and capitate. This muscle inserts on the radial and ulnar base of the first phalanx to flex, adduct, and abduct the thumb (Figure 9.143). Frequently, a sesamoid bone can be found in the insertion tendon on the radial side. The adductor pollicis also has two heads: The transverse head arises from the dorsal aspect of the third metacarpal, and the oblique head arises from numerous slips off the capitate, bases of the second and third metacarpals, and the sheath of the flexor carpi radialis tendon. The adductor pollicis inserts onto the base of the first phalanx of the thumb to provide adduction and assist in the opposition and flexion of the thumb (Figures 9.142 and 9.143). The opponens pollicis provides the main opposition for the thumb but also assists with adduction. It arises from the trapezium and flexor retinaculum and inserts onto the radial aspect of the first metacarpal (Figures 9.142 and 9.143). These muscles are also demonstrated in sequential Figures 9.128 through 9.140.
Hypothenar Group
The hypothenar group consists of three muscles: abductor digiti minimi, flexor digiti minimi brevis, and opponens digiti minimi. The abductor digiti minimi muscle arises from the pisiform and the flexor retinaculum to end in a flat tendon that inserts onto the ulnar base of the first phalanx of the little finger (Figures 9.142 and 9.143). The abductor digiti minimi muscle is the main abductor of the little finger. The flexor digiti minimi brevis muscle arises from the flexor retinaculum and the hook of the hamate. It fuses with the tendon of the abductor digiti minimi to insert on the base of the first phalanx of the fifth digit (Figures 9.142 and 9.143). The flexor digiti minimi brevis flexes at the MCP joint. Like the flexor digiti minimi brevis muscle, the opponens digiti minimi arises from the hook of the hamate and the flexor retinaculum (Figure 9.143). It inserts on the ulnar surface of the fifth metacarpal to bring the little finger into the position for opposition. For the hand muscles, see Figures 9.128 through 9.140.
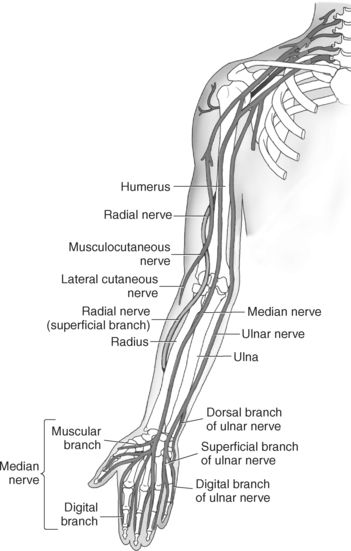
NEUROVASCULATURE
The neurovasculature of the upper extremity is composed primarily of the branches of the axillary and brachial arteries, their accompanying deep veins, a system of superficial veins, and the brachial plexus that innervates the upper extremity.
Arterial Supply
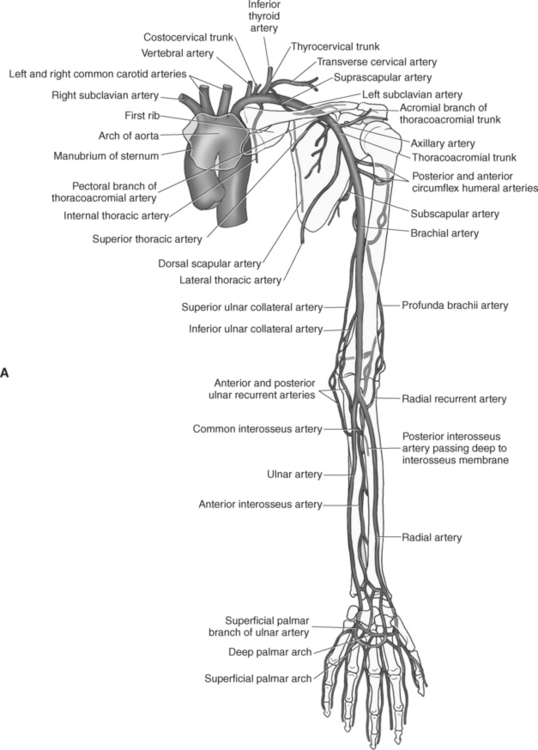
The primary arteries supplying the shoulder region include the axillary and brachial arteries (Figures 9.34 through 9.45 and 9.144, A). The axillary artery begins at the lateral border of the first rib as a continuation of the subclavian artery. It ends at the inferior border of the teres major muscle, where it passes into the arm and becomes the brachial artery. The axillary artery and its branches supply blood to numerous thoracic and shoulder structures, including the first and second intercostal spaces, axillary lymph nodes, mammary gland in women, and scapular, serratus anterior, pectoral, latissimus dorsi, deltoid, and triceps brachii muscles. The branches of the axillary artery typically include the superior thoracic, thoracoacromial, lateral thoracic, subscapular artery, and anterior and posterior humeral circumflex arteries. The brachial artery is the principal arterial supply to the arm. It courses inferiorly on the medial side of the humerus then continues anterior to the cubital fossa of the elbow. The brachial artery is relatively superficial and palpable throughout its course. It accompanies the median nerve, which crosses anterior to the artery in the middle of the arm. During its course, the brachial artery gives rise to numerous muscular branches, which include the profunda brachii, superior ulnar collateral, and inferior ulnar collateral arteries (Figure 9.144, A).
Elbow
The brachial artery divides at the cubital fossa into the radial and ulnar arteries (Figure 9.144, A).
The radial artery begins at the level of the head of the radius within the anterior compartment of the forearm. It courses beneath the brachioradialis muscle then continues its course just deep to the skin, along the lateral side of the anterior forearm to the wrist. It passes anterior to the radial styloid process to enter the hand. The most proximal branch of the radial artery is the radial recurrent artery, which supplies the brachioradialis, supinator, and brachialis muscles and the elbow joint. Within the forearm, the radial artery gives off several direct muscular branches. The ulnar artery also gives rise to several branches that supply the elbow and forearm. The first branch of the ulnar artery is the anterior ulnar recurrent artery, which supplies the brachialis and pronto teres muscles. It courses just anterior to the medial condyle of the humerus to anastomose with the inferior ulnar collateral branch of the brachial artery. The posterior ulnar recurrent artery courses behind the medial epicondyle of the humerus to anastomose with the superior ulnar collateral branch of the brachial artery. It supplies the flexor carpi ulnaris, pronator teres, and anconeus muscles. The common interosseous artery branches from the ulnar artery and almost immediately bifurcates into the anterior and posterior interosseous arteries. These arteries and their branches supply the median nerve, deep flexor and extensor muscles of the forearm, superficial extensor muscles of the forearm, and radius and ulna (Figures 9.57 through 9.67 and 9.87 through 9.98).
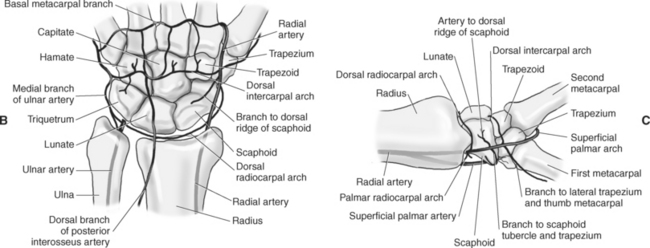
Wrist and Hand
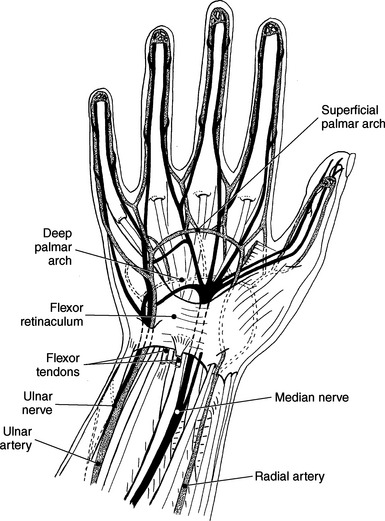
The terminal branches of the radial and ulnar arteries form the palmar arches of the wrist and hand. These arches emit branches that serve the wrist, palm, and digits (Figures 9.144 and 9.145). The palmar carpal arch or network is formed by the palmar carpal branches from the radial and ulnar arteries, the anterior interosseous artery, also a branch of the ulnar artery, and a recurrent branch from the deep palmar arch. These vessels supply the carpal bones and joints (Figure 9.144, A and C). The dorsal carpal arch or network is formed by dorsal carpal branches of the radial and ulnar arteries. The dorsal carpal arch also receives contributions from the anterior and posterior interosseous arteries. The arch lies close to the dorsal surface of the carpals and gives rise to three dorsal metacarpal arteries and branches that supply the distal regions of the ulna and radius, carpal bones, and intercarpal joints (Figure 9.144, A and C). The superficial palmar branch of the radial artery anastomoses with the superficial palmar branch of the ulnar artery to form the superficial palmar arch. This arch gives rise to three common palmar digital arteries that anastomose with the palmar metacarpal arteries from the deep palmar arch (Figure 9.144, A and C). The deep palmar arch is formed by deep palmar branches of the radial and ulnar arteries and is located approximately 1cm proximal to the superficial palmar arch. The deep palmar arch also gives rise to a recurrent branch that anastomoses with the palmar carpal branches of the radial and ulnar arteries (Figure 9.144, A).

Venous Drainage
The veins of the upper extremity are divided into deep and superficial (cutaneous) groups. Numerous anastomoses occur between the groups. The superficial venous system consists of extensive venous networks that are especially well developed within the upper extremity along with their accompanying arteries of the same name. The deep veins are often double and repeatedly anastomose with one another.
Shoulder
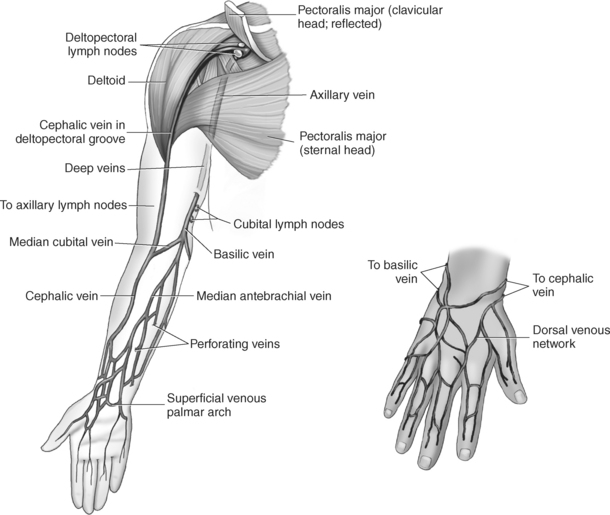
The veins of the upper arm include the brachial, cephalic, and basilic (Figure 9.146). The two deep brachial veins ascend the arm, one on either side of the brachial artery. The brachial veins begin in the elbow from the union of the ulnar and radial veins and end in the axillary vein near the lower margin of the subscapularis muscle. The two deep brachial veins may join to form one brachial vein during part of their course. The superficial veins of the upper arm include the cephalic and basilic. The cephalic vein courses from the radial side of the dorsal venous arch of the hand and then ascends to the midpoint of the forearm, where it curves around to the ventral surface of the forearm and ascends the lateral aspect of the upper arm, along the anterolateral border of the biceps brachii muscle, to open into the axillary vein, just below the clavicle. It drains the superficial parts of the lateral hand and lateral forearm. The basilic vein originates from the medial end of the dorsal venous arch of the hand. It then ascends the ulnar side of the forearm, along the medial surface of the biceps brachii muscle, in the upper arm, to form the axillary vein. The basilic vein drains the superficial parts of the medial side of the hand and medial side of the forearm. The large axillary vein lies on the medial side of the axillary artery. It extends from the lower border of the teres major muscle to the lateral surface of the first rib to continue as the subclavian vein. The axillary vein receives tributaries that correspond to the branches of the axillary artery (Figures 9.34 through 9.47).
Elbow
The large deep vein of the elbow is the brachial vein, which is formed by the union of the radial and ulnar veins. The superficial veins of the elbow include the cephalic, median cubital, basilica, and intermediate (median) antebrachial veins. The cephalic vein courses along the radial side of the elbow and may give rise to the median cubital vein, which ascends in an oblique and medial course to create an anastomosis between the basilic and cephalic veins (Figure 9.145). The median cubital vein is a common site for venipuncture. The basilic vein courses along the posteromedial aspect of the forearm, crosses the elbow, then takes a deep course in the axilla to joint the brachial vein. The intermediate (median) antebrachial vein transports blood from the superficial palmar venous arch and anterior forearm. It ascends the ventral side of the forearm on the ulnar side and typically ends in the basilic vein (Figures 9.147, 9.60 through 9.67, and 9.87 through 9.98).
Wrist and Hand
The superficial venous system forms a network at the dorsum of the hand termed the dorsal venous network (arch). It is fed by the subcutaneous dorsal metacarpal veins of the fingers and continues to the distal forearm, where it drains into three major superficial veins: the cephalic, basilic, and intermediate (median) antebrachial veins of the forearm. These large superficial veins anastomose frequently as they course superiorly. The deep and superficial palmer venous arches of the hand empty into the radial and ulnar veins that then unite to form the brachial vein of the arm (Figures 9.89, 9.92 and 9.95, 9.146, and 9.147).
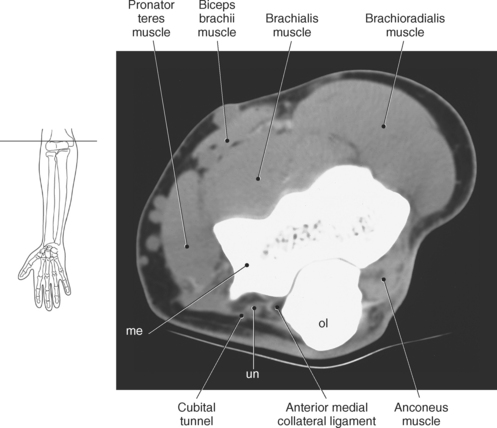
Brachial Plexus
The brachial plexus, also described in Chapter 4, is a large network of nerves that innervate the upper limb (Figures 9.38 and 9.148). It extends from the neck into the axilla. The brachial plexus is formed by the union of the ventral rami of nerves C5-C8 and the greater part of the T1 ventral ramus. The ventral rami from C5 and C6 unite to form a superior trunk, the ventral ramus of C7 continues as the middle trunk, and the ventral rami of C8 and T1 unite to form an inferior trunk. Each of these trunks divides into an anterior and posterior division. The anterior divisions supply the anterior (flexor) parts of the upper limb, and the posterior divisions supply the posterior (extensor) parts of the upper limb. These divisions form three cords (posterior, lateral, and medial) that continue to divide to form the median, ulnar, musculocutaneous, and radial nerves (sequential Figures 9.59 through 9.67 and 9.87 through 9.95). These nerves supply the muscles of the forearm and hand. The median nerve descends the cubital fossa deep to the median cubital vein. It supplies the pronator teres muscle of the arm and all the superficial and deep flexor muscles of the forearm, except the flexor carpi ulnaris muscle. It gives off an anterior interosseous branch that descends within the forearm to supply the flexor digitorum profundus muscle. The median nerve courses through the carpal tunnel of the wrist, typically superficial to the flexor tendons (Figure 9.147). It supplies flexors of the hand, skin of the wrist, thenar eminence, palm of the hand, and sides of the first three digits and lateral half of the fourth. At the elbow, the ulnar nerve passes between the medial epicondyle of the humerus and the olecranon process within the cubital tunnel to enter the medial side of the flexor compartment of the forearm (Figure 9.148). Posterior to the medial epicondyle, the ulnar nerve is superficial and easily palpable. It supplies the flexor carpi ulnaris muscle and the medial side of the flexor digitorum profundus muscle in the forearm before entering the hand. The ulnar nerve passes under the flexor retinaculum, along with the ulnar artery, to enter the palmar compartment of the hand (Figure 9.147). At this point, the ulnar nerve divides into superficial and deep terminal branches that supply the ulnar flexors of the hand as well as the skin on the medial side of the palm, medial half of the dorsum of the hand, fifth digit, and medial half of the fourth digit. The musculocutaneous nerve descends to the lateral side of the arm and elbow to innervate the flexors in the arm and the skin of the forearm, wrist, and thenar region of the hand (Figure 9.146). It emits branches that supply both heads of the biceps brachii muscle, the brachialis muscle, and the elbow joint. It innervates the skin of the dorsal surface of the arm. A continuation of the musculocutaneous nerve is the lateral cutaneous nerve, which terminates into cutaneous branches that supply the skin covering the radial side of the wrist and the thenar eminence. The radial nerve is the largest branch of the brachial plexus. It passes inferolaterally around the body of the humerus in the radial groove (Figure 9.146). It continues inferiorly between the brachialis and brachioradialis muscles to the level of the lateral epicondyle of the humerus, where it divides into deep and superficial branches. The deep branches supply all the extensors in the arm and forearm, and the cutaneous branches innervate the skin on the dorsal side of the arm and hand. The superficial branch, the direct continuation of the radial nerve, is entirely sensory. It supplies skin and fascia over the lateral two thirds of the dorsum of the hand, the dorsum of the thumb, and proximal parts of the lateral three and one half digits on their dorsal surfaces (Figures 9.57 through 9.67, 9.87 through 9.98, and 9.146 and 9.147).