Lower Extremity
The complex anatomy of the lower extremity joints is responsible for bearing the entire upper body weight and for accommodating the demands of movement placed on this system (Figure 10.1).
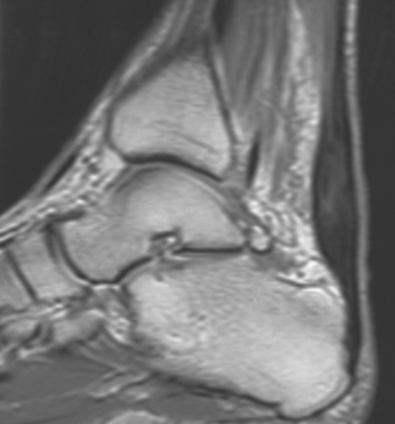
Figure 10.1 Sagittal, T2-weighted MR scan of ankle demonstrating thickening and edema in Achilles tendon.
HIP
The hip provides strength to carry the weight of the body in an erect position. This synovial ball-and-socket joint, created by the articulation of the femoral head to the acetabulum of the pelvis, allows for a wide range of motion.
Bony Anatomy
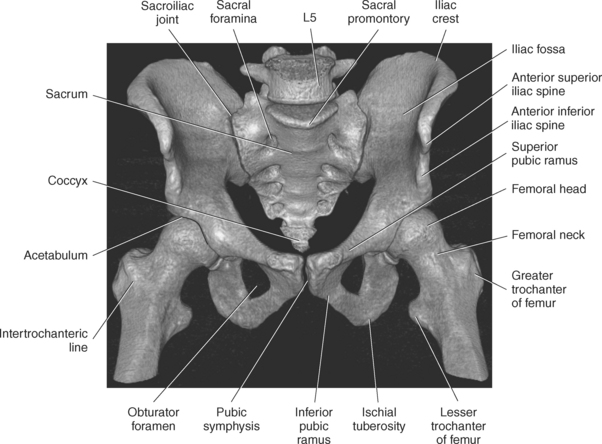
A cuplike cavity termed the acetabulum is created by the three bones of the pelvis: ilium, ischium, and pubis (Figure 10.2). In axial cross section, this area can be divided into sections known as the anterior and posterior columns (Figure 10.3). Within the acetabulum is a centrally located, nonarticulating depression called the acetabular fossa. It is formed mainly by the ischium and is filled with fat (Figure 10.4). A continuation of the acetabular fossa is the acetabular notch, which interrupts the smooth circumference of the acetabular rim below and functions as an attachment site for the transverse acetabular ligament (Figure 10.2).
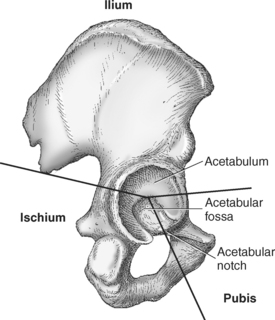
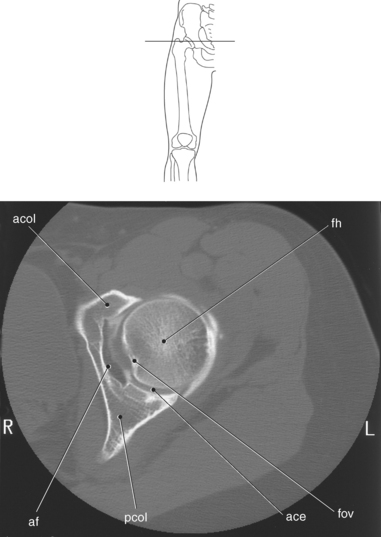
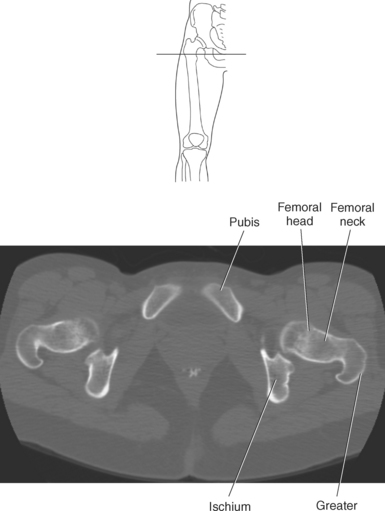
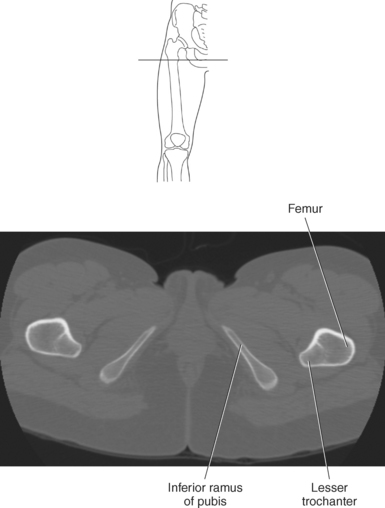
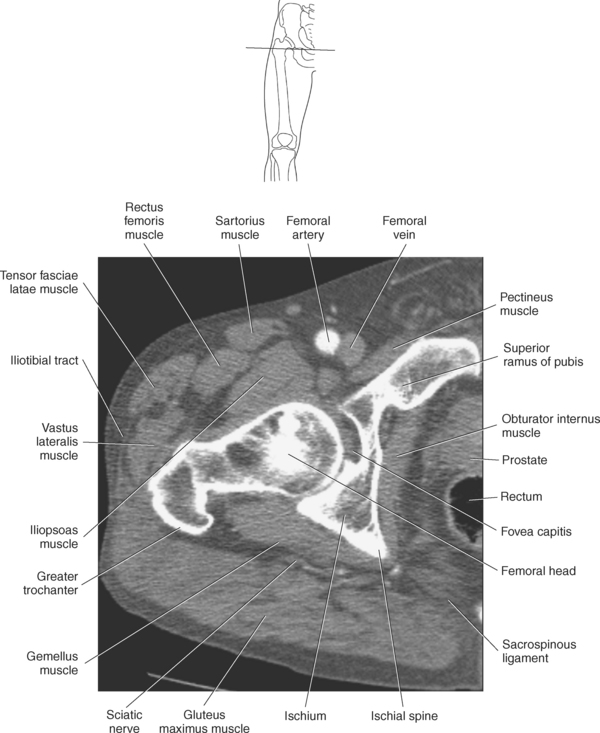
Figure 10.3 Axial CT scan of hip joint.
Key: acol, Anterior column; fh, femoral head; fov, fovea capitus; ace, acetabulum; pcol, posterior column; af, acetabular fossa.
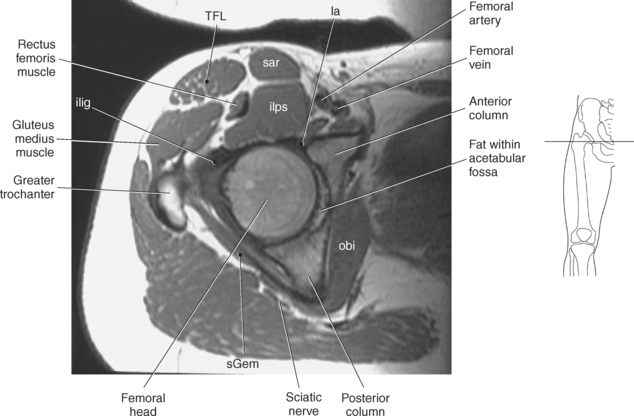
Figure 10.4 Axial, T1-weighted MR scan of hip.
Key: ilig, iliofemoral ligament; TFL, tensor fascia latae; sar, sartorius; ilps, iliopsoas; la, labrum; obi, obturator internus; sGem, superior gemellus.
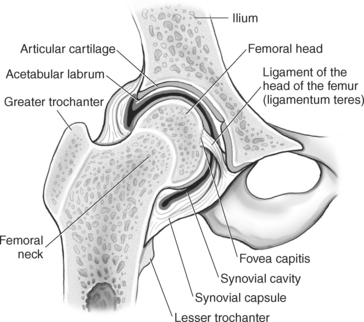
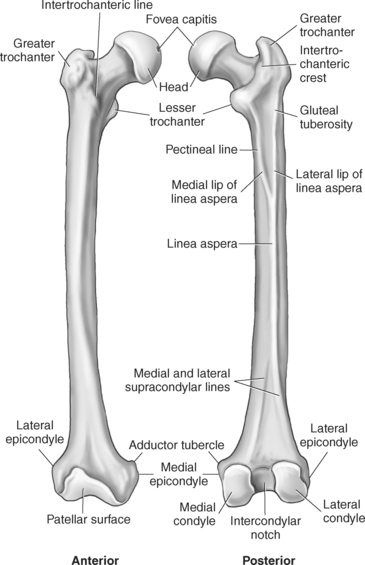
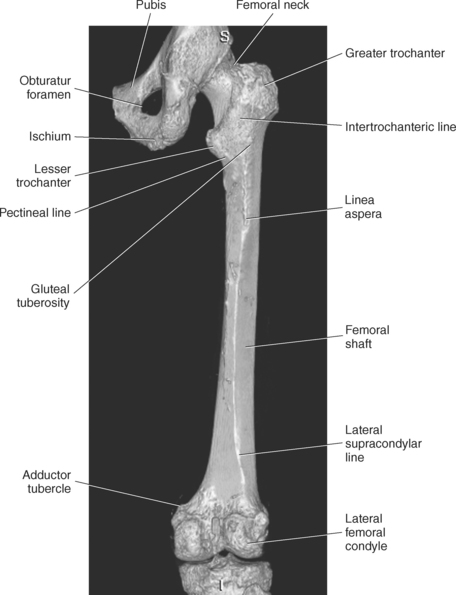
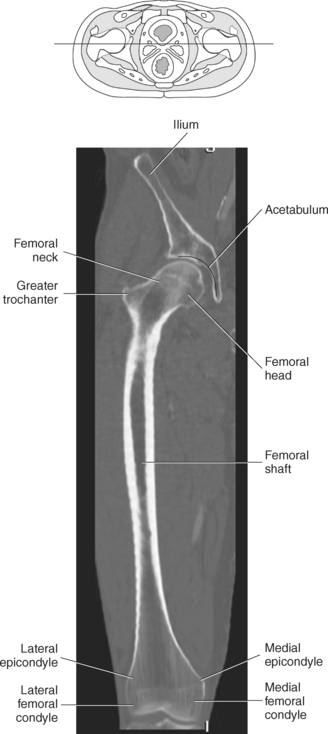
The femur is the longest, heaviest, and strongest bone in the body. The proximal end of the femur consists of a head, a neck, and two large processes: the greater and lesser trochanters (Figures 10.5 and 10.6). On the proximal portion of the femur is the smooth, rounded femoral head. The femoral head is covered entirely by articular cartilage, with the exception of a small centrally located pit termed the fovea capitis. The fovea capitis is an attachment site for the ligament of the head of the femur, also called the ligamentum teres, which transmits blood vessels to the femoral head (Figures 10.5 and 10.6). Attaching the head of the femur to the femoral shaft is the femoral neck. The neck extends obliquely from the head at an angle of approximately 120 degrees in an inferolateral direction to meet the shaft (Figure 10.5). The result of this angle is increased freedom of movement within the hip joint. At the distal end of the neck are two large bony prominences termed trochanters (Figures 10.5 through 10.8). The greater trochanter is situated at the junction of the neck with the shaft. The superior portion of the greater trochanter projects above the neck and curves slightly posteriorly and medially (Figure 10.9 and Figure 10.10). The greater trochanter provides attachment for several muscles of the gluteal region. The lesser trochanter is at the posteromedial portion of the proximal shaft and gives insertion to the tendon of the psoas major (Figures 10.9 and 10.10). The prominent ridge extending posteriorly between the trochanters at the base of the neck is the intertrochanteric crest (Figures 10.9 and 10.11). It provides an attachment site for the ischiofemoral ligament and part of the quadratus femoris tendon. Connecting the trochanters anteriorly is the less prominent ridge termed the intertrochanteric line, which provides attachment for the iliofemoral ligament and part of the vastus lateralis tendon (Figures 10.9 and 10.11). On the proximal and posterior end of the femoral shaft is a raised ridge termed the linea aspera. Its medial and lateral lips provide attachment sites for muscles of the posterior and medial compartments of the thigh. The pectineal line runs from the medial lip of the linea aspera to the lesser trochanter of the femur (Figures 10.9 and 10.11). It is the insertion site for the tendon of the pectineus muscle. The lateral lip is very rough and runs almost vertically upward to the base of the greater trochanter. The widened portion of the lateral lip, the gluteal tuberosity, is an attachment site for the gluteus maximus and adductor magnus muscles (Figures 10.9 and 10.11). The linea aspera extends down to the popliteal surface of the femur.
Labrum and Ligaments
The femoral head is held to the acetabulum by several major ligaments. The acetabular labrum, transverse acetabular ligament, iliofemoral ligament, ischiofemoral ligament, pubofemoral ligament, and ligamentum teres are demonstrated in Figures 10.12 through 10.20. The acetabular labrum, or cotyloid ligament, creates a fibrocartilaginous rim attached to the margin of the acetabulum. This labrum closely surrounds the femoral head, aiding to hold it in place by deepening the acetabular fossa, which adds increased stability to the joint (Figure 10.12). The inferior margin of the acetabulum is incomplete and is reinforced by the transverse acetabular ligament, a portion of the acetabular labrum, which spans the acetabular notch on the inferior edge of the acetabulum (Figure 10.12). As the transverse ligament abridges the acetabular notch, it transforms it into the acetabular foramen, which allows nerves and blood vessels to pass to and from the hip joint through this foramen. The iliofemoral ligament is among the strongest of the body, with many stabilizing functions as it spans from the anterior inferior iliac spine and rim of the acetabulum to insert on the intertrochanteric line of the femur (Figures 10.13 and 10.14). A primary function of this ligament is to provide a thick reinforcement to the anterior part of the hip joint. The ischiofemoral and pubofemoral ligaments, though difficult to distinguish, present a spiral configuration of femoral attachment (Figures 10.13 and 10.14). The ischiofemoral ligament arises from the ischium and courses in a spiral above the femoral neck to insert on the posterior femoral neck, whereas the pubofemoral ligament arises from the superior pubic ramus to radiate and insert onto the iliofemoral ligament and intertrochanteric line. The spiral configuration of these two ligaments is unique to humans and ensures the stability and function while controlling the overall position of the lower limb. The ligamentum teres is a somewhat flattened band that extends from the fovea capitis of the femoral head to attach to the rim of the acetabular notch as well as blend with the transverse ligament (Figure 10.12). This ligament contains the artery to the head of the femur. The ligamentum teres has little influence as a ligament but can assist to prevent dislocation of the hip. Ligaments of the hip are identified in Figures 10.15 through 10.20.
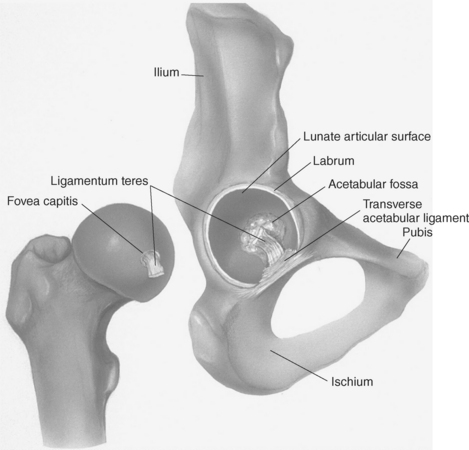
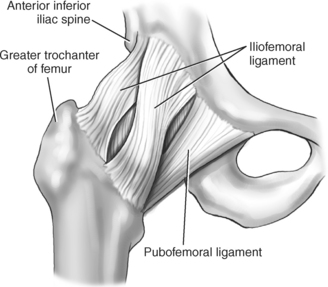
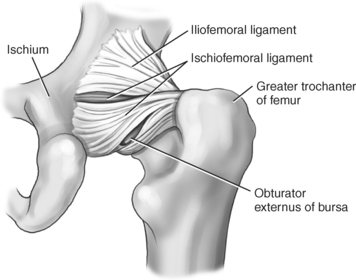
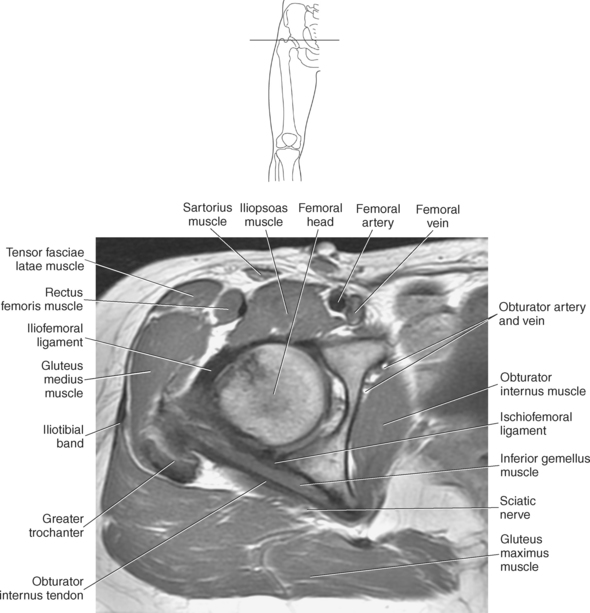
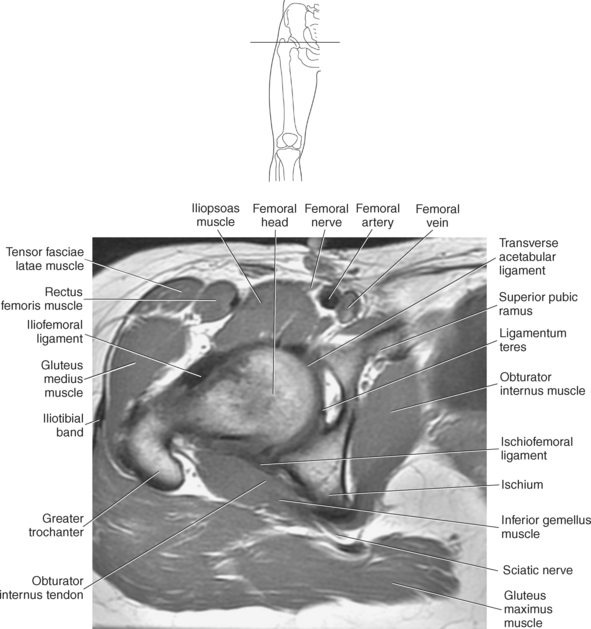
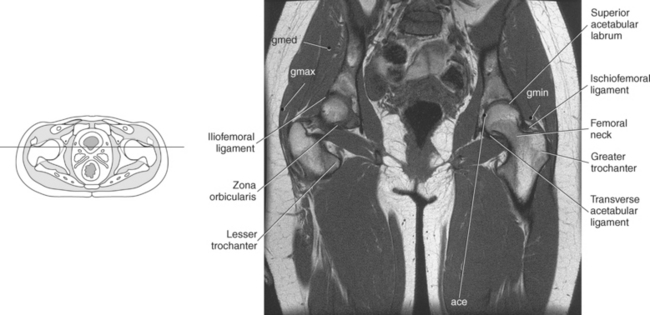
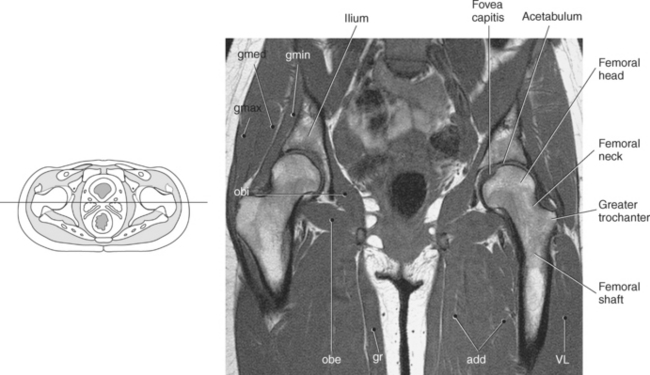
Figure 10.17 Coronal, T1-weighted MR scan of hips with ligaments and labrum.
Key: gmed, Gluteus medius; gmax, gluteus maximus; gmin, gluteus minimus; ace, acetabulum.
Articular Capsule of the Hip Joint
The fibrous capsule of the hip is strong and dense. It forms a sleeve that encloses the hip joint and most of the neck of the femur. Proximally, it is attached to the edge of the acetabulum, just distal to the acetabular labrum, and to the transverse ligament. Distally, the fibrous capsule is attached to the neck of the femur anteriorly to the intertrochanteric line and the root of the greater trochanter, and posteriorly to the neck, just proximal to the intertrochanteric crest. The capsule consists of two sets of fibers: circular and longitudinal. The circular fibers are deep and form the orbicular zone (zona orbicularis), a sling or collar around the femoral neck that constricts the capsule and helps to hold the femoral head in the acetabulum. Extending upward from the femoral neck are the longitudinal fibers, termed retinacula, that are most abundant at the superoanterior portion of the capsule. The retinacula contain blood vessels that supply the head and neck of the femur. They are reinforced by distinct bands or accessory ligaments, including the iliofemoral, pubofemoral, and ischiofemoral ligaments (Figures 10.13 through 10.20).
The synovial capsule of the hip joint lines the internal surface of the fibrous capsule. The synovial capsule forms a sleeve for the ligamentum teres, lines the acetabular fossa, and covers the fatty pad in the acetabular notch (Figure 10.5). It is attached to the edges of the acetabular fossa and to the transverse acetabular ligament. The synovial capsule protrudes inferior to the fibrous capsule on the posterior aspect and forms the obturator externus bursa, which protects the tendon of the obturator externus muscle (Figure 10.14).
Muscles of the Hip and Thigh
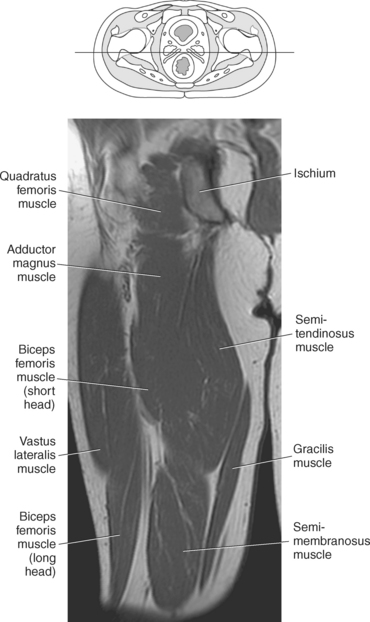
A complex arrangement of muscles around the hip joint and thigh produces the movements of the hip. They are described in this section as gluteal muscles and muscles of the thigh and are illustrated in Figures 10.20 through 10.29 and Table 10.1. The muscles of the gluteal region and thigh muscles may be separated into compartments by thickened sheets of deep fascia called fascial septa, thus allowing muscles of the lower extremity to be classified according to specific compartments in which they are located, such as gluteal, medial, and posterior compartments of the thigh.
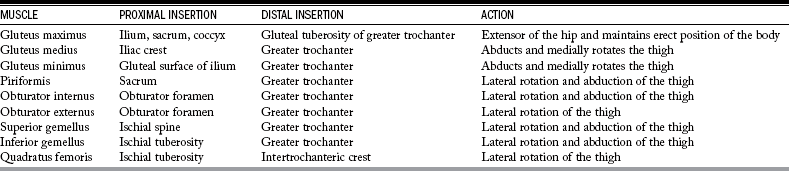
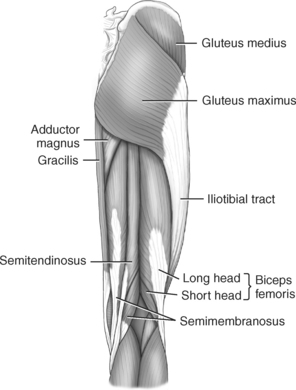
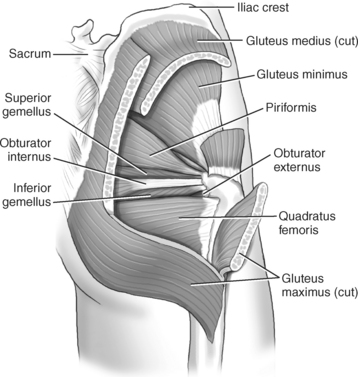
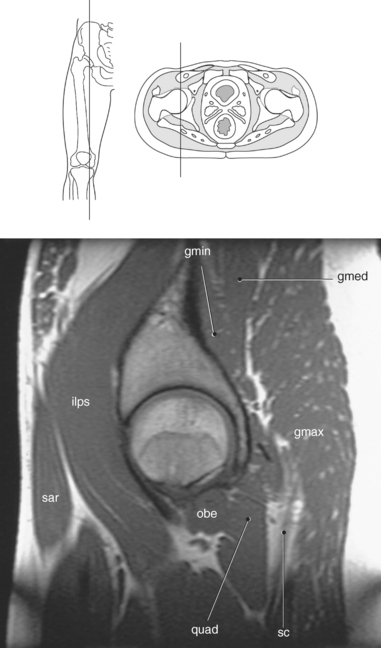
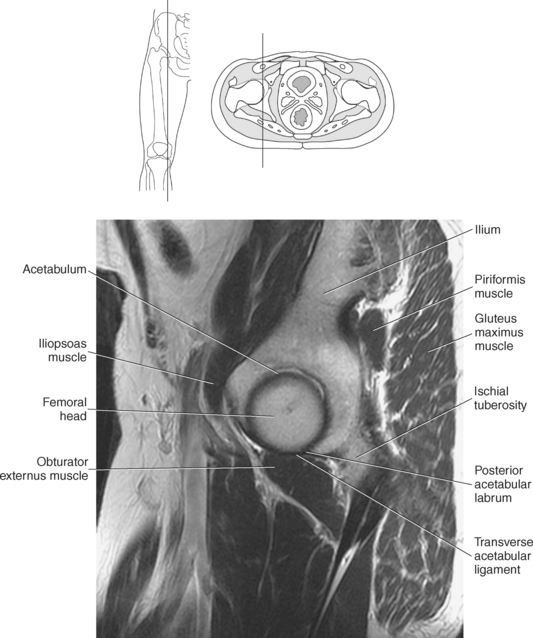
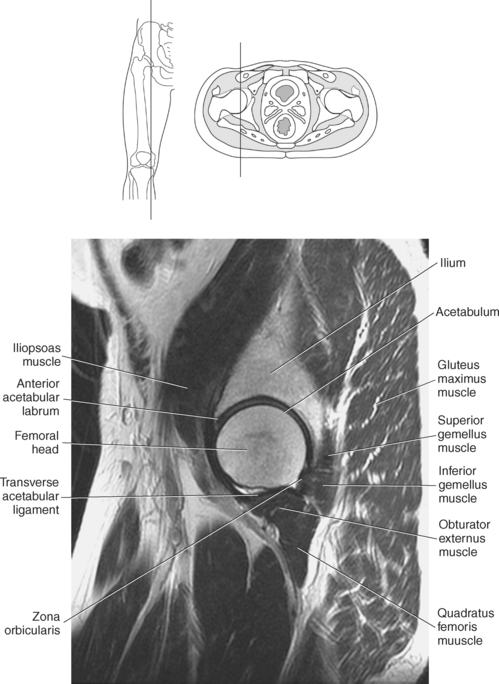
Figure 10.23 Sagittal, T1-weighted, MR scan of hip with muscles.
Key: gmin, Gluteus minimus; gmed, gluteus medius; ilps, iliopsoas; gmax, gluteus maximus; sar, sartorius; obe, obturator externus; quad, quadratus femoris; sc, sciatic nerve.
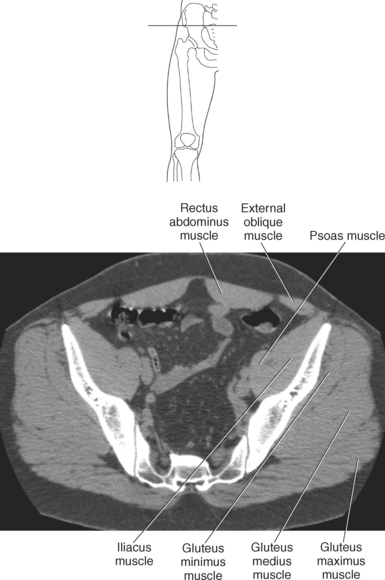
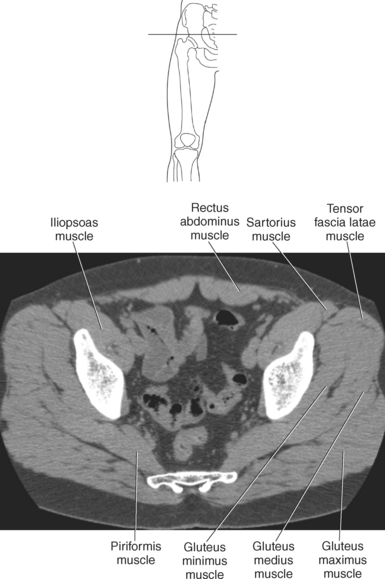
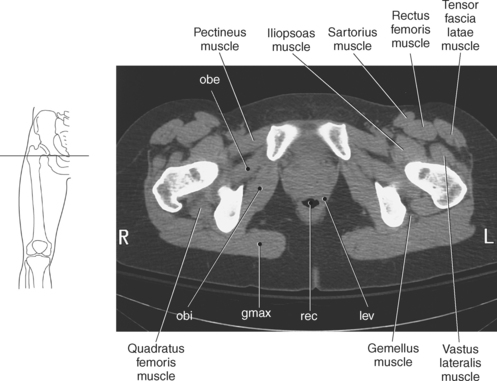
Figure 10.29 Axial CT scan of gluteal region with obturator muscles.
Key: obe, Obturator externus; obi, obturator internus; gmax, gluteus maximus; rec, rectum; lev, levator ani.
Muscles of the Gluteal Compartment
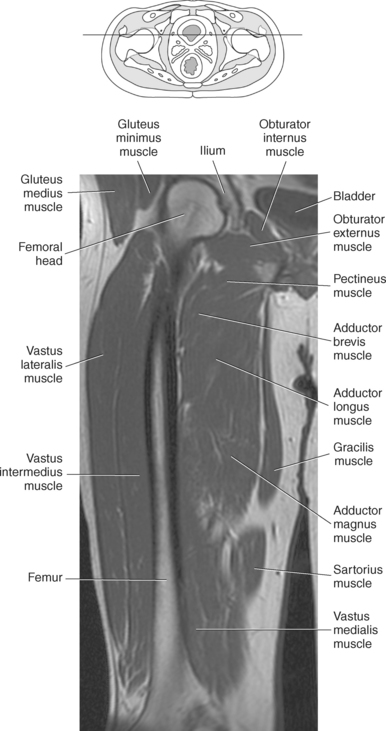
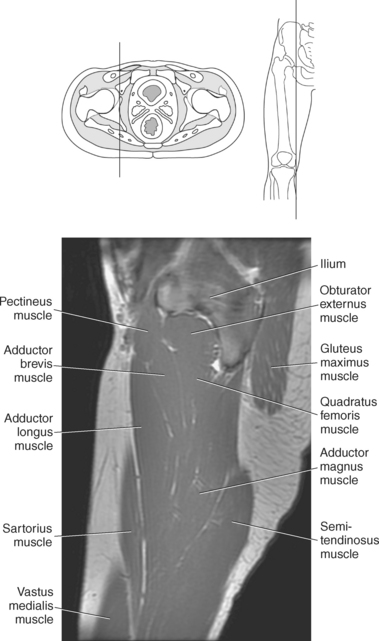
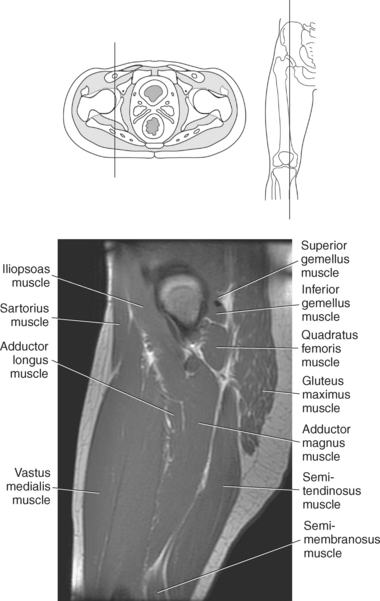
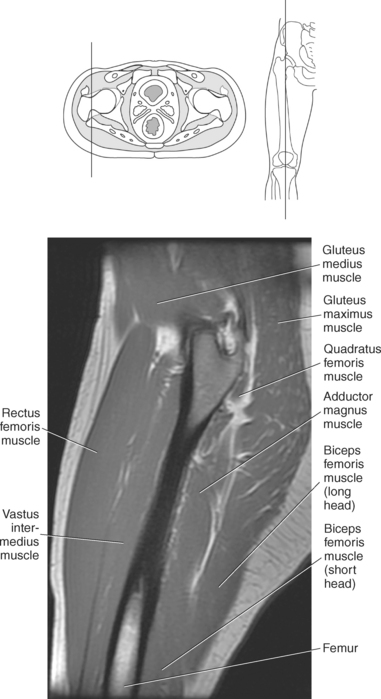
The superficial gluteus muscles include the gluteus maximus, gluteus medius, and gluteus minimus. The gluteus maximus muscle is the largest and most superficial of the gluteal muscle group. It is very powerful, is situated on the posterior aspect of the hip joint, acts primarily as an extensor of the hip, and is responsible for maintaining the erect position. The gluteus maximus originates from the ilium, sacrum, and coccyx to insert just distal to the gluteal tuberosity of the greater trochanter (Figures 10.21 through 10.29). The gluteus medius muscle is located on the lateral and upper part of the buttock. It originates from the iliac crest, just lateral to the gluteus maximus muscle, and is partially covered by the gluteus maximus along its medial one third. The gluteus medius is fan shaped as it spans from the iliac crest to insert on the superolateral aspect of the greater trochanter of the femur (Figures 10.22 through 10.29). The gluteus minimus muscle is the smallest of the gluteal muscles. It is triangular and completely covered by the gluteus medius. The upper attachment of the gluteus minimus is from the gluteal surface of the ilium, just inferior to that of the gluteus medius. Its tendon attaches to the anterosuperior aspect of the greater trochanter of the femur (Figures 10.22 through 10.29). The gluteus medius and minimus muscles act to abduct and medially rotate the thigh. The deep group of muscles, within the gluteal region, includes the piriformis, obturator internus, obturator externus, gemellus, and quadratus femoris, which are mainly lateral rotators of the thigh at the hip joint and act to stabilize the hip joint. The piriformis muscle originates from the inner surface of the sacrum between the sacral foramina. It passes laterally and anteriorly through the greater sciatic foramen to attach to the superior boundary of the greater trochanter of the femur (Figures 10.22, 10.25, and 10.28). The actions of the piriformis muscle include lateral rotation and abduction of the thigh. The obturator internus muscle is a thick fan-shaped muscle that like the piriformis muscle originates from the pelvis. It originates from the inner border of the obturator foramen then leaves the pelvis though the lesser sciatic foramen to reach its attachment to the greater trochanter of the femur (Figures 10.22, 10.26, and 10.29). Its primary actions are the same as those of the piriformis muscle: lateral rotation and abduction of the thigh. The obturator externus muscle arises from the outer border of the obturator foramen in the pelvis to essentially mirror the obturator internus muscle. It courses laterally around the posterior side of the neck of the femur to insert into the medial side of the greater trochanter and acts to laterally rotate the thigh (Figures 10.6, 10.22, 10.26, and 10.29). The two gemellus muscles (superior and inferior) are located along the superior and inferior boundaries of the obturator internus muscle and tendon (Figures 10.6 and 10.22). The superior gemellus muscle arises from the ischial spine, whereas the inferior gemellus muscle arises from the ischial tuberosity. Both muscles join with the tendon of the obturator internus muscle to insert into the medial surface of the greater trochanter (Figures 10.6, 10.22, and 10.29). The gemellus muscles also act to laterally rotate and abduct the thigh. The rectangular-shaped quadratus femoris muscle is located inferior to the obturator internus and gemellus muscles. It arises from the lateral border of the ischial tuberosity then courses laterally to insert on the intertrochanteric crest of the femur. The primary action of the quadratus femoris muscle is lateral rotation of the thigh (Figures 10.22, 10.23, 10.26, and 10.29). The muscles of the gluteal compartment are identified in Figures 10.21 through 10.29 and their functions are given in Table 10.1.
Muscles of the Anterior Thigh Compartment
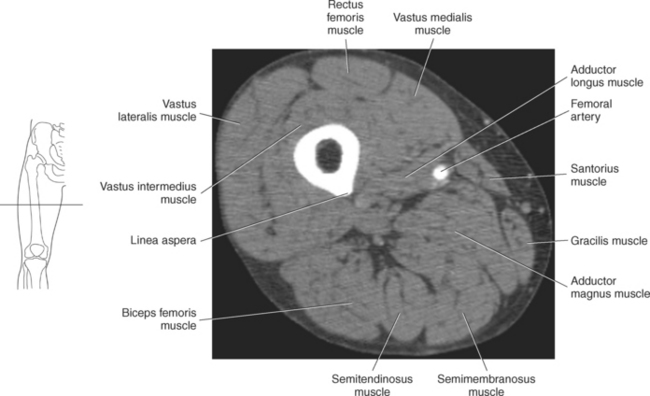
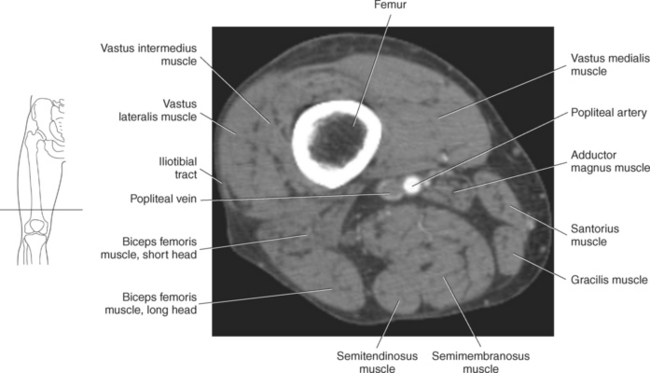
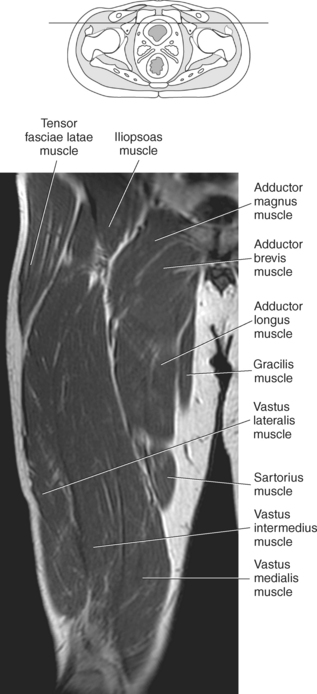
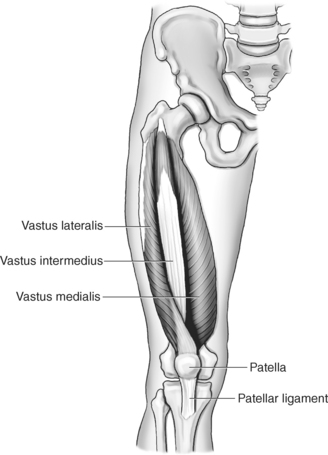
The muscles in the anterior compartment of the thigh act both to flex the hip joint and extend the knee joint. They include the iliopsoas muscle of the pelvis and the sartorius, quadriceps femoris, and tensor fasciae latae of the leg. These muscles are demonstrated in Figures 10.30 through 10.45 and described in Table 10.2. The powerful iliopsoas muscle is composed of the psoas major and iliacus muscles (Figures 10.27, 10.28, and 10.30). The psoas major muscle arises from the transverse processes of the lumbar vertebrae and courses inferiorly within the pelvis. It exits the pelvis as it courses under the inguinal ligament to enter the anterior compartment of the thigh. The tendon of the psoas major joins with the tendon of the iliacus muscle to pass anterior to the hip joint capsule and attach to the lesser trochanter of the femur. The iliacus muscle arises from the iliac fossa and courses along the lateral side of the psoas major muscle in the pelvis. These muscles act conjointly in flexing the thigh at the hip and stabilizing the hip joint. The sartorius muscle is known as the longest muscle in the body; it extends from the anterior superior iliac spine to the medial surface of the tibia near the tuberosity (Figures 10.30 through 10.45). It acts to flex, abduct, and laterally rotate the thigh. The biggest muscle in the body is the quadriceps femoris muscle, which covers almost all of the anterior surface and sides of the femur. It originates as four heads (rectus femoris, vastus lateralis, vastus medialis, and vastus intermedius) to create a powerful extensor of the knee (Figures 10.30 through 10.46). The superior ends of the four heads of the quadriceps femoris muscle arise from different locations, but their inferior tendons merge to form the quadriceps ligament that courses over the patella and continues as the patellar ligament in the knee (Figure 10.30). The rectus femoris originates from the anterior inferior iliac spine, the vastus lateralis from the greater trochanter and lateral lip of the linea aspera of the femur, the vastus medialis from the intertrochanteric line and medial lip of the linea aspera of the femur, and the vastus intermedius from the anterior and lateral surfaces of the body of the femur. All the parts of the quadriceps femoris act to extend the leg at the knee joint and through the actions of the rectus femoris, flex the hip joint. The tensor fascia latae muscle lies on the lateral side of the thigh, enclosed between two layers of the fascia. It is a short, thick, teardrop-shaped muscle located on the outer front corner of the ilium. As its name implies, it tightens the lateral fascia, thereby enabling the thigh muscles to act with increased power. It abducts, medially rotates, and flexes the thigh and helps to keep the knee extended. It originates from the anterior superior iliac spine and anterior part of the iliac crest and ends where the muscle inserts in the iliotibial tract (Figures 10.25, 10.26, 10.28, 10.29, and 10.30 through 10.42). The iliotibial tract, also called the iliotibial band or IT band, is a long, wide band of fascia that lies over the muscles on the outer surface of the thigh. This band is a thickening of the normal fascia that surrounds the entire leg. It arises from tendinous fibers of the tensor fascia latae and the gluteus maximus muscles. Acting almost like a ligament, this tendon helps mainly to stabilize the knee joint but also acts in flexing and extending the knee. It extends downward to insert on the lateral condyle of the tibia (Figures 10.30 through 10.42).
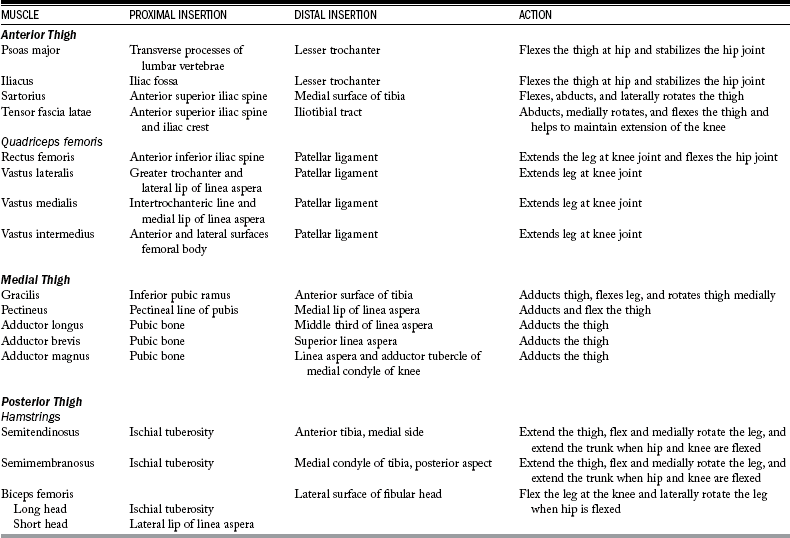
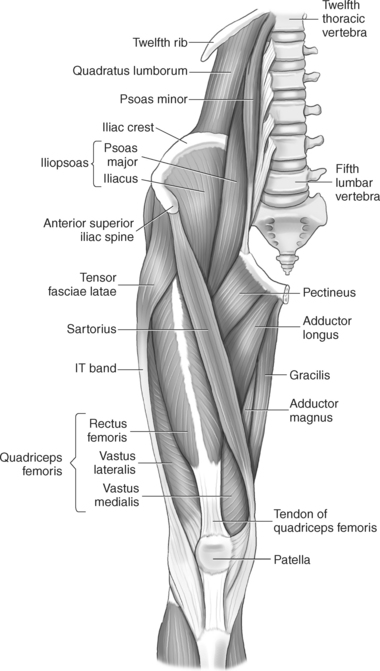
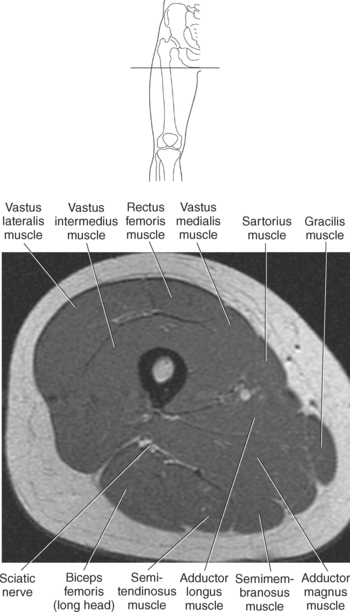
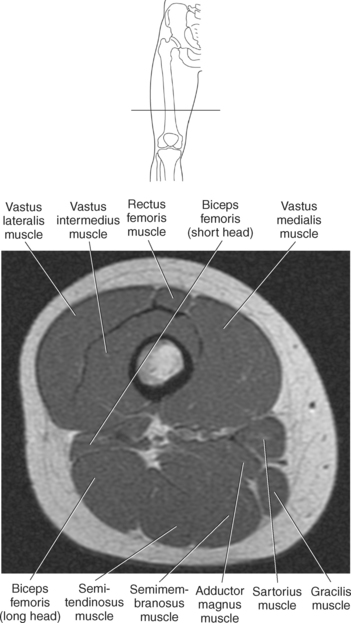
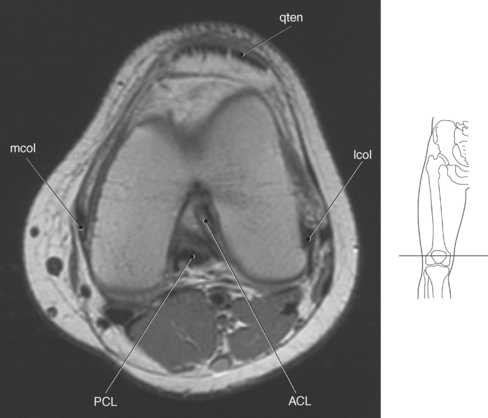
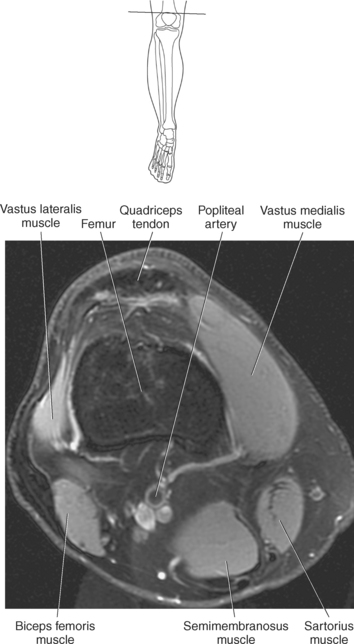
Figure 10.36 Axial, T1-weighted MR scan of distal femur.
Key: mcol, Medial collateral ligament; qten, quadriceps tendon; lcol, lateral collateral ligament; ACL, anterior cruciate ligament; PCL, posterior cruciate ligament.
The muscles of the anterior thigh compartment are identified in Figures 10.30 through 10.45, and their functions are given in Table 10.2.
Muscles of the Medial Thigh Compartment
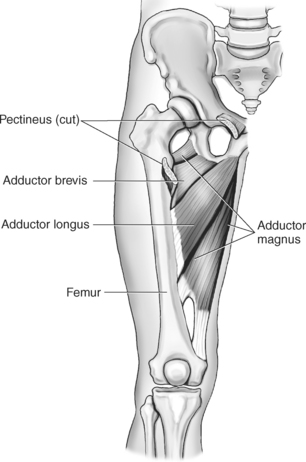
Adduction is the primary action of the medial thigh muscles. These muscles include the gracilis, pectineus, adductor longus, adductor brevis, and adductor magnus muscles, which are demonstrated in Figures 10.30 through 10.47 and described in Table 10.2. The long straplike gracilis muscle lies along the medial side of the thigh and knee. The gracilis muscle extends from the inferior ramus of the pubis and is the only medial thigh group to cross the knee joint as it inserts onto the anterior surface of the tibia just inferior to the medial condyle. In addition to adducting the thigh, the gracilis muscle acts to flex the leg and helps to rotate the thigh medially. Arising from the pectineal line of the pubis is the short, flat pectineus muscle. It lies medial to the psoas major muscle in the superior thigh, then narrows as it courses inferiorly to insert on the medial lip of the linea aspera, at the pectineal line, distal to the lesser trochanter of the femur (Figures 10.29 and 10.30). It acts to adduct and flex the thigh. The adductor muscle group, as named, acts to adduct the thigh and is composed of three muscles, the adductor longus, adductor brevis, and adductor magnus (Figures 10.30 through 10.45 and 10.47). These muscles originate at the pubic bone and fan out to insert along the length of the medial aspect of the femur. The adductor longus muscle is the most anterior muscle in the adductor group and attaches to the middle third of the linea aspera of the femur. The shorter adductor brevis muscle lies deep to the pectineus and adductor longus muscles. Its distal attachment is between the lesser trochanter and superior end of the linea aspera of the femur. The largest and most medial of the adductor group is the adductor magnus. It is situated posterior to the adductor brevis and adductor longus and anterior to the semitendinosus and semimembranosus muscles. It forms a large triangular sheet of muscle in the thigh and is composed of two parts, an adductor part and a hamstring part. The adductor portion of the adductor magnus has an extensive distal attachment on the linea aspera of the femur, whereas the hamstring part attaches to adductor tubercle on top of the medial condyle of the femur. The muscles of the medial thigh compartment are identified in Figures 10.30 through 10.47, and their functions are given in Table 10.2.
Muscles of the Posterior Thigh Compartment
The semitendinosus, semimembranosus, and biceps femoris are collectively known as the hamstrings (Figures 10.21 and 10.31 through 10.45). They make up the large mass of muscles that can be palpated on the posterior aspect of the thigh and are involved with extension of the hip, flexion of the knee, and rotation of the flexed knee. The semitendinosus muscle extends from the ischial tuberosity, courses on the medial aspect of the femur, then continues inferiorly around the medial tibial condyle and attaches to the medial side of the anterior tibial surface (Figures 10.21 and 10.31 through 10.39). It, along with the semimembranosus muscle, acts to extend the thigh, flex and medially rotate the leg, and extend the trunk when the thigh and leg are flexed. The semimembranosus also originates from the ischial tuberosity but attaches to the posterior part of the medial condyle of the tibia (Figures 10.21 and 10.31 through 10.39). The biceps femoris, as named, has two heads (long and short). The long head extends from the ischial tuberosity, whereas the short head extends from the lateral lip of the linea aspera of the femur. The biceps femoris extends inferiorly over the lateral part of the posterior surface of the knee to insert on the lateral surface of the fibular head. It acts to flex the leg at the knee joint and laterally rotate the leg when the leg is flexed. The muscles of the posterior thigh compartment are identified in Figures 10.21 and 10.31 through 10.45, and their functions are given in Table 10.2.
KNEE AND LOWER LEG
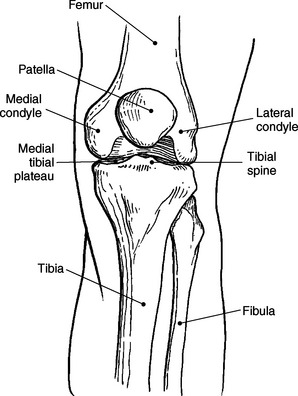
The bones that contribute to the knee joint and lower leg are the femur, tibia, patella, and fibula (Figure 10.48 and Figure 10.49). Cartilage covers the articular surfaces of the femur, tibia, and patella and helps to provide smooth movement within the knee joint.
Distal Femur
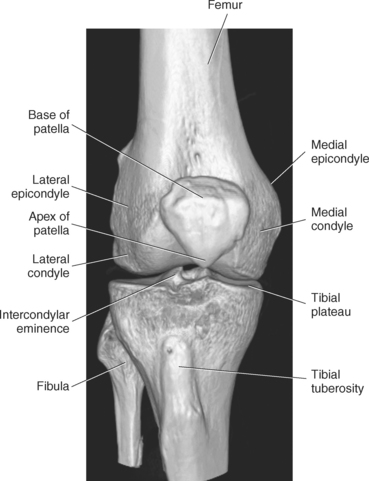
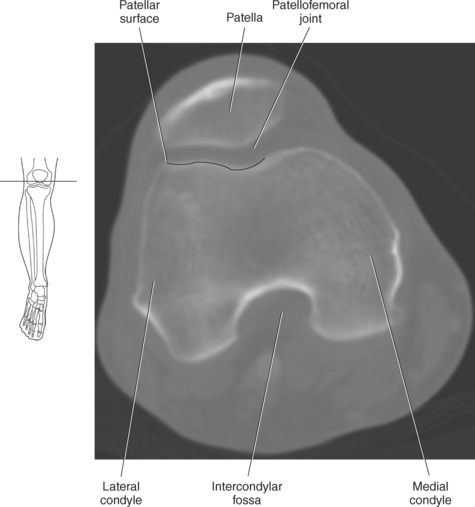
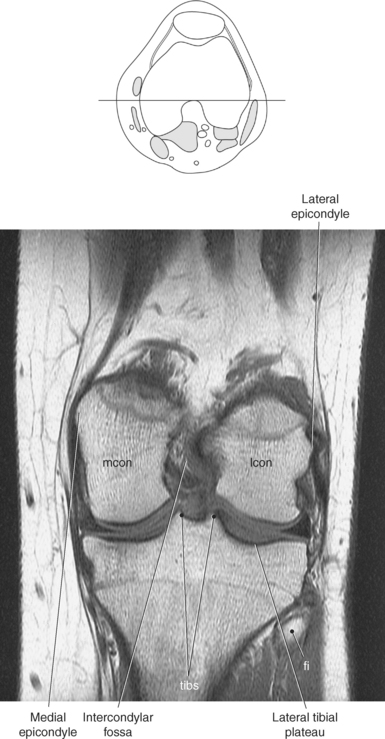
The distal portion of the femur broadens into two articular cartilage—covered projections called the medial and lateral condyles (Figures 10.50 through 10.54). The lateral femoral condyle is wider in front than in back, whereas the medial femoral condyle remains more consistent in width. The femoral condyles are connected anteriorly by the smooth patellar surface and separated posteriorly by the intercondylar fossa (Figure 10.51). On the side of each condyle is a raised edge called the medial and lateral epicondyle for the attachment of ligaments and muscles (Figures 10.52 and 10.53). A small projection located above the medial epicondyle is the adductor tubercle, which serves as an attachment for a portion of the adductor magnus muscle (Figures 10.9 and 10.11). On the posterior surface of the distal femur is a triangular area called the popliteal surface. The base of the triangle is located at the intercondylar line, which marks the beginning of the intercondylar fossa. The sides of the triangle are formed by the medial and lateral supracondylar lines, which are continuations of the linea aspera (Figures 10.9 and 10.11).
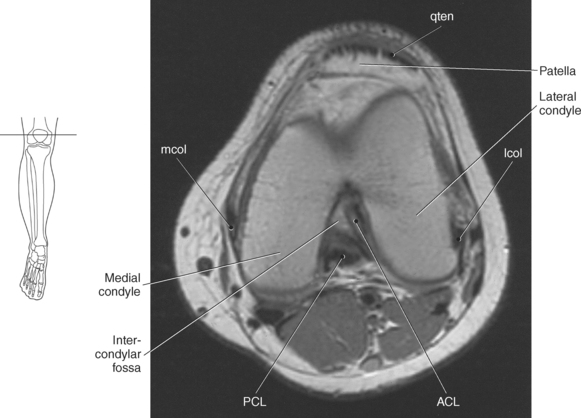
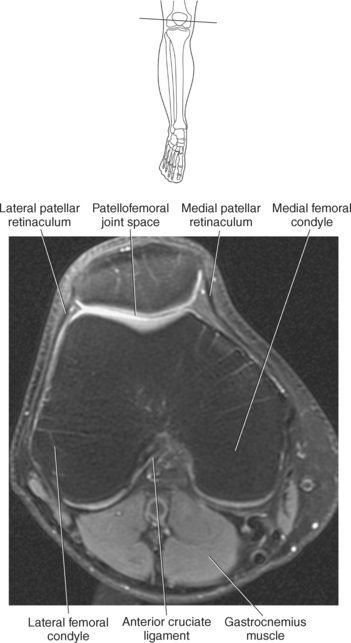
Figure 10.50 Axial, T1-weighted MR scan of distal femur.
Key: mcol, Medial collateral ligament; qten, quadriceps tendon; lcol, lateral collateral ligament; ACL, anterior cruciate ligament; PCL, posterior cruciate ligament.
Tibia
The tibia, also called the shin bone, has a widened proximal end that has two cartilaginous projections: the medial and lateral condyles (Figure 10.55). The superior articular surface of both condyles has a flattened surface called the tibial plateaus for articulation with the femoral condyles (Figures 10.55 through 10.57). The tibial condyles are separated by the intercondylar eminence (tibial spine), which ends in two peaks called the medial and lateral intercondylar tubercles; attachment sites for ligaments (Figures 10.48, 10.49, 10.52, and 10.55). The lateral tibial condyle has a small articular surface called the articular fibular surface, which articulates with the head of the fibula (Figures 10.58 and 10.59). The shaft of the tibia is triangular with a sharp anterior edge or crest that contains a bony projection called the tibial tuberosity for the attachment of the patellar ligament (Figure 10.60 and Figure 10.61). The medial margin of the shaft lies directly beneath the skin and is devoid of muscle, and the lateral surface serves as the attachment site for the interosseous membrane. The posterior surface has an obliquely oriented bony ridge called the soleal (popliteal) line, which gives rise to tendon fibers of the soleus muscle (Figure 10.55). The distal tibia has a flattened articular end with a medial extension that forms the medial malleolus (Figures 10.55, 10.62, and 10.63). The posterior surface of the medial malleolus has a small indentation, the malleolar groove, for the passage of the tibialis posterior and flexor digitorum longus tendons. On the lateral side of the distal tibia is a shallow indentation called the fibular notch, which provides a fibrous attachment with the distal fibula (Figures 10.55 and 10.62).
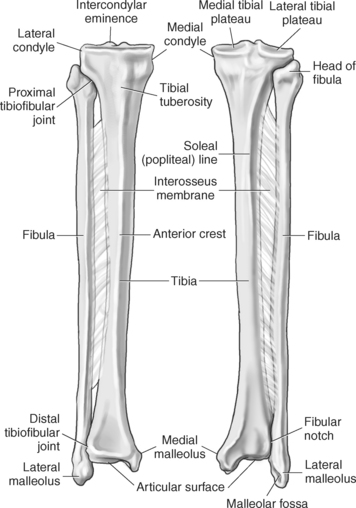
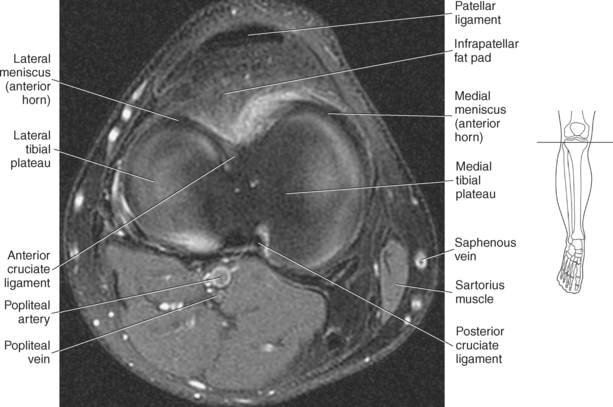
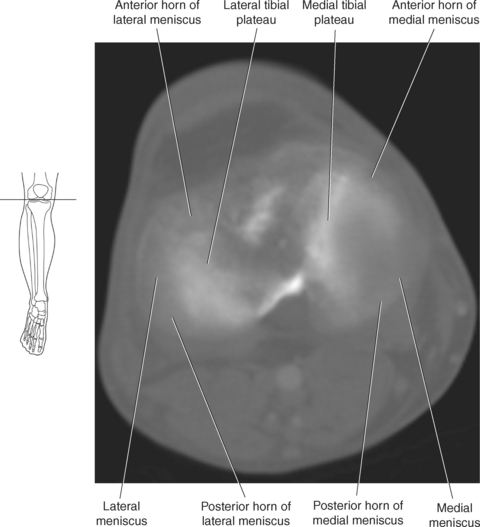
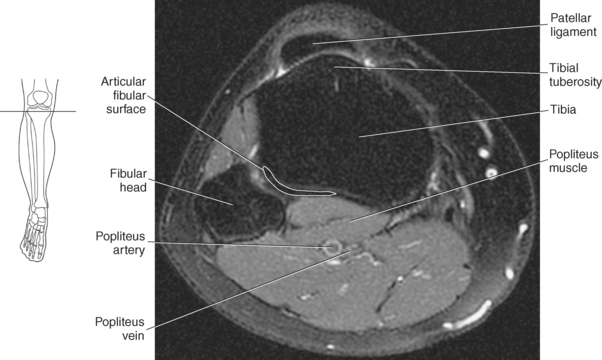
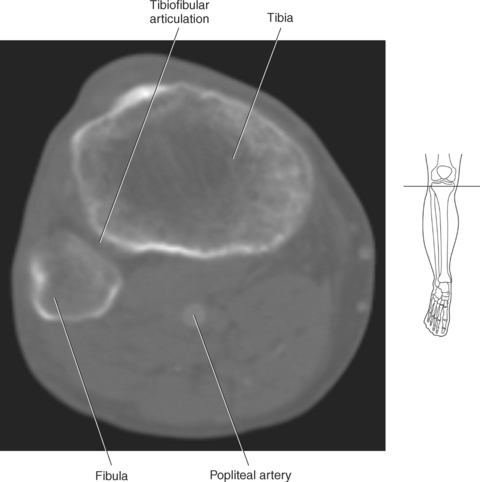
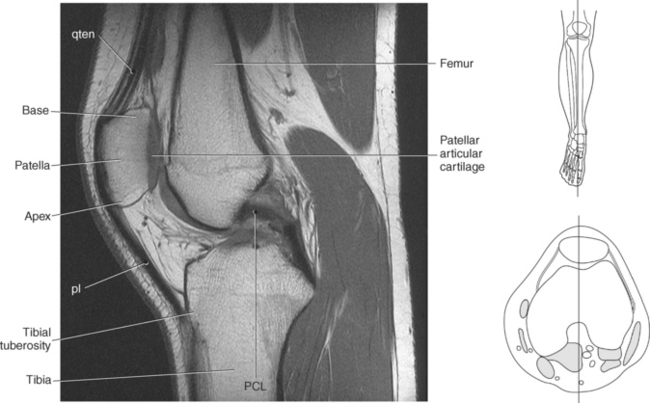
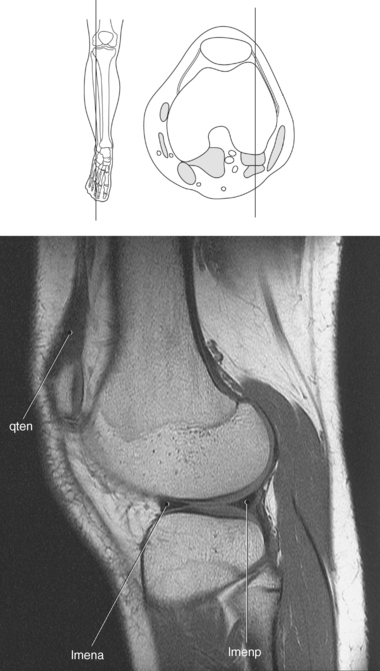
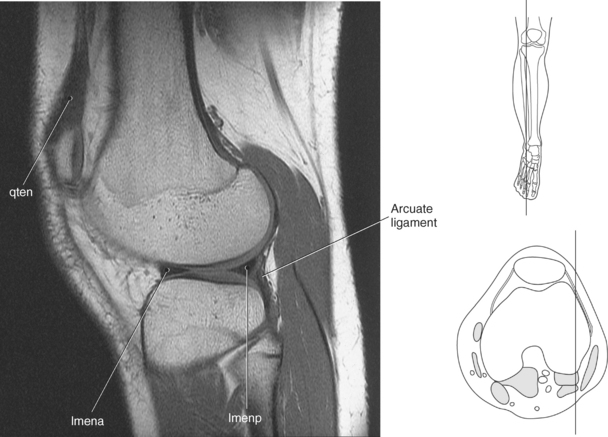
Figure 10.60 Midsagittal, T1-weighted MR scan of tibia.
Key: qten, Quadriceps tendon; pl, patellar ligament; PCL, posterior cruciate ligament.
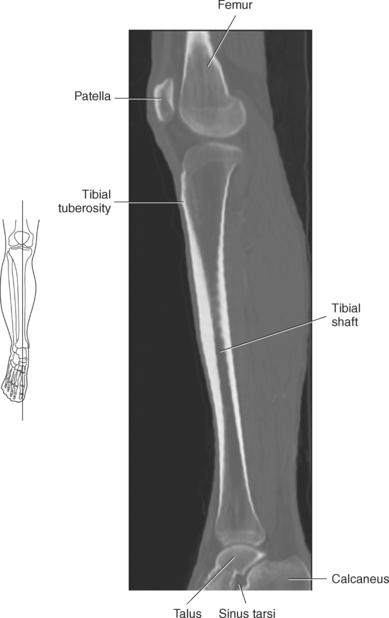
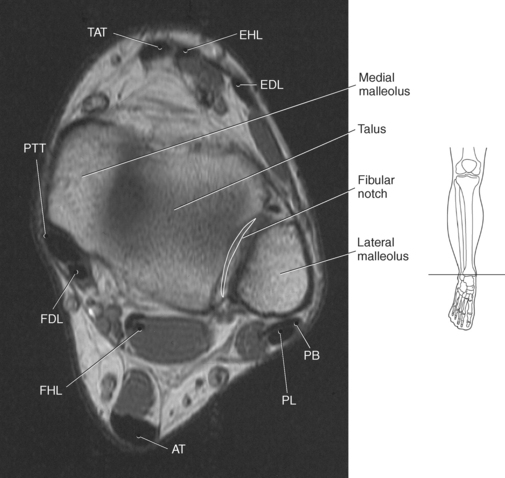
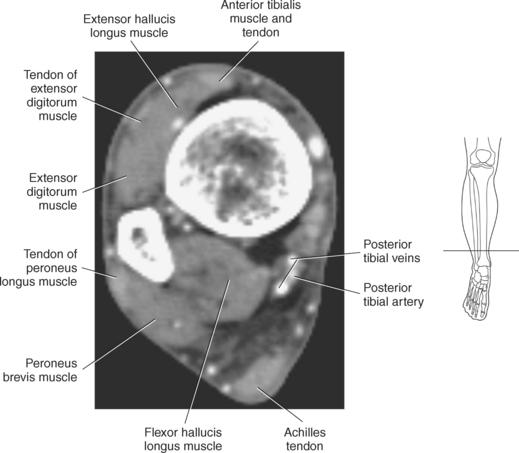
Figure 10.62 Axial, T1-weighted MR scan of ankle with malleoli.
Key: TAT, Tibialis anterior tendon; EHL, extensor hallucis longus; EDL, extensor digitorum longus; PB, peroneus brevis; PL, peroneus longus; AT, Achilles tendon; FHL, flexor hallucis longus; FDL, flexor digitorum longus; PTT, posterior tibialis tendon.
Fibula
The fibula is a long, relatively thin bone that has expanded proximal and distal ends. It is covered by muscles of the lower leg almost along its entire length. The proximal end is the head of the fibula, which ends in a sharp superior apex and medially has an articular surface for articulation with the lateral condyle of the tibia (Figures 10.55, 10.58, and 10.59). The distal end forms the lateral malleolus, which extends farther distally than the medial malleolus of the tibia (Figures 10.62 and 10.63). The medial surface of the lateral malleolus has an articular facet that articulates with the talus. Posterior to the malleolar articular surface is a small cavity called the malleolar fossa, which is where the posterior talofibular ligament is anchored. On the lateral surface of the lateral malleolus is a groove (malleolar groove) for the passage of the peroneus longus and brevis tendons (Figures 10.55, 10.62, and 10.63).
Patella and Patellofemoral Joint
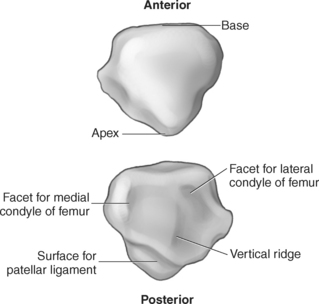
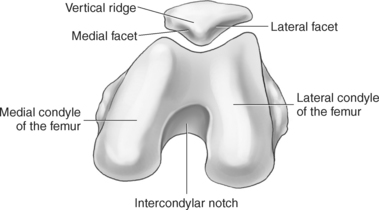
The patella is the largest sesamoid bone in the body and is embedded within the quadriceps tendon. It is a subcutaneous, flat, triangular bone with the broad base facing proximally and the pointed apex facing distally (Figure 10.64). The patella has an anterior and posterior surface and three borders: superior, medial, and lateral. The base of the patella has roughened areas for the attachment of the rectus femoris and vastus intermedius muscles, whereas the roughened medial and lateral borders receive attachment for the vastus medialis and lateralis muscles. The posterior surface is covered with the thickest articular cartilage found in the body and is centrally divided by a broad vertical ridge into medial and lateral facets. The larger lateral facet articulates with the lateral femoral condyle and the smaller medial facet articulates with the medial femoral condyle (Figure 10.65). The patella protects the anterior joint surface of the knee and functions to increase the leverage of the quadriceps extensor system (Figures 10.50, 10.51, 10.60, and 10.61).
Knee Joint
The knee is the largest and one of the most complex joints of the body. The bones that contribute to the knee joint are the femur, tibia, and patella (Figures 10.48 and 10.49). The knee has three separate articulations: two femorotibial and a patellofemoral articulation within the same synovial membrane. A supporting network of menisci, ligaments, tendons, and muscles functions together in order to meet the demands made on the knee.
Menisci and Ligaments
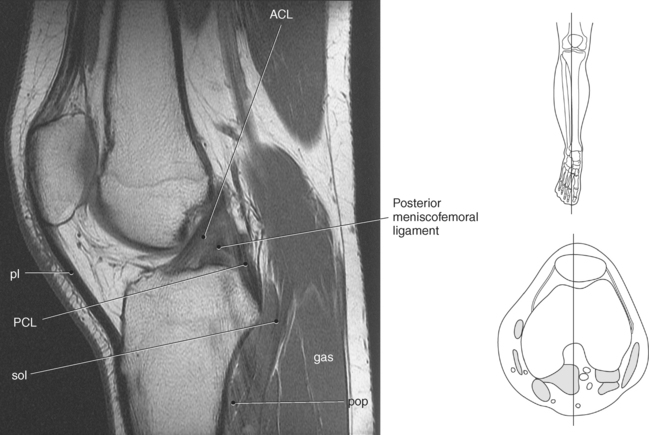
Located between the femoral condyles and tibial plateaus are the paired menisci (Figures 10.66 through 10.76). These C-shaped menisci, composed of fibrous connective tissue, cushion the articulation between the femoral condyles and tibial plateaus and are commonly divided into anterior and posterior horns. On cross section they appear wedge shaped, with a thickened outer margin that flattens medially (Figures 10.67 and 10.68). Their outer margins fuse with the joint capsule, and their anterior and posterior horns attach to the intercondylar eminence of the tibia. The menisci differ in size and shape. The medial meniscus is crescent shaped, with the posterior horn being wider than the anterior horn. The medial meniscus is attached to the medial collateral ligament, making it far less mobile than the lateral meniscus. The lateral meniscus almost forms a closed ring with anterior and posterior horns of approximately the same width. Two ligaments arise from the posterior horn of the lateral meniscus. The posterior meniscofemoral ligament (ligament of Wrisberg) passes behind the posterior cruciate ligament to attach to the medial femoral condyle. The anterior meniscofemoral ligament (ligament of Humphry) connects the posterior horn to the medial condyle, passing in front of the posterior cruciate ligament. The two menisci are connected anteriorly by the transverse ligament (Figures 10.66 and 10.67).
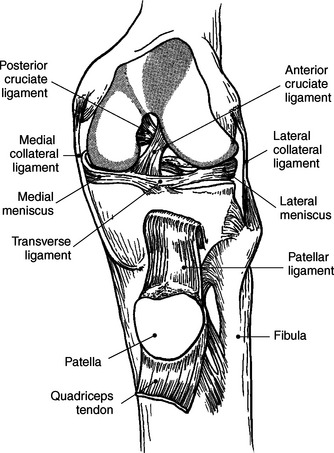
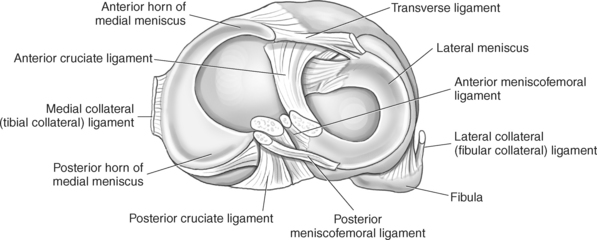
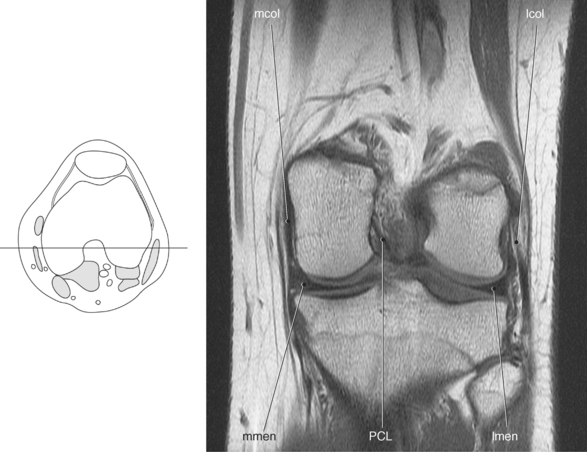
Figure 10.68 Coronal, T1-weighted MR scan of knee with meniscus and ligaments of knee.
Key: mcol, Medial collateral ligament; lcol, lateral collateral ligament; lmen, lateral meniscus; PCL, posterior cruciate ligament; mmen, medial meniscus.
Ligaments
The ligaments of the knee are divided into external (extracapsular) and internal (intracapsular) ligaments. The external ligaments are arranged around the knee and serve to strengthen and support the joint capsule. The internal ligaments are found within the joint capsule and serve to provide stability to the tibia and femur.
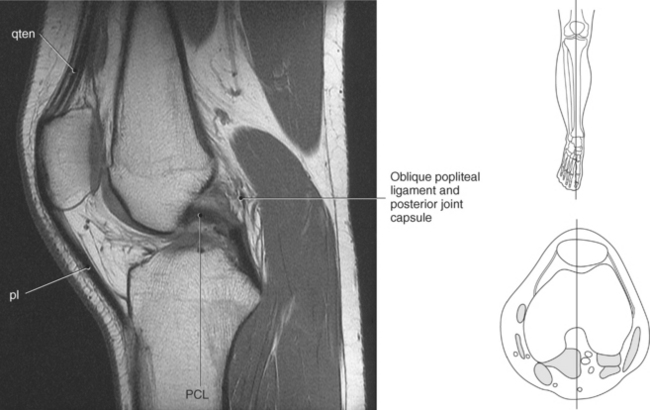
External ligaments of the knee include the collateral, patellar, and patellar retinaculum; oblique popliteal; and arcuate popliteal ligaments (Figure 10.77). The collateral ligaments provide support for the knee by reinforcing the joint capsule on the medial and lateral sides (Figures 10.66 and 10.68). The medial collateral (tibial collateral) ligament is a flattened triangular ligament that originates from the medial femoral epicondyle and extends to the medial tibial condyle, continuing to the medial shaft of the tibia. Along its path it fuses with the medial meniscus. The shorter, lateral collateral (fibular collateral) ligament is more of a rounded cord arising from the lateral femoral epicondyle and attaching to the head of the fibula. The anterior joint capsule is strengthened by the patellar ligament and patellar retinaculum. The patellar ligament is the strong thick band representing the continuation of the quadriceps tendon and extends from the patella to the tibial tuberosity (Figures 10.77, A, through 10.79). The patellar retinaculum is formed mainly by fibrous extensions and fascia of various muscles about the knee (Figure 10.70, 10.71, and 10.77, A). The medial patellar retinaculum is formed mainly by fibers from the vastus medialis muscle and runs distally to attach to the tibia anterior to the medial collateral ligament. The lateral patellar retinaculum consists of fibers from the vastus lateralis and rectus femoris muscles as well as the iliotibial tract and attaches distally to the lateral margin of the tibial tuberosity to increase stability of the lateral joint capsule. The oblique and arcuate popliteal ligaments help reinforce the dorsal surface of the joint capsule. The oblique popliteal ligament is an expansion of the semimembranosus tendon that reinforces the central region of the posterior joint capsule. It extends laterally to attach to the intercondylar line of the femur (Figures 10.71 and 10.79). The inferolateral portion of the posterior capsule is strengthened by the arcuate popliteal ligament as it passes superiorly from the apex of the fibular head to spread out over the posterior capsule with fibers continuing to the posterior intercondylar area and to the posterior surface of the lateral femoral condyle (Figure 10.71).
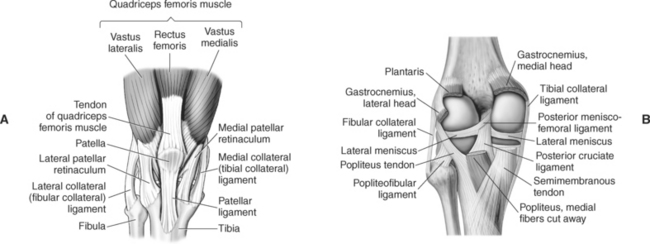
Figure 10.77 A, Anterior view of right knee with retinaculum and ligaments. B, Posterior view of right knee with joint capsule and ligaments.
Internal Ligaments
Cruciate (cross-shaped) ligaments are strong bands of fibers that provide anterior and posterior stability to the knee. The cruciate ligaments are located within the joint capsule but outside the synovial membrane (Figures 10.66 and 10.67). The anterior cruciate ligament arises from the anterior part of the tibial spine and extends to attach to the posterior part of the medial surface of the lateral femoral condyle (Figure 10.78). It helps prevent hyperextension and anterior displacement of the tibia. The posterior cruciate ligament is the stronger of the two and extends from the posterior tibial spine to the anterior portion of the medial surface of the medial femoral condyle (Figure 10.79). It functions to prevent hyperflexion and posterior displacement of the tibia (Figures 10.68 and 10.72 through 10.76).
Bursae
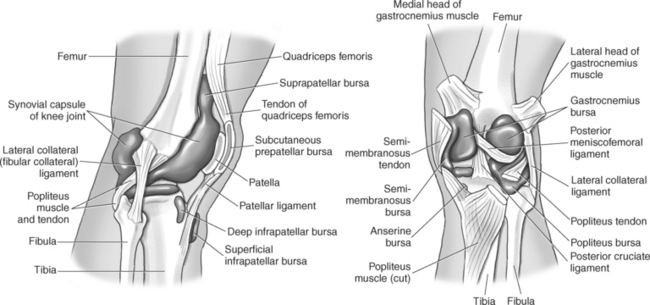
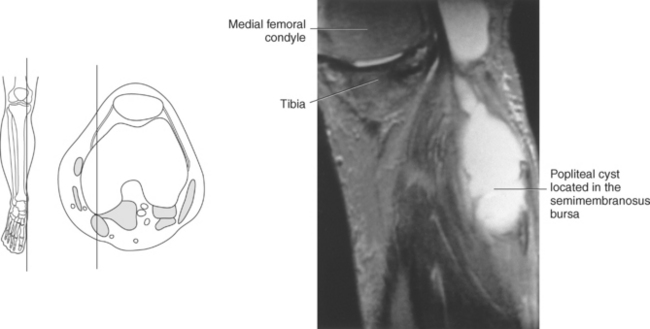
There are more than 10 bursae located around the knee joint owing to the number of muscles associated with the knee. The major bursa include the suprapatellar, prepatellar, infrapatellar (superficial and deep), gastrocnemius (medial and lateral), semimembranosus, and popliteus bursae (Figures 10.80 and 10.81). The suprapatellar (quadriceps) bursa is a large extension of the synovial capsule located between the femur and the quadriceps tendon. The subcutaneous prepatellar bursa lies between the anterior surface of the patella and the skin, whereas the superficial infrapatellar bursa lies over the patellar ligament between the skin and the tibial tuberosity. The deep infrapatellar bursa is a small bursa located beneath the patellar ligament and anterior to the tibia just above the tibial tuberosity. Behind each femoral condyle is usually a bursa for the respective head of the gastrocnemius muscle. The gastrocnemius bursae are located between each muscle head and the joint capsule. The semimembranosus bursa is located between the medial head of the gastrocnemius and semimembranosus tendon, and the small popliteus bursa lies between the lateral tibial condyle and the popliteus tendon. Bursae are difficult to see on cross-sectional images unless they are abnormal.
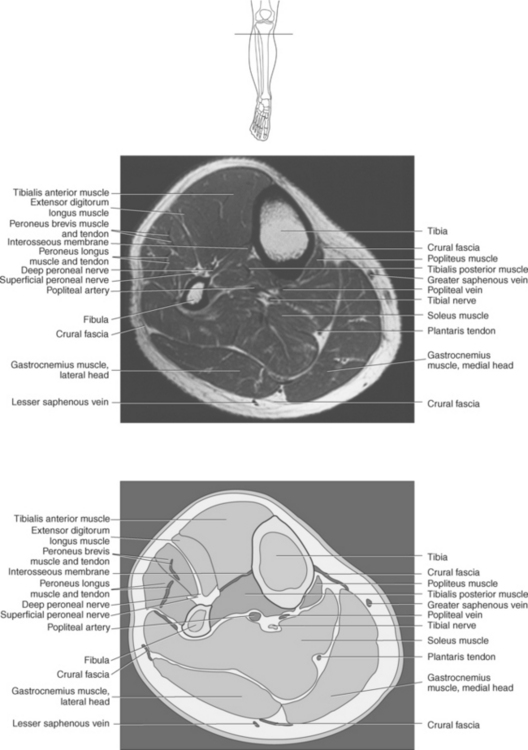
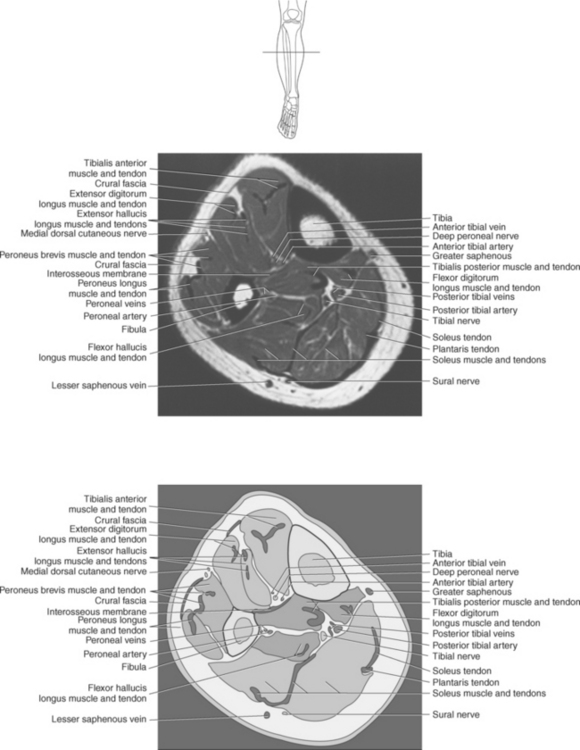
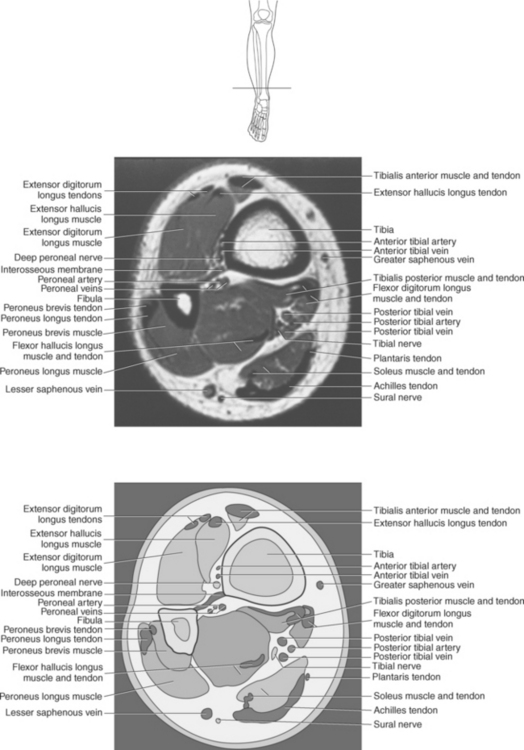
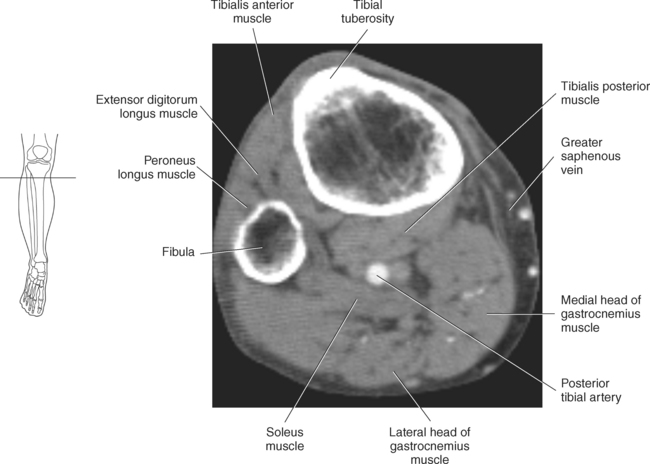
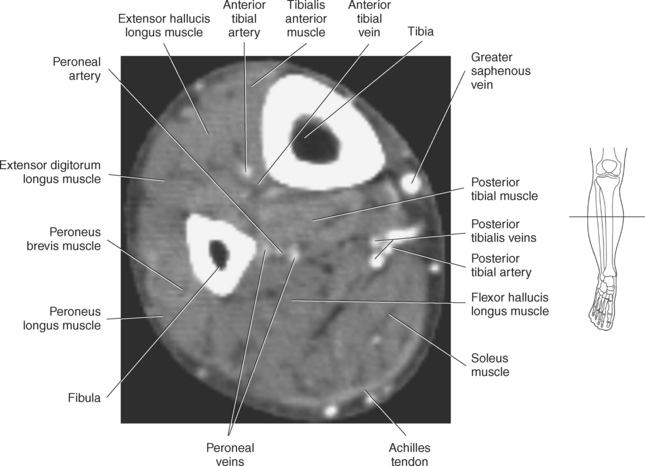
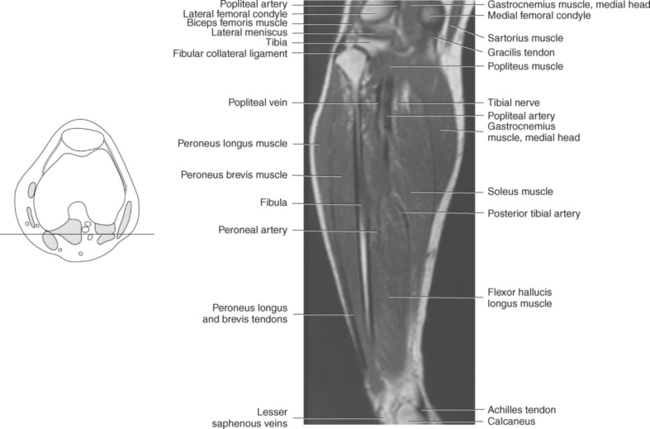
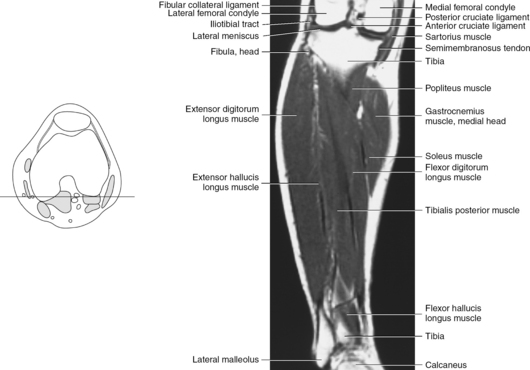
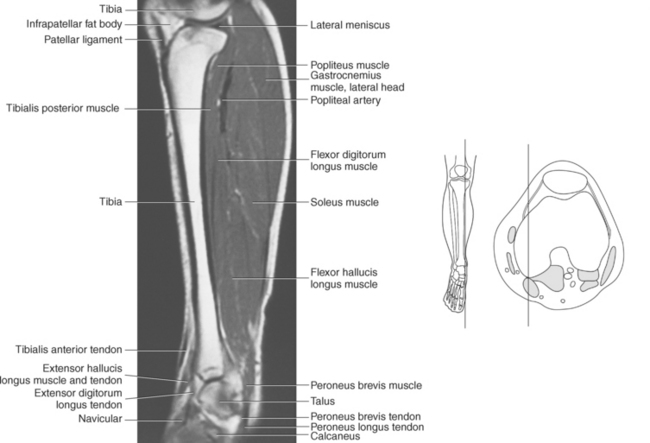
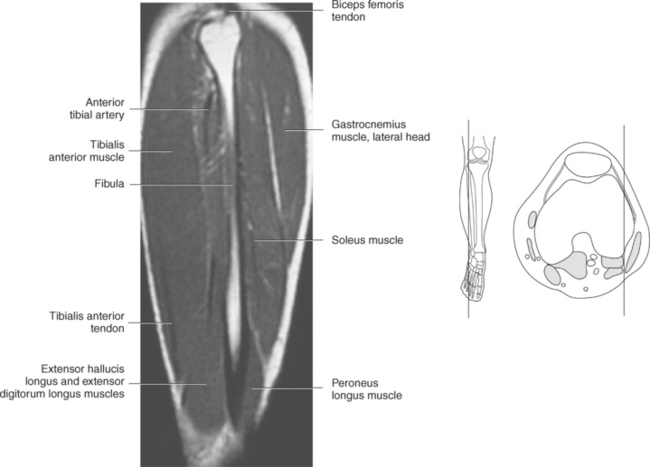
Muscles of the Lower Leg
With the exception of the popliteus, all muscles arising from the lower leg are attached to bones of the foot. The muscles of the lower leg can be classified according to their location. They are divided into anterior and posterior groups by the tibia, fibula, and interosseous membrane. The two main groups are divided again into subgroups or layers. These muscles are demonstrated in Figures 10.82 through 10.99 and described in Table 10.3.
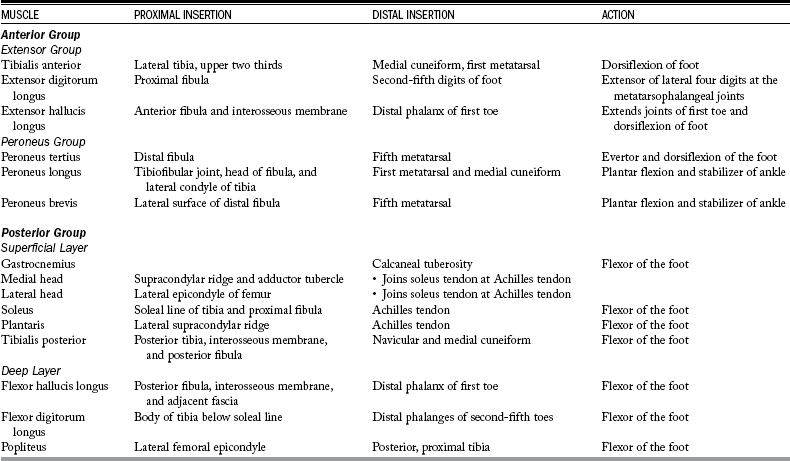
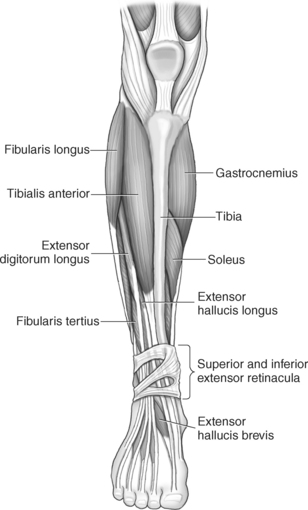
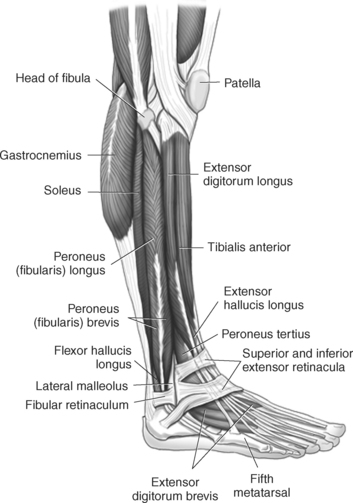
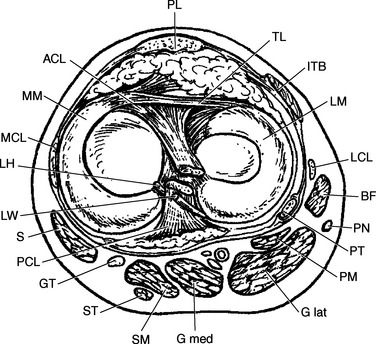
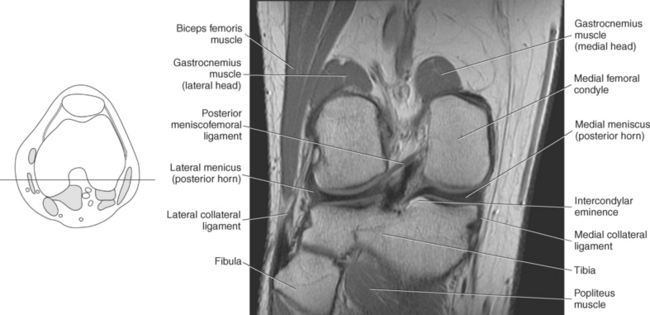
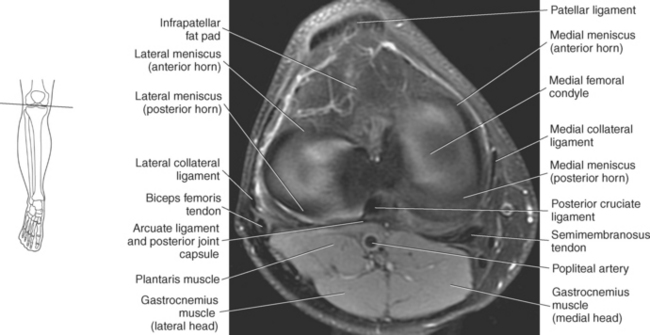
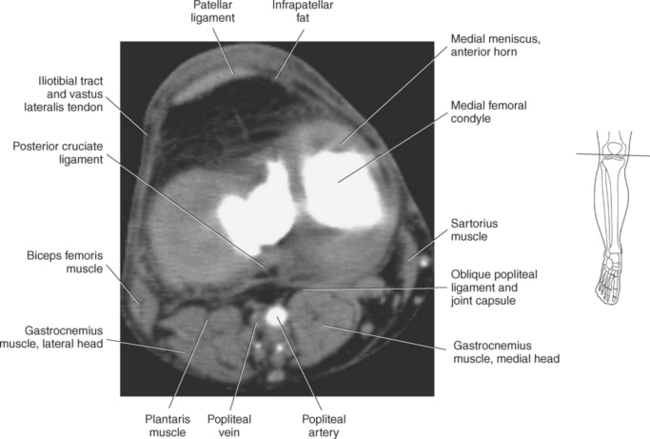
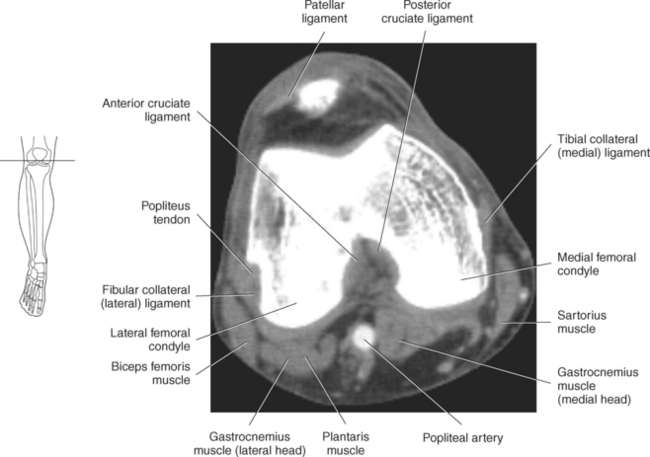
Figure 10.84 Axial view of knee with femoral condyles.
Key: PL, Patellar ligament; TL, transverse ligament; ITB, iliotibial band; LM, lateral meniscus; LCL, lateral collateral ligament; BF, biceps femoris; PN, peroneal nerve; PT, popliteus tendon; PM, plantaris muscle; G lat, gastrocnemius lateral head; G med, gastrocnemius medial head; SM, semimembranosus; ST, semitendinosus; GT, gracilis tendon; PCL, posterior cruciate ligament; S, sartorius; LW, ligaments of Wrisberg; LH, ligament of Humphrey; MCL, medial collateral ligament; MM, medial meniscus; ACL, anterior cruciate ligament.
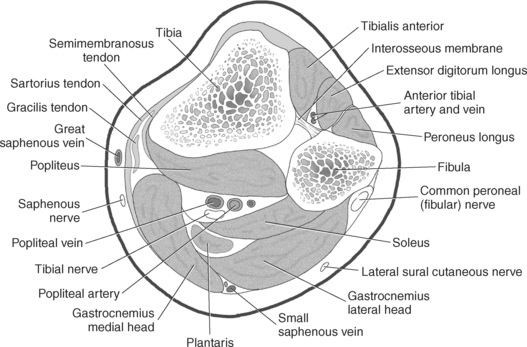
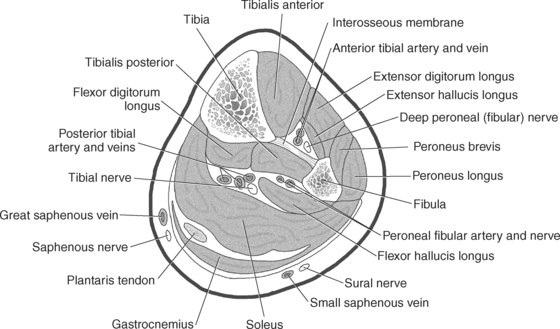
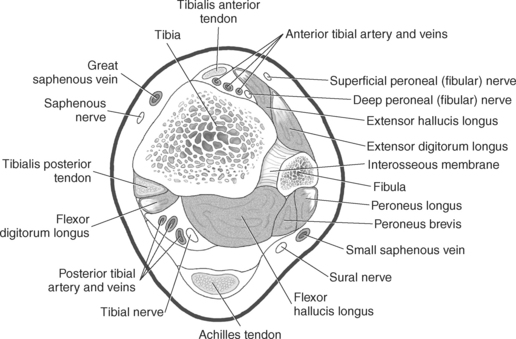
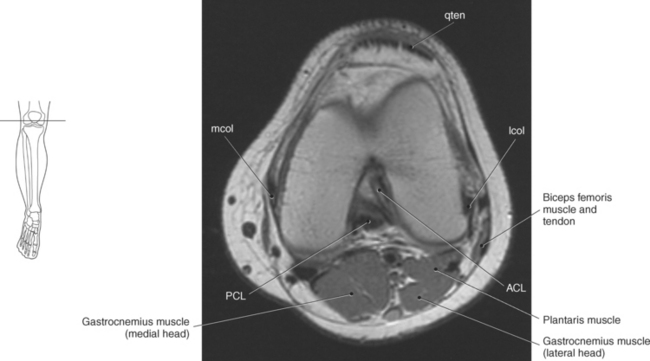
Figure 10.88 Axial, T1-weighted MR scan of distal femur.
Key: mcol, Medial collateral ligament; qten, quadriceps tendon; lcol, Lateral collateral ligament; ACL, anterior cruciate ligament; PCL, posterior cruciate ligament.
Anterior Group
The anterior muscle group can be subdivided into the extensor group located anteriorly and the peroneus group located laterally. The extensor group consists of the tibialis anterior, extensor digitorum longus, extensor hallucis longus, and peroneus tertius muscles, and the peroneus group includes the peroneus longus and brevis muscles.
Extensor Group
The tibialis anterior muscle is a long spindle-shaped muscle located just lateral to the anterior surface of the tibia. It arises from the upper two thirds of the lateral surface of the tibia and adjoining interosseous membrane, becoming tendinous over the lower third. The tibialis anterior runs distally and medially over the tibia to insert on the plantar surface of the medial cuneiform and first metatarsal. Its actions include dorsiflexion of the foot at the ankle joint and together with the tibialis posterior muscle it inverts the foot (Figures 10.82 through 10.99).
The extensor digitorum longus muscle is located lateral to the tibialis anterior muscle in the anterior aspect of the leg. It arises from the upper two thirds of the fibula and adjoining interosseous membrane and the lateral condyle of the tibia. The tendon of the extensor digitorum longus passes over the front of the ankle joint and gives rise to four separate tendons at the level of the inferior extensor retinaculum that run to the dorsal surface of the second through fifth digits. The extensor digitorum longus muscle is an extensor of the lateral four digits at the metatarsophalangeal joints (Figures 10.82 through 10.99).
The extensor hallucis longus muscle lies posterior to and between the tibialis anterior and extensor digitorum longus muscles. It arises from the middle half of the anterior fibula and interosseous membrane. The tendon of the extensor hallucis longus passes through the inferior extensor retinaculum to the base of the great toe and inserts into the distal phalanx. The extensor hallucis longus muscle extends all the joints of the great toe and provides dorsiflexion of the foot at the ankle joint (Figures 10.82 through 10.99).
The peroneus tertius muscle is considered by some to be a distal extension of the extensor digitorum longus muscle. It arises from the anterior surface of the lower fibula, and its tendon inserts on the dorsal aspect of the base of the fifth metatarsal. This muscle functions as a weak evertor and dorsiflexor of the foot at the ankle joint (Figure 10.83).
Peroneus Group
The two peroneus muscles act as plantar flexors but also stabilize the lateral ankle and longitudinal arch of the foot (Figures 10.82 and 10.83).
The peroneus (fibularis) longus muscle is located on the lateral side of the leg arising from the tibiofibular joint, the head of the fibula, and the lateral condyle of the tibia. The peroneus longus has a long belly and an even longer tendon. The tendon of the peroneus longus runs in a shallow groove behind the lateral malleolus, passing below the peroneal tubercle of the calcaneus and across the lateral side of the cuboid. It then runs obliquely across the sole of the foot to insert on the base of the first metatarsal and lateral surface of the medial cuneiform (Figures 10.82, 10.83, 10.94, and 10.95).
The peroneus (fibularis) brevis muscle is shorter and smaller than its counterpart. It lies under the peroneus longus, arising from the distal two thirds of the lateral surface of the fibula. The tendon of the peroneus brevis accompanies the tendon of the peroneus longus in a common synovial sheath behind the lateral malleolus, with the peroneus brevis just anterior to the peroneus longus. At approximately the level of the peroneal tubercle of the calcaneus, the tendons separate into their own synovial sheath, with the peroneus brevis tendon attaching to the tuberosity at the base of the fifth metatarsal (Figures 10.82, 10.83, 10.94, and 10.95).
Posterior Group
The posterior group is functionally considered the flexors, which are responsible for plantar flexion of the foot. This group is subdivided into the superficial layer consisting of the gastrocnemius, soleus, and plantaris muscles and the deep layer with the tibialis posterior, flexor hallucis longus, flexor digitorum longus, and popliteus muscles. These muscles are demonstrated in Figures 10.84 through 10.102 and described in Table 10.3.
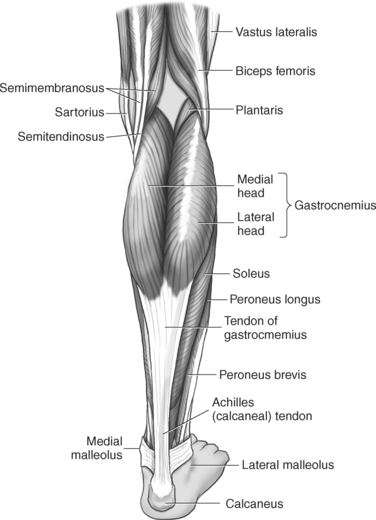
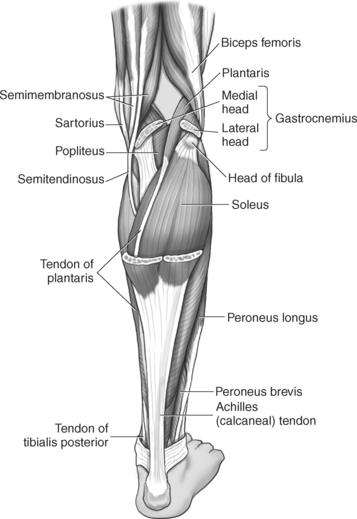
Superficial Layer
The gastrocnemius muscle is a prominent flexor of the foot and is responsible for giving the calf its shape on the back of the leg. It consists of two heads arising from the medial and lateral femoral condyles. The medial head arises from the medial supracondylar ridge and adductor tubercle on the popliteal surface of the femur. The lateral head arises just behind the lateral epicondyle on the outer surface of the lateral femoral condyle. The two heads form the lower boundaries of the popliteal fossa, and their fibers run distally where they join the tendon of the soleus muscle to form the Achilles tendon that inserts on the calcaneal tuberosity (Figures 10.84 through 10.100).
The soleus muscle is a broad, flat muscle located beneath the gastrocnemius. It arises from the soleal line on the posterior tibia and the upper third of the fibula. The muscle fibers run distally and merge with the tendon of the gastrocnemius to form the superficial Achilles tendon (Figures 10.84 through 10.101).
The plantaris muscle is a long, thin muscle that arises from the lowest part of the lateral supracondylar ridge, the adjacent popliteal surface, and joint capsule. The tendon runs inferiorly at an oblique angle between the gastrocnemius and soleus muscles to insert on the medial edge of the Achilles tendon (Figures 10.84 through 10.101).
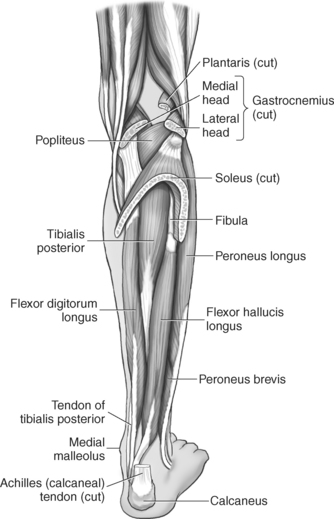
Deep Layer
The tibialis posterior muscle is the deepest muscle located on the back of the leg. It arises from the superolateral surface of the posterior tibia just below the soleal line, the interosseous membrane, and the posterior surface of the fibula. The tendon of the tibialis posterior passes through the malleolar groove of the tibia behind the medial malleolus to attach to the tuberosity of the navicular and plantar surface of the medial cuneiform bones (Figures 10.86 and 10.98 and 10.102).
The flexor hallucis longus muscle is a powerful muscle located beneath the gastrocnemius and soleus muscles. It arises from the distal two thirds of the posterior fibula, the interosseous membrane, and adjacent fascia. The tendon of the flexor hallucis longus runs distally, crossing over the dorsal aspect of the ankle, through the malleolar groove of the tibia to the sole of the foot, where it inserts into the base of the terminal phalanx of the first toe (Figures 10.86, 10.87, 10.90, 10.91, 10.94, 10.95, and 10.102).
The flexor digitorum longus muscle arises from the posterior surface of the body of the tibia immediately below the soleal line. The muscle descends along the tibial side of the leg to become tendinous just above the medial malleolus. The tendon of the flexor digitorum longus passes behind the medial malleolus to the sole of the foot, deep to the flexor hallucis longus, and divides into four individual tendons that insert into the bases of the distal phalanges of the second through fifth digits (Figures 10.86, 10.87, 10.90, 10.91, 10.94, 10.95, and 10.102).
The popliteus muscle is a thin triangular muscle that forms the lower floor of the popliteal fossa. It arises just below the lateral femoral epicondyle and extends obliquely to the triangular surface above the soleal (popliteal) line on the posterior tibia (Figures 10.85 and 10.102).
ANKLE AND FOOT
The bony anatomy of the ankle and foot includes the tarsus, metatarsus, and phalanges. The tarsus consists of seven bones: talus, calcaneus, navicular, cuboid, and three cuneiform bones. Five metatarsals and 14 phalanges make up the toes (Figures 10.103 through 10.125).
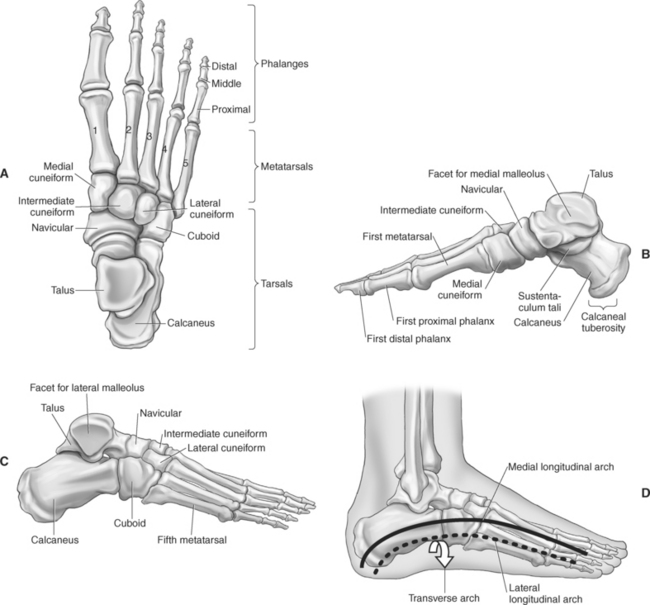
Figure 10.103 Bones of the right foot. A, Superior view. B, Medial view. C, Lateral view. D, Arches of foot.
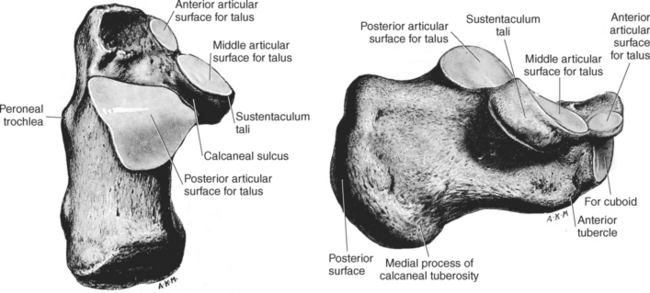
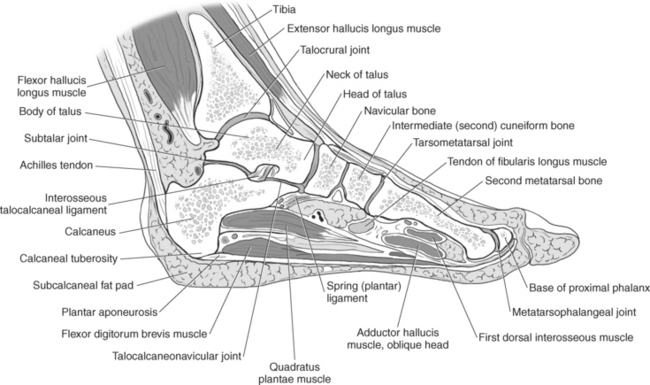
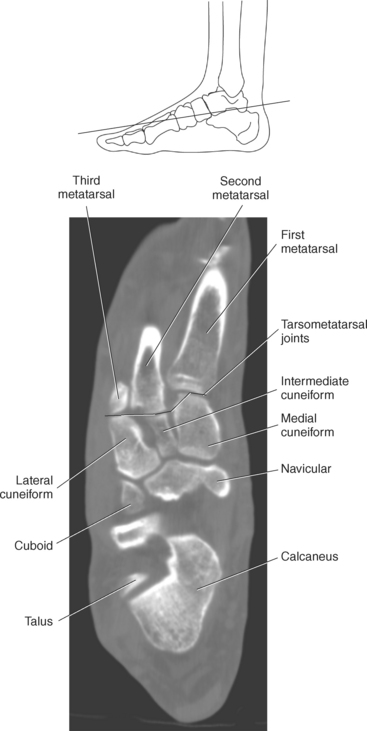
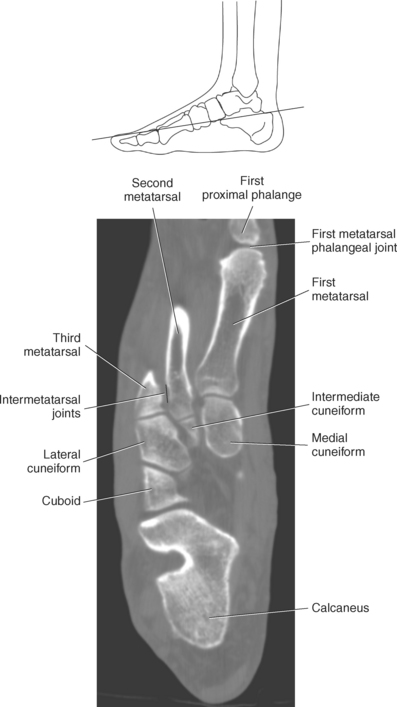
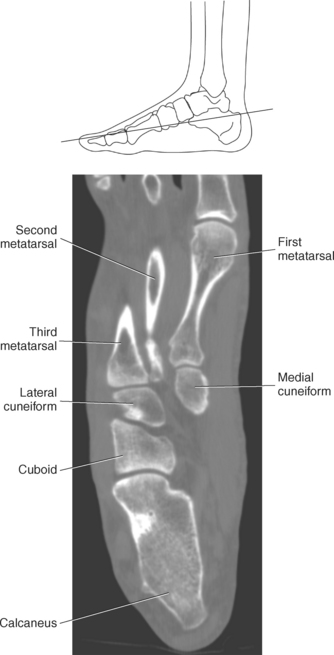
Figure 10.105 Sagittal section of foot.
Key: EHL, Extensor hallucis longus; EDL, extensor digitorum longus; af, acetabular fossa; IO, interosseus ligament; mf, medial facet; st, sinus tarsi; pf, posterior facet.
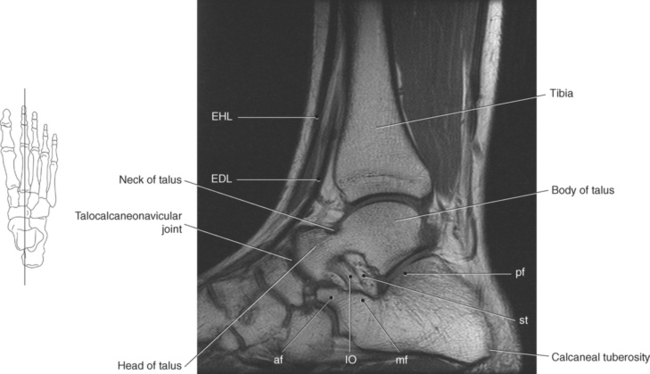
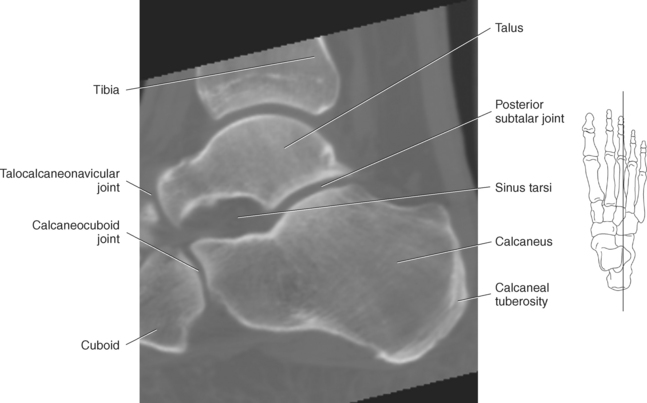
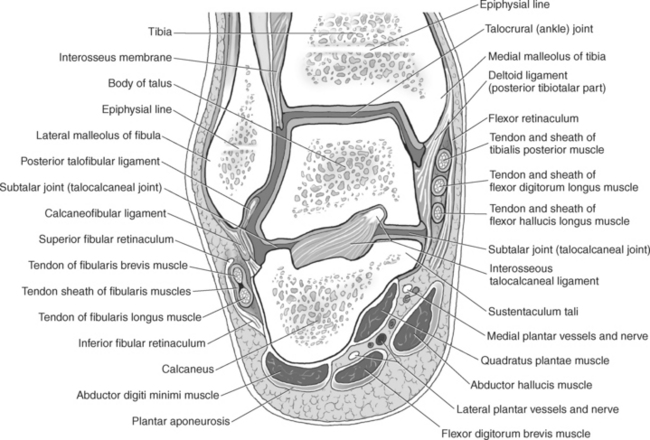

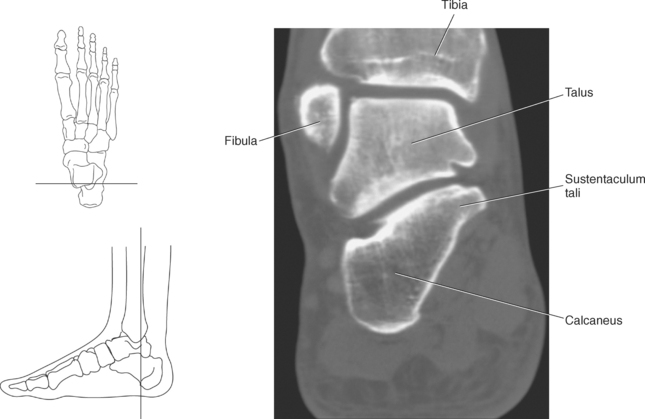
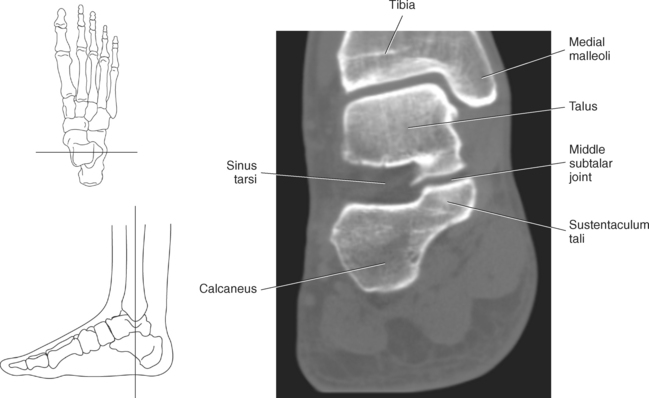
Figure 10.109 Coronal, T1-weighted MR scan of subtalar joint.
Key: ti, Tibia; del, deltoid ligament; ta, talus; C, calcaneus.
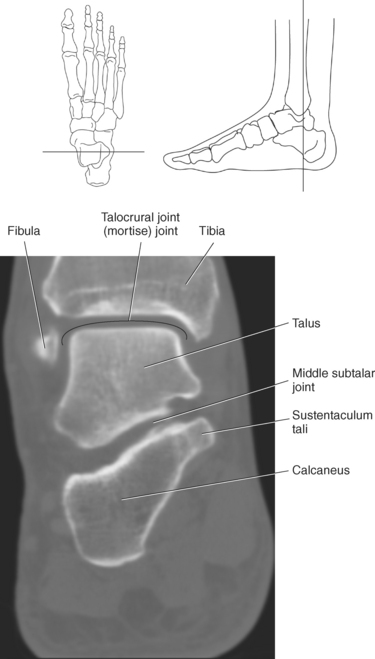
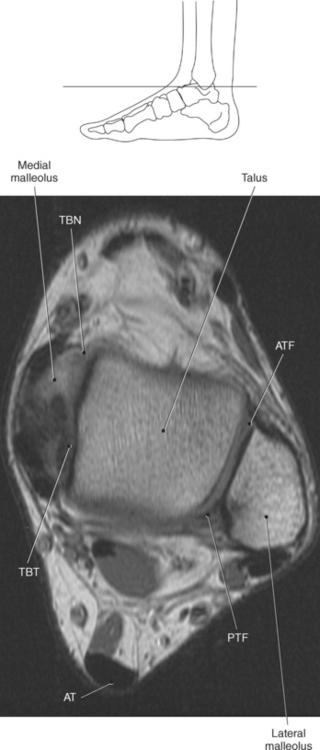
Figure 10.111 Axial, T1-weighted MR scan of ankle.
Key: TBN, Tibionavicular ligament; TBT, tibiotalar ligament; AT, Achilles tendon; PTF, posterior talofibular ligament; ATF, anterior talofibular ligament.
Tarsus
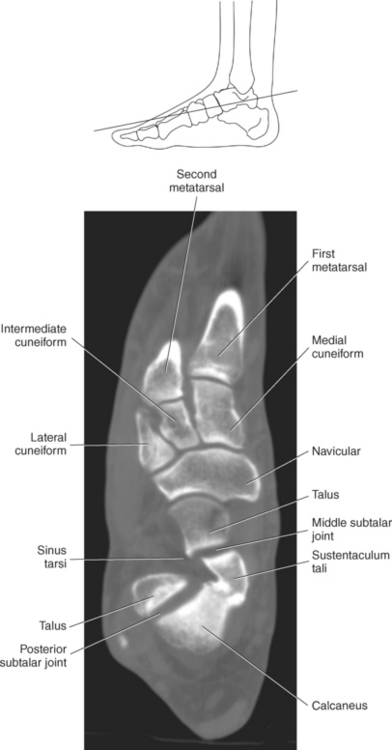
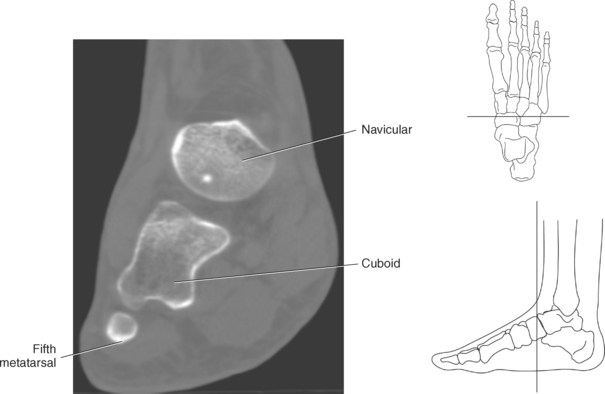
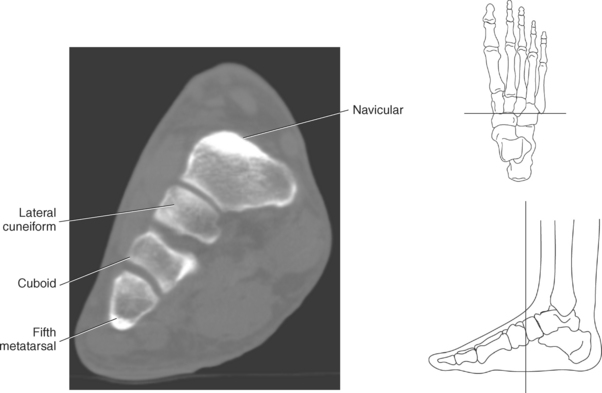
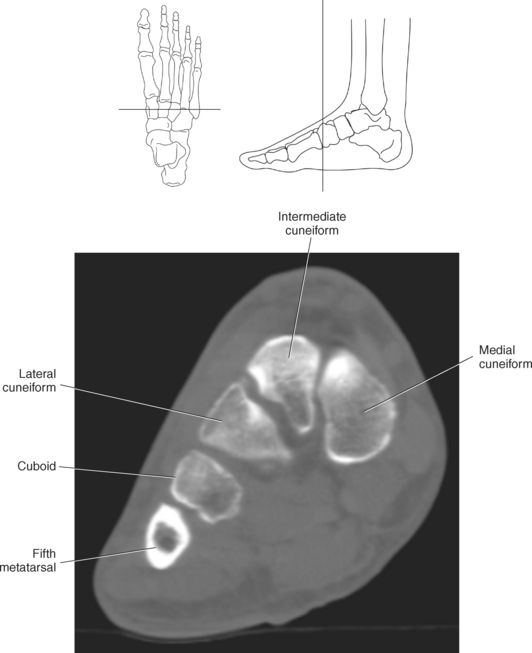
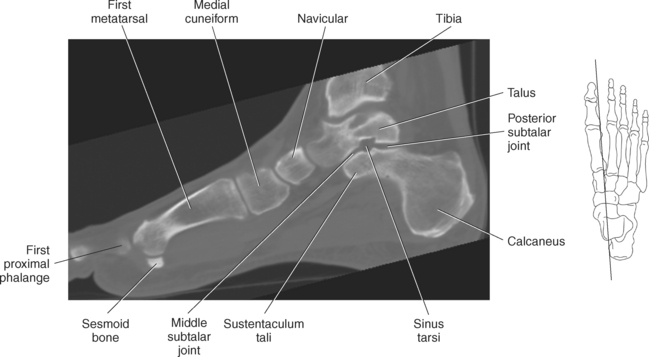
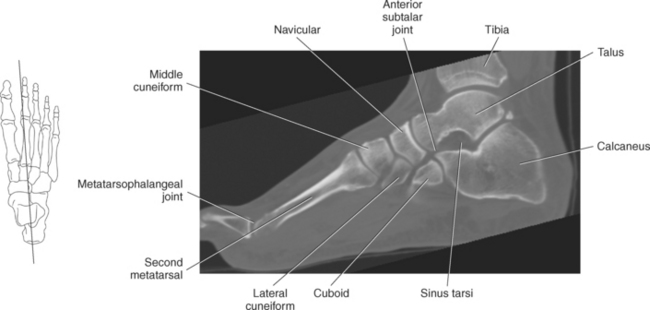
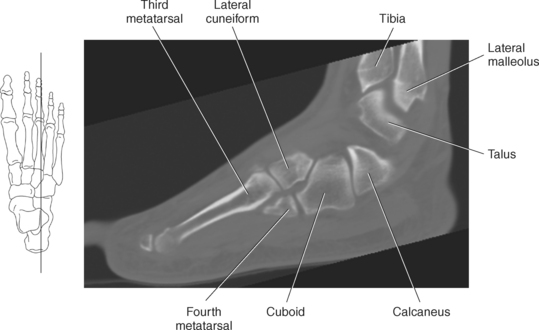
The talus (astragalus) is the second largest tarsal bone and is responsible, together with the calcaneus, for transmitting the entire weight of the body to the foot. The talus consists of a body, head, and neck. The body is wedge shaped with an upper articular surface (trochlea) that is wider in front than in back (Figures 10.103, 10.105, and 10.106). The trochlea provides articulation with the tibia (Figures 10.105 through 10.110). The head faces anteriorly to articulate with the navicular bone (Figure 10.105). The largest tarsal bone is the calcaneus, which lies beneath the talus. It has an elongated cuboid shape with a posterior surface comprising the prominence of the heel. On the medial surface of the calcaneus is a shelflike process termed the sustentaculum tali, which provides support for the talus (Figures 10.104 and 10.108 through 10.110). On the plantar surface of the posterior calcaneus is the large calcaneal tuberosity for insertion of ligaments and tendons (Figures 10.104 through 10.107). The articulation between the talus and calcaneus is termed the subtalar joint, which is composed of three articulations formed by the anterior, middle, and posterior facets (Figure 10.104). The smallest of the three is the anterior facet, which can be independent of or continuous with the middle facet. The middle facet lies on a ledge of bone projecting off the medial surface of the calcaneus at the sustentaculum tali (Figures 10.105 and 10.108 through 10.110). This shelf and the entire middle facet joint provide weight-bearing support to the medial side of the ankle. The posterior facet joint is the largest and provides support for most of the body of the talus (Figures 10.104 through 10.107). Separating this facet from the middle and anterior facet joints is the tarsal canal. This canal, containing blood vessels, fat, and the interosseous ligament, widens laterally to form the sinus tarsi (Figures 10.105 through 10.107). In addition to the talus and calcaneus, the cuboid, navicular, and three cuneiform bones comprise the remaining five tarsal bones of the foot (Figures 10.103 and 10.113 through 10.125). Lateral and anterior to the calcaneus is the cuboid bone, which articulates anteriorly with the bases of the fourth and fifth metatarsal bones. The navicular bone articulates posteriorly with the talus and anteriorly with the cuneiform bones on the medial side of the foot. The cuneiform bones are numbered from medial to lateral or termed medial, intermediate, and lateral and articulate anteriorly with the first three metatarsal bones.
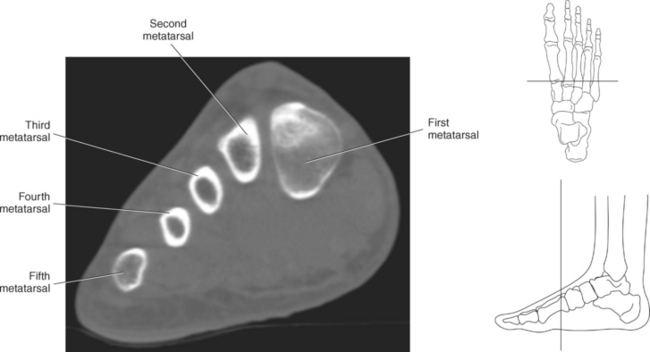
Metatarsals
The metatarsals are long, slender bones. There are five metatarsals in each foot, with each bone having a distal head, proximal base, and body or shaft in between. The heads articulate with the proximal phalanges of the toes and the bases articulate with the tarsus.
Phalanges
Each foot has 14 phalanges 3 phalanges for each toe except the great toe, which has just 2. The phalanges of the toes are shorter and stouter than their counterparts in the fingers (Figures 10.103 and 10.113 through 10.125).
Joints
The joints of the foot and ankle include the talocrural (ankle joint), intertarsal, tarsometatarsal and intermetatarsal, metatarsophalangeal, and interphalangeal joints.
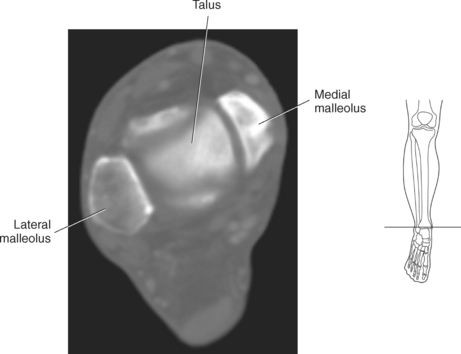
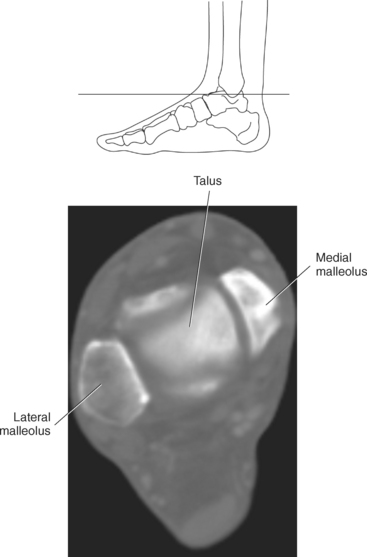
The talocrural joint (ankle joint) is created by the articulations between the tibia, fibula, and talus (astragalus). The tibia and fibula rest on the trochlear surface of the talus to form what is commonly termed the mortise joint, which allows for dorsal and plantar flexion. Both the tibia and fibula terminate distally in projections termed malleoli, which prevent medial and lateral displacement of the talus (Figures 10.108 through 10.110).
The intertarsal joints are created by the articulations between the tarsal bones and include the subtalar, talocalcaneonavicular, calcaneocuboid, transverse (mid-) tarsal, cuneonavicular, intercuneiform, and the cuneocuboid joints. The subtalar joint consists of the articulation between the talus and calcaneus and was discussed earlier (Figures 10.105 and 10.106). The subtalar joint provides the ability to invert and evert the foot. The talocalcaneonavicular and calcaneocuboid joints combine to form the transverse or midtarsal joint. This joint provides an irregular plane across the foot extending from side to side, with the talus and calcaneus located posteriorly and the navicular and cuboid located anteriorly (Figures 10.106 and 10.107). The transverse tarsal joint plays an important part in putting the spring in your step by acting as a shock absorber during the push-off phase of walking or running. The cuneonavicular, intercuneiform, and cuneocuboid joints contribute to the flexibility of the foot by providing a slight gliding movement between bones.
The tarsometatarsal joints exist between the bases of all five metatarsals and the anterior four tarsal bones (cuboid, three cuneiforms). The articulations between the tarsals and metatarsals permit only limited gliding movement between the bones (Figures 10.105 and 10.113 through 10.116). The intermetatarsal joints are the articulations between the bases of the lateral four metatarsals. The intermetatarsal joints permit a small degree of gliding between metatarsals and contribute to eversion and inversion of the foot (Figure 10.115).
Metatarsophalangeal Joints
The heads of the metatarsals articulate with the bases of the proximal phalanges at the metatarsophalangeal joints (Figures 10.105, 10.115, and 10.124). This articulation provides flexion and extension of the toes.
Interphalangeal Joints
The heads of the phalanges articulate with the bases of the more distal phalanges to create the interphalangeal joints. The interphalangeal joints are hinge joints that permit plantar and dorsiflexion of the phalanges (Figure 10.103).
Arches
The bones of the foot are arranged in transverse and longitudinal arches that provide the flexibility and resiliency of the foot to support the weight of the body, absorb shocks, and provide spring and lift during activity (Figure 10.103, B through D). The longitudinal arch (plantar arch) has two parts: one on the lateral side of the foot (lateral longitudinal arch) and one on the medial side of the foot (medial longitudinal arch). The bony landmarks for the longitudinal arch on the medial side is the head of the first metatarsal anteriorly and the calcaneal tuberosity posteriorly. On the lateral side the bony landmarks include the head of the fifth metatarsal anteriorly and the calcaneal tuberosity posteriorly. The medial longitudinal arch is more elastic and is associated with greater curvature, whereas the lateral longitudinal arch is flatter and less flexible because it makes contact with the ground. The longitudinal arches provide a firm base for support of the body in the upright position. The transverse arch is formed by the distal row of tarsal bones (cuboid, three cuneiforms) and the bases of the metatarsals that create a domed curve across the foot. The transverse arch is the major weight-bearing arch of the foot and helps to distribute body weight over the base of the foot. The integrity of arches is maintained by the tarsal, tarsometatarsal, and intermetatarsal joints and their supporting ligaments (Figure 10.103, D).
Fascia, Retinacula, and Ligaments
As in the wrist, fascia in various regions of the ankle will thicken to form retinacula. The retinacula form sheaths for stabilizing tendons crossing over the joints of the ankle. They are called the flexor, extensor, and peroneal retinacula after the tendons they serve (Figures 10.126 through 10.142). The flexor retinaculum is located between the medial malleolus and the medial tubercle of the calcaneus. It forms four tunnels for the passage of the tendons of the tibialis posterior, flexor digitorum longus, flexor hallucis longus muscles, and the posterior tibial vessels and nerve. The extensor retinaculum consists of two portions: an upper portion (superior extensor retinacula) and lower portion (inferior extensor retinacula). The superior extensor retinaculum runs horizontally between the tibia and fibula just above the ankle joint. It transmits the tendons of the tibialis anterior and extensor hallucis muscles. The inferior extensor retinaculum splits into two bands that extend across the dorsum of the foot, originating from the upper surface of the calcaneus and sinus tarsi. The upper band of the inferior extensor retinaculum attaches to the medial malleolus, whereas the lower band extends to the fascia on the medial side of the foot. The tendons of the extensor digitorum longus and peroneus tertius muscles run deep to the inferior extensor retinaculum. The peroneal retinacula split into two bands, forming the superior and inferior peroneal retinaculum. The superior peroneal retinaculum extends from the lateral side of the calcaneus to the posterior border of the lateral malleolus. The inferior peroneal retinaculum extends from the lateral side of the calcaneus to blend with the fibers of the inferior extensor retinaculum. The superior and inferior peroneal retinacula transmit the tendons for the peroneus brevis and peroneus longus muscles.
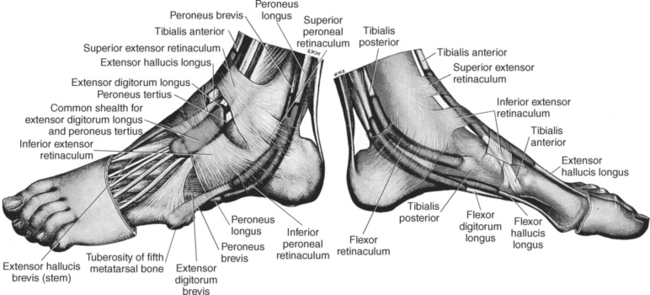
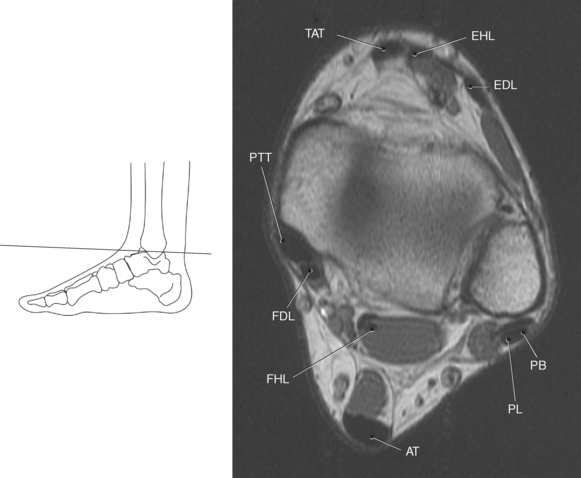
Figure 10.127 Axial, T1-weighted MR scan of ankle ligaments and tendons.
Key: TAT, Tibialis anterior tendon; EHL, extensor hallucis longus; EDL, extensor digitorum longus; PB, peroneus brevis; PL, peroneus longus; AT, Achilles tendon; FHL, flexor hallucis longus; FDL, flexor digitorum longus; PTT, posterior tibialis tendon.

Figure 10.129 Axial, T1-weighted MR scan of ankle ligaments and tendons.
Key: PTT, Posterior tibialis tendon; Sp, spring ligament; PB, peroneus brevis; PL, peroneus longus; AT, Achilles tendon; FHL, flexor hallucis longus; FDL, flexor digitorum longus.
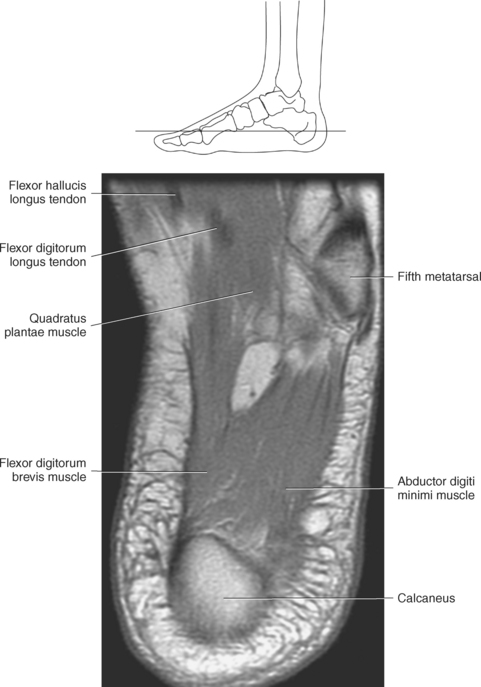
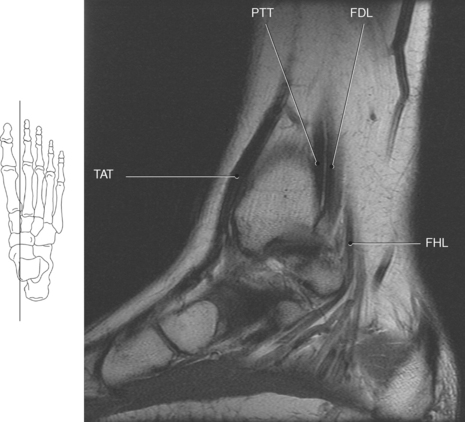
Figure 10.132 Sagittal, T1-weighted MR scan of ankle ligaments and tendons.
Key: TAT, Tibialis anterior tendon; PTT, posterior tibialis tendon; FDL, flexor digitorum longus; FHL, flexor hallucis longus.
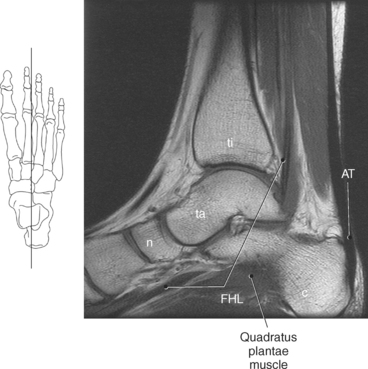
Figure 10.133 Sagittal, T1-weighted MR scan of ankle ligaments and tendons.
Key: ti, tibia; ta, talus; n, navicular; c, calcaneus; AT, Achilles tendon; FHL, flexor hallucis longus.
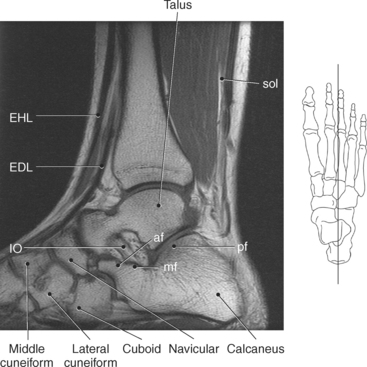
Figure 10.134 Sagittal, T1-weighted MR scan of ankle ligaments and tendons.
Key: FDL, flexor digitorum longus; EHL, extensor hallucis longus; EDL, extensor digitorum longus; sol, soleus muscle; IO, interosseus ligament; af, acetabular fossa; mf, medial facet; pf, posterior facet.

Figure 10.135 Sagittal, T1-weighted MR scan of ankle ligaments and tendons.
Key: fi, Fibula; PB, peroneus brevis; PL, peroneus longus.
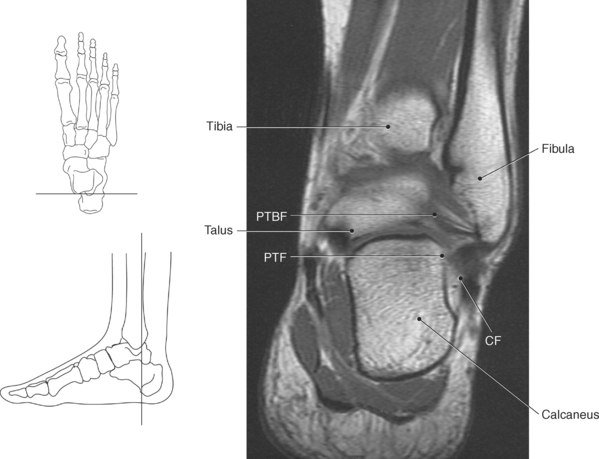
Figure 10.136 Coronal, T1-weighted MR scan of ankle ligaments and tendons.
Key: PTBF, posterior tibiofibular ligament; PTF, posterior talofibular ligament; CF, calcaneofibular ligament.
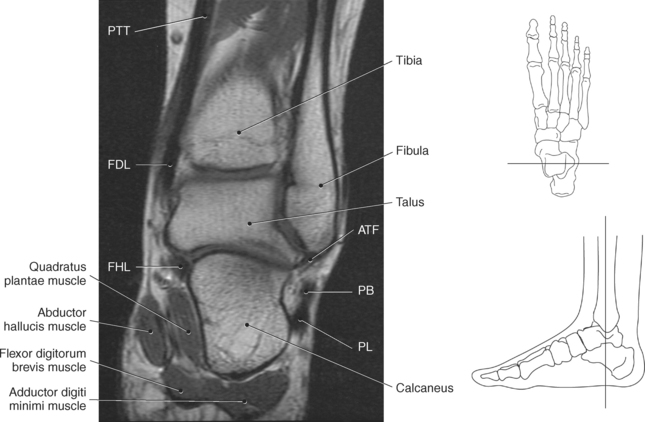
Figure 10.137 Coronal, T1-weighted MR scan of ankle ligaments and tendons.
Key: PTT, posterior tibialis tendon; FDL, flexor digitorum longus; FHL, flexor hallucis longus; ATF, anterior talofibular ligament; PB, peroneus brevis; PL, peroneus longus.
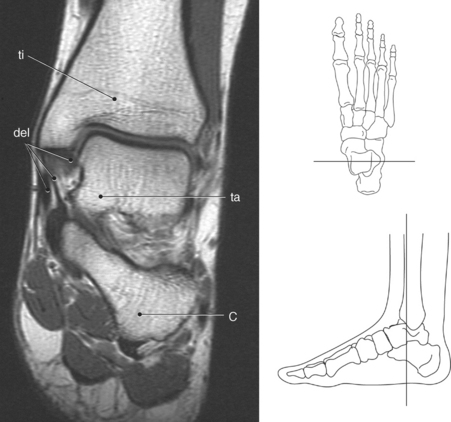
Figure 10.138 Coronal, T1-weighted MR scan of ankle ligaments and tendons.
Key: ti, tibia; del, deltoid ligaments; C, calcaneus.
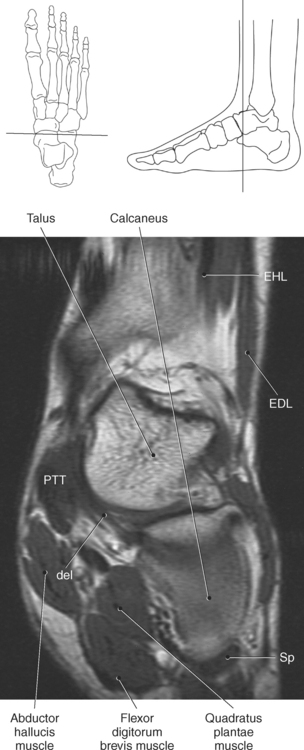
Figure 10.140 Coronal, T1-weighted MR scan of ankle ligaments and tendons.
Key: PTT, Posterior tibialis tendon; del, deltoid ligament; EHL, extensor hallucis longus; EDL, extensor digitorum longus; Sp, spring ligament.
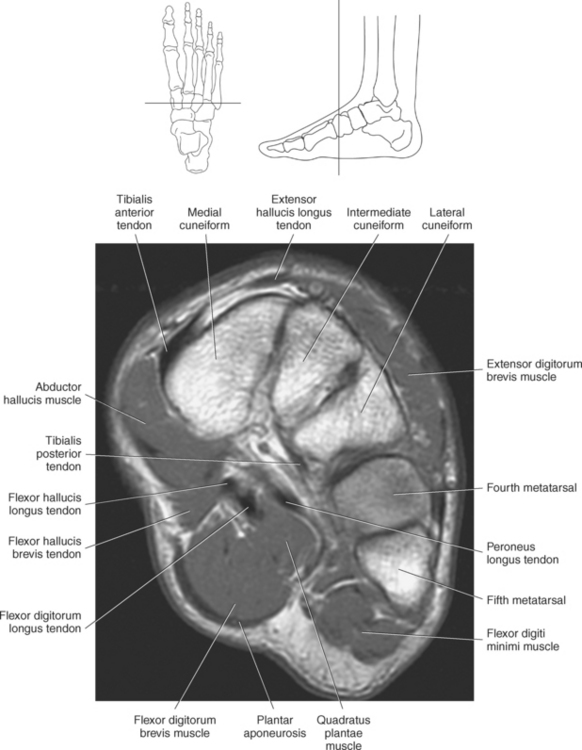

Figure 10.142 Coronal, T1-weighted MR scan of ankle ligaments and tendons.
Key: I, Interosseus muscle; LM, lumbrical muscle.
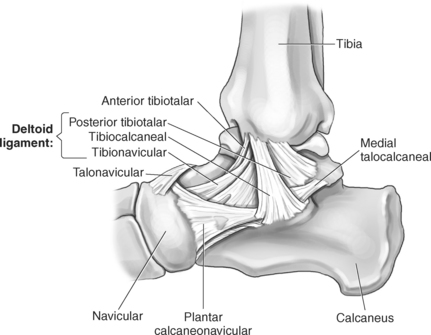
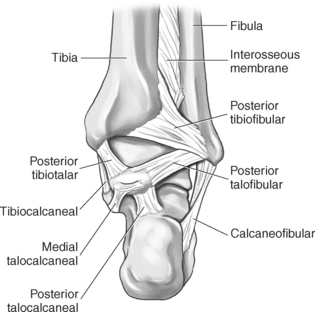
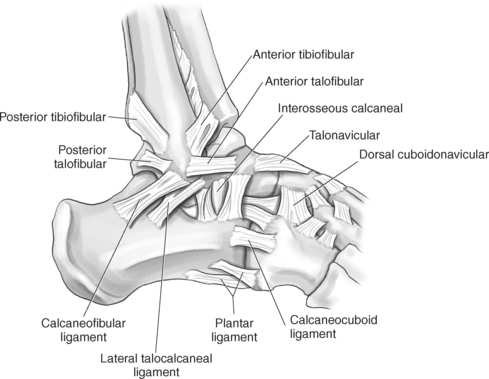
In addition to the retinacula, another area of thickened fascia is located on the plantar surface of the foot. The plantar aponeurosis (fascia) is approximately 80 layers thick, creating some of the thickest fascia within the human body. It begins at the inferior aspect of the calcaneus and spreads anteriorly into five separate slips that create the fibrous flexor sheaths of the toes (Figure 10.105). The plantar fascia is extremely important in maintaining the longitudinal arch of the foot. Other support structures of the ankle and foot include a complex architecture of multiple ligaments that provide necessary stability. The main support structures of the ankle include the deltoid ligament, lateral ligaments, spring (plantar) ligament, and interosseous ligament. The deltoid ligament provides medial support and is the strongest ligament in the ankle joint. It arises from the medial malleolus and fans out into three bands: tibiotalar ligament, tibiocalcaneal ligament, and tibionavicular ligament to insert on the talus, calcaneus, and navicular bone, respectively (Figure 10.143). The lateral border of the ankle joint is strengthened by several ligaments termed the anterior talofibular, calcaneofibular, posterior talofibular, anterior tibiofibular, and posterior tibiofibular ligaments (Figure 10.144 and Figure 10.145). All of these ligaments originate at the fibular malleolus and insert on the adjacent bone structures. The spring (plantar) ligament is a triangular band of fibers that arises from the sustentaculum tali and attaches to the posterior surface of the navicular bone (Figure 10.105). It is an important ligament in maintaining the longitudinal arch of the foot. A strong band of tissue binding the talus to the calcaneus is the interosseous (talocalcaneal) ligament, which is obliquely oriented in the sinus tarsi (Figures 10.105, 10.106, 10.108, 10.109, and 10.127 through 10.142).
Ligaments of the Toes
The metatarsophalangeal joint is strengthened laterally by strong collateral ligaments, dorsally from fibers of the extensor tendons, and underneath by the plantar ligament. The plantar ligament is a thick fibrocartilaginous plate that attaches to the proximal base of the proximal phalanges, the collateral ligaments, and the deep transverse metatarsal ligaments. The collateral ligaments extend from the heads of the metatarsal, fanning out to attach to the bases of the proximal phalanges. The heads of the second through fifth metatarsals are interconnected by the deep transverse metatarsal ligament. In a similar manner as the metatarsophalangeal joints, the interphalangeal joints are strengthened laterally by collateral ligaments and on the plantar surface by the plantar ligament.
Tendons
The musculotendinous structures of the ankle can be divided into posterior, anterior, medial, and lateral groups.
Posterior Group
The posterior group is composed of the single Achilles tendon (calcaneal), the largest and most powerful tendon of the body. The Achilles tendon arises from the gastrocnemius and soleus muscles and attaches to the calcaneal tuberosity on the posterior aspect of the calcaneus (Figures 10.101, 10.105, and 10.127 through 10.133).
Anterior Group
The anterior group is made up of the tibialis anterior, extensor hallucis longus, and extensor digitorum longus tendons, which are named medial to lateral and act to extend and dorsiflex the foot. The tibialis anterior muscle becomes tendinous at the distal tibia and attaches to the plantar and medial aspects of the first cuneiform and metatarsal bones. The tendon of the extensor hallucis longus muscle originates from the anterior fibula and inserts on the great toe. The most lateral of this group is the extensor digitorum longus tendon, which originates at the level of the lateral malleolus and inserts on the second through the fifth digits (Figures 10.126 through 10.142).
Medial Group
The medial group is composed of the posterior tibialis tendons, flexor digitorum longus, and flexor hallucis longus tendons, which as a group act to invert and plantar flex the foot. The posterior tibialis tendon fans out in multiple strands that insert on the plantar aspect of the sustentaculum tali, navicular bone, first cuneiform bone, and second through fourth metatarsal bones. Coursing posterior and lateral to the posterior tibialis tendon is the flexor digitorum longus tendon, which at its terminal portion inserts on the second through fourth phalanges. The tendon of the flexor hallucis longus muscle curves under the sustentaculum tali and then courses along the plantar surface of the foot to insert on the great toe (Figures 10.126 through 10.142).
Lateral Group
The two peroneus tendons, peroneus longus and peroneus brevis, make up the lateral group and act to evert, weakly plantar flex the foot, and stabilize the ankle joint laterally. These two tendons share a common tendinous sheath behind the lateral malleolus. Below the malleolus they diverge into separate tendon sheaths, with the peroneus brevis tendon inserting on the base of the fifth metatarsal and the peroneus longus tendon curving beneath the calcaneus to insert on the base of the first metatarsal and medial cuneiform bones (Figures 10.126 through 10.142).
Muscles
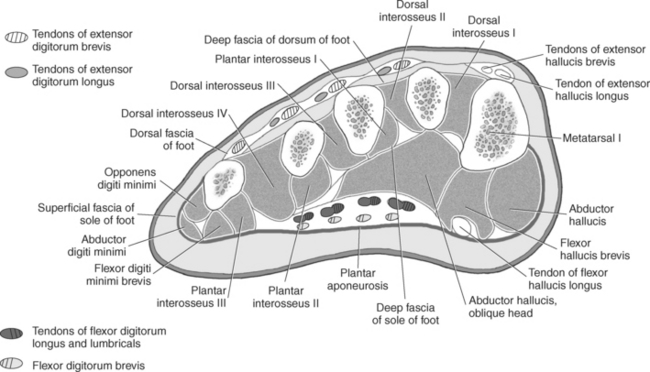
The muscles of the foot are divided into the muscles of the dorsum and muscles of the sole of the foot. These muscles are demonstrated in Figures 10.127 through 10.142 and 10.146 through 10.148 and are described in Table 10.4. The dorsal muscles include the extensor digitorum brevis and the extensor hallucis brevis muscles, which form a fleshy mass on the lateral part of the dorsal foot. The extensor digitorum brevis muscle arises from the anterior, upper surface of the calcaneus and passes obliquely across the dorsum to end in three tendons that insert onto the dorsal aponeurosis of the second through fourth digits (Figure 10.146). The extensor digitorum brevis muscle is responsible for dorsiflexion of the second through fourth digits. The extensor hallucis brevis muscle splits off of the extensor digitorum brevis muscle to insert on the dorsal aponeurosis of the first toe. It acts to dorsiflex the first digit (Figure 10.147, A). The muscles of the sole of the foot can be described by four muscular layers.
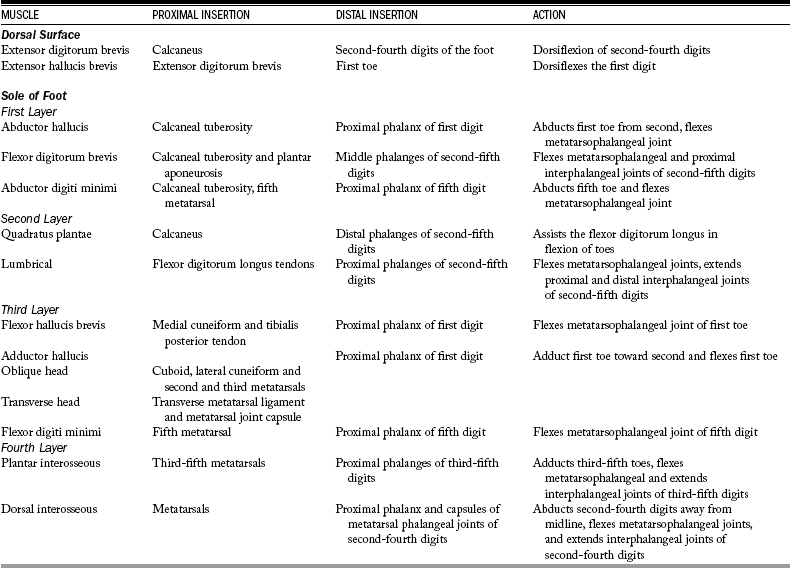
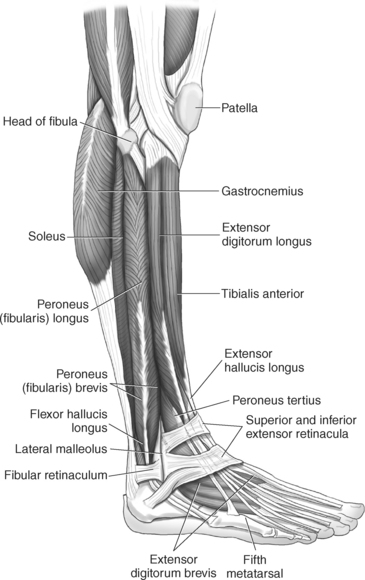
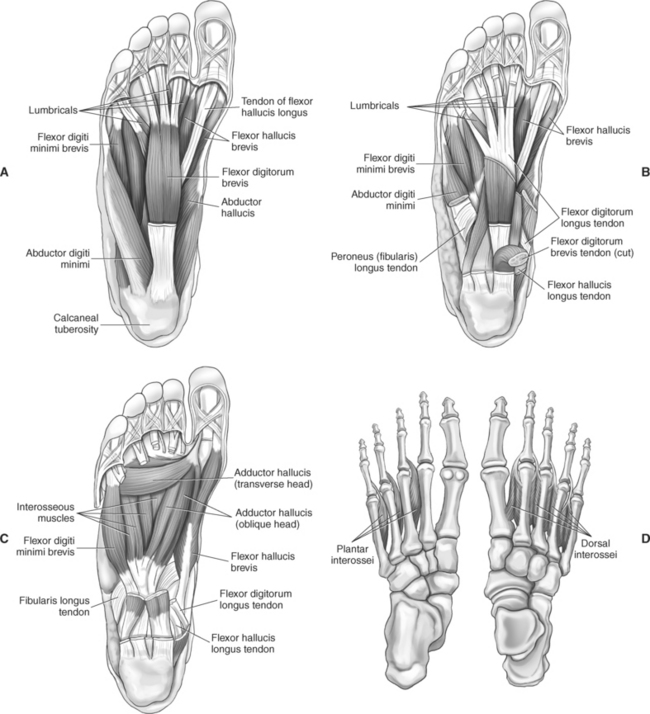
Figure 10.147 Dorsal view of muscles of right foot. A, First layer. B, Second layer. C, Third layer. D, Fourth layer.
First Layer
The muscles located within the first layer are the most superficial and include the abductor hallucis, flexor digitorum brevis, and abductor digiti minimi muscles (Figure 10.147, A). The abductor hallucis muscle arises from the medial process of the calcaneal tuberosity and lies along the medial border of the foot to insert on the medial base of the proximal phalanx of the first digit. The flexor digitorum brevis muscle also arises from the medial process of the calcaneal tuberosity as well as the plantar aponeurosis to insert on both sides of the middle phalanges of the lateral four digits. The abductor digiti minimi muscle arises from the lateral process of the calcaneal tuberosity, the tuberosity of the fifth metatarsal, and the plantar aponeurosis to form the lateral margin of the foot. It inserts on the lateral side of the base of the proximal phalanx of the fifth digit.
Second Layer
This layer is located deep to the first layer and includes the quadratus plantae and lumbrical muscles (Figure 10.147, B). The quadratus plantae muscle is a small flat muscle that arises as two small slips from the medial and lateral margins of the plantar surface of the calcaneus and joins with the tendon of the flexor digitorum longus that continues to the distal phalanges of the lateral four digits. The four small lumbrical muscles arise from the medial surfaces of the individual tendons of the flexor digitorum longus. They insert on the medial margin of the proximal phalanges of the second through fifth digits and extend into the extensor aponeurosis.
Third Layer
The third layer consists of three muscles: the flexor hallucis brevis, adductor hallucis, and flexor digiti minimi brevis muscles (Figure 10.147, C). The flexor hallucis brevis muscle arises from the medial cuneiform bone and the tibialis posterior tendon. It has two heads that cover the plantar surface of the first metatarsal extending to both sides of the base of the proximal phalanx of the first digit. The adductor hallucis muscle has two heads; the oblique head arises from the cuboid and lateral cuneiform bones and the bases of the second and third metatarsals, and the transverse head arises from the deep transverse metatarsal ligament and the metatarsal joint capsule. Both heads insert on the lateral side of the base of the proximal phalanx of the first digit. The slender flexor digiti minimi muscle arises from the base of the fifth metatarsal and inserts on the base of the proximal phalanx of the fifth digit.
Fourth Layer
This layer consists of the interosseous muscles (Figures 10.147, D and 10.148). Three plantar and four dorsal interossei muscles are located between the metatarsal bones. The plantar interosseous muscles arise from the bases and medial surfaces of the third through fifth metatarsals and insert on the medial sides of the bases of the proximal phalanges of the third through fifth digits. The dorsal interosseous muscles are larger than their plantar counterparts, arising from adjacent surfaces of the metatarsal bones and extending to attach to the sides of the proximal phalanx and capsules of the metatarsal phalangeal joints of the second through fourth digits (Figures 10.127 through 10.142 and 10.148).
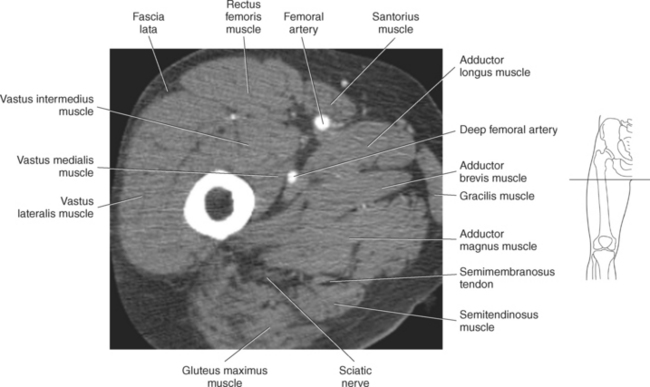
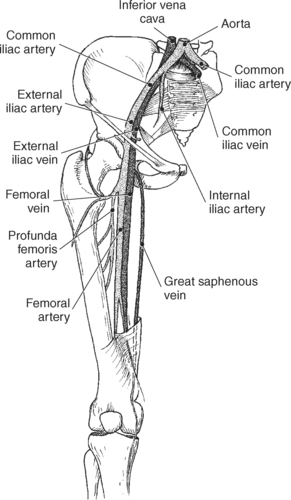
NEUROVASCULATURE
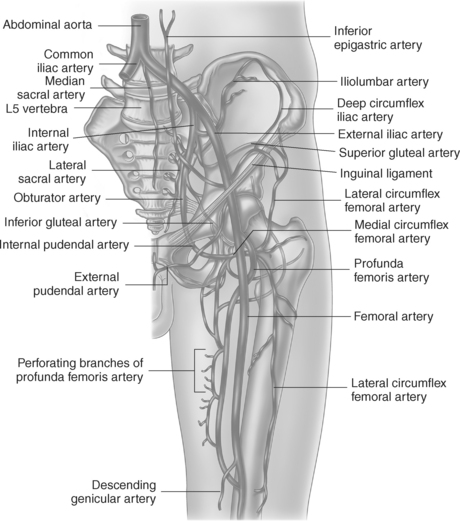
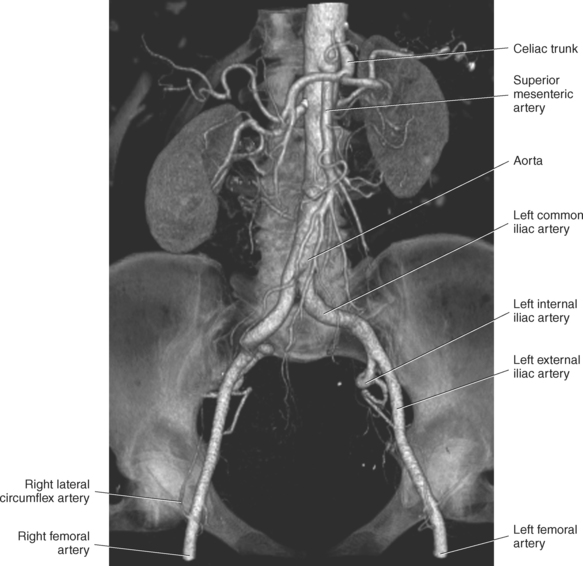
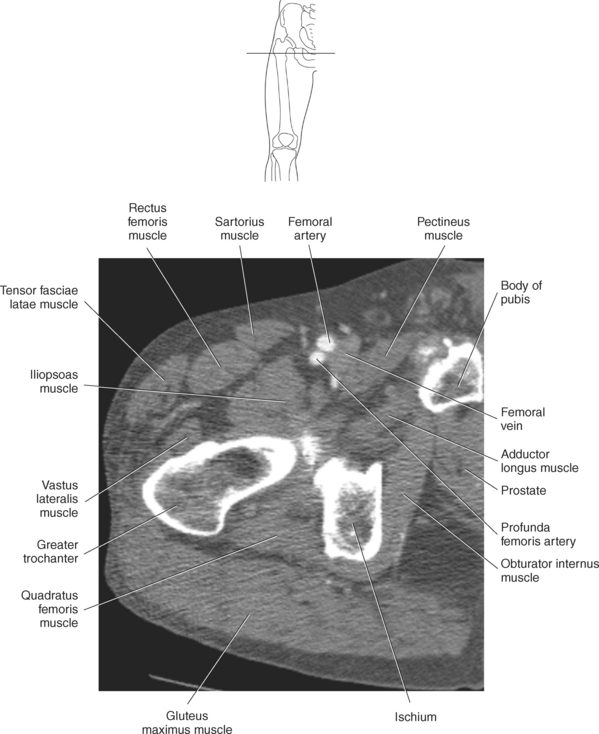
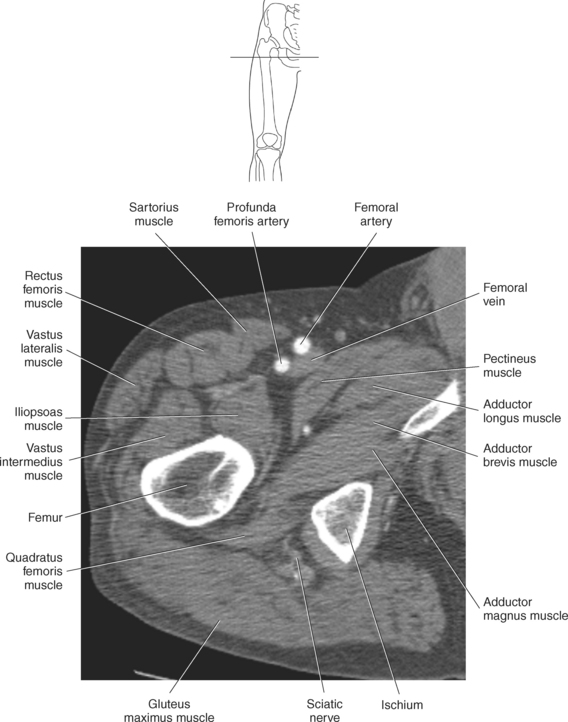
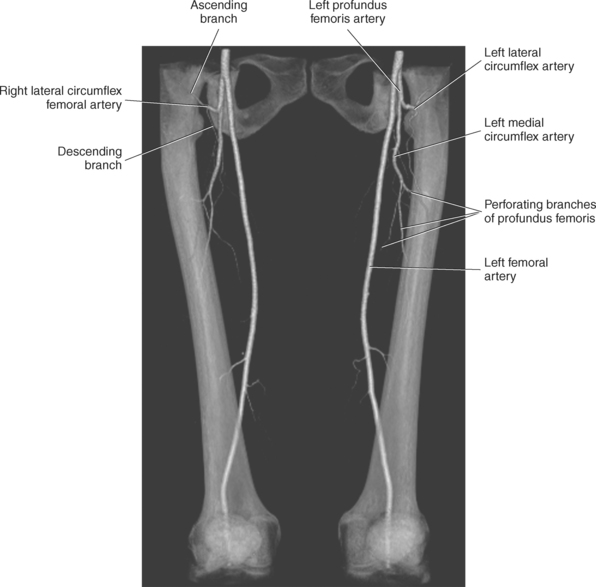
Traveling vertically along the anteromedian aspect of the hip is the femoral artery. The femoral artery, an extension of the external iliac artery, enters the anterior compartment of the thigh behind the inguinal ligament, where it is relatively superficial and easily palpable (Figures 10.149 through 10.153). It descends the thigh and continues through the opening in the adductor magnus muscle as the popliteal artery in the knee. The femoral artery and its main branches, superficial and deep, supply all the compartments of the thigh as well as the skin of the anterior abdominal wall, inguinal region, and external genitalia. The superficial branches of the femoral artery accompany the veins of the groin and include the inferior epigastric, superficial circumflex iliac, and the external pudendal arteries. The largest deep branch of the femoral artery is the profunda femoris artery, which arises from the posterolateral aspect of the femoral artery about 4 cm below the inguinal ligament and runs distally behind the femoral artery (Figures 10.151 through 10.153). It passes between the vastus medialis muscle and the muscles of the adductor group. The profundus femoris gives off two large branches: the medial and lateral circumflex femoral arteries (Figure 10.154 and Figure 10.155). The branches curve around the proximal femur and hip joint to supply the muscles of the adductor group and parts of the gluteal musculature, as well as the extensors and flexors at the thigh. The terminal branches of the profunda femoris artery are the perforating arteries (3-5) near the linea aspera that pass through the adductor muscles. One of the perforating arteries gives a large nutrient branch to the head of the femur (Figures 10.154 and 10.155).
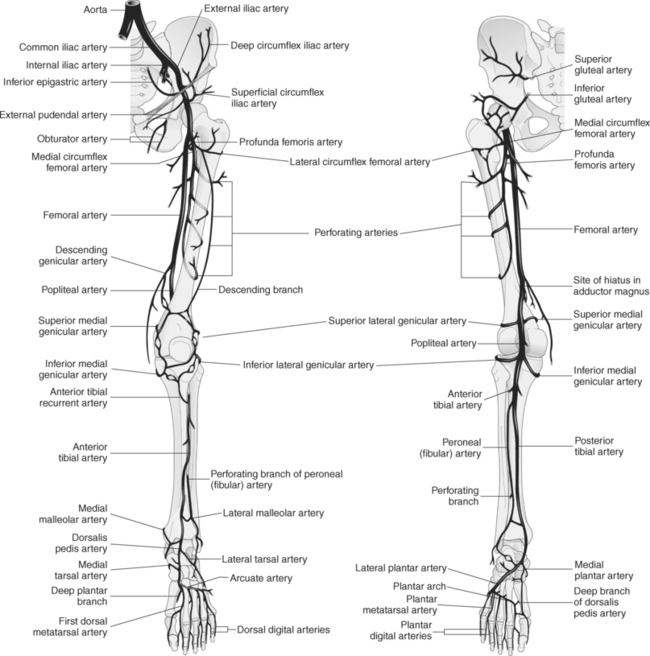
Popliteal Artery
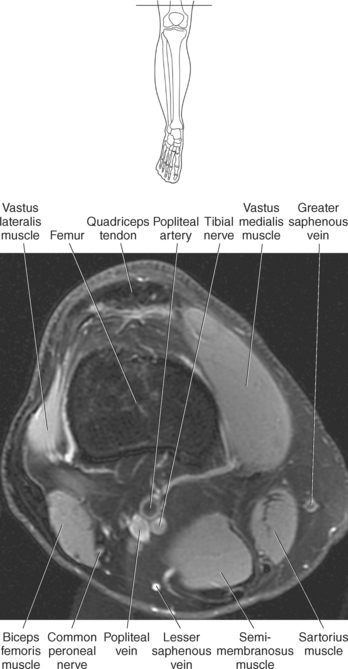
The popliteal artery is the continuation of the femoral artery. It runs deep near the bones of the knee joint during its course through the popliteal fossa. It passes distally over the popliteus muscle and divides into the anterior and posterior tibial arteries (Figures 10.154 through 10.156). The tibial nerve and popliteal vein accompany the popliteal artery, the tibial nerve being the most superficial of the structures in the popliteal fossa (Figure 10.157 and Figure 10.158). The popliteal artery supplies the surrounding muscles and forms a substantial plexus of articular branches anastomosing around the knee joint. The popliteal artery gives off branches to portions of the thigh muscles near the knee joint, dispatches the sural arteries distally to the gastrocnemius muscle, and supplies the knee joint with the anastomosing genicular arteries (lateral superior, lateral inferior, medial superior, medial inferior, and descending) (Figure 10.159).
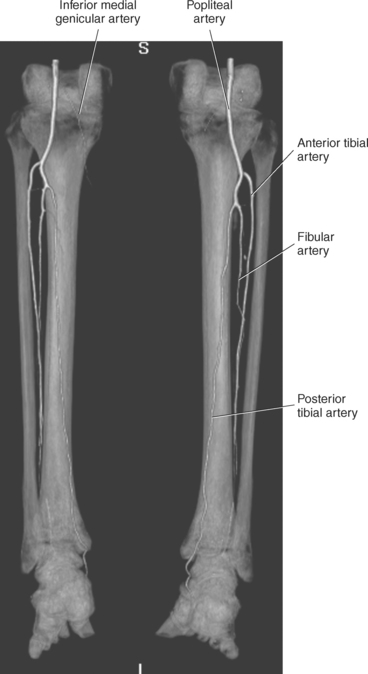
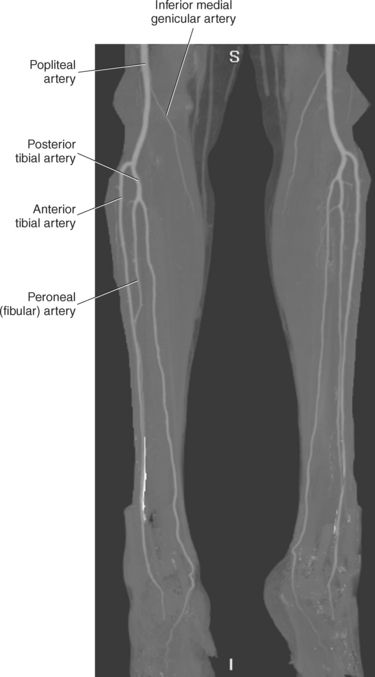
Anterior Tibial Artery
The anterior tibial artery courses anteriorly at the level of the fibular head into the anterior compartment of the lower leg. It runs distally as far as the anterior side of the ankle, where it becomes the dorsalis pedis artery. The branches of the anterior tibial artery are the posterior tibial recurrent, the anterior tibial recurrent, the medial anterior malleolar, the lateral anterior malleolar, and numerous muscular branches (Figures 10.154, 10.156, and 10.159).
Posterior Tibial Artery
The posterior tibial artery is usually larger than the anterior tibial artery. As it passes distally in the posterior compartment, it courses toward the medial side of the leg. The posterior tibial artery terminates by dividing into the medial and lateral plantar arteries in the foot. The peroneal (fibular) artery arises from the posterior tibial artery approximately 2 cm below the distal border of the popliteal muscle. It descends posteriorly along the medial aspect of the fibula and terminates on the lateral surface of the calcaneal tuberosity. Branches of the peroneal artery include the fibular nutrient, communicating, perforating, posterior lateral malleolar, and lateral calcaneal, as well as numerous muscular and cutaneous branches (Figures 10.154, 10.156, and 10.159).
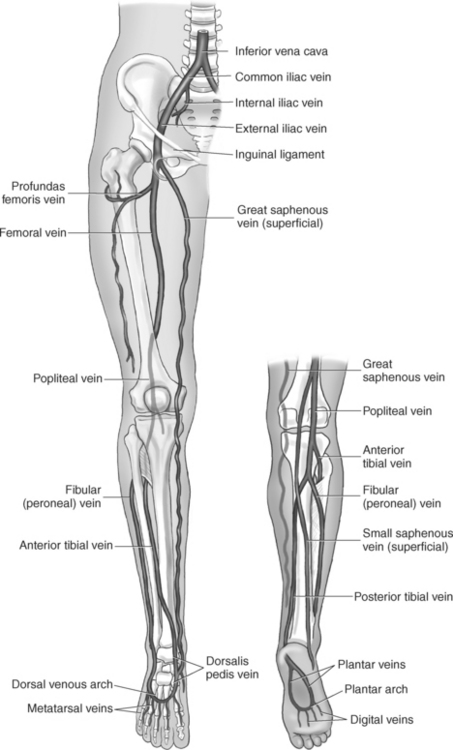
Veins
There are two groups of veins of the lower extremity: superficial and deep. The superficial veins arise in the foot from the dorsal venous arch and merge chiefly into two main trunks, the great saphenous and the small saphenous. The great saphenous vein ascends the medial aspect of the leg and thigh to drain into the femoral vein near the hip joint. From the lateral side of the foot, the small saphenous vein passes posterolaterally to join the popliteal vein (Figure 10.160). Between these two superficial veins and the system of the deep veins are numerous deep anastomoses. The deep veins accompany their corresponding arteries. The deep veins begin distally as venae comitantes of the anterior and posterior tibial veins that unite to form the popliteal vein. This becomes the femoral vein in the thigh, which courses medial to the femoral artery and continues deep to the inguinal ligament as the external iliac vein (Figures 10.151 through 10.153 and 10.160 and 10.161).
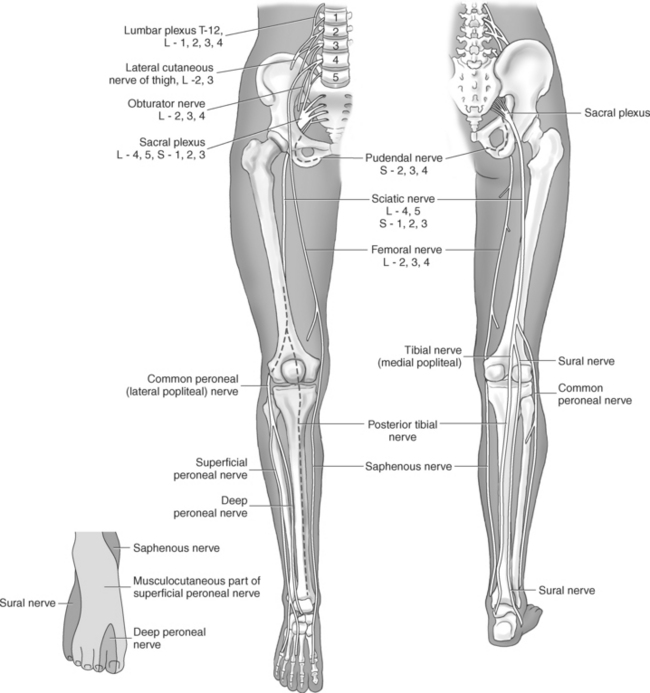
Nerves
The nerves of the lower extremity are derived from the lumbar and sacral plexuses (see Chapter 4). The femoral nerve enters the thigh beneath the inguinal ligament and divides into several superficial and deep branches to supply the anterior compartment of the thigh. The femoral nerve terminates as the saphenous nerve to innervate the skin on the medial side of the leg and foot. The obturator nerve courses through the obturator canal and immediately divides into anterior and posterior divisions to supply the medial compartment of the thigh. The sciatic nerve is the largest peripheral nerve in the body. Its branches supply the posterior compartment of the thigh and all compartments of the distal leg and foot. The sciatic nerve runs deep to the gluteus maximus muscle and descends in the midline of the thigh, where it usually divides into two terminal branches: the tibial and common peroneal (common fibular) nerves (Figures 10.153, 10.157, 10.158, and 10.162).