Dental Caries
 . Etiology of Dental Caries
. Etiology of Dental CariesDental caries is an irreversible microbial disease of the calcified tissues of the teeth, characterized by demineralization of the inorganic portion and destruction of the organic substance of the tooth, which often leads to cavitations. The word caries is derived from the Latin word meaning ‘rot’ or ‘decay’. It is a complex and dynamic process where a multitude of factors initiate and influence the progression of disease. Although effective methods are known for prevention and management of dental caries, it is a major health problem with manifestations persisting throughout life despite treatment. It is seen in all geographic areas in the world and affects persons of both genders in all races, all socioeconomic strata, and every age group. Some stay ‘caries-free’ for unknown reasons (Fig. 9-1). Despite extensive studies for more than a century, many aspects of etiology are still obscure, and efforts at prevention have been partially successful.

Figure 9-1 The caries-resistant and caries-susceptible mouth. Courtesy of A, Dr S Rohini, Chennai and B, Dr N Bhargavi, Department of Conservative Dentistry, Meenakshi Ammal Dental College, Chennai.
Epidemiology of Dental Caries
Caries in Prehistoric Man
Dental caries is probably a disease of modern civilization. Anthropologic studies of von Lenhossek revealed that the dolichocephalic skulls of men from preneolithic periods (12,000 BC) did not exhibit dental caries, but brachycephalic skulls of the neolithic period (12,000–3000 BC) contained carious teeth. Apparently the carious lesions were found at or just below the contact areas and an increased frequency of caries at the cementoenamel junction was noted.
Caries Incidence in Modern Societies
By about the 17th century, there was a significant increase in the total caries experience and a smaller increase in the number of carious lesions involving the interproximal contact areas of teeth, characteristic of the pattern and occurrence of caries in modern population.
Extensive studies on the incidence of dental caries from various geographic areas have illustrated the apparent influence of civilization on dental disease. Mellanby in 1934 reviewed the literature on caries in existing primitive races and noted that the incidence was invariably less than that in modern man suggesting isolated populations that have not acquired the dietary habits of modern, industrialized man retain a relative freedom from dental caries. Native population living in the North West territories of Canada, Alaska and Greenland who consumed native food, had a lower evidence of carious lesion (0.1%) compared to those living at trading posts (13%). A comparable effect of diet upon caries was demonstrated by Mellanby in studies on natives of Southern Rhodesia. The determinants of the carious process are essentially local and limited to the oral cavity. Although there may be a certain degree of racial resistance to dental caries, dietary factor appears to be more significant, especially since caries incidence is increased by contact with ‘civilized’ food.
Comprehensive Assessment of Dental Caries Prevalence in Modern-day Population
While dental caries is all pervading in highly industrialized societies, the caries experience varies greatly among countries and even within a country. The difference in caries rates noted in different parts of the world are extreme from rates fewer than one decayed, missing and filled (DMF) tooth per person at all ages up to 39 years in Ethiopia (Littleton, 1963) to 60 times greater in Alaska-Aleuts (Russel et al, 1961). Findings from the Interdepartmental Committee on Nutrition for National Defence (ICNND) and WHO studies (Barmes, 1981) indicate that caries prevalence follows definite regional patterns. It is generally lowest (0.5–1.7 DMF) in Asian and African countries and highest (12–18 DMF) in America and other Western countries. Consistently, low to moderate caries rates were found in populations of the Indo-Chinese peninsula, Malaysia, central and southern Thailand, Burma, South Vietnam, mainland China, Taiwan, India and New Guinea.
Generally, highly industrialized countries have the highest caries indices with decayed, missing, and filled teeth (DMFT) of approximately 4.5. However, within this large group of countries a very high caries pattern of over 5.6 DMFT occurs in New Zealand, Australia, Brazil, and Argentina.
DMF and def Index
The most commonly employed method to measure the extent of previous damage to permanent dentition is by a measure known as the DMF index. The designation DMF (T) is used to denote decayed, missing, and filled teeth; DMF(S) denotes decayed, missing and filled surfaces in permanent teeth and therefore takes into account the number of surfaces attacked on each tooth. A similar index def (t) or def (s) index is used for primary dentition. The DMF/def index can be used to quantify both caries prevalence and caries incidence in a given population. It is an arithmetic index of the cumulative caries attack in a population.
A commonly used modified form of this test is the caries increment, which refers to the number of new carious lesions occurring in a specified time interval, either for an individual or averaged over a population. The assessment of the caries increment involves at least two examinations—one at the beginning and one at the end of the period in question. In children, primary teeth may be lost due to natural exfoliation and, for the purpose of the def index, it is essential that the examiner designates as missing only those teeth that are lost due to caries.
Factors Affecting Caries Prevalence
Race
Some studies show remarkable differences in the caries experience between races. American blacks and whites, living in the same geographic areas under similar conditions, offer an excellent opportunity for comparison. Investigations indicate that the blacks have fewer carious lesions than the whites. Most studies concerning other races have been relatively unsatisfactory because of complicating factors such as differences in diet or exposure to fluoride, which tend to mask any differences due to racial background. Nevertheless, there is some evidence to indicate that blacks, Chinese, and East Indians have considerably less caries than American Whites. The English have a higher caries incidence than Italians, Russians, and Chinese.
Age
Carious lesions that result in cavitation are irreversible and therefore, cumulative with age. There is a strong correlation between age and DMF indices. Several studies have shown that by the age of 6 years, about 20% of children have experienced dental caries in their dentition and a DMFT of 0.5 can be expected. By the age of 12 years, 90% of children would have experienced a DMFT of approximately 5.5. The decayed, missing and filled surface (DMFS) accelerates at a greater rate than the DMFT beyond the age of eight years. By the age 12, an average DMFS of 7.5 is seen in most populations. In general, other reports of caries prevalence among children in various parts of the world show rates that seem to be comparable to those cited here. Another common element is that children from families in lower socioeconomic groups consistently have greater caries prevalence than their peers from families at a higher socioeconomic level.
Gender
Studies indicate that the total caries experience in permanent teeth is greater in females than in males of the same age. This is attributable largely to the fact that the teeth of girls erupt at an earlier age. This time difference is particularly significant during the formative years because teeth have been shown to be maximally susceptible to dental caries immediately after eruption since, the chemical structure of teeth in the immediate post eruptive stage is suboptimal in terms of caries resistance. As teeth are exposed to saliva and constituents in the diet, the outer layers of the tooth take up additional minerals from the oral environment in a process known as posteruptive maturation. This maturation process confers a greater resistance to dental caries on the tooth.
Familial
Siblings of individuals with high caries susceptibility are also generally caries active, whereas siblings of caries immune individuals generally exhibit low caries rates. Children of parents with a low caries experience also tend to have low caries; the converse is true for children whose parents have a high caries rate (Garn et al, 1976). Studies of the dental caries experience in monozygotic and dizygotic twins indicate that concordance for carious sites in monozygotic twins is much higher than in dizygotic twin pairs.
Current Trends in Caries Incidence
Significant data have been presented since the National Caries Program, USA in 1979–80 to substantiate numerous observations that there has been marked improvement in dental health as measured by prevalence of dental caries, especially in children and young adults, throughout the ‘civilized Western world’. Especially impressive was the increase in the percentage of children classified as caries-free in their permanent dentition. These changes had occurred in the absence of both fluoridation and organized preventive programs. This decrease in caries prevalence is also seen in England, Denmark, Ireland, the Netherlands, New Zealand, Norway, Scotland, and Sweden. A substantial decrease in the prevalence of dental caries has been reported from less developed countries. The cause for this widespread decline in the prevalence of dental caries is multifactorial. In some instances, communal water fluoridation has been present in the areas studied and in other cases organized preventive dentistry programs were available.
However, the time period involved in most of these studies coincides with the introduction and increased utilization of fluoride dentifrices and dietary fluoride supplements, as well as an increased awareness of the importance of oral health. The very limited studies available give no evidence that there is any change; for example, in the pervasiveness of Streptococcus mutans or any changes in dominant serotypes. Emphasis on improved physical health through food, exercise, and decreased carbohydrate consumption all may be the factors that have led to this decline.
Etiology of Dental Ca ries
The etiology of dental caries is generally agreed to be a complex problem complicated by many indirect factors that obscure the direct cause or causes. There is no universally accepted opinion for the etiology of dental caries. Numerous references on dental caries, including early theories attempting to explain its etiology, have been found in recorded history of ancient people. However, many theories have evolved through years of investigation and observation; the acidogenic theory of Miller (Miller’s chemico-parasitic theory), the proteolytic theory and the proteolysis chelation theory, are among those which have stood the test of time.
The Early Theories
The Legend of Worms
The earliest reference to tooth decay is probably from the ancient Sumerian text known as the ‘Legend of Worms’ from about 5,000 BC. The idea that caries is caused by worms was possibly prevalent for a long time as evident from the writings of Homer who made a reference to worms as the cause of toothache.
Endogenous Theories
Keeping with the humoral theory of Greek physicians, dental caries was thought to be produced by internal action of acids and corroding humors. Along with this, the early Greek physicians such as Hippocrates, Celsus, and Galen, proposed the vital theory of tooth decay, which postulated that tooth decay originated, like a bone gangrene, from within the tooth itself.
Chemical Theory
Parmly in 1820s observed that dental decay affected externally, not internally, as had been thought previously. It was proposed that an unidentified ‘chymal agent’ was responsible for caries. This was further supported by Robertson in 1835 who proposed that dental decay was caused by acid formed by fermentation of food particles around the teeth.
Parasitic Theory
The first to relate microorganisms to caries on a causative basis as early as 1843 was Erdl who described filamentous organisms in the membrane removed from teeth. Shortly thereafter, Ficnus in 1847, a German physician in Dresden, attributed dental caries to ‘denticolae’ the generic term he proposed for decay related microorganisms. Leber and Rottenstein, two German physicians, disseminated the idea that dental caries commenced as a chemical process but that living microorganisms continued the disintegration in both enamel and dentin. In addition to these observations, Clark (1871, 1879), Tomes (1873) and Magitot (1878) concurred that bacteria were essential to caries, although they suggested an exogenous source of the acids. In 1880, Underwood and Miller presented a septic theory with the hypothesis that acid capable of causing decalcification was produced by bacteria feeding on the organic fibrils of dentin. They reported sections of decayed dentin having micrococci as well as oval and rod shaped forms.
Miller’s Chemico-Parasitic Theory or The Acidogenic Theory
The chemico-parasitic theory is a blend of the above mentioned two theories. Willoughby D Miller, an American who was working at the University of Berlin, is probably the best known of the early investigators on dental caries. He published extensively on the results of his studies, beginning in 1882, which culminated in the hypothesis, “Dental decay is a chemico-parasitic process consisting of two stages, the decalcification of enamel, which results in its total destruction and the decalcification of dentin as a preliminary stage, followed by dissolution of the softened residue. In case of enamel; however, the second stage is practically wanting, the decalcification of enamel signifying its total destruction”. The acid, which affects this primary decalcification, is derived from the fermentation of starches and sugar lodged in the retaining centers of the teeth. Miller found that bread, meat and sugar incubated in vitro with saliva at body temperature, produced enough acid within 48 hours to decalcify sound dentin. Subsequently, he isolated numerous microorganisms from the oral cavity, many of which were acidogenic and some were proteolytic. Since a number of these bacterial forms were capable of forming lactic acid, Miller believed that caries was not caused by any single organism, but rather by a variety of microorganisms. He assigned an essential role to three factors in the caries process: the oral microorganisms in acid production and proteolysis; the carbohydrate substrate; and the acid which causes dissolution of tooth minerals. Miller’s chemico-parasitic theory is the backbone of current knowledge and understanding of the etiology of dental caries.
However, Miller’s chemico-parasitic theory could not explain the predilection of specific sites on a tooth to dental caries and the initiation of smooth surfaces. Also, why some populations are caries-free and the phenomenon of arrested caries. The concept of dental plaque adhering to teeth and serving to localize bacterial enzymatic activity was proposed later in 1897 by Williams. This theory has been accepted by majority of investigators in a form essentially unchanged since its inception. The bulk of scientific evidence does implicate carbohydrates, oral microorganisms and acids, and for this reason, these deserve further consideration.
Role of Carbohydrates
Reference has been made previously to the finding that members of isolated primitive societies who had a relatively low caries index manifested a remarkable increase in caries incidence after exposure to refined diets. The presence of readily fermentable carbohydrates has been thought to be responsible for their loss of caries resistance.
The early studies of Miller showed that when teeth were incubated in mixtures of saliva and bread or sugar, decalcification occurred. There was no effect on the teeth when meat or fat was used in place of the carbohydrate. Both cane sugar and cooked starches produced acid, but little acid was formed when raw starches were substituted. Volker and Pinkerton reported the production of similar quantities of acid from mixtures of either sucrose or starch incubated with saliva with no difference in acid production between raw and refined sugarcane. The etiology of dental caries involves interplay between oral bacteria, local carbohydrates and the tooth surface that may be shown as follows: Bacteria + sugars + teeth → organic acids → caries.
The cariogenic carbohydrates are dietary in origin, since uncontaminated human saliva contains only negligible amounts regardless of the blood sugar level. Salivary carbohydrates are bound to proteins and other compounds, and are not readily available for microbial degradation. The cariogenicity of a dietary carbohydrate varies with the frequency of ingestion, physical form, chemical composition, route of administration and presence of other food constituents. Sticky, solid carbohydrates, soft retentive foods those that are cleared slowly, monosaccharides and disaccharides are more caries-producing. Plaque organisms produce little acid from the sugar alcohols, sorbitol, and mannitol. Glucose or sucrose fed entirely by stomach tube or intravenously, does not contribute to decay as they are unavailable for microbial breakdown. Meals high in fat, protein or salt reduce the oral retentiveness of carbohydrates.
Role of Microorganisms
Miller demonstrated the presence of microorganisms within the tubules of decayed teeth. These were mainly cocci and leptothrix, as he called them, and laid the foundation for the role of acids elaborated by bacteria in caries production. In 1900, Goadby isolated a gram-positive bacillus from carious dentin and termed it B. necrodentalis. These, he concluded, played a role in decalcification of both enamel and dentin. Later he changed his views, stating that certain streptococci were the active cause of caries. Later in 1922, McIntosh, James and Lazarus-Barlow were concerned with microorganisms capable of lowering the pH to the degree that the enamel was softened. From carious dentin they isolated bacteria which they called Bacillus acidophilus odontolyticus. Around the same time, Clarke in Great Britain isolated a streptococcus from teeth that was found to be in the early stages of the disease. In 1924, he described a new streptococcus species, S. mutans, which was almost always isolated from carious lesions in the teeth of British patients. Although the work was confirmed three years later by McLean, scientific interest in S. mutans lay dormant until its rediscovery in the mid 1960s.
Many of the earlier workers focused attention on L. acidophilus because it was found with such frequency in caries-susceptible persons that it came to be regarded as of etiologic importance. In 1925, Bunting and Palmerlee reported the bacillary forms in every initial lesion of caries similar to those described by McIntosh and they termed them B. acidophilus. Bunting stated in 1928, so definite is this correlation between B. acidophilus and dental caries that, in the opinion of this group, the presence or absence of B. acidophilus in the mouth constitutes a definite criterion of the activity of dental caries that is more accurate than any clinical estimation could be. Furthermore, it was noted that there was a spontaneous cessation of caries coincident with the disappearance of B. acidophilus from the mouth, either from prophylactic, therapeutic or dietetic control.
Bunting, Nickerson and Hard carried out extensive studies on B. acidophilus and reported that it was almost universally absent in the mouths of caries-immune persons, but was usually present in the mouths of caries-susceptible persons. Similar findings were reported in 1927 by Jay and Voorhees, who also found that the presence of L. acidophilus in persons without active caries was often a presage of the development of cavities some months later. Jay reported the isolation of 12 strains of Leptothrix in 1927, but doubted their importance in the carious process even though they produced acid from carbohydrates.
Between this period and the 1940s, numerous studies were carried out in attempts to confirm or deny the existence of a microorganism responsible for dental caries. Harrison observed streptococci to predominate on the surfaces of non-carious rat molars, about half of the strains being acidogenic. On the other hand, in rats with carious lesions, the surface flora consisted primarily of lactobacilli. Microorganisms isolated from the deeper carious cavities were mainly acidogenic streptococci and he thus concluded that there was an apparent relationship of lactobacilli with initial caries and of streptococci with more advanced lesions of dentin. Florestano, in 1942, cultured organisms from the saliva of carious and noncarious persons and studied their acidogenic potential. Aciduric streptococci and staphylococci were isolated from both the groups. Their acid production and presence in large numbers suggested a role in dental caries equal to that of lactobacilli. Bacteriologic studies in recent years have helped clarify the role of various organisms in the etiology of dental caries. Considerable emphasis has been placed on the various diet-bacterial interactions, which are involved in lesion development on different tooth surfaces. Specific microorganisms as well as combinations of microorganisms, including Lactobacillus, S. mutans, Actinomyces species and others, have been studied. Although there may be disagreement as to specifics, there is little doubt that bacteria are indispensable to the production of caries. One or more organisms are implicated in the initiation of caries, while other distinctly different organisms may influence the progression of the disease. Also, there is good evidence that different diet–bacterial interactions are involved in root surface and coronal caries, and they may represent two different diseases from the ecological and microbiological point of view.
In 1960, Keyes demonstrated that under certain laboratory conditions, dental caries in hamsters and rats could be considered an infectious and transmissible disease and therefore subject to those biologic principles which govern any infectious process. Fitzgerald and Keyes showed that even in a so-called caries-inactive strain of hamster, oral inoculation of certain pure cultures of streptococci isolated from hamster caries would induce the typical picture of active dental caries. The caries-inactive strain of hamster was found to have a noncariogenic microflora. These findings have led to interesting speculation about the importance of streptococci in the etiology of dental caries.
Microbial Flora and Dental Caries
It is uniformly agreed that caries cannot occur without microorganisms. Several organisms have been found capable of inducing carious lesions when used as monocontaminants in gnotobiotic (germ-free) rats. These include the mutans group of streptococci, a Streptococcus salivarius strain, Streptococcus mitior, Streptococcus milleri, Streptococcus oralis, Streptococcus sanguis (different strains), Peptostreptococcus intermedius, Lactobacillus acidophilus, Lactobacillus casei, Actinomyces viscosus and Actinomyces naeslundii. In addition, in the same animal system, some streptococcis and lactobacilli such as Lactobacillus fermentum and Streptococcus lactis, were not able to induce caries, suggesting that not all organisms are cariogenic, at the same time caries will not occur even in the complete absence of microorganisms. Different organisms display certain selectivity for the tooth surface they localize and attack (Table 9-1).
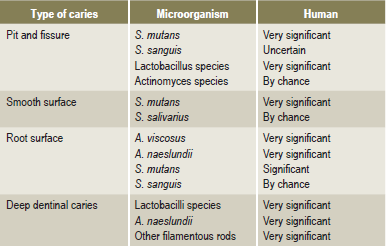
A wide variety of organisms are able to initiate pit and fissure caries as they colonize in these retentive areas. A limited number of organisms have proved to colonize smooth surfaces and S. mutans is very significant in this respect. Some of the organisms involved in root caries are different from those in other smooth surface lesions because the initial lesion involves the cementum or dentin and not enamel. Bacteriological sampling of plaque covering caries of the root surfaces has yielded predominantly Actinomyces viscosus. However, other studies have found no difference in the prevalence of A. viscosus on carious versus intact root surface. Strains of Nocardia and S. sanguis, besides causing enamel caries may, at times, also cause root caries. While in the deep dentinal caries, the predominant organism is Lactobacillus, the exact extent to which these organisms participate in human disease is yet to be explored.
Studies in humans are largely based on the mathematical relationship between various streptococci, lactobacilli and dental caries. Available data strongly suggest an active involvement of S. mutans in caries initiation. Strains of S. mutans isolated from humans have proved to be cariogenic in animal studies and S. mutans can almost always be found in plaques over incipient lesions involving pits and fissures or smooth tooth surfaces. Not all studies support a unique or sole relationship between S. mutans and the initiation of caries in humans. The characteristics and properties of some known potentially cariogenic plaque microorganisms are discussed.
Lactobacilli
Lactobacilli are gram-positive, nonspore forming rods that grow best under microaerophilic conditions. The isolation of lactobacilli has been made possible by the use of a selective agar medium (Rogosa) which suppresses the growth of most other organisms by its low pH. The genus Lactobacillus includes many species and represents about 1% of oral flora. Among the homofermentative isolates, L. casei and L. acidophilus are the most common, while hetero fermentative members mostly include, L. fermentum and L. brevis. The idea that lactobacilli are important in the carious process was owing to the fact that they are both acidogenic as well as aciduric and could therefore multiply in the low pH of plaque and carious lesions. Lactobacilli as a universal etiologic agent in dental caries is; however, questioned because the amount of acid formed by lactobacilli present in plaque is insignificant in comparison to that produced by other acidogenic oral organisms. The occurrence of lactobacilli in carious lesions and their increased numbers in plaque and saliva does not necessarily establish their causative role although they could be secondary invaders. This possibility is supported by the observations that lactobacilli are not detectable in plaques covering white spot lesions on smooth surfaces and their predominant sites are in deep fissures and in deep dentinal lesions, favoring their retention.
Oral Actinomyces
These are gram-positive, filamentous organisms that include A. naeslundii and A. viscosus which are facultative anaerobes and A. israelii and A. odontolyticus which are strict anaerobes. Actinomyces and Rothia species are found in human dental plaque in significant numbers and they have been isolated in high proportions from decayed root surfaces of human teeth. A. viscosus are acidogenic bacteria which, in addition to having intracellular polysaccharide stores, also form extracellular levans and heteropolysaccharides consisting of hexosamine and hexose. It is the predominant flora of plaque overlying root lesions, but its role in initiating these lesions is difficult to assess because A. viscosus is also found on sound root surfaces.
Veillonella
This is one of the gram-negative cocci commonly found in plaque. Interest in this group relates to its possible anticariogenicity. These organisms lack key enzymes involved in glycolysis and the hexose monophosphate shunt, and therefore do not utilize sugars as an energy source. Veillonella utilizes lactic acid by converting it to propionic and other weak acids. By this reaction, the stronger lactic acid with a pKa of 3.08 is converted to a less dissociated acid of pKa in the range of 4.7. It has also been observed that the veillonella strains increase in number in dental plaque after lactic acid producing organisms have first colonized. A positive correlation between veillonella and caries activity has been reported by some but contradicted by others.
Oral Streptococci
Of all the oral bacteria, streptococci have been studied most comprehensively. The most important species found in the oral cavity include: S. mutans, S. sanguis, S. mitior, S. salivarius, and S. milleri.
A Streptococcus that prevailed in many human carious lesions and first isolated in 1924 by Clarke was termed Streptococcus mutans. These bacteria are catalase negative, gram-positive cocci forming short to medium chains. On mitis salivarius agar, they grow as highly convex colonies. Unlike other oral streptococci, most strains of S.mutans can be selectively cultured in mitis salivarius agar containing 20% sucrose and 0.2% units/ml of bacitracin. Characteristically, S. mutans synthesizes insoluble polysaccharides from sucrose. It is homofermentative and is more aciduric than other oral streptococci.
Cariogenic strains of S. mutans contain a lysogenic bacteriophage which has not been isolated from non-cariogenic strains. Non-cariogenic strains are unable to adhere to glass and have decreased ability to form insoluble polysaccharides. In the oral cavity, S. mutans does not colonize the mouths of infants prior to the eruption of teeth. Likewise, it disappears from the mouth following the extraction of all teeth. Infants most likely become infected from their parents or from other individuals with whom they have frequent contact since these organisms are not found free living in nature and have only been isolated from humans and certain animals.
S. mutans forms a homogeneous group based on several phenotypic characteristics. However, based on nucleic acid base content and hybridization, S. mutans has been divided into five genotypes as S. mutans, S. rattus, S. sobrinus, S. cricetus, and S. ferus. Among, these, S. mutans and S. sobrinus are most commonly found in human plaque. S. mutans strains have also been divided into eight serotypes designated ‘a’ through ‘h’. The specific antigen for each serotype represents cell-wall constituents which have been isolated and chemically characterized as polysaccharides. Theoretical possibilities exist for inhibiting glucosyltransferase of several serotypes by an antiserum against purified glucose transferase of one single serotype.
The most important substrate for the involvement of S. mutans in the caries process is the disaccharide sucrose. Different pathways by which S. mutans may dissimilate sucrose, are by conversion of sucrose to adhesive extracellular carbohydrate polymers by cell bound and extracellular enzymes. The transport of sucrose into the cell interior is accompanied by direct phosphorylation for energy utilization through the glycolytic pathway, leading to lactic acid production and degradation of sucrose to free glucose and fructose by invertase. The intermediary metabolites from sucrose enter the glycolytic cycle or may be utilized in intracellular polymer synthesis in order to provide a reservoir for energy.
Most of the sucrose metabolized by S. mutans is utilized for its energy requirements and results in the production of lactic acid. Sucrose, which does not enter the cell, may be used for the extracellular synthesis of carbohydrate polymers. The ability of S. mutans to form adhesive plaques could explain its specific dependence on sucrose rather than other dietary carbohydrates.
It must be emphasized that S. mutans polymerizes the glucose and the fructose moieties of sucrose to synthesize glucans and fructans, which are two types of extracellular polymers. The enzymes responsible for the synthesis of extracellular glucans and fructans are called glucosyl- and fructosyltransferases, respectively. Synthesis of glucans from sucrose has been considered for several years to be the essential glue in S. mutans attachment to enamel and subsequent plaque formation. Two of the homopolymers of glucans are dextran and mutan. Mutan is an important constituent of fibrillar plaque matrix and is less soluble and more resistant to enzymatic attack than dextran.
Besides functioning as a resistant structural matrix, insoluble extracellular polysaccharides can act as a diffusion barrier. The transport of metabolites and salivary buffers into the plaque and the diffusion of acid out of the plaque may be affected by glucan. Besides producing glucan, certain oral bacteria can degrade this polymer and utilize it as a carbon source.
Fructans, on the other hand, unlike the mutan homopolymer of glucan, are generally soluble and can be degraded by plaque bacteria, thus serving as a reservoir of fermentable sugars for oral bacteria. A group of fructans produced by bacteria or created by breaking down other kinds of plant fructans are called levan beta 2, 6. Levans are both more soluble and more readily catabolized than glucans. Since levan hydrolysis is rapid, it may function as a short-term reservoir for the sustenance of bacterial anaerobic glycolysis in times of relative unavailability of dietary carbohydrate. Current opinion holds that this plaque component plays only a small role in the cariogenic potential of plaque because of the rapidity of its hydrolysis and the fact that it is purportedly not sticky.
Electron microscopic observation of the plaque formed by S. mutans reveals two types of extracellular products: a globular component, representing the water soluble, and a fibrillar component, the water insoluble glucan.
Lipoteichoic acid is another extracellular polymer that is found in cultures of S. mutans. These highly negatively charged compounds might contribute to the adhesiveness of bacteria. In addition to this, S. mutans strains have an ability to store intracellular glycogen amylopectin type polysaccharide, which provides a reservoir of substrate and enables prolonged periods of increased metabolic activity. Intracellular glycogen and extracellular polysaccharides serve as substrate reservoirs, which the organism may utilize for energy production, as the exogenous supplies of readily metabolized carbohydrate are depleted. In this fashion, both types of polysaccharides may play a role in the survival of organisms and in their potential to prolong acid production via glycolysis well beyond meal time.
It is known that sucrose-adapted S. mutans strains possess significant levels of invertase activity, and this enzyme is known to hydrolyze sucrose intracellularly to free glucose and fructose. Invertase is activated by inorganic phosphate and since phosphate accumulation is coupled with acid production, it is probable that one of the several mechanisms by which sucrose degradation is regulated in S. mutans is the activation of invertase by inorganic phosphate.
This is consistently present in plaque obtained from both carious and noncarious sites. Caries from this strain occurs primarily in occlusal fissures and is significantly less extensive than S. mutans, as it has low cariogenicity in experimental animals. This α-hemolytic Streptococcus species was originally isolated from patients with subacute bacterial endocarditis. The serology of S. sanguis is complex but they are easily identifiable on sucrose-containing media as small, firm colonies and form extracellular polysaccharides in sucrose broth.
This species is found in tongue, throat and in saliva but not in high numbers in dental plaque. It adheres well to epithelial surfaces but not to hard tissues and produces copious amounts of the water-soluble polymer of fructose called levan. Even though some strains of this organism have been shown to produce caries in experimental animals, their role in human dental caries is of minimal significance.
This is one of the most commonly isolated bacteria in the oral cavity. It produces soft, round and black-brown colonies on mitis salivarius agar. Along with S. sanguis it forms the most predominant organisms in dental plaque. However, its significance in human caries is assumed to be very minor.
Based on these observations from earlier studies, it is certain that bacteria, principally the gram-positive cocci and gram-positive pleomorphic rods, are essential for the development of caries. There is also a significant variation in the microbial flora associated with pit and fissure caries, smooth surface caries, root caries and deep dentinal caries. Since several factors may influence the formation, composition and metabolism of dental plaque, human dental caries may also be considered to be a diverse microbiologic disease. In the past, the total plaque was viewed as a pathogenic structure which had to be eliminated or reduced if caries was to be prevented. The present available data indicates that the qualitative nature of the flora in plaque determines the metabolism and the potential for caries production. This view is termed the Specific Plaque Hypothesis (Loesche, 1982), and according to this hypothesis, most but not necessarily all carious lesions are due to specific bacterial species. This concept suggests that cariogenesis is a specific bacterial infection and methods implemented for its elimination are more than just reduction of total plaque.
Role of Acids
The exact mechanism of carbohydrate degradation to form acids in the oral cavity by bacterial action is not known. It probably occurs through enzymatic breakdown of the sugar, and the acids formed are chiefly lactic acid, although others such as butyric acid are also formed. Since acid production is dependent upon a series of enzyme systems, methods of decreasing this acid formation by interference with certain enzymes could be an effective strategy to decrease caries.
The presence of acids in the oral cavity is of less significance than the localization of acids upon the tooth surface. This suggests a mechanism for holding acids, at a given point, for relatively long periods. Dental plaque fulfils this function. Acid production from carbohydrates have been extensively studied in human plaque. Generally, monosaccharides and disaccharides result in the greatest fall in plaque pH. On the other hand, acid formation is slower upon application of cooked starch. This is possibly because of the slower diffusion of larger starch molecules and acid production that occurs from the comparatively low concentration of maltose released from starch. Fermentation or glycolysis are ways of anaerobic catabolism of carbohydrates, which predominates in plaque and leads to acid production. The end products of glycolysis have the same empirical formulas as the starting substrate in that one molecule of glucose breaks into two molecules of lactic acid.
Organisms such as streptococci and lactobacilli ferment sugars, which produce 90% or more lactic acid as the end product; such bacteria are called homofermentative. Heterofermentatives produce a mixture of metabolites including other organic acids such as propionic, butyric, succinic, and ethanol using divergent metabolic pathways. For example, pyruvic acid, an intermediate metabolite in glycolysis, may be rendered to lactic acid by the enzyme lactic acid dehydrogenase or split into formic acid and acetyl coA by the enzyme pyruvate formate lyase. The acetyl coA is then converted into acetate and ethanol. The proportion of lactic acid or other organic acids formed by plaque may be markedly affected by growth conditions and by the bacterial types present. For example acid accumulation by S. mutans is substantially greater than by S. sanguis or S. mitis and Actinomyces are homolactic in anaerobic conditions but in the presence of carbon dioxide the fermentation is heterolactic with formate, acetate, lactate and succinate as their products.
Role of the Dental Plaque
Dental plaque (microbial plaque or bacterial plaque) is a structure of vital significance demonstrated for the first time in histologic preparations by Williams in 1897. It has been recognized for many years as a contributory factor to at least the initiation of the carious lesion.
Although Miller emphasized the role of foods and the acids produced by their bacterial degradation, he thought that the plaque protected enamel against attack by a carious process. In contrast, GV Black in 1899 regarded plaque to be important in the caries process and described it as “The gelatinous plaque of the caries fungus is a thin, transparent film that usually escapes observation, and which is revealed only by careful search. Neither it is the thick mass of material alba so frequently found upon the teeth, nor is the whitish gummy material known as sordes, which is often prominent in fevers and often present in the mouth in smaller quantities in the absence of fever.”
Plaque is the soft, nonmineralized, bacterial deposit which forms on teeth and dental prostheses that are not adequately cleaned. It characteristically forms on tooth surfaces which are not constantly cleansed, and appears as a tenacious, thin film, which may accumulate to a perceptible degree in 24–48 hours. A characteristic of plaque is that it resists removal by physiologic and oral cleansing forces such as saliva and tongue movement but is removable by toothbrushing. An important component of the dental plaque is acquired pellicle, which forms just prior to or concomitantly with bacterial colonization and may facilitate plaque formation. The pellicle is a glycoprotein that is derived from the saliva and is adsorbed on tooth surfaces. It is not dependent on bacteria but may serve as a nutrient for plaque microorganisms.
Dental plaque, or microcosm, as denoted by Arnim, is variable in both chemical and physical composition. It consists of salivary components such as mucin, desquamated epithelial cells and microorganisms. Plaque is composed of about 80% water and 20% solids. These are rich in bacteria with studies showing approximately 2×1011 bacteria per gram. Bacterial and salivary proteins comprise about one half of the dry weight of plaque. Plaque also contains carbohydrates and lipids, which account for approximately 25% of the plaque’s dry weight. Most of the carbohydrates in the matrix consist of polymers, glucans, fructans, and heterosaccharides synthesized by the bacteria. Some of these polymers are thought to play a role in bacterial attachment and cohesion, and others are more important as a reservoir of fermentable substrates metabolized by bacteria when other more readily utilized carbohydrates in plaque become depleted.
Inorganic components of plaque account for approximately 5–10% of the dry weight of plaque. The concentration of calcium and phosphate in dental plaque is several magnitudes higher than in saliva. This is thought to be due, in part, to the infiltration of salivary proteins containing these constituents in the bound form. These probably include statherin, the salivary protein which, by adsorbing onto early crystal nuclei and preventing crystal growth, maintains super saturation of the fluid phase of plaque with apatite. In addition, bacteria may accumulate polyphosphates, which bind to calcium. Most of the calcium found in plaque is non-ionic and solubilisation occurs as pH drops. Dental calculus (q.v.) is plaque in which mineralization has involved both the plaque matrix and the microorganisms. However, the free surface of calculus usually harbors living bacteria.
There is a general agreement that enamel caries begins beneath the dental plaque. The presence of a plaque; however, does not necessarily mean that a carious lesion will develop at that point. Variations in caries formation have been attributed to the nature of the plaque itself, to the saliva or to the tooth. Extensive study of the bacterial flora of the dental plaque has indicated a heterogeneous nature of the structure. Most workers have stressed the presence of filamentous microorganisms, which grow in long interlacing threads and have the property of adhering to smooth enamel surfaces. Smaller bacilli and cocci then become entrapped in this reticular meshwork. Aciduric and acidogenic streptococci and lactobacilli are particularly numerous in this setup. Occasionally, strains of the filamentous organisms are actively acidogenic through carbohydrate fermentation, but this does not appear to be a general feature of this group.
Bibby (1940) studied the characteristics of different strains of filamentous organisms isolated from dental plaques and noted their ability to adhere to smooth surfaces. Blayney and his associates (1942) pointed out that the time required for the development of definite cavitation representing early caries in an intact enamel surface was several months. Hemmens and his coworkers (1946) believed that dental plaque was the most likely starting point for investigations aimed at understanding the earliest stage of enamel caries. They examined numerous plaques from areas of children’s teeth which became carious during the course of investigation. Aciduric streptococci were the organisms most commonly isolated from plaques during the period of caries activity, being present in varying numbers in 86% of the plaques. α-streptococci were isolated from slightly over 50% of the plaques from carious surfaces and from 75% of those from noncarious surfaces. The greatest incidence of occurrence of lactobacilli in plaque was 57%, but these organisms increased in incidence during that period in which the carious lesions were developing.
Most investigations of the microbiology of the dental plaque have concluded that three basic groups of microorganisms predominate: streptococci, actinomyces and veillonellae. The major strains of streptococci present in plaque are S.mutans, S. sanguis, S. mitior, S. milleri and S. salivarius (uncommonly). Major actinomyces strains include A. viscosus, A. naeslundii, A. israelii, and Rothia dentocariosa. The veillonellae group are the anaerobic gram-negative cocci organisms, chiefly V. parvula and V. alcalescens. Of all these, Streptococcus mutans is considered to be the chief etiologic agent in human dental caries today.
Plaques are classified as supra or subgingival, according to the anatomical area in which they form. Supragingival plaques play an essential role in the pathogenesis of dental caries while marginal and subgingival plaques are responsible for the initiation of periodontal diseases.The amount of plaque can be assessed directly by clinical examination (Fig. 9-2). Often dye solutions, referred to as disclosing agents, are used to stain plaques for visual scoring. Although carious lesions will not develop without plaque, it should be emphasized that plaques can often be relatively innocuous, have buffering capacity and protecting the teeth from exposure to acids present in many foods. However, when plaques contain appreciable proportions of highly acidogenic bacteria such as S. mutans and are exposed to readily fermentable dietary sucrose, they produce sufficient concentrations of acids to demineralise the enamel.
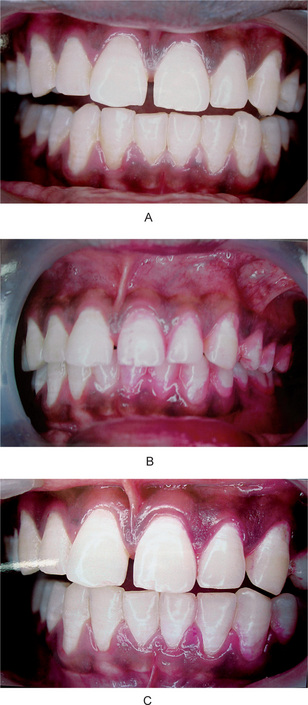
Figure 9-2 Dental plaque.
(A) The appearance of the teeth in all quadrants is similar, although the teeth on one side were not brushed for three days. (B) The dental plaque on the unbrushed teeth becomes obvious after the application of a disclosing solution. (C) Brushing the teeth and reapplying disclosing solution reveals that the plaque, if in an accessible area, is readily removed by brushing Courtesy of Dr L Natarajan and Dr Duliganti Santosh Reddy, Meenakshi Ammal Dental College, Chennai.
Mechanism of Plaque Formation
It is now known that the formation of dental plaque requires two types of specific bacterial adherent interactions. Firstly, bacteria attach selectively to the acquired pellicle, and secondly, bacteria accumulate via specific adhesive and cohesive interactions involving components of the plaque matrix and direct bacterial cell contact.
The pellicle appears as three distinct components. The subsurface component, below the surface of enamel having a dendritic configuration, the 1μm thick surface component closely associated with the surface of the tooth, and a suprasurface portion of 10 μm thickness which has a scalloped appearance. These amorphous organic films on the enamel surface may influence caries formation and bacterial adhesion. The acquired pellicle, like most proteinaceous adsorbed layers, is a membrane that may impart semipermeable properties to the enamel surface.
The role of the salivary pellicle in modifying plaque formation has been extensively studied because bacteria attached to salivary proteins adsorbed to the enamel rather than to the inorganic tooth surface. Some organisms such as S. salivarius, which are prominent on the dorsum of tongue and in saliva, do not adsorb well to teeth. Other organisms such as S. sanguis and A. viscosus, which are not as numerous in saliva, adsorb avidly to the pellicle and are prominent in developing new plaque. The important point is that organisms are not passively entrapped but rather selectively attached because of specific interactions involving their cell surface constituents and the macromolecules of salivary pellicle.
Bacterial Adherence
Almost all bacteria and all natural surfaces, including teeth have a net negative charge. In the first phase of loose association, the organisms are thought to be attracted on to the surface by van der Waals forces. Firm contact does not occur because of the repulsive effects of the negative electrostatic charges. The second phase of attachment results in firmer bonding and appears to involve polymeric substances on the surface of the bacterium which links the organisms to the target surface.The polymeric material may bind to the surface by the formation of hydrogen, hydrophobic, ionic or other types of bonds.
The adsorption of proteins and other materials to hydroxyapatite occurs via electrostatic attractions involving calcium and phosphate groups on the mineral surface. It may be that initial adsorption of bacteria such as S. mutans to the pellicle also involves electrostatic interactions. It has been postulated that cell wall teichoic acids, which contribute to the net negative charge possessed by bacteria, may form bridges with calcium ions onto the enamel or pellicle.
Bacteria appear to possess surface components that have recognition potential, which bind to specific receptors on the pellicle and other host tissues. These surface components are referred to as adhesins. Some adhesins bind to saccharide receptors. Protein adhesins, which bind to specific sugars, are called ‘lectins’. Other adhesins, which contain hydrophobic moieties, may interact with hydrophobic residues in specific receptor. Adhesins, therefore, permit bacterial cells to recognize and adhere to complex macromolecules.
Bacterial Accumulation
Both bacterially-derived polymers and salivary components appear to play important roles in this process. Early studies demonstrated that S. mutans accumulated on the teeth of rats or hamsters fed on diets rich in sucrose but not glucose. It was subsequently found that S. mutans synthesized extracellular glucans and fructans from sucrose but not from other common carbohydrates and that this polymer synthesis enabled the organism to accumulate in large masses. Most tooth-associated streptococci, actinomyces and neisseria can produce extracellular polymer glucan. More recently, several studies have suggested that S. mutans can adsorb on to hydroxyapatite without the synthesis of extracellular polymers and certain S. mutans serotypes can form plaque in the absence of sucrose. However, such plaques are less tenacious to enamel than are plaques formed by S.mutans in the presence of sucrose. More research is needed to further elucidate its role in plaque build-up and retention.
Role of pH of Dental Plaque
It was once thought that dental plaque, which is permeable to carbohydrates with the possible exception of starch, acted to hold the carbohydrates at a restricted site for a relatively long time. Stephan (1940) showed that this concept was incorrect and that carbohydrates permeating the plaque were degraded rapidly. He used an antimony microelectrode capable of measuring the pH in a dental plaque in situ. The pH of plaques in different persons varied, but averaged about 7.1 in caries-free persons and about 5.5 in persons with extreme caries activity.
Investigation of actual proximal cavities, opened mechanically, showed that the lowest pH varied from 4.6 to 4.1. Stephan also studied the pH in dental plaques after rinsing of the mouth with a 10% glucose or sucrose solution. Within two to five minutes after the rinse, the pH in the plaque dropped to between pH 4.5 and 5.0 and gradually returned to the initial pH level within one to two hours (Fig. 9-3). Further studies indicated differences in reductions in pH between caries free and caries-active subjects. The plaque pH in the caries-free group did not fall below 5.0 after the glucose rinse, while the pH in the caries active group dropped below 5.0 units after the glucose rinse in over half the cases.
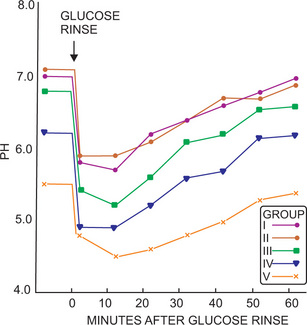
Figure 9-3 The pH curves of plaques on labial surfaces of maxillary anterior teeth in different caries activity groups.
Group I was caries-free; group II had caries previously, but was caries-inactive during the period of study; group III had slight caries activity; group IV had moderate caries activity; group V had extreme caries activity Courtesy of Dr Robert M Stephan: J Dent Res, 23: 257, 1944.
A drop in local pH below 5.5 causes demineralization of tooth surfaces. At a critical pH of 5.5, the tooth minerals act as buffers and they loose calcium and phosphate ions into the plaque. This type of buffering activity initially would help in maintaining the local pH at about 5.5. However, when the local pH falls below 5.0, subsurface demineralization is inevitable. This results in the formation of incipient caries, where the surface is intact but demineralization starts below the surface, a process known as subsurface demineralization. When the pH is lowered further it leads to the surface demineralization of enamel.
Factors Determining the Rate of Plaque Acid Production
The maxillary anterior teeth exhibited a greater pH drop in the plaque than the mandibular anterior teeth, indicating that the saliva influences plaque acid production. Brushing the teeth before the test carbohydrate rinse gave unsatisfactory plaque pH curves because of removal of plaque material.
Stralfors (1948) found a correlation between the lowest level to which the plaque pH dropped after the carbohydrate rinse and the lactobacillus count, utilizing this count as a test of caries activity. It was shown that persons with a higher pH have a lower lactobacillus count, and presumably, lower caries activity. Stralfors also reported that the plaque had greater buffering capacity than saliva owing to the presence of bicarbonates and proteins. Vratsanos and his colleagues studied plaque acidogenesis in caries-susceptible and caries-resistant patients and found that plaque pH in caries susceptible persons was lower (6.1 ± 0.3) than in caries resistant persons (7.3 ± 0.4) and that total plaque acid production was also significantly lower in the caries-resistant group.
Some studies have investigated substances capable of inhibiting the reduction in plaque pH after exposure to carbohydrate. Stephan and Miller (1943) applied several synthetic detergents and found at least partial inhibition of the pH drop. One drawback is the penetration of the plaque by inhibitory substances. In thin plaques, the inhibition is greater than in thick plaques. Application of urea was also found to be effective by Stephan, apparently because of hydrolysis by bacterial urease, with the subsequent formation of ammonium carbonate.
Role of Dextranase in Dental Plaque Reduction
An important discovery in dental caries was the recognition that certain cariogenic and highly acidogenic strains of streptococci, especially S. mutans, have the ability to metabolize dietary sucrose and synthesize glucan by utilizing cell surface and extracellular glucosyltransferase. This enzyme is considered to be of special importance in the establishment of S. mutans in the dental plaque. This appears to occur through glucan on the S. mutans cell surface acting as the primary binding site for the enzyme. This reaction then evokes new glucan synthesis from exogenous sucrose with subsequent adherence on to the enamel surface. This glucan is an insoluble, sticky or slimy gel, relatively inert, and resistant to bacterial hydrolytic enzymes, which causes plaque to adhere tenaciously to tooth surfaces. It also appears to act as a barrier against the diffusion of salivary buffers, which ordinarily would neutralize the acids formed in the plaque. Certain cariogenic bacteria are capable of storing intracellular polysaccharides, which may act as a reserve source of carbohydrate for fermentation and maintenance of acid production in the plaque during periods when the diet of the individual is sugar-free.
Both Bowen and Fitzgerald and his associates in 1968 studied dextranase, an enzyme produced by Penicillium funiculosum which hydrolyzes dextran (glucan) and found that it minimizes plaque formation and prevents smooth surface caries in experimental animals.
It is now agreed that the accumulation of dental plaque, even on a clean tooth surface, can result in dental caries in an individual susceptible to the disease and consuming a diet conducive to the disease. Parenthetically, it may be pointed out that plaque-forming streptococci, isolated from the gingival crevice, have been found to be morphologically and serologically similar to known cariogenic strains, thus suggesting a similar etiologic origin for both dental caries and periodontal disease.
The Proteolytic Theory
Although the evidence for the so-called acidogenic theory of dental caries is considerable, it is not wholly accepted as conclusive because much is circumstantial in nature. The proteolytic theory is an alternative explanation in which it has been proposed that the organic or protein elements are the initial pathways of invasion by microorganisms. As a proof of principle, it has been established that enamel contains approximately 0.56% by weight of organic matter.
Certain enamel structures are made up of organic material, such as enamel lamellae and enamel rod sheaths. Enamel lamellae might be important in the progress of dental caries, since they could serve as a pathway for microorganisms through the enamel. Baumgartner (1911) and Fleischmann (1914, 1921) demonstrated that microorganisms could invade the enamel lamellae, and stated that acids produced by these bacteria were capable of destroying the inorganic portion of the enamel.
Gottlieb (1944) and Gottlieb, Diamond and Applebaum (1946) postulated that caries is essentially a proteolytic process: the microorganisms invade the organic pathways and destroy them in their advance. They did admit that acid formation accompanied the proteolysis— Gottlieb held that yellow pigmentation was characteristic of caries and that this was due to pigment production by proteolytic organisms. A similar pigmentation has also been produced by exposing extracted caries-free teeth to pure cultures of lactobacilli in a synthetic medium containing glucose. If no glucose was present, no pigmentation occurred.
Frisbie, Nuckolls and Saunders (1944, 1947) described a microscopic phase of caries in which microorganisms could be demonstrated beneath an apparently intact enamel surface. In some cases, a bacterial plaque was found in position on the overlying enamel surface. Definite early white or brown carious lesions in the enamel exhibited similar but more advanced changes in the enamel matrix. These early lesions extended laterally beneath the intact surface, thus explaining the phenomenon, described by Thewlis, Darling and others, of a radiopaque layer overlying early carious lesions. Fosdick and Hutchinson (1965) ascribed the radiopaque layer to a maturation process in the tooth surface following exposure to the oral environment, which renders the pathways of diffusion at or near the surface less reactive to acids. Under these circumstances, acids have to penetrate to a considerable depth before meeting acid-soluble apatite crystals. Minor variations in the organic and inorganic structures of the tooth are therefore important in determining the pattern and progression rate of early caries.
Caries of the dentin was demonstrated by Frisbie and Nuckolls (1945, 1947) to be similar to that occurring in enamel. These investigators also pointed out that there might be some softening of dentin even though the overlying enamel appeared hard and intact. They assumed that acid would be neutralized before penetrating the full thickness of the enamel and therefore could not cause decalcification of less acid soluble dentin.
Pincus (1948, 1949) proposed that Nasmyth’s membrane and other enamel proteins are mucoproteins, which yield sulfuric acid upon hydrolysis. Lending support to this theory has been the isolation from the oral cavity of gram-negative bacilli capable of producing the enzyme sulfatase. This enzyme releases the combined sulfuric acid from the mucoprotein, but minimally unless the protein is first hydrolyzed to free the polysaccharide component. The liberated acid then dissolves the enamel, combining with the calcium to form calcium sulfate. Interestingly, this compound has been found in carious enamel but not in sound enamel. Sognnaes and Wislocki (1949, 1950) demonstrated the presence of an acid mucopolysaccharide in the interprismatic organic matter of mature enamel, but pointed out that sulfatase had not been demonstrated at the site of a carious lesion. Furthermore, no enzyme systems capable of attacking keratin have been demonstrated in the oral cavity, although other enzymes such as collagenase, hyaluronidase, phosphatase and mucinase, capable of attacking less resistant proteins, have been found.
Manley and Hardwick (1951) attempted to reconcile these two theories concerning the etiology of dental caries. They pointed out that, while the acidogenic and proteolytic mechanisms may be separate and distinct, they need not be so. Many bacteria produce acid from an appropriate carbohydrate substrate; some bacteria capable of producing acid from carbohydrate may even degrade protein in the absence of carbohydrate. On this basis, it has been proposed that there may be two types of carious lesions. In one type, microorganisms invade enamel lamellae, attack the enamel and involve the dentin before there is clinical evidence of caries. In the other, no enamel lamellae are present, and there is alteration of the enamel prior to invasion by microorganisms. This alteration is produced through decalcification of the enamel by acids formed by bacteria in a dental plaque overlying the enamel. The early lesions produced are those typically described as ‘chalky’ enamel.
Although the proteolysis of the organic matrix of dentin may eventually occur after demineralization, there is no satisfactory evidence to support the claim that the initial attack on enamel is proteolytic. In fact, gnotobiotic studies show that caries can occur in the absence of proteolytic organisms. The part played by proteolysis in the initiation of dental caries is likely to be of no significance, but its role in the progression of the more advanced carious lesions cannot be ruled out.
The Proteolysis-Chelation Theory
This theory proposed by Schatz et al (1955) implies a simultaneous microbial degradation of the organic components (hence, proteolysis) and the dissolution of the minerals of the tooth by the process known as chelation. However, this proposal deals with theoretical discussions of the dental disease and the chemical aspects of chelation, with little direct evidence for proteolysis chelation as a mechanism in the caries process.
Chelation is a process involving the complexing of a metallic ion to a complex substance through a coordinate covalent bond which results in a highly stable, poorly dissociated or weakly ionized compound (chelas: claw). Chelation is independent of pH of the medium, so that removal of such metallic ions as calcium from even a biological calcium-phosphorus system may occur at a neutral or even alkaline pH. Numerous naturally occurring biological chelating agents exist, the most common of these being citrate. Amino acids are also known to act as chelators, as well as hydroxy and ketoesters of the Meyerhoff-Embden system of glycolysis; phosphorylated and nonphosphorylated compounds in the hexose monophosphate shunt; polyphosphates including those involved in phosphorylation; carboxylates of the Krebs tricarboxylic acid cycle; certain antibiotics and fermentation products; some proteins, carbohydrates, lipids, nucleic acids and certain enzymes; amines, amidases and certain vitamins; and oxalates, tartrates, salicylate, polyhydric alcohols and even dicumarol.
The proteolysis-chelation theory considers dental caries to be a bacterial destruction of teeth where the initial attack is essentially on the organic components of enamel. The breakdown products of this organic matter have chelating properties and thereby dissolve the minerals in enamel. This results in the formation of substances which may form soluble chelates with the mineralized component of the tooth and thereby decalcify the enamel at a neutral or even alkaline pH. Enamel also contains other organic components besides amelogenin and non amelogenin proteins, such as mucopolysaccharides, lipids and citrates, which may be susceptible to bacterial attack and act as chelators. The proteolysis-chelation theory resolves the argument as to whether the initial attack of dental caries is on the organic or inorganic portion of enamel by stating that both may be attacked simultaneously.
However, several reconciliations have to be made if the proteolysis-chelation theory is to be accepted.These include the observation of:
• Increased caries incidence with increased sugar consumption.
• Increased lactobacillus count with high caries activity.
• Decreased caries incidence following topical or systemic administration of fluoride.
Increased caries incidence concomitant with increased carbohydrate consumption might occur through the action of the carbohydrate in stimulating or increasing proteolysis; producing conditions under which enamel proteins are less stable; and complexing calcium.
Increased caries incidence accompanying increased lactobacillus counts might be explained by the microorganisms being the result of the caries process, rather than its cause. Thus Schatz has suggested that:
• Proteolysis may provide ammonia which prevents a pH drop that would tend to inhibit growth of the lactobacilli.
• The release of calcium from hydroxyapatite by chelation might encourage the growth of lactobacilli, since calcium has been reported to produce this effect.
• Calcium exerts a vitamin-sparing action on some lactobacilli.
Reduced caries incidence concomitant with administration of fluoride might occur through the formation of fluorapatite, which strengthens the linkages between the organic and inorganic phases of the enamel, thereby preventing or reducing their complexing. Although Schatz’s theory is unique and reconciles some of the unexplained facts of the dental caries process, there is insufficient scientific data to permit sound evaluation. Jenkins and Dawes carried out studies to discover whether chelation plays a role in the etiology of caries. They concluded that saliva and plaque do not contain substances in sufficient concentrations to chelate calcium in detectable amounts from enamel. However, although chelation is unlikely to be involved in the initiation of the lesions, it may play a minor role in the established lesion when the plaque pH level returns to neutrality.
Several animal studies, such as those of Zipkin and of Larson and her associates, showed that the incorporation of a chelating agent, ethylenediamine tetraacetic acid (EDTA), into the cariogenic diet resulted in an increase in the severity of dental caries as well as a difference in the distribution pattern of the lesions. Although such evidence does not lend great strength to the proteolysis-chelation theory, at least it does not contradict it.
The Sucrose-Chelation Theory
Egglers-Lura (1967) proposed that sucrose itself, and not the acid derived from it, can cause dissolution of enamel by forming an ionized calcium saccharate. They postulated that calcium saccharates and calcium complexing intermediaries require inorganic phosphate, which is subsequently removed from the enamel by phosphorylating enzymes. However, reinvestigation by other workers failed to confirm this but showed that soluble complex can be formed, even at alkaline pH values, between sucrose and calcium oxide and calcium hydroxide, although not with calcium phosphate.
Current Concepts of Caries Etiology
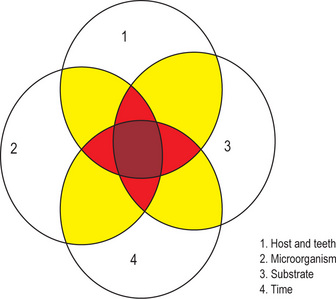
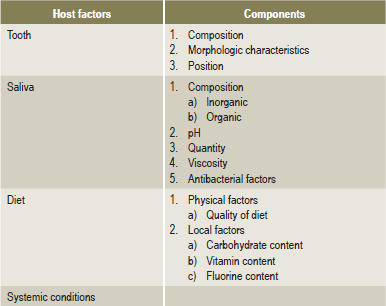
Dental caries is a multifactorial disease with interplay of three primary factors: the host, the microbial flora, and the substrate with time, as an inevitable fourth factor. In other words, caries requires a susceptible host, a cariogenic flora and a suitable substrate that must be present for a sufficient length of time (Fig. 9-4).Conversely, caries prevention is based upon attempts to increase the resistance of the host, lower the number of microorganisms in contact with the tooth and modify the substrate by selecting noncariogenic foodstuffs and reduce the time that the substrate is in the mouth.
The mere presence of microorganisms and a suitable substrate at a given point on a tooth surface is insufficient to establish a carious lesion in all individuals. Variations in caries incidence are due to the presence of a number of indirect or contributing factors.
A workshop on dental caries mechanisms and control techniques was held at the University of Michigan in 1947. This group listed a number of indirect factors that might influence the etiology of caries (Table 9-2).
Tooth Factor
The tooth factor or a susceptible tooth is the most important feature in caries etiology. The structure and composition of teeth undoubtedly influences the initiation and progression of a carious lesion. Studies on the chemical composition of enamel indicate that the surface enamel is more resistant to caries than subsurface enamel. Significant differences in fluoride content of sound and carious teeth have been reported. The enamel of sound teeth contain 0.0111 ± 0.0020% fluoride, while that of carious teeth contain 0.0069 ± 0.0011% fluoride. Microradiographs of the initial carious lesions also indicate a marked decalcification of the subsurface enamel while the surface is relatively intact.
The surface is lower in carbon dioxide, dissolves at a slower rate in acids, contains less water and has more inorganic material than subsurface enamel. These factors apparently contribute to caries resistance and are partly responsible for the slower disintegration of surface enamel than of the underlying enamel in initial carious lesions. Also, the concentration of phosphate and potassium in enamel remains relatively constant after the completion of mineralization of the tissue, suggesting that chemical changes on the enamel surface involve primarily the surface of apatite crystals and the inner lattice structure is less affected. Changes in enamel, such as a decrease in density and permeability and an increase in nitrogen and fluoride content, occur with age. These alterations are part of the posteruptive ‘maturation’ process whereby teeth become more resistant to caries with time.
Morphologic Characteristics of Tooth
The only morphologic feature which conceivably might predispose to the development of caries is the presence of deep, narrow occlusal fissures or buccal or lingual pits. Such fissures tend to trap food, bacteria and debris, and since defects are especially common in the base of fissures, caries may develop rapidly in these areas. Conversely, as attrition advances, the inclined planes become flattened, providing less opportunity for entrapment of food in the fissures, and the predisposition towards caries diminishes.
Certain surfaces of teeth are more prone to decay, whereas other surfaces rarely show decay. For example, in mandibular first molars, the likelihood of decay, in descending order, is occlusal, buccal, mesial, distal and lingual, whereas in maxillary first molars the order is occlusal, mesial, lingual, buccal and distal. On maxillary lateral incisors, the lingual surface is more susceptible to caries than the labial surface due to the frequent presence of a pit at this site. The most susceptible permanent teeth are the mandibular first molars, closely followed by the maxillary first molars and the mandibular and maxillary second molars. The mandibular incisors and canines are least likely to develop lesions.
All available evidence indicates that alteration of the tooth structure by disturbances in formation or in calcification is of only secondary importance in dental caries. The rate of caries progression may be influenced, but caries initiation is affected only to a very little extent.
Position
The position of the teeth seems to be an important factor in the etiology of dental caries. Teeth which are malaligned, out of position, rotated, or otherwise not normally situated may be difficult to cleanse and tend to favor the accumulation of food and debris. This, in susceptible persons, would be sufficient to cause caries in a tooth, which under normal circumstances of proper alignment, would conceivably not develop caries.
Saliva Factor
The fact that the teeth are in constant contact with, and bathed by saliva would suggest that they could profoundly influence the dental caries process (Table 9-3). The complex nature of saliva and variation in its composition are the challenges involved in establishing those factors which may directly influence dental health (Table 9-4).
Table 9-3
Salivary constituents and factors studied in relation to caries
| Inorganic constituents | Organic constituents | Enzymes, solids, and physical factors |
| Positive ions | Carbohydrates | Enzymes |
| Calcium | Glucose | Carbohydrases |
| Hydrogen | Amylase | |
| pH | Lipids | Maltase |
| Buffering power | Cholesterol | Proteases |
| Neutralizing power | Lecithin | Trypsin |
| Salivary factor | Oxidases | |
| Titratable alkalinity | Nitrogen | Catalase |
| Magnesium | Nonprotein | Oxidase |
| Potassium | Ammonia | Total solids |
| Negative ions | Nitrites | |
| Carbon dioxide | Urea | Physical factors |
| Carbonate | Amino acids | Conductivity |
| Chloride | Protein | Freezing point |
| Fluoride | Globulin | Osmotic pressure |
| Phosphate | Mucin | Specific gravity |
| Thiocyanate | Total protein | Surface tension |
| Ash peroxide | Miscellaneous | Viscosity |
| Peroxide |
Modified from F Krasnow: Biochemical analysis of saliva in relation to caries. Dent Cosmos, 78: 301, 1936.
Table 9-4
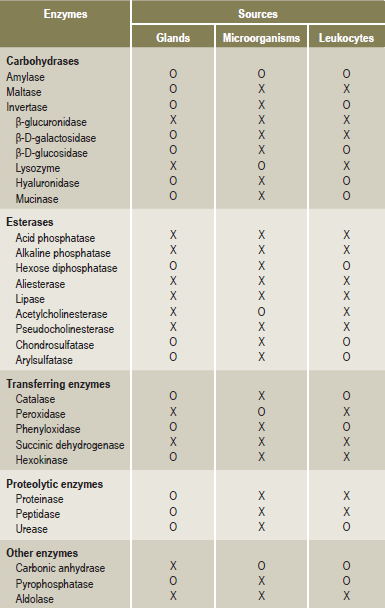
From H H Chauncey: Salivary enzymes. J Am Dent Assoc, 63: 360, 1961. Copyright by the American Dental Association. Reprinted with permission.
The composition of saliva varies between persons and exhibits no constant relation to composition of the blood. There have been many studies on the elementary composition of saliva and its approximate percentage under various circumstances, as well as the correlation with dental caries incidence.
Calcium and Phosphate Concentrations in Saliva
The inorganic phase of enamel consists of crystalline hydroxyapatite essentially in the form of calcium and phosphate complexes of various compositions. These complexes usually dissociate as the pH drops and result in free active concentration of ions. The solubility equilibrium exists when a chemical compound in the solid state is in chemical equilibrium with a solution of that compound. This is an example of dynamic equilibrium in that some individual molecules migrate between the solid and solution phases such that the rates of dissolution and precipitation are equal to one another. At equilibrium, the saliva as a solution is saturated and the ion activity product (IAP) is same as the solubility product (Ksp). If IAP = Ksp, then saturation index (SI) is zero, which means that the mineral is in equilibrium with solution. Under normal circumstances saliva is supersaturated with respect to enamel apatite, which not only prevents enamel from dissolving but even tends to precipitate apatite, in the surface enamel of carious lesions. If IAP is less than Ksp, then SI is negative, the saliva is unsaturated and the teeth would solubilize. If IAP is more than Ksp then SI is positive and saliva is supersaturated and mineral precipitates. Thus, calcium and phosphate in saliva forms an important natural defense mechanism against dissolution of teeth.
The phosphate concentration in saliva tends to fall as the flow rate of saliva increases, whilst the calcium concentration falls initially but then rises at higher flow rates. This is due to the associated increase in pH at high flow rates. The pH affects the IAP in two ways. Firstly, the fraction of total phosphate present as  ions (as opposed to
ions (as opposed to  ) increases markedly with pH. Secondly, the hydroxyl ion concentration also increases with pH.
) increases markedly with pH. Secondly, the hydroxyl ion concentration also increases with pH.
The concentrations of inorganic calcium and phosphorus show considerable variation, depending upon the rate of salivary flow. Currently no consistent relationship has been established between dental caries prevalence and the calcium and phosphorus content of saliva.
There are numerous other inorganic components such as sodium, magnesium, potassium, carbonate, chloride, and fluoride present in the saliva. With the exception of fluoride, these substances have not been thoroughly investigated. Thiocyanate has also been isolated from saliva, and at one time, was thought to inhibit the growth of microorganisms associated with dental caries. It is now conceded that thiocyanate probably has no effect either on the bacterial flora or on dental caries.
The organic constituents of saliva as a group have also been subjected to little more than a cursory examination.
The ammonia and urea content of saliva has been studied by many workers. Turkheim in 1925 noted that the saliva of caries immune persons exhibited greater ammonia content than saliva from persons with caries. Grove and Grove (1934) confirmed this finding and reported that the ammonia of saliva from caries susceptible individuals was about 0–8 mg/100 ml, where as the same in caries-immune individuals was about 4.0–10 mg/100 ml. It was suggested that a high ammonia concentration retarded plaque formation and neutralized acid, at least to some extent. However, White and Bunting, Youngberg and Karshan, among others, found no relation between salivary ammonia and dental caries. The average concentration of urea in saliva which is about 20 mg/100 ml in resting saliva and 13 mg/100 ml of stimulated saliva may be hydrolyzed to ammonium carbonate by urease, thus increasing the neutralizing power of the saliva. The amino acids of saliva have also been suggested as a source of ammonia nitrogen, although Kirch and coworkers could find no correlation between the amounts of amino acids in saliva and caries activity.
The presence of a secreted carbohydrate in the saliva has been argued by various workers. Young, in 1941, reported the presence of a reducing substance in saliva, which he assumed to be glucose. This substance ranged from 11.3–28.1 mg/100 ml in resting saliva and from 14–30 mg/100 ml in stimulated saliva. It was concluded that saliva is not rich in glucose. A number of different enzymes have been isolated from saliva. As shown in Table 9-4, these enzymes are derived from both intrinsic and extrinsic sources.
The most prominent and important oral enzyme is amylase, or ptyalin, a substance responsible for the degradation of starches. Parotid saliva is always higher in amylase content than saliva from the other glands. The relation between amylase activity and dental caries has been studied by numerous investigators with conflicting results.
pH of Saliva
The pH of saliva has been studied intensively because of the apparent relation of acidic pH of saliva to dental caries. However, inconsistent and conflicting data may arise from failure to collect the saliva under oil, thus reducing loss of carbon dioxide which would cause elevation of the pH.
The pH at which any particular saliva ceases to be saturated with calcium and phosphate is referred to as the ‘critical pH’; below this value, the inorganic material of the tooth may dissolve. Critical pH varies according to the calcium and phosphate concentration, but it is usually about 5.5. With increasing concentration of hydrogen ions in the plaque, more phosphate ions will leave the solid apatite phase.
Buffer Capacity of Saliva
The buffer capacity of the saliva, which may account for some of the observed differences between salivary pH and caries incidence is not necessarily reflected by the pH of the saliva. Karshan and his associates (1931) pointed out that titratable alkalinity is a better indicator of buffer capacity than the pH, but found that saliva from caries immune and caries susceptible persons exhibited essentially the same titratable alkalinity. White and Bunting in 1936 studied the carbon dioxide capacity of resting and stimulated saliva in caries free and caries susceptible children. Although the values for stimulated saliva were much higher than those for resting saliva, no remarkable differences were noted in the mean values. However, Karshan (1936) noted a significant difference in the mean value of carbon dioxide capacity of stimulated saliva between caries free group and caries active group, which was between 31.1 ml/100 ml of saliva and 19.5 ml/100 ml of saliva respectively. Sellman (1949) studied the buffer capacity of saliva and its relation to dental caries and found that the total amount of acid needed to reduce the salivary pH to a given pH level (6, 5, 4 and 3) was always greater for saliva from caries-resistant persons. Sullivan and Storvick (1950) also reported a significant inverse correlation between the DMF teeth and the buffer capacity of saliva.
The acid production, significant in the caries process, occurs at a localized site on the tooth. This site, particularly in the early stages of caries is protected by the dental plaque, which appears to act as an osmotic membrane preventing free exchange of ions. Thus, even though buffer ions are present in the saliva, they may not be totally available at specific sites. The entire problem of the buffering capacity of saliva and its relation to dental caries requires further investigation.
In saliva, the chief buffer systems are bicarbonate carbonic acid ( , pk1=6.1) and phosphate (
, pk1=6.1) and phosphate ( , pK2 = 6.8). pK marks the point on the curve where the pH changes the least. Variations in bicarbonate concentration are the chief determinants of salivary pH. Saliva is poorly buffered with a pH as low as 5.3 as seen in unstimulated saliva where the bicarbonate concentration is low, whereas the salivary bicarbonate concentration may reach as high as 60 mM at high flow rates and this type of saliva is well buffered with a pH as high as 7.8.
, pK2 = 6.8). pK marks the point on the curve where the pH changes the least. Variations in bicarbonate concentration are the chief determinants of salivary pH. Saliva is poorly buffered with a pH as low as 5.3 as seen in unstimulated saliva where the bicarbonate concentration is low, whereas the salivary bicarbonate concentration may reach as high as 60 mM at high flow rates and this type of saliva is well buffered with a pH as high as 7.8.
By virtue of the volatile nature of CO2 gas, the breakdown of bicarbonate by acids leads to the eventual escape ofCO2. The loss of CO2, in effect, removes the acid element of the bicarbonate carbonic acid system and reduces the change in the ratio of bicarbonate to carbonic acid. Most of the CO2 in saliva is in the form of bicarbonate, carbonate and dissolved CO2. When saliva is exposed to atmospheric air in the mouth or in a beaker, there is a loss of dissolved CO2 and an increase in pH, which may reach higher than 9. Further loss of CO2 occurs due to the presence of carbonic anhydrase in saliva. The rapid loss of CO2 from freshly secreted saliva and the rise of pH may be sufficient to cause the solubility product for hydroxyapatite to be exceeded leading to precipitation of this compound, as well as other calcium phosphate salts. These properties of saliva may be the reason why calculus formation is greatest in the area approximating the orifices of the parotid and submandibular salivary gland ducts.
The buffering capacity of saliva is a very significant property that affects the dental caries process. The bicarbonate in saliva is able to diffuse into the dental plaque to neutralize the acid formed from carbohydrate by the microorganisms. The higher the flow rate, the greater will be its buffering capacity. Dialysis of saliva, which removes both bicarbonate and phosphate but not protein, results in total loss of salivary buffering capacity. This indicates that salivary proteins can be disregarded as buffers in saliva. Further evidence of the importance of saliva as a buffer was demonstrated when the pH of carious lesions and of dental plaque was studied. Within active carious lesions, a pH gradient exists. The deep advancing edges of such lesions were more acidic than the shallower layers, which had a pH similar to that of saliva. In enlarged and exposed cavities that are emptied of their contents, the carious layerwas shallower and the pH closer to neutrality, probably because of better access to saliva.
Quantity of Saliva
The quantity of saliva secreted in a given period of time may, theoretically at least, influence caries incidence. This is especially evident in cases of salivary gland aplasia and xerostomia in which salivary flow may be entirely lacking, typically resulting in rampant dental caries. It has been found that the range of variation of resting saliva among different persons is greater than the range of stimulated saliva. Furthermore, when persons from a slow flowing group and from a fast-flowing group are stimulated, the flow of activated saliva from the two groups exhibits little difference, thus masking the natural difference. It seems probable that the rate of salivary flow is simply one additional factor which helps contribute to caries susceptibility or caries resistance. Mild increases or decreases in flow may be of little significance; However, total or near-total reduction in salivary flow adversely affects dental caries in an obvious manner.
Reduced salivary flow or hyposalivation is a consequence of pathological conditions or the use of antisialagogues. Under normal conditions, salivary flow is almost entirely under parasympathetic neural control. Drugs such as atropine, which affect the cholinergic parasympathetic nerves, produce decreased salivation. Hyposalivation also occurs in patients who are dehydrated due to conditions such as fever or prolonged diarrhea. Hyposalivation is also associated with diabetes, anemia, hypovitaminosis A or B, uremia and dehydrating disease of old age. Many of the common drugs administered to old people for a variety of health problems can result in xerostomia. A restriction in salivary flow leads to exacerbation of dental caries, as the removal of bacteria and food debris from the mouth are two important functions of saliva with respect to caries. Despite the continuous flow of saliva, dental plaque can accumulate at a rapid rate of (10–20 mg/day) in the absence of oral hygiene procedures but the rate of plaque accumulation appears to be even more rapid in patients with xerostomia (Llory et al, 1972).
Viscosity of Saliva
The viscosity of saliva accounting for differences in caries activity between different persons, appears to have an empiric foundation rather than a scientific basis, as judged by the paucity of pertinent experimental studies reported in scientific literature. Miller thought that salivary viscosity was not of great importance in the caries process since numerous cases could be found in which saliva was extremely viscous and the patients were free of caries. The reverse has also been shown where patients with an abundant, thin, watery saliva often exhibit rampant caries. The viscosity of the saliva is largely due to the mucin content, derived from the submandibular, sublingual and minor salivary glands, but the significance of this substance in relation to dental caries is not entirely clear.
Antibacterial Properties of Saliva
The antibacterial properties of saliva have been investigated by numerous workers in an attempt to explain the wide variation in caries incidence among different persons. Clough in 1934 tested 41 different salivas for their effect on the growth of L. acidophilus, utilizing ‘wells’ in seeded culture plates. The caries experience of the patients from whom the saliva was taken with the degree of bacterial inhibition could not be correlated. van Kesteren and associates found that the saliva probably contains at least two antibacterial substances, one of which resembled lysozyme, the other being distinctly different. Using L. acidophilus as the test organism, Hill in 1939 found that saliva from caries free person had a greater inhibiting effect than saliva from caries active persons.
A bacteriolytic factor in the saliva of caries immune persons, which was absent in saliva from caries susceptible ones, was reported by Green. This factor was active against lactobacilli and streptococci, and appeared to exert its lytic effect on cells commencing the process of division. Further studies indicated that the factor was a protein associated with the globulin fraction of saliva. Since it resembled some antibacterial factors in serum, it was apparently different from other reported salivary antibacterial substances.
Lysozyme (N-acetylmuramide glycanohydrolase)
A hydrolytic enzyme in saliva cleaves the β-1-4 linkage between N-acetylglucosamine and N-acetylmuramic acid, which constitute the repeating disaccharide unit of the cell wall peptidoglycan. In the presence of sodium lauryl sulfate, a detergent, lysozyme can lyse many cariogenic and noncariogenic streptococci and it has been found that the lysozyme activity is significantly greater in a group of caries free preschool children than in a caries susceptible group.
Salivary peroxidase system
The salivary glands secrete salivary peroxidase and thiocyanate (SCN–), which acts on hydrogen peroxide generated by certain bacteria. This oxidoreductase system catalyzes the oxidation of the thiocyanate ion to hypothiocyanate ion (OSCN–). The product OSCN– reacts readily with sulfhydril compounds of low molecular weight and thereby inactivates many bacterial enzymes of the glycolytic pathway and inhibit their growth.
This antibacterial system is known to be inhibitory towards L. acidophilus and S. cremoris, by preventing cells from accumulating lysine and glutamic acid, which are essential for growth. Further investigation is necessary to determine whether this enzyme can control cariogenic bacteria in vivo. The significance of antibacterial factors in saliva has been questioned by many workers, including Bibby (1956) who pointed out that regardless of the quality of the saliva, including the relative presence or absence of inhibitory principles, saliva always appears to contain bacteria capable of producing caries if carbohydrates are present.
Immunoglobulins
The predominant immunoglobulin class in saliva is secretory IgA or sIgA. Salivary IgA differs from serum IgA, Secretory IgA is a product of two different cell types where plasma cells synthesize polymeric IgA containing J chain of about 1.5 kD and glandular cells synthesize a glycoprotein secretory component (SC) of 7 kD. While the secretory component is attached entirely to one of the 2 IgA molecules, the J chain is attached to both. SC is a receptor for the polymeric immunoglobulin A containing J chain; the IgA binds to SC below the tight junction of glandular epithelial cells and is then transported across to the luminal surface. The presence of SC makes sIgA resistant to proteolytic enzymes. Purified salivary IgA and IgG fractions have been found with agglutinating activity against oral isolates of α-hemolytic streptococci. The existence of plasma cells located in salivary glands is of great interest because of the potential for producing a local response to an antigen. It is known that ingestion of inactivated S. mutans cells by germ free rats elicits salivary antibody formation as does the consumption of large numbers of S. mutans cells by human subjects (McGhee et al, 1978). The concentration of salivary IgA is approximately 4 mg/100 ml in stimulated submandibular and parotid saliva. However, its concentration is considerably higher in the secretions of minor salivary glands and reaches levels of about 30 mg/100 ml. Animal experiments suggest that both systemically and locally produced antibodies may operate to protect against caries. The latter involves the local immune mechanism via the saliva and the other involves gingival crevicular fluid, which is derived from plasma (Lehner, 1978).
The Diet Factor
The role of the diet and nutritional factors deserves special consideration because of the often observed differences in caries incidence of various populations who subsist on dissimilar diets. Although many clinical studies have been carried out in an attempt to study certain components of the diet with regard to caries, a number of variable factors have usually clouded the results. The use of experimental animals which are susceptible to destruction of the teeth similar to human dental caries has greatly aided the study of dietary considerations in dental caries (Fig. 9-5).
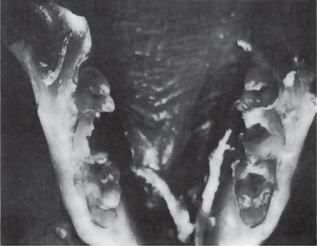
Physical Form
The physical nature of the diet has been suggested as one factor responsible for the difference in the caries experience between primitive and modern man. The diet of the primitive man consisted generally of raw unrefined foods containing a great deal of roughage, which cleanses the teeth of adherent debris during the usual masticatory excursions. In addition, the presence of soil and sand in incompletely cleaned vegetables in the primitive diet induced severe attrition of both occlusal and proximal surfaces of the teeth. This resulted in flattening of the occlusal and proximal surfaces causing a reduction in the probability of decay. In the modern diet, soft refined foods tend to cling tenaciously to the teeth and are not removed because of the general lack of roughage. Augmenting this collection of debris on the teeth is the reduction of mastication due to the softness of the diet. The detrimental effect of this decreased function on the periodontal apparatus should be obvious.
It has been demonstrated that mastication of food dramatically reduces the number of cultivable oral microorganisms. Since those areas of teeth that are exposed to the excursions of food are usually immune to caries, mechanical cleansing by detergent foods may have some value in caries control. Clinical studies have not confirmed that physical parameters are as important as the frequency of eating in determining cariogenicity of foods. The carbohydrate content of the diet has been almost universally accepted as one of the most important factors in the dental caries process and one of the few factors, which may be consciously altered as a preventive measure.
Epidemiological studies have shown that the incidence of dental caries differs immensely among population groups. Although part of the variance can be due to genetic factors, the diets of different ethnic groups probably account for the major differences. The prevalence of caries among native populations was very low and native diet did not contain any sucrose other than small amounts found in fruits and vegetables. As their diets changed to include products containing sugar, their prevalence increased.
Becks and his associates (1944) studied the effect of carbohydrate restriction on the L. acidophilus index and the caries experience in a group of 1,250 persons with rampant caries and in 265 caries free persons. Replacement of refined dietary carbohydrate with meat, eggs, vegetables, milk and milk products resulted in an 82% reduction in the lactobacillus index and in clinical evidence of extensive arrest of caries. The observation was made that some persons consumed large amounts of carbohydrate without acquiring caries, while others had rampant caries even though consuming very little carbohydrate. These workers were prompted to suggest that, in addition to excessive amounts of refined carbohydrates, other factors undoubtedly have a bearing on the disease.
Institutional studies were carried out in a mental institution at the Vipeholm Hospital near Lund, Sweden, more popularly known as the Vipeholm study. The institutional diet was nutritious but contained little sugar with no provision for between meal snacks. The dental caries rates in the inmates were relatively low. The experimental design divided the inmates into seven groups; sugar was introduced either at mealtime in bread and solution or between meals in caramels, toffee and chocolates. The conclusions from the study were that an increase in carbohydrate definitely increased the caries activity. The risk of sugar increasing caries activity was greatest when the sugar was consumed between meals and in a form that tends to be retained on the surfaces of the teeth.The increase in caries activity drastically reduced upon withdrawal of the sugar-rich foods.
Most importantly, the clearance time of the sugar correlated closely with caries activity. The Vipeholm study clearly showed that the physical form of carbohydrates, clearance time of sugars and the frequency of intake were more important in cariogenicity than the total amount of sugar ingested. Another large-scale and important experiment on caries in human subjects was carried out inTurku, Finland with the aim of comparing the cariogenicity of sucrose, fructose and xylitol. The basis of the experiment was that xylitol is a sweet substance not metabolized by plaque organisms. In addition to data indicating that xylitol would be an acceptable metabolite in humans, there was a dramatic reduction in the incidence of dental caries after two years of xylitol consumption. Fructose was as cariogenic as sucrose in the first 12 months but became less so at the end of 24 months.
In spite of the overwhelming evidence relating carbohydrate intake to dental caries, enough exceptions have been noted. In India among certain segments of the population there may be a high carbohydrate intake, but a very low caries incidence. A complicating factor has been the difficulty in obtaining data from human feeding studies under experimental conditions.
Carbohydrate Intolerance and Dental Caries
An intolerance to disaccharide or monosaccharide occurs because of a deficiency of a specific enzyme involved in the metabolism of the sugar is described as hereditary fructose intolerance syndrome. Hereditary fructose intolerance syndrome first described by Froesch in 1959 is an inborn error of fructose metabolism transmitted by an autosomal recessive gene. It is caused by remarkably reduced levels of hepatic fructose-1-phosphate aldolase, which splits fructose-1-phosphate into two to three carbon fragments to be further metabolized by the Embden-Meyerhof (EM) pathway. Persons affected with this metabolic disorder learns to avoid any food containing fructose because the ingestion of these foods causes symptoms of nausea, vomiting, malaise, tremor, excessive sweating and even coma due to fructosemia. Most of these symptoms can be attributable to secondary hypoglucosemia resulting from a block in glycogenolysis. However, they eat glucose, galactose, lactose and starch containing foods such as milk, dairy products, rice and noodles. Although there have been only a limited number of cases reported in the literature, the dental caries prevalence of these subjects have generally known to be extremely low. Caries, when found, is restricted to pits and fissures and is usually not found in smooth enamel surfaces.
Assessment of Cariogenic Potential of Diet
A number of different approaches have been used in attempting to develop reliable methods for measuring the caries inducing potential of individual foods. These include in vitro models of caries such as adhesiveness of foods, enamel demineralization, production of titratable acids, monitoring of plaque pH changes in vivo and in vitro, and animal testing to measure cariogenicity of individual foods fed to rodents under standardized conditions.
Many animal studies have been carried out in attempting to clarify some of the perplexing problems of dental caries. Some of these have dealt with the cariogenic effect of different carbohydrates, and it has been found that not all sugars have the same cariogenicity. The animal data must be interpreted with caution due to the entirely different ecologic system in the human mouth compared to experimental animal mouths.
However, some general conclusions may be drawn from the data in which experimental animals fed by stomach tube did not develop caries despite the prevalence of cariogenic microorganisms. The relationship between the sucrose content of the food or of the total diet and the resulting caries may not necessarily be linear but it is direct. Other animal studies have shown that the concentration of sucrose in the diet strongly influences the incidence of smooth surface and fissure caries. On a sound scientific basis, it is difficult to draw definite conclusions about the relation between dental caries and refined carbohydrates. Nevertheless, the bulk of available evidence indicates that a positive relationship exists, even though many other factors are also important.
Cariogenicity of Sucrose and other Carbohydrates
The principal carbohydrates available in human diets are starches, sucrose and some lactose, with less glucose, fructose or maltose. From a clinical standpoint the significant comparison is between starch and sucrose or between the two sucroses, as they have been labeled the primary culprit in the pathogenesis of dental caries. In many foods, such as cakes and pastries, sucrose coexists in a mixture with cooked starch. The key role of sucrose as a dietary substrate in the caries process on smooth surfaces can be explained on a biochemical basis. Dental plaque is a prerequisite for the development of smooth surface caries. The presence of extracellular polysaccharides, namely glucan and levan, has been clearly demonstrated in dental plaque. The glucans, particularly the water insoluble fraction, can serve as structural component of the plaque matrix and effect in gluing certain bacteria to the teeth.
The soluble levans and some of the soluble glucans are degradable by the plaque flora and may function as transient reserves of fermentable carbohydrates thereby prolonging the duration of acid production. These polysaccharides are synthesized by enzymes, which for most part are extracellular or bound to the cell surface and show a high specificity for sucrose as a substrate. Polysaccharide is built up by extrusion from the enzyme. The enzymes involved in the synthesis, glucosyl and fructosyl transferases, have been isolated and purified from S. sanguis and S. mutans.
These enzymes are highly specific for sucrose and will not utilize sugars such as fructose, glucose, maltose, or lactose. They have a large pH optimum of 5.2–7.0 coinciding with the pH range of dental plaque. As long as sucrose is present in plaque, the glucosyl transferase enzymes will continue to utilize it to form plaque matrix material and fructose. The latter can be readily fermented by the plaque flora to form organic acids. The glucosyl transferase (GTF) of the mutans group has received considerable attention and several isozymes have been isolated. There are two types of these enzymes:
• Those that synthesize a soluble glucan with predominantly 1,6-α-D-glucose sequences (GTF-S).
• Those that synthesize an insoluble, essentially linear 1,3-α-D-glucan (GTF-I).
By cooperative action of these enzymes, a sticky water insoluble polysaccharide is synthesized from sucrose that is a major factor in the accumulation of mutans group of streptococci on smooth surfaces of teeth. Starches are probably prevented from direct entry into plaque because of limited diffusion of such large molecules.
The first step in the catabolism of sugars is their transport into the cytoplasm of the microorganism. Sugars are transported either by a carrier mediated active transport (permease) system or group translocation (phosphotransferase system, PTS). Active transport releases sugar unmodified into the cytoplasm, whereas the sugar gets chemically modified to a phosphate ester before it appears inside the cell by group translocation. The uptake of sugars by oral streptococci (S. mutans, S. sanguis, and S. salivarius) involves a phosphoenol pyruvate dependent phosphotransferase system. Sucrose is utilized directly by S. mutans mostly via PTS, than via prior hydrolysis to glucose and fructose by invertase. The intracellular product, sucrose 6-phosphate is then cleaved by a sucrose 6-phosphate hydrolase, yielding glucose 6-phosphate and fructose. The sucrose 6-phosphate hydrolase has dual specificity for sucrose 6-phosphate and sucrose. Sugar phosphates are subsequently integrated into the catabolic pathways, which in the case of the oral streptococci is predominantly the EM pathway.
Maltose, lactose, fructose and glucose can be used by the oral flora for the synthesis of bacterial cell walls, capsular and intracellular polysaccharides and organic acids. The bulk of glucosyl and fructosyl moieties of sucrose are fermented to organic acid products. Sucrose is unique in that it can also serve in the formation of insoluble extracellular polysaccharides and thereby enhance plaque formation and microbial aggregation on the tooth surface. Of considerable ecological significance are some of the properties of these extracellular glucans, which are high molecular weight polymers of glucose. Many are sticky and insoluble, which makes them more resistant to oral bacterial degradation. Glucans cause clumping of specific strains of oral bacteria and can be adsorbed onto hydroxyapatite. Although the adherence of S. mutans to smooth surfaces is greatly increased by the production of glucans in the presence of sucrose, these organisms can attach to surfaces in the absence of sucrose, but at much lower levels.
Other Dietary Components of Dental Caries
Lipids
The medium chain fatty acids and their salts have antibacterial properties at low pH. The mechanism of action is not well defined. They serve as anionic surfactants and uncouple substrate transport and oxidative phosphorylation from electron transport in bacteria. Changes in cell permeability may be involved. Potassium nonanoate has been studied because, when added to a cariogenic diet fed to rats, it produced a significant reduction in the caries score. Human studies with a daily mouthwash containing nonanoate have demonstrated a change in the plaque flora, including a reduction in the proportion of acidogenic organisms. The potential of lipids as anticariogenic food additives requires further exploration.
Vitamin
The vitamin content of the diet has been reported by many workers to have a significant effect on dental caries incidence. Vitamin A deficiency has definite effects on developing teeth in animals and presumably in human beings as well, although only a few reports on dental disturbances in vitamin A deficiency in humans are available in literature. Vitamin D has probably been investigated with greater thoroughness in relation to dental caries than any other vitamin. There is general agreement on the necessity of vitamin D for the normal development of the teeth. Malformation, particularly enamel hypoplasia, has been described in the deficiency state by many workers. The relation of rickets to dental caries is not well defined, however. The only possible way in which infantile rickets could influence dental caries incidence is through an alteration in tooth structure, which makes the teeth more susceptible to caries. Pertinent clinical studies are not in agreement and many of the earlier studies are particularly confusing because of inaccurate reporting of data. Subsequent studies on the permanent teeth showed no differences in the caries incidence between the rachitic and control groups.
The effect of vitamin D supplement on the dental caries experience has also been studied to determine whether this might be of significant benefit. The evidence indicates that vitamin D supplements may reduce dental caries increment, particularly in children who may not be receiving adequate vitamin D. Ingestion of vitamin D in excess of adequate metabolic requirements has only a questionable effect on the caries experience. Although the effect of vitamin D on the dental caries experience is uncertain, its effect on forming dental structures cannot be overemphasized.
Vitamin K has been tested as a possible anticaries agent by virtue of its enzyme-inhibiting activity in the carbohydrate degradation cycle. There are no known effects of vitamin K deficiency on dental caries incidence.
Dreizen and his coworkers (1947) studied the effect of vitamin B deficiency diseases on dental caries in children. The malnourished children presented a remarkably lower caries increment than the group of well-nourished children. The data suggest that vitamin B complex deficiency may exert a caries-protective influence on the tooth, since several of the B vitamins are essential growth factors for the oral acidogenic flora and also serve as components of the coenzymes involved in glycolysis. Vitamin B6(pyridoxine) has been proposed as an anticaries agent on the hypothetical ground that it selectively alters the oral flora by promoting the growth of non-cariogenic organisms, which suppress the cariogenic forms (Strean, 1957). Slight to significant reduction in the caries increment of children and pregnant women have been reported following the use of pyridoxine-containing lozenges after each meal.
Vitamin C deficiency is well recognized for producing severe changes in the periodontal tissues and pulps of the teeth. A few studies have also been carried out to determine whether scurvy might be related to dental caries incidence or whether ascorbic acid supplements might prevent dental caries. The available scientific evidence indicates that there is no relation between scurvy and increased caries incidence in the human being. Furthermore, there is no evidence to indicate that vitamin C supplements would in any way protect against dental caries.
The calcium and phosphorus dietary intake has been popularly related to the dental caries experience, although the scientific evidence for this correlation is lacking. Disturbance in calcium and phosphorus metabolism during the period of tooth formation may result in severe enamel hypoplasia and defects of the dentin. But a calcium disturbance occurring after tooth formation has been completed, results in no changes in tooth substance itself. Albright and his associates in 1934 studied 16 cases of human hyperparathyroidism and noted that even though there was severe loss of calcium from the bone, the teeth remained intact.
The literature is replete with studies which show that phosphates are effective cariostatic agents when added to the cariogenic diets of laboratory rodents (Nizel and Harris, 1964). Their effectiveness depends on the anions and cations with which they are combined and on the foodstuffs with which they are fed. The caries reduction in rodents given supplemental phosphates involves a mechanism, which operates after the teeth have erupted. The results of clinical tests of phosphate additives for the purpose of controlling human caries have been equivocal. Available evidence indicates that there is no relation between dietary calcium and phosphorus and dental caries experience.
The fluoride content of the diet and of specific foodstuffs, in particular, has been investigated by numerous workers. Varying amounts of fluoride are found in many plant substances, depending to some extent upon the fluoride content of the soil in which they were grown. In general, the leaves of plants contain more fluoride than the stems, and the skin of fruit contains more than the pulp. There has been little attempt made to study the dietary fluoride in relation to dental caries as has been done for the fluoride content of drinking water. Some workers believe that dietary fluoride is relatively unimportant compared to fluoride in the drinking water because of its metabolic unavailability.
The effect of two additional trace minerals, selenium and vanadium, present in drinking water and food in certain localities, has been investigated for possible effects on dental caries by Tank and Storvick. Their studies indicate that dental caries rates were significantly higher in permanent teeth of persons residing in seleniferous areas than in nonseleniferous areas, but that a decrease in dental caries rates of permanent teeth was observed with increasing vanadium concentrations. The significance of these findings has not been clarified.
Systemic Factors
There are certain factors, dissociated from the local environment or at least not intimately associated with it, which have been related to dental caries incidence and which may be conveniently discussed under this general heading.
Heredity
Heredity has been linked with the dental caries incidence in scientific literature for many years. In 1899, GV Black wrote, “When the family remains in one locality, the children living under the conditions similar to those of the parents in their childhood, the susceptibility to caries will be very similar in the great majority of cases. This will hold good even to the particular teeth and localities first attacked, the order of occurrence of cavities, and the particular age at which they occur.”
This racial tendency for high caries or low caries incidence, in some instances at least, appears to follow hereditary patterns. The fact that local factors may easily alter this tendency (e.g. exposure to a highly refined diet inducing high caries experience) would indicate that heredity does not exert a strong influence in determining individual caries susceptibility. That it is a factor, however, cannot be denied since even in the experimental conditions, definite caries-susceptible and caries immune strains of rats and hamsters have been developed. Some of the earlier studies aimed primarily at confirming this heredity–caries relationship were carried out on different races living in the same geographic areas. Unfortunately, in any such study, there are uncontrollable factors which cannot be compensated. Dietary habits, food likes and dislikes, cooking habits and even toilet habits such as toothbrushing frequency and methods are often passed down from generation to generation, parents to offspring, may ultimately confound the pure effects of heredity.
One of the most significant studies is that reported by Klein in 1946 on the results of examination of 5,400 persons in 1,150 families of Japanese ancestry. In this study, the DMF was established for each individual, and 30% of the fathers with the lowest DMF rate were designated arbitrarily as ‘low DMF’. The 30% with the highest DMF were designated as ‘high DMF’, while the middle 40% were classified as ‘middle DMF’. The same groupings were used for the mothers and for the sons and daughters of these parents. It was found that a ‘high DMF’ father and ‘high DMF’ mother produced offsprings with a ‘high DMF’ rate. On the other hand, if the father and mother were both ‘low DMF’, the children also were in a ‘low DMF’ group. The differences between these two extremes became more pronounced with increasing age. However, the results were so consistent that it was difficult to exclude the view that dental caries in children involved strong familial vectors, probably with a genetic basis and perhaps sex-linked (Fig. 9-6).
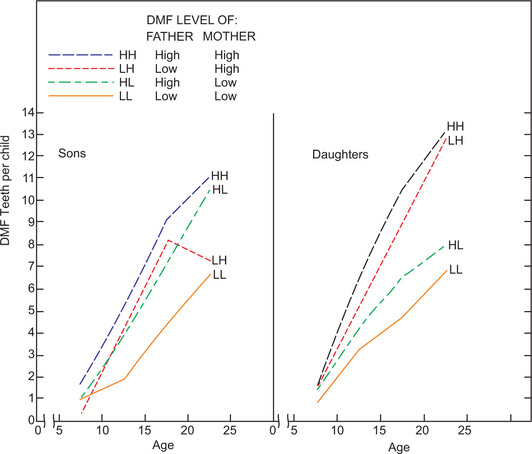
Figure 9-6 Heredity and dental caries.
The relation between DMF levels of sons and daughters and DMF levels of fathers and mothers, by age of offspring, is illustrated (From H Klein: The family and dental disease. IV: dental disease [DMF] experience in parents and offspring. J Am Dent Assoc, 33: 735, 1946).
There is still no indisputable evidence that heredity per se has a definite relation to dental caries incidence. The possibility exists that if there is any such relation, it may be mediated through inheritance of tooth form or structure, which predisposes to caries immunity or susceptibility. The problem is of such complexity that more intensive investigation is necessary before any positive conclusions can be drawn.
Pregnancy and Lactation
Studies relating to lactation and caries incidence are too few to contribute any significant data for clarifying this problem. Evidence suggests that there is no correlation between the dental caries experience and pregnancy per se or between caries and the number of pregnancies. It should also be remembered that there is no mechanism for the physiologic withdrawal of calcium from teeth so that a developing fetus cannot calcify at the expense of the mother’s teeth.
Deakins (1943) and Deakins and Looby (1943) studied the specific gravity of dentin as an indication of its mineral content and found that there were no significant differences in dentin samples from carious teeth of pregnant and nonpregnant women. They concluded that there was no calcium withdrawal from sound dentin during pregnancy.
It is a fairly common clinical observation that a woman, during the later stages of pregnancy or shortly after delivery, will manifest a significant increase in caries activity. In nearly all cases, thorough questioning will reveal that the woman has neglected her ordinary oral care because of the pressure of other duties attendant to the birth of the baby. Thus the increased caries incidence, though indirectly due to pregnancy, may actually be a local problem of neglect.
Clinical Aspects of Dental Caries
Clinical Classification of Caries
There is no universally accepted classification of dental caries. It may be classified according to three basic factors depending on morphology, dynamics and chronology.
According to the morphology or anatomical site of the lesion on an individual tooth, caries is classified as: (1) pit or fissure caries (Fig. 9-7 A, B), and (2) smooth surface caries.

Depending on the rate of carious progression, the process is classified as: (1) acute dental caries, and (2) chronic dental caries. It can also be a primary (virgin) caries, attacking previously intact surface (Fig. 9-8), or a secondary (recurrent) caries–occurring around the margins of a restoration (Fig. 9-9). It can also be classified as infancy (soother or nursing bottle caries) and adolescent caries based on chronology.
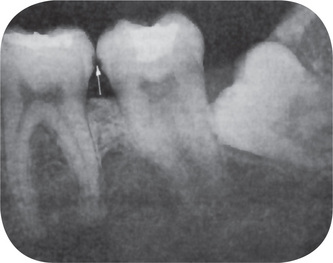
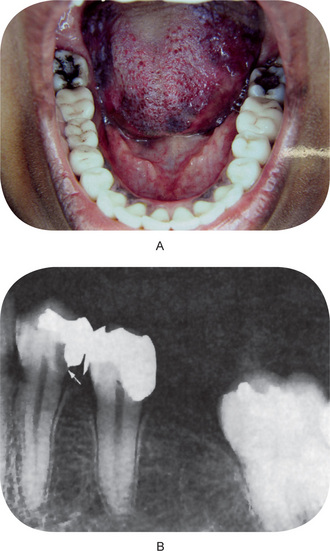
Figure 9-9 (A) Recurrent caries beneath a faulty restoration. (B) Secondary caries around the margins of restoration. A, Courtesy of Dr V Gopikrishna, Department of Conservative Dentistry, Meenakshi Ammal Dental College, Chennai.
Pit and Fissure Caries
The commonest and simplest classification of dental caries is based on relative susceptibility of surfaces of teeth. Pit and fissure caries of the primary type develops on the occlusal surface of molars and premolars, buccal and lingual surface of the molars and the palatal surface of the maxillary incisors. Pits and fissures with high steep walls and narrow bases are those most prone to develop caries due to their mechanical characteristics, which result in poor self-cleansing features. These deep pits or fissures are sometimes considered developmental faults, particularly since the enamel in the extreme depth is often very thin or even occasionally absent. Deep and narrow pits and fissures favor the retention of food debris along with microorganisms, and caries may result from fermentation of this food and the formation of acid.
Pits and fissures affected by early caries may appear brown or black and will feel slightly soft and ‘catch’ a fine explorer point. The enamel directly bordering the pit or fissure may appear opaque bluish white as it becomes undermined. This undermining occurs through lateral spread of the caries at the dentinoenamel junction, and it may be a rapid process if the enamel in the base of the pit or fissure is thin.
The lateral spread of caries at the junction as well as penetration into the dentin along the dentinal tubules may be extensive without fracturing away the overhanging enamel. Thus, there may be a large carious lesion with only a tiny point of opening. This undermined enamel may suddenly give way under the stress of mastication, or the dentist may suddenly open into a large cavity when excavating the pit or fissure. This phenomenon was the origin of the mistaken idea of ‘internal caries’, the view that a tooth may decay from inside outward. Needless to say, a point of penetration is always present. It should not be inferred that all pit and fissure caries begin with a narrow penetration point and develop a large cavitation with overhanging enamel. In many cases, the lesion begins as an open cavity and becomes progressively larger. In this type of caries the progress of the disease is usually much slower and pulp involvement is often delayed.
Smooth Surface Caries
Smooth surface caries (Fig. 9-10A) of the primary type is caries that develops on the proximal surfaces of the teeth or on the gingival third of the buccal and lingual surfaces. Seldom does caries occur on other areas of the teeth, except in cases of malposed or malformed teeth, because of the self-cleansing properties of these areas. Unlike pit or fissure caries, which is not dependent on the development of a definite, grossly recognizable plaque for the initiation of caries, smooth surface caries is generally preceded by the formation of a microbial plaque. This ensures the retention of carbohydrate and microorganisms on the tooth surface in an area not habitually cleansed and subsequent formation of acid to initiate the caries process.
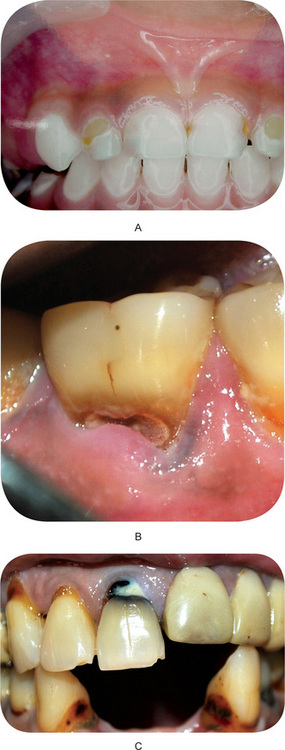
Figure 9-10 (A) Smooth surface caries. (B) Cervical Caries. (C) Root Caries. Courtesy of A, Dr MS Muthu, Dr Sarath Asokan, Department of Pedodontics, Meenakshi Ammal Dental College, Chennai, Dr Joshua Sheih,Emmanuel Dental Clinic, Chennai and B, C, Dr Joshua Sheih,Emmanuel Dental Clinic, Chennai.
Proximal caries usually begins just below the contact point and appears in the early stage as a faint white opacity of the enamel without apparent loss of continuity of the enamel surface (Fig. 9-11). In some cases it appears as a yellow or brown pigmented area, but in either event is usually rather well demarcated. The early white chalky spot becomes slightly roughened owing to superficial decalcification of the enamel.
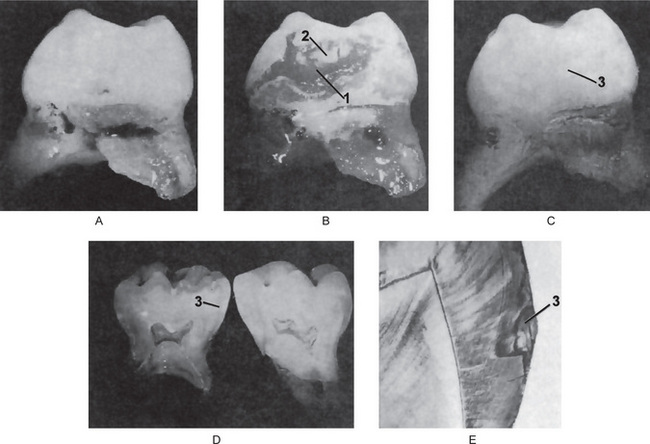
Figure 9-11 Smooth surface caries
The bacterial plaque is difficult to see (A) unless stained by a disclosing solution (B). The plaque (1) is disclosed by aqueous basic fuchsin. Note the absence of the plaque at the contact point (2). (C) The plaque is mechanically removed, revealing the chalky white spot of early enamel caries (3). (D) The tooth is split to show the extent of the carious lesion (3). (E) Photomicrograph of a ground section through the carious lesion (3).
As the caries penetrates the enamel, the enamel surrounding the lesion assumes a bluish-white appearance similar to that seen sometimes around carious pits or fissures. This is particularly apparent as lateral spread of caries occurs at the dentinoenamel junction. The more rapid type of caries usually produces a small area of penetration; the slower forms an open and shallow cavity. It is not uncommon for proximal caries to extend both buccally and lingually, but seldom does the cavity encroach upon areas accessible to excursion of food or to the toothbrush.
Linear Enamel Caries
An atypical form of dental caries that has been observed in the primary dentition of children in Latin American and Asian countries. The lesions predominate on the labial surface of the anterior maxillary teeth in the region of the neonatal line, which results from metabolic disturbances such as hypocalcemia or trauma at birth. A variant of the linear enamel form of caries in the primary teeth of children in the far East has been named odontoclasia. The morphological aspects of this type of caries are atypical and results in gross destruction of the labial surfaces of incisor teeth.
Cervical Caries
This type of caries occurs on buccal, lingual or labial surfaces and usually extends from the area opposite the gingival crest occlusally to the convexity of the tooth surface marking the self-cleansing portion of this surface. It extends laterally towards the proximal surfaces, and on occassion, extends beneath the free margin of the gingiva (Fig. 9-10B). Thus, the typical cervical carious lesion is a crescent-shaped cavity beginning, as a slightly roughened chalky area which gradually becomes excavated. Cervical caries is almost always an open cavity and does not present the narrow point of penetration seen commonly in pit or fissure caries and proximal caries. Cervical caries occurs on any tooth without predilection and is directly related to lack of oral hygiene. Of all forms of dental caries on different areas of the tooth, there is least excuse for cervical caries, since it can be prevented in nearly every instance by proper oral hygiene practice.
Root Caries
Root caries is defined by Hazen and his colleagues as “a soft, progressive lesion that is found anywhere on the root surface that has lost connective tissue attachment and is exposed to the oral environment”. This type of caries is predominantly found in dentitions of the older age groups with significant gingival recession and exposed root surfaces (Fig. 9-10C). At one time, it was also referred to as ‘caries of cementum’. Root caries initiates on mineralized cementum and dentin surfaces which have greater organic component than enamel tissue. Root surface caries in contemporary populations occurs most frequently on the buccal and lingual surfaces of roots.
There are few published studies on the prevalence of root caries. However, it is generally recognized that the longer lifespan of persons today, with the retention of teeth into the later decades of life, has increased the number of people in the population exhibiting gingival recession with clinical exposure of cemental surfaces and, thereby, probably increasing the prevalence of root caries. Enamel may become secondarily involved if it is undermined during the progression of the lesion. Dental plaque and microbial invasion are an essential part of the cause and progression of this lesion. However, there is some evidence that the microorganisms involved in root caries are different from those involved in coronal caries, being filamentous rather than coccal.
Microorganisms appear to invade the cementum either along Sharpey’s fibers or between bundles of fibers, in a manner comparable to invasion along dentinal tubules. Since cementum is formed in concentric layers and presents a lamellated appearance, the microorganisms tend to spread laterally between the various layers. Irregular mineralization on this cemental surface may often be seen at the same time, probably representing the beginning of calculus formation. After decalcification of the cementum, destruction of the remaining matrix occurs similar to the process in dentin, with ultimate softening and destruction of this tissue. As the caries process continues, there is invasion of microorganisms into underlying dentinal tubules, subsequent matrix destruction and finally pulpal involvement.
Most investigators have felt that once caries involves the dentin, the process is identical with coronal dentinal caries. However, it has been pointed out that since there are more dentinal tubules per unit area in the crown than in the root of the tooth, one may expect differences in the rate of caries progression and the amount of dentinal sclerosis present. The intraoral distribution patterns for root caries revealed that the teeth most frequently affected were the mandibular molars, the mandibular premolars, and the maxillary canines in descending order. The mandibular incisors were the least frequently affected teeth. It was also noted that the interproximal surfaces were affected most frequently in the maxillary arch, while the buccal surfaces were attacked most frequently in the mandibular arch.
The effect of fluoride on root caries was studied by Stamm and Banting, and the authors concluded that the lifelong consumption of fluoridated water is capable of significantly reducing the prevalence of root surface caries, which may itself be a growing dental public health problem in the adult population.
Classification Based on Severity and Rate of Progression
Acute Dental Caries
Acute dental caries is that form of caries which runs a rapid clinical course and results in early pulp involvement by the carious process. It occurs most frequently in children and young adults, presumably because the dentinal tubules are open and show no sclerosis. The process is usually so rapid that there is little time for the deposition of reparative dentin.
The initial entrance of the carious lesion remains small, while the rapid spread of the process at the dentinoenamel junction and diffuse involvement of the dentin produce a large internal excavation. It has been suggested that saliva does not easily penetrate the small opening to the carious lesion so that, as acids are formed, there is little opportunity for buffering or neutralization. In acute caries the dentin is usually stained light yellow rather than the darker brown of chronic caries (Fig. 9-12). Pain is more apt to be a feature of acute caries than of chronic caries, but this is not an invariable finding.

Rampant Caries
A condition which is characterized by sudden, rapid and almost uncontrollable destruction of teeth, affecting surfaces of teeth that are relatively caries free. These include the proximal and cervical surfaces of the mandibular incisors which are normally relatively caries free. A caries increment of 10 or more new carious lesions over a period of about one year is characteristic of rampant caries. Rampant caries (Fig. 9-13) is most often observed in the primary dentition of young children and the permanent dentition of teenagers. Dietary factors affecting oral substrate and oral flora and physiological factors affecting saliva are often significant in the development of rampant caries.

Nursing Bottle Caries
Is also called nursing caries, baby bottle syndrome, and bottle mouth syndrome. This is an unfortunate form of rampant caries affecting the deciduous dentition. It has been variously attributed to prolonged use of:
Almost invariably, there is habitual use of one of the above after one year of age, usually as an aid for sleeping at night or at naptime.
The disease presents clinically as widespread carious destruction of deciduous teeth, most commonly the four maxillary incisors, followed by the first molars and then the cuspids if the habit is prolonged. It has been emphasized that it is the absence of caries in the mandibular incisors which distinguishes this disease from ordinary rampant caries (Fig. 9-14). The carious process in affected teeth may be so severe that only root stumps remain.

When milk or other forms of carbohydrate are cleared rapidly from the mouth, they are not highly cariogenic. However, if they pool in the mouth when the baby falls asleep, the repetitious act soon leads to severe caries. The mandibular incisors usually escape because they are covered and protected by the tongue. It is essential that parents be made aware of this condition.
Adolescent Caries
There are two chronological periods when acute, rapidly progressing caries is commonly observed. Acute exacerbations in caries rates are usually seen at 4–8 years of age and at 11–18 years of age. The acute caries attack in the latter period is usually characterized as adolescent caries. These are usually seen in teeth and surfaces that are relatively immune to caries, with a relatively small opening in enamel and with extensive undermining of enamel. Because of rapid progression of lesion there is little time for the formation of reparative dentin. It is important to detect cases of rampant caries in the adolescent at an early stage so that preventive procedures may be rigorously applied.
Chronic Dental Caries
Chronic dental caries is that form which progresses slowly and tends to involve the pulp much later than acute caries. It is most common in adults. The entrance to the lesion is almost invariably larger. Because of this there is not only less food retention, but also greater access of saliva. The slow progress of the lesion allows sufficient time for both sclerosis of the dentinal tubules and deposition of reparative dentin in response to adverse irritation. The carious dentin is often stained dark brown.
Although there is considerable surface destruction of tooth substance, the cavity is generally a shallow one with a minimum softening of dentin. There is little undermining of enamel and only moderate lateral spread of caries at the dentinoenamel junction. Pain is not a common feature of chronic caries because of the protection afforded to the pulp by secondary dentin.
Recurrent Caries
Recurrent caries is that type which occurs in the immediate vicinity of a restoration. It is usually due to inadequate extension of the original restoration, which favors retention of debris, or to poor adaptation of the filling material to the cavity, which produces a ‘leaky margin’. In either event, the renewed caries follows the same general pattern as primary caries. It has been thought that recurrent caries occurs beneath restorations where the carious dentin has not removed before inserting the filling.
Arrested Caries
Arrested caries has been described as caries which becomes static and does not show any tendency for further progression. The deciduous and permanent dentitions are both affected by this condition. It occurs almost exclusively in caries of occlusal surfaces and is characterized by a large open cavity in which there is lack of food retention and in which the superficially softened and decalcified dentin is gradually burnished until it takes on a brown stained, polished appearance and is hard. This has been referred to as ‘eburnation of dentin’ (Fig. 9-15). Sclerosis of dentinal tubules and secondary dentin formation commonly occur in cases of arrested caries.

Figure 9-15 Arrested caries
The dentin is dark brown, hard and shiny. The enamel is not appreciably undermined Courtesy of Dr Spencer Lilly, Meenakshi Ammal Dental College, Chennai.
Another form of arrested caries is that sometimes seen on the proximal surfaces of teeth in cases in which the adjacent approximating tooth has been extracted, revealing a brown stained area at or just below the contact point of the retained tooth. This represents very early caries which, in many cases, is arrested following the extraction because of the formation of a self-cleansing area.
Caries arrest following the topical application of stannous fluoride solution has been reported by Muhler in as high as 22–25% of tooth surfaces originally diagnosed as carious. When areas that had been considered incipient carious lesions, demineralized areas, etchings or frank carious lesions were treated with the stannous fluoride solution, teeth appeared to be apparently sound, but manifested certain typical acquired characteristics:
• The presence of brown pigmentation
• The change from a soft to a hard texture
• The change from a chalky whiteness to light brown
• No increase in the size of the lesion
• No further progress of the lesion as long as the pigmentation remained.
Muhler stated that smaller the size of the lesion at the time of the initial application of stannous fluoride, greater the chance of caries arrest.
Radiation Caries
The development of rampant caries in patients undergoing radiation therapy in the head and neck region is referred to as radiation caries. It differs from the other types of caries by involving the cusp tips, incisal edges and the cervical areas. Rate of progression is faster when compared to the former. It starts as a diffuse area of demineralization encircling the entire crown of the tooth at the cervical portion and proceeds further to result in amputation of the crown at the gingival margin.
It is widely accepted that xerostomia is one of the complications of radiation to the head and neck region due to the involvement of salivary glands by the radiation. Besides the reduced salivary secretion there is change in the properties of saliva, which include increased viscosity, low pH. Multiple doses of radiation also weaken the dentinoenamel junction.
Frank et al, 1965 and Baden, 1970 described three forms of dental defects following irradiation namely,
1. A characteristic caries like lesion usually completely encirclle the neck of the tooth. Amputations of the crowns may occur due to this type of lesion. Sometimes extension to labial, buccal, or lingual surfaces is also observed.
2. Brown to black discoloration of the crown. The occlusal surface of posterior teeth and incisal edges of anterior teeth wear away.
3. A spot depression which spreads from incisal or occlusal edges on the labial or buccal and lingual surfaces.
In time, the enamel is destroyed with partial disintegration of dentin leaving the crown reduced to an irregularly shaped discolored stump projecting over gingiva.
The effect of X-rays upon the cellular elements in human saliva in experiments on healthy male adults was studied by Watanabe and he showed an increased threshold of leukopedesis of mature leukocytes into saliva. The duration of this increased leukopedesis was dependent upon the amount of radiation.
Experiments of Selvaraj and Sbarra showed the role of the host in dental caries development. Lesser hydrogen peroxide production and impaired bactericidal activity was obtained in phagocytizing neutrophil leukocytes isolated from irradiated animals was noted by them. The association of irradiation caries with increased migration of neutrophil leukocytes into the oral cavity and increased excretion of lysosomal enzymes into the oral environment should be considered in dental caries development research as quoted by Janez John Gabrovsek.
Enamel Caries Remineralization
This process, also described under the terms ‘caries reversibility’ and ‘consolidation’ of the early enamel carious lesion, has received increased attention in recent years, chiefly due to recognition of its more common occurrence than formerly believed.
A natural biologia remineralizing process exists in the mouth which is responsible for the maintenance of tooth surfaces by precipitation of mineral salts from saliva. It is further suggested that the fluoride ion plays a role in stimulating the remineralization process by increasing the rate of deposition of calcium phosphate and enhancing the degree of remineralization achieved, and by becoming incorporated itself into the mineral, produces a remineralized enamel with a reduced acid solubility. Clinical evidence for the remineralization phenomenon occurring in vivo is well documented. It is also well established that this can only take place if cavitation has not occurred.
Caries Susceptibility of Jaw Quadrants, Individual Teeth and Tooth Surfaces
Caries Susceptibility of Jaw Quadrants
This has been shown by numerous investigators to exhibit a bilateral distribution between the right and left quadrants of both maxillary and mandibular arches. Although unilateral caries is found in some persons, it occurs with random distribution. In a relatively large sample of the population, the right and left sides of the mouth are involved with equal frequency. This horizontal relation is closer than either a vertical or a diagonal one. It was reported by Scott in 1944, for example, that bilateral caries was found in over 95% of a group of 300 persons whose dental radiographs were studied.
There is general acceptance of the numerous reports that the maxillary arch is more frequently involved by caries than the mandibular arch. This appears to hold true despite the extremely high incidence of carious mandibular first molars, since this is compensated for by the general immunity of mandibular anterior teeth. The reason for this difference between the arches in caries susceptibility is not well documented. It may relate to gravity and the fact that saliva with its buffering action would tend to drain from the upper teeth and collect around the lower. It is of interest that in the laboratory rat, mandibular caries far surpasses maxillary caries.
Caries Susceptibility of Individual Teeth
This has been studied by numerous investigators, and it has been found that, there is a definite order of caries attack for the different teeth of both the deciduous and the permanent dentitions.
Klein and Palmer in 1941 studied the problem of individual tooth susceptibility, pointing out that the teeth farthest back in the mouth are most frequently carious and that these are the teeth with the pits, fissures and broadest contact points.
The posteruptive tooth age is also an important factor, but probably minor compared to other factors such as tooth morphology, structure and position in the mouth as concluded by Healey and Cheyne.