Histopathology of Dental Caries
The study of morphological and biochemical events of dental caries is challenging because of technical problems involved in the preparation of hard tissue for examination. The morphological changes associated with caries have been studied extensively. The principal manner in which caries of the enamel has been studied is through the use of ground sections of teeth that are usually between 60 μm and 100 μm in thickness. Since the carious process is one involving demineralization, the decalcification usually results in complete loss of enamel unless special methods are used. This has materially impeded the investigation of dental caries at the microscopic level. Microradiography of carious lesions offers the distinct advantage in that the photodensity of the image on the film is directly related to the amount of mineral. Microdensitometric tracings of this image permit quantitative measurement of the degree of demineralization. The application of transmission and scanning electron microscopy to the study of dental caries has added greatly to our understanding of this disease, as has utilization of other techniques, including histochemical studies, and the use of radioactive isotopes.
For ease of understanding, the histopathology of dental caries will be considered under the general headings of caries of enamel, of dentin, and of cementum.
Caries of the Enamel
Most of the histological description of enamel caries is in relation to early lesions. The carious process varies slightly depending on the occurrence of the lesion either on smooth surfaces or in pits and fissures. Accordingly, the caries of enamel is discussed under these headings.
Smooth Surface Caries
The earliest macroscopic evidence of incipient caries on the smooth surface is the appearance of an area of decalcification beneath the dental plaque, which resembles a smooth chalky white area (Figs. 9-11, 9-16). It is best observed on an extracted tooth, usually at the cervical margin of the interdental facet referred to as white spot. The enamel surface overlying the white spot is hard and shiny and cannot be distinguished from the surface of adjacent sound enamel using a sharp explorer point. Intact surface lesions may also appear brownish when they are described as brown spots. This largely depends on the degree of exogenous material adsorbed by the porous region.
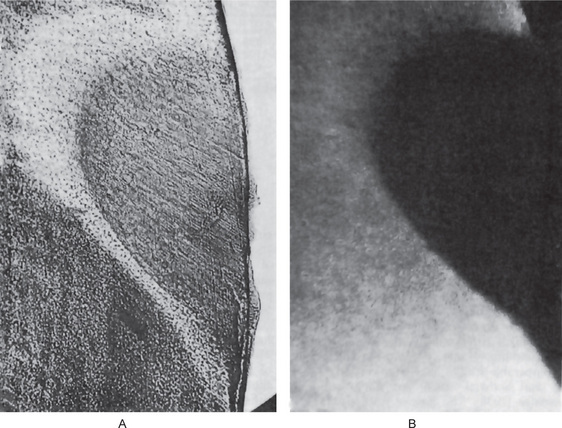
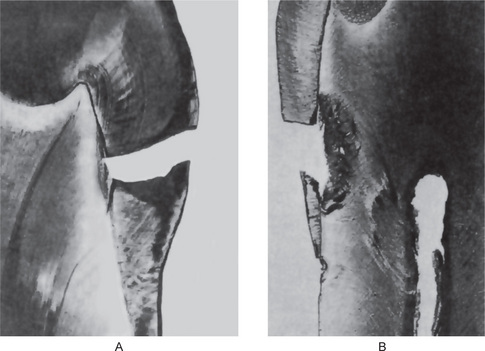
Figure 9-16 Early enamel caries
A photomicrograph through a chalky area of enamel (A) shows a demonstrable change without actual cavitation. The Grenz-ray picture (B) shows loss of mineral in this area Courtesy of Dr Edmund Applebaum.
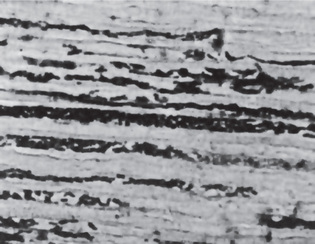
Study of early lesions by the transmission electron microscope, particularly by Scott and his associates, has revealed that the first change is usually a loss of the interprismatic or interrod substance of the enamel with increased prominence of the rods. In some instances, the initial change seems to consist of roughening of the ends of the enamel rods, suggesting that the prism may be more susceptible to early attack (Fig. 9-17). Another change in early enamel caries is the accentuation of the incremental lines of Retzius (Fig. 9-18). This conspicuous appearance of the calcification lines is an optical phenomenon due to loss of minerals, which causes the organic structures to appear more prominent. There may also be accentuation of perikymata which are the external manifestation of striae of Retzius.
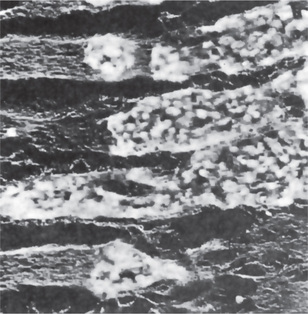
Figure 9-17 Early enamel caries
Electron photomicrograph of demineralized enamel showing microorganisms apparently localized within prisms in early stage of caries. The specimen was cut from a tooth slice and demineralized for 18 hours in 5% trichloroacetic acid. Original magnification: X 7500 Courtesy of Dr David B Scott; From DB Scott and JT Albright: Oral Surg, 7: 64, 1954.
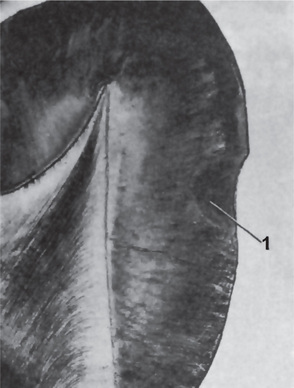
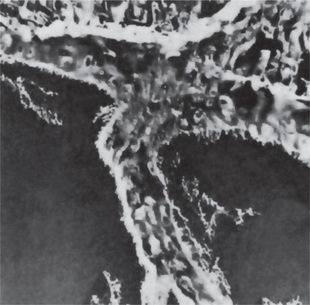
Figure 9-18 Early enamel caries
Accentuation of striae of Retzius (1) as it crosses the carious lesion is illustrated.
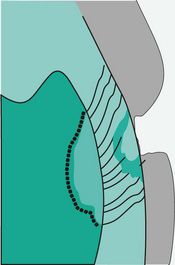
As this process advances and involves deeper layers of enamel, it will be noted that smooth surface caries, particularly of proximal surface has a distinctive shape. It forms a triangular or cone-shaped lesion with the apex toward the junction and the base toward the surface of tooth (Fig. 9-19). There is an eventual loss of continuity of the enamel surface, and the surface feels rough to the point of an explorer (Fig. 9-20).

Figure 9-19 Advanced enamel caries with early invol ve ment of dentin
The typical pyramidal shape of the proximal enamel lesion is apparent.
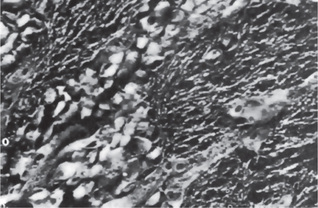
Figure 9-20 Advanced enamel caries
Electron photomicrograph of demineralized enamel showing the presence of matrix fibrils in advanced stage of caries. A tooth slice was demineralized for 11 days in 5% formic acid, and the specimen was cut from the demineralized enamel. Original magnification: X 10,000 Courtesy of Dr David B Scott; from DB Scott and JT Albright: Oral Surg, 7: 64, 1954.
Pit and Fissure Caries
The carious process in pits and fissures does not differ in nature from smooth surface caries except for its anatomical and histological variations. The occlusal fissures are deep invaginations of enamel that have been described as broad or narrow funnels, constricted hour glasses, multiple invaginations with inverted Y-shaped divisions and irregularly shaped (Fig. 9-21). The carious lesion starts along the fissure walls rather than at the base and visual changes such as chalkiness or yellow, brown or black discoloration may be seen. If the enamel in the bottom of the pit or fissure is thin, early dentin involvement frequently occurs. When caries occurs in a pit and fissure, it follows the direction of the enamel rods and characteristically forms a triangular or cone-shaped lesion with its apex at the outer surface and base toward the dentinoenamel junction (Fig. 9-22). It should be noted that the general shape of the lesion here is just the opposite of that occurring on smooth surface. Because of this, greater number of dentinal tubules are involved when the lesion reaches the dentinoenamel junction. Pit and fissure caries, usually produce greater cavitations than smooth surface caries.
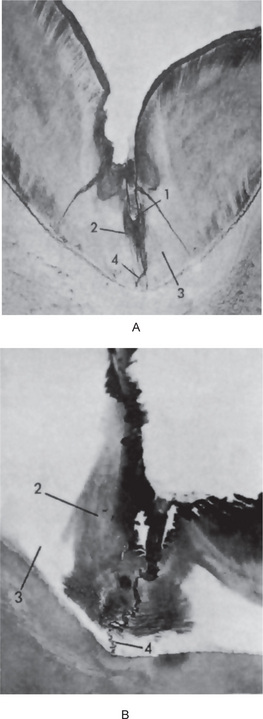
Figure 9-21 Fissure caries of enamel
Ground section of tooth (A) shows the bacterial plaque (1), carious enamel (2) and noncarious enamel (3). The decalcified section (B) illustrates that the carious enamel (2) is not lost during preparation of the section as is noncarious enamel (3). Enamel lamella is shown at (4).

Figure 9-22 Fissure caries of enamel
The lesion is pyramidal in shape and generally follows the direction of the enamel rods. Note the depth of the actual fissure (1).
The carious lesion is more prone to be stained with a brown pigment in pits and fissures. In newly erupted teeth, a brown stain is indicative of underlying decay, while in teeth of older individuals it may be due to arrested lesions. Occasionally, enamel lamellae are found at the base of pits and fissures and their role in caries initiation has been dealt with (Fig. 9-23). Histochemical staining of early lesions of enamel has shown them to be more permeable to methyl green and to contain free calcium ions detected with Alizarin red. Normal enamel remains uncolored by these dyes. Some lesions also react with PAS reagent in demineralized zones probably due to ingress of exogenous organic material rather than the release of endogenous mucoprotein in the enamel (Sullivan, 1954).
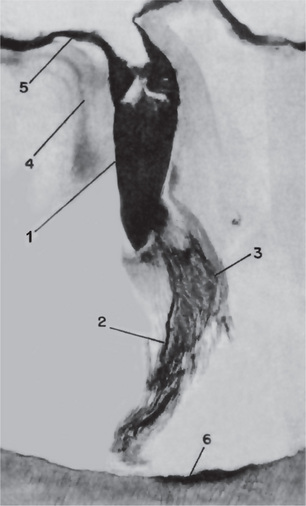
Figure 9-23 Fissure caries
Decalcified section of a tooth demonstrating a bacterial plaque (1), enamel lamella (2), carious enamel (3), accentuated striae of Retzius (4), enamel cuticle (5) and early caries of dentin (6). Courtesy of Dr Edmund Applebaum.
The histological features of the initial carious lesion in enamel have been described by a number of workers. Evidences support the concept that in early stages caries causes minimal damage to the outer smooth surface but considerable demineralization below the surface. The initial lesion has been divided into different zones based upon its histological appearance when longitudinal ground sections are examined with the light microscope. Four zones are clearly distinguishable, starting from the inner advancing front of the lesion. These are the: (1) translucent zone (2) dark zone (3) body of the lesion and (4) surface layer.
Zone 1. The translucent zone
This lies at the advancing front of the enamel lesion and is the first recognizable zone of alteration from normal enamel. It is not always present as only about half of the lesions demonstrate a translucent zone at their advancing front. It is observable when a longitudinal ground section is examined in a clearing agent having a refractive index identical to that of enamel. Quinoline is suitable since its refractive index is identical to that of the enamel (RI 1.62). When ground section is examined in transmitted light after imbibition with quinoline, the translucent zone appears structureless. The spaces or pores created in the tissue at this stage of enamel caries are located at prism boundaries and other junctional sites. Therefore, when the pores are filled with a medium having the same refractive index as enamel, normal structural markings are no longer visible. By means of polarized light it has been shown that this zone is slightly more porous than sound enamel, having a pore volume of 1% compared with 0.1% in sound enamel. The fluoride content of translucent zone enamel has shown to be increased relative to adjacent sound enamel beside preferential removal of magnesium and carbonate rich mineral without any evidence of protein loss.
Zone 2. The dark zone
This lies adjacent and superficial to the translucent zone. It has been referred to as the ‘positive zone’, because it is usually present. This zone is formed as a result of demineralization and appears dark brown in ground sections examined by transmitted light after imbibition with quinoline. Polarized light studies show that the dark zone has a pore volume of 2–4%. When examined with the polarizing microscope after imbibition with quinoline, the dark zone shows positive birefringence in contrast to the negative birefringence of sound enamel. These effects have been shown to be due to the presence of very small pores in the zone besides the relative large pores that are present in the first stage, the translucent zone (Fig 9-24). Therefore, when a ground section is examined in a mounting medium such as quinoline, the relatively large molecules of the medium are unable to penetrate the micro pore system of the dark zone. Since the micro pores remain filled with air or vapor, light is scattered on passing through the zone, causing brown discoloration of the dark zone. In a similar manner, the presence of a medium or low refractive index within the micro pore system is responsible for the reversal of birefringence when examined in polarized light. If a ground section is examined in an aqueous medium having a small molecule which penetrates the micro pores, the dark zone is no longer seen. The above work led to the conclusion that the formation of a micro pore system must be regarded as a result of demineralization. The increased level of demineralization in the dark zone of carious lesion has been confirmed with microradiography as the region of visible radiolucency often extends into it. It has been reported by some that the appearance of the dark zone was due to remineralization occurring at the advancing front of the lesion.
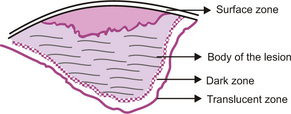
Zone 3. The body of lesion
This zone lies between the relatively unaffected surface layer and the dark zone. It is the area of greatest demineralization. In polarized light, the zone shows a pore volume of 5% in spaces near the periphery, to 25% in the center of the intact lesion. When a longitudinal ground section is examined in quinoline with transmitted light, the body of the lesion appears relatively translucent compared with sound enamel. However, the striae of Retzius within this region are well marked and therefore appear enhanced in contrast to the translucency of the area. When the section is examined with polarized light after imbibition with water, the body of the lesion shows as a region of positive birefringence in contrast to sound enamel. Microradiographs confirm the reduced mineral content of this zone and a reduction of 24% mineral per unit volume is noted compared with sound enamel and also a corresponding increase in unbound water and organic content due to the ingress of bacteria and saliva.
Zone 4. The surface zone
When examining an initial carious lesion with the polarizing microscope, the surface zone is an important feature. The quantitative studies of the surface zone indicate a partial demineralization of about 1–4% along with a pore volume of less than 5% of spaces. After imbibing with a medium like water, although the porous subsurface zone is seen to be positively birefringent, the surface zone retains a negative birefringence. This relatively unaffected surface zone is also identifiable on microradiographs as it is sharply demarcated from the underlying radiolucent regions of the lesion. Thus, the surface zone, when examined by the polarizing microscope has been defined as the zone of negative birefringence, superficial to the positively birefringent body of the lesion seen when the section is examined in water. It is important to realize that all the four histological zones of the initial enamel lesion cannot be seen when examined in a single medium.
The surface zone remains intact and also well mineralized because it is a site where calcium and phosphate ions, released by subsurface dissolution, become re-precipitated. This process is referred to as remineralization. The high fluoride concentration of enamel surface would favor remineralization. The surface zone is thus maintained at a relatively low level of demineralization through lesion formation and progression. Eventually, the surface zone is demineralized, usually at the stage when the lesion has penetrated some way into the dentin.
Scott and Wyckoff reported that there is no direct relation between the occurrence of enamel lamellae and smooth surface caries on the basis of electron microscopic studies. They have pointed out that in those cases in which lamellae appear to be associated with caries, the association is only by chance (Fig. 9-25).
Ultrastructural Changes in Enamel Caries
Ultrastructural techniques in caries research have proved to be demanding because of difficulties involved in the preparation of ultra thin sections from enamel. The first alteration found in enamel is the scattered destruction of individual apatite crystals, both within the enamel prisms and at their boundaries. Studies attempting to describe features of carious enamel by transmission electron microscope reveal that progressive dissolution of crystals results in broadening of the intercrystalline spaces when seen in transverse sections. However, obvious spacing and damage to crystals were not detectable unless the sections came from areas having a pore volume of 10–25 %, which was identifiable only in the body of the enamel carious lesion. High resolution electron microscope shows that carious dissolution starts in the center of one end of the crystal and develops anisotropically along the lattice C-axis. Since dislocations or linear lattice defects are evident in biological or synthetic apatite, dissolution extends across accounting for greater demineralization. As the number of dissolved crystals increases, the densely calcified tissue becomes progressively more porous. In addition to crystal damage in the carious process, a different crystal form has been found at prism border in carious enamel.
These crystals at the prism boundary are larger, isodiametric and electron dense than elsewhere, their average size being greater than the crystals in sound enamel. These larger crystals are thought to be the result of remineralization of crystals that have resisted dissolution. Eventually, with diffuse destruction of the apatite crystals, numerous bacteria can be observed invading the enamel lesion.
Caries of the Dentin
Caries in enamel is clearly a dynamic process, but this tissue is devoid of cells and is therefore incapable of reacting in a vital manner; whereas dentin, being a part of the dentin pulp complex is able to mount a reparative response. Caries of the dentin begins with the natural spread of the disease process along the dentinoenamel junction and the rapid involvement of great numbers of dentinal tubules, each of which acts as a potential pathway leading to the dental pulp along which the microorganisms may travel at a variable rate of speed, depending upon a number of factors (Fig. 9-26). In some instances, carious invasion appears to occur through an enamel lamella so that little, if any, visible alteration in the enamel occurs. Thus, when lateral spread at the dentinoenamel junction takes place with the involvement of underlying dentin, a cavity of considerable size may form with only slight clinically evident changes in the overlying enamel.
Early Dentinal Changes
The initial penetration of the dentin by caries may result in alterations in the dentin previously described as dentinal sclerosis. This dentinal sclerosis is a reaction of vital dentinal tubules and a vital pulp in which there is calcification of the dentinal tubules that tends to seal them off against further penetration by microorganisms. The formation of sclerotic dentin is minimal in rapidly advancing caries and is most prominent in slow chronic caries. By reflected light the sclerotic dentin appears dark.
All the four zones of enamel caries cannot be seen with same immersion medium.
The appearance of fatty degeneration of odontoblast process, with the deposition of fat globules, precedes even the early sclerotic dentinal changes. The use of the term ‘fatty degeneration’ has been questioned since it is not a degenerative process. Two types of lipid staining have been seen, one of which is more superficial and probably of bacterial origin. The other type may be due to unmasking of lipids present in the intratubular dentin by demineralization. This can be demonstrated only by the application to fresh dentin of special stains such as Sudan red, which selectively stains fat. The significance of this phenomenon is not known, although it has been suggested that fat contributes to the impermeability of the dentinal tubules. Fatty degeneration may be a predisposing factor favoring sclerosis of the tubules.
Except in unusual cases of arrested caries, continued destruction of dentin inevitably occurs despite attempts at walling off one part of the tooth. The rate at which the carious destruction progresses, tends to be slower in older adults than in young because of the generalized dentinal sclerosis that occurs as a part of the aging process. Close examination of the dentin behind a zone of sclerosis formed in response to caries will reveal decalcification of the dentin, which appears to occur slightly in advance of the bacterial invasion of the tubules. In the earliest stages of caries, when only a few tubules are involved, microorganisms may be found penetrating these tubules before there is any clinical evidence of the carious process (Figs. 9-27, 9-28). These have been termed pioneer bacteria.
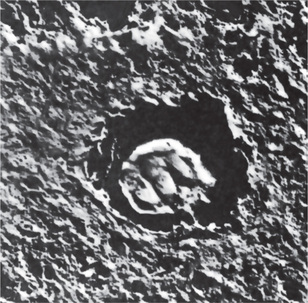
Figure 9-27 Caries of the dentin
Electron photomicrograph of demineralized carious dentin showing bacteria in a dentinal fiber. Specimen cut from tooth slice and demineralized 3 days in 5% trichloroacetic acid. Original magnification: X 16,500 Courtesy of Dr David B Scott; from DB Scott and JT Albright: Oral Surg, 7: 64, 1954.
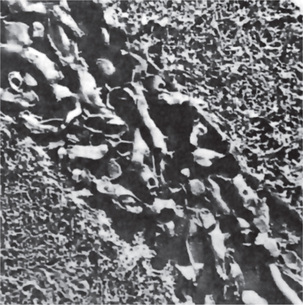
Figure 9-28 Caries of the dentin
Electron photomicrograph of demineralized carious dentin showing bacteria in a dentinal tubule. Specimen cut from tooth slice and demineralized 3 days in 10% acid. Original magnification: X 10,000 Courtesy of Dr David B Scott; from DB Scott and JT Albright: Oral Surg, 7: 64, 1954.
The initial decalcification of dentin involves the walls of the tubules, allowing them to distend slightly as they become packed with masses of microorganisms (Fig. 9-29). Study of individual tubules will usually show almost pure forms of bacteria in each one. Thus one tubule may be filled with coccal forms, while the adjacent tubules may contain only bacilli or thread forms (Fig. 9-30).
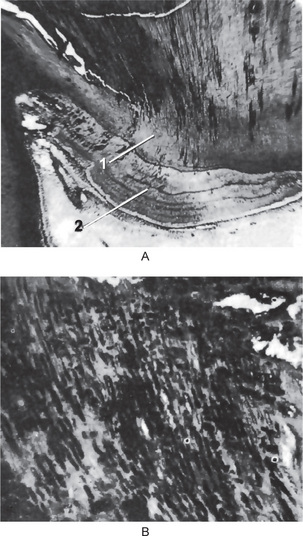
Figure 9-29 Caries of dentin
The low-power photomicrograph (A) shows involvement of both primary (1) and secondary dentin (2) by the carious process. In the high-power photomicrograph (B) the dentinal tubules are seen packed with microorganisms.
It is evident that the microorganisms, as they penetrate farther and farther into the dentin, become more and more separated from the carbohydrate substrate upon which the bacteria depend. The high protein content of dentin would favor the growth of those microorganisms which have the ability to utilize this protein in their metabolism. Thus, proteolytic organisms would appear to predominate in deeper caries of the dentin, while acidogenic forms are more prominent in early caries.
The observation that the morphological type of the bacteria in deep carious dentin is different from that of the bacteria in initial caries substantiates the hypothesis that initiation and progression of dental caries are two distinct processes and must be differentiated. The evidence indicates that the organisms responsible for the initiation of caries are subsequently replaced by others as the environmental conditions occasioned by the advancing carious lesion are altered. Nevertheless, many microorganisms do have both acidogenic and proteolytic properties.
Advanced Dentinal Changes
The decalcification of the walls of individual tubules leads to their confluence, although the general structure of the organic matrix is maintained for some time.
A thickening and swelling of the sheath of Neumann may sometimes be noted at irregular intervals along the course of involved dentinal tubules, in addition to an increase in the diameter of dentinal tubules due to the packing of tubules by microorganisms (Fig. 9-31). Tiny ‘liquefaction foci’, described by Miller, are formed by focal coalescence and breakdown of a few dentinal tubules (Fig. 9-32). This ‘focus’ is an ovoid area of destruction, parallel to the course of the tubules and filled with necrotic debris which tends to increase in size by expansion. This produces compression and distortion of adjacent dentinal tubules so that their course is bent around the ‘liquefaction focus’. In areas of interglobular dentin, decalcification and confluence of tubules occur rapidly. The presence of considerable amounts of interglobular dentin accounts for the rapid spread of caries in so-called malacotic or soft teeth.
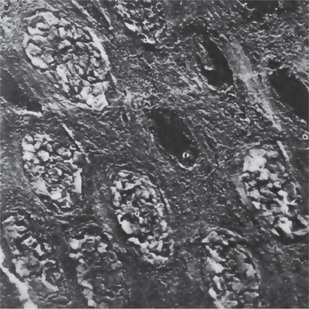
Figure 9-31 Caries of dentin
Electron photomicrograph of demineralized carious dentin shows packing by bacteria of dentinal tubules cut in cross-section. Original magnification: X 10,000 Courtesy of Dr David B Scott.

Figure 9-32 Caries of dentin
The tubules contain microorganisms. There are liquefaction necrosis (1) and clefts (2) in the carious dentin (periodic acid-Schiff stain).
It has been pointed out that acidogenic organisms are apparently responsible for the initial decalcification of dentin occurring in the caries process, but that another mechanism must be necessary for the ultimate destruction of the remaining organic matrix. The most logical explanation is that this matrix is destroyed by the action of proteolytic enzymes produced by microorganisms deep in the cavity. This enzymatic digestion is of maximal activity only when the organic matrix is decalcified; there is little effect on the intact dentin.
Early dentinal caries
Fatty degeneration of odontoblast process

• Reaction of vital pulp—calcification of dentinal tubules (DT)
• Seals off DT from further penetration of microorganisms
• Minimal in rapidly advancing caries
• Sclerotic dentin—appear white in transmitted light Decalcification of dentinal tubules
• Above dentinal sclerosis → zone of decalcification
• Occurs in advance of bacterial invasion of DT
The destruction of dentin through a process of decalcification followed by proteolysis occurs at numerous focal areas, which eventually coalesce to form a necrotic mass of dentin of leathery consistency. Clefts are rather common in this softened dentin, although they are rare in chronic caries, since the formation of a great deal of softened necrotic dentin is unusual. These clefts extend at right angles to the dentinal tubules and appear to be due to extension of the carious process along the lateral branches of the tubules or along the matrix fibers which run in this direction (Fig. 9-33). These clefts parallel the incremental lines of the dentin, which are due to alternating resting periods during the calcification of the dentin. The clefts account for the manner in which carious dentin can often be excavated by peeling away thin layers with hand instruments.
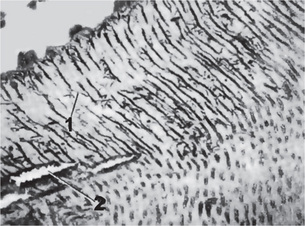
Figure 9-33 Caries of dentin
Lateral branches of the dentinal tubules (1) are filled with microorganisms. Note the typical transverse clefts (2).
As the carious lesion progresses, various zones of carious dentin may be distinguished which grossly tend to assume the shape of a triangle with the apex toward the pulp and the base toward the enamel. Beginning pulpally at the advancing edge of the lesion adjacent to the normal dentin, these zones are as follows:
Secondary Dentin Involvement
The carious involvement of secondary dentin does not differ remarkably from the involvement of primary dentin, except that it is usually somewhat slower because the dentinal tubules are fewer in number and more irregular in their course, thus delaying the penetration of the invading microorganisms. Sooner or later; however, the involvement of pulp results with ensuing inflammation and necrosis. Occasionally, caries will spread laterally at the junction of the primary and secondary dentin and produce a separation of the two layers.
Diagnosis of Dental Caries
Radiographic Diagnosis
The radiograph is a necessary adjunct to a complete oral examination by the dentist. Although many carious lesions are accessible and visible for easy diagnosis, there is a great percentage of lesions, chiefly interproximal in location, which are not found by the routine examination with mouth mirror and explorer. It has been pointed out previously that the use of radiograph may reveal 50% more cavities than may be found by visual examination alone.
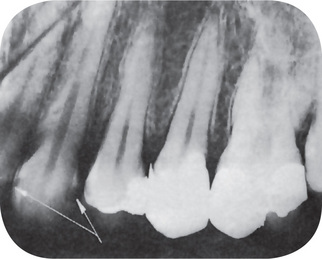
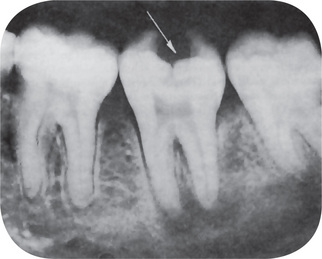
The interproximal carious lesion is most easily recognized on the radiograph and appears in early lesions as a small, triangular radiolucent area of enamel, and later of the dentin, occurring approximately at the contact point (Fig. 9-34). Though radiograph is of little value in the diagnosis of occlusal cavities, because of the irregularity of the surface and the superimposition of cusps, it plays a significant role in assessing the proximity to the pulp chamber (Fig. 9-35). The radiograph is similarly unsuited for use in the detection of small cavities in buccal or lingual pits or at the cervical margin.
Alternative methods for early detection of dental caries have been emphasized to understand the nature of the carious process. Among the newer technologies that are being explored, a few of interest are discussed in brief.
Infrared Laser Fluorescence
Infrared laser fluorescence instrument was developed for the detection and quantification of dental caries of occlusal and smooth surfaces. It uses a laser light source and a fiberoptic cable that transmits the light to a handheld probe with a fiberoptic eye at the tip. The light is absorbed and induces infrared fluorescence which is collected at the probe tip and transmitted through ascending fibers, and processed and presented on a display window as an integer between 0 and 99. Increased fluorescence reflects carious tooth substance particularly for numerical value higher than about 20. The material responsible for fluorescence is under investigation but appears to be bacterial metabolites, particularly porphyrins.
Digital Imaging Fiberoptic Transillumination
Conventional clinical caries examination routinely use transillumination to identify lesions located on interproximal surfaces of anterior teeth. Recently, fiberoptic transillumination has become available for clinical use. It provides an intense light beam that is transmitted through a fiberoptic cable to a specially designed probe to permit the use of transillumination on the proximal surfaces of posterior teeth.
Digital imaging fiberoptic transillumination is a further advancement of this technology in which the visually observed images are captured using a digital charged coupled device camera and sent to a computer for analysis, using dedicated algorithm.
Quantitative Light Fluorescence
Quantitative light fluorescence (QLF) is a dental diagnostic tool for quantitative assessment of dental caries lesions, dental plaque, bacterial activity, calculus, staining, and tooth whitening. QLF uses the principle of fluorescence to detect dental caries. With QLF, real-time fluorescent images are captured into the computer and stored in an image database. Optional quantitative analysis tools enable the user to quantify parameters like mineral loss, lesion depth, lesion size, stain size and severity with high precision and repeatability. The QLF method is based on the autofluorescence of teeth. When teeth are illuminated with high intensity blue light, they will start to emit light in the green part of the spectrum. The contrast between demineralized enamel and sound enamel increases almost by a factor of 10. The digital image processing system calculates the size and severity of the lesion.
Methods of Caries Control
The control of dental caries presents one of the greatest challenges that must be dealt with by the dental professionals. It is not sufficient that we try to perfect techniques to repair damage to the dental apparatus once it has occurred. It has been a general failing of the healing profession that the treatment of disease has been overemphasized and prevention minimized. Research in dentistry for a better understanding of the carious process has not been lacking and there have been definite accomplishments in the field of caries control. Methods are at hand for producing a substantial reduction in dental caries experience, provided that the patient are properly educated. The most promising methods of caries control will be discussed in this section, along with the experimental evidence upon which their use has been predicted. These suggested methods of control may be classified into three general types:
Chemical Measures of Caries Control
A vast number of chemical substances have been proposed to control dental caries. The use of some of these have been both emperial and based on experimental evidence. These include substances which:
• Alter the tooth surface or tooth structure
• Interfere with carbohydrate degradation through enzymatic alterations
In the light of our present knowledge, each of these may theoretically be of benefit in controlling caries. The final proof, however, depends on thorough clinical trials.
Substances which Alter the Tooth Surface or Tooth Structure
Of the chemical substances falling within this category, fluorine appears to be the most promising and hence has been most widely tested. The exposure of the teeth to fluoride through professional application of fluoride solutions, gels, foams and varnishes plus exposure from dentifrices and other fluoride preparations used at home is beneficial in preventing dental caries.
Fluorine
The association of fluorine and dental caries dates back to GV Black and Frederick S McKay, who recognized that the teeth with severe degree of mottling have greater immunity to dental caries than normal teeth. Fluorine as a member of halogen family, because of its electronegative properties makes it extremely reactive. In mineralized tissues such as bones and teeth, it occurs as the apatite salt of fluoridated hydroxyapatite. Fluorine has been administered principally in two ways: through the communal water supply and by topical application.
Fluoridation of Water Supplies
The studies of Dean and other members of the United States Public Health Service were instrumental in establishing an inverse relation between the fluorine content of the communal water supply and the dental caries experience. These studies have been carried out in numerous cities throughout the United States and have generally indicated that persons residing for their entire lives in an area where significant amount of fluorine are naturally present in the drinking water exhibited less caries than persons born and raised in fluoride-free areas. If persons are born in a fluoride area, but are removed from exposure to fluoride containing water at variable times after birth, their caries experience increases proportionately.
Many clinical studies have reported that a reduction in the caries experience is not necessarily dependent upon the presence of mottled enamel. Hodge and Smith clearly showed the relation between the fluoride content of water, the index of dental fluorosis and the DMF rate based upon public health data. This data demonstrates the optimum ppm levels of fluoride in drinking water which may produce maximal amount of protection against caries with minimal hazard of fluorosis. These workers have pointed out that a two-fold factor of safety exists between the protective level of 1 ppm of fluoride and the level necessary to produce significant clinical fluorosis.
However, the optimal concentration depends on the annual average maximum daily air temperature in the community (temperature influences the amount of water ingested). In temperate zones of North America, where the annual average maximum daily air temperature ranges between 14.7°C and 17.7°C, the optimal level of fluoride is 1 ppm.
In Africa and Asia, the optimal level is not known and may differ, requiring increased water consumption. The natural occurrence of fluoride in the drinking water and the attendant reduced caries incidence suggested that the artificial addition of fluoride to the communal water supply might result in a similar reduction in caries. In addition, it has been indicated that the fluoride content of caries free teeth is higher than carious teeth.
One of the first experimental clinical studies of artificial fluoridation was that carried out in two cities in New York, Kingston and Newburgh. The water supply of Kingston was low in fluoride (less than 0.15 ppm); so Kingston served as the control city. Sufficient fluoride was added to the water of Newburgh to raise the level to 1.0–1.2 ppm. The results of caries examinations completed eight to nine years after the initiation of fluoridation in Newburgh were reported by Ast and his coworkers, which indicated that the DMF rate among Newburgh children was 60% lower than that among Kingston children. The DMF rate of the first permanent molars in the Newburgh children was only about 50% of that among Kingston children. There was not a single missing first permanent molar in Newburgh children even though approximately 7% of the first permanent molars were missing in the 9- and 10- year-old children residing in Kingston. Newburgh children in the 6- to 9-year-old age range exhibited over three times as many caries free deciduous teeth as the Kingston group.
Since central water supplies are not available to large segments of the world’s population, considerable research related to the effect of school water fluoridation on dental caries has been conducted using even higher concentrations of fluoride. Currently recommended level for school water fluoridation is 4–5 times the optimum amount recommended for community water fluoridation in the same geographic area. In Asia, the only Malaysian state that fluoridated its water supplies was Johore. A vast reduction in the caries experience was noted following this. In Singapore, fluoridation of the water supply began in 1956 and by 1970, two million people were receiving fluoridated water.
Good reviews on the subject of fluoridation and caries prevention have been published by Ericsson (1977) and Fejerskov and coworkers in 1981. Careful studies of chronic toxicity by many workers have failed to reveal the slightest detrimental effect caused by fluoridation of the water supply. Opponents of water fluoridation have questioned its safety, yet careful comparison of communities with optimal versus those with suboptimal levels of fluoride in the water supplies reveals no significant differences in the frequency of birth defects or mortality statistics. Blood cell counts, hemoglobin level and urine analyses have always been within normal limits, and there has been no evidence of alterations in development of bones. It must be concluded that fluoridation of water is not only an absolutely safe procedure, but also a highly beneficial one because of its caries protective action.
Mechanism of Action of Ingested Fluoride
The mechanism of action of fluoride in the drinking water has been discussed by many workers, and several theories have been proposed. Since fluoride inhibits enzymes by inactivating the coenzyme portion of the enolase system, and specifically by inhibiting the conversion of 2-phosphoglyceric acid to (enol) phosphopyruvic acid, it has been thought to protect against caries by preventing carbohydrate degradation. But the level of fluoride taken in is so low, the dilution factor by saliva is so great and the oral clearance is so rapid that this mechanism is generally dismissed as insignificant.
The L. acidophilus counts of the saliva of patients in cities with varying amounts of fluoride in the drinking water received considerable attention by the United States Public Health Service workers in earlier studies. The scientific consensus based upon these studies is that the L. acidophilus counts are more closely associated with caries activity than with the fluoride content of the water supply. Thus, the mechanism of action of fluoride does not appear to be through inhibition of microorganisms.
The most widely accepted theory on the mechanism of action of ingested fluoride is that of alteration of the structure of the developing tooth through systemic absorption of the element. Such a mechanism would explain the clinical observation of greater caries protection of children residing in fluoride areas during tooth formation as compared to the caries experience of children moving into such an area after tooth crown formation has been completed. The exact means whereby fluoride would alter the tooth structure to resist caries has not been completely established, but it is probably through the incorporation of fluorine into the crystal lattice structure of enamel, with the formation of a fluorapatite producing less acid soluble enamel.
Fluoride Supplements
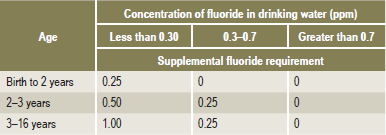
Where communal water fluoridation is not feasible, fluoride tablets, drops, or lozenges have been proven definitely to be effective cariostatic agents, provided such supplements are taken on a daily basis from birth to about 14 years. The cariostatic effects of fluoride supplements have ranged from less then 10% to more than 80%, depending on how soon after birth, supplementation starts, the degree of fulfilment and the dosage. The correct dosage in prescribing fluoride supplements depends on two factors: the age of the child and the existing fluoride concentration in the water supply (Table 9-5). Failure to determine the fluoride concentration in the water source can result in overdosage and consequent dental fluorosis. For young infants, drops are more convenient and can be added to foods such as cereals or beverages such as milk formula or juices. For older children, whose primary teeth have erupted, fluoride tablets or lozenges are indicated as these provide both systemic benefits when swallowed and topical benefits as they are swished around the mouth. The concentration of total fluoride in human milk is about 0.05 ppm and cow’s milk about 0.1 ppm. Nevertheless, in most cases there is no need to supplement breast fed children who reside in optimally fluoridated areas.
Topical Application of Fluoride
The second manner in which fluoride is used for the prevention of dental caries is by topical or local application to the teeth. The first suggestion that such a technique might be effective was explained in the work of Volker and his associates when they reported that the exposure of powdered enamel to solutions of sodium fluoride resulted in a reduction in the solubility of enamel. Subsequent work indicated that the enamel adsorbed fluoride onto its surface. Although the exact mechanism is not known, it appears that there is formation of either a calcium fluoride or a calcium fluorapatite.
Numerous laboratory studies have been carried out to improve the means of decreasing enamel solubility. Thus various fluoride compounds have been tested at varying pH levels. Although early studies dealt with sodium fluoride, it was subsequently found that potassium, ammonium and even lead fluoride were effective in reducing enamel solubility. Muhler and van Huysen found that tin fluoride was an even more effective fluoride compound.
Professionally applied topical fluoride preparations usually contain 2% sodium fluoride, 8% stannous fluoride, or 1.23% acidulated phosphate fluoride.
It was only natural that some attempt would be made to decrease the solubility of ‘whole’ enamel in vivo by exposing it to a relatively concentrated fluoride solution, thereby adsorbing some of the material onto the surface. This, theoretically, should result in a greater resistance of the tooth to acid decalcification. A great many clinical studies have been carried out and the majority has conclusively demonstrated the benefit of topical application of fluoride.
Sodium Fluoride
Neutral sodium fluoride was the first to be used in early clinical trials tested in the 1940s and were shown to reduce caries by about 30%. This technique first proposed by Knutson et al, involved the cleaning of the teeth with pumice paste followed by a four-minute topical application of 2% sodium fluoride solution at pH 7. The initial topical application was then followed by three similar applications at weekly intervals, except that no prophylaxis was carried out at these subsequent visits. The treatment series was recommended at ages 3, 7, 10 and 13 years. The disadvantage of this technique was that the patient had to make four visits to the dentist within a relatively short time. However, sodium fluoride as a topical agent had many advantages in that it is chemically stable, has an acceptable taste, nonirritating to gingiva and does not discolor the teeth.
Stannous Fluoride (SnF2)
The first clinical trial of SnF2 was conducted by Howell et al, in 1955. The procedure again involved coronal polishing and application of stannous fluoride for four minutes semiannually. The advantages of using SnF2 were rapid penetration of tin fluoride and formation of a highly insoluble tin-fluorophosphate complex on enamel surfaces. The disadvantages of aqueous SnF2 far outweighed advantages in that it is unstable and should be prepared fresh for every treatment, its naturally low pH make it astringent, it produces discoloration of the teeth particularly in hypocalcified areas, and the solution has a metallic taste.
In order to overcome some of the disadvantages of a freshly prepared 8.5–10% solution of SnF2, stannous fluoride gel containing 0.4% SnF2 in methylcellulose and glycerin base was developed. This was flavored with cinnamon or grape and remained stable for 15 months. However, for fluoride ion to be released, the gel should be diluted with water following its application to the teeth. This material was found to be effective in postradiation cancer patients and for reducing decalcification around bands in orthodontic patients.
To allow topical fluoride to react with the enamel for more time and thereby increase its uptake, fluoride varnishes have been developed. Some of these are Duraphat which contains 2.26% fluoride in an alcoholic suspension and fluor protector which contains 0.7% fluoride in a polyurethane varnish.
Many problems had to be investigated in the early studies, such as the number of applications necessary to derive maximal benefit in caries reduction, the appropriate interval between applications and the optimal concentration of fluoride solution. Reported studies indicate that the topical application of sodium fluoride to the teeth of children has a significant favorable effect in reducing the dental caries incidence.
A great many clinical studies on the effectiveness of topical application of stannous fluoride in reducing the incidence of dental caries have been reported. For example, Muhler treated the teeth of a group of 232 children, 6–17 years of age, with a single topical application of 8% solution of stannous fluoride; 228 children of a similar age were treated with distilled water and served as controls. All children in this study had resided for their entire lifetime in an area in which fluoride had been added to the communal water supply, and thus the experiment tested an additional beneficial anticariogenic effect of topical fluoride under optimal communal fluoride conditions. At the end of 12 months, Muhler found a 35% reduction of DMF teeth in the stannous fluoride treated group, thus indicating an extension of benefit of fluoride therapy in children already benefiting from communal water fluoridation.
Many other studies testing the clinical anticariogenic effectiveness of topical stannous fluoride solution have been reported in the literature, and the results are generally uniform in their findings of benefit of this compound.
By far the most useful fluoride therapy is the application of acidulated phosphate fluoride (APF) in the form of a solution or gel. The use of these agents provides a 25–40% reduction in caries. APF agent has to be applied for four minutes usually in a disposable tray applicator. APF agents have a pH of approximately 3 and contain 1.23% fluoride and 0.1 M orthophosphoric acid. The low pH favors more rapid fluoride uptake by enamel and the presence of the orthophosphate prevents enamel dissolution by the common ion effect. The application of these solutions or gels is often preceded by a coronal polishing. This removes exogenous stains and plaque but does not affect the cariostatic potential of topical fluoride gel.
Two studies by Muhler and his associates (1965), using a stannous fluoride-phosphate system, found exceptional reductions in caries incidence, and it appeared that this modality is more effective than either stannous fluoride alone or the acidulated sodium fluoride phosphate mixture.
Another method for the topical application of fluoride to prevent dental caries, suggested by Bibby and his associates, is that it could be used in a prophylactic paste. There are numerous studies; however, in which stannous fluoride has been incorporated in a prophylactic paste with either a lava pumice or silex base. In general, it has been reported that stannous fluoride in a prophylactic paste provides caries reductions of between 30 and 40% in both children and adults, in the presence or absence of fluoride in the communal water supply. Also tested was a stannous fluoride-zirconium silicate paste used as a patient-applied treatment procedure.
One of the most effective means of caries reduction involves the daily self-application of 0.5% fluoride gel (5000 ppm F), about 40% of the concentration used for professional office applications in custom fitted trays for five minutes. This form of self-therapy is best suited for high caries risk patients who are sufficiently motivated to conform to the daily regimen. It is appropriate for those school going children and patients who have received therapeutic radiation in the head and neck region. Self-application by brushing with 0.4% stannous fluoride gel (1000 ppm F) has been used as an alternative to the custom-fitted tray method.
The mechanism by which fluoride works also depends on the conditions of its use. For example, at the high fluoride concentrations (12,000–22,600 ppm F) used for topical therapy, there is at least a temporary effect on bacterial metabolism, inhibiting glycolysis and suppressing S. mutans. At lower concentrations, such as systemic fluoride provided by water fluoridation or supplements of topical fluoride from dentifrices and mouth rinses, there is an uptake of fluoride by hydroxyapatite, rendering it less soluble and improving its crystallinity.
Fluoride Dentifrices
This is another method of applying fluoride. The first fluoride containing dentifrice reported to decrease in the incidence of caries as compared with the similar use of a nonfluoride dentifrice, contained stannous fluoride (0.4%) together with calcium pyrophosphate that had been heat treated to increase its compatibility with fluoride.
Sodium monofluorophosphate (MFP) has been used as a therapeutic agent in dentifrices. In the USA, MFP at 0.76% or 1,000 ppm is the most commonly used therapeutic ingredient in commercial toothpastes. Similarly, sodium fluoride was tested in toothpastes with acrylic particles or hydrated silica used as an abrasive. Because of its significant cariostatic benefits, several commercial products use sodium fluoride as the active therapeutic ingredient. A sodium fluoride formulation of 1,100 ppm with silica abrasive was found more effective than the stannous fluoride-calcium pyrophosphate dentifrice because of greater availability of fluoride. However, the degree of effectiveness varies with different dentifrice formulations.
It is generally recognized that the most effective mass reduction in dental caries is afforded by communal fluoridation. This procedure is unavailable; however, in many communities and rural areas. Therefore, it is possible that the use of more than one of the other effective anticariogenic agents may produce cumulative effects. The use of ‘multiple principles of preventive dentistry’ is highly effective.
Fluoride Mouthwashes or Rinses
There has been extensive clinical trial of mouthwashes or rinses containing fluoride used either as a mouthwash to flush the oral cavity, or in a few instances, by application with a toothbrush in efforts to prevent dental caries. For geographic areas where it is impossible to fluoridate the water supplies because of the lack of a central water system, alternative measures should be considered in the form of school-based fluoride mouthrinse program. One of the most important outcomes of early trials with neutral sodium fluoride, acidulated phosphate fluoride and stannous fluoride rinses was the recognition that supervised fluoride rinse programs could reduce caries by 20–50%. NaF was recommended for school-based use over others because it was easy to prepare and had an acceptable taste.
Rinsing is a simple and inexpensive method of utilizing fluoride to inhibit dental caries. This has been proven so unequivocally that the Council on Dental Therapeutics of the American Dental Association has recognized neutral sodium fluoride and acidulated phosphate fluoride rinses as effective caries preventive agents (1975) as well as stannous fluoride rinse (1980). Since rinsing can be performed as an individual caries-preventive measure at home or as a school-based group preventive program, the dentist must be familiar with the different techniques involved, because they vary considerably with the different circumstances and objectives.
One of the earliest large-scale successful clinical trials was reported by Torell and Ericsson in 1965. They undertook a two-year study to evaluate the caries reducing effects of various methods of local application of fluorides. Of six experimental groups, each containing approximately 200 children, 10 years of age, several groups developed significantly less caries compared with control groups.
The vast majority of succeeding studies were aimed not at continuously proving the value of fluoride mouthrinses as a caries-preventive agent, but rather at defining the best technical methods to use in achieving the desired result. Thus, many different fluoride concentrations were tested, ranging from 0.01% to 0.66% NaF, and many rinsing frequencies tried, ranging from twice a day to three or four times a year. These studies are too numerous to review individually, but they have basically given rise to the two chief techniques used nowdays:
• The low potency/high frequency technique, usually recommended for home use.
• The high potency/low frequency technique, usually recommended for school based programs.
The extreme importance of fluoride rinsing as a caries inhibiting technique mandates periodic thorough review and update of these procedures by all practicing dentists.
Bis-biguanides
Chlorhexidine and alexidine have received the most attention as potential anticaries agents, since they have been shown to be effective antiplaque agents. It has been shown by in vitro studies that chlorhexidine is adsorbed onto tooth surfaces and salivary mucins, and then released very slowly in an active form.
The effect of chlorhexidine on the growth of human dental plaque has been studied by Harrap in persons using a chlorhexidine gluconate dentifrice. He found highly significant reductions in plaque growth that were related to the concentrations of the drug. In contrast, Johansen and his colleagues could find no effect on the plaque index as a result of the use of chlorhexidine dentifrice by a group of dental students, although possible favorable effects on caries were noted. Unfortunately, chlorhexidine has a bitter taste, produces a brownish discoloration of hard and soft tissues and may produce a painful desquamation of mucosa.
Silver Nitrate
Silver nitrate impregnation of teeth was used clinically for many years to prevent or arrest dental caries. The earlier workers believed that the silver ‘plugged’ the enamel, either the organic invasion pathways such as the enamel lamellae or the inorganic pathways, combining with the soluble inorganic portion of enamel to form a less soluble combination. Klein and Knutson investigated the effect of ammoniacal silver nitrate on the caries experience in a group of 700 children, ranging in age from 5–12 years and found no significant differences in the caries attack rate between treated and untreated teeth. Carious lesions present at the time of silver nitrate treatment had extended to approximately the same degree in both treated and control teeth. This study was in contrast to one of Younger, who applied silver nitrate precipitated with calcium chloride to the teeth of 25 children, 5–12 years of age, and reported a reduced caries incidence. In a later study, Younger reported a similar reduction in caries in a group of children who were 8–13 years of age.
Zinc Chloride and Potassium Ferrocyanide
Gottlieb, in accordance with his theories of the importance of the protein matrix of the enamel in the dental caries process, proposed that the use of a solution of zinc chloride and potassium ferrocyanide would effectively impregnate the enamel and seal off caries invasion pathway.
Ast and his associates tested the effect of these substances in a group of children 12–15 years of age. The teeth on one side of the mouth were impregnated, while those on the opposite side served as controls. After one year, no significant differences were noted between the two sides in the number of new carious surfaces. A similar result was obtained from a study by Pelton on a group of 100 children ranging from 8–14 yeas of age and a study of Anderson and Knutson on 299 children ranging in age from 7–15 years in whom the total new decayed or filled surfaces after approximately one year were essentially the same for treated and untreated teeth.
The available evidence indicates that the use of substances to impregnate the enamel and thus block organic pathways of caries is of little clinical value.
Substances which Interfere with Carbohydrate Degradation through Enzymatic Alterations
There are many substances known to have the ability to interfere with enzyme systems responsible for carbohydrate degradation and the subsequent formation of acid. If such an inhibitor is to be effective in the clinical prevention of dental caries, it must reach the susceptible areas of the mouth in sufficient concentration at the time at which the sugar undergoes breakdown.
Vitamin K
Synthetic vitamin K (2-methyl-1, 4-naphthoquinone) was suggested by Fosdick and his coworkers to be of potential value in the prevention of caries on the basis of certain studies in vitro. In these studies, the vitamin K was found to prevent acid formation in incubated mixtures of glucose and saliva. Many of the quinones have been found to have a similar action, but none has been superior to synthetic vitamin K.
The clinical effectiveness of this vitamin K was tested by Burrill and his associates. A group of students received a chewing gum containing the synthetic vitamin K and sodium bisulfite, and were instructed to chew this gum for at least 10 minutes after eating any food. The control group received the same chewing gum without the vitamin K. The occurrence of new cavities was determined at 12- and 18 month intervals, at which time it was found that the incidence of new carious lesions was decreased by 48% and 42% respectively, for the two intervals in the experimental group. Thus there is evidence to indicate that the naphthoquinones may be of value in preventing caries.
Sarcoside
A method for screening potential anticariogenic compounds was suggested by Fosdick and his coworkers in 1953, based on the ability of some compounds to penetrate the dental plaque and prevent pH fall below a level of 5.5 after a carbohydrate rinse. They tested several hundred compounds and noted that two of these were promising enzyme inhibitors or ‘antienzymes’: sodium N-lauroyl sarcosinate and sodium dehydroacetate.
Brudevold and Little continued investigation of this sarcoside in patients who brushed their teeth with solutions of the material and then measured the fall in pH of plaque material from proximal surfaces after a sugar rinse. The effectiveness of a toothpaste containing sodium lauroyl sarcoside and dehydroacetic acid was also studied. All tests were negative, and it was concluded that the sarcoside did not reduce acid production in subsurface material of bulky plaque.
The effect of sodium lauroyl and palmitoyl sarcosinate in reducing the solubility of powdered enamel was studied by Volker and his associates. The palmitoyl compound was found to be better than the lauroyl, and in concentrations of 0.01% to 1.0%, was found to be as effective as sodium fluoride in reducing enamel solubility in the presence of acids.
Substances which Interfere with Bacterial Growth and Metabolism
An alternative method for preventing enzymatic degradation of carbohydrates to acids is the prevention of, or at least interference with, bacterial growth and metabolism. There are, of course, great numbers of bactericidal or bacteriostatic agents, but the number of these which are compatible with the oral mucous membranes and with continued good health are small.
Urea and Ammonium Compounds
Urea and ammonium compounds have been tested extensively for use in the oral cavity as anticariogenic agents. The urea in particular was found useful after the preliminary report of Wach and his associates that a quinine-urea solution prevented acid formation in tests in vitro on carbohydrate-saliva mixtures. They also noted that the oral bacteria count was decreased after the use of a quinine-urea mouthwash and that the salivary pH generally increased to a value over 8 and remained high for approximately an hour.
Stephan continued the study of urea and found that a 40–50% solution of urea applied to dental plaques for several minutes prevented the typical pH fall following a carbohydrate rinse for periods up to 24 hours. The evidence indicates that urea, upon degradation by urease, releases ammonia, which acts to neutralize acids formed through carbohydrate digestion and interferes with bacterial growth.
Kesel and his associates reported that dibasic ammonium phosphate in both mouthwash and dentifrice caused a reduction in oral Lactobacillus counts. Studies in vitro indicated that the combination of 5% dibasic ammonium phosphate and 3% urea was even more effective as a bacteriostatic agent and in preventing acid formation than either substance alone.
Other workers, such as Jenkins and Wright have indicated that the ammonium ion plays no specific role in inhibiting growth of acidogenic microorganisms. The ammonium ion has failed to inhibit the growth of lactobacilli in the studies of Kirchheimer and Douglas, while the work of Ludwick and Fosdick showed no relation between the ammonia content of oral cavity and caries immunity.
Cohen and Donzanti reported the results of a study on a group of 169 children using a dentifrice containing 13% urea and 3% diammonium phosphate and 137 children using a similar dentifrice without these two ingredients. Brushing was supervised in the schools twice daily. At the end of one year the mean number of new carious teeth was 1.01 in the control group, but only 0.78 in the experimental group, and a 23% reduction in caries incidence. By the end of the second year, the number of new carious teeth in the control group was 2.27 and in the experimental group 1.70, and a reduction of 25% in caries incidence.
Hawes and Bibby reported the results of a study on 372 children between the ages of 7 and 13 who brushed their teeth for a period of one year under supervision with a dentifrice containing 12% urea (carbamide) and urease. Bacteriologic studies showed that the Lactobacillus counts of the children using the therapeutic dentifrice were not affected to any greater extent than those of the children using the cosmetic dentifrice. The 177 children in the control group exhibited an average increase of 9.01 total tooth surfaces decayed and filled, while the test group, composed of 196 children, presented an average of 9.33 surfaces decayed and filled during the test period. The difference between the two groups was approximately 4% and indicated that the urea dentifrice failed to produce any significant reduction in occurrence of new caries under the conditions of this study.
Although there are some studies to indicate that ammoniated dentifrices are capable of producing some reduction in dental caries incidence, the magnitude of this reduction, particularly in persons whose toothbrushing habits are not controlled or supervised, is not so great as to justify recommending them for widespread use as an anticariogenic agent.
Chlorophyll, the green pigment of plants, has been proposed as an anticariogenic agent on the basis of a number of in vitro and animal studies. Shafer and Hein reported that a watersoluble form of chlorophyll, sodium copper chlorophyllin, was capable of preventing or reducing the pH fall in carbohydrate- saliva mixtures in vitro. The same workers found that the incidence of experimental caries in hamsters was reduced when a chlorophyllin solution was substituted for the drinking water of these animals, but that the Lactobacillus counts were not affected. Other workers, such as Griffiths and Rapp and Nevin and Bibby, have reported that chlorophyll is bacteriostatic with respect to many oral microorganisms, including lactobacilli, streptococci and micrococci.
There have been no clinical studies reported testing the effect of water-soluble chlorophyll on dental caries experience. A number of short-term clinical studies have suggested that this compound may be of some use in reducing mouth odors and allaying gingivitis. Results however have been inconclusive.
Nitrofurans are derivatives of furfural, which itself is derived from pentoses. They have been found to exert a bacteriostatic and bactericidal action on many gram-positive and gram-negative organisms, and on this basis, have been tested by Dreizen and his associates for their ability to inhibit acid production. A number of different nitrofuran compounds were utilized in this study, and it was reported that, even in low concentrations, acid production in saliva from caries active persons was prevented in nearly all cases.
Hufstader and his associates tested the effect of furacin (2-nitro-5-furaldehyde semicarbazone) incorporated in chewing gum on the oral Lactobacillus counts of a group of students. During the 10-day test period during which only a sugar coated gum was chewed, the Lactobacillus counts were definitely increased in the majority of patients. Chewing gum containing furacin did not reduce the oral Lactobacillus count.
The effectiveness of furadroxyl (5-nitro-2- furaldehyde-2-hydroxyethyl semicarbazone) in preventing dental caries was tested clinically by Dreizen and Spies through use of the compound incorporated in a chewing gum. Although the number of patients in each group was relatively small, the data indicated that the nitrofuran compound significantly reduced the dental caries experience and that this substance may have potential use as an anticariogenic agent.
Penicillin has been tested as an anticariogenic compound because of its antibiotic property, which is the ability of the product of an organism to inhibit the normal biologic processes of other organisms. The effects of oral Lactobacillus counts of a dentifrice containing 1,000 units of penicillin per gram were studied by Hill in a group of 10 students. A remarkable reduction from an average of 72,000 colony count to an average of 300 was found after the use of dentifrice for five weeks. After discontinuing the use of dentifrice, the count stayed low for three months and then returned to the same high level. The reduction in colonies were noted with the resumption of penicillin dentifrice, but was considerably slower. A second study was carried out by Hill on a group of orphanage children, and though full cooperation was doubtful, there was some tendency for reduction in Lactobacillus counts in the group who brushed their teeth with a penicillin dentifrice. White and her associates reported that small amounts of penicillin did not greatly alter the balance of the normal oral flora, although larger doses resulted in an increase of gram-negative organisms of the genera Aerobacter and Escherichia, apparently owing to their replacing that part of the flora destroyed by the penicillin.
The effect of prolonged use of a penicillin dentifrice was studied by Fitzgerald and his associates. Their results indicated that after the use of dentifrice for eight months or longer, there were no changes in the Lactobacillus counts attributable to the penicillin. However, there was no increase in numbers of penicillin-fast lactobacilli.
Studies of Zander and Bibby indicated that penicillin effectively interfered with the production of acid in carbohydrate- saliva mixtures even in quantities as low as 10 units in 5 ml of the total solution. These investigators also reported the effect of brushing the teeth of hamsters with a penicillin dentifrice. Brushing with a penicillin toothpaste resulted in a remarkable reduction in caries. McClure and Hewitt reported complete inhibition of caries in rats by administering penicillin to the experimental animals in the food and drinking water.
A clinical study was designed by Hill and Kniesner revealed no significant differences in new carious surfaces between control and experimental groups even though there was a reduction in Lactobacillus counts in the experimental group. Such a finding only emphasizes the difficulty in attempting to relate caries susceptibility or caries activity with the Lactobacillus count.
The results appear to indicate that penicillin is not a particularly effective anticariogenic agent. The wisdom of using this material for such a purpose has been further questioned by many because of the possibility of development of penicillin-resistant pathogenic microorganisms and sensitization.
Other Antibiotics
A variety of other antibiotics have been tested, in both experimental animal and clinical trials, for potential use as anticaries agents. These, along with other chemotherapeutic agents, have been reviewed by Johnson and Rozanis with special reference to plaque control. These investigators also pointed out that some of the problems in using these drugs in humans include the possible induction of resistant strains of microorganisms, the possibility of allergic reactions, the occurrence of side effects such as nausea and diarrhea, and the expense of long-term use. They also characterized the ‘ideal’ antibiotic for use as an anticaries agent as being one which has a very narrow spectrum directed toward plaque-forming microorganisms, is not in general use against systemic diseases, is neither toxic nor allergenic and is retained in the tissue in an active state for a prolonged period with a predilection for the oral cavity.
Erythromycin was tested by Lobene and his associates, who reported a 35% decrease in plaque formation after a seven-day test period of rinsing and then swallowing the agent four times a day. This effect was lost rapidly when the drug was withdrawn in three of four patients, and in addition, all developed diarrhea as a side effect.
Kanamycin has been evaluated by Loesche and his associates for its effects on dental plaque in a small low-caries group when the antibiotic was applied topically for a few weeks and for one year. While there was some improvement in gingivitis scores, plaque scores were not changed despite some physicochemical changes in the plaque.
Spiramycin was noted by Keyes and his colleagues to be the most effective of nine antibacterial agents tested in hamsters for controlling dental plaque, caries and periodontal lesions. However, the clinical trials have been somewhat conflicting as to the beneficial effects of the drug on dental plaque. It would appear that any benefits derived are considerably less than highly significant.
Tetracycline was reported by Löe and his coworkers to decrease plaque scores when used as 0.5% mouthwash three times a day for five days in place of mechanical oral hygiene. However, there is little additional information available concerning its potential use as an anticaries agent.
Tyrothricin was reported by Shiere to be responsible for a 35% reduction in the incidence of new decayed and filled permanent tooth surfaces in children 7–14 years of age after one year and for a 26% reduction in the incidence of such surfaces after two years during a controlled clinical trial of brushing with a 0.05% tyrothricin toothpaste.
Vancomycin has been reported by DePaola and his associates to temporarily suppress S. mutans when applied to the teeth of children as a 15% gel on five successive days. The microorganisms generally could not be detected on teeth for one week following the cessation of treatment. A similar diminution in S. mutans was found following testing with a 1% vancomycin paste. DePaola and his colleagues also conducted a one-year clinical trial on the effect of topically applied vancomycin on dental caries increment. They found a statistically significant reduction in dental caries experience in fissures but not on smooth surfaces in the experimental groups. Furthermore, they found that caries reduction was significant in newly erupting teeth but not in teeth already present in the mouth at the initiation of the study. Thus, this antibiotic also does not appear to satisfy sufficient criteria for universal use as an anticaries agent.
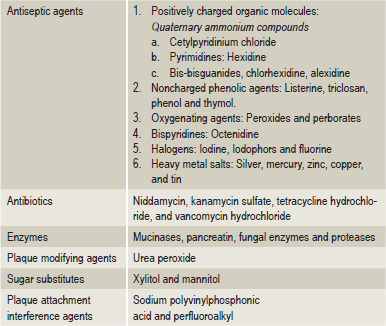
Plaque Control Agents (Table 9-6)
Caries Vaccine
Interest in a vaccine for dental caries protection dates back to a period when the lactobacilli were thought to be of paramount importance in the initiation of dental caries. By means of immunization with a homologous Lactobacillus vaccine, in 1944 Williams was partially successful in reducing the number of lactobacilli in human saliva. The recognition of the important role that S. mutans plays in the initiation of caries has led to a reawakening of interest in the vaccine approach, as evidenced by the numerous experimental attempts to control caries immunologically in laboratory animals such as the rat and monkey. Although results have always been encouraging, development of a caries vaccine is considered a highly desirable goal because of the potentially important public health implications. Considering the properties of S. mutans, which are associated with its cariogenicity, an antibody (immunologic) approach to caries control could theoretically be accomplished by a number of mechanisms, including:
• Interfering with adherence, colonization and dissemination of the organisms in the oral cavity.
• Reducing its ‘stickiness’ by altering its polysaccharide metabolism.
• Altering the ability of the microorganism to produce acid.
Although recent studies have shown that an antibody can reach the oral environment via saliva or gingival crevicular fluid, much more research will be necessary before a caries vaccine becomes available to the general public. Many important unanswered questions remain about the effectiveness of mode and route of immunogen administration, dosages and schedules of immunization, types of immunogen and adjuvants, possible adverse reactions and crossreactivity of immunogens, and effectiveness in monitoring the immune response to immunization procedures.
Nutritional Measures for Caries Control
The importance of diet, particularly sucrose containing foods and beverages in cariogenesis, is well known. On an individual basis, the dentist, dental hygienist and/ or dietitian consultant can provide information on safe foods and drinks. But the ultimate responsibility for diet modification lies on the individual. Voluntary dietary restriction may suit some patients and certainly reduce caries as evidenced by persons who have hereditary fructose intolerance. The function of the dental office personnel in diet modification is one of counseling, providing information, motivation and encouragement. The diet used in caries prevention is essentially a healthy, adequate, balanced diet and resembles a normal diet except for the exclusion of a few food components and eating practices.
Microbiological examination provides an objective method for assessment of the patient’s cooperation. Changes in dietary habits are reflected within a couple of weeks in corresponding reductions in the numbers of oral lactobacilli and Streptococcus mutans. Follow-up visits are advised so that the patient’s diet can be rechecked and further modifications adopted if necessary.
The control of dental caries through nutritional or dietary means is impossible to achieve on the basis of a mass prevention program and, for this reason, is relatively unimportant in public health and preventive dentistry in contrast to fluoridation of water supplies. Accordingly, caries control by dietary modification on a public health scale requires the help and cooperation of the food industry if it has to have any serious impact. Strict statutory definitions cover claims that products are ‘anticavity’, ‘noncariogenic’, and ‘less cariogenic’. It is important, however, for the dentist in private practice to understand the significance of controlling caries in individual patients by dietary measures. In many persons, particularly those suffering from rampant caries, every means at the disposal of the dentist must be utilized to preserve the dentition.
The chief nutritional measure advocated for the control of dental caries is restriction of refined carbohydrate intake. Only the most cooperative patient will adhere rigidly to the type of diet designed to reduce sugar consumption drastically. For this reason, clinical studies on large groups of patients for the purpose of ascertaining the extent of caries reduction that would occur with restriction of sugar consumption are difficult to carry out. This count frequently has been used to study sugar restriction because of the apparent relation between the oral Lactobacillus count and carbohydrate intake. This does not necessarily imply that a causative relation exists between the Lactobacillus and dental caries activity.
One of the best known studies dealing with the effect of dietary carbohydrate restriction on dental caries incidence is that of Becks and his coworkers. This project was designed to investigate the association of dental caries and the L. acidophilus indices in patients with rampant caries and in caries free persons, as well as the effect of carbohydrate reduction on the Lactobacillus count and on subsequent caries experience in a group of patients with rampant caries.
A close correlation between caries activity and the Lactobacillus index was found in this study.
Phosphated Diets
The results of clinical tests of dietary phosphate additions for the sole purpose of controlling human dental caries are as yet inconclusive. Stralfors mixed 2% dibasic calcium phosphate into the bread, flour, and sugar used in a school lunch program in Sweden and obtained a significant reduction in caries incidence in the maxillary incisors over a two-year period. Ship and Mickelsen found no meaningful reduction in the caries attack rate of children consuming a diet in which flour used in the preparation of bakery products was supplemented with 2% calcium acid phosphate for three years. The cariostatic superiority of sodium dihydrogen phosphate over calcium acid phosphate was attributed to the greater systemic action of the sodium salt as demonstrated by radiophosphorus uptake studies on sound and carious enamel. The possibility that dicalcium phosphate may be caries inhibitory in the human, if permitted to remain in the oral cavity long enough, has lately been demonstrated by Finn and Jamison, who had children chew a sugar containing gum supplemented with 225 mg dicalcium phosphate per stick for 20 minutes five times daily. After 30 months on this regimen, there was a significant reduction in caries increment compared to that of a group using an unphosphated sugar gum.
In Australia, Harris and Beveridge obtained a 30% reduction in caries in 1,400 children restricted to a diet in which calcium sucrose phosphate was added to the carbohydrate component at levels ranging from 0.2–1.0%. They hypothesized that the calcium sucrose phosphate penetrates the surface crystalline layers of enamel, tightening the attachment between crystals. This reinforcing action protects enamel from disintegration by acids.
Despite the apparent importance of caries control through nutritional measures, there is a remarkable dearth of controlled studies by which one may judge the value of such procedures. This attests to the difficulties which would be involved in imposing such measures on large groups of patients.
Mechanical Measures for Caries Control
The control of dental caries by mechanical measures refers to procedures specifically designed for and aimed at removal of plaque from tooth surfaces. Although the saying “A clean tooth does not decay” is not based upon sound scientific evidence, it seems reasonable that a tooth surface free from the accumulation of microorganisms and carbohydrate substances could not become carious.
There are numerous means of cleansing the tooth mechanically, and these were reviewed and classified by Hine in a discussion of caries control measures as:
He further pointed out that although most investigators have stressed the importance of maintaining oral hygiene in preventing dental caries, no evidence was cited to support these statements. Experienced clinicians know that filthy teeth do not always decay and that, conversely, ‘clean’ teeth often become carious. Although progress has been made in identifying the pathogens which play a role in dental caries, the primary method in preventing dental diseases remain mechanical removal of plaque and promotion of the remineralization of the tooth surface.
Oral Prophylaxis
In the control of periodontal disease, the value of routine scaling and polishing of the teeth at periodic intervals of three or six months cannot be denied. Yet since dental plaque formation occurs within a matter of hours to a day or two after complete removal of the structure, there is probably little value, if any, in prophylaxis for the control of dental caries. Hine pointed out that the careful polishing of roughened tooth surfaces and the correction of faulty restorations is probably of more importance than the mechanical cleansing of the tooth by prophylaxis. These procedures might conceivably reduce the retention of food debris and decrease the formation of bacterial plaques, thereby reducing the development of new carious lesions. Many studies have demonstrated that, in dental caries, the pathogenicity of plaque is related to the numbers of S. mutans and related species present. In contrast, the plaques associated with gingival inflammation are characterized by a predominance of gram-negative flora rather than the predominantly grampositive flora found in health. This transition seems to coincide with inflammatory changes that occur at the gingival margins. Plaque control efforts should be directed towards two goals: limiting the numbers of S. mutans in dental plaques for the prevention of caries by mechanical elimination of supragingival plaque and limitation of dietary sucrose and secondly, maintaining the predominantly gram-positive flora associated with gingival health by mechanical removal of plaque from the subgingival area on a regular basis.
Toothbrushing
This is the most widely accepted technique for plaque removal on teeth. The value of toothbrushing in the control of dental caries has been argued by many authorities. It cannot be denied that there are some individuals who have never used a toothbrush and yet are free of caries. These persons are certainly exceptional and may prove that the inherent caries resistance of the individual may be of greater importance than local factors. On the other hand, there are many persons who conscientiously brush their teeth at least twice a day and yet suffer from a serious amount of dental caries. Since most persons delay brushing their teeth after meals for varying periods of time and since, acid production in the dental plaques occurs within a matter of minutes after the ingestion of carbohydrate, as Stephan has shown, a high caries incidence despite persistent toothbrushing is at least understandable.
Another factor in the explanation of the failure of toothbrushing to prevent dental caries lies in the difficulty of reaching all exposed surfaces of teeth upon which plaques may form with the brush. In considerable number of patients, brushing does not reach all areas of the teeth. Indeed, it is ironic that most patients spend the greatest amount of time brushing buccal, labial and lingual surfaces, which are not so prone to decay as the more inaccessible interproximals and the deep fissures of occlusal surfaces into which toothbrush bristles will not reach (Fig. 9-36).
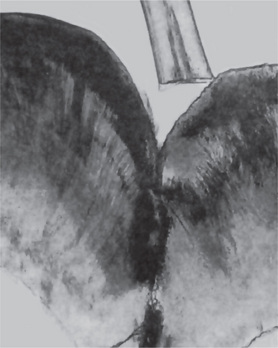
Figure 9-36 Toothbrushing
A ground section of a tooth shows the relative size of an occlusal fissure compared with a single bristle from a standard toothbrush to illustrate the difficulty which may be encountered in attempting to cleanse the depth of these fissures.
The extent to which plaque is removed is related to the duration of brushing. A minimum time of five minutes daily has been recommended for brushing or flossing or using other interproximal cleansing aids. The thoroughness of toothbrushing is usually measured by plaque or oral hygiene scores. However, no consistent relationship is demonstrable since the two indices gauge items that occur considerably over different time intervals.
As an alternative to measuring the efficacy of plaque removal, some investigators have studied the diligence of toothbrushing, using questionnaires about brushing frequency. For example, it has been reported that children who brush twice or more per day had significantly less caries than children who brushed only once a day or less. Since a majority of children use fluoride-containing dentifrice, these results may be due to increased contact with a topical fluoride agent rather than to mechanical cleansing of tooth surface.
A number of studies have indicated that toothbrushing will reduce the number of bacteria in the oral cavity; but in view of the countless millions of microorganisms remaining in the oral cavity, the significance of removing a certain but undoubtedly small percentage is probably negligible. There are several studies on the effect of toothbrushing on the incidence of experimental dental caries in animals. In a study testing the effect of a penicillin dentifrice on caries in hamsters, Zander and Bibby found that simply brushing the teeth of animals with controlled nonmedicated toothpaste resulted in a 69% reduction in caries as compared to a group in which the teeth were not brushed. Subsequent studies in other animals have demonstrated similar results.
Although toothbrushing would seem to be important, not all clinical studies completely support this idea.
Mouthrinsing
The use of a mouthwash for the benefit of its action in loosening food debris from the teeth has been suggested to be of value as a caries control measure. There is no scientific evidence to confirm this suggestion, and mouthwashes would appear to be of only limited value except for the fluoride mouthwashes previously discussed.
Dextranase, an agent which is sought to disperse dental plaque by hydrolyzing the streptococcal polysaccharides in vitro, has been used in mouthrinses. This has been tested in clinical trials by using various durations and frequencies of rinsing, ranging from one minute, four times per day to five minutes, seven times per day. Rinsing with these enzyme solutions does not prevent the development of plaque, although the proportion of S. mutans in plaque was seen to be reduced. The use of dextranase as a caries control agent represents an attractive concept of disease control in which the therapeutic agent is directed at a specific metabolic product of the causative organism rather than at the organism itself.
Dental Floss
Dental flossing has been shown to be effective in removing plaque from an area gingival to the contact areas on proximal surfaces of teeth, an area impossible to reach with the toothbrush. There is general agreement that flossing is necessary if interproximal gingival health is to be maintained, but opinions differ as to the value of flossing in preventing dental caries. The research findings regarding control or prevention of dental caries by flossing are contradictory. Most studies involved children, and thus digital aptitude in manipulating the dental floss is an important variable. Fluoridated dental floss successfully reduced interproximal colonization by S. mutans as shown by the studies of Gillings.
Oral Irrigators
The custom of flushing the mouth for therapeutic purposes dates from antiquity. However, the use of flushing devices was first reported in the early 1900s. Most of these reports with regards to treating the dental infection by flushing are concerned with the beneficial effects of oral irrigation on gingival infections. No reports have referred to the effect of irrigation on the control of dental caries.
Detergent Foods
Some workers have related the high caries incidence among modern civilized races to the unrestrained use of soft, sticky, and refined foods, which tend to adhere to the teeth. It has been stated that fibrous foods in the diets prevent lodging of food in pits and fissures of teeth, and in addition, act as a detergents.
A number of studies have indicated that the act of eating removes a relatively large number of microorganisms from the oral cavity. Crowley and Rickert reported that after eating, there was a reduction of as high as 78% of bacteria that could be recovered from the mouth. It is only reasonable to state that hard, fibrous food would be more beneficial in mechanically cleansing the oral cavity than soft, and sticky food. It also appears acceptable that the adherence of soft foods to the teeth would predispose to the development of more caries than would be found in a mouth kept relatively clean by a fibrous diet. Yet, despite recommendations that the eating of fibrous foods, either as a part of the diet or simply after meals, is beneficial as a caries control measure, there is no scientific evidence based upon controlled studies in human beings to indicate that this is true.
Chewing Gum
It has been suggested that the chewing of gum would tend to prevent dental caries by its mechanical cleansing action. But most chewing gums contain a considerable amount of carbohydrate, and this might actually increase caries susceptibility.
Xylitol, a pentose alcohol found naturally in variety of fruits and vegetable, and obtained commercially from birch trees, coconut shells and cottonseed hulls, has been proposed as a possible sugar substitute. Several studies have provided dietary xylitol in the form of xylitol sweetened chewing gum as an addon without attempting to restrict sucrose intake. Short-term chewing of xylitol gum (two packages per day for four weeks) significantly reduced salivary levels and plaque proportions of S. mutans, whereas sorbitol or fructose sweetened gum had no such effect. Xylitol, due to its organoleptic properties, stimulates salivation thereby increasing plaque pH and thus promotes remineralization. It is thus used as a sweetener in noncariogenic confectionary and less frequently in dietetic foods.
Chewing gum has been utilized as a vehicle for delivery of fluoride (Fluomin, 0.25 mg F). Peak fluoride concentrations were in the range of 15–25 ppm in the first five minutes after the ingestion of a 0.25 mg preparation. However, the fluoride concentration decreased rapidly by about 30 minutes reaching a level of 1 ppm. However, with regular follow-up, the use of chewing gum may indeed have a perceptible cariostatic effect.
Pit and Fissure Sealants
Pits and fissures of occlusal surfaces are among the most difficult areas on teeth to keep clean and from which to remove plaque. Because of this, it was suggested many years ago that prophylactic odontotomy, the preparation of cavities in these areas and their restoration by some material such as amalgam had to be carried out before extensive decay developed. In this way, these caries susceptible pit and fissure areas would be made less susceptible to subsequent caries. The use of polymers as fissure sealants, and to a lesser extent, as coatings owes its origin to Gore, who in 1939 had used solutions of cellulose nitrate inorganic solvents to fill the surface enamel which was made porous by the action of acids in the saliva. The sealant is not necessarily required to fill the entire depth of the fissure, but it must extend along its entire length, bonding firmly at the fissure entry. Although some bacteria sealed within fissures may remain viable for extended periods of time, they do not produce sufficient acid to initiate caries if deprived of a continuous external source of fermentable carbohydrate.
A major breakthrough in the efforts to produce an effective sealant occurred when Buonocore reported greatly improved retention of an acrylic filling material to an enamel surface that had been etched with a 50% phosphoric acid solution. The etchant, referred to as a conditioning agent, removes surface layers and a part of the enamel surface to about 5–10 μm and thereby produces surface irregularity into which the resin materials penetrate and polymerize. The pit and fissure sealants, generally used in conjunction with an acid pretreatment to enhance their retention, contain either cyanoacrylate, polyurethane or the adduct of bisphenol A and glycidyl methacrylate (BIS-GMA) as major components. BIS-GMA, an epoxy resin is currently the resin component of most composite resin materials. Others include Duraphat a varnish preparation containing sodium fluoride. The advantage of this material is that it sets on the moist tooth surface as a thin film and functions as an extended fluoride application than as a true sealant.
Glass-ionomer cement, has an impressive cariostatic effect because of its high fluoride content, has been used as a fissure sealant.
Cueto and Buonocore (1967) reported that a cyanoacrylate sealant, applied every six months, resulted in an 86% reduction in caries after one year. Ripa and Cole, utilizing the same type of sealant, reported that 85 first permanent molars had 84.3% less occlusal caries than an equal number of controls after one year. Buonocore tested 60 patients using bisphenol A-glycidyl methacrylate containing benzoin methyl ether, making the curing process sensitive to ultraviolet light. He reported that there was a caries reduction of 100% after one year, and 99% after two years in the permanent molars. In the tested deciduous teeth, he reported an 87% protection.
Thus, the evidences accrued indicate that pit and fissure sealants are an additional aid in the prevention of one form of dental caries. Boudreau and Jerge (1976) concluded that sealants were effective in preventing occlusal decay, although they re-emphasized what most investigators had suggested that occlusal sealants should be but one component of a multiple approach to a preventive dentistry program.
Caries Activity Tests
Clinical examination of carious lesions with a probe and mirror, coupled with radiographs, neither predicts caries activity nor a patient’s susceptibility to dental caries. A reliable laboratory test for measuring caries activity offers a valuable adjunct for patient motivation in a caries prevention program. Caries activity refers to the increment of active lesions (new or recurrent lesions) over a slated period of time. Caries susceptibility refers to the inherent tendency of the host and target tissue, the tooth, to be afflicted by the caries process. This is the susceptibility of a tooth to a caries producing environment. A caries activity test measures the degrees to which the local environmental challenge (e.g. dietary effect on microbial growth and metabolism) favors the probability of carious lesions. A caries activity test establishes the need for personalized preventive measures provides an index of the success of therapeutic procedures and monitors the effectiveness of education program.
Several biochemical and microbiological tests, which are suitable for use in a dental office, have been developed as indices of caries activity, keeping in mind that bacterial flora, the local substrate for bacteria in the oral cavity and the host may all interact in determining the caries activity. The interpretations of these laboratory tests are; however more reliable with a good clinical assessment.
Lactobacillus Colony Test
The oldest and the most widely used microbiological method for assessing the caries activity is the Lactobacillus colony count. This method, measures the number of aciduric bacteria in a patient’s saliva by counting the number of colonies which appear on tomato peptone agar plates, a selective medium with pH 5.0, after inoculation of the patient’s saliva and incubation. An improved selective media with an acidic pH having high amounts of acetate, salts and lower surface tension that is highly selective for growth of Lactobacillus is the Rogosa’s medium. The colonies grown on media upon incubation reflect the number of aciduric flora in the patient’s saliva. The lactobacilli count is interpreted as shown in Table 9-7.
Table 9-7
Results and interpretation of lactobacilli count in relation to caries activity
| No. of lactobacilli per ml of saliva | Caries activity |
| 0–1000 | Little or none |
| 1000–5000 | Slight |
| 5000–10,000 | Moderate |
| > 10,000 | Marked |
Quantitating lactobacilli in paraffin stimulated saliva can give variable counts, thus limiting the usefulness of caries activity. However, by repeated salivary sampling, the lactobacilli count may be an important measure of caries activity and is used as a reference test for new caries activity tests.
Colorimetric Snyder Test
This test developed by Snyder in 1951 is based on the rate of acid produced when a sample of stimulated saliva is inoculated into a glucose and agar containing medium of pH 4.7–5.0. The medium has bromocresol green as a color indicator, which changes from blue-green at pH 4.7–5.0 to yellow at pH 4.0, indirectly checking the presence of acidogenic and aciduric microorganisms. The acid produced by the oral acidogenic flora is detected by the changes in pH indicator, and is compared to an uninoculated control tube after 24, 48 and 72 hours of incubation. Snyder’s test is charted for interpretation as follows (Table 9-8). The Snyder test is simple and correlates well with Lactobacillus colony count. Neither the Snyder test nor the Lactobacillus colony count can predict the extent of expectancy of caries with any reliability for one individual, but are of value in assessing the oral environmental cariogenic challenge.
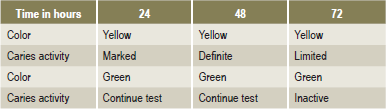
Swab Test
The principle involving the swab test is essentially the same as Snyder test, where the aciduric and acidogenic elements of the oral flora are measured after appropriate incubation periods by employing a color indicator in the test medium and recording the pH directly. The test involves sampling the oral flora by swabbing the buccal surfaces of teeth with a cotton applicator, which is subsequently incubated in the medium.
The pH following a 48-hour incubation is read on a pH meter or the color change is read by use of color comparator. A pH of 4.1 and below denotes marked caries activity; 4.2–4.4 is considered active; 4.5–4.6 is considered slightly active; and a pH of 4.6 and above is considered as caries inactive.
Salivary S. mutans Level Test
The problem with regard to S. mutans caries activity test is that it accounts for less than 1% of the total flora of plaque and their numbers are extremely variable even from the same site. As S. mutans harbor at specific sites, the salivary S. mutans count does not ascertain its location on teeth or assess its degree of infection at a given site. It is also understandably difficult to distinguish a carrier state from a cariogenic infection based on S. mutans numbers alone. However a clinician could use these counts as an add-on in caries management.
The number of S. mutans forming units per unit volume of saliva is the fundamental basis of this test. Plaque samples from distinct sites such as pits and fissures or from a proximal area are, however, more appropriate for detecting and quantitating S. mutans that have colonized on teeth. Saliva, on the other hand, provides a workable alternative as it may not be practical to sample a large number of dental sites for evaluation. The test involves incubation of the sample obtained using tongue blades or a wooden spatula on Mitis Salivarius Agar (MSA), a selective streptococcal medium with increased concentration of sucrose (20%) and 0.2U bacitracin per ml to suppress the growth of most non S. mutans colonies. Agar plates are incubated at 37° C for 48 hours 95% N2- 5% CO2.
Levels of S. mutans greater than 105 are indicative of an acceptable cariogenic challenge because colonization does not occur until the level of S. mutans reaches 4.5×104/ml for smooth surface and 103/ml of occlusal fissures. Several clinical studies have corroborated the finding that the percentage of S. mutans in saliva increases significantly as a function of the DMFS score. There is thus substantial evidence for associating high S. mutans counts with caries activity.
S. mutans Dip-slide Method
This test classifies salivary samples according to estimates of S. mutans colonies growing on modified MSA. In this method, the stimulated saliva is collected for five minutes and is poured over the agar coated slide, totally wetting the surface and the excess allowed to drain off. After the slides are dry, the bacitracin disks are placed in the middle of the inoculated agar, about 1 cm from each other. The slide is then incubated in a tube containing a CO2 tablet for 48 hours. A zone of inhibition 10–20 mm in diameter is formed around each bacitracin disk. If present, S. mutans appears as small blue colonies growing within the zone of inhibition. The colony density is compared with a model chart and classified as 0 (negligible), 1 (less than 100,000), 2 (100,000–1000,000) 3 (more than 1000,000) S. mutans CFU/ml of saliva.
Buffer Capacity Test
This test evaluates the quantity of acid required to lower the pH of saliva through an arbitrary pH interval or, in other words, the amount of acid or base necessary to bring color indicators to their end point. Importantly, buffer capacity could be quantitated either using a pH meter or color indicators. This test relates the buffering capacity of saliva and caries activity. Patients with increased proneness to carious lesions have a lower buffering capacity in their saliva than saliva of those who are relatively free.
Enamel Solubility Test
The Fosdick calcium dissolution test measures a milligram of powdered enamel dissolved in four hours by acid formed when the patient’s saliva is mixed with glucose and powdered enamel. Even though the correlation is reportedly good from limited studies, the test is not simple and requires trained personnel and the cost involved is high. A test similar to the Fosdick calcium dissolution is available where the pH achieved at the end after four hours is measured instead of the amount of calcium dissolved. This caries susceptibility test is not suited for office procedures.
Salivary Reductase Test
The salivary reductase test is yet another caries susceptibility assay to measure the rate at which the indicator molecule diazoresorcinol, changes from blue to red to colorless or whitish on reduction by the mixed salivary flora. The activity of the reductase enzyme present in salivary bacteria is measured by this test. No incubation procedures are required and the caries conduciveness reading is taken in 15 minutes (Table 9-9). Some investigators have concluded that this test does not give accurate results and may not be of diagnostic value, while others have proposed that this test is rather a measure of oral hygiene status of individual. However, caries free adults exhibit low or negative scores on the reductase test.
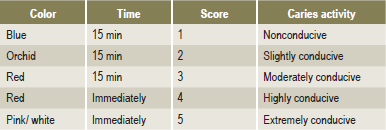
None of the above caries activity tests are comprehensive or reliable indicators of expected caries activity. This is not surprising as caries activity tests measure a single parameter such as acids produced or colony counts of a bacterial species. Dental caries being a multifactorial disease far outweighs the caries predictive tests which do not include factors involved in caries resistance such as fluoride exposure, maturation of enamel, or immune protection. The combined use of several selected tests is the best predictor of expected caries activity. The caries activity test thus provides indirect evidence that an aciduric and acidogenic flora is associated with the development of dental caries. The management of patients with increased caries proneness becomes less complicated by the effective use of caries activity tests which offer measurable parameters and accordingly institute a novel therapeutic approach.
References
Afonsky, D. Saliva and its relation to oral health: a survey of the literature montgomery. Ala: University of Alabama Press, 1961.
American Association for the Advancement of Science, Fluorine and Dental Health. Am Assoc Adv Sci. 1942. [Washington DC].
American Dental Association, Bureau of Economic Research and Statistics. Survey of needs for dental care. J Am Dent Assoc. 1953; 45:706. [46: 200, 562, 1953;47: 206, 340, 572, 1953.].
Idem. 1959 survey of dental practice. J Am Dent Assoc. 1961; 60:750. [791, 1960; 61: 128, 373, 520, 749, 1960; 62: 116, 220, 453, 627, 764].
Idem. The 1977 Survey of Dental Practice Chicago, 1977. American Dental Association, Council on Dental Therapeutics. J Am Dent Assoc. 1960; 61:272. [Evaluation of Crest Toothpaste].
Idem. Council classifies fluoride mouthrinses. J Am Dent Assoc. 1975; 91:1250.
Anderson, R.W., Knutson, J.W. Effect of topically applied zinc chloride and potassium ferrocyanide on dental caries experience. Public Health Rep. 1951; 66:1064.
Idem. An evaluation of the role of vitamins and minerals in the control of caries. In: Easlick K.A., ed. Dental Caries, Mechanism and Present Control Technics as Evaluated at the University of Michigan Workshop. St Louis: CV Mosby, 1948.
Arnim, S.S. Microcosms of the human mouth. J Tenn Dent Assoc. 1959; 39:3.
Arnold, F.A., Jr., An evaluation of the effectiveness as caries control measures ofingested fluorides in water, food, bone flour, and proprietary preparationsEaslick K.A., ed. Dental Caries, Mechanism and Present Control Technics andEvaluated at the University of Michigan Workshop, 1948. [CV Mosby, St Louis].
Idem. The production of carious lesions in the molar teeth of hamsters (C auratus). Public Health Rep. 1942; 57:1599.
Arnold, F.A., Jr., Dean, H.T., Knutson, J.W. Effect of fluoridated public water supplies on dental caries prevalence. Public Health Rep. 1953; 68:141.
Ast, D.B., Chase, H.C. The Newburgh-Kingston caries-fluorine study IV: dental findings after six years of water fluoridation. Oral Surg. 1953; 6:114.
Ast, D.B., Bushel, A., Chase, H.C. A clinical study of caries prophylaxis with zinc chloride and potassium ferrocyanide. J Am Dent Assoc. 1950; 41:437.
Ast, D.B., Finn, S.B., Chse, H.C. Newburgh-Kingston caries-fluorine study III: further analysis of dental findings, including the permanent and deciduous dentitions after four years of water fluoridation. J Am Dent Assoc. 1951; 42:188.
Ast, D.B., Bushel, A., Wachs, B., Chase, H.C. Newburgh-Kingston caries-fluorine study VIII: combined clinical and roentgenographic dental findings after 8 years of fluoride experience. J Am Dent Assoc. 1955; 50:680.
Ast, D.B., Smith, D.J., Wachs, B., Cantwell, K.T. Newburgh-Kingston caries-fluorine study XIV: combined clinical and roentgenographic dental findings after ten years of fluoride experience. J Am Dent Assoc. 1956; 52:314.
Averill, H.M., Bibby, B.G. A clinical test of additions of phosphate to the diet of children. J Dent Res. 1964; 43:1150.
Averill, H.M., Freire, P.S., Bibby, G.G. The effect of dietary phosphate supplements on dental caries incidence in tropical. Brazil Arch Oral Biol. 1966; 11:315.
Backer-Dirks, O. Posteruptive changes in dental enamel. J Dent Res. 1966; 45:503.
Baden, E. Environmental pathology of the teeth. In: Thoma’s Oral Pathology. Gorlin, RJ, Goldman, HM. CV: Mosby, st Louis Louis; 1970:184.
Barmes, D.E. International comparative analysis of the findings in Yamanashi in Onisi: Dental Health care in Japan. In: Progressive report on Yamanashi survey of WHO/ICS. Tokyo: Ishiyaku; 1981.
Becks, H. The physical consistency of food and refined carbohydrate restrictions— their effect on caries. In: Easlick K.A., ed. Dental Caries, Mechanism and Present Control Technics as Evaluated at the University of Michigan Workshop. St Louis: CV Mosby, 1948.
Becks, H., Jensen, A.L., Millarr, C.B. Rampant dental caries: prevention and prognosis: a five year clinical survey. J Am Dent Assoc. 1944; 31:1189.
Bellinger, W.R. The dental implications of fluorine: a review of the literature. J Am Dent Assoc. 1947; 34:719.
Berman, K.S., Gibbons, R.J. Iodophilic polysaccharide synthesis by human and rodent oral bacteria. Arch Oral Biol. 1966; 11:533.
Bibby, B.G. Fluoride mouthwashes, fluoride dentifrices, and other uses of fluorides in control of caries. In: Easlick K.A., ed. Dental Caries, Mechanism and Present Control Technics as Evaluated at the University of Michigan Workshop. St Louis: CV Mosby, 1948.
Bibby, B.G. A study of a pigmented dental plaque. J Dent Res. 1931; 11:855.
Bibby, B.G. Saliva and dental caries. In: Muhler J.C., Hine M.K., eds. A Symposium on Preventive Dentistry. St Louis: CV Mosby, 1956.
Bibby, B.G., The use of fluorine in the prevention of dental caries. J Am Dent Assoc. 1944:228.
Bibby, B.G., Zander, H.A., McKelleget, M., Labunsky, B. Preliminary reports on the effect on dental caries of the use of sodium fluoride in a prophylactic cleaning mixture and in a mouthwash. J Dent Res. 1946; 25:207.
Bilbiie, V., Steiber, C., Popescu, A. The bacterial dental plaque as an ecologic system. Int Dent J. 1971; 21:322.
Black, G.V. Susceptibility and immunity to dental caries. Dent Cosmos. 1899; 41:826.
Black, G.V., McKay, F.S. Mottled teeth; an endemic developmental imperfection of the enamel of the teeth heretofore unknown in the literature of dentistry. Dent Cosmos. 1916; 58:129.
Blackerby, P.E., Jr. Comparative analysis of dental conditions among white and negro children of rural and semirural communities. J Am Dent Assoc. 1939; 26:1574.
Blayney, J.R., Greco, J.F. The Evanston dental caries study IX: the value of roentgenological vs clinical procedures for the recognition of early carious lesions on proximal surfaces of teeth. J Dent Res. 1952; 31:341.
Blayney, J.R., Bradel, S.F., Harrison, R.W., Hemmens, E.S. Continuous clinical and bacteriologic study of proximal surfaces of premolar teeth before and after the onset of caries. J Am Dent Assoc. 1942; 29:1645.
Bodecker, C.F. Preliminary communication upon a method of decalcifying structures containing minute quantities of organic matter, with special reference to the enamel. Dent Rev. 1905; 19:448.
Bodecker, C.F. Die Bakterien im Schmelzgewebe als ursache karioser. Vorgange Vjschr Zahnkeilk. 1928; 44:242.
Boudreau, G.E., Jerge, C.R. The efficacy of sealant treatment in the prevention of dental caries: a review and interpretation of the literature. J Am Dent Assoc. 1976; 92:383.
Bowen, W.H. Nature of plaque. Oral Sci Rev. 1976; 9:3.
Bowen, W.H., Genco, R.N., O’Brien, T.C. Immunologic Aspects of Dental Caries Special Supplement to Immunology Abstracts. Washington DC: Information Retrieval Inc, 1976.
Boyd, J.D., Drain, C.L., Stearns, G. Metabolic studies of children with dental caries. J Biol Chem. 1933; 103:327.
Bransby, E.R., Knowles, E.M. A comparison of the effect of enemy occupation and postwar conditions on the incidence of dental caries in children in the Channel Islands in relation to diet and food supplies. Br Dent J. 1949; 87:236.
Brawley, R.E., Sedwick, J.H. Studies concerning the oral cavity and saliva. J Dent Res. 1940; 19:315.
Brekhus, P.J. A report of dental caries in 10, 445 university students. J Am Dent Assoc. 1931; 18:1350.
Briner, W.W. Plaque in relation to dental caries and periodontal disease. Int Dent J. 1971; 21:293.
Brodsky, R.H., Schick, B., Vollmer, H., Prevention of dental caries by massive doses of vitamin D. Am J Dis Child. 1941:1183.
Brooks, J.D., Mertz-Fairhurst, E.J., Della-Giustiana, V.E., Williams, J.E., et al. A comparative study of two pit and fissure sealants: three-year results in Augusta, Georgia. J Am Dent Assoc. 1979; 99:42.
Brown, W.E., König, K.G. Cariostatic Mechanisms of Fluoride: proceedings of a workshop organized by the American Dental Association Health Foundation and the National Institute of Dental Research. Caries Res. 11(Suppl 1), 1977.
Brudevold, F., Little, M.F. Effect of certain antienzymes on acid production in plaque. J Dent Res. 1954; 33:703.
Brudevold, F., Little, M.F., Rowley, J. Acid-reducing effect of ‘antienzymes’ in the mouth. J Am Dent Assoc. 1955; 50:18.
Brudevold F, McCann HG, Gron P. Caries resistance as related to the chemistry of the enamel in GEW Wolstenholme and M O’ConnorCaries Resistant Teeth. Little Brown, Boston, 1965
Brunelle, J.A., Carlos, J.P. Changes in the prevalence of dental caries in US schoolchildren, 1961–1980. J Dent Res. 1982; 61:1346.
Bunting, R.W. Studies of the relation of bacillus acidophilus to dental caries. J Dent Res. 1928; 8:222.
Bunting, R.W., Nickerson, G., Hard, D.G. Further studies of the relation of bacillus acidophilus to dental caries. Dent Cosmos. 1926; 68:931.
Buonocore, M.G. Adhesive sealing of pits and fissures for caries prevention with use of ultraviolet light. J Am Dent Assoc. 1970; 80:324.
Buonocore, M.G. Caries prevention in pits and fissures sealed with an adhesive resin polymerized by ultraviolet light: a two year study of a single adhesive application. J Am Dent Assoc. 1971; 82:1090.
Burrill, D.Y., Calandra, J.C., Tilden, E.D., Fosdick, L.S. The effect of 2-methyl-1, 4-naphthoquinone on the incidence of dental caries. J Dent Res. 1945; 24:273.
Chauncey, H.H. Salivary enzymes. J Am Dent Assoc. 1961; 63:360.
Cheyne, V.D., Horne, E.V. The value of the roentgenograph in the detection of carious lesions. J Dent Res. 1948; 27:59.
Clarke, J.K. On the bacterial factor in the aetiology of dental caries. Br J Exp Path. 1924; 5:141.
Clough, O.W. Inhibition of bacterial growth by human saliva. J Dent Res. 1934; 14:164.
Cohen, A., Donzanti, A. Two year clinical study of caries control with high-urea ammoniated dentifrice. J Am Dent Assoc. 1954; 49:185.
Compton, F.H., Burgess, R.C., Mondrow, T.G., Grainger, R.M., et al. The riverdale preschool dental project. J Can Dent Assoc. 1959; 25:478.
Conchie, J.M., McCombie, F., Hole, L.W. Three years of supervised toothbrushing with a fluoridephosphate solution. J Public Health Dent. 1969; 29:11.
Cons, N.C., Janerich, D.T. Albany topical fluoride study: 2 year preliminary report. Int Am Dent Res Abstract. 1969; 545.
Crabb, H.S. Enamel caries: observations on the histology and pattern of progress of the approximal lesion. Br Dent J. 1966; 121:115. [167].
Crabb, H.S. Observations on the histology of the carious attack on enamel and related developmental faults. Adv Fluorine Res. 1966; 4:225.
Crawford, H.M. Clinical results of impregnation. Texas Dent J, 67, 52. 1949.
Crowley, M.C., Rickert, U.G. A method for estimating the bacterial content of the mouth by direct count. J Bacteriol. 1935; 30:395.
Cueto, E.I., Buonocore, M.G. Sealing of pits and fissures with an adhesive resin: its use in caries prevention. J Am Dent Assoc. 1967; 75:121.
Davies, G.N., King, R.M. The effectiveness of an ammonium ion tooth powder in the control of dental caries. J Dent Res. 1951; 30:645.
Day, CDM. Nutritional deficiencies and dental caries in Northern India. Br Dent J. 1944; 70:115. [143].
Deakins, M. Effect of pregnancy on the mineral content of dentin of human teeth. J Dent Res. 1943; 22:198.
Deakins, M., Looby, J. Effect of pregnancy on mineral content of human teeth. Am J Obstet Gynecol. 1943; 6:265.
Dean, H.T. Fluorine and dental caries. Am J Orthod Oral Surg. 1947; 33:49.
Dean, H.T. Fluorine in the control of dental caries. J Am Dent Assoc. 1956; 52:1.
Dean, H.T., Arnold, F.A., Elvove, E. Domestic water and dental caries V: additional studies of the relation of fluoride domestic waters to dental caries experience in 4,425 white children, aged 12 to 14 years, of 13 cities in 4 states. Public Health Rep. 1942; 57:1155.
Dean, H.T., McKay, F.S., Elvove, E. Mottled enamel survey of Bauxite, Arkansas, ten years after a change in the common water supply. Public Health Rep. 1938; 53:1736.
Del, Regato JA. Dental lesions observed after roentgen therapy in cancer of the buccal cavity, pharynx and larynx. Am J Roentgen. 1939; 42:404–410.
DePaola, P.F., Jordan, H.V., Berg, J. Temporary suppression of Streptococcus mutans in humans through topical application of vancomycin. Arch Oral Biol. 1974; 53:108.
DePaola, P.F., Jordan, H.V., Soparkar, P.M. Inhibition of dental caries in school children by topically applied vancomycin. Arch Oral Biol. 1977; 22:187.
DePaola, P.F., Soparkar, P.M., Tavares, M., Allukian, M., Jr. A dental survey of Massachusetts school children. J Dent Res. 1982; 61:1356.
Dragiff, D.A., Karshan, M. Effect of pregnancy on the chemical composition of human dentin. J Dent Res. 1943; 2:261.
Dreizen, S. Diet and dental decay. Postgrad Med. 1968; 43:233.
Dreizen, S., Spies, T.D. Decalcification and discoloration of intact non-carious human tooth crowns. Oral Surg. 1951; 4:388.
Dreizen, S., Spies, T.D. Effectiveness of a chewing gum containing nitrofuran in the prevention of dental caries. J Am Dent Assoc. 1951; 43:147.
Dreizen, S., Greene, H.I., Spies, T.D. In vitro studies of the dental caries inhibiting properties of some selected nitrofuran compounds. J Dent Res. 1949; 28:288.
Dreizen, S., Mann, A.W., Spies, T.D., Skinner, T.A. Prevalence of dental caries in malnourished children: a clinical study. Am J Dis Child. 1947; 74:265.
Easlick K.A., ed. Dental Caries, Mechanism and Present Control Technics as Evaluated at the University of Michigan Workshop. St Louis: CV Mosby, 1948.
East, B.R. Mean annual hours of sunshine and the incidence of dental caries. Am J Public Health. 1939; 29:777.
East, B.R. Relationship of dental caries in city children to sex, age, and environment. Am J Dis Child. 1941; 61:494.
East, B.R., Kaiser, H. Relation of dental caries in rural children to sex, age, and environment. Am J Dis Child. 1940; 60:1289.
Eisenbrandt, L.L. Studies of the pH of saliva. J Dent Res. 1944; 23:363.
Ericsson, Y. Enamel-apatite solubility. Investigations into the calcium phosphate equilibrium between enamel and saliva and its relation to dental caries. Acta Odontol Scand. 1949; 8(Suppl 3):1.
Ericsson, S.Y. Cariostatic mechanisms of fluorides: clinical observations. Caries Res. 1977; 11(Suppl 1):2.
Fejerskov, O., Thylstrup, A., Larsen, M.J. Rational use of fluorides in caries prevention: a concept based on possible cariostatic mechanisms. Acta Odontol Scand. 1981; 39:241.
Finn, S.B., Jamison, H.C. The effect of a dicalcium phosphate chewing gum on caries incidence in children: 30-month results. J Am Dent Assoc. 1967; 74:987.
Fitzgerald, D.B., Stevens, R., Fitzgerald, R.J., Mandel, I.D. Comparative cariogenicity of Streptococcus mutans strains isolated from caries-active and caries-resistant adults. J Dent Res. 1977; 56:894.
Fitzgerald, R.J. The microbial ecology of plaque in relation to dental caries: in H Stiles, W Loesche, and T O’BrienMicrobial aspects of dental caries. Suppl Microbiol Abstr. 1976; 3:849.
Fitzgerald, R.J., Jordan, H.V., Stanley, H.R. Experimental caries and gingival pathologic changes in the gnotobiotic rat. J Dent Res. 1960; 39:923.
Fitzgerald, R.J., Keyes, P.H. Demonstration of the etiologic role of streptococci in experimental caries in the hamster. J Am Dent Assoc. 1960; 61:9.
Fitzgerald, R.J., Zander, H.A., Jordan, H.U. The effects of a penicillin dentifrice on oral lactobacilli. J Am Dent Assoc. 1950; 4:62.
Fleischmann, L. The etiology of dental caries. Dent Cosmos. 1914; 66:1379.
Fleischmann, L. Zur Pathogenese der Zahnkaries. Z Stomatol. 1921; 19:153.
Florestano, H.J. Acidogenic properties of certain oral microorganisms. J Dent Res. 1942; 21:263.
Florestano, H.J., Faber, J.E., James, L.H. Studies of the relationship between diastatic activity of saliva and incidence of dental caries. J Am Dent Assoc. 1941; 28:1799.
Fosdick, L.S. The degradation of sugars in the mouth and the use of chewing gum and vitamin K in the control of dental caries. J Dent Res. 1948; 27:235.
Fosdick, L.S., Fancher, O.E., Calandra, J.C. The effect of synthetic vitamin K on the rate of acid formation in the mouth. Science. 1942; 96:45.
Fosdick, L.S., Calandra, J.C., Blackwell, R.Q., Burrill, J.H. A new approach to the problem of dental caries control. J Dent Res. 1953; 32:486.
Fosdick, L.S., Hutchinson, APW. The mechanism of caries of dental enamel. Ann N Y Acad Sci. 1965; 131:758.
Frank, R.M., Herdly, J., Philippe, E. Acquired dental defects and salivary gland lesions after irradiation for carcinoma. J Am Dent Assoc. 1965; 70:868–883.
Frisbie, H.E. Caries of the dentin. J Dent Res. 1945; 24:195.
Frisbie, H.E., Nuckolls, J. Caries of the enamel. J Dent Res. 1947; 26:181.
Frisbie, H.E., Nuckolls, J., Saunders, JB de CM. Distribution of the organic matrix of the enamel in the human tooth and its relation to the histopathology of caries. J Am Coll Dent. 1944; 11:243.
Gibbons, H.J., Socransky, S.S. Intracellular polysaccharide storage by organisms in dental plaque, its relation to dental caries and microbial ecology of the oral cavity. Arch Oral Biol. 1962; 7:73.
Garn, S.M., Rowe, N.H., Clark, D.C. Parent child similarities in dental caries rates. J Dent Res. 1976; 55:1129.
Gibbons, R.J., Van Houte, J. Bacterial adherence in oral microbial ecology. Annu Rev Microbiol. 1975; 29:19.
Gish, C.W., Mercer, V.H. Child self-application of a zirconium silicate-stannous fluoride anticariogenic paste: clinical results after 1 and 2 years. IADR Abstract 552. 1969.
Gish, C.W., Muhler, J.C. Effect on dental caries in children in a natural fluoride area of combined use of three agents containing stannous fluoride: a prophylactic paste, a solution and a dentifrice. J Am Dent Assoc. 1965; 70:914.
Gish, C.W., Muhler, J.C., Howell, C.L. A new approach to the topical application of fluorides for the reduction of dental caries in children: results at the end of five years. J Dent Child. 1962; 29:65.
Glass, R.L. The First International Conference on the Declining Prevalence of Dental Caries. J Dent Res. 1982; 61:1301. [ed].
Glass, R.L. Secular changes in caries prevalence in two Massachusetts towns. J Dent Res. 1982; 61:1352.
Goadby, K.W. Micro-organisms in dental caries. J Br Dent Assoc. 1900; 21:65.
Gordon, Nikiforuk. Understanding dental caries 2 prevention: basic and clinical aspects. Basel, New York: Karger, 1985; 225–242.
Gottlieb, B. Untersuchungen über die organische Substanzim Schmelz menschlicher. Zahne Ost-Ung Vjschr Zahnheilk. 1915; 31:19.
Gottlieb, B. Dental caries. J Dent Res. 1944; 23:141.
Gottlieb, B. Histopathology of enamel caries. J Dent Res. 1944; 23:169.
Gottlieb, B. New concept of the caries problem and its clinical application. J Am Dent Assoc. 1944; 31:1482. [1489, 1598].
Gottlieb, B., Diamond, M., Applebaum, E. The caries problem. Am J Orthod Oral Surg. 1946; 32:365.
Green, G.E. A bacteriolytic agent in salivary globulin of caries-immune human beings. J Dent Res. 1959; 38:262.
Griffiths, B., Rapp, G.W. The effect of water-soluble chlorophyll on mouth organisms. J Dent Res. 1950; 29:690. [(Abst)].
Grove, C.T., Grove, C.J. Chemical study of human saliva indicating that ammonia is an immunizing factor in dental caries. J Am Dent Assoc. 1935; 22:247.
Gustafsson, B.E., Quensel, C.E., Lanke, L.S., Lundqvist, C., et al. Vipeholm dental caries study. The effect of different levels of carbohydrate intake on caries activity in 436 individuals observed for 5 years. Acta Odontol Scand. 1954; 11:232.
Hadden, W.C. Basic data on health care needs of adults ages 25–74 years, United States, 1971–75 Vital and Health statistics. In: Series 11, Data from the National Health Survey; no 218 DHHS publication no (PHS) 81–1668. Washington DC: Government Printing Office; 1980.
Hardwick, J.L., Manley, E.B. Caries of enamel II: acidogenic caries. Br Dent J. 1952; 92:225.
Harrap, G.J. Assessment of the effect of dentifrices on the growth of dental plaque. J Clin Periodontol. 1974; 1:166.
Harris, R., Beveride, J. Report to the Australian Dental Congress. Dent Abstr, 12. 1967.
Harrison, R.W., Opal, Z.Z. Comparative studies on lactobacilli isolated from the mouth and intestin. J Dent Res. 1944; 23:1.
Harvey, C.R., Kelly, J.E. Decayed, missing and filled teeth among persons 1–74 years, United States 1971–74 Vital and health statistics: Series 11, Data from the National Health Survey; no 223 DHHS publication no (PHS) 81–1673. Washington DC: Government Printing Office, 1981.
Hawes, R.R., Bibby, B.G. Evaluation of a dentifrice containing carbamide and urease. J Am Dent Assoc. 1953; 46:280.
Hazen, S.P., Chilton, N.W., Mumma, R.D., Jr. The problem of root caries I: literature review and clinical description. J Am Dent Assoc. 1973; 86:137.
Healey, H.J., Cheyne, V.D. Comparison of caries prevalence between freshman students in two midwestern universities. J Am Dent Assoc. 1943; 30:692.
Hein, J.W., Shafer, W.G. Chlorophyll as a potential caries-preventive agent. Penn Dent J (Phila. 1949; 16:221.
Helmcke, J.G. Dental caries in the light of electron microscopy. Int Dent J. 1962; 12:322.
Hemmens, E.S., Blayney, J.R., Bradel, S.F. The microbic flora of the dental plaque in relation to the beginning of caries. J Dent, Res. 1946; 25:195.
Henschel, C.J., Lieber, L. Caries incidence reduction by unsupervised used of 27.5% ammonium therapy dentifrice. J Dent Res. 1949; 28:248.
Hill, I.N., Blayney, J.R., Wolf, W. The Evanston dental caries study XI: the caries experience rates of 12, 13- and 14-year-old children after exposure to fluoridated water for fifty-nine to seventy months. J Dent Res. 1955; 34:77.
Hill, T.J. A salivary factor which influences the growth of L acidophilus and is an expression of susceptibility or resistance to dental caries. J Am Dent Assoc. 1939; 26:239.
Hill, T.J. Therapeutic dentifrices: panel discussion. J Am Dent Assoc. 1954; 48:1.
Hill, T.J. The use of penicillin in dental caries control. J Dent Res. 1948; 27:259.
Hill, T.J. Fluoride dentifrices. J Am Dent Assoc. 1959; 59:1121.
Hill, T.J., Kniesner, A.H. Penicillin dentifrice and dental caries experience in children. J Dent Res. 1949; 28:263.
Hill, T.J., Sims, J., Newman, M. The effect of penicillin dentifrice on the control of dental caries. J Dent Res. 1953; 32:448.
Hine, M.K. Prophylaxis, Toothbrushing, and home care of the mouth as caries control measures. In: Easlick K.A., ed. Dental Caries, Mechanism and Present Control Technics as Evaluated at the University of Michigan Workshop. St Louis: CV Mosby, 1948.
Hine, M.K. Some public health aspects of water fluoridation. In: Shaw J.H., ed. Fluoridation as a Public Health Measure. Washington DC: American Association for Advancement of Science, 1948.
Howell, C.L., Gish, G.W., Smiley, R.D., Muhler, J.C. Effect of topically applied stannous fluoride on dental caries experience in children. J Am Dent Assoc. 1955; 50:14.
Hufstader, R.D., Anderson, V.J., Phatak, N., Snyder, M.L. Effect of a selected nitrofuran, furacin, on the oral lactobacillus count. J Dent Res. 1950; 29:794.
Hunt, H.R., Hoppert, C.A., Erwin, W.G. Inheritance of susceptibility to caries in albino rats (Musnorvegicus. J Dent Res. 1944; 23:385.
Janez, John Gabrovsek. Dental Caries. A Dent on Dogma. Part 5, Priory Lodge Education Ltd. 1997.
Jay, P. An anaerobe isolated from dental caries. J Bacteriol. 1927; 14:385.
Jay, P., Voorhees, R.S. B acidophilus and dental caries. Dent Cosmos. 1927; 69:977.
Jay, P., Hadley, F.P., Bunting, R.W., Koehne, M. Observations on relationship of L acidophilus to dental caries in children during experimental feeding of candy. J Am Dent Assoc. 1936; 23:846.
Jenkins, G.N. A critique of the proteolysis-chelation theory of caries. Brit Dent J. 1961; 111:311.
Jenkins, G.N., Wright, D.E. The role of ammonia in dental caries: Part II. Br Dent J. 1951; 90:117.
Johansen, J.R., Gjermo, P., Eriksen, H.M. Effect of 2 years’ use of chlorhexidine-containing dentifrices on plaque, gingivitis and caries. Scand J Dent Res. 1975; 83:288.
Johnson, R.H., Rozanis, J. A reivew of chemotherapeutic plaque control. Oral Surg. 1979; 47:136.
Jordan, H.V., Keyes, P.H. In vitro methods for the study of plaque formation and carious lesions. Arch Oral Biol. 1966; 11:793.
Kammerman, A.M., Starkey, P.E. Nursing caries: a case history. J Ind Dent Assoc. 1981; 60:7.
Karshan, M. Factors in human saliva correlated with the presence and activity of dental caries. J Dent Res. 1935–36; 15:383.
Karshan, M. Do calcium and phosphorus in saliva differ significantly in caries-free and active-caries groups? J Dent Res. 1942; 21:83.
Karshan, M., Krasnow, F., Krejci, L.E. A study of blood and saliva in relation to immunity and susceptibility to dental caries. J Dent Res. 1931; 11:573.
Katz, R.V. Root caries: clinical implications of the current epidemiologic data. Northwest Dent. 1981; 60:306.
Katz, R.V., Hazen, S.P., Chilton, N.W., Mumma, RD Jr. Prevalence and distribution of root caries in an adult population. Caries Res. 1982; 16:265.
Kerr, D.W., Kesel, R.G. Two-year caries control study utilizing oral hygiene and an ammoniated dentifrice. J Am Dent Assoc. 1951; 42:180.
Kesel, R.G. The effectiveness of dentifrices, mouthwashes, and ammonia-urea compounds in the control of dental caries. In: Easlick K.A., ed. Dental Caries, Mechanism and Present Control Technics an Evaluated at the University of Michigan Workshop. St Louis: CV Mosby, 1948.
Kesel, R.G., O’Donnell, J.F., Kirch, E.R., Wach, E.C. The biological production and therapeutic use of ammonia in the oral cavity in relation to dental caries prevention. J Am Dent Assoc. 1946; 33:695.
Keyes, P.H. The infectious and transmissible nature of experimental dental caries. Arch Oral Biol. 1960; 1:304.
Keyes, P.H. Questions raised by the infectious and transmissible nature of experimental caries. Conference on Oral Biology. J Dent Res. 1960 (Abst 9; 39:1086.
Keyes, P.H., Rowberry, S.A., Englander, H.R., Fitzgerald, R.J. Bio-assays of medicaments for the control of dentobacterial plaque, dental caries, and periodontal lesions in Syrian hamsters. J Oral Ther Pharm. 1966; 3:157.
Kirch, E.R., Kesel, R.G., O’Donnell, J.F., Wach, E.C. Amino acids in human saliva. J Dent Res. 1947; 26:297.
Kirchheimer, W.F., Dougals, H.C. The failure of ammonium ions to inhibit the growth of oral lactobacilli. J Dent Res. 1950; 29:320.
Klein, H. The family and dental disease IV: dental disease (DMF) experience in parents and offspring. J Am Dent Assoc. 1946; 33:735.
Klein, H., Knutson, J.W. Studies on dental caries XIII: effect of ammoniacal silver nitrate on caries in the first permanent molar. J Am Dent Assoc. 1942; 29:1420.
Klein, H., Palmer, C.E. Dental caries in brothers and sisters of immune and susceptible children. Milbank Mem Fund Q. 1940; 18:67.
Kligler, I.J. A biochemical study and differentiation of oral bacteria, with special reference to dental caries. J Am Dent Soc. 1915; 10:141. [282, 445].
Klock, B., Krasse, B. The effect of caries preventive measure in children with high numbers of S. mutans and lactobacilli. Scand J Dent Res. 1978; 86:221.
Knutson, J.W. An evaluation of the effectiveness as a caries control measure of the topical application of solutions of fluorides. In: Easlick K.A., ed. Dental Caries, Mechanism and Present Control Technics as Evaluated at the University of Michigan Workshop. St Louis: CV Mosby, 1948.
Knutson, J.W., Armstrong, W.D. The effect of topically applied sodium fluoride on dental caries experience III: report of findings for the third study year. Public Health Rep. 1946; 61:1683.
Krasnow, F. Biochemical analysis of saliva in relation to caries. Dent Cosmos. 1936; 78:301.
Krasnow, F., Oblatt, A.B. Salivary cholesterol. J Dent Res. 1937; 16:151.
Larson, R.H. The effect of EDTA on the pattern of caries development and its association with biologic changes in the rat. J Dent Res. 1959; 38:1207.
Larson, R.H., Zipkin, I., Rubin, M. Effect of administration of EDTA by various routes on dental caries in the rat. Arch Oral Biol. 1961; 5:49.
Lazansky, J.P., Robinson, L., Radofsky, L. Factors influencing the incidence of bacteremias following surgical procedures in the oral cavity. J Dent Res. 1949; 28:533.
Littleton, N.W. Dental Caries and periodontal diseases among: ethiopian civilians. Public Health Rep. 1963; 78:631.
Lobene, R.R., Brion, M., Socransky, S.S. Effect of erythromycin on dental plaque and plaque-forming microorganisms. J Periodontol. 1969; 40:287.
Löe, H., Theilade, E., Jensen, S.B., Schiött, C.R. Expermental gingivitis in man III: the influence of antibiotics on gingival plaque development. J Periodont Res. 1967; 2:282.
Löe, H., von, der Fehr FR, Schiött, C.R. Inhibition of experinental caries by plaque prevention: the effect of chlorhexidine mouthrinses. Scand J Dent Res. 1972; 80:1.
Loesche, W.J. Chemotherapy of dental plaque infections. Oral Sci Rev. 1976; 9:65.
Loesche, W.J., Nafe, D. Reduction of supragingival plaque accumulations in institutionalized Down’s syndrome patients by periodic treatment with topical kanamycin. Arch Oral Biol. 1973; 81:1131.
Loesche, W.J., Hockett, R.N., Syed, S.A. Reduction in proportions of dental plaque streptococci following a 5-day kanamycin treatment. J Periodont Res. 1977; 12:1.
Loesche, W.J., Rowan, J., Straffon, L.H., Loos, P.J. The association of Streptococcus mutans with human dental decay. Infect Immun. 1975; 11:1252.
Ludwick, L.S., Fosdick, L.S. The ammonia content of the mouth. J Dent, Res. 1950; 29:38.
Lunin, M., Mandel, I.D. Clinical evaluation of the penicillin dentifrice. J Am Dent Assoc. 1955; 51:696.
Magitot, E. Treatise on Dental Caries: experimental and therapeutic investigations translated by TH Chandler. Boston: Osgood Houghton, 1878.
Malherbe, M., Ockerse, T. Dental caries in a high and low incidence area in South Africa: a study of possible contributory factors with special reference to diet. S Afr J Med Sci. 1944; 9:75.
Mandel, I.D. Histological, histochemical and other aspects of caries initiation. J Am Dent Assoc. 1955; 51:432.
Mandel, I.D. Dental caries. Am Sci. 1979; 67:680.
Manley, E.B., Hardwick, J.L. Caries of enamel I: the significance of enamel lamellae. Br Dent J. 1951; 91:36.
Mann, A.W., Dreizen, S., Spies, T.D., Hunt, F.M. A comparison of dental caries activity in malnourished and well-nourished patients. J Am Dent Assoc. 1947; 34:244.
Mansbridge, J.N. Heredity and dental caries. J Dent Res. 1959; 38:337.
Matsumiya, S. Recent advances in dental caries research by electron microscopy. Int Dept J. 1962; 12:433.
McClure, F.J. Cariostatic effect of phosphates. Science. 1964; 144:1337.
McClure, F.J., Hewitt, W.L. The relation of penicillin to induced rat dental caries and oral lactobacillus. J Dent Res. 1947; 25:441.
McDonald, R.E. Human saliva: a study of the rate of flow and viscosity and its relationship to dental caries. MS Thesis, Indiana University, 1950.
McHugh WD. Dental Plaque. Churchill Livingstone, Edinburgh, 1970
McIntosh, J., James, W.W., Lazarus-Barlow, P. An investigation into the aetiology of dental caries I: the nature of the destructive agent and the production of artificial caries. Br Dent J. 1922; 43:728.
McKay, F.S. The relation of mottled enamel to caries. J Am Dent Assoc. 1928; 15:1429.
Mellanby, M. Diet and the teeth: an experimental study III: the effect of diet on dental structure and disease in man. Med Research Council Special Rept (191. 1934.
Mellanby, M. Effect of diet on the resistance of teeth to caries. Proc R Soc Med, 16: pt. 1923; 3:74.
Mellanby, M. The relation of caries to the structure of the teeth. Br Dent J. 1923; 44:1.
Miller, W.D. die Mikroorganismen des. Mundhohle Leipzig, 1889.
Miller, W.D. Microorganisms of the Human Mouth. Philadelphia: SS White Publishing Company, 1890.
Miller, W.D. New theories concerning decay of teeth. Dent Cosmos. 1905; 47:1293.
Moulton FR. (ed). Dental Caries and Fluorine American Association for the Advancement of Science. Washington DC, 1946
Muhler, J.C. The effect of a single topical application of stannous fluoride on the incidence of dental caries in adults. J Dent Res. 1958; 37:448.
Muhler, J.C. The effectiveness of stannous fluoride in children residing in an optimal communal fluoride area. J Dent Child. 1960; 27:51.
Muhler, J.C. Stannous fluoride enamel pigmentation evidence of caries arrestment. J Dent Child. 1960; 27:157.
Muhler, J.C. Mass treatment of children with a stannous fluoridezirconium silicate self-administered prophylactic paste for partial control of dental caries. J Am Coll Dent. 1968; 35:45.
Muhler, J.C., Day, H.G. Effect of stannous fluoride, stannous chloride and sodium fluoride on the incidence of dental lesions in rats fed a caries-producing diet. J Am Dent Assoc. 1950; 41:528.
Muhler, J.C.Hine M.K., ed. A Symposium on Preventive Dentistry. St Louis: CV Mosby, 1956.
Muhler, JC. Van Huysen G. Solubility of enamel protected by sodium fluoride and other compounds. J Dent Res. 1947; 26:119.
Muhler, J.C. The effect of a stannous fluoride-containing dentifrice on dental caries in adults. J Dent Res. 1956; 35:49.
Muhler, J.C., Stookey, G.K., Bixler, D. Evaluation of the anticariogenic effect of mixtures of stannous fluoride and soluble phosphates. J Dent Child. 1965; 3:154.
Mummery, J.R. On the relations which dental caries, as discovered amongst the ancient inhabitants of Britain and amongst existing aboriginal races, may be supposed to hold to their food and social condition. Trans Odontol Soc. 1870; 2:7.
National Center for Health Statistics, CS Wilder: dental visits, volume and interval since last visit, United States, 1978–79. Vital and Health Statistics Series 10, No 138, DHHS Pub No (PHS) 82–1566. Government Printing Office, Washington DC, 1982.
Nevin, T.A., Bibby, G.B. The effect of water-soluble chlorophyll on pure cultures of organisms commonly found in the oral cavity. J Dent Res. 1951; 30:469. [Abst].
Newbrun E. Cariology (4th ed). Williams and Wilkins, Baltimore, 1976
Nigel, A.E., Harris, R.S. The effects of phosphates on experimental dental caries: a literature review. J Dent Res. 1964; 43:1123.
Nolte W.A., ed. Oral Microbiology with Basic Microbiology and Immunology. St Louis: CV Mosby, 1982. [4th ed].
Orland, F.J., Blayney, J.R., Harrison, R.W., Reynier, J.A., et al. Experimental caries in germfree rats inoculated with enterococci. J Am Dent Assoc. 1955; 50:254.
Peffley, G.E., Muhler, J.C. The effect of a commercial stannous fluoride dentifrice under controlled brushing habits on dental caries incidence in children: preliminary report. J Dent Res. 1960; 39:871.
Pelton, W.J. The effect of zinc chloride and potassium ferrocyanide as a caries prophylaxis. J Dent Res. 1950; 29:756.
Pickerill, H.P., Champtaluop, S.T. The bacteriology of the mouth in Maori children, being part of an investigation into the cause of immunity to dental disease in the Maori of the Uriwera country, New Zealand. Br Med J. 1913; 2:1482.
Pincus, P. Further tests on human enamel protein. Biochem J. 1948; 42:219.
Pincus, P. Production of dental caries. Br Med J. 1949; 2:358.
Poole, D.F.G., Newman, H.N. Dental plaque and oral health. Nature. 1971; 234:329.
Price, W.A. Eskimo and Indian field studies in Alaska and Canada. J Am Dent Assoc. 1936; 23:417.
Protheroe, D.H. A study to determine the effect of topical application of stannous fluoride on dental caries in young adults. R Can Dent Corps Q. 1962; 3:20.
Rapp, G.W. Fifteen minute caries test. Ill Dent J. 1962; 31:290–295.
Read, T.T., Knowles, E.M. A study of the diet and habits of school children in relation to freedom from or susceptibility to dental caries. Br Dent J. 1938; 64:185.
Restarski, J.S. Incidence of dental caries among pureblooded Samoans. US Naval Med Bull. 1941; 41:1713.
Ripa, L.W. Fluoride rinsing: what dentists should know. J Am Dent Assoc. 1981; 102:477.
Ripa, L.W., Cole, W.W. Occlusal sealing and caries prevention: results 12 months after a single application of adhesive resin. J Den Res. 1970; 49:171.
Ripa, L.W., Leske, G.S., Sposato, A., Rebich, T. NaF solution: results of a demonstration program after four school years. J Am Dent Assoc. 1981; 102:482.
Robinson, HBG. Dental caries and the metabolism of calcium. J Am Dent Assoc. 1943; 30:357.
Robinson, H.B.G. The effect of systemic disease on the caries process: pregnancy, endocrinopathies, osteomalacia, emotional disturbances and others. In: Easlick K.A., ed. Dental Caries, Mechanism and Present Control Technics as Evaluated at the University of Michigan Workshop. St Louis: CV Mosby, 1948.
Rosebury, T., Karshan, M. Dietary habits of Kuskokwim Eskimos with varying degrees of dental caries. J Dent Res. 1937; 16:307.
Rowe N.H., ed. Proceedings of symposium on incipient caries of enamel University of Michigan: School of Dentistry, 1977. [Ann Arbor].
Russell, A.L., Consoazio, C.F., White, C.L. Dental caries and nutrition in Eskimo scouts of the Alaska National Guard. J Dent Res. 1961; 40:594.
Russell, B.G., Bay, L.M. Oral use of chlorhexidine gluconate toothpaste in epileptic children. Scand J Dent Res. 1978; 86:52.
Sampson, WEA. Dental examination of the inhabitants of the Island of Tristan da Cunha. Br Dent J. 1932; 53:397.
Schatz, A., Martin, J.J. Keratin utilization by oral microflora. Proc Pa Acad Sci. 1955; 29:48.
Schatz, A., Martin, J.J. Destruction of bone and tooth by proteolysis-chelation: its inhibition by fluoride and application to dental caries. N Y J Dent. 1960; 30:124.
Schatz, A., Martin, J.J. The proteolysis-chelation theory of dental caries. J Am Dent Assoc. 1962; 65:368.
Schatz, A., Karlson, K.E., Martin, J.J. Destruction of tooth organic matter by oral keratinolytic microorganisms. N Y State Dent J. 1955; 21:438.
Schatz, A., Karlson, K.E., Martin, J.J., Schatz, V. The proteolysis-chelation theory of dental caries. Odontol Revy. 1957; 8:154.
Schatz, A., Karlson, K.E., Martin, J.J., Schatz, V., et al. Some philosophical considerations on the proteolysis-chelation theory of dental caries. Proc Pa Acad Sci. 1958; 32:20.
Schour, I., Massler, M. Dental caries experience in postwar Italy (1945) I: prevalence in various age groups. J Am Dent Assoc. 1947; 35:1.
Schwartz, J. The teeth of the Massai. J Dent Res. 1946; 25:17.
Scott, D.B. A study of the bilateral incidence of carious lesions. J Dent Res. 1944; 23:105.
Scott, D.B., Albright, J.T. Electron microscopy of carious enamel and dentine. Oral Surg. 1954; 7:64.
Sebelius, C.L. Variations in dental caries: rates among white and Negro children. J Am Dent, Assoc. 1944; 31:544.
Sellman, S. The buffer value of saliva and its relation to dental caries. Acta Odontol Scand. 1949; 8:244.
Selvaraj, R.J., Sbarra, A.J. Role of the phagocyte in host-parasite interactions. J Bacteriol. 1967; 94:149–156.
Shafer, W.G., Hein, J.W. Further studies on the effect of chlorophyllin on experimental dental caries. J Dent Res. 1950; 29:666.
Shafer, W.G., Hein, J.W. Further studies on the inhibition of experimental caries by sodium copper chlorophyllin. J Dent Res. 1951; 30:510.
Shannon, I.L. Salivary sodium, potassium and chloride levels in subjects classified as to dental caries experience. J Dent Res. 1958; 37:401.
Shelling, D.H., Anderson, G.M. Relation of rickets and vitamin D to the incidence of dental caries, enamel hypoplasia and malocclusion in children. J Am Dent Assoc. 1936; 23:840.
Ship, I.I., Mickelsen, O. The effects of calcium acid phosphate on dental caries in children: a controlled clinical trial. J Dent Res. 1964; 43:1144.
Shiere, F.R. The effectiveness of a tyrothricin dentifrice in the control of dental caries. J Dent Res. 1957; 36:237.
Silverstone, L.M. The primary translucent zone of enamel caries and of artificial carieslike lesions. Br Dent J. 1966; 120:461.
Snyder, M.L. Laboratory methods in the clinical evaluation of caries activity. J Am Dent Assoc. 1951; 41:400.
Sognnaes, R.F. Advances in Experimental Caries Research. Washington DC: American Association for the Advancement of Science, 1955.
Sognnaes, R.F., Wislocki, G.B. Histochemical observations on enamel and dentine undergoing carious destruction. Oral Surg. 1950; 3:1283.
Stack, M.V. Organic constituents of enamel. J Am Dent Assoc. 1954; 48:297.
Stallard, R.E. A Textbook of Preventive Dentistry (2nd ed. Philadelphia: WB Saunders, 1982.
Stamm, J.W., Banting, D.W. Comparison of root caries prevalence in adults with lifelong residence in fluoridated and non-fluoridated communities. J Dent Res. 1980; 59:405. [Abst].
Stephan, R.M. Relative importance of polysaccharides, disaccharides and monosaccharides in the production of caries. J Am Dent Assoc. 1938; 37:530.
Stephan, R.M. Changes in H-ion concentration on tooth surfaces and in carious lesions. J Am Dent Assoc. 1940; 27:718.
Stephan, R.M. Two factors of possible importance in relation to the etiology and treatment of dental caries and other dental diseases. Science. 1940; 92:578.
Stephan, R.M. The effect of urea in counteracting the influence of carbohydrates on the pH of dental plaques. J Dent Res. 1943; 22:63.
Stephan, R.M. Intra-oral hydrogen-ion concentrations associated with dental caries activity. J Dent Res. 1944; 23:257.
Stephan, R.M. Some local factors in the development of cavities: plaques, acidity, aciduric bacteria, proteolytic bacteria. In: Easlick K.A., ed. Dental Caries, Mechanism and Present Control Technics as Evaluated at the University of Michigan Workshop. St Louis: CV Mosby, 1948.
Stephan, R.M., Miller, B.F. The effect of synthetic detergents on pH changes in dental plaques. J Dent Res. 1943; 22:53.
Stevens, R.H., Mandel, I.D. Streptococcus mutans serotypes in caries-resistant and cariessusceptible adults. J Dent Res. 1977; 56:1044.
Stookey, G.K., Carroll, R.A., Muhler, J.C. The clinical effectiveness of phosphate-enriched breakfast cereals on the incidence of dental caries in children: results after 2 years. J Am Dent Assoc. 1967; 74:752.
Stralfors, A. The acid fermentation in the dental plaques in situ compared with lactobacillus count. J Dent Res. 1948; 27:576.
Stralfors, A. The effect of calcium phosphate on dental caries in school children. J Dent Res. 1964; 43:1137.
Strean, L.F. Vitamin B6 und Zahnkaries Schweiz. Mschr Zahnheilk. 1957; 67:981.
Sullivan, J.H., Storvick, C.A. Correlation of saliva analyses with dental examinations of 574 freshmen at Oregon State College. J Dent Res. 1950; 29:165.
Sumnicht, R.W. Research in preventive dentistry. J Am Dent Assoc. 1969; 79:1194.
Taber, L.B. Sugar and dental caries, a symposium. J Calif Dent Assoc. 1950; 26:3. [ed; May- June].
Tang, J.M., et al. Dental caries prevalence and treatment levels in Arizone preschool children. Public Health Rep. 1997; 112:319–331.
Tank, G., Storvick, C.A. Effect of naturally occurring selenium and vanadium on dental caries. J Dent Res. 1960; 39:473.
Theilade, E., Theilade, J. Role of plaque in the etiology of periodontal disease and caries. Oral Sci Rev. 1976; 9:23.
Thewlis, J. X-ray analysis of teeth. Br J Radiol. 1932; 5:353.
Thewlis, J. X-ray examination of teeth. Br Dent J. 1934; 57:457.
Thylstrup, A., Fejerskov, O. Textbook of clinical cariology. (2nd ed). 1996.
Torell, P., Ericsson, Y. Two-year clinical tests with different methods of local cariespreventive fluorine applications in Swedish school-children. Acta Odontol Scand. 1965; 23:287.
Toverud, G. Decrease in caries frequency in Norwegian children during World War II. J Am Dent Assoc. 1949; 39:127.
Turkheim, H. Salivary content of mucin, ammonia, sodium chloride and calcium. D Monat Zahnh. 1925; 43:897.
Turner, N.C., Crowell, G.E. Dental caries and tryptophane deficiency. J Dent Res. 1947; 26:99.
Underwood, A.S., Milles, W.T. An investigation into the effects of organisms upon the teeth and alveolar portions of the jaws. Trans Int Med Cong (7th Session. 1881; 3:523.
Van, Kesteren M, Bibby, B.G., Berry, G.P. Studies on the antibacterial factors of human saliva. J Bacteriol. 1942; 43:573.
Volker, J.F. Effect of fluorine on solubility of enamel and dentin. Proc Soc Exp Biol Med. 1939; 42:725.
Volker, J.F. The effect of chewing gum on the teeth and supporting structures. J Am Dent Assoc. 1948; 36:23.
Volker, J.F., Pinkerton, D.M. Acid production in saliva-carbohydrate mixtures. J Dent Res. 1947; 26:229.
Volker, J.F., Fosdick, L.S., Manahan, R.D., Manly, R.S. Effect of sodium N-palmitoyl sarcosinate on tooth enamel solubility. Proc Soc Exp Biol Med. 1954; 87:332.
Volker, J.F., Hodge, H.C., Wilson, H.J., van Voorhis, S.M. The absorptionof fluorides by enamel, dentin, bone, and hydroxyapatite as shown by the radioactive isotope. J Biol Chem. 1940; 134:543.
Vratsanos, S.M., Abelson, D.C., Mandel, I.D. Plaque acidogenesis and caries resistance. J Dent Res. 1979; 58:425. [(Abst)].
Wach, E.C., O’Donnell, J.F., Hine, M.K. Effects of a mouth rinse on oral acidogenic bacteria. J Am Dent Assoc. 1942; 29:61.
Wainwright, W.W. Human saliva XV Inorganic phosphorus content of resting saliva of 650 healthy individuals. J Dent Res. 1943; 22:403.
Watanabe, The effect of roentgen irradiation upon the cellular elements in the human saliva. Oral Surg, 4: 89-107, 1951.
Watkins, D.K. Lysosomes and Radiation Injury: In Lysosomes in Biology and Pathology. Dingle JT, Dean RT. New York: North Holland Publishing Co. Amsterdam Oxford, American Elsevier Publishing Co. Inc, 1975;. [eds].
Weisenstein, P., Radike, A., Robinson, HBG. Clinical studies of dental caries in small groups of children; dentifrice, brushing and participation effects. J Dent Res. 1954; 33:690. [(Abst)].
Weddell, J.A., Klein, A.I. Socioeconomic correlation of oral disease in six to thirty six month children. Pediatr Dent. 1981; 3:306–311.
Westbrook, J.L., Miller, A.S., Chilton, N.W., Williams, F.L., et al. Root surface caries: a clinical, histopathologic and microbiographic investigation. Caries Res. 1974; 8:249.
White, B.J., Kniesner, A.H., Hill, T.J. Effect of small amounts of penicillin on the oral bacterial flora. J Dent Res. 1949; 28:267.
White, J., Bunting, R.W. An investigation into the possible relationship of ammonia in the saliva and dental caries. J Am Dent Assoc. 1935; 22:468.
White, J. A comparison of the chemical composition of stimulated and resting saliva of caries-free and caries-susceptible children. Am J Physiol. 1936; 117:529.
Williams, J.L. A contribution to the study of pathology of enamel. Dent Cosmos. 1897; 39:169. [269, 353].
Williams, N.B. Immunization of human beings with oral lactobacilli. J Dent Res. 1944; 23:403.
Wislocki, G.B., Sognnaes, R.F. The organic elements of the enamel V. Histochemical reactions of the organic matter in undecalcified enamel. J Dent Res. 1949; 28:678.
Woldring, M.G. Free amino acids of human saliva: a chromatographic investigation. J Dent Res. 1955; 34:248.
Wright, C.Z., Banting, D.W., Feasby, W.H., The Dorchester dental flossing study: final report. Clin Prev Dent 1979; 1:23 http://www.inspektor.nl/dental/qlfmain.htm
Young, D. Past and present methods and results of sugar analysis of saliva. J Dent Res. 1941; 20:597.
Youngburg, G.E. Salivary ammonia and its relation to dental caries. J Dent Res. 1935–36; 15:247.
Younger, H.B. Clinical results of caries prophylaxis by impregnation. Tex Dent J. 1949; 67:96.
Zander, H.A. The effectiveness of the topical application of silver salts in the control of caries. In: Easlick K.A., ed. Dental Caries, Mechanism and Present Control Technics as Evaluated at the University of Michigan Workshop. St Louis: CV Mosby, 1948.
Zander, H.A. Effect of a penicillin dentifrice on caries incidence in school children. J Am Dent, Assoc. 1950; 40:469.
Zander, H.A., Bibby, B.G. Penicillin and caries activity. J Dent Res. 1947; 26:365.
Zipkin, I. Caries potentiating effect of ethylene diamine tetraacetic acid in the rat. Proc Soc Exp Biol Med. 1953; 82:80.
Ziskin, D.E. The incidence of dental caries in pregnant women. Am J Obstet Gynecol. 1926; 12:710.
Ziskin, D.E., Hotelling, H. Effect of pregnancy, mouth acidity, and age on dental caries. J Dent Res. 1937; 16:507.