The general principles of history taking
An extensive knowledge of medical facts is not useful unless a doctor is able to extract accurate and succinct information from a sick person about his or her illness, and then synthesise the data. This is how you make an accurate diagnosis. In all branches of medicine, the development of a rational plan of management depends on a correct diagnosis or a sensible, differential diagnosis (list of possible diagnoses). Except for patients who are extremely ill, taking a careful medical history should precede both examination and treatment.
Taking the medical history is the first step in making a diagnosis; it will be used to direct the physical examination and will usually determine what investigations are appropriate. More often than not, an accurate history suggests the correct diagnosis, whereas the physical examination and subsequent investigations merely serve to confirm this impression.1,2 Text box 1.1 shows the consultation sequence.
Great diagnosticians have been feted by history and you will see their names live on in this book: Hippocrates, Osler, Mayo, Addison and Cushing to name a few. History taking involves more than listening: you must observe actively (a part of physical examination). Noting the discomfort of a patient who has abdominal pain, for example, will influence the interpretation of the history. Remember that the history is the least-expensive way of making a diagnosis.
Changes in medical education mean that much student teaching is now conducted away from the traditional hospital ward. Students must learn how to take a medical history in any and every setting, but obviously adjustments to the technique must be made for patients seen in busy surgeries or outpatient departments. Much information about a patient’s previous medical history may already be available in hospital or clinic records (some regrettably inaccurately recorded, so be on your guard); the detail needed will vary depending on the complexity of the presenting problem and on whether the visit is a follow-up or a new consultation.
Bedside manner and establishing rapport
History taking requires practice and depends very much on the doctor–patient relationship.3 It is important to try to put the patient at ease immediately, because unless a rapport is established, the history taking is likely to be unrewarding.
Remember that patients tell doctors and even medical students things they would tell no one else. It is essential that these matters be kept confidential as far as possible. There should be no problem in discussing a patient with a colleague, but unless the colleague is directly involved in the patient’s management the patient should not be identified. This applies to discussion of patients and their results at clinical meetings. In open meetings, the patient’s name should be removed from displayed tests and documents.
There is no doubt that the treatment of a patient begins the moment one reaches the bedside or the patient enters the consulting rooms. The patient’s first impressions of a doctor’s professional manner will have a lasting effect. One of the axioms of the medical profession is primum non nocere (the first thing is to cause no harm).4 An unkind and thoughtless approach to questioning and examining a patient can cause harm before any treatment has had the opportunity to do so. You should aim to leave the patient feeling better for your visit. This is a difficult technique to teach.
Much has been written about the correct way to interview patients, but each doctor has to develop his or her own method, guided by experience gained from clinical teachers and patients themselves.5–8 To help establish this good relationship, the student or doctor must make a deliberate point of introducing him- or herself and explaining his or her role (see Figure 1.1). A student might say: ‘Good afternoon, Mrs Evans. My name is Jane Smith. I am Dr Osler’s medical student. She has asked me to come and see you.’ A patient seen at a clinic should be asked to come and sit down, and be directed to a chair. The door should be shut or, if the patient is in the ward, the curtains drawn to provide some privacy. The clinician should sit down beside or near the patient so as to be close to eye level and give the impression that the interview will be an unhurried one.9,10

It is important here to address the patient respectfully, look at him or her (not the computer) and use his or her name and title. Some general remarks about the weather, hospital food or the crowded waiting room may be appropriate to help put the patient at ease, but these must not be patronising.
Obtaining the history
Start with an open-ended question and listen actively—patients will ‘tell you the diagnosis’ if you take the time to listen to the story in their own words and synthesise what they are saying based on your knowledge of pathophysiology.
Allow the patient to tell the story first and avoid the almost overwhelming urge to interrupt. It usually takes only two to three minutes for the patient to run out of steam, but you will have learnt a lot in that short time. Encourage the patient to continue telling you about his or her main problem or problems from the beginning. Then ask specific questions to fill in all the gaps.
At the end of the history and examination, a detailed record is made. However, many clinicians find it useful to make rough notes during the interview. Tell patients you will be doing this but will also be listening to them. With practice, note taking can be done without any loss of rapport. Pausing to make a note of a patient’s answer to a question and engaging his or her eyes directly can help, and indicates that the story is being taken seriously.
Many clinics and hospitals use computer records, which may be displayed on a computer screen on the desk. Notes are sometimes added to these during the interview via a keyboard. It can be very off-putting for a patient when the interviewing doctor looks entirely at the computer screen rather than at the patient. With practice it is possible to enter data while maintaining eye contact with a patient, but at first it is probably preferable to make written notes and transcribe or dictate them later.
The final record must be a sequential, accurate account of the development and course of the illness or illnesses of the patient (see Appendix I, page 571). There are a number of methods of recording this information. Hospitals may have printed forms with spaces for recording specific information. This applies especially to routine admissions (e.g. for minor surgical procedures). Follow-up consultation questions and notes will be briefer than those of the initial consultation; obviously, many questions are only relevant for the initial consultation. When a patient is seen repeatedly at a clinic or in a general practice setting, the current presenting history may be listed as an ‘active’ problem and the past history as a series of ‘inactive’ or ‘still active’ problems.
A sick patient will sometimes emphasise irrelevant facts and forget about very important symptoms. For this reason, a systematic approach to history taking and recording is crucial.11 List 1.1 outlines a history-taking sequence, but the detail required depends on the complexity of the presenting illness.
Introductory questions
In order to obtain a thorough history the clinician must establish a good relationship, interview in a logical manner, listen carefully, interrupt appropriately and usually only after allowing the patient to tell the initial story, note nonverbal clues and correctly interpret the information obtained.
The next step after introducing oneself should be to find out the patient’s major symptoms or medical problems. Asking the patient ‘What brought you here today?’ can be unwise, as it often promotes the reply ‘an ambulance’ or ‘a car’. This little joke wears thin after some years in clinical practice. It is best to attempt a conversational approach and ask the patient ‘What has been the trouble or problem recently?’ or ‘When were you last quite well?’ For a follow-up consultation some reference to the last visit is appropriate, for example: ‘How have things been going since I saw you last?’ or ‘It’s about … weeks since I saw you last, isn’t it? What’s been happening since then?’ This lets the patient know the clinician hasn’t forgotten him or her.
Some have suggested that the clinician begin with questions about more general aspects of the patient’s life. There is a danger that this attempt to establish early rapport will seem intrusive to a person who has come for help about a specific problem, albeit one related to other aspects of life. This type of general and personal information may be better approached once the clinician has shown an interest in the presenting problem or as part of the social history—usually intrusive questions should be deferred to a subsequent consultation when the patient and clinician know each other better. The best approach and timing of this part of the interview will vary, depending on the nature of the presenting problem and the patient’s and clinician’s attitude.
When a patient stops volunteering information, the question ‘What else?’ will usually help start the conversation up again, and can be repeated several times if necessary.8 On the other hand, some direction may be necessary to keep a garrulous patient on track later during the interview.
It is necessary to ask specific questions to test diagnostic hypotheses. For example, the patient may not have noticed an association between the occurrence of chest discomfort and exercise (typical of angina) unless asked specifically. It may also be helpful to give a list of possible answers. A patient with suspected angina who is unable to describe the symptom may be asked if the sensation is sharp, dull, heavy or burning. The reply that it is sharp makes angina less likely.
Appropriate (but not exaggerated) reassuring gestures are of value to maintain the flow of conversation. If the patient stops giving the story spontaneously, it can be useful to provide a short summary of what has already been said and encourage him or her to continue.
The clinician must learn to listen with an open mind.10 The temptation to leap to a diagnostic decision before the patient has had the chance to describe all the symptoms in his or her own words should be resisted. Avoid using pseudo-medical terms and if the patient uses them, find out exactly what is meant by them, as misinterpretation of medical terms is common.
Patients’ descriptions of their symptoms may vary as they are subjected to repeated questioning by increasingly senior medical staff. The patient who has described his chest pain as sharp and left-sided to the medical student may tell the registrar that the pain is dull and in the centre of his chest. These discrepancies come as no surprise to experienced clinicians; they are sometimes the result of the patient having had time to reflect on his or her symptoms. This does mean, however, that very important aspects of the story should be checked by asking follow-up questions, such as: ‘Can you show me exactly where the pain is?’ and ‘What do you mean by sharp?’
Some patients may have medical problems that make the interview difficult for them; these include deafness and problems with speech and memory. These must be recognised by the clinician if the interview is to be successful. See Chapter 2 for more details.
Presenting (principal) symptom
Not uncommonly, a patient has many symptoms. An attempt must be made to decide which symptom led the patient to present. It must be remembered that the patient’s and the doctor’s ideas of what constitutes a serious problem may differ. A patient with symptoms of a cold who also, in passing, mentions that he has recently coughed up blood (haemoptysis) may need more attention to his chest than to his nose. Find out what problem or symptom most concerns the patient. Patients are unlikely to be satisfied with their consultation if the thing that troubles them the most is not dealt with, even if it is a minor problem for which reassurance is all that is required. Record each presenting symptom or symptoms in the patient’s own words, avoiding technical terms at this stage.
Whenever you identify a major complaint or symptom, think of the following as you are trying to unravel the story and ask questions to try to find out:
1. Where is the problem? (probable anatomical diagnosis)
2. What is the nature of the symptom? (likely pathological diagnosis)
3. How does it affect the patient? (physiological and functional diagnosis)
A diagnosis is not just about a name; you are trying to determine the likely disease process so that you can advise the patient of the prognosis and plan management.
History of the presenting illness
Each of the presenting problems has to be talked about in detail with the patient, but in the first part of the interview the patient should lead the discussion. In the second part the doctor should take more control and ask specific questions. When writing down the history of the presenting illness, the events should be placed in chronological order; this might have to be done later when the whole history has been obtained. If numerous systems are affected, the events should be placed in chronological order for each system. Remember, patients may have multiple problems, some that are interdependent and some not. In the older person multiple problems are the rule, not the exception. Your job is to identify them all accurately and create a full medical picture of the individual.
CURRENT SYMPTOMS
Certain information should routinely be sought for each current symptom if this hasn’t been volunteered by the patient. The mnemonic SOCRATES summarises the questions that should be asked about most symptoms:
Site
Ask where the symptom is exactly and whether it is localised or diffuse. Ask the patient to point to the actual site on the body.
Some symptoms are not localised. Patients who complain of dizziness do not localise this to any particular site—but vertigo may sometimes involve a feeling of movement within the head and to that extent is localised. Other symptoms that are not localised include cough, shortness of breath (dyspnoea) and change in weight.
Onset (mode of onset and pattern)
Find out whether the symptom came on rapidly, gradually or instantaneously. Some cardiac arrhythmias are of instantaneous onset and offset. Sudden loss of consciousness (syncope) with immediate recovery occurs with cardiac but not neurological disease. Ask whether the symptom has been present continuously or intermittently. Find out whether the symptom is getting worse or better, and, if so, when the change occurred. For example, the exertional breathlessness of chronic obstructive pulmonary disease may come on with less and less activity as it worsens. Find out what the patient was doing at the time the symptom began. For example, severe breathlessness that wakes a patient from sleep is very suggestive of cardiac failure.
Character
Here it is necessary to ask the patient what is meant by the symptom; to describe its character. If the patient complains of dizziness, does this mean the room spins around (vertigo) or is it more a feeling of impending loss of consciousness? Does indigestion mean abdominal pain, heartburn, fullness after eating, excess wind or a change in bowel habit? If there is pain, is it sharp, dull, stabbing, boring, burning or cramp-like?
Radiation of pain or discomfort
Determine whether the symptom, if localised, radiates; this mainly applies if the symptom is pain. Certain patterns of radiation are typical of a condition or even diagnostic, e.g. the nerve root distribution of pain associated with herpes zoster (shingles).
Alleviating factors
Ask whether anything makes the symptom better. For example, the pain of pericarditis may be relieved when a patient sits up, while heartburn from acid reflux may be relieved by drinking milk or taking an antacid. Have analgesic medications been used to control the pain? Have narcotics been required?
Timing
Find out when the symptom first began and try to date this as accurately as possible. For example, ask the patient what the first thing was that he or she noticed was ‘unusual’ or ‘wrong’. Ask whether the patient has had a similar illness in the past. It is often helpful to ask patients when they last felt entirely well. In a patient with long-standing symptoms, ask why he or she decided to see the doctor at this time.
Exacerbating factors
Ask whether anything makes the symptom worse. The slightest movement may exacerbate the abdominal pain of peritonitis or the pain in the big toe caused by gout.
Severity
This is subjective. The best way to assess severity is to ask the patient whether the symptom interferes with normal activities or sleep. Severity can be graded from mild to very severe. A mild symptom can be ignored by the patient, while a moderate symptom cannot be ignored but does not interfere with daily activities. A severe symptom interferes with daily activities, while a very severe symptom markedly interferes with most activities. Alternatively, pain or discomfort can be graded on a 10-point scale from 0 (no discomfort) to 10 (unbearable). (However, asking patients who are in severe pain to provide a number out of 10 seems at best a distraction and at worst rather unkind.) A face scale using pictures of different faces to represent pain severity from no pain (0) to very much pain (10) can be useful in practice.12
A number of other methods of quantifying pain are available (e.g. the visual analogue scale, whereby the patient is asked to mark the severity of pain on a 10-centimetre horizontal line). Note that all of these scales are more useful for comparing the subjective severity of pain over time than for absolute severity—for example, comparing before and after certain treatment has been started.
The severity of some symptoms can be quantified more precisely; for example, shortness of breath on exertion occurring after walking 10 metres on flat ground is more severe than shortness of breath occurring after walking 90 metres up a hill. Central chest pain from angina occurring at rest is more significant than angina occurring while running 90 metres to catch a bus.
It is relevant to quantify the severity of each symptom—but also to remember that symptoms a patient considers mild may be very significant.
ASSOCIATED SYMPTOMS
Here an attempt is made to uncover in a systematic way symptoms that might be expected to be associated with disease of a particular area. Initial and most thorough attention must be given to the system that includes the presenting problem (see Questions box 1.1, pages 14–16). Remember that while a single symptom may provide the clue that leads to the correct diagnosis, usually it is the combination of characteristic symptoms that most reliably suggests the diagnosis.
Questions box 1.1
Enquire about common symptoms and three or four of the common disorders in each major system listed below. Not all of these questions should be asked of every patient. Adjust the detail of questions based on the presenting problem, the patient’s age and the answers to the preliminary questions.
 denotes symptoms for the possible diagnosis of an urgent or dangerous (alarm) problem.
denotes symptoms for the possible diagnosis of an urgent or dangerous (alarm) problem.
1. Have you had any pain or pressure in your chest, neck or arm? (Myocardial ischaemia)
2. Are you short of breath on exertion? How much exertion is necessary?
3. Have you ever woken up at night short of breath? (Cardiac failure)
4. Can you lie flat without feeling breathless?
5. Have you had swelling of your ankles?
6. Have you noticed your heart racing or beating irregularly?
7. Have you had blackouts without warning? (Stokes-Adams attacks)
8. Have you felt dizzy or blacked out when exercising? (Severe aortic stenosis or hypertrophic cardiomyopathy)
9. Do you have pain in your legs on exercise?
10. Do you have cold or blue hands or feet?
11. Have you ever had rheumatic fever, a heart attack or high blood pressure?
1. Are you ever short of breath? Has this come on suddenly? (Pulmonary embolism)
3. Is your cough associated with shivers and shakes (rigors) and breathlessness and chest pain? (Pneumonia)
5. Have you coughed up blood? (Bronchial carcinoma)
6. What type of work have you done? (Occupational lung disease)
7. Do you snore loudly? Do you fall asleep easily during the day? When? Have you fallen asleep while driving? Obtain a sleep history.
8. Do you ever have wheezing when you are short of breath?
1. Are you troubled by indigestion? What do you mean by indigestion?
3. Have you had any difficulty swallowing? (Oesophageal cancer)
4. Have you had vomiting, or vomited blood? (Gastrointestinal bleeding)
5. Have you had pain or discomfort in your abdomen?
6. Have you had any abdominal bloating or distension?
7. Has your bowel habit changed recently? (Carcinoma of the colon)
8. How many bowel motions a week do you usually pass?
9. Have you lost control of your bowels or had accidents (faecal incontinence)?
10. Have you seen blood in your motions? (Gastrointestinal bleeding)
11. Have your bowel motions been black? (Gastrointestinal bleeding)
12. Have you lost weight recently without dieting? (Carcinoma of the colon)
13. Have your eyes or skin ever been yellow?
14. Have you ever had hepatitis, peptic ulceration, colitis or bowel cancer?
1. Do you have difficulty or pain on passing urine?
2. Is your urine stream as good as it used to be?
3. Is there a delay before you start to pass urine? (Applies mostly to men)
4. Is there dribbling at the end?
5. Do you have to get up at night to pass urine?
6. Are you passing larger or smaller amounts of urine?
7. Has the urine colour changed?
8. Have you seen blood in your urine? (Urinary tract malignancy)
9. Have you any problems with your sex life? Difficulty obtaining or maintaining an erection?
10. Have you noticed any rashes or lumps on your genitals?
11. Have you ever had a sexually transmitted disease?
12. Have you ever had a urinary tract infection or kidney stone?
14. Do you have excessive pain or bleeding with your periods?
2. Have you had fevers, or shivers and shakes (rigors)?
3. Do you have difficulty stopping a small cut from bleeding? (Bleeding disorder)
4. Have you noticed any lumps under your arms, or in your neck or groin? (Haematological malignancy)
5. Have you ever had blood clots in your legs or in the lungs?
1. Do you have painful or stiff joints?
2. Are any of your joints red, swollen and painful?
3. Have you had a skin rash recently?
4. Do you have any back or neck pain?
5. Have your eyes been dry or red?
6. Have you ever had a dry mouth or mouth ulcers?
7. Have you been diagnosed as having rheumatoid arthritis or gout?
8. Do your fingers ever become painful and become white and blue in the cold?
1. Have you noticed any swelling in your neck?
3. Do you prefer hot or cold weather?
4. Have you had a thyroid problem or diabetes?
5. Have you noticed increased sweating?
6. Have you been troubled by fatigue?
7. Have you noticed any change in your appearance, hair, skin or voice?
8. Have you been unusually thirsty lately? Or lost weight? (New onset of diabetes)
Reproductive and breast history (women)
1. How many pregnancies have you had?
2. Have you had any miscarriages?
3. Have you had high blood pressure or diabetes in pregnancy?
4. Were there any other complications during your pregnancies or deliveries?
5. Have you had a Caesarean section?
6. Have you had any bleeding or discharge from your breasts or felt any lumps there? (Carcinoma of the breast)
Neurological system and mental state
2. Is your headache very severe and did it begin very suddenly? (Subarachnoid haemorrhage)
3. Have you had fainting episodes, fits or blackouts?
4. Do you have trouble seeing or hearing?
6. Have you had weakness, numbness or clumsiness in your arms or legs?
7. Have you ever had a stroke or head injury?
8. Have you had difficulty sleeping?
9. Do you feel sad or depressed, or have problems with your ‘nerves’?
1. Have you had problems with falls or loss of balance? (High fracture risk)
2. Do you walk with a frame or stick?
3. Do you take sleeping tablets or sedatives? (Falls risk)
4. Do you take blood pressure tablets? (Postural hypotension and falls risk)
5. Have you been tested for osteoporosis?
6. Can you manage at home without help?
7. Are you affected by arthritis?
8. Have you had problems with your memory or with managing things like paying bills? (Cognitive decline)
9. How do you manage your various tablets? (Risk of polypharmacy and confusion of doses)
THE EFFECT OF THE ILLNESS
A serious illness can change a person’s life—for example, a chronic illness may prevent work or further education. The psychological and physical effects of a serious health problem may be devastating and, of course, people respond differently to similar problems. Even after full recovery from a life-threatening illness, some people may be permanently affected by loss of confidence or self-esteem. There may be continuing anxieties about the capability of supporting a family. Try to find out how the patient and his or her family have been affected. How has the patient coped so far, and what are his or her expectations and hopes for the future with regard to health? What explanations of the condition has the patient been given or obtained (e.g. from the internet)?
Helping a patient to manage ill-health is a large part of the clinician’s duty. This depends on sympathetic and realistic explanations of the probable future course of the disease and the effects of treatment.
Drug and treatment history
Ask the patient whether he or she is currently taking any tablets or medicines (the use of the word ‘drug’ may cause alarm); the patient will often describe these by colour or size rather than by name and dose. Then ask the patient to show you all his or her medications (see Figure 1.2), if possible, and list them. Note the dose, length of use, indication for each drug and any side effects.

Figure 1.2 (a) Medications packed for hospital discharge. (b) A Webster packet; medications packed for the patient by the pharmacy by time and day of the week
This drug list may provide a useful clue to chronic or past illnesses, otherwise forgotten. For example, a patient who denies a history of high blood pressure may remember when asked why he or she is taking an anti-hypertensive drug having an elevated blood pressure in the past. Remember that some drugs are prescribed as transdermal patches or subcutaneous implants (e.g. contraceptives and hormonal treatment of carcinoma of the prostate). Ask whether the drugs were taken as prescribed. Always ask specifically whether a woman is taking the contraceptive pill, because many who take it do not consider it a medicine or tablet. The same is true of inhalers, or what many patients call their ‘puffers’.
To remind the patient, it is often worthwhile to ask about the use of classes of drugs. A basic list should include questions about treatment for blood pressure, high cholesterol, diabetes, arthritis, anxiety or depression, erectile dysfunction (no longer called impotence), contraception, hormone replacement, epilepsy and anticoagulation and the use of antibiotics. Also ask if the patient is taking any over-the-counter preparations (e.g. aspirin, antihistamines, vitamins). Aspirin and standard non-steroidal anti-inflammatory drugs (NSAIDs), but not paracetamol (acetaminophen), can cause gastrointestinal bleeding. Patients with chronic pain may consume large amounts of analgesics, including drugs containing opioids such as codeine and morphine. A careful history of the period of use of opioids and the quantities used is important, because they are drugs of dependence.
Many patients have printed copies of parts of their electronic records with lists of drugs. Unless these are updated regularly, they tend to contain names of drugs the patient no longer uses. Ask about each drug on the list—whether it is still being taken and what it is for. It is very common for patients to say they have not used certain drugs on their list for years. Update the list for the patient if you are in charge of his or her care.
There may be some medications or treatments the patient has had in the past which remain relevant. These include corticosteroids, chemotherapeutic agents (anti-cancer drugs) and radiotherapy. Often patients, especially those with a chronic disease, are very well informed about their condition and their treatment. However, some allowance must be made for patients’ non-medical interpretation of what happened.10
Note any adverse reactions in the past. Also ask specifically about any allergy to drugs (often a skin reaction or episode of bronchospasm) and what the allergic reaction actually involved, to help decide if it was really an allergic reaction.13 Patients often confuse an allergy with a side effect of a drug.
Approximately 50% of people now use ‘natural remedies’ of various types. They may not feel that these are a relevant part of their medical history, but these chemicals, like any drug, may have adverse effects. Indeed, some have been found to be adulterated with drugs such as steroids and NSAIDs. More information about these substances and their effects is becoming available and there is an increasing responsibility for clinicians to be aware of them and to ask about them directly.
Ask about ‘recreational’ or street drug use. The use of intravenous drugs has many implications for the patient’s health. Ask whether any attempt has been made to avoid sharing needles. This may protect against the injection of viruses, but not against bacterial infection from the use of impure substances. Cocaine use has become a common cause of myocardial infarction in young people in some countries. Acutely ill patients may have taken overdoses of drugs whose purity has been underestimated (especially narcotics) or taken drugs without knowing what they are. The use of amphetamine-like drugs at parties can be associated with dehydration with electrolyte abnormalities and psychotic symptoms. Here an attempt to find out more detail from the patient or other party-goers is essential.
Not all medical problems are treated with drugs. Ask about courses of physiotherapy or rehabilitation for musculoskeletal problems or injuries, or to help recovery following surgery or a severe illness. Certain gastrointestinal conditions are treated with dietary supplements (e.g. pancreatic enzymes for chronic pancreatitis) or restrictions (e.g. of gluten for coeliac disease).
Past history
Some patients may feel that questions about past problems and the more general questions asked in the systems review (page 14) are somewhat intrusive. It may be best to preface these questions by saying something like, ‘I need to ask you some questions about your past medical problems and general health. These may affect your current investigations and treatment.’
Ask the patient whether he or she has had any serious illnesses, operations or admissions to hospital in the past, including any obstetric or gynaecological problems. Where relevant obtain the details. Do not forget to enquire about childhood illnesses. Ask about past blood transfusion (including when and what for). Serious or chronic childhood illnesses may have interfered with a child’s education and social activities like sport. Ask what the patient remembers and thinks about this.
Previous illnesses or operations may have a direct bearing on the patient’s current health. It is worth asking specifically about certain operations that have a continuing effect on the patient’s health; for example, operations for malignancy, bowel surgery or cardiac surgery, especially valve surgery. Implanted prostheses are common in surgical, orthopaedic and cardiac procedures. These may involve a risk of infection of the foreign body, while magnetic metals—especially most cardiac pacemakers—are a contraindication to magnetic resonance imaging (MRI). Chronic kidney disease may be a contraindication to X-rays using iodine contrast materials and MRI scanning using gadolinium contrast. Pregnancy is usually a contraindication to radiation exposure (X-rays and nuclear scans—remember that CT scans cause hundreds of times the radiation exposure of simple X-rays).
The patient may believe that he or she has had a particular diagnosis made in the past, but careful questioning may reveal this as unlikely. For example, the patient may mention a previous duodenal ulcer, but not have had any investigations or treatment for it, which makes the diagnosis less certain. Therefore, it is important to obtain the particulars of each relevant past illness, including the symptoms experienced, tests performed and treatments prescribed. The mature clinician needs to maintain an objective scepticism about the information that is obtained from the patient.
Patients with chronic illnesses may have had their condition managed with the help of various doctors and at specialised clinics. For example, patients with diabetes mellitus are often managed by a team of health professionals including diabetic educators, nurses and dieticians. Find out what supervision and treatment these have provided. For example, who does the patient contact if there is a problem with the insulin dose, and does the patient know what to do (an action plan) if there is an urgent or a dangerous complication? Patients with chronic diseases are often very much involved in their own care and are very well informed about aspects of their treatment. For example, diabetics should keep records of their home-measured blood sugar levels, heart failure patients should monitor their weight daily and so on. These patients will often make their own adjustments to their medication doses. Assessing a patient’s understanding of and confidence in making these changes should be part of the history taking.
It should be routine to find out whether the adult patient has had the usual immunisations (e.g. mumps, measles, rubella, tetanus etc) as well as other recent immunisations (e.g. for human papilloma virus [HPV], hepatitis B, pneumococcal disease, Haemophilus influenzae or influenza).
MENSTRUAL HISTORY
For women, a menstrual history should be obtained; it is particularly relevant for a patient with abdominal pain, a suspected endocrine disease or genitourinary symptoms. Write down the date of the last menstrual period. Ask about the age at which menstruation began, whether the periods are regular or whether menopause has occurred. Ask whether the symptoms occur at a particular time in the menstrual cycle. Do not forget to ask a woman of childbearing age if there is a possibility of pregnancy; this, for example, may preclude the use of certain investigations or drugs.14 Observing the well-known axiom that ‘every woman of childbearing years is pregnant until proven otherwise’ can prevent unnecessary danger to the unborn child and avoid embarrassment for the unwary clinician. Ask about any miscarriages. Record gravida (the number of pregnancies) and para (the number of births of babies over 20 weeks’ gestation).
Social history
This is the time to find out more about the patient as a person. The questions should be asked in an interested and conversational way and should not sound like a routine learned by rote. For example, chronic pain can affect relationships, employment, income and leisure activities, and it is your job to understand these matters in order to provide the best possible care plan.
UPBRINGING AND EDUCATION LEVEL
Ask first about the places of birth and residence, and the level of education obtained (including problems with schooling caused by childhood illnesses). This can influence the way things need to be explained to the patient. Recent migrants may have been exposed to infectious diseases like tuberculosis; ethnic background is important in some diseases, such as thalassaemia and sickle cell anaemia.
MARITAL STATUS, SOCIAL SUPPORT AND LIVING CONDITIONS
To determine the patient’s marital status, ask who is living at home with the patient. Find out about the health of the spouse and any children. Check if there are any other household members. Establish who is the patient’s main ‘caregiver’. ‘Matter of fact’ questions about sexual activity may be very relevant. For example, erectile dysfunction may occur in neurological conditions, debilitating illness or psychiatric disease. Questions about living arrangements are particularly important for chronic or disabling illnesses, where it is necessary to know what social support is available and whether the patient is able to manage at home (e.g. the number of steps required to access the house, or the location of the toilet).
Ask if the patient considers him- or herself to be a spiritual person. Spirituality is an important factor, especially in the care of dying patients, in the creation of living wills and in understanding the support network available for the patient.
The presence of pets in the home may be important if infections or allergies are suspected.
Ask about mobility; for example, if an adult patient is still driving and how he or she gets to the shops and appointments.
DIET AND EXERCISE
Ask about the adequacy of the patient’s diet, who does the cooking, the availability of ‘meals on wheels’ and other services such as house cleaning. Also ask how physically active the patient is.
OCCUPATION AND HOBBIES
Ask the patient about present occupation;15 the WHACS mnemonic is useful here:16
Finding out exactly what the patient does at work can be helpful, as some occupations (and hobbies) are linked to disease (see Text box 1.2). Note particularly any work exposure to dusts, chemicals or disease; for example, mine and industrial workers may have the disease asbestosis. Find out if any similar problems have affected fellow workers. Checking on hobbies can also be informative (e.g. bird fanciers and lung disease; use of solvents).
OVERSEAS TRAVEL
If an infectious disease is a possibility, ask about recent overseas travel, destinations visited and how the patient lived when away (e.g. did he or she drink unbottled water and eat local foods, or dine at expensive international hotels?). Ask about the patient’s immunisation status and whether any prophylactic drugs (e.g. for malaria) were taken during the travel period.
SMOKING
The patient may claim to be a non-smoker if he or she stopped smoking that morning. Therefore, ask whether the patient has ever smoked and, if so, how many cigarettes (or cigars or pipes) were smoked a day and for how many years. Find out whether the patient has stopped smoking and, if so, when this was. It is necessary to ask how many packets of cigarettes per day the patient has smoked and for how many years the patient has smoked. An estimate should be made of the number of packet-years of smoking. Remember that this estimate is based on 20-cigarette packetsa and that packets of cigarettes are getting larger; curiously, most manufacturers now make packets of 30 or 35. More recently, giant packets of 50 have appeared: these are too large to fit into a pocket and must be carried in the hands as a constant reminder to the patient of his or her addiction.
Cigarette smoking is a risk factor for vascular disease, chronic lung disease, several cancers and peptic ulceration, and may damage the fetus (see List 1.2). The more recent the exposure and the greater the number of packet-years, the greater the risk of these problems becomes. Cigar and pipe smokers typically inhale less smoke than cigarette smokers and overall mortality rates are correspondingly lower in this group, except from carcinoma of the oral cavity, larynx and oesophagus.
ALCOHOL USE
Ask whether the patient drinks alcohol.17 If so, ask what type, how much and how often. Excessive use of alcohol is common in the community; if the patient claims to be a social drinker, find out exactly what this means. In a glass of wine, a nip (or shot) of spirits, a glass of port or sherry or a 200 mL (7 oz) glass of beer there are approximately 8–10 g of alcohol (1 unit = 8 g).
Guidelines for safe drinking levels vary around the world.18 The National Health & Medical Research Council (NHMRC) in Australia recommends a maximum alcohol intake of no more than 2 standard drinks per day on average and no more than 4 standard drinks on a single day with two alcohol-free days per week.19 In the United Kingdom, the current recommended safe limits are 21 units (168 g of ethanol) per week for men and 14 units (112 g of ethanol) for women; weekly consumption of more than 50 units for men and 35 units for women is considered to place the user in a high-risk group. In the United States, the National Institute on Alcohol Abuse and Alcoholism (NIAAA) suggests that the following alcohol levels are harmful: for men under the age of 65, an average of more than 14 standard drinks per week (or more than 4 drinks on any day); and for women and all adults 65 years and older an average of more than 7 standard drinks per week. Alcohol becomes a major risk factor for liver disease in men who consume more than 80 g daily and women who consume more than 40 g daily for 5 years or longer.
Alcoholics are notoriously unreliable about describing their alcohol intake, so it may be important to suspend belief and sometimes (with the patient’s permission) talk to relatives.
Certain questions can be helpful in making a diagnosis of alcoholism; these are referred to as the CAGE questions:20
Have you ever felt you ought to Cut down on your drinking?
Have people Annoyed you by criticising your drinking?
Have you ever felt bad or Guilty about your drinking?
Have you ever had a drink first thing in the morning to steady your nerves or get rid of a hangover? (Eye opener)
If the patient answers ‘yes’ to any two of these questions, this suggests that he or she has a serious alcohol dependence problem (77% sensitivity, 79% specificity), but the screening often misses unhealthy alcohol use.
A more useful screening test to identify unhealthy drinking comprises three simple questions (AUDIT-C):
1. How often do you have a drink containing alcohol?
2. How many drinks containing alcohol do you have on a typical day when you are drinking alcohol?
3. How often do you have 6 or more alcoholic drinks on one occasion?
Each question is scored from 0 (never) to 4 (4 or more times per week). Positive scores for unhealthy (excess) drinking are:
• 3 or more for women (73% sensitivity, 91% specificity)
• 4 or more for men (86% sensitivity, 89% specificity).21
An even simpler screening question is to ask, ‘How many times in the past year have you had 5 (for men; 4 for women) or more drinks in a day?’ A score of over 0 (or ‘I don’t remember’) suggests alcohol use in the unhealthy range. This question performs almost as well as the AUDIT-C screening.22
The complications of alcohol abuse are summarised in List 1.3.
ANALGESICS AND STREET DRUGS
Over-the-counter analgesics can cause harm—for example, if an alcoholic has just a bit too much paracetamol it may lead to acute liver failure.
Ask whether the patient has ever used marijuana, has tried other street drugs or has ever shot up. An excellent screening question that is 100% sensitive (and 74% specific) is to ask, ‘How many times in the past year have you used an illegal drug or used a prescription medication for non-medical reasons?’23 Asking about ‘recreational’ or street drug use, if not already known, is important.
MOOD
Depression severe enough to cause distress to a patient is common: it has a prevalence of up to 8%.24 Depression can be the result of any significant medical illness; in fact, the incidence of depression increases threefold for these patients. Patients with underlying depression may find illness more difficult to cope with or even develop somatisation disorders (see page 20). Questioning patients about depression can be difficult. A common approach is to ask first, ‘How are things going at home and at work at the moment?’ Questions about depressed mood (see page 20) and anhedonia (loss of interest or pleasure in activities previously enjoyed) can be helpful. Major depression is unlikely if the answer to these questions is ‘no’.
Certain medical conditions such as hypothyroidism or Cushing’s disease can be direct causes of depression.
If depression seems likely, detailed questions about suicide risk should be asked. There is no evidence that asking such questions increases the risk of suicide (see page 24).25
SEXUAL HISTORY
The sexual history may be relevant; if so, specific questions should be asked (see page 20).
Family history
Many diseases run in families. For example, ischaemic heart disease that has developed at a young age in parents or siblings is a major risk factor for ischaemic heart disease in their offspring. Various malignancies, such as breast and large-bowel carcinoma, are more common in certain families. Both genetic and common environmental exposures may explain these familial associations. Some diseases (e.g. haemophilia) are directly inherited.26 Patient reporting of a family history of malignancy is not always accurate. However, two important cancers—bowel and breast—are accurately reported by patients.
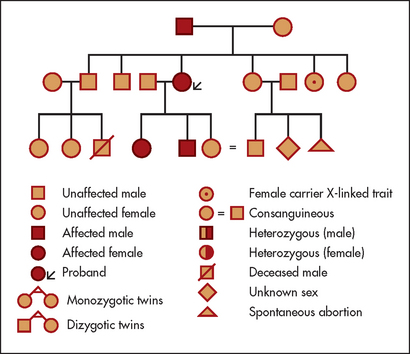
Ask about any history of a similar illness in the family. Enquire about the health and, if relevant, the causes of death and ages of death of the parents and siblings. If there is any suggestion of a hereditary disease, a complete family tree should be compiled showing all members affected (see Figure 1.3). Patients can be reluctant to mention that they have relatives with mental illness, epilepsy or cancer, so ask tactfully about these diseases. Consanguinity (usually first cousins marrying) increases the probability of autosomal recessive abnormalities in the children; ask about this if the pedigree is suggestive.
Systems review
As well as detailed questioning about the system likely to be diseased, it is essential to ask about important symptoms and disorders in other systems (see Questions box 1.1), otherwise important diseases may be missed.27,28 An experienced clinician will perform a targeted systems review, based on information already obtained from the patient; clearly it is not realistic to ask anyone all of the listed questions.
When recording the systems review, list important negative answers (‘relevant negatives’). Remember: if other recent symptoms are unmasked, more details must be sought; relevant information is then added to the history of the presenting illness.
Before completing the history, it is often valuable to ask what the patient thinks is wrong and what he or she is most concerned about. General and sympathetic questions about the effect of a chronic or severe illness on the patient’s life are important for establishing rapport and for finding out what else might be needed (both medical and non-medical) to help the patient.
Major presenting symptoms for each system are described in the following chapters. Examples of supplementary important questions to ask about past history, social history and family history are also given there for each system.
Skills in history-taking
Your aim should be to obtain information that will help establish the likely anatomical and physiological disturbances present, the aetiology of the presenting symptoms and the impact of the symptoms on the patient’s ability to function.29 (In Chapter 2, some advice on how to take the history in more challenging circumstances is considered.) This type of information will help you plan the diagnostic investigations and treatment, and to discuss the findings with, or present them to, a colleague if necessary. First, however, a comprehensive and systematic physical examination is required.
These skills can be obtained and maintained only by practice.30
References
1. Longson, D. The clinical consultation. J R Coll Physicians Lond. 1983; 17:192–195. [Outlines the principles of hypothesis generation and testing during the clinical evaluation.].
2. Nardone, DA, Johnson, GK, Faryna, A, et al. A model for the diagnostic medical interview: nonverbal, verbal and cognitive assessments. J Gen Intern Med. 1992; 7:437–442. [Verbal and nonverbal questions and diagnostic reasoning are reviewed in this useful article.].
3. Bellet, PS, Maloney, MJ. The importance of empathy as an interviewing skill in medicine. JAMA. 1991; 266:1831–1832. Distinguishes between empathy, reassurance and patient education.
4. Brewin, T. Primum non nocere. Lancet. 1994; 344:1487–1488. [Reviews a key principle in clinical management.].
5. Platt, FW, McMath, JC. Clinical hypocompetence: the interview. Ann Intern Med. 1979; 91:898–902. [A valuable review of potential flaws in interviewing, condensed into five syndromes: inadequate content, database flaws, defects in hypothesis generation, failure to obtain primary data and a controlling style.].
6. Coulehan, JL, et al. ‘Tell me about yourself’: the patient-centred interview. Ann Intern Med. 2001; 134:1079–1084.
7. Fogarty, L, et al. Can 40 seconds of compassion reduce patient anxiety. J Clin Oncol. 1999; 17:371–379.
8. Barrier, P, et al. Two words to improve physician–patient communication: what else. Mayo Clin Proc. 2003; 78:211–214. [Ask ‘What else?’ whenever the interview pauses to obtain an optimal history.].
9. Blau, JN. Time to let the patient speak. BMJ. 1999; 298:39. [The average doctor’s uninterrupted narrative with a patient lasts less than 2 minutes (and often much less!), which is too brief. Open interviewing is vital for accurate history taking.].
10. Smith, RC, Hoppe, RB. The patient’s story: integrating the patient- and physician-centered approaches to interviewing. Ann Intern Med. 1991; 115:470–477. [Patients tell stories of their illness, integrating both the medical and psychosocial aspects. Both need to be obtained, and this article reviews ways to do this and to interpret the information.].
11. Beckman, H, Markakis, K, Suchman, A, Frankel, R. Getting the most from a 20-minute visit. Am J Gastroenterol. 1994; 89:662–664. [A lot of information can be obtained from a patient, even when time is limited, if the history is taken logically.].
12. Tomlinson, D, von Baeyer, CL, Stinson, JN, Sung, L. A systematic review of faces scales for the self-report of pain intensity in children. Pediatrics. 2010; 126(5):e1168–e1198.
13. Salkind, AR, Cuddy, PG, Foxworth, JW. The rational clinical examination. Is this patient allergic to penicillin? An evidence-based analysis of the likelihood of penicillin allergy. JAMA. 2001; 285(19):2498–2505.
14. Ramosaka, EA, Sacchetti, AD, Nepp, M. Reliability of patient history in determining the possibility of pregnancy. Ann Emerg Med. 1989; 18:48–50. [In this study, one in 10 women who denied the possibility of pregnancy had a positive pregnancy test.].
15. Newman, LS. Occupational illness. N Engl J Med. 1995; 333:1128–1134. [The importance of knowing the occupation for the diagnosis of an illness cannot be overemphasised.].
16. Blue, AV, Chessman, AW, Gilbert, GE, Schuman, SH, Mainous, AG. Medical students’ abilities to take an occupational history: use of the WHACS mnemonic. J Occup Environ Med. 2000; 42(11):1050–1053.
17. Kitchens, JM. Does this patient have an alcohol problem. JAMA. 1994; 272:1782–1787. [A useful guide to making this assessment.].
18. Friedmann, PD. Clinical practice. Alcohol use in adults. N Engl J Med. 2013; 368(4):365–373.
19. www.nhmrc.gov.au/your-health/alcohol-guidelines.
20. Beresford, TP, Blow, FC, Hill, E, Singer, K, Lucey, MR. Comparison of CAGE questionnaire and computer-assisted laboratory profiles in screening for covert alcoholism. Lancet. 1990; 336:482–485.
21. Bradley, KA, DeBenedetti, AF, Volk, RJ, et al. AUDIT-C as a brief screen for alcohol misuse in primary care. Alcohol Clin Exp Res. 2007; 31:1208.
22. Smith, PC, Schmidt, SM, Allensworth-Davies, D, Saitz, R. Primary care validation of a single-question alcohol screening test. J Gen Intern Med. 2009; 24:783–788.
23. Smith, PC, Schmidt, SM, Allensworth-Davies, D, Saitz, R. A single-question screening test for drug use in primary care. Arch Intern Med. 2010; 170(13):1155–1160.
24. World Health Organization. Depression. www.who.int/mentalhealth/management/depression/definition/en.
25. Zimmerman, M, Lish, DT, et al. Suicide ideation among urban medical outpatients. J Gen Intern Med. 1995; 10(10):573–576.
26. Rich, EC, Burke, W, Heaton, CJ, Haga, S, Pinsky, L, Short, MP, Acheson, L. Reconsidering the family history in primary care. J Gen Intern Med. 2004; 19(3):273–280.
27. Hoffbrand, BI. Away with the system review: a plea for parsimony. BMJ. 1989; 198:817–819. [Presents the case that the systems review approach is not valuable. A focused review still seems to be useful in practice (see reference 28 below).].
28. Boland, BJ, Wollan, PC, Silverstein, MD. Review of systems, physical examination, and routine test for case-finding in ambulatory patients. Am J Med Sci. 1995; 309:194–200. [A systems review can identify unsuspected clinically important conditions.].
29. Simpson, M, Buchman, R, Stewart, M, et al. Doctor–patient communication: the Toronto consensus statement. BMJ. 1991; 303:1385–1387. [Most complaints about doctors relate to failure of adequate communication. Encouraging patients to discuss their major concerns without interruption or premature closure enhances satisfaction and yet takes little time (average 90 seconds). Factors that improve communication include using appropriate open-ended questions, giving frequent summaries, and using clarification and negotiation. These skills can be learned but require practice.].
30. Henderson MC, Tierney LM, Smetana GW, eds. The patient history. An evidence-based approach to differential diagnosis. New York: McGraw-Hill Lange, 2012.
a20 cigarettes a day for a year = 1 packet-year.