Correlation of physical signs and respiratory disease
Life cannot bee maintained without respiration, neither can respiration bee performed without motion.
Respiratory distress: respiratory failure
A severe respiratory illness may be a medical emergency. Many of the respiratory illnesses discussed below and some non-respiratory illnesses (see List 11.1) can result in acute respiratory problems and it is important to recognise signs that suggest there is an urgent problem. These signs include:
• cyanosis or low SpO2 on oximetry
• use of accessory muscles of respiration
• greatly increased or reduced respiratory rate
There may be signs of an underlying respiratory illness (see Table 11.1).
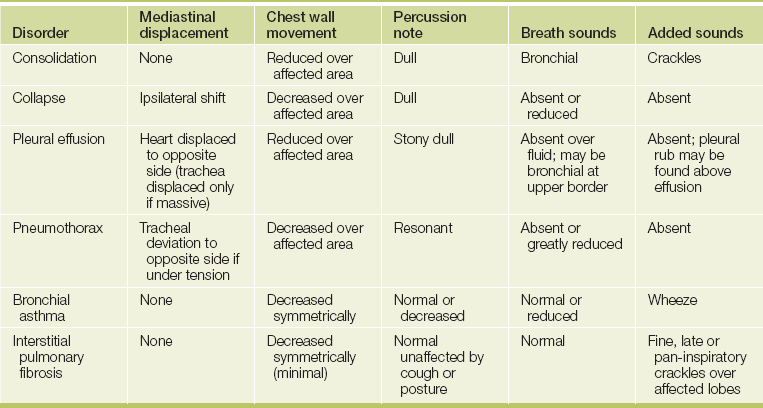
Consolidation (lobar pneumonia)
Pneumonia is defined as inflammation of the lung that is characterised by exudation into the alveoli (see Good signs guide 11.1). X-ray changes of new shadowing in one or more lung segments (lobes) are present. Pneumonia is now classified as:
GOOD SIGNS GUIDE 11.1 Pneumonia
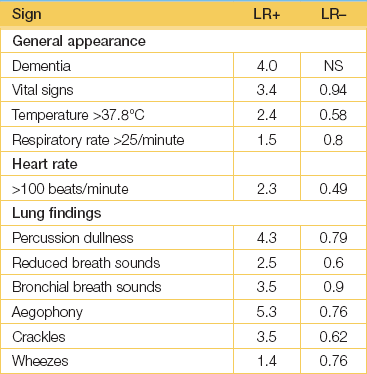
(Heckerling PS, Tape TG et al. Clinical prediction rule for pulmonary infiltrates. Ann Intern Med 1990; 113(9):664-670.)
This classification allows prediction of the likely pathogens and assists in the choice of antibiotics for treatment. The signs of lobar pneumonia are characteristic and are referred to clinically as consolidation.1
There may be a history of the sudden onset of malaise, chest pain, dyspnoea and fever. Patients may appear very ill and the vital signs—including the temperature, respiratory rate and blood pressure—must be recorded. There may be signs of cyanosis and exhaustion in sick patients. The term bronchopneumonia refers to lung infection characterised by more patchy X-ray changes that often affect both lower lobes. The clinical signs of consolidation may be absent.
Atelectasis (collapse)
If a bronchus is obstructed by a tumour mass, retained secretions or a prolonged presence of a foreign body, the air in the part of the lung supplied by the bronchus is absorbed and the affected part of the lung collapses.
SIGNS
• Trachea: displaced towards the collapsed side.
• Expansion: reduced on the affected side with flattening of the chest wall on the same side.
• Percussion: dull over the collapsed area.
• Breath sounds: reduced, often without bronchial breathing above the area of atelectasis when a tumour is the cause, because the airways are not patent.
Note: (1) There may be no signs with complete lobar collapse. (2) The early changes after the inhalation of a foreign body may be over-inflation of the affected side.
Pleural effusion
This is a collection of fluid in the pleural space. Note that pleural collections consisting of blood (haemothorax), chyle (chylothorax) or pus (empyema) have specific names and are not called pleural effusions, although the physical signs are similar.
SIGNS
CAUSES
• Transudate (Light’s criteria): (1) cardiac failure; (2) hypoalbuminaemia from the nephrotic syndrome or chronic liver disease; (3) hypothyroidism.
• Exudate (Light’s criteriaa): (1) pneumonia; (2) neoplasm—bronchial carcinoma, metastatic carcinoma, mesothelioma; (3) tuberculosis; (4) pulmonary infarction; (5) subphrenic abscess; (6) acute pancreatitis; (7) connective tissue disease such as rheumatoid arthritis, systemic lupus erythematosus; (8) drugs such as methysergide, cytotoxics; (9) irradiation; (10) trauma; (11) Meigs’ syndromeb (ovarian fibroma causing pleural effusion and ascites).
• Haemothorax (blood in the pleural space): (1) severe trauma to the chest; (2) rupture of a pleural adhesion containing a blood vessel.
• Chylothorax (milky-appearing pleural fluid due to leakage of lymph): (1) trauma or surgery to the thoracic duct; (2) carcinoma or lymphoma involving the thoracic duct.
• Empyema (pus in the pleural space): (1) pneumonia; (2) lung abscess; (3) bronchiectasis; (4) tuberculosis; (5) penetrating chest wound.
YELLOW NAIL SYNDROME
This is a rare condition that is caused by hypoplasia of the lymphatic system. The nails are thickened and yellow (see Figure 11.1) and there is separation of the distal nail plate from the nail bed (onycholysis). It may be associated with a pleural effusion and bronchiectasis, and usually with lymphoedema of the legs.

Figure 11.1 Yellow nail syndrome: (a) hands; (b) feet (From McDonald FS, ed. Mayo Clinic images in internal medicine, with permission. © Mayo Clinic Scientific Press and CRC Press.)
Pneumothorax
Leakage of air from the lung or a chest wall puncture into the pleural space causes a pneumothorax.
CAUSES
Secondary
• Traumatic: rib fracture, penetrating chest wall injury, or during pleural or pericardial aspiration.
• Iatrogenicc (caused by medical intervention): following the insertion of a central venous catheter.
• Emphysema with rupture of bullae, usually in middle-aged or elderly patients with generalised emphysema.
• Rarer causes include asthma, lung abscess, bronchial carcinoma, eosinophilic granuloma, lymphangioleiomyomatosis (LAM—premenopausal women), end-stage fibrosis or Marfan’s syndrome.
Tension pneumothorax
This occurs when there is a communication between the lung and the pleural space, with a flap of tissue acting as a valve, allowing air to enter the pleural space during inspiration and preventing it from leaving during expiration. A tension pneumothorax results from air accumulating under increasing pressure in the pleural space; it causes considerable displacement of the mediastinum with obstruction and kinking of the great vessels, and represents a medical emergency.
Bronchiectasis
This is a pathological dilation of the bronchi, resulting in impaired clearance of mucus and chronic infection. A history of chronic cough and purulent sputum since childhood is virtually diagnostic.
SIGNS
Most likely during an exacerbation of the condition.
• Systemic signs: fever, cachexia; sinusitis (70%).
• Sputum: voluminous, purulent, foul-smelling, sometimes bloodstained.
• Breath sounds: Coarse pan-inspiratory or late inspiratory crackles over the affected lobe.
• Signs of severe bronchiectasis: very copious amounts of sputum and haemoptysis, clubbing, cyanosis, widespread crackles, signs of airways obstruction, signs of respiratory failure and cor pulmonale, signs of secondary amyloidosis (e.g. oedema from proteinuria, cardiac failure, enlarged liver and spleen, carpal tunnel syndrome).
CAUSES
• Congenital: (1) primary ciliary dyskinesia (including the immotile cilia syndrome); (2) cystic fibrosis; (3) congenital hypogammaglobulinaemia.
• Acquired: (1) infections in childhood, such as whooping cough, pneumonia or measles; (2) localised disease such as a foreign body, a bronchial adenoma or tuberculosis; (3) allergic bronchopulmonary aspergillosis—this causes proximal bronchiectasis.
Bronchial asthma
This may be defined as paroxysmal recurrent attacks of wheezing (or in childhood of cough) due to airways narrowing, which changes in severity over short periods of time.
SIGNS
• Prolonged forced expiratory time (decreased peak flow, decreased FEV1).
• Use of accessory muscles of respiration.
• Hyperinflated chest (increased anteroposterior diameter with high shoulders and, on percussion, decreased liver dullness).
• Inspiratory and expiratory wheezes.
• Signs of severe asthma: appearance of exhaustion and fear, inability to speak because of breathlessness, drowsiness due to hypercapnia (preterminal), cyanosis (a very sinister sign), tachycardia (pulse above 130 beats/minute correlates with significant hypoxaemia), pulsus paradoxus (more than 20 mmHg), reduced breath sounds or a ‘silent’ chest.
Chronic obstructive pulmonary disease
Chronic obstructive pulmonary disease (COPD, chronic airflow limitation; see Good signs guide 11.2) represents a spectrum of abnormalities from predominantly emphysema, where there is pathologically an increase beyond normal in the size of the air spaces distal to the terminal bronchioles, to chronic bronchitis, where there is mucous gland hypertrophy, increased numbers of goblet cells and hypersecretion of mucus in the bronchial tree resulting in a chronic cough and sputum. COPD limitation does not cause clubbing or haemoptysis. Some 50% of patients with chronic bronchitis have emphysema, so there may be considerable overlapping of signs.2
The diagnosis can often be made on the basis of three findings:
1. A history of heavy smoking (more than 40 packet-years, LR 12; less than 20 packet-years, LR 0.53).
If two or three of these are present, the positive LR of COPD is 25.7.
SIGNS
Patients are usually not cyanosed but are dyspnoeic, and used to be called ‘pink puffers’. The signs result from hyperinflation.
• Barrel-shaped chest with increased anteroposterior diameter.
• Pursed-lip breathing (this occurs in emphysema and not in chronic bronchitis): expiration through partly closed lips increases the end-expiratory pressure and keeps airways open, helping to minimise air trapping.
• Use of accessory muscles of respiration and drawing in of the lower intercostal muscles with inspiration.
• Drowsiness or even coma may be a sign of CO2 retention indicating a worsening of the patient’s chronically increased CO2 levels. It may be caused by the administration of oxygen supplements (look for the oxygen mask), which further diminishes the patient’s respiratory drive.d This is type II respiratory failure.
• CO2 retention also leads to warm peripheries, bounding pulses and sometimes a flapping tremor.
• Palpation: reduced expansion and a hyperinflated chest, Hoover’s sign, tracheal tug.
• Percussion: hyperresonant with decreased liver dullness.
• Breath sounds: decreased, early inspiratory crackles.
• Signs of right heart failure may occur, but only late in the course of the disease.
Chronic bronchitis
This is defined clinically as the daily production of sputum for 3 months a year for at least 2 consecutive years. It is not now diagnosed as a separate entity from COPD and is probably of mostly historical interest.
SIGNS
The signs are the result of bronchial hypersecretion and airways obstruction.
• Loose cough and sputum (mucoid or mucopurulent), particularly in the morning shortly after wakening, and lessening as the day progresses.
• Cyanosis: these patients were sometimes called ‘blue bloaters’ because of the cyanosis present in the latter stages and associated oedema from right ventricular failure.
• Palpation: hyperinflated chest with reduced expansion.
• Percussion: increased resonance.
• Breath sounds: reduced with end-expiratory high- or low-pitched wheezes and early inspiratory crackles.
Interstitial lung disease (ILD)
Diffuse fibrosis of the lung parenchyma impairs gas transfer and causes ventilation–perfusion mismatching. This fibrosis may be the result of inflammation (alveolitis and interstitial inflammation) or granulomatous disease (see List 11.2). It has often no known cause (idiopathic interstitial fibrosis) or is secondary to a disease of unknown aetiology (e.g. sarcoidosis, connective tissue disease). It can result from inhalation of mineral dusts (focal fibrosis), replacement of lung tissue following disease that damages the lungs (e.g. aspiration pneumonia, tuberculosis). Collagen diseases and vasculitis are important causes.
SIGNS
• General: dyspnoea, cyanosis and clubbing may be present.
• Palpation: expansion is slightly reduced.
• Auscultation: fine (Velcro-like) late inspiratory or pan-inspiratory crackles heard over the affected lobes.
• Signs of associated connective tissue disease: rheumatoid arthritis, systemic lupus erythematosus, scleroderma, Sjögren’se syndrome, polymyositis and dermatomyositis.
CAUSES
• Upper lobe predominant: SCART
S ilicosis (progressive massive fibrosis), sarcoidosis
C oal workers’ pneumoconiosis (progressive massive fibrosis), cystic fibrosis, chronic allergic alveolitis, chronic eosinophilic pneumonitis
A nkylosing spondylitis, allergic bronchopulmonary aspergillosis, alveolar haemorrhage syndromes
• Lower lobe predominant: RASIO
R heumatoid arthritis, other collagen vascular diseases
A sbestosis, acute allergic alveolitis, acute eosinophilic pneumonitis
S cleroderma (systemic sclerosis)
I diopathic interstitial fibrosis
O ther (drugs, e.g. busulfan, bleomycin, nitrofurantoin, hydralazine, methotrexate, amiodarone).
Tuberculosis
PRIMARY TUBERCULOSIS
A Ghonf focus with hilar lymphadenopathy occurs usually in children.
Usually no abnormal chest signs are found, but segmental collapse, due to bronchial obstruction by the hilar lymph nodes, occasionally occurs. Erythema nodosum (page 224) is an important associated sign, but is rare.
POST-PRIMARY TUBERCULOSIS
The causes of post-primary or adult tuberculosis are reactivation of a primary lesion or occasionally reinfection. Immune suppression and malnutrition predispose to reactivation of tuberculosis.
There are often no chest signs. The clues to the diagnosis are the classical symptoms of cough, haemoptysis, weight loss, night sweats and malaise.
MILIARY TUBERCULOSIS
Widespread haematogenous dissemination of tubercle bacilli causes multiple millet-seed tuberculous nodules in various organs—spleen, liver, lymph nodes, kidneys, brain or joints. Miliary tuberculosis may complicate both childhood and adult tuberculosis.
Fever, anaemia and cachexia are the general signs. The patient may also be dyspnoeic, and pleural effusions, lymphadenopathy, hepatosplenomegaly or signs of meningitis may be present.
MEDIASTINAL COMPRESSION
Mediastinal structures may be compressed by a variety of pathological masses, including carcinoma of the lung (90%), other tumours (lymphoma, thymoma, dermoid cyst), a large retrosternal goitre or, rarely, an aortic aneurysm.
SIGNS
• Superior vena caval obstruction:g the face is plethoric and cyanosed with periorbital oedema (see Figure 11.2); the eyes may show exophthalmos, conjunctival injection and venous dilation in the fundi; in the neck the JVP is raised but not pulsatile, the thyroid may be enlarged and there may be supraclavicular lymphadenopathy and a positive Pemberton’s sign; the chest may show dilated collateral vessels or signs of lung carcinoma.
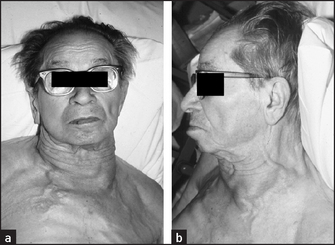
Figure 11.2 Superior vena caval obstruction (a) from the front (b) from the side (From Mangione S. Physical diagnosis secrets, 2nd edn. Mosby, 2007.)
• Tracheal compression: stridor, usually accompanied by respiratory distress.
• Recurrent laryngeal nerve involvement: hoarseness of the voice.
• Paralysis of the phrenic nerve: dullness to percussion at the affected base, which does not change with deep inspiration (abnormal tidal percussion), and absent breath sounds suggest a paralysed diaphragm due to phrenic nerve involvement.
Carcinoma of the lung
RESPIRATORY AND CHEST SIGNS
APICAL (PANCOAST’S) TUMOUR
Signs: Horner’s syndrome, recurrent laryngeal nerve palsy (hoarseness) due to a C8/T1 nerve root lesion.
NON-METASTATIC EXTRAPULMONARY MANIFESTATIONS
• Anorexia, weight loss, cachexia, fever.
• Endocrine changes: (1) hypercalcaemia, due to secretion of parathyroid hormone-like substances, occurs in squamous cell carcinoma; (2) hyponatraemia—antidiuretic hormone is released by small (oat) cell carcinomas; (3) ectopic adrenocorticotrophic hormone (ACTH) syndrome (small cell carcinoma); (4) carcinoid syndromeh; (5) gynaecomastia (gonadotrophins—rare; more often squamous cell); (6) hypoglycaemia (insulin-like peptide from squamous cell carcinoma).
• Neurological manifestations: Eaton-Lamberti syndrome (progressive muscle weakness) and retinal blindness (small cell carcinoma), peripheral neuropathy, subacute cerebellar degeneration, polymyositis, cortical degeneration.
• Haematological features: migrating venous thrombophlebitis, disseminated intravascular coagulation, anaemia.
• Skin: acanthosis nigricans, dermatomyositis (rare).
• Renal: nephrotic syndrome due to membranous glomerulonephritis (rare).
Sarcoidosis
This is a systemic disease, characterised by the presence of non-caseating granulomas that commonly affect the lungs, skin, eyes, lymph nodes, liver, spleen and the nervous system. The aetiology is unknown. There may be no pulmonary signs.
EXTRAPULMONARY SIGNS
• Skin: lupus pernio (violaceous patches on the face, especially the nose, fingers or toes), pink nodules and plaques (granulomata) in old scars, erythema nodosum on the shins.
• Eyes: ciliary injection, anterior uveitis.
• Lymph nodes: generalised lymphadenopathy.
• Liver and spleen: enlarged (uncommon).
• Parotids: gland enlargement (uncommon).
• Central nervous system: cranial nerve lesions, peripheral neuropathy (uncommon).
• Musculoskeletal system: arthralgia, swollen fingers, bone cysts (rare).
• Heart: heart block presenting as syncope, cor pulmonale (both rare).
Pulmonary embolism (PE)
Embolism to the lungs often occurs without symptoms or signs. One should always entertain this diagnosis if there has been sudden and unexplained dyspnoea when a patient has risk factors for embolism (see List 11.3). Pleuritic chest pain and haemoptysis occur only when there is infarction. Syncope or the sudden onset of severe substernal pain can occur with massive embolism.
SIGNS
• General signs: tachycardia, tachypnoea, fever (with infarction).
• Lungs: pleural friction rub if infarction has occurred.
• Massive embolism: elevated JVP, right ventricular gallop, right ventricular heave, tricuspid regurgitation murmur, palpable pulmonary component of the second heart sound (P2), gallop (S3 and/or S4).
• Signs of deep venous thrombosis: fewer than 50% of patients have clinical evidence of a source.
Note: A firm diagnosis cannot be made on the symptoms and signs alone.
References
1. Metlay, JP, Kappor, WN, Fine, MJ. Does this patient have community-acquired pneumonia? Diagnosing pneumonia by history and physical examination. JAMA. 1997; 278:1440–1445. [Normal vital signs and normal chest auscultation substantially reduce the likelihood of pneumonia, but a chest X-ray is required for a firm diagnosis.].
2. Holloman, DR, Simmel, DL, Goldberg, JS. Diagnosis of obstructive airways disease from the clinical examination. J Gen Intern Med. 1993; 8:63–68. [A history of smoking, self-reported wheezing and wheezing detected at auscultation combined had a high predictive value for chronic obstructive airways disease. The forced expiratory time added little additional information to these predictors.].
3. Holleman, DR, Simel, DL. Does the clinical examination predict airflow limitation. JAMA. 1995; 273(4):313–319.
aThe formal definition of an exudate is that the fluid has at least one of the following (Light’s) criteria; (1) fluid protein/serum protein >0.5; (2) pleural fluid LDH/serum LDH >0.6; (3) pleural fluid LDH >2/3 normal upper limit of LDH in serum. The fluid is otherwise a transudate.
bJoe Vincent Meigs (1892–1963), Professor of Gynaecology at Harvard, described this in 1937.
cIatros means physician in Greek.
dThis is called type II respiratory failure. Type I failure is associated with a normal or low PCO2 and can be due to acute lung problems (asthma, pneumonia, pneumothorax) or chronic conditions (ILD).
eHenrik Samuel Conrad Sjögren (1899–1986), Stockholm ophthalmologist. He described the syndrome in 1933.
fAnton Ghon (1866–1936), Austrian pathologist and Professor of Anatomical Pathology in Prague. He described the lesion in 1912.
gFirst described by William Hunter (1718–83, brother of John Hunter) in a patient with a syphilitic aortic aneurysm.
hThis rare neuro-endocrine tumour may arise in the bronchi but most often begins in the gut, usually the small bowel. It may secrete 5-hydroxytryptophan (5-HT). This is normally cleared from the circulation in the liver, but when hepatic metastases are present it reaches the systemic circulation and can cause wheezing and flushing: carcinoid syndrome.
iML Eaton (1905–58), 20th-century American physician, and EH Lambert (1915–2003), American neurologist.