Correlation of physical signs and gastrointestinal disease
Examination of the acute abdomen
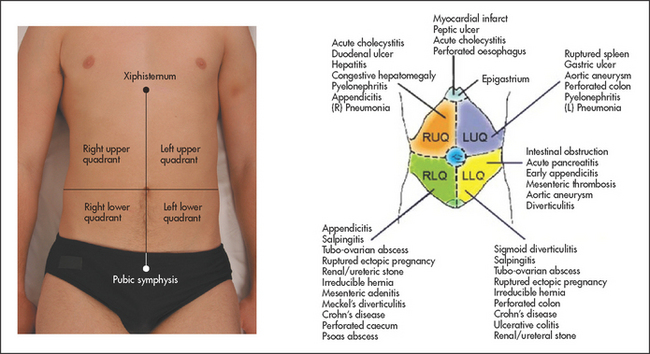
It is very important to try to determine whether a patient who presents with acute abdominal pain requires an urgent operation or whether careful observation with reassessment is the best course of action.1,2 First, take note of the general appearance of the patient. The patient who is obviously distressed with pain or who looks unwell often is, and conversely some reassurance can be gained if a patient does not look sick and appears comfortable (see Figure 15.1).
Assess the patient’s vital signs immediately and recheck these at frequent intervals. Signs of reduced circulating blood volume and dehydration—including tachycardia, postural hypotension, tachypnoea, vasoconstriction and sweating—are of great concern. These signs associated with abdominal pain are usually an indication of substantial intra-abdominal blood loss (such as a ruptured aortic aneurysm), or of substantial fluid losses (e.g. due to acute pancreatitis) or of septic shock (as with a perforated viscus or abscess). Take the patient’s temperature.
Inspect the abdomen. Look particularly for lack of movement with respiration, with splinting of the abdominal wall muscles. Note any abdominal distension, visible peristalsis or other lumps and masses, without forgetting the groin region and hernias. Note also any abdominal scars and enquire as to their nature and age.
Palpate very gently. The presence or absence of peritonism is first assessed. Peritonism is an inflammation that causes pain when peritoneal surfaces are moved relative to each other (see Good signs guide 15.1). Traditionally, rebound tenderness is used to assess whether peritonism is present or not. However, if peritonism is present, this test is far more uncomfortable (and cruel) than eliciting tenderness to light percussion. If the patient is extremely apprehensive, ask him or her first to cough; the reaction will be a guide to the degree of peritonism and also its location. Palpation is then continued slowly, but more deeply if possible and if masses are sought. Do not forget to palpate for the pulsatile mass of a ruptured aneurysm. This may be quite indistinct.
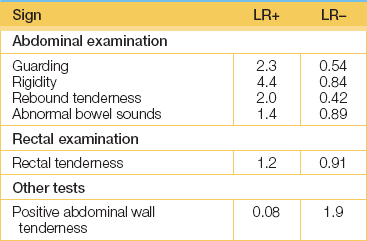
Then perform light percussion over areas of tenderness. If generalised peritonitis is present, this almost invariably necessitates a surgical approach, with the notable exception of acute pancreatitis.
Examine for hernias. The presence of a hernia does not necessarily mean that this is the cause of pathology, as they are quite common. However, a tender or irreducible hernia is more likely to be of significance, particularly if this has only very recently been noticed by the patient or has recently become tender.
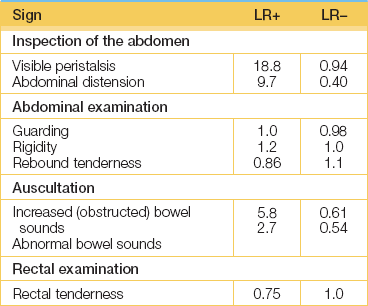
Auscultation is now performed. In the presence of a bowel obstruction bowel sounds (see Good signs guide 15.2) will be louder, more frequent and high-pitched. In an ileus from any cause, bowel sounds are usually reduced or absent.
Rectal and vaginal examinations may be important but the findings are not very helpful for the diagnosis of appendicitis or obstruction; note any tenderness (and its location), masses or blood loss. Per rectal blood should make the examiner think of acute colitis (e.g. Crohn’s disease, ulcerative colitis, ischaemic colitis or infectious colitis) or of mesenteric ischaemia. A purulent vaginal discharge suggests salpingitis.
Urinalysis may show glycosuria and ketonuria in diabetic ketoacidosis (which can cause acute abdominal pain), haematuria in renal colic, bili rubinuria in cholangitis or proteinuria in pyelonephritis.
Examine the respiratory system for signs of consolidation, a pleural rub or pleural effusion, and examine the cardiovascular system for atrial fibrillation (a major cause of embolism to a mesenteric artery) or for signs of a myocardial infarction. Examine the back for evidence of spinal disease that may radiate to the abdomen. Remember that herpes zoster may cause abdominal pain before the typical vesicles erupt.
Consider the symptoms and signs of appendicitis1 (see Good signs guide 15.3). Malaise and fever are usually associated with abdominal pain, which is at first worst in the hypogastrium and then moves to the right iliac fossa. The examination will often reveal tenderness and guarding in the right iliac fossa. The pain and tenderness are usually maximum over McBurney’sa point. McBurney described this point as 3.8 to 5 centimetres along a line from the anterior superior iliac spine to the umbilicus. Rovsing’sb sign is another way of testing rebound tenderness. Press over the patient’s left lower quadrant, then release quickly; this causes pain in the right iliac fossa. The psoas sign is positive when the patient lies on the left side and the clinician attempts to extend the right hip. If this is painful and resisted, the sign is positive. When the appendix causes pelvic inflammation, rectal examination evokes tenderness on the right side. These signs are of variable usefulness.
GOOD SIGNS GUIDE 15.3 Appendicitis
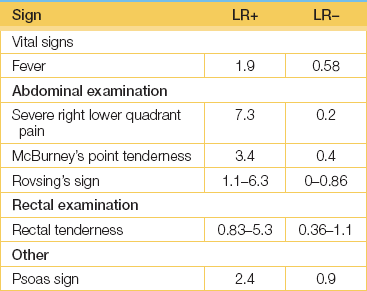
(Adapted from Simel DL, Rennie D. The rational clinical examination: evidence-based diagnosis. New York: McGraw-Hill, 2009, Table 5.3.)
Remember that in elderly patients these signs may be reduced or absent.2
ACUTE ABDOMEN AFTER BLUNT TRAUMA
You must assess for intra-abdominal injuries after blunt trauma to the abdomen, such as is common after a motor vehicle accident. A careful clinical assessment to look for shock and abdominal signs should be followed by targeted investigations, most notably an emergency abdominal ultrasound.
Take the patient’s pulse and blood pressure. Hypotension is an indicator of intra-abdominal injury (LR, 5.2). Look for bruising. Note the presence of the seat-belt sign from trauma with bruising over the area of impact (likelihood ratio for injury [LR] range, 5.6 to 9.9). Also look for abdominal distension (LR, 3.8). Palpate for rebound tenderness (LR, 6.5) and guarding (LR, 3.7). Note that no abdominal tenderness on palpation is not sufficient to exclude intra-abdominal injury (summary LR, 0.61).
Do an emergency ultrasound as this is more accurate than physical examination. The presence of intraperitoneal fluid or organ injury on bedside ultrasound assessment indicates the need for urgent surgical consultation (adjusted summary LR, 30). A normal ultrasound result is strongly reassuring (adjusted summary LR, 0.26).3
Liver disease
There are many signs that point to chronic liver disease. The likelihood ratios are summarised in Good signs guide 15.4.
SIGNS
• Hands: leuconychia, clubbing, palmar erythema, bruising, asterixis.
• Face: jaundice, scratch marks, spider naevi, fetor hepaticus.
• Chest: gynaecomastia, loss of body hair, spider naevi, bruising, pectoral muscle wasting.
• Abdomen: hepatosplenomegaly, ascites, signs of portal hypertension, testicular atrophy.
• Legs: oedema, muscle wasting, bruising.
• Fever: may occur in up to one-third of patients with advanced cirrhosis (particularly when this is secondary to alcohol) or if there is infected ascites.
The presence of two or more of the following signs strongly suggests cirrhosis: (1) spider naevi; (2) palmar erythema; (3) ascites; (4) hepatomegaly (firm liver); (5) abnormal collateral veins on the abdomen; and (6) hepatic encephatopathy.
Portal hypertension
SIGNS
• Splenomegaly: correlates poorly with the degree of portal hypertension.
• Collateral veins: haematemesis (from oesophageal or gastric varices).
CAUSES
(a) Pre-sinusoidal: (i) portal vein compression (e.g. lymphoma, carcinoma); (ii) intravascular clotting (e.g. in polycythaemia); (iii) umbilical vein phlebitis.
(b) Intrahepatic: (i) sarcoid, lymphoma or leukaemic infiltrates; (ii) congenital hepatic fibrosis.
(c) Post-sinusoidal: (i) hepatic vein outflow obstruction (Budd-Chiari syndrome) may be idiopathic, or caused by myeloproliferative disease, cancer (kidney, pancreas, liver), the contraceptive pill or pregnancy, paroxysmal nocturnal haemoglobinuria (PNH), fibrous membrane, trauma, schistosomiasis; (ii) veno-occlusive disease; (iii) constrictive pericarditis; (iv) chronic cardiac failure.
Hepatic encephalopathy
GRADING
| Grade 0 | Normal mental state. |
| Grade 1 | Mental changes (lack of awareness, anxiety, euphoria, reduced attention span, impaired ability to add and subtract). |
| Grade 2 | Lethargy, disorientation (for time), personality changes, inappropriate behaviour. |
| Grade 3 | Stupor, but responsive to stimuli; gross disorientation, confusion. |
| Grade 4 | Coma. |
CAUSES
• Acute liver failure (e.g. post-viral hepatitis, alcoholic hepatitis).
• Chronic portosystemic encephalopathy (e.g. from a portacaval shunt).
Encephalopathy may be precipitated by:
• Diarrhoea, diuretics or vomiting (resulting in hypokalaemia, which may increase renal ammonia and other toxin production, or alkalosis, which may increase the amount of ammonia and other toxins that cross the blood–brain barrier).
• Gastrointestinal bleeding or a relatively high-protein diet (causing an acute increase in nitrogenous contents in the bowel).
• Infection (e.g. urinary tract, chest or spontaneous bacterial peritonitis).
• Acute liver cell decompensation (e.g. from an alcoholic binge or a hepatoma).
Dysphagia
Dysphagia (difficulty in swallowing) and odynophagia (pain on swallowing) are important symptoms of underlying organic disease. It is important to examine such patients carefully for likely causes, particularly cancer (see List 13.2, page 175).
SIGNS
• General inspection. Note weight loss, due to decreased food intake or oesophageal cancer per se.
• The hands. Inspect the nails for koilonychia and the palmar creases for pallor indicative of anaemia. Iron deficiency anaemia can be associated with an upper oesophageal web, which is a thin structure consisting of mucosa and submucosa but not muscle. Iron deficiency anaemia and dysphagia due to an upper oesophageal web is called the Plummer-Vinsonc (or sometimes the Paterson-Brown-Kellyd) syndrome. Also examine the hands for signs of scleroderma.
• The mouth. Inspect the mucosa for ulceration or infection (e.g. candidiasis), which can cause odynophagia. Examine the lower cranial nerves for evidence of bulbar or pseudobulbar palsy.
• The neck. Palpate the supraclavicular nodes, which may occasionally be involved with oesophageal cancer; examine for evidence of retrosternal thyroid enlargement. A mass on the left side of the neck that is accompanied by gurgling sounds may rarely be caused by a Zenker’se diverticulum, an outpouching of the posterior hypopharyngeal wall.
• The lungs. Examine for evidence of aspiration into the lungs (due to overflow of retained material, gastro-oesophageal reflux or, rarely, the development of a tracheo-oesophageal reflux from oesophageal cancer).
• The abdomen. Feel for hepatomegaly due to secondary deposits from oesophageal cancer and for an epigastric mass from a gastric cancer; perform a rectal examination to exclude melaena (albeit uncommon with oesophageal disease).
Gastrointestinal bleeding
Haematemesis, melaena or massive rectal bleeding are dramatic signs of gastrointestinal haemorrhage. It is important in such a case to assess the amount of blood loss and attempt to determine the likely site of bleeding. Haematemesis indicates bleeding from a site proximal to, or in, the duodenum.
ASSESSING DEGREE OF BLOOD LOSS
First take the pulse rate and the blood pressure with the patient lying and sitting. As a general rule, loss of 1.5 litres or more of blood volume over a few hours results in a fall in cardiac output, causing hypotension and tachycardia. A pulse rate of more than 100 beats per minute, a systolic blood pressure of less than 100 mmHg or a 15 mmHg postural fall in systolic blood pressure suggests severe recent blood loss. The signs depend to some extent on the state of the patient’s cardiovascular system. Those who have pre-existing cardiovascular disease will become shocked much earlier than young, fit patients with a normal cardiovascular system.
Once signs of shock are present, massive blood loss has occurred. These signs include peripheral cyanosis with cold extremities, clammy skin, dyspnoea and air hunger; the patient will be anxious. The blood pressure is low, with a compensating tachycardia, and urine output is reduced or absent. These are ominous signs in patients with gastrointestinal haemorrhage. Urgent resuscitative measures must be instituted.
DETERMINING THE POSSIBLE BLEEDING SITE
The causes of acute gastrointestinal haemorrhage are listed in Table 13.1 (see page 178).
Examine the patient with acute upper gastrointestinal bleeding for signs of chronic liver disease and portal hypertension. Part of the assessment should include inspection of the vomitus and stools (see page 215) and a rectal examination (critical; see page 211). Melaena definitely increases the likelihood that a patient has an upper gastrointestinal bleed (LR, 25).4
Remember that, of patients with chronic liver disease and upper gastrointestinal bleeding, only about half are bleeding from varices. The others are usually bleeding from peptic ulceration (either acute or chronic). Look for evidence of a bleeding diathesis (generalised bruising or petechiae).
Finally, examine the patient for any evidence of skin lesions that can be associated with vascular anomalies in the gastrointestinal tract, although these are rare (see Table 13.1 on page 178 and Table 14.1 on pages 185–6).
For example, pseudoxanthoma elasticum is an autosomal recessive disorder of elastic fibres that results in xanthoma-like yellowish nodules, particularly in the axillae or neck (see Figure 15.2). These patients may also have angioid streaks of the optic fundus and angiomatous malformations of blood vessels that can bleed into the gastrointestinal tract. Ehlers-Danlos syndrome is a group of connective tissue disorders resulting in fragile and hyperextensible skin (see Figure 15.3). In a number of types, blood vessels are involved. Type IV is characterised by gastrointestinal tract bleeding, spontaneous bowel perforation, minimal skin hyperelasticity and minimal joint hyperextension.
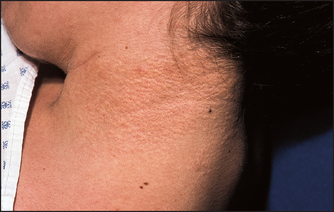
Figure 15.2 Pseudoxanthoma elasticum (axillae or neck) (From Paller AS, Mancini AJ. Hurwitz clinical pediatric dermatology, 4th edn. Saunders 2011.)

Figure 15.3 Ehlers-Danlos syndrome: (a) arms; (b) hands Abnormal elasticity of the skin is typical of the Ehlers-Danlos syndrome. The skin may be greatly stretched and takes much longer than normal to return to its normal position. It is also more fragile than normal. Joint hypermobility occurs in type III Ehlers-Danlos syndrome.
Examine the patient with acute lower gastrointestinal bleeding as described above, paying close attention to the abdominal examination and the rectal examination. Inspect the stools and test them for blood. Note that blood clots in the stool (LR, 0.05) decreases the likelihood of bleeding from the upper gut and directs you to the colon (but this is not an absolute rule).
Inflammatory bowel disease
Inflammatory bowel disease refers to two chronic idiopathic diseases of the gastrointestinal tract: ulcerative colitis and Crohn’s disease.
ULCERATIVE COLITIS
In the gastrointestinal tract only the large bowel is affected. Occasionally the terminal ileum can be secondarily involved (backwash ileitis). The disease almost always involves the rectum and may extend, without skip areas, to involve a variable part of the colon.
• Abdominal signs: if there is proctitis only, there are usually no abnormal external findings (except at sigmoidoscopy and biopsy); occasionally, anal fissures are present; with colitis, in the uncomplicated case the abdominal examination may be normal or there may be tenderness and guarding (page 198) over the affected colon.
• Signs of complications: local signs include the following: (1) toxic dilation (megacolon)—one of the most feared complications in which there are signs of distension, generalised guarding and rigidity (peritonism), pyrexia and tachycardia; (2) massive bleeding or perforation; (3) carcinoma—there is an increased incidence of colonic cancer in extensive, long-standing ulcerative colitis.
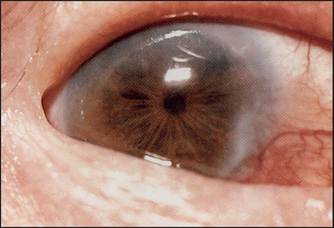
• Systemic signs include: (1) chronic liver disease—primary sclerosing cholangitis or cirrhosis; (2) anaemia—due to chronic disease per se, or blood loss, or autoimmune haemolysis; (3) arthritis—there may be a peripheral non-deforming arthropathy affecting particularly the knees, ankles and wrists (10%), and there may be signs of ankylosing spondylitis in 3% of affected patients; (4) skin manifestations: erythema nodosum (2%) consists of tender red nodules usually on the shins (see Figure 15.4); pyoderma gangrenosum (rare) starts as a tender, red raised area that becomes bullous and ulcerates (see Figure 15.5)—it may occur anywhere but is often on the anterior aspects of the legs; mouth ulcers are common and are due to aphthous ulceration (5%); finger clubbing may be present; (5) ocular changes include conjunctivitis, iritis and episcleritis (see Figure 15.6), which are strongly associated with arthritis and skin rash. (Conjunctivitis is an inflammation of the conjunctiva, which then appears red and swollen: the eye itself is not tender. Iritis is an inflammation of the iris with central scleral injection, which radiates out from the pupil: the eye is tender. Episcleritis is a nodule of inflammation on the scleral surface.)
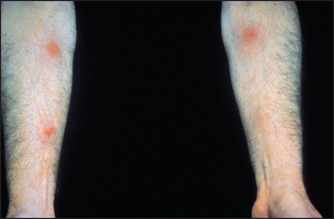
Figure 15.4 Erythema nodosum (From McDonald FS, ed. Mayo Clinic images in internal medicine, with permission. © Mayo Clinic Scientific Press and CRC Press.)

CROHN’S DISEASE
The whole of the gastrointestinal tract may be affected from the mouth to the anus. However, most commonly the terminal ileum, with or without the colon, is involved.
• Abdominal signs: if the condition affects only the terminal ileum there are often no abnormal findings, although tenderness, fullness or a mass (either soft or firm) in the right iliac fossa may be present. Occasionally, there may be signs of an abdominal abscess: these patients may have a high swinging fever, localised tenderness, a palpable mass and evidence of bowel obstruction (pain, vomiting and constipation with dehydration, abdominal distension and tenderness, and an empty rectum). Anal disease is common, including skin tags, fissures, fistulae and abscesses. Colonic involvement produces the same signs as ulcerative colitis.
• Signs of complications: these are similar to those of ulcerative colitis with the following exceptions: (1) liver disease—primary sclerosing cholangitis is less common; (2) osteomalacia and osteoporosis, which may occur in patients with extensive terminal ileal involvement, results in bone tenderness and fracture; (3) signs of malabsorption may be present; (4) finger clubbing is more common; (5) signs of gastrointestinal malignancy (small bowel or colonic carcinoma) incidence is increased; (6) the incidence of gallstones and renal stones is increased; (7) renal disease due to pyelonephritis, hydronephrosis or very rarely secondary amyloidosis may occur.
Malabsorption and nutritional status
Numerous diseases can cause maldigestion or malabsorption of food. Fat, protein and/or carbohydrate absorption may be affected.
SIGNS
• General: wasting (protein and fat malabsorption), folds of loose skin (recent weight loss), pallor (anaemia) or pigmentation (e.g. as in Whipple’sf disease).
• Stools: steatorrhoea (pale, bulky and offensive stools).
• Mouth: glossitis and angular stomatitis (deficiency in vitamin B2, vitamin B6, vitamin B12, folate or niacin), intraoral purpura (vitamin K deficiency) or hyperkeratotic white patches (vitamin A deficiency; see Figure 15.7).

Figure 15.7 Vitamin A deficiency (From Tyring S et al. Tropical dermatology, 1st edn. Churchill Livingstone 2005.)
• Limbs: bruising (vitamin K deficiency), oedema (protein deficiency), peripheral neuropathy (vitamin B12 or thiamine deficiency), bone pain (vitamin D deficiency).
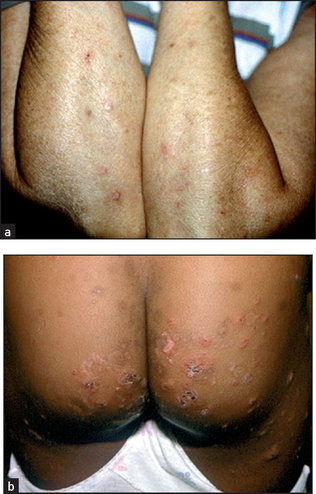
• Signs suggesting the underlying cause: in the abdomen these include scars from previous surgery, such as a gastrectomy, operations for Crohn’s disease or massive small bowel resection; on the skin dermatitis herpetiformis (itchy red lumps on the extensor surfaces; see Figure 15.8) may be found—this condition is strongly associated with coeliac disease and the histocompatibility antigen HLA-B8; there may be signs of chronic liver disease, or signs of inflammatory bowel disease.
CLASSIFICATION OF MALABSORPTION
• Lipolytic phase defects (pancreatic enzyme deficiency): (1) chronic pancreatitis; (2) cystic fibrosis.
• Micellar phase defects (bile salt deficiency): (1) extrahepatic biliary obstruction; (2) chronic liver disease; (3) bacterial overgrowth; (4) terminal ileal disease, such as Crohn’s disease or resection.
• Mucosal defects (diseased epithelial lining): (1) coeliac disease; (2) tropical sprue; (3) lymphoma; (4) Whipple’s disease (which causes pigmentation and arthritis; see Figure 15.9); (5) bowel ischaemia or resection; (6) amyloidosis; (7) hypogammaglobulinaemia; (8) HIV infection.

Figure 15.9 Pigmentation in Whipple’s disease (From Schaller J, Carlson JA. Journal of the American Academy of Dermatology Copyright © 2008, American Academy of Dermatology, Inc.)
• Delivery phase defects (inability to transport fat out of cells to lymphatics): (1) intestinal lymphangiectasia; (2) abetalipoproteinaemia; (3) carcinomatous infiltration of lymphatics.
References
1. Wagner, JM, Mckinney, WP, Carpenter, JL. Does this patient have appendicitis. JAMA. 1996; 276:1589–1594. [A ‘must read’ that discusses the key symptoms and signs that help make the correct diagnosis.].
2. Murtagh, J. Acute abdominal pain: a diagnostic approach. Aust Fam Phys. 1994; 23:358–361. [364–374].
3. Nishijima, DK, Simel, DL, Wisner, DH, Holmes, JF. Does this adult patient have a blunt intra-abdominal injury. JAMA. 2012; 307(14):1517–1527.
4. Srygley, FD, Gerardo, CJ, Tran, T, Fisher, DA. Does this patient have a severe upper gastrointestinal bleed. JAMA. 2012; 307(10):1072–1079.
aCharles McBurney (1845–1913), New York surgeon, described this sign to the New York Surgical Society in 1889.
bThorkild Rovsing (1862–1937), professor of surgery, Copenhagen.
cHenry Plummer (1874–1936), physician at the Mayo Clinic, described the syndrome in 1912; Porter Vinson (1890–1959), physician, Medical College Virginia, described the syndrome in 1919.
dDonald Paterson (1863–1939), Cardiff otolaryngologist, and Adam Brown-Kelly (1865–1941), Glasgow otolaryngologist, described this syndrome in 1919.
eFriedrich Albert Zenker (1825–1898), Munich pathologist.
fGeorge Hoyt Whipple (1878–1976), Baltimore pathologist, described this rare disease characterised by diarrhoea, arthralgia, central nervous system signs and pigmentation. He shared the 1934 Nobel Prize for work on liver treatment in anaemia and coined the word thalassaemia.