The neurological examination: speech and higher centres
By the time the general and neurological history has been taken, the presence of any disorder of speech is likely to be apparent.
Examination of speech
It is important to distinguish between dysphasia (dominant higher centre disorder in the use of symbols for communication—language), dysarthria (difficulty with articulation) and dysphonia (altered quality of the voice with reduction in volume as a result of vocal cord disease). If the nature of the abnormality is not obvious, before going on to compartmentalised tests, ask the patient to talk freely—propositional or free speech. In a normal clinical encounter this will have already come from history taking. In viva voce examinations or OSCEs, ask the patient to describe the room, his or her clothes or job or daily activities in order to promote flowing speech. Then test comprehension. This is done first without eliciting language—for example, ‘Touch your chin, then your nose and then your ear’; and then with yes and no questions—for example, ‘Do you put your shoes on before your socks?’ Then test repetition—for example, ‘Repeat the phrase “no ifs, ands or buts”.’
To complete the screening, ask the patient to name two objects pointed at, and to say a phrase such as ‘British Constitution’ or ‘West Register Street’ (page 474).
There is no need to examine further if no abnormality of speech is detected in this way.
If there is an abnormality, proceed as outlined in List 33.1.
DYSPHASIA
There are four main types of dysphasia:1 receptive, expressive, nominal and conductive. The expressive aphasias are forms of motor apraxia; this means the inability to perform deliberate actions in the absence of paralysis.
1. Receptive (posterior) dysphasia. This is where the patient cannot understand the spoken word (auditory dysphasia) or the written word (alexia). This condition is suggested when the patient is unable to understand any commands or questions or to recognise written words in the absence of deafness or blindness. Speech is fluent but disorganised. It occurs with a lesion (infarction, haemorrhage or space-occupying tumour) in the dominant hemisphere in the posterior part of the first temporal gyrus (Wernicke’sa area).
2. Expressive (anterior) dysphasia. This is present when the patient understands, but cannot answer appropriately. Speech is non-fluent. This occurs with a lesion in the posterior part of the dominant third frontal gyrus (Broca’sb area). Certain types of speech may be retained by these patients. These include automatic speech; the patient may be able to recite word series such as the days of the week or letters of the alphabet. Sometimes emotional speech may be preserved so that when frustrated or upset the patient may be able to swear fluently. In the same way the patient may be able to sing familiar songs while being unable to speak the words. It is important to remember that unless the lesion responsible for these defects is very large there may be no reduction in the patient’s higher intellectual functions, memory or judgement. Some patients may incorrectly be considered psychotic, because of their disorganised speech.
3. Nominal dysphasia. All types of dysphasia cause difficulty naming objects. There is also a specific type of nominal dysphasia, whereby objects cannot be named (e.g. the nib of a pen) but other aspects of speech are normal. The patient may use long sentences to overcome failure to find the correct word (circumlocution). It occurs with a lesion of the dominant posterior temporoparietal area. Other causes include encephalopathy or the intracranial pressure effects of a distinct space-occupying lesion; it may also occur in the recovery phase from any dysphasia. Its localising value is therefore doubtful.
4. Conductive dysphasia. This is present when the patient repeats statements and names objects poorly, but can follow commands. It is thought to be caused by a lesion of the arcuate fasciculus and/or other fibres linking Wernicke’s and Broca’s areas.
The detailed examination for dysphasia is set out in List 33.1. If the speech is fluent, but conveys information with paraphasic errors, such as ‘treen’ for ‘train’ (i.e. using a word of similar sound or spelling to the one intended),c the main possibilities are nominal, receptive and conductive dysphasia. Test for these by asking the patient to name an object, repeat a statement after you and then follow commands. If these are abnormal, ask the patient to read and write, but remember that some patients may be illiterate.
If the speech is slow, hesitant and non-fluent, expressive dysphasia is more likely and exactly the same procedure is followed. It is important to note that many dysphasias will have mixed elements. Large lesions in the dominant hemisphere may cause global dysphasia.
DYSARTHRIA
Here there is no disorder of the content of speech but a difficulty with articulation. It can occur because of abnormalities at a number of levels. Upper motor neurone lesions of the cranial nerves, extrapyramidal conditions (e.g. Parkinson’s disease) and cerebellar lesions cause disturbances to the rhythm of speech.
Ask the patient to say a phrase such as ‘British Constitution’ or ‘Peter Piper picked a peck of pickled peppers’.
Pseudobulbar palsy is an upper motor neurone weakness that causes a spastic dysarthria (it sounds as if the patient is trying to squeeze out words from tight lips), paralysis of the facial muscles and difficulty chewing and swallowing. The cause is infarction in both internal capsules. This causes interruption of the descending pyramidal tracts to the brainstem motor nuclei. The jaw jerk is usually increased. These patients tend to be very emotional and laugh and cry inappropriately. Their facial expressions become very animated at these times in contrast to their inability to control their facial expressions voluntarily.d This phenomenon occurs because the nuclei that control motor responses to emotion do not reside in the motor cortex.
Patients who have bilateral lesions of the ninth and tenth cranial nerves are at risk of aspirating fluids or solids into their lungs if they try to eat or drink. Certain bedside tests can be performed to see if it is safe for them to eat or drink. These traditionally include the level of consciousness, the gag reflex, pharyngeal sensation and testing swallowing water. The water swallowing test involves asking the patient to repeatedly sip 5–10 mL of water. Coughing, choking or a fall in blood arterial oxygen saturation makes the test positive.
Bulbar palsies cause a nasal speech, while facial muscle weakness causes slurred speech. Extrapyramidal disease can be responsible for monotonous speech, as it causes bradykinesia and muscular rigidity. Other causes of dysarthria include alcohol intoxication and cerebellar disease. These result in loss of coordination and slow, slurred and often explosive speech, or speech broken up into syllables, called scanning speech.
Mouth ulceration or disease may occasionally mimic dysarthria. Each of these causes must be considered and examined for as appropriate.
The cerebral hemispheres
Parietal, temporal and frontal lobe functions are tested if the patient is disoriented or has dysphasia, or if cognitive decline (dementia) is suspected. If the patient has a receptive aphasia, however, these tests cannot be performed. Their examination is otherwise not routine (see List 33.2).
PARIETAL LOBE FUNCTION
The parietal lobe is concerned with the reception and analysis of sensory information.
Dominant lobe signs
A lesion of the dominant parietal lobe in the angular gyrus causes a distinct clinical syndrome called Gerstmann’se syndrome. Test for this in the following manner.
1. Ask the patient to perform simple arithmetical calculations—for example, serial 7s (take 7 from 100, then 7 from the answer and so on). The inability to do this at least with partial accuracy is called acalculia.
2. Ask the patient to write—inability is called agraphia.
3. Test for left–right disorientation by asking the patient to show you his or her right and then left hand. If this is correctly performed, ask the patient to touch his or her left ear with the right hand and vice versa. Inability to do this is called left–right disorientation.
4. Ask the patient to name his or her fingers— inability to do this is called finger agnosia. This inability may extend to identification of the examiner’s fingers. The agnosias are receptive defects involving the inability to understand the meaning of stimulations of different types.
A mnemonic for these four dominant parietal lobe signs is AALF:
Remember that Gerstmann’s syndrome can be diagnosed only if the higher centres are intact. A demented patient would not be able to perform many of these tests.
Non-dominant and non-localising parietal lobe signs (cortical sensation)
Cortical sensations are those that require processing at a higher level than simple sensation. They rely on an intact simple sensation, especially touch and pinprick.
• Graphaesthesia is the ability to recognise numbers or letters drawn on the skin. Use a pointed object or pencil to draw numbers on the skin (see Figure 33.1).

Figure 33.1 Agraphaesthesia: ‘What number have I drawn?’ Patient’s reply: ‘One’ Avoid the use of an indelible pencil. (Courtesy of Glenn McCulloch)
• Tactile extinction is the ability to feel a stimulus when it is applied to each side separately, but not on one side when both sides are stimulated. Touch the patient (with their eyes shut, not yours) first on one hand and then on the other, and then on both together. Ask on which side the touch is felt. The normal response is ‘both’ when stimulation is applied to each side. It is important that the hands be touched simultaneously.
Now test for general signs of parietal lobe dysfunction.
• Look for sensory and visual inattention. When one arm or leg is tested at a time, sensation is normal, but when both sides are tested simultaneously the sensation is appreciated only on the normal side. A right-sided parietal lesion will lead to inattention on the left side and vice versa.
• Formal visual field testing is also important, as parietal, temporal and occipital lesions can give distinctive defects.
• Examine now for astereognosis (tactile agnosia), which is the inability, with eyes closed, to recognise an object placed in the hand when the ordinary sensory modalities are intact. A parietal lobe lesion results in astereognosis on the opposite side.
• Agraphaesthesia may also be present; this is the inability to appreciate a number drawn on the hand on the opposite side to a parietal lesion (see Figure 33.1).
• Two-point discrimination testing involves the ability to distinguish a single point from two points close together (see Figure 33.2). The minimal separation that can be distinguished is about 3 centimetres on the hand or foot and 0.6 centimetres on the fingertips. A compass can be used for this test. Ask the patient to shut the eyes and then say whether one or two points can be felt. Bring the compass points closer together and test intermittently with just one point.
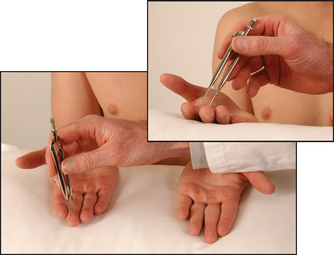
Figure 33.2 Two-point discrimination: ‘Can you feel one point or two?’ (Courtesy of Glenn McCulloch)
• Examine for dressing and constructional apraxia. Dressing apraxia is tested by taking the patient’s pyjama top or cardigan, turning it inside out and asking him or her to put it back on. Patients with a non-dominant parietal lobe lesion may find this impossible to do. Constructional apraxia is tested by asking the patient to copy an object that you have drawn (e.g. a tree or a house—see Figure 33.3(a) and (b)).
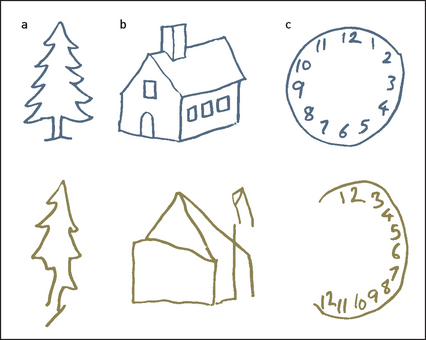
• Next test spatial neglect by asking the patient to fill in the numbers on an empty clock face (see Figure 33.3(c)). Patients with a right parietal lesion may fill in numbers only on the left side (the other side of the clock face is ignored). Spatial neglect also occurs with dominant parietal lobe lesions but is less common.
TEMPORAL LOBE FUNCTION
This lobe is concerned with short-term and long-term memory. Test short-term memory by the name, address, flower test—ask the patient to remember a name, address and the names of three flowers, and repeat them immediately. Then ask the patient five minutes later to repeat the names again. Test long-term memory by asking, for example, what year World War II ended. Memory may be impaired in dementia from any cause.
An alert patient with a severe memory disturbance may make up stories to fill any gaps in his or her memory. This is called confabulation and is typical of the syndrome of Korsakoff’sf psychosis (amnesic dementia). Confabulation can be tested by asking the patient whether he or she has met you before. However, be prepared for the very long, detailed and completely false story that may follow.
Korsakoff’s psychosis occurs most commonly in alcoholics (where there is loss of nerve cells in the thalamic nuclei and mammillary bodies), and rarely with head injury, tumour, anoxic encephalopathy or encephalitis. It is characterised by retrograde amnesia (memory loss for events before the onset of the illness) and an inability to memorise new information, in a patient who is alert, responsive and capable of problem-solving.
FRONTAL LOBE FUNCTION
Frontal lobe damage as a result of tumours or surgery (or both), or diffuse disease such as dementia or HIV infection, may cause changes in emotion, memory, judgement, carelessness about personal habits and disinhibition. There may be persistent or alternating irritability and euphoria.g These features may be clear when the history is taken but may need to be reinforced by interviewing relatives or friends. Changes of this sort in a previously reserved personality may be obvious and very distressing to relatives.
First assess the primitive reflexes. There is controversy concerning their significance; they are not normally present in adults but may reappear in normal old age.2 The presence of an isolated primitive reflex may not be abnormal, but multiple primitive reflexes are usually associated with diffuse cerebral disease involving the frontal lobes and frontal association areas more than other parts of the brain. Dementia, encephalopathy and neoplasms are all possible causes.
1. Grasp reflex: run your fingers across the palm of the patient’s hand, which will grasp your fingers involuntarily on the side contralateral to the lesion.
2. Palmomental reflex: ipsilateral contraction of the ipsilateral mentalis muscle occurs when you stroke the thenar eminence firmly with a key or thumb nail. Contraction of the mentalis causes protrusion and lifting of the lower lip. This is best considered as the beginning of a wince in response to pain. The response can also be elicited by painful stimulus to other parts of the body. The response is bilateral in about 50% of cases. A unilateral lesion does not necessarily correspond to the side of the lesion in the brain.
3. Pout and snout reflexes: stroking or tapping with the tendon hammer over or above the upper lip induces pouting movements of the lips. This can occur with many intracranial lesions. The sucking reflex is an extension of this. The stimulation may produce sucking, chewing and swallowing movements. It is not a localising sign.
Next ask the patient to interpret a proverb, such as ‘A rolling stone gathers no moss’. Patients with frontal lobe disease give concrete explanations of proverbs. Test for loss of smell (anosmia) and for gait apraxia, where there is marked unsteadiness in walking, which can be bizarre—the feet typically behave as if glued to the floor, causing a strange shuffling gait. Look in the fundi; you may rarely see optic atrophy on the side of a frontal lobe space-occupying lesion caused by compression of the optic nerve, and papilloedema on the opposite side due to secondarily raised intracranial pressure (Foster Kennedyh syndrome).
aKarl Wernicke (1848–1904), professor of neurology at Breslau, described receptive aphasia in 1874. He was killed while riding his bicycle.
bPierre Broca (1824–1880), professor of surgery at Paris, described this area in 1861. He described muscular dystrophy before Duchenne.
cSometimes a word of similar meaning is used (e.g. ‘go’ for ‘start’): this is called semantic paraphrasia.
dThis syndrome should probably be called ‘pseudo-pontine-bulbar palsy’ since the motor nuclei of the fifth and seventh nerves are in the pons, not the medulla (bulbs).
eJosef Gerstmann (1887–1969), Austrian-born neuropsychiatrist who worked in the United States.
fSergei Sergeyevich Korsakoff (1853–1900), Russian psychiatrist and great humanitarian, described the syndrome in 1887.
gEuphoria may cause a lack of seriousness, and the repetition of bad jokes and puns (witzelsucht).
hRobert Foster Kennedy (1884–1952), a New York neurologist.