The eyes, ears, nose and throat
The examination of the eyes and ears, nose and throat is important for any medical patient because these small parts of the body may be involved in local or systemic disease.
Eyes
EXAMINATION ANATOMY
The structure of the eye is shown in Figure 38.1.1 There are three layers that make up the eye ball:
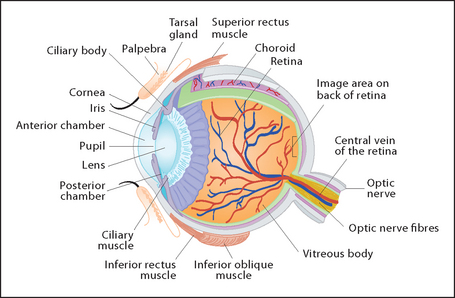
• The inner or neural layer forms the retina itself and has inner and outer layers. The outer layer contains pigmented cells and the inner layer, which is continuous with the optic nerve, contains the photoreceptor rod (night and peripheral vision) and cone (central and colour vision) cells.
• The central layer is called the uveal tract. It forms the iris and ciliary body anteriorly and the choroid posteriorly. The choroid is a vascular structure. It supplies the optic nerve, the fovea (area of most acute vision) and the posterior two-thirds of the retina. The ciliary body produces the aqueous humour. This transparent fluid lies behind the cornea and fills the anterior chamber of the eye. The aqueous humour moves through the pupil and drains through a trabecular meshwork at the acute angle of the anterior chamber. The lens sits behind the cornea and is suspended from ligaments of the ciliary body.
• The outer layer is fibrous. The anterior part, the cornea, is transparent and the rest makes up the sclera. The main volume of the eyeball is filled with vitreous humour, which is a transparent gel.
The anatomy of the optic nerve is described in Chapter 32.
The eyelids provide and distribute moisture to the corneas from three types of glands (two small and one large). The two types of small lacrimala glands within the eyelids secrete tears and produce mucin and oil. These are sufficient to lubricate the eyelids and the cornea in normal circumstances. Emotion or a foreign body, however, will stimulate the large lacrimal glands that lie between the bony orbital wall laterally and the eyeball and the lateral rectus muscle medially. From each gland duct, big volumes of tears drain into the upper part of the lid. Tears either evaporate or are drained via the medial edge of the eye into the lacrimal canaliculi and on into the lacrimal sac, the lacrimal duct, the inferior nasal meatus and thence to the nose—and, if necessary, into a handkerchief. The conjunctiva is a mucous membrane that lines the eyelids and keeps them slippery on the inside.
HISTORY
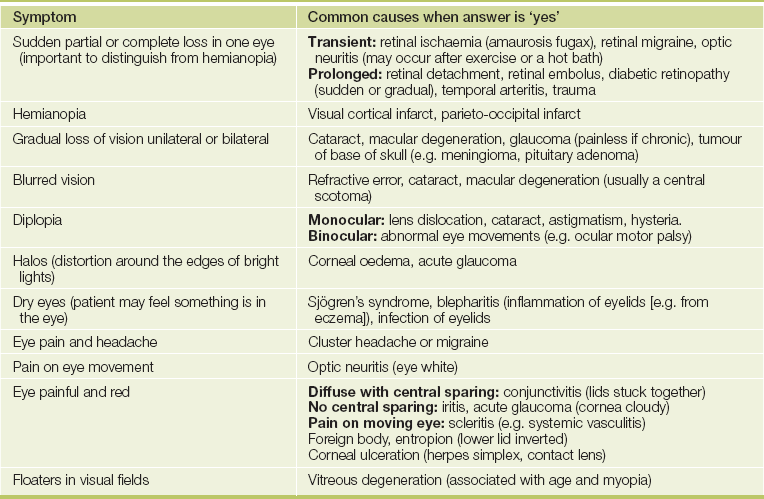
Presenting symptoms include pain or discomfort and redness (see Table 38.2 later in the chapter and Questions box 38.1), loss or distortion of vision and dry or watery eyes and infection of the eye lids and associated structures. Loss of vision and other visual symptoms (see Table 38.1 and Questions box 38.2) are also discussed in Chapter 32.
Questions box 38.1
Questions to ask the patient with a painful red eye
 denotes symptoms for the possible diagnosis of an urgent or dangerous problem.
denotes symptoms for the possible diagnosis of an urgent or dangerous problem.
1. Do you wear contact lenses? (Corneal ulceration)
2. Is it painful when you move your eyes? (Iritis or scleritis)
3. Are the lids stuck together in the morning? (Conjunctivitis)
4. Have you had an injury or worked with dust, metal grinders or welding equipment? (Injury, foreign body or flash burn)
Questions box 38.2
Questions to ask the patient with sudden visual loss
denotes symptoms for the possible diagnosis of an urgent or dangerous problem.
1. Does the abnormality persist when you close each eye in turn? (Visual field loss)
2. Was the sensation as if a curtain was drawn across your vision? Has your vision come back? (Amaurosis fugax)
3. Have you had previous strokes of fibrillation of your heart? (Retinal embolus, cortical infarct)
4. Has your eye been painful? (Acute glaucoma, iritis)
5. Have you injured your eye or head? (Trauma to eye or optic nerve)
6. Have you had preceding visual disturbance e.g. flashing lights? (Migraine)
7. Have you had severe headache on the same side? (Temporal arteritis)
8. Have you had weakness or tingling in your arms or legs, or bowel or bladder disturbance? (Multiple sclerosis and optic neuritis)
9. Are you a diabetic? (Diabetic retinopathy with haemorrhage)
More general questions include asking about a history of arthritis or known vasculitis, multiple sclerosis or thyroid disease; occupation and exposure to metal fragments or arc welding; use of contact lenses; previous history of vascular disease; diabetes or atrial fibrillation; and smoking. Conjunctivitis is a feature of measles (see Figure 38.2).

Ask about previous eye problems or surgery including laser correction surgery. Have the intraocular pressures been measured recently?
Take a drug history. Ask about eye drops and drugs such as corticosteroids (cataracts), anticholinergics (glaucoma from acute angle closure), amiodarone (corneal deposits), chloroquine and chlorpromazine (retinal toxicity) and ethambutol and isoniazid (optic neuropathy).
EXAMINATION METHOD
Sit the patient at the edge of the bed. Stand well back at first, and note the following:
1. Ptosis (drooping of one or both upper eyelids).
• yellow (deposits of bilirubin in jaundice)
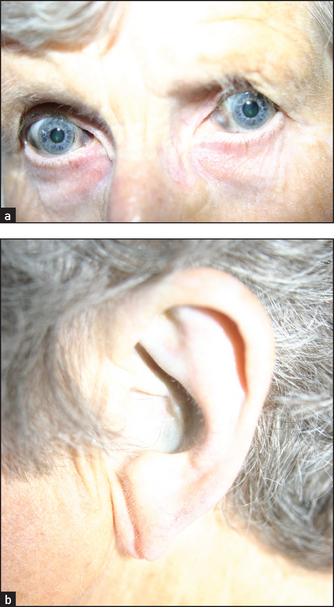
• blue (which may be due to osteogenesis imperfecta, because the thin sclerae allow the choroidal pigment to show through; blue sclerae can also occur in families without osteogenesis imperfecta); blue–grey scleral discolouration occurs in patients with ochronosis, due to the accumulation of homogentisic acid in connective tissue in this inherited condition; the concha of the ear is often affected (see Figure 38.3), as are the joints and heart valves
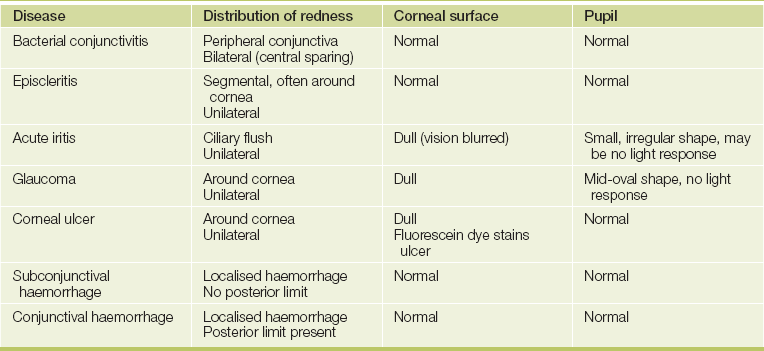
• red (iritis or scleritis, which causes central inflammation; or conjunctivitis, which causes more peripheral inflammation often with pus; or subconjunctival haemorrhage, which causes influent blood as a result of trauma; see Table 38.2 and List 38.1)
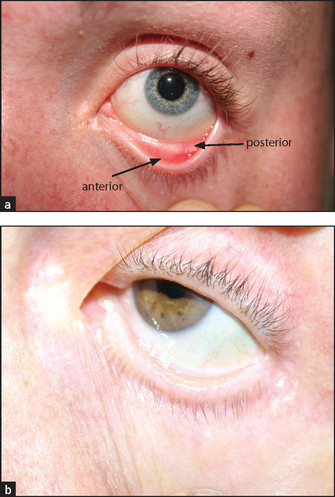
• scleral pallor, which occurs in anaemia—pull down the lower lid and look for the normal contrast between the pearly white posterior conjunctiva and the red anterior part; loss of this contrast is a reliable sign of anaemia (see Figure 38.4(b)).
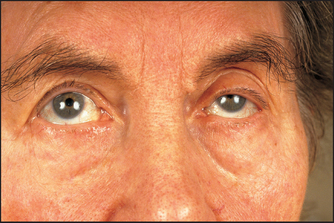
Look from behind and above the patient for exophthalmos, which is prominence of the eyes. If there is actual protrusion of the eyes from the orbits, this is called proptosis. It is best detected by looking at the eyes from above the forehead; protrusion beyond the supraorbital ridge is abnormal. If exophthalmos is present, examine specifically for thyroid eye disease: lid lag (the patient follows your finger as it descends—the upper lid lags behind the pupil), chemosis (oedema of the bulbar conjunctiva), corneal ulceration and ophthalmoplegia (weakness of upward gaze). Look then for any corneal abnormalities, such as band keratopathy or arcus senilis.
Look for corneal ulceration, which may be obvious if severe. A strip coated with sterile fluorescein will stain corneal ulcers and make them easily visible.
Proceed as for the cranial nerve examination—that is, testing visual acuity, visual fields and pupillary responses to light and accommodation. Interruption of the sympathetic innervation of the eye at any point results in Horner’s syndrome (partial ptosis and a constricted but reactive pupil). Perceptible anisocoria (inequality of the diameters of the pupils) has been found in 20% of healthy people. Remember also that elderly people quite often have imperceptible pupillary light reactions.
Test the eye movements (see Figure 38.5). Look also for fatiguability of eye muscles by asking the patient to look up at a hat-pin or finger for about half a minute. In myasthenia gravis the muscles tire and the eyelids begin to droop.
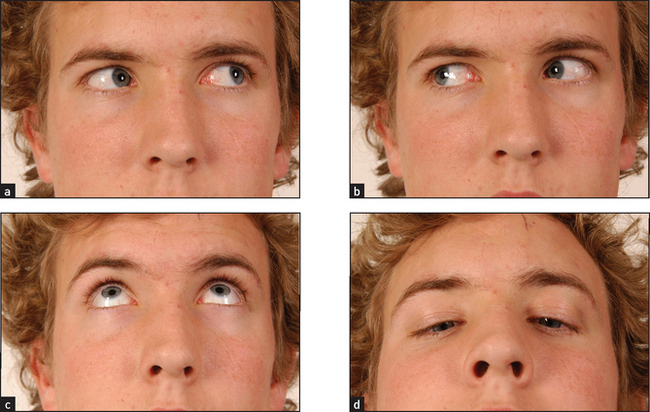
Figure 38.5 The cranial nerves III, IV and VI: voluntary eye movements (a) ‘Look to the left.’ (b) ‘Look to the right.’ (c) ‘Look up.’ (d) ‘Look down.’ (Courtesy of Glenn McCulloch)
Test colour vision if acuity is not poor. Ishihara test plates (where coloured spots form numbers) can be used. Red desaturation (impaired ability to see red objects) can occur with optic nerve disease. Red–green colour blindness affects 7% of males (X-linked recessive).
Test the corneal reflex (see also page 416).
Perform fundoscopy. Successful ophthalmoscopy requires considerable practice. It is important that it be performed in reduced ambient lighting so that the patient’s pupils are at least partly dilated and you are not distracted. It can be easier to perform the examination, especially of the fundi, through the patient’s spectacles. Otherwise, the patient’s refractive error should be corrected by use of the appropriate ophthalmoscope lens. The patient should be asked to stare at a point on the opposite wall or on the ceiling and to ignore the light of the ophthalmoscope. Patients will often attempt to focus on the ophthalmoscope light and should be asked not to do this.
Begin by examining the cornea. Use your right eye to examine the patient’s right eye, and vice versa. Turn the ophthalmoscope lens to +20 and examine the cornea from about 20 centimetres away from the patient. Look particularly for corneal ulceration. Turn the lens gradually down to 0 while moving closer to the patient. Structures, including the lens, the humour and the retina, at increasing distance into the eye will swim into focus.
Examine the retinas (see Figure 38.6; see also Figure 32.10 on page 408). Focus on one of the retinal arteries and follow it into the optic disc. The normal disc is round and paler than the surrounding retina. The margin of the disc is usually sharply outlined but will appear blurred if there is papilloedema or papillitis, or pale if there is optic atrophy. Look at the rest of the retina, especially for haemorrhages and the retinal changes of diabetes mellitus or hypertension.
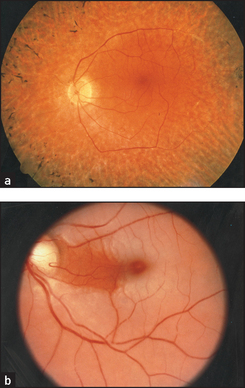
Figure 38.6 Retinal photographs (a) Retinitis pigmentosa; (b) central retinal artery occlusion. (Courtesy of Lions Eye Institute)
There are four types of haemorrhages: streaky haemorrhages near the vessels (linear or flame-shaped); large ecchymoses that obliterate the vessels; petechiae, which may be confused with microaneurysms; and subhyaloid haemorrhages (large effusions of blood that have a crescentic shape and well-marked borders; a fluid level may be seen). The first two types of haemorrhage occur in hypertensive and diabetic retinopathy. They may also result from any cause of raised intracranial pressure or venous engorgement, or from a bleeding disorder. The third type occurs in diabetes mellitus, and the fourth is characteristic of subarachnoid haemorrhage.
There are two main types of retinal change in diabetes mellitus: non-proliferative and proliferative. Non-proliferative changes include: (1) two types of haemorrhages occur specifically in diabetics—dot haemorrhages, which occur in the inner retinal layers, and blot haemorrhages, which are larger and occur more superficially in the nerve fibre layer; (2) microaneurysms (tiny bulges in the vessel wall), which are due to vessel wall damage; and (3) two types of exudates—hard exudates, which have straight edges and are due to leakage of protein from damaged arteriolar walls, and soft exudates (cottonwool spots), which have a fluffy appearance and are due to microinfarcts. Proliferative changes include new vessel formation, which can lead to retinal detachment or vitreous haemorrhage.
Hypertensive changes can be classified from grades 1 to 4:
| Grade 1 | ’Silver wiring’ of the arteries only (sclerosis of the vessel wall reduces its transparency so that the central light streak becomes broader and shinier) |
| Grade 2 | Silver wiring of arteries plus arteriovenous nipping or nicking (indentation or deflection of the veins where they are crossed by the arteries) |
| Grade 3 | Grade 2 plus haemorrhages (flame-shaped) and exudates (soft— cottonwool spots due to ischaemia, or hard—lipid residues from leaking vessels) |
| Grade 4 | Grade 3 changes plus papilloedema. |
It is important to describe the changes present rather than just give a grade.
Inspect carefully for central retinal artery occlusion, where the whole fundus appears milky-white because of retinal oedema and the arteries become greatly reduced in diameter. This presents with sudden, painless unilateral blindness and is a medical emergency.
Central retinal vein thrombosis causes tortuous retinal veins and haemorrhages scattered over the whole retina, particularly occurring alongside the veins (‘blood and thunder retina’). This presents with sudden painless loss of vision, which is not total.
Retinitis pigmentosa causes a scattering of black pigment in a criss-cross pattern. This will be missed if the periphery of the retina is not examined.
In retinal detachment, the retina may appear elevated or folded. The patient describes a ‘shade coming down’, flashes of light or showers of black dots. A diagnosis requires immediate referral to try to prevent total detachment and irrevocable blindness.
White spots occur in choroiditis and when active have a fluffy edge (e.g. in toxoplasmosis, sarcoidosis).
Finally, ask the patient to look directly at the light. This allows you to locate and inspect the macula. Macular degeneration is the leading cause of blindness; central vision is lost. Drussen formation occurs in macular degeneration—small deposits are seen under the epithelium in the central retina. Macular degeneration may occur secondary to an atrophic or a neovascularisation process.
Palpate the orbits for tenderness. Auscultate the eyes with the bell of the stethoscope—the eye being tested is shut while the other is open and the patient is asked to stop breathing. Listen for a bruit that may be a sign of an arteriovenous malformation or a vascular tumour.
Feel for the pre-auricular node (adenoviral conjunctivitis).
Consider the possibility that the patient may have a glass eye. This should be suspected if visual acuity is zero in one eye and no pupillary reaction is apparent. Attempts to examine and interpret the fundus of a glass eye will amuse the patient but are always unsuccessful.
The causes of common eye abnormalities are summarised in List 38.2.
LIST 38.2 Causes of eye abnormalities
2. Endocrine (e.g. diabetes mellitus, steroids)
3. Hereditary or congenital (e.g. dystrophia myotonica, Refsum’s disease*)
1. Space-occupying lesion (causing raised intracranial pressure) or a retro-orbital mass
2. Hydrocephalus (large cerebral ventricles)
Obstructive (a block in the ventricle, aqueduct or outlet to the fourth ventricle—e.g. tumour)
Increased formation of CSF (e.g. choroid plexus papilloma—rare)
Decreased absorption of CSF (e.g. tumour causing venous compression, subarachnoid space obstruction from meningitis)
3. Benign intracranial hypertension (pseudotumour cerebri) (small or normal-sized ventricles)
1. Chronic papilloedema or optic neuritis
2. Optic nerve pressure or division
5. Familial (e.g. retinitis pigmentosa, Leber’s† disease, Friedreich’s ataxia)
Causes of retinitis pigmentosa
1. Congenital (associated with cataract and deaf-mutism)
2. Laurence–Moon–Biedl syndrome‡
*Sigvald Refsum, (1907–1991), Norwegian physician.
†Theodor von Leber (1840–1917), Göttingen and Heidelberg ophthalmologist.
‡John Laurence (1830–1874), London ophthalmologist; Robert Charles Moon (1844–1914), American ophthalmologist; and Arthur Biedl (1869–1933), professor of physiology, Prague.
DIPLOPIA
Most cases of diplopia (about 60%) are not due to a cranial nerve abnormality. It is important to have an approach to the problem that will help work out the cause.
First find out whether the diplopia is monocular (25%) or binocular. Monocular diplopia persists when one eye is covered. It is usually due to an eye problem such as astigmatism, dislocated lens, uneven contact lens surface or thick spectacles and some types of cataract. It disappears if the patient looks through a pin hole. Although it is said to be due to hysteria, this is a very rare cause.
If the diplopia is binocular, consider the common causes:
1. Cranial nerve palsy (III, IV or VI)—look for ptosis, pupil changes (III), abnormal eye movements.
2. Eye muscle disease (myasthenia gravis)—worse later in the day, worse after prolonged upward gaze and associated with bilateral ptosis.
3. Thyroid ophthalmopathy—proptosis, lid lag, chemosis.
4. Trauma to the orbit—history or signs of trauma.
5. Internuclear ophthalmoplegia—associated neurological signs.
HORNER’S SYNDROME
EXAMINATION ANATOMY
Interruption of the sympathetic innervation of the eye at any point (see Figure 38.7) results in Horner’sb syndrome (see List 38.3).
Clinical approach
The syndrome includes partial ptosis (as sympathetic fibres supply the smooth muscle of both eyelids) and a constricted pupil (unbalanced parasympathetic action) that reacts normally to light (see Figure 38.7). Remember the other causes of ptosis (see Table 38.3).
TABLE 38.3
| Cause | Associated features |
| Age-related stretching of the levator muscle or aponeurosis | Common, often asymmetrical |
| Orbital tumour or inflammation | Orbital abnormality |
| Constricted pupil, reduced sweating | Homer’s syndrome |
| Eye ’down and out’, dilated pupil | Third nerve palsy |
| Myasthenia gravis or dystrophia myotonica | Extraocular muscle palsies, muscle weakness |
| Congenital or idiopathic |
Test for a difference (decrease) in the sweating over each eyebrow with the back of the finger (absence of this sign does not exclude the diagnosis).c
Horner’s syndrome may be part of the lateral medullary syndromed
Next ask the patient to speak and note any hoarseness of the voice, which may be due to recurrent laryngeal nerve palsy from lung carcinoma or from a lower cranial nerve lesion.
Now look at the hands for clubbing and test for weakness of finger abduction. If any of these signs is present, perform a respiratory examination, concentrating on the apices of the lungs for signs of lung carcinoma.
Examine the neck for lymphadenopathy, thyroid carcinoma and a carotid aneurysm or bruit. Syringomyelia may rarely be a cause of this syndrome, so the examination should be completed by testing for dissociated sensory loss. Remember, syringomyelia may cause a bilateral Horner’s syndrome.
IRITIS
Iritis (anterior uveitis) presents with pain, photophobia and unilateral eye redness (see Table 38.2 and List 38.1). On examination of the eye, there is classically a ciliary flush with dilated vessels around the iris. Hypopyon refers to pus in the anterior chamber; a fluid level may be seen. The pupil is usually irregular. There may also be new vessel formation over the iris.
Iritis is associated with inflammatory arthropathies that are linked to HLA-B27 positivity, including ankylosing spondylitis, inflammatory bowel disease, Reiter’s syndrome and Behçet’s disease with an acute presentation. Chronic iritis can be linked to juvenile rheumatoid arthritis, as well as sarcoidosis and syphilis.
Keratitis is inflammation of the cornea and may be due to ulceration (often a result of herpes simplex infection) or injury (e.g. from metal fragments in grinders or flash burns in arc welders). Contact lens wearers who do not clean their lenses properly are also at risk. Severe proptosis or a facial nerve palsy that prevents lid closure can be a mechanical cause.
Scleritis presents similarly but with bilateral painful red eyes; it is also associated with the same HLA-B27 arthropathies. Eye movements are painful in scleritis.
GLAUCOMA
Here prolonged elevation of intraocular pressure induces progressive visual loss. Closed-angle (narrow-angle) glaucoma is due to a rapid pressure increase. Symptoms include severe eye pain, halos around lights and nausea; it is an ocular emergency. You may see a fixed mid-dilated pupil, conjunctival hyperaemia and corneal redness; intraocular pressure on measurement is increased. The condition occurs secondary to iris neovascularisation (e.g. new renal formation in diabetes mellitus) or primarily from an anomalous iris (e.g. genetic). Acute glaucoma can be precipitated by anticholinergic drugs (e.g. amitriptyline).
SHINGLES
Herpes zoster involving the first (ophthalmic) division of the trigeminal nerve may result in uveitis and keratitis and threaten vision. The tip of the nose, cornea and iris are all innervated by the nasociliary nerve (a branch of the trigeminal nerve; see Figures 38.8 and 38.9). The appearance of vesicles on the tip of the nose (Hutchinson’se vesicles) in a patient with herpes zoster indicates an increased risk of ophthalmic complication (LR+ 3.5).2


EYELID
A number of conditions of the eyelid are worth remembering:
1. Stye of the eyelid (hordeolum) is an infection typically caused by Staphylococcus aureus; it is tender.
2. Chalazion is a slowly enlarging non-tender nodule of the eyelid (see Figure 38.10; sterile inflammation of the meibomian glands if deep, or of the sebaceous glands if superficial).

3. Dacrocystitis is infection of a lacrimal gland or of the lacrimal duct (see Figure 38.11).

Figure 38.11 Dacrocystitis (Courtesy of Dr A Watson, Infectious Diseases Department, The Canberra Hospital)
4. Orbital cellulitis may spread to involve the eyelid (see Figure 38.12).

Figure 38.12 Orbital cellulitis (Courtesy of Dr A Watson, Infectious Diseases Department, The Canberra Hospital)
5. Ectropion is a drooping of the lower lid when it loses its elasticity in old age and falls away from the sclera. This interrupts tear drainage, the eye becomes dry and tears spill over the patient’s cheek.
6. Entropium is the opposite. Scarring or thickening of the lower lid leads to corneal abrasion from inverted lashes.
Ears
EXAMINATION ANATOMY
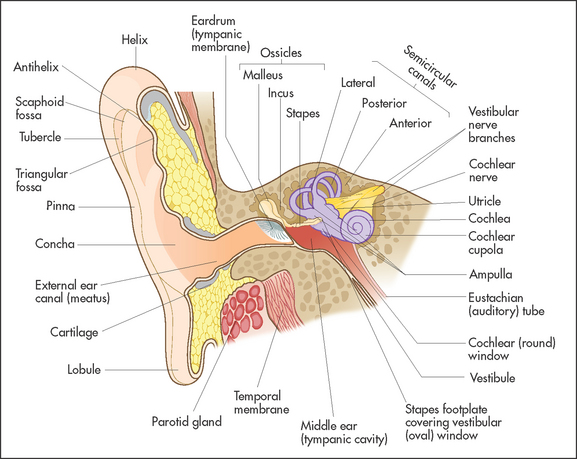
The ear is divided into three parts; the outer, middle and inner ear:
• The outer ear comprises the pinna, the external auditory canal and the ear drum (tympanic membrane), which are easily assessed with simple equipment (see Figure 36.13). Glands in the skin of the auditory canal secrete cerumen.f As cells desquamate from the outer surface of the ear drum they combine with cerumen and migrate outwards to produce normal ear wax.
• The middle ear includes the inner layer of the tympanic membrane, the tympanic cavity (epi-meso-hypotympanum), the ossicles (malleus, incus and stapesg), the Eustachian tube and mastoid air cells. The Eustachian tube connects the middle ear with the nasopharynx. A branch of the facial nerve, the chorda tympani,h enters the tympanic cavity through its posterior wall and traverses the pars flaccid of the tympanic membrane, over the neck of the malleus adjacent to the mucosa, on its way back from receiving taste sensation from the front of the tongue.
• The inner ear (labyrinth) has vestibular (concerned with balance) and cochlear (concerned with hearing) parts. The vestibular part includes the semicircular canals that lie at right angles to each other. Movements of the head disturb the endolymph, a fluid that fills the canals. This stimulates hairs, which cause nerve impulses to travel in the vestibular part of the eighth nerve. Movement of the stapes on the oval window of the cochlear stimulates hair cells in the cochlear, which convert this movement into nerve impulses that travel in the cochlear part of the eighth nerve.
HISTORY
Patients may have symptoms from any of the three parts of the ear:
1. Outer ear: symptoms include itch, erythema and discharge (perforated drum and infection or otitis externa; see List 38.4). The pinna can be damaged by trauma or affected by acquired or inherited diseases of cartilage. Otorrhoea is a more chronic scanty but offensive discharge. It may be due to a cholesteatoma. This is a growth of stratified squamous epithelium that begins in the middle ear or mastoid. It is a benign, slowly growing lesion that destroys bone and ear tissue as it grows. When perforation of the tympanic membrane occurs, cheesy white discharge can occur. It results in loss of hearing if the ossicles are involved. Accumulations of ear wax are a cause of deafness.
2. Middle ear: symptoms include infection, which is common in children, and causes pain and, if the eardrum ruptures, a purulent discharge. Otosclerosis is an inherited abnormality that affects the ossicles and causes deafness. Middle ear tumours and chronic middle ear infection are a cause of deafness.
3. Inner ear: deafness and balance problems including vertigo are the usual symptoms of inner ear disease. Tinnitus, which is usually described as a ‘ringing in the ears’, occurs with most types of inner ear disease.
A patient who complains of deafness needs to be asked about the effect of the condition on work, family life and social activities. Ask about the severity of the deafness, the age of onset and the rapidity of onset. Also enquire what coping mechanisms have been tried. These may include hearing aids, sign language and support groups. People who have been deaf from childhood may have speech problems and educational difficulties. All these need to be assessed.
For any patient who presents with deafness, certain questions may help determine the cause (see Questions box 38.3). Sometimes the way a patient speaks during the interview can be helpful. Patients with conductive deafness hear their own voices by bone conduction and often think they are speaking loudly but they tend to speak softly. Those with sensorineural deafness do not hear their own voices well and tend to speak loudly.
Tests of hearing can also provide information about the severity and anatomical site of hearing loss.
EXAMINATION METHOD
Ear examination consists of inspection and palpation, otoscopy, tuning fork assessment, testing hearing and peripheral vestibular examination. In some cases lower cranial nerve assessment is indicated.
Inspect the position of the pinna and note its size and shape. Note any scars or swelling around the ears. Look for an obvious accessory auricle (separate piece of cartilage away from the pinna), cauliflower ears (haematomas from recurrent trauma, which obscure the normal anatomical features of the pinna) and bat ears (protrusion of the ears from the side of the head).
Look for inflammation externally and any obvious ear discharge. Inspect the auditory meatus and outer ear. There are four types of otitis externa, a condition associated with inflammation of the skin of the external canal:
1. Acute localised otitis externa involves the outer third of the auditory canal where the skin overlies cartilage and hair follicles are present. It is a form of furunculosis and is usually a result of S. aureus infection.
2. Acute diffuse otitis externa is often called swimmer’s ear although it occurs in people who have not been swimming. Excessive moisture, heat and humidity, loss of protective cerumen and an increase in pH are responsible for skin maceration and irritation. Infection may occur with Pseudomonas aeruginosa. The initial symptom is itching, which can progress to pain and is made worse by movement of the pinna. The appearance on examination ranges from mild erythema to severe erythema and swelling. There may be a small amount of white, clumpy discharge.
3. Chronic otitis externa is usually the result of repeated local irritation. This may be due to persistent drainage of a chronic middle ear infection but can also be caused by the insertion of foreign bodies into the ear (e.g. cotton swabs, ear picks). Itch is a more prominent symptom than pain. The appearance is of scaly erythematous dermatitis. It must be distinguished from other forms of dermatitis such as psoriasis, atopic dermatitis and seborrhoeic dermatitis.
4. Malignant (invasive) otitis externa is an aggressive and sometimes life-threatening condition. It affects elderly diabetics and immunocompromised patients. It begins in the external auditory canal and spreads slowly inwards. Untreated it can cause osteomyelitis of the base of the skull and reach the meninges and the brain. Pseudomonas infection is the most common cause but other organisms can be responsible. Deep otalgia is the most predominant symptom. The appearance at first is like that of severe chronic otitis externa. On examination there is discharge and the canal appears swollen and erythematous.
Then look for signs of gouty tophi (nodular, firm, pale and non-tender chalky depositions of urate in the cartilage of the ear, specific but not sensitive for gout).
Palpate the pinna for swelling or nodules. Pull down the pinna gently; the manoeuvre is often painful when there is infection of the external canal.
Otoscope examination of the ears requires use of an earpiece that fits comfortably in the ear canal to allow inspection of the ear canal and tympanic membrane (see Figure 38.14). This examination is essential for any patient presenting with an upper respiratory tract infection, any symptom related to the ears, dizziness, facial weakness or head injury. Always examine both ears!
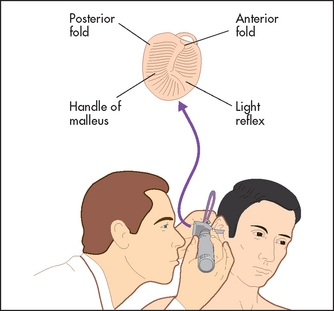
The correct technique is as follows. Ask the patient to turn his or her head slightly to the side, then pull the pinna up, out and back to straighten the ear canal and provide optimal vision. Stretch out the fingers of your hand holding the otoscope to touch the patient’s cheek, to steady the instrument and to prevent sudden movements of the patient’s head. When examining the patient’s right ear, the otoscope is preferably held in a downward position with the right hand, while using the left hand to pull the pinna. An alternative position involves holding the otoscope upwards, but there is a risk that if the patient moves suddenly injury is more likely to occur.
Look at the external canal for any evidence of inflammation (e.g. redness or swelling) or discharge. There should be no tenderness unless there is inflammation. Ear wax is usually white or yellowish, and translucent and shiny; it can be moist or hard and impacted. It may obscure the view of the tympanic membrane. Blood or cerebrospinal fluid (watery, clear fluid) may be seen in the canal if there is a fracture at the base of the skull. In patients with herpes zoster, there may be vesicles (fluid-filled blisters) on the posterior wall around the external auditory meatus.
Inspect the tympanic membrane (ear drum) by introducing the speculum further into the canal in a forward but downward direction. The normal tympanic membrane is a pearly grey colour. It is ovoid in shape and semi-transparent (see Figure 38.15). The upper fifth is called the pars flaccida and the lower four-fifths are called the pars tensa. The handle of the malleus is often visible near the centre of the pars tensa. From the lower end of the handle a bright cone of light should be visible: the light reflex. The presence or absence of the light reflex is not a sensitive or a specific sign of disease (see Figures 38.16 and 38.17). Note the colour, transparency and any evidence of dilated blood vessels (hyperaemia—a sign of otitis media; see Figure 38.17). Look for bulging or retraction of the tympanic membrane. Bulging can suggest underlying fluid or pus in the middle ear. Retraction means a reduction in pressure in the middle ear and is a sign of a blocked Eustachian tube. Perforation of the tympanic membrane should be noted (see Figure 38.18).
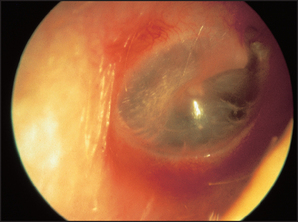
Figure 38.15 The tympanic membrane as viewed through an otoscope (From Mir MA. Atlas of clinical diagnosis, 2nd edn. Edinburgh: Saunders, 2003, with permission.)
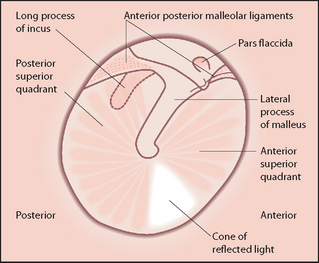
Figure 38.16 The detail of the tympanic membrane (From Mir MA. Atlas of clinical diagnosis, 2nd edn. Edinburgh: Saunders, 2003, with permission.)
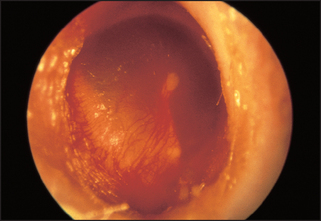
Figure 38.17 Otitis media with hyperaemia of the tympanic membrane (From Mir MA. Atlas of clinical diagnosis, 2nd edn. Edinburgh: Saunders, 2003, with permission.)
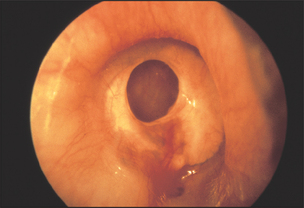
Figure 38.18 Perforated tympanic membrane (From Mir MA. Atlas of clinical diagnosis, 2nd edn. Edinburgh: Saunders, 2003, with permission.)
If a middle ear infection is suspected, pneumatic auriscopy can be useful. Use a speculum large enough to occlude the external canal snugly. Attach a rubber squeeze bulb to the otoscope. When the bulb is squeezed gently, air pressure in the canal is increased and the tympanic membrane should move promptly inwards. Absence of, or a decrease in, movement is a sign of fluid in the middle ear.
To test hearing, whisper numbers or words such as ‘mark’ or ‘park’ into one of the patient’s ears while the other ear is distracted by movement of your finger in the auditory canal or the canal is occluded by pressure on the tragus. It is important to stand behind the patient to prevent lip reading. Then repeat the process with the other ear. With practice, the normal range of hearing is appreciated. If a patient says he or she is deaf, or the whisper test is positive, formal hearing testing (audiometry) is indicated.3
Traditionally, Rinné’s and Weber’s tests are performed if deafness is suspected, but these are not very useful screening tests3:
1. Rinné’s test: place a vibrating 512 Hz tuning fork on the mastoid process. When the sound is no longer heard move the fork close to the auditory meatus where, if air conduction is (as is normal) better than bone conduction, it will again be audible.
2. Weber’s test: place a vibrating 512 Hz fork at the centre of the patient’s forehead. Nerve deafness causes the sound to be heard better in the normal ear, but with conduction deafness the sound is heard better in the abnormal ear.
Nose and sinuses
EXAMINATION ANATOMY
The upper one-third of the nose is formed by the two nasal bones and the lower two-thirds are formed from cartilage (see Figure 38.19). Cartilage divides the nose into its two cavities. The nasal bones articulate with the frontal bones and the maxilla. On the lateral walls of the nose the three pairs of nasal turbinates (superior, middle and inferior) cause turbulence as air enters the nose. This makes small particles drop onto the nasal mucosa, where cilia sweep them into the nasopharynx. The air is also warmed and humidified in the nose. Below each turbinate is a meatus named for the turbinate above it.
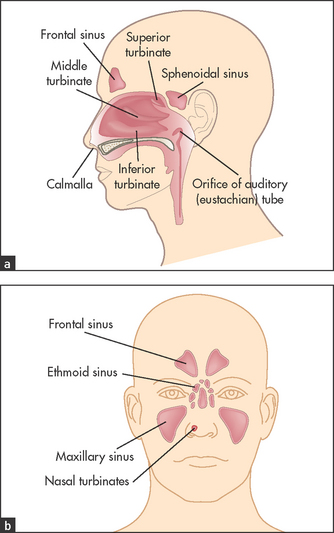
Figures 38.19 Anatomy of the nose (a) Coronal view of paranasal sinuses; and (b) sagittal view of paranasal sinuses.
The frontal, maxillary and anterior ethmoid sinuses drain via the middle meatus. The posterior ethmoid sinus drains via the superior meatus. Drainage is assisted as a result of action of the ciliated epithelium. The maxillary sinus drains upwards against gravity through its ostium into the nasal cavity. This explains the importance of postural drainage for the treatment of bacterial sinusitis and why water drips from swimmers’ noses when they bend over to dry their hair. The nasolacrimal duct drains into the inferior meatus. Drainage can be interrupted as a result of oedema (e.g. allergic rhinitis), mechanical obstruction (e.g. nasal polyps) or impaired ciliary function (Kartagener’s syndrome).
The turbinates are vascular structures and their blood supply is under autonomic control. Sympathetic stimulation causes vasoconstriction and shrinkage of the turbinates. Parasympathetic stimulation causes vasodilation, swelling and sometimes obstruction of airflow and a watery discharge. The blood supply to the nose is from the internal and external carotid arteries. The blood vessels of the anterior nasal septum meet at Little’si area. This is about 2 centimetres from the nares (nostrils). Nose bleeds often come from this vascular area.
The nerve supply of the nose includes the olfactory nerve, which supplies the olfactory epithelium in the upper part of the nose. Fibres of the olfactory nerve pass through the cribriform plate of the ethmoid bone to reach the olfactory bulb in the brain. The rest of the inside of the nose is supplied by branches of the trigeminal nerve.
The vascular nasal mucosa produces mucus, which contains immunoglobulins. Mucus and the nasal hairs (vibrissae) trap particles and prevent them entering the lungs. The mucus is swept backwards by cilia and swallowed.
HISTORY
Common presenting problems include the following:
• Nasal discharge (a runny nose): consider allergy (watery discharge), a cold (coryza; more viscous discharge with or without fever and systemic symptoms) or sinusitis or a foreign body (purulent discharge)—see Questions box 38.4.
• Blocked nose: cold, foreign body, deviated nasal septum.
• Epistaxis: trauma, allergy or a cold. Ask about anti-coagulation and use of anti-platelet drugs.
• Anosmia or reduced sense of smell (often with apparent loss of taste): consider mechanical obstruction due to polyps, infection or trauma if there is complete anosmia.
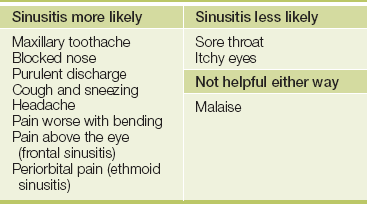
• Symptoms of sinusitis: ‘sinus trouble again’, cough, nasal congestion, sneezing, facial pain or headache worse with bending forwards, purulent discharge—see Table 38.4.
EXAMINATION METHOD
Nose and sinus examination consists of inspection, palpation and testing the sense of smell.
Inspect the skin. The patient concerned about a big nose may have a rhinophyma.j This enlargement and distortion of the skin of the nose is due to sebaceous gland enlargement. It is often associated with rosacea. Note any nasal deviation (best seen from behind the patient and looking down). Note any periorbital swelling (e.g. from sinusitis). Inspect the nares by pressing the tip of the nose upwards with the thumb.
Palpate the nasal bones. Then feel for facial swelling or signs of inflammation. Block each nostril to assess any obstruction by asking the patient to inhale. If there is a history of anosmia (loss of smell), test smell as described in Chapter 32 (cranial nerve I).
A saddle-nose deformity (collapse of the nasal septum) can occur in Wegener’s granulomatosis and relapsing polychondritis.
Examine inside the nose using a nasal speculum. This simple device with two blades can be used to open the nares. Hold the device in your left hand and introduce it into the patient’s nose with the blades facing up and down. The blades should not rest or be pushed against the nasal septum. Use your other hand to steady and move the patient’s head so that the inside of the nose can be seen. Your left index finger should rest against the patient’s nose to steady the upper blade. Note:
1. deviation or perforation of the anterior septum
2. the colour of the mucosa—usually a rich dark-red colour (darker than the oral mucosa) and smooth, moist and clean
3. the presence of bleeding, swelling or exudate
4. the presence of polyps—most often seen near the middle meatus
6. signs of bleeding at Little’s area if epistaxis has occurred
7. the presence and nature of discharge (e.g. watery, purulent, bloody)
SINUSITIS
Sinusitis is inflammation of the paranasal sinuses. Pain and tenderness over the sinuses occurs, which in adults is classified as acute if less than 4 weeks in duration, subacute if 4–12 weeks in duration and chronic if greater than 12 weeks in duration. Most acute sinusitis is secondary to viral infection.4
Acute bacterial sinusitis (see Figure 38.20) can occur after viral infection or in the setting of allergic rhinitis, in patients with anatomical abnormalities such as nasal septal deformity or polyps in the nose, or in immunocompromised patients. The most common bacterial causes of sinusitis are Streptococcus pneumoniae and Haemophilus influenzae. The four key clinical features suggesting that sinusitis may be bacterial are: (1) worsening symptoms after early improvement (a biphasic illness pattern); (2) purulent discharge from the nose; (3) tooth or facial pain over the maxillary sinus (especially if unilateral); and (4) tenderness over the maxillary sinus (unilaterally). Fever may occur.

Figure 38.20 Bacterial ethmoidal sinusitis (Courtesy of Dr A Watson, Infectious Diseases Department, The Canberra Hospital)
Complications of acute bacterial sinusitis can include orbital cellulitis, meningitis, cavernous sinus thrombosis, brain abscess and osteolitis of the sinus bones. Therefore, if patients present with any of the following warning signs—periorbital oedema, visual changes or changes in mental status—you should be concerned about complicated bacterial sinusitis. Orbital cellulitis typically presents with erythema of the eyelid, oedema of the eyelid and proptosis. Periorbital cellulitis is a more benign condition caused by primary infection of the skin around the orbit.
Potential mimickers of acute bacterial sinusitis include Wegner’s granulomatosis, carcinoma or lymphoma, sarcoidosis and, in immunocompromised or diabetic patients, fungal sinusitis. Chronic sinusitis presents with chronic sinus congestion, postnasal drip, cough, headache and bad breath.
Rhinocerebral mucormycosis is a fungal infection that destroys the sinuses. A black eschar may be seen on the nasal mucosa or palate.
Examination
There are two commonly used ways of illuminating the sinuses. The simpler method is to place a bright torch or proprietary transilluminoscope in the patient’s mouth. The room must be completely dark and the patient must seal the lips around the device. Normal sinuses are visible through the skin of the face and appear as a warm glow. This method has the advantage that the two sides can be compared. The second method avoids the need to clean the torch between examinations. Place the torch over the infraorbital rim and shield your eyes from the light while peering into the patient’s mouth to look for illumination of the hard palate.
Mouth and throat
EXAMINATION ANATOMY
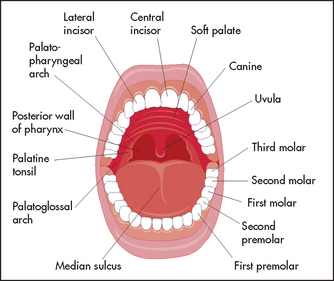
The main structures of the oral cavity (see Figure 38.21) are as follows:
• The lips are covered in a thin epidermis and have numerous vascular papillae (the cause of their red colour).
• The tongue is attached to the hyoid bone. Its functions include eating and speech and it is the main area where taste is detected. It has a central sagittal median sulcus that ends posteriorly at the foramen caecum. The surface is rough because of its covering of papillae. The fungiform papillae are found on the tip and sides of the tongue. The largest papillae lie in front of the caecum and are called the circumvallate papillae. They divide the tongue into the posterior one-third and the anterior two-thirds.
• The hard palate is a concave bony structure. Anteriorly its mucosa has raised folds called rugae. The soft palate is muscular and flexible. It ends at the uvula, which helps close off the nasopharynx during swallowing.
• The taste buds are found on the sides of the papillae. The chorda tympani, which is a division of the facial nerve, receives taste input from the anterior two-thirds of the tongue and the glossopharyngeal nerve from the posterior one-third. Salty taste is detected at the sides of the tongue, sweet taste at the tip of the tongue and sourness and bitterness from the posterior third (glossopharyngeal nerve).
• The salivary glands lubricate the mouth and contain digestive enzymes including amylase. The largest are the parotid glands, which lie in front of the ears. They drain via Stensen’s duct and through a papilla opposite the upper first molars. The submandibular glands are next in size. They are located below the angle of the mandible. They drain through Wharton’s duct to papillae on either side of the frenulum below the tongue. The sublingual gland is found on the floor of the mouth beneath the tongue and drains through numerous small ducts.
HISTORY
The important symptoms of mouth and throat disease include the following:
• Pain in the mouth or throat (see Questions box 38.5).
• Ulceration (see Questions box 38.6).
• Bleeding: ask where the blood seems to be coming from (e.g. gums, throat or coughed up). Find out if the patient is aware of a mass in the mouth or throat, whether there is bleeding anywhere else and whether he or she is taking anti-platelet or anti-coagulant drugs.
• A mass or lump in the mouth: ask if this is painful (infection) or not, how long it has been present and whether it has been bleeding (neoplasm).
• Dry mouth: ask about medications (e.g. anti-depressants, antihistamines), previous radiotherapy (damage to salivary glands), dry eyes (sicca syndrome) and thrush (Candida infection is an association).
• Dysphagia: ask if the patient has difficulty swallowing only solids (oesophageal stricture or tumour) or liquids and solids (oesophageal motility problems). Is the problem associated with a sore throat (tonsillitis)?
• Dysphonia (difficulty with speech; see Questions box 38.7).
EXAMINATION METHOD
Throat examination consists of inspection and palpation.
Inspect the lips for herpetic ulcers, Peutz-Jeghers syndrome, cyanosis and masses. The most common cause is a mucocele. These cystic painless lesions can be as large as a few centimetres in diameter. They are caused by traumatic damage or obstruction of a small salivary gland.
Look at the buccal mucosa, palate and teeth. Using a light, push the buccal mucosa out of the way with a tongue depressor. Note any signs of inflammation (e.g. redness, swelling). Look at the parotid duct opening (for inflammation). White painless plaques (leucoplakia) may be present on the gingivae, tongue or buccal mucosa. This is a precancerous condition. Lichen planus also causes a white painless lesion in the mouth. It has a reticulated pattern. Look for masses and ulcerated lesions. Inspect the teeth for obvious decay and infection.
Look at the gingivae for hypertrophy (associated with phenytoin use, leukaemia and pregnancy), bleeding and inflammation. Erythroplakia is a mucosal abnormality characterised by red granular papules that bleed easily. It has more malignant potential than leucoplakia.
Inspect the tongue first in the mouth, then ask the patient to poke it out to one side and then the other. Weakness of the tongue due to neurological or muscular disease may be seen. Look for masses and mucosal changes as with the rest of the mouth. The surface of the tongue may show localised red areas denuded of papillae surrounded by white or yellow margins and looking rather like a map. This is called geographical tongue and is quite benign. Elongation and pigmentation (from food or tobacco staining or certain microorganisms) of the papillae makes the tongue look black and hairy. This is also benign. A tongue with exaggerated fissures is called a scrotal tongue; it is also benign. Look for evidence of Candida infection (see Figure 38.23). These white lesions cover an inflamed mucosa and may be the result of immunodeficiency or recent antibiotic use.

Figure 38.23 Candidiasis (Courtesy of Dr A Watson, Infectious Diseases Department, The Canberra Hospital)
Inspect the floor of the mouth and under the tongue. Ask the patient to lift the tongue up onto the hard palate to give you a good view. Large veins may be visible under the tongue in elderly people. These are benign and are not a cause of bleeding. Inspect the mucosal surfaces for the abnormalities described above. There may also be a ranula.k This is a large mucus retention cyst. These can be quite large and although painless eventually interfere with eating and speech.
Inspect the hard and soft palates for similar mucosal lesions and the hard palate for petechiae. A common benign finding is a bony swelling of the posterior part of the hard palate. This occurs in the midline and is often lobulated. It is called a torus palatinusl
Feel the tongue with your gloved hand. Hold it with some gauze with one hand and palpate with the other. The anterior two-thirds can usually be palpated without provoking the gag reflex. Feel for induration (hardening) of any lesion (a sign of malignancy).
Now feel the floor of the mouth. Using both gloved hands, feel with your right index finger pointing downwards under the tongue and your left index finger under the chin and pushing upwards. Use the thumb and third finger of your left hand to push the patient’s cheeks in between the teeth; this is a precaution that prevents your finger being bitten. Feel between your fingers for masses and tenderness. Feel the submandibular salivary glands.
Ask the patient to say ‘Ah’, then inspect the oropharynx and uvula (there is often a need to press a tongue depressor on the tongue to see properly—and using two tongue depressors can help even further). The tongue should be pushed forwards behind the front teeth. Applying the depressor too far back will cause gagging; too far forward and the tongue will roll up and obscure the pharynx. Inspect the tonsils (note the size, shape and colour, and any discharge or membrane—they involute in adults and may not be seen). Enlarged tonsils with a covering of membrane or pus are typical of viral or bacterial tonsillitis. Enlargement may occur in patients with leukaemia and lymphoma.
Examine the cervical lymph nodes.
Things to look, feel and listen for in the mouth and throat examination include:
2. the state of the teeth and gums
3. gum and tongue ulcers (herpes simplex, aphthous ulcers [see Figure 38.22], candidiasis [see Figure 38.23])

Figure 38.22 Buccal ulcer (Courtesy of Dr A Watson, Infectious Diseases Department, The Canberra Hospital)
4. mucosal mass (consider malignancy)
6. Koplik’s spot (measles; see Figure 38.24)

Figure 38.24 Koplik’s spot (measles) (Courtesy of Dr A Watson, Infectious Diseases Department, The Canberra Hospital)
7. tongue: smooth (iron, B12 deficiency), big (acromegaly, tumour), wasted and fasciculating (motor neuron disease), ulcers and white patches
8. tonsils: present or absent, inflamed or covered in pus; enlarged (lymphoma)
9. salivary glands: size and tenderness; squeeze to express pus through the salivary duct
10. the draining lymph nodes: tenderness and enlargement (see Figure 38.25)

PHARYNGITIS
A sore throat due to an exudative pharyngitis in adults is usually secondary to infection. The specific causes of pharyngitis include viruses (especially Epstein-Barr virus [EBV] in adolescents) in about 50% of cases, while about 10% of cases are due to the group A beta-haemolytic streptococci (see Figure 38.26). Neisseria gonorrhoea is an uncommon cause of pharyngitis in adults, and primary HIV infection is an occasional cause; typically, there are sexual risk factors present in the history. The other two most important viruses are herpes simplex and adenovirus. Many cases of pharyngitis are of unknown cause. Clinically, there is redness of the pharynx with or without ulceration.

Figure 38.26 Streptococcal throat (Courtesy of Dr A Watson, Infectious Diseases Department, The Canberra Hospital)
Clinical criteria help determine whether pharyngitis may be due to beta-haemolytic streptococcus or not (the four-item Centor score):5
If all four criteria are present, this helps predict the presence of this infection, while the absence of the last three strongly suggests that the infection is not due to beta-haemolytic streptococcus. It is important to recognise this because beta-haemolytic streptococcus infection of the pharynx can lead to direct infectious complications (otitis media, sinusitis, peritonsillar abscess [quinsy] and submandibular space infection [Ludwig’sm angina]) and to indirect complications (acute rheumatic fever and glomerulonephritis). Glomerulonephritis is not prevented by antibiotic therapy.
SUPRAGLOTTITIS (EPIGLOTTITIS)
Supraglottitis is a rare but important cause of sore throat.6 This disease classically presents with a triad of sore throat, painful swallowing (odynophagia) and fever. The patient may uncommonly have stridor, which may be misdiagnosed as asthma; here there is inspiratory wheeze due to the inflammation above the epiglottis. Pooling of secretions is another clue to the diagnosis. Urgent medical attention is indicated to prevent airway obstruction.
Common investigations
CT scans can be commonly used in the diagnosis of sinusitis and nasopharyngeal tumours. They can help identify the spread of infection into the brain and orbits (see Figures 38.27 and 38.28).
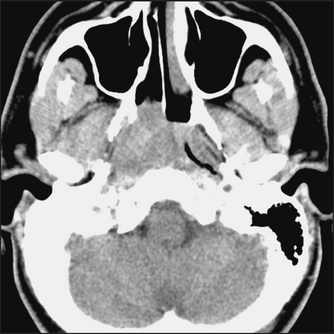
Figure 38.27 Nasopharyngeal carcinoma This CT scan shows a soft-tissue mass obstructing the right nasopharynx and right Eustachian tube. (Haaga. CCT and MRI of the whole body, 5th edn. Mosby, 2008.)
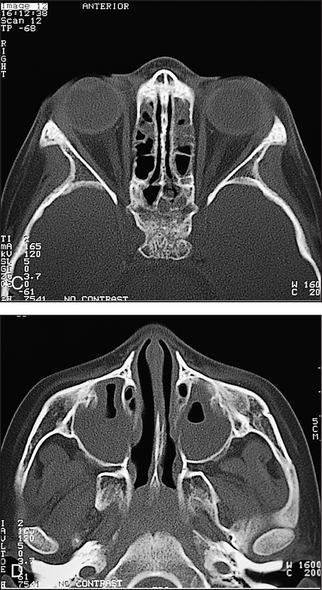
Figure 38.28 Acute sinusitis This CT scan coronal view shows opacification of the right maxillary sinus; the left is almost completely opacified, with only a small air pocket visible. (Zitelli, Davis. Atlas of pediatric physical diagnosis, 5th edn. Elsevier, 2007.)
The visual fields can be mapped accurately with a visual field chart. Retinal photographs are often used for the screening of diabetic patients.
References
1. Robinett, DA, Kahn, DH. The physical examination of the eye. Emerg Med Clin N Am. 2008; 26:1–16. [An excellent summary of eye anatomy and examination.].
2. McGee, S. Evidence-based clinical diagnosis, 3rd edn. St Louis: Saunders, 2012.
3. Bagai, A, Thavendiranathan, P, Detsky, AS. Does this patient have hearing impairment. JAMA. 2006; 295(4):416–428.
4. Gwaltney, JM, Sydnor, A, et al. Etiology and antimicrobial treatment of acute sinusitis. Ann Otol Rhinol Larygol Suppl. 1981; 90(3pt 3):68–71.
5. McIsaac, WJ, Kellner, JD, Aufricht, P, Vanjaka, A, Low, DE. Empirical validation of guidelines for the management of pharyngitis in children and adults. JAMA. 2004; 291(13):1587–1595.
6. Cirilli, AR. Emergency evaluation and management of the sore throat. Emerg Med Clin North Am. 2013; 31(2):501–515.
aFrom the Latin word for tear, lacrima. Hence the famous phrase in The Aeneid when Aeneas sees the depictions of the fall of Troy on the new walls of Carthage and becomes very emotional, saying ‘Sunt lacrimae rerum’—there are tears for things.
bJohann Friedrich Horner (1831–1886), professor of ophthalmology, Zürich, described this in 1869.
cEnophthalmos, or retraction of the eye, which is often mentioned as a feature of Horner’s syndrome, probably does not occur in humans. It may occur in cats. Horner’s original paper was very specific about miosis and ptosis, but only casually mentioned that ‘the position of the eye seemed very slightly inward’. Apparent enophthalmos results from a combination of ptosis and an elevated lower lid (upside-down ptosis).
dOcclusion of any of the following vessels may result in this syndrome: vertebral; posterior inferior cerebellar; superior, middle or inferior lateral medullary arteries.
eSir Jonathon Hutchinson (1828–1913). Among other appointments he was surgeon to Moorfields Eye Hospital. He was president of the Royal College of Surgeons in 1889, elected to the Royal Society in 1882 and knighted in 1908.
fFrom the Latin word for wax. Cerula, the diminutive, means a little piece of wax.
gFrom the Latin for hammer, anvil and stirrup.
hFrom the Latin for the string of a musical instrument and a drum.
iWilliam Little (1810–94), a surgeon at St Luke’s hospital in New York, described this area in 1843.
jFrom the Greek words meaning nose and an inflamed swelling.
kFrom the Latin word for tadpole or little frog.
lFrom the Latin for a swelling or protuberance.
mWilhelm Ludwig (1790–1865) was an army surgeon during the Napoleonic wars and a Russian prisoner of war for 2 years. He became court doctor to King Frederick II and was professor of surgery and midwifery at Tübingen. He described submandibular cellulitis in his first paper, published 20 years after he became a professor. The patient described was Queen Catherine of Würtenberg.