The neurological examination: the cranial nerves
EXAMINATION ANATOMY
More than for any other system of the body, neurological diagnosis depends on localising the anatomical site of the lesion—in the brain, spinal cord or peripheral nerve. Figure 32.1 shows the gross anatomy of the brain and the major functional areas.

As a preliminary to the neurological assessment, the clinician should obtain some biographical information from the patient, including age, place of birth, left- or right-handedness, occupation and level of education.
The examination of the nervous system and the interpretation of findings require a lot of practice. In a viva voce examination, this system more than any other requires a polished technique. The signs need to be elicited carefully because the precise anatomical localisation of any lesions can often be determined this way. It is important, therefore, to remember some elementary neuroanatomy.
Examination can be long and difficult and it is said to take much of a day if absolutely everything that can be done (including psychometric assessment) is done. This is obviously impractical, but a screening examination that will uncover most signs takes only a relatively short time.
The following aspects of the examination should be attended to:
1. General, including examination for neck stiffness, assessment of the higher centres, speech and abnormal movements.
3. Upper limbs. Motor system: inspection, tone, power, reflexes, coordination. Sensory system: pinprick sensation, proprioception, vibration sense, light touch.
4. Lower limbs: as for the upper limbs, but including assessment of walking (gait).
General signs
CONSCIOUSNESS
Note the level of consciousness. If the patient is unconscious,a look for responses to various stimuli (page 478).
NECK STIFFNESS
Any patient with an acute neurological illness or who is febrile or has altered mental status must be assessed for signs of meningism.1
With the patient lying flat in bed, slip your hand under the occiput and gently flex the neck passively (i.e. without assistance from the patient). Bring the chin up to approach the chest wall. Meningism may be caused by pyogenic or other infection of the meninges, or by blood in the subarachnoid space secondary to subarachnoid haemorrhage. There is resistance to neck flexion due to painful spasm of the extensor muscles of the neck. Other causes of resistance to neck flexion are characterised by an equal resistance to head rotation. They include: (1) cervical spondylosis; (2) after cervical fusion; (3) Parkinson’s disease; and (4) raised intracranial pressure, especially if there is impending tonsillar herniation. The Brudzinskib sign is spontaneous flexion of the hips during flexion of the neck by the examiner and indicates meningism.
Kernig’sc sign should also be elicited if meningitis is suspected. Flex each hip in turn, then attempt to straighten the knee while keeping the hip flexed. This is greatly limited by spasm of the hamstrings (which in turn causes pain) when there is meningism due to an inflammatory exudate around the lumbar spinal roots.
Although the diagnostic value has been questioned (combined meningeal signs had a positive LR of 0.92 and a negative LR of 0.88),1 these signs are useful clinically and they have good specificity. However, even the absence of all three items in the classical meningitis triad—fever, headache and neck stiffness—does not rule out meningitis (i.e. it is not very sensitive).2
HANDEDNESS
Shake the patient’s hand and ask if he or she is right- or left-handed. This is polite and allows you to assess the likely dominant hemisphere—94% of right-handed people and about 50% of left-handed people have a dominant left hemisphere. There is division of function between the two hemispheres, the most obvious distinction being that the dominant hemisphere controls language and mathematical functions.
ORIENTATION
Test orientation in person, place and time by asking the patient his or her name, present location and the date (patients who have been in hospital for long periods often get the day wrong as one day seems very much like another in hospital). Disorientation is not a specific localising sign and may be acute and reversible (delirium) or chronic and irreversible (dementia). The mini-mental state examination is a useful way to document the progress of a confusional state or dementia over time.
Next we focus on the head and neck—in particular, the cranial nerves. Subsequent chapters cover speech and the upper and lower limb neurological examinations.
The cranial nerves
Examination anatomy
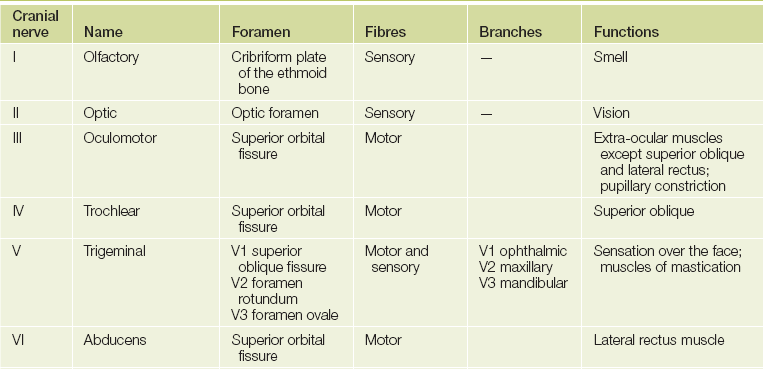
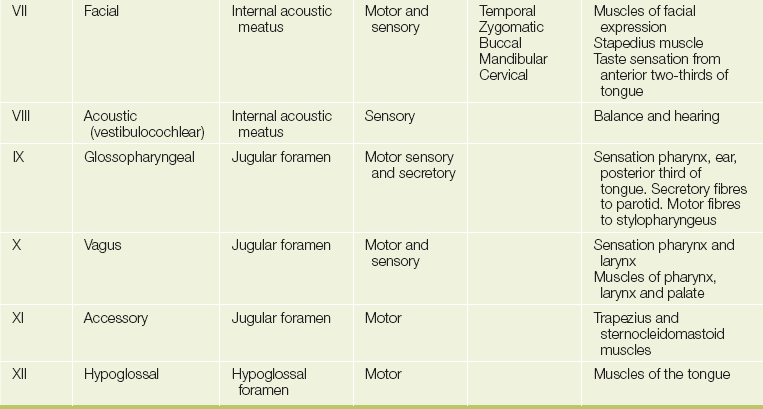
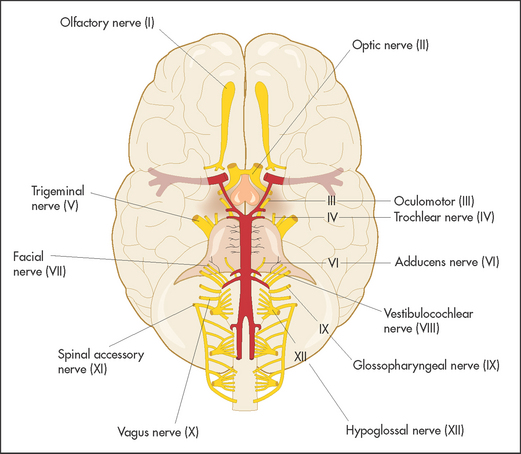
The cranial nervesd (see Figure 32.2 and Table 32.1) arise as direct extensions of the brain (I and II) or from the brainstem (midbrain, pons and medulla)—see Figures 32.12, 32.19 and 32.36 later in the chapter.
GENERAL INSPECTION
If possible, position the patient so that he or she is sitting over the edge of the bed. Look at the patient’s head, face and neck. Acromegaly (page 364), Paget’s disease (page 382) or basilar invagination may be obvious. A careful general inspection may reveal signs easily missed when each cranial nerve is examined separately. This is particularly true of ptosis (page 408), proptosis (page 510), pupillary inequality (page 408), skew deviation of the eyes and facial asymmetry. Inspect the whole scalp for craniotomy scars and the skin for neurofibromas (see Figure 32.3). Look for skin lesions: for example, a capillary or cavernous haemangioma is seen on the face in the distribution of the trigeminal (V) nerve in the Sturge-Webere syndrome. It is associated with an intracranial venous haemangioma of the leptomeninges and with seizures.

Figure 32.3 Subcutaneous neurofibromas in neurofibromatosis type I, associated with optic nerve and pontine gliomas (acoustic neuromas occur in type II)
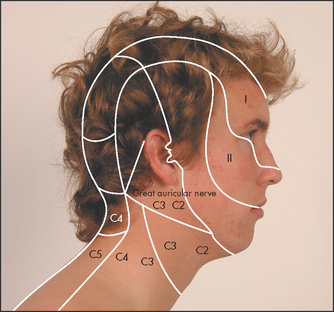
Herpes zoster (shingles) often appears in a nerve distribution as well as helping with the diagnosis of this painful rash. The characteristic distribution of the lesions demonstrates the anatomy of the nerve involved (see Figures 32.4 and 32.22).

Figure 32.4 Herpes zoster in the ophthalmic division of the facial nerve showing the nerve distribution
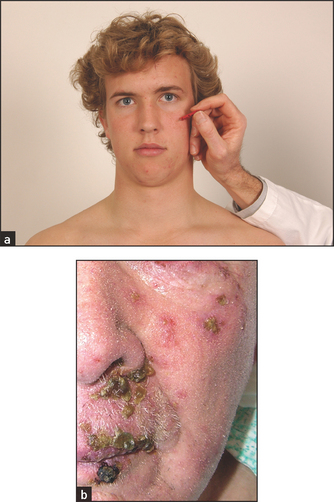
Figure 32.22 (a) Facial sensation V, maxillary division: ‘Does this feel sharp or blunt?’—test all three divisions on each side (b) Herpes zoster in distribution of the maxillary nerve showing distribution of the nerve ((a) Courtesy of Glenn McCulloch)
The cranial nerves are usually tested in approximately the order of their number.3
THE FIRST (OLFACTORY) NERVE
Examination anatomy
The first (olfactory) nervef is a purely sensory nerve whose fibres arise in the mucous membrane of the nose and pass through the cribriform plate of the ethmoid bone to synapse in the olfactory bulb. From here the olfactory tract runs under the frontal lobe and terminates in the medial temporal lobe on the same side.
Examination of the nose and sense of smell
Note the external appearance of the nose. Look for rash or deformity. Then examine the nasal vestibule by elevating the tip of the nose (in adults a speculum is usually needed to give an adequate view).
The first nerve is not tested routinely. If the patient complains of loss of smell (anosmia) or there are other signs suggesting a frontal or temporal lobe lesion, then it should be examined. Anosmic patients sometimes complain of loss of taste rather than loss of smell because the sense of smell plays a large part in the appreciation of taste. Test each nostril separately with a series of bottles containing essences of familiar smells, such as coffee, vanilla and peppermint (this is traditional, but not very reliable). Pungent substances such as ammonia should not be used, first because they upset the patient and second because noxious stimuli of this sort are detected by sensory fibres of the fifth (trigeminal) nerve. An easy way to test smell is to use the isopropyl alcohol wipes present in most hospital clinics. These have a distinctive and non-pungent smell.
Examination of the nasal passages must be performed if anosmia is present. Polyps and mucosal thickening may be seen and may explain the findings.
Causes of anosmia
Most cases of anosmia are bilateral. Causes include: (1) upper respiratory tract infection (most common); (2) smoking and increasing age; (3) ethmoid tumours; (4) basal skull fracture or frontal fracture, or after pituitary surgery; (5) congenital—for example, Kallmann’s syndrome (hypogonadotrophic hypogonadism); (6) meningioma of the olfactory groove; and (7) following meningitis. The main unilateral causes are head trauma without a fracture, or an early meningioma of the olfactory groove.g
THE SECOND (OPTIC) NERVE
Examination anatomy
The optic nerve is not really a nerve but an extension of fibres of the central nervous system that unites the retinas with the brain. It is purely sensory, contains about a million fibres and extends for about 5 centimetres (see Figure 32.5), passing through the optic foramen close to the ophthalmic artery and joining the nerve from the other side at the base of the brain to form the optic chiasm. The spatial orientation of fibres from different parts of the fundus is preserved so that fibres from the lower part of the retina are found in the inferior part of the chiasm, and vice versa. Fibres from the temporal visual fields (the nasal halves of the retinas) cross in the chiasm, whereas those from the nasal visual fields do not. Fibres for the light reflex from the optic chiasm finish in the superior colliculus, whence connections occur with both third nerve nuclei. The remainder of the fibres leaving the chiasm are concerned with vision and travel in the optic tract to the lateral geniculate body. From here the fibres form the optic radiation and pass through the posterior part of the internal capsule, finishing in the visual cortex of the occipital lobe. In their course they splay out so that fibres serving the lower quadrants course through the parietal lobe, while those for the upper quadrants traverse the temporal lobe. The result of the decussation of fibres in the optic chiasm is that fibres from the left visual field terminate in the right occipital lobe, and fibres from the right visual field terminate in the left occipital lobe.
History
The majority of visual symptoms involve reduction in visual acuity. These are discussed in detail with the physical examination findings. Some patients notice a more specific change, which will help direct the examination. Ask about the time course of the visual disturbance and whether it seems to involve the vision of one eye or one visual field. Sudden loss of vision in one eye (often described as an awareness of a curtain being drawn across the eye) may be due to an embolus to the retina. These are called negative visual symptoms. There is usually, but not always, spontaneous return of vision. This is termed amaurosis fugax. Migraine attacks may be preceded by subjective visual changes, including scintillating scotomas, photophobia, blurred vision or hemianopia. Visual hallucinations such as flashing lights and distortions of vision are called positive visual symptoms. They can also occur in psychotic states or as the aura of an epileptic seizure.
More gradual loss of vision has many possible causes.
Examination
Assess visual acuity, visual fields and the fundi.
Visual acuity is tested with the patient wearing his or her spectacles, if used for reading or driving, as refractive errors are not considered to be cranial nerve abnormalities. Use a hand-held eye chart or a Snellen’s charth on the wall. Each eye is tested separately, while the other is covered by a small card.
Formal testing with a standard Snellen’s chart requires the patient to be 6 metres from the chart. Unless a very large room is available, this is done using a mirror. Normal visual acuity is present when the line marked 6 can be read correctly with each eye (6/6 acuity). The examination will be quicker if the patient is asked to read the smallest line possible. If poor visual acuity improves when the patient is asked to read the chart through a pin-hole, refractive error is likely to be the cause. A patient who is unable to read even the largest letter of the chart should be asked to count fingers held up in front of each eye in turn, and if this is not possible, then perception of hand movement is tested. Failing this, test for light perception with a torch.
Any abnormality of the lens, cornea, fundus or optic nerve pathway can cause reduction in visual acuity:
• Causes of bilateral blindness of rapid onset include bilateral occipital lobe infarction, bilateral occipital lobe trauma, bilateral optic nerve damage (as with methyl alcohol poisoning) and hysteria.
• Sudden blindness in one eye can be due to retinal artery or vein occlusion, temporal arteritis (the artery may appear prominent and be tender to palpation; see Figure 32.6), non-arteritic ischaemic optic neuropathy and, occasionally, optic neuritis or migraine.

Figure 32.6 A visibly enlarged temporal artery in a patient with headache (Klippel JH, Dieppe PA (eds). Rheumatology, 2nd edn. Philadelphia: Mosby, 1997.)
• Bilateral blindness of gradual onset may be caused by cataracts, acute glaucoma, macular degeneration, diabetic retinopathy (vitreous haemorrhages), bilateral optic nerve or chiasmal compression, and bilateral optic nerve damage—for example, tobacco amblyopia (blindness due to retinal disease).
Visual fields are examined by confrontation (see Figure 32.7). Always remove a patient’s spectacles first. Your head should be level with the patient’s head. Use a white- or red-tipped hat pin or pen. Test each eye separately. Hold the pin at arm’s length with the coloured head upwards. It should be positioned halfway between you and the patient, and brought in from just outside your peripheral vision until the patient can see it. Make sure that the patient is staring directly at your eye and explain that he or she is looking for the first sight of the pin out of the corner of the eye. When the right eye is being tested the patient should look straight into your left eye. The patient’s head should be at arm’s length and the eye not being tested should be covered. The pin should be brought into the visual field from the four main directions, diagonally towards the centre of the field of vision.
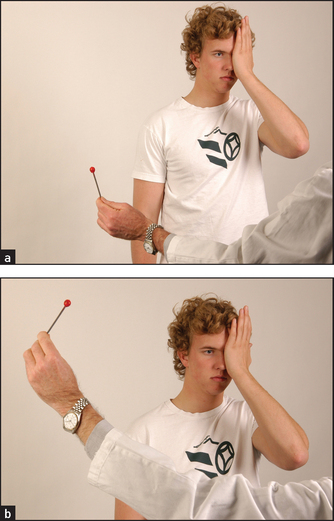
Figure 32.7 Visual field testing: ‘Tell me when you first see the red pin come into view’ (Courtesy of Glenn McCulloch)
Next the blind spot can be mapped out by asking about disappearance of the pin around the centre of the field of vision of each eye. Move the pin slowly across the field of vision. A large central scotoma will lead to its apparent temporary disappearance and then reappearance. Only a gross enlargement may be detectable.
The red pin can also be used at this point to test for optic nerve pathology. Ask the patient to compare the colour of the pin when it is looked at with one eye covered at a time. The red colour will appear less intense or ‘washed out’ when the bad eye is used.
If the patient has such poor acuity that a pin is difficult to see, map the fields with your fingers. You can also use your fingers to perform a quick screening test of the visual fields. Usually you hold up two fingers and bring them into the centre of vision in the four quadrants. Wiggle your fingers and ask the patient to say ‘yes’ when movement of the fingers is first seen. The following patterns of visual field loss may be detected (see Figures 32.8 and 32.9):
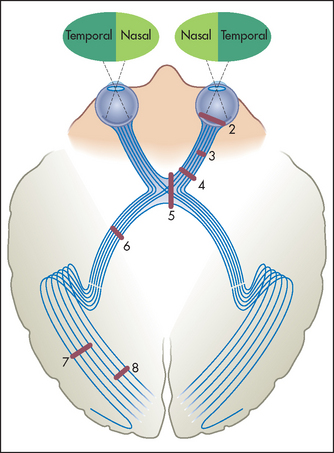
Figure 32.8 The visual fields and optic pathways
Numbers indicate sites of lesions producing field defects shown in Figure 32.9. (Adapted from Snell RS, Westmoreland BF. Clinical neuroanatomy for medical students, 4th edn. Boston: Little Brown, 1997.) Little Brown
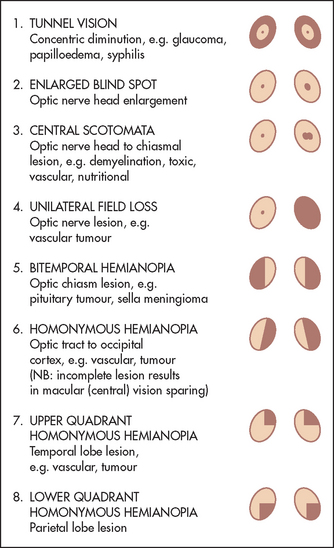
Figure 32.9 Visual field defects with lesions at various levels along the optic pathway, at sites indicated in Figure 32.8 (Adapted from Bickerstaff ER, Spillane JA. Neurological examination in clinical practice, 5th edn. Oxford: Blackwell, 1989.) Blackwell
• Concentric diminution of the field (tunnel vision) may be caused by glaucoma, retinal abnormalities such as chorioretinitis or retinitis pigmentosa, papilloedema or acute ischaemia, as with migraine. Normally, even a reduced field of vision widens as objects are moved further away. Tubular diminution of the visual fields suggests hysteria. There is always a small area close to the centre of the visual fields where there is no vision (the blind spot). This is the area where the optic disc is seen on fundoscopy and is the point where the optic nerve joins the retina. The blind spot enlarges with papilloedema.
• Central scotomata, or loss of central (macular) vision, may be due to demyelination of the optic nerve (multiple sclerosis causes unilateral or asymmetrical bilateral scotomata); toxic causes, such as methyl alcohol (symmetrical bilateral scotomata); nutritional causes, such as tobacco or alcohol amblyopia (symmetrical central or centrocaecal scotomata); vascular lesions (unilateral); and gliomas of the optic nerve (unilateral).
• Total unilateral visual loss is due to a lesion of the optic nerve or to unilateral eye disease.
• Bitemporal hemianopia is due to a lesion that affects the centre of the optic chiasm, damaging fibres from the nasal halves of the retinas as they decussate. This will result in loss of both temporal halves of the visual fields. Causes include a pituitary tumour, a craniopharyngioma and a suprasellar meningioma.
• Binasal hemianopia is very rare and is due to bilateral lesions affecting the uncrossed optic fibres, such as atheroma of the internal carotid siphon.
• Homonymous hemianopia is due to a lesion that damages the optic tract or radiation, affecting the visual field on the right or left side. For example, left temporal and right nasal field loss will occur with a right-sided lesion. The exact nature of the defect depends on the site of interruption of the fibres. In the optic tract the defect is usually complete—there is no macular sparing. In the more posterior optic radiation the macular vision is usually spared if the cause is ischaemia, but not if a destructive process such as tumour or haemorrhage is responsible. The macular cortical area is thought to have some additional blood supply from the anterior and middle cerebral arteries.
• Homonymous quadrantanopia is loss of the upper or lower homonymous quadrants of the visual fields. This may be due to temporal lobe lesions (e.g. vascular lesions or tumours), which cause upper quadrantanopia, or parietal lobe lesions (e.g. vascular lesions or tumours), which cause lower quadrantanopia.
The presence of an abnormality has diagnostic value (LR+ 4.2 to 6.8),4 but absence is largely unhelpful.
Fundoscopy does not begin with examination of the fundus, but rather with visualisation of the cornea with the ophthalmoscope. Use your right eye to look in the patient’s right eye, and vice versa. This prevents contact between the noses of the patient and the examiner in the midline. Keep your head vertical so that the patient can fix with the other eye.
Begin with the ophthalmoscope on the +20 lens setting, with the patient gazing into the distance. This prevents reflex pupil contraction, which occurs if the patient attempts to accommodate. Look first at the cornea and iris, and then at the lens. Large corneal ulcers may be visible, as may undulation of the rim of the iris, which is due to previous lens and lens capsule extraction and is called iridodonesis.i
By racking the ophthalmoscope down towards 0, the focus can be shifted towards the fundus. Opacities in the lens (cataracts) may prevent inspection of the fundus. When the retina is in focus, search first for the optic disc. This is done by following a large retinal vein back towards the disc. All these veins radiate from the optic disc.
The margins of the disc must be examined with care. The disc itself is usually a shallow cup with a clearly outlined rim. Loss of the normal depression of the optic disc will cause blurring at the margins and is called papilloedema (see Figure 32.10(a)). It indicates raised intracranial pressure. If papilloedema is suspected, the retinal veins should be examined for spontaneous pulsations. When these are present raised intracranial pressure is excluded, but their absence does not prove the pressure is raised.5 If the appearance of papilloedema is associated with demyelination in the anterior part of the optic nerve, it is called papillitis. These two can be distinguished because papillitis causes visual loss but papilloedema does not.
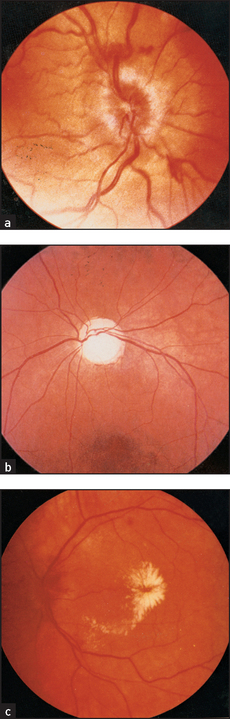
Figure 32.10 Fundoscopy in the neurological patient (a) Papilloedema; (b) optic atrophy; (c) grade 4 hypertensive retinopathy, with papilloedema, a ‘macular star’ of hard exudates collecting around the fovea, and retinal oedema. (Courtesy of Lions Eye Institute)
Next note the colour of the optic disc. Normally, it is a rich yellow colour in contrast to the rest of the fundus, which is a rich red colour. The fundus may be pigmented in some diseases and in patients with pigmented skin. When the optic disc has a pale insipid white colour, optic atrophy is usually present (see Figure 32.10(b)).
Each of the four quadrants of the retina should be examined systematically for abnormalities. Look especially for diabetic and hypertensive changes (see Figure 32.10(c)). Note haemorrhages or exudates.
THE THIRD (OCULOMOTOR), FOURTH (TROCHLEAR) AND SIXTH (ABDUCENS) NERVES—THE OCULAR NERVES
Examination anatomy
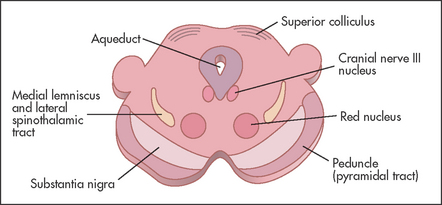
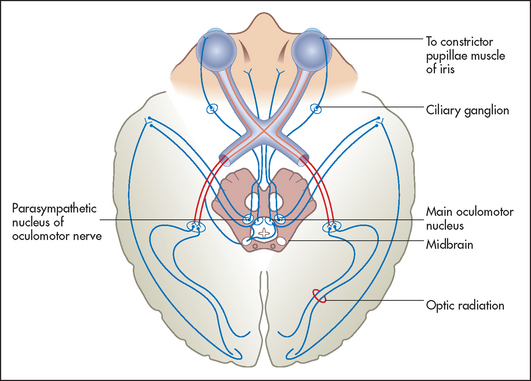
The size of the pupils depends on a balance of parasympathetic and sympathetic innervation. The parasympathetic innervation to the eyes is supplied by the Edinger-Westphalj nucleus of the third nerve (stimulation of these fibres causes pupillary constriction: miosis). The sympathetic innervation to the eye (stimulation causes pupillary dilation: mydriasis) is as follows: fibres from the hypothalamus go to the ciliospinal centre in the spinal cord at C8, T1 and T2, where they synapse, and from there second-order neurones exit via the anterior ramus in the thoracic trunk and synapse in the superior cervical ganglion in the neck; and third-order neurones travel from here with the internal carotid artery to the eye. In addition, the pupillary reflexes (see Figure 32.11) depend for their afferent limb on the optic nerve (see Figure 32.5). Constriction of the pupil in response to light is relayed by the optic nerve and tract to the superior colliculus and then to the Edinger-Westphal nucleus of the third nerve in the midbrain. Efferent motor fibres from the oculomotor nucleus (see Figure 32.12) travel in the wall of the cavernous sinus, where they are in association with the fourth, the ophthalmic division of the fifth and the sixth cranial nerves (see Figure 32.20 on page 415). These nerves leave the skull together through the superior orbital fissure. The iridoconstrictor fibres terminate in the ciliary ganglion, whence postganglionic fibres arise to innervate the iris. The rest of the third nerve supplies all the ocular muscles except the superior oblique (fourth nerve) and the lateral rectus (sixth nerve) muscles. The third nerve also supplies the levator palpebrae superioris, which elevates the eyelid (see Figure 32.13(a)).
Examination
Assess the pupils and movements of the eye.
The pupils
With the patient looking at an object at an intermediate distance, examine the pupils for size, shape, equality and regularity. Slight differences in pupil size (up to 20%) may be normal.k
Look for ptosis (drooping) of one or both eyelids. Remember that ectropion or drooping of the lower lid is a common degenerative problem in old age but can also be caused by a seventh nerve palsy or facial scarring. There is often eye irritation and watering associated with it because of defective tear drainage.
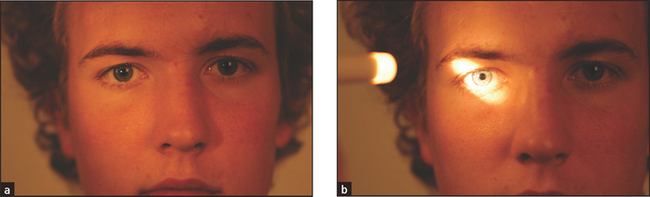
Test the light reflex. Using a pocket torch, shine the light from the side (so the patient does not focus on the light and accommodate) into one of the pupils to assess its reaction to light. Inspect both pupils and repeat this procedure on the other side. Normally, the pupil into which the light is shone constricts briskly—this is the direct response to light. Simultaneously, the other pupil constricts in the same way. This is called the consensual response to light.
Move the torch in an arc from pupil to pupil. If an eye has optic atrophy or severely reduced visual acuity from another cause, the affected pupil will dilate paradoxically after a short time when the torch is moved from the normal eye to the abnormal eye. This is called an afferent pupillary defect (or the Marcus Gunnl pupillary sign). It occurs because an eye with severely reduced acuity has reduced afferent impulses so that the light reflex is markedly decreased. When the light is shone from the normal eye to the abnormal one the pupil dilates, as reflex pupillary constriction in the abnormal eye is so reduced that relaxation after the consensual response dominates.
Now test accommodation. Ask the patient to look into the distance and then to focus his or her eyes on an object such as a finger or a white-tipped hat pin brought to a point about 30 centimetres in front of the nose. There is normally constriction of both pupils—the accommodation response. It depends on a pathway from the visual association cortex descending to the third nerve nucleus. Causes of an absent light reflex with an intact accommodation reflex include a midbrain lesion (e.g. the Argyll Robertson pupil of syphilis), a ciliary ganglion lesion (e.g. Adie’sm pupil) or Parinaud’sn syndrome (page 414). Failure of accommodation alone may occur occasionally with a midbrain lesion or with cortical blindness.
Eye movements
Here failure of eye movement, double vision (diplopia) and nystagmus are assessed.
Normally the eyes move in parallel except during convergence. When they move out of alignment the patient is said to have strabismus or a squint. This abnormality may be due to a cranial nerve palsy (III, IV or VI), and in these cases the angle of alignment changes depending on the direction of gaze (an incomitant squint). When the malalignment of the eye movement remains constant for any direction of gaze the squint is said to be concomitant. Concomitant squints are common in children and may be idiopathic or occasionally caused by an intracranial mass. Strabismus is associated with diplopia unless one of the images has been suppressed by the brain. This can happen quite quickly in children and may lead to severe visual loss in that eye—amblyopia.
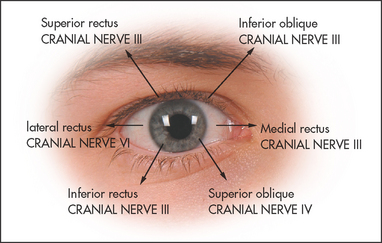
Ask the patient to look at the invaluable hat pin.o Assess voluntary eye movements in both eyes first. Ask the patient to look laterally right and left, then up and down (see Figure 32.14). Remember that the lateral rectus (sixth nerve) only moves the eyes horizontally outwards, while the medial rectus (third nerve) only moves the eyes horizontally inwards. The remainder of the muscle movements are a little more complicated. When the eye is abducted, the elevator is the superior rectus (third nerve), while the depressor is the inferior rectus (third nerve). When the eye is adducted, the elevator is the inferior oblique (third nerve) while the depressor is the superior oblique (fourth nerve; see Figure 32.13). The practical upshot of all this is that the testing of pure movement (i.e. one muscle only) for elevation and depression is performed first with the eye adducted and then with it abducted. Therefore, ask the patient to follow the moving hat pin, held 30–40 centimetres from the patient and moved in an H pattern, with both eyes and to say if double images are seen in any direction.
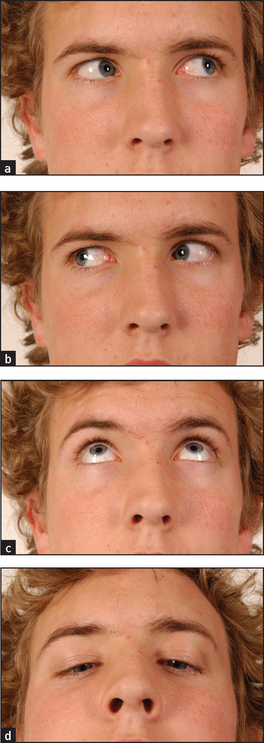
Figure 32.14 Cranial nerves III, IV and VI: voluntary eye movements (a) ‘Look to the left.’ (b) ‘Look to the right.’ (c) ‘Look up.’ (d) ‘Look down.’ (Courtesy of Glenn McCulloch)
The problem with testing in this way is that it is quite difficult for anyone to look up when the eyes are abducted or adducted and most people develop some diplopia when they try.p It is probably better to test vertical gaze with the patient staring straight ahead. The third nerve is still responsible for upward gaze. Horizontal movements will be abnormal for abduction on that side if there is a sixth nerve palsy and for adduction if there is a third nerve palsy. Moving the pin in a cross pattern will enable this testing. Move the pin so that the patient looks down and to the right and then down and to the left. A fourth nerve palsy will lead to failure of movement and to diplopia on the side where the patient looks down and in.
Diplopia can be an early sign of ocular muscle weakness because the light falls on different parts of the corresponding retina due to slight movement differences. If diplopia is present, further testing is necessary. The false image is usually paler, less distinct and always more peripheral than the real one. Ask the patient whether the two images lie side by side or one above the other. If they are side by side, only the lateral or medial recti can be responsible. If they lie one above the other, then either of the obliques or the superior or inferior recti may be involved. To decide which pair of muscles is responsible, ask in which direction there is maximum image separation. Separation is greatest in the direction in which the weak muscle has its purest action. At the point of maximum separation, cover one eye and find out which image disappears. Loss of the lateral image indicates that the covered eye is responsible. Diplopia that persists when one eye is covered (monocular diplopia) can be due to astigmatism, myopia, a dislocated lens, cataract or hysteria.
Note failure of movement of either eye in any direction. This indicates ocular muscle involvement. If any abnormality is detected, then each eye must be tested separately. Cover the other eye with a card or your hand. Abnormal eye movement may be due to III, IV or VI nerve palsy, or to an abnormality of conjugate gaze.
Features of a third nerve lesion
These are complete ptosis (partial ptosis may occur with an incomplete lesion), divergent strabismus (eye ‘down and out’) and a dilated pupil that is unreactive to direct light (the consensual reaction in the opposite normal eye is intact) and unreactive to accommodation (see Figure 32.15). Always try to exclude a fourth (trochlear) nerve lesion when a third nerve lesion is present. One way to do this is by tilting the patient’s head to the same side as the lesion. The affected eye will intort if the fourth nerve is intact. (Remember SIN—the Superior oblique INtorts the eye.)
Aetiology of a third nerve palsy
Third nerve lesions are most commonly related to trauma or are idiopathic. Central causes include vascular lesions in the brainstem, tumours and, rarely, demyelination. Peripheral causes include: (1) compressive lesions, such as an aneurysm (usually on the posterior communicating artery), tumour, basal meningitis, nasopharyngeal carcinoma or orbital lesions—for example, Tolosa-Hunt syndrome (superior orbital fissure syndrome—painful lesions of III, IV, VI and the first division of V); and (2) ischaemia or infarction, as in arteritis, diabetes mellitus and migraine.
Features of a fourth nerve lesion
Test this nerve by asking the patient to turn the eye in and then try to look down: a lesion results in paralysis of the superior oblique with weakness of downward (and outward) movement. The patient may walk around with his or her head tilted away from the lesion—that is, to the opposite shoulder (this allows the patient to maintain binocular vision).
An isolated fourth nerve palsy is rare and is usually idiopathic or related to trauma. It may occasionally occur with lesions of the cerebral peduncle.
Features of a sixth nerve lesion
These are failure of lateral movement, convergent strabismus and diplopia. These signs are maximal on looking to the affected side, and the images are horizontal and parallel to each other. The outermost image from the affected eye disappears on covering this eye (this image is usually also more blurred).
Aetiology of a sixth nerve palsy
Bilateral lesions may be due to trauma or Wernicke’s encephalopathy (a syndrome of ophthalmoplegia, confusion and ataxia, which is often associated with Korsakoff’s psychosis due to thiamine deficiency). Mononeuritis multiplex and raised intracranial pressure are also causes of sixth nerve palsy.
Unilateral sixth nerve lesions are most commonly idiopathic or related to trauma. They may have a central (e.g. vascular lesion or tumour) or peripheral (e.g. raised intracranial pressure or diabetes mellitus) origin.
Abnormalities of conjugate gaze
Normal eye movements occur in an organised fashion so that the visual axes remain in the same plane throughout. There are centres for conjugate gaze in the frontal lobe for saccadic movements and in the occipital lobe for pursuit movements. Conjugate movement to the right is controlled from the left side of the brain. From these centres fibres travel to the region of the sixth nerve nucleus, from which area the medial longitudinal fasciculus coordinates movement with the contralateral third nerve (medial rectus) nucleus (see Figure 32.16). A brainstem lesion causes ipsilateral paralysis of horizontal conjugate gaze, and a frontal lobe lesion causes contralateral paralysis of horizontal conjugate gaze.
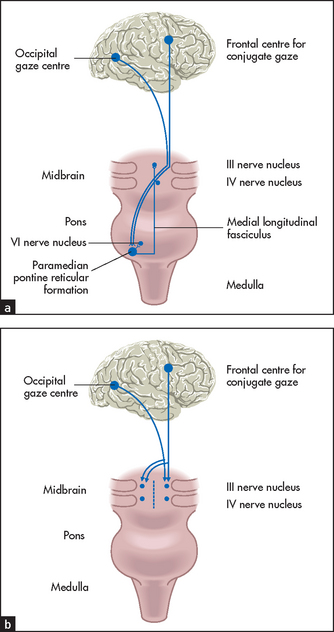
Figure 32.16 Horizontal (a) and vertical (b) eye movements (Adapted from Lance JW, McLeod JG. A physiological approach to clinical neurology, 3rd edn. London: Butterworths, 1981.) Butterworths
There are a number of possible causes for deviation of the eyes to one side. For example, deviation of the eyes to the left can result from: (1) a destructive lesion (usually vascular or neoplastic), which involves the pathways between the left frontal lobes and the oculomotor nuclei; (2) a destructive lesion of the right side of the brainstem; or (3) an irritative lesion, such as an epileptic focus, of the right frontal lobe, which stimulates deviation of the eyes to the left.
Supranuclear palsy is loss of vertical or horizontal gaze, or both (see Figure 32.17). The clinical features that distinguish this from third, fourth and sixth nerve palsies include: (1) both eyes are affected; (2) pupils may be fixed and are often unequal; (3) there is usually no diplopia; and (4) the reflex eye movements—for example, on flexing and extending the neck—are usually intact.
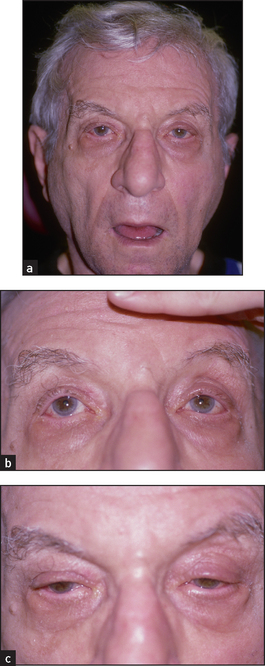
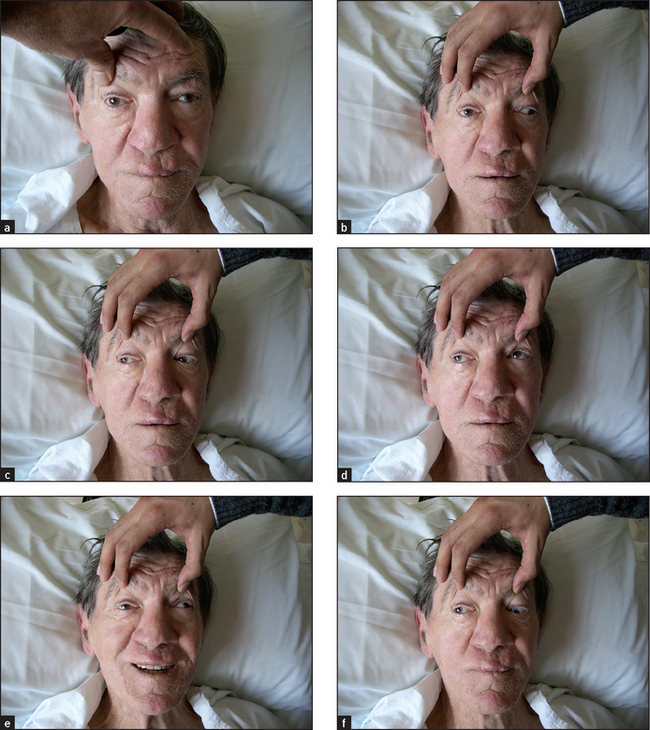
Figure 32.17 Supranuclear palsy (a) Characteristic stare; (b) upward gaze (limited); (c) downward gaze (limited). (Liu GT. Neuro-ophthalmology: diagnosis and management. Elsevier, 2010.)
In progressive supranuclear palsy (or Steele Richardson Olszewski syndromeq) there is loss of vertical and later of horizontal gaze, which is associated with extrapyramidal signs, neck rigidity and dementia. Reflex eye movements on neck flexion and extension are preserved until late in the course of the disease.
Parinaud’s syndrome is loss of vertical gaze often associated with nystagmus on attempted convergence (see below). There are pseudo-Argyll Robertson pupils. The causes of Parinaud’s syndrome include a pinealoma, multiple sclerosis and vascular lesions.
Involuntary upward deviation of the eyes (oculogyric crisis) occurs with post-encephalitic Parkinson’s disease and may be seen in patients sensitive to phenothiazine derivatives or in patients on levodopa therapy.
One-and-a-half syndrome is rare but important to recognise. These patients have a horizontal gaze palsy when looking to one side (the ‘one’) plus impaired adduction on looking to the other side (the ‘and-a-half’). Other features often include turning out (exotropia) of the eye opposite the side of the lesion (paralytic pontine exotropia). One-and-a-half syndrome can be caused by a stroke (infarct), plaque of multiple sclerosis or tumour in the dorsal pons.
Nystagmus
The eyes are normally maintained at rest in the midline by the balance of tone between opposing ocular muscles. Disturbance of this tone, which depends on impulses from the retina, the muscles of the eyes themselves and various vestibular and central connections, allows the eyes to drift in one direction. This drift is corrected by a quick movement (saccadic) back to the original position. When these movements occur repeatedly, nystagmus is said to be present. The direction of the nystagmus is defined as that of the fast (correcting) movement, although it is the slow drift that is abnormal. Nystagmus from any cause tends to be accentuated by gaze in a direction away from the midline. In many instances nystagmus is not present when the eyes are at rest and is detected only when the eyes are deviated (gaze-evoked nystagmus). At the extremes of gaze, fine nystagmus is normal (physiological). Therefore, test for nystagmus by asking the patient to follow your pin out to 30° from the central gaze position.
Nystagmus may be jerky or pendular:
• Jerky horizontal nystagmus may be due to: (1) a vestibular lesion (acute lesions cause nystagmus away from the side of the lesion, while chronic lesions cause nystagmus to the side of the lesion); (2) a cerebellar lesion (unilateral diseases cause nystagmus to the side of the lesion); (3) toxic causes, such as phenytoin and alcohol (may also cause vertical nystagmus but less often); and (4) internuclear ophthalmoplegia. Internuclear ophthalmoplegia (see Figure 32.18) is present when there is nystagmus in the abducting eye and failure of adduction of the other (affected) side. This is due to a lesion of the medial longitudinal fasciculus. The most common cause in young adults with bilateral involvement is multiple sclerosis; in the elderly, vascular disease is an important cause.
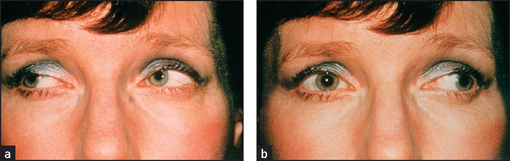
Figure 32.18 Internuclear ophthalmoplegia: (a) ‘Look right’ (normal); (b) ‘Look left’ (nystagmus left eye, failure of adduction right eye [affected side]) (McAlpine’s multiple sclerosis, 4th edn. 2006.)
• Jerky vertical nystagmus may be due to a brainstem lesion. Vertical nystagmus means nystagmus where the oscillations are in a vertical direction. Upbeat nystagmus suggests a lesion in the midbrain or floor of the fourth ventricle, while downbeat nystagmus suggests a foramen magnum lesion. Phenytoin or alcohol can also cause this abnormality.
• Pendular nystagmus is present when the nystagmus phases are equal in duration. Its cause may be retinal (decreased macular vision, e.g. albinism) or congenital. This condition is thought to occur as a result of poor vision or increased sensitivity to light. It develops in childhood and occurs as the patient performs searching movements in an attempt to fixate or improve the visual impulses.
A summary of how to approach the medical eye examination is provided in Chapter 38.
THE FIFTH (TRIGEMINAL) NERVE
Examination anatomy
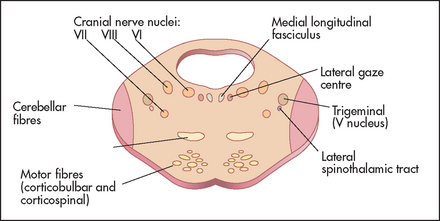
This nerve contains both sensory and motor fibres. Its motor nucleus and its sensory nucleus for touch lie in the pons (see Figure 32.19), its proprioceptive nucleus lies in the midbrain, while its nucleus serving pain and temperature sensation descends through the medulla to reach the upper cervical cord. It is the largest of the cranial nerves.
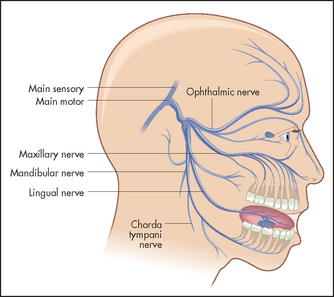
The nerve itself leaves the pons from the cerebellopontine angle and runs over the temporal lobe in the middle cranial fossa. At the petrous temporal bone the nerve forms the trigeminal (Gasserianr) ganglion and from here the three sensory divisions arise. The first (ophthalmic) division runs in the cavernous sinus with the third nerve and emerges from the superior orbital fissure to supply the skin of the forehead, the cornea and the conjunctiva. The second (maxillary) division emerges from the infraorbital foramen and supplies the skin in the middle of the face and the mucous membranes of the upper part of the mouth, the palate and the nasopharynx. The third and largest (mandibular) division runs with the motor part of the nerve, leaving the skull through the foramen ovale to supply the skin of the lower jaw and the mucous membranes of the lower part of the mouth (see Figures 32.20 and 32.21).
Pain and temperature fibres from the face run from the pons through the medulla as low as the upper cervical cord, terminating in the spinal tract nucleus as they descend. The second-order neurones arise in this nucleus and ascend again as the ventral trigeminothalamic tract. Touch and proprioceptive fibres terminate in the pontine or main sensory and mesencephalic nuclei, respectively, to form the dorsal and the ventral mesencephalic tracts. Because of this segregation in the brainstem, lesions of the medulla or upper spinal cord can cause a dissociated sensory loss of the face—loss of pain and temperature sensation, but retention of touch and proprioception.
The motor part of the nerve supplies the muscles of mastication.
History
Pain in the distribution of part of the trigeminal nerve is common. Tic douloureux (trigeminal neuralgia) is a sudden severe shooting pain in one of the divisions of the nerve. It is more common in elderly people. The occurrence in a young woman suggests multiple sclerosis. The pain is brief but very distressing. It may be precipitated by an activity such as eating or brushing the teeth. The pain is caused by a pontine lesion or by compression of the trigeminal nerve by a vascular abnormality. Pain due to sinusitis, dental abscess, malignant disease of the sinuses and herpes zoster may be felt in a trigeminal nerve distribution. Muscle weakness of the trigeminal nerve may lead the patient to complain of difficulty eating or talking.
Examination
Test the corneal reflex. Lightly touch the cornea (not the conjunctiva) with a wisp of cottonwool brought to the eye from the side. Reflex blinking of both eyes is a normal response. Ask the patient whether he or she feels the touch of the cottonwool. The sensory component of the reflex is mediated by the ophthalmic division of the fifth nerve, while the reflex blink (motor) results from facial nerve innervation of the orbicularis oculi muscles. Absence of corneal sensation is associated with corneal ulceration.
Note: If blinking occurs only with the contralateral eye this indicates an ipsilateral seventh nerve palsy. The patient will then still feel the touch of the cottonwool on the cornea.
Test facial sensation in the three divisions of the nerve, comparing each side with the other (see Figure 32.22(a)). Test first with the sharp end of a new disposable neurological pin for pain sensation (never use an old pin in these days of hepatitis B, HIV etc).6 Apply the pin lightly to the skin and ask the patient whether it feels sharp or dull. Some examiners ask patients to shut their eyes. Loss of pain sensation will result in the pinprick feeling dull. An area of dull sensation should be mapped by testing pinprick sensation progressively: testing should go from the dull to the sharp area. Test also above the forehead progressively back over the top of the head. If the ophthalmic division is affected, sensation will return when the C2 dermatome is reached (see Figure 32.21).
It is important to exercise caution: too much pressure may leave a little trail of bloody spots, which is embarrassing. Temperature is not tested routinely unless syringobulbia is suspected, as temperature loss usually accompanies loss of pain sensation.
With the patient’s eyes closed, use a new piece of cottonwool to test light touch in the same way. Instruct the patient to say ‘yes’ each time the touch of the cottonwool is felt (do not stroke the skin). Proprioception loss is not routinely tested on the face (and indeed it would be rather a difficult thing to do).
Now examine the motor division of the nerve. Begin by inspecting for wasting of the temporal and masseter muscles. Ask the patient to clench the teeth, then palpate for contraction of the masseter above the mandible (see Figure 32.23). The strength of these muscles can be tested by asking the patient to bite forcefully onto a wooden tongue depressor with the molar teeth. The depth of the teeth marks on each side gives an indication of the relative strength of the muscles. You can attempt to withdraw the tongue depressor as the patient bites it. A bite of normal strength will prevent this. Then get the patient to hold open the mouth (pterygoid muscles) while you attempt to force it shut. A unilateral lesion of the motor division causes the jaw to deviate towards the weak (affected) side.

Figure 32.23 Cranial nerve V (motor): ‘Clench your jaw’—feel the masseter muscles (Courtesy of Glenn McCulloch)
A clinically obvious upper motor neurone lesion of the twelfth nerve is usually bilateral and results in a small immobile tongue. The combination of bilateral upper motor neurone lesions of the ninth, tenth and twelfth nerves is called pseudobulbar palsy.s
Causes of a fifth nerve palsy
Central (pons, medulla and upper cervical cord) causes include a vascular lesion, tumour or syringobulbia. Peripheral (middle fossa) causes include an aneurysm, tumour (secondary or primary) or chronic meningitis. Trigeminal ganglion (petrous temporal bone) causes include a trigeminal neuroma, meningioma or fracture of the middle fossa. Cavernous sinus causes involve the ophthalmic division only and are usually associated with third, fourth and sixth nerve palsies. They include aneurysm, tumour or thrombosis.
Remember, if there is total loss of sensation in all three divisions of the nerve, this suggests that the level of the lesion is at the ganglion or the sensory root—for example, an acoustic neuroma (see Figure 32.25). If there is total sensory loss in one division only, this suggests a postganglionic lesion. The ophthalmic division is most commonly affected because it runs in the cavernous sinus and through the orbital fissure, where it is vulnerable to a number of different insults.
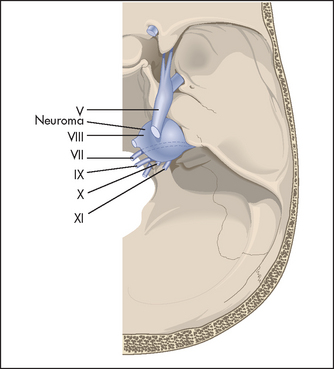
Figure 32.25 Cerebellopontine angle tumour A neuroma arising from the acoustic (VIII) nerve compresses adjacent structures, including the trigeminal (V) and facial (VII) nerves, the brainstem and the cerebellum (removed to permit the cranial nerves to be seen). (Adapted from Simon RP, Aminoff MJ, Greenberg DA, Clinical neurology. Appleton & Lange, 1989.)

If there is dissociated sensory loss (loss of pain, but preservation of touch sensation), this suggests a brainstem or upper cord lesion, such as syringobulbia, foramen magnum tumour or infarction in the territory of the posterior inferior cerebellar artery. If touch sensation is lost but pain sensation is preserved, this is usually due to an abnormality of the pontine nuclei, such as a vascular lesion or tumour. Motor loss can also be central or peripheral.
Irritative motor changes
Convulsive seizures that involve the precentral gyrus can include clenching of the jaw and biting of the tongue. Parkinson’s disease and essential tremor can cause a rhythmic tremor of the lips or jaw. Trismus is a forceful clenching of the jaw that can occur in tetanus and encephalitis. The patient may be unable to open the mouth. Repetitive chewing and yawning movements can occur as an effect of antipsychotic drugs (tardive orofacial dyskinesias).
THE SEVENTH (FACIAL) NERVE
Examination anatomy
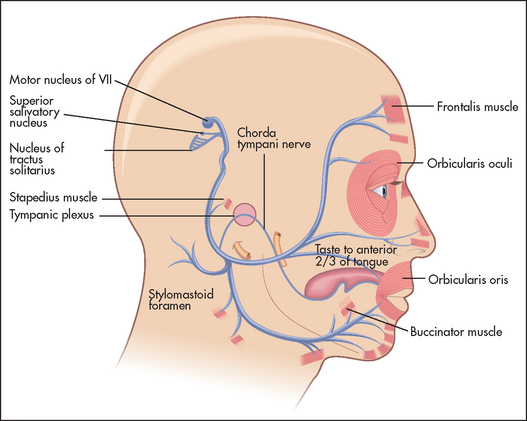
The seventh nerve nucleus lies in the pons next to the sixth cranial nerve nucleus (see Figure 32.2). The nerve (see Figure 32.26) leaves the pons with the eighth nerve through the cerebellopontine angle. After entering the facial canal it enlarges to become the geniculate ganglion. The branch that supplies the stapedius muscle is given off from within the facial canal. The chorda tympani (containing taste fibres from the anterior two-thirds of the tongue) joins the nerve in the facial canal. The seventh nerve leaves the skull via the stylomastoid foramen. It then passes through the middle of the parotid gland and supplies the muscles of facial expression. The frontalis muscle receives upper motor innervation bilaterally; the other muscles receive innervation from the contralateral cortex.
History
The patient may have noticed the onset of difficulty with speaking and keeping liquids in the mouth or may have noticed facial asymmetry in the mirror. He or she may be aware of dryness of the eyes (decreased lacrimation) or the mouth (decreased salivary production). Paralysis of the stapedius muscle can cause hyperacusis or intolerance of loud or high-pitched sounds. Normal contraction of the stapedius muscle occurs in response to loud rebarbative noises such as popular music and dampens movement of the ossicles.
Examination
Inspect for facial asymmetry, as a seventh nerve palsy can cause unilateral drooping of the corner of the mouth, and smoothing of the wrinkled forehead and the nasolabial fold (see Figure 32.27). However, symmetry may be maintained when facial nerve palsies are bilateral.

Figure 32.27 Left upper motor neurone facial weakness, showing drooping of the corner of the mouth, flattened nasolabial fold and sparing of the forehead; the lesion is in the right side of the brain
Test the muscle power. Ask the patient to look up so as to wrinkle the forehead (see Figure 32.28). Look for loss of wrinkling and feel the muscle strength by pushing down against the corrugation on each side. This movement is relatively preserved on the side of an upper motor neurone lesion (a lesion that occurs above the level of the brainstem nucleus) because of bilateral cortical representation of these muscles. The remaining muscles of facial expression are usually affected on the side of an upper motor neurone lesion, although occasionally the orbicularis oculi muscles are preserved. Ask the patient to puff out the cheeks (see Figure 32.29). Look for asymmetry.

Figure 32.28 Cranial nerve VII: ‘Look up to wrinkle your forehead’ (normal) (Courtesy of Glenn McCulloch)

In a lower motor neurone lesion (at the level of the nucleus or nerve root), all muscles of facial expression are affected on the side of the lesion.
Next, ask the patient to shut the eyes tightly (see Figure 32.30). Compare how deeply the eyelashes are buried on the two sides and then try to force open each eye. Check whether Bell’st phenomenon is evident. Bell’s phenomenon is present in everyone, although not usually visible unless a person has a VII nerve palsy. In this case, when the patient attempts to shut the eye on the side of a lower motor neurone VII nerve palsy, there is upward movement of the eyeball and incomplete closure of the eyelid. Next ask the patient to grin (see Figure 32.31) and compare the nasolabial grooves, which are smooth on the weak side.
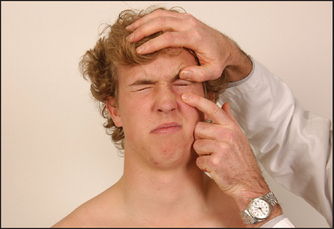
Figure 32.30 Cranial nerve VII: ‘Shut your eyes tight and stop me opening them’ (normal) (Courtesy of Glenn McCulloch)

Figure 32.31 Cranial nerve VII: ‘Show me your teeth’ (normal) (Before asking this question, make sure the patient’s teeth are not in a container beside the bed.) (Courtesy of Glenn McCulloch)
If a lower motor neurone lesion is detected, check quickly for the ear and palatal vesicles of herpes zoster of the geniculate ganglion—the Ramsay Huntu syndrome.
A facial paralysis due to a cortical lesion may spare facial movements due to emotion such as crying or smiling, and indeed these movements may be exaggerated. The opposite abnormality (preservation of voluntary but loss of emotional movements) can also occur as a result of lesions in a number of areas, including the frontal lobes.
Examining for taste on the anterior two-thirds of the tongue is not usually required. If necessary, it can be tested by asking the patient to protrude the tongue to one side: sugar, vinegar, salt and quinine (sweet, sour, saline and bitter) are placed one at a time on each side of the tongue. The patient indicates the taste by pointing to a card with the various tastes listed on it. The mouth is rinsed with water between each sample.
Causes of a seventh (facial) nerve palsy
Vascular lesions or tumours are the common causes of upper motor neurone lesions (supranuclear). Note that lesions of the frontal lobes may cause weakness of the emotional movements of the face alone; voluntary movements are preserved.
In lower motor neurone lesions pontine causes (often associated with V and VI lesions) include vascular lesions, tumours, syringobulbia and multiple sclerosis. Posterior fossa lesions include an acoustic neuroma, a meningioma or chronic meningitis. At the level of the petrous temporal bone (Bell’s palsy [an idiopathic acute paralysis of the nerve; see Figure 32.32]), a fracture, the Ramsay Hunt syndrome or otitis media may occur, while the parotid gland may be affected by a tumour or sarcoidosis. Remember, Bell’s palsy is the most common cause (up to 80%) of a facial nerve palsy.v

Figure 32.32 Bell’s palsy on the right side (From Mayo Clinic Images, with permission. © Mayo Clinic Scientific Press and CRC Press.)
Regrowth of the nerve fibres that occurs as the patient recovers from Bell’s palsy can lead to aberrant connections. The most striking is the regrowth of fibres meant for the salivary gland to the lacrimal gland in up to 5% of patients. This leads to tear formation when a patient eats: crocodile tears.
Bilateral facial weakness may be due to the Guillain-Barré syndrome, sarcoidosis, bilateral parotid disease, Lyme disease or, rarely, mononeuritis multiplex. Myopathy and myasthenia gravis can also cause bilateral facial weakness, but in these cases it is not due to facial nerve involvement.
Unilateral loss of taste, without other abnormalities, can occur with middle-ear lesions involving the chorda tympani or lingual nerve, but these are very rare.
Irritative changes
Tonic and clonic movements of the facial muscles can occur in seizures. Various abnormal movements of the facial muscles can occur as a result of basal ganglia or extrapyramidal abnormalities. These include athetoid and dystonic movements. Irritative lesions in the brainstem can cause increased secretion of saliva (sialorrhoea). This can also occur in Parkinson’s disease or accompany attacks of nausea.
THE EIGHTH (ACOUSTIC) NERVE
Examination anatomy
The eighth (acoustic) nerve has two components: the cochlear, with afferent fibres subserving hearing; and the vestibular, containing afferent fibres subserving balance. Fibres for hearing originate in the organ of Cortiw and run to the cochlear nuclei in the pons. From here there is bilateral transmission to the medial geniculate bodies and thence to the superior gyrus of the temporal lobes. Fibres for balance begin in the utricle and semicircular canals, and join auditory fibres in the facial canal. They then enter the brainstem at the cerebellopontine angle. After entering the pons, vestibular fibres run widely throughout the brainstem and the cerebellum.
History
Loss of hearing may have been noticed by the patient or complained of by his or her relatives or friends. Unilateral hearing loss is much more likely to be due to a nerve lesion and must be identified. Also find out if this has been of gradual or sudden onset, whether there is a family history of deafness and whether the patient has had occupational or recreational exposure to loud noise (e.g. boilermaker, retired rock musician) without hearing protection. There may be a history of trauma or recurrent ear infections.
Examination of the ear and hearing
Look to see if the patient is wearing a hearing aid; if so, remove it. Examine the pinna and look for scars behind the ears. Pull on the pinna gently (it is tender if the patient has external ear disease or temporomandibular joint disease). Feel for nodes (pre- and post-auricular) that may indicate disease of the external auditory meatus.
Inspect the patient’s external auditory meatus. The adult canal angulates, so in order to see the eardrum it is necessary to pull up and backwards on the auricle before inserting the otoscope. The normal eardrum (tympanic membrane) is pearly grey and concave. Look for wax or other obstructions, and inspect the eardrum for inflammation or perforation (see Chapter 38).
Next, test hearing. A simple test involves covering the opposite auditory meatus with a finger, and moving it about as a distraction while whispering a number in the other ear. This should be standardised by the use of set numbers for different tones. For example, the number 68 is used to test high tone and 100 is used to test low tone. Whispering should be performed towards the end of expiration in an attempt to standardise the volume and at about 60 centimetres from the patient’s ear. Your larynx should not vibrate if the whispering is soft enough. If partial deafness is suspected, perform Rinné’s and Weber’s tests:
• Rinné’sx test—a 512 or 256 Hz vibrating tuning fork is placed on the mastoid process, behind the ear, and when the sound is no longer heard it is placed in line with the external meatus (see Figure 32.33). Normally the note is audible at the external meatus. If the patient has nerve deafness, the note is audible at the external meatus, as air and bone conduction are reduced equally, so that air conduction is better (as is normal). This is termed Rinné-positive. If there is a conduction (middle ear) deafness, no note is audible at the external meatus. This is termed Rinné-negative.
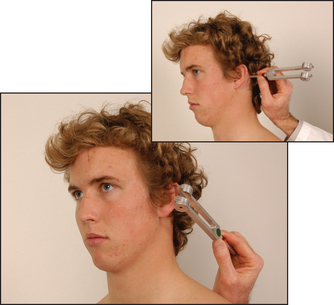
Figure 32.33 Cranial nerve VIII, Rinné’s test: ‘Where does it sound louder?’ (Courtesy of Glenn McCulloch)
• Weber’sy test—a vibrating 256 or 512 Hz tuning fork is positioned on the centre of the forehead (see Figure 32.34). Normally the sound is heard in the centre of the forehead. Nerve deafness causes the sound to be heard better in the normal ear. A patient with a conduction deafness finds the sound louder in the abnormal ear.

Causes of deafness
Unilateral nerve deafness may be due to: (1) tumours, such as an acoustic neuroma; (2) trauma, such as fracture of the petrous temporal bone; or (3) vascular disease of the internal auditory artery (rare). Bilateral nerve deafness may be due to: (1) environmental exposure to noise; (2) degeneration, such as presbyacusis; (3) toxicity, such as aspirin, gentamicin or alcohol; (4) infection, such as congenital rubella syndrome, congenital syphilis; or (vi) Ménière’s disease. Brainstem disease is a rare cause of bilateral deafness. Conduction deafness may be due to: (1) wax; (2) otitis media; (3) otosclerosis; or (4) Paget’s disease of bone.
Examination of vestibular function
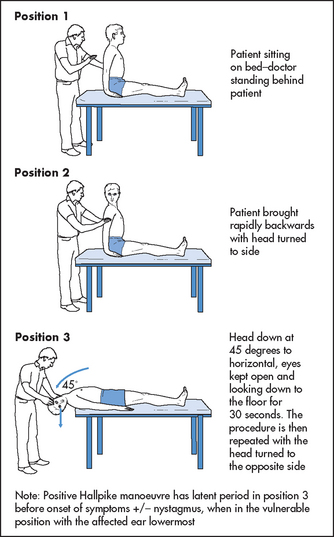
If the patient complains of vertigo, the Hallpikez manoeuvre should be performed (see Figure 32.35). Have the patient sit up and warn him or her what is about to occur, then grasp the patient’s head between your hands and get him or her to lie back quickly so that the head lies 45° below the horizontal with the patient’s head turned to one side. Ask the patient to keep the eyes open. If the test is positive, after a short latent period vertigo and nystagmus (rotatory) towards the affected (lowermost) ear occur for several seconds and then abate and are not reproducible for 10–15 minutes. This result is seen in the condition called benign paroxysmal positioning vertigo (BPPV). It occurs with repositioning of the head and then abates so that the old name, benign positional vertigo, is not really appropriate. It is due to a disorder in the utricle and occurs, for example, following infection, trauma or vascular disease. It is caused by the presence of concretions in the semicircular canals. Inertia of these concretions following movement of the head causes the illusion of movement and nystagmus. If there is no latent period, no fatiguability or the nystagmus persists or is variable, this suggests that there is a lesion of the brainstem (e.g. multiple sclerosis) or the cerebellum (e.g. metastatic carcinoma).
Causes of vestibular abnormalities
Labyrinthine causes include acute labyrinthitis, motion sickness, streptomycin toxicity or, rarely, Ménière’s disease. Vestibular causes include vestibular neuronitis as well as many of the causes of nerve deafness.
In the brainstem, vascular lesions, tumours of the cerebellum or fourth ventricle, demyelination or vasospastic conditions such as migraine may involve the central connections of the vestibular system.
Vertigo may be associated with temporal lobe dysfunction (e.g. ischaemia or complex partial seizures).
THE NINTH (GLOSSOPHARYNGEAL) AND TENTH (VAGUS) NERVES
Examination anatomy
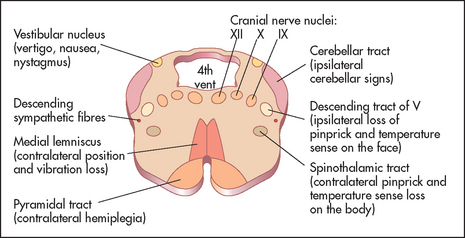
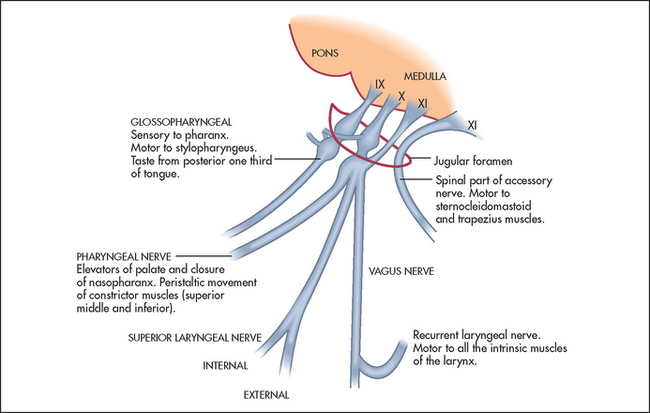
These nerves have motor, sensory and autonomic functions. Nerve fibres from nuclei in the medulla (see Figure 32.36) form multiple nerve rootlets as they exit the medulla. These join to form the ninth and tenth nerves, and also contribute to the eleventh nerve. The nerves emerge from the skull through the jugular foramen (see Figure 32.37). The ninth nerve receives sensory fibres from the nasopharynx, the pharynx, the middle and inner ear and from the posterior third of the tongue (including taste fibres). It also carries secretory fibres to the parotid gland. The tenth nerve receives sensory fibres from the pharynx and the larynx, and innervates muscles of the pharynx, the larynx and the palate.
History
A lesion of the glossopharyngeal nerve may cause the patient no definite symptoms, but difficulty in swallowing dry foods may have been noticed. Glossopharyngeal neuralgia is a tic douloureux of the ninth nerve. The patient experiences sudden shooting pains that radiate from one side of the throat to the ear. There may be trigger areas in the throat and attacks can be brought on by chewing or swallowing.
Unilateral vagus nerve paralysis may cause difficulty in initiating the swallowing of solids and liquids, and hoarseness.
Examination
Ask the patient to open the mouth and inspect the palate with a torch. Note any displacement of the uvula. Then ask the patient to say ‘Ah!’ (see Figure 32.38). Normally, the posterior edge of the soft palate—the velumaa—rises symmetrically. If the uvula is drawn to one side this indicates a unilateral tenth nerve palsy. Note that the uvula is drawn towards the normal side.aa

Figure 32.38 Cranial nerve X: ‘Say “Ah”’—look for asymmetrical movement of the uvula (Courtesy of Glenn McCulloch)
Testing for the gag reflex (ninth is the sensory component and tenth the motor component) is traditional but not necessary.7 A better alternative is to touch the back of the pharynx on each side (rather than the soft palate) with a spatula. The patient is asked if the touch of the spatula (ninth) is felt each time. Normally, there is reflex contraction of the soft palate. If contraction is absent and sensation is intact, this suggests a tenth nerve palsy. The most common cause of a reduced gag reflex is old age. Of more concern is the patient with an exaggerated but still normal reflex: this can lead to vomiting onto the examining clinician.
Ask the patient to speak in order to assess hoarseness (which may occur with a unilateral recurrent laryngeal nerve lesion), and then to cough. Listen for the characteristic bovine cough that occurs with recurrent laryngeal nerve lesions. It is not necessary routinely to test taste on the posterior third of the tongue (ninth nerve).
Test the patient’s ability to swallow a small amount of water and watch for regurgitation into the nose, or coughing.
Causes of a ninth (glossopharyngeal) and tenth (vagus) nerve palsy
Central causes are vascular lesions (e.g. lateral medullary infarction, due to vertebral or posterior inferior cerebellar artery disease), tumours, syringobulbia and motor neurone disease. Peripheral (posterior fossa) lesions comprise aneurysms at the base of the skull, tumours, chronic meningitis or the Guillain-Barré syndrome.
THE ELEVENTH (ACCESSORY) NERVE
Examination anatomy
The central portion of this nerve arises in the medulla close to the nuclei of the ninth, tenth and twelfth nerves and its spinal portion arises from the upper five cervical segments. It leaves the skull with the ninth and tenth nerves through the jugular foramen (see Figure 32.37). Its central division provides motor fibres to the vagus and the spinal division innervates the trapezius and the sternocleidomastoid muscles. The motor fibres that supply the sternocleidomastoid muscle are thought to cross twice so that cortical control of the muscle is ipsilateral. This makes sense when one remembers that the muscle turns the head to the opposite side. This means that the hemisphere that receives information from and controls one side of the body also turns the head to face that side.
Examination
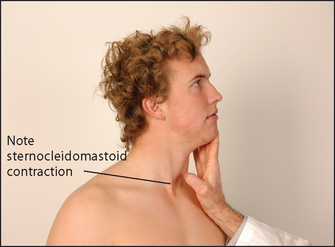
Ask the patient to shrug the shoulders (see Figure 32.39). Feel the bulk of the trapezius muscles and attempt to push the shoulders down. Then instruct the patient to turn the head to the side against resistance (your hand; see Figure 32.40). Remember that the right sternocleidomastoid turns the head to the left. Feel the muscle bulk of the sternocleidomastoids.

Figure 32.39 (a) Cranial nerve XI: ‘Shrug your shoulders—push up hard’ (b) Wasting of the left trapezius muscle ((a) Courtesy of Glenn McCulloch)
Weakness of these muscles is less common than torticollis, which is due to overactivity of multiple neck muscles. It is a complex movement disorder. The head appears turned to one side either permanently or in spasms. Ask the patient to turn the head to face forwards. This is usually possible at least briefly, but look to see whether he or she needs to use the hands to push the head straight.
Causes of eleventh nerve palsy
Unilateral causes are trauma involving the neck or the base of the skull, poliomyelitis, basilar invagination (platybasia), syringomyelia and tumours near the jugular foramen. Bilateral causes comprise motor neurone disease, poliomyelitis and the Guillain-Barré syndrome. Note: Bilateral sternocleidomastoid and trapezius weakness also occurs in muscular dystrophy (especially dystrophia myotonica).
THE TWELFTH (HYPOGLOSSAL) NERVE
Examination anatomy
This nerve also arises from the medulla. It leaves the skull via the hypoglossal foramen. It is the motor nerve for the tongue.
History
The patient with bilateral hypoglossal nerve paresis may have noticed difficulty in swallowing and a sensation of choking if the tongue slips back into the throat. There are no sensory changes caused by hypoglossal nerve abnormalities, and unilateral disease rarely causes symptoms.
Examination
Inspect the tongue at rest on the floor of the mouth. The normal tongue may move a little, especially when protruded, but is not wasted. Look for wasting and fasciculations (fine, irregular, non-rhythmical muscle fibre contractions). These signs indicate a lower motor neurone lesion. Fasciculations may be unilateral or bilateral (see Figure 32.41).
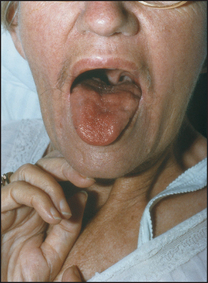
Ask the patient to stick out the tongue (see Figure 32.42), which may deviate towards the weaker (affected) side if there is a unilateral lower motor neurone lesion (see Figure 32.43). The tongue, like the face and the palate, has a bilateral upper motor neurone innervation in most people, so a unilateral upper motor neurone lesion often causes no deviation.


Figure 32.43 (a and b) Right hypoglossal (XII) nerve palsy, lower motor neurone lesion: ‘Stick out your tongue’
A clinically obvious upper motor neurone lesion of the twelfth nerve is usually bilateral and results in a small immobile tongue. The combination of bilateral upper motor neurone lesions of the ninth, tenth and twelfth nerves is called pseudobulbar palsy.
A lower motor neurone lesion of the twelfth nerve causes fasciculation, wasting and weakness. If the lesion is bilateral, it causes dysarthria.
Movement disorders may affect the tongue. In Parkinson’s disease there may be a coarse tremor of the tongue, made worse by speaking or protruding the tongue. Athetoid, choreiform and tardive dyskinesia can all involve the tongue.
Causes of twelfth nerve palsy
Bilateral upper motor neurone lesions may be due to vascular lesions, motor neurone disease or tumours, such as metastases to the base of the skull.bb
Unilateral lower motor neurone lesions with a central cause include vascular lesions, such as thrombosis of the vertebral artery, motor neurone disease and syringobulbia. Peripheral causes include: in the posterior fossa, aneurysms or tumours, chronic meningitis and trauma; in the upper neck, tumours or lymphadenopathy; and the Arnold-Chiaribb malformation. The Arnold-Chiari malformation is a congenital malformation of the base of the skull with herniation of a tongue of cerebellum and medulla into the spinal canal, causing lower cranial nerve palsies, cerebellar limb signs (due to tonsillar compression) and upper motor neurone signs in the legs.
Causes of bilateral lower motor neurone lesions include motor neurone disease, the Guillain-Barré syndrome, poliomyelitis and the Arnold-Chiari malformation.
MULTIPLE CRANIAL NERVE LESIONS
The anatomical courses of the cranial nerves mean they can be affected in groups by single lesions that damage them when they run close to each other. Certain disease processes may also interfere with a number of the cranial nerves. There are a number of syndromes that result from abnormalities of groups of cranial nerves:
• Unilateral III, IV, V and VI involvement suggests a lesion in the cavernous sinus.
• Unilateral V, VII and VIII involvement suggests a cerebellopontine angle lesion (usually a tumour).
• Unilateral IX, X and XI involvement suggests a jugular foramen lesion.
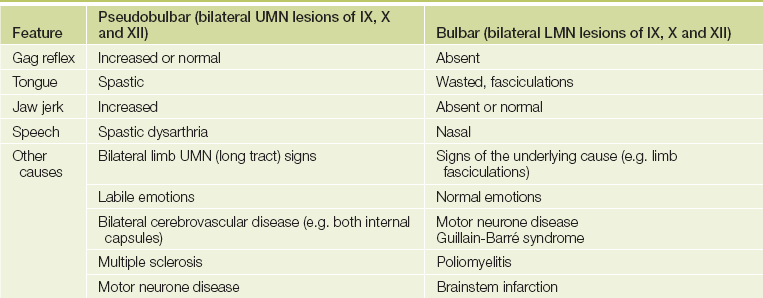
• Combined bilateral X, XI and XII involvement suggests bulbar palsy if lower motor neurone changes are present and pseudobulbar palsy if there are upper motor neurone signs. The clinical features of pseudobulbar and bulbar palsies are shown in Table 32.2, and the causes of multiple cranial nerve palsies are listed in List 32.1.
• Weakness of the eye and facial muscles that worsens with repeated contraction suggests myasthenia. Weakness of the eye muscles that does not conform to a cranial nerve distribution may be due to orbital myopathy. Here the pattern of weakness does not fit with any cranial nerve abnormality.
Head and neck
Inspect and palpate the skull for scars (previous surgery or trauma) and lumps, such as may be caused by a meningioma or a sarcoma. Auscultate the skull by placing the diaphragm of the stethoscope on the frontal bone, and then on the lateral occipital bones, and then place the bell over each eye (with the opposite eye open). Ask the patient to hold his or her breath each time. Bruits heard over the skull may be due to an arteriovenous malformation, advanced Paget’s disease or a vascular meningioma, or they may be conducted from the carotids.
CAROTID BRUITS
Examination anatomy
The left common carotid artery arises directly from the aorta and the right arises from the brachiocephalic artery, which is the first branch of the aortic arch. The common carotids run up from the level of the sternoclavicular joint and back through the neck to divide at the level of the upper border of the thyroid cartilage into the external and internal carotids. The external carotids continue to the parotid glands where they terminate and branch into the superficial temporal and mandibular arteries. The internal carotid climbs to the base of the skull and enters it via the carotid canal in the temporal bone (see Figure 32.44).
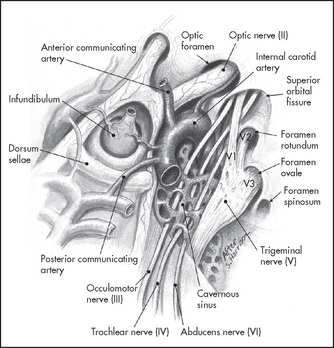
Figure 32.44 Anatomy of the carotid artery (Ducic Y. Operative techniques in otolaryngology. Head and Neck Surgery 2010; 21(1):9–18.)
It is traditional to listen for carotid bruits with the bell of the stethoscope placed somewhere between the angle of the jaw and the upper end of the thyroid cartilage, but no method has been shown to be better than any other.
Carotid bruits are common, being found in 20% of children and 1% of adults. They are more common in patients with increased cardiac output (anaemia, thyrotoxicosis and haemodialysis fistula). They must be distinguished from the conducted murmur of aortic stenosis (louder over the praecordium) and from venous hums (diastolic component and abolished by gentle pressure on the neck above the stethoscope).
The significance of a bruit is its association with carotid artery stenosis and stroke. The LR+ for significant carotid stenosis (70–99% stenosis by Doppler ultrasound) is about 4.8 In symptomatic patients (ipsilateral previous transient ischaemic attack or stroke) a bruit predicts significant stenosis with a very similar LR+. The absence of a bruit does not rule out a significant lesion.
There is general agreement that the presence of a bruit indicates an increased risk of atherosclerotic disease and in younger patients (<75), at least, an increase in risk of stroke to an annual incidence of 1–3%.9 However, since the correct treatment of these patients has not been established, various groups have recommended that asymptomatic patients should not be examined for the presence of a carotid bruit lest its discovery cause unnecessary alarm and tests.10
INTRODUCTION (STEM)cccc
‘This patient is a volunteer actor, but let us assume that he has had a stroke that has affected his vision. Please examine his second, third, fourth and sixth cranial nerves.’
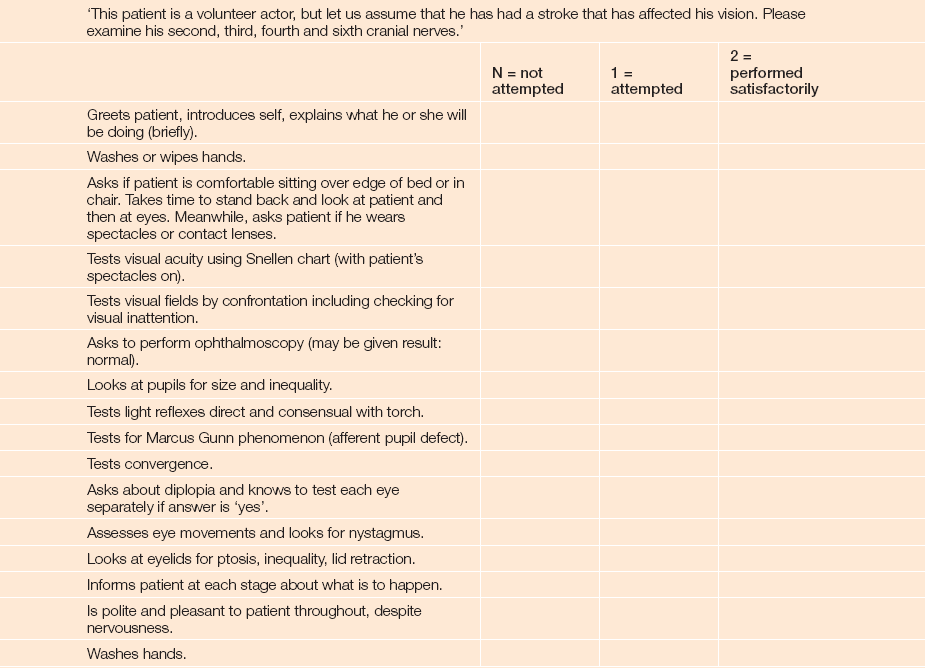
In a case like this there are unlikely to be any abnormal findings. The examiners are therefore especially interested in the student’s technique and understanding of the reasons why the examination is conducted in the way that it is. It is not necessary to perform the examination in exactly this order but no major step should be left out. The stem in this case contains important information. The patient is an actor, so abnormal findings are unlikely.
The examiners have asked for the examination of specific cranial nerves, so it is important not to waste time on examining other nerves. Note the emphasis in the examining sheet on hand-washing and a considerate approach to the patient.
ccThis is usually written on the marking sheet and is standardised for each case to avoid misleading any student
References
1. Thomas, KE, Hasbun, R, Jekel, J, et al. The diagnostic accuracy of Kernig’s sign, Brudzinski’s sign, and nuchal rigidity in adults with suspected meningitis. Clin Infect Dis. 2002; 35:46–52.
2. Van de Beek, D, De Gans, J, et al. Clinical features and prognostic factors in adults with bacterial meningitis. N Engl J Med. 2004; 351(18):1849–1859.
3. Steinberg, D. Scientific neurology and the history of the clinical examination of the cranial nerves. Semin Neurol. 2002; 22:349–356. [An interesting historical review that explains the background to the modern understanding of cranial nerve function and structure.].
4. McGee, S. Evidence-based physical diagnosis, 3rd edn. St Louis: Saunders, 2012.
5. Levin, DE. The clinical significance of spontaneous pulsations of the retinal vein. Arch Neurol. 1978; 35:37–40. [Elevated intracranial pressure is excluded if pulsations are observed in the retinal veins. However, the absence of pulsations in the retinal veins does not necessarily mean that intracranial pressure is elevated.].
6. Nelson, KR. Use new pins for each neurologic examination [Letter]. New Engl J Med. 1986; 314:581. [A cautionary tale.].
7. Ruffin, et al. Gag reflex in disease [Letter]. Chest. 1987; 92:1130. [This suggests that many normal people may have an absent gag reflex.].
8. De Virgilio, Toosie, K, et al. Asymptomatic carotid artery stenosis screening in patients with lower extremity atherosclerosis: a prospective study. Ann Vasc Surg. 1997; 11(4):374–377.
9. US Preventive Services Task Force. Screening for asymptomatic carotid artery stenosis. Guide to clinical preventive services, 2nd edn., Baltimore: Lippincott Williams & Wilkins; 1996:53–61.
10. Pickett, CA, Jackson, JL, Hemann, BA, Atwood, JE. Carotid bruits and cerebrovascular disease risk: a meta-analysis. Stroke. 2010; 41(10):2295–2302. [The presence of a carotid bruit does signify an increased stroke risk but does not identify critical carotid stenosis. Absence of a carotid bruit on auscultation cannot exclude carotid stenosis.].
aIf the patient in an OSCE exam is unconscious, it may be best to ask if another patient can be provided.
bJosef Brudzinski (1874–1917), Polish paediatrician, described this in 1909.
cVladimir Kernig (1840–1917), St Petersburg neurologist, described this in 1882.
dThe anatomy and function of the cranial nerves was well established by the late 19th century. Galen identified at least seven of the cranial nerves in the 2nd century. These were probably the optic, the oculomotor, the sensory part of the trigeminal, the motor part of the trigeminal, the facial, the vestibular, the glossopharyngeal (including the vagus and accessory) and the hypoglossal.
eWilliam Allen Sturge (1850–1919), British physician, described this in 1879, and Frederick Parkes Weber (1863–1962), London physician, described it in 1922.
fSamuel von Sommerring (1755–1830) is responsible for the modern classification of 12 cranial nerves. He separated the vestibular from the facial, and the glossopharyngeal from the vagus and accessory.
gOther abnormalities of smell are hyperosmia and parosmia. Hyperosmia is an increase in the sensitivity of the sense of smell. It is often a sign of psychosis or hysteria but may occur with migraine, during menstruation and in cases of encephalitis. Parosmia is a perversion of the sense of smell. It can occur following trauma to the head and in some psychoses. Olfactory hallucinations are more often than not a result of an organic lesion and suggest an irritating lesion in the olfactory cortex.
hHermann Snellen (1834–1908), Dutch ophthalmologist, invented this chart in 1862.
iModern cataract surgery leaves the lens capsule in place so that iridodonesis does not occur.
jLudwig Edinger (1855–1918), Frankfurt neurologist, and Carl Friedrich Otto Westphal (1833–90), Berlin neurologist.
kGross differences are abnormal and called anisocoria. A small amount of fluctuation in the size of the pupils is normal and called pupillary unrest. More pronounced rhythmical contraction and dilation of the pupils is called hippus; this may follow recovery from a third nerve palsy or occur during sleepiness. This is not often of any significance and is not a localising sign except when it is present as a rare sign of severe aortic regurgitation.
lRobert Marcus Gunn (1850–1909), London ophthalmologist, described the defect in 1883.
mWilliam Adie (1886–1935), Australian neurologist working in Britain, described this in 1931.
nHenri Parinaud (1844–1905), French ophthalmologist, described this in 1889.
oThe presence of these pins in the lapel of a well-cut white coat or expensive suit often indicates that the wearer is a neurologist.
pHumans began as hunters on the savannah; there were no predators threatening us from above, so our eye movements evolved to give us better horizontal movement than vertical movement. Healthy elderly people have quite poor upward gaze.
qJ Steele and J Richardson, Canadian neurologists, described this in 1964.
rJohann Laurenz Gasser (1723–65), professor of anatomy, Vienna.
sTesting of the sneeze reflex is not routine. Here, stimulation or irritation of the nasal mucosa with a hair or small piece of string is followed by contraction of the muscles of the nasopharynx and thorax. The afferent limb of this arc is through the trigeminal nerve and the efferent limb through the facial, glossopharyngeal, vagus and trigeminal nerves, and the motor nerves of the cervical spine. The reflex centre is in the brainstem and upper spinal cord.
tSir Charles Bell (1774–1842), professor of anatomy at London’s Royal College of Surgeons, later professor of surgery at Edinburgh, described facial nerve palsy in 1821.
uJames Ramsay Hunt (1874–1937), American neurologist.
vA patient with an old Bell’s palsy may exhibit synkinesis. When the patient blinks, the corner of the mouth twitches; when the lips are protruded, the affected eye closes.
wAlfonso Corti (1822–1888), Italian anatomist, described this in 1851.
xHeinrich Adolf Rinné (1819–1968), German ear specialist, described his test in 1855 using a 512 Hz fork.
yErnest Heinrich Weber (1795–1878), German physiologist.
zCharles Hallpike (1900–79), English ear, nose and throat surgeon.
aaVelum means ‘curtain’ in Latin.
bbbb Julies Arnold (1835–1915) and Hans Chiari (1851–1916), German pathologists, described this in 1894.