The breasts
Breast examination is a vitally important part of the general physical examination. In women aged 40 and older, a screening physical examination for breast cancer may be advised (e.g. monthly self-examination by the patient and yearly examination by the doctor), but there is no convincing evidence of the value of breast self-examination.1
Examination anatomy
The attachment of the female breast extends from the clavicle superiorly to the ‘bra line’ (sixth rib) inferiorly and from the sternum to the midaxillary line (see Figure 39.1). The area covered is more rectangular than circular. The axillary tail is an extension of the superolateral part of the breast up towards the axilla. This tail extends along the lower border of the pectoralis major muscle and may pass through the deep fascia to approach the axillary lymph nodes.
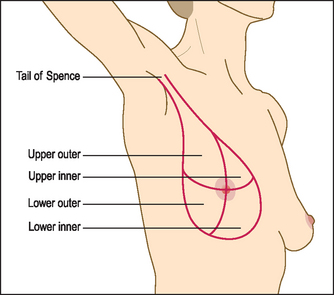
Figure 39.1 Breast anatomy (Douglas G, Nicol F, Robertson C. Macleod’s clinical examination, Churchill Livingstone: 2009.)
Breast tissue has fatty, glandular and fibrous components. Except during lactation, most of the bulk of the breast is adipose tissue. There is a surrounding superficial fascia attached to the skin and pectoral fascia by ligaments. The normal breast does not have a homogeneous feel but is somewhat lumpy.
There are a number of benign abnormalities of the breast that change the texture or appearance of the breast, including:
History
The history is imperative. Essential questions to ask include the length of time any mass has been noticed, the presence of pain, any change in size or texture over time, relationship to the menstrual cycle, and any nipple discharge. Ask whether the patient has conducted regular self-examinations and discovered a change in her breast. Ask about previous cyst aspirations.
Find out about risk factors for breast cancer, including any family history of breast or ovarian cancer (and age affected), previous personal history of breast cancer, obesity, early menarche and late menopause, late first pregnancy, mantle radiation, heavy alcohol use and use of oestrogens post-menopausally. A personal history of atypical hyperplasia (ductal or lobular) increases the risk of breast cancer 3 to 5 times. However, three-quarters of patients presenting with a breast cancer have no known risk factors.
The breast cancer genes BRCA1 and BRCA2 are associated with a strong risk of breast (and ovarian) cancer, as well as breast cancer in men. Patients with a strong family history of breast or ovarian cancer should be asked if genetic testing has been carried out. Screening mammography is generally recommended for all women from the age of 50 years.2
Enlargement of the male breasts (gynaecomastia; page 376) is often a result of hormone or drug treatment (e.g. for carcinoma of the prostate or with aldactone). It is often tender. Bilateral enlargement is usually benign but unilateral enlargement may be due to malignancy. Since malignancy is more common in men with gynaecomastia, asymmetrical enlargement should arouse concern. Carcinoma of the male breast is over 100 times less frequent than female breast carcinoma. Since there is less breast tissue present in men and the condition is often not thought of, disease tends to be locally advanced at the time of diagnosis.
Examination
When it is done properly, the examination takes some time to perform (about 3 minutes per breast).3 The need for examination must obviously be explained to the patient at the start. The patient should be offered a chaperone.
The examination is only just over 50% sensitive for carcinoma but specificity is as high as 90%. The likelihood ratio of a positive examination is 14.1 and the LR of a negative examination is 0.47.4
INSPECTION
Ask the patient to sit up with her chest fully exposed. There is controversy about the value of inspection of the breasts as part of the examination, but advanced cancers may be obvious at this stage. Look at the nipples for retraction (due to cancer or fibrosis; in some patients retraction may be normal, so it is important to ask if it is long-standing) and Paget’s disease of the breast (where underlying breast cancer causes a unilateral red, bleeding skin). Asymmetry of breast size is common, and it is important to ask the woman if any asymmetry is new.
Next inspect the rest of the skin. Look for visible veins (which if unilateral suggest a cancer), skin dimpling and peau d’orange skin (where advanced breast cancer causes oedematous skin pitted by the sweat glands).
A persistent erythematous plaque in the areola area may be contact dermatitis or skin irritation, but if asymmetrical or it has not responded to treatment this may be the malignancy Paget’s disease of the breast.
Ask the patient to raise her arms above her head and then lower them slowly. Look for tethering of the nipples or skin, a shift in the relative position of the nipples or a fixed mass distorting the breast (see Figure 39.2).

Figure 39.2 Carcinoma of the right breast, showing elevation of the breast, dimpling of the skin and retraction of the nipple
Note whether there are any obvious visible masses in the axillae.
Next ask her to rest her hands on her hips and then press her hands against her hips (the pectoral contraction manoeuvre). This accentuates areas of dimpling or fixation.
Conditions unrelated to the breast may be found incidentally, such as pectus excavatum or carinatum, distended veins related to inferior vena caval (IVC) obstruction and signs of virilisation such as acne and hirsutism.
PALPATION
Examine both the supraclavicular and the axillary regions for lymphadenopathy. It may be difficult, however, to distinguish an axillary fat pad from an enlarged lymph node.
Then ask the patient to lie down. The examination can be performed only if the breast tissue is flattened against the chest wall. If the breasts are large, it can be helpful to have the patient place her hand behind her head for palpation of the lateral aspect of the breast and bring her elbow up level with the shoulder for palpation of the medial side of the breast.
Palpation is performed gently with the pulps of the middle three fingers parallel to the contour of the breast. Feel the four quadrants of each breast systematically (see Figure 39.3(a)). Do not pinch the breast as you may mistakenly think you feel a mass. The total examination should involve a rectangular area bordered by the clavicle, the sternum, the midaxillary line and the bra line. Start in the axilla and palpate in a line down to the bra line inferiorly. The pattern of palpation is like that of mowing a lawn, a series of vertical strips that cover the whole of the rectangle (see Figure 39.3(b)). There is no single correct way to palpate the breast, as long as all sections are palpated. Palpation may also be performed by quadrant, in a spiral fashion from the nipple outwards or in a ‘flower petal’ pattern radiating around the breast from the nipple outwards.
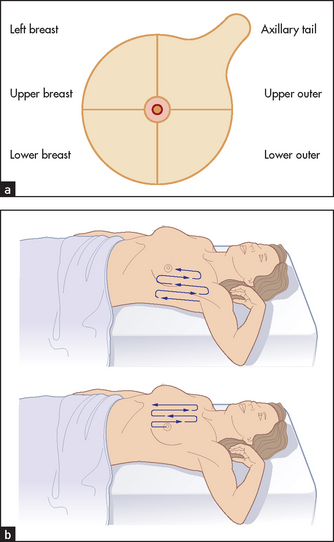
Each area is palpated three times, using small circular movements and slightly increasing pressure. Palpation is more difficult when a breast implant is present. It is probably best to examine such a patient in a supine position and to keep the ipsilateral arm down at her side.
Next feel behind the nipple for lumps and note if any fluid can be expressed: bright blood (from a duct papilloma, fibroadenosis or carcinoma), yellow serous fluid (fibroadenosis) or serous fluid (early pregnancy), milky fluid (lactation) or green fluid (mammary duct ectasia).
Do not mistake normal breast structures for a mass.5 You may feel a rib or costochondral junction normally on deep palpation. The inferior ridge of breast tissue (inframammary fold) may be felt and is symmetrical. You may feel normal rubbery-type plaques (fibroglandular tissue), especially in the upper outer quadrant. It is normal to feel firm breast tissue at the areola border, and the upper outer quadrant of the breast is often dense.
Evaluation of a breast lump
The following five points need to be carefully elucidated if a lump is detected.
1. Position: the breast quadrant involved and proximity to the nipple.
2. Size, shape and consistency: a hard, irregular nodule is characteristic of carcinoma; a hard, smooth regular nodule is more likely to be a fibroadenoma, especially in a young woman.
3. Tenderness: suggests an inflammatory or a cystic lesion; breast cancer is usually not tender, although inflammatory breast cancer is associated with tenderness.
4. Fixation: mobility is determined by taking the breast between the hands and moving it over the chest wall; in advanced carcinoma the lump may be fixed to the chest wall.
5. Single or multiple lesions present: multiple nodules suggest benign cystic disease or fibroadenosis.
Remember that lumps found on breast examination may not involve breast tissue: these include lipomas and sebaceous cysts.
Remember also that many normal breasts have palpable lumps and that although benign lumps tend to be soft, moveable and regular, they can also have the characteristics of malignant lumps.5 Causes of a lump in the breast are listed in Table 39.1.
TABLE 39.1
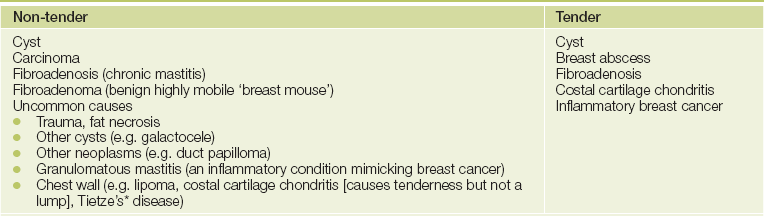
*Alexander Tietze (1864-1927), chief surgeon, Allerheiligen Hospital, Breslau, Poland. He described the condition in 1921.
In men with true gynaecomastia, a disc of breast tissue can be palpated under the areola. This is not present in men who are merely obese. Causes of breast enlargement in men are presented on page 376.
References
1. Riley, M, Dobson, M, Jones, E, Kirst, N. Health maintenance in women. Am Fam Physician. 2013; 87(1):30–37. [Describes current guidelines for screening for breast cancer and other cancers in women.].
2. Kerlikowske, K, Smith-Bindman, R, Ljung, BM, et al. Evaluation of abnormal mammography results and palpable breast abnormalities. Ann Intern Med. 2003; 139:274–284. [Discusses how to approach interpreting mammogram reports and the next steps.].
3. Fenton, JJ, Rolnick, SJ, Harris, EL, et al. Specificity of clinical breast examination in community practice. J Gen Intern Med. 2007; 22(3):332–427. [Screening breast examinations in clinical practice are highly specific but insensitive. A normal exam is reassuring.].
4. Barton, MB, Harris, R, Fletcher, SW. Does this patient have breast cancer. JAMA. 1999; 282:1270–1280. [The clinical breast examination has an overall specificity that is high (94%) but the sensitivity is poor (54%). Unfortunately, interobserver variation seems to be high.].
5. Pruthi, S. Detection and evaluation of a palpable breast mass. Mayo Clin Proc. 2001; 76:641–647. [Most breast masses are benign but malignancy must be excluded. If cancer is suspected but mammography is negative, further testing is indicated.].