Correlation of physical signs and endocrine disease
Calcium metabolism
PRIMARY HYPERPARATHYROIDISM
This is due to excess parathyroid hormone (see List 29.1), which results in an increased serum calcium level, increased renal phosphate excretion and increased formation of 1,25-dihydroxycholecalciferol by activation of adenylcyclase in the bone and kidneys. Primary hyperparathyroidism causes problems with ‘stones’ (renal stones), ‘bones’ (osteopenia and pseudogout), ‘abdominal groans’ (constipation, peptic ulcer and pancreatitis) and ‘psychological moans’ (confusion) (see Questions box 29.1).
Questions box 29.1
Questions to ask the patient with suspected hyperparathyroidism
 denotes symptoms for the possible diagnosis of an urgent or dangerous problem.
denotes symptoms for the possible diagnosis of an urgent or dangerous problem.
1. Have you had kidney stones?
2. Have you had any fractures?
3. Have you been troubled by abdominal pain? Have you had constipation?
4. Have you been depressed or had hallucinations? (Psychiatric disorders)
5. Have you had episodes of confusion, irritability, extreme tiredness or even unconsciousness? (Neurological symptoms)
Other causes of hypercalcaemia are outlined in List 29.2.
General inspection
Note the mental state of the patient. Severe hypercalcaemia may cause coma or convulsions. Assess hydration (polyuria from hypercalcaemia may cause dehydration).
THE MEN SYNDROMES
The multiple endocrine neoplasias (MENs), types I and II, are autosomal dominant conditions. Hyperparathyroidism may be associated with both. MEN type I (due to a mutation on chromosome 11) is associated with tumours of the parathyroid, pituitary and pancreatic islet cells. MEN type IIA (due to a mutation on chromosome 10 involving the c-ret proto-oncogene) is associated with medullary carcinoma of the thyroid, hyperparathyroidism and phaeochromocytoma. MEN type IIB is characterised by mucosal neuromas (often on the lips and tongue; see Figure 29.1) and medullary carcinoma of the thyroid plus phaeochromocytoma.

HYPOPARATHYROIDISM
Hypoparathyroidism results in hypocalcaemia with neuromuscular consequences (tetany) (see Questions Box 29.2). It is usually a postoperative complication after thyroidectomy, but can be idiopathic. Hypocalcaemia can also result from end-organ resistance to parathyroid hormone (pseudohypoparathyroidism; see List 29.3).
Questions box 29.2
Look first for Trousseau’s and Chvostek’s signs. Trousseau’s sign is elicited with a blood pressure cuff placed on the arm with the pressure raised above the patient’s systolic pressure. Typical contraction of the hand occurs within 2 minutes when hypocalcaemia has caused neuromuscular irritability. The thumb becomes strongly adducted, and the fingers are extended, except at the metacarpophalangeal joints. The appearance is that of an obstetrician about to remove the placenta manually and is called the main d’accoucheur.
Chvostek’s sign is performed by tapping gently over the facial (seventh) cranial nerve under the ear. The nerve is hyperexcitable in hypocalcaemia and a brisk muscular twitch occurs on the same side of the face.
Next test for hyperreflexia, again due to neuromuscular irritability.
Look at the nails for fragility and monilial infection. Note any dryness of the skin. Go to the face and look for deformity of the teeth. Examine the eyes for cataracts or papilloedema. These signs may all occur in idiopathic hypoparathyroidism, an autoimmune disease. Cataracts may also follow surgically induced hypoparathyroidism.
Pseudohypoparathyroidism
In pseudohypoparathyroidism the patients have tetany (due to hypocalcaemia) as well as typical skeletal abnormalities. These include short stature, a round face, a short neck, thin stocky build and very characteristically short fourth or fifth fingers or toes (due to metacarpal or metatarsal shortening; this can be unilateral or bilateral; see Figure 29.2). Ask the patient to make a fist to demonstrate the characteristic clinical signs.

Osteoporosis and osteomalacia
These bone diseases have endocrine and non-endocrine causes (see List 29.4). Osteoporosis is a failure of production of normal bone matrix, which leads to a reduction in bone mass and an increased risk of fractures. Many cases are a result of the relative hypogonadism that occurs with age, but often in combination with reduced vitamin D levels. Although the reduced bone mineral density that occurs in elderly people and is associated with fractures is called osteoporosis, it is usually at least partly the result of osteomalacia. In women, conditions that reduce oestrogen increase the risk: hypogonadism before menopause (e.g. anorexia nervosa), menopause, anti-oestrogenic drugs, smoking and being underweight.
Osteomalacia means defective bone mineralisation. It is usually due to low vitamin D levels, which lead to inadequate calcium absorption. This results in secondary hyperparathyroidism, which helps maintain serum calcium levels but at the expense of increased osteoclast activity and loss of calcium from the skeleton. When the condition occurs in childhood it causes rickets.
Many patients are asymptomatic but common symptoms (see Questions box 29.3) include unexpected fractures (especially of the vertebral bodies and associated with severe back pain, hip and wrist fractures); some people notice loss of height as a result of the development of thoracic kyphosis. The diagnosis may have been made from an X-ray taken for another reason or as a result of a screening bone mineral density (DEXA) scan.
The examination
Measure the patient’s height using a stadiometer (an upright bar with a sliding scale). Comparing this measured height with the patient’s recollection of previous height measurements has been shown to be an accurate way of detecting a change in height. Thoracic kyphosis can be measured as is done for patients with ankylosing spondylitis by measuring the occiput-to-wall distance (see Figure 29.3). Inability of the patient when standing straight to touch the wall with the back of the head is considered abnormal (LR+ 3.8)1 and serial measurements of the occiput to wall distance can be helpful in following the course of the disease.

Lumbar fractures can be assessed by measuring the rib-to-pelvis distance (see Figure 29.4). Have the patient stand facing away from you with arms extended. Insert your fingers between the lower costal margin and the superior surface of the pelvis in the midaxillary line. Normally, more than two fingers can be inserted (LR+ 3.8).2
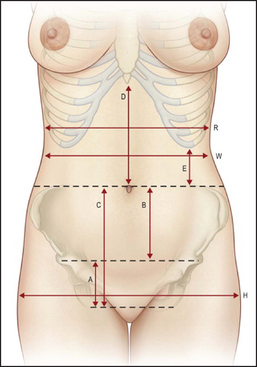
Figure 29.4 The ribs-to-pelvis distance Anatomical landmarks. Normal abdominal anatomical proportions. The approximate measurements for an average female abdomen are listed. These vary according to individual height and bone structure. The umbilicus is located in line with the most superior point of the iliac crest in 99% of patients. (A) Distance between top of mons and anterior valvar commissure. Average height is 5–7 cm. (B) Distance between umbilicus and top of mons. Average height is 11–13 cm. (C) = (A + B) Distance between umbilicus and top of anterior and vulvar commissure (C = D). (E) Distance between the costal marginal and the iliac crest. The proportion of this distance to the width of the base of the rib cage (R) determines whether the patient is long waisted or short waisted. The normal proportion (E:R) is roughly 1:3 (long waisted approaches 1:2, short waisted approaches 1:3). The rib cage tapers inferiorly. A narrower lower rib cage relative to the width under the armpits helps to emphasize the waist by creating a subtle V. (H) Hip width. A wider pelvis than rib cage emphasises the waist; the waist is more defined when R<H. (W) Natural waist—the narrowest point of the torso. (Note that the umbilicus usually sits below the natural waist by about 1–4 cm). Relative to the hips, this waist-to-hip (W:H) ratio in healthy women is roughly 0.72:1; in healthy men, it is roughly 0.83:1. Note that the natural contour of the healthy abdomen reveals a subtle epigastric sagittal depression transitioning to a mild infraumbilical convexity. A subtle vertical sulcus at ‘eh’ lateral rectus border, which is more distinct in a muscular person, may also be seen. (Neligan PC. Plastic surgery, 3rd edn, 6-volume set. Elsevier, 2013.)
If the patient reports recent severe back pain, feel for tenderness over the spine. Remember, however, that fractures of the vertebral body may not cause localised tenderness—sometimes percussion over the area may elicit tenderness. Remember also that the differential diagnosis for these fractures includes malignancy (e.g. myeloma).
Syndromes associated with short stature
These conditions begin in childhood.
General inspection
First measure the height of the patient; in children this should be compared with percentile charts for age and sex. Look for the classical appearance of Turner’s syndrome (see Figure 29.5), Down syndrome, achondroplasia or rickets (see Figure 29.6), which may explain the short stature. The height of parents and siblings should be checked as well.

Figure 29.5 Turner’s syndrome (Wales JKH, Wit JM, Rogol AD. Pediatric endocrinology and growth, 2nd edn. Philadelphia: Saunders, 2003.)

Note any evidence of weight loss, including loose skinfolds, which may suggest a nutritional cause (starvation, malabsorption or protein loss). Look for signs of hypopituitarism or hypothyroidism, or steroid excess. Sexual precocity (early onset of secondary sexual characteristics) causes relative tallness at first but short stature later.
TURNER’S SYNDROME (45XO)
Sexual infantilism (failure of development of secondary sexual characteristics)—female genitalia (see Figure 29.5) Look for:
• Upper limbs. Lymphoedema of the hands; short fourth metacarpal bones; hyperplastic nails; increased carrying angle; hypertension.
• Facies. Micrognathia (small chin); epicanthic folds ptosis; fish-like mouth; deformed or low-set ears; hearing loss.
• Neck. Webbing of the neck; low hairline; redundant skinfolds on the back of the neck.
• Chest. Widely spaced nipples (a shield-like chest); coarctation of the aorta.
• Other. Pigmented naevi; keloid formation; lymphoedema of the legs.
DOWN SYNDROME (TRISOMY 21)
• Facies. Oblique orbital fissures; conjunctivitis; Brushfield spots on the iris; small simple ears; flat nasal bridge; mouth hanging open; protruding tongue; narrow high-arched palate.
• Hands. Short broad hands; incurving fifth finger; single palmar crease; hyperflexible joints.
• Chest. Congenital heart disease; especially endocardial cushion defects.
• Other. Straight pubic hair; gaps between the first and second toes; mental deficiency usually present.
ACHONDROPLASIA (DWARFISM)
This is an autosomal-dominant disease of cartilage caused by mutation of the fibroblast growth factor receptor gene. Short stature, short limbs, normal trunk, relatively large head, saddle-shaped nose, exaggerated lumbar lordosis and occasionally spinal cord compression are features. Look for:
RICKETS
Defective mineralisation of the growing skeleton (see Figure 29.6), due to lack of vitamin D (e.g. nutritional or chronic renal failure) or hypophosphataemia (e.g. renal tubular disorders). Look for:
• Upper limbs. Tetany; hypotonia, proximal myopathy; bowing of the radius and ulna.
• Facies. Frontal bossing; parietal flattening.
• Chest. ‘Rickety rosary’—thickening of costochondral junctions; Harrison’s groove—indentation of lower ribs at the diaphragmatic attachment.
• Lower limbs. Bowing of femur and tibia; hypotonia, proximal myopathy; fractures.
Hirsutism
This is excessive hairiness in a woman beyond what is considered normal for her race (see List 29.5). It is caused by androgen (including testosterone) excess. In the examination of such a patient, it is important to decide whether virilisation is also present. Virilisation is the appearance of male secondary sexual characteristics (clitoromegaly, frontal hair recession, male body habitus and deepening of the voice) and indicates that excessive androgen is present.
General inspection
Ask the patient to undress to her underwear. Note the hair distribution over the face (see Figure 29.7) and in the midline, front and back. In general, an obvious male balding pattern (a receding hairline), hair over the beard area or on the back and chest and hair in the escutcheon (umbilicus to groin in the midline) is usually abnormal. Look for obvious acromegaly or Cushing’s syndrome and for the skin changes of porphyria cutanea tarda.

Figure 29.7 Hirsutism due to the polycystic ovary syndrome (Black M. Obstetric and gynecologic dermatology, 3rd edn. Mosby, 2008.)
Ask the patient to remove her underclothing and lie flat. Look for signs of virilism. These include breast atrophy and increased muscle bulk of the arms and legs, male pattern of pubic hair and enlargement of the clitoris. Look in the axillae; the patient with polycystic ovarian syndrome may have acanthosis nigricans (and associated insulin resistance).
Gynaecomastia
Gynaecomastia is ‘true’ enlargement of the male breasts (see Figure 29.8).3 Careful examination will detect up to 4 centimetres of palpable breast tissue in 30% of normal young men; this percentage increases with age. These men are unaware of any breast abnormality. Gynaecomastia occurs in up to 50% of adolescent boys, and also in elderly men in whom it is due to falling testosterone levels. Fat deposition (‘false’ enlargement) in obese men can be confused with gynaecomastia.
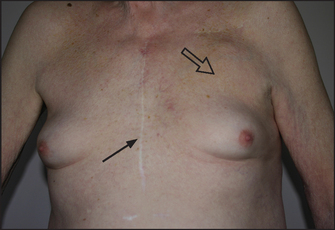
Figure 29.8 Gynaecomastia This patient takes spironolactone for heart failure. Note median sternotomy scar (arrow) and defibrillator box (open arrow).
Examine the breasts (see Chapter 39) for evidence of localised disease (e.g. malignancy, which is rare), tenderness, which indicates rapid growth, and any discharge from the nipple. Detection of breast tissue in men is best performed with the patient sitting up. Squeeze the breast behind the patient’s nipple between the thumb and forefinger. Try to detect an edge between subcutaneous fat and true breast tissue.
Examine the genitalia for sexual ambiguity and the testes for absence or a reduced size. Note any loss of secondary sexual characteristics.
Look especially for signs of Klinefelter’s syndrome (see Figure 29.9). These patients are tall, have decreased body hair and have characteristically small, firm testes.
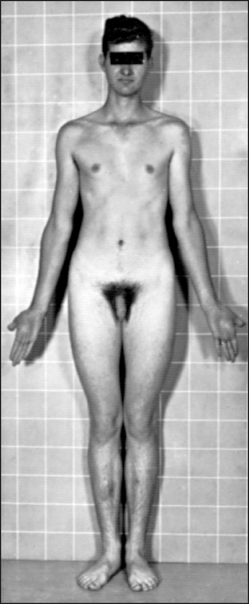
Figure 29.9 Klinefelter’s syndrome; note the long limbs, narrow shoulders and chest, and relatively small genitals (Grumbach MM, Hughes IA, Conte FA. Disorders of sex differentiation. In Larsen PR, Kronenberg HM, Melmed S, Polonsky KS (eds). Williams textbook of endocrinology, 10th edn. Philadelphia: Saunders, 2003).
Look also for signs of panhypopituitarism or chronic liver disease. Thyrotoxicosis can occasionally be a cause.
Finally, examine the visual fields and fundi for evidence of a pituitary tumour.
Causes of pathological gynaecomastia are summarised in List 29.6.
Diabetes mellitus
Diabetes mellitusa is characterised by hyperglycaemia due to an absolute or a relative deficiency of insulin. The causes of diabetes are outlined in List 29.7. The disease can present with asymptomatic glycosuria detected on routine physical examination or with symptoms of diabetes (see List 27.1 on page 351), ranging from polyuria to coma as a result of diabetic ketoacidosis (see Questions box 29.4).
Questions box 29.4
Questions to ask the diabetic patient
denotes symptoms for the possible diagnosis of an urgent or dangerous problem.
1. What was your age at the time the diabetes was diagnosed?
2. Did you require insulin from the start?
3. What was the problem that led to the diagnosis? (Polyuria, thirst, weight loss, recurrent skin infections, screening assessment)
4. What previous and current drug treatment are you taking for diabetes?
5. What diet has been prescribed? What do you understand about your diabetic diet?
6. What blood sugar testing do you do? What are the usual results?
7. Have you had any problems with hypoglycaemia (treatment-induced low blood sugar)? Have you had episodes of sweating, confusion, malaise or unconsciousness?
8. Do you know what action should be taken if these acute symptoms (of hypo- or hyperglycaemia) occur? (Check sugar level, take glucose tablet, go to hospital)
9. Have you had ketoacidosis (very high blood sugar associated with acidosis) and needed admission to hospital? (Polyuria, dehydration, confusion, unconsciousness)
10. Have you had complications of diabetes—eyes, nerves, blood vessels, kidneys?
11. What regular testing has been performed for these problems?
12. How do you and your family cope with this chronic condition?
General inspection
Assess for evidence of dehydration because the osmotic diuresis caused by a glucose load in the urine can cause massive fluid loss. Note obesity (type 2 diabetics are usually obese) or signs of recent weight loss (this can be evidence of uncontrolled glycosuria).
Look for one of the abnormal endocrine facies (e.g. Cushing’s syndrome or acromegaly) and for pigmentation (e.g. haemochromatosis—bronze diabetes) as these may cause secondary diabetes.
The patient may be comatose due to dehydration, acidosis or plasma hyperosmolality. Kussmaul’s breathing (‘air hunger’) is present in diabetic ketoacidosis due to the acidosis (this occurs because fat metabolism is increased to compensate for the lack of availability of glucose; excess acetyl-coenzyme A is produced, which is converted in the liver to ketone bodies, and two of these are organic acids).
Lower limbs
Unlike most other systematic examinations, assessment of the diabetic can profitably begin with the legs, as many of the major physical signs are to be found here. In particular, vascular and neurological abnormalities in the feet must not be missed.4
Inspection
Look at the skin. The skin of the feet and lower legs may be hairless and atrophied due to small-vessel vascular disease and resultant ischaemia (the mechanism is uncertain, but may be related to lipoprotein alterations in the vessel walls).
Note any leg ulcers, particularly on the toes or any area of the feet exposed to pressure (see Figure 29.11). These ulcers are due to a combination of ischaemia and peripheral neuropathy (the cause of the neuropathy is unknown, but may be related to small vessel ischaemia and glycosylation of neural proteins). Look at the ankles for signs of a Charcot’s joint (grossly deformed disorganised joints, due to loss of proprioception or pain, or both; this leads to recurrent and unnoticed injury to the joint). Damage to the skin unprotected by pain sensation can also occur.

Figure 29.11 Diabetic (neuropathic) ulcer (From McDonald FS, ed. Mayo Clinic images in internal medicine, with permission. © Mayo Clinic Scientific Press and CRC Press.)
Look for superficial skin infection, such as boils, cellulitis and fungal infections. These are more common in diabetics because of a combination of high tissue glucose levels and ischaemia, which provides a favourable environment for the growth of organisms.
Note any pigmented scars (late diabetic dermopathy). There may be small rounded plaques with raised borders lying in a linear fashion over the shins (diabetic dermopathy).
Necrobiosis lipoidica diabeticorum is a reasonably specific skin manifestation of diabetes mellitus, but is rare (fewer than 1% of diabetics; see Figure 29.12). It is found over the shins, where a central yellow scarred area is surrounded by a red margin when the condition is active. These plaques may ulcerate.

Figure 29.12 Necrobiosis lipoidica diabeticorum (From McDonald FS, ed. Mayo Clinic images in internal medicine, with permission. © Mayo Clinic Scientific Press and CRC Press.)
TEXT BOX 29.1 A summary of the examination of the diabetic patient

Pigmentation—haemochromatosis, etc
Fundi—cataracts, rubeosis, retinal disease
Carotid arteries—palpate, auscultate
Liver—fat infiltration; rarely haemochromatosis
Urine analysis—glycosuria, ketones, proteinuria
Look at the thighs for insulin injection sites. These may be associated with localised fat atrophy and fat hypertrophy, and may be related to impure insulin use, which causes a localised immune reaction (modern genetically engineered insulins have made these rare). Note any quadriceps muscle wasting due to femoral nerve mononeuropathy, which is called (inaccurately) diabetic amyotrophy.
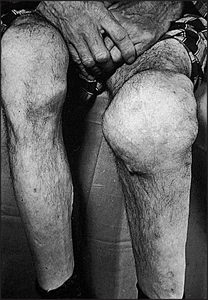
Inspect the knees for Charcot’s joints (see Figure 29.13).
Upper limbs
Look at the nails for signs of Candida infection. Take the patient’s blood pressure lying and standing, as diabetic autonomic neuropathy can cause postural hypotension.
Face
Test visual acuity. This may be permanently impaired because of retinal disease or temporarily disturbed because of changes in the shape of the lens associated with hyperglycaemia and water retention. Look for Argyll Robertson pupils,b which are a rare complication of diabetes.
Using the ophthalmoscope, begin by examining for rubeosis (new blood vessel formation over the iris, which can cause glaucoma; see Figure 29.14). Then note any cataracts, which are related to sorbitol deposition in the lens (when glucose is present in high concentrations in the tissues it is converted to sorbitol by aldose reductase).
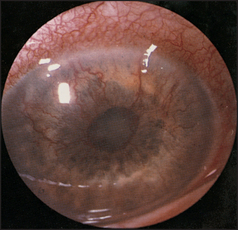
Figure 29.14 Rubeosis iridis Shows new vessels on the anterior surface of the iris. These are secondary to ischaemia (often due to diabetes). (Dr Chris Kennedy and Professor Ian Constable, Lions Eye Institute, Perth)
Now examine the retina, where many exciting changes may await the fundoscopist. There are two main types of retinal change in diabetes: non-proliferative and proliferative.
Non-proliferative changes (see Figure 29.15) are directly related to ischaemia of blood vessels and include: (1) two types of haemorrhages—dot haemorrhages, which occur in the inner retinal layers, and blot haemorrhages, which are larger and occur more superficially in the nerve fibre layer; (2) microaneurysms, which are due to vessel wall damage; and (3) two types of exudates—hard exudates, which have straight edges, and soft exudates (cottonwool spots), which have a fluffy appearance.
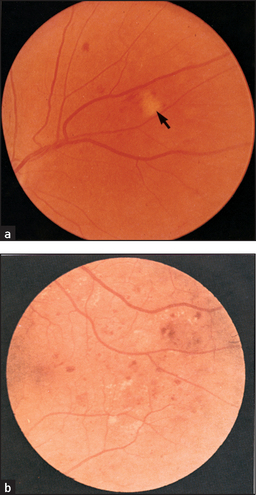
Figure 29.15 Diabetic retinopathy (a) Soft exudate (arrow) and small haemorrhages. (b) Microaneurysms (dots), retinal haemorrhages (blots) and hard yellow exudates. (Dr Chris Kennedy and Professor Ian Constable, Lions Eye Institute, Perth)
Proliferative changes (see Figure 29.16) are changes in blood vessels in response to ischaemia of the retina. They are characterised by new vessel formation, which can lead to vitreal haemorrhage, scar formation and eventually retinal detachment. The detached retina appears as an opalescent sheet that balloons forwards into the vitreous. The underlying choroid is visible through the detached retina as a bright red-coloured sheet. Look also for laser scars (small brown or yellow spots), which are secondary to photocoagulation of new vessels by laser therapy.
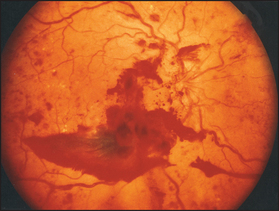
Figure 29.16 Proliferative diabetic retinopathy (Dr Chris Kennedy and Professor Ian Constable, Lions Eye Institute, Perth)
Assess the third, fourth and sixth cranial nerves. In particular, examine for a diabetic third nerve palsy from ischaemia, which usually spares the pupil (as infarction of the third nerve affects the inner pupillary fibres more than the outer fibres; in this way it differs from compressive lesions, which have the opposite effect).
Other cranial nerves may be affected sometimes because of cerebrovascular accidents (large vessel atheroma). Rarely, rhinocerebral mucormycosis may develop in very poorly controlled diabetic patients, causing periorbital and perinasal swelling and cranial nerve palsies.
Look in the ears for evidence of infection. The rare malignant otitis externa, usually due to Pseudomonas aeruginosa, causes a mound of granulation tissue in the external canal, and facial nerve palsy in 50% of cases.
Neck and shoulders
Examine the carotid arteries for evidence of vascular disease. Rarely, there may be thickening of the skin of the upper back and shoulders (scleroedema diabeticorum—this diffuse cutaneous infiltration has a very different distribution from sclerderma, with which it is sometimes confused). Look for acanthosis nigricans—associated with insulin resistance.
Urinalysis
Test for glucose and protein. Diabetic nephropathy (from glomerulonephritis, renal arterial disease or pyelonephritis) can cause proteinuria. The presence of nitrite and/or blood is of value as asymptomatic urinary tract infections can occur. In advanced disease there may be signs of renal failure.
Paget’s disease
Paget’sc disease (osteitis deformans) is characterised by excessive reabsorption of bone by osteoclasts and compensatory disorganised deposition of new bone. It is possibly a disease of viral origin.
General inspection
Note short stature (due to bending of the long bones of the limbs) and any obvious deformity of the head and lower limbs.
Head and face
Inspect the scalp for enlargement in the frontal and parietal areas and measure the head circumference (>55 centimetres is usually abnormal). There may be prominent skull veins. Palpate for increased bony warmth and auscultate over the skull for systolic bruits. Both of these are due to increased vascularity of the skull vault. Oddly enough, bronchial breath sounds may be audible over the pagetic skull through the stethoscope. These are due to increased bone conduction of air. An area of very localised bony swelling and warmth may indicate development of a bony sarcoma (1% of cases of Paget’s disease may develop this complication).
Examine the eyes. Assess visual acuity and visual fields, and look in the fundi for angioid streaks and optic atrophy. Retinitis pigmentosa occurs rather more rarely. Test for hearing loss (due to bony ossicle involvement or eighth nerve compression by bony enlargement).
Examine the remaining cranial nerves; all may be involved because of bony overgrowth of the foramina or be caused by basilar invagination (platybasia; where the posterior fossa becomes flat and the basal angle increased).
Neck
Patients with basilar invagination have a short neck and low hairline. The head is held in extension and neck movements are decreased. Assess the jugular venous pressure, as a high output cardiac failure may be present, particularly if there is coexistent ischaemic heart disease.
Back
Inspect for kyphosis (due to vertebral involvement causing collapse of the vertebral bodies). Tap for localised tenderness, feel for warmth and auscultate for systolic bruits over the vertebral bodies.
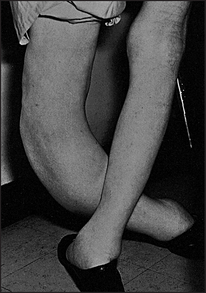
Legs
Inspect for anterior bowing of the tibia and lateral bowing of the femur (see Figure 29.17). Feel for bony warmth and tenderness. Note any changes of osteoarthritis in the hips and knees, which often coexist with Paget’s disease. Note any localised warm swelling, which may indicate sarcoma.
Examine for evidence of paraplegia, which is uncommon but can occur due to cord compression by bone or vascular shunting in the spinal cord. Rarely, cerebellar signs may be present due to platybasia.
References
1. Siminoski, K, Lee, K, et al. Accuracy of physical examination for detection of thoracis vertebral fractures. J Bone Miner Res. 2003; 18(suppl 2):S82.
2. Siminoski, K, Warshawaski, RS, et al. Accuracy of physical examination using the rib–pelvis distance for detection of lumbar vertebral fractures. Am J Med. 2003; 115(3):233–236.
3. Braunstein, GD. Gynecomastia. N Engl J Med. 1993; 328:490–495. [A good review.].
4. Edelson, GW, Armstrong, DG, Lavery, LA, Ciacco, G. The acutely infected diabetic foot is not adequately evaluated in an inpatient setting. Arch Intern Med. 1996; 156:2372–2378. [All patients evaluated had undergone a less than adequate foot examination. Of admitted patients, 31% did not have their pedal pulses documented and 60% were not evaluated for the presence or absence of protective sensation.].
aThis disease was called diabetes by ancient Greek and Roman physicians because the word diabetes means a siphon, referring to the large urine volume. Rather courageously, they distinguished diabetes mellitus from diabetes insipidus by the sweet taste of the urine: mellitus, ‘sweet, honeyed’; insipidus, ‘tasteless’.
bDouglas Argyll Robertson (1837–1909), a Scottish ophthalmic surgeon and President of the Royal College of Surgeons, described these in 1869. The pupils are small, irregular and unequal, and react briskly to accommodation but not to light. Tertiary syphilis is another cause.
cSir James Paget (1814–99), a surgeon at St Bartholomew’s Hospital, London, was also Queen Victoria’s doctor.