The skin, nails and lumps



Figure 40.8 Zosteriform rash of the left buttock (Courtesy of Dr A Watson, Infectious Diseases Department, The Canberra Hospital)

Figure 40.17 Stevens-Johnson syndrome (Courtesy of Dr A Watson, Infectious Diseases Department, The Canberra Hospital)
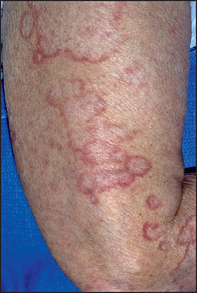
Figure 40.22 Granuloma annulare (James W. Andrews’ diseases of the skin: clinical dermatology, 11th edn. Saunders, 2011.)

Figure 40.33 Metastatic melanoma (O’Neill JK et al. Melanoma with an unknown primary: a case series. Journal of Plastic, Reconstructive & Aesthetic Surgery 2010; 63(12):2071–2080.)
Examination anatomy
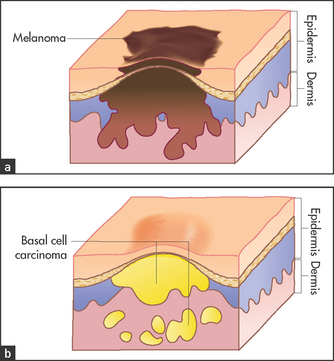
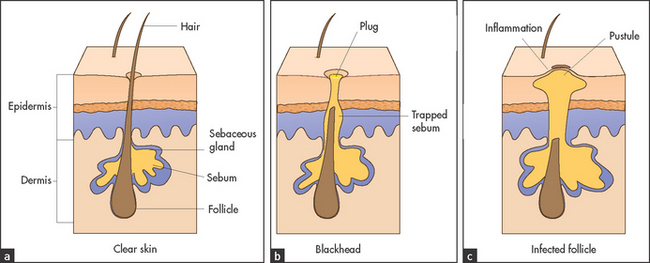
Figure 40.1 shows the three main layers of the skin: the epidermis, dermis and subcutaneous fat. These layers can all be involved in skin diseases in varying combinations. For example, most skin tumours arise in the epidermis (see Figure 40.2), some bullous eruptions occur at the epidermo-dermal junction, and lipomas are tumours of subcutaneous fat. The skin appendages, which include the sweat (eccrine and apocrine) glands, hair follicles (see Figure 40.3) and the nails, are common sites of infection.
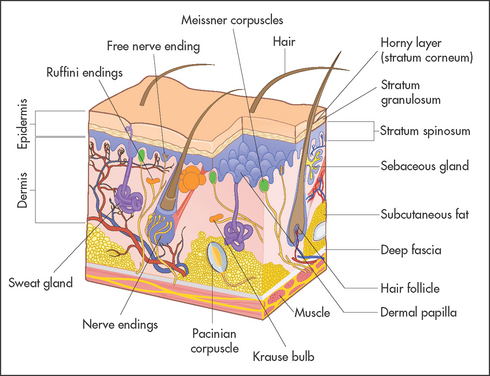
The eccrine glands are present everywhere except in the nail beds and on some mucosal surfaces. They are able to secrete over 5 litres of sweat per day. The apocrine glands are found in association with hair follicles but are confined to certain areas of the body, including the axillae, the pubis, the perineum and the nipples. They secrete a viscous fluid whose function is unclear in humans.
The nails are formed from heavily keratinised cells that grow from the nail matrix. The matrix grows in a semilunar shape and appears as the lunules in normal finger and toe nails. Hair is also the product of specialised epithelial cells and grows from the hair matrix within the hair follicle.
Dermatological history
For any patient with a rash or skin condition, it is important to determine when and where it began, its distribution, whether it has changed over time, its relationship to sun exposure or heat or cold, and any response to treatment1 (see Questions box 40.1). Ask if pruritus is associated; localised pruritus is usually due to dermatological disease. Determine whether pain or disturbed sensation has occurred; for example, inflammation and oedema can produce pain in the skin, while disease involving neurovascular bundles or nerves can produce anaesthesia (e.g. leprosy, syphilis). Constitutional symptoms such as fever, headache, fatigue, anorexia and weight loss also need to be documented.
Ask about a past history of rashes or allergic reactions. Asthma, eczema or hay fever suggests atopy. Similarly, evidence of systemic disease in the past may be important in a patient with a rash (e.g. diabetes mellitus, connective tissue disease, inflammatory bowel disease).a
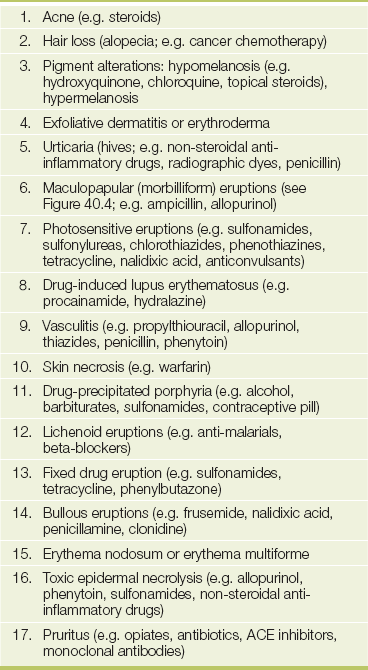
A detailed social history needs to be obtained regarding occupation and hobbies, as chemical exposure and contact with animals or plants can all induce dermatitis. All medications that have been taken must be documented. Orally ingested or parenteral medications can cause a whole host of cutaneous lesions and can mimic many skin diseases (see Table 40.1). Similarly, a family history of atopic dermatitis, hay fever or skin infestation can be helpful.
General principles of physical examination of the skin
The aim of this chapter is to provide an approach to the diagnosis of skin diseases.2,3 Particular emphasis will be placed on cutaneous signs as indications of systemic disease. Other chapters have included the usual clues that can be used to arrive at a particular diagnosis. This chapter tries to unify the concept of ‘inspection’ as a valuable starting point in the examination of the patient.
Ask the patient to undress. The whole surface of the skin and its appendages should be carefully inspected (see List 40.1).
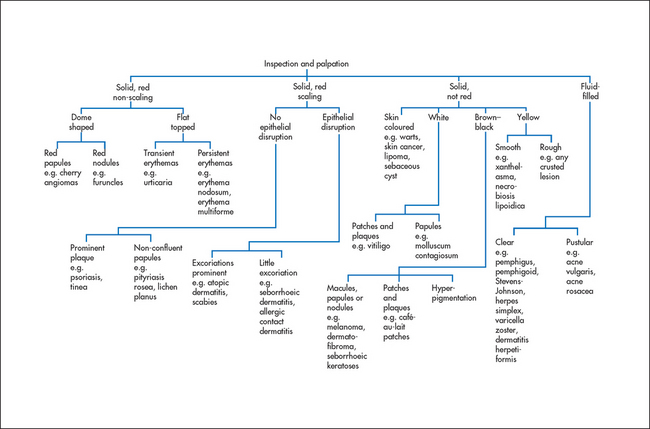
When examining actual skin lesions, a number of features should be documented. First, each lesion should be described precisely, including colour and shape. Use the appropriate dermatological terminology (see Table 40.2), even though this may seem to make dermatological diseases more, rather than less, mysterious. As many dermatological diagnoses are purely descriptive, a good description will often be of considerable help in making the diagnosis. Second, the distribution of the lesions should be noted, as certain distributions suggest specific diagnoses. Third, the pattern of the lesions—such as linear, annular (ring-shaped), reticulated (net-like), serpiginous (snake-like) or grouped—also helps establish the diagnosis. Then palpate the lesions, noting consistency, tenderness, temperature, depth and mobility. Types of skin lesions are shown in Figure 40.5 and a clinical algorithm for diagnosis is presented in Figure 40.6.
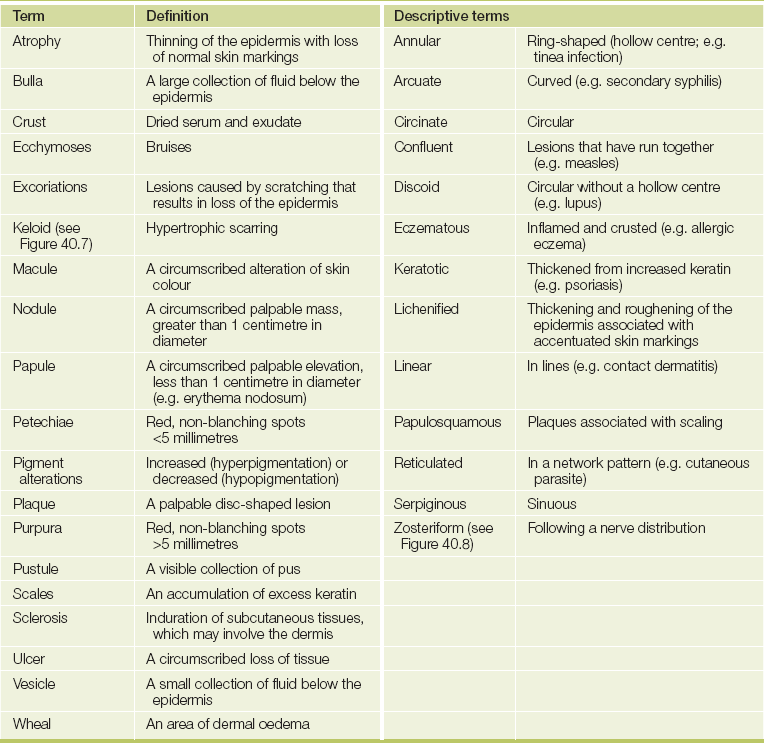
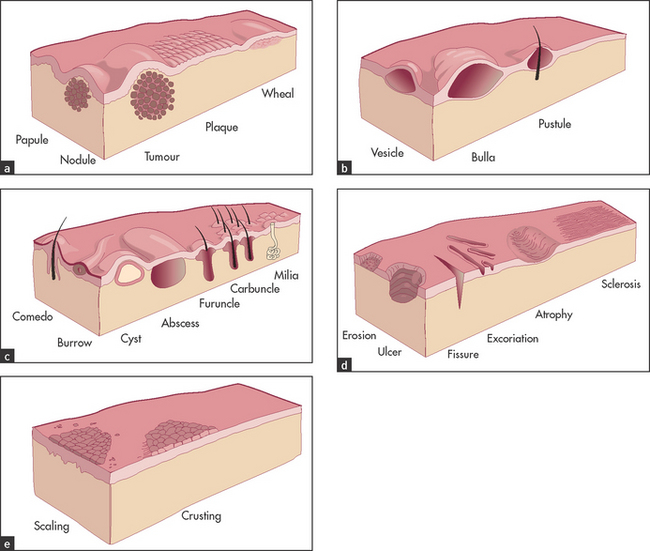
Figure 40.5 Types of skin lesions (a) Primary skin lesions, palpable with solid mass; (b) primary skin lesions, palpable and fluid-filled; (c) special primary skin lesions; (d) secondary skin lesions, below the skin plane; (e) secondary skin lesions, above the skin plane. (Adapted from Schwartz M. Textbook of physical diagnosis, 4th edn. Philadelphia: Saunders, 2002.)
How to approach the clinical diagnosis of a lump
First, determine the lump’s site, size, shape, mobility, consistency and tenderness. Next, evaluate in what tissue layer the lump is situated. If it is in the skin (e.g. sebaceous cyst, epidermoid cyst, papilloma), it should move when the skin is moved, but if it is in the subcutaneous tissue (e.g. neurofibroma, lipoma), the skin can be moved over the lump. If it is in the muscle or tendon (e.g. tumour), then contraction of the muscle or tendon will limit the lump’s mobility. If it is in a nerve, pressing on the lump may result in pins and needles being felt in the distribution of the nerve, and the lump cannot be moved in the longitudinal axis but can be moved in the transverse axis. If it is in bone, the lump will be immobile.
Determine whether the lump is fluctuant (i.e. contains fluid). Place one forefinger (the ‘watching’ finger) halfway between the centre and the periphery of the lump. Place the forefinger from your other hand (the ‘displacing’ finger) diagonally opposite the watching finger at an equal distance from the centre of the lump. Press with the displacing finger and keep the watching finger still. If the lump contains fluid, the watching finger will be displaced in both axes of the lump (i.e. fluctuation is present).
Place a small torch behind the lump to determine whether it can be transilluminated. Light will be transmitted through a cystic lump, which will appear to glow when transilluminated.
Note any associated signs of inflammation (i.e. heat, redness, tenderness and swellingb).
Look for similar lumps elsewhere, such as multiple subcutaneous swellings from neurofibromas or lipomas. Neurofibromas are smaller than lipomas. They look hard but are remarkably soft; they occur in neurofibromatosis type 1 (von Recklinghausen’sc disease). They continue to increase in number throughout life and are associated with café-au-lait spots and sometimes spinal neurofibromas.
If an inflammatory or a neoplastic lump is suspected, remember always to examine the regional lymphatic field and the other lymph node groups.
Correlation of physical signs and skin disease
There are many different skin diseases with varied physical signs (see Figure 40.6). With each major sign the groups of common important diseases that should be considered will be listed.
PRURITUS
Pruritus simply means itching. It may be either generalised or localised. Scratch marks are generally present. Localised pruritus is usually caused by a dermatological condition such as dermatitis or eczema. Generalised pruritus may be caused by primary skin disease, systemic disease or psychogenic factors.
To determine the cause of the pruritus it is essential to examine the skin in detail (see List 40.2). Excoriations are caused by scratching, regardless of the underlying cause. Specific features of cutaneous diseases such as dermatitis, scabies (see Figure 40.9) or the blisters of dermatitis herpetiformis should be looked for.

Figure 40.9 Scabies Scattered fine papules with severe itching. Finger web involvement is common. (Reeves JT, Maibach H. Clinical dermatology illustrated: a regional approach, 3rd edn. Sydney: McLennan & Petty, 2000.) McLennan & Petty
When primary skin diseases have been excluded, a detailed history and examination should be undertaken to consider the various systemic diseases outlined in List 40.3.
ERYTHROSQUAMOUS ERUPTIONS
Erythrosquamous eruptions are made up of lesions that are red and scaly. They may be well demarcated or have diffuse borders. They may be itchy or asymptomatic.
When attempting to establish a diagnosis of an erythrosquamous eruption, the history is very important. Ask about the time course of the eruption, about a family history of similar skin diseases and whether or not there is a family history of atopy. The presence or absence of itching and the distribution of the lesions (often on the extensor surfaces of the limbs) also give clues about the diagnosis.
Asymptomatic lesions on the palms and soles are suggestive of secondary syphilis, whereas itchy lesions in the same location would be more suggestive of lichen planus (see Figures 40.10 and 40.11). Lichen planus is occasionally associated with primary biliary cirrhosis and other liver diseases, chronic graft-versus-host disease and drugs (e.g. penicillamine, ACE inhibitors). Scattered lesions of recent origin on the trunk would be more suggestive of pityriasis rosea (see Figure 40.12), whereas more widespread, diffuse and intensely itchy lesions would be more suggestive of nummular eczema (see Figure 40.13 and List 40.4).

Figure 40.10 Lichen planus, with polygonal flat-topped violaceous lesions. (Reeves JT, Maibach H. Clinical dermatology illustrated: a regional approach, 2nd edn. © 1991, MacLennan & Petty Pty Ltd.) MacLennan & Petty Pty Ltd.

Figure 40.11 Lichen planus, with development of lesions in an area of trauma—the ‘Koebner’ phenomenon. (Reeves JT, Maibach H. Clinical dermatology illustrated: a regional approach, 2nd edn. © 1991, MacLennan & Petty Pty Ltd.) MacLennan & Petty Pty Ltd.
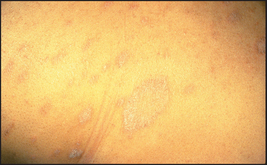
Figure 40.12 Pityriasis rosea, with scattered scaly oval lesions on the trunk and a larger ‘herald’ patch. (Reeves JT, Maibach H. Clinical dermatology illustrated: a regional approach, 2nd edn. © 1991, MacLennan & Petty Pty Ltd.) MacLennan & Petty Pty Ltd.

Figure 40.13 (a) Nummular eczema—typical scattered coin-like lesions of indolent dermatitis; (b) nummular eczema, close-up view of typical lesions; (c) nummular eczema ((a) Reeves JT, Maibach H. Clinical dermatology illustrated: a regional approach, 2nd edn. © 1991, MacLennan & Petty Pty Ltd; (b) Halberg M. Nummular eczema. The Journal of Emergency Medicine 2011; 43(5):e327–e328; (c) Courtesy of Dr A Watson, Infectious Diseases Department, The Canberra Hospital)
Scaly lesions with a well-demarcated edge over the extensor surfaces are usually due to psoriasis (see Figures 40.14 and 40.15).

Figure 40.14 (a) Psoriasis—typical bright-red, scaly plaque with silvery scale over a joint; (b) psoriasis of the scalp in the hair line ((a) Reeves JT, Maibach H. Clinical dermatology illustrated: a regional approach, 2nd edn. © 1991, MacLennan & Petty Pty Ltd; (b) Courtesy of Dr A Watson, Infectious Diseases Department, The Canberra Hospital)
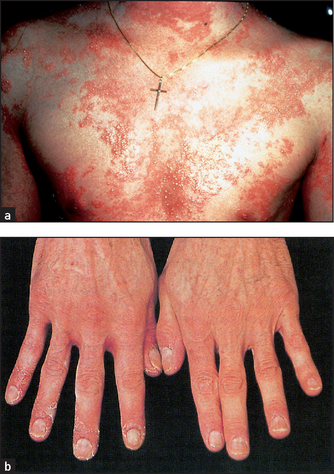
Figure 40.15 (a) Acute widespread pustular psoriasis Often the eruption is bright-red with bizarre patterns and pustules predominantly at the margins. (b) Pustular psoriasis of the hands ((a) Reeves JT, Maibach H. Clinical dermatology illustrated: a regional approach, 2nd edn. © 1991, MacLennan & Petty Pty Ltd; (b) Hochberg. Rheumatology, 5th edn. Mosby, 2010.)
BLISTERING ERUPTIONS
There are a number of different diseases that will present with either vesicles or blisters (see List 40.5). Dermatitis can present as a blistering eruption, particularly acute contact dermatitis (see Figure 40.16 and also Questions box 40.2).
Questions box 40.2
Questions to ask the patient with a blistering eruption
 denotes symptoms for the possible diagnosis of an urgent or dangerous problem.
denotes symptoms for the possible diagnosis of an urgent or dangerous problem.
1. Have you had blisters on the backs of your hands that break easily and are worse if you have been in the sun? (Porphyria cutanea tarda)
2. Have you had sores or blisters in your mouth that came on before the skin blisters? (Pemphigus vulgaris)
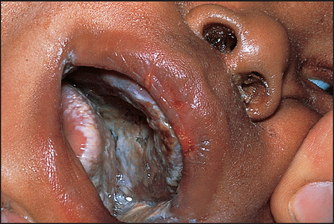
3. Did the inside of your mouth become ulcerated and painful suddenly? (Stevens-Johnson syndrome; see Figure 40.17)
4. Was the blister on your lip or genitals, and was it preceded by itching or burning? (Herpes simplex)
5. Were the blisters preceded by some days of severe pain and burning in the areas where the blisters have broken out? (Herpes zoster)
6. Did you notice pink spots on the skin that were itchy before the blisters appeared? (Bullous pemphigoid)

Figure 40.16 Allergic contact dermatitis From over-the-counter topical medication rubbed over congested sinuses. (Courtesy of Dr A Watson, Infectious Diseases Department, The Canberra Hospital)
Clinical features of bullous eruptions
Viral blisters such as those of herpes simplex virus infection (see Figure 40.18) have a distinctive morphology (grouped vesicles on an erythematous background).

Figure 40.18 Primary herpes simplex virus infection in an adult Shows typical widespread distribution around the mouth. (Reeves JT, Maibach H. Clinical dermatology illustrated: a regional approach, 2nd edn. © 1991, MacLennan & Petty Pty Ltd.) MacLennan & Petty Pty Ltd.
Bullous pemphigoid is a rare disease usually affecting older patients. Blisters are widespread, have a thick roof and tend not to rupture easily (see Figure 40.19).

Pemphigus vulgaris is much more severe (see Figure 40.20). It has thin-roofed blisters that readily rupture and form crusts. The affected superficial skin can be moved over the deeper layer (Nikolsky’sd sign). Oral ulcers are common.

Figure 40.20 Pemphigus vulgaris (Reeves JT, Maibach H. Clinical dermatology illustrated: a regional approach, 2nd edn. © 1991, MacLennan & Petty Pty Ltd.) MacLennan & Petty Pty Ltd.
Dermatitis herpetiformis is characterised by a very itchy widespread vesicular or bullous eruption.
Porphyria cutanea tarda is characterised by clear or haemorrhagic tense blisters on the hands and other sun-exposed areas, hyperpigmentation and increased facial hair; many patients have hepatitis C and alcohol can induce symptoms (due to decreased uroporphyrinogen decarboxylase).
ERYTHRODERMA
Erythroderma is best thought of as the end-stage of numerous skin conditions (see List 40.6). The erythrodermic patient has involvement of nearly all the skin with an erythematous inflammatory process, often with exfoliation. There is usually associated oedema and loss of muscle mass. This represents that most unusual occurrence, a dermatological emergency.
An attempt should be made to determine the underlying cause of the erythroderma, and this is best done based on the history and examination. Specific treatment can then be directed at the underlying cause. Some patients with erythroderma will develop profound metabolic changes (including hypoalbuminaemia and extra-renal water loss), and these patients require constant supervision and monitoring until they have recovered from the acute phase of their illness.
The most common cause is eczema, which is usually of the atopic variety. These patients often have an intense pruritus. Some of them will develop a chronic unremitting erythroderma.
PUSTULAR AND CRUSTED LESIONS
The clinical appearance of a pustular lesion results from accumulation of neutrophils. Such collections usually indicate an infective process; however, sterile pustules may form as part of a number of skin diseases due to the release of chemotactic factors following an immunological reaction.
A crust is a yellowish crystalline material that is found on the skin; it is made up of desiccated serum.
It is essential to determine whether or not a pustular lesion (or a group of pustular lesions) represents a primarily infectious process or an inflammatory dermatological condition. For example, pustular lesions on the hands and feet may either be due to tinea infection or be a primary pustular psoriasis or palmoplantar pustulosis (see List 40.7 and Questions box 40.3).
DERMAL PLAQUES
Plaques are localised thickenings of the skin that are usually caused by changes in the dermis or subcutaneous fat. These may be due to chronic inflammatory processes or scarring sclerotic processes (see List 40.8).
The pattern of involvement of the plaques, the age of the patient and other clinical features should enable a diagnosis to be established.
Sweet’s syndrome is a condition involving painful red plaques and a high fever (acute febrile neutrophilic dermatosis); 10% have leukaemia.
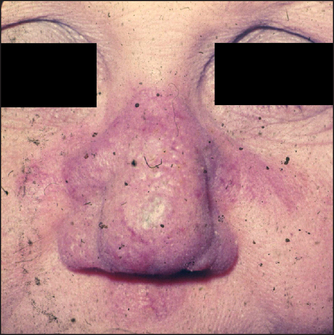
Lupus pernio (see Figure 40.21) appears as violaceous papules and plaques. It occurs in some patients with sarcoidosis.
ERYTHEMA NODOSUM
This is the best known of the group of diseases classified as nodular vasculitis. The lesions of erythema nodosum are usually found below the knee in the pretibial area and are erythematous, palpable and tender (see Figure 15.4 on page 224). There may be an associated fever (see List 40.9). The condition is common after streptococcal and viral infections, and can occur with oral contraceptive and sulfonamide use and with sarcoidosis and inflammatory bowel disease. However, the skin changes in sarcoidosis can mimic almost any skin disease (except vesicles).
ERYTHEMA MULTIFORME
This is a distinctive inflammatory reaction of skin and mucosa. It is not a systemic disease. Characteristic discrete target lesions occur, particularly on the distal extremities (see Figure 40.23). The periphery of these lesions is red, whereas the centre becomes bluish or even purpuric. The lesions can become bullous, and severe cases of this syndrome involve widespread desquamation of the mucosal surfaces (the Stevens-Johnsone syndrome). In many cases the condition is precipitated by clinical or subclinical herpes simplex virus infection. Other causes include Mycoplasma pneumoniae, histoplasmosis, malignancy, sarcoidosis and drugs (including those that can cause toxic epidermal necrolysis). Sometimes no underlying cause will be established.

Figure 40.23 Erythema multiforme Shows classic iris or target lesions, secondary to herpes simplex virus infection of the lips. (Reeves JT, Maibach H. Clinical dermatology illustrated: a regional approach, 2nd edn. © 1991, MacLennan & Petty Pty Ltd.)
Toxic epidermal necrolysis, on the other hand, is a systemic condition and usually secondary to a drug reaction. It results in a peeling of large skin areas. The major causes include penicillin, sulfonamides, phenytoin and non-steroidal anti-inflammatory drugs.
CELLULITIS AND ERYSIPELAS
Cellulitis (see Figure 40.24) is inflammation of the subcutaneous tissues. It is usually due to bacterial infection and occurs mostly in the legs. Erysipelas is a more superficial infection involving the lower dermis and subcutaneous tissue (see Figure 40.25). It can occur on the face or the legs. The two can be difficult to differentiate but erysipelas has a characteristic raised edge as a result of dermal involvement. Both are most often a result of beta-haemolytic streptococcus. There may be associated fever and malaise. There may also be an obvious entry point for the organism, such as tinea pedis, a varicose ulcer or a predisposing condition such as diabetes.


FOLLICULITIS, FURUNCLES AND CARBUNCLES
These conditions are all infections of hair follicles of varying severity.
Folliculitis is a superficial inflammation of a hair follicle. Many cases are due to staphylococcal infection but they can be caused by injury or chemicals. The condition is common and usually resolves spontaneously after a week or so. If the infection becomes deeper, it becomes a furuncle (or boil) and if it spreads to involve a number of adjacent hair follicles it becomes a carbuncle. These can be up to 10 centimetres in size. They can occur anywhere on the skin but are common on the buttocks, neck and anogenital area. They are very painful and often associated with systemic symptoms. Staphylococcal organisms are usually responsible. These deep lesions heal by rupturing and exuding pus. They often leave a scar. Draining lymph nodes may be enlarged and tender.
The condition hidradenitis suppurativa, which especially affects obese young women, is associated with furunculosis. The condition involves the apocrine glands in the axillae, the groin and the submammary areas.
Intertrigo is an infection in skin folds where moist skin rubs together. Candida albicans infection is often present (see Figure 40.26). Chronic mucocutaneous candidiasis is rare with chronic skin disease and severe thrush.
OTHER INFECTIONS
Viral infections can lead to skin reactions. Measles is an example of an infection causing a viral exanthema (see Figure 40.27). Many viruses including cytomegalovirus (CMV), Epstein-Barr virus (EBV), coxsackievirus and the conversion illness after HIV infection can cause a similar rash. Patients with EBV infection treated with amoxicillin develop a characteristic rash (see Figure 40.28). Meningococcal septicaemia causes a severe petechial rash (see Figure 40.29).

Figure 40.27 Viral exanthema (Courtesy of Dr A Watson, Infectious Diseases Department, The Canberra Hospital)

Figure 40.28 EBV infection after amoxicillin (Courtesy of Dr A Watson, Infectious Diseases Department, The Canberra Hospital)
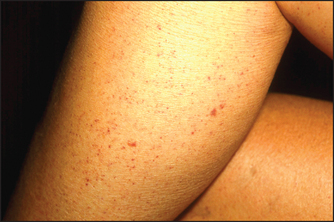
Figure 40.29 Petechial rash (Marks J, Miller J. Lookingbill & Marks’ principles of dermatology, 4th edn. Saunders, 2006.)
Nonspecific urethritis and Shigella dysentery infection may be associated with keratoderma blenorrhagica; horny scales appear on the palms and soles of the feet (see Figure 40.30). Molluscum contagiosum is an infectious viral disease of the skin characterised by discrete waxy dome-shaped nodules, often with a central umbilicum (see Figure 40.31).
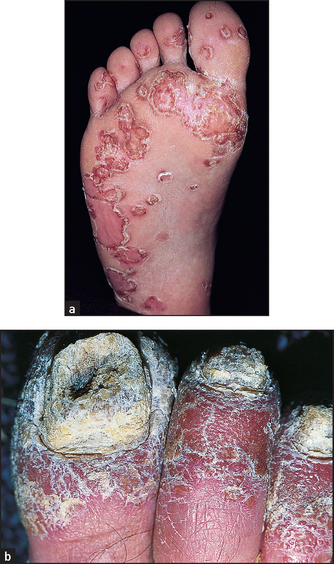
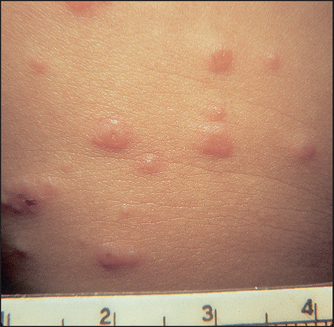
Figure 40.31 Molluscum contagiosum (Black M. Obstetric and gynaecologic dermatology, 3rd edn. Mosby, 2008.)
Fungal skin infections include tinea, which often involves the foot (tinea pedis; see Figure 40.32). It is caused by any of a number of fungal species.

HYPERPIGMENTATION
The presence of hyperpigmentation can be a clue to underlying systemic disease (see List 40.10).
FLUSHING AND SWEATING
Flushing of the skin may sometimes be observed, especially on the face, by the examiner. Some of the causes of this phenomenon are presented in List 40.11.
Excessive sweating (hyperhidrosis) can occur with thyrotoxicosis, phaeochromocytoma, acromegaly, hypoglycaemia, autonomic dysfunction, anxiety, fever and menopause.
SKIN TUMOURS
Skin tumours are very common and are usually benign (see List 40.12).4 Most malignant skin tumours can be cured if they are detected early and treated appropriately (see List 40.13).
Skin cancer often occurs in those predisposed individuals (with the fair skin of Celtic or Northern European origin) who undergo chronic exposure to ultraviolet light. Skin cancers may present as flat scaly lesions or as raised scaly or smooth lesions. They may be large or small and they may eventually ulcerate. All non-healing ulcers should be considered to be skin cancer, until proven otherwise.
The earliest lesions are actinic (solar) keratoses, which are pink macules or papules surmounted by adherent scale (see Figure 40.34). Basal cell carcinoma is characteristically a translucent papule with a depressed centre and a rolled border with ectatic capillaries (see Figure 40.35). Squamous cell carcinoma is typically an opaque papule or plaque that is often eroded or scaly (see Figure 40.36).

Figure 40.34 Actinic keratosis, slightly eroded and scaly Higher on the forehead additional granular keratosis could be easily palpated. (Reeves JT, Maibach H. Clinical dermatology illustrated: a regional approach, 2nd edn. © 1991, MacLennan & Petty Pty Ltd.)
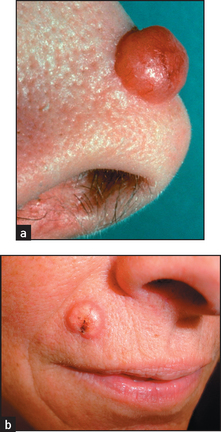
Figure 40.35 (a) Basal cell carcinoma: noted the rolled edges. (b) Pigmented basal cell carcinoma, with pearly quality and depressed centre, in a patient with sun-damaged skin. (Pfenninger J. Pfenninger and Fowler’s procedures for primary care, 3rd edn. Mosby, 2010.)

Figure 40.36 Squamous cell carcinoma (Reeves JT, Maibach H. Clinical dermatology illustrated: a regional approach, 2nd edn. © 1991, MacLennan & Petty Pty Ltd.) MacLennan & Petty Pty Ltd.
Malignant melanomas are usually deeply pigmented lesions that are enlarging and have an irregular notched border (see Figure 40.37). There is often variation of pigment within the lesion. Malignant melanoma is likely if the lesion is:
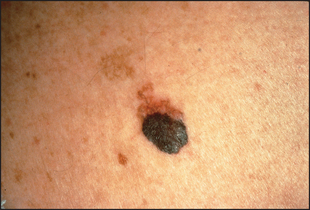
Figure 40.37 Superficial spreading melanoma, still confined to the upper dermis (© Dr Loren E Golitz)
Patients with numerous large and unusual pigmented naevi (dysplastic naevus syndrome) are at an increased risk of developing malignant melanoma.7
The nails
Systemic disease is commonly associated with changes in the patient’s finger (and toe) nails and in the nail beds. The slow growth of the nails means that the temporal course of an illness may be seen in nail changes. Many of these findings have been described in other chapters but important features of nail changes are dealt with here.
Fungal infection of the nails (onychomycosis; see Figure 40.38) is the most common nail abnormality: it makes up 40% of all nail disorders and 30% of all cutaneous fungal infections. The characteristic findings are pitting, thickening, ridging and deformity. The changes can be indistinguishable from those of psoriasis. Candidal nail infections are less common than those due to dermatophytes. Candidal nail infection (diagnosed by microscopy and culture) suggests the possibility of chronic mucocutaneous candidiasis, which is a rare condition associated with polyendocrinopathies.

Figure 40.38 Onychomycosis: fungal infection of the nails (Reeves JT, Maibach H. Clinical dermatology illustrated: a regional approach, 2nd edn. © 1991, MacLennan & Petty Pty Ltd.) MacLennan & Petty Pty Ltd.
Nail involvement occurs in about 25% of patients with psoriasis (see Figure 40.39). The characteristic abnormality is pitting. This can also occur in fungal infections, chronic paronychia, lichen planus and alopecia areata. Psoriasis is also the most common cause of onycholysis. Rarer changes in psoriatic nails include longitudinal ridging (onychorrhexis), proximal transverse ridging, subungual hyper-keratosis and yellow–brown discolouration.

Figure 40.39 Nail involvement occurs in about 25% of patients with psoriasis (Reeves JT, Maibach H. Clinical dermatology illustrated: a regional approach, 2nd edn. © 1991, MacLennan & Petty Pty Ltd.) MacLennan & Petty Pty Ltd.
The presence of nailfold telangiectasias is an important sign in a number of systemic disorders, including systemic lupus erythematosus, scleroderma and Raynaud’s phenomenon. These changes are not very specific and considerable variation in nailfold capillary shape is present in healthy people. In patients with dermatomyositis, nailfold telangiectasias are associated with hypertrophy of the cuticle and small haemorrhagic infarcts. Raynaud’s is also associated with nail changes caused by the inadequate blood supply. These include brittleness, longitudinal ridging, splitting, flattening, onycholysis, koilonychia and a redder than normal nail bed.
Clubbing is an important nail abnormality. It has been described in patients with HIV infection, and its severity seems proportional to the degree of immunosuppression. HIV infection is also associated with onychomycosis and longitudinal melonychia (dark line in the nail), secondary to treatment with zidovudine.
TEXT BOX 40-1 The dermatological examination: a suggested method
Even if the patient shows the examiner only a small single area of abnormality, proceed to examine all the skin.
After obtaining good lighting conditions and asking the patient to disrobe, begin by looking at the nails and hands. Paronychia is an infection of the skin surrounding the nails. Other changes to note include pitting (psoriasis, fungal infections) and onycholysis (e.g. thyrotoxicosis, psoriasis). Dark staining under the nail may indicate a subungual melanoma. Linear splinter haemorrhages (e.g. vasculitis) or telangiectasias (e.g. systemic lupus erythematosus) may be seen in the nail bed.
A purplish discolouration in streaks over the knuckles may indicate dermatomyositis. Also look at the backs of the hands and forearms for the characteristic blisters of porphyria, which occur on the exposed skin. Papules and scratch marks on the acks of the hands, between the fingers and around the wrists may indicate scabies. Viral warts are common on the hands.
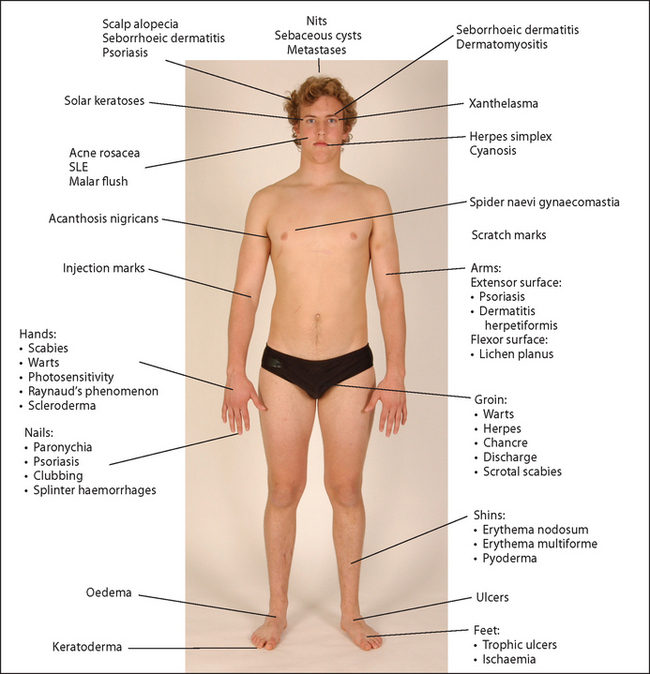
Figure 40.40 Sites of some important skin lesions of the limbs, face and trunk SLE = systemic lupus erythematosus. (Courtesy of Glenn McCulloch)
Look at the palms for Dupuytren’s contracture, pigmented flat junctional moles (which have a high risk of becoming malignant) and xanthomata in the palmar creases.
Next look at the forearms, where lichen planus may occur on the flexor surfaces (characterised by small shiny, purple-coloured papules) and psoriasis may be present on the extensor surfaces. Palpable purpura—raised bruising that indicates bleeding into the skin—may be seen on the arms and indicates vasculitis. Acanthosis nigricans can occur in the axillae.
Inspect the patient’s hair and scalp. Decide whether or not the hair is dry and whether the distribution is normal. Alopecia may indicate male pattern baldness, recent severe illness, hypothyroidism or thyrotoxicosis. Patches of alopecia occur in the disease alopecia areata. Short broken-off hairs occur typically in systemic lupus erythematosus. In psoriasis there are silvery scales, which may be seen on the skin of the scalp. Metastatic deposits may rarely be felt as firm nodules within the skin of the scalp. Sebaceous cysts are common. The unfortunate examiner may find nits sticking to the head hairs.
Move down now to the eyebrows and look for scaling and greasiness, which are found in seborrhoeic dermatitis. A purplish erythema occurs around the eyelids in dermatomyositis. Xanthelasmata are seen near the eyelid.
Look at the face for rosacea, which causes bright erythema of the nose, cheeks, forehead and chin, and occasionally pustules and rhinophyma (disfiguring swelling of the nose). Acne causes papules, pustules and scars involving the face, neck and upper trunk. The butterfly rash of systemic lupus erythematosus occurs across the cheeks but is rare. Spider naevi may be present. Ulcerating lesions on the face may include basal cell carcinoma, squamous cell carcinoma or, rarely, tuberculosis (lupus vulgaris).
Benign tumours of the face include keratoa-canthoma (a volcano-like lesion from a sebaceous gland) and congenital haemangiomas.
Look for the blisters of herpes zoster, which may occur strictly in the distribution of one of the divisions of the trigeminal nerve.
Inspect the neck, which is prone to many of the lesions that occur on the face. Rarely, the redundant loose skin of pseudoxanthoma elasticum will be seen around the neck.
Go on to inspect the trunk, where any of the childhood exanthems produce their characteristic rashes. Look for spider naevi. Campbell de Morgan spots are commonly found on the abdomen (and chest), as are flat, greasy, yellow-coloured seborrhoeic warts. Erythema marginatum (rheumatic fever) occurs on the chest and abdomen. Herpes zoster may be seen overlying any of the dermatome distributions.
Metastases from internal malignancies may rarely occur anywhere on the skin. Neurofibromas are soft flesh-coloured tumours; when associated with more than five ‘café-au-lait’ spots (brownish, irregular lesions) they suggest neurofibromatosis (von Recklinghausen’s disease). Pigmented moles are seen on the trunk and evidence of malignancy must be looked for with these. The patient’s buttocks and sacrum must be examined for bedsores, and the abdomen and thighs may have areas of fat atrophy or hypertrophy from insulin injections.
Go to the legs, where erythema nodosum or erythema multiforme may be seen on the shins. Necrobiosis lipoidica diabeticorum affects the skin over the tibia in diabetics. Pretibial myxoedema also occurs over the shins. Look for ulcers on either side of the lower part of the leg. Livedo reticularis is a net-like, red reticular rash that occurs in vasculitis, the anti-phospholipid syndrome and with atheroembolism.
Inspect the feet for the characteristic lesion of Reiter’s disease called keratoderma blennorrhagica, where crusted lesions spread across the sole because of the fusion of vesicles and pustules. Look at the foot for signs of ischaemia, associated with wasting of the skin and skin appendages. Trophic ulcers may be seen in patients with peripheral neuropathy (e.g. diabetes mellitus). Always separate the toes to look for melanomas.
References
1. Marks, R. Diagnosis in dermatology. Tricks of the trade. Aus Fam Physician. 2001; 30(11):1028–1032. [A useful guide on clinical clues.].
2. Ashton, RE. Teaching non-dermatologists to examine the skin: a review of the literature and some recommendations. Brit J Derm. 1995; 132:221–225. [Presents a good scheme that can be used to describe any skin lesion.].
3. Schwarzenberger, K. The essentials of the complete skin examination. Med Clin Nth Am. 1998; 82:981–999. [Guidance on a thorough examination approach.].
4. Preston, DS, Stern, RS. Nonmelanoma cancers of the skin. N Engl J Med. 1992; 327:649–662. [Provides useful information on discriminating between worrying and non-worrying lesions, and includes colour photographs.].
5. Whitehead, JD, Gichnik, JM. Does this patient have a mole or a melanoma. JAMA. 1998; 279:696–701. [The ABCD checklist (asymmetry, border irregularity, irregular colour, diameter >6 millimetres) has a sensitivity over 90% and a specificity over 95% for identifying malignant melanoma.].
6. Abbasi, NR, Shaw, HM, Rigel, DS, et al. Early diagnosis of cutaneous melanoma: rewriting the ABC criteria. JAMA. 2004; 292:2771–2776. [Changes (evolving) of symptoms or signs (size, shape, pruritus, tenderness, bleeding or colour) are additional evidence for the presence of melanoma.].
7. Shenenberger, DW. Cutaneous malignant melanoma: a primary care perspective. Am Fam Physician. 2012; 85(2):161–168. [An update on the clinical approach and management.].
aWhen a dermatologist cannot decide the cause of a rash this question can help. If the patient says that he or she has had the rash before, the clinician can then say with confidence ‘Well, you’ve got it again.’
bThese four cardinal signs were described by Celsus in the 8th volume of his medical book which taught those who were interested surgical techniques. After performing surgery readers were warned to look out for the four cardinal signs of post-surgical inflammation—‘calor, rubor, dolor and tumor’. Modern surgeons have added loss of function to these signs.
cFrederich von Recklinghausen (1833–1910). He was Virchow’s assistant in Berlin and then professor of pathology in Strasbourg from 1872. He described this disease in 1882 and haemochromatosis in 1889.
dPyotr Vasilyevich Nikolsky (1855–1940), Kiev and Warsaw dermatologist. Nikolsky’s sign also occurs in staphylococcal scalded skin syndrome and toxic epidermal necrolysis.
eAlbert Mason Stevens (1884–1945), New York paediatrician, and Frank C Johnson (1894–1934), American physician.