Assessment of the geriatric patient
There is lack of universal agreement on what constitutes the age cut-off that defines a geriatric patient. Only 140 years ago, old age was set above 50. Today in the Western world as people (and their doctors) age the cut-off may be extended above 65a (what highly competent older doctor in practice would want to be classified as geriatric?). Arbitrary distinctions currently drawn between the young old (65–74), the middle old (75–84) and the oldest old (85+) do not necessarily reflect biological age. The number of oldest old is growing steadily: this change will increasingly challenge health systems and has major resource implications for the future.
Geriatric patients tend to report fewer symptoms but have more diseases that are chronic. Hence, disease presentation is more likely to be atypical, so spending time taking the history is critical. Emphasis must be placed on the big four issues in older people:
You need to determine falls risk, mobility, coping and safety among other issues (see List 42.1 and Question box 42.1). Functional impairment and dementia are very important health issues to identify in older patients. Hearing and visual impairment, as well as cognitive decline, can impair history taking (see List 42.2).
History taking in geriatric patients: special considerations
1. Presenting complaint: only one complaint is unusual!
2. Past history: record the patient’s immunisation status, especially for pneumococcus, influenza and tetanus.
3. Medications: many patients will be taking multiple medications for several diseases, not all of which they may really need (polypharmacy). A comprehensive list including reason for use is important in terms of planning management. Any new symptoms may be from polypharmacy.
• Accommodation: find out whether the patient lives in a house or flat or in some form of assisted or serviced accommodation and who else lives there. Ask about the health and mobility of other people in the house and the proximity of younger relatives and friends.
• Exercise: exercise is safe in the elderly, in general, and improves flexibility, balance, endurance and strength, which can assist with maintenance of independent function as well as improving quality of life. It reduces the risk of falls.
• Smoking: the details should be acquired as usual. Stopping smoking improves lung function even in people over the age of 60. Furthermore, advice to stop smoking is as successful in older patients as in younger ones.
• Alcohol use: alcohol intake is not uncommon and should always be recorded in the notes.
• Abuse and neglect: these can be problems in this age group. Careful questioning, often over a number of interviews, may help uncover such problems.
5. Review of systems: concentrate especially on vision, hearing, chewing and dentition, weight changes, faecal and urinary incontinence, recurrent falls (see List 42.3), a history of fractures and foot disease.
Falls are an important cause of mortality in the elderly and are usually multifactorial: postural dizziness, poor vision, cognitive impairment, foot problems, impaired bone mineral density and gait problems can all contribute to or exacerbate the problem. A patient is more likely to have further falls if he or she has a history of three or more falls, or if during the past year a fall resulted in injury or if he or she currently has arthritis or Parkinson’s disease.2
Ask about the layout of the patient’s house, including the number of steps and the presence of railings, for example, in the bathroom.
Ask about depression, because this is a common problem in the elderly and needs to be recognised and treated.
• Instrumental activities of daily living (IADLs): ask about using the telephone, shopping, preparing food, housekeeping, doing the laundry, driving and taking medicine.
• Physical activities of daily living (ADLs): ask about bathing, dressing, toileting and handling money; these can be affected by many different chronic illnesses.
• End-of-life and treatment decisions: patients generally prefer this topic to be brought up actively by their doctor. It is worth encouraging the patient to place his or her preferences in writing about decisions such as ‘do not resuscitate’ orders and advance care planning.
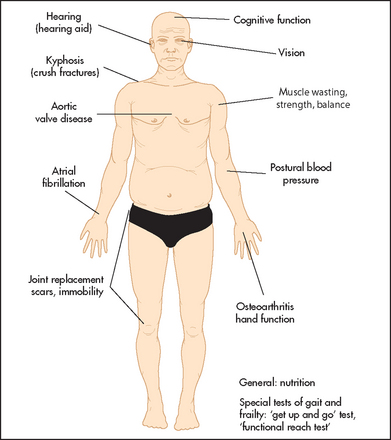
Physical examination in geriatric patients: special considerations
A complete examination is required as usual, but think about the following areas as you go about obtaining the data.
1. General assessment: check for postural blood pressure changes.
Assess hydration, which may be impaired in older patients with cognitive dysfunction.
Look at the patient’s skin carefully for pressure sores or evidence of bruises from falls or elder abuse. Look at the skin for any evidence of skin cancer.
Measure the patient’s weight and height to calculate the body mass index, as weight loss is common in the elderly.
2. Heart: if a systolic murmur is heard, consider whether this may be aortic stenosis which, if severe, is likely to require evaluation.
Ankle swelling may indicate venous insufficiency or antihypertensive drug use (e.g. calcium antagonists) rather than congestive cardiac failure. Ischaemic heart disease is common but often silent in the elderly.
3. Chest: shortness of breath may be due to lung or cardiac disease, and these often coexist in the elderly.
4. Gastrointestinal system: look at the dentition and look for dry mouth, which may impair eating. Note signs of recent weight loss.
A mass may be felt in the left lower quadrant in patients with constipation from hard stool; this will clear with treatment of the constipation.
The aorta may be palpable in the thin elderly patient. This may be falsely interpreted as an aneurysm, but if the aorta seems significantly enlarged, an aortic aneurysm needs to be excluded. If the aneurysm is leaking, the classical presentation includes back pain, abdominal distension, shock and poor asymmetrical peripheral pulses in the legs.
Perform a rectal examination and rule out faecal impaction, particularly if there is a history of faecal or urinary incontinence.
An enlarged bladder may be felt in patients with acute urinary retention; this problem can present with delirium.
5. Nervous system: evaluation of mental status and cognitive function should be routine in geriatric patients. The mini-mental state assessment is useful here. If a patient is confused it is important to distinguish cognitive decline (dementia) from an acute confusional state (delirium; Tables 37.5 and 37.6 on page 503).
Primitive reflexes such as the glabellar tap, palmar mental reflex and grasp reflex are found in those of increasing age and may be evidence of dementia.
Carefully assess gait (which may include gait speed over 8 metres with a stopwatch: normal gait speed in healthy elderly people ranges from 1.1 to 1.5 metres/second) and balance.2
Further test gait with the ‘get up and go’ test (see Figure 42.1): ask the patient to stand up out of a chair, walk 3 metres, turn around 180°, return to the chair and sit down. Assess the following:
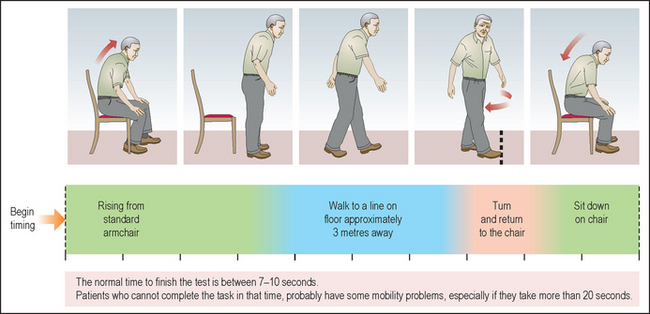
Figure 42.1 ‘Get up and go’ test 1. ‘Stand up now for me and walk over to here.’ 2. ‘Now turn around and walk back.’ 3. ‘Now come and sit down again.’ Difficulty standing up from a chair indicates an increased falls risk.1 (Elder A, MacDonald E. Macleod’s clinical examination, 13th edn. Copyright © 2013 Elsevier Ltd All rights reserved.)
• Patient in the chair: Does the patient have trouble getting out of a chair with or without arms?
• Patient standing near the chair: Is the patient unsteady?
• Patient walking: Is the gait abnormal? Unsteady, Parkinsonian, hemiplegic, needs stick, frame etc?
Look for abnormalities in gait, balance and power. The test can be graded from 1 (normal) to 5 (severely impaired) but is usually timed (fixing the walking distance), comparing the time taken to age-adjusted normal values (however, these times appear to have limited diagnostic value).3 Look carefully for lower leg weakness and test power if needed.4,5
Test frailty for falls risk using the ‘functional reach’ test. Ask the patient to stand with his or her fist extended alongside a wall, then lean forwards as far as possible. The patient should be able to move the fist along the wall without taking a step or losing stability. Measure the length of movement. A distance of less than 15 centimetres suggests an increased falls risk.6
6. Eyes and ears: check the patient’s vision and hearing as these may impair independent living. Does the patient have a hearing aid in place? Does the patient have cataracts that are interfering with vision?
7. Rheumatological system: examine for deformities and functional disabilities, including the feet.
8. Breasts: perform a breast examination in women, as the incidence of breast cancer greatly increases with age.
References
1. Whooley, MA, Avins, AL, Miranda, J, Browner, WS. Case-finding instruments for depression: two questions are as good as many. J Gen Intern Med. 1997; 12:439–445.
2. Studenski, S, Perera, S, Patel, K, et al. Gait speed and survival in older adults. JAMA. 2011; 305:50–58. [Gait speed is a measure of frailty. Faster walkers have better survival.].
3. Schoene, D, Wu, SM, Mikolaizak, AS, et al. Discriminative ability and predictive validity of the timed up and go test in identifying older people who fall: systematic review and meta-analysis. J Am Geriatr Soc. 2013; 61:202–208. [‘Get up and go’ test times have only poor-to-moderate diagnostic accuracy.].
4. Nevitt, MC, Cummings, SR, Kidd, S, Black, D. Risk factors for recurrent nonsyncopal falls: a prospective study. JAMA. 1989; 261:2663–2668. [The history identifies those at higher risk of falls. Risk factors include three or more falls or a fall with injury in the previous year, arthritis, Parkinson’s disease, difficulty standing up from a chair or difficulty performing a tandem walk.].
5. Tinetti, ME. Clinical practice. Preventing falls in elderly persons. N Engl J Med. 2003; 348:42–49. [Practical management advice.].
6. Fleming, KC, Evans, JM, Weber, DC, Chutka, DS. Practical functional assessment of elderly persons: a primary-care approach. Mayo Clin Proc. 1995; 70:890–910. [Useful screening test advice is given. The ‘functional reach’ test is useful for predicting increased falls risk.].
aAsk any relatives who are over 65 if they think that they are old: 70 is the new 50!