The psychiatric history and mental health examination
This chapter deals with the psychiatric history and the mental state examination. The practising clinician must have an understanding of psychiatric illness and know how to perform a psychiatric interview and a mental state examination. This is because there is considerable overlap between psychiatric and physical illness.
Psychiatric disorders (especially anxiety and depression) are common, and people suffering from these conditions often have medical problems. Appropriate management of these patients requires an understanding of the intercurrent psychiatric disorder and the effect of that disorder on the primary medical problem. A medical illness may, in some instances, present as a psychiatric illness. For example, some endocrine disorders, such as myxoedema, may present with depression. On the other hand, some psychiatric disorders may present medically. Panic disorder (or acute anxiety) may be mistaken for an acute myocardial infarction. Furthermore, a patient’s psychological state may interfere with the course of a medical illness; it may lead in some cases to exaggeration of the symptoms and in others to denial of the severity of physical symptoms.
The psychiatric history generally follows the same format as the standard medical history, and the principles described in Chapters 1 and 2 apply just as much here as in any history taking.1 One should enquire about the history of the present illness, the past psychiatric and medical history, and the social and family history. However, the psychiatric history aims to elicit more detail about the patient’s illness from a broad perspective, focusing not only on symptoms but also on the patient’s social background, psychological functioning and life circumstances (a biopsychosocial approach). There is, therefore, more attention paid to the developmental, personal and social history than is normal for a standard medical history.
The method of psychiatric history taking is somewhat different from the standard medical interview. The psychiatric interview aims to be therapeutic as well as diagnostic. In the course of the interview it is hoped that the patient will be able to talk about his or her problems and their context. In doing so, patients should gain some relief from their distress by airing their problems. For this to take place, the clinician’s attitude needs to be unhurried, patient and understanding. The psychiatric history also aims to gain an understanding of how the patient’s problem arose from a biological, interpersonal, social and psychological perspective, so that the best management plan can be worked out. In this way, the psychiatric interview is similar to the general medical interview. These factors are also important in relation to any illness, especially if it is a chronic or life-threatening problem. Psychiatric and physical problems often coexist and each affects the other. A comprehensive medical interview should therefore encompass both physical and psychological concerns.
Obtaining the history
The clinician taking a psychiatric history wants the patient to tell his or her story in his or her own words. In this way the patient will be more likely to report the most important aspects of the illness. Of course, this technique also applies to the general medical interview. It is best achieved using a non-directive approach with open-ended questions. Open-ended questions are those to which the patient responds with a narrative (or a description about what has been happening) rather than a simple factual response. They give patients an opportunity to talk about their problems in their own words. Closed questions, on the other hand, are more likely to elicit ‘yes’ or ‘no’ responses. For example, in the assessment of a patient with depression, a closed question would be: ‘Have you been depressed?’ An open-ended question would be: ‘Tell me about how you have been feeling.’ At first glance it might appear that the open-ended question is less efficient, as it could take longer to find out about a range of symptoms. However, with a careful and judicious approach, open-ended questioning—by permitting the patient to tell the story—will enable the clinician to get a comprehensive history efficiently. This is not to say that targeted, more-closed questions must not be used—they are necessary to elicit information on certain symptoms.
It takes experience and practice to feel confident and unembarrassed when interviewing patients who have difficult psychiatric problems that may be associated with a certain stigma or where the questioning is about sexual or intimate problems. This is certainly not the place to make judgements about or appear shocked by what a patient is saying. Of course, appearing sympathetic about the patient’s difficulties is necessary here, as it is with any medical interview.
While the patient is telling his or her story, you should begin to formulate hypotheses about the problem or diagnosis. These hypotheses are tested by asking more-focused questions later in the interview, at which point a diagnostic hypothesis can be rejected or pursued further. For example, a patient may describe tiredness and lethargy, an inability to concentrate and loss of appetite. These symptoms will suggest a diagnosis of depression. Follow-up questions should focus on this possibility. You should ask questions about other symptoms of depression such as: ‘How have you been feeling in yourself?’, ‘What has your mood been like?’ and ‘How have you been sleeping?’
INTRODUCTORY QUESTIONS
The assessment of psychiatric symptoms should start with non-threatening questions. After introducing yourself, it can be useful to begin by asking about basic demographic information (age, marital status, occupation, whom the patient lives with) and then make the patient feel at ease by discussing some neutral topic. In some cases the presenting problem will be an obvious psychiatric or psychological one. For example, a patient may say, ‘I’ve come to see you because I’ve been feeling very depressed.’ However, even such an apparently definite psychiatric problem may have a medical cause, such as hypothyroidism or a recent serious medical illness. More often, the presenting problem will be a more general one, such as ‘I have no energy and feel tired all the time’. This may be due to a depressive illness or could have a medical cause such as anaemia. Remember that psychiatric and medical problems are intimately entwined. It is rare for an interview to focus purely on psychiatric problems.
HISTORY OF THE PRESENTING ILLNESS
In assessing the history of the presenting illness, you need to cover a number of areas.
The problem
Find out the nature of the patient’s problem, and the patient’s perception of his or her difficulties. This can, of course, be difficult if the patient is psychotic and does not believe a problem exists at all. In these cases a corroborative history must be taken. For example, a manic patient may consider that there is nothing wrong and that his or her behaviour is reasonable, whereas the patient’s partner is able to recognise that ordering an expensive new sports car when the family is impoverished is a problem.
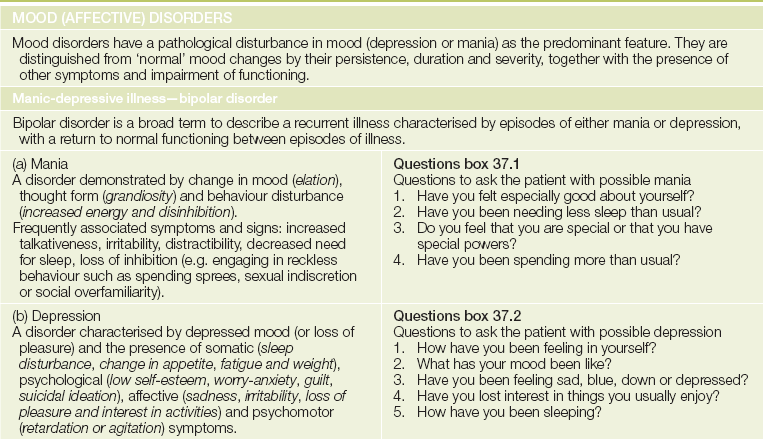
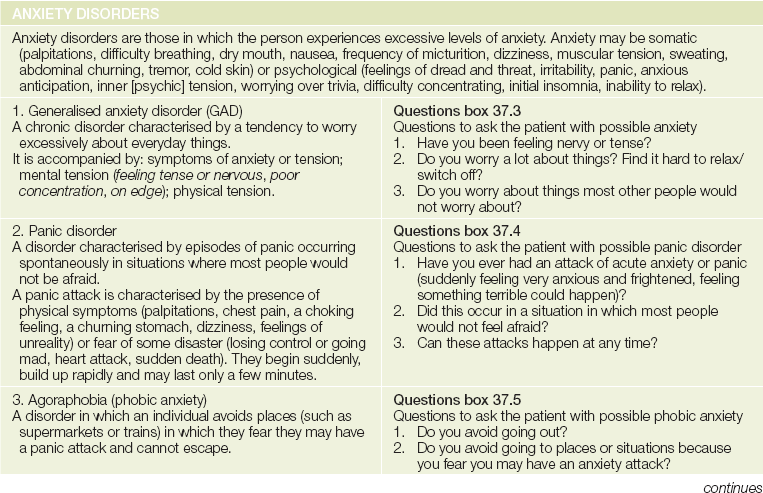
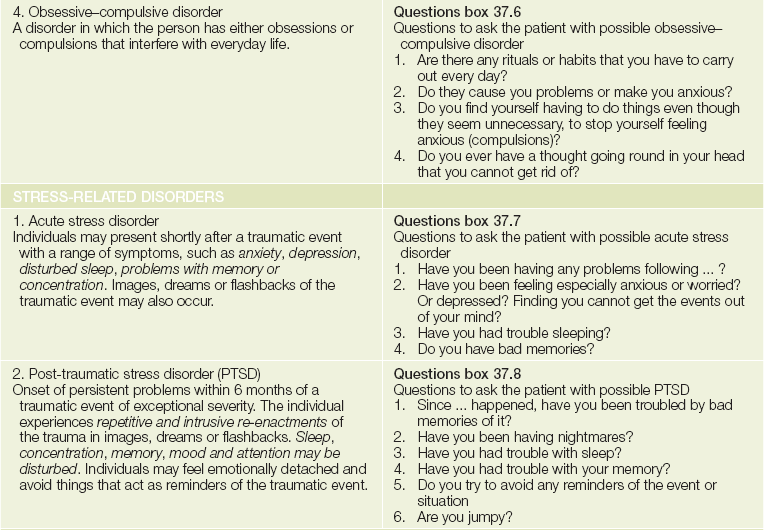
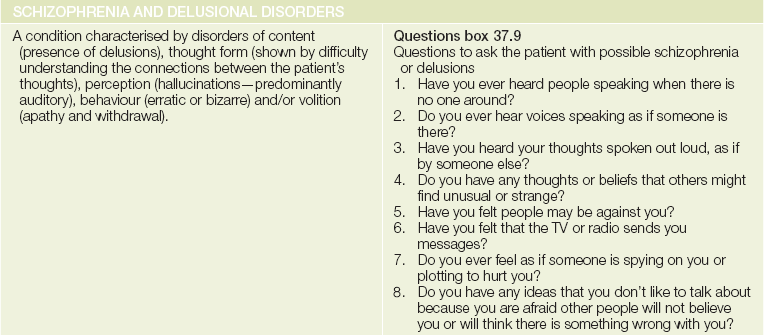
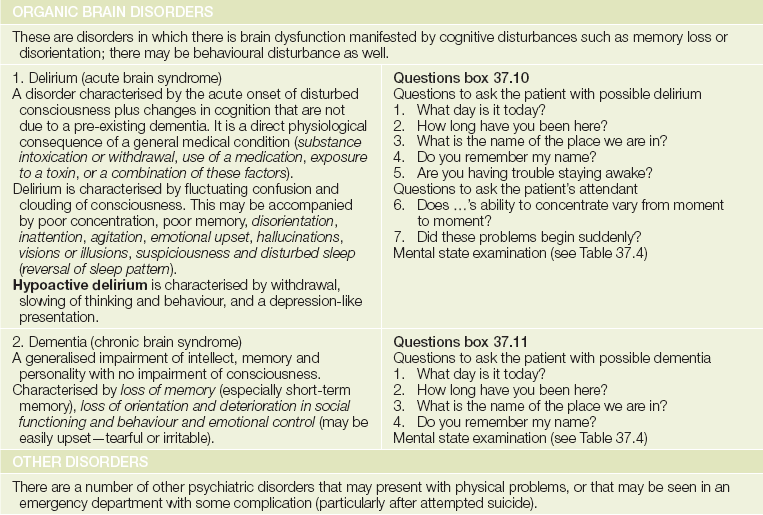
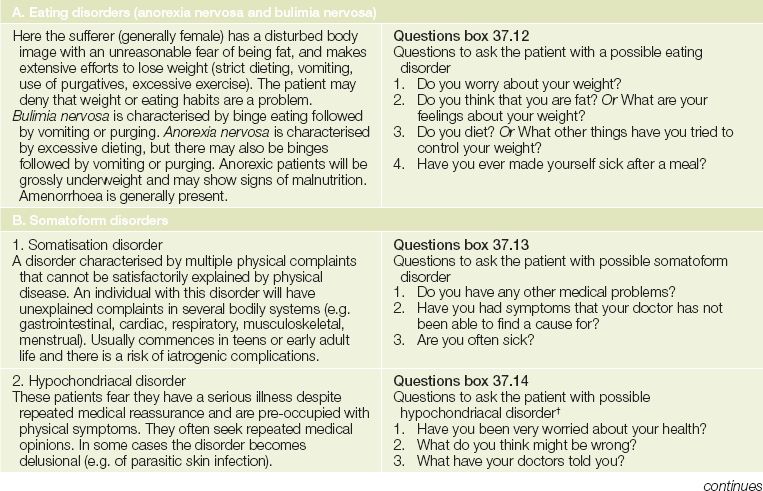
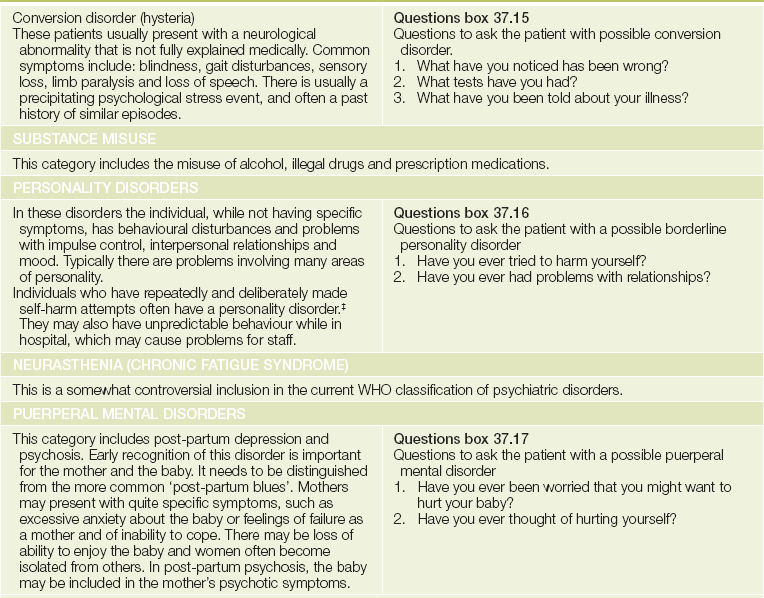
A range of symptoms commonly found in psychiatric disorders needs to be reviewed in the course of assessing the history of the present illness. These include mood change, anxiety, worry, sleep patterns, appetite, hallucinations and delusions. A set of simple screening questions for each of the major diagnoses is listed withinTable 37.1.
TABLE 37.1
The common psychiatric disorders* and their screening questions
† Alfons Jakob (1884-1931), professor of neurology in Hamburg from 1924, had more than 200 cases of neurosyphilis on his ward at a time; he died of osteomyelitis. Jakob described this cerebral atrophy in 1920 and before Hans Creutzeld (1885-1933).
‡Depression can be a cause of attempted self-harm but in this case it is not usually deliberate.
*Based on the WHO International Classification of Disease, 10th edn (ICD-10). ICD-11 will be published in 2014.
It is especially important to ask about symptoms of anxiety and depression (the most common psychiatric disorders). A simple screening approach to determine whether the patient has depression is to ask him or her:2
• In the past month, have you felt down, depressed or hopeless?
• Have you felt little interest or pleasure in doing things?
If the patient answers ‘yes’ to either question, you need to explore the possibility of depression in detail (LR+ 2.9, LR– 0.05).2 Remember, use of such screening questions in all patients (where there will be a low prevalence—i.e. a low pre-test probability of depression) will lead to many false positive responses.3
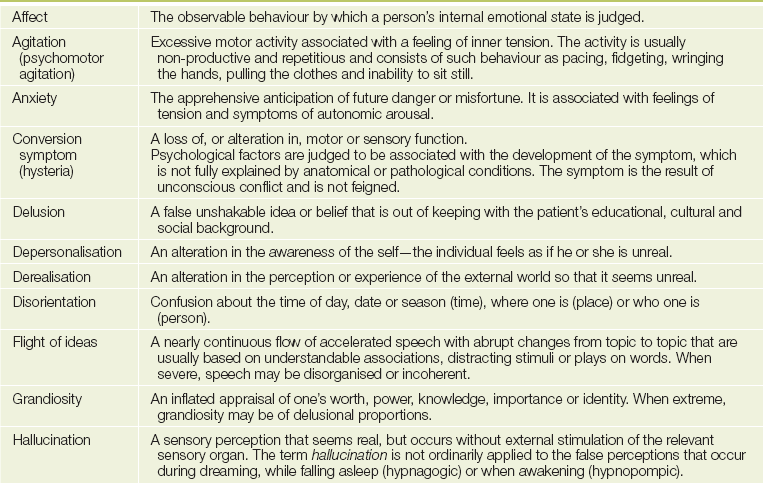
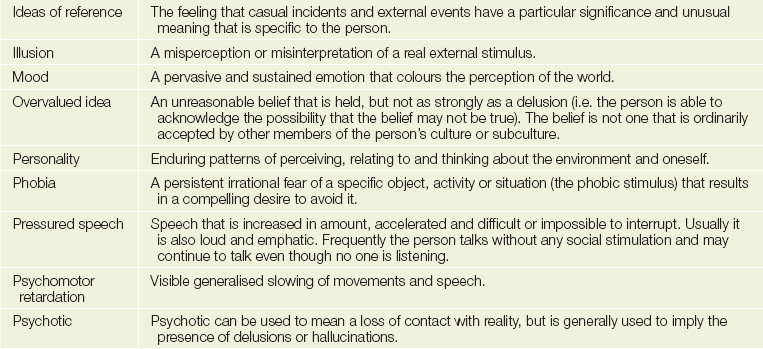
The definitions of other symptoms are given inTable 37.2. It is important to ask about drug usage (legal and illegal) as well as alcohol and caffeine intake (which may be associated with anxiety disorders).
Precipitating events
Psychiatric illness rarely occurs for no reason and there is generally an event that has precipitated the illness, even though this may not be obvious at the beginning. Such events include a range of experiences that may have affected the patient or a member of the patient’s social network. Events such as physical illness, drug treatment or treatment non-adherence may be implicated as precipitants. Patients with psychiatric illnesses have a possibly undeserved reputation for non-compliance. It may be no more common than in non-psychiatric patients but when it occurs it can be a major contribution to relapse.
Risk
An assessment of the patient’s risk of harm, either to others or to him- or herself, is essential: this will indicate whether the patient needs to be treated involuntarily. Patients with psychotic illness may, in some circumstances, need to be treated involuntarily under the relevant legislation (e.g. Mental Health Act). While the exact details for involuntary treatment are different under individual mental health laws, the essential features are generally that: (1) a person has a mental illness; and (2) the person is a danger to self or others. Assessment of danger to others is difficult, with the best predictor being a history of past threat or harm to others. It is best to err on the side of caution in such cases. Assessment of suicide risk needs to be made with sensitivity and using a direct approach, as shown in Text box 37.1.
PAST HISTORY AND TREATMENT HISTORY
Both the past psychiatric history and the medical history should be assessed. The past medical history should be evaluated in the same way as the general medical history. An assessment should be made of stresses that may have contributed to past episodes of illness and that may have led to relapse. For the past psychiatric history, it is important to obtain not only the diagnosis but also the treatment the patient has had, and its outcome.
Ask about previous non-drug treatment including counselling, psychotherapy and electroconvulsive therapy (ECT), and whether the patient thought the treatment was effective. Was the patient ever admitted to a psychiatric unit, and for how long?
Find out what drug treatment has been tried, the class (see Table 37.3) of psychiatric medication, its effectiveness and any side effects. The antipsychotic drugs in particular have common long-term side effects (see List 37.1).
TABLE 37.3
Classes of psychiatric drugs and their major indications
| Anti-anxiety (e.g. benzodiazepines, beta-blockers [control somatic symptoms]) | For anxiety disorders, insomnia, alcohol withdrawal |
| Antipsychotic (e.g. atypical antipsychotics, phenothiazines, butyrophenones, major tranquillisers) | For schizophrenia, mania, delirium |
| Antidepressants (e.g. tricyclics, selective serotonin reuptake inhibitors [SSRIs] and serotonin-noradrenaline reuptake inhibitors [SNRIs]) | For depression, anxiety disorders, obsessive-compulsive disorder |
| Mood-stabilising (e.g. lithium, anti-convulsants— carbamazepine, sodium valproate) | For prevention of manic depression or treatment of mania |
FAMILY HISTORY
There is a familial component in many psychiatric disorders. Two aspects must be assessed in the family history.
First, ask the patient tactfully if anyone in the family has had any psychiatric or mental illness or has committed suicide. Also ask if anyone in the family has had any treatment for psychological problems, such as anxiety, depression, agoraphobia,a eating disorders or drug and alcohol problems (these last few areas are often not considered by patients to be psychiatric or mental illnesses).
Second, try to determine what sort of family the patient grew up in. Drawing up a family tree is a useful way of finding this out. Factual details about each family member can be included in this family tree (age, mental state, health). In the psychiatric history one also needs to know what type of person each family member is, and how family members get on with each other. It is worth exploring how much care (or neglect) the patient received from each parent, and how controlling or protective each was. These two factors have been shown to be important in contributing to psychiatric illness. Ask about the quality of the parental relationship and the general family atmosphere.
Childhood abuse (emotional, physical or sexual)4 may be an important predisposing event for many illnesses, and should be enquired about. This can be elicited by saying something like, ‘Sometimes children can have had some unpleasant experiences—I wonder if you had any? Did anyone ever harm you? Or hit you? How about interfering with you sexually? Could you tell me more about that and what happened?’
Taking a detailed family history in this way sets the scene for the patient’s developmental history, which should be taken next.
SOCIAL AND PERSONAL HISTORY
Open-ended questions are again the best way to obtain the personal and social history. Ask the patient something like, ‘Could you tell me a bit about your background, your development, what sort of childhood you had, what are the important things you remember from your childhood?’, and then allow the patient to tell his or her own story. During the course of this narrative, the patient may require some prompting to add information about important issues such as the birth history (schizophrenia is known to be associated with perinatal morbidity) and early development, and whether there were significant problems in early childhood, such as head injuries or serious infections. How did the patient cope with early separations, particularly when starting primary school and going on to secondary school (difficulty in separation may be a risk factor for panic disorder or abnormal illness behaviour). The patient should be asked about peer relationships, friendships, school, academic ability, adolescence and teenage relationships. The adult history should focus predominantly on the quality of intimate relationships and the social support network, especially whether there are people in whom the patient can confide.
The patient’s living circumstances should be asked about in the same way as for a medical history. There should also be a focus on the patient’s occupation: not only on the type of job but also on how he or she copes with work or, if he or she does not work, how that is coped with.
Premorbid personality
An assessment should be made of the patient’s premorbid personality. Ask the patient to describe him- or herself. The personality can be described using the predominant trait, such as obsessional, nervy or highly strung; it is not necessary to use official systems to describe a patient’s personality. In the assessment of premorbid personality it is important to evaluate both positive and negative aspects of the person, how he or she copes or responds to the strains of life, what type of interests he or she has, and what other strengths and weaknesses are present.
The mental state examination
While assessing the patient, carefully make observations about appearance, behaviour, patterns of speech, attitude to the examiner and ways of interacting. These observations are brought together in a systematic fashion in the mental state examination. This is not something that is ‘done’ at the conclusion of taking a history; it is an essential part of the total process of assessing the patient.5
However, there are a number of tests that need to be conducted in a formalised way as part of the mental state examination. These include assessing the patient’s cognitive state (orientation, memory, attention, registration) and enquiring about perceptual disturbances and, in some cases, disorders of thought. The mental state examination provides valuable diagnostic information; with some disorders, it is this examination that gives most of the diagnostic clues.
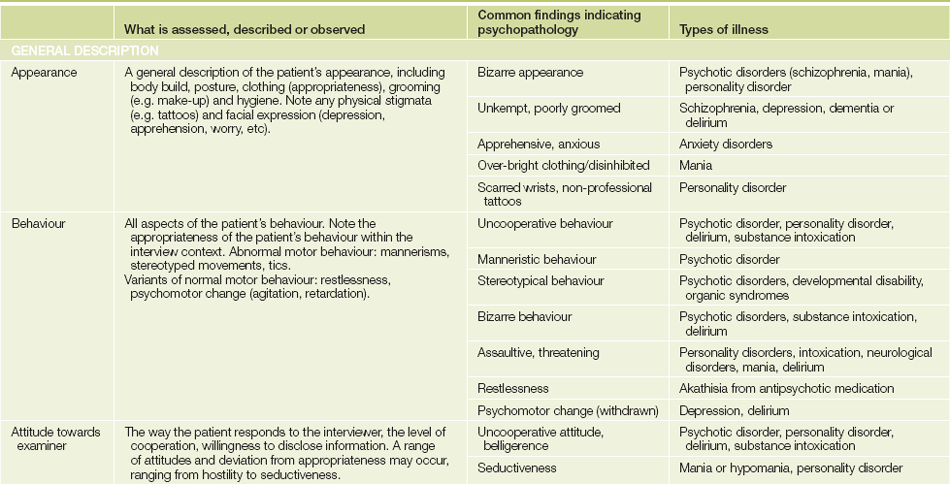
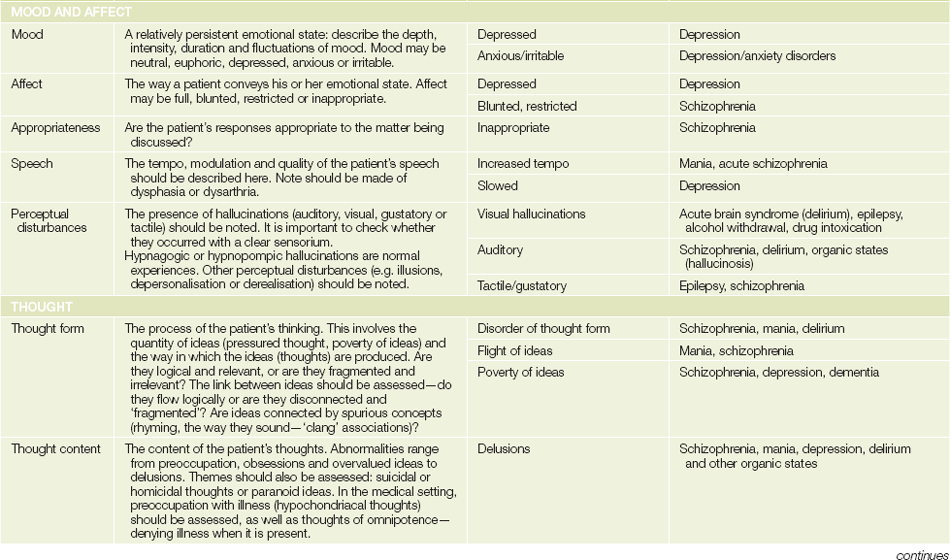
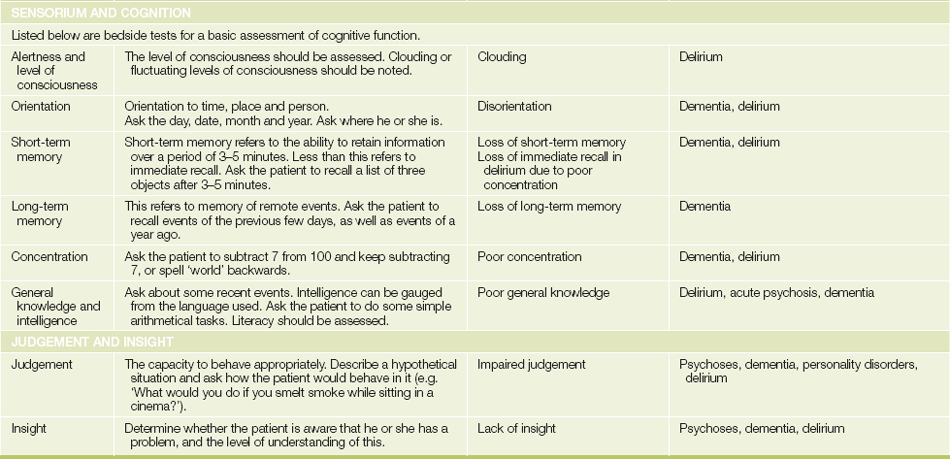
The headings under which the mental state is recorded are shown inTable 37.4, together with some simple bedside tests for assessing cognitive function. Also shown in Table 37.4 are some abnormal features of the mental state examination that are commonly found in psychiatric disorders.
When cognitive dysfunction is suspected, as in patients with dementia,6 a more detailed examination of cognitive function should be carried out. A widely used tool for doing this has been the mini-mental state examination (MMSE)™,6 which assesses aspects of orientation, memory and concentration. The MMSE is copyright protected. Another useful screening tool is the simple three-step (3-minute) Mini Cog™ test.7 For this test, ask the patient to remember three words (repeat them up to three times to make sure that he or she has captured the words correctly). Next, ask the patient to draw a clock face with numbers and then draw the hands at a specified time (e.g. 11.10). Then ask the patient to repeat the original three words. Scoring is out of 5: 1 point for each word remembered and 2 for a correct clock face drawing (0 if not fully correct). A total score of 0–2 supports a diagnosis of dementia.
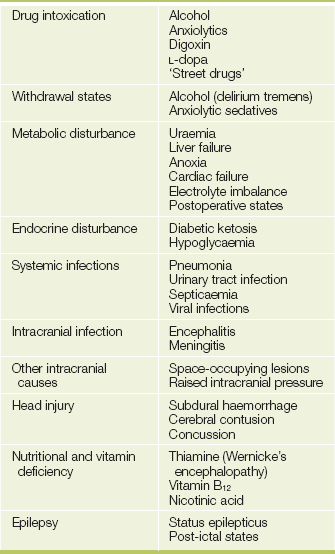
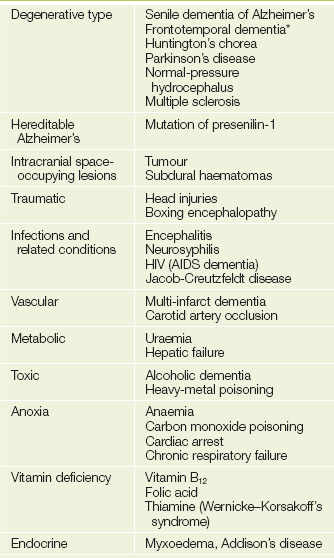
Some of the common causes of delirium and dementia are listed in Tables 37.5 and 37.6.
The diagnosis
At the conclusion of the psychiatric history, which should include a general physical examination, a provisional diagnosis and formulation should be made. Essentially, the diagnostic formulation is a means of pulling together, in a succinct yet comprehensive manner, your understanding of the patient’s problem.
Psychiatric disorders generally arise through a combination of biological, psychological and psychosocial factors, and each of these needs to be considered when a patient’s problem is being assessed (a biopsychosocial approach). The patient’s problem needs to be understood longitudinally, by defining biophysical factors that may have predisposed to the illness and, more immediately, may have precipitated the illness, and factors that may be contributing to the person remaining ill (perpetuating factors). A simple grid can be used for assessing the patient in this manner (see Table 37.7). Here biological, psychological or psychosocial factors that predispose to, precipitate or perpetuate the psychiatric illness are identified. Perpetuating factors are very important, particularly among medically ill patients, as it may be the medical or physical illness that maintains the patient’s psychiatric problem. By the same token, psychological factors may perpetuate a patient’s medical illness.

An example of such a formulation grid is shown inTable 37.8 for a 53-year-old man who becomes depressed after a myocardial infarction. He has a family history of depression (a genetic predisposing factor) and chronic low self-esteem (a psychological predisposing factor), which he coped with by succeeding in business. He has few friends and his marriage is unsatisfactory (a psychosocial factor). He had his infarct one week after he heard that he would not be promoted at work (a psychological factor) and his job was at risk (a psychosocial precipitant). His insecurity about work and his failing marriage, together with his low self-esteem, are maintaining his illness, as are the biological changes to the neurotransmitter system.

Understanding the patient in this manner helps you to plan an effective management approach that will focus on all the relevant factors, so that, for the patient in this example, a combination of antidepressants, marital counselling and assertiveness training (to build self-esteem) can be organised.
A good psychiatric history will provide a comprehensive understanding of the patient and will permit appropriate management to be planned. This is immensely rewarding for the clinician, and will also be of considerable benefit to the patient.
References
1. Kopelman, MD. Structured psychiatric interview: psychiatric history and assessment of the mental state. Br J Hosp Med. 1994; 52:93–98. [Know how to take a psychiatric history.].
2. Arroll, B, Khin, N, Kerse, N. Screening for depression in primary care with two verbally asked questions: cross sectional study. BMJ. 2003; 327:1144–1146. [Two questions help identify depression: one positive answer should be followed up.].
3. Gilbody, S, Sheldon, T, Wessely, S. Should we screen for depression. BMJ. 2006; 332:1027–1030. [Routinely screening for depression in practice is questioned because of the low pre-test probability.].
4. Drossman, DA, Talley, NJ, Lesserman, J, et al. Sexual and physical abuse and gastrointestinal illness. Ann Intern Med. 1995; 123:782–794. [An excellent clinical summary of abuse in the genesis of illness and how to screen for abuse.].
5. Johnson, J, Sims, R, Gottlieb, G. Differential diagnosis of dementia, delirium and depression. Implications for drug therapy. Drugs and Aging. 1994; 5:431–445. [The differential diagnosis hinges on a careful clinical evaluation. Dementia is defined as a chronic loss of intellectual or cognitive function of sufficient severity to interfere with social or occupational function. Delirium is an acute disturbance of consciousness marked by an attention deficit and a change in cognitive ability.].
6. Folstein, MF, Folstein, SE, McHugh, PR. Mini Mental State. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975; 12:189–198. [This is a useful instrument but is now copyright protected (see Wikipedia for details).].
7. Borson, S, Scanlan, J, Brush, M, Vitaliano, P, Dokmak, A. The Mini-Cog: a cognitive ‘vital signs’ measure for dementia screening in multi-lingual elderly. Int J Geriatr Psychiatry. 2000; 15(11):1021–1027. [A useful and quick screening test for dementia.].
aFrom the Greek, meaning ‘fear of the market place’.