Assessment of the acutely ill patient
Initial assessment
During your training, you will be expected to become expert in basic cardiac life support and advanced cardiac life support, and this training must be refreshed regularly. If you come across an obviously very ill patient, the first step is to ask, ‘Are you okay?’ If the patient is unresponsive on gentle shaking, quickly check whether the airway is patent and if he or she is breathing, then rapidly assess the circulation. This should all take no more than 10 seconds. Start cardiopulmonary resuscitation (CPR; see Figure 43.1) if the patient is not breathing (or is just gasping) or has no pulse, and try to send someone else to call for help. Current guidelines emphasise the importance of adequate chest compressions during CPR (at least 100/minute, compressing the centre of the chest 5 centimetres with each downward compression, and no interruptions—remember to push hard and fast).1
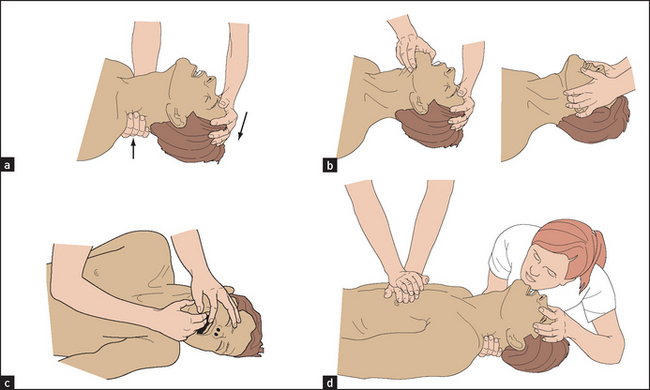
Figure 43.1 Resuscitation. (a) Head-tilt; (b) jaw thrust and jaw tilt manoeuvres to open the airway; (c) clearing the airway; and (d) cardiopulmonary resuscitation. (Baker T, Nikolic G, O’Connor S. Practical cardiology, 2nd edn. Sydney, Elsevier, 2008.)
If the patient is clearly responding appropriately to questions, and the skin is normal in colour as well as warm and dry, the patient is much less likely to need urgent intervention before appropriate history taking and a full examination are completed. If the patient’s level of consciousness becomes impaired, recheck the airway, breathing and circulation (ABCs), check the serum glucose (you must not miss hypoglycaemia) and obtain intravenous access immediately.
An acutely ill patient who presents to hospital may be able to give some history. Ask:
If possible, while beginning your physical assessment (see Figure 43.2) ask about previous medical problems such as heart disease, diabetes, asthma or depression. If the patient is accompanied by others, ask these people if they have any more information. Look for an alert bracelet and for a list of medications in the patient’s pockets.
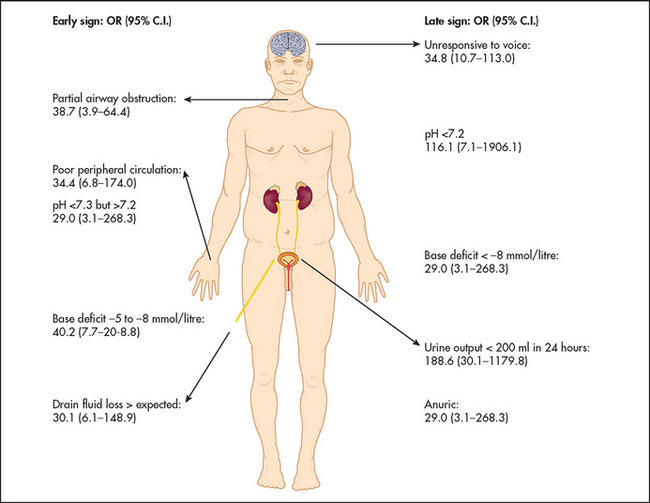
Figure 43.2 Assessment of the acutely ill patient: ‘Top five’ early and late signs of physiological deterioration with the odd (OR) for death (Robertson LC. Recognizing the critically ill patient. Anaesthesia and Intensive Care Medicine, 2013; 14(1):11–14.)
A = Airway
Obstructed? Look for injury
B = Breathing
1. Inspect chest for trauma
2. Look for chest wall movement
3. Is the patient using the accessory muscle of respiration?
4. Auscultate lungs for equal breath sounds
C = Circulation
1. Pulse: radial or femoral; rate and rhythm
2. Blood pressure
3. Perfusion: colour, temperature
D = Disability
1. Conscious state: Glasgow Coma Scale
2. Pupillary responses
3. Abnormal movements: epileptiform
4. Localising signs (e.g. hyperreflexia)
Other
1. Signs of injury
2. Medical alert bracelet
3. Medication list in pocket
Level of consciousness
Assess the patient’s level of consciousness using the AVPU system:
If the patient only responds to a painful stimulus or is unresponsive, assess him or her using the Glasgow Coma Scale (page 480).
Gather key data, as summarised by the mnemonic AMPLE:
If the patient is tachypnoeic, check pulse oximetry and start oxygen therapy unless there is a known contraindication.
If the patient is bradycardic or tachycardic, obtain an ECG.
Further examination (see List 43.1)
Check the patient’s blood pressure and other vital signs. If the patient is hypotensive, consider an intravenous fluid challenge, and organise to regularly measure the heart rate, blood pressure, respiratory rate and hourly urinary output (if necessary by inserting a urinary catheter).
Assess the capillary refill time by depressing the finger- or toenail until it blanches and recording the time it takes for the colour to become normal again, which is usually less than 2 seconds. A delayed capillary refill time occurs in hypovolaemic or cardiogenic shock.
Examine the patient’s chest for any obvious evidence of tension pneumothorax (characterised by increased breath sounds over the side of the tension pneumothorax, shift of the heart away from the tension pneumothorax, palpable subcutaneous emphysema and greatly distended next veins).
Assess the patient for possible cardiac tamponade (which can present with distended neck veins, as well as low blood pressure and pulsus paradoxus).
Examine the body for any evidence of obvious bleeding or other trauma.2
Look at the skin for a meningococcal rash (see Figure 43.3). Angio-oedema (see Figure 43.4) can occur in anaphylaxis.
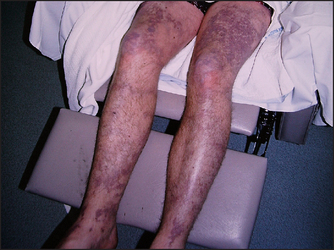
Figure 43.3 Meningococcal rash (Courtesy of Dr A Watson, Infectious Diseases Department, The Canberra Hospital)
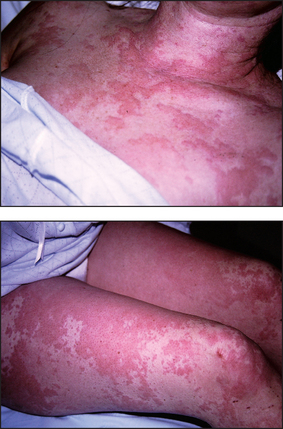
Figure 43.4 Angio-oedema (Courtesy of Dr A Watson, Infectious Diseases Department, The Canberra Hospital)
Measure the patient’s temperature. If it is elevated, consider taking blood and urine cultures.
References
1. Berg, RA, Hemphill, R, Abella, BS, et al. Part 5: adult basic life support. 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2010; 122:S685–S705. [Know how to do basic and advanced cardiac life support—and remain competent.].
2. Joshi, N, Lira, A, Mehta, N, Paladino, L, Sinert, R. Diagnostic accuracy of history, physical examination, and bedside ultrasound for diagnosis of extremity fractures in the emergency department: a systematic review. Acad Emerg Med. 2013; 20(1):1–15. [Physical examination is not sufficient to diagnose a limb fracture: an X-ray remains the gold standard.].