Chapter 4 Collaborative decision making
INTRODUCTION
One of the great debates in health care in the 21st century centres on the tension between patient-centred health care and evidence-based practice. Within this debate lies an important clinical reasoning issue, namely the patient’s role in clinical decision making. This chapter explores Franziska Trede’s doctoral research (supervised by Joy Higgs and Rodd Rothwell), which investigated explorations and experiences of emancipatory practice and collaborative decision making involving patients (or clients), relevant others (families, carers, advocates) and practitioners (Trede 2006, Trede & Higgs 2003, Trede et al 2003). (Please note that although we acknowledge the importance of the term client in many fields of health practice and health promotion, and to clients themselves, in order to probe into the need for a critical perspective – or at least its consideration and challenge – we use the term patient in most of this chapter, it being the common term used in traditional healthcare settings.)
Of particular significance in this research was the consideration of the interests of participants in the decision-making process. Healthcare practitioners participating in this study were asked to reflect on how they made decisions, what criteria they used to justify their approach to decision making and what role they assigned to, or encouraged in, their patients in the decision-making process. A critical hermeneutic approach was used to interpret interview transcripts and identify interests, assumptions, motivations and biases that the practitioners brought to their decision-making practice. In this chapter we report on a critical practice perspective on collaborative decision making.
WHY COLLABORATE IN THE DECISION-MAKING PROCESS?
Practitioners make numerous daily decisions about their patients: which questions to ask, which label or diagnosis to assign, which treatment options to discuss, which information to share or not share with patients, which treatment interventions and care plans to pursue. The way decisions are made impacts on patients’ persistence with treatment, sense of ownership, control and perceptions of healthcare outcomes. For many patients, the more they participate in decision-making processes the more likely they are to be well informed, involved, satisfied and feeling valued (Trede & Higgs 2003).
Many factors support the case for collaboration in decision making (Hall & Visser 2000), including ethical issues related to quality of life (Mueller et al 2004), legal issues regarding informed consent (Braddock et al 1997), the patient’s right to self-determination (Snapshot 2004), patient safety and the duty to prevent and do no harm (Winokur & Beauregard 2005), and cultural safety in terms of respecting and valuing diversity (Richardson & Carryer 2005). Patient dissatisfaction with communication aspects of health care has been shown to contribute to 40% of health complaints, implying that decisions were not collaborative but were imposed (NSW Health Care Complaints Commission 2005). Collaboration and communication are now considered as important as delivering care (Department of Health and Ageing 2000). These expectations are influenced by such factors as changing societal attitudes to health and patients’ rights, cultural variations in attitudes towards health care, the advocacy of community support and patient groups, increasing litigiousness, improved patient education and greater availability of health information.
AGREEING ON DECISIONS DOES NOT NECESSARILY EQUATE WITH COLLABORATION
Patients may indicate their agreement with health professionals’ decisions explicitly or implicitly through actual or apparent compliance with treatment or healthcare programmes. However, practitioners need to consider whether this agreement is genuine. Patients enter healthcare situations with a wide range of preparedness for the events that will unfold during their journey of ill-health or disability and for the processes of decision making they encounter. They may or may not have had time to investigate the nature of their condition or its medical management, to prepare mentally, physically or emotionally for the health situation they are facing, and to develop a position on what they would like their health outcome to be. In addition, they commonly do not have the relevant medical knowledge or expertise adequately to understand the nature of the condition, the treatment options and potential health outcomes. So, when it comes to the point of agreeing with a health professional or healthcare team in decision making, the patient’s agreement could be influenced by many ‘entry’ factors. Any agreement or otherwise could also be influenced by factors within the communication or interaction, such as the relationship built up with the practitioner(s), language or cultural familiarity or barriers, aspects of behaviour such as intentions, motivations and practitioners’ practice models (e.g. biomedical, biopsychosocial and emancipatory models). In addition, decision-making processes are influenced by professional authority, professional roles, and expectations held by professional groups and the community.
When clinicians and patients share the same values, intentions and interests, agreement is more likely. However, agreement or compliance that is unarticulated or unquestioned may not be true agreement at all. It is tempting to assume that patients adopt the role that practitioners assign to them, without checking with patients either at the point of decision making or during subsequent treatment programmes. Are patients reporting honestly on their perceptions of progress or their pain levels, etc? A critical perspective to decision making reminds us that commonality of values and interests between patients and practitioners should not be taken for granted.
SHARED OR MUTUAL DECISION MAKING
It is interesting to note that most of the literature on decision making has a tendency to use the term shared decision making rather than collaborative decision making. Makoul & Clayman (2006), in a systematic review of the literature on shared decision making, found great fluidity in what was understood by the term, ranging from clinician-led to patient-led decision making. The authors listed essential elements of shared decision making as: defining the problem, presenting the options, identifying patient values and preferences as well as doctor knowledge, and clarifying understanding. This checklist reflects the transactional procedures in decision making but it falls short of considering how various interests and motivations influence the reasoning behind decision making. Instead it is useful to consider a series of questions that helps to clarify assumptions about knowledge and how knowledge is generated (Edwards et al 2004). When is it appropriate to be practitioner-centred and when patient-centred? Who has permission to define the problem? Who is authorized to identify and legitimize what all the options are? How are patients invited and encouraged to share their values? Whose understanding needs clarification? What counts as knowledge and evidence?
To adopt a critical perspective towards answering the above questions and to pursue collaborative decision making in a critical frame of reference requires also pursuing awareness of ‘self’, ‘the other’, and the wider clinical and patient context. To understand this perspective we turn to the work of Habermas, a prominent critical social scientist and philosopher who developed a theory of knowledge and human interest (1972). Interests are the motivations, intentions and goals that guide behaviours.
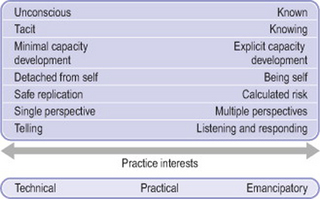
Habermas divided interests into three categories, technical, practical and emancipatory. He argued that technical interest has a scientific bias and aims for technical success, practical interest has a pragmatic bias and aims for consensual understanding, whereas emancipatory interest is directed towards critique and emancipation, and aims for critical understanding. We discussed and illustrated the relationship between interest and practice in Chapter 3 (see especially Table 3.1).
COLLABORATIVE DECISION MAKING FROM A CRITICAL PERSPECTIVE
Many scholars have delineated the dualism between practitioner-centred and patient-centred care (e.g. Arnetz et al 2004), leaving the reader and practitioner appreciating differences between these terms but not helping them to communicate and transcend this dualism. A critical perspective in this context starts with critical self-awareness of what motivates professional bias, professional authority and professional roles, and illuminates the various interests and interpretations underpinning practice approaches, especially those interests that pursue and drive power rather than reason. For example, adopting a critical perspective means seeking first to understand the historical and social factors and influences that have led practice to be accepted and valued the way it is (in a given context) and then to challenge and change this practice with the goal of emancipating those who are restricted or disempowered by it. Within this framework, practitioner-centred practice is typically practice that favours technical rationalism and those in power (commonly the practitioners), whereas in truly (critical) patient-centred practice the practitioner seeks to share knowledge and power with the patient and to respect the input the patient can make to clinical decision making and healthcare management.
People who reason with scientific rationality and objectivity risk silencing emotional, cultural and self-determining rationality. Such communication occurs when practitioners are firmly entrenched in the biomedical model, see evidence-based practice as driven by and contained within scientific method research, and seek an objective and authoritarian pattern of interaction and communication with patients. This practice approach can be highly altruistic, or it can be focused on other interests such as practitioner authority, economic and technical rationalism, and income generation. In each case it is practitioner-centred rather than patient-centred in a critical sense.
Those who reason with cultural and historical rationality tend to silence science and objectivity. Their practice is more patient-centred and can react in an anti-science manner to biomedical model practices. Wellness model advocates and practitioners fit into this category. They have questioned the values and cultural norms of the hegemonic practice model and favour greater levels of person- and patient-centredness. These practitioners embrace subjectivity and holistic approaches to health care but retain their position of authority. This is patient-centredness within a ‘caring for’ (rather than an egalitarian) frame of reference.
Both these perspectives neglect the goal of emancipating patients from the dualism between practitioner-centred and patient-centred care and its potential manipulation and coercion. By comparison, the ideology of a critical perspective to collaboration is a commitment to critical rationality (Habermas 1972).
This leads to consideration of what a collaborative decision-making approach that is informed by a critical perspective would be like. Habermas developed his theory of communicative actions based on a critical perspective of intersubjective communications and interpretations (1984, 1987). This theory describes ideal speech situations (in our case collaborative decision making) as undistorted, open, egalitarian debates that silence unwarranted authority and tradition. Making the intentions and arguments for decisions transparent is seen as the key to making truly collaborative decisions. In addition, collaborative decision making requires critique (including self-critique) and moderation of interests, values and expectations of all parties involved in the decision-making process, and safe, democratizing and caring environments to foster open transparent collaboration where patients feel they are listened to and taken seriously.
In ideal decision-making processes, all involved are aware of their own interests and motivations; this clarifies the reasoning process and enables collaborators to reach critical decisions that include objective, emotional, political, cultural and other factors. The interests of critical rationality and collaborative decision-making processes are emancipatory in that the goal is to find consensus free from traditions, domination and hidden motives. Decisions that are based on critical self-reflection, mutual respect and interest in emancipation are collaborative decisions and are differentiated from false consensus (Roderick 1986).
The arguments in favour of adopting a critical perspective on collaborative decision making are as follows:
The way practitioners define themselves as professionals informs the way they make decisions. Practitioners who see themselves as the expert authority who knows best might find it confronting to have patients collaborate and ‘contaminate’ their decisions based on best practice. They assume that patients come to them to get advice and comply with it. Healthcare practice today remains predominantly influenced by the biomedical model discourse that assigns decision-making power to healthcare professionals. Practitioners who locate themselves in the medical model may describe decision making as a practitioner-led, transactional, linear process in which periodic checking of understanding is recommended. The focus of decision making in the medical model is traditionally based on certainty and prediction of biomedical aspects (Whitney 2003). The implication is that collaboration is necessary only when outcomes of decisions are unpredictable and uncertain. There is a place for practitioner-led decision making, especially in acute situations; however, there is also a place for patient-led decisions. Collaboration is based on the conviction that inclusiveness and critical self-reflection produce better outcomes for patients than empirico-analytical precision. Collaborative decision making is based on inclusive evidence that entails embracing uncertainty and recognizing diversity of patients, clinicians and therapeutic environments (Jones et al 2006). A critical approach helps practitioners to become conscious of their choices in decision making because hidden agendas and bias are made explicit.
OPERATIONALIZING COLLABORATIVE DECISION MAKING FROM A CRITICAL SOCIAL SCIENCE PERSPECTIVE
Shifting towards collaborative decision making requires a capacity to redefine professional practice knowledge, professional authority and professional relations between clinicians and patients. In some fields of health professional practice (e.g. occupational therapy, nursing, speech pathology, physiotherapy) there have been moves away from professional authority models in terms of such issues and strategies as:
AN EXPLORATION OF A CRITICAL SOCIAL SCIENCE PERSPECTIVE IN CLINICAL PRACTICE: IMPLICATIONS FOR COLLABORATIVE DECISION MAKING
As authors and researchers, our interest in examining collaborative decision making lies in fostering and employing critique and emancipation from both unreflective and intentional dominance in decision making. We see collaborative decision making as a strategy enabling practitioners to liberate themselves from unnecessary constraints, to work authentically with patients, to empower patients to reclaim responsibility for their health, autonomy, dignity and self-determination. The intention of collaboration in critical practice is to engage in dialogue and to democratize roles. Collaboration starts with critique, scepticism and curiosity to deepen understanding and to identify the scope of common ground for change. In our research, critique of decision making focused on four closely interrelated dimensions:
Franziska explored these four dimensions by engaging in critical transformative dialogues with three physiotherapist practitioner groups. In Chapter 3we reported on five prototypes (the uninformed, the unconvinced, the contemplators, the transformers and the champions) who represented the way the research participants engaged (or did not engage) with a critical social science perspective in their practice. Here we take each of these prototypes in turn and consider their implications for collaborative decision making.
STUDY GROUP 1
The uninformed
The first group of participants had no prior experience with critical social sciences as a field of study or practice approach and were not involved in education sessions on this topic during the study. To be uninformed about particular approaches to practice does not imply the absence of an approach in one’s practice. However, it is likely that practitioners who have received no education or information about practice approaches that differ greatly from the status quo will tend to adopt the approved, hegemonic approach of the professional or workplace setting. In Franziska’s research, participants who were uninformed about a critical practice approach were not aware of their interests and how those interests influenced their decisions; they often said they did not know what their patients really wanted and what their goals were. The uninformed group’s practice interests were blurred. Practitioners did not think in terms of models or interests but reacted to presenting challenges. There seemed to be a lack of reflexivity. The uninformed had unknowingly adopted the mainstream approach to decision making. However, there was a tendency towards technical rather than emancipatory interests. Figure 4.1 illustrates the continuum and the extreme ends of the various practice models. Collaboration with patients in decision making was limited. In the following accounts of the study, pseudonyms are used for all participants to preserve anonymity.
When Hilda, one of the participants in the study, was asked to describe how she negotiated with patients who did not want to comply with her treatment, she provided a typical example of well-intended but unreflective decision-making processes when she replied:
You have to just keep talking to them and just keep explaining; and by telling them what bad things are going to happen, which isn’t a very nice thing to do, but, if they’re still not complying then you just, I mean, you can’t treat them. (Hilda)
Patients’ needs were equated with a need to bring abnormal medical symptoms back as close to normal as possible. Although she would ask patients how they felt and what they thought they needed, Hilda would use technical, clinical findings to determine (without consulting with the patient) which treatment approach was appropriate. There appeared to be little incorporation of patient perspectives into her needs assessment and treatment plans. Collaboration seemed to be equated with compliance. Felix, another participant, started to think more deeply about how he negotiated decision making with his patients:
You try to get the patient involved as much as possible, definitely. Explain to them the possible strategies that are involved. And, of course, then you ask them are they okay with it – are they willing to go through with all that – be it some form of manual treatment or some form of exercise. You tell them how long you expect them to be coming for, so you ask them are they willing to put up with that, are they going to participate in the treatment exercises and so on. So, in that way, do you think that means they’re participating? Do you think that’s actually getting them actively involved? It’s not really, is it? Not really, now that I’m thinking more about it. It’s almost like you’re telling them what to do, really, aren’t you? But you’re informing them about what you’re doing, though … I thought I was trying to get them involved by informing them as much as possible. That’s all. That’s the way I do it. I don’t actually ask them ‘what do you think we should do about this?’ and get them to sort of come up with it. (Felix)
Felix first portrayed himself as a patient-including physiotherapist, but he noticed that he was not really engaging patients in the decision-making process. His professional relations emphasized his professional status and claimed professional power over patients. Physiotherapists need patients at least to cooperate, especially for exercise therapy. There is a difference between patient participation as a result of egalitarian negotiations and patient participation arising from imposed management strategies based on the therapist’s technical reasoning. The difference lies in the interest and motivation that guides communication between the therapist and patient. Felix showed little interest in the patient’s perspective. He was keen to operationalize his technical interests. Another participant learned about collaborative reasoning by reflecting upon a critical incident that made her question the way she tended to make clinical decisions:
The penny dropped for me only after 10 years of clinical experience. I had [a patient with] an above-knee amputation and he had a prosthesis. He walked perfectly in the gym. I had him walk without a limp. I was really pleased with all this. Then I met him downtown in the shopping centre: he had his knee locked, he was walking on the inner quarter of his foot, foot stuck out at right angle and he was perfectly happy. I stood and looked at him and thought ‘I can make you walk perfectly without a limp but you don’t want to do that’. And you know when he came to treatment he would do it but obviously he wasn’t feeling safe and he didn’t want to do it that way and that is that. I think I wanted him to do what I wanted. I was trying to be a perfectionist. And it has also to do with all the other physiotherapists. They are checking on you that you are doing it all properly. (Jill)
Seeing her patient mobilizing in a non-ideal way but with confidence and seeing him integrated into a social community life made Jill start to question her goal-setting practices and her professional interests. Why should she make patients walk without a limp if all they wanted was to walk safely? Jill became aware of clashes between professional and patient goals. She was aware of peer expectations and she felt pressured to comply with the professional physiotherapy culture. Collaborative decision making is influenced not only by the stakeholders of decisions but also by the practice culture and the workplace environment.
STUDY GROUP 2
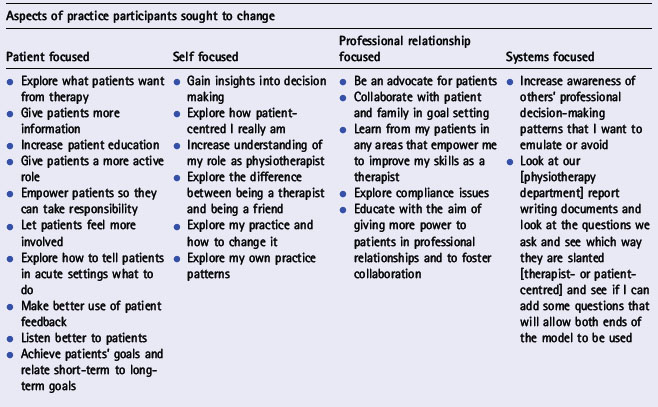
The second participant group received education about critical social science as part of a pre-implementation workshop. They were asked to trial changing self-selected aspects of their practice towards a more critical approach. Table 4.1 lists the strategies participants wrote down in their action plans to identify their focus of change. These strategies addressed concerns relating to the therapist, the patient and their professional relationship. Strategies focused on therapist interest, on patient interest, or on collaboration and dialogue. Participants who chose to focus on self appeared to be more willing to critique self than those who chose to focus on patients, colleagues or the healthcare system. Different levels of engagement characterize the unconvinced, the contemplators, the transformers and the champions.
The unconvinced
Dorothy, who fitted the unconvinced prototype, equated collaboration with compliance. She felt that patients had to understand physiotherapy reasoning but she did not think that physiotherapists had to understand the way patients reasoned. She did not challenge the biomedical interests that influenced the way she reached decisions.
Giving the patients options is definitely making them feel more in control and you get a better response out of them. They don’t just feel like sitting there having things done to them. They are having a bit more of a say what is happening to them. So it is good for both. (Dorothy)
Dorothy experienced working in collaboration with patients as positive. However, her understanding of collaboration was narrowly defined because she limited the patients she chose to collaborate with. She noticed that patients who shared her values and expectations made her more relaxed and she was able to give them choice. These patients did not challenge her practice. What Dorothy described as collaboration was patient compliance. With difficult patients she felt she had to be more forceful.
You get a few people that you need to push or you are not going to get anywhere with them. Patients with stubborn personality won’t do anything no matter what reason you give them. (Dorothy)
Dorothy categorized patients who did not agree with her as difficult people with stubborn personalities. It appeared that either patients worked with her or she had to use professional power to get patients to comply. She did not acknowledge her motivations and interests and she did not practise self-critique.
The contemplators
This group of therapists struggled with the concept of collaboration and patient emancipation. They interpreted collaboration as allowing patients to dominate them and they rejected this approach to decision making. However, they could see some benefits in trying to work with patients by ‘making practice suitable to patient’s background, as much as their biomedical illnesses allowed’.
I am trying to turn the patients’ concerns around to mine. I guess that is what I would like so that we are working together. So it’s all about educating them about what they need to do. (Petra)
Petra understood collaborative decision making as persuading patients to adopt the physiotherapist’s perspective. It was not based on egalitarian principles; the biomedical perspective prevailed unchallenged. Petra’s practice values remained firmly grounded in the acute medical model despite appreciation of patients’ individual fears and needs. Petra believed that once patients were familiar with their acute conditions they could be empowered to take more control and determine their own treatment routine in consultation.
Doing-to patients saves lives and prevents complications. Doing-to is simple and straightforward. It means following my duty of care. In acute [settings] you focus on biomedical signs and you cannot always develop a relationship with the human being. In chronic settings you have time to develop a professional/personal relationship. In long-term rehabilitation you need to consider the human being more. It is more relaxing, working slower with patients. (Petra)
This quote succinctly describes the attitude of the contemplators who saw collaboration as optional and not suitable in some settings. The attitude was that practitioners have permission to assume professional power over their patients due to their professional status and knowledge. Thus professional relationships in the healthcare context start with uneven power relationships, where practitioners have more power than patients. When the participants were asked to rethink and democratize their relationships with patients, the implication was that patients had to be taken more seriously as people with a role to play in clinical decision making and self-management. In exploring collaboration the participants were challenged to listen critically to patients and develop open dialogue with patients.
The transformers
Those participants who trialled democratizing their relationships with patients and who were willing to challenge their use of professional power were classified as transformers. Jocelyn, for example, became more attentive to interests and to her patients’ expectations of physiotherapy. She found that some patients had clear expectations and knew what they wanted. When comparing these with her own professional expectations and goals Jocelyn experienced conflict. She described an incident with an 80-year-old patient who could not carry her shopping home but otherwise was able to be fully independent. Jocelyn noted the decreased range of motion in her shoulder joint and she wanted to work first on increasing range of motion and then on strengthening muscles. However, her patient was not interested in increasing range of motion.
I could see that [this] patient was not interested in my plan. I thought this wasn’t particularly functional [wanting to increase strength before increasing range of motion] but she was able to do everything: cook, clean etc. The only thing she couldn’t do was go shopping because she couldn’t carry anything. So, that was really glaring in my face. This is what she wants to do. I am not sure if I always pick that up. (Jocelyn)
In this situation Jocelyn appeared comfortable going along with her patient’s goals. Her decision was influenced by her patient’s age. Had her patient been younger she might have insisted on improving range of motion as well. Jocelyn made decisions in the context of her patient’s age and function and with a critical stance to self. She was willing to reconsider, in this situation. However, generally speaking, Jocelyn was not content to allow patients to lead treatment plans.
I am not so comfortable [with that]. I feel it takes away some of my authority or professional expertise when I say to them, ‘what would you like to do in physiotherapy?’ because they don’t know physiotherapy technique and they say ‘I don’t know. You should know, you are the physiotherapist’. (Jocelyn)
Jocelyn could see that professional power is a flexible commodity. Simply handing it over was not a useful and critical approach. She would need to use it wisely and with critical awareness in each clinical situation. Jocelyn developed critical awareness of her patients’ expectations, their ideas and their capacity to contribute and participate. This insight enabled her to make more appropriate use of professional power and expand her skills to build more democratic professional relationships.
Corinne displayed a capacity for critical self-reflection in relation to her issues around professional authority and power relations. Corinne had over 30 years of clinical experience and her area of expertise was outpatient physiotherapy. She questioned her practice and surprised herself:
After the pre-implementation workshop I have been taking more notice of what I am doing with people and I was very surprised to find that I do tend to use quite a lot of physiotherapy [practitioner] power. I was actually very surprised to notice that. I had an incident the other day: I was doing something with a quite young lady and I was palpating her knee and she pushed my hand away and said ‘you are hurting me’. I considered this palpation was appropriate for her age, health and all that. Well it was funny, it was more a – ‘think of my feelings’ reaction – rather than – ‘Oh dear [sorry]’ – but I thought ‘how dare you’. I am not used to being treated like that (laughter). I didn’t consider my palpation being too severe and I was thinking, ‘oh, I don’t like this’. The way she said it did not sit well with me. (Corinne)
Corinne did not like to be told that her professional judgement about touch was wrong from the patient’s perspective. Corinne was reminded that she had no control over her patient’s pain perception. However, the patient’s manner conveyed an assertiveness that Corinne was not used to. Collaboration means working together and includes listening and talking as well as giving and taking. Corinne viewed each treatment as a learning process for herself as well as for her patients:
I want to learn from patients so that I can improve my own skills. I think that every treatment session is a learning session for me. (Corinne)
Corinne learned to recognize that she was not the only expert or the professional who should know all the answers. She could appreciate that patients had relevant knowledge as well. Corinne learned to reframe herself as a facilitator of collaborative decision making. She not only transformed her approach to practice and her view of herself as a professional, but she also learned about practice as a collaborative transformation.
The champions
Participants who had operationalized collaborative decision making and endorsed the values of inclusion and power-sharing were labelled champions or advocates of the critical social science approach. These participants were sceptical and critical of professional authority that was taken for granted and automatically assumed. Raymond, one of this group, saw himself as a scientist, a critical self-reflector and a patient collaborator.
Is physiotherapy a social science? To me it is, and my colleagues will hit me over the head. I think there are the arts and the sciences. It is somewhere between the two. You have to oscillate all the time to facilitate an outcome for the patient. So I have this pulling force in me all the time. I value the scientific and searching for the evidence but I am worried about the patient. (Raymond)
Raymond saw himself as integrating biomedical facts with patients’ perceptions of their healthcare needs and condition. He defined his practice as ‘doing qualitative medicine’. He recognized that a collaborative approach to decision making did not exclude propositional or scientific knowledge but it also required non-propositional knowledge to achieve emancipatory outcomes. Champions do not make decisions without continually checking their impact with individual patients; they regard patients as social, cultural and political human beings.
You cannot tell a teenager to stop smoking. You need to look at their social issues. I practise physiotherapy like that. First [I consider] scientific knowledge and then social beliefs and patient knowledge. (Raymond)
In analysing the interviews with the champion group a number of factors that indicated participants’ capacity or inclination for participating in collaborative decision making were identified. These included:
The champions in this study were distinguished from the other groups in that they used their human agency to facilitate change in their patients. This change was greater than biomedical improvement because it was initiated in collaboration with patients, so that treatment interventions were appropriate and meaningful for both physiotherapist and patient.
CONCLUSION
Collaboration can be improved and better understood when people start being more open to learning and understanding the other party’s interests and goals, and when they ask questions to enable others to elaborate on their perspective and values. Understanding the other person by illuminating their interests and biases and doing the same with oneself is part of gaining a critical perspective. Beyond listening more attentively and respecting diversity, it is important to act on this increased understanding and move towards collaboration. Cultivating curiosity and addressing one’s limits of collaboration is a starting point to becoming more aware of when, how, what and why decision making needs to be collaborative. A critical perspective fosters practitioners’ confidence to communicate democratically with patients with the goal of making appropriate decisions. It helps clinicians to make conscious choices about the degree of collaboration that is appropriate in each clinical situation.
Arnetz JE, Almin I, Bergström K, et al. Active patient involvement in the establishment of physical therapy goals: effects on treatment outcome and quality of care. Advances in Physiotherapy. 2004;6:50-69.
Braddock CHIII, Fihn SD, Levison W, et al. How doctors and patients discuss routine clinical decisions: informed decision making in the outpatient setting. Journal of General Internal Medicine. 1997;12(60):339-345.
Department of Health and Ageing. Public health practice in Australia today: a statement of core functions. 2000. Online. Available: www.nphp.gov.au/publication/phpractice/phprac/pdf 24 July 2006
Edwards I, Jones M, Higgs J, et al. What is collaborative reasoning? Advances in Physiotherapy. 2004;6:70-83.
Habermas J. (trans J J Shapiro). Knowledge and human interest. London: Heinemann. 1972.
Habermas J. The theory of communicative action. Reason and the rationalization of society, Vol 1. Oxford: Polity Press. 1984. (trans. T McCarthy).
Habermas J. The theory of communicative action. The critique of functionalist reason, Vol 2. Oxford: Polity Press. 1987. (trans. T McCarthy).
Hall JA, Visser A. Health communication in the century of the patient. Patient Education and Counseling. 2000;41(2):115-116.
Jones M, Grimmer K, Edwards I, et al. Challenges in applying best evidence to physiotherapy. Internet Journal of Allied Health Sciences and Practice. 4(3), 2006. Online. Available: http://ijahsp.nova.edu/ 9 June 2007
Makoul G, Clayman ML. An integrative model of shared decision making in medical encounters. Patient Education and Counseling. 2006;60(3):301-312.
Mueller PS, Hook CC, Fleming KC. Ethical issues in geriatrics: a guide for clinicians. Mayo Clinic Proceedings. 2004;79:554-562.
NSW Health Care Complaints Commission. Annual Report 2004–5. 2005. Online. Available: www.hccc.nsw.gov.au/downloads/ar/04-05pdf 24 July 2006
Richardson F, Carryer J. Teaching cultural safety in a New Zealand nursing education program. Journal of Nursing Education. 2005;44(5):201-208.
Roderick R. Habermas and the foundations of critical theory. New York: St Martin’s, 1986.
Snapshot. Empowered patients are more satisfied with their care. Snapshot: An Electronic Newsletter. 2004;3(3):1-3.
Trede FV. A critical practice model for physiotherapy. Australia: University of Sydney, 2006. Unpublished PhD thesis
Trede F, Higgs J. Re-framing the clinician’s role in collaborative clinical decision making: re-thinking practice knowledge and the notion of clinician–patient relationships. Learning in Health and Social Care. 2003;2(2):66-73.
Trede F, Higgs J, Jones M, et al. Emancipatory practice: a model for physiotherapy practice? Focus on Health Professional Education: A Multidisciplinary Journal. 2003;5(2):1-13.
Whitney SN. A new model of medical decisions: exploring the limits of shared decision making. Medical Decision Making. 2003;23:275-280.
Winokur SC, Beauregard KJ. Patient safety: mindful, meaningful and fulfilling. Frontiers of Health Services Management. 2005;22(1):17-32.