Basic Nursing Concepts Care Plans
This chapter has several clinical conditions or situations that may be present in the patient with other medical conditions. These conditions include mood disorders, substance abuse, and death and dying. In addition, this chapter includes several therapeutic interventions that may be used as part of the management of many clinical conditions. These interventions include blood component therapy, central venous access devices, enteral nutrition, and total parenteral nutrition. These care plans were in previous editions of the book in the various body systems chapters. A new care plan has been added to this edition that focuses on the care of the patient experiencing surgery. These care plans have been placed together in this chapter for ease in accessing the information. The care plans follow the same format used for care plans for medical disorders.
Surgical Experience: Preoperative and Postoperative Care
 = Independent
= Independent  = Collaborative
= Collaborative For additional care plans and an Online Care Plan Constructor, go to http://evolve.elsevier.com/Gulanick/.
For additional care plans and an Online Care Plan Constructor, go to http://evolve.elsevier.com/Gulanick/.
Major; Minor; Elective; Urgent; Emergency; General Surgery; Ambulatory Surgery; Same-Day Surgery; Outpatient Surgery; Minimally-Invasive (Fiberoptic) Surgery
Patients undergo surgery for a variety of purposes. These purposes include exploration and diagnosis, excision and removal of diseased body parts, palliation of disease symptoms, restoration or reconstruction of body parts or functions, and cosmetic improvement in physical appearance. Most surgeries are planned and considered elective. Advances in surgical and anesthesia techniques have led to shortened lengths of stay. Many surgical procedures that in the past required several days of inpatient care now are performed in the outpatient or ambulatory setting. The patient is discharged within a few hours after recovery from the effects of anesthesia. Surgical procedures that previously required open incisions are now performed using minimally invasive techniques.
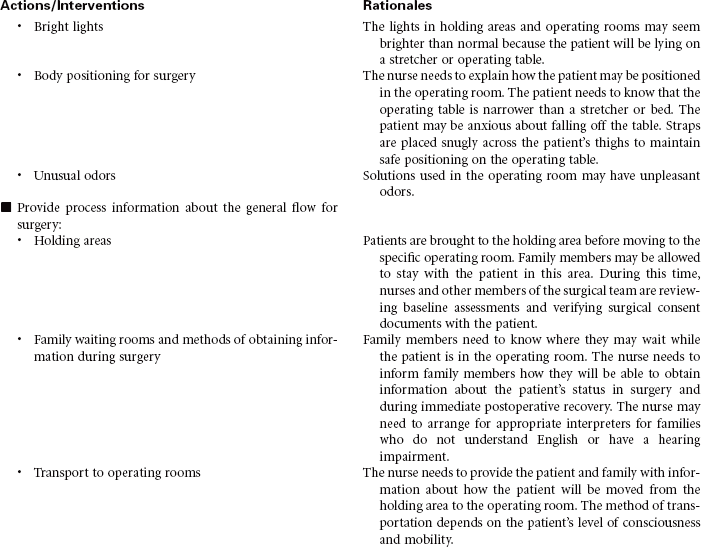
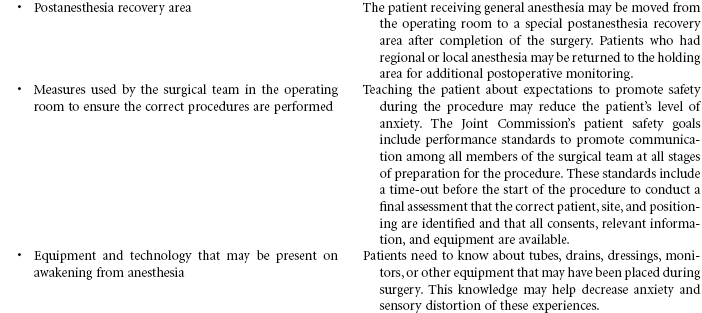
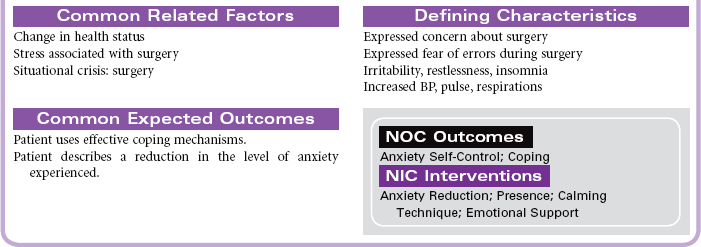
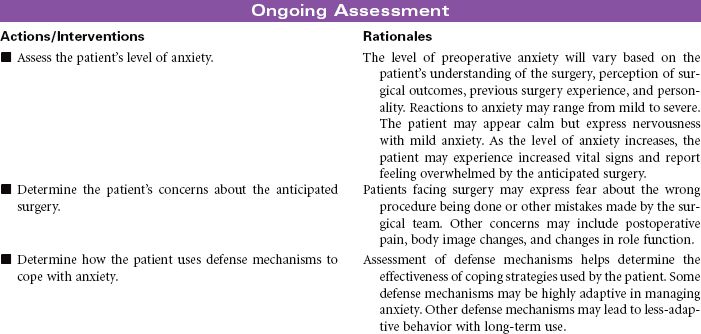
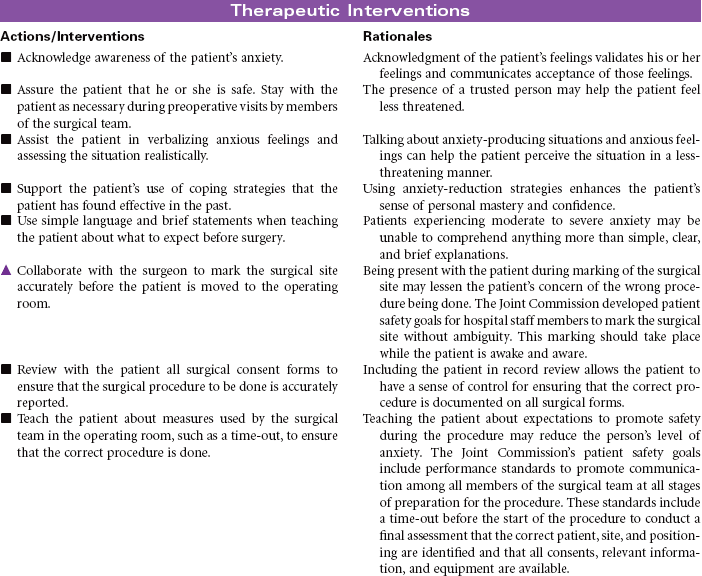
The primary focus of nursing care during the preoperative phase of the surgical experience is teaching the patient and family members. Preoperative teaching includes three types of information: sensory, procedural, and process. Because the time for patient and family teaching has decreased, a team approach is usually most effective. Teaching begins in the outpatient setting and is reinforced when the patient arrives at the hospital or surgery center on the day of surgery.
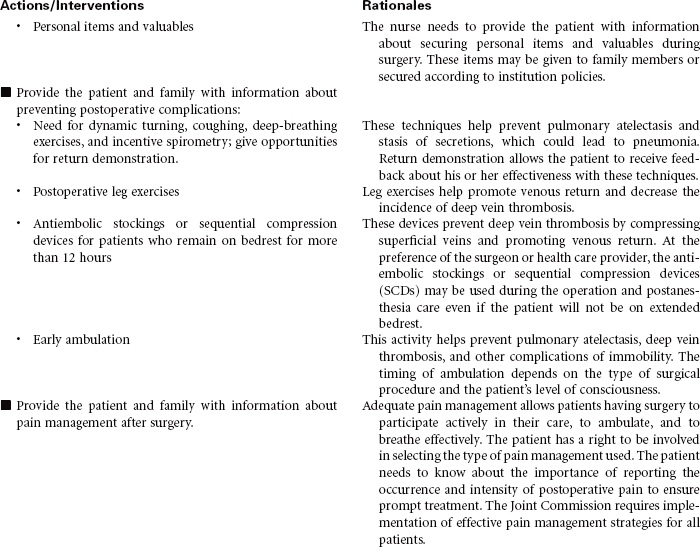
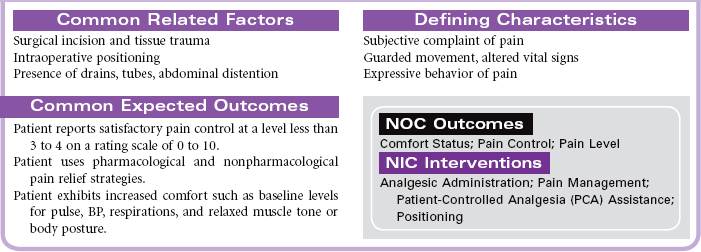
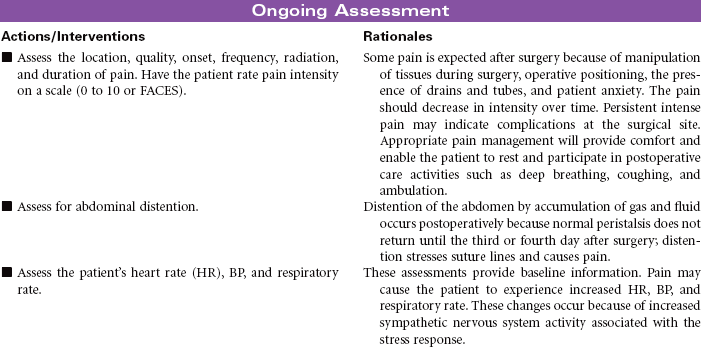
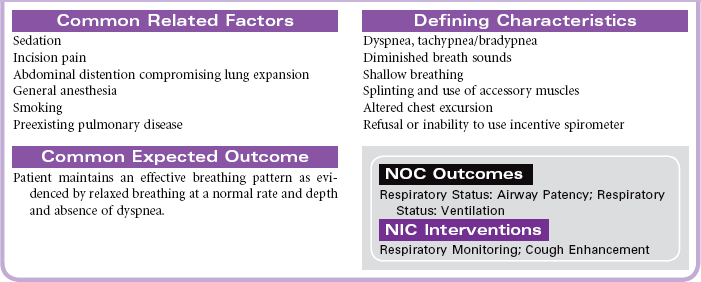
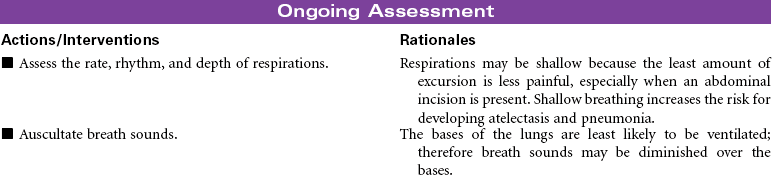
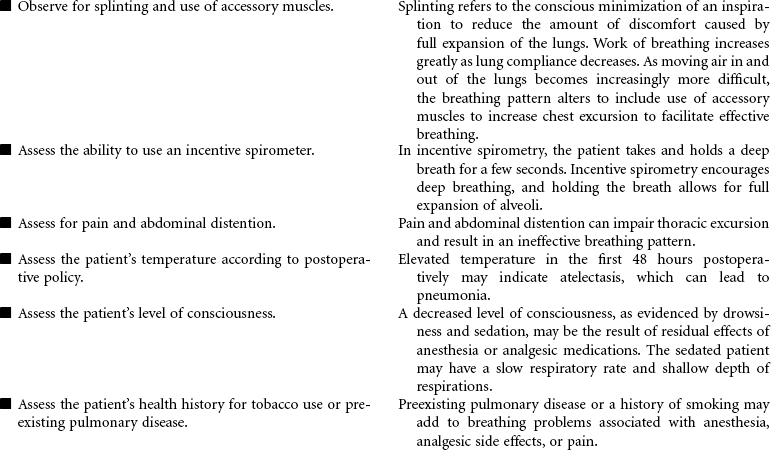
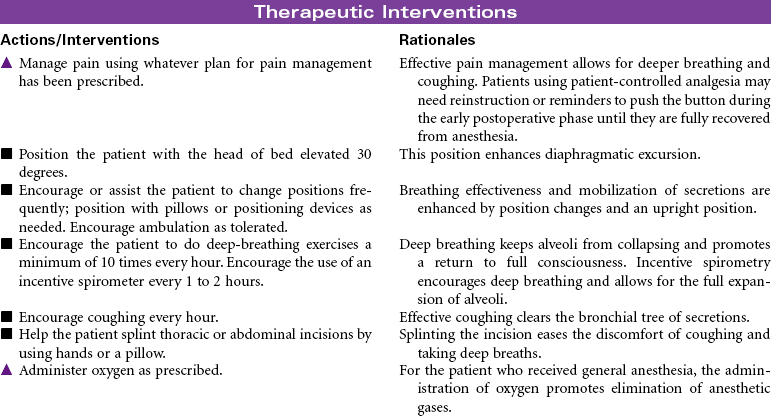
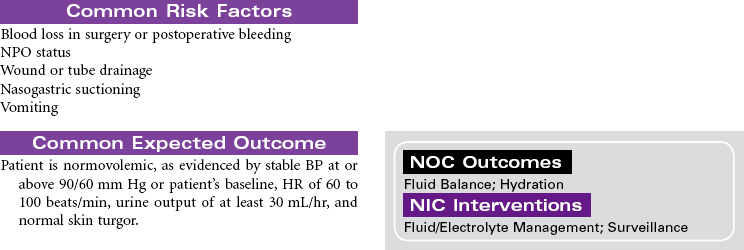
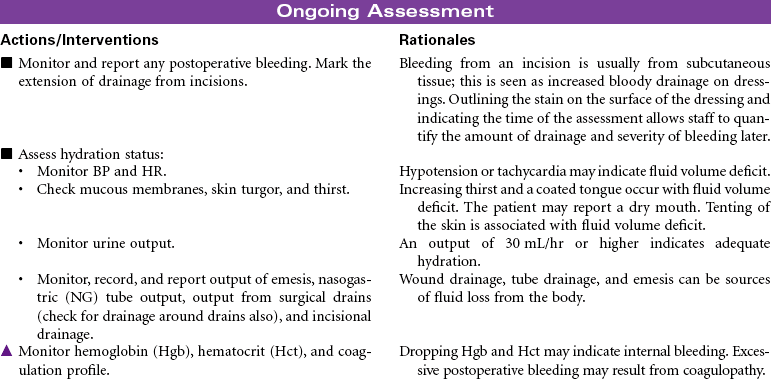
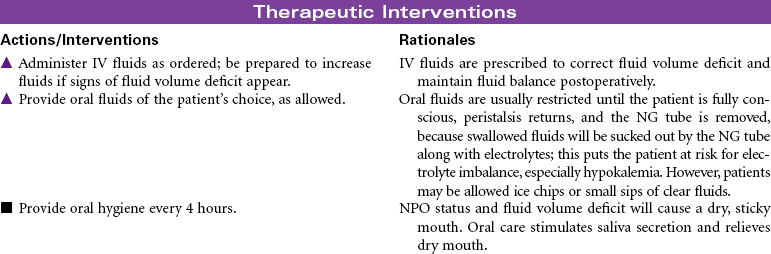
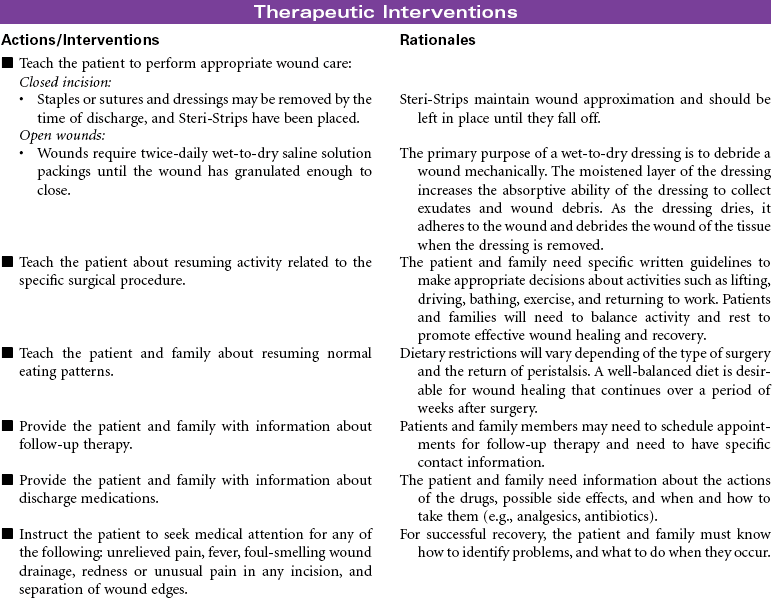
Nursing care during the postoperative phase focuses on pain management, prevention of complications, and preparation for convalescence at home. Patient and family teaching that began preoperatively continues during the postoperative phase and prepares the patient and family to continue care after discharge to home. Because of shorter lengths of stay, patients are discharged with more complex care requirements.

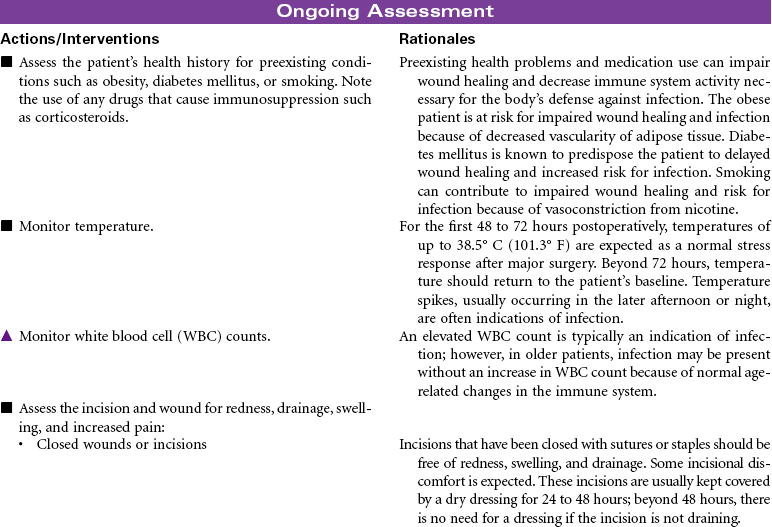
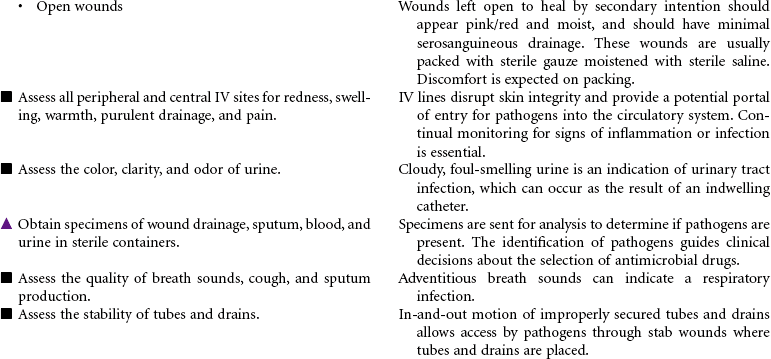
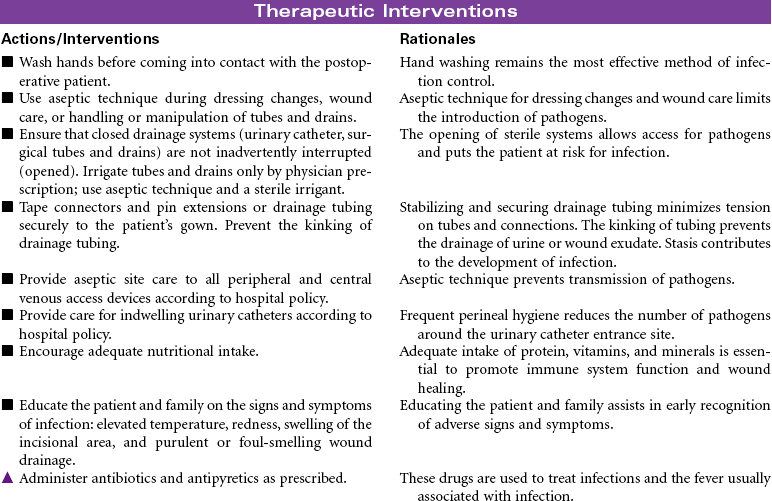
 Risk for Impaired Abdominal Wound Healing
Risk for Impaired Abdominal Wound Healing

Blood Component Therapy
Whole Blood; Packed Red Blood Cells (RBCs); Random Donor; Platelet Pheresis Packs; Platelets; Fresh Frozen Plasma; Albumin; Coagulation Factors; Autotransfusion
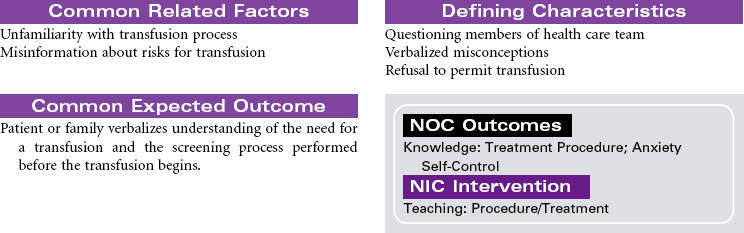
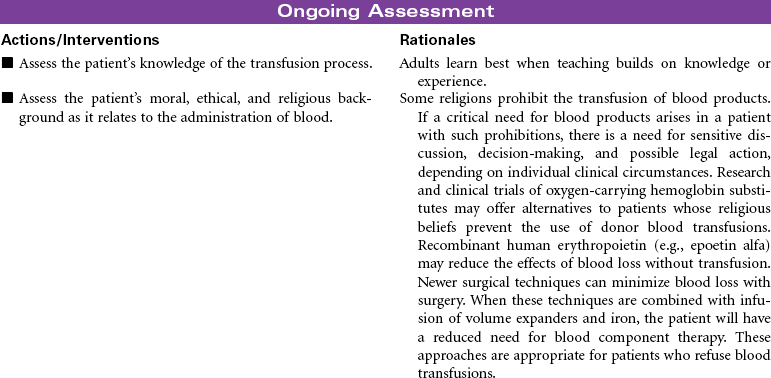
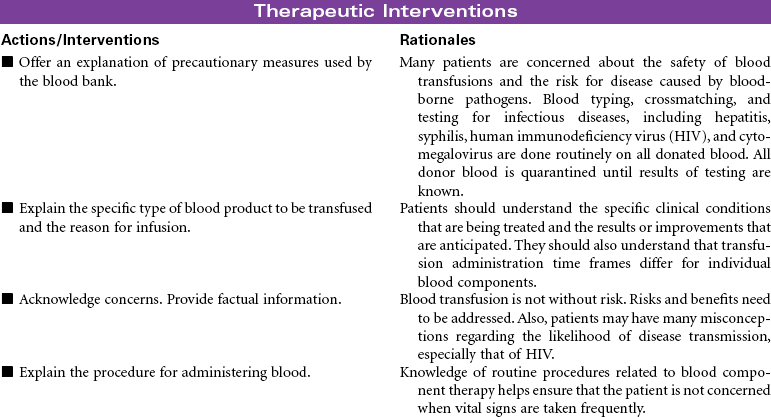
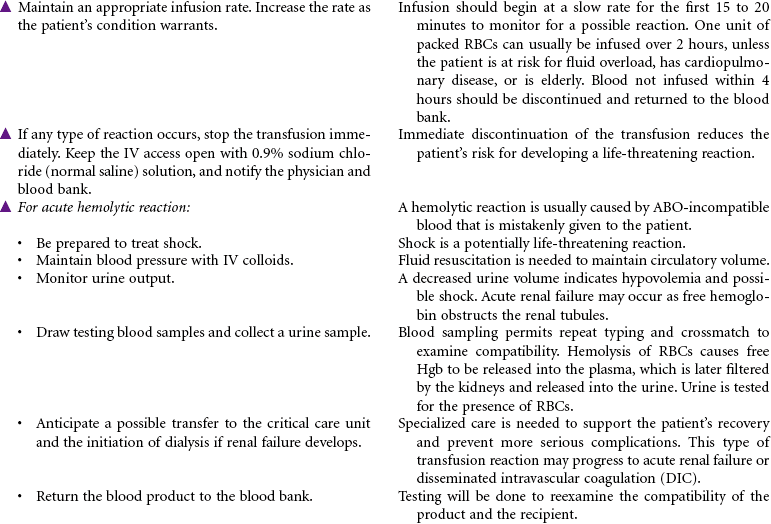
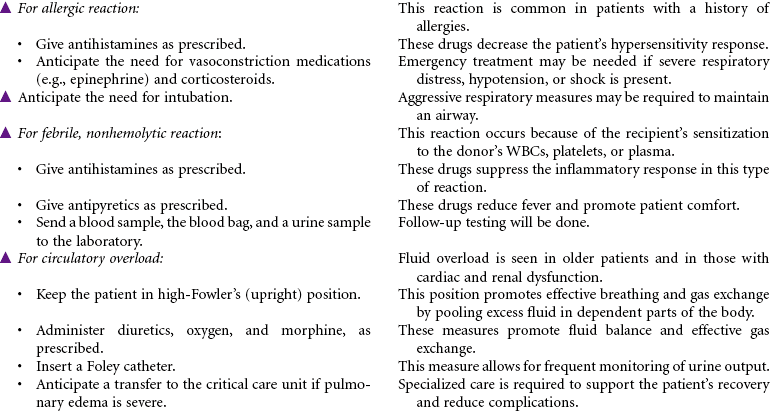
Blood component therapy is used in the management of a variety of clinical disorders. IV administration of blood and blood products is used to restore circulating volume and to replace the cellular components of the blood. Advances in medical technology have significantly improved the safety of blood transfusion therapy. Blood is commonly typed by the ABO system, the Rh system, and human leukocyte antigen found on tissue cells, blood leukocytes, and platelets. Today, specific blood component therapy has essentially replaced the practice of whole blood transfusions. Specific components may consist of RBCs, fresh frozen plasma, platelets, granulocytes (WBCs), specific coagulation factors (e.g., cryoprecipitate, factors VIII and IX), and volume expanders such as albumin and plasma protein fraction. This use of blood components has expanded the availability of replacement therapy to more patients with reduced risk for side effects. Blood components can be modified in several ways to treat high-risk patients, such as stem cell transplant patients and severely immunocompromised chemotherapy patients. Modifications may include irradiating RBCs, volume-reducing platelets, leukocyte reduction, washing RBCs and platelets for patients with severe plasma allergies, and providing cytomegalovirus-seronegative cellular components.
Several types of transfusion options exist for blood component therapy. Homologous transfusions use blood products collected from random donors. Autologous transfusions use blood products donated by the patient for his or her own use. The blood is collected either by planned preprocedure donations that store blood until needed or by blood salvage, which collects, filters, and then returns the patient’s blood that is lost during a surgical procedure or an acute trauma by use of an automatic “cell saver device.” Directed transfusions use blood donations by one person that are directed to a specific recipient. Blood component therapy can be safely administered by qualified nurses in the hospital, ambulatory care, and home setting.
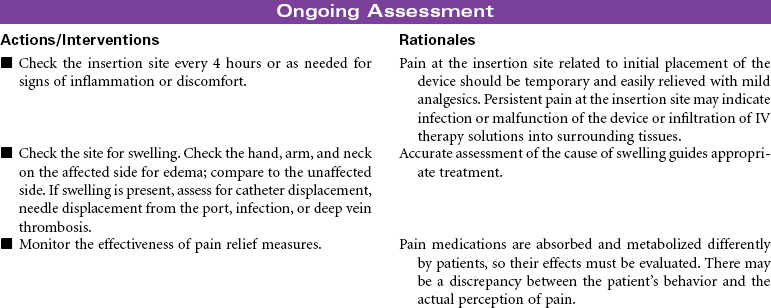
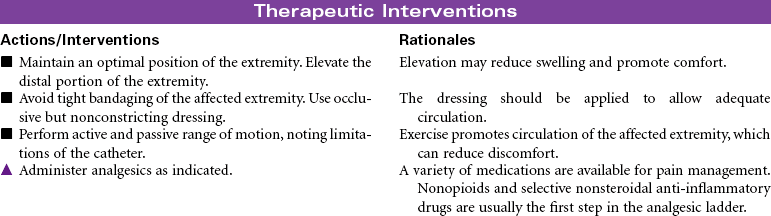
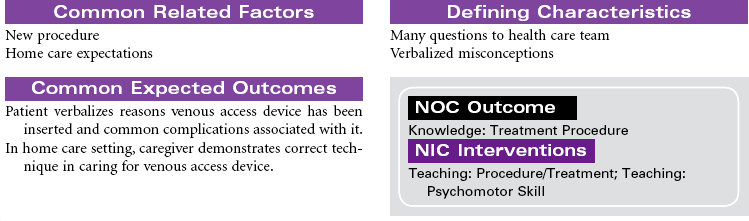
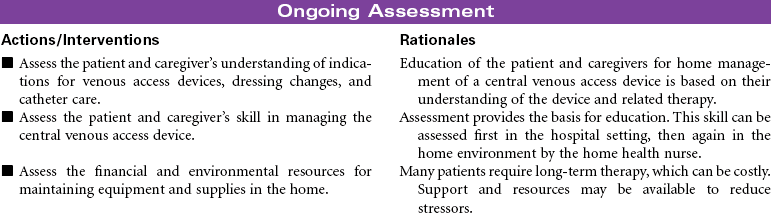
Central Venous Access Devices
Implantable Ports; Peripherally Inserted Central Catheter; Tunneled and Nontunneled Catheters
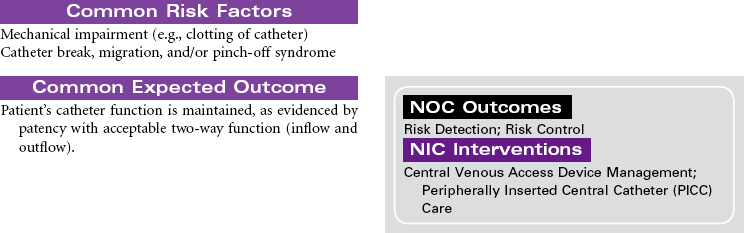
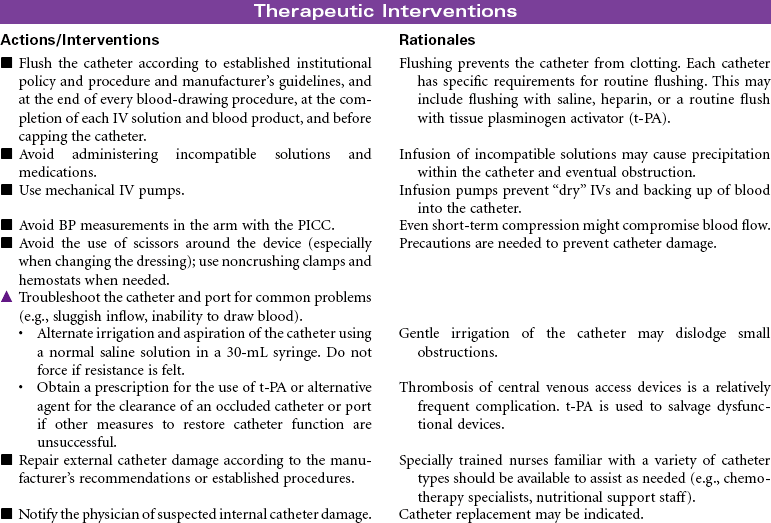
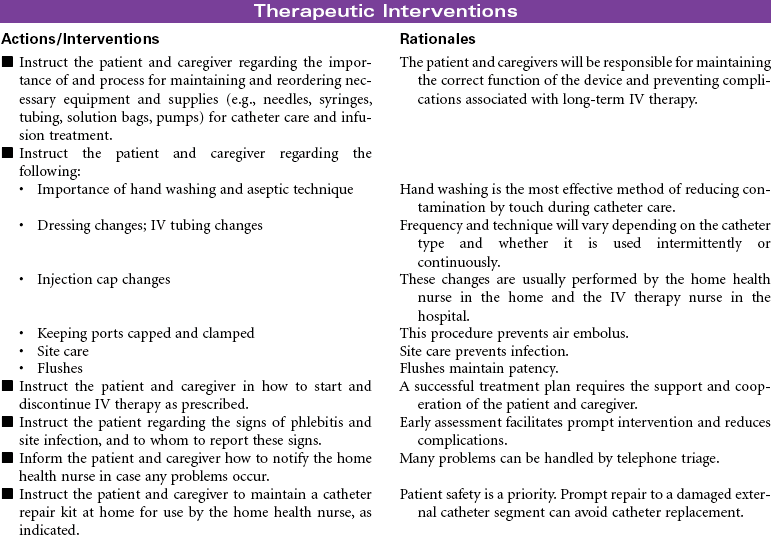
Central venous access devices are indwelling catheters placed in large vessels using a variety of approaches. These catheters or devices are indicated for multiple blood draws; total parenteral nutrition; blood administration; intermittent or continuous medication administration, especially with vesicant agents or chemotherapy; parenteral fluids; and long-term venous access. Central venous access devices are beneficial for patients who receive IV therapies that require the hemodilution of large central veins. Patients with limited peripheral venous access also benefit from placement of a central venous access device for IV therapy and blood draws. Catheters can be implanted for as long as 1 to 2 years.
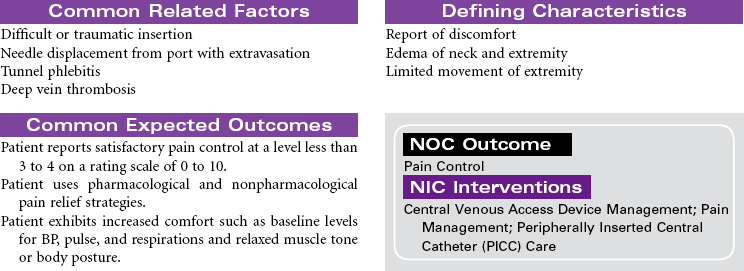
Types of devices include the following: nontunneled (or percutaneous) central catheter suitable for short-term (fewer than 6 weeks) use, inserted via the subclavian vein; peripherally inserted central catheters (PICC lines) used for intermediate-length therapy (3 to 12 months) that are inserted via the cephalic or basilic vein into the superior vena cava; tunneled catheters that can remain in place for 10 years or more, surgically implanted with an external access on the upper chest; and an implanted infusion port, also used for long-term management, that has a catheter attached to a reservoir surgically implanted in a subcutaneous pocket, thereby avoiding an external catheter.
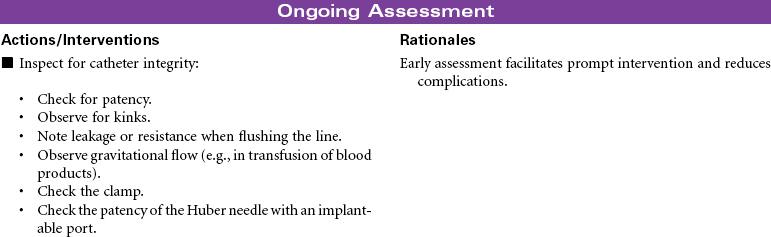
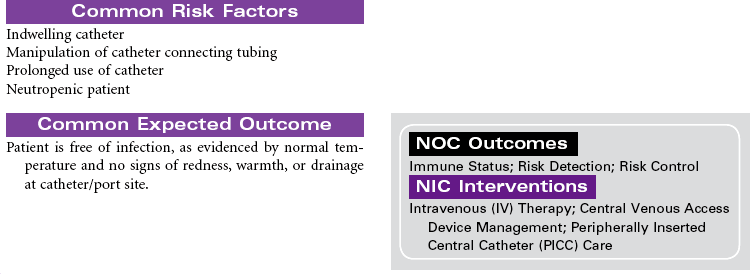
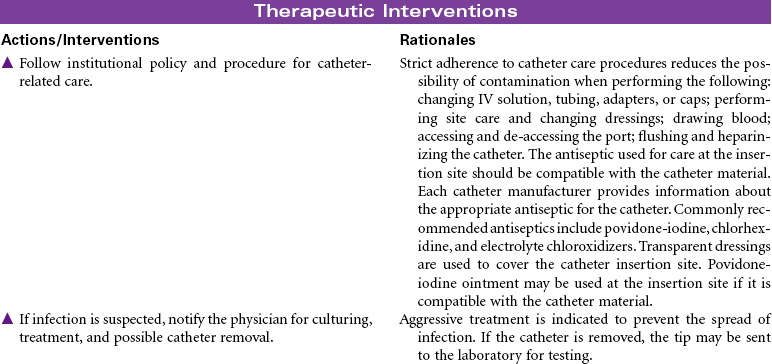
Each catheter has specific requirements for flushing, heparinization, and dressing changes. Common complications include phlebitis, infection, and catheter occlusion. These types of access devices are encountered not only in the hospital but also in the ambulatory care and home setting.

Total Parenteral Nutrition
Intravenous (IV) Hyperalimentation
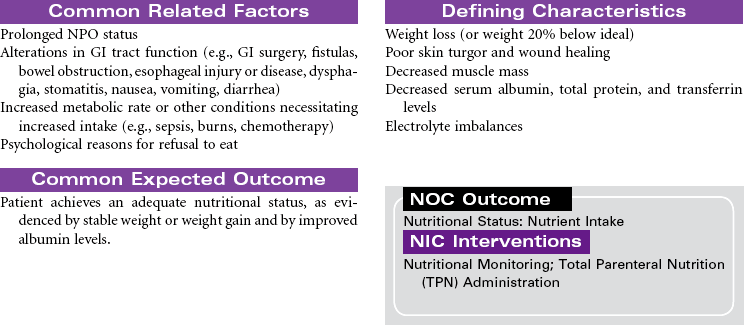
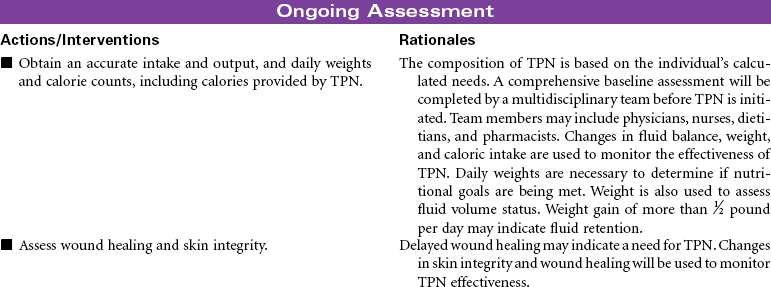
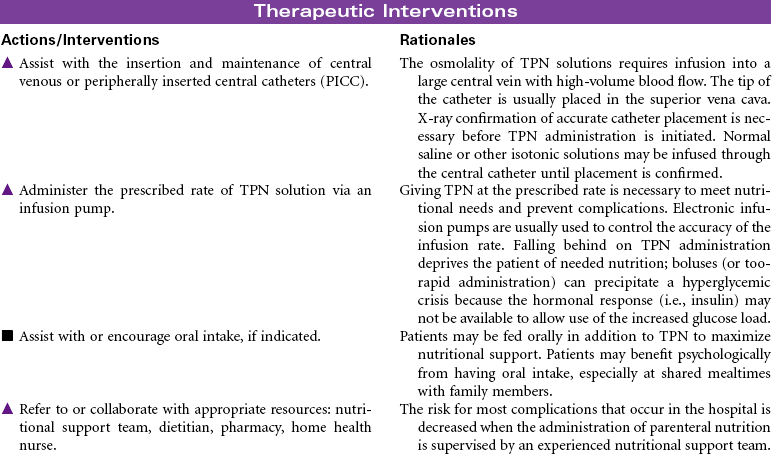
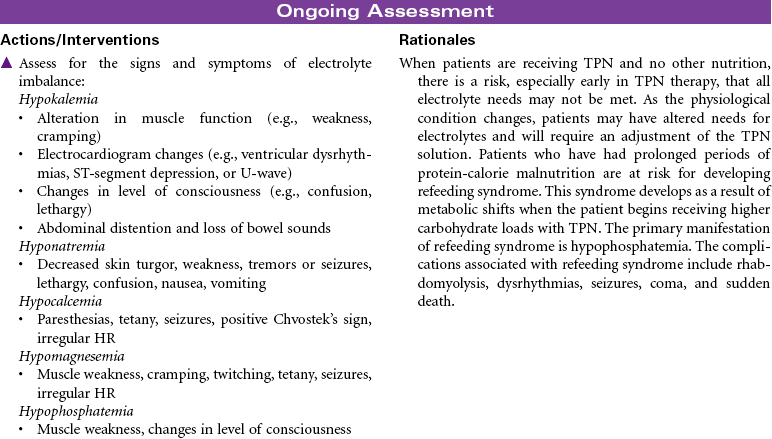
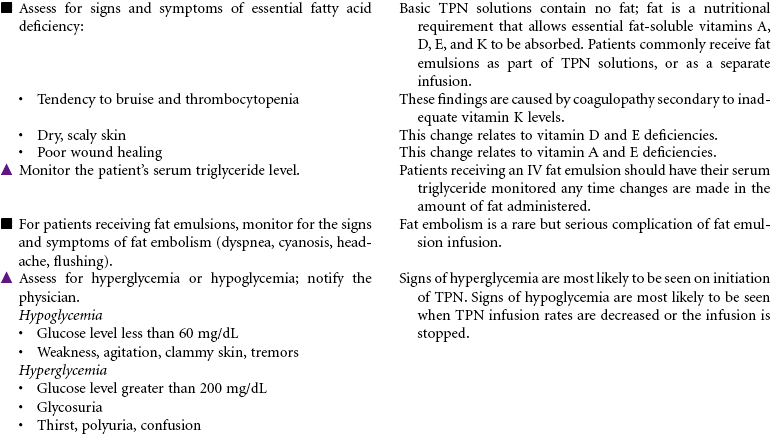
Total parenteral nutrition (TPN) is the administration of nutrients via a central vein. TPN therapy is necessary when the gastrointestinal (GI) tract cannot be used or when oral intake is not sufficient to meet the patient’s nutritional needs. TPN solutions are hypertonic and may contain 20% to 60% glucose and 3.5% to 10% protein (in the form of amino acids), 10% to 30% fat emulsion, electrolytes, vitamins, minerals, and trace elements. These solutions can be modified, depending on the presence of organ system impairment or the specific nutritional needs of the patient. Fluid and electrolyte status require frequent monitoring while receiving TPN. TPN is often used in hospital, long-term, and subacute care, but it is also used in the home care setting. This care plan addresses nursing care needs that may occur in any of these settings.


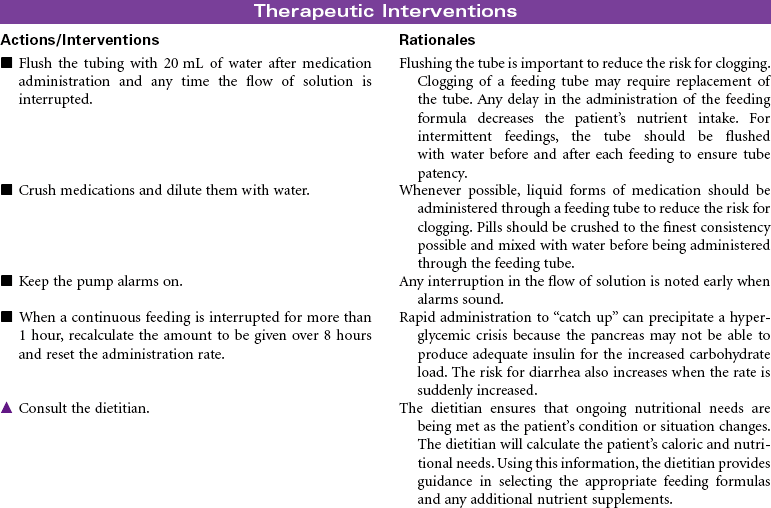
Enteral Tube Feeding (Enteral Nutrition)
Enteral Hyperalimentation; G-Tube; Jejunostomy; Duodenostomy; PEG Tube; Dobhoff Tube
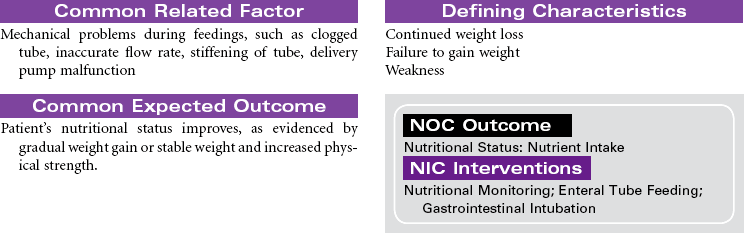
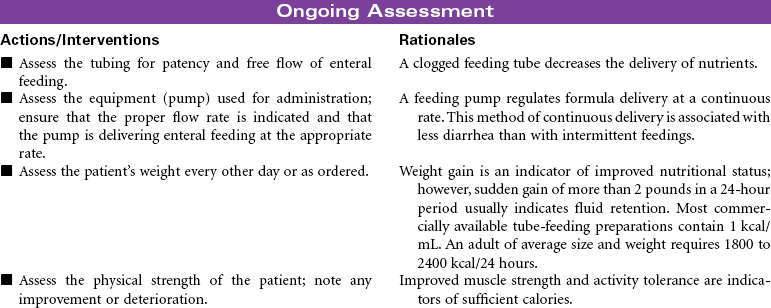
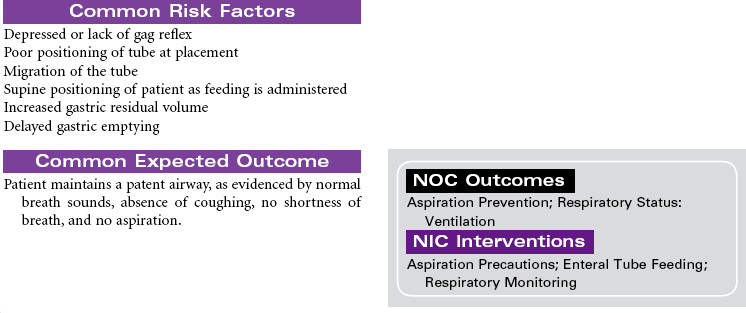
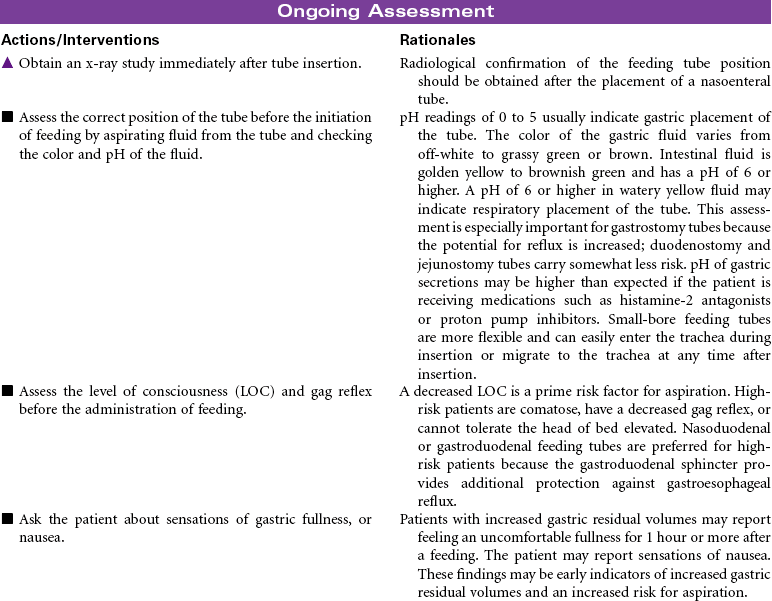
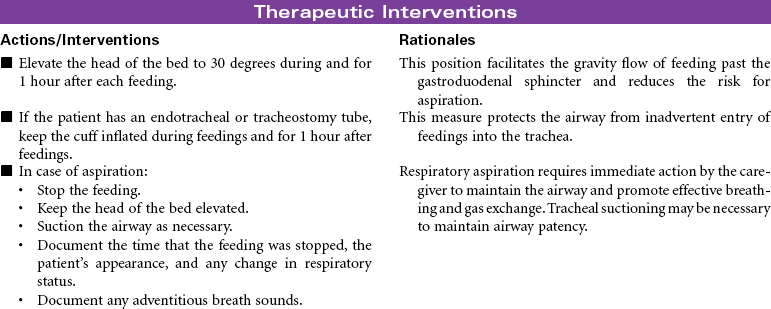
Enteral tube feedings provide nutrition using a nasogastric tube, a gastrostomy tube, or a tube placed in the duodenum or jejunum. Tubes may be inserted through the external nares or may be placed through a small incision into the stomach or small intestine. Enteral tube feedings are indicated for patients who have a functional gastrointestinal system but are unable to maintain adequate nutritional intake orally. Clinical conditions that may limit the patient’s ability to maintain adequate oral intake include cancer, facial fractures, burn injury, and psychiatric problems such as dementia. Research indicates that critically ill patients receiving enteral tube feedings tend to have better outcomes and fewer complications. The problems associated with the administration of enteral tube feedings include pulmonary aspiration of feeding formula, diarrhea, and fluid and electrolyte imbalances. Feedings may be continuous or intermittent (bolus). Enteral tube feedings can be more cost effective than TPN. Enteral feeding may occur in the hospital, in long-term care, or in home care. The focus of this care plan is the prevention and management of problems commonly associated with enteral feeding.

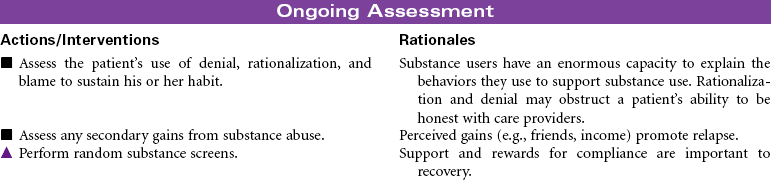
Substance Abuse and Dependence
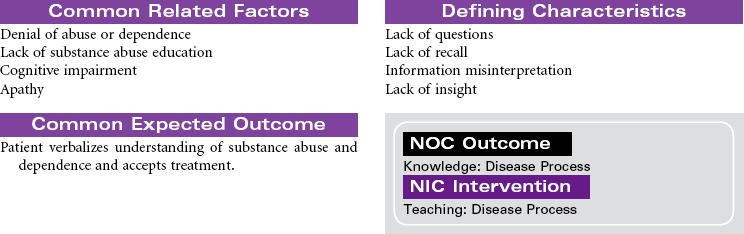
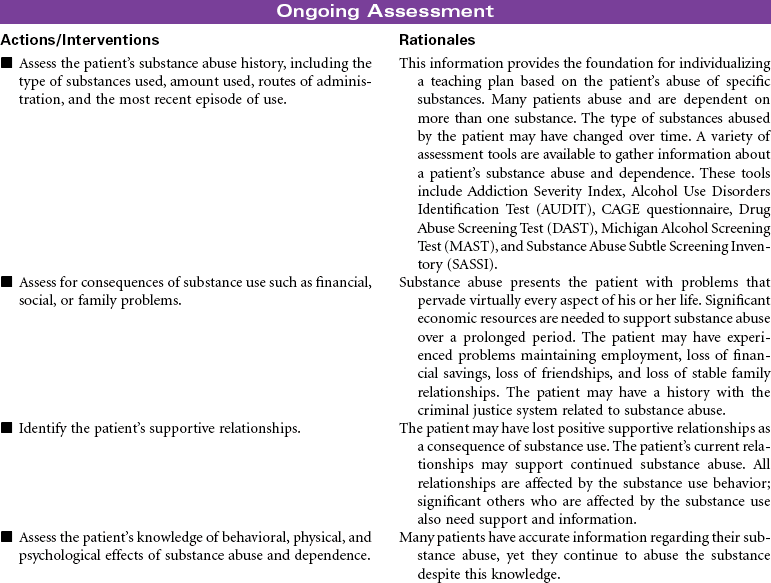
Substance abuse is a maladaptive pattern of substance use. The Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) criteria for this pattern includes a single behavior or constellation of behaviors within a 12-month period: failure to fulfill major role obligations (e.g., at work or within family), substance use in dangerous situations (e.g., while driving or operating heavy equipment), substance use that results in legal problems (e.g., arrest for driving under the influence), and social and interpersonal problems (e.g., arguments, domestic violence). Substances that may be abused include alcohol, prescription drugs, and illegal drugs.
Substance dependence is a pattern of substance use that results in biochemical, psychological, and behavioral changes. The DSM-IV criteria for this pattern includes at least three of the following maladaptive behaviors within a 12-month period: (1) tolerance (the need for increased amounts of the substance to achieve the desired effect or a diminished effect from use of the same amount of the substance); (2) withdrawal (symptoms occur when the substance is withheld or the substance must be used in specific amounts to prevent withdrawal symptoms); (3) need for greater amounts of the substance over longer periods than was originally intended; (4) failure of efforts to stop substance use; (5) increased time spent in activities that support obtaining, using, and recovering from the substance (drug-seeking behavior); (6) abandonment of activities that were once important (e.g., sports, school) because of substance use; (7) continued substance use despite realization that problems are made worse by the substance use.
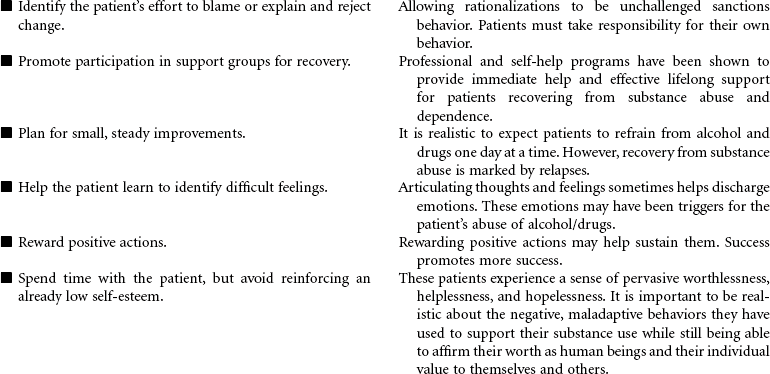
The problem of substance abuse and dependence crosses all gender, age, racial, social, and economic boundaries. The patterns of substance abuse and dependence begin with a voluntary choice to use the substance. With continued use of the substance the person loses the ability to choose not to use it. The person’s behavior becomes marked by a compulsive need to find and consume the drug or alcohol. This change in behavior is related to prolonged exposure to the substance and its effect on brain function. Substance abuse and dependence is a multidimensional problem. Effective treatment programs address these complex dimensions and their consequences. Substance disorders may be part of a dual diagnosis in which substance disorder is the primary or secondary problem with another mental health disorder. Both problems require treatment. A patient may be hospitalized during the initial withdrawal phase of treatment, but treatment must continue on an outpatient basis. Because substance disorders are relapsing disorders, remission and recovery require continuous treatments.



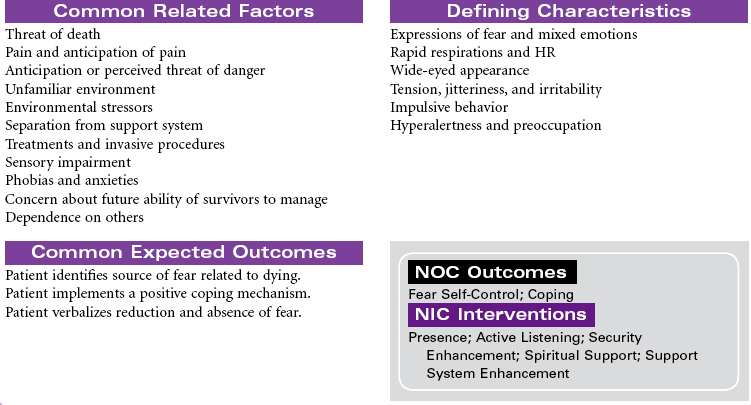
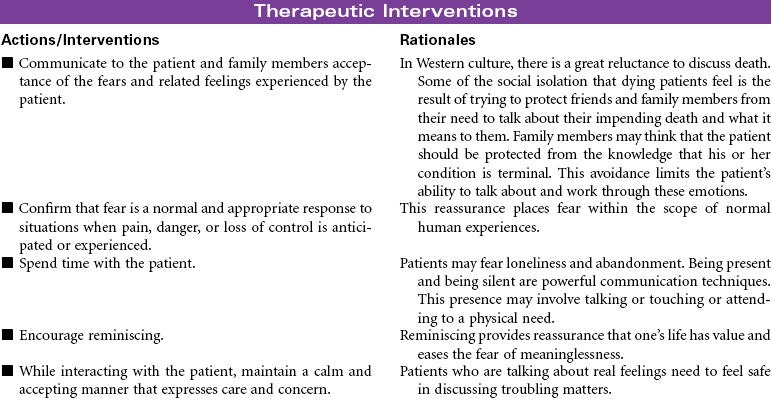
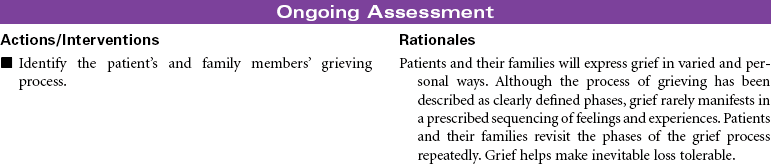
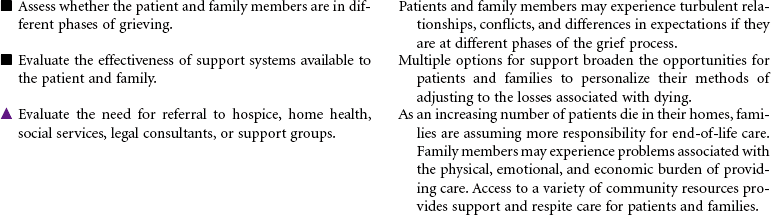
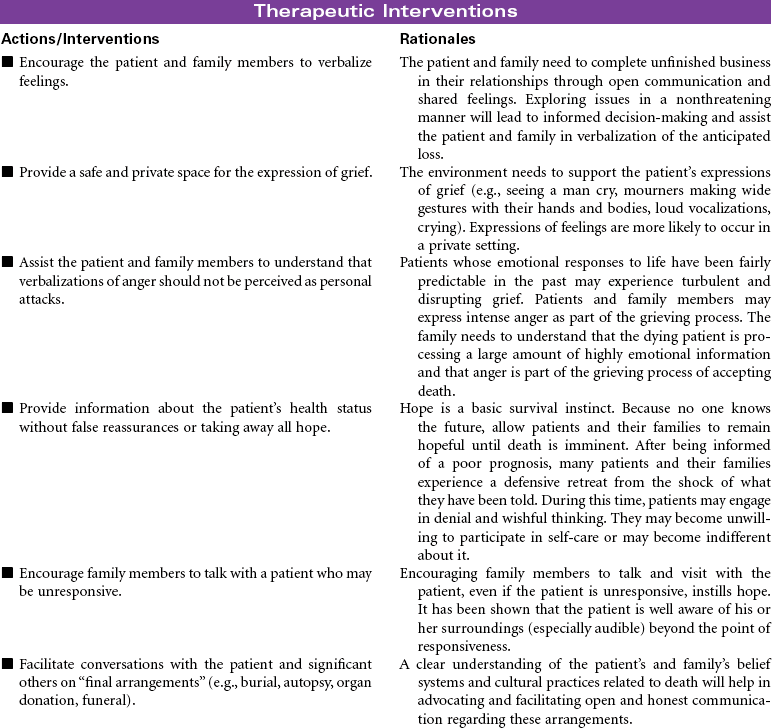
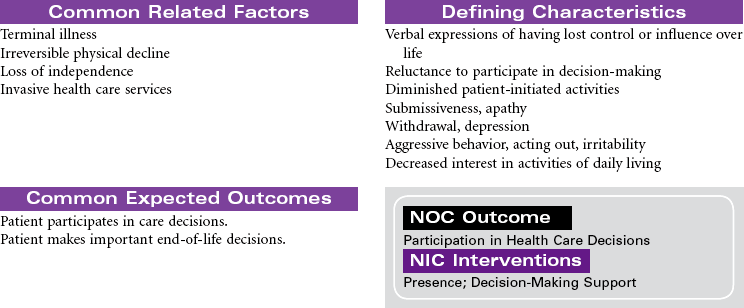
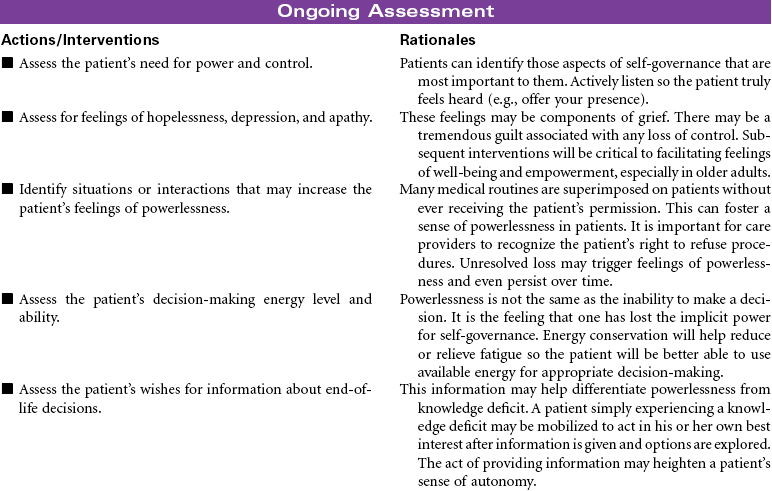
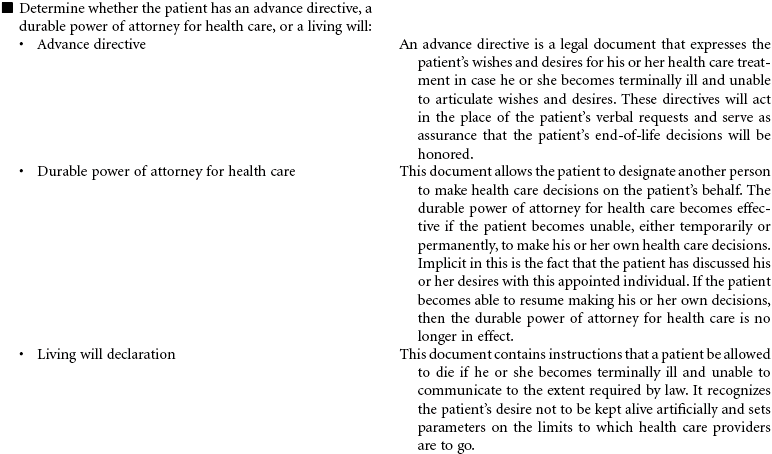
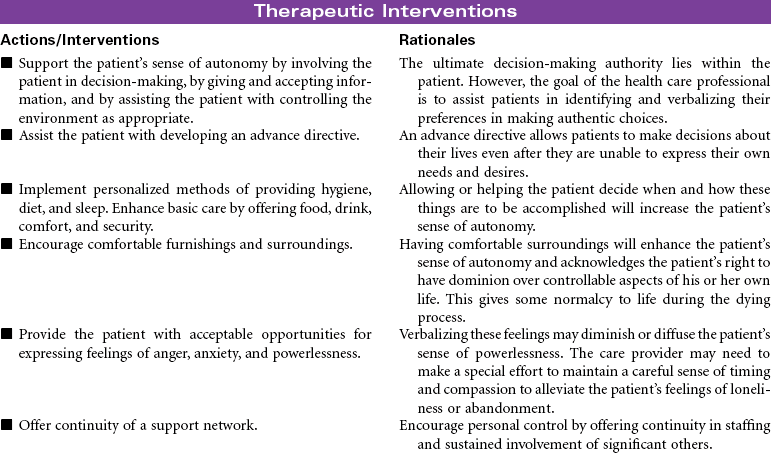
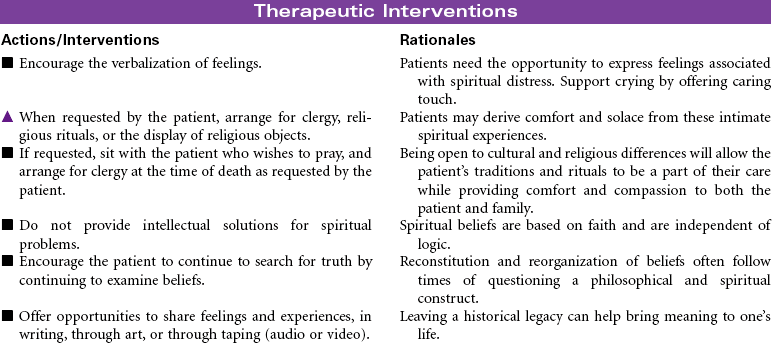
Death and Dying: End-of-Life Issues
Dying is part of living. It is an active process, but it is rare when we are able to mark the beginning or the middle of an individual’s dying. The end, of course, is death. There are individuals who report having come back from death and who have shared their memories of their experiences, but no one has been able to report on the state of actual death. Because death remains an unknown, it is a source of great mystery and endless speculation. Assisting patients and their families with making quality-of-life and end-of-life decisions to achieve a peaceful death is a daunting task for the health care professional in the context of the twenty-first century.
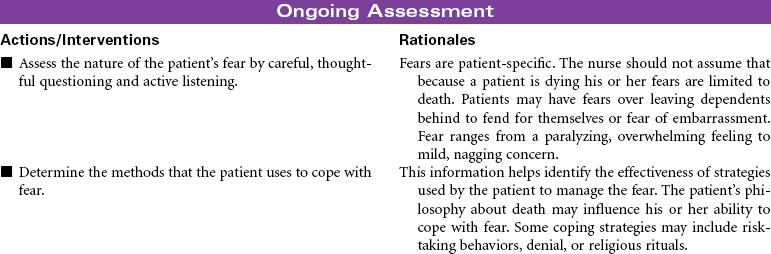
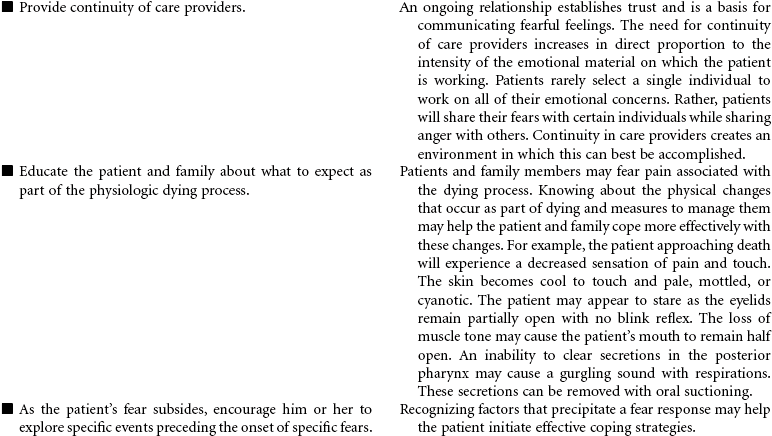
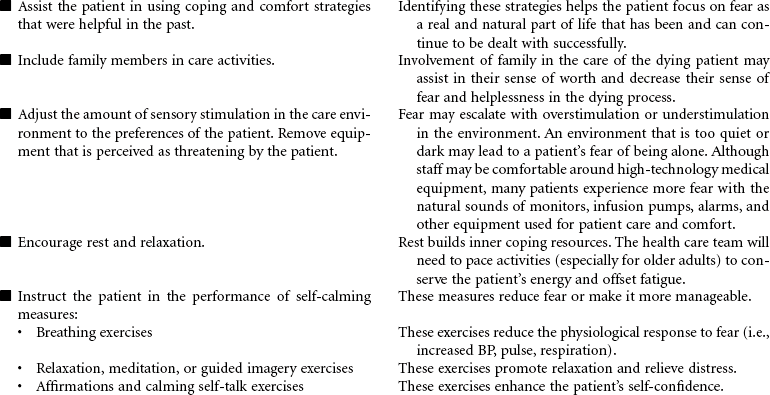
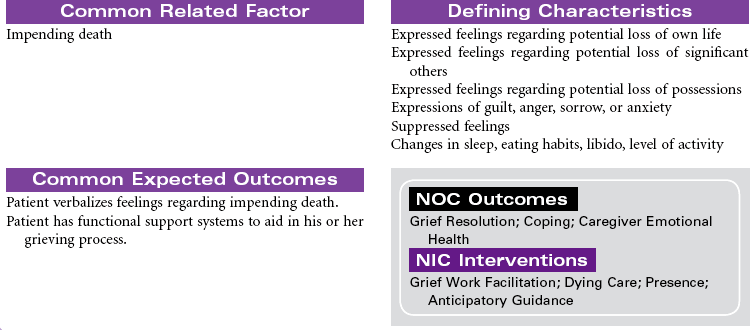
Still, much is known about dying. The process has been observed from time immemorial. Each person dies in his or her own way. This process is influenced by cultural norms, family traditions, and the people and setting among which a person’s death takes place. The patient at the end of life may experience both actual and anticipatory losses. Pain, diminished abilities, fear, discomfort, massive dysfunction of organ systems (with or without the application of ever more complicated measures to prolong life), and the resounding implications his or her death will have on others require the patient to integrate enormous amounts of information and undergo extraordinarily complicated emotions.
Health professionals who understand the inevitability of a patient’s death may seek to provide patients with an opportunity for a “good death,” or a positive dying experience. Although the characteristics of a good death will vary, most providers agree that patients should be allowed to die with dignity, surrounded by loved ones and free of pain, with everything having been done that could have been done. Caring for patients and their families or significant others at the end of life is the essence of nursing. Nurses experience a rich opportunity to observe the grace and goodness of the human spirit within those final hours. This care plan addresses the emotional aspects of death and dying in accordance with the Hospice and Palliative Nurses Association’s Statement on the Scope and Standards of Hospice and Palliative Nursing Practice.


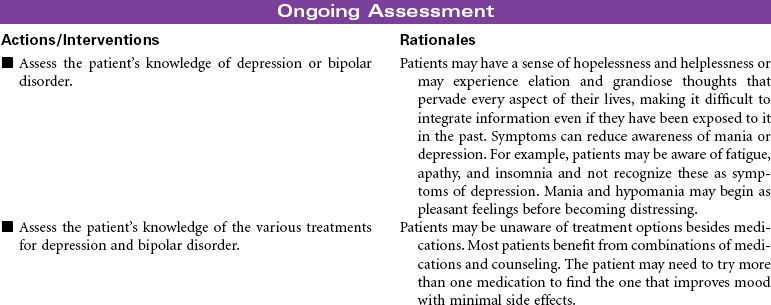
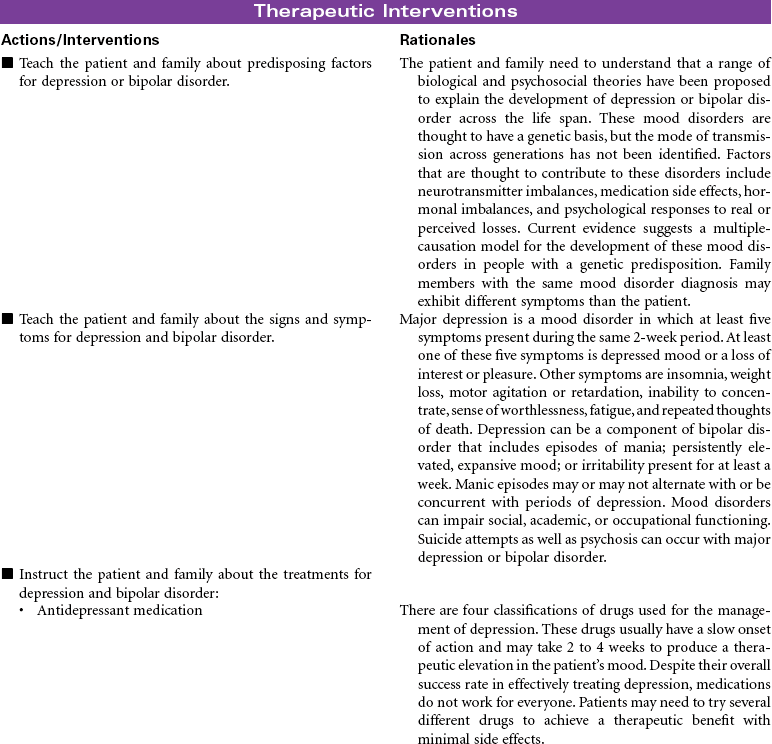
Common Mood Disorders: Depression and Bipolar Disorder
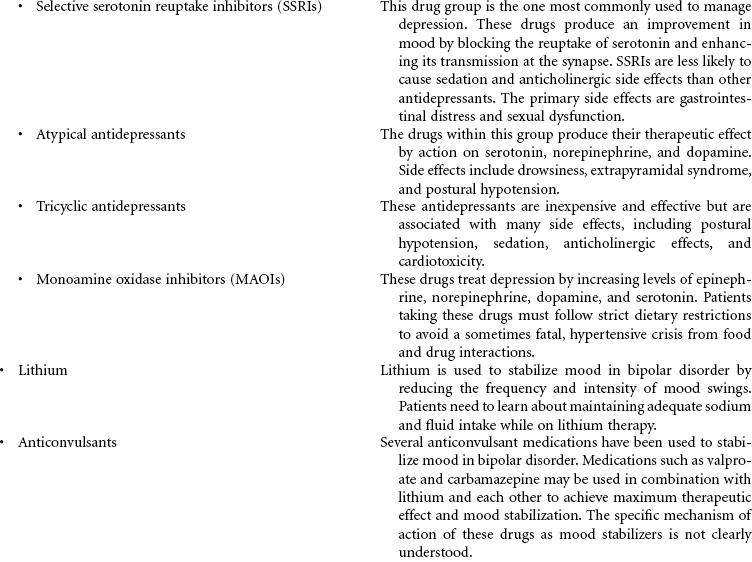
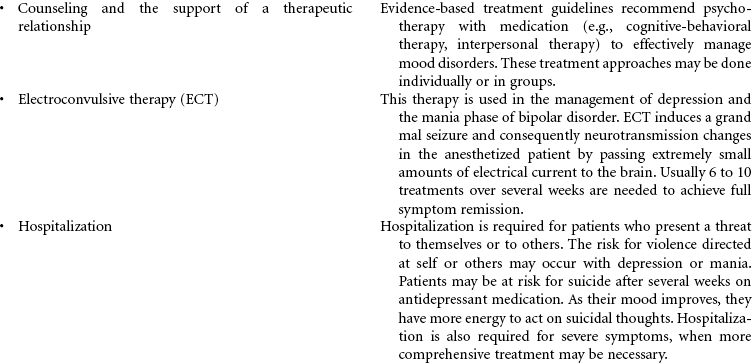
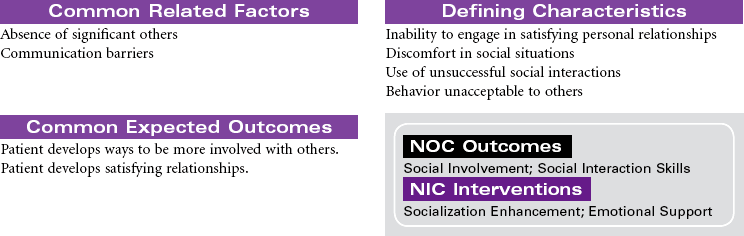
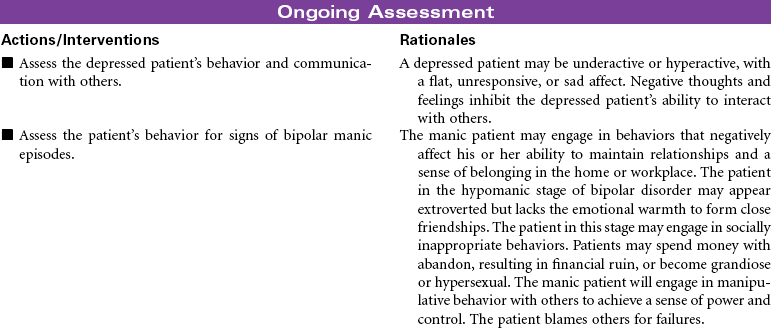
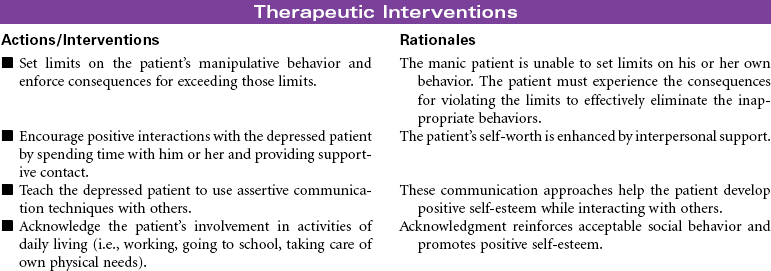
Depression is characterized by feelings of unworthiness, profound sadness, anxiety, apathy, and hopelessness. A loss of interest and pleasure in usual activities is common. Behavioral characteristics may include slowing of physical activity or agitation, unintentional weight loss, decreased ability to concentrate or problem-solve, and alterations in sleeping, eating, and libido. Depression is diagnosed more often in women than in men, but this is generally because women are more likely to seek health care, including treatment for depression. The incidence of depression in men is probably underreported. More men express symptoms with behaviors not generally associated with depression, such as substance abuse and gambling. Depression is a common disorder in the elderly. The manifestations of depression may be misinterpreted as symptoms of other disorders associated with aging. Every effort is made to stabilize and treat the depressed patient in an outpatient setting, but a strong indicator for hospitalization would be attempted suicide, active suicide intent, or impulsive suicidal behaviors. Bipolar disorder, also called manic-depressive illness, is a mood disorder that is characterized by shifts in the person’s mood, thinking, energy, and functional ability. The mood swings in bipolar disorder can range from severe depression to severe mania. Some patients with bipolar disorder may have a mixed bipolar state with symptoms of both mania and depression. Effective treatment can limit the frequency and intensity of mood swings. The common mood disorders have an impact not only on the patient but also on the patient’s family.
 Impaired Social Interaction
Impaired Social Interaction

For additional care plans and an Online Care Plan Constructor, go to http://evolve.elsevier.com/Gulanick/.