Nursing Diagnosis Care Plans
For additional care plans and an Online Care Plan Constructor, go to  at http://evolve.elsevier.com/Gulanick
at http://evolve.elsevier.com/Gulanick
 Activity Intolerance
Activity Intolerance
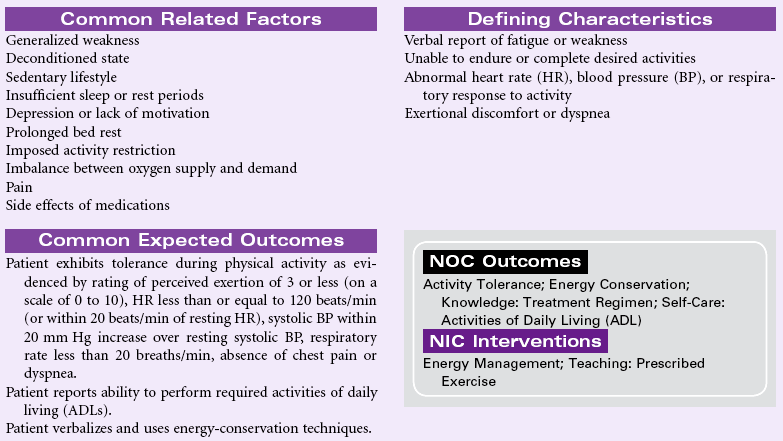
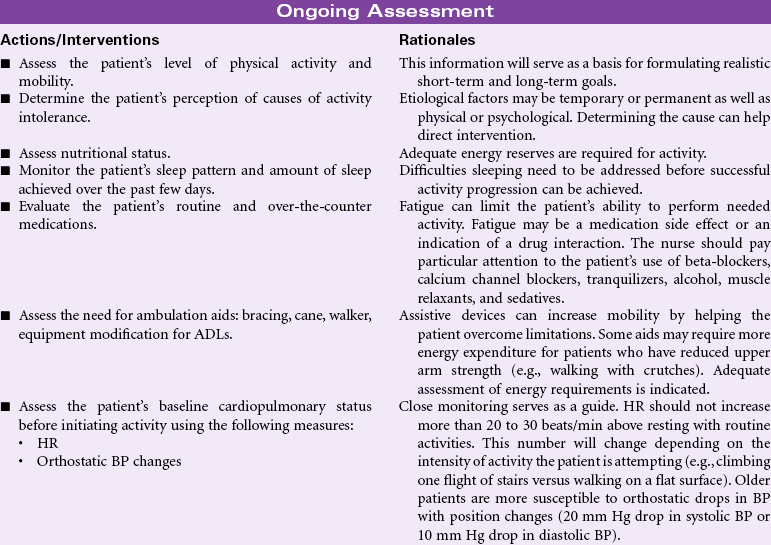
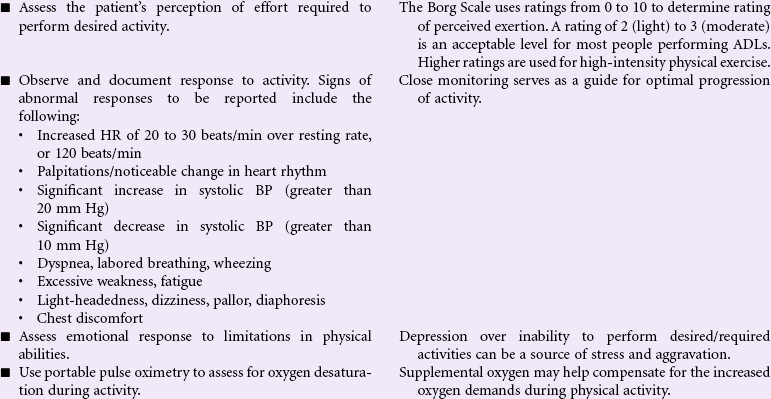
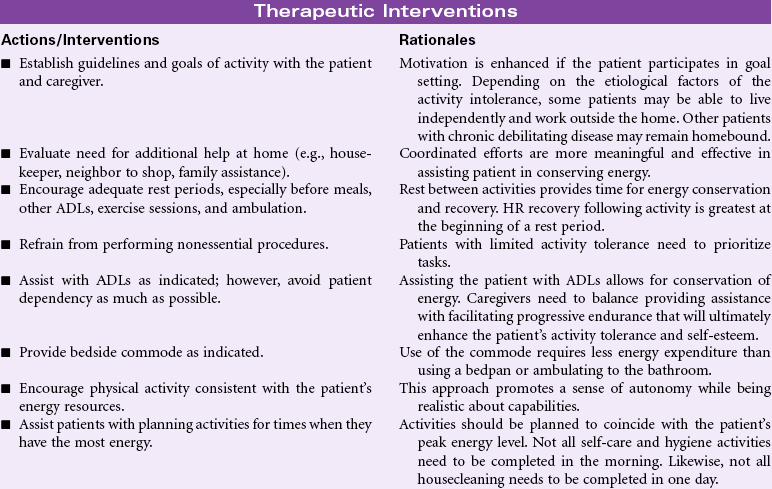
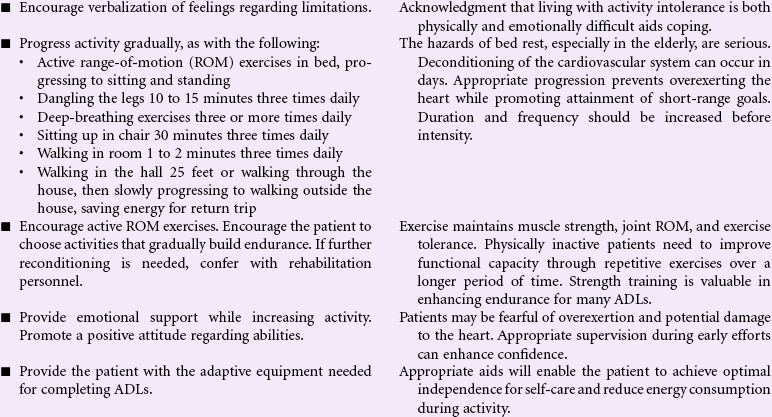
Definition: Insufficient physiological or psychological energy to endure or complete required or desired daily activities
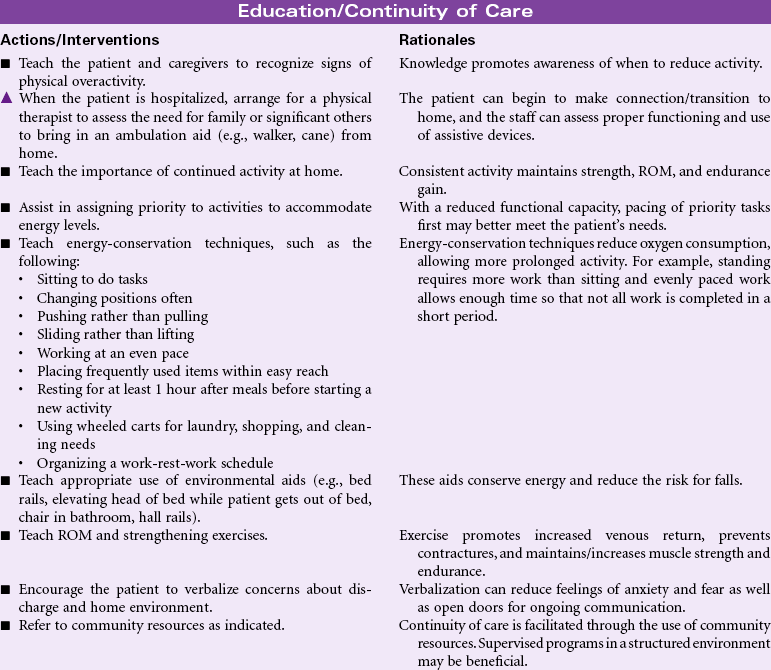
Most activity intolerance is related to generalized weakness and debilitation secondary to acute or chronic illness and disease. This is especially apparent in older patients with a history of orthopedic, cardiopulmonary, diabetic, or pulmonary-related problems. The aging process itself causes reduction in muscle strength and function, which can impair the ability to maintain activity. Activity intolerance may also be related to factors such as obesity, malnourishment, anemia, side effects of medications (e.g., beta-blockers), or emotional states (e.g., depression or lack of confidence to exert oneself). Nursing goals are to reduce the effects of inactivity, promote optimal physical activity, and assist the patient with maintaining a satisfactory quality of life.
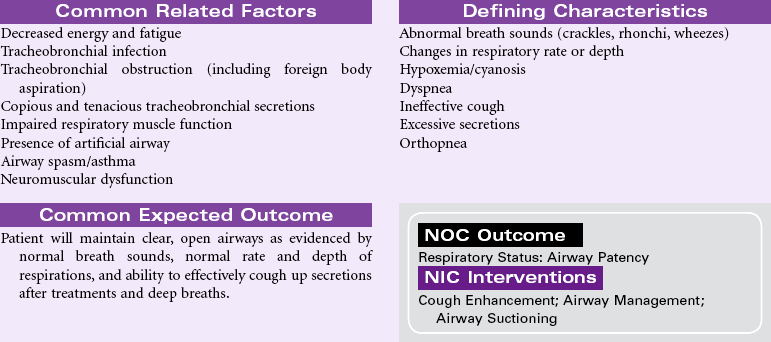
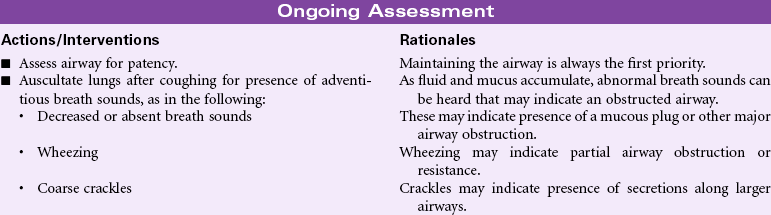
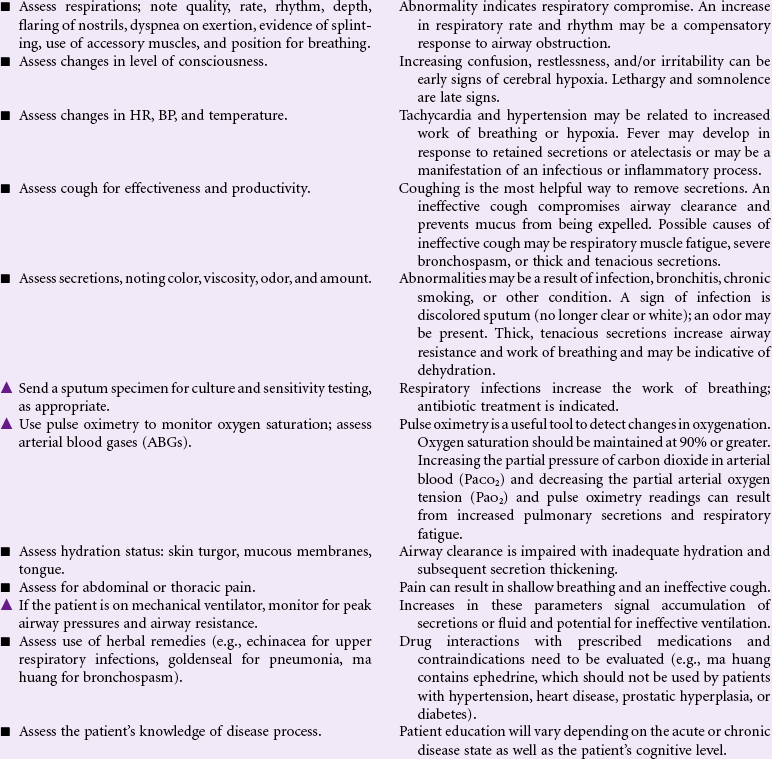
Ineffective Airway Clearance
Definition: Inability to clear secretions or obstructions from the respiratory tract to maintain a clear airway
Maintaining a patent airway is vital to life. Coughing is the main mechanism for clearing the airway. However, the cough may be ineffective in both normal and disease states secondary to factors such as pain from surgical incisions or trauma, respiratory muscle fatigue, or neuromuscular weakness. Other mechanisms that exist in the lower bronchioles and alveoli to maintain the airway include the mucociliary system, macrophages, and the lymphatics. Factors such as anesthesia and dehydration can affect function of the mucociliary system. Likewise, conditions that cause increased production of secretions (e.g., pneumonia, bronchitis, chemical irritants) can overtax these mechanisms. Ineffective airway clearance can be an acute (e.g., postoperative recovery) or chronic (e.g., from cerebrovascular accident [CVA] or spinal cord injury) problem. Older patients, who have an increased incidence of emphysema and a higher prevalence of chronic cough or sputum production, are at high risk.


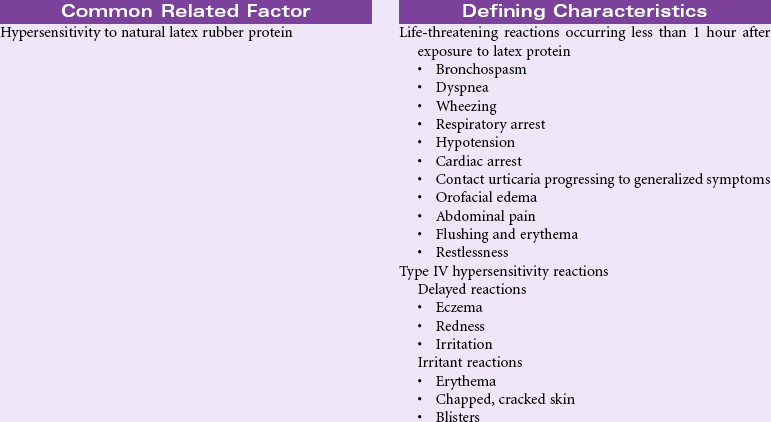
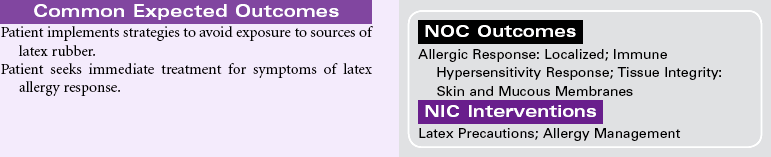
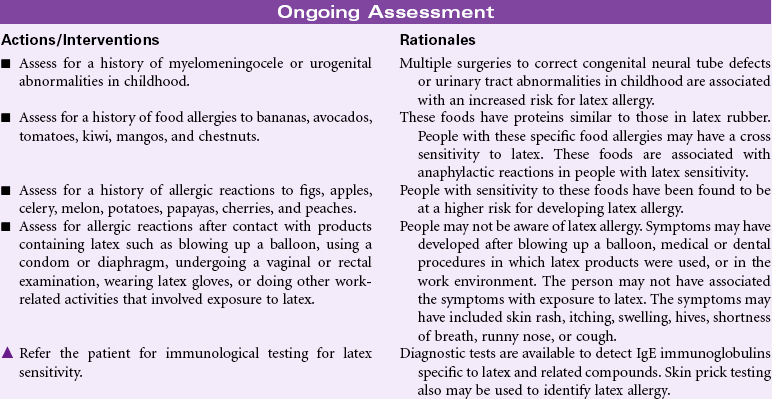
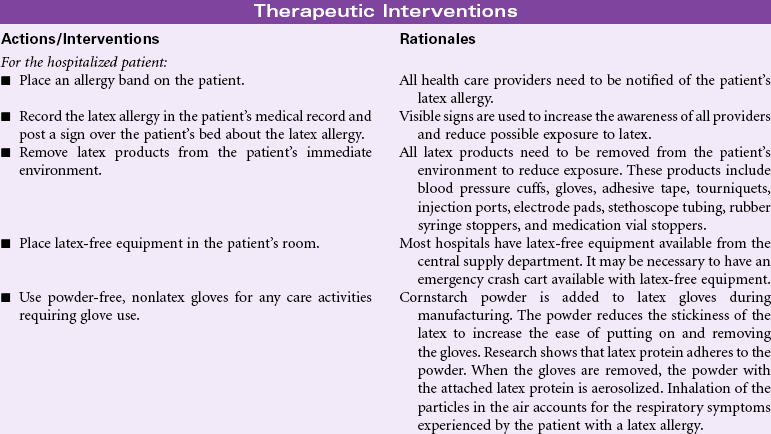
Latex Allergy Response
Definition: A hypersensitive reaction to natural latex rubber products
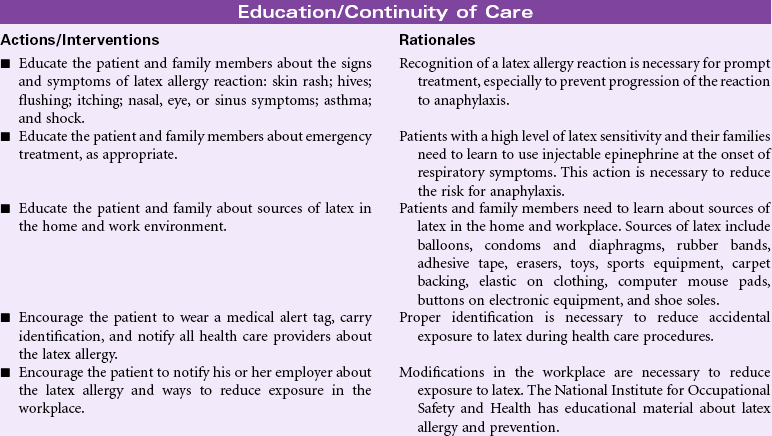
Latex allergy is a hypersensitivity reaction to the proteins in natural rubber latex derived from the sap of the rubber tree, Hevea brasiliensis. Products made from synthetic rubber may be called latex but do not contain the proteins known to cause an allergic response. The incidence of latex allergy increased after 1985 with the introduction of standard precautions to prevent the spread of bloodborne pathogens such as the human immunodeficiency virus. Soft rubber products such as gloves have the highest content of latex protein and the most potential to cause an allergic response. The people at highest risk for latex allergy include those who wear latex gloves as part of their jobs, such as health care workers, food service workers, housekeepers, and hairdressers. People employed in industries that manufacture latex rubber products are at risk, too. Another group of people at risk are those who undergo repeated surgeries, especially if the surgeries begin in childhood. Evidence indicates a high incidence of latex allergy in people with spina bifida who have had multiple surgeries in childhood. People with a variety of food allergies and sensitivities also have increased risk for latex allergy. Natural latex rubber allergies are IgE-mediated reactions to at least 10 different low-molecular-weight, water-soluble proteins contained in the rubber tree sap. The range of hypersensitivity reactions to latex rubber includes mild to severe contact dermatitis, respiratory allergic symptoms, and anaphylaxis.
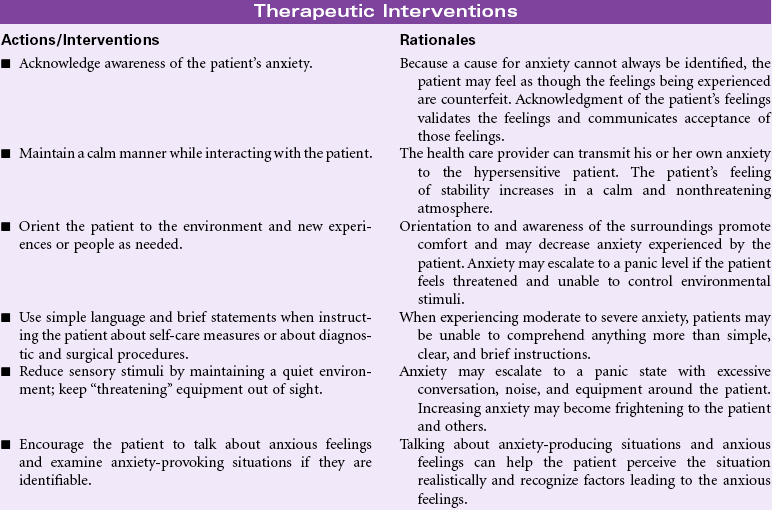
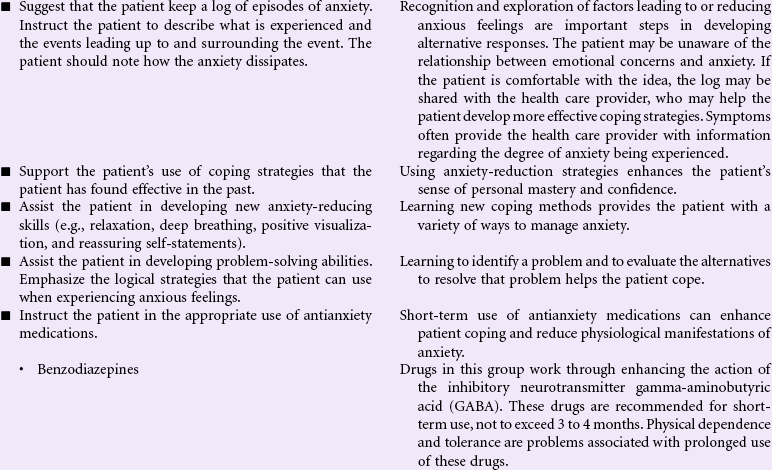
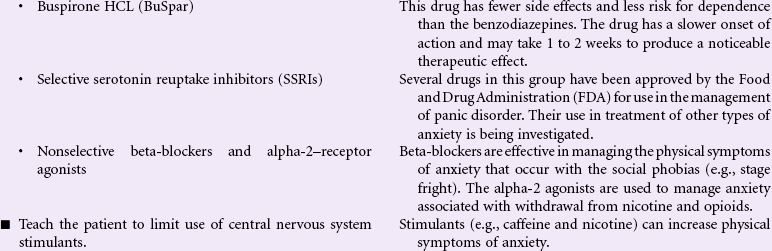
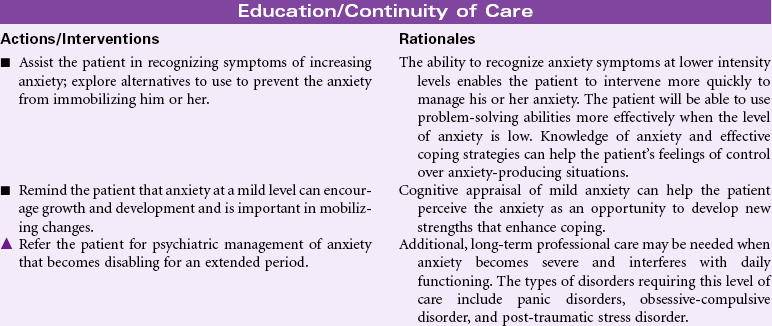
Anxiety
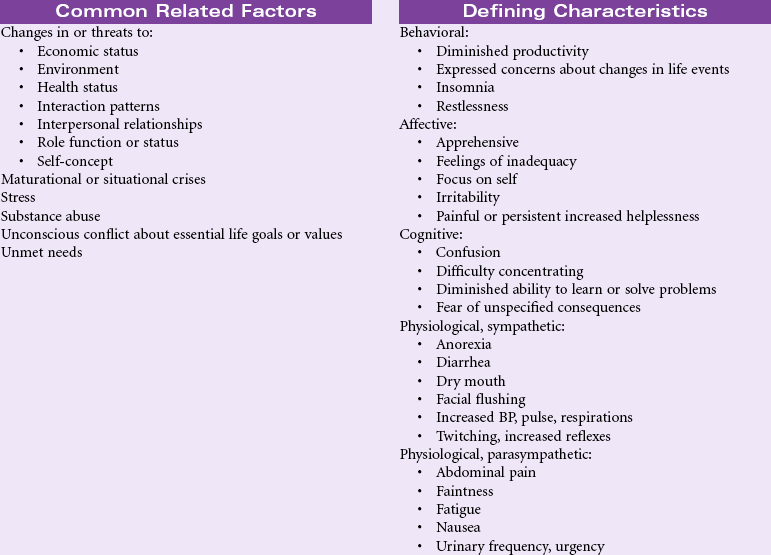
Definition: Vague, uneasy feeling of discomfort or dread accompanied by an autonomic response (the source often nonspecific or unknown to the individual); a feeling of apprehension caused by anticipation of danger. It is an alerting signal that warns of impending danger and enables the individual to take measures to deal with the threat.
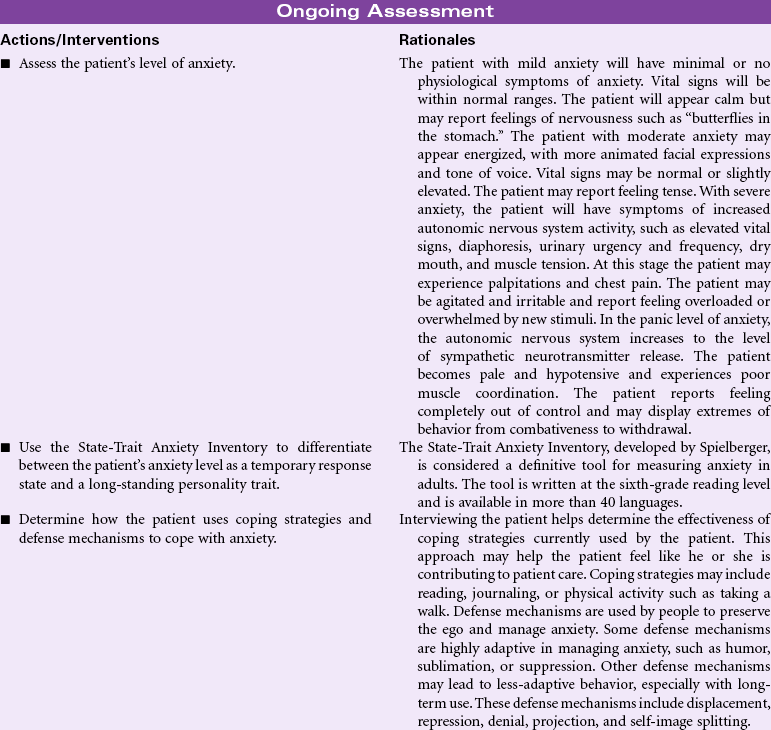
Anxiety represents an emotional response to environmental stressors and is therefore part of the person’s stress response. Each individual’s experience with anxiety is different. Some people are able to use the emotional edge that anxiety provokes to stimulate creativity or problem-solving abilities; others can become immobilized to a pathological degree. These pathological anxiety disorders include panic attacks, social phobias, specific phobias, obsessive-compulsive disorder, and post-traumatic stress disorder. Anxiety is generally categorized into four levels: mild, moderate, severe, and panic. Mild anxiety can enhance a person’s perception of the environment and readiness to respond. Moderate anxiety is associated with a narrowing of the person’s perception of the situation. The person with moderate anxiety may be more creative and more effective in solving problems. Severe anxiety is associated with increasing emotional and physical feelings of discomfort. Perceptions are further narrowed. The person with severe anxiety begins to manifest excessive autonomic nervous system signs of the fight-or-flight stress response. The person in a panic stage of anxiety has distorted perceptions of the situation. His or her thinking skills become limited and irrational. The person may be unable to make decisions. In the severe and panic stages of anxiety, the nurse needs to intervene to promote patient safety. The nurse can encounter the anxious patient anywhere in the hospital or community. The presence of the nurse may lend support to the anxious patient and provide strategies for effectively coping with anxious moments or panic attacks.
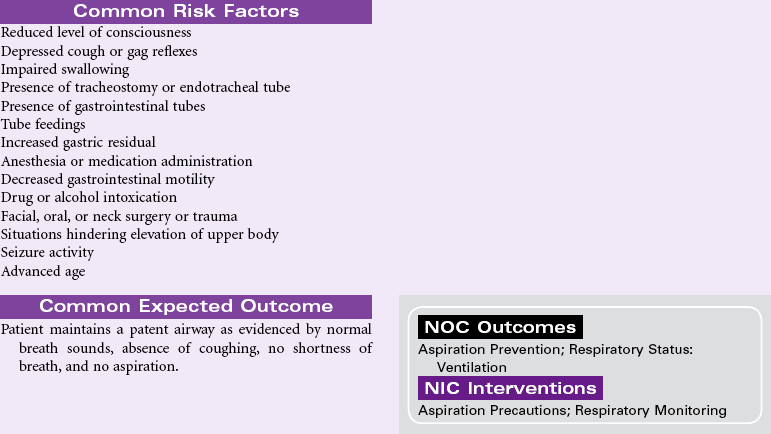
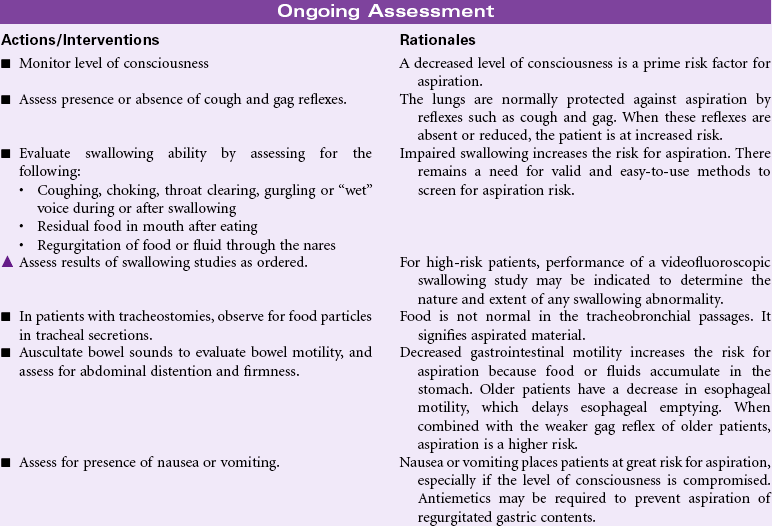
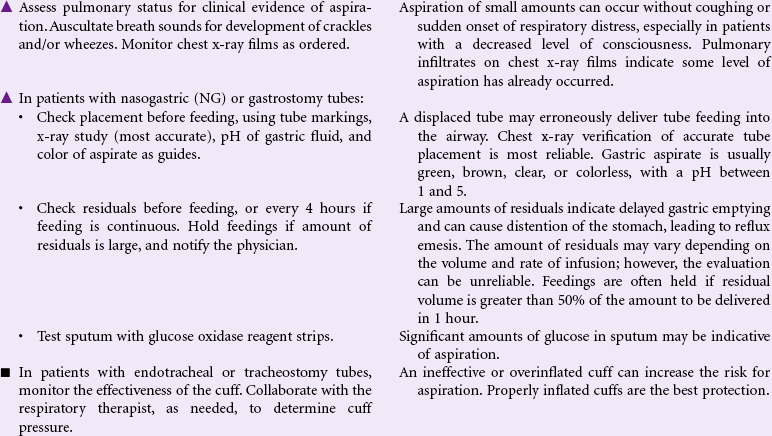
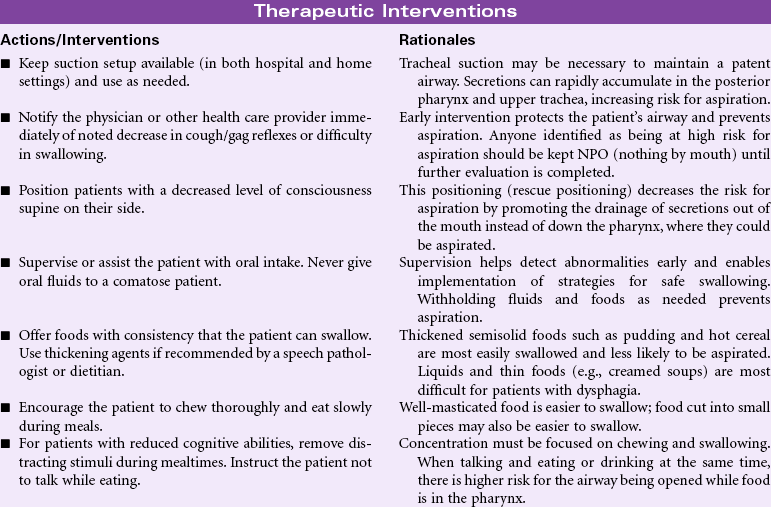
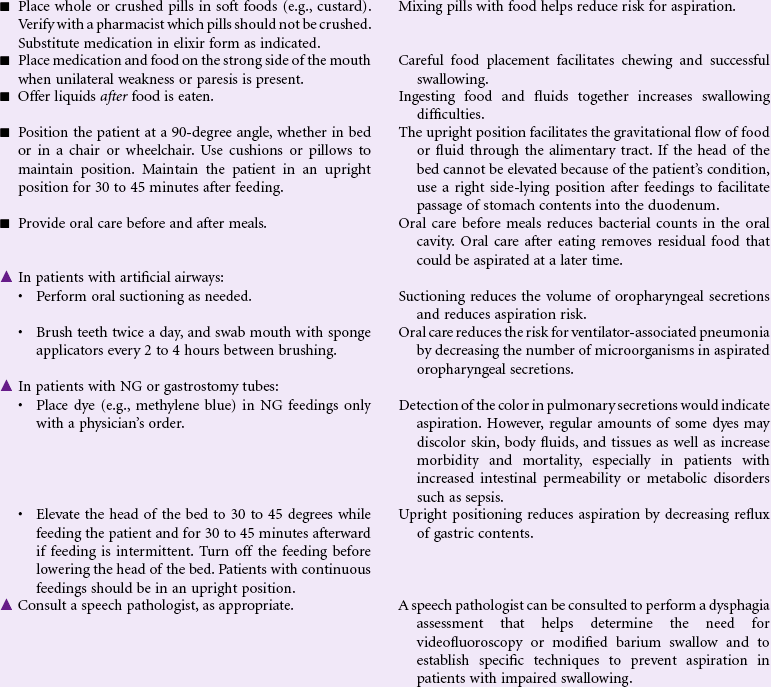
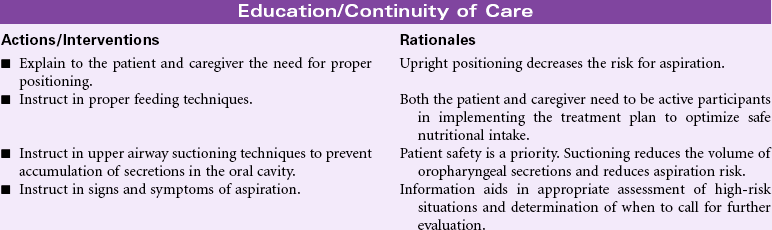
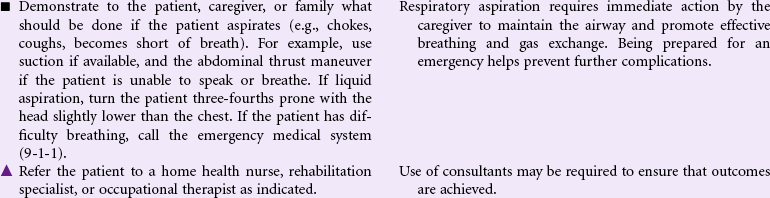
Risk for Aspiration
Definition: At risk for entry of gastrointestinal secretions, oropharyngeal secretions, solids, or fluids into tracheobronchial passages
Aspiration is the entry of secretions or materials such as foods or liquids into the trachea and lungs and occurs when protective reflexes are decreased or compromised. Aspiration from the oropharynx into the lungs can result in aspiration pneumonia. Depending on the acidity of the aspirate, even small amounts of gastric acid contents can damage lung tissue, resulting in chemical pneumonitis. Both acute and chronic conditions can place patients at risk for aspiration. Acute conditions, such as postanesthesia effects from surgery or diagnostic tests, occur predominantly in the acute care setting. Chronic conditions, including altered consciousness from head injury, spinal cord injury, neuromuscular weakness, hemiplegia and dysphagia from stroke, use of tube feedings for nutrition, and artificial airway devices such as tracheostomies, may be encountered in the home, rehabilitative, or hospital setting. Older and cognitively impaired patients are at high risk. Aspiration is a common cause of death in comatose patients. The National Quality Forum recommends that every patient should be evaluated for aspiration risk upon admission and periodically during the patient’s stay.
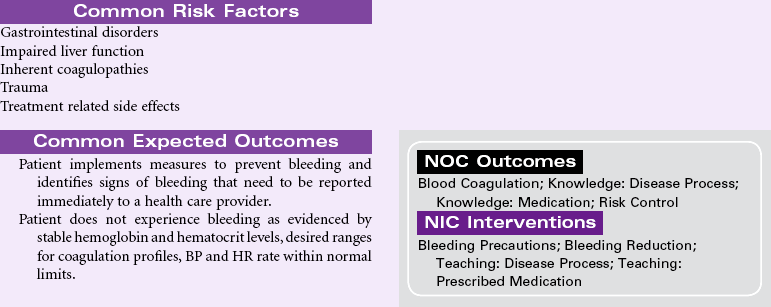
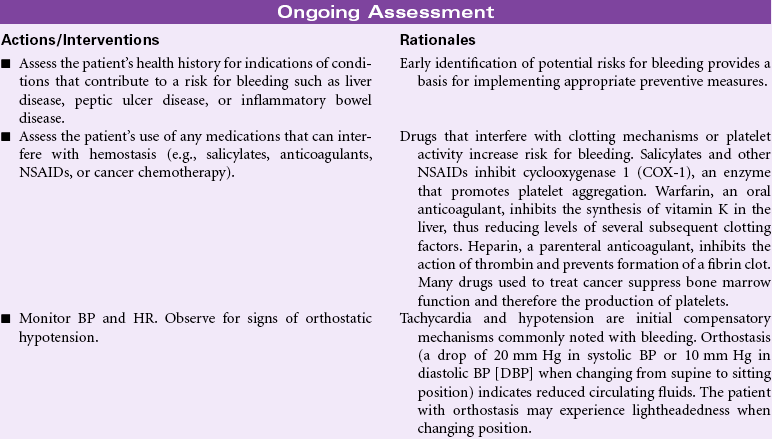
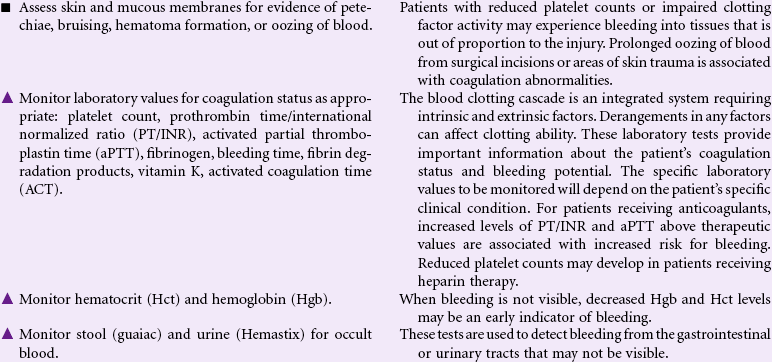
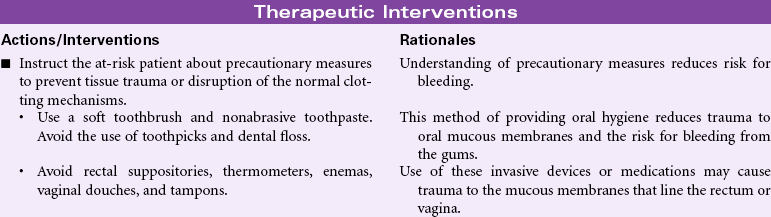
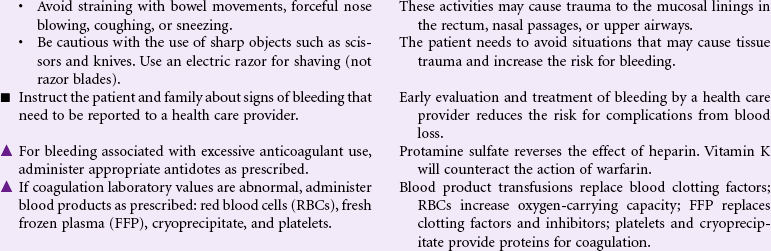
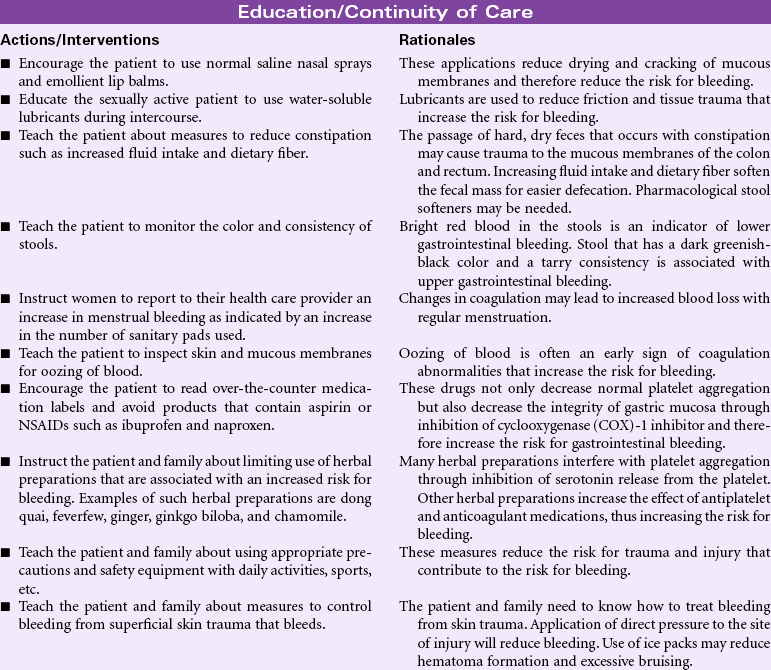
Risk for Bleeding
Definition: At risk for a decrease in blood volume that may compromise health
A patient may experience bleeding when disease or the effects of disease treatments disrupt the normal mechanisms that support hemostasis. Some diseases such as hemophilia interfere with genetic expression of normal clotting factors. Risk for bleeding occurs with disorders that decrease the quantity or quality of circulating platelets (thrombocytopenia). Cancers of the blood and blood-forming organs are associated with a decrease in production of platelets from the bone marrow. Immune thrombocytopenic purpura (ITP) is associated with increased destruction of platelets. Impaired liver function leads to a decrease in the synthesis of clotting factors. Any condition that disrupts the “closed circuit” integrity of the circulatory system increases the risk for bleeding. Examples of these conditions include major organ surgery, traumatic injury, and the many inflammatory or ulcerative disorders of the gastrointestinal system, (e.g., peptic ulcer disease, inflammatory bowel disease). Drugs that suppress bone marrow function or interfere with the action of normal clotting factors increases the patient’s risk for bleeding as a side effect. These drugs include anticoagulants, nonsteroidal anti-inflammatory drugs (NSAIDs), and cancer chemotherapy agents. Herbal preparations may contribute to risk for bleeding through direct effect on clotting factors or interactions with anticoagulants.
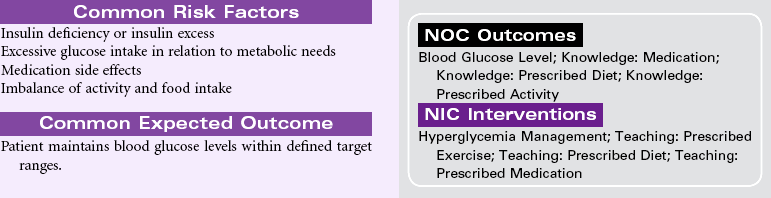
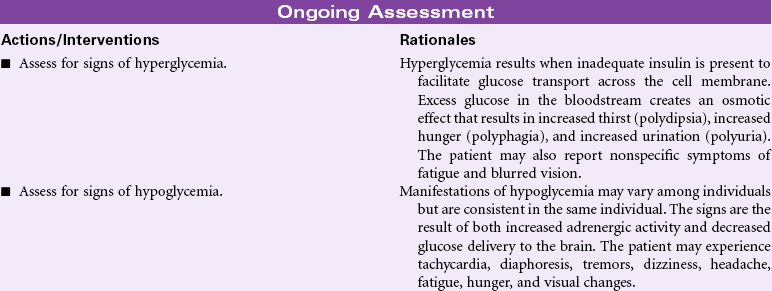
Risk for Unstable Blood Glucose Level
Definition: Risk for variation of blood glucose/sugar levels from the normal range
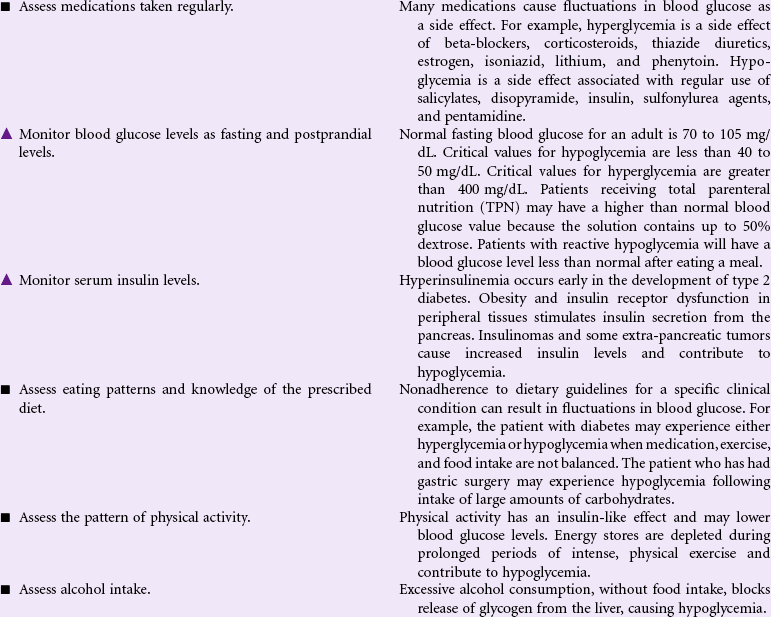
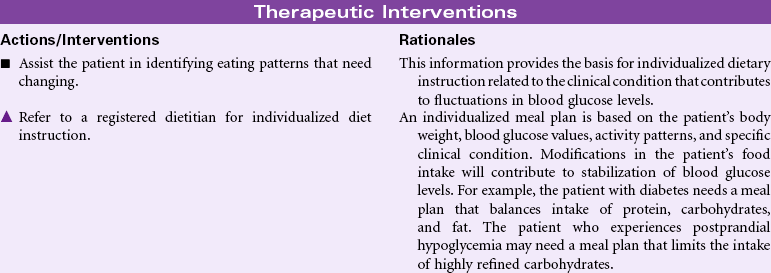
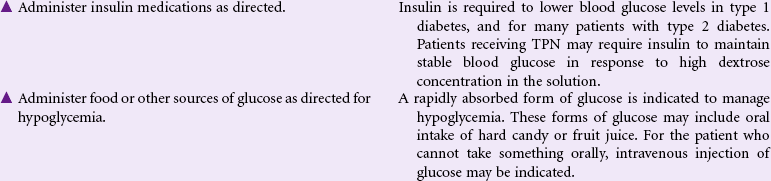
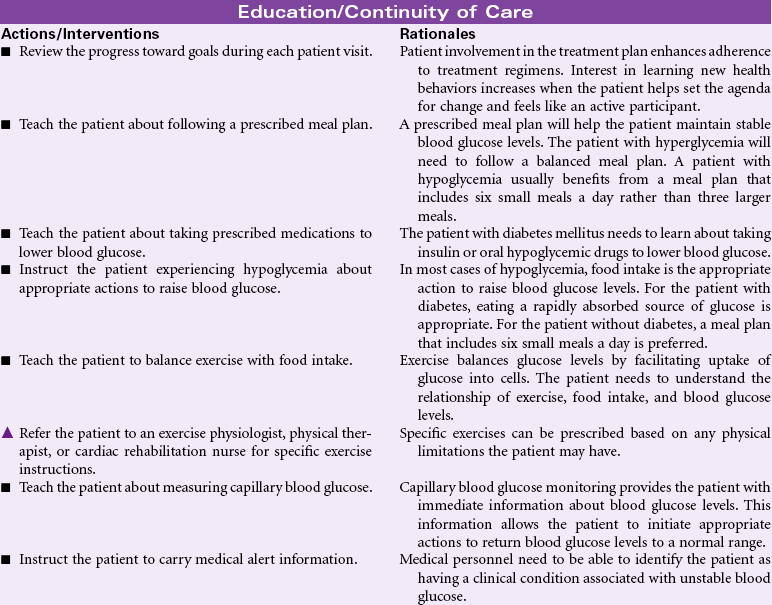
Serum glucose is regulated by a complex interaction of insulin and glucagon. Insulin is secreted by the beta cells of the islets of Langerhans in the pancreas in response to elevated levels of blood glucose. This pancreatic hormone facilitates the movement of glucose across the cell membranes to be used for metabolic activity. The alpha cells of the islets of Langerhans secrete glucagon when blood glucose levels are low. Glucagon facilitates the conversion of stored glycogen to glucose. When cells are unable to use blood glucose as a metabolic fuel, glucagon stimulates the breakdown of fatty acids and protein. Elevated blood glucose levels (hyperglycemia) may occur in a variety of clinical situations. Diabetes mellitus is the most common disorder associated with elevated blood glucose levels. Prolonged physiological stress contributes to hyperglycemia through increased levels of cortisol as part of the neuro-endocrine stress response. Intravenous infusions containing dextrose may cause elevated blood glucose. Many drugs have hyperglycemia as a side effect.
Hypoglycemia occurs most often as the result of excess insulin administration in the person with diabetes mellitus. In the person without diabetes, hypoglycemia may occur with excess alcohol consumption, prolonged fasting and starvation states, adrenal insufficiency, and eating disorders such as anorexia nervosa. Hypoglycemia after meals may be related to gastric bypass surgery or excess consumption of refined carbohydrates and is the result of increased insulin secretion. This care plan focuses on general nursing care for the person who experiences fluctuations in blood glucose.
Disturbed Body Image
Definition: Confusion in mental picture of one’s physical self
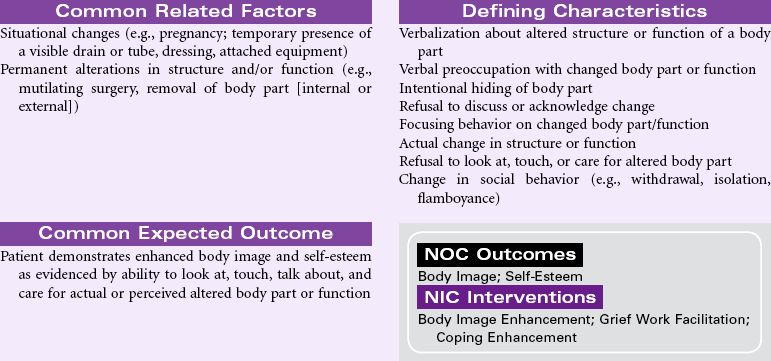
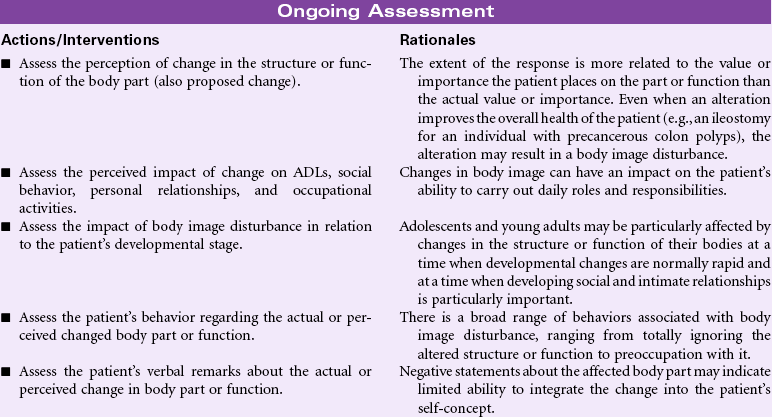
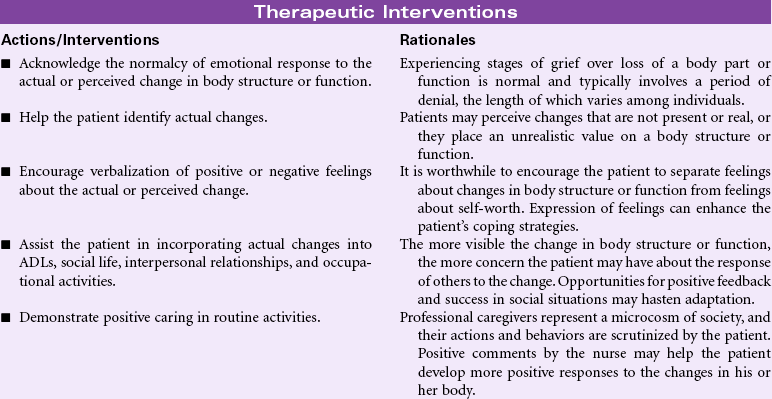
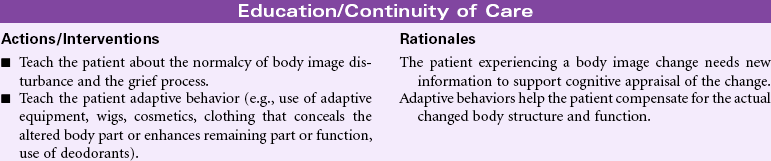
Body image is the attitude a person has about the actual or perceived structure or function of all or parts of his or her body. This attitude is dynamic and is altered through interaction with other people and situations, and it is influenced by age and developmental level. As an important part of one’s self-concept, body image disturbance can have a profound impact on how individuals view their overall selves.
Throughout the life span, changes in a person’s body related to normal growth and development can result in changes in the person’s body image. For example, a woman may experience disturbed body image during pregnancy. Physical changes associated with aging may result in body image disturbance for the older adult.
Societal and cultural norms for ideal body shape, size, and appearance have a significant influence on a person’s body image. Variations from the norm can result in body image disturbance. The value that an individual places on a body part or function may be more important in determining the degree of disturbance than the actual alteration in the structure or function. Therefore the loss of a limb may result in a greater body image disturbance for an athlete than for a computer programmer. The loss of a breast to a fashion model or a hysterectomy in a nulliparous woman may cause serious body image disturbances even though the overall health of the individual has been improved. Removal of skin lesions, altered elimination resulting from bowel or bladder surgery, and head and neck resections are other examples that can lead to body image disturbance. Chronic illness can contribute to changes in the person’s body image related to decline in body function.
The nurse’s assessment of the perceived alteration and importance placed by the patient on the altered structure or function will be very important in planning care to address body image disturbance.

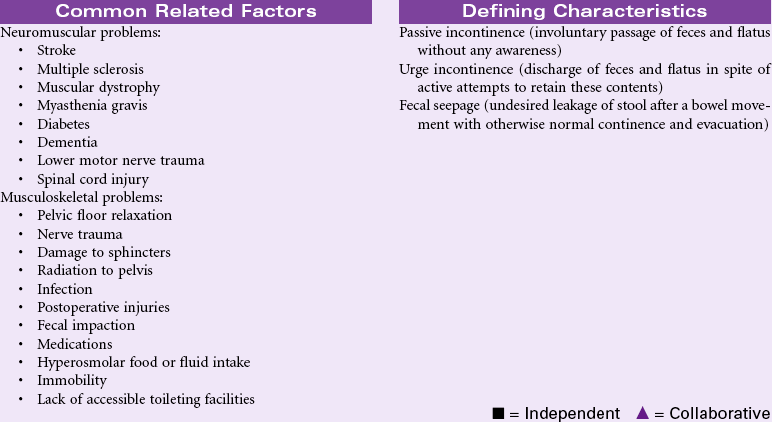
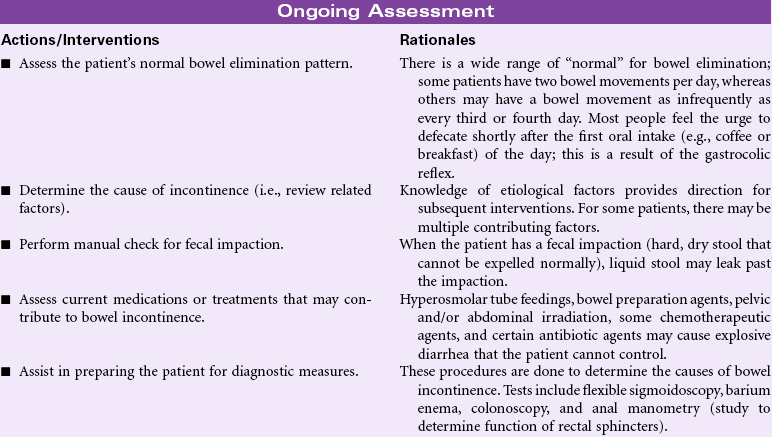
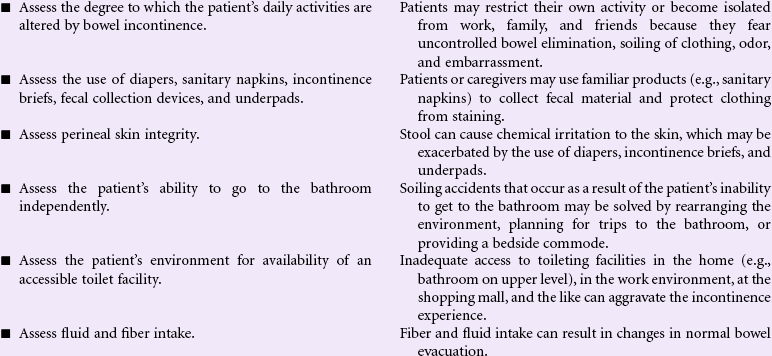
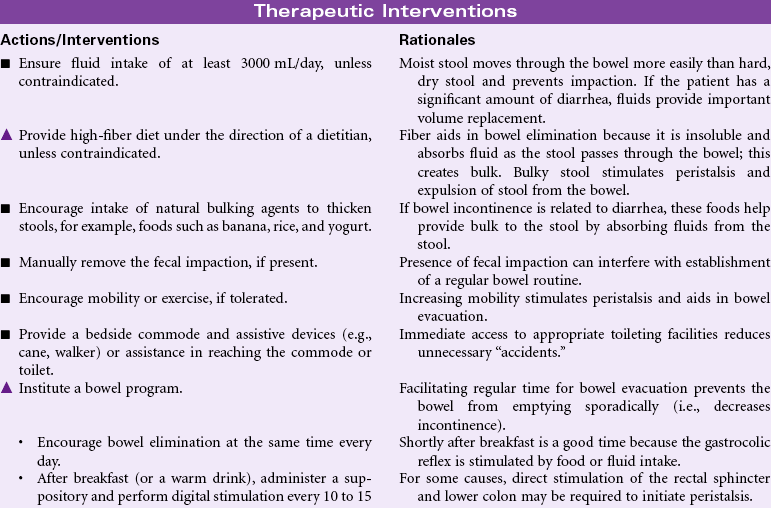
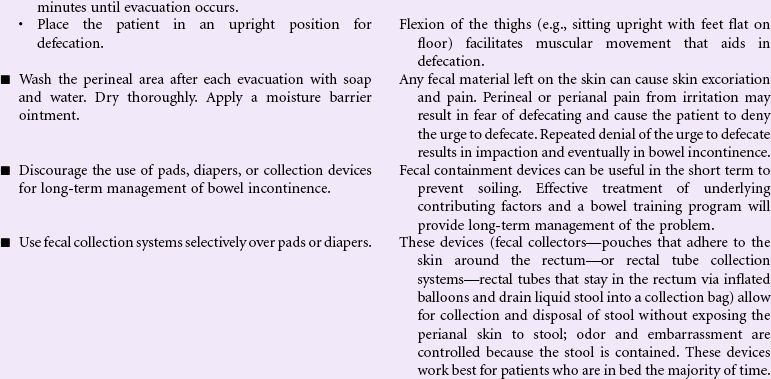
Bowel Incontinence
Definition: Change in normal bowel habits characterized by involuntary passage of stool
Bowel incontinence, also called fecal incontinence, may occur as a result of injury to nerves and other structures involved in normal defecation or as the result of diseases that alter the normal function of defecation. Treatment of bowel incontinence depends on the cause. Injury to rectal, anal, or nerve tissue from trauma, childbirth, radiation, or surgery, can result in bowel incontinence. Infection with resultant diarrhea or neurological disease such as stroke, multiple sclerosis, and diabetes mellitus can also result in bowel incontinence. In older patients, dementia can contribute to bowel incontinence when the individual cannot respond to normal physiological cues for defecation. Normal aging causes changes in the intestinal musculature that may contribute to bowel incontinence. Fecal impaction, as a result of chronic constipation or denial of the defecation urge, can result in involuntary leakage of stool past the impaction. Loss of mobility can result in functional bowel incontinence when the person is unable to reach the toilet in a timely manner. Loss of bowel continence is an embarrassing problem that leads to social isolation, and it is one of the most common reasons that older patients are admitted to long-term care facilities. Goals of management include reestablishing a continent bowel elimination pattern, preventing loss of skin integrity, and/or planning management of fecal incontinence in a manner that preserves the individual’s self-esteem.


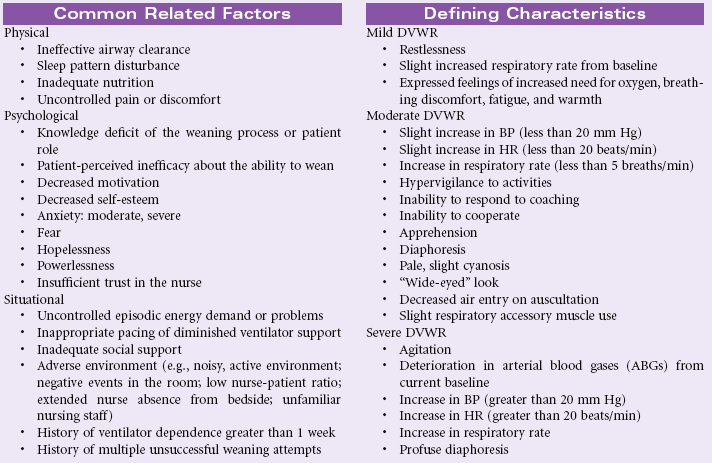
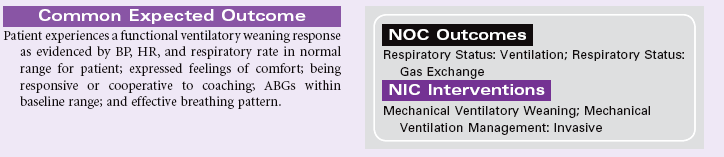
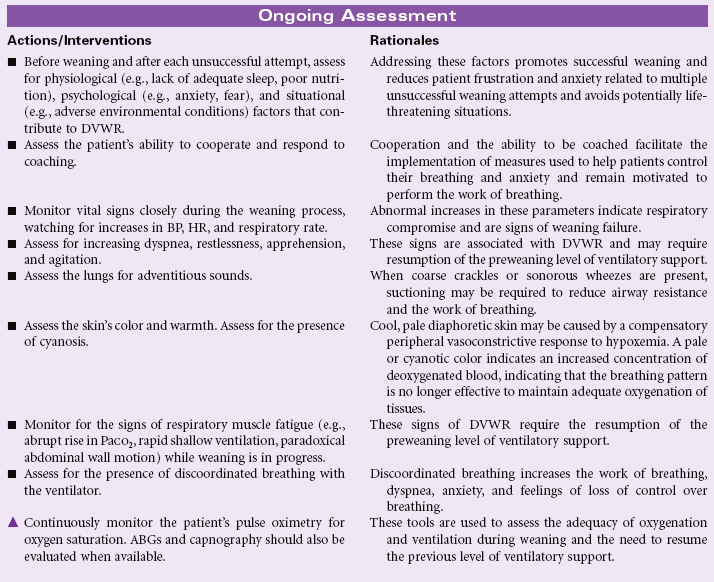
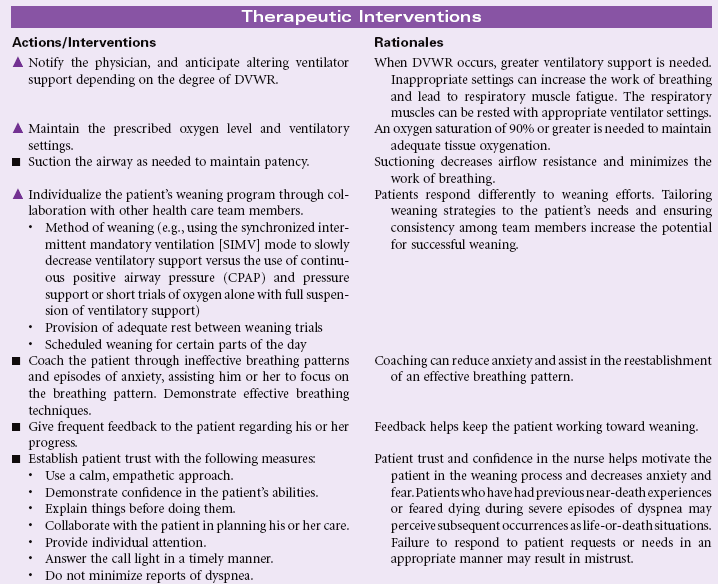
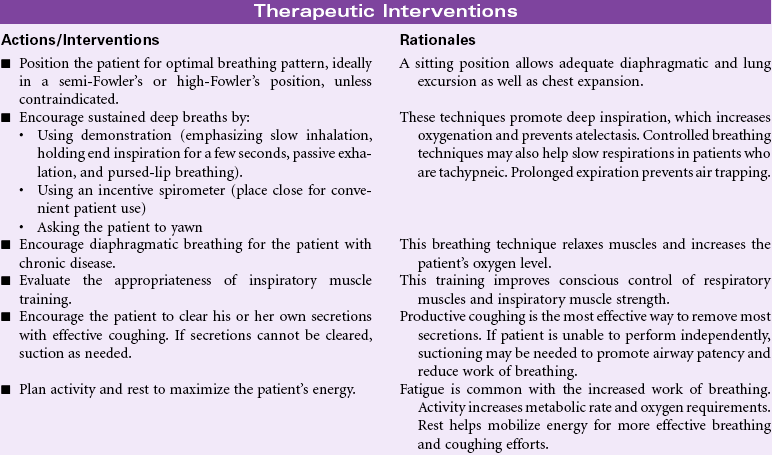
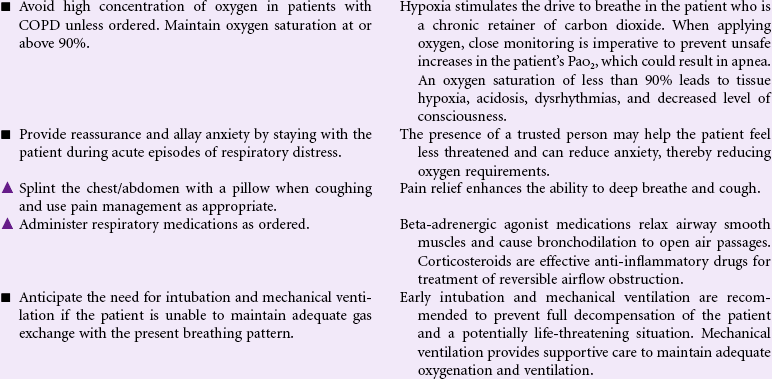
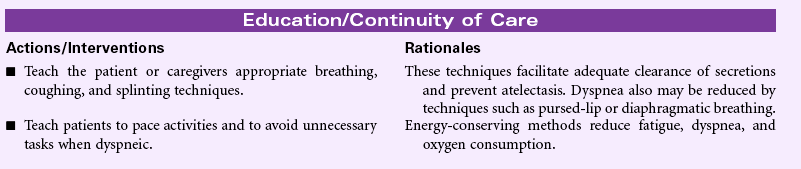
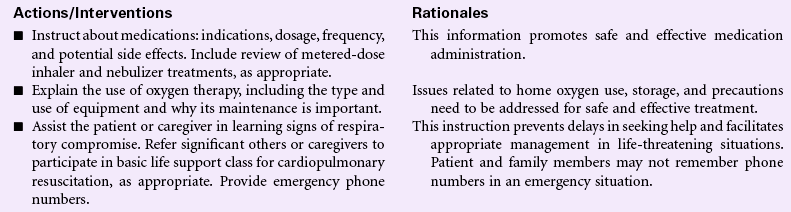
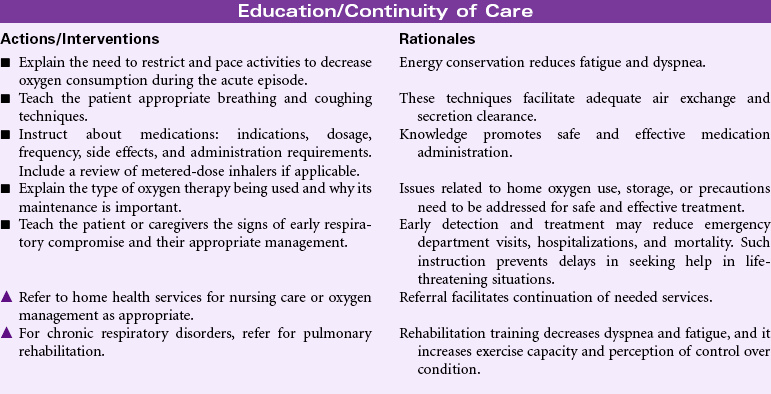
Ineffective Breathing Pattern
Definition: Inspiration and/or expiration that does not provide adequate ventilation
Ineffective breathing patterns are considered a state in which the rate, depth, timing, rhythm, or chest/abdominal wall excursion during inspiration, expiration, or both do not maintain optimum ventilation for the individual. Most acute pulmonary deterioration is preceded by a change in breathing pattern. Respiratory failure may be associated with changes in respiratory rate, abdominal and thoracic patterns for inspiration and expiration, and in depth of ventilation. Breathing pattern changes may occur in a multitude of conditions: heart failure, airway obstruction, respiratory infection, neuromuscular impairment, trauma or surgery resulting in musculoskeletal impairment/pain, diaphragmatic paralysis, cognitive impairment and anxiety, metabolic abnormalities (e.g., diabetic ketoacidosis, uremia, or thyroid dysfunction), peritonitis, drug overdose, pleural inflammation, and chronic respiratory disorders such as asthma or chronic obstructive pulmonary disease (COPD).
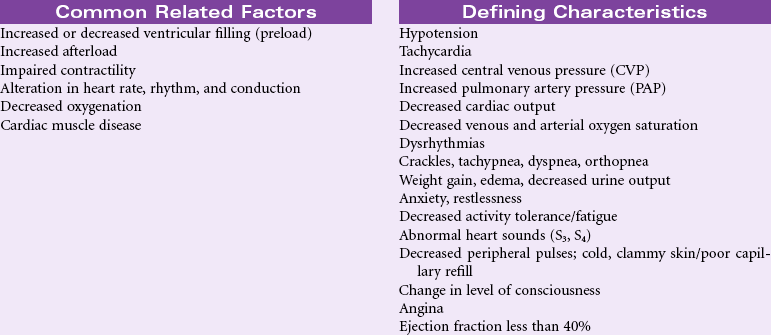
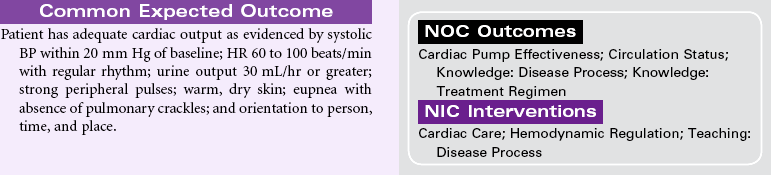
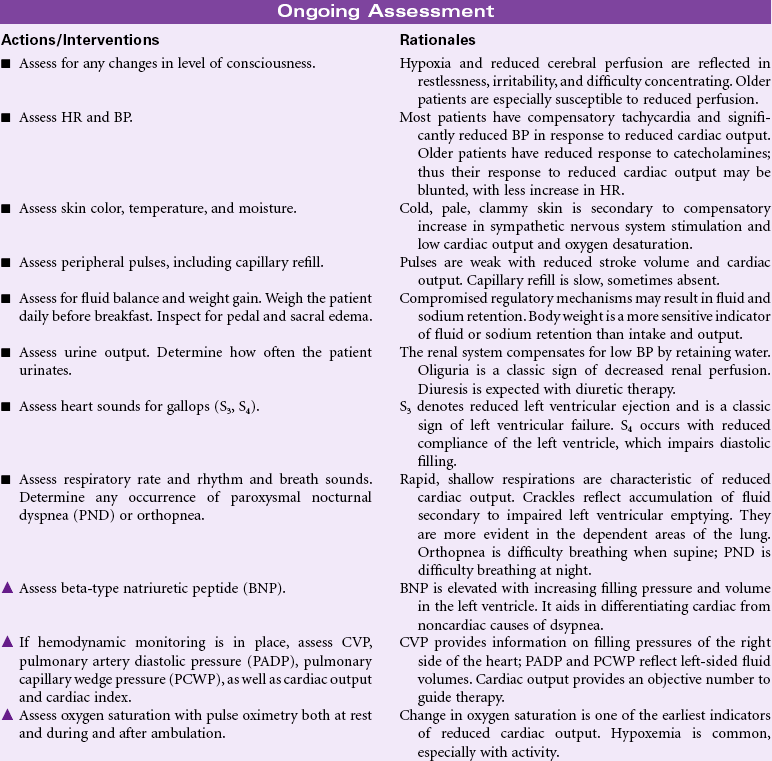
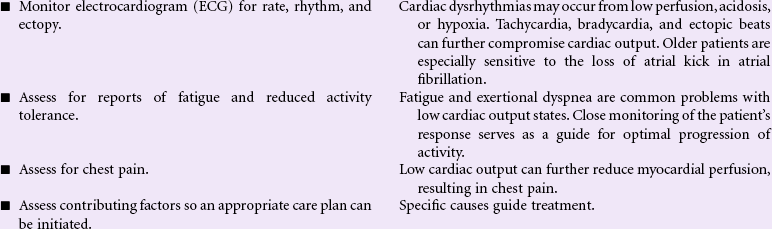
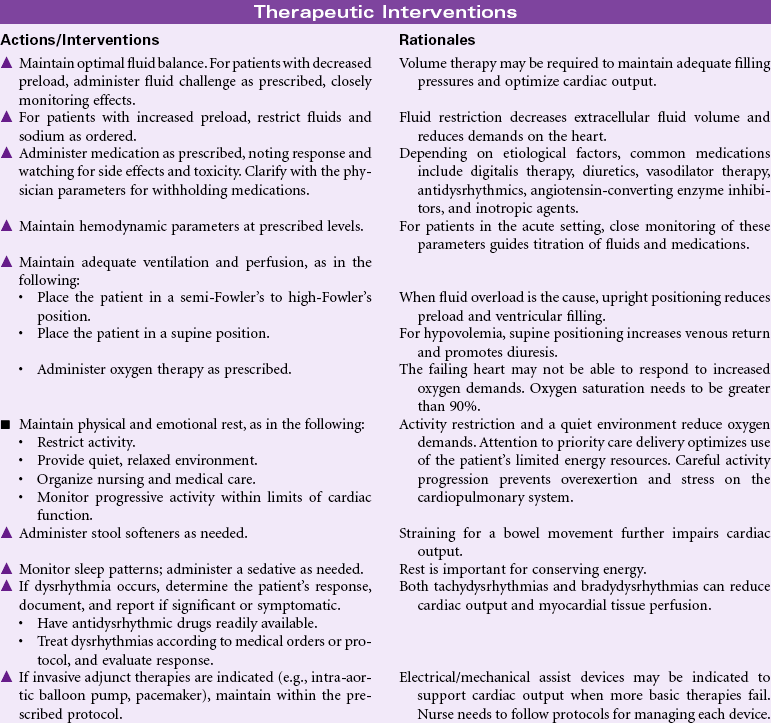
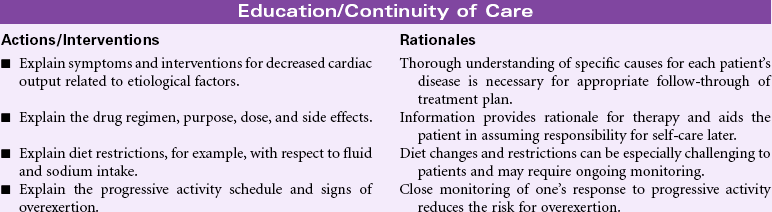
Decreased Cardiac Output
Definition: Inadequate blood pumped by the heart to meet the metabolic demands of the body
Common causes of reduced cardiac output include myocardial infarction, hypertension, valvular heart disease, congenital heart disease, cardiomyopathy, pulmonary disease, arrhythmias, drug effects, fluid overload, decreased fluid volume, and electrolyte imbalance. Older patients are especially at risk because the aging process causes reduced compliance of the ventricles, which further reduces contractility and cardiac output. Patients may have acute, temporary problems or experience chronic, debilitating effects of decreased cardiac output. Patients may be managed in an acute care, ambulatory care, or home care setting.
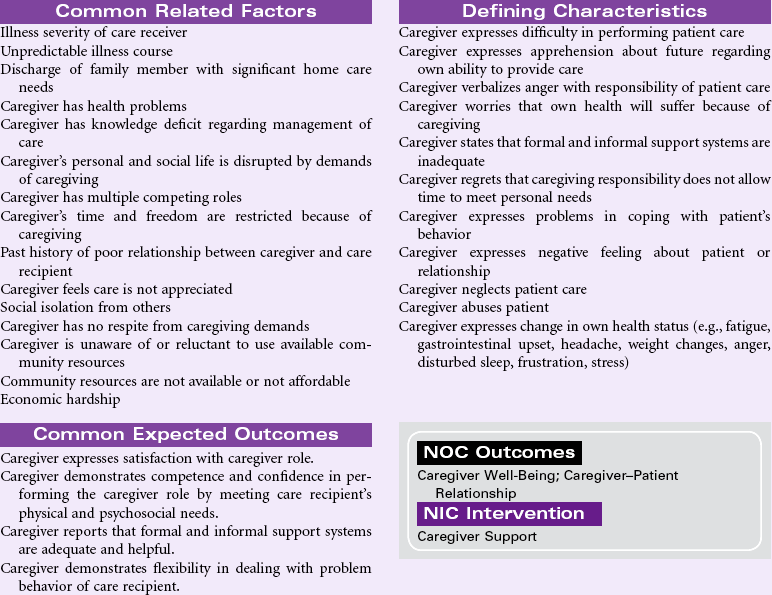
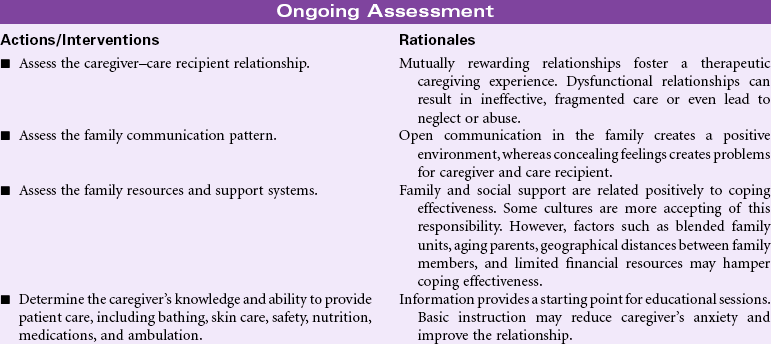
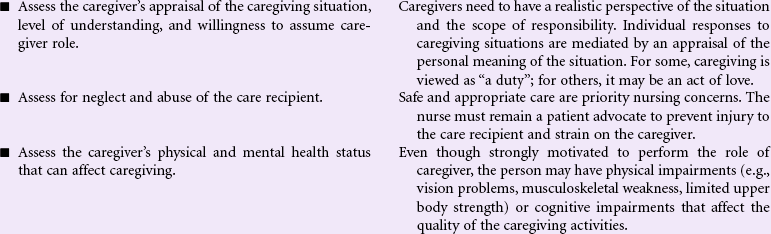
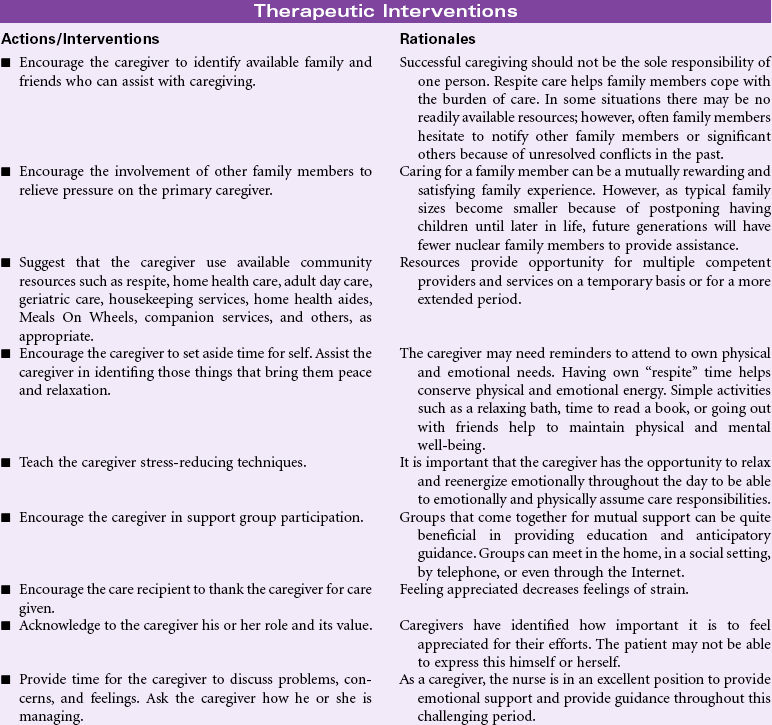
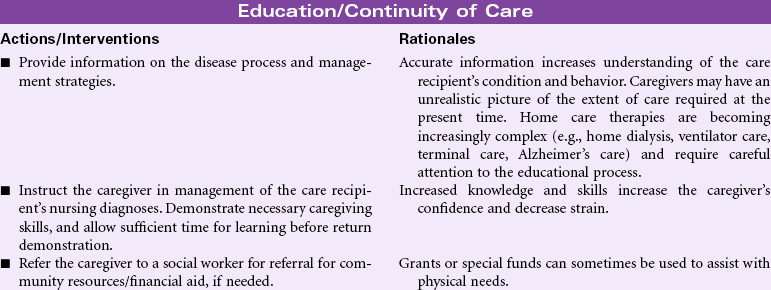
Caregiver Role Strain
Definition: Difficulty in performing family caregiver role
The focus of this care plan is on the supportive care rendered by family members, significant others, or caregivers responsible for meeting the physical/emotional needs of the patient. With limited access to health care for many people, most diseases are diagnosed and managed in the outpatient setting. Rapid hospital discharges for even the most complex health problems result in the care of acute and chronic illnesses being essentially managed in the home environment. Today’s health care environment places high expectations on the designated caregiver, whether a family member or someone for hire. For many older patients, the only caregiver is a fragile spouse overwhelmed by his or her own health problems. Even in cultures in which care of the ill is the anticipated responsibility of family members, the complexities of today’s medical regimens, the chronicity of some disease processes, and the burdens of the caregiver’s own family or environmental milieu provide an overwhelming challenge. Caregivers have special needs for knowledge and skills in managing the required activities, access to affordable community resources, and recognition that the care they are providing is important and appreciated. Moreover, caregivers can be considered “secondary patients” who are at high risk for injury and adverse events. Nurses can assist caregivers by providing the requisite education and skill training and offering support through home visits; special clinic sessions; telephone access for questions and comfort; innovative strategies, such as telephone or computer support or “chat groups”; opportunities for respite care; and guidance in engaging in activities that promote their own health (nutrition, exercise, sleep, stress management).

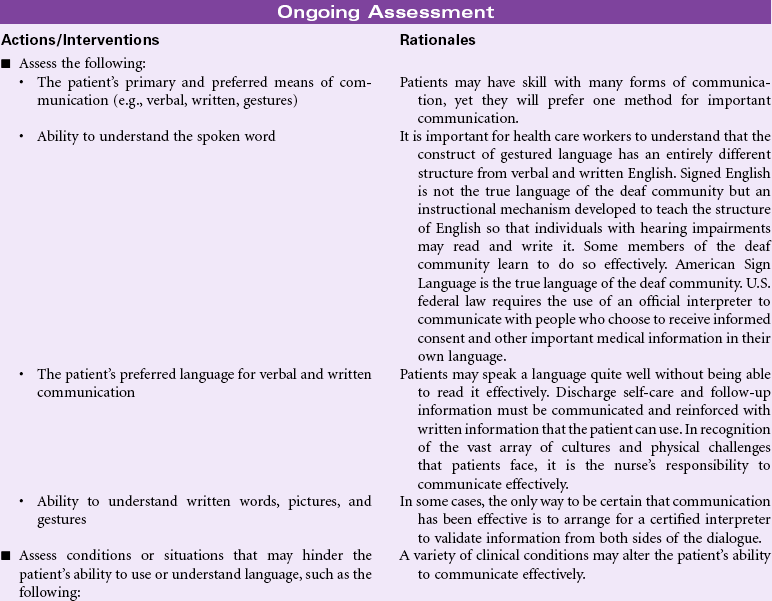
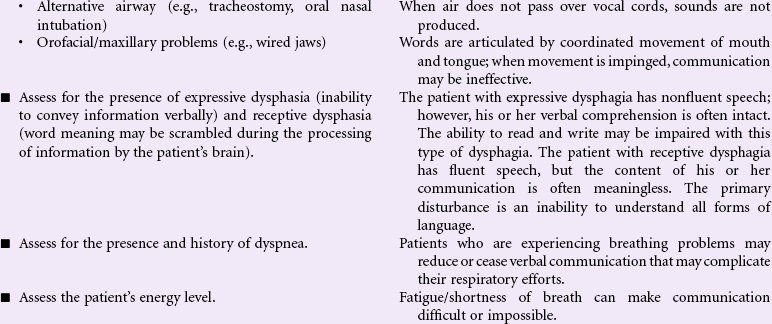
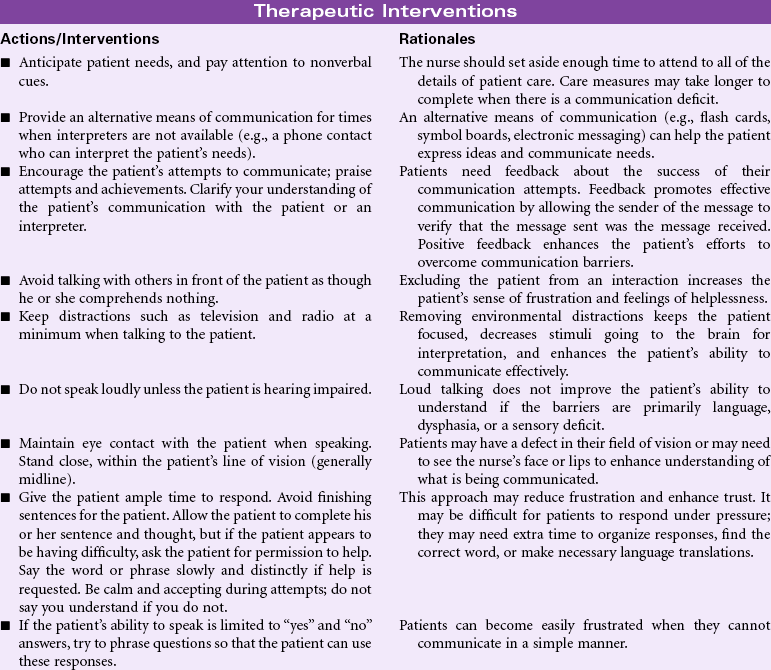
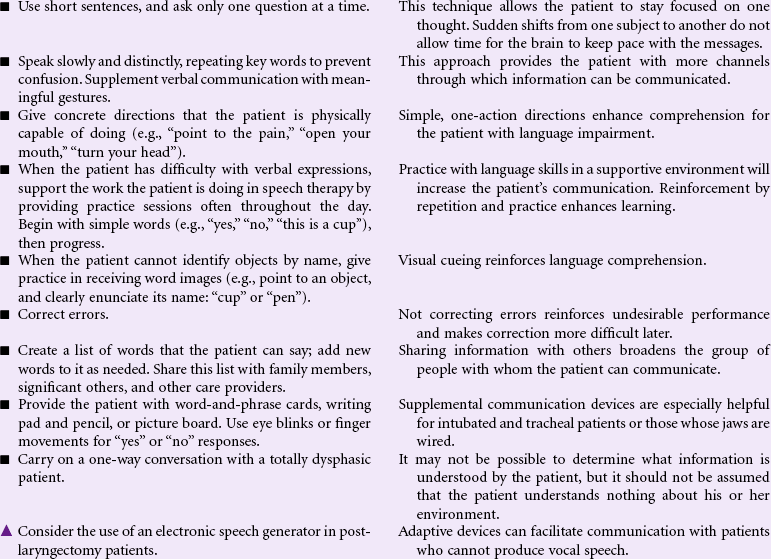
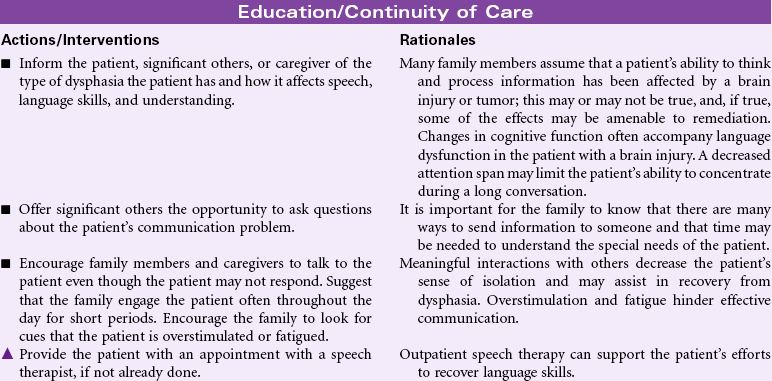
Impaired Verbal Communication
Definition: Decreased, delayed, or absent ability to receive, process, transmit, and use a system of symbols
Human communication takes many forms. People communicate verbally through the vocalization of a system of sounds that has been formalized into a language. They communicate using body movements to supplement, emphasize, or even alter what is being verbally communicated. In some cases, such as American Sign Language (the formal language of the deaf community) or Signed English, communication is conducted entirely through hand gestures that may or may not be accompanied by body movements and pantomime. Language can be read by watching an individual’s lips to observe words as they are shaped. Humans communicate through touch, intuition, written means, art, and sometimes a combination of all of the mechanisms. Communication implies the sending of information as well as the receiving of information. When communication is received, it ceases to be the sole product of the sender as the entire experiential history of the receiver takes over and interprets the information sent. At its best, effective communication is a dialogue that not only involves the transmission of information but also clarification of points made, expansion of ideas and concepts, and exploration of factors that fall out of the original thoughts transmitted. Communication is a multifaceted, kinetic, reciprocal process. Communication may be impaired for any number of reasons, but rarely are all avenues for communication compromised at one time. The task for the nurse, whether encountering the patient in the hospital or in the community, becomes recognizing when communication has become ineffective and then using strategies to improve transmission of information.

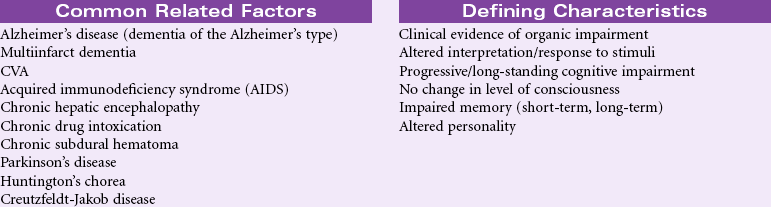
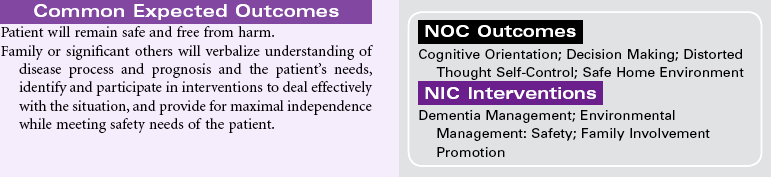
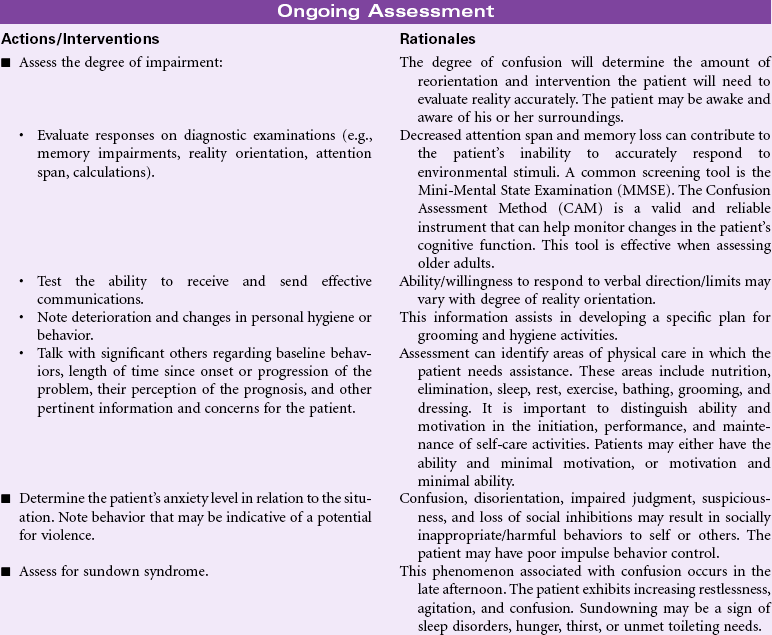
Chronic Confusion
Definition: An irreversible, long-standing, and/or progressive deterioration of intellect and personality characterized by decreased ability to interpret environmental stimuli, decreased capacity for intellectual thought processes, and manifested by disturbances of memory, orientation, and behavior
Chronic confusion is not limited to any one age-group, gender, or clinical problem. Chronic confusion can occur in a variety of settings, including the home, hospital, and long-term care facilities. Although often associated with older adults with dementia, younger adults with chronic illnesses also may be affected. Depression, multiple sclerosis, brain infections and tumors, repeated head trauma (as seen in athletes), abnormalities resulting from hypertension, diabetes, anemia, endocrine disorders, malnutrition, and vascular disorders are examples of illnesses that may be associated with chronic confusion. The person with chronic confusion experiences a gradual but progressive decline in cognitive function. Over months or years, the person has increasing problems with memory, comprehension, judgment, abstract thinking, and reasoning. The loss of cognitive ability may result in problems for the person with communication, ADLs, and emotional stability. Chronic confusion can have a profound impact on family members and family processes as the patient requires more direct supervision and care. This care plan discusses the management of chronic confusion in any setting. It also identifies the importance of addressing the needs of the caregivers.

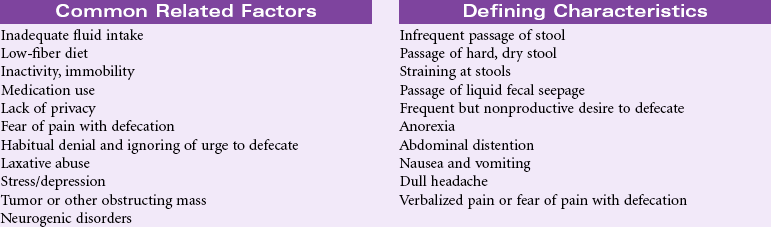
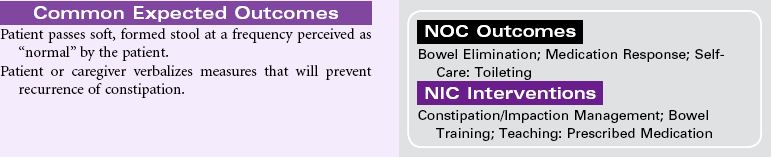
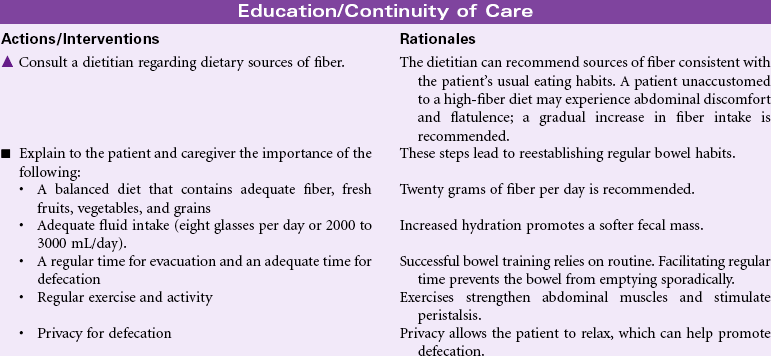
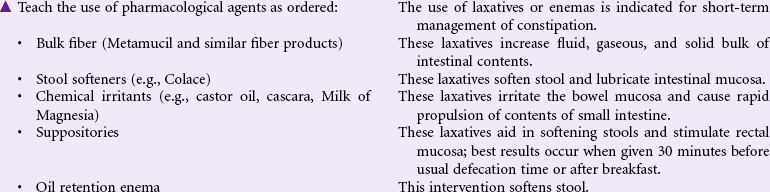
Constipation
Definition: Decrease in normal frequency of defecation accompanied by difficult or incomplete passage of stool and/or passage of excessively hard, dry stool
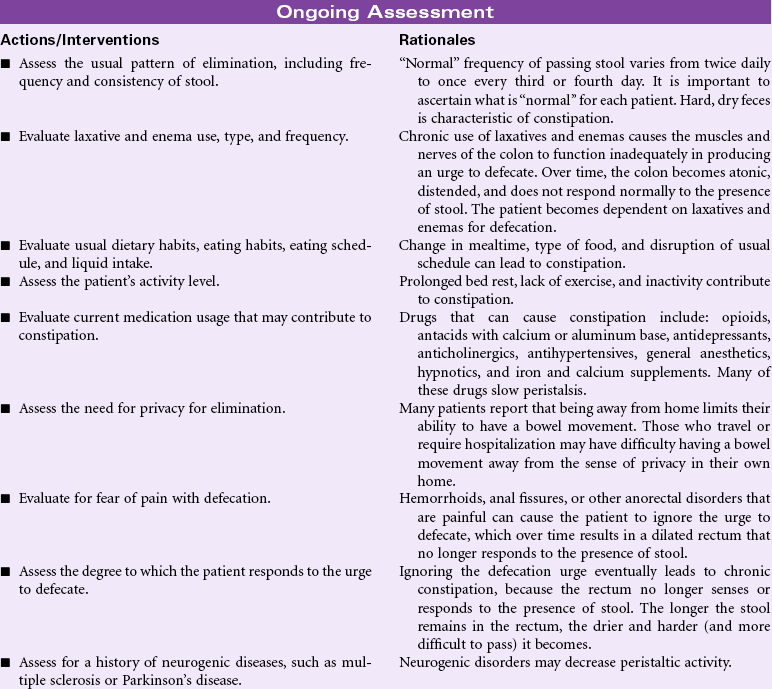
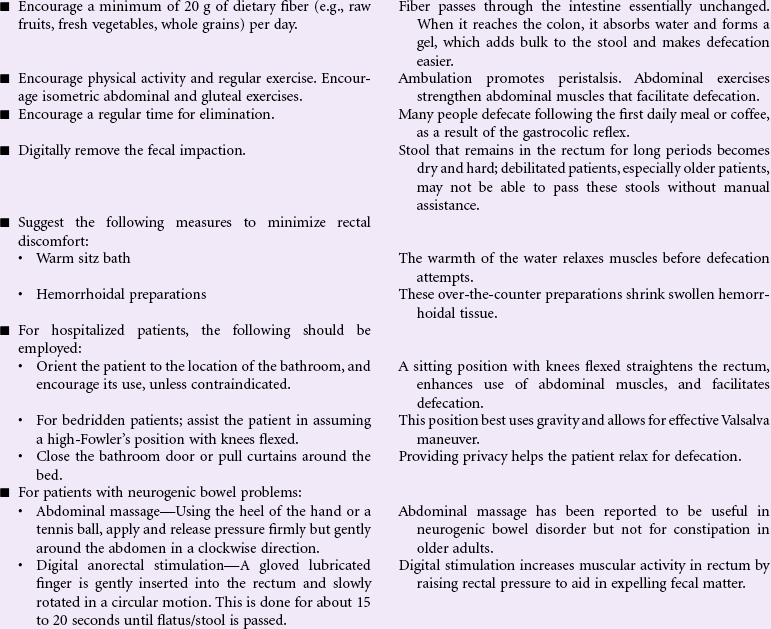
Constipation is a common, yet complex problem; it is especially prevalent among older patients. Diet, exercise, and daily routine are important factors in maintaining normal bowel patterns. Too little fluid, too little fiber, inactivity or immobility, and disruption in daily routines can result in constipation. Use of medications, particularly opioid analgesics or overuse of laxatives or enemas, can cause constipation. Patients who ignore the need to defecate for long periods are at risk for developing constipation. Psychological disorders such as stress and depression can cause constipation. Because privacy with defecation is an issue for most people, being away from home, hospitalized, or otherwise being deprived of adequate privacy can result in constipation. Because “normal” patterns of bowel elimination vary so widely from individual to individual, some people believe they are constipated if a day passes without a bowel movement; for others, every third or fourth day is normal. Chronic constipation can result in the development of hemorrhoids; diverticulosis (particularly in older patients who have a high incidence of diverticulitis); straining at stool, and although rare, perforation of the colon. Constipation is usually episodic, although it can become a lifelong, chronic problem. Because tumors of the colon and rectum can result in obstipation (complete lack of passage of stool), it is important to rule out these possibilities. Nonpharmacological management (fluids, activity, and fiber) remains the most effective treatment for constipation.

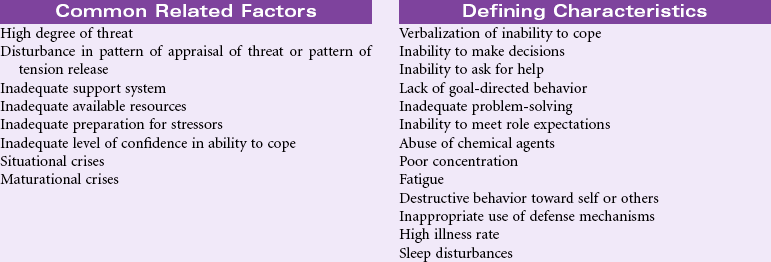
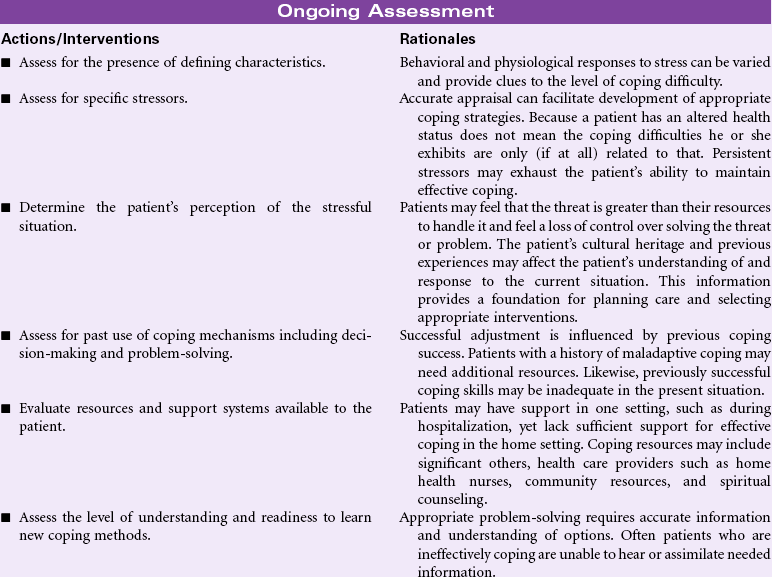
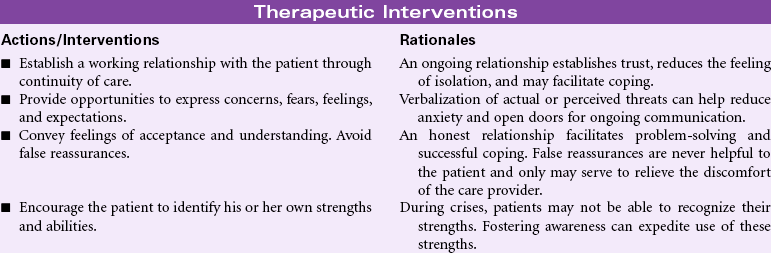
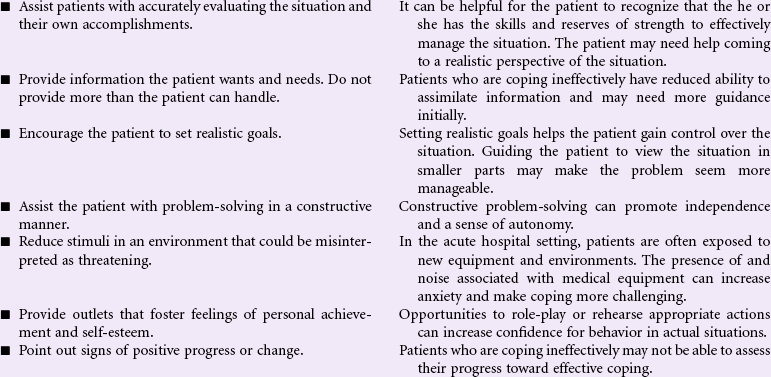
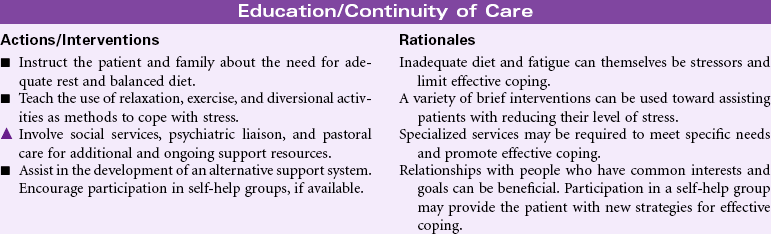
Ineffective Coping
Definition: Inability to form a valid appraisal of the stressors, inadequate choices of practiced responses, and/or inability to use available resources
For most people, everyday life includes its share of stressors and demands, ranging from family, work, and professional role responsibilities to major life events such as divorce, illness, and the death of loved ones. How one responds to such stressors depends in part on the person’s coping resources. Such resources can include optimistic beliefs, social support networks, personal health and energy, problem-solving skills, and material resources. Sociocultural and religious factors may influence how people view and handle their problems. Some cultures may prefer privacy and avoid sharing their fears in public, even to health care providers. As resources become limited and problems become more acute, this strategy may prove ineffective. Vulnerable populations such as older patients, those in adverse socioeconomic situations, those with complex medical problems such as substance abuse, or those who find themselves suddenly physically challenged may not have the resources or skills to cope with their acute or chronic stressors. Such problems can occur in any setting (e.g., during hospitalization for an acute event, in the home or rehabilitation environment as a result of chronic illness, or in response to another threat or loss).

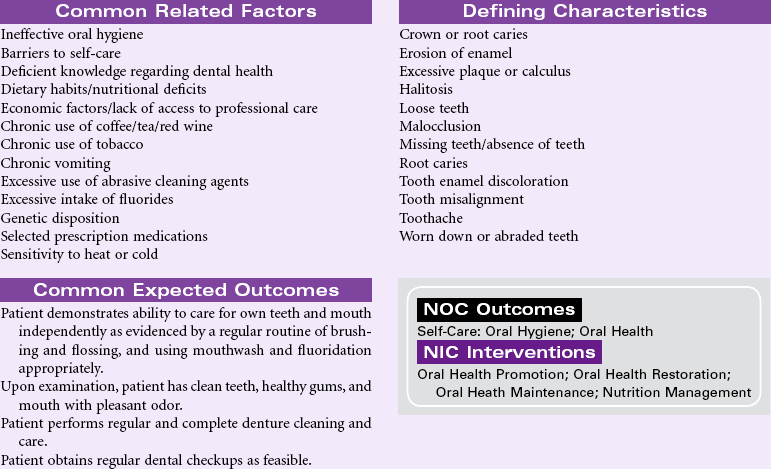
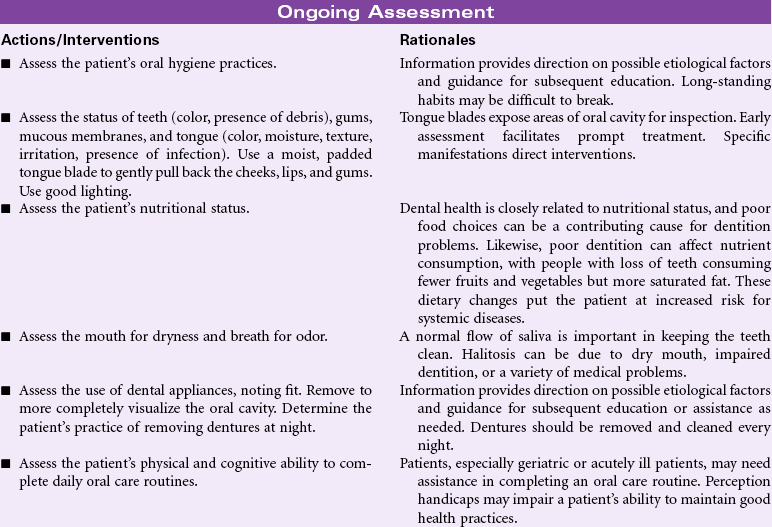
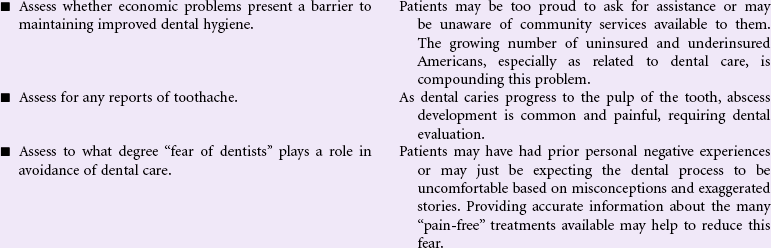
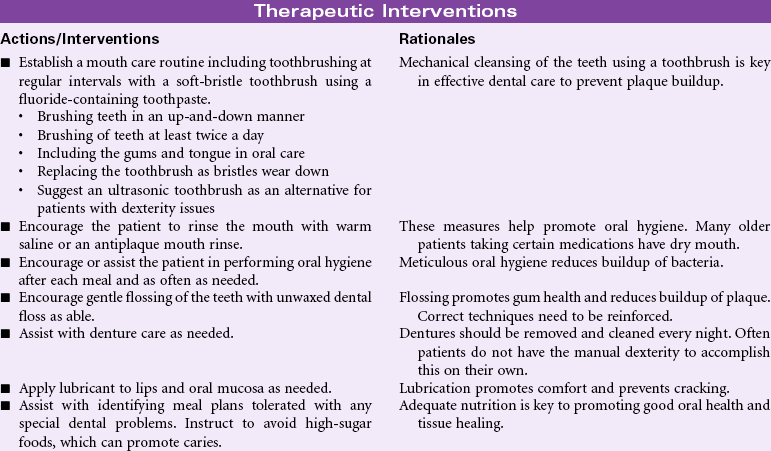
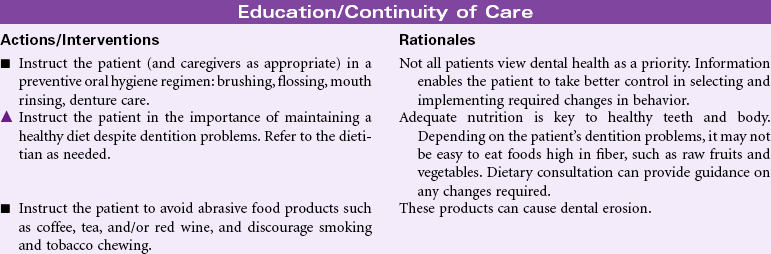
Impaired Dentition
Definition: Disruption in tooth development/eruption patterns or structural integrity of individual teeth
Good oral health can affect a person’s quality of life through such aspects as appearance, self-esteem, enjoyment from food, absence from dental pain and infections, and overall improved health status. Recent studies have examined the relationship between dentition status and dietary habits. It has been shown that many of the foods avoided by people with poor dentition status (e.g., high-fiber fruits, vegetables) are the ones found to be protective against cardiovascular disease, stroke, metabolic syndrome, and some cancers. Similarly, many people with tooth loss choose easier-to-eat foods containing more saturated fat and refined carbohydrates, putting them at great health risk. Oral health measures to prevent dental caries and tooth loss need to be addressed throughout one’s life, especially among older adults, who are at the greatest risk for systemic health problems related to impaired dentition.

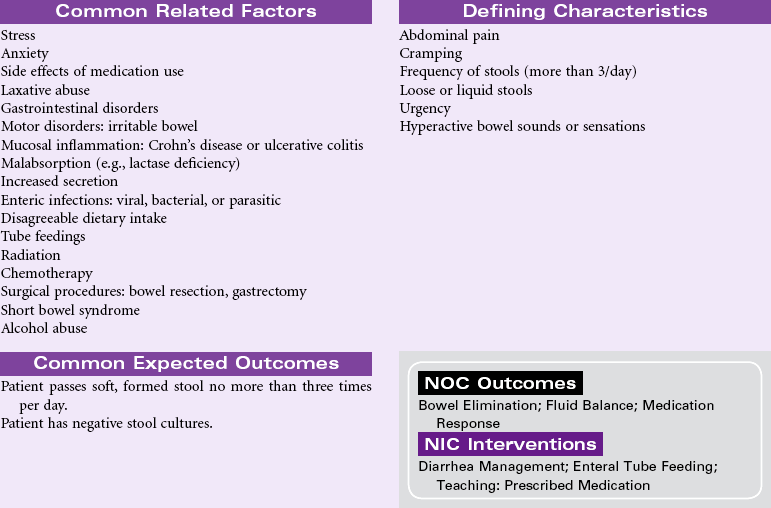
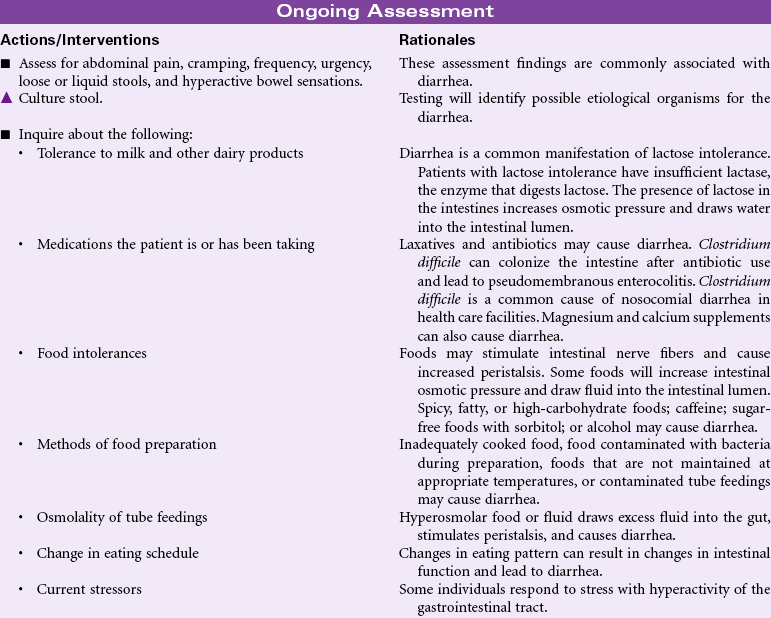
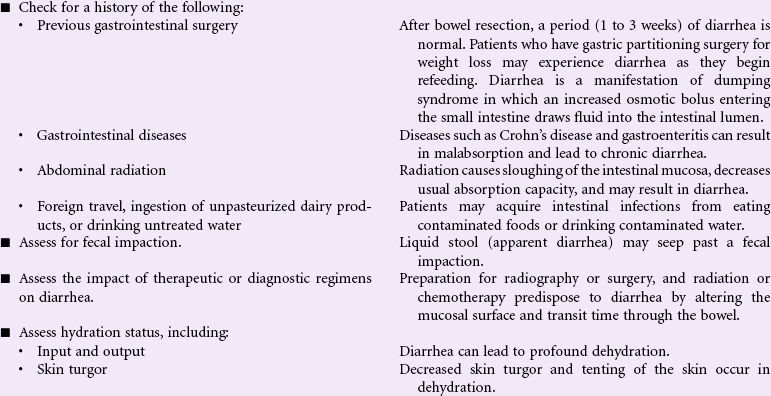
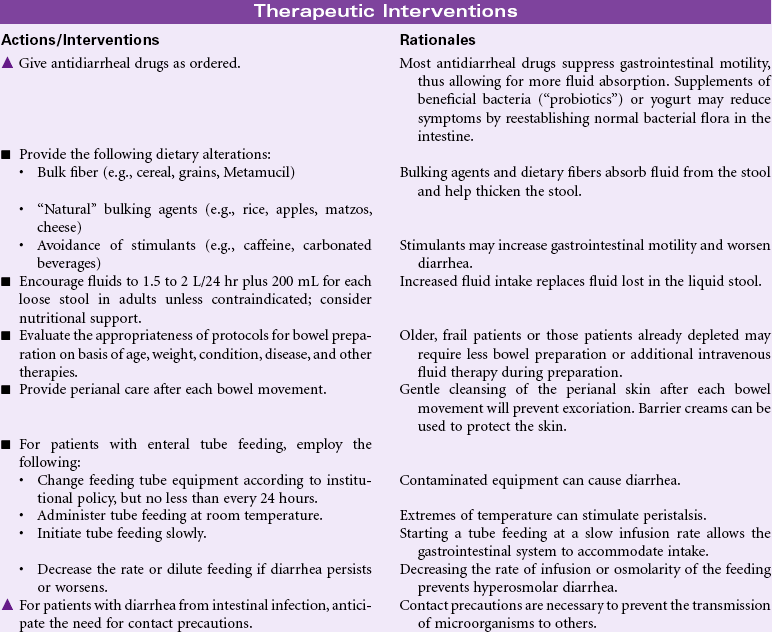
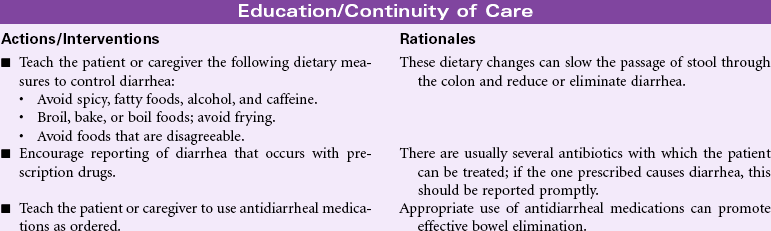
Diarrhea
Definition: Passage of loose, unformed stools
Diarrhea may result from a variety of factors, including intestinal malabsorption disorders, increased secretion of fluid by the intestinal mucosa, and hypermotility of the intestine. Diarrhea may result from infection (i.e., viral, bacterial, or parasitic); inflammatory bowel diseases (e.g., Crohn’s disease); side effects of drugs (e.g., antibiotics); increased osmotic loads (e.g., tube feedings); radiation; or increased intestinal motility such as with irritable bowel disease. Diarrhea may be an acute, short-lived episode of increased bowel elimination or it may be a long-term, chronic problem for the patient. Problems associated with diarrhea include fluid and electrolyte imbalances, impaired nutrition, and altered skin integrity. In older patients, or those with chronic disease, diarrhea can be life threatening. Treatment is based on addressing the cause of the diarrhea, replacing fluids and electrolytes, providing nutrition, and maintaining skin integrity. Health care workers and other caregivers must take precautions (e.g., diligent hand washing) to avoid transmission of infection associated with some causes of diarrhea.

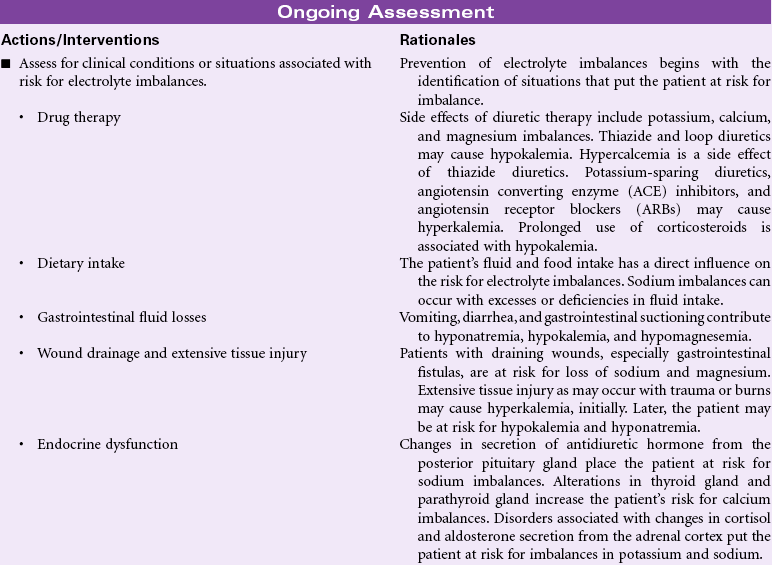
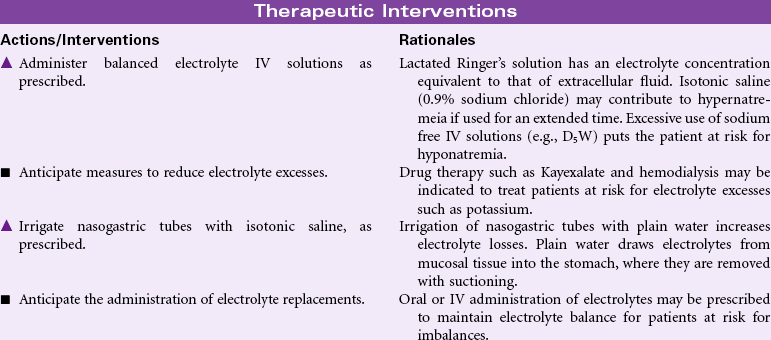
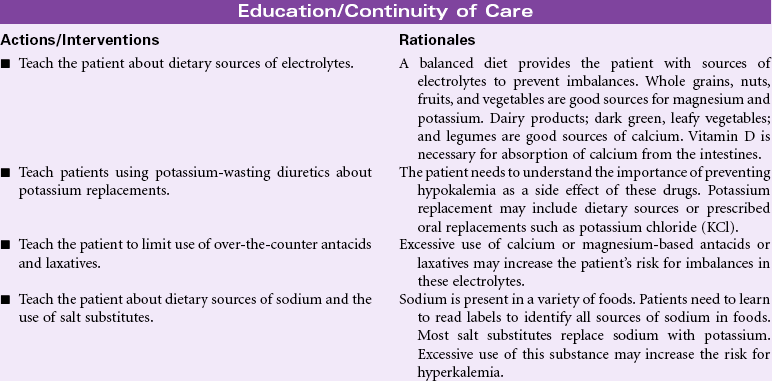
Risk for Electrolyte Imbalance
Definition: At risk for change in serum electrolyte levels that may compromise health
Many clinical disorders and their treatments place the patient at risk for imbalances in serum electrolyte concentrations. Imbalanced dietary intake may contribute to electrolyte imbalances. Electrolyte losses may occur from draining wounds and fistulas, especially gastrointestinal fistulas. Imbalances in sodium and chloride concentrations occur most often in situations related to fluid imbalances, especially gastrointestinal fluid losses such as vomiting, diarrhea, or suctioning. Alterations in secretion of antidiuretic hormone and aldosterone put the patient at risk for sodium imbalances. The risk for potassium imbalances increases in patients receiving diuretics. Diarrhea, renal failure, and altered aldosterone secretion also contribute to the patient’s risk for potassium imbalance. Alterations in thyroid and parathyroid function put the patient at risk for calcium imbalances. Magnesium imbalances often occur in the same situations as calcium and potassium imbalances. Changes in aldosterone secretion influence magnesium balance. Electrolyte imbalances affect a variety of functions in the body. The patient with an electrolyte imbalance may experience problems with fluid balance, muscle tone and strength, bone density, electrical conduction in the heart, wound healing, and renal stones. This care plan focuses on imbalances of sodium, potassium, calcium, and magnesium.

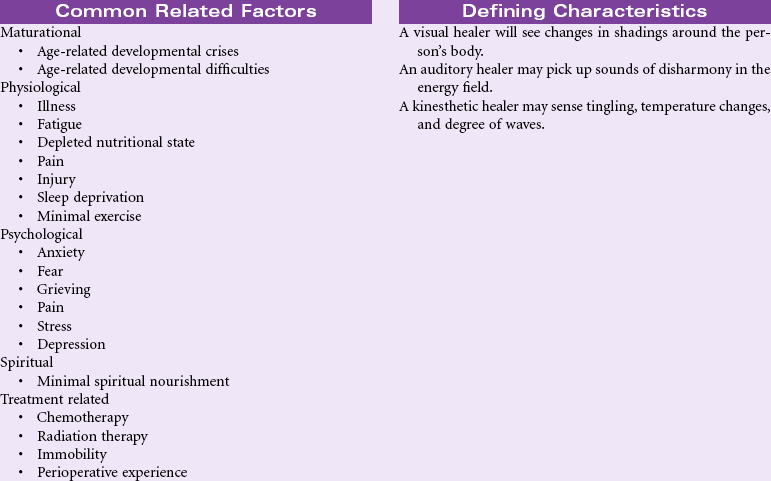
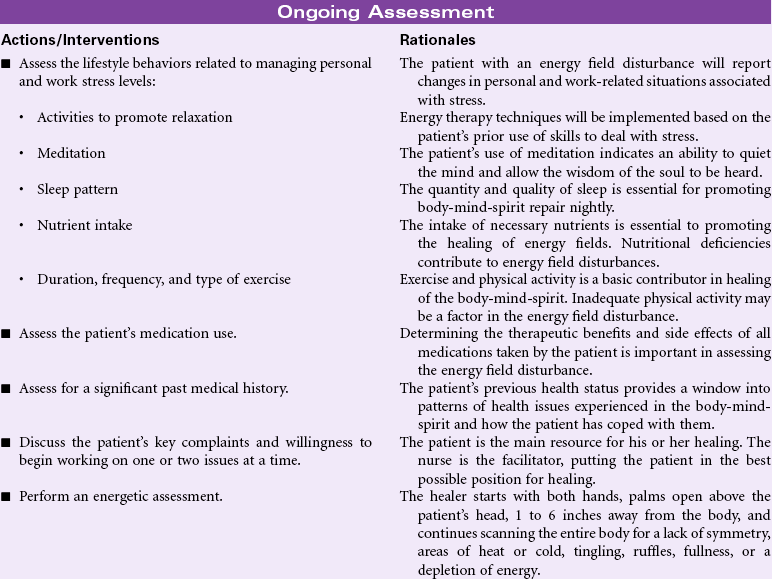
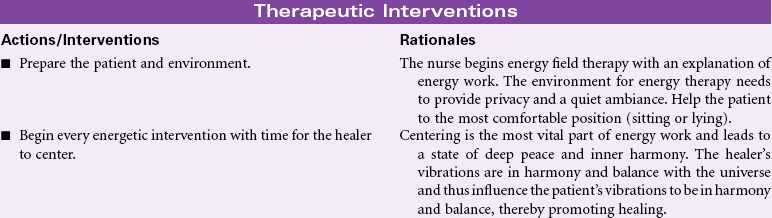
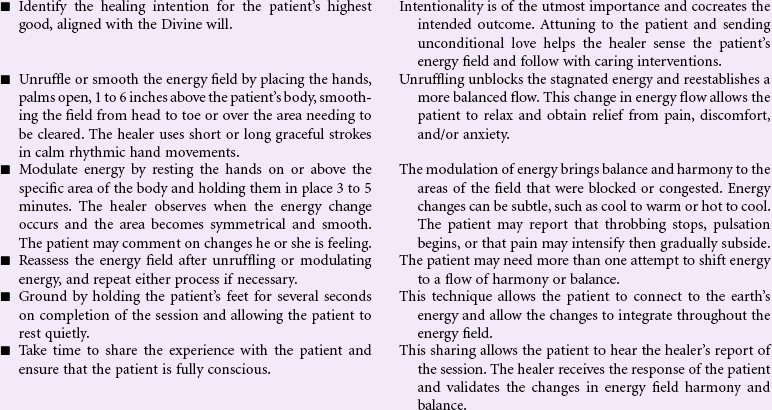
Disturbed Energy Field
Definition: Disruption of the flow of energy surrounding a person’s being that results in a disharmony of the body, mind, or spirit
Each person is an open energy system. The energy field is one aspect of the human energy system, the other parts being the chakras and meridians. This threefold system is vibrational in nature and continuously interacts within itself and with all other systems of the body. In energy field disruption the patient may present any number of concerns indicating disharmony and imbalance in one or more of these energy systems (e.g., pain, fatigue, stress, depression, addiction, nausea, also side effects from anesthesia and various therapies).
In many cases the patient has tried several avenues of Western medicine and is not satisfied with the results. Treatment of the physical problem by surgical procedure or medication is often not adequate to bring balance and harmony to the person. The integration of energy work from the traditions of Eastern medicine with Western medicine is ideal. Energy-based therapies may identify problems before symptoms develop in the body. Nurses can help patients heal in body, mind, and spirit by using energy techniques grounded in traditions thousands of years old (i.e., Reiki, Therapeutic Touch, Healing Touch, and other energy therapies). Nurses acquainted with energy work can assist the patient with healing and restoring energy field balance in any patient care setting, including hospital, home, long-term care, or ambulatory care. This care plan is limited to the most basic energy therapy techniques.
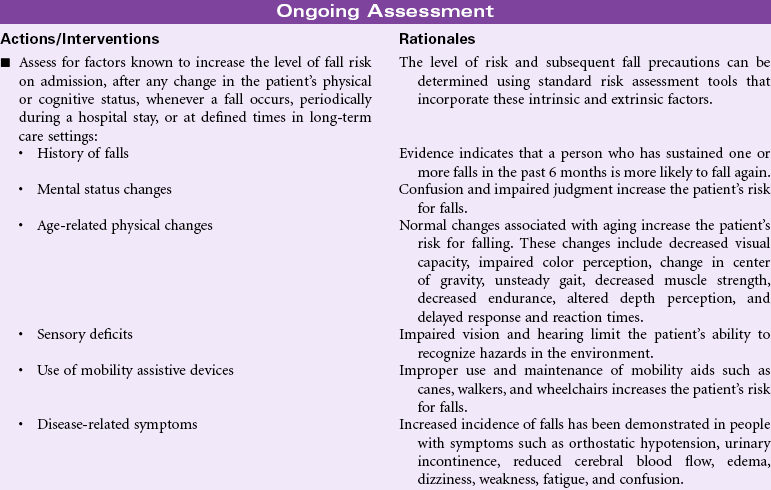
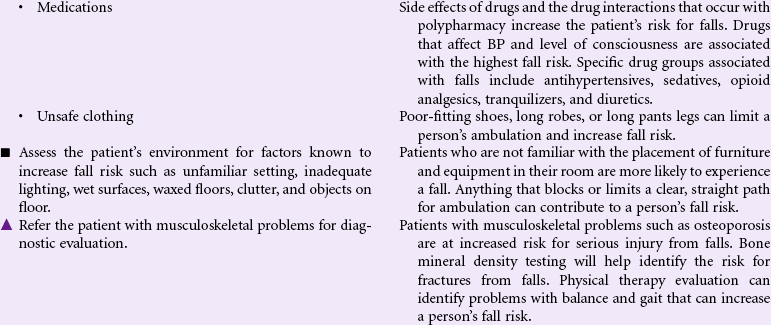
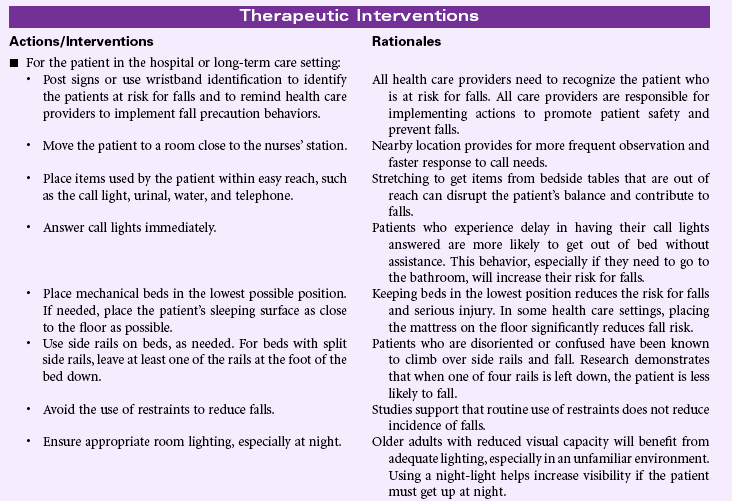
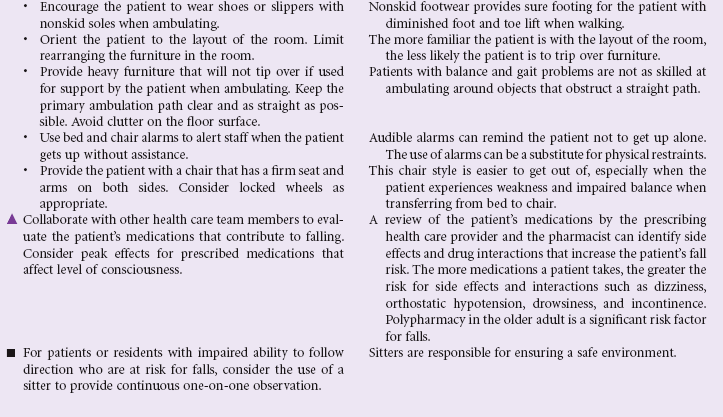
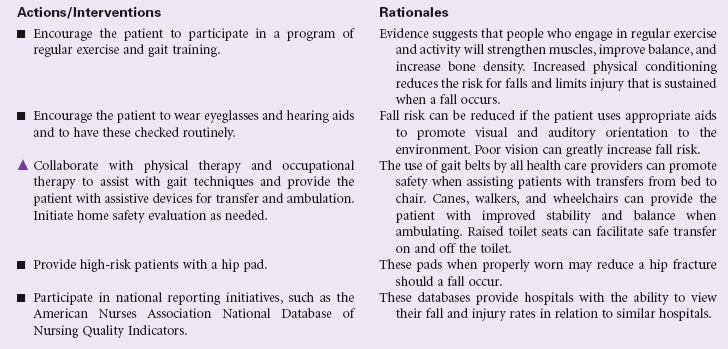
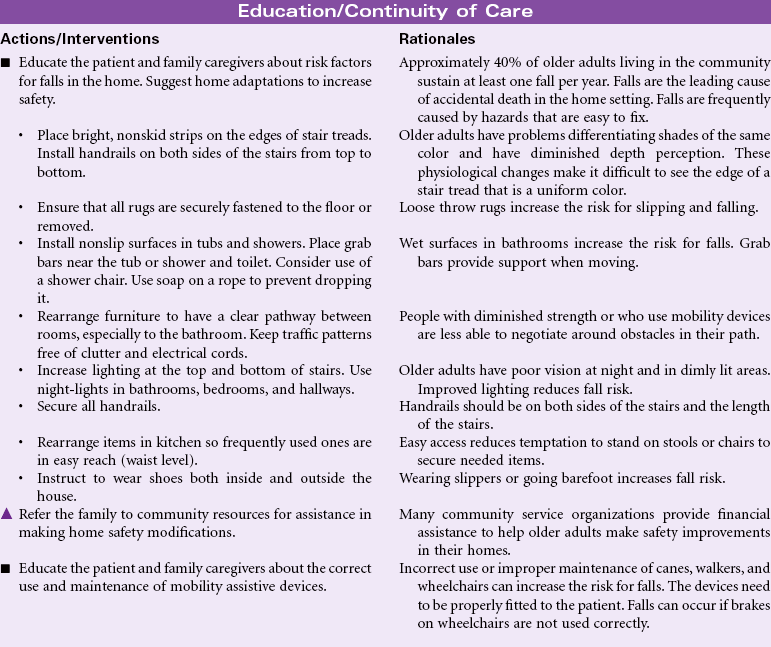
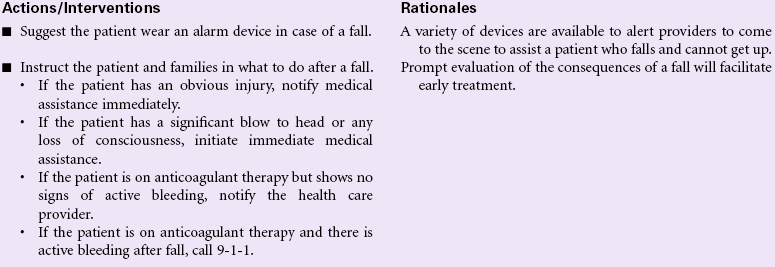
Risk for Falls
Definition: Increased susceptibility to falling that may cause physical harm
Falls are a major safety risk for adults, especially older adults. According to the Centers for Disease Control and Prevention (CDC), approximately one in three community-dwelling adults older than age 65 fall each year, and women fall more frequently than men in this age-group. This number increases to approximately 75% of nursing home residents because of their older age, frailty, chronic medical conditions, and cognitive impairments. Fall-related injuries are the most common cause of accidental death in individuals older than 65 years. Injuries sustained as a result of a fall include soft tissue injury, fractures (hip, spine, and wrist), and traumatic brain injury. Fall-related injuries are associated with prolonged hospitalization for older adults. For those surviving a fall, the quality of life is significantly changed after a fall-related injury.
The morbidity, mortality, and economic burdens resulting from patient falls pose serious risk management issues facing the health care industry. Patient falls are caused by multiple factors. Prevention of falls is an important dimension of the nursing care of patients in hospitals and long-term care settings. In 2005, The Joint Commission added the requirement for fall risk assessment and periodic reassessment as a National Patient Safety Goal in the acute care setting, and in 2006 added the requisite of implementing and evaluating a fall prevention program. The Nursing Home Quality Initiative project has a similar focus for that population. Implementation of successful fall prevention programs is an essential part of nursing care in any health care setting and requires a multifaceted approach. The Agency for Healthcare Research and Quality (AHRQ) provides a comprehensive review of risk assessment instruments for various settings, selected prevention strategies, and recommendations from evidence-based practice and research implications. Nurses also have a major role in educating patients, families, and caregivers about the prevention of falls across the care continuum.
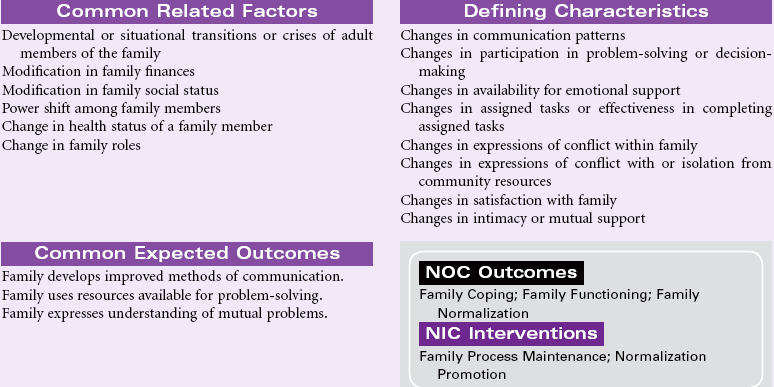
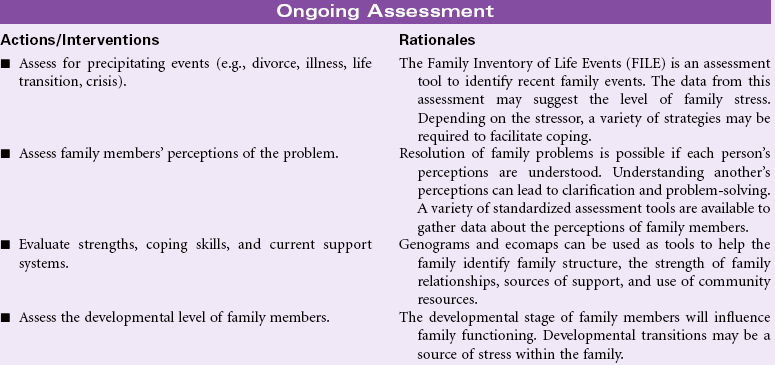
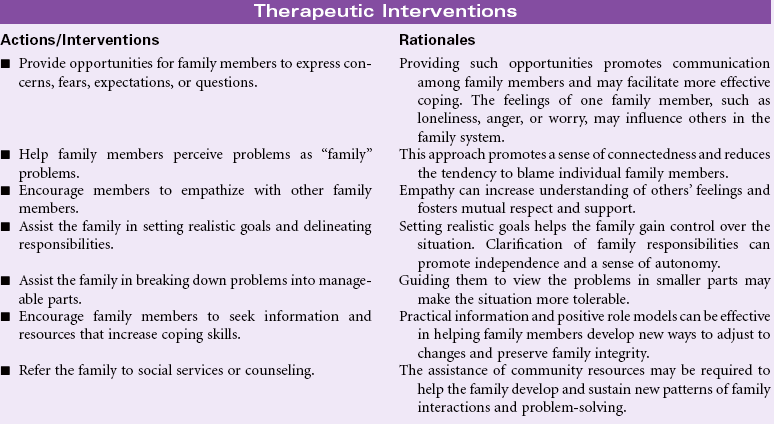
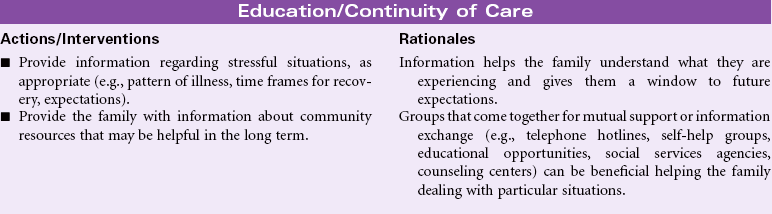
Interrupted Family Processes
Definition: Change in family relationships and/or functioning
Interrupted family processes occur as a result of the inability of one or more members of the family to adjust or perform. The result of this inability to adjust is family dysfunction and an interruption in the development of the family. Family development is closely related to the developmental changes experienced by adult members. Over time, families must adjust to change within the family structure brought on by both expected and unexpected events, including illness or death of a member/changes in social or economic strengths precipitated by divorce, retirement, and loss of employment. The addition of new family members through birth or adoption may require adaptation to new roles and status for existing family members. Health care providers must also be aware of the changing constellation of families: gay couples raising children, single parents with children, older grandparents responsible for grandchildren or foster children, and other situations.
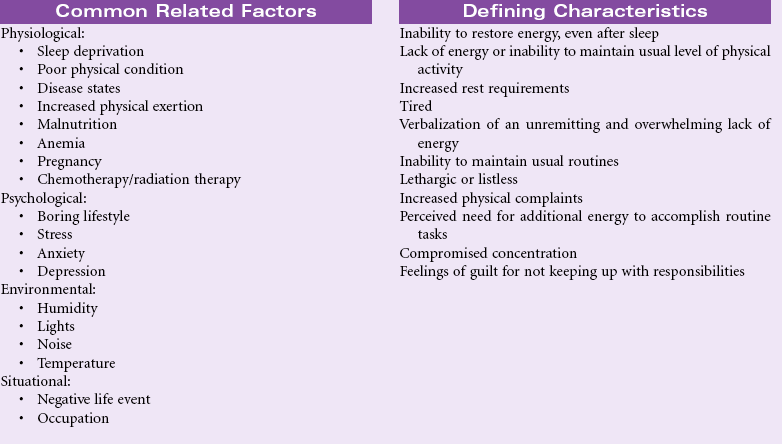
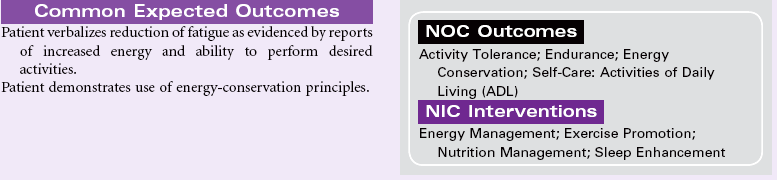
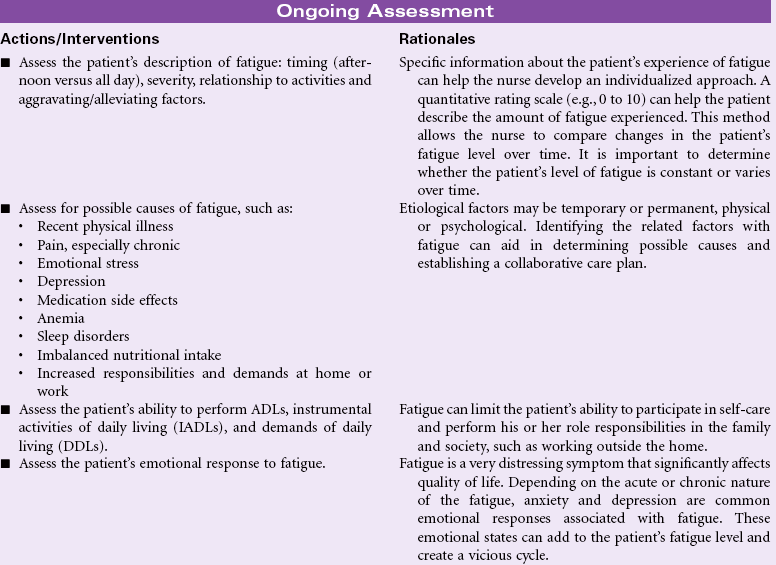
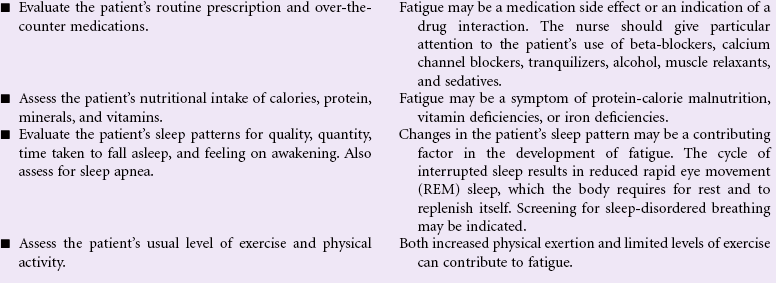
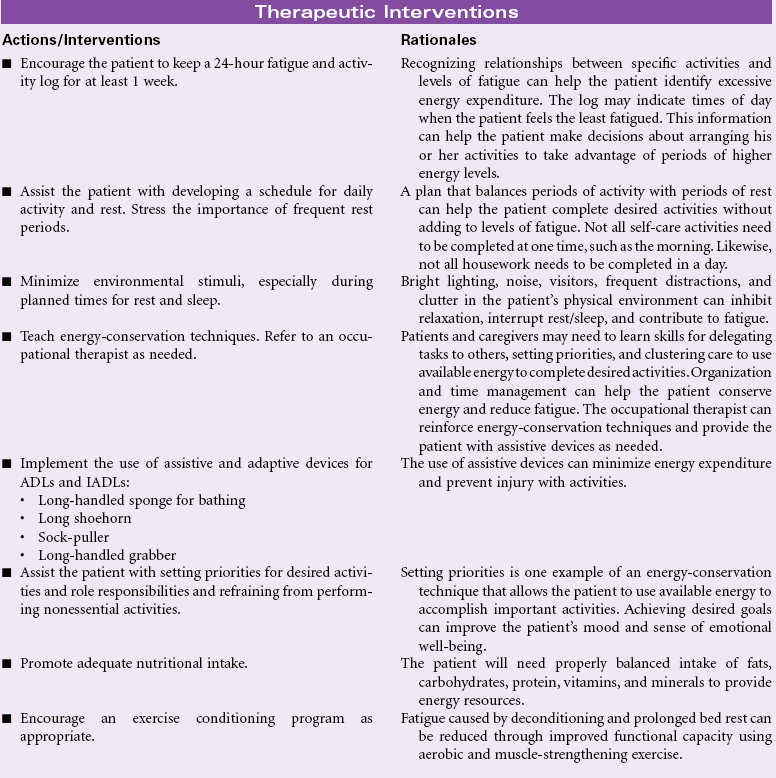
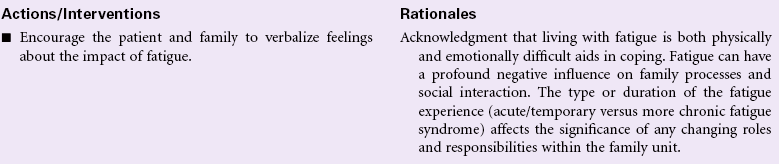
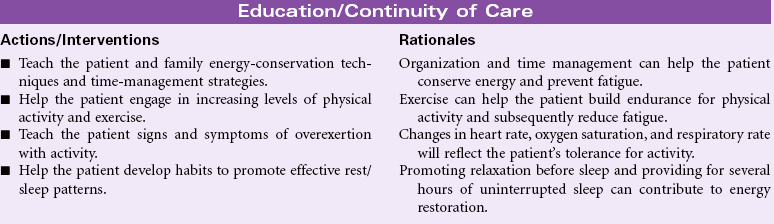
Fatigue
Definition: An overwhelming sustained sense of exhaustion and decreased capacity for physical and mental work at usual level
Fatigue is a subjective complaint with both acute and chronic illnesses. In an acute illness, fatigue may have a protective function that keeps the person from sustaining injury from overwork in a weakened condition. As a common symptom, fatigue is associated with a variety of physical and psychological conditions. Fatigue is a prominent finding in many viral infections such as hepatitis. Patients with rheumatoid arthritis, fibromyalgia, systemic lupus erythematosus, myasthenia gravis, and depression report fatigue as a profound symptom that reduces their ability to participate in their own care and fulfill role responsibilities. Fatigue has become the most common and distressing complaint for patients with cancer, especially during treatment. The patient with a chronic illness experiencing fatigue may be unable to work full-time and maintain acceptable performance on the job. The economic impact on the individual and the family can be significant. The social effects of fatigue occur as the person decreases his or her participation in social activities. Recently, attention has focused on sleep-disordered breathing as a cause for daytime somnolence, fatigue, and decreased alertness. Common screening methods are available.
Chronic fatigue syndrome is a poorly understood condition that is characterized by prolonged, debilitating fatigue, neurological problems, general pain, gastrointestinal problems, and flulike symptoms. Although the exact cause of chronic fatigue syndrome is not known, one theory suggests that the disorder may represent an abnormal response of the immune system to highly stressful physiological or psychological events.
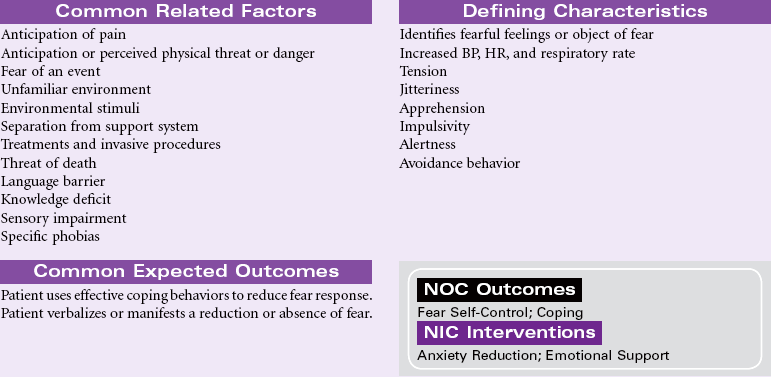
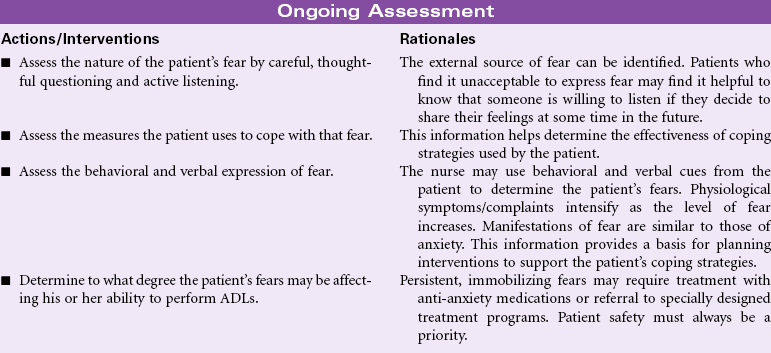
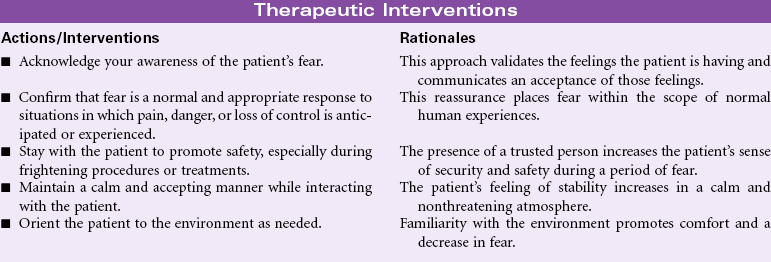
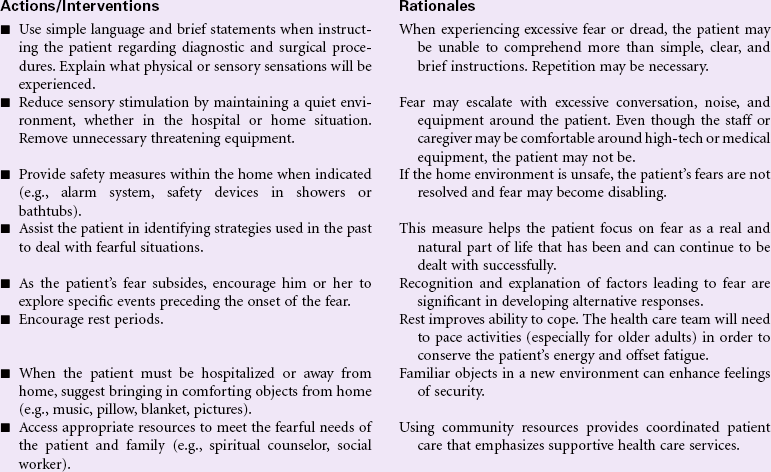
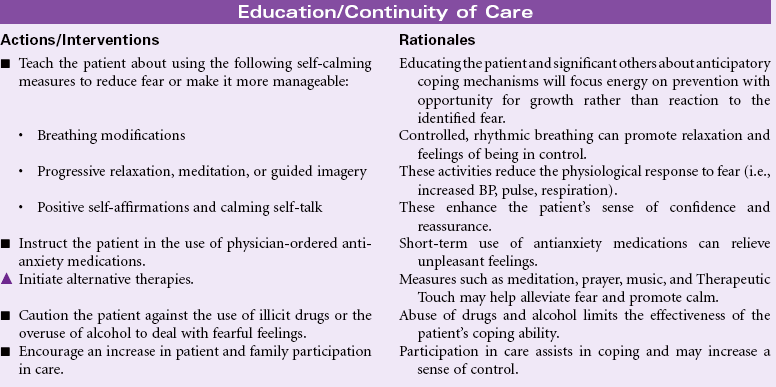
Fear
Definition: Response to perceived threat that is consciously recognized as a danger
Fear is a strong and unpleasant emotion caused by the awareness or anticipation of pain or danger. This emotion is primarily externally motivated and source-specific; that is, the individual experiencing the fear can identify the person, place, or thing precipitating this feeling. The factors that precipitate fear are, to some extent, universal; fear of death, pain, and bodily injury are common to most people. Other fears are derived from the life experiences of the individual person. How fear is expressed may be strongly influenced by the culture, age, or gender of the person under consideration. In some cultures it may be unacceptable to express fear regardless of the precipitating factors. Rather than manifesting outward signs of fear as described in the defining characteristics, responses may range from risk-taking behavior to expressions of bravado and defiance of fear as a legitimate feeling. In other cultures fear may be freely expressed and manifestations may be universally accepted. In addition to one’s own individual ways of coping with the feeling of fear, there are aspects of coping that are cultural as well. Some cultures control fear through the use of magic, mysticism, or religiosity. Whatever one’s mechanism for controlling and coping with fear, it is a normal part of everyone’s life. The nurse may encounter the fearful patient in the community, during the performance of diagnostic testing in an outpatient setting, or during hospitalization. The nurse must learn to identify when patients are experiencing fear and must find ways to assist them in a respectful way to negotiate these feelings. The nurse must also learn to identify when fear becomes so persistent and pervasive that it impairs an individual’s ability to carry on his or her activities of daily living. Under these circumstances, referral can be made to programs designed to assist the patient in overcoming phobias and other truly debilitating fears.
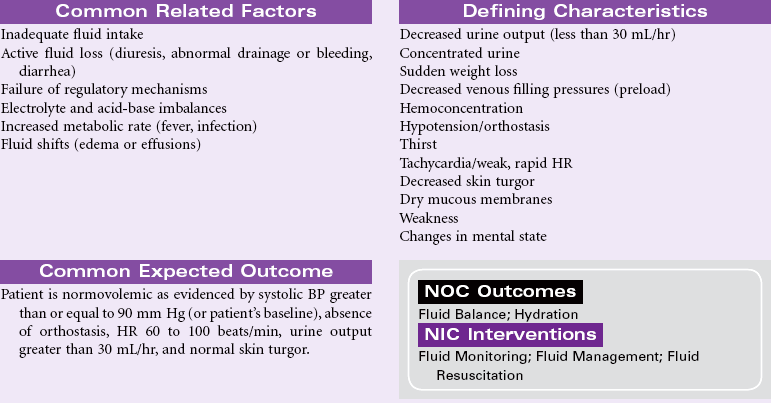
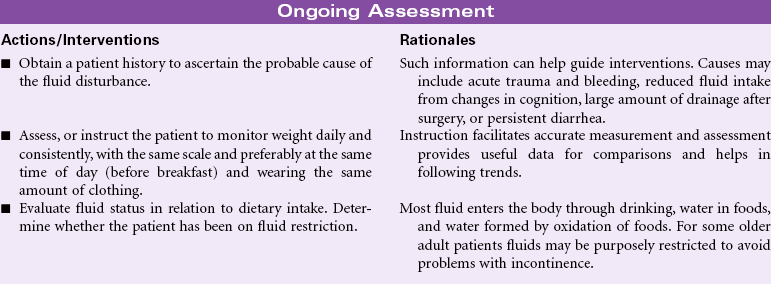
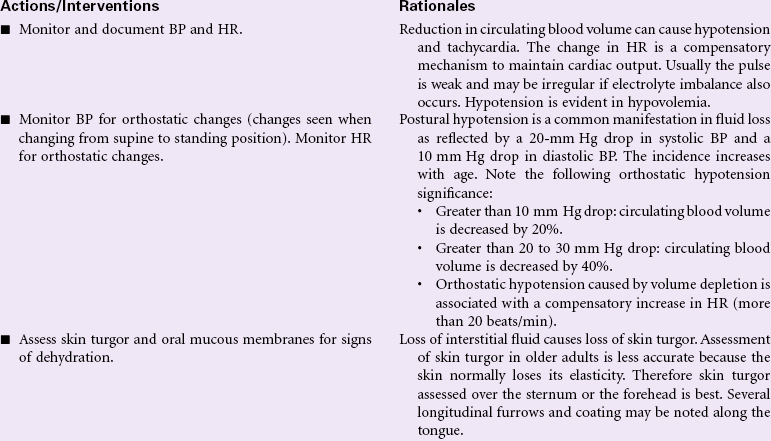
Deficient Fluid Volume
Definition: Decreased intravascular, interstitial, and/or intracellular fluid. This refers to dehydration, water loss alone without change in sodium
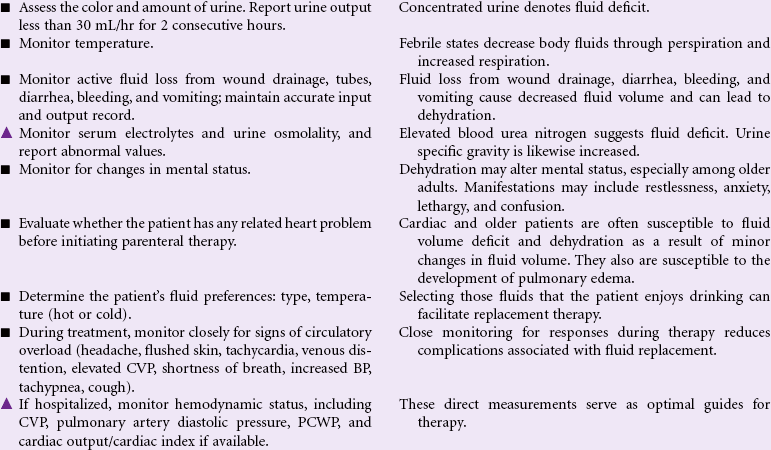
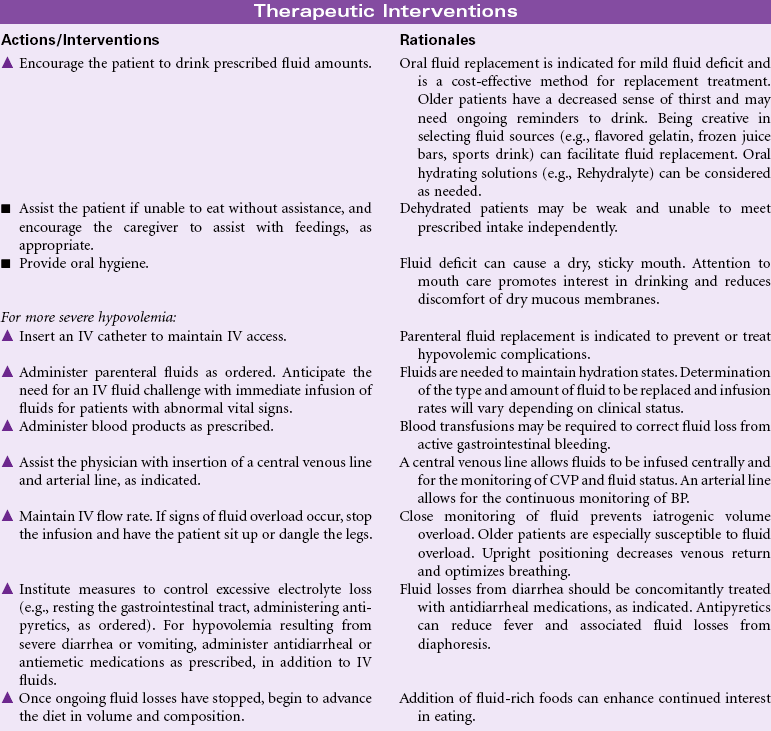
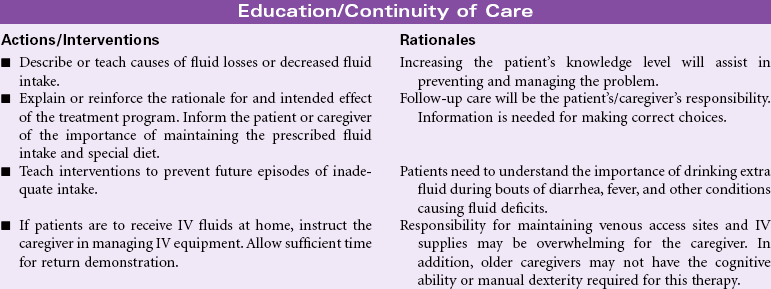
Fluid volume deficit, or hypovolemia, occurs from a loss of body fluid or the shift of fluids into the third space, or from a reduced fluid intake. Common sources for fluid loss are the gastrointestinal tract, polyuria, and increased perspiration. Fluid volume deficit may be an acute or chronic condition managed in the hospital, outpatient center, or home setting. The therapeutic goal is to treat the underlying disorder and return the extracellular fluid compartment to normal. Treatment consists of restoring fluid volume and correcting any electrolyte imbalances. Early recognition and treatment are paramount to prevent potentially life-threatening hypovolemic shock. Older patients are more likely to develop fluid imbalances.

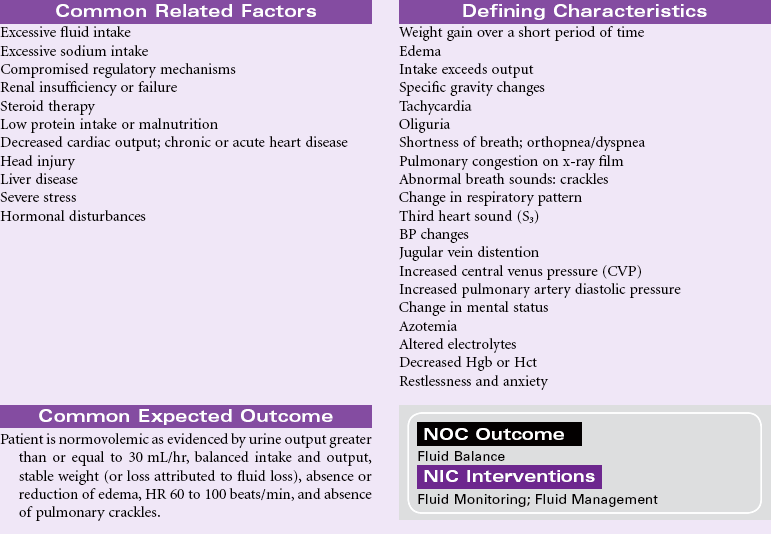
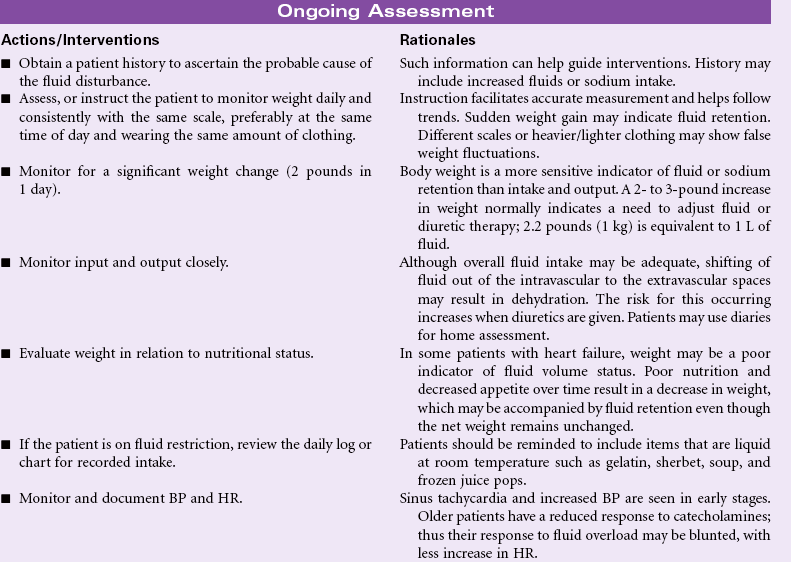
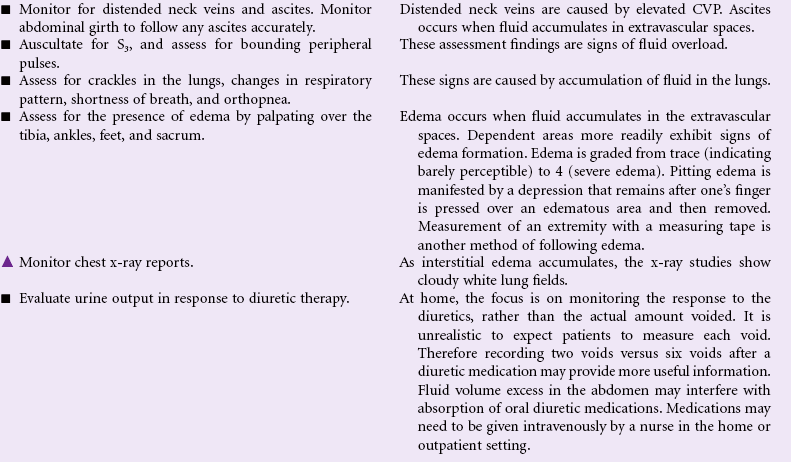
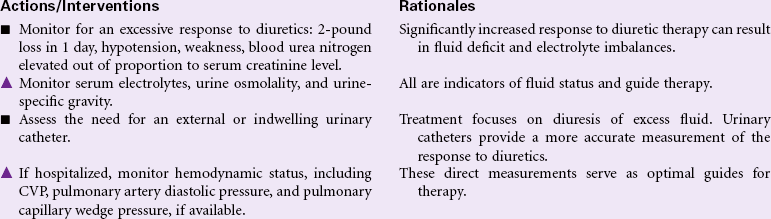
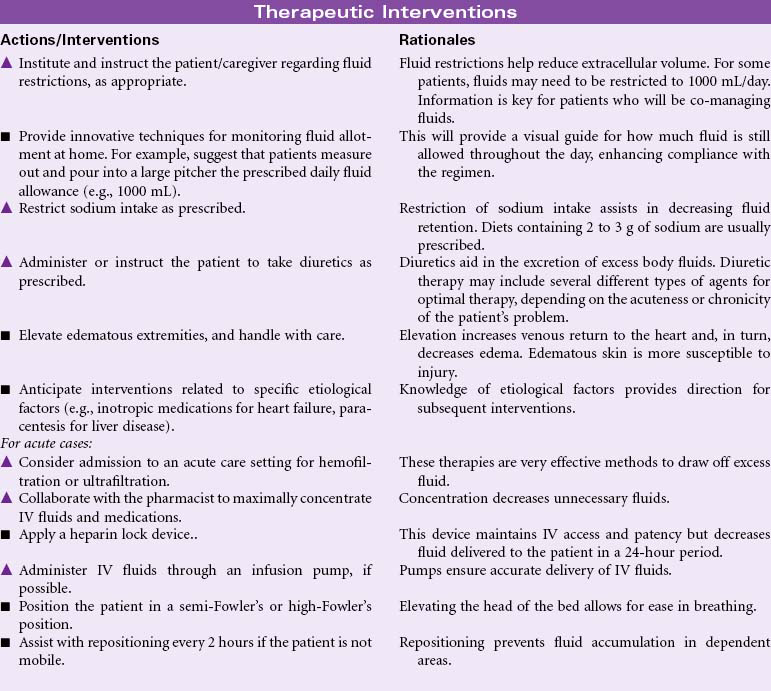
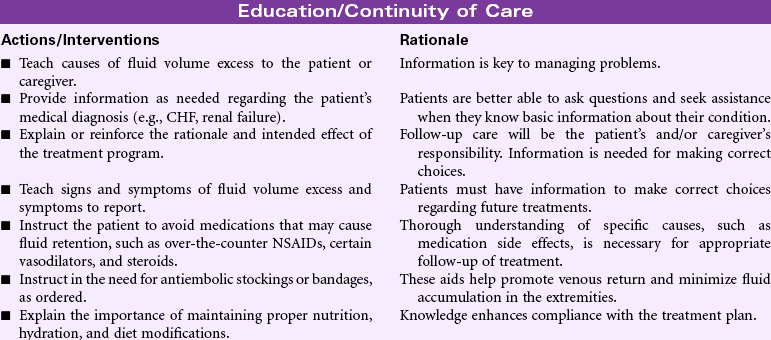
Excess Fluid Volume
Definition: Increased isotonic fluid retention
Fluid volume excess, or hypervolemia, occurs from an increase in total body sodium content and an increase in total body water. This fluid excess usually results from compromised regulatory mechanisms for sodium and water as seen in congestive heart failure (CHF), kidney failure, and liver failure. It may also be caused by excessive intake of sodium from foods, IV solutions, medications, or diagnostic contrast dyes. Hypervolemia may be an acute or chronic condition managed in the hospital, outpatient center, or home setting. The therapeutic goal is to treat the underlying disorder and return the extracellular fluid compartment to normal. Treatment consists of fluid and sodium restriction and the use of diuretics. For acute cases, ultrafiltration or dialysis may be required.
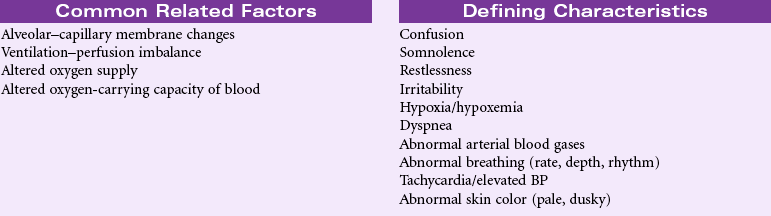
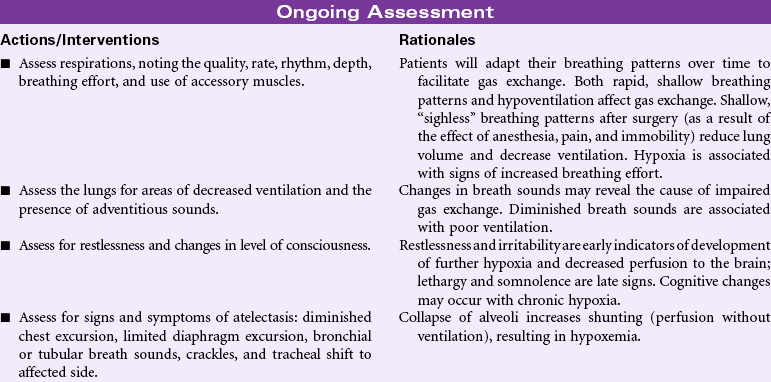
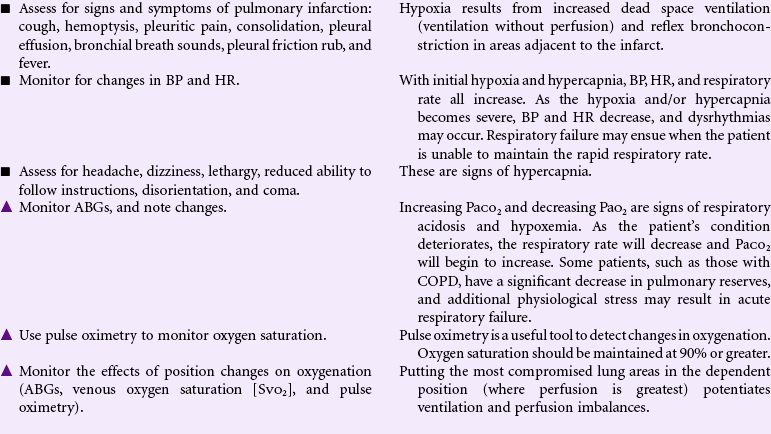
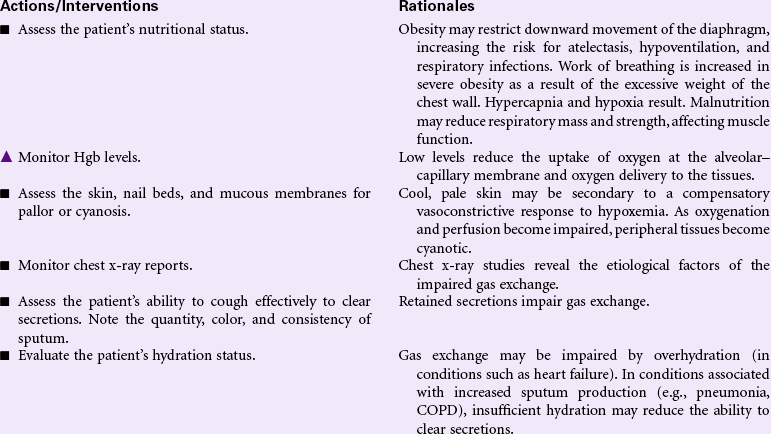
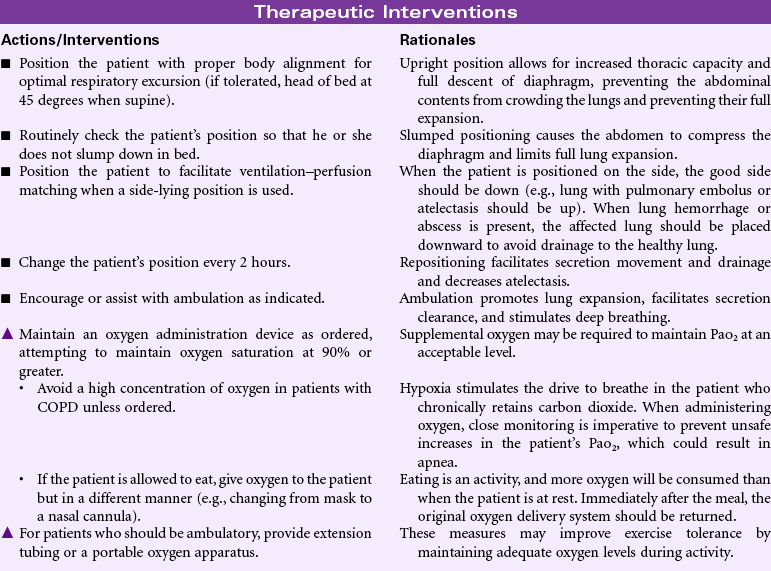
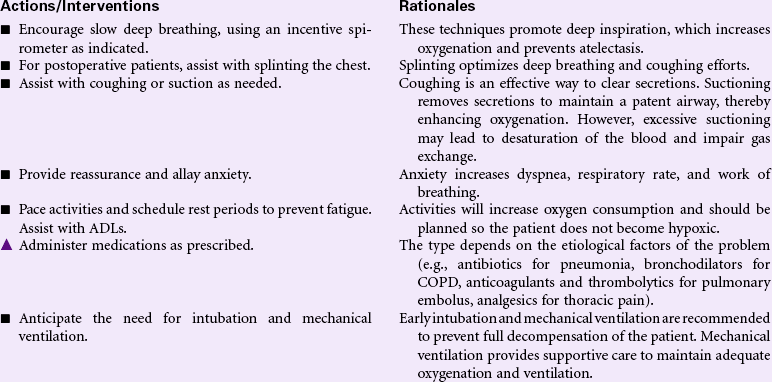
Impaired Gas Exchange
Definition: Excess or deficit in oxygenation and/or carbon dioxide elimination at the alveolar–capillary membrane
By the process of diffusion, the exchange of oxygen and carbon dioxide occurs in the alveolar–capillary membrane area. The relationship between ventilation (airflow) and perfusion (blood flow) affects the efficiency of the gas exchange. Normally a balance exists between ventilation and perfusion; however, certain conditions can offset this balance, resulting in impaired gas exchange. Altered blood flow from a pulmonary embolus, decreased cardiac output, or shock can cause ventilation without perfusion. Conditions that cause changes or collapse of the alveoli (e.g., atelectasis, pneumonia, pulmonary edema, and acute respiratory distress syndrome) impair ventilation. Other factors affecting gas exchange include high altitudes, hypoventilation, and altered oxygen-carrying capacity of the blood from reduced hemoglobin. Older patients have a decrease in pulmonary blood flow and diffusion as well as reduced ventilation in the dependent regions of the lung, where perfusion is greatest. Chronic conditions (e.g., COPD) put these patients at greater risk for hypoxia. Other patients at risk for impaired gas exchange include those with a history of smoking or pulmonary problems, obesity, prolonged periods of immobility, and chest or upper abdominal incisions.

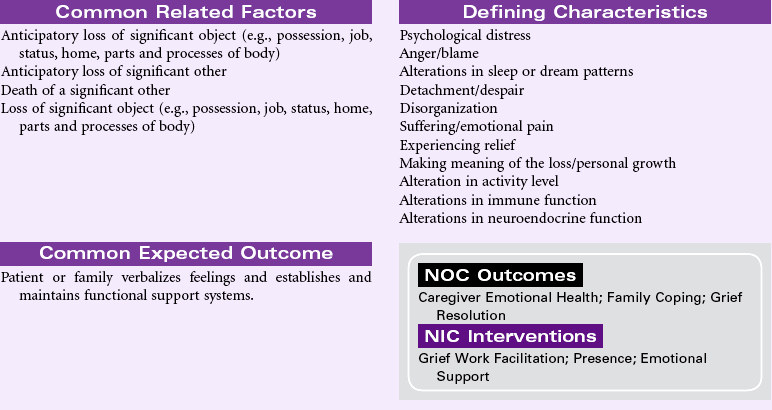
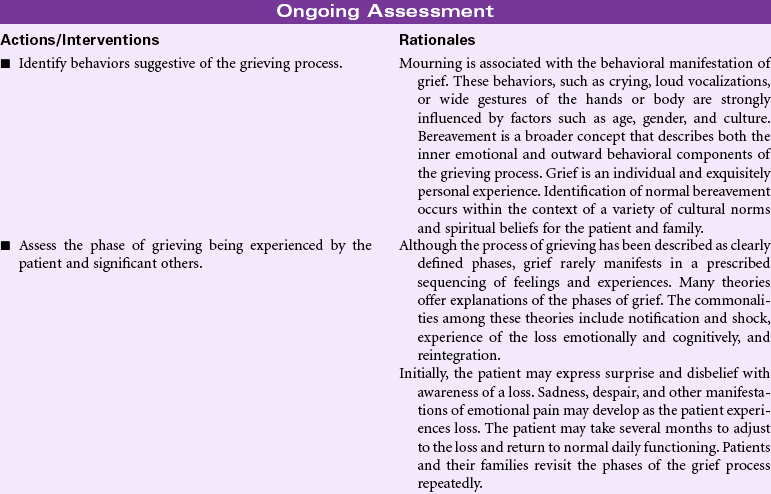
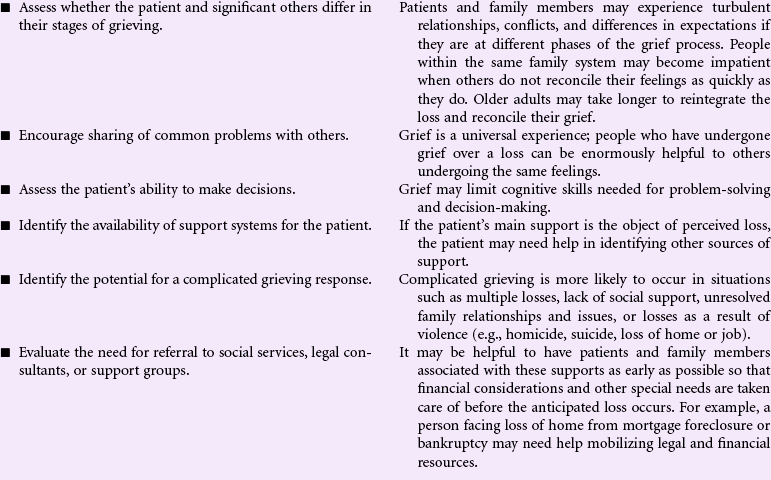
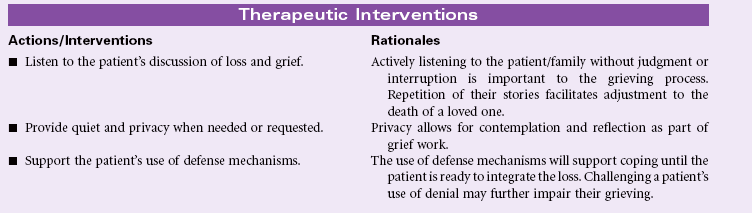
Grieving
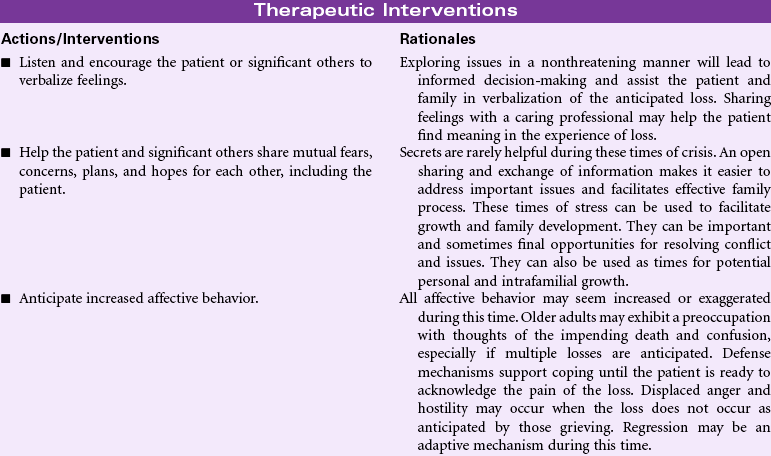
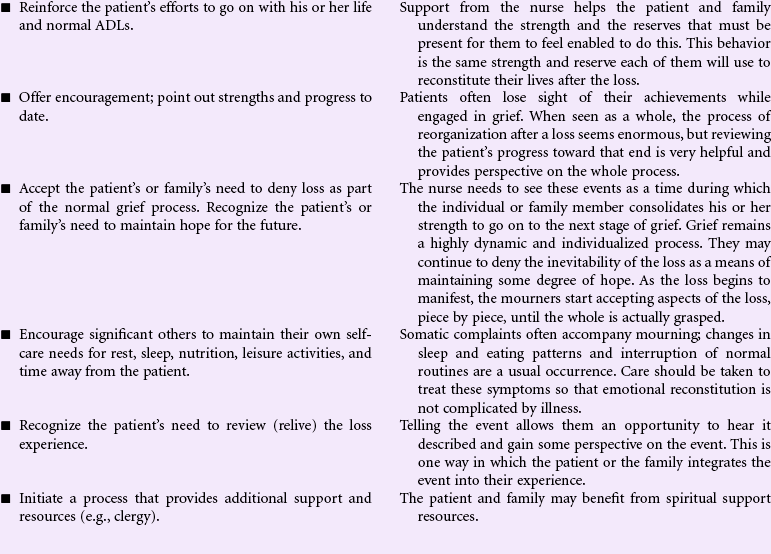
Definition: A normal complex process that includes emotional, physical, spiritual, social, and intellectual responses and behaviors by which individuals, families, and communities incorporate an actual, anticipated, or perceived loss into their daily lives
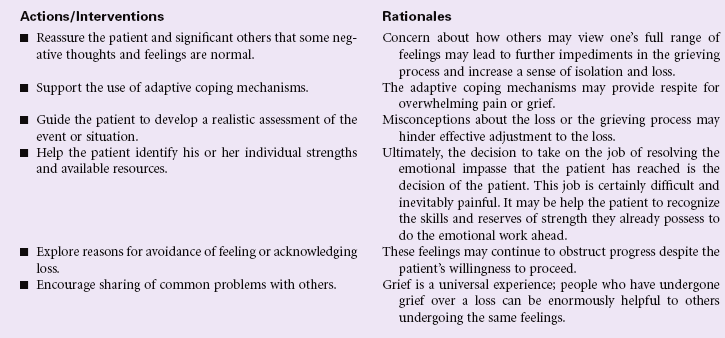
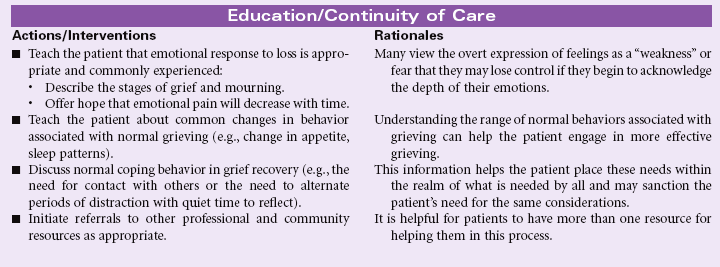
Grieving is an individual’s emotional response to a perceived or actual loss. Patients may experience grieving associated with the death of a loved one or loss of a body part. People grieve when they learn of a terminal diagnosis for themselves or a loved one. Grieving may be experienced by patients and their families as they face long-term illness or disability, divorce, loss of employment, or loss of home or personal possessions. Grief is an aspect of the human condition that touches every individual, but how an individual or a family system responds to loss and how grief is expressed varies widely. That process is strongly influenced by factors such as age, gender, and culture, as well as personal and intrafamilial reserves and strengths. The nurse will encounter the patient and family experiencing grief in the hospital setting, but increasingly, with more hospice and palliative care services provided in the community, the nurse will find patients struggling with these issues in their own homes, where professional help may be limited or fragmented. This care plan discusses measures the nurse can use to help the patient and family members begin the process of grieving. Additional interventions related to death and dying can be found on p. 276.

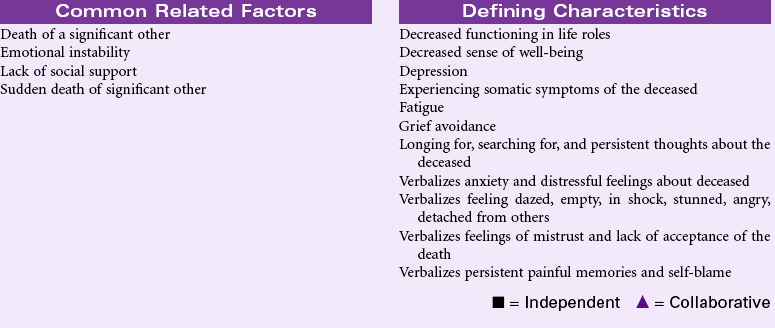
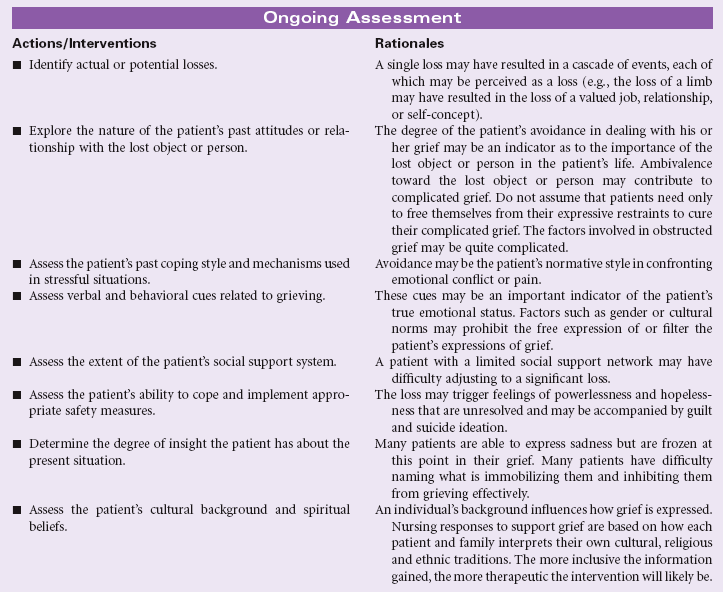
Complicated Grieving
Definition: A disorder that occurs after the death of a significant other, in which the experience of distress accompanying bereavement fails to follow normative expectations and manifests in functional impairment
Complicated grieving is a state in which an individual has significant difficulty adjusting to an actual or perceived loss. This period of prolonged bereavement may subsequently impair further the individual’s daily functioning. Complicated grief may be marked by a broad range of behaviors, including pervasive denial or a refusal to partake in self-care measures or ADLs. It may be marked by excessive use of alcohol or drugs or the inability to maintain one’s business or home life. Because all of these behaviors can be seen at one time or another as an emotional response in individuals who are mourning a loss, a distinction must be made between the transient use of these normal adaptive grief responses and their use to the extent that it paralyzes the person’s ability to grow and develop as an individual. Because there is no temporal restriction on the time it takes to mourn a loss, the most reliable indicator may be the mourner himself or herself. When an individual reaches a point when he or she is discomforted by the inability to go on with his or her life, then the issue of complicated or dysfunctional grieving bears exploration. The nurse may encounter patients experiencing complicated grief in the outpatient setting or in the hospital. They may have physical symptoms reflective of their inability to monitor or care for their own health, or they may have symptoms reflective of chronic emotional or physical illness. Complicated grief may be the outcome of an individual’s experience of being at odds with gender, cultural, or their own behavioral norms, which prohibits them from grieving successfully. The nurse may be in a position to help individuals recognize the role that complicated grief has played in their current impasse, and the nurse may be able to help the patient create a framework and environment in which it is safe to begin to mourn.

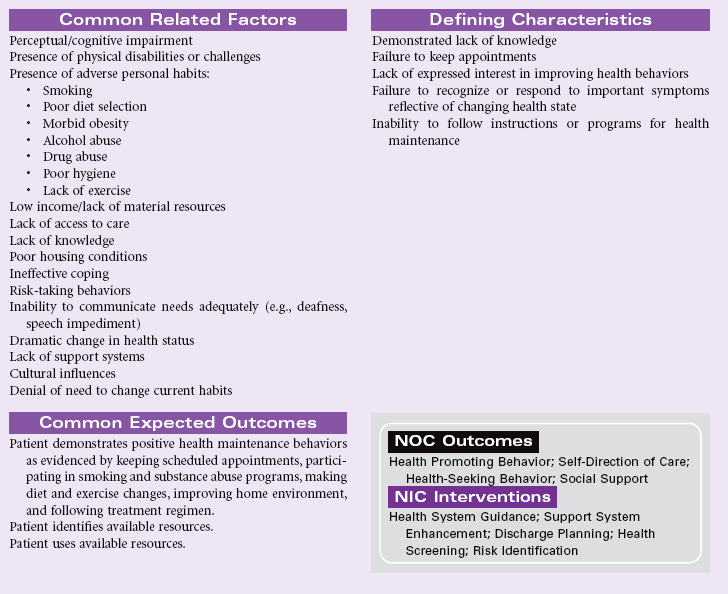
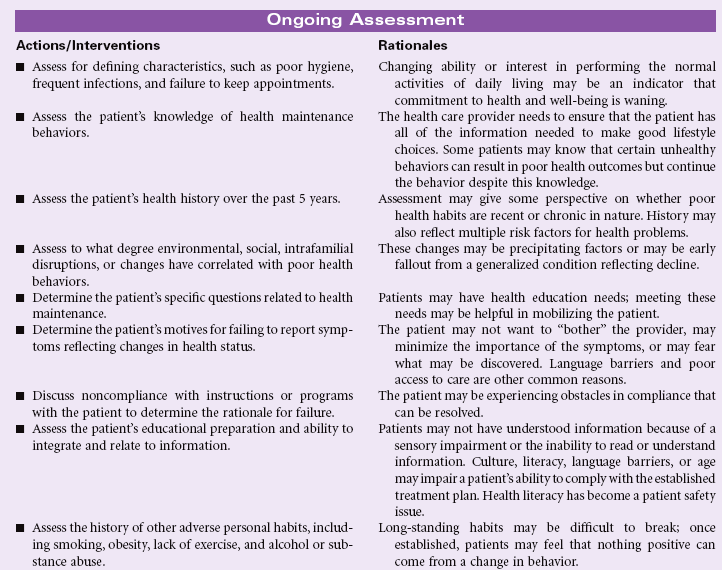
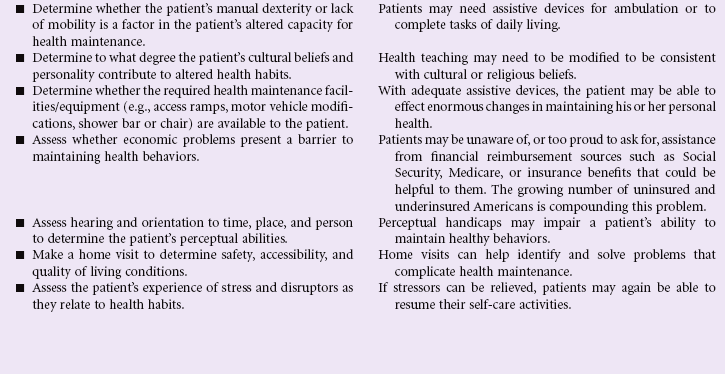
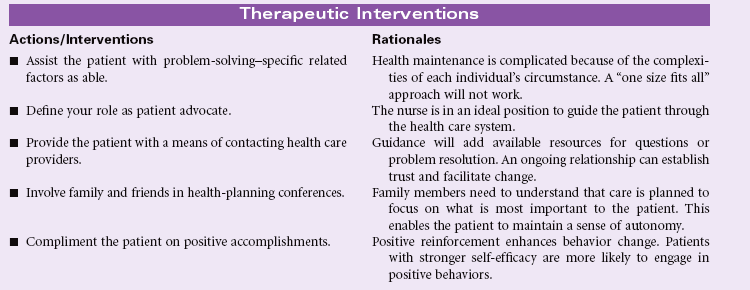
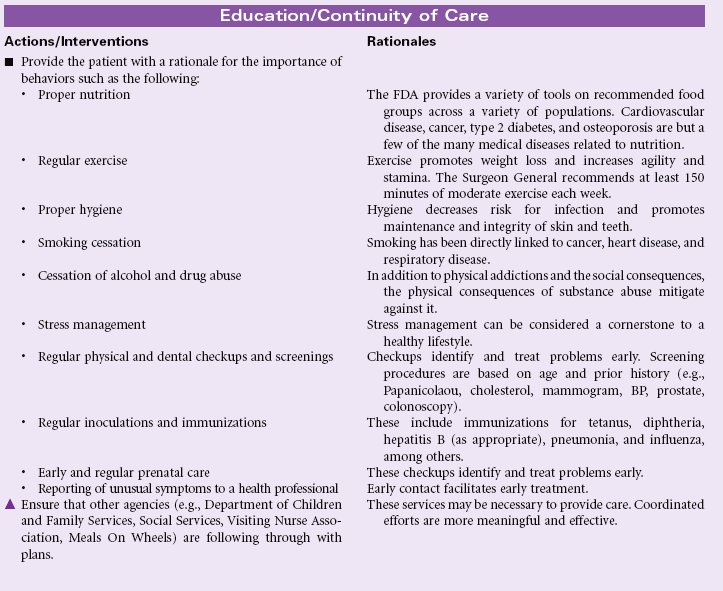
Ineffective Health Maintenance
Definition: Inability to identify, manage, and/or seek help to maintain health
Ineffective health maintenance reflects a change in an individual’s ability to perform the functions necessary to maintain health or wellness. That individual may already manifest symptoms of existing or impending physical ailment or display behaviors that are strongly or certainly linked to disease. The nurse’s role is to identify factors that contribute to an individual’s inability to maintain healthy behavior and implement measures that will result in improved health maintenance activities. The nurse may encounter these patients either in the hospital or in the community; the increased presence of the nurse in the community and home health settings improves the ability to assess patients in their own environment. Patients most likely to experience more than transient alterations in their ability to maintain their health are those whose age or infirmity (either physical or emotional) absorb much of their resources or those for whom the economic challenges of daily life negate an interest in personal health. The task before the nurse is to identify measures that will be successful in empowering patients to maintain their own health within the limits of their ability.
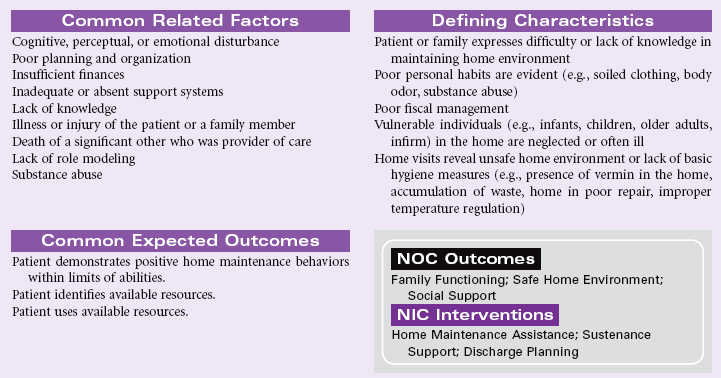
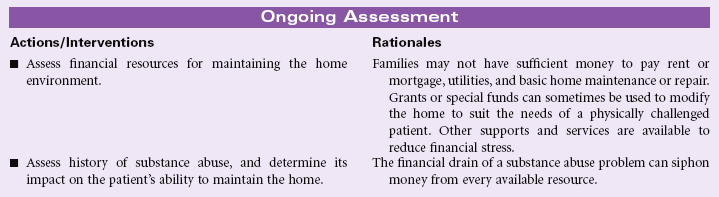
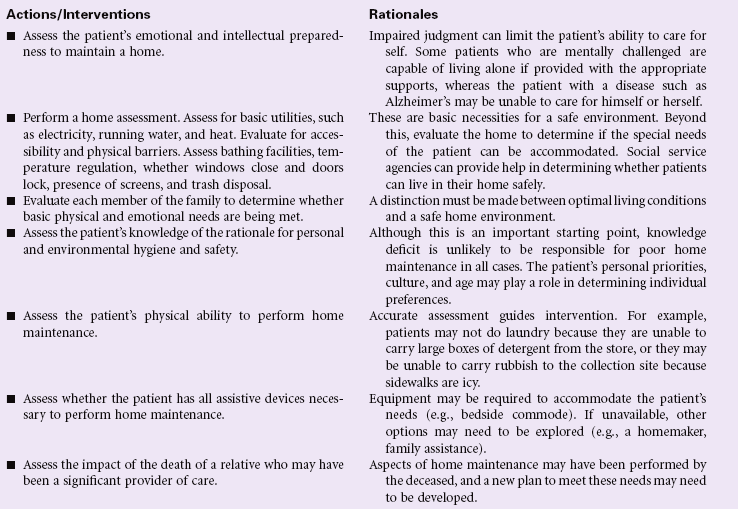
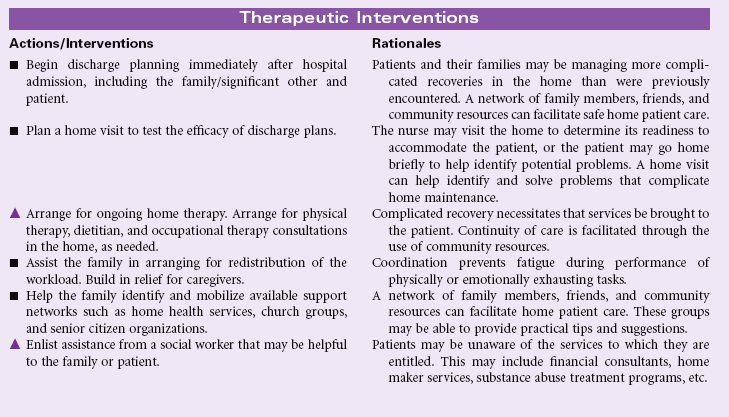
Impaired Home Maintenance
Definition: Inability to independently maintain a safe growth-promoting immediate environment
Individuals within a home establish a normative pattern of operation. A vast number of factors can negatively affect that operational baseline. When this happens, an individual or an entire family may experience a disruption that is significant enough to impair the management of the home environment. Health or safety may be threatened, and there may be a threat to relationships or to the physical well-being of the people living in the home. An inability to perform the activities necessary to maintain a home may be the result of the development of chronic mental or physical disabilities, or acute conditions or circumstances that severely affect the vulnerable members of the household. As a result of early hospital discharges, nurses are coordinating complicated recovery regimens in the homes of patients. The patient’s home must be safe and suited to the recovery needs of the individual. Patients must have the resources needed to provide for themselves and their families during recovery or following a debilitating illness. Because there is considerable room for cultural and intrafamilial variations in the maintenance of a home, the nurse should be guided by principles of safety when evaluating a home environment.
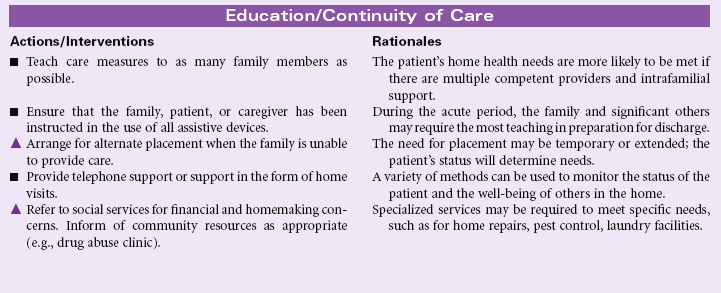
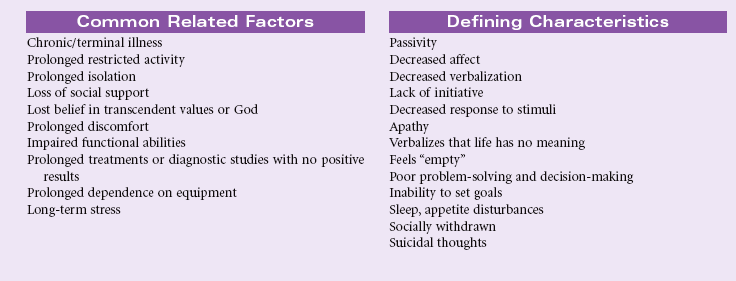
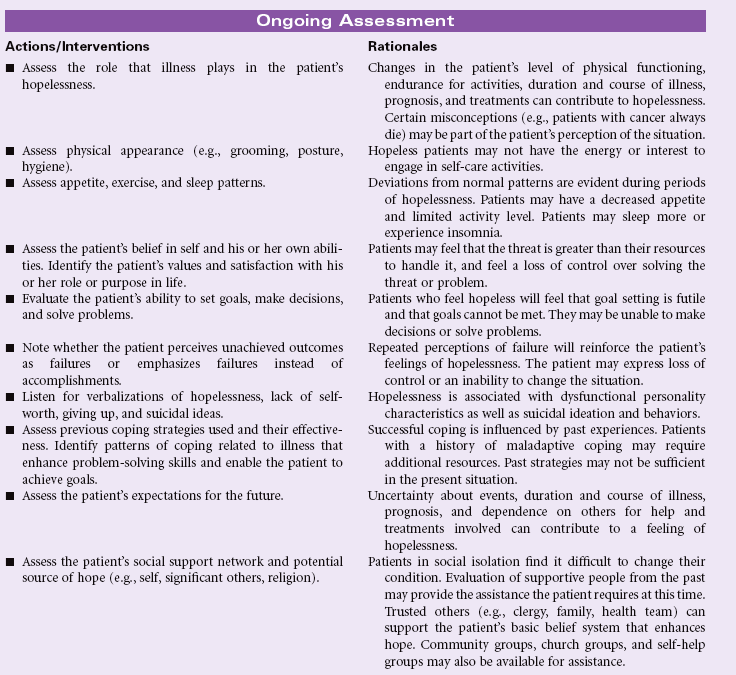
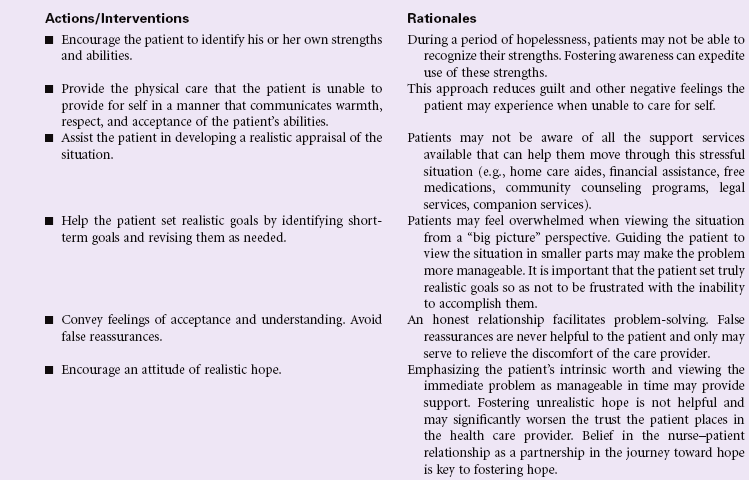
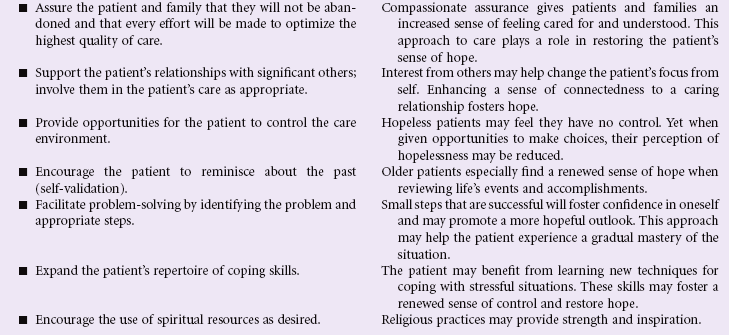
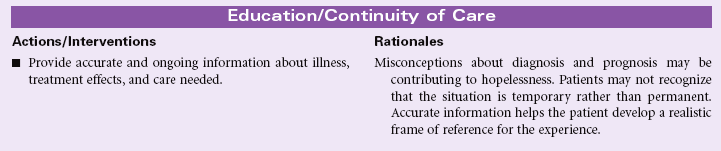
Hopelessness
Definition: Subjective state in which an individual sees limited or no alternatives or personal choices available and is unable to mobilize energy on own behalf
A person may experience hopelessness in response to a sudden event, such as spinal cord injury that leaves the patient with permanent paralysis. Hopelessness may be the result of a lifetime of multiple stresses and losses that leave the patient no longer able to mobilize the energy needed to act in his or her own behalf. Chronic diseases associated with progressive loss of functional ability may contribute to the patient’s sense of hopelessness, especially if the person sees no chance for improvement with continued treatment. Hopelessness is evident in patients living in social isolation, who are lonely and have no social support system or resources. Patients living in poverty, the homeless, and those with limited access to health care all may feel hopeless about changing their health care status and being able to cope with life events. Loss of belief in God’s care or loss of trust in prior spiritual beliefs may foster a sense of hopelessness.



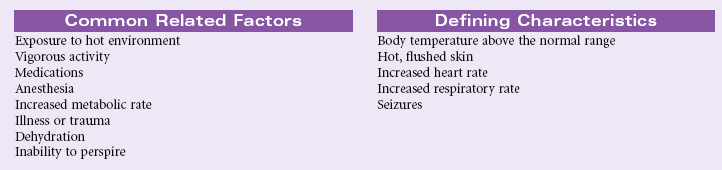
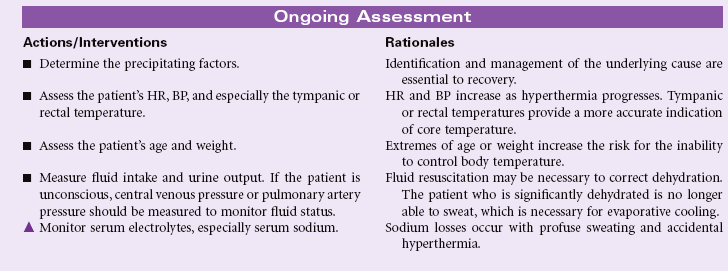
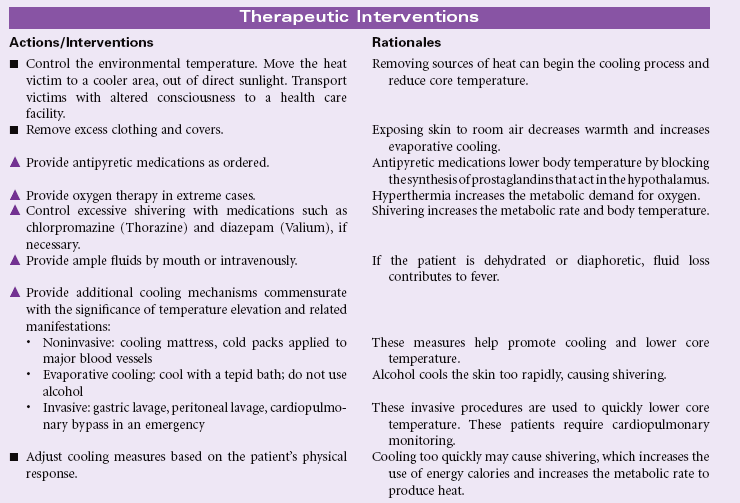
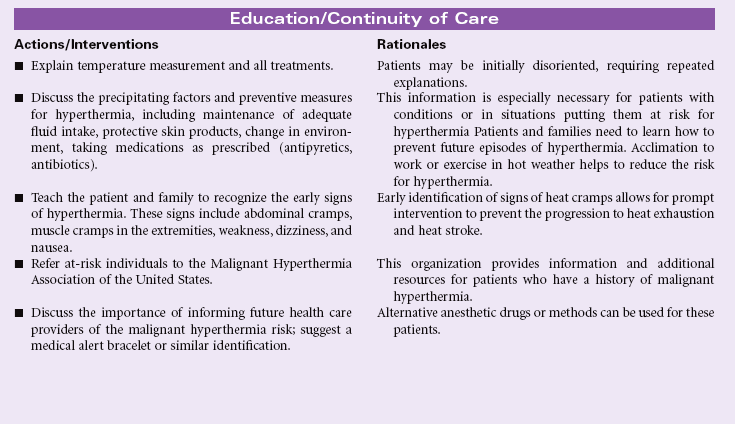
Hyperthermia
Definition: Body temperature elevated above normal range
Hyperthermia is a sustained core temperature above the normal variance, usually greater than 39° C (102.2° F). Adults may experience nerve damage and seizures when core body temperature is 41° C (105.8° F). Temperatures of 43° C (109.4° F) or higher are incompatible with life. Hyperthermia differs from fever in that the hypothalamic set point is not reset at a higher level. Also, hyperthermia is not stimulated by pyrogens, such as occurs with infection. Many cases of hyperthermia result from the combined effects of activity and salt and water deprivation in a hot environment, such as when athletes perform in extremely hot weather or when older adults avoid the use of air conditioning because of expense. Hyperthermia may occur more readily in persons who have endocrine disorders; use alcohol; or take diuretics, anticholinergics, or phototoxic agents. Forms of accidental hyperthermia include heat cramps, heat exhaustion, and heat stroke. Malignant hyperthermia is a life-threatening response to various anesthetic agents. This inherited disorder affects calcium metabolism in muscle cells, causing fever, muscle rigidity, metabolic acidosis, dysrhythmic tachycardia, hypertension, and hypoxia. Careful evaluation of preoperative patients is essential for prevention.

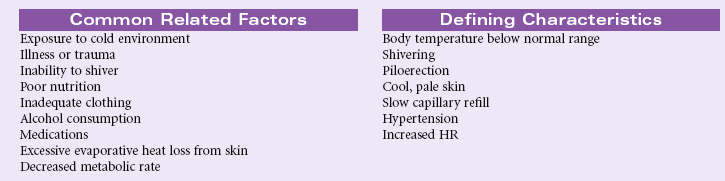
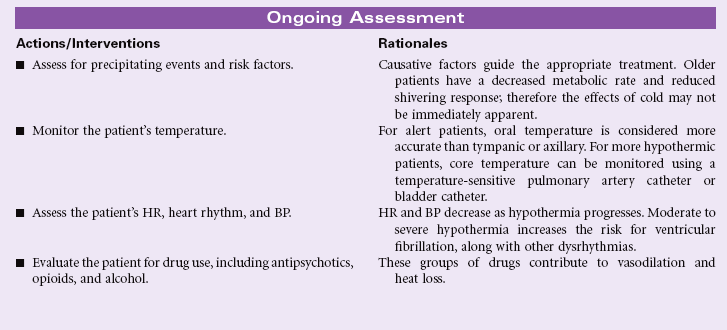
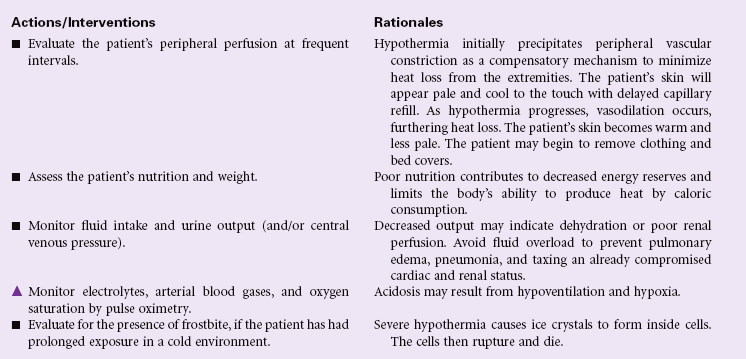
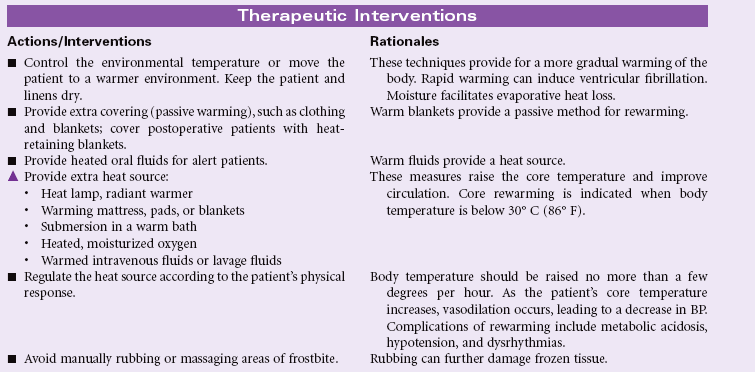
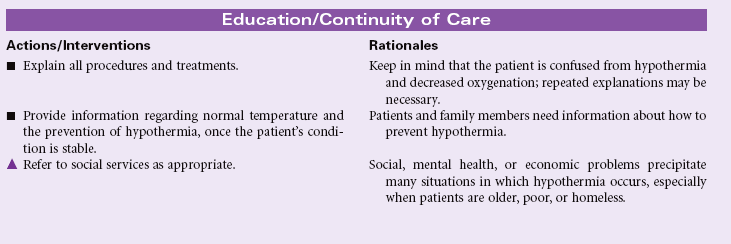
Hypothermia
Definition: Body temperature below normal range
Hypothermia is a core temperature at a significantly lower level than normal; usually lower than 35° C (95° F) measured by the tympanic and rectal routes. Hypothermia results when the body cannot produce heat at a rate equal to that lost to the environment through conduction, convection, radiation, or evaporation. Core temperature below 3°C (89.6° F) is severe and life threatening. Hypothermia can be classified as inadvertent (seen postoperatively), intentional (for medical purposes), or accidental (exposure related). Older adults are especially vulnerable to accidental hypothermia because of age-related alterations in normal thermoregulation.

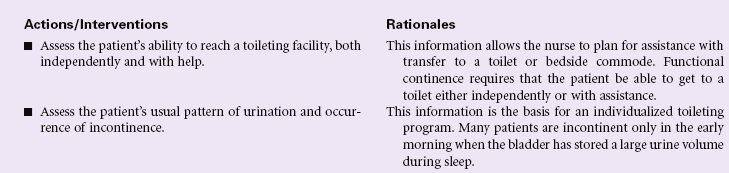
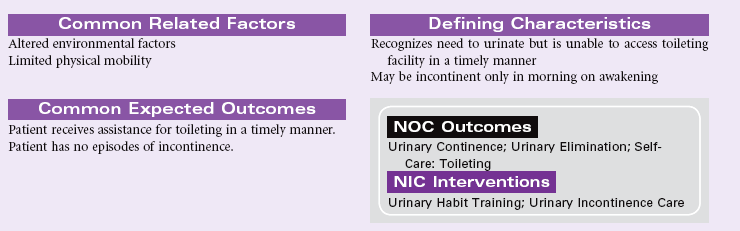
Functional Urinary Incontinence
Definition: Inability of usually continent person to reach toilet in time to avoid unintentional loss of urine
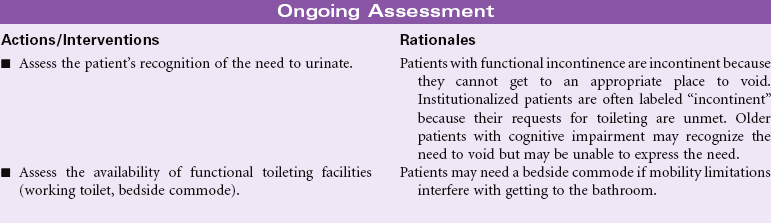
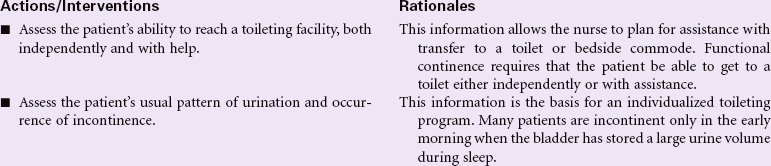
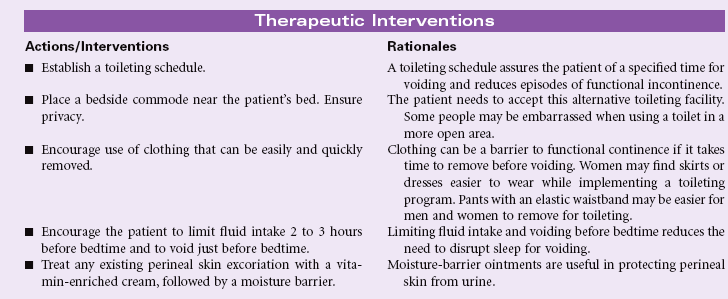
The person with functional urinary incontinence has normal function of the neurological control mechanisms for urination. The bladder is able to fill and store urine appropriately. The person is able to recognize the urge to void. The most common problem is environmental barriers that make it difficult for the person to reach an appropriate receptacle for voiding. This type of incontinence occurs more often in older adults, who have mobility limitations. People with arthritis of the hands may have difficulty undoing clothing buttons or zippers to prepare for voiding. The patient with limited mobility may be dependent on others for help transferring to a bedside commode or ambulating to the bathroom. If mobility assistance is not readily available, the person is not able to suppress the urge to void and becomes incontinent. Wet clothing, urine odor, and the loss of independence for toileting contribute to the person’s feelings of embarrassment in this situation. Over time the person may have changes in body image and self-concept.
Reflex Urinary Incontinence
Definition: Involuntary loss of urine at somewhat predictable intervals when a specific bladder volume is reached
Reflex urinary incontinence represents dysfunction of the normal neurological control mechanisms for coordination of detrusor contraction and sphincter relaxation. Neurological disorders in the detrusor motor area of the brain result in detrusor hyperreflexia. Examples of such disorders include strokes, traumatic brain injury, hydrocephalus, tumors, Alzheimer’s disease, and multiple sclerosis. Cervical and thoracic spinal cord injuries and Guillain-Barré syndrome may cause detrusor hyperreflexia with sphincter dyssynergia. The patient with reflex incontinence experiences periodic urination without an awareness of needing to void. Urination is frequent throughout the day and night. Urine volume is consistent with each voiding. Residual urine volumes are usually less than 50 mL. Urodynamic studies will indicate detrusor contraction when bladder volume reaches a specific amount.
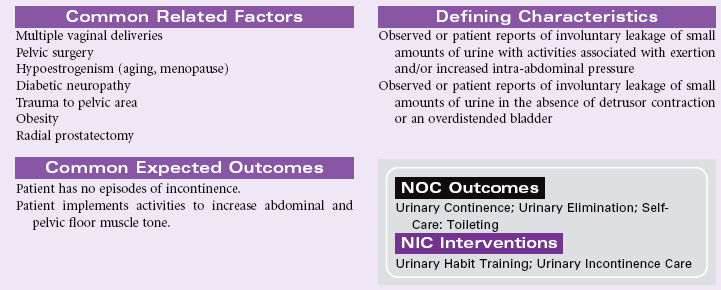
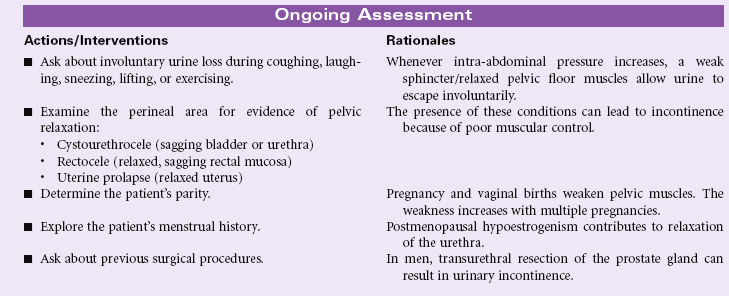
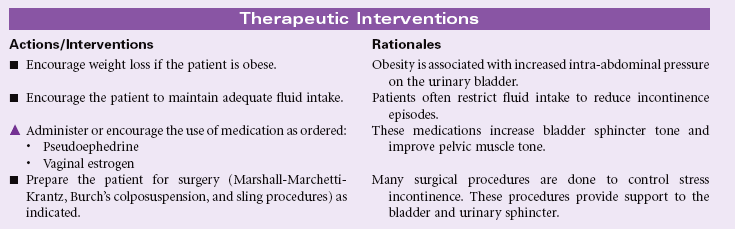
Stress Urinary Incontinence
Definition: Sudden leakage of urine with activities that increase intraabdominal pressure
Stress incontinence occurs more often in women than men. The predisposing factors for women include pregnancy, obesity, decreased estrogen levels associated with menopause, and surgery involving the lower abdominal area. Men may develop stress incontinence following surgical treatment for benign prostatic hyperplasia or prostate cancer. These factors contribute to a decrease in muscle tone at the urethrovesical junction. When the muscles of the abdomen and pelvic floor are weak, they no longer provide support for the urinary sphincter. The urinary sphincter cannot remain constricted with increasing abdominal pressure. Straining with defecation, laughing, sneezing, coughing, heavy lifting, jumping, or running are examples of activities that increase intraabdominal pressure and lead to stress incontinence. The amount of urine lost may vary from a few drops to 100 mL or more. Regardless of the amount of urine lost during a stress incontinence episode, the person may experience embarrassment and changes in body image and self-concept. As a result, the person may decrease social interactions and physical activities to minimize the risks of incontinence occurring in public situations.
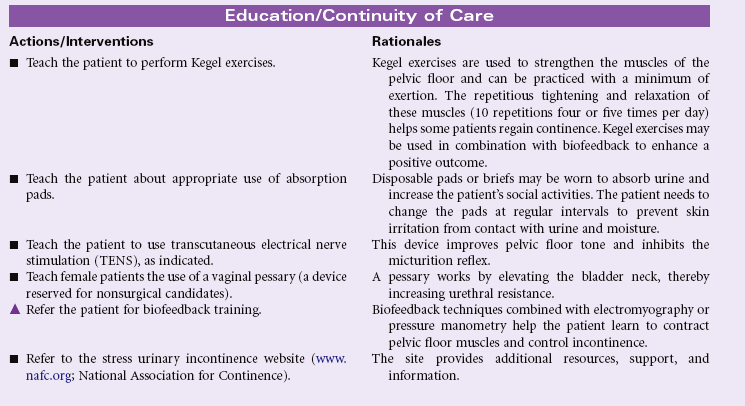
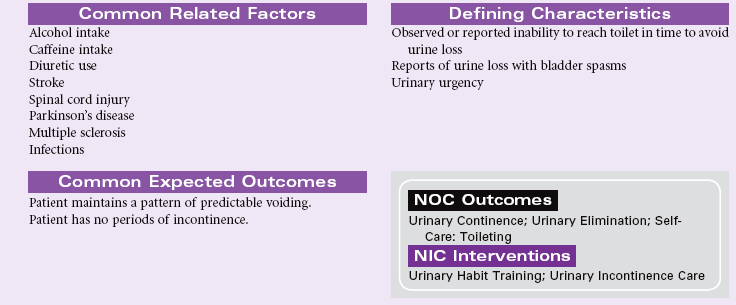
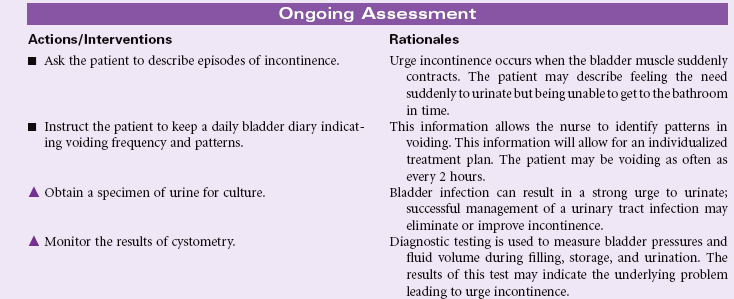
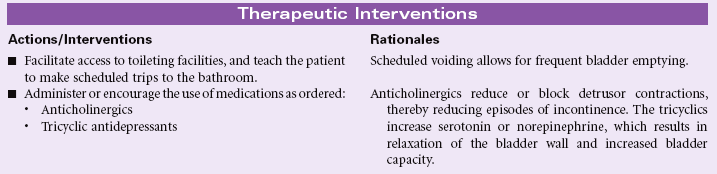
Urge Urinary Incontinence
Definition: Involuntary passage of urine occurring soon after a strong sense of urgency to void
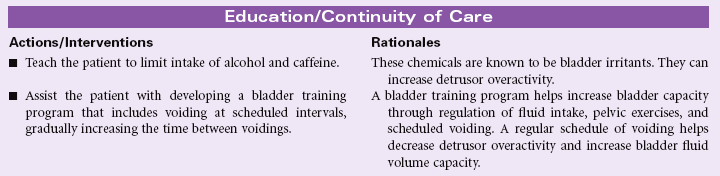
Urge urinary incontinence is associated with overactivity or uncontrolled contraction of the detrusor muscle. The person has uncontrolled passage of urine within a few seconds to a few minutes after feeling a strong sense of urgency to void. The person is unable to voluntarily suppress voiding once the urge is felt. Urge incontinence may develop as a result of spinal cord lesions or following pelvic surgery. Central nervous system disorders such as Alzheimer’s disease, multiple sclerosis, and Parkinson’s disease may contribute to urge incontinence. Overactivity of the detrusor may be the result of interstitial cystitis, urinary tract infection, or pelvic radiation. Excessive alcohol or caffeine intake may stimulate urge incontinence. As with other types of urinary incontinence, the person with urge incontinence may experience embarrassment with loss of control of urinary elimination. The person begins to plan activities to be close to a toilet at all times. This change in behavior may affect the person’s social interaction and work performance.

Risk for Infection
Definition: At increased risk for being invaded by pathogenic organisms
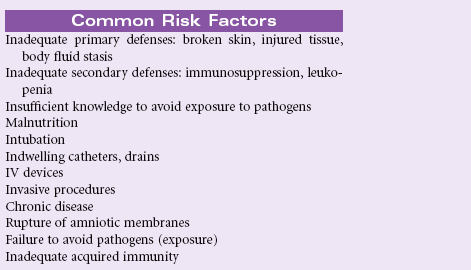
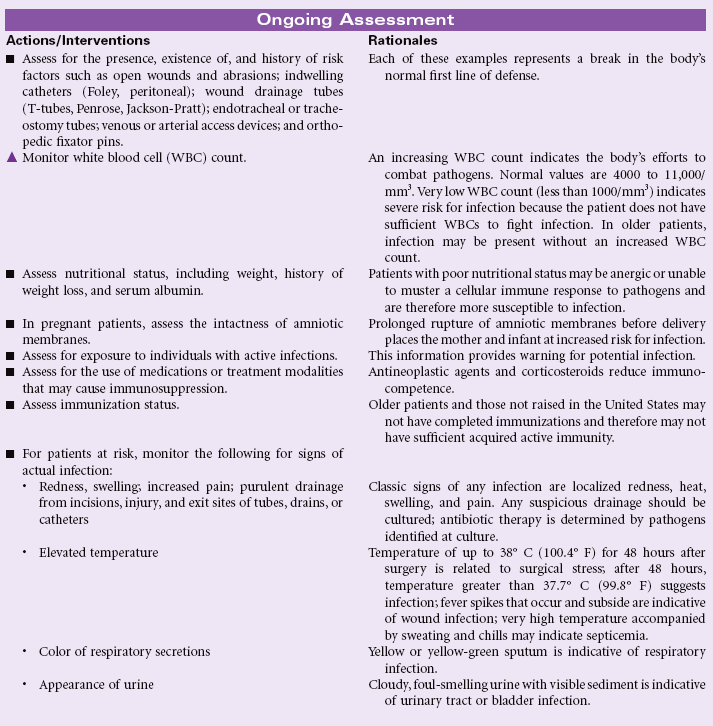
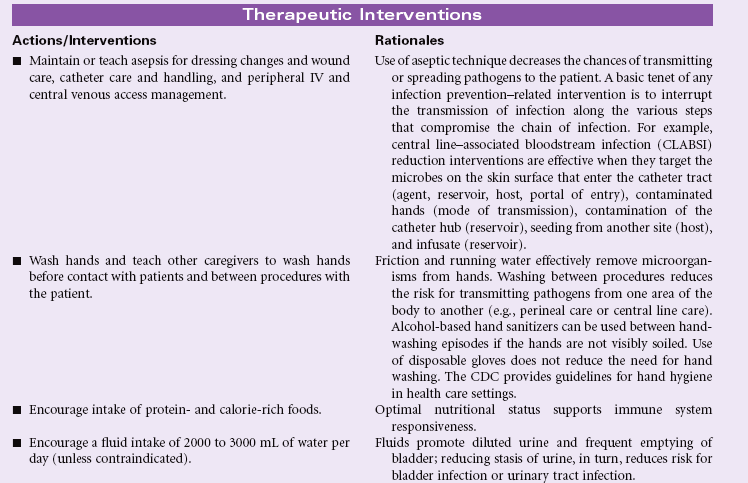
People at risk for infection are those whose natural defense mechanisms are inadequate to protect them from the inevitable injuries and exposures that occur throughout the course of living. Infections occur when an organism (e.g., bacterium, virus, fungus, or other parasite) invades a susceptible host. Breaks in the integument, the body’s first line of defense, and/or the mucous membranes allow invasion by pathogens. If the patient’s immune system cannot combat the invading organism adequately, an infection occurs. Open wounds, traumatic or surgical, can be sites for infection; soft tissues (cells, fat, muscle) and organs (kidneys, lungs) can also be sites for infection after trauma, invasive procedures, or invasion of pathogens carried through the bloodstream or lymphatic system. Infections can be transmitted by contact or through airborne transmission, sexual contact, or sharing of IV drug paraphernalia. Being malnourished, having inadequate resources for sanitary living conditions, and lacking knowledge about disease transmission place individuals at risk for infection. Health care workers, to protect themselves and others from disease transmission, must understand how to take precautions to prevent transmission. Because identification of infected individuals is not always apparent, standard precautions recommended by the Centers for Disease Control and Prevention (CDC) are widely practiced. The Agency for Healthcare Research and Quality (AHRQ) published important guidelines and recommendations in this resource: Patient Safety and Quality: An Evidence-Based Handbook for Nurses. In addition, the Occupational Safety and Health Administration (OSHA) set forth the Bloodborne Pathogens Standard, developed to protect workers and the public from infection. Ease of and increase in world travel also have increased opportunities for transmission of disease from abroad. Infections prolong healing and can result in death if untreated. Antimicrobials are used to treat infections when susceptibility is present. Organisms may become resistant to antimicrobials, requiring multiple antimicrobial therapy. For some organisms no antimicrobial is effective, such as the human immunodeficiency virus (HIV).


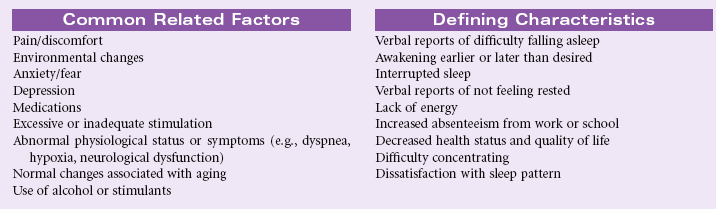
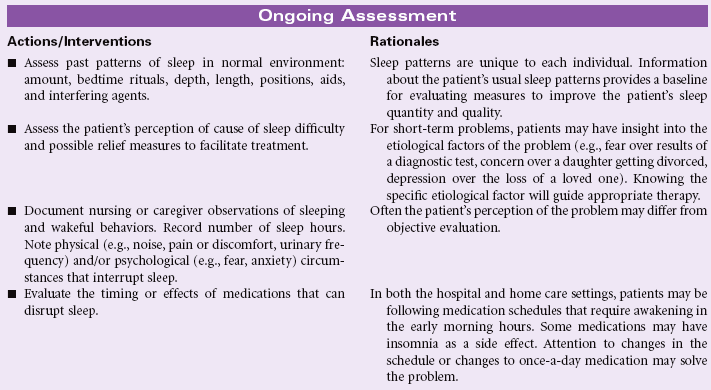
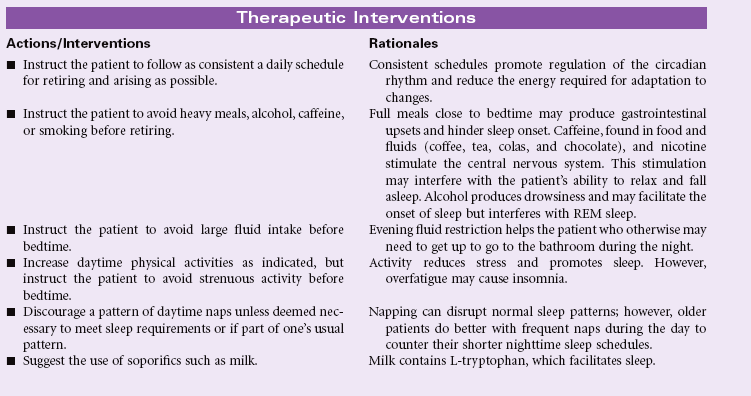
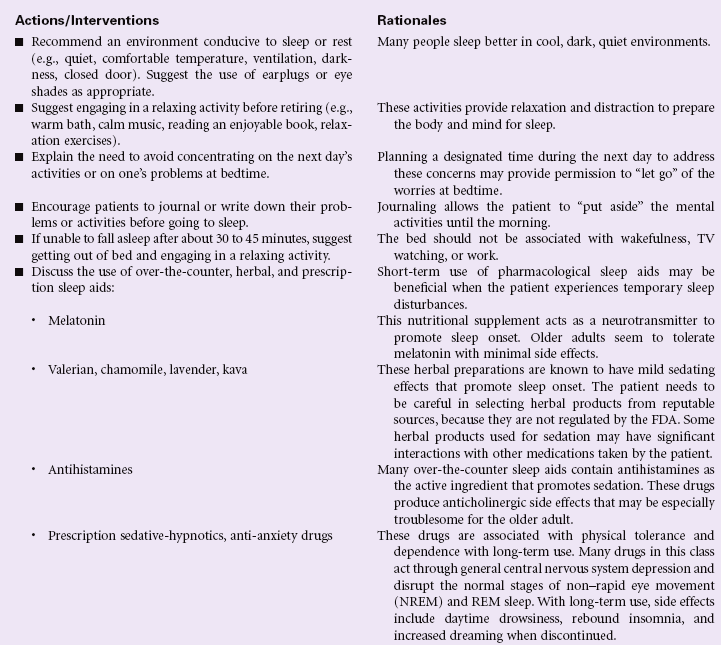
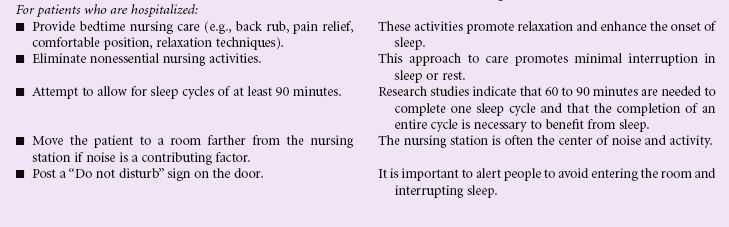
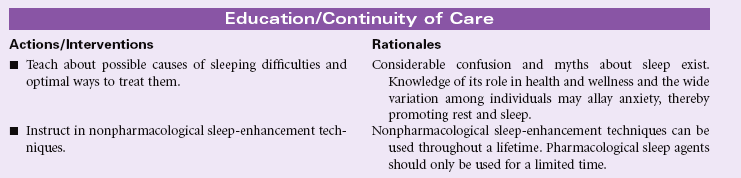
Insomnia
Definition: A disruption in amount and quality of sleep that impairs functioning
Sleep is required to provide energy for physical and mental activities. The disruption in the individual’s usual diurnal pattern of sleep and wakefulness may be temporary or chronic. Short-term insomnia may occur in response to changes in work schedules, temporary stressors, or travel across several time zones. Long-term insomnia is associated with alcohol and drug abuse, chronic pain, chronic depression, obesity, and aging. Such disruptions may result in both subjective distress and apparent impairment in functional abilities. Sleep patterns can be affected by environment, especially in hospital critical care units. These patients experience insomnia secondary to the noisy, bright environment and frequent monitoring and treatments. Such sleep disturbance is a significant stressor in the intensive care unit and can affect recovery. The care plan focuses on nursing care to manage insomnia in the acute care and home setting.

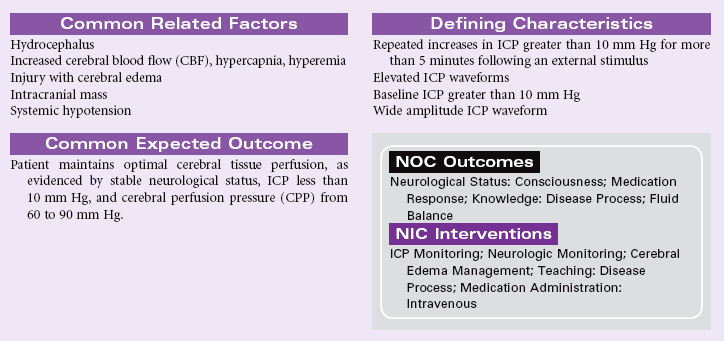
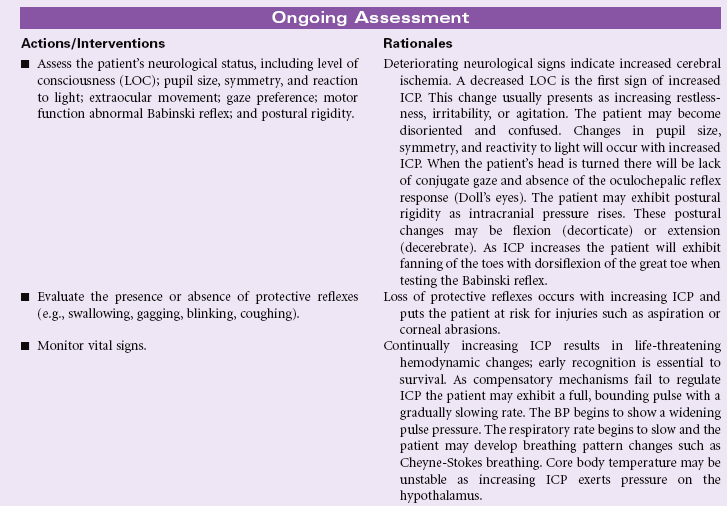
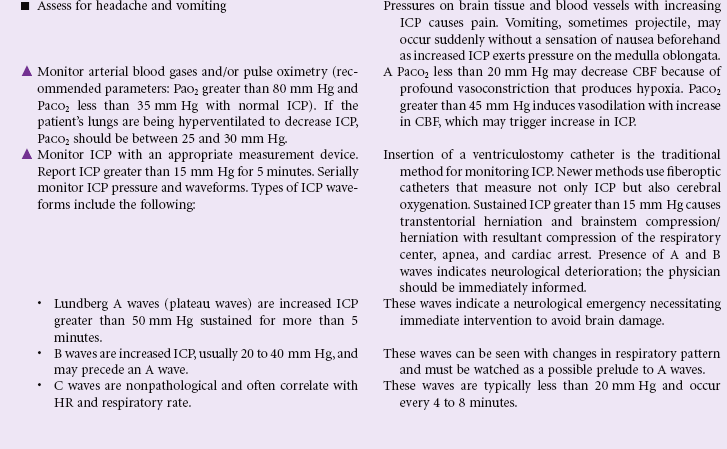
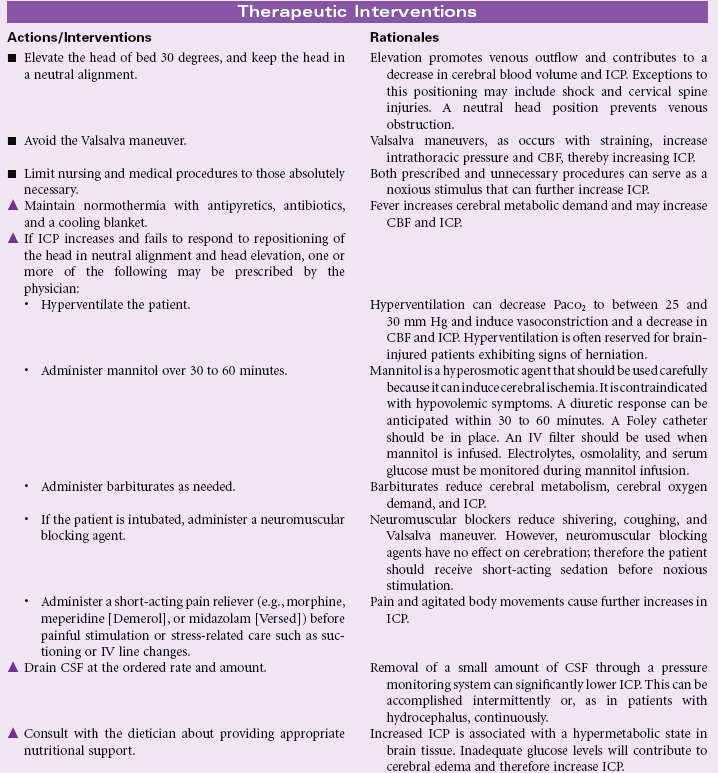
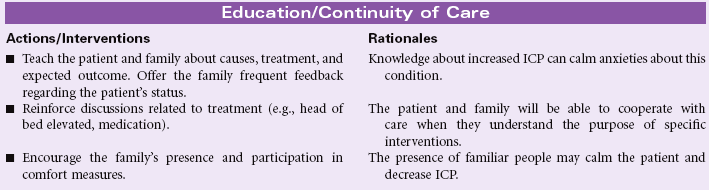
Decreased Intracranial Adaptive Capacity
Definition: Intracranial fluid dynamic mechanisms that normally compensate for increases in intracranial volumes are compromised, resulting in repeated disproportionate increases in intracranial pressure in response to a variety of noxious and non-noxious stimuli
Intracranial pressure (ICP) reflects the pressure exerted by the intracranial components of blood, brain, and cerebrospinal fluid (CSF), each ordinarily remaining at a constant volume within the rigid skull structure. Any additional fluid or mass (e.g., subdural hematoma, tumor, abscess) increases the pressure within the cranial vault. Because the total volume cannot change (Monro-Kellie hypothesis), blood, CSF, and ultimately brain tissue are forced out of the vault. The normal range of ICP is 5 to 15 mm Hg; elevations above that level occur normally but readily return to baseline parameters as a result of the adaptive capacity or compensatory mechanisms of the brain, blood, and CSF, such as vasoconstriction and increased venous outflow. In the event of disease, trauma, or a pathological condition, disturbances in autoregulation occur, and ICP is increased and sustained. Exceptions include people with unfused skull fractures (the skull is no longer rigid at the fracture site), infants whose suture lines are not yet fused (this is normal to accommodate growth), and older patients whose brain tissues have shrunk, taking up less volume in the skull (allowing for abnormal tissue growth or intracranial bleeding to occur for a longer period before ICP increases).

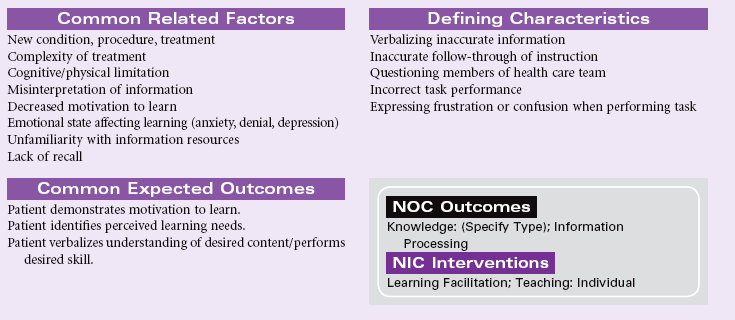
Deficient Knowledge
Definition: Absence or deficiency of cognitive information related to specific topic
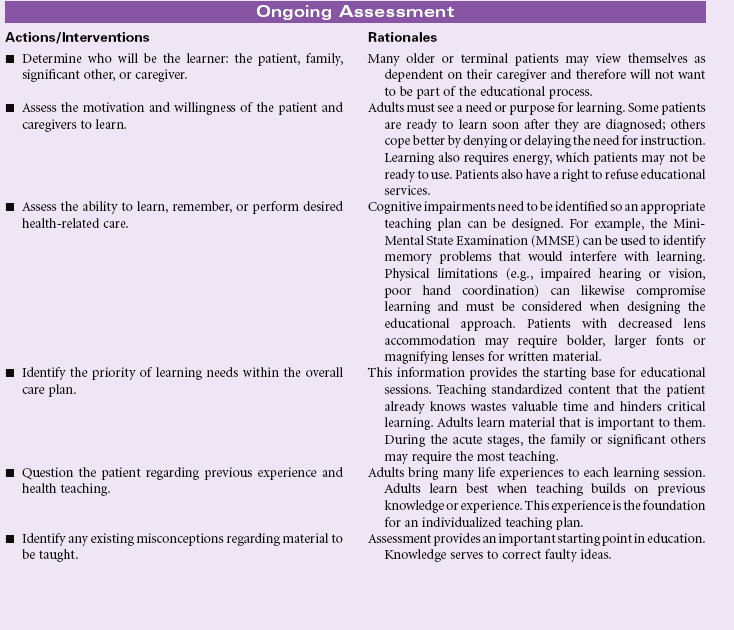
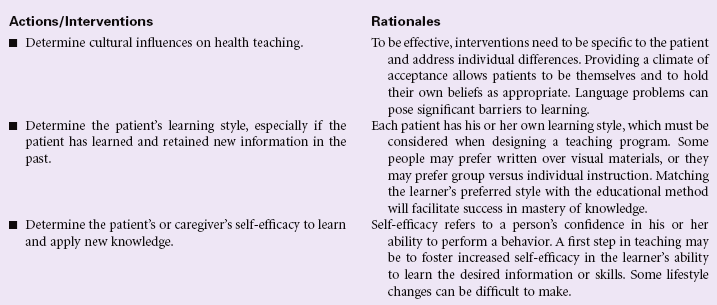
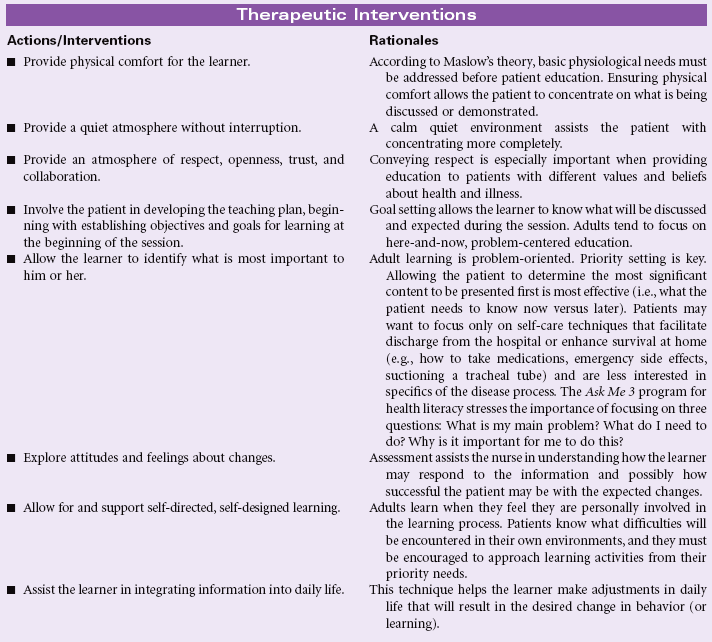
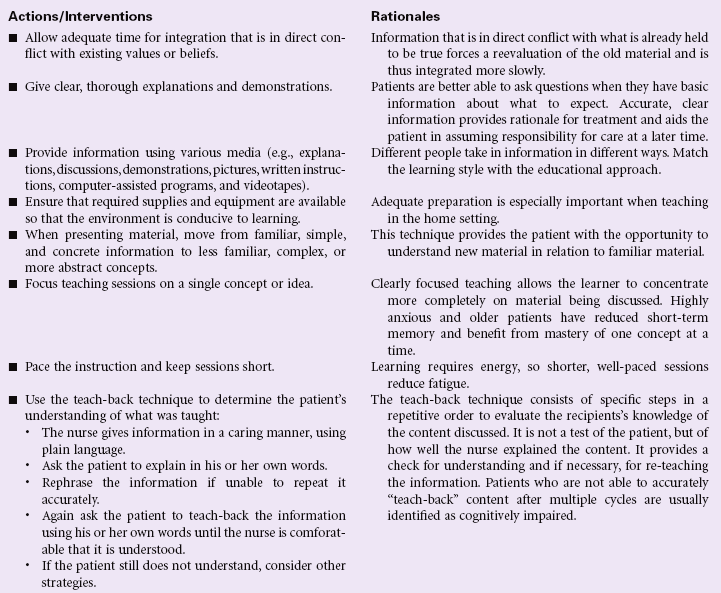
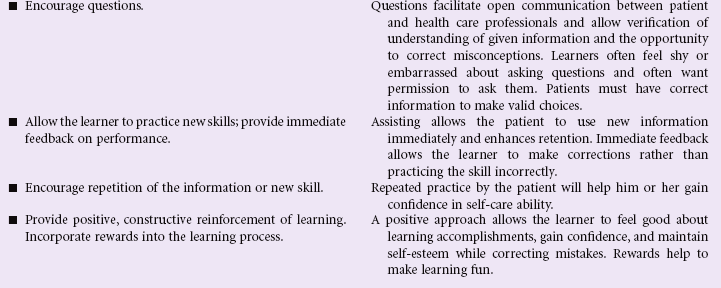
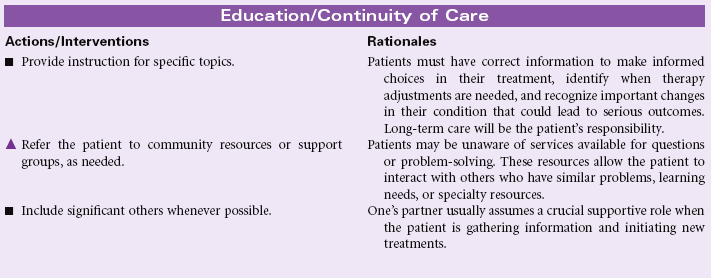
Knowledge deficit is a lack of cognitive information or psychomotor skills required for health recovery, maintenance, or health promotion. Teaching may take place in a hospital, ambulatory care, or home setting. The learner may be the patient, a family member, a significant other, or a caregiver unrelated to the patient. Learning may involve any of the three domains: cognitive domain (intellectual activities, problem-solving, and others); affective domain (feelings, attitudes, belief); and psychomotor domain (physical skills or procedures). The nurse must decide with the learner what to teach, when to teach, and how to teach the mutually agreed-upon content. Adult learning principles guide the teaching-learning process. Information should be made available when the patient wants and needs it, at the pace the patient determines, and using the teaching strategy the patient deems most effective. Many factors influence patient education, including age, cognitive level, developmental stage, physical limitations (e.g., visual, hearing, balance, hand coordination, strength), the primary disease process and comorbidities, and sociocultural factors. Older patients need more time for teaching and may have sensory-perceptual deficits/cognitive changes that may require a modification in teaching techniques. Certain ethnic and religious groups hold unique beliefs and health practices that must be considered when designing a teaching plan. These practices may vary from home remedies (e.g., special soups, poultices) and alternative therapies (e.g., massage, biofeedback, energy healing, macrobiotics, or megavitamins in place of prescribed medications) to reliance on an elder in the family to coordinate the care plan. Patients with low literacy skills will require educational programs that include more simplified treatment regimens, simplified teaching tools (e.g., cartoons, lower readability levels), a slower presentation pace, and techniques for cueing patients to initiate certain behaviors (e.g., pill schedule posted on refrigerator, timer for taking medications).The National Patient Safety Foundation has identified the pervasiveness of low health literacy and its implications for poorer health outcomes. It has launched the Ask Me 3 initiative to improve health communication between patients and providers.
Although the acute hospital setting provides challenges for patient education because of the high acuity and emotional stress inherent in this environment, the home setting can be similarly challenging because of the high expectations for patients or caregivers to self-manage complex procedures such as IV therapy, dialysis, or even ventilator care in the home. Caregivers are often overwhelmed by the responsibility delegated to them by the health care professionals. Many have their own health problems and may be unable to perform all the behaviors assigned to them because of visual limitations, generalized weakness, or feelings of inadequacy or exhaustion.
This care plan describes adult learning principles that can be incorporated into a teaching plan for use in any health care setting.

Sedentary Lifestyle
Definition: Reports a habit of life that is characterized by a low physical activity level
Today’s social changes have shifted lifestyles of once high physical effort to more sedentary ways of life, making physical inactivity a national problem. Unfortunately, many individuals do not actively seek out regular exercise routines, with more than 60% of Americans not exercising on a regular basis and 25% not exercising at all. The following table uses number of steps walked per day as a way to quantify levels of physical activity.
| Sedentary lifestyle | <5000 steps per day |
| Low active | 5000-7499 steps per day |
| Somewhat active | 7500-9999 steps per day |
| Active | 10,000-12,500 steps per day |
| Highly active | >12,500 steps per day |
From Tudor-Locke C, Bassett DR: How many steps/day are enough? Preliminary pedometer indices for public health, Sports Med 34(1):1, 2004.
Lack of physical activity can lead to many chronic conditions, including diabetes, heart disease, obesity, and various cancers. The 2008 Physical Activity Guidelines for Americans provides a science-based prescription for assisting individuals with improving their health through regular physical activity. Health benefits are attainable by individuals of all ages and even those with chronic medical problems. Stressful and busy lifestyles, socioeconomic factors, physical constraints, and lack of motivation are all barriers that can contribute to low physical activity. Nursing objectives are to educate patients on the importance of adopting an active lifestyle and to assist patients in finding ways to personalize the recommended exercise prescription.

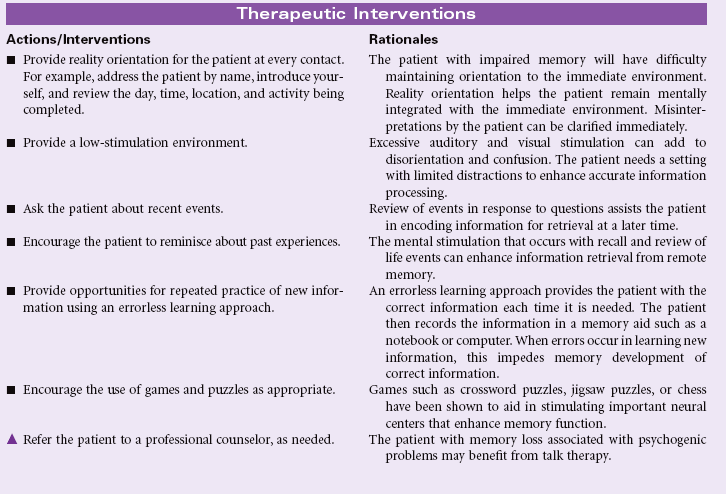
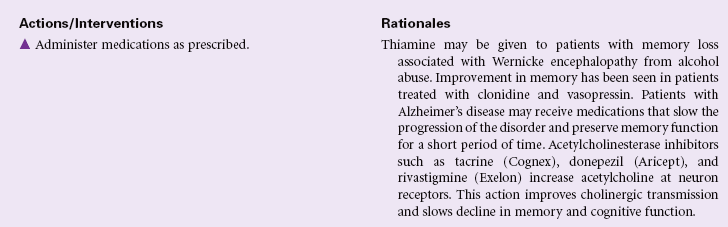
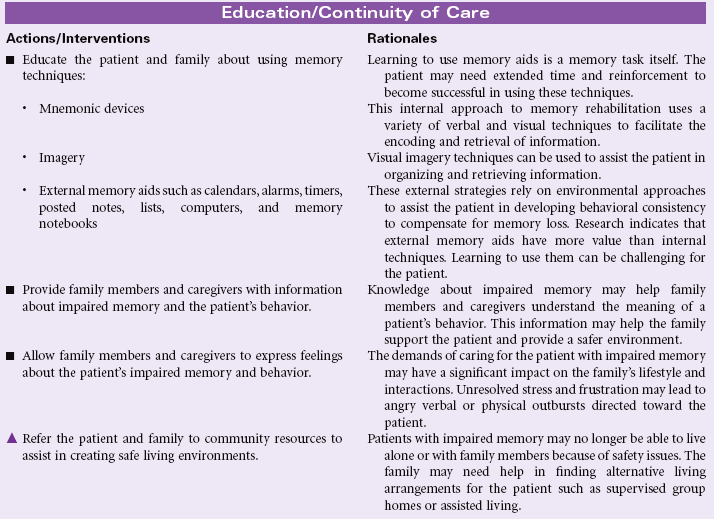
Impaired Memory
Definition: Inability to remember or recall bits of information or behavioral skills
Memory is the result of a complicated cognitive process used by an individual for learning, storing, and retrieving information. Cognitive abilities for reasoning, problem-solving, interpreting information, and communication are dependent on the diverse and complex neural network that supports information processing. Structurally, memories are formed by the complex interactions of the hippocampus, thalamus, hypothalamus, and temporal lobes. Any change that disrupts these neural networks may result in problems with transferring information between immediate, short-term, and long-term memory. Amnesia is the complete loss of memory ability. This type of memory impairment represents an inability to recall previously learned information and an inability to learn new information. Memory impairment may be temporary or permanent. Situations that are associated with impaired memory include seizures, head trauma, strokes, cerebral infections, brain tumors, vitamin B1 deficiency with alcohol abuse, personality disorders, and progressive degenerative dementias. Any clinical condition associated with decreased cardiac output or general hypoperfusion may contribute to impaired memory. Changes in recent memory often occur with organic disorders such as delirium, dementia, or chronic alcohol abuse. Diminished long-term or remote memory is associated with damage to the area of the cerebral cortex used for storage of that memory. This type of memory loss is seen in Alzheimer’s disease. Post-traumatic amnesia is an indicator of the severity of a closed head injury. Slowing of information processing and impaired episodic memory are common problems with head trauma. This care plan focuses on general care to support memory for the patient in the acute care or home setting.
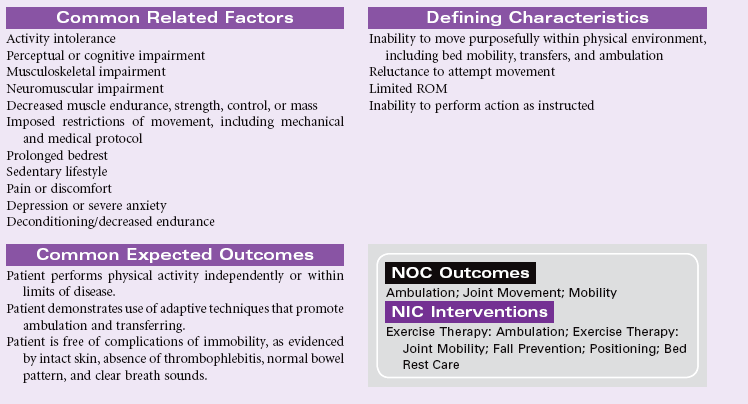
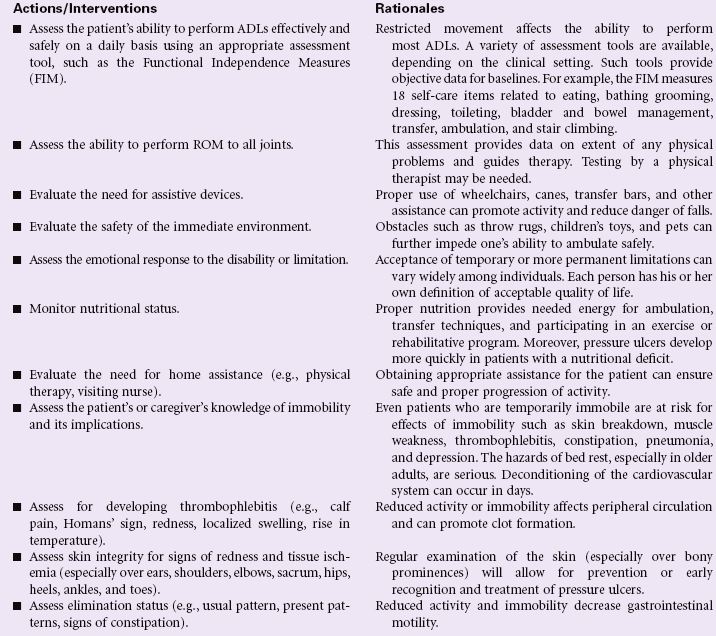
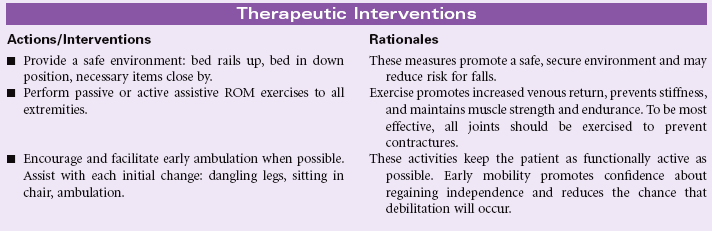
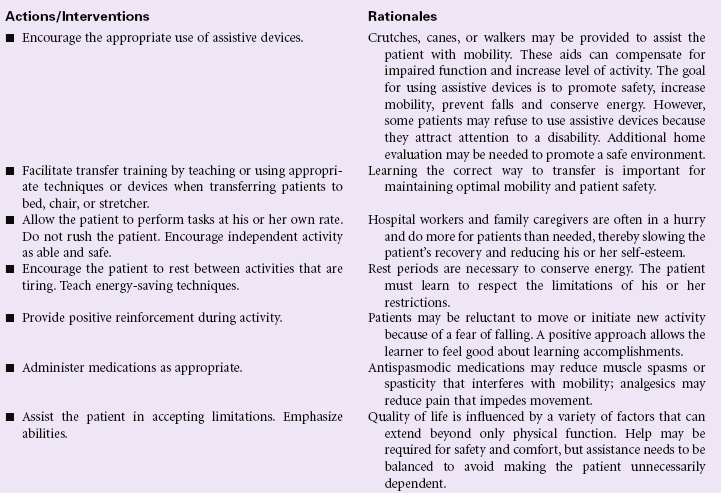
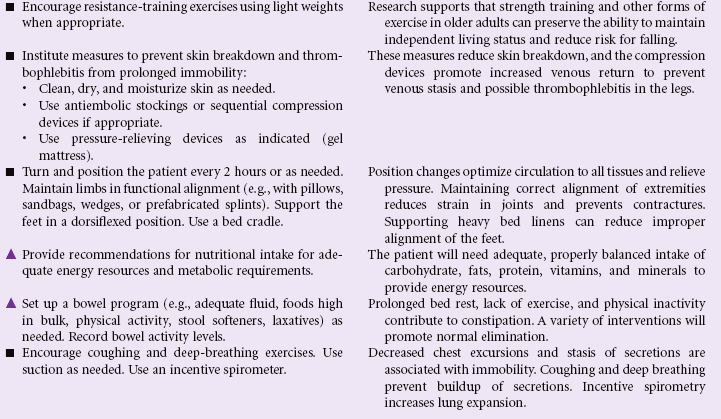
Impaired Physical Mobility
Definition: Limitation in independent, purposeful physical movement of the body or of one or more extremities
Alteration in mobility may be a temporary or more permanent problem. Most disease and rehabilitative states involve some degree of immobility (e.g., as seen in strokes, leg fracture, trauma, morbid obesity, multiple sclerosis). With the longer life expectancy for most Americans, the incidence of disease and disability continues to grow. With shorter hospital stays, patients are being transferred to rehabilitation facilities or sent home for physical therapy in the home environment.
Mobility is also related to body changes from aging. Loss of muscle mass, reduction in muscle strength and function, stiffer and less mobile joints, and gait changes affecting balance can significantly compromise the mobility of older patients. Mobility is paramount if older patients are to maintain any independent living. Restricted movement affects the performance of most ADLs. Older patients are also at increased risk for the complications of immobility. Nursing goals are to maintain functional ability, prevent additional impairment of physical activity, and ensure a safe environment.

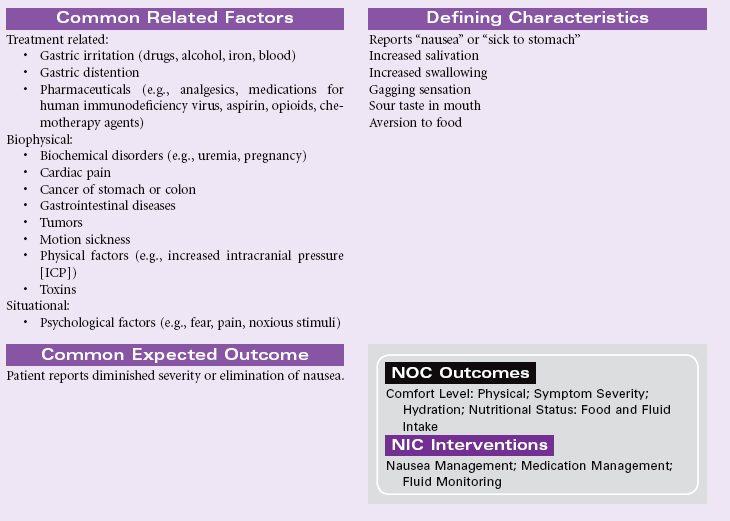
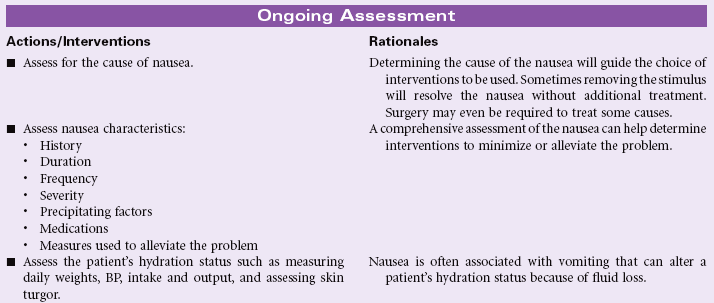
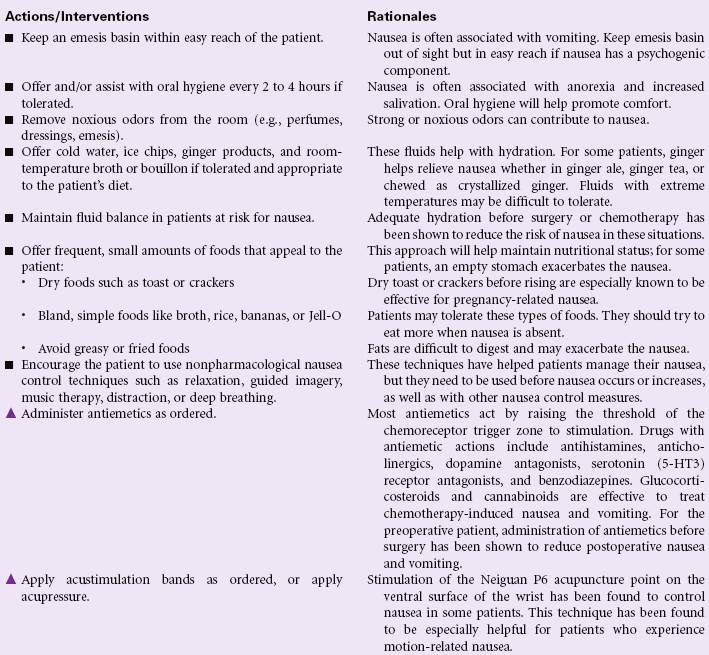
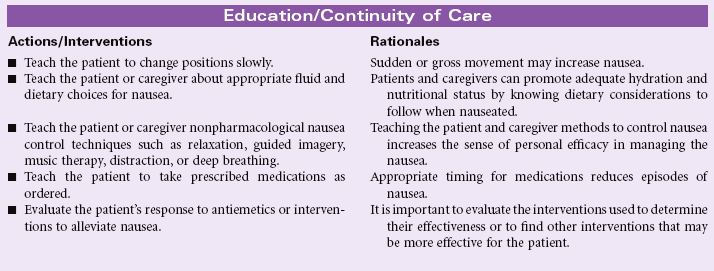
Nausea
Definition: An unpleasant, wavelike sensation in the back of the throat, epigastrium, or throughout the abdomen that may or may not lead to vomiting
Nausea is a common and distressing symptom with a myriad of causes, including intracranial or labyrinthine lesions, chemical stimulation of the vomiting center by most medications, ingestion of toxins (chemotherapy), inhalation of anesthetic gases, microorganisms in the gastrointestinal tract, gastrointestinal obstruction, or mucosal diseases. Decreased motility and delayed emptying of the stomach are the underlying physiological factors for most causes of nausea. Decreased peristalsis in the intestines may also contribute to nausea. Nausea may have psychogenic origins, which should be considered in cases of chronic nausea or gastroparesis. Nausea can also be associated with severe pain or aberrant motion such as in carsickness or seasickness. During the first trimester of pregnancy, nausea is common and may be related to excessive hormone production. For most women, this subsides by their second trimester; for other women, mild nausea may persist throughout the pregnancy. Because nausea is a subjective experience, the patient may find others are not supportive of their symptom if it is not associated with vomiting.


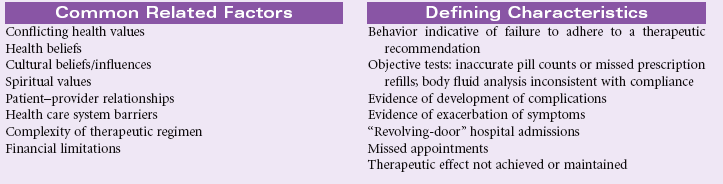
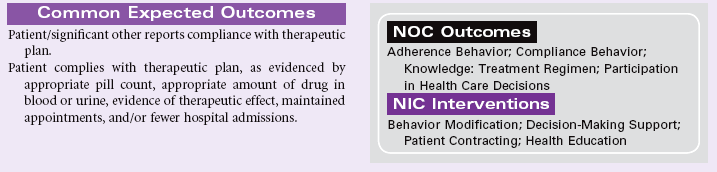
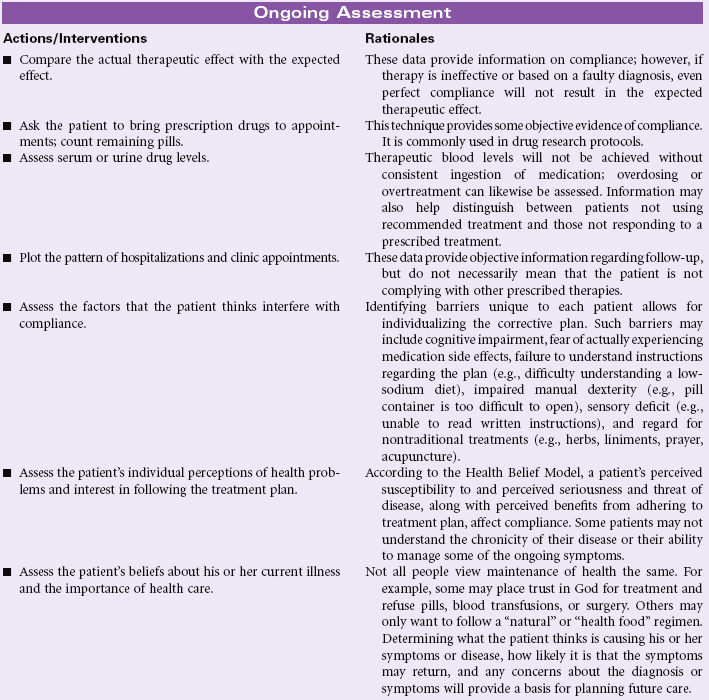
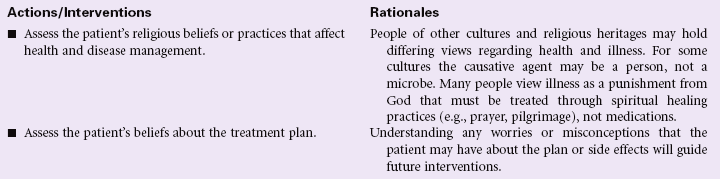
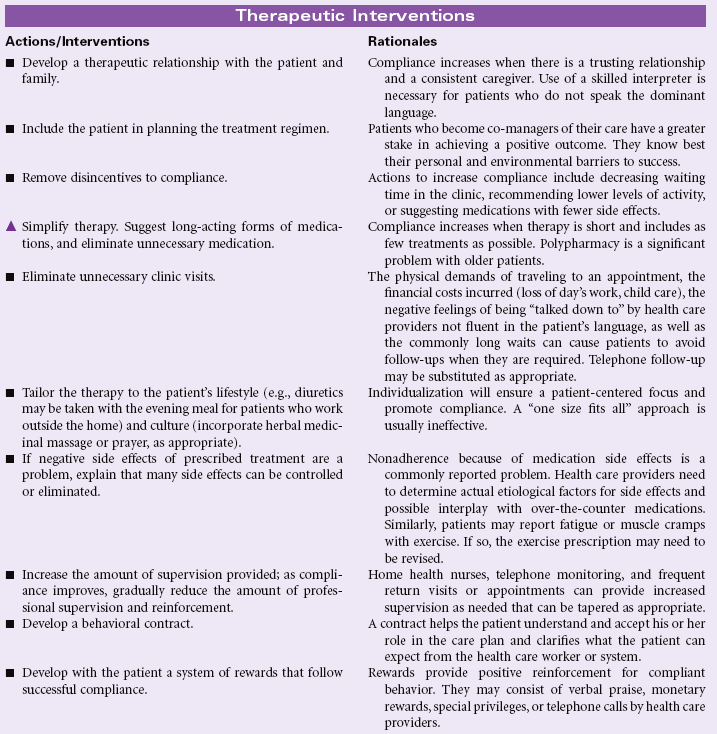
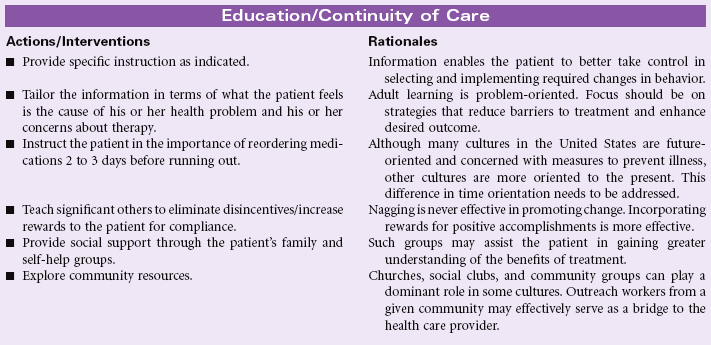
Noncompliance
Definition: Behavior of person and/or caregiver that fails to coincide with a health-promoting or therapeutic plan agreed on by the person (and/or family and/or community) and health care professional. In the presence of an agreed-on health-promoting or therapeutic plan, a person’s or caregiver’s behavior is fully or partially nonadherent and may lead to clinically ineffective or partially ineffective outcomes
The fact that a patient has attained knowledge regarding the treatment plan does not guarantee compliance. Failure to follow the prescribed plan may be related to a number of factors. Much research has been conducted in this area to identify key predictive factors. Several theoretical models, such as the Health Belief Model, Theory of Reasoned Decision Making, and Theory of Planned Behavior, serve to explain those factors that influence patient compliance. Patients are more likely to comply when they believe that they are susceptible to an illness or disease that could seriously affect their health, that certain behaviors will reduce the likelihood of contracting the disease, that the prescribed actions are less threatening than the disease itself, and when normative groups support the change. Factors that may predict noncompliance include past history of noncompliance, stressful lifestyles, contrary cultural or religious beliefs and values, lack of social support, lack of financial resources, and compromised emotional state. People living in adverse social situations (e.g., battered women, homeless individuals, those living amid street violence, the unemployed, or those in poverty) may purposefully defer following medical recommendations until their acute socioeconomic situation is improved. The rising costs of health care and the growing number of uninsured and underinsured patients often force patients with limited incomes to choose between food and medications. The problem is especially complex for older patients living on fixed incomes but requiring complex and costly medical therapies.
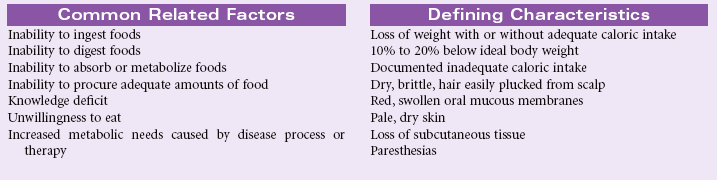
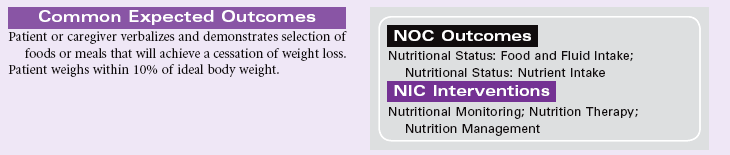
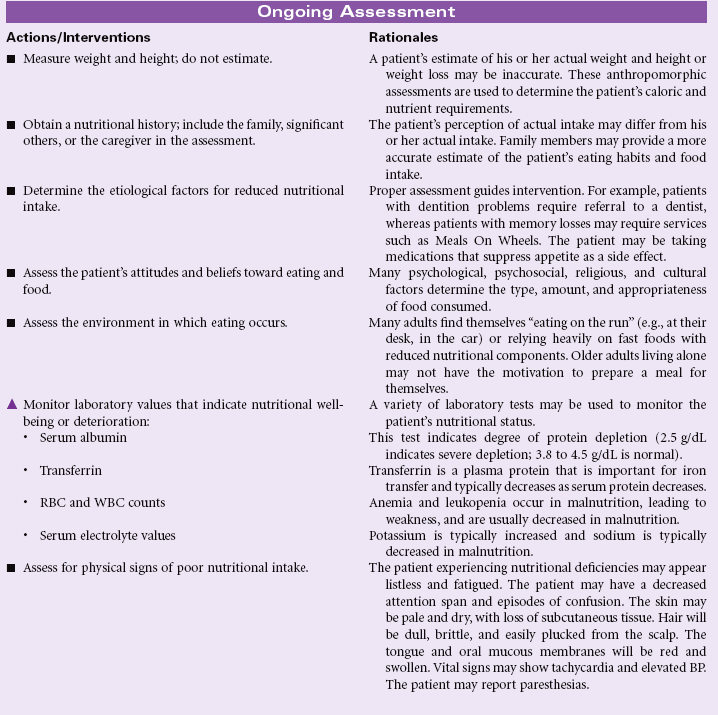
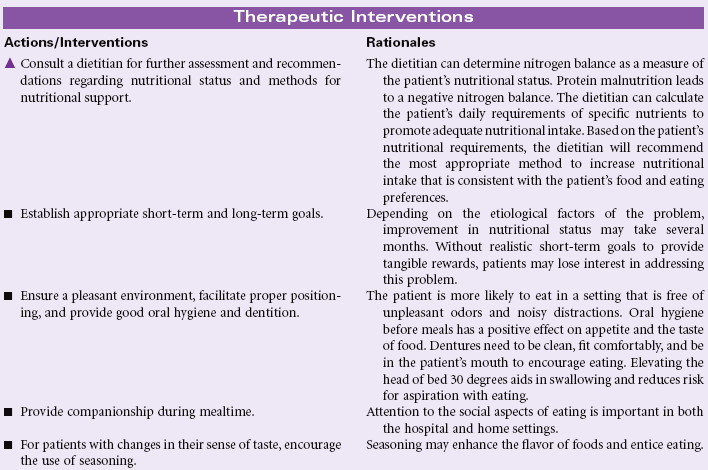
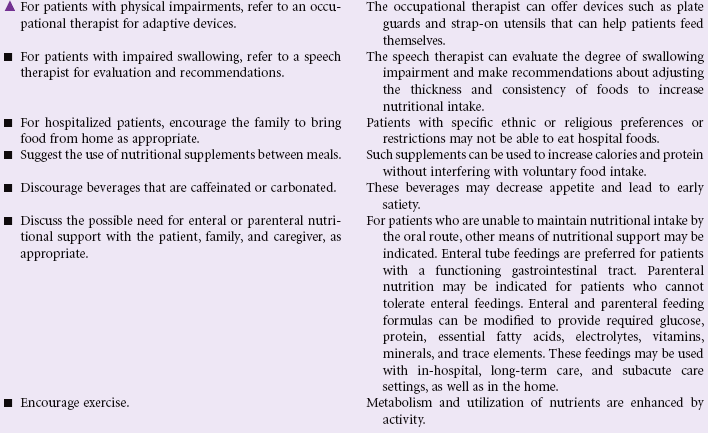
Imbalanced Nutrition: Less Than Body Requirements
Definition: Intake of nutrients insufficient to meet metabolic needs
Adequate nutrition is necessary to meet the body’s demands. Nutritional status can be affected by disease or injury states (e.g., gastrointestinal malabsorption, cancer, burns); physical factors (e.g., muscle weakness, poor dentition, activity intolerance, pain, substance abuse); social factors (e.g., lack of financial resources to obtain nutritious foods); or psychological factors (e.g., depression, boredom, dementia). During times of illness (e.g., trauma, surgery, sepsis, burns), adequate nutrition plays an important role in healing and recovery. Cultural and religious factors strongly affect the food habits of patients. Women exhibit a higher incidence of voluntary restriction of food intake secondary to anorexia, bulimia, and self-constructed fad dieting. Patients who are older experience problems in nutrition related to lack of financial resources, cognitive impairments causing them to forget to eat, physical limitations that interfere with preparing food, deterioration of their sense of taste and smell, reduction of gastric secretion that accompanies aging and interferes with digestion, and social isolation and boredom that cause a lack of interest in eating. This care plan addresses general concerns related to nutritional deficits for the hospital or home setting.
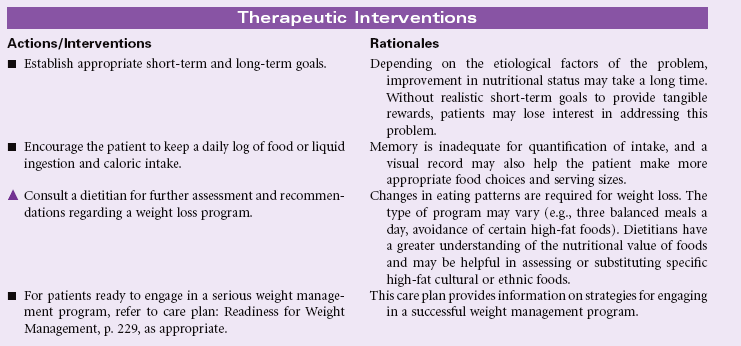
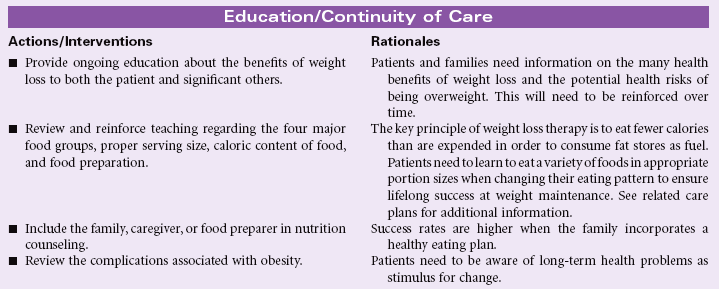
Imbalanced Nutrition: More Than Body Requirements
Definition: Intake of nutrients that exceeds metabolic needs
Obesity is a growing problem in the United States and is now reaching pandemic proportions, accounting for significant other health problems, including cardiovascular disease, type 2 diabetes mellitus, sleep disorders, infertility in women, aggravated musculoskeletal problems, and shortened life expectancy. Women are more likely to be overweight than men. African Americans and Hispanic individuals are more likely to be overweight than Caucasians. Factors that affect weight gain include genetics, sedentary lifestyle, emotional factors associated with dysfunctional eating, disease states such as diabetes mellitus and Cushing’s syndrome, and cultural or ethnic influences on eating. Overall nutritional requirements of older patients are similar to those of younger individuals, except calories should be reduced because of their leaner body mass.
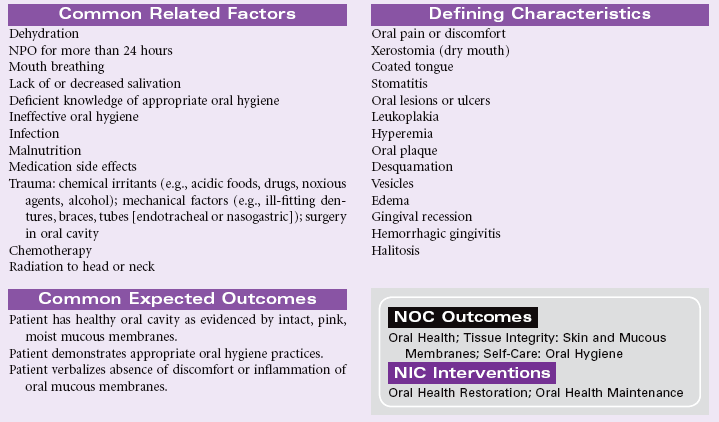
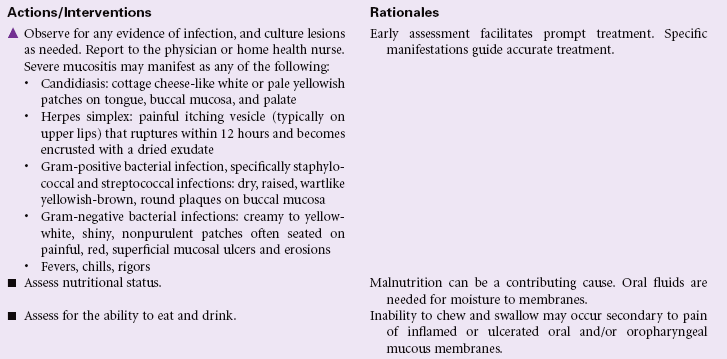
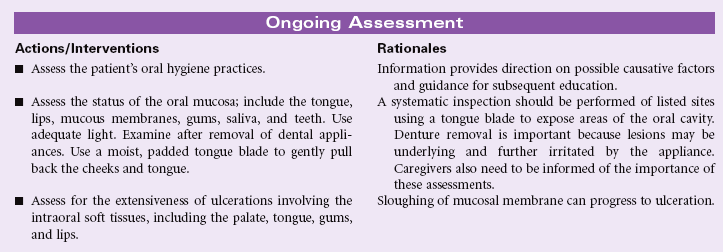
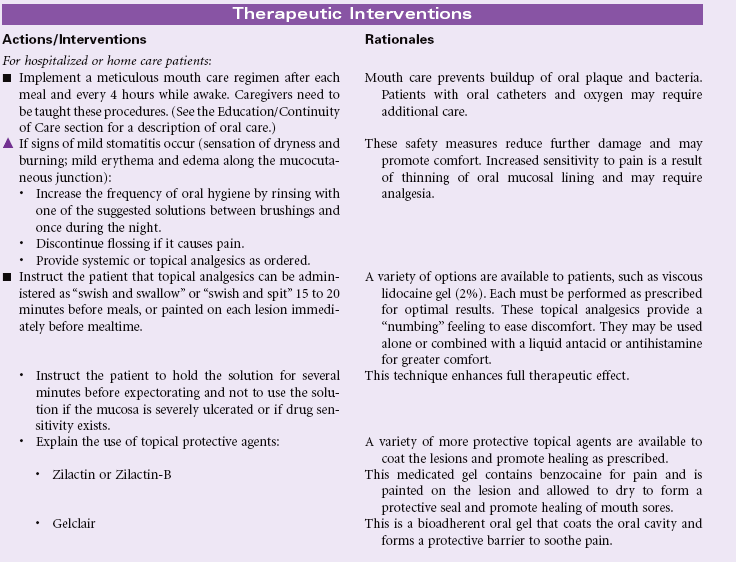
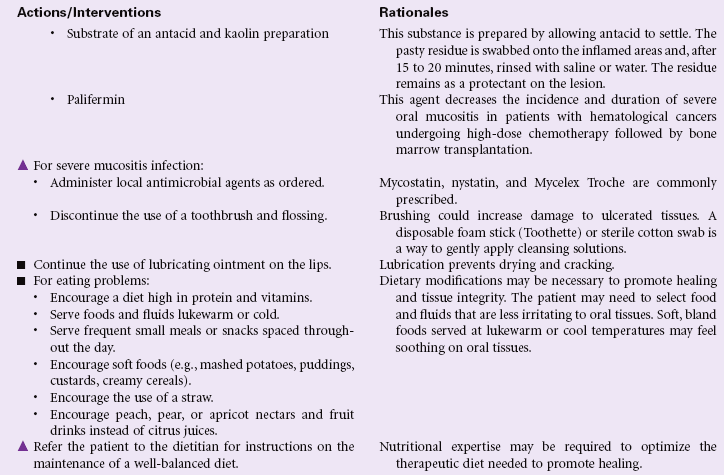
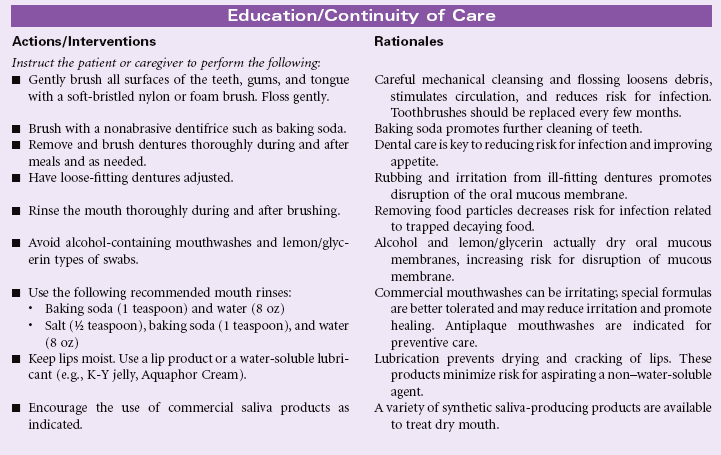
Impaired Oral Mucous Membrane
Definition: Disruption of the lips and/or soft tissue of the oral cavity
Minor irritations of the oral mucous membrane occur occasionally in all people and are usually viral-related, self-limiting, and easily treated. Patients who have severe stomatitis often have an underlying illness. Patients who are immunocompromised, such as the oncology patient receiving chemotherapy, are often affected with severe tissue disruption and pain. Infections such as candidiasis, if left untreated, can spread through the entire gastrointestinal tract, causing further complications and sometimes perineal pain. Oral mucous membrane problems can be encountered in any setting, especially in home care and hospice settings.

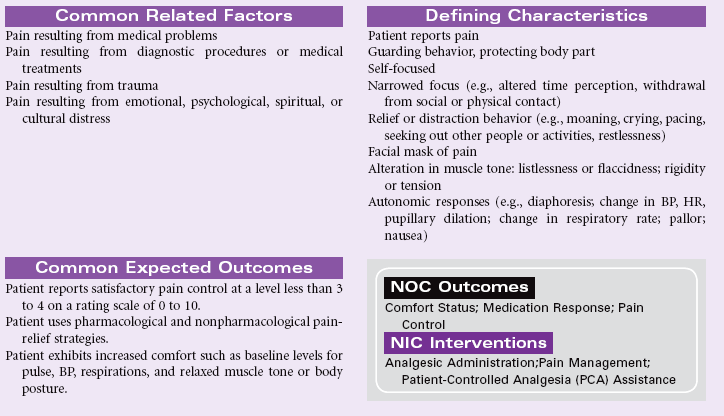
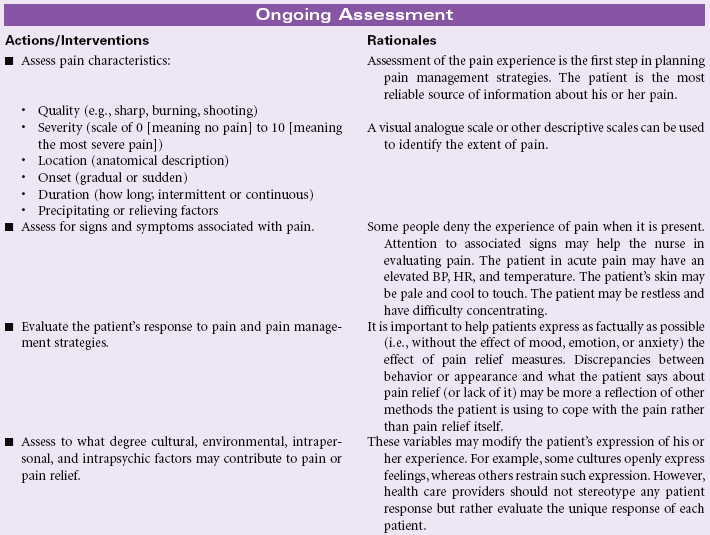
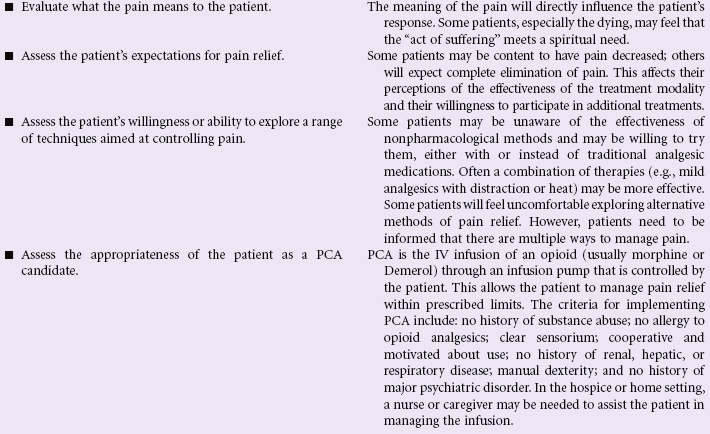
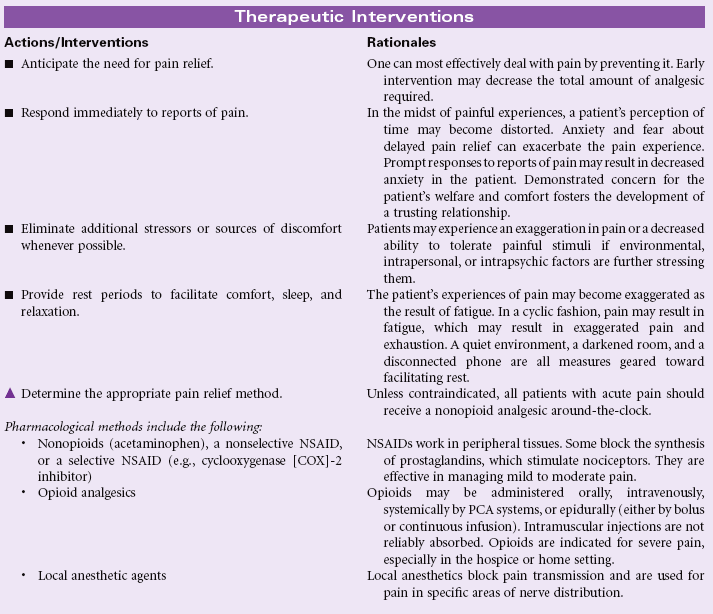
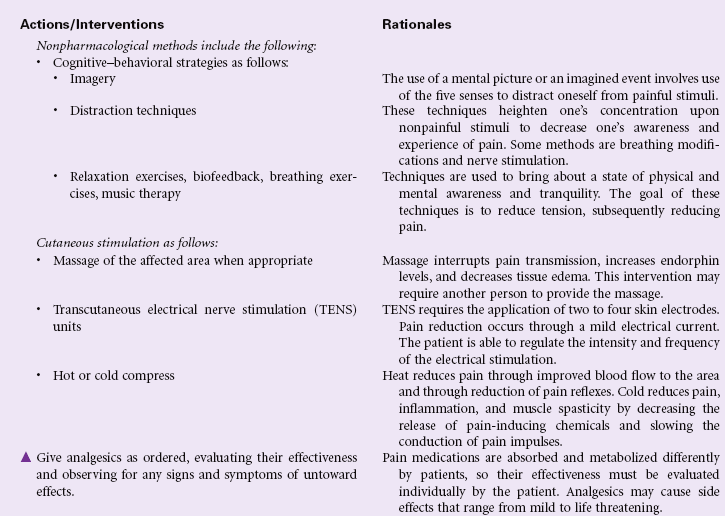
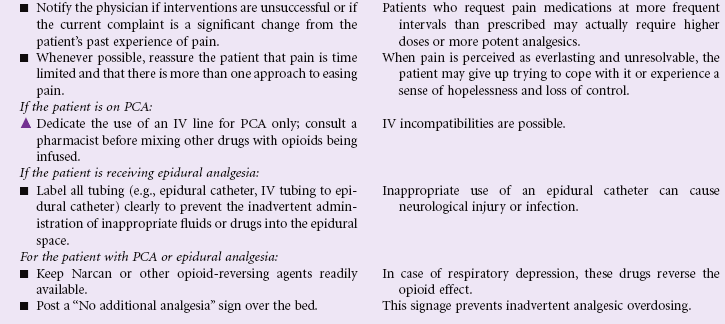
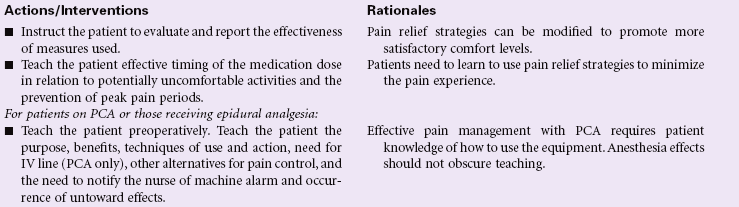
Acute Pain
Definition: Unpleasant sensory and emotional experience arising from actual or potential tissue damage or described in terms of such damage (International Association for the Study of Pain); sudden or slow onset of any intensity from mild to severe with an anticipated or predictable end and a duration of less than 6 months
Pain is a highly subjective state in which a variety of unpleasant sensations and a wide range of distressing factors may be experienced by the patient. Acute pain serves a protective function to make the patient aware of an injury or illness. The sudden onset of acute pain prompts the patient to seek relief. The physiological manifestations that occur with acute pain result from the body’s response to pain as a stressor. The patient’s cultural background, emotions, and psychological or spiritual distress may contribute to the suffering with acute pain. Pain assessment can be challenging, especially in older patients, in whom cognitive impairment and sensory-perceptual deficits are more common. This care plan focuses on the assessment and management of acute pain in the hospital or home care settings.


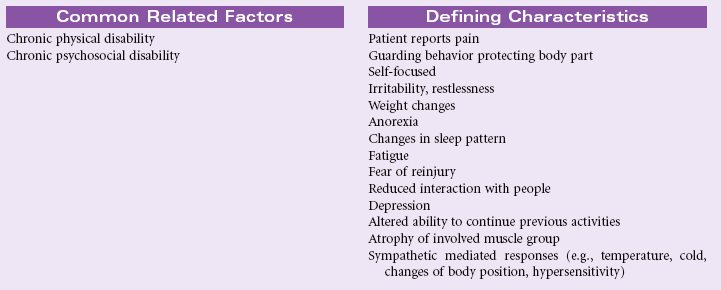
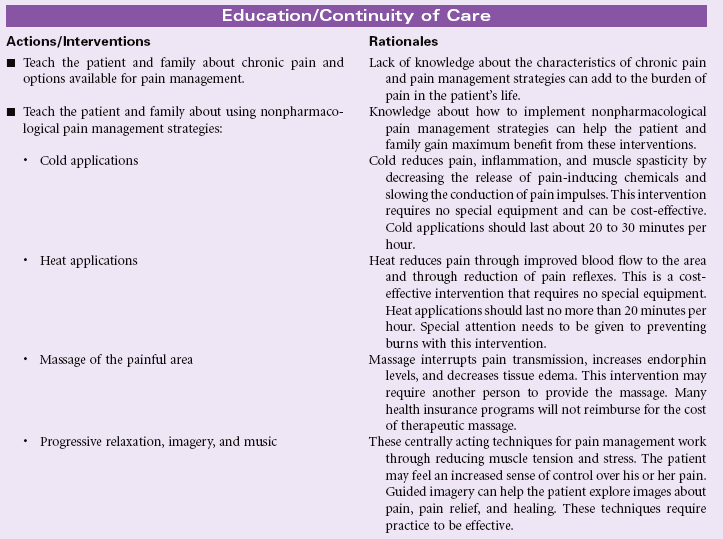
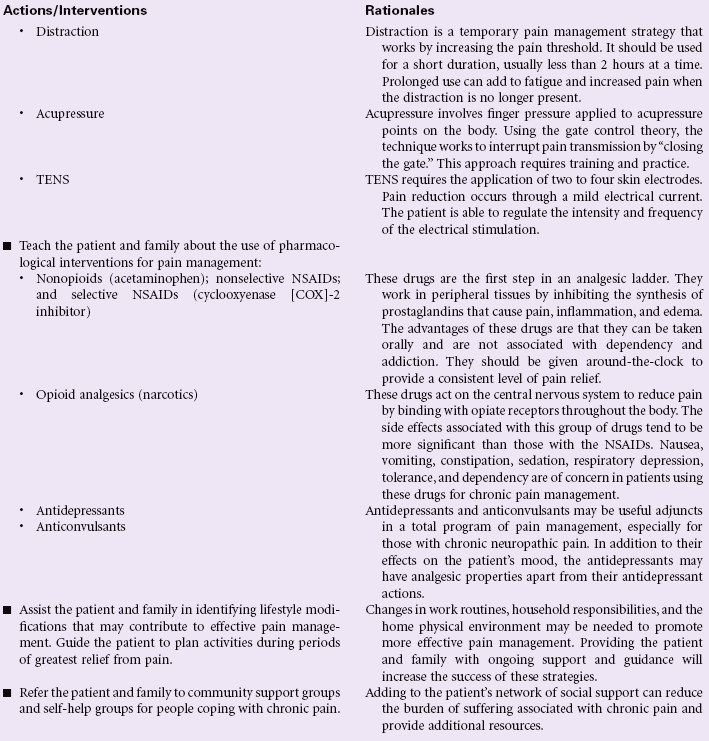
Chronic Pain
Definition: Unpleasant sensory and emotional experience arising from actual or potential tissue damage or described in terms of such damage (International Association for the Study of Pain); sudden or slow onset of any intensity from mild to severe, constant or recurring without an anticipated or predictable end and a duration of greater than 6 months
Chronic pain may be classified as chronic malignant pain or chronic nonmalignant pain. In the former, the pain is associated with a specific cause such as cancer. With chronic nonmalignant pain, the original tissue injury is not progressive or has been healed but the patient continues to experience pain. Identifying an organic cause for this type of chronic pain is more difficult.
Chronic pain differs from acute pain in that it is harder for the patient to provide specific information about the location and the intensity of the pain. Over time it becomes more difficult for the patient to differentiate the exact location of the pain and clearly identify the intensity of the pain. The patient with chronic pain often does not present with behaviors and physiological changes associated with acute pain. Family members, friends, co-workers, employers, and health care providers question the legitimacy of the patient’s pain reports because the patient may not look like someone in pain. The patient may be accused of using pain to gain attention or to avoid work and family responsibilities. With chronic pain, the patient’s level of suffering usually increases over time. Chronic pain can have a profound impact on the patient’s activities of daily living, mobility, activity tolerance, ability to work, role performance, financial status, mood, emotional status, spirituality, family interactions, and social interactions.

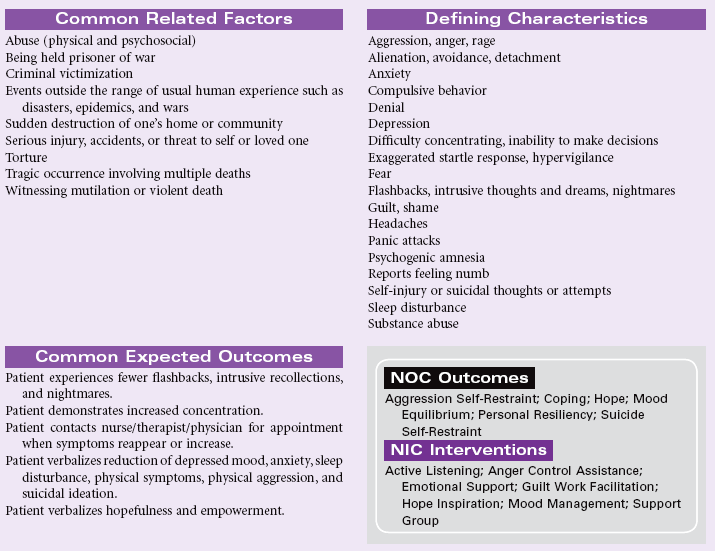
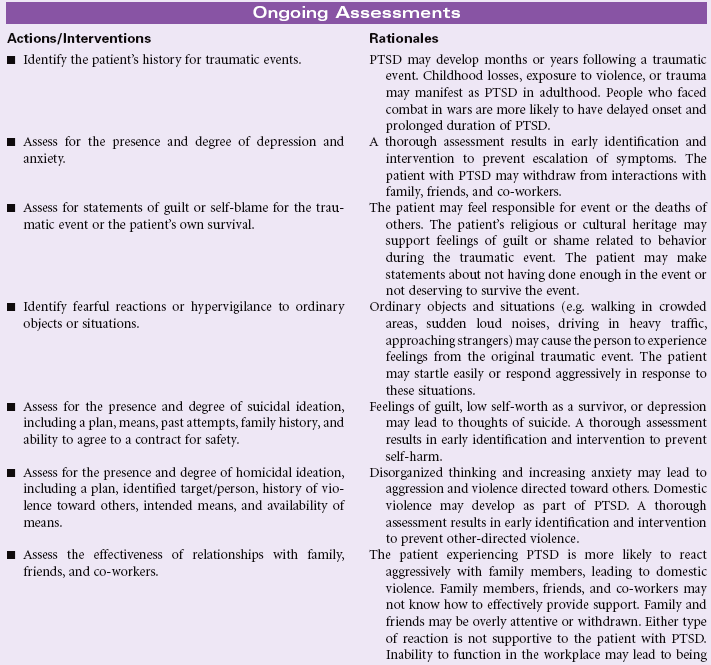
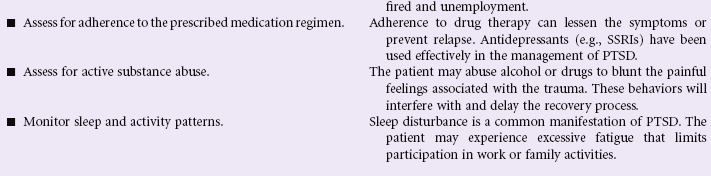
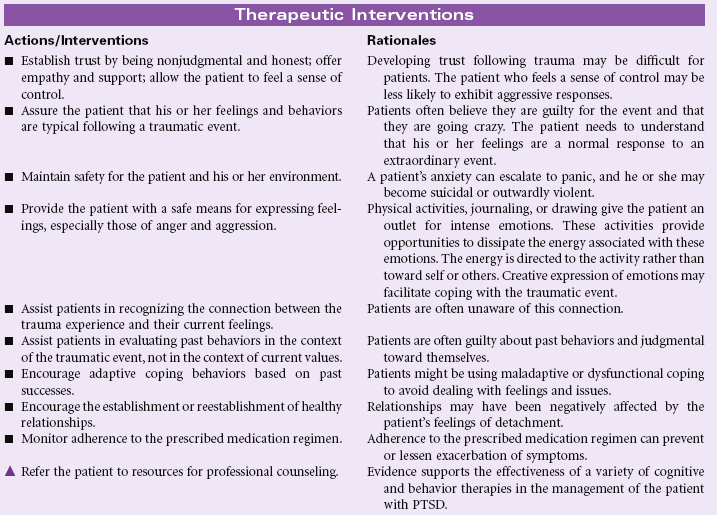
Post-Trauma Syndrome
Definition: Sustained maladaptive response to a traumatic, overwhelming event
Post-trauma syndrome, also called post-traumatic stress disorder (PTSD), occurs in individuals who have experienced, witnessed, or been confronted by an event or events that have involved actual or threatened death or serious injury or a threat to the physical integrity of self or others. New evidence suggests that patients who sustain traumatic brain injury, especially concussion force injury, develop PTSD. The individual’s response with PTSD involves intense fear, helplessness, or horror. Typically the maladaptive response(s) continue beyond 1 month, causing significant distress or impairment in social, occupational, physical, spiritual, or psychological functioning. These maladaptive responses may be acute or chronic.
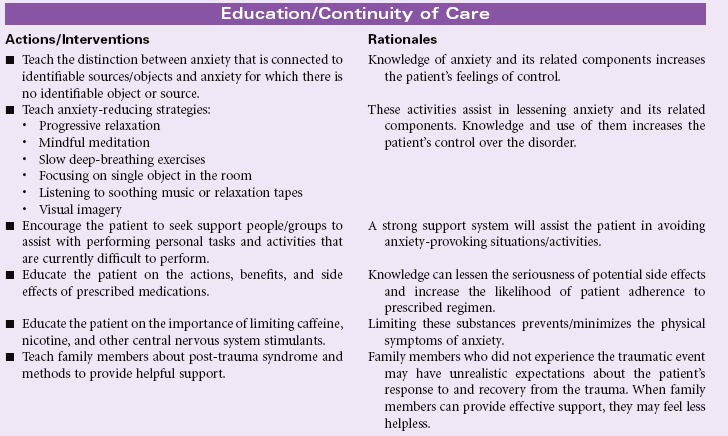
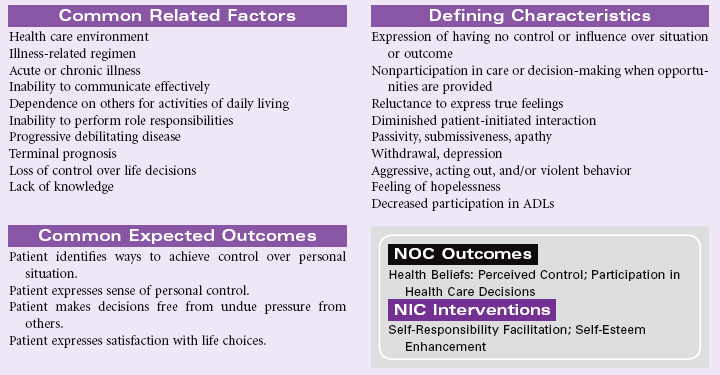
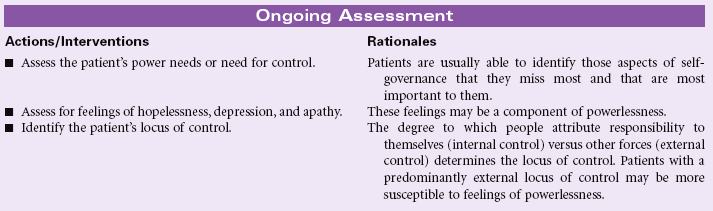
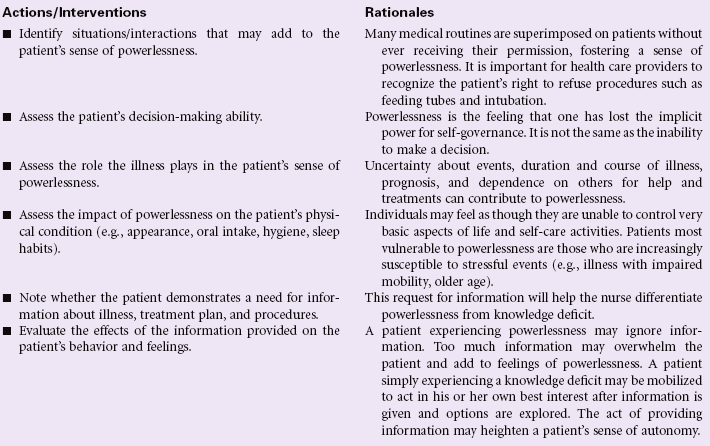
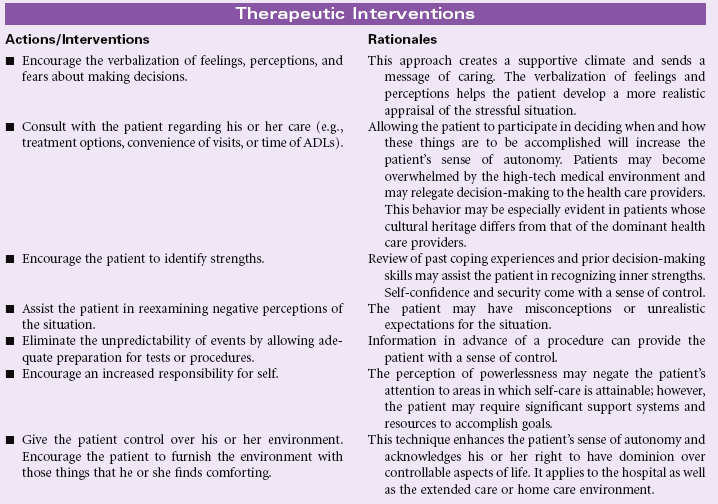
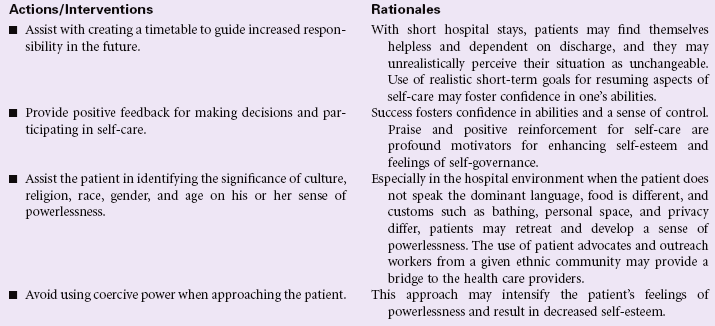
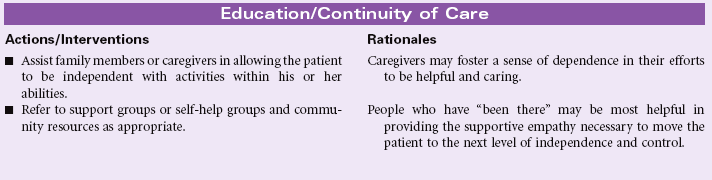
Powerlessness
Definition: Perception that one’s own action will not significantly affect an outcome; a perceived lack of control over a current situation or immediate happening
Powerlessness may be expressed at any time during a patient’s illness. During an acute episode, people used to being in control may temporarily find themselves unable to navigate the health care system and environment. The medical jargon, the swiftness with which decisions are expected to be made, and the vast array of health care providers to which the patient has to relate can all cause a feeling of powerlessness. This response is compounded by patients of cultural, religious, or ethnic backgrounds that differ from those of the dominant health care providers. Patients with chronic, debilitating, or terminal illnesses may have long-term feelings of powerlessness because they are unable to change their inevitable outcomes. Older patients are especially susceptible to the threat of loss of control and increasing dependence that comes with aging, as well as the consequences of illness and disease. Patients suffering from feelings of powerlessness may be seen in the hospital, ambulatory care, rehabilitation, or home care environment.
Rape-Trauma Syndrome
Definition: Sustained maladaptive response to a forced, violent sexual penetration against the victim’s will and consent
Rape-trauma syndrome refers to the immediate period of psychological disorganization and the long-term process of reorganization that occur as a result of attempted or actual sexual assault. Every survivor of sexual assault will express unique emotional needs and may respond differently to rape. However, almost all survivors, male and female, experience elements of the syndrome as a response to the extreme stress, profound fear of death, and sense of violation and vulnerability. Sexual assault survivors may suffer various effects of this violent crime for the remainder of their lives. Recovery from the physical trauma associated with the rape may prolong and complicate the survivor’s response to and recovery from the psychological trauma. Cultural bias, social attitudes, and preconceived ideas about rape victims may make it difficult for victims to report the crime. These biases and attitudes also make effective recovery more difficult for survivors. Improved education about the impact of rape on survivors has led to more supportive responses by law enforcement officers, emergency care first responders, and emergency department care providers.
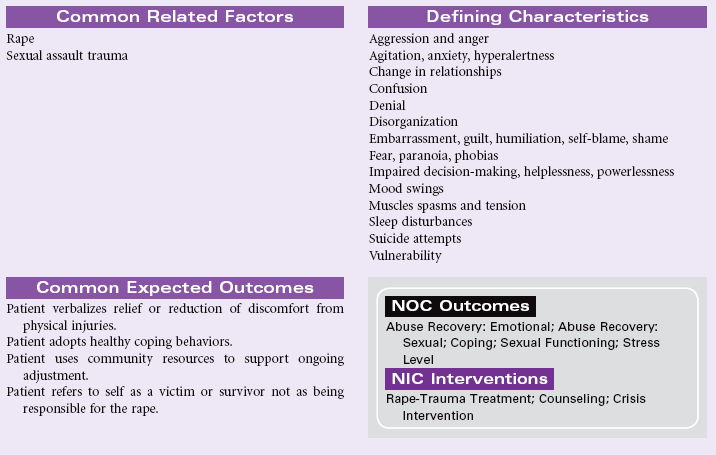
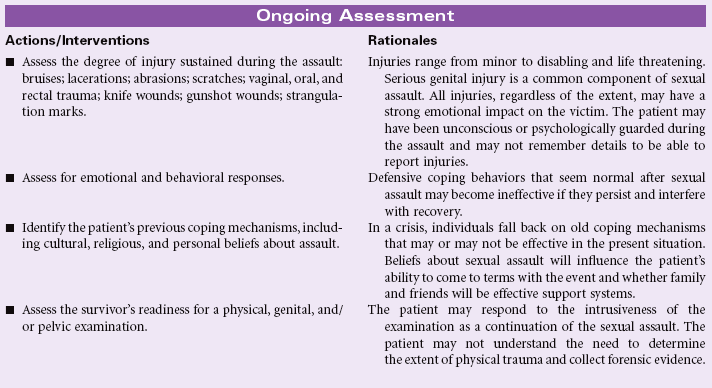
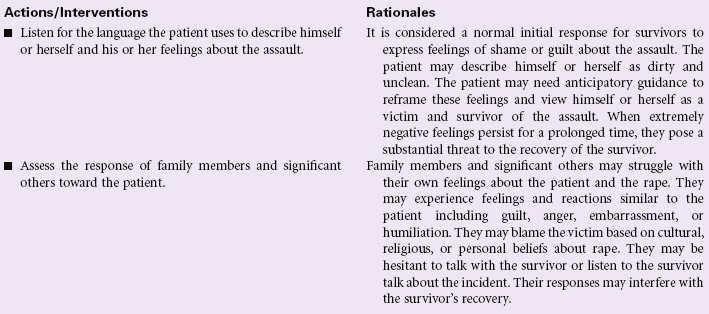
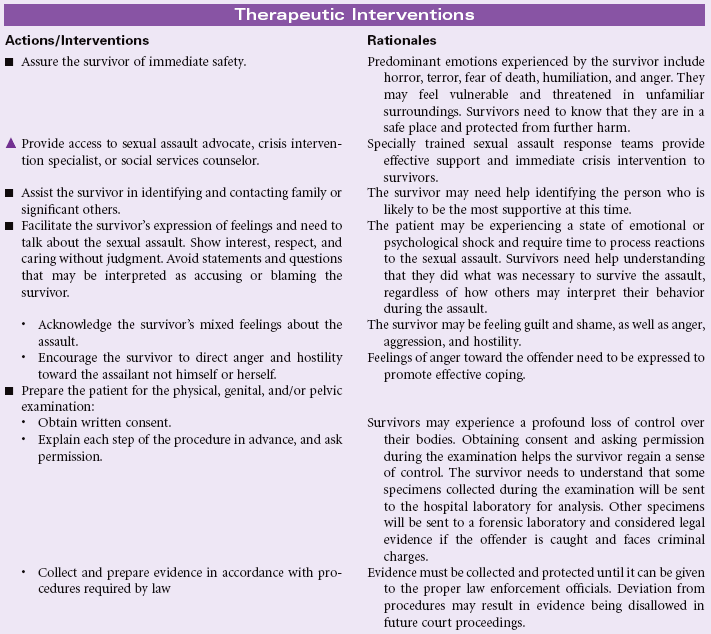
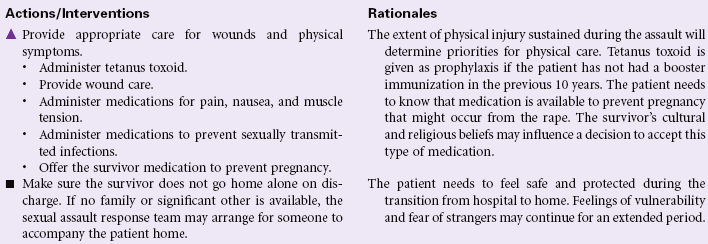
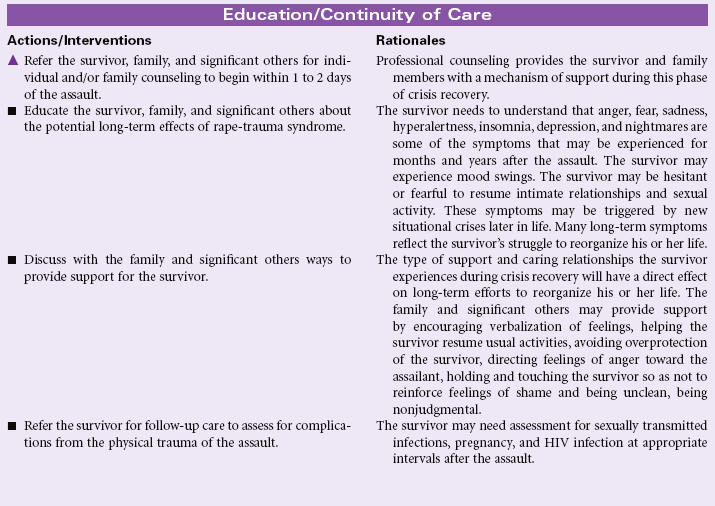
Relocation Stress Syndrome
Definition: Physiological and/or psychological disturbance following transfer from one environment to another
The physiological and psychological stress associated with relocation is now recognized as so extreme that it is associated with the stress of divorce or the death of a loved one. Adjustment to moving from what was once familiar to what is a new environment can last for several months to several years and longer. Current evidence suggests that recovery from a significant move leads to significant decline in the person’s health and many times leads to death. The degree of severity depends on many variables such as age, stage of life, personality, number of concurrent losses, amount of preparation, and the degree and type of support before, during, and after the move. Older adults, in particular, are at high risk for experiencing the negative impact of relocation. This syndrome may also be seen in the hospitalized patient who experiences several hospital locations within one hospital stay.
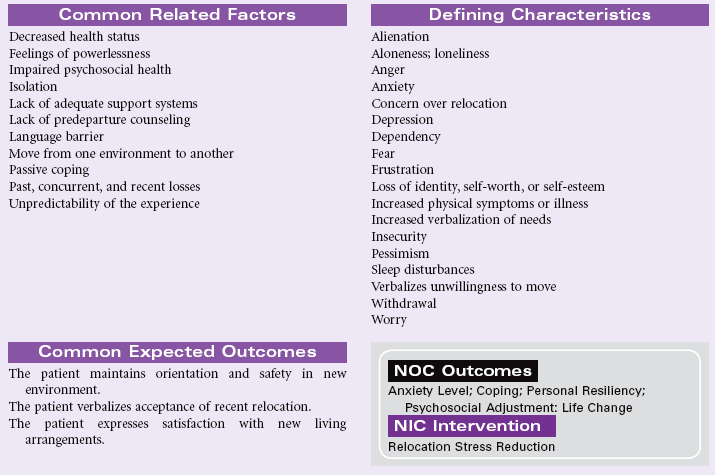
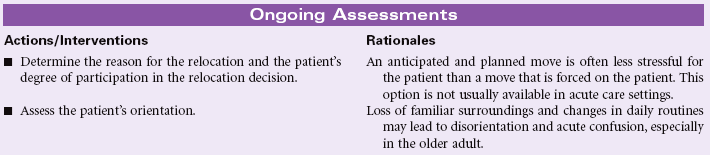
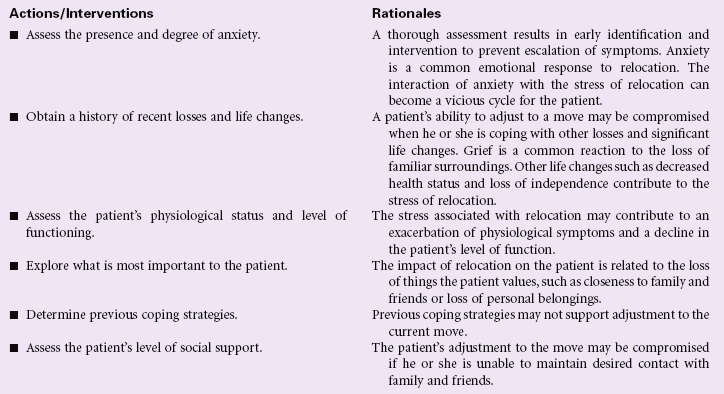
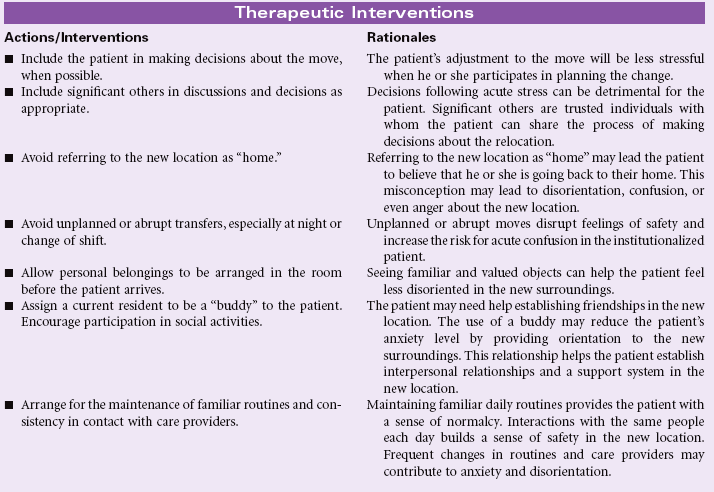
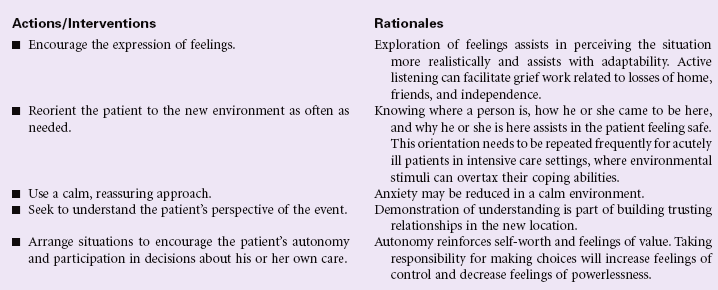
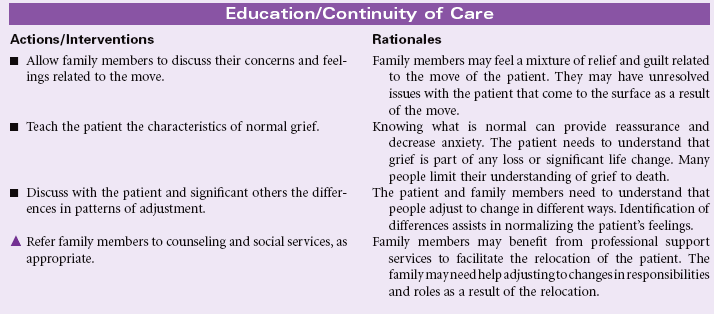
Self-Care Deficit
Definition: Impaired ability to perform or complete activities of daily living for oneself, such as feeding, dressing, bathing, toileting
The nurse may encounter the patient with a self-care deficit in the hospital or in the community. The deficit may be the result of transient limitations, such as those one might experience while recuperating from surgery, or the result of progressive deterioration that erodes the individual’s ability or willingness to perform the activities required to care for himself or herself. Patients who are depressed or those with low levels of motivation may not have the interest to engage in self-care activitities. Careful examination of the patient’s deficit is required to be certain that the patient is not failing at self-care because of a lack of material resources or a problem with arranging the environment to suit the patient’s physical limitations. The nurse coordinates services to maximize the independence of the patient and to ensure that the environment the patient lives in is safe and supportive of his or her special needs. This care plan combines a variety of self-care deficits into one comprehensive plan.
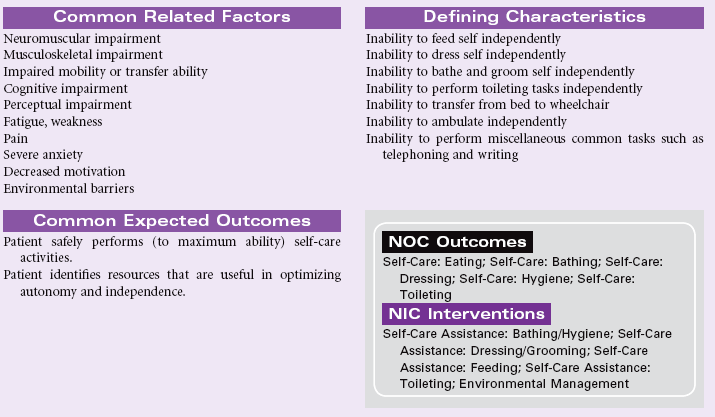
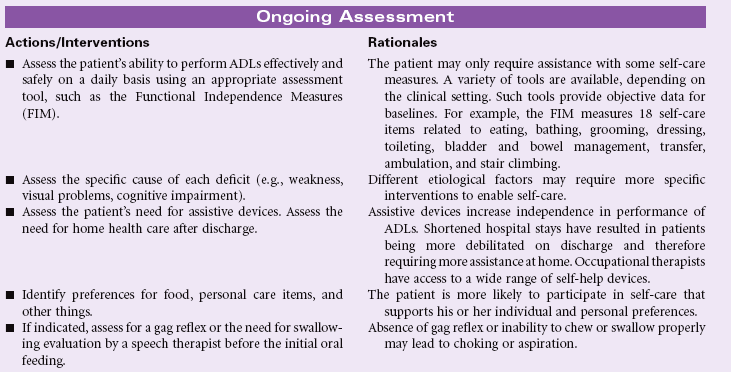
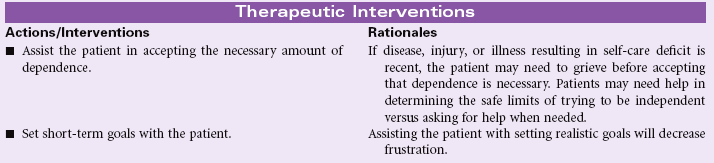
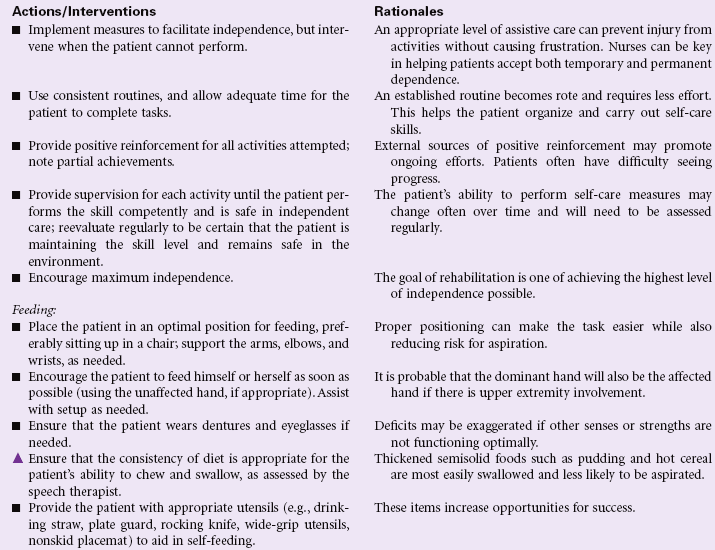
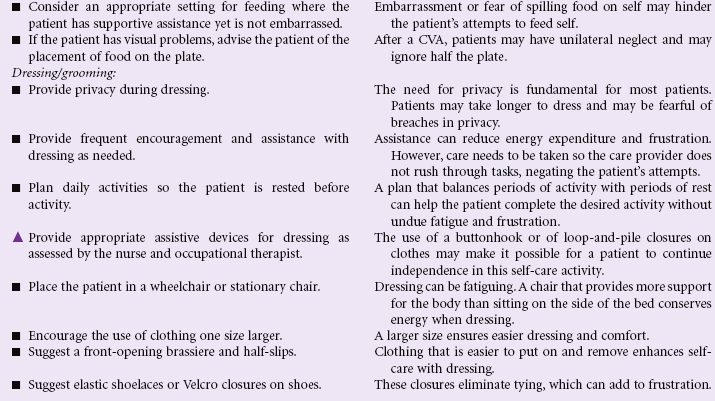
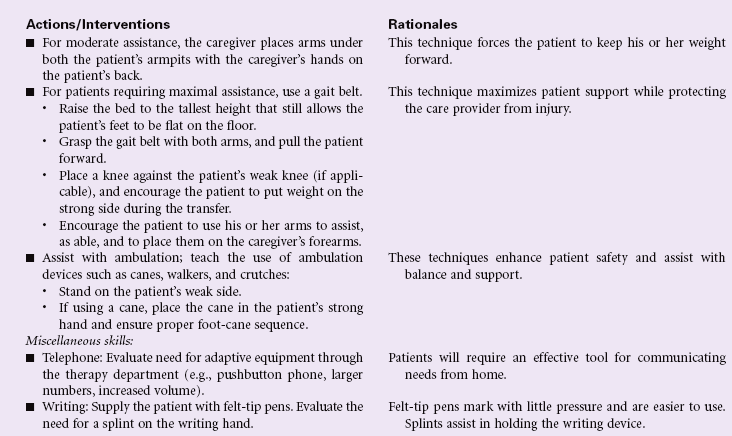
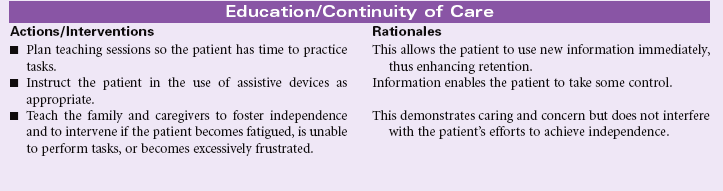
Situational Low Self-Esteem
Definition: Development of a negative perception of self-worth in response to current situation (specify)
Self-esteem is a component of an individual’s self-concept. Positive self-esteem is based on the person’s feeling worthwhile and capable of responding to challenges and stressors. Low self-esteem represents a mild to marked alteration in an individual’s view of himself or herself, including negative self-evaluation or negative feelings about self or capabilities. This change in self-esteem is a temporary state in response to feeling unable to manage the current situation. A person’s self-esteem is affected by (and may also affect) his or her ability to function in the larger world and relate to others within it. Self-esteem disturbance may be expressed directly or indirectly. Cultural norms, gender, and age are variables that influence how an individual perceives himself or herself. The emotional work that patients do to enhance self-esteem takes weeks, months, or even years and may require professional help beyond the scope of the bedside or community nurse. A caring individual, who is able to identify the special needs of the patient struggling with self-esteem issues, is in a unique position to provide support and compassion, enhancing the work the patient must do.
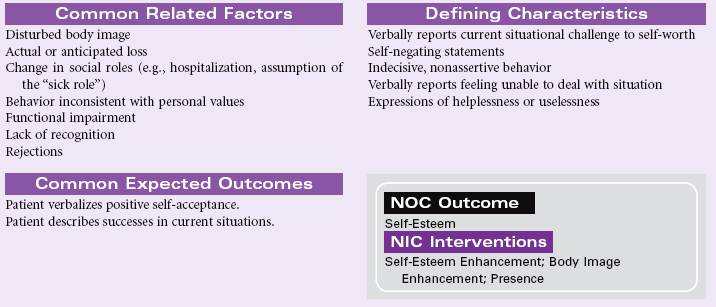
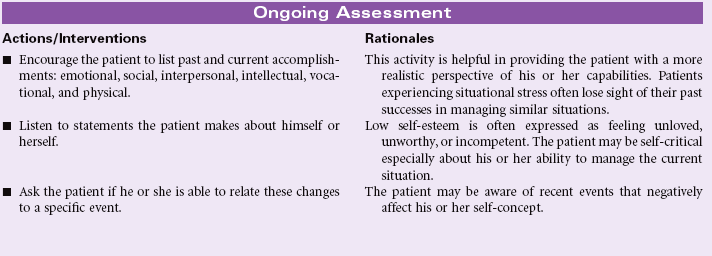
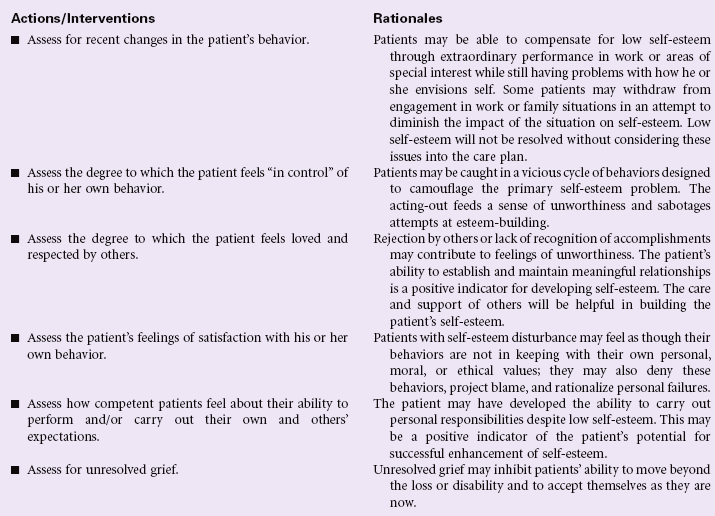
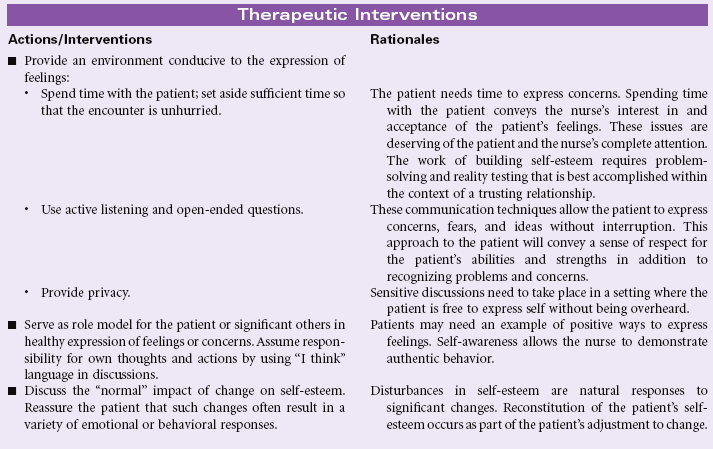
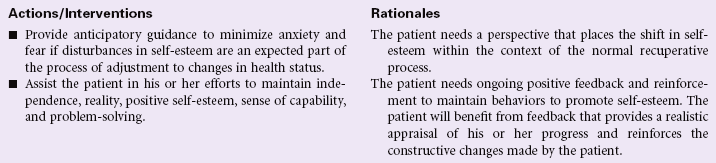
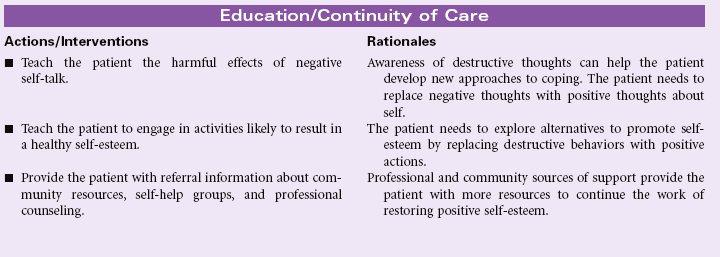
 Disturbed Sensory Perception: Auditory
Disturbed Sensory Perception: Auditory
Definition: Change in the amount or patterning of incoming stimuli accompanied by a diminished, exaggerated, distorted, or impaired response to such stimuli
Adults may experience hearing loss as the result of trauma, infection, or exposure to persistently loud occupational and/or environmental noise. Older adults may experience gradual hearing loss as part of the normal aging process. Conductive hearing loss is associated with problems affecting the outer ear and middle ear. These problems include impacted cerumen and infection. Sensorineural hearing loss occurs with inner ear disorders or impaired function of cranial nerve VIII. Aging, noise exposure, and ototoxicity from some drugs contribute to this type of hearing loss. When hearing loss is profound and precedes language development, the ability to learn speech and interact with hearing peers can be severely impaired. When hearing is impaired or lost later in life, serious emotional and social consequences can occur, including depression and isolation. Some causes of hearing loss are surgically correctable. Many hearing assistive devices and services are available to help hearing-impaired individuals. Nursing interventions with the hearing impaired are aimed at assisting the individual in effective communication despite the loss of normal hearing.
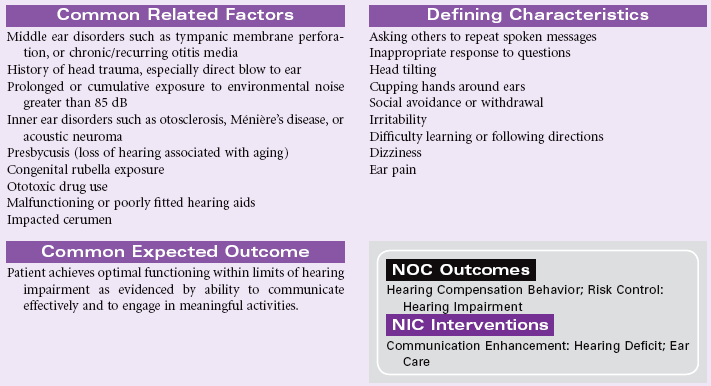
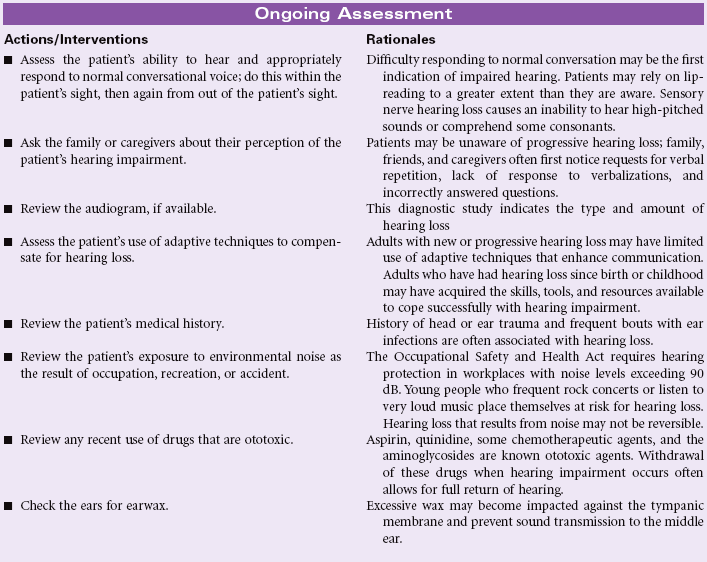
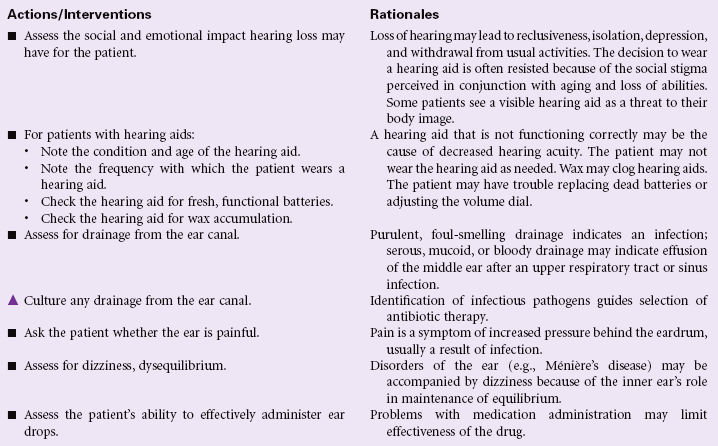
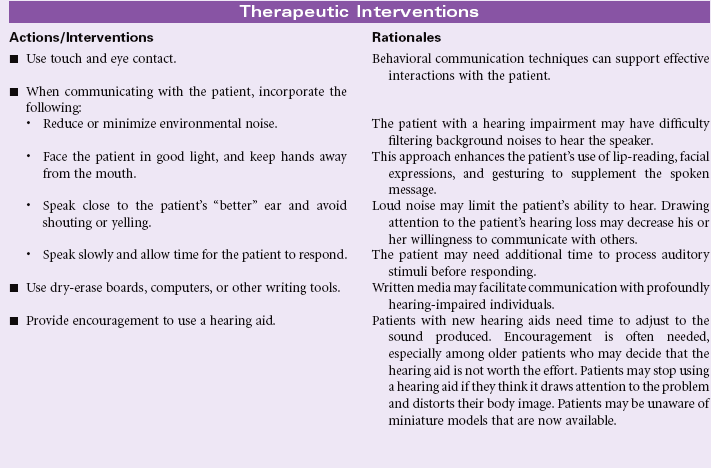
Disturbed Sensory Perception: Visual
Definition: Change in the amount or patterning of incoming stimuli accompanied by a diminished, exaggerated, distorted, or impaired response to such stimuli
Visual impairment affects a significant number of people across the life span. Refractive errors are the most common form of visual problem. These correctable visual impairments include myopia, hyperopia, presbyopia, and astigmatism. Correction occurs with glasses, contact lenses, or surgery. Chronic diseases such as diabetes mellitus, glaucoma, and macular degeneration cause visual impairment that may not be correctable and may lead to blindness. Cataracts contribute to visual impairment that may be corrected through surgery and lens replacement. Infections, trauma, drugs, and diseases of the brain may also cause temporary or permanent visual impairment. Changes in visual acuity may interfere with the person’s ADLs and productivity at work, school, or home. Loss of vision threatens the safety of the individual and puts the person at risk for falls and other injuries. Visual impairment may affect the person’s psychological, emotional, and social well-being as he or she copes with adapting to the loss while attempting to remain independent. Dependence on devices to correct or adapt to visual impairment may affect the person’s body image and self-concept.
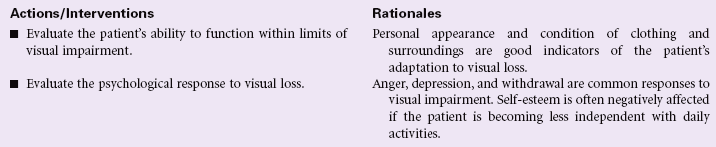
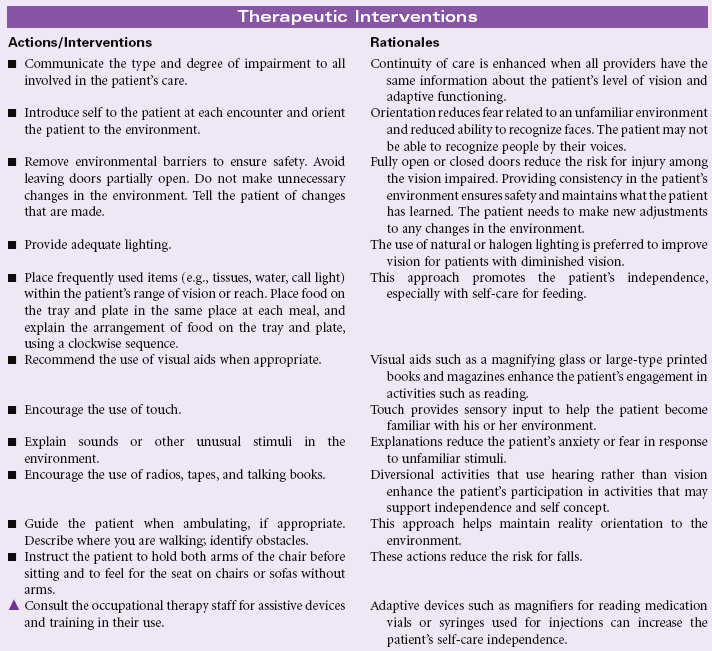

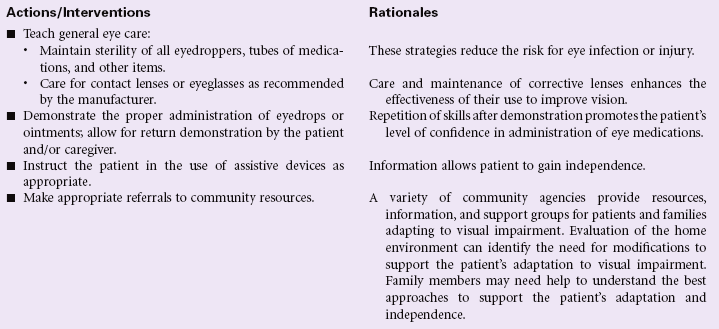
Ineffective Sexuality Pattern
Definition: Expressions of concern regarding own sexuality
A patient or significant other may express concern regarding the means or manner of sexual expression or physical intimacy within their relationship. Alterations in human sexual response may be related to genetic, physiological, emotional, cognitive, religious, and/or sociocultural factors or to a combination of these factors. All of these factors play a role in determining what is normative for each individual within a relationship. The problem of altered patterns of sexuality is not limited to a single gender, age, or cultural group; it is a potential problem for all patients, whether the nurse encounters them in the hospital or in the community. It is probable that most couples encounter some point in their relationship where patterns of sexual expression become altered to the dissatisfaction of one or both members. The ability to communicate effectively, to seek professional help whenever necessary, and to modify existing patterns to the mutual satisfaction of both members are skills that enable the couple to grow and evolve in this aspect of their relationship. The nurse is in a unique position to provide anticipatory guidance relative to altered patterns of sexual function when the problem is an inevitable or probable result of illness or disability. The ability to discuss these issues openly when the patient raises concerns about sexual expression highlights the legitimacy of the couple’s feelings and the normalcy of sexual expression as a part of intimacy, as well as emotional and physical well-being.
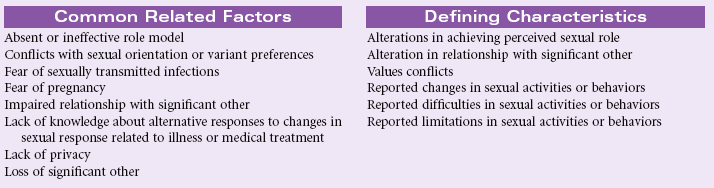
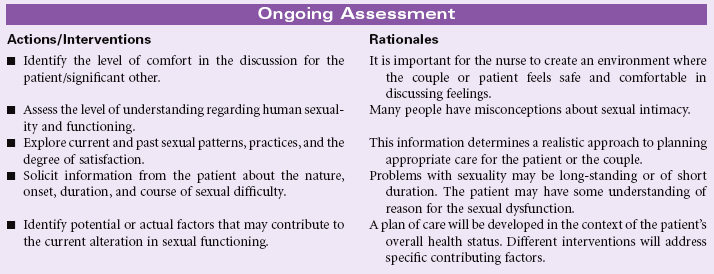
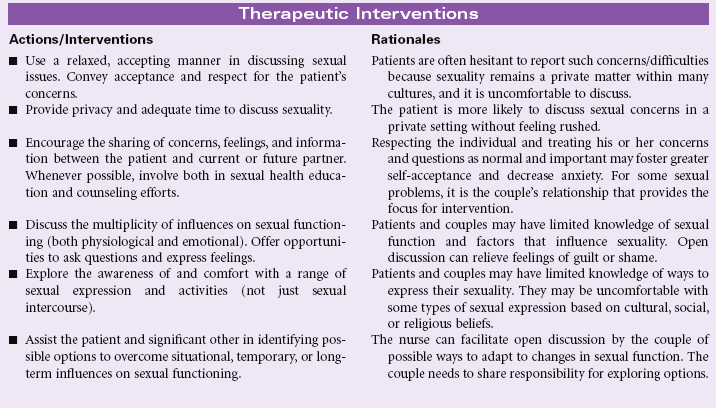
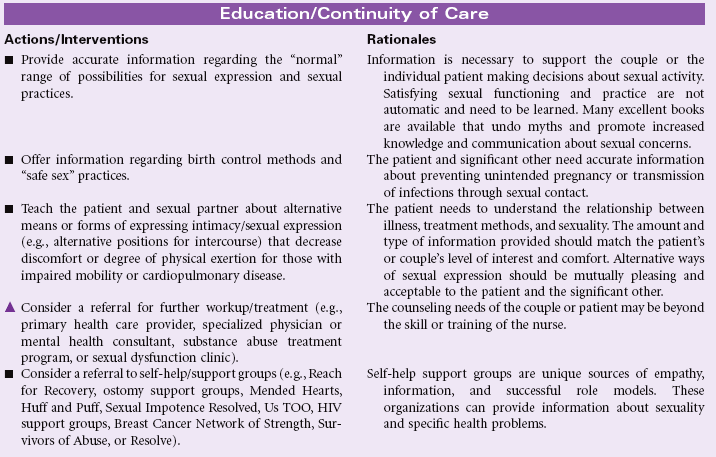
Risk for Impaired Skin Integrity
Definition: At risk for skin being adversely altered
Maintenance of skin integrity and prevention of pressure ulcers is identified as a key marker of quality care. The Centers for Medicare and Medicaid Services (CMS) and The Joint Commission (TJC) have identified pressure ulcer prevention as one of the first major nursing- sensitive outcomes. Although the literature suggests that not all pressure ulcers can be prevented, the nurse is in a key role to implement comprehensive guidelines to aid in the prevention and early detection of impaired skin integrity. Nurses must be aware of the myriad factors that place patients at risk for skin breakdown. The literature reports that pressure ulcers can develop in 2 to 6 hours; thus identifying at-risk individuals is key.
Immobility, which leads to pressure, shear, and friction, is the factor most likely to put an individual at risk for altered skin integrity. Advanced age, the normal loss of elasticity, inadequate nutrition, environmental moisture (especially from incontinence), and vascular insufficiency potentiate the effects of pressure and hasten the development of skin breakdown. Groups of people with the highest risk for altered skin integrity are those with spinal injuries, those who are confined to bed or wheelchair for prolonged periods of time, those with edema, and those who have altered sensation that triggers the normal protective weight shifting. Pressure relief and pressure redistribution devices for the prevention of skin breakdown include a wide range of surfaces, specialty beds and mattresses, and other devices. Preventive measures are usually not reimbursable, even though costs related to treatment once breakdown occurs are greater.
Evidence is accumulating to support the significant reductions in the prevalence of pressure ulcers when a standardized program for prevention is implemented. Several guidelines can be found in the literature. This care plan is based on recommendations from the National Pressure Ulcer Advisory Panel (NPUAC), the National Guideline Clearinghouse, and the Agency for Healthcare Research and Quality (AHRQ).
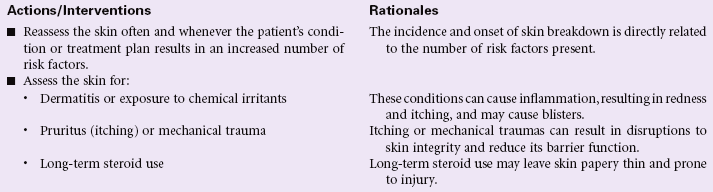
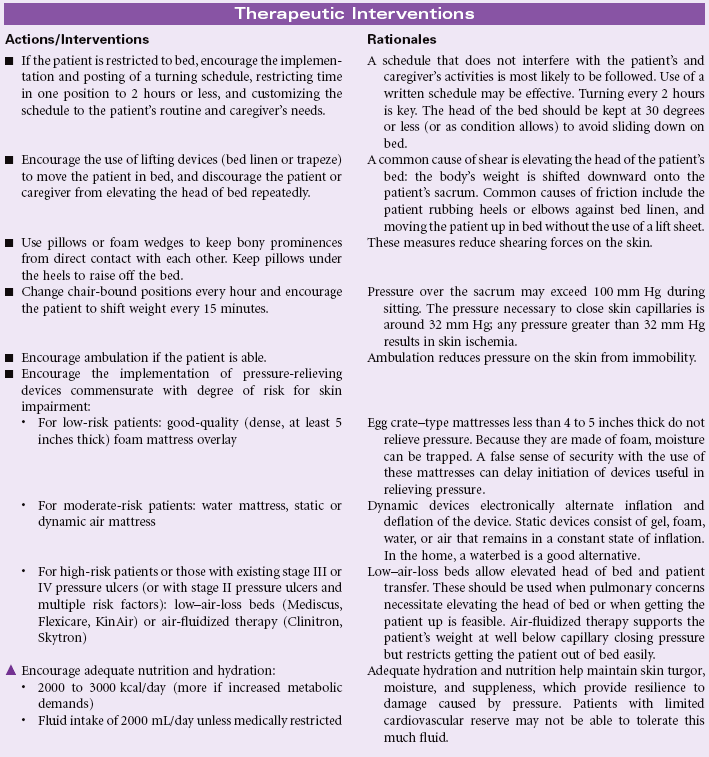
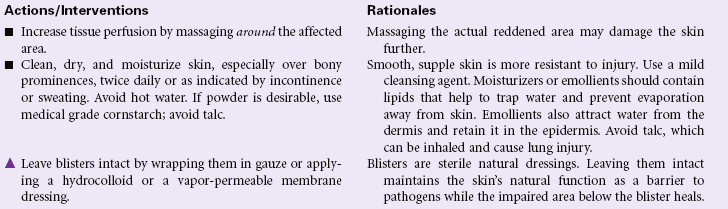
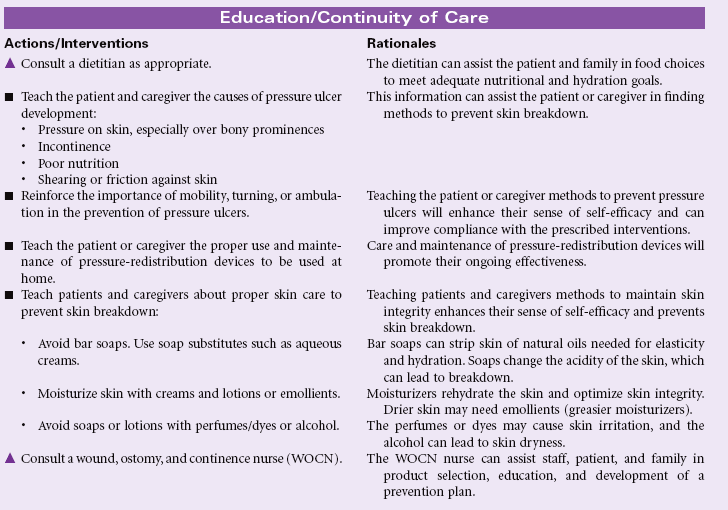
Spiritual Distress
Definition: Impaired ability to experience and integrate meaning and purpose in life through connectedness with self, others, art, music, literature, nature, and/or a power greater than oneself
Spiritual distress is an experience of profound disharmony in the person’s belief or value system that threatens the meaning of his or her life. During spiritual distress the patient may lose hope, question his or her belief system, or feel separated from his or her personal source of comfort and strength. Pain, chronic or terminal illness, impending surgery, and the death of a loved one are crises that may cause spiritual distress. Prescribed treatments may present conflicts with the person’s values, beliefs, or faith traditions. The health care environment may limit the person’s ability to engage in practices or rituals that support spiritual well-being and a sense of connectedness. Being physically separated from family and familiar culture contributes to feeling alone and abandoned. Nurses in the hospital, home care, and ambulatory settings can assist the patient in reestablishing a sense of spiritual well-being.
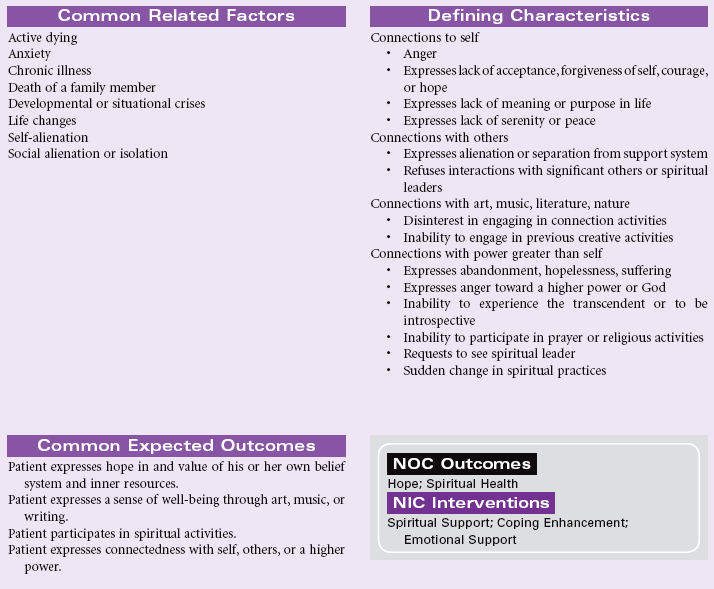
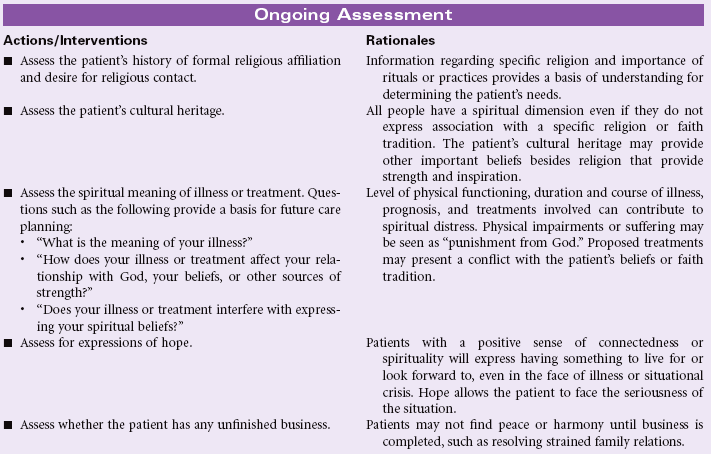
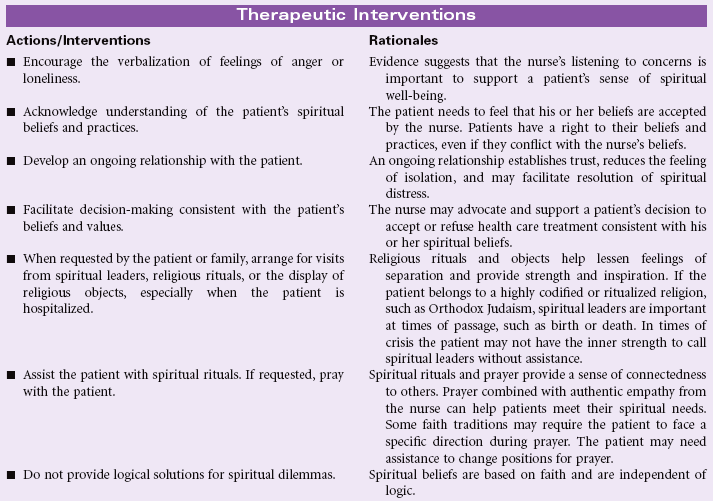

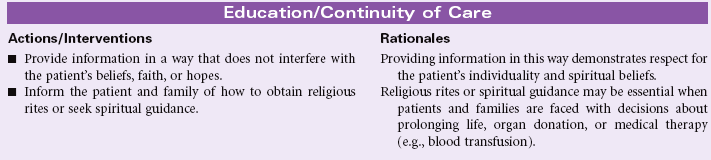
Risk for Suicide
Definition: At risk for self-inflicted, life-threatening injury
The overwhelming majority of patients who attempt suicide have a psychiatric disorder. However, suicide is not a mental health disorder. The patient who is depressed or who has a bipolar disorder may attempt suicide in response to acute symptoms. The patient with schizophrenia or an organic brain disorder that includes psychosis may respond to voices that tell the patient to hurt himself or herself. Other diagnoses in which suicide is observed as a behavior include personality disorders, where patients may establish a pattern of self-injury as a way to handle feelings of anger, anxiety, and substance abuse.
A variety of theories have been proposed to explain factors that lead a person to attempt suicide. Patients may use suicide to end prolonged distress, suffering, pain, or disability. Suicide is seen by some as a means of dealing with a sense of utter hopelessness, feelings of desperation or rage, a cry for help, or a means to punish someone. Suicide may be a carefully planned event that the patient has prepared as a final choice or an impulsive act in response to a specific precipitating event perceived as overwhelming. The causes and effects of suicide are the focus of widespread debate in the popular press, among health professionals, and in the courts. Whatever the circumstances, the effects of suicide resonate in the lives of family members and friends as well as the larger community for years afterward.
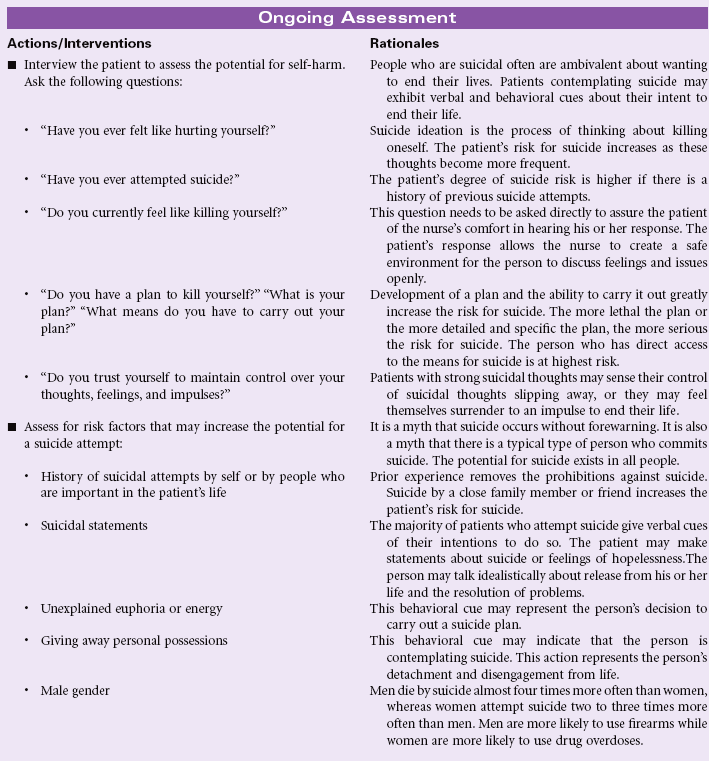
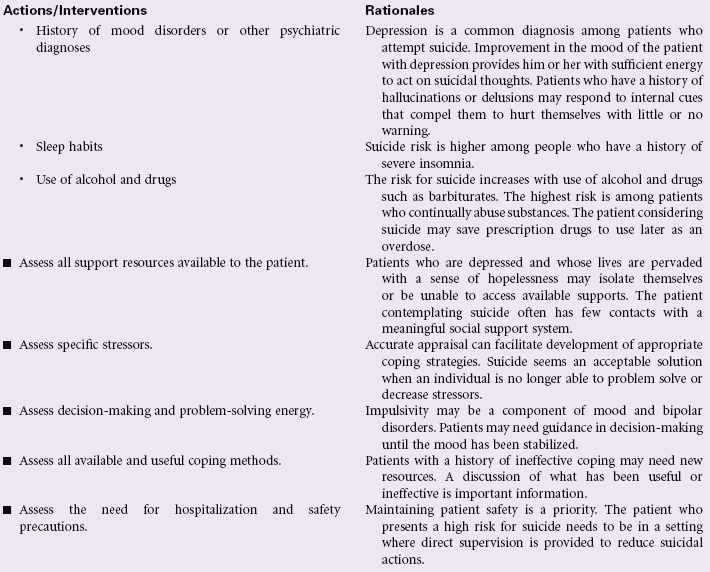
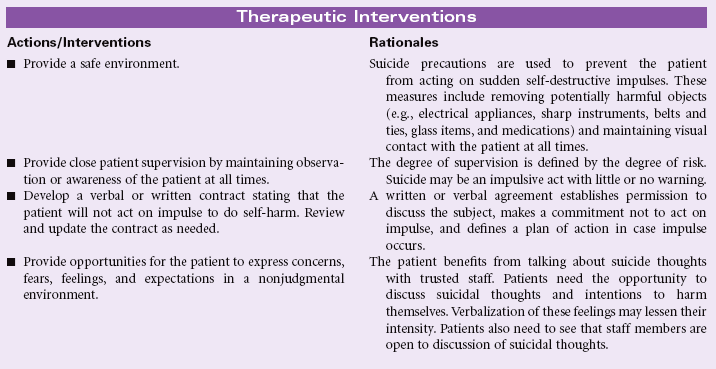
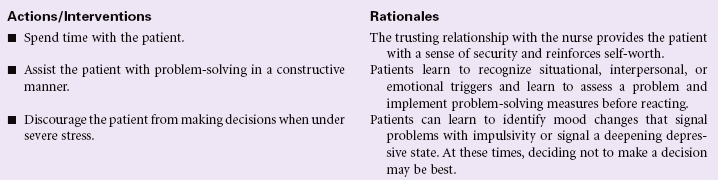
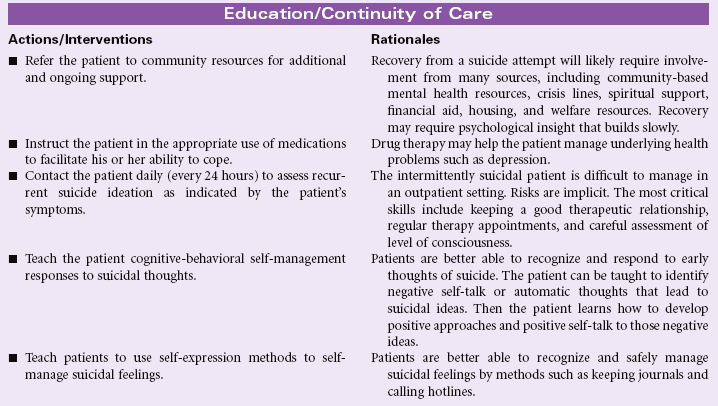
Impaired Swallowing
Definition: Abnormal functioning of the swallowing mechanism associated with deficits in oral, pharyngeal, or esophageal structure or function
Impaired swallowing can be a temporary or permanent complication that can be life threatening. Aspiration of food or fluid is the most serious complication. Impaired swallowing can be caused by a structural problem, interruption or dysfunction of neural pathways, decreased strength or excursion of muscles involved in mastication, facial paralysis, or perceptual impairment. Swallowing difficulties are a common complaint among older adults, in those individuals who have had a stroke, suffered head trauma, have head or neck cancer, or experience progressive neurological diseases like Parkinson’s disease, multiple sclerosis, and amyotrophic lateral sclerosis. Dysphagia severity rating scales are available to guide extent of modification in diet plan.
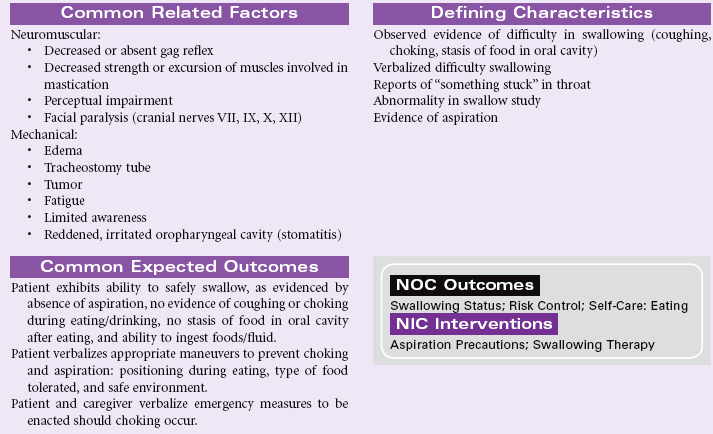
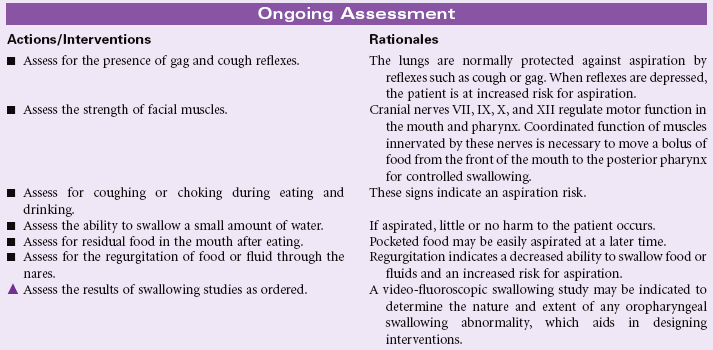
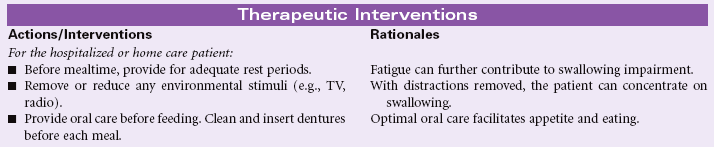
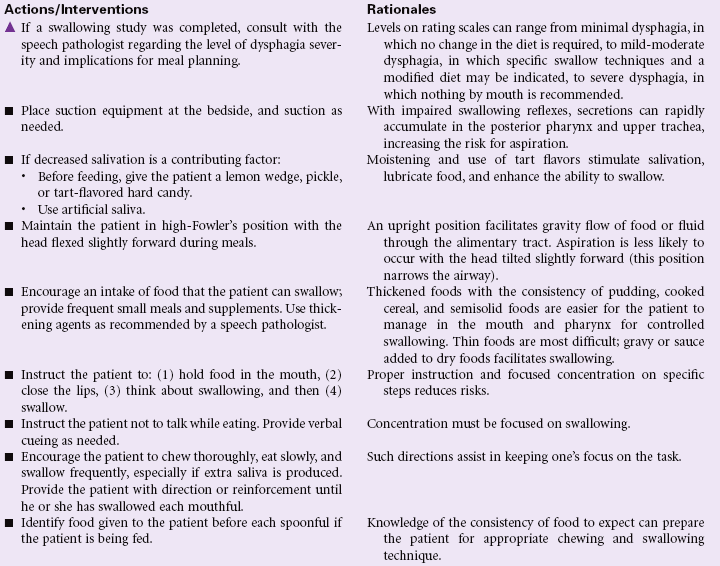
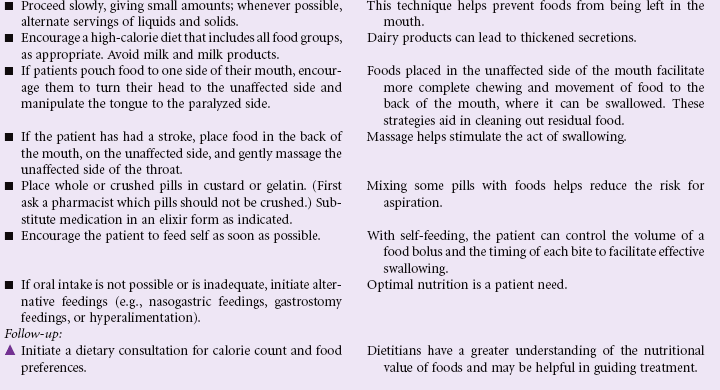
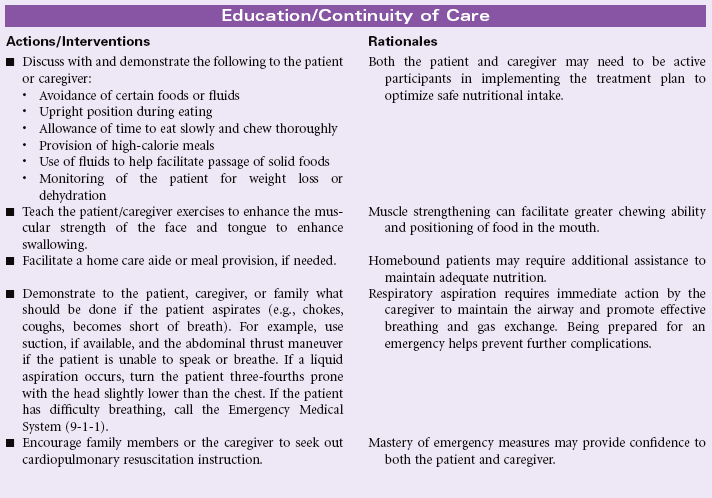
Ineffective Therapeutic Regimen Management
Definition: Pattern of regulating and integrating into daily living a program for treatment of illness and the sequelae of illness that is unsatisfactory for meeting specific health goals
With the ongoing changes in health care, patients are being expected to be co-managers of their care. They are being discharged from hospitals earlier and are faced with increasingly complex therapeutic regimens to be handled in the home environment. Likewise, patients with chronic illness often have limited access to health care providers and are expected to assume responsibility for managing the nuances of their disease (e.g., heart failure patients taking an extra furosemide [Lasix] tablet for a 2-pound weight gain).
Patients with sensory perception deficits, altered cognition, or financial limitations and those who lack support systems may find themselves overwhelmed and unable to follow the treatment plan. Older patients, who often experience most of these problems, are especially at high risk for ineffective management of the therapeutic plan. Other vulnerable populations include patients living in adverse social conditions (e.g., poverty, unemployment, little education); patients with emotional problems (e.g., depression over the illness being treated or other life crises or problems); and patients with substance abuse problems. Culture, ethnicity, and religion may influence one’s health beliefs, health practices (e.g., folk medicine, alternative therapies), access to health services, and assertiveness in pursuing specific health care services.
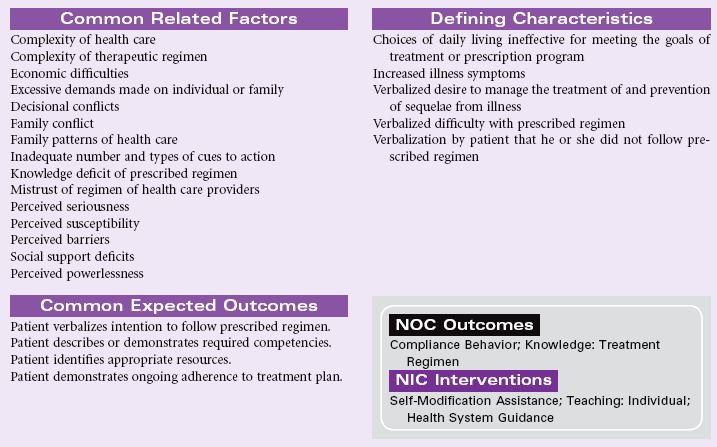
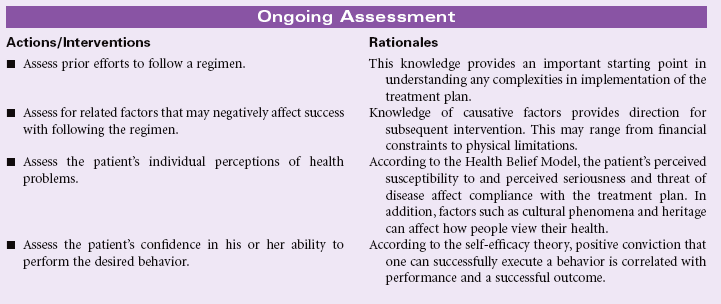
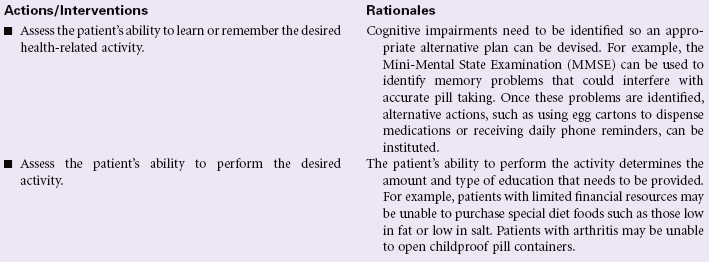
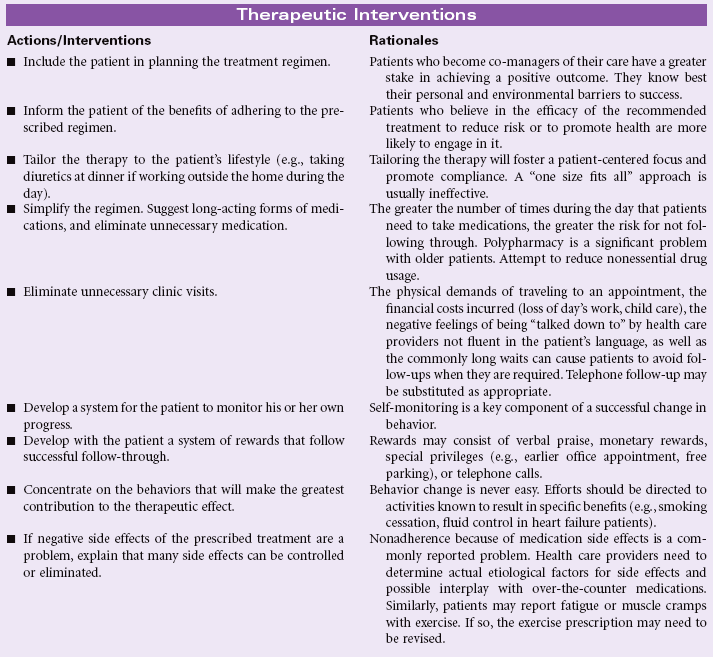

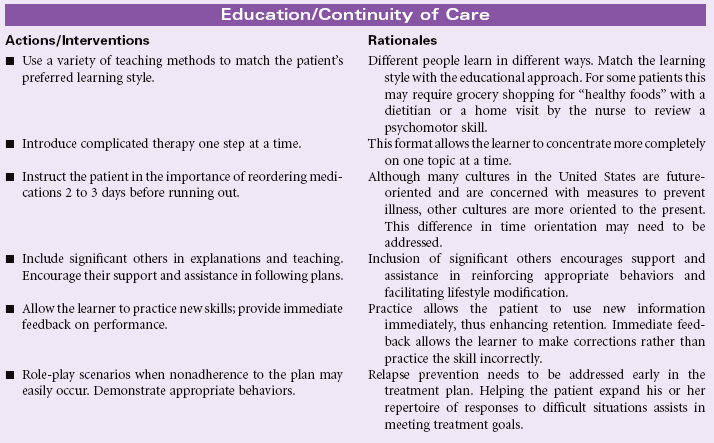
Impaired Tissue Integrity
Definition: Damage to mucous membrane, corneal, integumentary, or subcutaneous tissues
The mucous membranes, cornea, skin, and subcutaneous tissues serve as part of the person’s first line of defense against threats from the external environment. These tissues can be damaged by physical trauma, including thermal injury (e.g., frostbite); chemical injury such as reactions to drugs, especially chemotherapeutic drugs; radiation; and ischemia. Sometimes damaged tissue is able to regenerate, whereas other times the damaged tissue may be replaced by connective tissue. If untreated, impaired tissue places the person at risk for local or systemic infection and/or necrosis (tissue death). People at risk for impaired tissue integrity include older adults, the homeless, individuals undergoing cancer chemotherapy, and individuals with altered sensation.
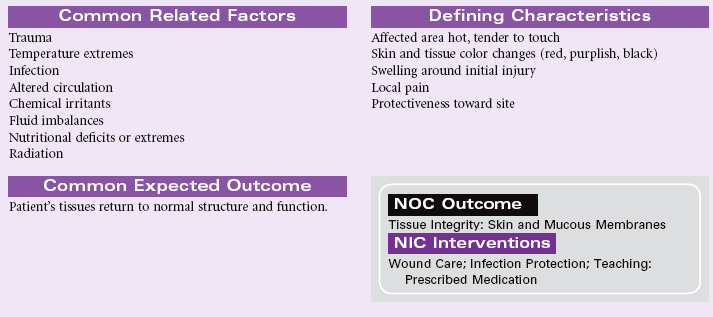
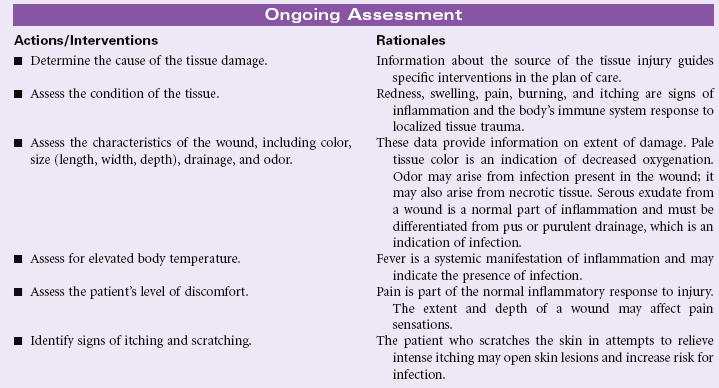

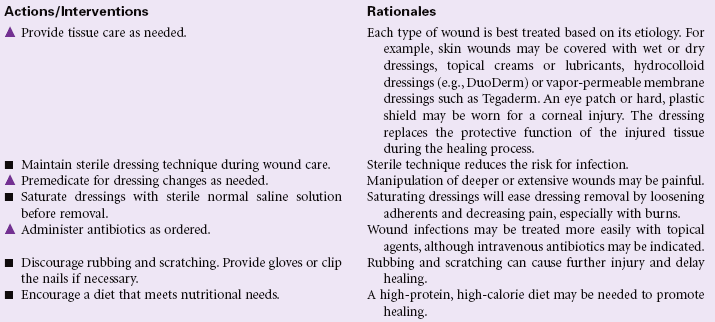
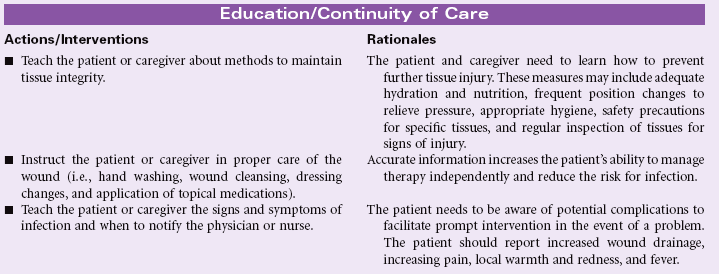
Ineffective Peripheral Tissue Perfusion
Definition: Decrease in oxygen resulting in failure to nourish the tissues at the capillary level
Reduced arterial blood flow causes decreased nutrition and oxygenation at the cellular level. Decreased tissue perfusion can be transient, with few or minimal consequences to the health of the patient, or it can be more acute or protracted, with potentially devastating effects on the patient. Diminished tissue perfusion, which is chronic, invariably results in tissue or organ damage or death. Management is directed at removing vasoconstricting factors, improving peripheral blood flow, and reducing metabolic demands on the body. In practice, patients often present with a combination of causative factors. Therefore this care plan will focus on the general assessment and therapeutic interventions common to many causes. The reader is referred to the more specific medical disorder care plans that follow in later chapters. A list of some of these is provided toward the end of this care plan.
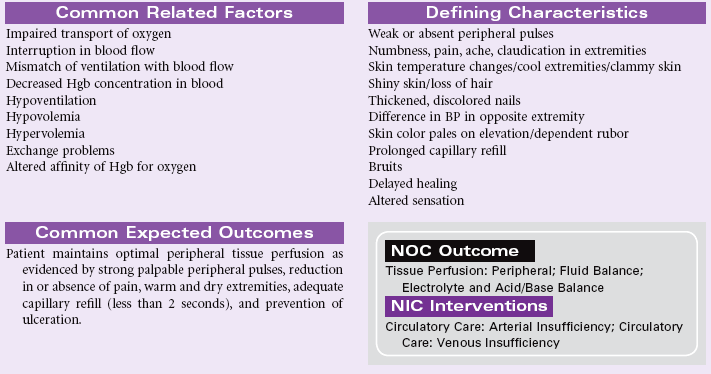
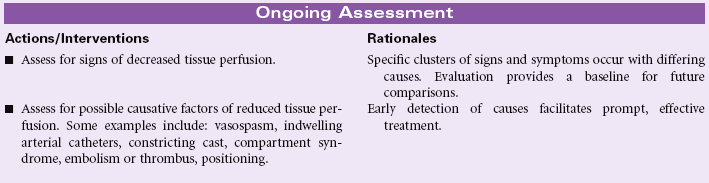
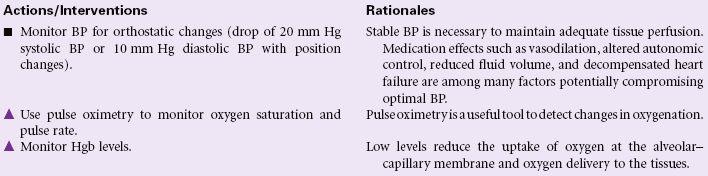
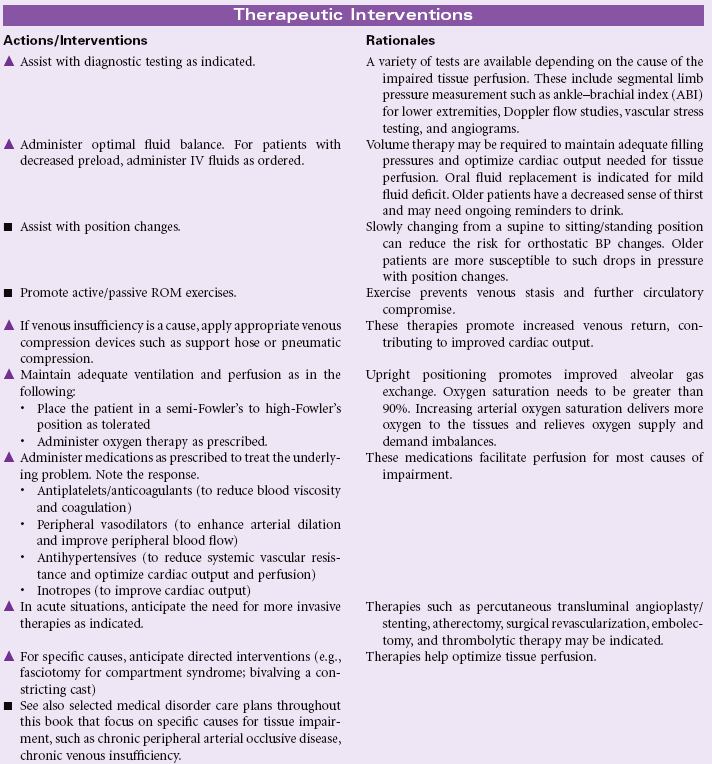
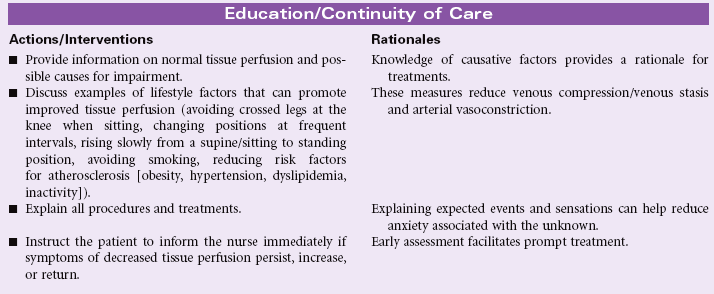
Urinary Retention
Definition: Incomplete emptying of the bladder
Urinary retention may occur in conjunction with or independent of urinary incontinence. Urinary retention, the inability to empty the bladder even though urine is present, may occur as a side effect of certain medications, including anesthetic agents, antihypertensives, antihistamines, antispasmodics, and anticholinergics. These drugs interfere with the nerve impulses necessary to cause relaxation of the sphincters, which allow urination. Obstruction of outflow is another cause of urinary retention. Most commonly, this type of obstruction in men is the result of benign prostatic hyperplasia. Women may experience urinary retention if their bladder sags (cystocele) or if it is pulled out of position by a sagging colon (rectocele).
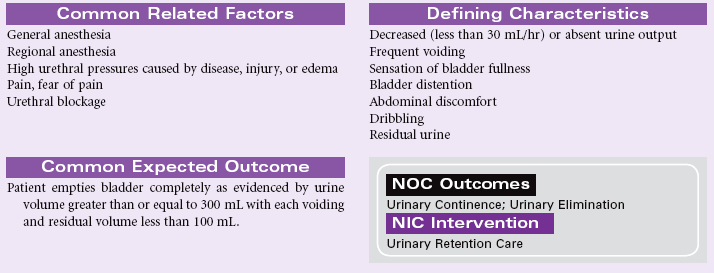
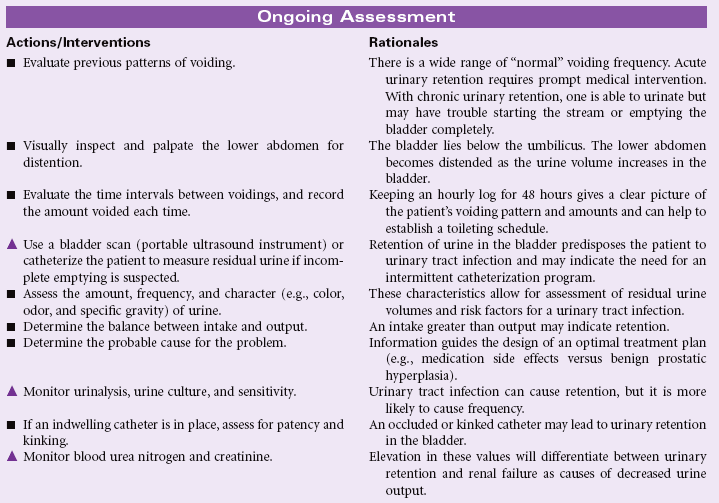
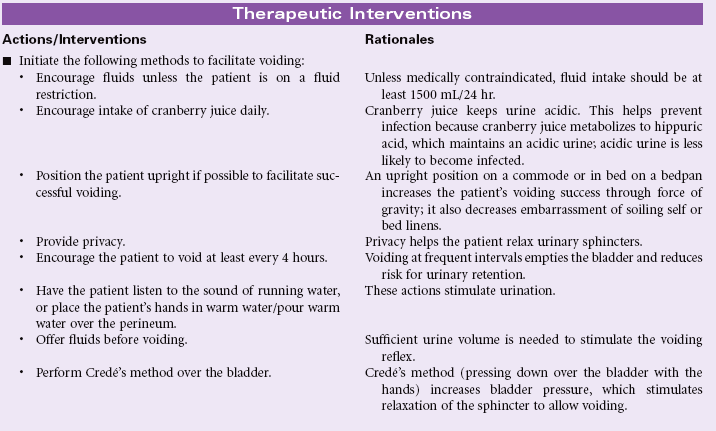
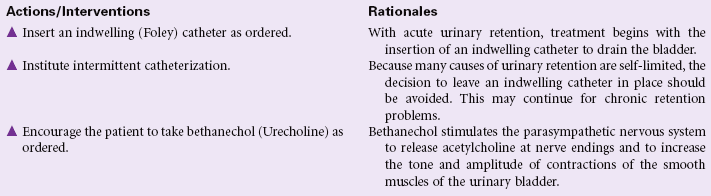
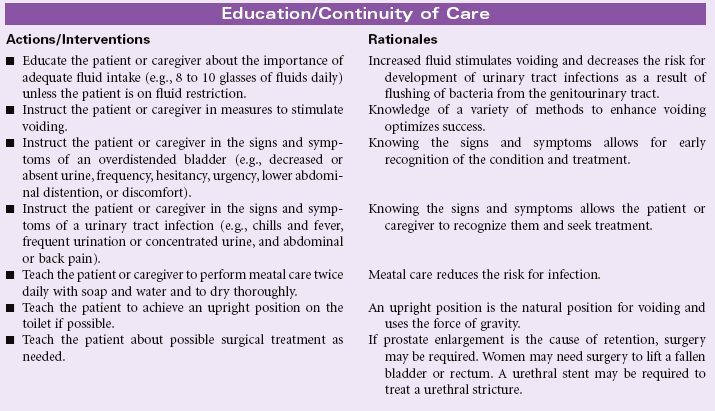
Dysfunctional Ventilatory Weaning Response
Definition: Inability to adjust to lowered levels of mechanical ventilator support that interrupts and prolongs the weaning process
A patient is who is reliant on ventilatory support and unable to tolerate the weaning process is experiencing dysfunctional ventilatory weaning response (DVWR). This may result from physiological, psychological, or situational factors. Their influence should be evaluated before weaning and after each unsuccessful weaning attempt. In addition to the listed related factors, physiological factors associated with the inability to wean may include left ventricular failure, use of medications that depress the respiratory drive (e.g., sedatives, opioids) or cause respiratory muscle weakness (neuromuscular blocking agents or aminoglycosides), alterations in metabolic status (hypophosphatemia, hypothyroidism, hypomagnesemia), acid-base imbalances (metabolic acidosis, respiratory alkalosis), respiratory tract infection, overhydration, anemia, significant alterations in vital signs, abnormal weaning parameters (negative inspiratory force, tidal volume, vital capacity, minute ventilation, rapid shallow breathing index), and a fractional concentration of oxygen in inspired gas (Fio2) of greater than 0.50 on the ventilator. Additional psychological factors may include psychological ventilator dependence and agitation associated with intensive care unit psychosis, delirium, increased anxiety, and fear. Inability to wean may also be a result of lack of motivation secondary to depression, cognitive impairments, or personality disorders. Unfavorable situational factors such as an inappropriate weaning plan may also contribute to weaning failure. When abnormalities or adverse conditions are identified, the weaning plan should incorporate measures to eliminate them or minimize their effects so the risk for DVWR is reduced. Weaning may be postponed when the patient does not demonstrate readiness to wean. This reduces patient frustration and anxiety and avoids potentially life-threatening situations.