12 Fluid, Electrolyte, and Endocrine Problems
 Be sure to check out the supplementary content available at http://evolve.elsevier.com/Hazinski.
Be sure to check out the supplementary content available at http://evolve.elsevier.com/Hazinski.
Pearls
• The term osmolality refers to the concentration of solute (electrolytes and proteins) per liter of fluid. Serum osmolality reflects extracellular fluid osmolality. It can be estimated with the following formula:

Note: This formula does not reflect the influence of plasma proteins or administered osmotic agents such as mannitol. It may be inaccurate in the presence of severe hyperglycemia and hyperlipemia.
• Acute changes in serum sodium and osmolality can cause acute water shifts between the intracellular and extracellular spaces. An acute fall in serum sodium concentration and osmolality and the resulting intracellular water shift can cause cerebral edema. If neurologic symptoms develop, urgent treatment is needed. In general, significant water shifts into and out of the vascular space are poorly tolerated.
• Critical care practitioners use the child's estimated maintenance fluid requirement as a baseline and individualize administered fluid and electrolytes to meet patient needs.
• With the development of acidosis or alkalosis, the serum potassium concentration will change in a direction opposite the change in serum pH, in response to reciprocal potassium and hydrogen ion shifts into and out of the cell.
• If the level of consciousness of the child with diabetic ketoacidosis (DKA) deteriorates during treatment, cerebral edema may be present and urgent intervention is needed. If clinical signs of cerebral edema develop, immediate treatment with intravenous (IV) mannitol or hypertonic saline is needed. If the child's ability to protect the airway or spontaneous ventilation deteriorates, intubation and mechanical ventilation are indicated.
Introduction
Small disruptions in fluid or electrolyte homeostasis or endocrine function can result in significant clinical changes in critically ill infants and children. These disruptions may be a primary problem, or they may be secondary to critical illness, critical injury, or therapeutic interventions (e.g., medication administration, fluid resuscitation).
Anatomy and physiology
Body fluids contain water and solutes. These solutes are positively or negatively charged electrolytes (e.g., Na+, K+, Cl−) and nonelectrolytes (e.g., glucose, urea). Fluid and electrolyte homeostasis is present when fluid and electrolyte balance is maintained within narrow limits despite significant variations in dietary intake, metabolic rate, and renal function.
Fluid Compartments
Water accounts for 65% to 80% of total body weight. The total body water (TBW) volume and distribution are influenced by factors such as age, gender, adipose content, and skeletal muscle mass (Table 12-1). TBW is divided into two compartments (see Evolve Table 12-1 and Evolve Fig. 12-1 in the Chapter 12 Supplement on the Evolve Website for more information): intracellular fluid (ICF) and extracellular fluid (ECF) compartments (Fig. 12-1).
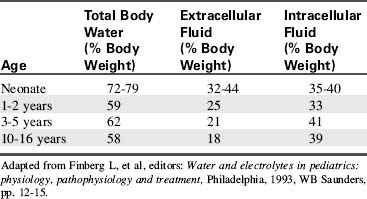
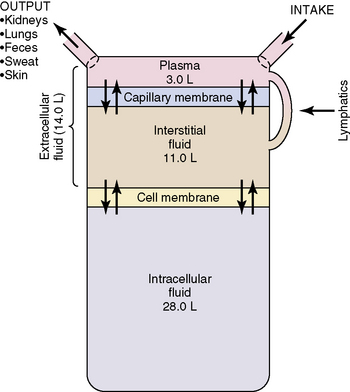
Fig. 12-1 Body fluid compartments showing values for an average 70-kg person.
(From Guyton AC, Hall JE, editors: Textbook of medical physiology, ed 11. Philadelphia, 2006, WB Saunders, p. 292, Fig. 29-1.)
ICF Compartment
The ICF is within the cell membranes. It is the largest fluid compartment, comprising approximately 33% of body weight by 1 year of age. Potassium and phosphate are the primary intracellular electrolytes.
ECF Compartment
The ECF is composed of intravascular fluid (plasma or serum), interstitial fluid (lymph), and transcellular water. The ECF comprises almost half of the body weight in the full-term infant; this percentage declines as the child grows.
Sodium and chloride are the primary electrolytes of the ECF. Although the largest volume within the ECF is interstitial fluid (20% of TBW), it is the plasma or intravascular volume that is essential to cardiac output and systemic perfusion. Transcellular water typically accounts for a small percentage of TBW and is found in the pleural, pericardial, peritoneal, and joint spaces. During some disease states, the volume of transcellular fluid increases.
Fluid Shifts
Fluid compartments are separated by selectively permeable membranes. These membranes permit movement of water and some solutes (e.g., electrolytes) from one compartment to another. This movement of fluids and electrolytes occurs through osmosis, diffusion, active transport, and filtration. If osmolality becomes unequal between compartments, water shifts to restore equilibrium (see section, Role of Osmolality).
Developmental Considerations
Renal function, metabolic rate, body surface area (BSA), and fluid requirements change with development. The infant kidney is unable to concentrate urine until approximately 3 months of age, and it is relatively inefficient at concentrating urine until approximately 2 years of age. In the first years of life the kidneys are also inefficient at excreting electrolytes and waste products, and they are unable to effectively conserve or excrete sodium, acidify urine, or handle large quantities of solute-free water. As a result, infants and small children are less able to maintain homeostasis with sudden, acute changes in fluid and electrolyte intake or output.
Energy requirements (per kilogram body weight) and metabolic rate are higher in infancy and childhood (for further information, see Chapter 14). The ratio of BSA to volume is significantly higher in infants and children than in adults. As a result, pediatric evaporative fluid losses and fluid requirements per kilogram body weight are higher than those of adults.
Insensible water loss (IWL) is fluid lost through the skin, via evaporation and sweat, and through the respiratory tract. Normal IWL is approximately 300 to 400 mL/m2 BSA per day (for more detailed information, see Evolve Table 12-2 in the Chapter 12 Supplement on the Evolve Website). Fever increases IWL by approximately 0.42 mL/kg per hour for each degree Celsius increase above 37° C. Increased IWL can occur with increased air movement across the skin, and with tachypnea, unless inspired air is humidified. IWL decreases when ambient and inspired air are humidified.
Table 12-2 Formulas for Estimating Daily Maintenance Fluid and Electrolyte Requirements for Children
| Daily Requirements | Hourly Requirements | |
| Fluid Requirements Estimated from Weight* | ||
| Newborn (up to 72 hr after birth) | 60-100 mL/kg (newborns are born with excess body water) | – |
| Up to 10 kg | 100 mL/kg (can increase up to 150 mL/kg to provide caloric requirements if renal and cardiac function are adequate) | 4 mL/kg |
| 11-20 kg | 1000 mL for the first 10 kg + 50 mL/kg for each kg over 10 kg | 40 mL for first 10 kg + 2 mL/kg for each kg over 10 kg |
| 21-30 kg | 1500 mL for the first 20 kg + 25 mL/kg for each kg over 20 kg | 60 mL for first 20 kg + 1 mL/kg for each kg over 20 kg |
| Fluid Requirements Estimated from Body Surface Area (BSA) | ||
| Maintenance | 1500 mL/m2 BSA | – |
| Insensible losses | 300-400 mL/m2 BSA | – |
| Electrolytes | ||
| Sodium (Na) | 2-4 mEq/kg | – |
| Potassium (K) | 1-2 mEq/kg | – |
| Chloride (Cl) | 2-3 mEq/kg | – |
| Calcium (Ca) | 0.5-3 mEq/kg | – |
| Phosphorous (Phos) | 0.5-2 mmol/kg | – |
| Magnesium (Mg) | 0.4-0.9 mEq/kg | – |
* The “maintenance” fluids calculated by these formulas must only be used as a starting point to determine the fluid requirements of an individual patient. If intravascular volume is adequate, children with cardiac, pulmonary, or renal failure or increased intracranial pressure should generally receive less than these calculated “maintenance” fluids. The formula utilizing body weight generally results in a generous “maintenance” fluid total.
Fluid and electrolyte requirements will vary with age and clinical condition. Normal baseline fluid and electrolyte requirements are listed in Table 12-2. Critical care practitioners use estimated maintenance fluid requirements as a baseline and individualize administered fluid and electrolytes to meet patient needs.
Fluid, Electrolyte, and Glucose Balance
Role of Osmolality
The term osmolality refers to the concentration of solute (electrolytes and proteins) per liter of fluid. Serum osmolality reflects ECF osmolality. It can be estimated with the following formula*:

Because sodium is the primary electrolyte that determines serum osmolality, a major increase or decrease in serum sodium concentration will increase or decrease the serum osmolality, respectively.
Changes in the osmolality of one body fluid compartment will affect all other compartments. Water shifts between the ICF and the ECF compartments in response to changes in the osmolality of either compartment, moving from the compartment of lower osmolality to the compartment of higher osmolality until osmolality equilibrates. When the osmolality of the extracellular compartment (including the vascular space) decreases, water will shift from the extracellular compartment into cells (Fig. 12-2). Conversely, when the osmolality of the extracellular compartment (including the vascular space) increases, water will shift from the intracellular to the extracellular compartment (including into the vascular space). The volume and acuity of the water shift, as well as likely clinical significance, is determined by the magnitude and acuity of the osmolality gradient between compartments. Significant water shifts can cause neurologic complications.
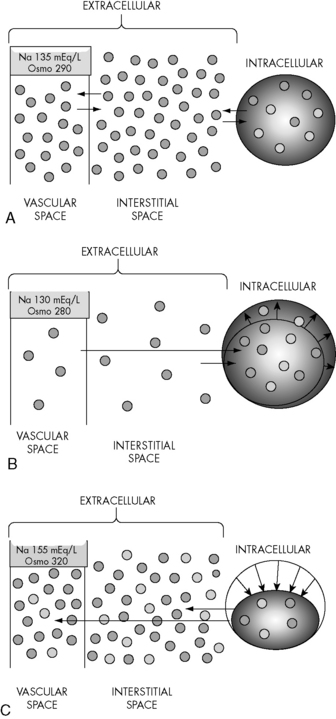
Fig. 12-2 Water shifts with changes in serum sodium and osmolality. A, Normal. Free water shifts between extracellular and intracellular compartments and across the semipermeable vascular membrane (between the vascular and interstitial spaces) to maintain osmotic equilibrium. B, Effects of acute fall in serum osmolality. An acute fall in serum sodium and osmolality cause water to shift from the extracellular (including the vascular space) to the intracellular compartment. Intracellular water volume increases until osmolality equilibrates. The smaller inside circle (under the word “Intracellular”) represents original cell size. The black arrows schematically represent the effects of the shift of water into the intracellular compartment. C, Effects of acute rise in serum osmolality. An acute rise in serum sodium and osmolality cause water to shift from the intracellular to extracellular (including into vascular space) compartment. Intracellular water volume decreases until osmolality equilibrates. The larger outside circle (under the word “Intracellular”) represents original cell size. The arrows schematically represent the effects of the shift of free water from the intracellular to the extracellular compartment.
Renal Influences
The kidneys help maintain fluid balance through filtration and selective reabsorption. Changes in the glomerular filtration rate (GFR) alter the amount of water and sodium excreted or reabsorbed by the kidneys. Expansion of intravascular volume normally increases the GFR, increasing sodium and water excretion. When intravascular volume is depleted, the GFR falls and sodium and water excretion decrease (i.e., more sodium and water are reabsorbed into plasma from the renal filtrate). As noted previously, the kidney is less able to concentrate urine during the first months of life. (See Chapter 13 for more detailed information.)
Endocrine Influences
Several hormones contribute to regulation of fluid and electrolyte balance.
Antidiuretic Hormone (ADH, Vasopressin)
ADH, also known as vasopressin and as arginine vasopressin, is manufactured in the hypothalamus and stored in and released by the posterior pituitary in response to a rise in serum osmolality, a decrease in circulating blood volume (volume depletion), or a decrease in blood pressure. ADH acts on vasopressor-2 receptors of cells in the renal collecting ducts and distal tubules, increasing the permeability of these cells to water; this results in reabsorption of water from the filtrate and returns water to the circulation. Urine volume decreases and urine concentration increases. ADH secretion does not influence the rate of sodium reabsorption, but the serum sodium concentration typically falls because it is diluted by the reabsorbed water.
Negative feedback mechanisms normally regulate ADH secretion to maintain a serum osmolality of 275 to 295 mOsm/L. Osmolality receptors located in the brain are stimulated by a rise in serum osmolality (e.g., above 285 mOsm/L or a rise of at least 2%). Volume-sensitive receptors (located in the left atrium and thoracic vessels) and baroreceptors (stretch receptors located in the ascending aorta, pulmonary arteries, and carotid sinus) are stimulated by volume depletion and hypotension. Additional causes of ADH secretion include stress, trauma and severe pain (through activation of cholinergic neurotransmitters in the hypothalamus), angiotensin II, and some medications.3 A normal or low serum osmolality, hypertension, and an increase in left atrial stretch should inhibit ADH secretion.
Although endogenous ADH does not affect vascular tone, exogenous (administered) vasopressin can cause vasoconstriction and increase blood pressure. For further information regarding use vasopressin, see Chapters 6 and 14.
Aldosterone
Aldosterone, a mineralocorticoid, is secreted by the adrenal cortex in response to sodium depletion, hyperkalemia, or elevated levels of angiotensin II or adrenocorticotrophic hormone. Aldosterone increases sodium reabsorption by the intestine, the renal distal tubules, and collecting ducts; this increases both sodium and water reabsorption. Aldosterone increases renal secretion of potassium and hydrogen ions.
Natriuretic Peptides
The natriuretic peptides are salt-losing hormones that influence blood volume and blood pressure. Atrial natriuretic peptide (ANP) is synthesized, stored, and released by atrial myocytes in response to atrial distension, endothelin, and sympathetic nervous system and angiotensin II stimulation. Increased ANP is present during hypervolemia and congestive heart failure.
Brain natriuretic peptide is synthesized in the brain and in the ventricles of the heart. Brain natriuretic peptide release is triggered by the same conditions that trigger ANP release, and it has similar physiologic actions. Brain natriuretic peptide is a sensitive diagnostic marker for heart failure (see Congestive Heart Failure in Chapter 8).
Natriuretic peptides are involved in the long-term regulation of sodium and water balance, blood volume, and blood pressure. These hormones decrease aldosterone release, increase GFR, produce natriuresis (sodium excretion in urine) and diuresis (potassium sparing), and they decrease renin release, thereby decreasing angiotensin II. These actions reduce blood volume and central venous pressure, cardiac output, and arterial blood pressure. Chronic elevation of natriuretic peptides appears to decrease arterial blood pressure primarily by decreasing systemic vascular resistance.
Serum Glucose in Critically Ill or Injured Children
Although a serum glucose concentration of 60 to 180 mg/dL is normally maintained over a wide range of conditions, critically ill or injured children often develop hypoglycemia or hyperglycemia. Infants have high glucose needs and low glycogen stores, so they can rapidly become hypoglycemic during critical illness or injury.24 Providers should monitor serum glucose concentration with point-of-care testing, if possible, and treat hypoglycemia as needed. Treatment of hypoglycemia should avoid frequent, intermittent bolus administration of large quantities of glucose; provision of a continuous source of glucose is preferable.
Hyperglycemia can result from steroid administration, stress response, relative hypoinsulinemia, or insulin resistance and has been associated with increased mortality in critically ill children in some studies. A prospective, randomized study of tight control of serum glucose concentration in critically ill children (targeted to age-adjusted normal fasting glucose concentration) reduced critical care unit mortality,37 but was associated with episodes of hypoglycemia. In general, an insulin infusion (0.5-1 unit regular insulin/kg per hour) is often titrated during the first 18 to 24 hours of critical care therapy to maintain the serum glucose concentration less than 150 mg/dL (range will vary; use your unit protocol). Careful monitoring is required to avoid and treat episodes of hypoglycemia. The ultimate value versus risk of this approach is still under investigation.
Electrolyte homeostasis and common imbalances
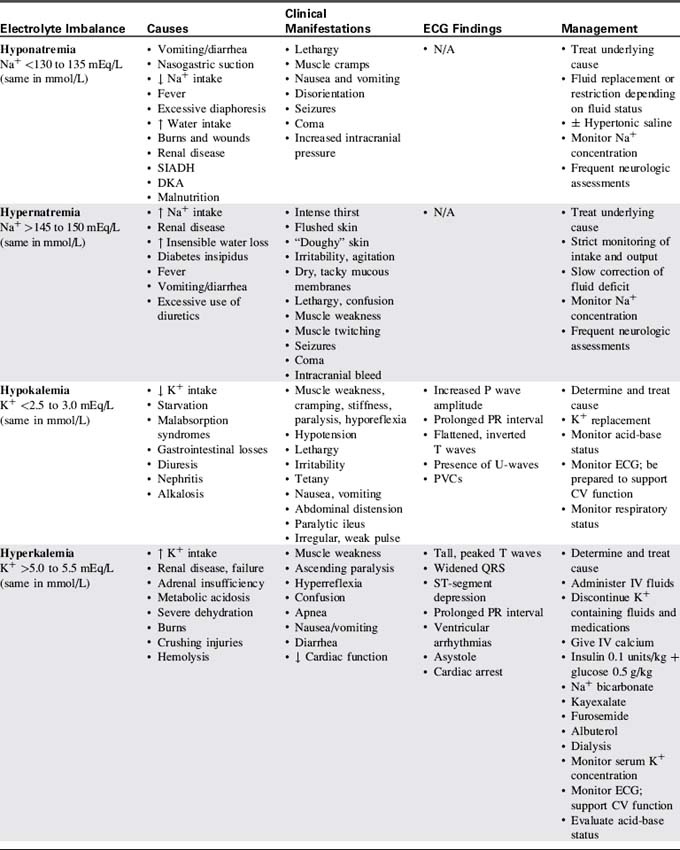
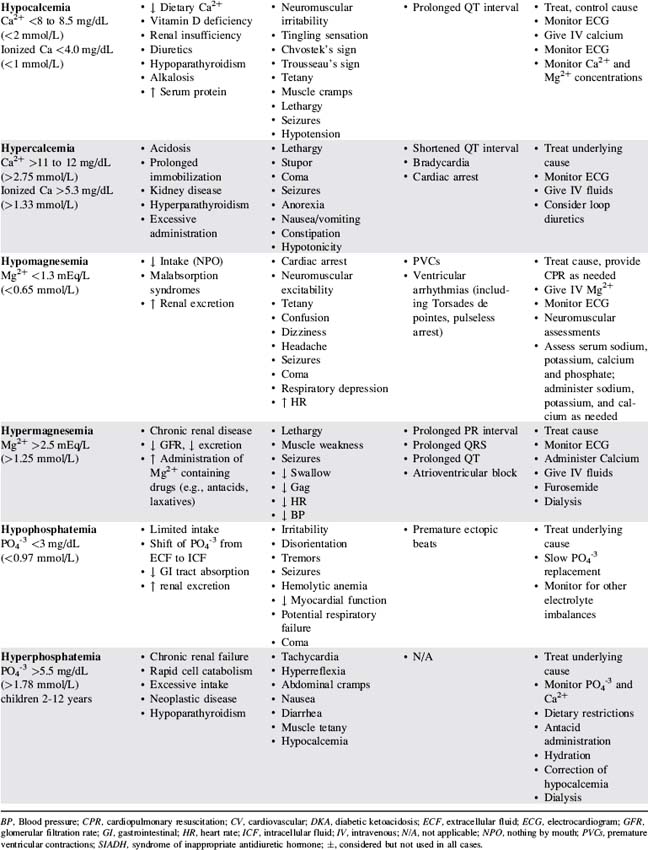
Table 12-3 presents a summary of electrolyte imbalances and associated clinical manifestations in critically ill infants and children. In the following sections, approximate ranges for normal and abnormal serum electrolyte concentrations are listed, but providers should use normal ranges referenced by the clinical laboratory in their practice settings.
Sodium Homeostasis
Sodium (Na+), the primary extracellular cation, plays an important role in the regulation of action potentials in skeletal muscles, nerves, and the myocardium; maintenance of acid-base balance; and maintenance of ECF balance. The normal serum sodium concentration is approximately 135 to 145 mEq/L.
Alterations in sodium and fluid balance often occur concurrently and can alter serum osmolality. An abnormal serum sodium concentration often results from fluid volume deficit or excess. GFR and aldosterone secretion both affect sodium balance.
Sodium Imbalance: Hyponatremia
Etiology
Hyponatremia is a low serum sodium concentration, typically less than 130 to 135 mEq/L. It often develops as a complication of disease or therapy. The critically ill infant or child can develop hyponatremia from excessive water intake relative to sodium, excess water retention, increased sodium loss, or a combination of these factors.10
Hyponatremia can occur in conjunction with hypervolemia, euvolemia, or hypovolemia. Hypervolemic hyponatremia is associated with water intoxication, nephrotic syndrome, cardiac failure, renal failure, and the syndrome of inappropriate antidiuretic hormone (SIADH). Hypovolemic hyponatremia can occur with renal losses (e.g., osmotic diuresis, renal tubular acidosis) or extrarenal losses (e.g., diarrhea, vomiting, burns).10 Other potential causes include adrenal insufficiency, excessive use of diuretics, and cerebral salt-wasting syndrome.
A laboratory report of a low serum sodium concentration can be misleading. These pseudohyponatremic states are associated with hyperlipidemia, hyperproteinemia, or hyperglycemia. In hyperlipidemia or hyperproteinemia, the lipid or protein displaces fluid from serum, decreasing the relative volume of water and electrolytes. As a result, the reported serum sodium concentration will be low. The total body sodium actually may be normal, although its concentration (in milliequivalents per liter of plasma, or mEq/L) is reduced. Hyperlipidemia of this degree usually produces a milky white plasma.
Because the serum osmolality is determined by the combined effects of particles (solutes) in the serum—especially the sodium, glucose, and blood urea nitrogen—the serum osmolality can be normal if a fall in the concentration of one solute is accompanied by a commensurate (in osmotic effect) increase in the concentration of another solute. With significant hyperglycemia, the high glucose concentration increases serum osmolality, drawing fluid into the vascular space; this may artificially reduce the serum sodium concentration. The significance of this dilutional effect is debatable—the serum sodium concentration may still influence osmotic changes to which the cells are exposed. To estimate the potential effect of severe hyperglycemia on the serum sodium concentration, for every 100 mg/dL rise in serum glucose above normal, the serum sodium concentration is likely to be depressed approximately 1.6 mEq/L below 135 mEq/L.
Pathophysiology and Clinical Signs and Symptoms
An isolated decrease in serum sodium concentration (i.e., without a rise in glucose or blood urea nitrogen) reduces serum osmolality; an acute fall in serum osmolality produces a shift of water from the extracellular compartment (including vascular space) to the intracellular compartment. This fluid shift can cause swelling of cells (edema). Because there is limited capacity for volume expansion within the skull, swelling of brain cells (cerebral edema) can have catastrophic consequences, such as brain herniation and death.
The volume of water shift and the severity of clinical manifestations with hyponatremia are directly related to the acuity and the magnitude of the fall in serum sodium and osmolality. Infants and children who develop hyponatremia that gradually worsens over several days or weeks (e.g., with adrenocortical insufficiency) typically have milder clinical manifestations and may be asymptomatic until the serum sodium is very low.26
Acute hyponatremia that develops within hours or days (i.e., <48 hours) is more likely to produce cerebral edema.26 Seizures and coma are associated with a serum sodium concentration less than 120 mEq/L.
Management
If the child is at risk for hyponatremia, providers should closely monitor the child's serum sodium concentration to detect and promptly treat hyponatremia before it becomes severe. Frequent neurologic assessments are indicated. Notify an on-call provider immediately if the child develops altered level of consciousness, seizures, or signs of increased intracranial pressure.
Hyponatremia associated with neurologic symptoms is a neurologic emergency. Urgent treatment includes administration of 2 to 4 mL/kg of 3% saline (513 mEq sodium/L, or 0.513 mEq/mL); this will typically raise the child's serum sodium concentration approximately 1 to 2 mEq/L and raise serum osmolality sufficiently to slow the intracellular water shift. If the SIADH produces seizures or other severe symptoms, hyponatremia and water intoxication can be treated acutely by administration of hypertonic saline (2-4 mL/kg of 3% saline) and furosemide (1-2 mg/kg). These medications will increase the serum sodium concentration and eliminate excess free water (see section, Specific Diseases, Syndrome of Inappropriate Antidiuretic Hormone).
Management of hyponatremia includes restoration of appropriate intravascular volume, replacement of the sodium deficit, and identification and treatment of the underlying cause. Symptomatic hypovolemia is treated with boluses of normal saline or lactated Ringer's solution. Management of hypervolemic hyponatremia may include fluid restriction and administration of loop diuretics.
Once the child's neurologic status is stable and perfusion is adequate, plans are made to replace the sodium deficit. The following formula36 is used to calculate the sodium deficit:
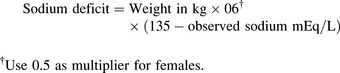
During treatment of hyponatremia, providers must closely monitor the serum sodium concentration and the rate of rise in the concentration. If the serum sodium and osmolality are raised too rapidly, the resulting water shifts from the cellular to the extracellular (including intravascular) compartments can produce neurologic complications including intracranial bleeding (Box 12-1). In general, the serum sodium should be raised no faster than approximately 0.5-1.0 mEq/L per hour.35 Additional important assessments include strict monitoring of intake and output, urine specific gravity, serum electrolytes, serum osmolality, and daily weights.
Box 12-1 Advanced Concepts: Potential Central Nervous System Complications of Rapid Changes in Serum Sodium and Osmolality
The brain does not tolerate rapid or significant water shifts into and out of the cells. A shift of water into brain cells—such as that occurring with an acute fall in serum sodium concentration and serum osmolality—is likely to produce cerebral edema. A rapid shift of water from cells, including brain cells, can cause the cells to shrink and can result in cerebral dysfunction. Cells in the gray matter and tissue in the white matter in the brain swell and shrink at different rates when water shifts occur. As a result, significant water shifts between intracellular and extracellular compartments in the brain can cause tearing of cerebral bridging veins and intracranial bleeding.
Rapid correction of hyponatremia has been shown to result in cerebral dysfunction, linked with damage to the myelin sheath of neurons. This myelinolysis is called central pontine myelinolysis if it occurs in the pons (brainstem) and osmotic demyelinization syndrome if it occurs elsewhere in the brain. Signs of brain dysfunction can include decreased level of consciousness, lack of coordination, paralysis, and dysphagia. Because there is no known treatment for such cerebral dysfunction, and it can cause permanent disability, prevention is critical. In general, unless neurologic symptoms indicate the need for more aggressive treatment, providers should aim to correct hyponatremia or hypernatremia no faster than approximately 0.5 mEq/L per hour (or 10-12 mEq/L per day). For more information, consult the National Institutes of Health Web site: http://www.ninds.nih.gov/disorders/central_pontine/central_pontine_myelinolysis.htm.
Sodium Imbalances: Hypernatremia
Etiology
Hypernatremia (serum Na+ >145-150 mEq/L) occurs less frequently than hyponatremia. One of the body's major defenses against hypernatremia is thirst. Infants, small children, and any children with significant developmental delay, decreased level of consciousness, or critical illness have an increased risk of hypernatremia during episodes of fluid loss, because they may not be able to signal caregivers of thirst or drink additional fluids.
Hypernatremia is most likely to result from a water deficit (e.g., dehydration, diuretic use, diabetes insipidus, DI). Less commonly, hypernatremia can result from excessive sodium intake, such as if powder for infant formula is incorrectly diluted. The child with hypernatremia may be hypovolemic, euvolemic, or hypervolemic; therefore, it is important to assess the child's fluid volume status when determining the cause of the hypernatremia.
Pathophysiology and Clinical Signs and Symptoms
Hypernatremia typically increases the serum osmolality. The rise in osmolality stimulates the posterior pituitary to release ADH, which increases renal water reabsorption until the osmolality returns to normal. The increased osmolality associated with hypernatremia also leads to a shift in water from the intracellular to the extracellular compartment, including into the vascular space. This water movement from the cells can cause cellular dehydration and central nervous system dysfunction. Complications including subdural, subarachnoid, and intracerebral bleeding and sinus vein thrombosis can develop with acute and severe increases in serum sodium concentration and the resulting water shift (see Box 12-1). Permanent central nervous system dysfunction can result when the serum sodium concentration is extremely high (e.g., >165-170 mEq/L).12 When serum osmolality is chronically elevated, brain cells will generate idiogenic osmoles to maintain cell volume (Box 12-2).
Box 12-2 Advanced Concepts: The Role of Idiogenic Osmoles in Brain Cells
When extracellular (including serum) osmolality rises, water shifts from the intracellular to the extracellular compartment, and cells typically shrink. When the serum osmolality is chronically elevated, brain cells generate idiogenic osmoles (e.g., glycine and taurine) to help brain cells maintain normal cell volume despite a water shift to the extracellular space. These idiogenic osmoles, however, may contribute to cerebral edema if a high serum osmolality is lowered too rapidly.
Patients who are unable to produce and/or respond to ADH (e.g., patients with DI) are at risk for development of significant hypernatremia and hypovolemia. These patients must be closely monitored to detect and treat these complications before they become severe.
Management
If the patient with hypernatremia has signs of inadequate tissue perfusion (i.e., shock), administer isotonic crystalloid by bolus (20 mL/kg) until perfusion is adequate. Avoid excessive bolus fluid administration (i.e., beyond that needed to treat shock), because it can contribute to a rapid fall in serum sodium and osmolality resulting in cerebral edema and other neurologic complications (see Box 12-2).
Once shock is corrected, estimate the fluid deficit and plan to replace the deficit over 48 to 72 hours, while providing for maintenance fluid requirements as well as for replacement of any ongoing additional fluid losses (e.g., persistent diarrhea). The type of IV fluids administered will vary depending on the rate at which the serum sodium is falling during therapy. Generally, the serum sodium should decrease at a rate no faster than 0.5 to 1.0 mEq/L per hour.
Monitor patients for the clinical manifestations of cerebral edema throughout the course of their treatment. Management of the child with hypervolemic hypernatremia will typically involve loop diuretics and decreased sodium administration.
Potassium Homeostasis
Potassium is the primary intracellular cation (i.e., a positively charged ion). The magnitude of the transmembrane (i.e., between intracellular and extracellular) potassium gradient determines the excitability of nerve and muscle cells (including skeletal and heart muscle) and the rate of conduction of nerve impulses. Potassium also plays a significant role in the maintenance of acid-base balance.
The normal serum potassium (K+) concentration is 3.0 to 5.0 mEq/L. The intracellular potassium concentration is much higher, approximately 150 mEq/L.28 Small alterations in serum potassium concentration can significantly affect the transmembrane gradient and therefore neuromuscular and cardiac function. The serum K+ concentration is affected by potassium intake and excretion, renal regulation, and serum pH. Because the intravascular (serum) potassium concentration represents only a small proportion of the total body potassium, accurate interpretation of the child's potassium balance requires consideration of the child's clinical status and acid-base balance.
Potassium ions normally shift between the intra- and extracellular compartments with changes in the serum pH (see Evolve Fig. 12-2 in the Chapter 12 Supplement on the Evolve Website). When the serum hydrogen ion concentration increases (i.e., with acidosis or a fall in pH), hydrogen moves from the extracellular to the intracellular compartment, where it is buffered. To maintain a balance of cation movement across cell membranes, the intracellular movement of hydrogen ions is associated with an extracellular shift of potassium. Thus, acidosis or a fall in pH (e.g., with correction of alkalosis) is associated with a rise in serum potassium concentration. In contrast, alkalosis or a rise in serum pH (e.g., with treatment of acidosis) is associated with a fall in serum potassium, because hydrogen ion shifts out of cells and is replaced by potassium.
The change in serum potassium concentration associated with changes in serum pH will always be in the direction opposite the change in pH. That is, if the pH falls (as in acidosis) the serum potassium usually rises; as acidosis is corrected (the pH rises) the serum potassium should fall. Hypokalemia with acidosis is particularly dangerous: as acidosis is treated and the serum pH rises, the serum potassium concentration will fall further. Thus, correction of acidosis in the child with hypokalemia and acidosis may result in a dangerously low serum potassium concentration. The potassium concentration should always be evaluated in light of the patient's present acid-base status, and likely changes in potassium concentration should be anticipated in response to changes in acid-base status that will result from planned therapy.
The kidneys play a critical role in potassium homeostasis. Renal failure limits the kidney's ability to excrete potassium and may result in hyperkalemia (see Chapter 13).
Potassium Imbalances: Hypokalemia
Etiology
Causes of hypokalemia (serum K+ concentration <2.5 to 3.0 mEq/L) can be classified into three general categories: inadequate potassium intake (rare, but may be iatrogenic), shifts of potassium from the extracellular to the intracellular compartment (e.g., with alkalosis or a rise in serum pH), or excessive losses of potassium (see Evolve Fig. 12-3 in the Chapter 12 Supplement on the Evolve Website for more information). Critically ill patients often develop true potassium deficit following the use of diuretics, especially loop and thiazide diuretics. Some antimicrobial agents (e.g., amphotericin B or carbenicillin) can increase renal potassium losses. Hypokalemia also is associated with severe hypochloremia and the potassium-wasting Bartter's syndrome.
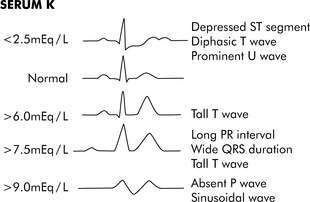
Fig. 12-3 Electrocardiogram changes with hypokalemia and hyperkalemia.
(From Park MK, Guntheroth WG: How to read pediatric ECGs, ed 3, St. Louis, 1992, Mosby, p. 108.)
Because gastrointestinal fluids all contain significant amounts of potassium in the form of potassium chloride salt, vomiting, diarrhea, intestinal fistulas of the small intestine or colon, ileostomy drainage, or gastric suctioning can all result in potassium losses as well as loss of hydrogen ions and chloride.
Pathophysiology and Clinical Signs and Symptoms
The large quantity of intracellular potassium serves as a reservoir to help maintain intravascular potassium concentration despite potassium loss. When the serum potassium concentration begins to decline, some intracellular potassium, known as the exchangeable potassium, moves from the intracellular space to the extracellular compartment (including the vascular space). Only when this amount of exchangeable potassium is depleted will further extracellular potassium loss produce a fall in serum potassium concentration. Thus, the serum potassium concentration may be normal or even elevated when a total body potassium deficit is present.
Evaluation of the patient's potassium balance is further complicated by potassium shifts between the intracellular and extracellular compartments that result from administration of some medications and with changes in acid-base balance. β-Adrenergic agonists (e.g., inhaled albuterol) can cause a fall in serum potassium, whereas α-adrenergic agents can cause a rise in serum potassium. β-Adrenergic agonists increase intracellular sodium ion movement that stimulates the sodium-potassium pump to move sodium out of the cells. For every three sodium ions pumped out of cells, two potassium ions are allowed to enter cells. Thus, potassium shifts from the extracellular (including vascular) to the intracellular space.
Alpha-adrenergic agents can cause a rise in serum potassium, because potassium shifts from the intracellular to the extracellular (including vascular) space. Insulin administration can produce a fall in the serum potassium concentration, because insulin stimulates cellular uptake of potassium.
Acute alkalosis or a rise in serum pH (e.g., during treatment of acidosis) will cause a fall in serum potassium concentration, because hydrogen ion shifts out of the cell and is replaced by potassium (i.e., potassium moves into the cells). If the serum potassium concentration is within the normal range and the child's serum pH then rises (e.g., as occurs with treatment of acidosis) hypokalemia may result.
Hypokalemia may also result from increased renal potassium excretion. This hypokalemia can be associated with metabolic alkalosis, renal tubular acidosis, and DKA. Hypokalemia can perpetuate metabolic alkalosis, particularly if either condition is chronic. When the serum potassium concentration is low, the kidney vigorously reabsorbs potassium and must excrete hydrogen ions. As a result, it may be necessary to treat the child's hypokalemia to correct significant alkalosis.
Excessive renal potassium losses can also result from increased mineralocorticoid activity and increased delivery of sodium to the distal nephron. Excessive renal potassium losses have been associated with administration of antibiotics such as carbenicillin (and other penicillins), amphotericin B, gentamicin and aminoglycosides. A common cause of hypokalemia in the critically ill patient is the use of diuretics, especially loop and thiazide diuretics.
Chronic hypokalemia can change renal concentrating ability and cause polyuria. The kidney has little ability to conserve potassium when body potassium stores become low; as a result, urinary potassium excretion will remain greater than 20 mEq/L once hypokalemia persists for 10 to 20 days.
Although some potassium is lost with vomiting, diarrhea, and loss of other gastrointestinal fluids, potassium losses are exacerbated by intravascular volume contraction. Hypovolemia stimulates aldosterone secretion, which produces sodium and water retention, but it increases hydrogen ion and potassium excretion.
Hypokalemia can cause hyperpolarization of nerve and muscle cells, leading to muscle weakness, slowed nerve impulse conduction, and decreased muscle contraction. Hypokalemia can cause characteristic electrocardiogram (ECG) changes, including development of a U-wave (Fig. 12-3).
Management
Nurses should watch for ECG changes in patients with or at risk for development of hypokalemia. Patients with preexisting cardiac disease may be particularly likely to develop arrhythmias with even mild hypokalemia. Because hypokalemia will potentiate the effects and potential toxic effects of digitalis glycosides (as the result of depressive effects on the sodium-potassium adenosine triphosphatase pump), it is very important to monitor and maintain serum potassium concentration and promptly treat hypokalemia in patients receiving digitalis.
The appropriate speed and method of potassium replacement is based on the severity of the hypokalemia and the child's clinical condition (including acid-base balance, renal function and urine output). Replacement is typically indicated if the serum potassium concentration is below 3 mEq/L or if the child becomes symptomatic. Enteral replacement in a dose of 0.5-1 mEq/kg will usually correct mild, asymptomatic hypokalemia.17 The dose may be repeated every 4 to 8 hours.
IV potassium administration is indicated when the serum potassium concentration is less than 2.5 mEq/L or when milder levels of hypokalemia are present in patients who cannot receive enteral replacement (Box 12-3). A typical IV supplement dose is 0.5 to 1.0 mEq/kg, infused over approximately 1 to 3 hours.6,17 Dilute the potassium adequately and administer it over several hours to prevent bolus or rapid delivery that can produce lethal arrhythmias. Closely monitor the child's serum potassium concentration and ECG.
Box 12-3 Recommended Intravenous Potassium Dose and Administration Guidelines*
• Daily: 2-5 mEq/kg per day in parenteral nutrition fluid or in divided doses
• Supplement: 0.5-1.0 mEq/kg per dose administered over 1-3 hours via syringe or infusion pump
• Typical maximum concentration
Information consistent with Lacy CF, et al: Lexicomp's drug information handbook, ed 18. Hudson, OH, 2009, Lexicomp; and Custer JW, Rau RE: The Harriet Lane handbook, ed 18, Philadelphia, 2009, Mosby-Elsevier.
* See also institutional guidelines.
The Institute for Safe Medication Practices lists IV potassium among drugs with heightened risk of causing patient harm when administered in error. Most institutions have developed policies regarding IV potassium supplement infusions that incorporate patient safety checks, frequent laboratory verification of serum potassium concentration, and pharmacy preparation of solutions.
If hypokalemia is induced by an acute respiratory or metabolic alkalosis, the treatment of choice is correction of the alkalosis. Potassium administration is rarely necessary.
Potassium Imbalances: Hyperkalemia
Etiology
Hyperkalemia (serum potassium >5.0-5.5 mEq/L) can cause life-threatening arrhythmias; it can result from potassium administration, extracellular (including into the intravascular space) shift of potassium ions associated with a fall in serum pH, significant cell destruction (and release of intracellular potassium), or reduced renal excretion of potassium ions.
Pseudohyperkalemia is a high reported serum potassium concentration caused by release of intracellular potassium at the time of phlebotomy or in the specimen after collection.28 Intracellular potassium is released during fingerstick or other traumatic blood sampling and can be released in a blood specimen after collection in patients with severe leukocytosis or thrombocytosis. Pseudohyperkalemia should be considered when an unexpected high serum potassium concentration is reported by the laboratory in patients who are asymptomatic and have an otherwise normal electrolyte and/or acid-base status. If there is a question about the accuracy of a high reported serum potassium concentration in an asymptomatic patient, the concentration should be rechecked before therapy is initiated to reduce the serum potassium.
Pathophysiology and Clinical Signs and Symptoms
A rise in serum potassium concentration in the healthy patient is usually transient because enhanced renal excretion can quickly return the serum potassium concentration to normal. However, if the rate of potassium accumulation exceeds the rate of renal potassium excretion, the serum potassium concentration will rise.
A rise in serum potassium is associated with a fall in serum pH, because potassium shifts from the intracellular to the extracellular compartment (including into the vascular space). Theoretically, for each 0.1 fall in the arterial pH, the serum potassium concentration can be expected to rise 0.6 to 0.8 mEq/L. When the acidosis is corrected (i.e., the serum pH rises), the serum potassium concentration should fall. In this situation, hypokalemia with acidosis is particularly dangerous, because correction of the acidosis can be associated with development of severe hypokalemia. Conversely, because alkalosis lowers the serum potassium concentration (see Hypokalemia, earlier), a high serum potassium concentration in an alkalotic patient is significant and will likely rise further when the alkalosis is corrected.
Additional causes of extracellular (including intravascular) shifts in potassium are: insulin deficiency, rapid cell breakdown, burns, trauma, hyperosmolality (e.g., hyperglycemia, mannitol administration), rhabdomyolysis, and the administration of succinylcholine.23 Unless the amount of cellular potassium release is excessive, such as in crushing injuries, tumor necrosis syndrome, or administration of succinylcholine, such an extracellular potassium shift alone rarely causes clinically significant hyperkalemia.23
Decreased potassium elimination can result from renal dysfunction or the administration of medications such as potassium-sparing diuretics. Although both acute and chronic renal failure can cause hyperkalemia, patients with acute renal failure are at higher risk for life-threatening hyperkalemia because the potassium concentration often rises quite rapidly, before the body is able to mount a compensatory response.28 Acidosis or cell injury in these patients will likely worsen the severity of the hyperkalemia.
Hyperkalemia can produce characteristic changes in the ECG such as a tall, peaked T wave, followed by widening of the QRS complex, S-T segment depression, and decreased R-wave amplitude (see Fig. 12-3). If the serum potassium concentration continues to rise, the P-R interval is prolonged, the amplitude of the P wave decreases, and finally the P wave disappears. Ultimately the patient's rhythm deteriorates into a classic sine wave. Ventricular arrhythmias or fibrillation can occur at any point during this progression.
Management
Critical care management of hyperkalemia includes recognition of at-risk patients, and rapid identification and correction of the hyperkalemia. Priorities of management are determined by the child's clinical presentation (for more information regarding treatment of hyperkalemia in the patient with renal failure, see Chapter 13).
If the serum potassium concentration is less than 6.5 mEq/L and no ECG changes are present, it may be sufficient to discontinue potassium in IV fluids and medications and closely monitor the patient and the serum potassium concentration. Administration of polystyrene sulfonate (Kayexalate) may be warranted to increase intestinal potassium removal (it results in the exchange of sodium for potassium in the intestinal lumen). Polystyrene sulfonate may also bind calcium and magnesium; therefore, providers should monitor serum concentration of these electrolytes and assess patients for the clinical manifestations of hypocalcemia and hypomagnesemia.
Immediate intervention is required when the serum potassium concentration is greater than 6.5 to 7.0 mEq/L or is associated with ECG changes (see Fig. 12-3). Although the evidence supporting emergent therapies for hyperkalemia is largely anecdotal, widely accepted goals are to stabilize the myocardial cellular membrane, expand the ECF volume, shift potassium into the cells, and remove potassium from the body (Table 12-4).16,19,20,24
Table 12-4 Emergent Management of Hyperkalemia
| Management Goal | Intervention | Comments |
| Stabilize myocardium | Calcium salts |
Onset of action occurs within minutes and lasts for approximately 30 min* |
| Expand ECF volume | Intravenous fluids | Decrease serum concentration of potassium |
| Shift potassium into the ICF | Sodium bicarbonate | Results in an intracellular shift of potassium; it may take up to 60 min for this to occur,* and the effects can last several hours; acid-base status must be monitored closely.† Monitor children with respiratory failure carefully, because buffering of sodium bicarbonate increases CO2 and may worsen respiratory acidosis if the lungs cannot clear CO2. Hypernatremia may develop as complication of this therapy. |
| Insulin and glucose/dextrose | Administration of insulin (0.1 unit regular insulin/kg) will activate the sodium-potassium pump, resulting in increased cellular uptake of potassium; insulin should be administered in conjunction with glucose/dextrose.† The decrease in serum potassium occurs within 15 min and lasts approximately 60 min.* | |
| Albuterol | Activates the sodium-potassium pump and stimulates the pancreas to release insulin, thereby causing an intracellular shift of potassium; administer albuterol in conjunction with insulin to produce cumulative effect in lowering serum potassium‡ | |
| Remove potassium from the body | Kayexalate | Decreases potassium absorption in the intestine |
| IV furosemide (thiazide diuretic) | May not be a viable option in infants or children with hyperkalemia and impaired renal function | |
| Dialysis | Indicated for hyperkalemia refractory to medical management |
ECF, Extracellular fluid; ICF, intracellular fluid; IV, intravenous.
* Ahee P, Crowe AV: The management of hyperkalemia in the emergency department. J Accid Emerg Med 17:188-191, 2000.
† Jones RE, Brashers VL, Huether SE: Alterations of hormonal regulation. In: McCance KL, Huether SE, editors: Pathophysiology: the biologic basis for disease in adults and children, ed 6. Philadelphia, 2009, Mosby-Elsevier.
‡ Chmielewski CM: Hyperkalemic emergencies: mechanisms, manifestations and management. Crit Care Nursing Clin North Am 10:449-458, 1998.
Calcium Homeostasis
Calcium (Ca2+) is the most abundant mineral in the body. Calcium, phosphorous, and magnesium are important in nerve impulse transmission, smooth and cardiac muscle contraction, bone composition, and activation of cellular enzymatic processes.
Most of the body's calcium stores are found in bones and teeth, with the remainder in soft tissue and serum. Approximately 50% of serum calcium is bound to anions or protein and is unavailable for use by the body. The remaining 50% is ionized; it is this ionized serum calcium that influences cardiac function, muscle contraction, nerve impulse transmission, and coagulation.
The serum albumin concentration and acid-base status will affect the serum ionized calcium concentration. An increase in serum albumin will decrease the portion of the total serum calcium that is ionized, because more calcium will bind albumin. The serum ionized calcium concentration will rise with acidosis (a fall in serum pH) and fall with alkalosis (a rise in serum pH). Thus, the serum ionized calcium concentration changes in a direction opposite the pH.
Serum calcium concentration is tightly regulated through the effects of parathyroid hormone (PTH), calcitonin, and vitamin D and their effects on calcium and phosphate deposition and resorption from bone, absorption in the intestine, and reabsorption and excretion in the kidney. A fall in serum ionized calcium concentration stimulates PTH production and secretion, which in turn increases intestinal calcium absorption, increases renal calcium reabsorption, and inhibits renal phosphate reabsorption; therefore, more phosphate is excreted in the urine. PTH also mobilizes calcium from bone, so the serum calcium rises and the serum phosphate falls. These activities increase renal activation of vitamin D, which enhances calcium absorption in the intestines, calcium liberation from bone, and calcium reabsorption in the kidneys.
When the serum ionized calcium concentration rises, PTH is suppressed, vitamin D is not activated, and calcitonin decreases intestinal calcium absorption and renal tubular calcium reabsorption and decreases osteoclastic activity in the bone.
Calcium Imbalances: Hypocalcemia
Etiology
Hypocalcemia (total Ca2+ <8.0 to 8.5 mg/dL [<2.0 mmol/L]; ionized Ca2+ <4.0 mg/dL [<1.0 mmol/L]) is associated with significant morbidity and mortality in critically ill infants and children. Hypocalcemia can result from inadequate calcium intake, reduced calcium absorption, or excessive calcium excretion (Box 12-4).
The serum ionized calcium concentration will fall if the serum albumin concentration or serum pH rise (e.g., during correction of acidosis or with development of alkalosis). Hypocalcemia can develop after administration of stored whole blood or packed cells preserved with citrate, phosphate, and dextran, because serum ionized calcium can precipitate with the phosphate anticoagulant and can be bound by the citrate. Hyperphosphatemia will also produce hypocalcemia because the phosphate precipitates with calcium.
Pathophysiology and Clinical Signs and Symptoms
When the serum ionized calcium falls, PTH secretion and vitamin D act to increase the serum calcium and lower the serum phosphate. Both PTH and vitamin D increase intestinal calcium absorption and renal calcium reabsorption and decrease renal phosphate reabsorption. Both contribute to the liberation of calcium and phosphate from bone (osteoclastic activity).
Signs and symptoms of hypocalcemia result from increased neuromuscular excitability and can include tingling, muscle cramps, lethargy, carpal-pedal spasm, seizures, and prolonged QT interval on ECG. A classic sign of hypocalcemia is Chvostek's sign, which is elicited by tapping on the facial nerve at the temple. A positive sign is a twitch of the lip or facial muscles near the nose. Trosseau's sign is the development of carpal pedal spasm after an extremity artery is occluded for 3 minutes. Severe hypocalcemia can produce muscle tetany.
Management
Management of hypocalcemia includes correction of the cause, administration of calcium supplements as needed, and monitoring for cardiac, neuromuscular, and neurologic dysfunction. Any concurrent conditions (e.g., hyperphosphatemia, hypomagnesemia, respiratory alkalosis) must be identified and treated as indicated.
The healthcare team should immediately treat any acute episode of hypocalcemia in children at risk for impending cardiovascular or neurologic failure. Calcium chloride is the calcium supplement of choice for infants and children, because it provides greater bioavailability of calcium.11,16a An IV dose of 20 mg/kg of 10% calcium chloride provides 5.4 mg/kg of elemental calcium. Calcium gluconate can be used in neonates (IV dose of 60-100 mg/kg of 10% calcium gluconate provides approximately 5.4-9 mg/kg). Administer IV calcium by slow push or infusion and monitor for arrhythmias. Rapid administration of calcium salts (faster than 100 mg/min) is not recommended because it may produce bradycardia and asystole.24,32
Calcium Imbalances: Hypercalcemia
Etiology
Hypercalcemia (total serum calcium >11-12 mg/dL [>2.75 mmol/L]) is an excess of calcium in the extracellular (including vascular) compartment. A serum calcium concentration greater than 15 mg/dL can be life threatening. Although hypercalcemia is not common, it may be seen in critically ill infants and children with hyponatremia, hyperkalemia, resolution of chronic renal failure, and prolonged immobility. Children with acute leukemias or a large tumor burden can also develop clinically significant hypercalcemia. Hemoconcentration can cause pseudohypercalcemia in hypovolemic patients. In addition, excessive calcium administration to treat hypocalcemia can cause iatrogenic hypercalcemia.
Pathophysiology and Clinical Signs and Symptoms
Hypercalcemia develops when an excessive amount of calcium moves from the bones and intestines into the ECF, overwhelming the regulatory hormones (vitamin D and PTH) and renal excretory systems, and if the function of either of these systems is compromised. Both serum albumin (protein) and pH can affect the serum ionized calcium concentration. An increase in serum protein concentration will increase total serum calcium concentration, but will reduce the ionized calcium concentration because more calcium is bound to protein. A fall in serum pH (acidosis) will decrease serum binding of calcium, so will increase ionized calcium.
Hypercalcemia produces a reciprocal fall in serum phosphate and can produce complications similar to hyperparathyroidism, including renal stones and osteoporosis. Severe hypercalcemia can produce a polyuria-polydipsia syndrome with dehydration. If the polyuria produces dehydration, renal excretion of calcium is reduced, exacerbating the hypercalcemia.
Hypercalcemia decreases excitability of nerve and muscle cells and can cause neuromuscular pain and tingling. Symptoms are often vague and may not be significant until the serum calcium concentration exceeds 12 mg/dL.
Management
Management of hypercalcemia includes identifying the underlying cause, reducing the concentration of calcium in the ECF, and managing clinical manifestations. In patients with known hypercalcemia or in those at risk for its development, it is essential to closely monitor neuromuscular and cardiac function.
A serum calcium concentration greater than 15 mg/dL can be life threatening and requires immediate treatment. Treatment is typically achieved through administration of IV fluids to expand the ECF and loop diuretics to enhance calcium excretion. Thiazide diuretics are contraindicated because they limit calcium excretion.
With life-threatening hypercalcemia, aggressive therapy is needed to reduce the serum calcium. Drugs are typically administered to reduce the serum calcium concentration over several days: biphosphonate inhibits bone reabsorption, calcitonin inhibits calcium reabsorption from bone, mithracin reduces osteoclast activity, and gallium nitrate interferes with osteoclast function (for more information, see Table 15-2).4 Administration of a biphosphate such as pamidronate (1 mg/kg) may be indicated in severe hypercalcemia. It can cause mild to moderate hypophosphatemia, hypomagnesemia, and transient hypocalcemia at 2 to 10 days after administration9; therefore, it will be important to monitor these electrolytes.
Magnesium Homeostasis
Magnesium (Mg2+) is the second most abundant cation inside cells; less than 1% of total magnesium is located in the extracellular (including intravascular) compartment. The normal serum magnesium concentration ranges from 1.5 to 2.5 mEq/L.
The three primary roles of magnesium are enzyme and biochemical activation, mediation of skeletal muscle tension, and inhibition of electrical activity at the neuromuscular junction. Magnesium plays an essential role in the metabolism of adenosine triphosphate (ATP), the source of cellular energy.
Magnesium is absorbed in the gastrointestinal tract (absorption varies directly with intake) and eliminated or reabsorbed by the kidney as needed. Calcitriol and PTH enhance magnesium intestinal absorption and renal reabsorption. Renal magnesium reabsorption appears to vary directly with the GFR; therefore, renal failure can produce hypomagnesemia. Hypomagnesemia is often associated with hyponatremia, hypokalemia, hypocalcemia, and hyperphosphatemia (see Hypomagnesemia).
Magnesium Imbalances: Hypomagnesemia
Etiology
Hypomagnesemia (serum magnesium <1.3 mg/dL [0.65 mmol/L]) is common in hospitalized patients, especially those with chronic illness. Hypomagnesemia results from decreased intestinal magnesium absorption or renal failure with increased renal magnesium losses. Diuretics and DKA with osmotic diuresis can produce hypomagnesemia.
Pathophysiology and Clinical Signs and Symptoms
Decreased intestinal absorption of magnesium may be intrinsic or induced by medications (e.g., laxatives) or disease.30 Medical conditions associated with decreased absorption include pancreatitis, severe or chronic diarrhea, prolonged vomiting, malabsorption syndromes, and intestinal and biliary fistulas. Prolonged gastric suctioning can reduce serum magnesium.
Increased renal excretion of magnesium can also be caused by medications such as diuretics (especially loop diuretics), aminoglycosides, amphotericin B, cisplatin, and cyclosporine. Medical conditions that cause rapid diuresis (e.g., DKA; hyperosmolar, hyperglycemic, or nonketotic coma) can also cause an increase in magnesium excretion.
Hypomagnesemia can cause lethal ventricular arrhythmias, including torsades de points and ventricular fibrillation. Because magnesium is essential to ATP metabolism, hypomagnesemia can damage the sodium-potassium pump, which depends on ATP to function properly.
Hypomagnesemia can be associated with additional electrolyte imbalances and with complications of the primary disease (e.g., renal failure). Hypomagnesemia causes an extracellular potassium shift that may transiently increase serum potassium. However, hypomagnesemia also causes increased urinary losses of sodium, potassium, phosphate, and hydrogen; therefore, it typically causes deficiency of these electrolytes. Hypomagnesemia can also produce hypocalcemia and hyperphosphatemia through impairment of PTH synthesis or secretion. Signs of hypomagnesemia are similar to signs of hypocalcemia, including possible tingling, muscle cramps, Chvostek's sign, tetany, and seizures (see under Hypocalcemia).
Management
If hypomagnesemia produces ventricular arrhythmias, cardiopulmonary resuscitation is needed (see Chapter 6) with bolus magnesium administration.24 Acute hypomagnesemia in children at risk for impending cardiovascular or neurologic failure is treated immediately with IV administration of magnesium sulfate (25-50 mg/kg infusion over 10-20 minutes or longer).24 Monitor for arrhythmias and hemodynamic instability during administration of magnesium supplements.30
Additional critical care management of an acute episode of hypomagnesemia includes correction of the cause and administration of other electrolyte supplements as needed. Treatment of hyponatremia, hypokalemia, and hypocalcemia is often necessary (see sections on Hyponatremia, Hypokalemia, and Hypocalcemia in this chapter for more information).
Monitor cardiac, muscular, and neurologic function throughout therapy. Although altered neuromuscular excitability is the most common feature of hypomagnesemia, patients can develop respiratory muscle depression and hypoventilation, requiring mechanical ventilation.
Magnesium Imbalance: Hypermagnesemia
Etiology
Hypermagnesemia (serum magnesium >2.5 mg/dL [1.25 mmol/L]) is far less common than hypomagnesemia. Hypermagnesemia can result from decreased renal excretion of potassium or, less commonly, an increase in magnesium intake through the intestine.
Pathophysiology, Clinical Signs, and Symptoms
Hypermagnesemia usually results from decreased renal excretion of magnesium, most commonly caused by chronic renal failure. Increased magnesium load and intestinal absorption may complicate the use of magnesium-containing laxatives or antacids.
Clinical signs and symptoms are associated with decreased neuromuscular and cardiovascular function. These signs and symptoms can include weakness, neurologic or respiratory depression, bradycardia, and hypotension.
Management
Patients at risk for hypermagnesemia should be monitored closely, because severe hypermagnesemia can lead to coma or cardiac arrest.27 Management of the pediatric patient with hypermagnesemia includes identification and correction of the cause and administration of calcium salts and IV fluids. Calcium salts antagonize magnesium and can reverse cardiac complications.
If renal function is normal, administration of IV fluids will facilitate renal excretion of magnesium. Dialysis may be indicated, particularly for children with renal failure.
Dehydration and hypovolemia
Dehydration occurs when the loss of all fluids and electrolytes exceeds intake. Hypovolemia is intravascular volume depletion, and can cause circulatory collapse.
Etiology
Dehydration with resulting hypovolemia is common in critically ill infants and children. Dehydration can result from excessive loss of fluids and electrolytes (e.g., diarrhea or vomiting), shifts of fluids and electrolytes into nonaccessible third spaces (e.g., burns or after abdominal surgery), and decreased intake of fluid and electrolytes (e.g., impaired thirst mechanism, dysphagia, or prolonged NPO status with inadequate IV therapy).
Gastrointestinal fluid loss from diarrhea is the most common cause of dehydration in infants and children. Increased insensible fluid losses can also contribute to dehydration.
In the critically ill child, “third spacing” is a common cause of intravascular volume loss.31 “Third spacing” is a shift of fluid from the vascular space to a space that is neither intravascular nor intracellular. The third space may be interstitial (e.g., with septic shock), on the surface of a burn, or even into the bowel lumen. With third spacing of fluid, a significant volume of fluid is unavailable to the circulation to support cardiac output and systemic perfusion. Third spacing of fluid can develop in conditions such as ascites, pancreatitis, burns, peritonitis, sepsis, and intestinal obstruction. Such third-spacing results in inadequate intravascular volume that can compromise systemic perfusion.
Pathophysiology
Dehydration is classified by severity and by its effect on serum sodium concentration. Hyponatremic dehydration (serum Na+ <130 mEq/L) occurs when there is a relatively greater loss of sodium than water, so the serum sodium concentration falls. This effect is often seen when gastrointestinal fluid losses are replaced with water or other hypotonic solution (e.g., 5% dextrose and water).22 The resulting hyponatremia creates an osmolality gradient between the extracellular (including vascular) and intracellular compartments, so that water shifts from the vascular and interstitial spaces to the intracellular compartment. This water shift increases the severity of the clinical signs of (intravascular) volume depletion at any given volume deficit.
Hypernatremic dehydration (serum Na+ >150 mEq/L) develops when there is a relatively greater loss of water than sodium (e.g., untreated DI). The resulting hypernatremia increases the extracellular osmolality, so that water shifts from the cellular to the extracellular compartment (i.e., intravascular and interstitial spaces). This free water shift decreases the severity of the clinical signs of volume depletion that will be present at any given volume deficit.
Clinical Signs and Symptoms
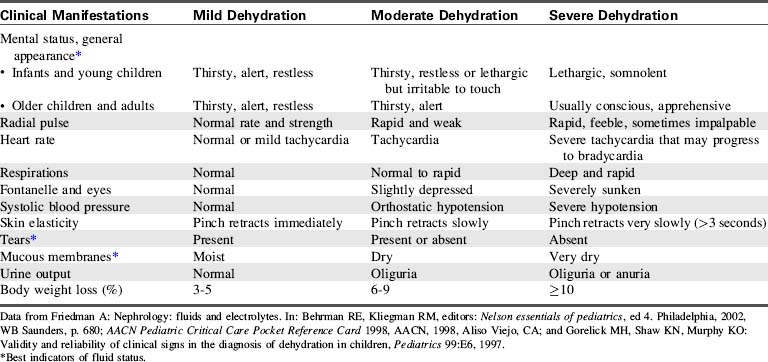
The clinical manifestations of dehydration will vary based on the severity of the fluid deficit and the serum sodium concentration. Table 12-5 shows a comparison of the clinical manifestations of mild, moderate and severe dehydration.
Management
The severity of a child's fluid volume deficit is estimated on the basis of weight loss, clinical manifestations and diagnostic studies. If a weight before illness is available, 1 kg of weight loss is equivalent to 1000 mL (1 L) of fluid loss.
If signs of shock are present (i.e., signs of poor peripheral perfusion or hypotension), initial management focuses on restoring intravascular volume to treat shock. Typically, 20 mL/kg IV boluses of isotonic crystalloid are administered until signs of shock are corrected. Infants or children with a severe fluid volume deficit may require resuscitation with 60 mL/kg or more of isotonic crystalloid.11
During volume resuscitation, providers should closely monitor signs of systemic perfusion (including mental status, skin perfusion and urine output), heart rate and blood pressure, to evaluate response to therapy. The fluid bolus administration is repeated, as needed. If volume resuscitation is adequate, the blood pressure and signs of systemic perfusion and blood pressure should improve and the heart rate should decrease toward normal; if the child fails to improve, additional boluses are needed or there may be other causes of the child's shock. See Chapter 6 for further details of the management of hypovolemic shock.
Once initial fluid resuscitation is complete, ongoing management includes estimation and replacement of water and electrolyte deficits. In isotonatremic or hyponatremic dehydration, the fluid and electrolyte deficit is typically replaced over a period of 24 to 36 hours to restore intravascular volume within a short period of time while preventing overexpansion of the ECF.10 In the presence of hyponatremic dehydration, the need for sodium replacement should be carefully evaluated.
In hypernatremic dehydration, replacement of fluid and electrolyte deficit is typically accomplished more slowly, over a period of 48 to 72 hours. The goal is to prevent rapid decreases in the serum sodium and osmolality during rehydration because such decreases can produce an intracellular water shift and neurologic complications. Replacement fluids to treat the fluid deficit are administered in addition to routine maintenance fluids (see Table 12-2) and replacement of any ongoing fluid losses (e.g., emesis or diarrhea).
Guidelines for parenteral fluid therapy
Parenteral fluid therapy is ubiquitous in pediatric critical care. See Table 12-6 for a comparison of common parenteral fluid solutions.
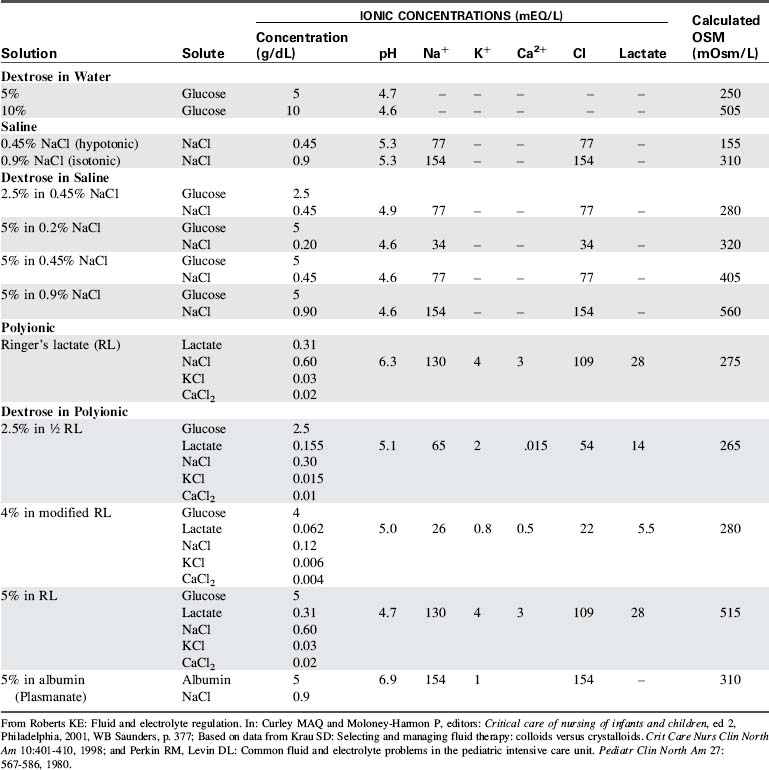
IV maintenance fluids are administered to provide daily free water and electrolyte requirements in a fasting patient. Fluid administration rate for each patient begins with an estimation of maintenance fluid requirements based on the formula developed by Holliday and Segar in 1957.13 These estimated requirements are then tailored to meet the needs of the patient.
For many years, hypotonic crystalloids (e.g., 5% dextrose with 0.2% sodium chloride) were routinely used for maintenance and replacement fluids for critically ill infants and children, based on the assumption that critically ill patients were likely to have a tendency to retain sodium and water. However, after reports of fatal hyponatremia in hospitalized children,1,2,21 a systematic review of the literature by Choong et al.5 estimated that the odds of developing hyponatremia after administration of hypotonic solutions were 17-fold higher than with administration of isotonic solutions. In addition, the administration of isotonic solutions was not associated with hypernatremia; in fact, some patients receiving isotonic fluids still developed hyponatremia.5
Currently, there is insufficient evidence to identify use of a single IV fluid (e.g., hypotonic or isotonic) as the standard of care for pediatric maintenance therapy. Until clinical trials compare the safety and efficacy of different IV fluid regimens, practitioners must continue to individualize IV fluid selection and administration rate for each patient.3,5 Providers should monitor serum electrolytes and clinical status during parenteral fluid therapy to prevent or rapidly detect and treat any imbalances that develop.
Specific diseases
Syndrome of Inappropriate Antidiuretic Hormone
Etiology
SIADH is characterized by ADH secretion in the absence of a physiologic stimulus. Patients with SIADH demonstrate low serum osmolality, hyponatremia, and hypervolemia. Causes of SIADH include central nervous system injury (e.g., surgery, tumor, traumatic brain injury) or infection, disease or damage to the pituitary stalk or hypothalamus, holoprosencephaly, spinal cord injury or surgery, chemotherapy, pulmonary disease, and liver disease.34 The critically ill patient with any of these conditions requires close monitoring for the development of SIADH.
Pathophysiology
ADH secretion results in increased permeability of the renal collecting ducts and distal tubules to water, resulting in increased water reabsorption, increased intravascular volume, and decreased urine volume. As a result, patients with SIADH develop a state of hypervolemia with dilutional hyponatremia (i.e., the dilutional effect of increased intravascular water).
Clinical Signs and Symptoms
Clinical manifestations of SIADH include adequate circulating volume, signs of hyponatremia, and decreased serum osmolality discussed in the second section of this chapter (see Hyponatremia). Urine volume is low (output typically <0.5 mL/kg per hour), with inappropriately high urine osmolality.
Laboratory studies consistent with SIADH include a low serum sodium (typically <130 mEq/L) and osmolality (<275 mOsm/L) with high urine sodium, specific gravity, and osmolality.
Management
Management of SIADH is targeted at the prevention of complications associated with hyponatremia. Early detection of neurologic deterioration is critical; therefore, frequent neurologic assessments are needed. If neurologic complications develop, including a change in mental status or seizure activity, immediate treatment includes administration of hypertonic saline (e.g., 2-4 mL/kg of 3% saline should raise serum sodium approximately 1 to 2 mEq/L) and loop diuretics (e.g., furosemide).34 These therapies should raise the serum sodium sufficiently to slow the intracellular water shift.
Treatment of SIADH includes restriction of free water intake (to approximately half or two-thirds of estimated maintenance fluid requirements) and close monitoring of neurologic function, fluid intake and output, urine specific gravity, and serum sodium.
Cerebral Salt Wasting
Etiology
Cerebral salt wasting (CSW) is caused by increased circulating levels of ANP with resulting natriuresis and contraction of intravascular volume, including potential hypovolemia. Causes of CSW are the same as those causing SIADH (see sections, Specific Diseases and Syndrome of Inappropriate Antidiuretic Hormone). When CSW is associated with a head injury, it typically develops 2 to 7 days after the injury. CSW can also complicate congestive heart failure, Cushing's syndrome, DKA, and hyperaldosteronism.33
Pathophysiology
Intracranial disease or injury and complications of other disease are thought to alter neurologic secretion of ANP and other natriuretic peptides.25 Increased circulating levels of ANP lead to increased excretion of a large amount of sodium in a high volume of urine. Like SIADH, CSW produces hyponatremia with a low serum osmolality and a high urine sodium and urine osmolality. However, because ANP and other natriuretic peptides produce a high urine volume, the patient also develops mild to moderate dehydration.34
Clinical Signs and Symptoms
Clinical manifestations of CSW include the signs and symptoms of hyponatremia (see “Hyponatremia” earlier in chapter) and those of mild to moderate dehydration (see Table 12-5). Laboratory studies confirm hyponatremia (serum Na+ <130 mEq/L) and increased urinary sodium (urine Na+ >80 mEq/L). Although not routinely monitored, serum levels of ANP are increased.33
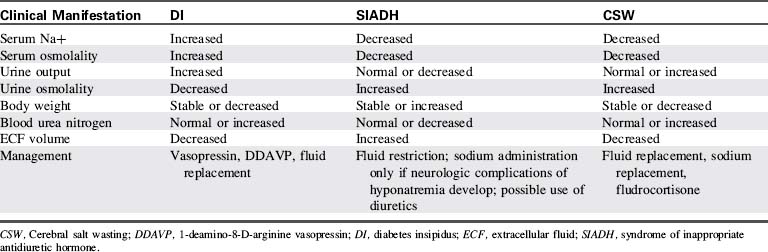
Management
Because the priorities of management differ, it is important to distinguish CSW from SIADH (Table 12-7).14,33 Treatment of CSW includes sodium replacement with oral salts or hypertonic saline, volume replacement with isotonic crystalloids, and vigilant monitoring for and prompt treatment of adverse effects of hyponatremia and hypovolemia.25 Mineralocorticoid therapy (fludrocortisone) can enhance sodium reabsorption and expand intravascular fluid volume in patients with CSW.29
Diabetes Insipidus
Etiology
DI is caused by a deficiency of ADH secretion (neurogenic or central DI) or an insensitivity of renal receptors to ADH (nephrogenic DI). Neurogenic DI is caused most commonly by lesions of the central nervous system (pituitary tumors, Langerhans cell histiocytosis, germinoma, craniopharyngioma, suprasellar tumors) or the resection of these lesions. DI also occurs as a complication of brain death from severe traumatic brain injury. Inherited mutations in the vasopressin gene are uncommon causes of central DI without associated central nervous system pathology.
Nephrogenic DI can be hereditary or acquired. The renal ADH receptor is carried on the X chromosome, resulting in a male predominance of inherited (X-linked) nephrogenic DI. DI can complicate drug administration or damage to the renal tubules. Amphotericin B, loop diuretics, and some anesthetics have been reported to cause reversible DI. Irreversible nephrogenic DI results from a loss of ADH sensitivity secondary to renal disease or an insult that interferes with the kidneys' ability to concentrate water.
Pathophysiology
A deficit of ADH or lack of renal response to ADH results in decreased reabsorption of water by the renal distal tubules, so a significant volume of water is lost in the urine. As a result of this free water loss, unless fluid replacement is provided, patients can rapidly develop significant hypovolemia and hypernatremia (concentration effect).
Clinical Signs and Symptoms
The classic clinical manifestations of DI include polyuria, hypernatremia, and intense thirst. If not recognized early, the infant or child with DI can rapidly develop hypovolemic shock. In the chronic state, the excessive water intake associated with DI leads to anorexia, weight loss, and a catabolic state.
Patients at risk should be monitored closely for the clinical manifestations of hypovolemia and hypernatremia. Laboratory studies consistent with DI (see Table 12-7) include elevated serum sodium (Na+ >150 mEq/L) and osmolality (>295 mOsm/L) and low urine osmolality (<100-200 mOsm/L).33
Management
Critical care management of DI includes administration of exogenous vasopressin (aqueous vasopressin [5-10 units subcutaneously] or lysine vasopressin [2-4 units IV]) or the vasopressin analog, 1-Deamino-8-d-Arginine Vasopressin (DDAVP[5-20 mcg intranasally every 12-24 hours]), careful fluid replacement, close monitoring of fluid intake and output, and close monitoring of serum sodium and other electrolytes.33,34 While urine volume is high, it is also important to monitor for the signs and symptoms of hypovolemic shock and support electrolyte balance.
When urine output is high, urine output is totaled typically every 10 or 15 minutes. In the next equal time interval (i.e., the next 10 or 15 minutes), the volume lost in the urine is replaced milliliter for milliliter (typically alternating 5% dextrose and water with 5% dextrose and 0.2% sodium chloride). Replacement fluid is added to maintenance fluid requirements and must also include replacement of any additional sources of fluid loss (e.g., gastric drainage).
Diabetic Ketoacidosis
Etiology
DKA is a life-threatening complication of diabetes mellitus that includes the combination of severe hyperglycemia and ketoacidosis. Approximately 40% of children with diabetes mellitus present with DKA as their first clinical manifestation of diabetes mellitus.25
Type I diabetes mellitus in children results from a loss of insulin-secreting pancreatic beta cells. The most common form of type I diabetes is triggered by a combination of genetic susceptibility and environmental factors, including some viruses, that produce autoimmune destruction of beta cells.15
Pathophysiology
DKA results from a severe deficiency of insulin that impairs glucose uptake into the cell. To correct the ensuing energy deficit, there is an increase in counter-regulatory hormones such as glucagon, catecholamines, cortisol, and growth hormone in an attempt to produce more glucose. As a result, the serum glucose concentration is extremely high, but glucose uptake by the cells continues to be impaired. A state of intracellular energy debt ensues, resulting in derangements in the metabolism of fat, protein, and carbohydrates. Gluconeogenesis occurs, with the breakdown of proteins and lipids to make amino acids and fatty acids available as energy substrates.
Ketoacids—acetoacetic acid and beta-hydroxybutyric acid—are released from adipocytes in instances of prolonged insulin deficiency. The presence of high levels of these circulating ketoacids results in ketoacidosis.34 Children with DKA always experience acidosis and hyperosmolar dehydration with glucosuria and osmotic diuresis.
Deficits of sodium, potassium, and phosphate are always present. Although there are urinary losses of these electrolytes, the presence of severe dehydration and hemoconcentration with acidosis (producing an extracellular potassium shift) may initially mask these deficiencies. As a result, the child may have normal or even elevated serum sodium, potassium, and phosphate concentrations despite total body deficits of these electrolytes. After treatment and rehydration, the serum electrolyte concentrations fall, and hyponatremia and hypokalemia develop. Hypokalemia can contribute to cardiac arrhythmias and death on rare occasions if it is not corrected quickly (see section, Clinical Signs and Symptoms).
Finally, dehydration, acidosis, and osmotic water shifts into brain cells (see Box 12-1) can contribute to life-threatening cerebral edema or intracranial thrombotic events.18 A major difference between children and adults with DKA is the susceptibility of the young to potentially fatal episodes of cerebral edema. Proposed mechanisms of cerebral edema include: accumulation of intracellular idiogenic osmoles (see Box 12-2); vasopressin and atrial natriuretic factor producing water retention, natriuresis, and hyponatremia; disruption in cell membrane ion exchange processes, causing intracellular ion movement and cell swelling; hypoxia and ischemia; ketones and acidosis contributing to the inflammatory cascade; and abnormalities in water (aquaporin) channels in the glial cells of the brain.18
Symptomatic cerebral edema in children with DKA can cause death or neurologic devastation.20 Additional intracranial pathologic conditions—including bleeding, thrombosis, infarction or emboli—can cause altered mental status in children with DKA.18
Clinical Signs and Symptoms
Children with DKA have severe hyperglycemia (serum glucose ≥180 mg/dL or >10 mmol/L) and ketoacidosis. Additional signs and symptoms are related to the severity of the resulting hyperosmolality, volume depletion, and acidosis. Children with DKA generally present with a 5% to 10% fluid deficit7 caused by the massive water losses secondary to glucosuria.
Acidosis results from the extremely large quantity of ketoacids in the blood. Acetoacetic acid may be reduced to beta-hydroxybutyric acid or decarboxylated to acetone. This ketonemia produces the classic “fruity breath” in children with DKA. The resulting urinary excretion of these ketone bodies, ketonuria, causes further osmotic loss of fluids and electrolytes. In the presence of acidosis, the body develops compensatory hyperpnea or Kussmaul breathing, a classic sign of DKA.
As noted previously, the serum sodium, potassium, and phosphate concentrations may be low, normal, or high but deficits of these electrolytes are present. The serum sodium should be interpreted in light of the serum glucose concentration (each 100 mg/dL rise in serum glucose above 180 mg/dL is likely to depress the serum sodium 1.6 mEq/L below 135 mEq/L). The serum potassium should be evaluated in the context of the serum pH: acidosis causes an extracellular shift in potassium, so the serum potassium rises. After treatment and rehydration, serum electrolyte concentrations fall; therefore, hyponatremia and hypokalemia can develop with attendant complications (see the Chapter 12 Supplement on the Evolve Website for a case study that demonstrates typical serum sodium and glucose values in a patient with DKA).
Dehydration, acidosis and osmotic fluid shifts in the brain can contribute to life-threatening cerebral edema or intracranial thrombotic events. These central nervous system complications can produce decreased responsiveness, posturing, abnormal respiratory patterns, and signs of increased intracranial pressure and cerebral herniation.18 Table 12-8 shows a summary of the clinical manifestations of DKA and their underlying mechanisms.
Table 12-8 Clinical Manifestations of Diabetic Ketoacidosis
| Signs and Symptoms | Underlying Mechanisms |
| Hyperglycemia, dehydration, cardiovascular collapse | Osmotic diuresis secondary to hyperglycemia |
| Acidosis | Accumulation of ketoacids and lactic acid in serum from lipolysis, resulting in increased H+ concentration in serum |
| Electrolyte imbalance: sodium | Total body hyponatremia because of passive loss of electrolytes as a result of osmotic diuresis; however, serum sodium may be high as a result of hemoconcentration |
| Electrolyte imbalance: potassium | In acidosis, potassium shifts from ICF to ECF; therefore, initially serum potassium may be normal or even high, but will decrease as a result of osmotic diuresis and correction of acidosis |
| Cardiac arrhythmia | Hypokalemia or hyperkalemia |
| Ketonuria | Serum ketone levels rise above the renal threshold and are spilled in the urine |
| Hyperpnea | Compensatory mechanism; effort to blow off excess CO2 and thereby correct the degree of acidosis |
| Mental status changes, cerebral edema | Possibly related to rate of correction of hyperglycemia, level of acidosis, fluid shifts |
ECF, Extracellular fluid; ICF, intracellular fluid.
From Trimarchi T: Endocrine critical care problems. In: Curley MAQ, Moloney-Harmon PA, editors: Critical care nursing of infants and children, ed 2, Philadelphia, 2001, WB Saunders, p. 817.
Management
Priorities of management of DKA in order of importance are: assessment and support of neurologic function (including support of patent airway and effective ventilation), assessment and support of circulation (including volume resuscitation), insulin therapy, and restoration and maintenance of electrolyte, glucose and acid-base balance (Box 12-5). Consideration is also given to confounding factors, such as infection, injury or other patient problems.
Box 12-5 Priorities of Management of Diabetic Ketoacidosis in Order of Importance*
1. Assess and support neurologic function, including support of patent airway and effective ventilation
2. Assess and stabilize circulation (including fluid resuscitation)
4. Restore and maintain electrolyte, glucose and acid-base balance
5. Identify confounding factors (infection, drugs, injury, other diagnoses)
* Perform serial assessments throughout care and immediately notify provider of any deterioration.
Although very few children present with neurologic compromise (primarily cerebral edema) this can be a very poor prognostic indicator. Most who present with this finding perish and those who survive are often severely neurologically compromised with little or no independent function.20
If the child's level of consciousness deteriorates, cerebral edema may be present, and urgent intervention is needed (see diagnostic criteria for cerebral edema21a in Box 12-6). If clinical signs of cerebral edema develop, immediate treatment with IV mannitol (0.2-1.0 g/kg over 30-60 minutes) is indicated. Hypertonic saline (e.g., 3% sodium chloride, 10 mL/kg, administered IV over 30 minutes) may be used as an alternative to mannitol. If the child's ability to protect the airway or spontaneous ventilation deteriorates, intubation and mechanical ventilation are indicated.
Box 12-6 Bedside Neurologic Evaluation of Children with Diabetic Ketoacidosis
Diagnostic Criteria for Possible Cerebral Edema*
Minor Criteria†
From Muir AB, et al: Cerebral edema in childhood diabetic ketoacidosis. Diabetes Care 24:1541-1546, 2004.
The child's volume deficit is initially treated with the administration of normal saline or lactated Ringer's. The quantity of fluid administered is determined by the patient's clinical severity; if shock is present, bolus administration of isotonic crystalloids is needed. For less significant volume deficit, typically 10 to 20 mL/kg is administered over 1 to 2 hours and repeated as needed.18 Replacement of the total fluid deficit is planned over approximately 48 hours or longer. Isotonic crystalloids are used for initial fluid replacement; the sodium content may then be reduced to 0.45% sodium chloride with potassium added as the child's condition stabilizes.
Replacement of insulin is generally accomplished by continuous IV infusion. An infusion of regular insulin (0.05 to 0.1 unit/kg per hour) is titrated to gradually reduce the serum glucose at the rate of approximately 50 to 100 mg/dL per hour. Simultaneous infusion of 10% glucose IV can be titrated to control the maximum rate of decline in the serum glucose to no more than 100 mg/dL per hour. Glucose infusion is preferable to slowing the insulin infusion, because reducing the insulin dose can worsen the patient's acidosis.18
As noted previously, patients with DKA typically have deficits of water, sodium, potassium, and phosphate. Although serum electrolyte concentrations may be normal at the time of initial clinical presentation, with treatment hyponatremia, hypokalemia, and hypophosphatemia are likely to be present. Replacement fluids are selected to address these deficits. Some landmark studies suggest that phosphate replacement is of no clinical value.8,38 There is no evidence that the addition of sodium bicarbonate to correct acidosis is of value, and it may contribute to hypokalemia and cerebral edema.18 To prevent a fall in serum osmolality when the serum glucose is reduced, the serum sodium concentration should rise approximately 1.6 mEq/L for every 100 mg/dL fall in serum glucose concentration.
Providers should look for evidence of confounding factors in a child with DKA. These factors include infection, illicit use of drugs or other medications, injury, or other intracranial pathologic finding. Most of these factors will aggravate acidosis and slow the recovery from DKA.
Box 12-7 contains a typical management plan for children with DKA. As a general rule, patients in DKA recover from acidosis within 24 hours after presentation.
Box 12-7 Management Plan for Children with Diabetic Ketoacidosis
1. First Priority: Perform repeat assessments of neurologic function, airway and ventilation
2. Second priority: Assess and stabilize circulation (including acute management of severe hyperkalemia associated with acidosis).
Use of an infusion of regular insulin without a bolus loading dose is recommended to allow for careful titration of intravenous fluids as serum glucose concentration begins to decrease. The infusion enables control of the rate of decrease and helps prevent iatrogenic hypoglycemia. A rapid decrease in serum glucose level is known to precipitate central pontine myelinolysis and may also be associated with development of global cerebral edema in patients with diabetic ketoacidosis (DKA).
4. Assess and maintain serum sodium concentration.
5. Treat potassium and phosphate imbalance.
 Treat severe hyperkalemia (>7 mEq/L and ECG changes) with calcium and consider sodium bicarbonate administration (see Table 12-4). The absence of ketones and serum glucose <200 mg/dL indicates readiness for transition to subcutaneous closing.
Treat severe hyperkalemia (>7 mEq/L and ECG changes) with calcium and consider sodium bicarbonate administration (see Table 12-4). The absence of ketones and serum glucose <200 mg/dL indicates readiness for transition to subcutaneous closing.7. Assess for infection (most frequent cause of DKA)
Modified from Trimarchi T: Endocrine problems in critically ill children: an overview. AACN Clin Issues 17:66-78, 2006.
Adrenal Insufficiency
Etiology
Adrenal insufficiency can be either primary or secondary and includes several conditions that result in a deficiency of glucocorticoids (cortisol) and mineralocorticoids (aldosterone). Adrenal insufficiency also results in decreased production and release of catecholamines.
Primary adrenocortical deficiency (Addison's disease) results from disease states that prevent the adrenal glands from producing cortisol or aldosterone. These diseases include: congenital adrenal hypoplasia, tuberculous adrenalitis, autoimmune adrenalitis, adrenoleukodystrophy, and adrenal hemorrhage. In addition, recessively inherited defects in the synthesis of cortisol and aldosterone constitute the congenital adrenal hyperplasia syndromes and are among the most common causes of primary adrenocortical insufficiency in neonates (1 in 16,000 births).
Secondary adrenocortical deficiency occurs as the result of interrupted communication in the hypothalamic-pituitary-adrenal axis. Secondary adrenal insufficiency is due to deficiencies in corticotrophin releasing hormone (CRH) from the hypothalamus or adrenocorticotropic hormone from the anterior pituitary.15 The most common cause of adrenal insufficiency in children is the abrupt cessation of administration of exogenous corticosteroids.34 Adrenal insufficiency should be considered in any critically ill child with persistent shock despite fluid resuscitation and vasopressor therapy (e.g., unresponsive or fluid-refractory septic shock).
Pathophysiology
With primary adrenal disease, there is frequently a deficiency of both aldosterone and glucocorticoids, whereas pituitary disease can lead to diminished adrenocorticotropic hormone secretion and an isolated deficiency of glucocorticoids only.
• Aldosterone deficiency leads to decreased renal reabsorption of sodium and water and increased reabsorption of potassium.
• Isolated glucocorticoid deficiency results in hypoglycemia, elevated levels of ADH (as in SIADH, producing hypervolemia and dilutional hyponatremia), and decreased secretion of and responsiveness to catecholamines. This condition in turn results in the development of myocardial depression, hypotension, and diminished arterial tone.
The combination of aldosterone and glucocorticoid deficiencies can cause severe hypotension. Isolated deficit of glucocorticoids in the presence of a significant stressor (e.g., sepsis) can also produce vasodilation and shock.
Clinical Signs and Symptoms
The initial presentation of acute adrenal insufficiency is often that of profound circulatory failure with the clinical manifestations of hypovolemic, distributive, and cardiogenic shock (see Chapter 6.) Children may also exhibit hyponatremia, hyperkalemia, and hypoglycemia and their corresponding clinical manifestations, as presented earlier in this chapter.
Management
Management of children with adrenal insufficiency is directed at preventing the complications associated with shock and hypoglycemia and correcting electrolyte imbalances. Emergent resuscitative measures include bolus fluid administration as needed and administration of vasoactive agents to increase heart rate, cardiac contractility, peripheral vascular resistance, and systemic perfusion.
Treatment for aldosterone deficiency and volume depletion includes judicious fluid resuscitation with an isotonic crystalloid (typically normal saline, possibly with 5% or 10% dextrose) to expand intravascular volume. Excessive fluid replacement can be harmful in instances of isolated glucocorticoid deficiency when SIADH is already present. If the child exhibits the clinical manifestations of hyperkalemia, urgent treatment with calcium, glucose plus insulin, and other strategies listed in Table 12-4 are needed.
Emergent replacement of glucocorticoids is accomplished through IV administration of stress doses of hydrocortisone (25-50 mg/m2 body surface area per day by IV continuous infusion or divided into 4-8 doses). Vigilant monitoring of fluid and electrolyte balance is a key component of the nursing care of the child with acute adrenal insufficiency.
Diagnostic tests
Diagnostic studies are a key component in identifying disruptions in fluid or electrolyte balance. Table 12-9 provides an overview of the most common diagnostic tests used to evaluate fluid balance. However, these diagnostic studies are just one piece of the puzzle when evaluating a child with a disruption in fluid or electrolyte balance. The laboratory results should be evaluated in light of the child's history and clinical presentation.
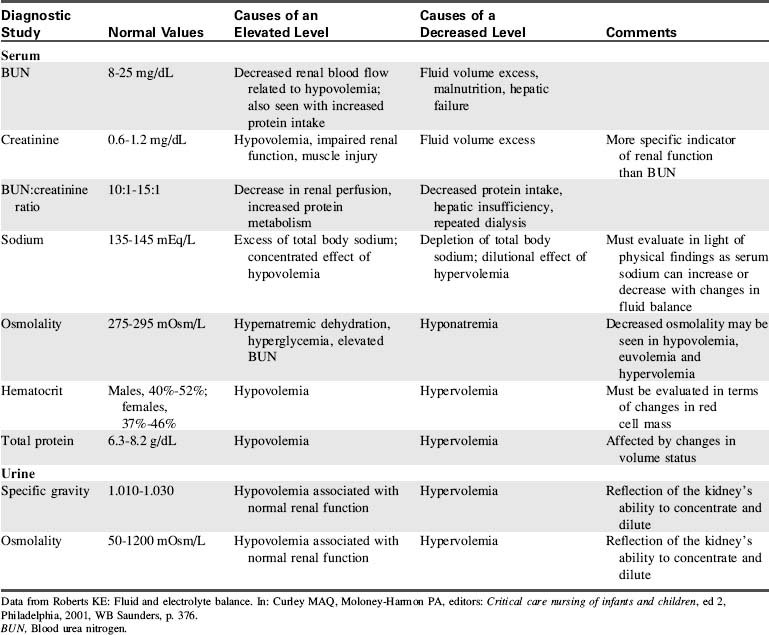
1 Arieff A.I., Ayus J.C., Fraser C.L. Hyponatraemia and death or permanent brain damage in healthy children. BMJ. 1992;304:1218-1222.
2 Armon K., et al. Hyponatremia and hypokalemia during intravenous fluid administration. Arch Dis Child. 2008;93:285-287.
3 Beck C.E. Hypotonic versus isotonic maintenance intravenous fluid therapy in hospitalized children: a systematic review. Clin Pediatr. 2007;46:764-770.
4 Brashers V.L., Jones R.E. Mechanisms of hormonal regulation. In McCance K.L., Huether S.E., editors: Pathophysiology: the biologic basis for disease in adults and children, ed 6, Philadelphia: Mosby-Elsevier, 2009.
5 Choong K., et al. Hypotonic versus isotonic saline in hospitalized children: a systematic review. Arch Dis Child. 2006;91:828-835.
6 Custer J.W., Rau R.E. The Harriet Lane handbook, ed 18. Philadelphia: Mosby-Elsevier; 2009.
7 Dunger D.B., et al. European Society for Paediatric Endocrinology/Lawson Wilkins Pediatric Endocrine Society consensus statement on diabetic ketoacidosis in children and adolescents. Pediatrics. 2004;113:e133-e140.
8 Fisher J.N., Kitabchi A.E. A randomized study of phosphate therapy in the treatment of diabetic ketoacidosis. J Clin Endocrinol Metab. 1983;57:177-180.
9 Elisaf M., Kalaitzidis R., Siamopoulos K.C. Multiple electrolyte abnormalities after pamidronate administration. Nephron. 1998;79:337-339.
10 Friedman A.L. Nephrology: fluid and electrolytes. In: Behrman R.E., Kliegman R.M., editors. Nelson essentials of pediatrics. ed 4. Philadelphia: WB Saunders; 2002:671-709.
11 Hazinski M.F., et al. Fluid therapy and medications for shock and cardiac arrest. In: PALS provider manual. Dallas: American Heart Association; 2002.
12 Hellerstein S. Fluids and electrolytes: clinical aspects. Pediatr Rev. 1993;14:103-115.
13 Holliday M.A., Segar W.E. The maintenance need for water in parenteral fluid therapy. Pediatrics. 1957;19:823-832.
14 Jimenez R., et al. Cerebral salt wasting syndrome in children with acute central nervous system injury. Ped Neuro. 2006;35:261-263.
15 Jones R.E., Brashers V.L., Huether S.E. Alterations of hormonal regulation. In McCance K.L., Huether S.E., editors: Pathophysiology: the biologic basis for disease in adults and children, ed 6, Philadelphia: Mosby-Elsevier, 2009.
16 Kamel K.S., Wei C. Controversial issues in the treatment of hyperkalemia. Nephrol Dial Transplant. 2003;18:2215-2218.
17 Lacy C.F., et al. Lexicomp's drug information handbook, ed 18. Hudson, OH: Lexicomp; 2009.
17a Kleinman ME, Chameides L, Schexnayder SM, et al. Part 14: pediatric advanced life support: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2010;122(18 Suppl 3):S876-908.
18 Levin D.L. Cerebral edema in diabetic ketoacidosis. Pediatr Crit Care Med. 2008;9:320-329.
19 Mahoney B.A., et al. Emergency interventions for hyperkalaemia. Cochrane Database Syst Rev. 2005. April 18 (2) CD003235
20 Marcin J.P., et alAmerican Academy of Pediatrics. The Pediatric Emergency Medicine Collaborative Research Committee: factors associated with adverse outcomes in children with diabetic ketoacidosis-related cerebral edema. J Pediatr. 2002;141:793-797.
21 Moritz M.L., Ayus J.C. Prevention of hospital-acquired hyponatremia: a case for using isotonic saline. Pediatrics. 2003;111:227-230.
21a Muir A.B., et al. Cerebral edema in childhood diabetic ketoacidosis. Diabetes Care. 2004;24:1541-1546.
22 Neville K.A., et al. Isotonic is better than hypotonic saline for intravenous rehydration of children with gastroenteritis: a prospective randomized study. Arch Dis Child. 2006;91:226-232.
23 Nyirenda MJ, et al: Clinical review: hyperkalemia, Br Med J 339:4114
24 Ralston M., et al. PALS provider manual. Dallas: American Heart Association; 2006.
25 Relvas M.S. Endocrine emergencies. In: Conway E.E., editor. Pediatric multiprofessional critical care review. Des Plaines, IL: Society of Critical Care Medicine; 2006:365-376.
26 Reynolds M., Padfield P.L., Seckl J.R. Disorders of sodium balance. Br Med J. 2006;332:702-705.
27 Roberts K.E. Fluid and electrolyte regulation. In Curley M.A.Q., Moloney-Harmon P., editors: Critical care nursing of infants and children, ed 2, Philadelphia: WB Saunders, 2001.
28 Schaefer T.J., Wolford R.W. Disorders of potassium. Emerg Med Clin North Am. 2005;23:723-747.
29 Springate J. Cerebral salt wasting. Available at: http://www.emedicine.com/ped/topic354.htm, 2008. Accessed July 4
30 Springate J.E., Kala G.K. Hypomagnesemia. Available at: http://emedicine.medscape.com/article/922142-overview, 2010. Accessed January 4
31 Stark J. A comprehensive analysis of the fluid and electrolytes system. Crit Care Nursing Clin North Am. 1998;10:471-475.
32 Styne D.M., Glaser N.S. Endocrinology. In: Behrman R.E., Kliegman R.M., editors. Nelson essentials of pediatrics. ed 4. Philadelphia: WB Saunders; 2002:711-766.
33 Trimarchi T. Endocrine critical care problems. In: Curley M.A.Q., Moloney-Harmon P.A., editors. Critical care nursing of infants and children. ed 2. Philadelphia: WB Saunders; 2001:805-819.
34 Trimarchi T. Endocrine problems in critically ill children: an overview. AACN Clin Issues. 2006;17:66-78.
35 Vellaichamy M. Hypernatremia. Available at: http://www.emedicine.com/ped/topic1082.htm, 2008. Accessed July 4
36 Vellaichamy M. Hyponatremia. Available at: http://www.emedicine.com/ped/topic1124.htm, 2008. Accessed July 4
37 Vlasselaers D., et al. Intensive insulin therapy for patients in paediatric intensive care: a prospective, randomised controlled study. Lancet. 2009;373:547-556.
38 Wilson H.K., et al. Phosphate therapy in diabetic ketoacidosis. Arch Intern Med. 1982;142:517-520.
* This formula does not reflect the influence of plasma proteins or administered osmotic agents such as mannitol. It may be inaccurate in the presence of severe hyperglycemia and hyperlipemia.