Pruritus and Dysesthesia
Definitions
• Pruritus: an unpleasant sensation of the skin that elicits a desire to scratch.
• Dysesthesia: an unpleasant, abnormal sensation that can be either spontaneous or evoked; abnormal, unpleasant sensations may include pain, pruritus (‘neuropathic itch’), tingling, burning, ‘pins and needles’.
Pruritus
• The most common skin-related symptom in dermatology; can have a profound negative impact on a patient's quality of life.
• Results from the activation of the sensory nervous system, involving four sequential levels: the peripheral nervous system → the dorsal root ganglia → the spinal cord → and the brain.
• There are multiple etiologies of pruritus, and it is often a major clinical challenge to diagnose the underlying etiology and to adequately treat.
Etiologies
• May arise secondary to a number of conditions:
– Dermatologic disorders (Table 4.1).
Table 4.1
Common dermatologic diseases with pruritus as a major symptom.
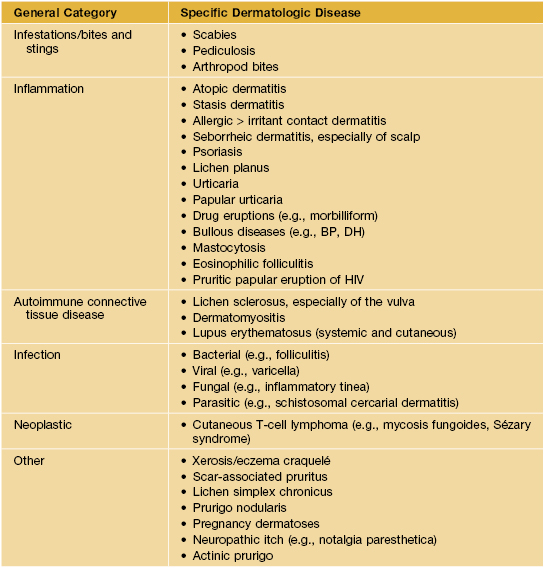
BP, bullous pemphigoid; DH, dermatitis herpetiformis.
– Allergic or hypersensitivity syndromes.
– Systemic diseases (10–25%) and malignancies (Table 4.2; Figs. 4.1 and 4.2).
Table 4.2
Approach to the patient with generalized pruritus and no obvious specific skin disease.
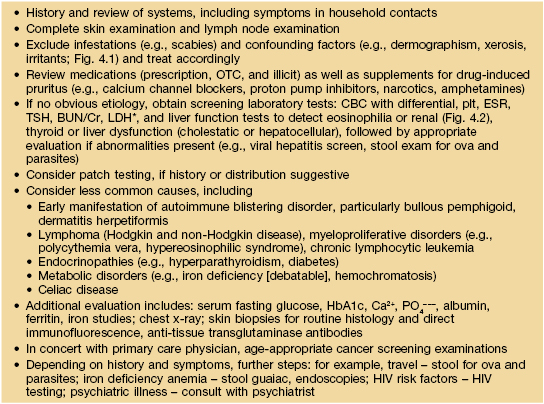
* LDH is often used in a manner similar to an ESR, especially in patients with lymphoma.
BUN, blood urea nitrogen; CBC, complete blood count; Cr, creatinine; ESR, erythrocyte sedimentation rate; HIV, human immunodeficiency virus; LDH, lactic dehydrogenase; OTC, over-the-counter; plt, platelets; TSH, thyroid-stimulating hormone.

Fig. 4.1 Extreme xerosis associated with pruritus in an HIV-infected patient. Courtesy, Elke Weisshaar, MD and Jeffrey D. Bernhard, MD.

Fig. 4.2 Xerosis and pruritus in a patient with chronic renal failure on hemodialysis. There are a few papules of acquired perforating dermatosis admixed with the scratch marks. Courtesy, Jean L. Bolognia, MD.
– Toxins associated with kidney or liver dysfunction.
– Neurologic disorders (see text below).
– Psychiatric conditions (see Chapter 5).
• May also be primary or idiopathic – that is, no readily apparent skin disease, underlying etiology, or associated condition.
• Most patients with pruritus due to an underlying dermatologic disorder present with characteristic or diagnostic skin lesions (e.g., dermatitis of the flexures in atopic dermatitis; see Table 4.1).
• In primary pruritus and secondary pruritus NOT due to an underlying dermatologic disorder, the lesions are usually nonspecific (e.g., linear excoriations [Fig. 4.3], prurigo simplex, prurigo nodularis [Fig. 4.4]).

Fig. 4.3 Linear excoriations on the leg. Although this patient had atopic dermatitis, similar lesions can be seen in patients with ‘primary’ or ‘idiopathic’ pruritus. Courtesy, Elke Weisshaar, MD and Jeffrey D. Bernhard, MD.

Fig. 4.4 Prurigo nodularis. Firm papulonodules on the extensor forearm due to repeated scratching and picking. Courtesy, Ronald P. Rapini, MD.
Diagnostic Pearls
• Patients with chronic, idiopathic pruritus need serial examinations because pruritus can antedate clinical manifestations of the underlying disorder (e.g., lymphoma) or with time, more specific lesions may appear (e.g., bullous pemphigoid).
• Sparing of the mid upper back, an area of patient-hand inaccessibility (‘butterfly sign’) (Fig. 4.5), is suggestive of pruritus NOT associated with a dermatologic disorder; note, however, this sign is not seen in those who use back scratchers or similar devices.
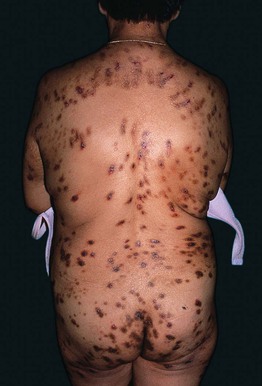
Fig. 4.5 Multiple lesions of prurigo nodularis. Note the sparing of the mid upper back (‘butterfly sign’).
• Aquagenic pruritus, provoked by cooling of the skin after emergence from a bath, is often idiopathic but may be a sign of polycythemia vera.
• Of note, some patients may have a combination of specific and nonspecific skin lesions and both may be due to an underlying systemic disorder (e.g., eosinophilic folliculitis associated with HIV infection/AIDS).
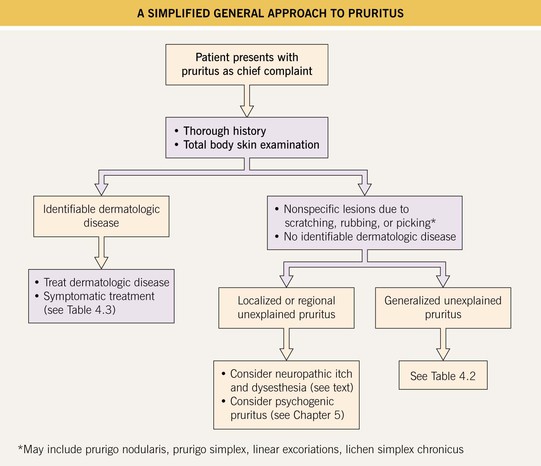
Approach to the Patient with Pruritus
• Identifying the underlying etiology of a patient's pruritus is important in determining the appropriate management.
• A simplified approach to the patient with pruritus is presented in Fig. 4.6.
Management of Pruritus
• General treatment measures for pruritus are outlined in Table 4.3.
Table 4.3
Treatment for pruritus/dysesthesia – general measures.
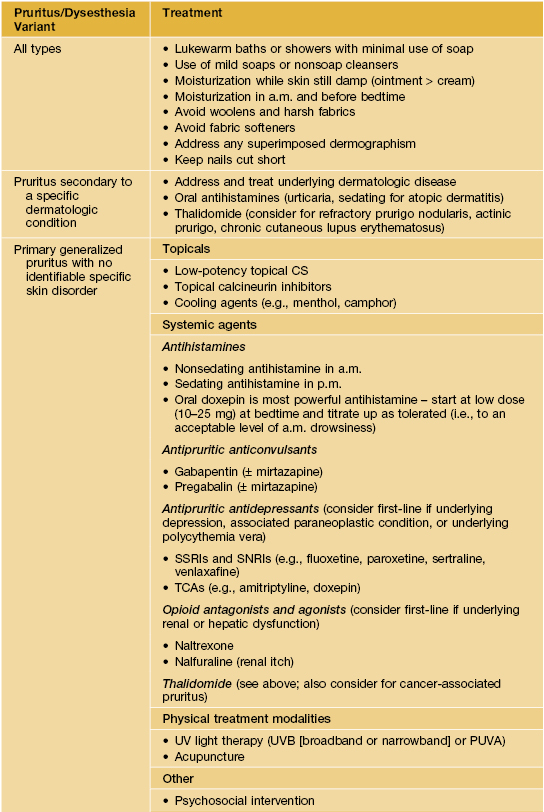
SNRIs, selective norepinephrine reuptake inhibitors; SSRIs, selective serotonin reuptake inhibitors; TCAs, tricyclic antidepressants.
Classic Clinical Findings from Chronic Pruritus
Lichen Simplex Chronicus (LSC)
• Skin-colored to pink or hyperpigmented plaques with exaggerated skin lines and a leathery appearance due to repeated, often habitual, scratching or rubbing (Fig. 4.7).

Fig. 4.7 Lichen simplex chronicus of the lateral neck. Note the increased skin markings. Use of topical corticosteroids can lead to a shiny appearance and a rim of hypopigmentation. Courtesy, Elke Weisshaar, MD and Jeffrey D. Bernhard, MD.
• Favors the posterior neck and occipital scalp (Fig. 4.8), anogenital region (Fig. 4.9), and ankles as well as the extensor surface of the forearms and shins.

Fig. 4.8 Lichen simplex chronicus of the posterior neck. The increased skin markings have been likened to the bark of a tree. Courtesy, Ronald P. Rapini, MD.

Fig. 4.9 Lichen simplex chronicus of the scrotum. Secondary pigmentary changes are seen more commonly in darkly pigmented skin. Courtesy, Louis A. Fragola, Jr., MD.
• LSC may be superimposed upon a specific cutaneous disorder, most commonly atopic dermatitis.
• In addition to symptomatic relief (e.g., topical anesthetics such as pramoxine), disruption of the itch–scratch cycle requires discussion of possible psychosocial issues (e.g., stress, depression, anxiety).
• Rx: potent topical CS, often under occlusion (e.g., hydrocolloid dressings), can be helpful.
• Other Rx: intralesional CS or use of an office-applied dressing (e.g., Unna boot) may be required.
Prurigo Nodularis
• Multiple, discrete, firm papulonodules with central scale-crust due to chronic and repetitive scratching and picking.
• Degree of pruritus can vary from moderate to intense.
• Lesions usually favor the extensor surfaces of the extremities (see Fig. 4.4), upper back, and buttocks, but they can be widespread in easily reachable areas (Fig. 4.10).

Fig. 4.10 Widespread prurigo nodularis. This patient had underlying atopic dermatitis. Courtesy, Elke Weisshaar, MD and Jeffrey D. Bernhard, MD.
• Disruption of the itch–scratch cycle requires symptomatic relief and discussion of psychosocial issues as in LSC (see above).
• Rx: depending on the number of lesions, varies from superpotent topical or intralesional CS to phototherapy (UVB [broadband or narrowband] or PUVA) and thalidomide.
• If no underlying reversible disorder is detected (see Table 4.2), prurigo nodularis can be difficult to treat.
Neurologic Etiologies of Pruritus and Dysesthesia
• The same neurological diseases that can cause neuropathic pain and dysesthesia can also cause neuropathic itch, with some differences (e.g., opioid pain relievers that help treat neuropathic pain may cause or worsen neuropathic itch).
Neuropathic Itch
• Neuropathic itch syndromes are typically due to either peripheral (PNS) or central nervous system (CNS) disorders and can be further categorized into focal or regional presentations.
• CNS-related neuropathic itch syndromes involve abnormalities of the brain.
• PNS-related neuropathic itch syndromes involve abnormalities of the spinal cord, cranial or spinal nerve roots, or peripheral nerves.
• Neuropathic itch is more likely to develop in the head and neck region than on the lower body (e.g., facial zoster is more likely to cause post-herpetic itch [PHI] than zoster on the torso).
• Neuropathic itch differs in quality from other forms of pruritus and often makes afflicted individuals want to ‘dig at’ or ‘gouge out’ their skin; it is not responsive to antihistamines, but patients may find relief with application of ice packs.
• Patients with neuropathic itch often present first to a dermatologist.
Trigeminal Trophic Syndrome (TTS)
• A type of intractable facial neuropathic itch characterized by ‘painless scratching’ to the point of self-harm and cutaneous ulceration.
• Classically involves the nasal ala and typically results from impingement or damage to the sensory portion of the trigeminal nerve (Figs. 4.11 and 4.12).
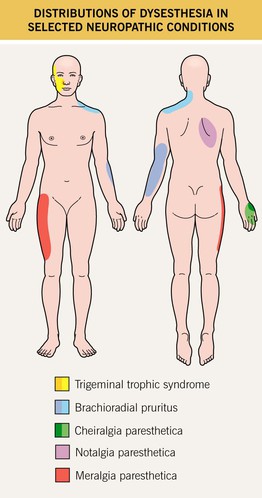
Fig. 4.11 Distributions of dysesthesia in selected neuropathic conditions. Cheiralgia paresthetica is caused by entrapment of the superficial branch of the radial nerve. Darker shades indicate more common areas of involvement. Courtesy, Karynne O. Duncan, MD.


Fig. 4.12 Trigeminal trophic syndrome. Erosions and ulcerations with hemorrhagic crusts favor the ala nasi (A, B). Obvious linear excoriations are seen in the second patient (B). Courtesy, Kalman Watsky, MD.
• Common inciting factors include iatrogenesis (ablation of the Gasserian ganglion to treat intractable trigeminal neuralgia), infection (varicella zoster virus [VZV], herpes simplex virus), stroke (infarction of the posterior cerebellar artery), CNS tumors or their resultant treatment.
• Clinically may present as a small crust that develops into a crescentic ulcer that may gradually extend to involve the cheek and upper lip.
• The nasal tip is usually spared because its nerve supply is derived from the external branch of the anterior ethmoidal nerve.
• Treatment is difficult and should involve protective barriers, patient education, and surgical consultation; oral pimozide and carbamazepine have been anecdotally reported as helpful.
Radiculopathies
• Characterized by a pattern of focal or regional neurological dysfunction that is caused by ‘injury’ to a single sensory nerve root (SNR) or less often to a few adjacent nerve roots, resulting in pruritus or dysesthesia.
• ‘Injuries’ that can cause damage to these SNRs may include (1) impingement from spinal osteoarthritis; (2) distal impingement or irritation by inflamed muscles or connective tissues; (3) infections (e.g., VZV, Lyme disease, leprosy); and (4) other rare causes, such as tumors (schwannomas, metastases), vascular malformations, and cysts.
• The abnormal sensation (e.g., pruritus or other dysesthesia) is perceived in the skin area that is innervated by the damaged SNR(s), and these areas are known as dermatomes (see Fig. 67.10).
• Clinical presentations are usually unilateral and on the side of the damaged SNR, but occasionally may be bilateral.
• The evaluation of an unexplained radiculopathy should include a neurologic examination.
• If the symptoms are severe, sudden in onset, or worsen significantly, then radiologic imaging (magnetic resonance imaging is most sensitive) of the appropriate area of the spine can be performed.
• If radiologic imaging is negative, electromyogram and nerve conduction studies can be considered.
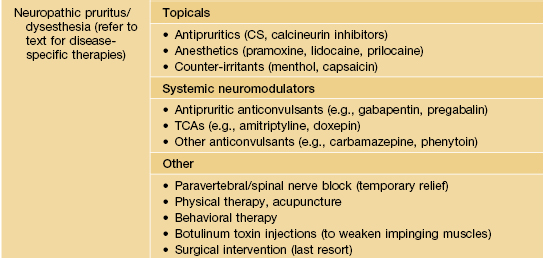
• In general, symptomatic treatment may include (1) topical agents (e.g., anesthetics, capsaicin); (2) various oral neuromodulators (e.g., gabapentin, pregabalin, other anticonvulsants); (3) physical therapy and acupuncture (if underlying muscle or connective tissue inflammation); and (4) botulinum toxin injections to weaken impinging muscles, if deemed safe.
• Several classic radiculopathies encountered in dermatology are (1) ‘shingles’ or post-herpetic neuralgia (PHN) or post-herpetic itch (PHI); (2) notalgia paresthetica; (3) brachioradial pruritus, and (4) meralgia paresthetica (Fig. 4.11).
Notalgia Paresthetica
• Affects roughly 10% of the adult population and thought to be related to SNR impingement at the level of the spinal cord due to osteoarthritis or more distally, due to impingement or irritation from inflamed muscles or other connective tissue.
• Presents with focal, intense pruritus of the upper back, most commonly along the medial scapular borders (see Fig. 4.11); sometimes the pruritus is accompanied by other dysesthesias (e.g., pain, burning).
• Often, a hyperpigmented patch that is a result of chronic rubbing is seen in the area of pruritus (Fig. 4.13).

Fig. 4.13 Notalgia paresthetica. A circumscribed area of hyperpigmentation on the left mid back (overlying the medial aspect of the scapula) due to chronic rubbing and scratching. The patient complained of significant pruritus in that area. An incidental café au lait macule is on the right mid back. Courtesy, Jean L. Bolognia, MD.
• DDx: macular amyloidosis, which is also due to chronic rubbing and is probably a related entity; both disorders can be a cutaneous marker of Sipple syndrome, especially if the onset is during childhood or adolescence.
• Rx: topical capsaicin, a natural plant product that depletes substance P from cutaneous nerve endings, 5 times daily for 1 week followed by 3 times daily for 3–6 weeks may be effective.
• Other Rx: topical anesthetics, gabapentin, and acupuncture.
Brachioradial Pruritus
• Chronic, intermittent pruritus or burning pain of the dorsolateral aspects of the forearms and elbows; sometimes more extensive area of involvement (e.g., shoulder region) (see Fig. 4.11).
• Most patients have photodamaged skin and degenerative cervical spine disease, with UV light exposure and heat serving as triggers.
• The patient can often precisely delineate the affected area with a marking pen, and within this area are excoriations, prurigo simplex lesions, and sometimes even scarring (Fig. 4.14).

Fig. 4.14 Brachioradial pruritus. The affected area is outlined by ink. Courtesy, Elke Weisshaar, MD and Jeffrey D. Bernhard, MD.
• The ‘ice-pack sign’ is another diagnostic clue, because application of ice is often reported as the only modality that provides relief.
• Rx: sun protection, cold packs, topical medications (pramoxine, capsaicin), oral neuromodulating drugs (gabapentin, amitriptyline).
Meralgia Paresthetica
• Due to impingement of the lateral femoral cutaneous nerve as it passes through the inguinal ligament; rarely due to trauma or ischemia.
• Presents with pruritus or dysesthesia of the anterolateral thigh, most often numbness or burning pain (Fig. 4.15; see Fig. 4.11).

Fig. 4.15 Meralgia paresthetica. A circumscribed area of hyperpigmentation, lichenification, and hypertrichosis due to chronic rubbing and scratching.
• Predisposing factors include obesity, pregnancy, tight clothing, and, rarely, mass effect from tumor or hemorrhage.
• Rx: removal of the cause of compression, focal nerve block at the inguinal ligament, and lastly surgical decompression.
Small Fiber Polyneuropathies (SFPN)
• Perhaps the most common cause of chronic pruritus in the following areas: bilateral feet; feet and legs; hands and legs; or other widespread bilateral areas of the body.
• Typically presents with pruritus, dysesthesias, paresthesias, and/or neuropathic pain in a ‘stocking-glove’ distribution; muscle function is usually intact.
• If the diagnosis of SFPN is suspected based on history and neurologic examination, then potentially treatable causes should be identified, including.
– Fasting blood glucose, HbA1c (diabetes mellitus).
– Serum B12, RBC folate, methylmalonic acid, homocysteine, and copper levels (B12, folate, or copper deficiencies).
– Serum (SPEP) and urine (UPEP) protein electrophoreses, immunofixation and serum-free light-chain analysis (monoclonal gammopathy).
– CBC with differential and platelets (hematologic malignancies).
• For SFPN, there are two diagnostic tests:
– Immunohistochemical staining (e.g., anti-PGP9.5) of a (nontraumatized) distal leg skin punch biopsy specimen to evaluate the small nerve fibers (requires a special fixative).
– Autoimmune function testing (e.g., sweat functioning).
Dysesthesia Syndromes
• Typically caused by an underlying neurological disorder (either peripheral or central), but it is not always identifiable.
• Several locoregional dysesthesia syndromes are encountered in dermatology: burning mouth syndrome (orodynia), burning scalp syndrome (scalp dysesthesia), and several dysesthetic anogenital syndromes.
• DDx: includes psychogenic pruritus/dysesthesia (see Chapter 5).
Burning Mouth Syndrome (Orodynia)
• Burning mucosal pain without clinically detectable oral lesions; most commonly affects middle-aged to elderly women.
• Typically bilateral, involving the anterior two-thirds of the tongue, palate, and lower lip.
• Diagnosis requires exclusion of secondary causes such as malignancy (e.g., oral SCC), vitamin deficiencies (e.g., folate, B12), candidiasis, xerostomia (e.g., previous radiation therapy, Sjögren syndrome), contact stomatitis, and ill-fitting dentures.
• Depression and anxiety are more common in patients with burning mouth syndrome.
• Rx: oral tricyclic antidepressants and gabapentin in addition to topical anesthetics (e.g., lidocaine, dyclonine) and mouthwashes (various combinations of tetracycline, hydrocortisone, diphenhydramine, nystatin, and Maalox®).
Burning Scalp Syndrome (Scalp Dysesthesia)
• Diffuse scalp burning, pain, pruritus, numbness or tingling without any specific cutaneous lesions.
• Strongly correlated with underlying depression and anxiety.
• Occasionally associated with primary neurologic disorders (e.g., multiple sclerosis).
• Diagnosis requires exclusion and treatment of secondary causes, such as seborrheic dermatitis, folliculitis, lichen planopilaris, allergic or irritant contact dermatitis, dermatomyositis, and discoid lupus erythematosus.
Dysesthetic Anogenital Syndromes
• Various names: pruritus ani, anodynia, pruritus vulvae, vulvodynia, pruritus scroti, scrotodynia, penile pain syndrome.
• Severe, intractable pruritus or dysesthesia despite either a normal clinical examination or the presence of nonspecific cutaneous findings.
• When all typical secondary causes of anogenital pruritus and dysesthesia have been investigated and treated (e.g., candidiasis, fecal incontinence; see Chapter 60), and the patient still has symptoms, consider lumbosacral radiculopathy (imaging studies), dermographism (trial of oral antihistamines), and contact dermatitis (patch testing).
• If no etiology detected, consider both psychiatric counseling and treatment with a neuromodulator medication (e.g., tricyclic antidepressant or gabapentin).
For further information see Ch. 6. From Dermatology, Third Edition.