Psychocutaneous Disorders
Introduction
• Psychodermatology refers to any aspect of dermatology in which psychological factors play a significant role.
• Psychodermatologic disorders can be classified in two ways: (1) by the specific psychodermatologic condition or (2) by the underlying psychopathology (Fig. 5.1).
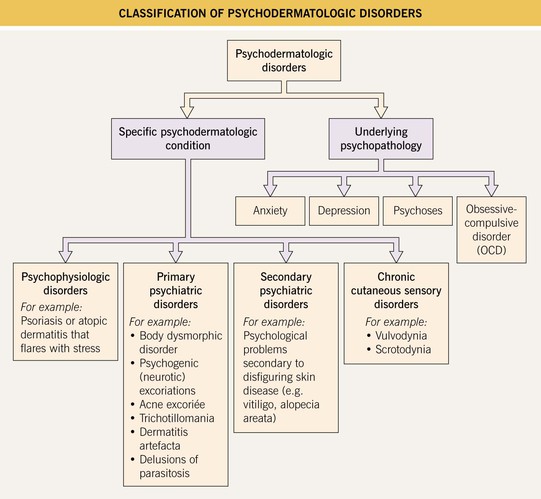
• Treatment is simplified by basing the choice of psychotropic medication or therapy on the underlying psychopathology (Table 5.1).
Table 5.1
Common psychotropic medications used in dermatology.
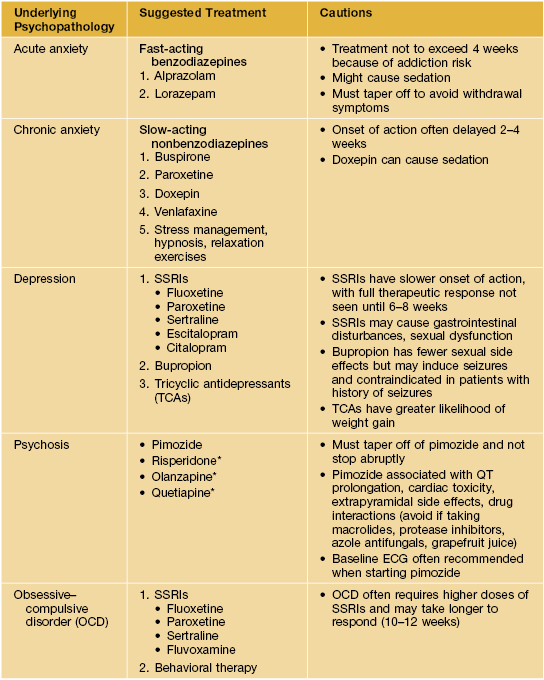
* Increasing frequency of use because of lower risk of tardive dyskinesia, compared with pimozide.
SSRI, selective serotonin reuptake inhibitors.
• The more commonly encountered primary psychiatric disorders in dermatology include body dysmorphic disorder, psychogenic (neurotic) excoriations, acne excoriée, trichotillomania, dermatitis artefacta, and delusions of parasitosis.
• Because many of these patients with primary psychiatric disorders present to the dermatologist and not the psychiatrist, it is important to establish the correct diagnosis and to offer appropriate treatment options.
The More Common Primary Psychiatric Disorders Seen in Dermatology
Body Dysmorphic Disorder
• Characterized by a distressing or impairing preoccupation with a nonexistent or slight defect in appearance.
• On a psychiatric spectrum from obsessional to delusional.
• Mean age of onset is 30–35 years; females = males; present in up to 10–15% of dermatologic patients.
• Patients usually concerned with nose, mouth, hair, breasts, or genitalia.
• Often adopt obsessional (e.g., numerous visits to physician for reassurance), ritualistic (e.g., excessive grooming routines), or delusional (e.g., multiple unnecessary surgeries) behaviors.
• Consider and assess for this diagnosis in patients seeking multiple cosmetic procedures.
• Rx: selective serotonin reuptake inhibitors (SSRIs) for obsessive–compulsive disorder (OCD) variant or antipsychotics for delusional variant.
Psychogenic (Neurotic) Excoriations
• A conscious, repetitive, uncontrollable desire to pick, rub, or scratch skin.
• On a psychiatric spectrum most closely related to OCD but may also be an expression of generalized anxiety disorder or depression.
• Most common in middle-age; females > males.
• Favors scalp, face, upper back, extensor forearms, shins, buttocks.
• Lesions usually in all stages of evolution: erosions (prurigo simplex), deep circular or linear ulcerations with hypertrophic borders, hypo- or hyperpigmented scars (Fig. 5.2); admixed well-healed scars point to chronicity.

Fig. 5.2 Psychogenic (neurotic) excoriations. Deep, angulated, unnatural-shaped ulceration on the chin. Courtesy, Kalman Watsky, MD.
• DDx: (1) underlying causes of primary pruritus (see Chapter 4); (2) underlying primary cutaneous disorder (e.g., folliculitis).
• Rx: symptomatic treatment of pruritus (topicals, oral antihistamines); tricyclic antidepressants (TCAs) or SSRIs (if underlying depression); SSRIs (if underlying OCD); consultation with a psychiatrist.
Acne Excoriée
• Considered a subset of psychogenic (neurotic) excoriations, characterized by ritualistic picking of acne lesions (Fig. 5.3).

Fig. 5.3 Acne excoriée. This patient compulsively picked at his acne lesions. Courtesy, Richard Odom, MD.
• Often associated with OCD; most common in young females.
• Rx: aggressively treat underlying acne; TCAs or SSRIs (if underlying depression); SSRIs (if underlying OCD); consultation with a psychiatrist.
Trichotillomania
• Defined as hair loss from a patient's repetitive self-pulling of hair.
• On a psychiatric spectrum from inattentive habitual hair pulling to impulse disorder to OCD to other underlying psychiatric disorder.
• Most helpful to approach the patient by age of onset, in terms of discussing prognosis and treatment.
– Preschool onset: typically benign course; most children outgrow the habit; Rx involves bringing awareness to parents and patient.
– Pre-adolescent to young adult onset: more chronic, relapsing course; on a spectrum from habit/unawareness to underlying psychopathology; Rx includes bringing awareness, behavioral modification therapy, psychotropic medications as necessary.
– Adult onset: more protracted course; often due to underlying psychopathology; Rx most often entails referral to psychiatrist/psychologist and treatment of underlying psychiatric disorder.
• Peak onset ages 8–12 years; females > males.
• Most commonly scalp hair, but also eyebrows, eyelashes, or pubic hair.
• Classically see hairs of varying lengths distributed within the area of alopecia; uninvolved areas are normal (Fig. 5.4).

• Sometimes associated ritualistic behavior or trichophagy.
• DDx: other causes of non-scarring alopecia (e.g., alopecia areata, tinea capitis).
• A helpful diagnostic test is the ‘clipped hair square,’ in which a small section of hair is clipped close to the scalp with scissors; in trichotillomania the hairs (being too short to pull out) display uniform hair regrowth.
• Rx: behavioral modification is primary treatment; psychosocial support; SSRIs; case reports of N-acetyl cysteine replacement.
Cutting (Self-Injury)
• Cutting is a form of nonsuicidal self-injury that has received increased attention by the medical community and media in recent years.
• It is a practice in which the individual makes small cuts on his/her body, most often on the arms and legs, with a sharp instrument such as a razor blade.
• Typically seen in adolescents and young adults (females > males) as a maladaptive response to psychological distress; may also be a symptom of an underlying psychological disorder (e.g., anxiety, depression, borderline personality disorder).
• In contrast to dermatitis artefacta, patients acknowledge that they inflicted the lesions upon themselves.
• Clinically, lesions present as an admixture of linear erosions or well-healed scars, often in an array of parallel lines (likened to ‘railroad ties’); some individuals will cut words into their skin; with time, the cutting will typically escalate to more frequent and numerous lesions.
• Unexplained, recurrent ‘cuts and scratches’ on the forearms and legs of adolescents should arouse suspicion for this behavior.
• Rx: familial and psychological support; treatment of underlying psychopathology.
Dermatitis Artefacta
• Characterized by self-inflicted lesions as a means to satisfy a psychological need that is not consciously understood; self-denial.
• Rare disorder; majority of patients suffer from borderline personality disorder; may have underlying depression and/or anxiety.
• Onset typically in adolescence or young adulthood; females >> males.
• Lesions often appear in easy-to-reach areas and appear in bizarre shapes and configurations; may employ outside instruments (Fig. 5.5).




Fig. 5.5 Dermatitis artefacta. A ‘Bizarre’ and unnatural appearance of the skin with angulated borders, possibly created with a sharp instrument. B Lesions in multiple stages of evolution, from circular, crusted erosions to ‘bizarre-shaped’ erosions on the mid-shin to hyperpigmented scars. This teenage girl denied knowing how the lesions developed or having any role in the process. C Scars from cigarette burns. D Unusual, linear, hypertrophic scars resulting from self-carving with a sharp instrument. A, Courtesy, John Koo, MD; C, Courtesy, Ronald P. Rapini, MD; D, Courtesy, M. Joyce Rico, MD.
• DDx: (1) primary dermatologic disorder; (2) monosymptomatic hypochondriacal disorder; (3) malingering (conscious gain); (4) OCD; (5) Münchhausen syndrome by proxy.
• Rx: symptomatic treatment of wounds; psychosocial support; psychotropic medications tailored to underlying psychopathology.
Delusions of Parasitosis
• A monosymptomatic, hypochondriacal psychosis characterized by a fixed and false (delusional) belief that an individual is infested with parasites, despite any objective evidence.
• This delusion is ‘encapsulated’ and other mental functions are usually intact.
• Typical onset is in the mid 50s–60s.
• Patients often bring in bits of skin, lint, and other specimens to prove the existence of the supposed parasites (Fig. 5.6).
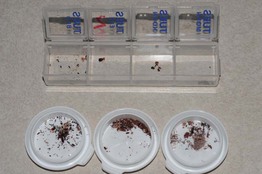
Fig. 5.6 Delusions of parasitosis. Samples of alleged ‘parasites’ brought in by a patient (‘matchbox sign’). Courtesy, Kalman Watsky, MD.
• Often experience ‘formication,’ which is a cutaneous sensation of crawling, biting, and/or stinging.
• DDx: (1) legitimate primary dermatologic disorder; (2) true formication without delusion; (3) formication plus delusion, related to substance abuse (e.g., methamphetamines); (4) delusional ideation (i.e., mentally fixated but not completely inflexible).
• A recent investigation by the Centers for Disease Control and Prevention supported the categorization of Morgellons disease as a form of delusions of parasitosis.
• Rx: establish rapport with patient first; pimozide or atypical antipsychotics.
For further information see Ch. 7. From Dermatology, Third Edition.