Oral Diseases
• In addition to common benign lesions such as bite fibromas and mucoceles, oral findings often represent clues to the diagnosis of skin disorders (e.g. lichen planus, early pemphigus vulgaris) or cutaneous signs of systemic disease (Table 59.1).
• Oral manifestations of infectious diseases (e.g. candidiasis, viral enanthems, findings associated with HIV infection) are covered in the chapters focused on these conditions.
Common Oral Mucosal Findings
Fordyce Granules
• ‘Free’ sebaceous glands (i.e. not associated with hair follicles) evident in as many as 75% of adults.
• Multiple 1- to 2-mm yellowish papules on the vermilion lips (upper > lower) and oral mucosa (especially buccal).
Geographic Tongue (Migratory Glossitis)
• Incidental finding on the dorsum of the tongue in ~2–3% of the population; may occasionally be associated with psoriasis, especially pustular variants.
• Well-demarcated areas of erythema and atrophy of the filiform papillae, surrounded by a whitish, hyperkeratotic serpiginous border (Fig. 59.1); lesions tend to migrate over time, may affect other oral sites, and are occasionally associated with a burning sensation.

Fig. 59.1 Geographic tongue. A florid example, demonstrating well-delineated areas of erythema partially surrounded by white serpiginous borders. Courtesy, Carl M. Allen, MD, and Charles Camisa, MD.
Scrotal (Fissured) Tongue
• Asymptomatic finding that is occasionally associated with conditions such as granulomatous cheilitis (see below) and Down syndrome.
• Multiple grooves or furrows are present on the dorsal tongue, especially centrally (Fig. 59.2).

Fig. 59.2 Fissured tongue. Numerous asymptomatic furrows and grooves on the dorsal tongue. Courtesy, Carl M. Allen, MD, and Charles Camisa, MD.
Hairy Tongue (Black Hairy Tongue)
• Reflects accumulation of keratin on the dorsum of the tongue; contributing factors may include poor oral hygiene, smoking, and a soft diet.
• Confluence of hairlike projections, which represent elongated papillae, with yellowish to brown-black discoloration (Fig. 59.3); may have exogenous staining from food, tobacco, or chromogenic bacteria (especially following antibiotic therapy); some patients report an unpleasant odor or taste.
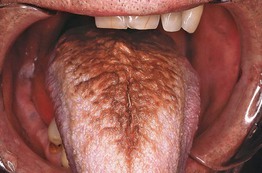
Fig. 59.3 Hairy tongue. The dorsum of the tongue exhibits marked accumulation of keratin and brown discoloration. Courtesy, Carl M. Allen, MD, and Charles Camisa, MD.
• DDx: pigmented papillae of the tongue (in individuals with darkly pigmented skin).
Leukoedema
• Normal variant that is more often evident in smokers and individuals with darkly pigmented skin.
• Grayish-white, opalescent, sometimes ‘moth-eaten’ appearance of the buccal > labial mucosa; typically becomes less evident upon stretching.
Median Rhomboid Glossitis
• Found in ~1% of adults, often associated with local overgrowth of Candida.
• Well-demarcated diamond- or oval-shaped area of erythema and atrophy on the dorsum of the tongue (Fig. 59.4).

Fig. 59.4 Median rhomboid glossitis. On the dorsum of the tongue (anterior to the circumvallate papillae), there is a well-demarcated, smooth area with loss of the filiform papillae.
• Rx: clotrimazole troches or oral fluconazole (for dosage, see Table 64.5).
Periodontal and Dental Conditions with Dermatologic Relevance
Desquamative Gingivitis
• Clinical finding that can occur in several immune-mediated vesicular and erosive disorders (Fig. 59.5); favors women over 40 years of age.
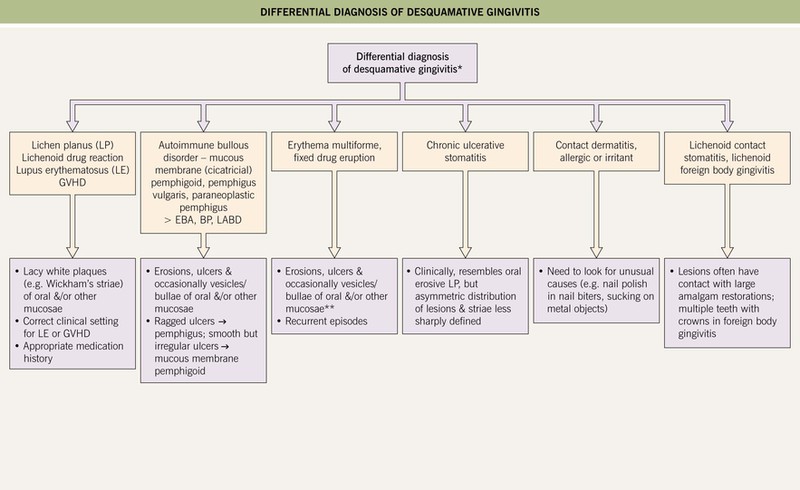
Fig. 59.5 Differential diagnosis of desquamative gingivitis. If the gingivae are painful, hemorrhagic, and necrotic with punched-out interdental papillae, then necrotizing ulcerative gingivitis (trench mouth) should also be considered. *No cutaneous lesions present. **Erythema multiforme is more likely to affect other mucosal sites. BP, bullous pemphigoid; EBA, epidermolysis bullosa acquisita; LABD, linear IgA bullous dermatosis. Courtesy, Carl M. Allen, MD, and Charles Camisa, MD.
• Diffuse gingival erythema with varying degrees of sloughing and erosion; frequently painful.
• Because desquamative gingivitis is often a manifestation of mucous membrane (cicatricial) pemphigoid and other autoimmune bullous disorders, evaluation should include routine histology plus direct and indirect immunofluorescence studies (see Chapter 23).
• Rx: treatment of underlying condition plus meticulous oral hygiene.
Gingival Enlargement (Hyperplasia, Overgrowth)
• Systemic medications and other causes of gingival enlargement are listed in Table 59.2.
Table 59.2
Causes of gingival enlargement.
Another term for Wegener’s granulomatosis is granulomatosis with polyangiitis (Wegener's).
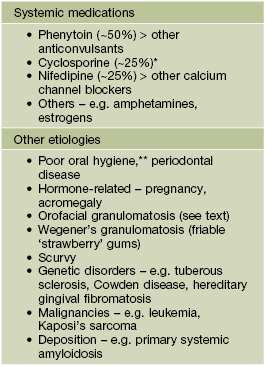
* Consider substitution with oral tacrolimus.
** Often contributes to gingival enlargement related to drugs and other factors.
• Drug-related gingival enlargement typically develops during the first year of administration and is first evident in the interdental papillae.
Dental Sinus
• Occurs in the setting of a chronic periapical abscess in a carious tooth.
• Intraoral (‘parulis’): soft, nontender, erythematous papule on the alveolar process in the region of the affected tooth.
• Cutaneous: erythematous papule, often with an umbilicated or ulcerated center; found on the chin or submandibular region (mandibular teeth) > the cheek or upper lip (maxillary teeth) (Fig. 59.6).


Fig. 59.6 Cutaneous sinuses of dental origin. These skin lesions can be associated with mandibular (A) or, less often, maxillary (B) teeth. The erythematous papule may be mistaken for a pyogenic granuloma or neoplasm. A, Courtesy, Judit Stenn, MD; B, Courtesy, Carl M. Allen, MD, and Charles Camisa, MD.
Sequelae of Trauma or Toxic Insults
Fibroma (Bite Fibroma)
• Results from reactive connective tissue hyperplasia in response to local trauma.
• Smooth pink papulonodule; most often located on the labial mucosa, especially of the lateral lower lip, or along the ‘bite line’ of the buccal mucosa.
• Rx: if bothersome, excision with histologic evaluation to exclude a neoplastic condition.
Morsicatio Buccarum (Chronic Cheek Chewing)
• Characteristic mucosal changes related to habitual chewing or biting.
• Shaggy white mucosa, usually bilaterally in the buccal region along the ‘bite line’ (Fig. 59.7).

Fig. 59.7 Cheek chewing (morsicatio buccarum). Repetitive nibbling of the superficial layers of the epithelium resulted in these changes. Note that the characteristic shaggy, white lesion approximates the area where the upper and lower teeth meet. Courtesy, Carl M. Allen, MD, and Charles Camisa, MD.
Mucocele
• Translucent to bluish papule due to disruption of a minor salivary gland duct, most often located on the lower mucosal lip (Fig. 59.8; see Chapter 90).

Fig. 59.8 Mucocele. Soft nodule with bluish hue in a typical location: lower lateral labial mucosa. Courtesy, Carl M. Allen, MD, and Charles Camisa, MD.
Chemotherapy- and Radiation Therapy-Induced Mucositis
• Results from cytotoxic effects on the oral epithelium, especially in the setting of neutropenia; typically develops 4–7 days after administration of chemotherapy and ≥2 weeks after beginning radiation therapy.
• Multiple erosions and/or ulcerations favor the gingivae, lateral tongue, and buccal mucosa; self-limited.
• DDx: herpetic or candidal infections (may be concomitant).
• Rx: topical anesthetics, analgesics, maintenance of oral hygiene; palifermin (recombinant human keratinocyte growth factor) can reduce severity but produces whitish discoloration of the dorsum of the tongue due to hyperkeratosis.
Cheilitis
• The differential diagnosis of cheilitis and clues to determining the etiology are outlined in Fig. 13.5; granulomatous cheilitis is discussed below.
• Cheilitis glandularis, seen primarily in men with a history of chronic sun exposure and/or lip irritation, is characterized by inflammatory hyperplasia of the lower labial salivary glands; this results in tiny erythematous macules (at sites of salivary ducts) and variable hypertrophy of the lower lip (Fig. 59.9).

Fig. 59.9 Cheilitis glandularis. Erythematous macules on the mucosal lower lip at sites of inflamed salivary gland ducts. There is also evidence of actinic cheilitis. Courtesy, Carl M. Allen, MD, and Charles Camisa, MD.
Other Inflammatory Conditions
Aphthae (Aphthous Stomatitis; Canker Sores)
• Common condition characterized by recurrent oral ulcers, with a peak prevalence during the second and third decades of life; outbreaks may be triggered by trauma, psychological stress, or hormonal fluctuations.
• Minor aphthae (most frequent form): painful, round to ovoid, shallow ulcers that are usually <5 mm in diameter; feature a yellowish-white to gray pseudomembranous base, well-defined border, and prominent erythematous rim (Fig. 59.10); favor the buccal or labial mucosa and typically heal in 1–2 weeks without scarring.

Fig. 59.10 Recurrent aphthous stomatitis. Shallow, creamy-white ulceration surrounded by an intensely red halo and located on nonkeratinized mucosa, representing a classic presentation. Courtesy, Carl M. Allen, MD, and Charles Camisa, MD.
• Major aphthae: larger (>1 cm), deeper ulcers that persist for up to 6 weeks; occasionally affect keratinized mucosa (e.g. dorsum of tongue, hard palate, attached gingiva) as well as nonkeratinized mucosa, may heal with scarring, and are more common in HIV-infected individuals.
• Herpetiform aphthae: simultaneous development of numerous small lesions that tend to coalesce; tends to favor nonkeratinized mucosa, unlike recurrent oral HSV, which favors keratinized mucosa.
• Complex aphthosis: frequent outbreaks of multiple (≥3) oral aphthae, or recurrent genital as well as oral aphthae, in the absence of Behçet's disease (see Chapter 21).
• Recurrent aphthae can occur in the setting of systemic disorders such as inflammatory bowel disease, SLE, and Behçet's disease (see Table 59.1).
• DDx: in addition to associated systemic conditions, may include HSV infection, trauma, and the disorders listed in Fig. 59.5.
• Rx: superpotent topical CS gel, topical analgesics; if severe or frequent recurrences: vitamin B12, colchicine, dapsone, thalidomide (the latter is especially helpful for major aphthae).
Granulomatous Cheilitis and Other Forms of Orofacial Granulomatosis
• The term orofacial granulomatosis refers to non-infectious, non-necrotizing granulomatous inflammation of the lips, face, and/or oral cavity; this term includes isolated granulomatous cheilitis as well as manifestations of Crohn's disease and sarcoidosis (see Table 59.1); usually develops during the second or third decade of life.
• Granulomatous cheilitis presents as diffuse swelling of the lip(s) (lower > upper or both) that can initially be intermittent (raising the possibility of angioedema) but is eventually persistent (Fig. 59.11); patients may have oral cobblestoning, recurrent aphthae, and gingival enlargement, and the less frequent association with a scrotal tongue and/or facial nerve palsy is referred to as Melkersson–Rosenthal syndrome.

Fig. 59.11 Orofacial granulomatosis. Note the swelling of the lips (lower > upper) and angular cheilitis in this 10-year-old boy with Crohn's disease. Courtesy, Julie V. Schaffer, MD.
• Rx: intralesional CS, topical calcineurin inhibitors, dapsone, tetracyclines (given for several months), thalidomide or TNF inhibitors (for severe disease); patients should be evaluated for signs of Crohn's disease and sarcoidosis.
Contact Stomatitis
• Irritant or allergic contact stomatitis can result from a variety of foods, food additives, and materials used in dentistry; in particular, cinnamon flavoring and dental amalgam (‘silver’ fillings) can lead to a lichenoid mucositis histologically.
• Shaggy white or erythematous areas, most often on the buccal mucosa or lateral tongue; lacy white streaks (resembling lichen planus) or erosions may be seen (Fig. 59.12).

Fig. 59.12 Contact stomatitis from artificial cinnamon flavoring. Use of artificial cinnamon-flavored gum caused this shaggy, white keratotic lesion of the buccal mucosa. Courtesy, Carl M. Allen, MD, and Charles Camisa, MD.
• Rx: evaluation with patch testing and avoidance of offending agents, sometimes requiring replacement of amalgam with other materials.
Nicotine Stomatitis
• Presents as gray-white discoloration of the palate, often with umbilicated papules that represent inflamed salivary ducts (Fig. 59.13).

Fig. 59.13 Nicotine stomatitis. Gray-white palatal mucosa with numerous umbilicated papules representing inflamed palatal mucous glands. Courtesy, Carl M. Allen, MD, and Charles Camisa, MD.
Atrophic Glossitis
• Manifestation of several nutritional deficiencies (e.g. vitamin B12 [pernicious anemia], folate, iron, niacin [pellagra], riboflavin; see Chapter 43) and candidiasis.
• Presents with a smooth, ‘beefy red’ tongue (Fig. 59.14); involvement may initially be patchy but is eventually diffuse and may be associated with a burning sensation or sore mouth.
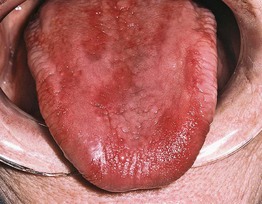
Fig. 59.14 Atrophic glossitis due to pernicious anemia plus candidiasis. Erythematous, atrophic tongue as a manifestation of pernicious anemia with a superimposed candidal infection. Courtesy, Carl M. Allen, MD, and Charles Camisa, MD.
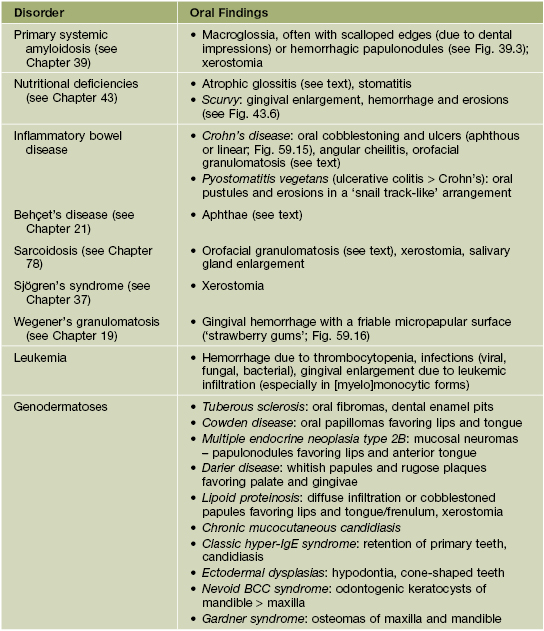
Oral Signs of Systemic Disease
• Systemic diseases that can present with oral findings are listed in Table 59.1 (Figs. 59.15 and 59.16).

Fig. 59.15 Crohn's disease. Linear ulceration of the mandibular vestibule is the classic oral manifestation of this disease. Courtesy, Carl M. Allen, MD, and Charles Camisa, MD.

Fig. 59.16 Wegener's granulomatosis – strawberry gums. The affected areas of the gingiva are red-purple, micropapular, and friable, with a resemblance to ripe strawberries. Courtesy, Carl M. Allen, MD, and Charles Camisa, MD.
Premalignant and Malignant Conditions
Leukoplakia and Erythroplakia
• Leukoplakia refers to a white patch or plaque on the oral mucosa that cannot be clinicopathologically characterized as a specific disease process; typically occurs in middle-aged and older adults (men > women), especially those who use tobacco ± alcohol, and is regarded as a premalignant condition for SCC.
– Often a homogeneous white patch or plaque, but may be nonhomogeneous and ‘speckled’ (e.g. white flecks on a red base); usually has sharply demarcated borders (Fig. 59.17).

Fig. 59.17 Leukoplakia. Sharply demarcated, white plaque involving the ventral surface of the tongue and floor of the mouth. Courtesy, Carl M. Allen, MD, and Charles Camisa, MD.
• Similarly, erythroplakia is defined as a red intraoral patch or slightly elevated, velvety plaque that cannot be diagnosed as a particular disease; biopsies usually show more severe epithelial dysplasia than leukoplakia.
• Often affects the buccal mucosa, lower inner lip, floor of the mouth, and lateral or ventral tongue.
• The degree of histologic epithelial dysplasia influences the risk of transformation to SCC; nonhomogeneous leukoplakia, erythroplakia, and lesions located on the floor of the mouth or lateral/ventral tongue also have higher malignant potential.
• DDx of leukoplakia: may include SCC, lichen planus, candidiasis, morsicatio buccarum (see above), and nicotine or contact stomatitis.
• After elimination of possible causative factors (e.g. tobacco use, candidiasis, irritation/trauma) for 2–6 weeks, persistent lesions should be biopsied.
• Rx: for leukoplakia with moderate to severe dysplasia or in high-risk sites and for erythroplakia – excision, cryosurgery, or laser ablation; all patients need longitudinal evaluation and should avoid carcinogenic habits.
• Proliferative verrucous leukoplakia, which tends to occur in women without traditional risk factors, is characterized by multifocal red and white patches that eventually develop a verrucous surface; difficult to treat and associated with high risk of transformation to SCC.
Squamous Cell Carcinoma
• Most common malignancy of the oral cavity, favoring middle-aged and older men; risk factors include tobacco and alcohol use, HPV infection (see Chapter 66), and betel nut chewing.
• May present as an ulcer, exophytic mass, or area of induration; most often on the lateral or ventral tongue and floor of the mouth (Fig. 59.18).

Fig. 59.18 Squamous cell carcinoma. Ulcerated, indurated, exophytic mass involving the right lateral border of the tongue, a typical presentation and site for this tumor. Courtesy, Carl M. Allen, MD, and Charles Camisa, MD.
• DDx: leukoplakia, traumatic ulcer (Fig. 59.19), salivary gland tumor, amelanotic melanoma.

Fig. 59.19 Traumatic ulcer. This lesion on the lateral tongue has a yellow fibrinopurulent membrane and white hyperkeratotic border. Compare this to the oral SCC depicted in Fig. 59.18, which presented as an ulcerated, indurated mass. Courtesy, Carl M. Allen, MD, and Charles Camisa, MD.
• Rx: combinations of surgery, radiation therapy (especially if HPV-associated), and chemotherapy.
• Verrucous carcinoma (oral florid papillomatosis) is a low-grade variant of SCC that presents as slowly growing, exophytic papillomatous masses that favor the buccal mucosa and gingiva; Rx: excision, traditionally avoiding radiation therapy due to a possible association with anaplastic transformation.
Melanoma
• Uncommon oral malignancy that favors middle-aged and older men; often diagnosed at a locally advanced stage.
• Pigmented (with findings similar to cutaneous melanoma; see Chapter 93) > amelanotic, with a predilection for the hard palate and maxillary gingivae.
• DDx: for pigmented lesions – foreign body tattoo (Fig. 59.20), blue nevus, oral melanotic macule, physiologic pigmentation.

Fig. 59.20 Amalgam tattoo. Foreign body tattoos are the most common cause of acquired oral pigmentation, and most of them are due to implantation of dental amalgam. In this patient, the amalgam was used to seal the apices of endodontically treated teeth, resulting in tattooing of the maxillary vestibule. Courtesy, Carl M. Allen, MD, and Charles Camisa, MD.
For further information see Ch. 72. From Dermatology, Third Edition.