Benign Epithelial Tumors and Proliferations
Seborrheic Keratosis
• Begin to appear during the 4th decade of life and then gradually increase in number.
• Macular, papular, or verrucous; colors vary from white to black but most commonly brown.
• Typically has a ‘stuck-on’ appearance with a smooth to verrucous surface (Fig. 89.1).
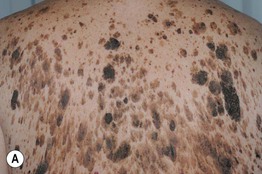

Fig. 89.1 Seborrheic keratoses. A Multiple seborrheic keratoses on the back, with some in a pattern that has been likened to raindrops. B Sharply demarcated pigmented papules and plaques with a papillomatous surface and horn pseudocysts. Note the ‘stuck-on’ appearance. A, Courtesy, Kalman Watsky, MD.
• Spares the palms, soles, and mucosal surfaces.
• May resemble a melanoma clinically but has no pigment network (by dermoscopy) and has horn pseudocysts.
• Sudden appearance of multiple lesions may be associated with internal malignancy (sign of Leser–Trélat) or erythroderma; the former may also be associated with skin tags, irritated seborrheic keratoses, tripe palms, and acanthosis nigricans.
• Histopathology: a spectrum of different architectures, most commonly acanthotic, papillomatous and hyperkeratotic, or irritated (Fig. 89.2).
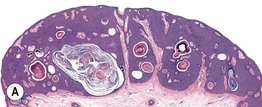
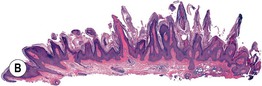
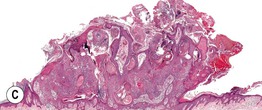
Fig. 89.2 Seborrheic keratoses – spectrum of histologic subtypes. A Acanthotic type with lobular hyperplasia with prominent horn cysts. B Papillomatous or hyperkeratotic type with church spires of papillomatosis and hyperkeratosis. C Irritated seborrheic keratosis. Exophytic lesion with papillomatosis, hyperkeratosis, hemorrhagic crust, and dermal inflammation. A, B, Courtesy, Luis Requena, MD; C, Courtesy, Lorenzo Cerroni, MD.
– Dermatosis papulosa nigra (Fig. 89.3): common in dark-skinned individuals; 1- to 5-mm hyperpigmented papules on the face.

Fig. 89.3 Dermatosis papulosa nigra. Multiple hyperpigmented papules with typical location on the cheeks. Courtesy, Luis Requena, MD.
– Stucco keratosis (Fig. 89.4): 1- to 4-mm gray-white papules on the lower extremities (especially dorsal feet and ankles) of older adults.

Fig. 89.4 Stucco keratoses. Multiple gray-white keratotic papules on the ankle and dorsal foot. Courtesy, Jean L. Bolognia, MD.
– Inverted follicular keratosis: endophytic variant of seborrheic keratosis; tan to pink papule, typically on the face of adults.
Acrokeratosis Verruciformis
• Autosomal dominant disorder; sometimes associated with Darier disease.
• Multiple, skin-colored, flat-wart-like papules on dorsal aspect of hands and feet.
• Benign neoplasm of keratinocytes showing papillomatosis with overlying hyperkeratosis in ‘church spires’.
Clear Cell Acanthoma
• Red, shiny papule or plaque, sometimes with a peripheral collarette of scale (Fig. 89.5).

Fig. 89.5 Clear cell acanthoma. Well-demarcated, dark, red, shiny papule with a wafer-like collarette of scale. Courtesy, Luis Requena, MD.
• Histopathology: acanthosis of characteristically well-demarcated pale or clear keratinocytes with overlying parakeratosis.
Large Cell Acanthoma
• Variably colored papule or plaque in sun-exposed sites in older individuals (Fig. 89.6).

Fig. 89.6 Large cell acanthoma. Well-demarcated, thin, pink-brown plaque. Courtesy, Luis Requena, MD.
• A variant of actinic keratosis and seborrheic keratosis.
• Histopathology: orthokeratosis overlying a thin epidermis composed of enlarged keratinocytes.
Porokeratosis
• Several different types (Table 89.1; Fig. 89.7).
Table 89.1
Types of porokeratosis.
| Type | Clinical Features |
| Porokeratosis of Mibelli | Plaque that arises during infancy or childhood, usually on a distal extremity; usually several cm in diameter |
| Disseminated superficial actinic porokeratosis | Pink to brown papules and plaques with peripheral scale; arise in sun-exposed sites, especially the forearms and shins; usually measure from a few mm to 1.5 cm; in some patients, autosomal dominant inheritance |
| Large-sized lesions | In immunocompromised patients, especially solid organ transplant recipients |
| Linear porokeratosis | Streaks along the lines of Blaschko; arise during infancy or childhood Risk of development of squamous cell carcinoma |
| Punctate porokeratosis | 1- to 2-mm palmoplantar papules; arise during adolescence or adulthood |
| Porokeratosis palmaris et plantaris et disseminata | Palmoplantar papules in addition to involvement of the trunk, extremities, and even mucous membranes; onset during childhood or adolescence |
| Porokeratosis ptychotropica | Erythematous plaque, sometimes with smaller peripheral papules, in the gluteal cleft or folds |





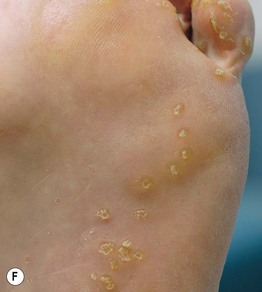
Fig. 89.7 Porokeratoses. A Porokeratosis of Mibelli on the hand of a child. B Actinic porokeratosis in a renal transplant patient with significant solar damage. Note the narrow, elevated rim. C, D Multiple lesions of disseminated superficial actinic porokeratosis (DSAP) with obvious peripheral keratotic rims; lesions can range in color from light brown to pink. E Several streaks of linear porokeratosis on the lower extremity. F Multiple keratotic papules on the plantar surface due to punctate porokeratosis. B, C, D, Courtesy, Jean L. Bolognia, MD; F, Courtesy, Kalman Watsky, MD.
• All have a distinctive thread-like border of scale that corresponds histopathologically to the cornoid lamella (column of parakeratosis histologically).
• The most common form, disseminated superficial actinic porokeratosis (DSAP), is sometimes misdiagnosed as multiple actinic keratoses.
Epidermal Nevus (See Chapter 51)
• Hyperpigmented (rarely hypopigmented) papules and plaques (Fig. 89.8) along Blaschko's lines.

Fig. 89.8 Epidermal nevus. Verrucous hyperpigmented plaques. An individual papule, in isolation, resembles a seborrheic keratosis. Courtesy, Kalman Watsky, MD.
• Verrucous, keratotic, velvety or barely elevated.
• May have a sebaceous or other adnexal component (i.e. nevus sebaceus), especially if on the scalp or face.
• Can be caused by mosaicism for mutations in FGFR3 (fibroblast growth factor receptor-3), PIK3CA, HRAS (also in nevus sebaceus), keratin 1 or 10 (if histologic finding of epidermolytic hyperkeratosis), and other genes.
• May be associated with extracutaneous manifestations (see Chapter 51).
Inflammatory Linear Verrucous Epidermal Nevus (See Chapter 51)
• Linear, pruritic, psoriasiform (erythematous with scale) plaques, usually on an extremity.
• 75% appear before age 5 years.
• DDx: primarily linear psoriasis (see Chapter 6).
Nevus Comedonicus
• Linear plaques composed of grouped comedones; may develop inflammatory acneiform lesions.
• 50% present at birth; otherwise, generally appear before age 10 years.
Flegel's Disease (Hyperkeratosis Lenticularis Perstans)
• Rare; may have an autosomal dominant inheritance.
• Onset usually during adulthood.
• Lentil-like keratotic papules on the distal lower extremities (Fig. 89.9).

Fig. 89.9 Flegel’s disease. Scaly pink to pink-brown papules on lateral foot. Courtesy, Peter Heald, MD.
Cutaneous Horn
• Clinical term for marked hyperkeratosis arising from a papule or nodule (Fig. 89.10).


Fig. 89.10 Cutaneous horn. A This cutaneous horn arose from an actinic keratosis. B Striking column of hyperkeratosis with hyperplasia of the underlying epidermis. B, Courtesy, Luis Requena, MD.
• The base of the lesion most commonly represents an actinic keratosis, seborrheic keratosis, verruca, or squamous cell carcinoma.
Solitary Lichenoid Keratosis/Lichen Planus-Like Keratosis
• Pink to pink-brown papule or plaque (Fig. 89.11); arises in chronically sun-damaged skin, most commonly on the chest, extensor upper extremities, and shins.
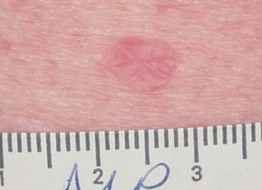
Fig. 89.11 Lichenoid keratosis. Pink, flat-topped papule in a fair-skinned individual. Courtesy, Jean L. Bolognia, MD.
• Clinically mimics an actinic keratosis and nonmelanoma skin cancer.
• Table 89.2 lists other solitary keratoses.
Table 89.2
Examples of other solitary keratoses.
| Solitary Lesion | Histologic Features of Solitary Lesion |
| Epidermolytic acanthoma | Epidermolytic hyperkeratosis (also seen in epidermolytic ichthyosis and some epidermal nevi) |
| Warty dyskeratoma | Resembles Darier disease |
| Acantholytic acanthoma | Resembles pemphigus vulgaris |
Confluent and Reticulated Papillomatosis (of Gougerot and Carteaud)
• Scaly to verrucous hyperpigmented plaques.
• Centrally confluent and reticulated at periphery (Fig. 89.12).

Fig. 89.12 Confluent and reticulated papillomatosis (CARP). Multiple hyperpigmented papules that are confluent centrally and assume a reticulated pattern laterally. Courtesy, Julie V. Schaffer, MD.
For further information see Ch. 109. From Dermatology, Third Edition.