Nonextraction Class II Correction
Ram S. Nanda, Tarisai C. Dandajena, Ravindra Nanda
Nonextraction treatment has gained in popularity in the orthodontic community since the second half of the twentieth century. This is due to the paradigm shift from focusing on the dentition to appraising the whole face. The careful selection of patients and timing of treatment are essential to the success of nonextraction treatment. When planning nonextraction treatment, we opt to use early treatment, redirection of growth, saving leeway space, guidance of eruption, and mechanics that aim to achieve distal movement of the maxillary molars. For a successful outcome, it is necessary before the initiation of treatment to take into consideration the type of malocclusion, facial type, required arch perimeter, individual growth, and motivation of the patient.
Class II, Division 1 malocclusion has been described as the most frequent treatment problem in orthodontic practice. It is estimated that about 35% of American children have Class II malocclusions. Distal movement of the maxillary first molars is a common goal in the treatment of the Class II molar relationship and in the resolution of tooth size–arch length discrepancy in the maxillary arch.
Early treatment is the key to successful treatment of Class II malocclusions. During the 1940s and 1950s Kloehn1 suggested the use of headgear during the transitional dentition to correct molar relations. In the 1960s Ricketts et al.2 promoted the bioprogressive philosophy, which used utility arches, quad helix, and cervical facebow headgear among several other innovative appliance systems. However, the real impetus behind nonextraction treatment was the realization that for far too long orthodontists had focused on the placement of the denture on the basal bone without sufficient regard to the facial integument. Research findings on long-term retention of treated dentitions revealed that relapse was common in both extraction and nonextraction treatment modalities. Cetlin and Ten Hoeve3 showed stable results for nonextraction treatment of patients with severe malocclusions. The thickness of facial soft tissue integument varies among individuals and its growth pattern is specific to individuals throughout their lifespan and not just during the period of active growth.4 In view of these findings, the nonextraction treatment modality has become a treatment of choice for select groups of patients.
Patient Selection
Patients need to be carefully selected for nonextraction treatment. Prospective patients to be treated using maxillary molar distalization techniques should exhibit a Class II dental relation or a minor skeletal Class II relation. A Class II relationship with mesial migration of maxillary molars due to premature loss of the primary molar is preferred. The patient should have minimal or no mandibular arch length discrepancy, preferably with mesofacial or brachyfacial types, and potential remaining growth. A low mandibular plane angle is most suitable because in high angle the distal movement of molars will tend to open the bite due to the extrusive force component. Even a full Class II relationship can be corrected if treated earlier. Recently, Kim et al.5 have shown that an occlusion established at an early age is more likely to be maintained despite the differential growth of the jaws.
A variety of appliances has been used, including ones that require patient cooperation and ones that do not.
Biomechanical Principles
The adequate force for distal movement of the molars is in the range of 150 to 250 g. The type of movement can be either translation or controlled tipping followed by uprighting. Translation movement requires the force to pass through the center of resistance (see Chapter 4). Therefore, when using any type of appliance, it is necessary to evaluate the force system of that appliance and to be informed about the side effects. Anchorage considerations include extrusion of molars and mesial movement of the anterior segment. To obtain the maximum benefit the distal resistance (the presence of second or third molars), growth in the tuberosity region, and functional interferences should be checked.
Treatment Modalities for Maxillary Molar Distalization
Several treatment modalities exist for the distal movement of the maxillary molars. These can be with either fixed or removable appliances, and intraoral or extraoral. The extraoral approach can use cervical, occipital, or high-pull headgear. The intraoral mechanics can be inter-arch or intra-arch. Of the inter-arch appliances, the Herbst, Twin Force bite corrector, Jasper jumper, and SAIF spring constitute fixed functional appliances that do not require patient compliance. Class II elastics with the jig and bimetric arch (Wilson appliance) require patient compliance. The transpalatal arch, coil springs, repelling magnets, K-loop,7 pendulum, Jones jig, and distal jet are intra-arch appliances. These appliances can be used as single entities or combined with another appliance. Some of these appliances are discussed below.
Headgear
Kingsley8 first introduced the extraoral method of applying traction to the maxillary arch to retract maxillary incisors. Later, Angle9 described and illustrated the headgear he used in the treatment of patients with Class II, Division 1 malocclusion. Both Kingsley and Angle used astonishingly modern-looking appliances, apparently with reasonable success. At the beginning of the twentieth century, the introduction of intermaxillary elastics resulted in the discontinuation of extraoral anchorage. This was not due to its ineffectiveness, but rather because it was considered an unnecessary complication.
By 1920 Angle and his followers were convinced that Class II and III elastics not only moved teeth but also caused significant skeletal changes, stimulating the growth of one jaw while restraining the other. If intraoral elastics could produce a true stimulation of mandibular growth while simultaneously restraining the maxilla, there would be no reason either to ask a patient to wear an extraoral appliance or to initiate treatment while waiting for the permanent teeth to erupt.
When cephalometric evaluations became available in the 1940s, they did not support the idea that significant skeletal changes occurred in response to intraoral forces. In 1936 Oppenheim10 strongly advocated extraoral anchorage therapy. Later, Kloehn1 demonstrated impressive results with headgear in the early treatment of Class II malocclusion. He stated that, during the transitional dentition, cervical traction can retard or even halt the forward growth of the maxilla and assist in moving maxillary teeth distally to correct developing Class II relationships.
While the distal movement of the molars by headgear may not be questionable, the changes that take place within the temporomandibular joint (TMJ) complex have not been well explained. Animal studies have shown remodeling of the condyle-glenoid fossa complex: apposition in the posterior compartment and resorption in the anterior compartment.11–13 Cephalometric studies have shown little or no change in the size of the mandible with the use of functional appliances such as headgear. It is possible that the lateral cephalogram is not sensitive enough to isolate these changes. The orthopedic forces applied by headgear cannot be ignored, however.
Extraoral traction has some demonstrable important advantages. These include maximum anchorage, ability to adjust the force levels, and control of bodily or tipping movement. It can assist in correcting transverse deficiencies by expanding the inner bow. The extrusive component of the cervical headgear will allow for bite opening in deep bite patients. If vertical control is a concern in a high-angle patient, a high-pull facebow headgear will control the extrusive force component.
There are limitations in the use of extraoral traction, of which the need for patient compliance is perhaps the most important. Besides compliance, the type of force delivered by the appliance is intermittent, with tooth movement usually being slower. We have found that prolonged use of headgear can delay the eruption of maxillary second molars or even lead to their impaction. This may not be a problem if treatment is initiated at the appropriate age of 9 years and for a limited time. In such cases the second molars need to be monitored if treatment is completed prior to their eruption. Extraction of the second molars may be considered if the presence of the third molars is radiographically documented. Despite these limitations, extraoral traction is perhaps one of the most effective ways to obtain distal movement of maxillary molars and a successful nonextraction treatment plan.
A decision to extract the second molars may be made in severe Class II cases where maximum retraction of the first molars is required. As mentioned, radiographic documentation for the presence of the third molars is important. Figure 12-1 documents a case in which extraction of the maxillary second molars was performed prior to their eruption. A mandibular lip bumper engaged to the mandibular first molar bands was used to align and unravel the minor mandibular crowding. The maxillary premolars were allowed to passively drift back. Retraction of the anterior segment, however, required active mechanics and this was accomplished using a T-loop. Class II elastics were used for 1 month. During this process the headgear was used as anchorage and the patient wore it only at bedtime.

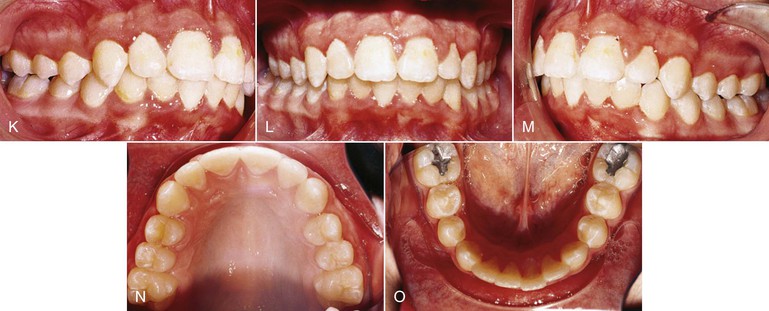
Figure 12-1 Headgear treatment. A–E, Pre-treatment intraoral photographs. A stainless steel crown is present on the exfoliating maxillary left second primary molar. F–J, Progress photographs show the lip bumper in place. K–O, Intraoral photographs 1 month post-treatment. Total treatment time was 23 months.
The headgear may be used effectively in cases of asymmetrical Class II correction. In such cases there is asymmetrical adjustment of the outer bow, one side being longer than the other.14,15 The longer arm of the outer bow will be placed on the side where correction of the Class II molar relationship is desired. Asymmetrically positioning the center of the outer bows while the arms are kept the same length may not achieve the same results as altering the lengths of the outer bows. This is because in the first instance the force applied will pass through the center, while in the latter instance there is an asymmetrical distribution of the moments. The greater moment is applied to the longer side.14,15 Of importance, however, is the need for patient compliance.
Care should be taken to adjust the facebow so as to achieve the desired result. In open bite, for example, care should be taken to avoid extrusion of the molars, while in cases of low mandibular plane angle extrusion of the molars may be a desired consequence. In such patients, then, application of the force above the center of resistance with the strap pulling down and backward will produce extrusion with distal movement.16 Figure 12-2 shows the various movements that can be obtained using the facebow headgear depending on the point of force application.16
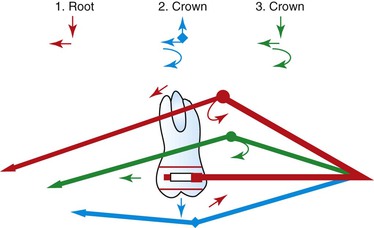
Figure 12-2 Forces and moments generated by the facebow headgear. 1, Force is above the center of resistance—the result is extrusion, mesial moment, and distal movement of the root. 2, Force is below the center of resistance in an upward direction—the effect is distal crown movement, clockwise moment, and an intrusive effect. 3, Force is below the center of resistance in a downward direction—the effect is extrusion, distal crown movement, and clockwise moment.
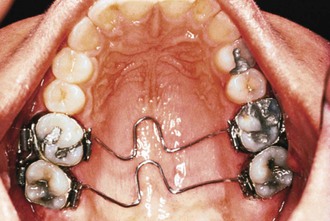
Vertical Holding Appliance
Some clinicians and investigators have sought ways to augment the extraoral traction. One method is the combined use of a vertical holding appliance (VHA)17,18 and high-pull headgear. The VHA (Fig. 12-3) has been recommended for treatment of high-angle patients where there is an important need to control the vertical dimension. It is fabricated from a 0.040-inch wire with a helix just distal to each maxillary first molar. Two more helices are placed at the center of the appliance, and these are separated by a V-bend to which is molded an acrylic button the size of a dime. The most mesial portion of this appliance (i.e., the acrylic button) should lie on a line that connects the mesial margins of the maxillary first molars. The button should also be 2- to 5-mm away from the palate. The VHA achieves the treatment objectives by way of an intrusive and distally directed force. The result is intrusion and distal movement of the molars. This is a fixed functional appliance since the forces are achieved from the functional activity of the tongue. In a study conducted at the University of Oklahoma,19 excellent results were achieved using the VHA compared to other methods.
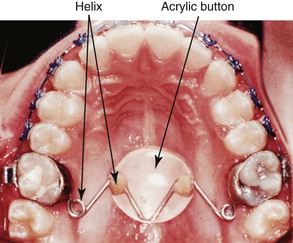
Figure 12-3 Vertical holding appliance (VHA). The first set of helices is positioned distal to the maxillary first molar and the second set is under the acrylic but not inside it. Only the V-bend attaches the 0.040-inch wire to the acrylic.
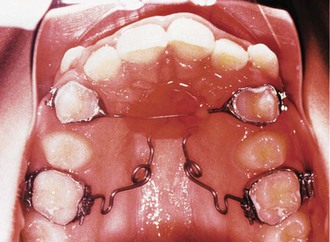
Though initially recommended for use in combination with headgear, we have noted that the VHA on its own is useful for correction of Class II malocclusion. Figure 12-4 documents a patient whose initial treatment plan was for treatment with a straight-pull facebow headgear, but she declined to use it. The patient was put under observation for 6 months while the VHA was cemented to the maxillary first molars. A fixed lingual arch (FLA) was also cemented to the mandibular arch for maintenance of the leeway space. Even though the leeway space may not always be available,19 the FLA can be used to control the vertical dimension during the growth period.20 After 6 months, correction of the Class II malocclusion was observed. No other appliance was used during this period.

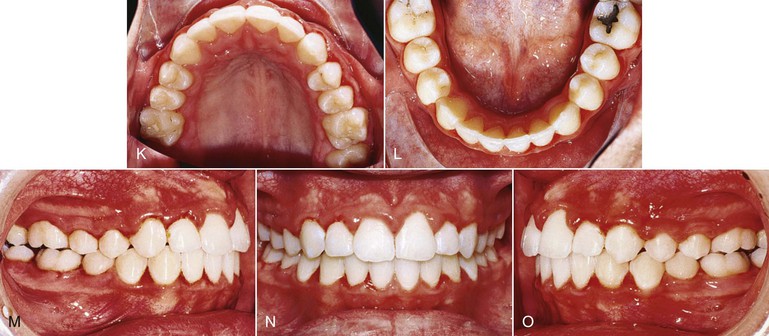
Figure 12-4 Class II, Division 1 malocclusion treated with a vertical holding appliance (VHA). A–E, Pre-treatment intraoral photographs of a Class II, Division 1 subdivision left malocclusion. F–J, Progress photographs showing a VHA cemented to the maxillary first molars and a fixed lingual arch (FLA) cemented to the mandibular first molars. These photographs were taken 6 months after delivery of the VHA and FLA. K–O, Final records at completion of treatment.
Although the forces generated by the VHA have not been measured, measurement of the forces applied to the transpalatal arch (TPA) from the tongue20 suggest that these forces may reach very high levels considering the size of the Nance button to which the 0.040-inch wire is attached. Chiba et al.21 noted that maximum pressure was applied to the TPA during deglutition when the appliance was engaged to the maxillary second molars. Also, this pressure was at its maximum when the TPA was positioned 6-mm from the palate.
Cervical Facebow with Removable Maxillary Plate
Cetlin has proposed the treatment of Class II relationships using a combination of TPAs (Fig. 12-5), cervical headgear, and a removable maxillary plate with auxiliary springs. This treatment modality requires correction of maxillary molar rotations (which in Class II are usually rotated mesiolingually) prior to distal movement and then distalization. The derotation of the molars in a distobuccal direction may produce a space gain of as much as 2- to 3-mm on each side. Once the rotations are corrected, distal movement can be initiated. The distal movement of the maxillary molars is achieved by means of a removable maxillary plate to which is attached some auxiliary springs. The springs deliver a distally directed force of approximately 30 g that is augmented by a cervical-pull facebow headgear with approximately 150 g of force. Once again, the outer bows of the facebow must be positioned such that the side effects from the headgear are minimized. No extrusive forces should be applied when extrusion is not desired, as these will result in opening of the bite from extrusion of the molars and clockwise rotation of the mandible.
Cervical Facebow Headgear
Some studies on molar distalization with cervical facebow headgear have reported negative effects, including extrusion of maxillary first molars, downward anterior tipping of palatal and occlusal planes, posterior rotation of the mandible with resultant steepening of the mandibular plane, and an increase in the anterior lower face height. Many of these clinical studies are of variable duration, some have small patient samples, and some lack information on compliance and usage of the appliance. The credibility of these studies is further compromised by poor documentation of force magnitude, direction of force, duration of force application, physiological age of the patients, and biological response.
Kloehn popularized and reported the successful usage of the cervical facebow headgear.1 He demonstrated in many patients that this was an important and useful method of maxillary molar distalization and correction of Class II molar relation in developing dentitions. Along with the molars, the premolars also drifted distally through the pull of the transseptal fibers. A retrospective study was conducted on the records of patients treated by Dr. John S. Kloehn.22,23 Eighty-five pre- and post-treatment records were selected from 125 patients based on the Class II first molar relationship prior to treatment on the transitional or permanent dentition, nonextraction treatment, and good cooperation. A common treatment protocol that was followed for successful treatment of these patients was alternate adjustment of the outer facebow below or above the line of occlusion every 6 to 12 weeks. The outer bow is bent downward during the first 6 to 12 weeks and then it is bent upward for a period of equal duration. The rationale for this treatment protocol can be appreciated by looking at Figure 12-2, which analyzes the forces and moments applied to the maxillary first molars with each adjustment. With this treatment regimen, there was no change in the anterior face height. However, an average tipping of the palatal plane of 1.5 degrees was observed, an indication of the orthopedic effect of the headgear. It was concluded that the cervical-pull headgear can be used effectively for maxillary molar distalization without detrimental effects. However, patient compliance with the treatment regimen is a serious issue, as social and peer pressures on children make it almost impossible for them to accept the facebow headgear regimen.
Jig
Another appliance that can be used with either patient compliance or patient noncompliance is the jig. The jig can be easily fabricated at chairside and used to correct either bilateral or unilateral Class II, Division 1 malocclusions (Fig. 12-6). In patients with poor compliance, the appliance can be tied in using long nickel-titanium (Ni-Ti) coil springs with an external tubing to minimize patient discomfort. These springs are very small in diameter and do not cause more discomfort than the SAIF springs. The SAIF spring is bulky, compared to the Ni-Ti spring (Fig. 12-7), and it can be tied from the mandibular first or second molar to the maxillary canine hook. Figure 12-6 shows an example of a patient treated with a unilateral jig.

Figure 12-6 Patient with a unilateral Class II, Division 1 malocclusion treated with a jig. The maxillary left canine was blocked out and could not erupt. A–E, Pre-treatment records showing Class II, Division 1 subdivision left. F–J, Final records after 12 months of treatment. No exposure of the unerupted canine was performed and the canine erupted as soon as space was created.

Bimetric (Wilson) Arch
Wilson24 introduced the bimetric arch into the orthodontic literature in 1955 at a time when there was considerable argument between proponents of extraction and of nonextraction with expansion. The appliance consists of a labial arch made of a 0.040-inch posterior section and a 0.020-inch anterior section. Hooks for Class II elastics are soldered onto the anterior end of the 0.040-inch section and an adjustable omega loop is placed in the premolar region of the 0.040-inch section. The appliance is activated by placement of an open coil spring between the omega loop and the maxillary first molar. Continued activation of the appliance can be achieved by opening the omega loop, thereby compressing the open coil against the molar. The bimetric arch, as it would look in the mouth, is shown in Figure 12-8.

With patient compliance, a limitation to the use of the appliance, a Class I molar relationship can be achieved in as little as 6 to 12 weeks.25–27 In a noncompliant patient, side effects can lead to flaring of the incisors.27 Both distal movement and distal tipping of the maxillary molars are observed with the Wilson appliance.25,27 Upon achievement of a Class I relationship, the second premolar can be allowed to drift back and the appliance may not be removed until this relationship is achieved.27 Of importance during the use of Class II elastics is stability of the mandibular molars, which can be achieved in one of three ways: FLA, removable lingual arch (RLA), or lip bumper. The lip bumper has the added advantage of uprighting the mandibular molars and unraveling mandibular anterior crowding, if present.
Fixed Noncompliance Appliances
To overcome the problem of patient compliance, several fixed noncompliance appliances have been introduced, especially during the last two decades. These include the Herbst, Twin Force bite corrector, repelling magnets, pendulum appliance, compressed stainless steel or Ni-Ti springs, Jones jig, and distal jet. The majority of these appliances have been reported to achieve the same amount of molar distalization as the headgear. They also have side effects that need to be considered.
Pendulum Appliance
Hilgers28 introduced an appliance for Class II correction in the noncompliant patient to expand the maxilla and simultaneously rotate and distalize the maxillary first molars. The pendulum appliance provides the clinician with the ability to distalize molars unilaterally and bilaterally. The type of force delivered is continuous and it requires minimal patient cooperation.
The appliance consists of a palatal acrylic button that is about 25-mm in diameter with distalization springs made of 0.032-inch beta-titanium wire that originate from the palatal acrylic and are engaged in lingual sheaths on maxillary first molar bands (Fig. 12-9). It is bonded to the first and second premolars with wires embedded in the acrylic. It needs only a one-time activation of 60 to 70 degrees, producing a force of 230 g per side. It produces a swinging arch, or pendulum of force, from the palate to the molars. A loop within each spring can be adjusted to allow for expansion and prevent any tendency for the maxillary molar to move lingually into a crossbite. Once the molars are distalized, they may be stabilized with a Nance button attached to the maxillary first molars, a headgear, or a fixed appliance, along with a maxillary utility archwire or a stopped continuous archwire. Usually after molar distalization, the second premolar is released from the anchor unit and allowed to drift distally. According to Hilgers,28 it is not unusual to see as much as 5-mm of distal molar movement in 3 to 4 months of treatment with this appliance.
Evaluation of the treatment effects has shown that there is a difference in response between patients with erupting second molars and those with second molars in occlusion. Patients with erupted second molars will experience an extrusion of these teeth with subsequent opening of the bite, which is observed by an increase in the mandibular plane angle, increased lower anterior face height, and a reduced overbite.29,30 Table 12-1 shows some of the results observed from a cephalometric analysis of patients treated with the pendulum appliance. The response differs between individuals with a low and a high mandibular plane angle. In another study, patients in the angle >25 degrees group showed an increase in the lower anterior vertical height (4.13-mm) that was greater than that in the patients in the low and average groups (1.97- and 2.84-mm, respectively).29
TABLE 12-1
Effects of the Pendulum Appliance
mvt, Movement.
Adapted from Ghosh J, Nanda RS. Evaluation of an intraoral maxillary molar distalization technique. Am J Orthod Dentofacial Orthop. 1996;110:639–646.
A common finding in studies that have evaluated the pendulum appliance is distal tipping of the maxillary first molars and anterior tipping of the premolars.29,30 An important side effect of this appliance is undesirable anterior displacement of anterior teeth. However, this appliance presents an effective method for molar distalization with minimal dependence on patient compliance.31 Other advantages include ease of fabrication, one-time activation, adjustment of the springs if necessary to correct minor transverse and vertical molar positions, and patient acceptance. Modifications of the pendulum appliance with removable arms have been introduced.32–34 Such a modified appliance makes it easier to adjust and stabilize the appliance upon completion of molar distal movement.
Distal Jet
Carano and Testa35 first described the distal jet as a fixed lingual appliance that required no compliance from the patient. They claimed that it could produce translatory movement of the maxillary molars in 4 to 6 months.
The original appliance35 has had some modification36,37 and now consists of a bilateral piston and tube arrangement (Fig. 12-10). The tube is embedded in an acrylic palatal button supported by attachments to the first or second premolars. This tube extends distally, adjacent to the palatal tissues and parallel to the occlusal plane, to the first molars. A bayonet wire inserted into the lingual sheath on the first molar bands extends into the tube, much like a piston. A superelastic Ni-Ti open coil spring is placed around this piston and tube arrangement, along with an activation collar used to compress the spring distally. This collar is pushed distally to compress the coil spring once every 4 to 6 weeks during distalization. The mesial set screw in the collar is locked onto the tube with a small Allen wrench in an aluminum handle.
Upon completion of distalization of the molars, the appliance is converted to a palatal holding arch by removing the coil spring (peeling it off the tube with utility pliers) and locking the activation collar over the junction of the tube and piston; the mesial set screw is locked onto the tube and the distal set screw is locked onto the piston, thereby creating a solid support from the first molars to the Nance button. The supporting wire is then sectioned from the premolars and the Nance button with a dental handpiece and a burr.
Other than clinical reports from users of the appliance,36–38 no research has clearly documented the effects of the distal jet. Studies conducted at the University of Oklahoma39,40 revealed that the distal jet was indeed a good tool for distalizing maxillary molars but there could also be anchorage loss during its use, although less than reported for other appliances such as the pendulum. Minimal tipping of the maxillary molars was observed during the treatment period due to the force application near the center of resistance of the maxillary molars. The patients evaluated were in their growth period and some of the distalization achieved was lost during retraction of the anterior teeth. However, this was compensated for by anterior movement of the mandibular molars. Upon completion of distalization of the molars and during the rest of the treatment phase, it is necessary to use some other appliance to hold the molars back.37,38 A Jasper jumper41,42 or a short Twin Force bite corrector6 may serve this purpose well since neither requires compliance by the patient.
Jones Jig Appliance
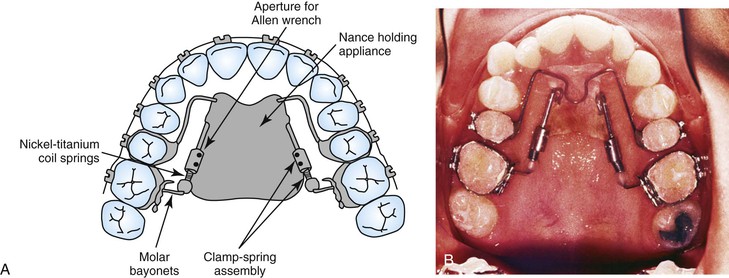
The Jones jig appliance43 is an intraoral noncompliance distalization appliance (Fig. 12-11). It has a modified Nance appliance banded to the second bicuspids, with the Jones jig assemblies tied in place. It consists of a palatal acrylic button of 0.50-inch diameter anchored to the second premolar with a bonded 0.036-inch wire. One arm of the jig fits into a 0.045-inch headgear tube and the second arm fits into a 0.018-inch tube on the first molar. The activation is delivered from the Ni-Ti coil spring tied to the second premolar bracket. The force applied is between 70 and 75 g and average treatment time is 6.35 ± 2.75 months.
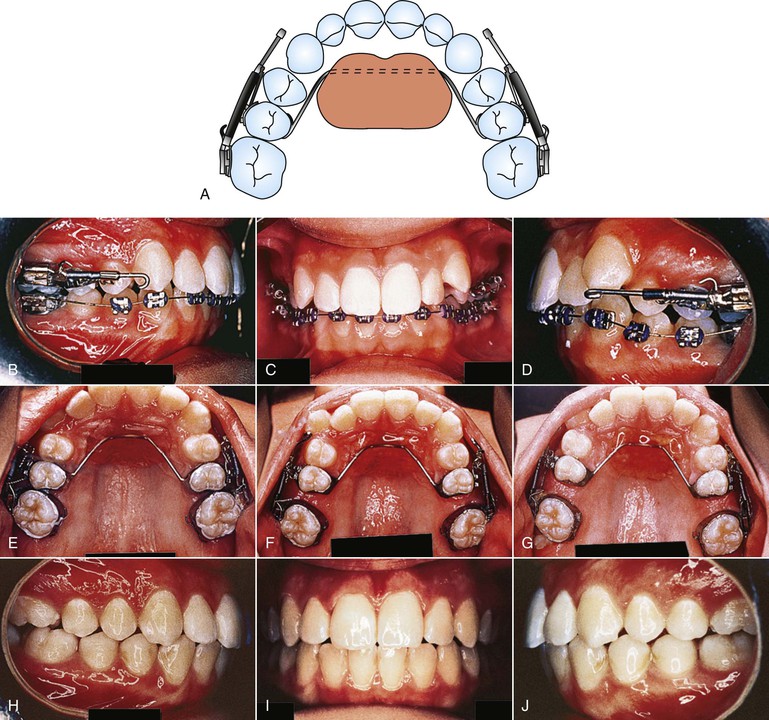
Figure 12-11 Jones jig appliance. A, Schematic of the modified Nance appliance banded to the second bicuspids with the Jones jig assemblies tied into place. B–D, Pre-treatment photographs of a patient with a Class II, Division 1 malocclusion, showing the activated appliance. E-G, Intraoral palatal photographs at (from left to right) initial delivery (0 months), 2 months, and 4 months of appliance activation. H–J, Treatment completion. Total treatment time was 24 months. The majority of the time was spent distalizing the premolars, canines, and incisors.
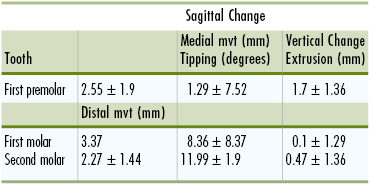
Despite reports of successful correction of Class II malocclusions with the Jones jig, there has been no comprehensive study of molar movement and loss of anchorage during the use of this appliance. To validate its effectiveness, a study was conducted on the patients treated in the office of Dr. Richard Jones, the clinician credited with the design and use of this appliance.44 The sample of 72 patients (26 male and 46 female) was unique. The average age before treatment was 13.8 ± 4.38 years. The results showed molar correction for Class II to Class I malocclusions due primarily to distal movement of the molars. The mean maxillary first molar distal movement was 2.51-mm, with distal tipping of 7.53 degrees. The mean reciprocal mesial movement of the maxillary premolar was 2.0-mm, with mesial tipping of 4.76 degrees. The maxillary first molar extruded 0.14-mm while the maxillary premolar extruded 1.88-mm. The maxillary second molars also moved 2.02-mm and tipped distally 7.89 degrees. Table 12-2 shows the sagittal and vertical movements that accompany the molar distalization procedure with the Jones jig. The changes are highly variable, a factor that should be noted when considering treatment options.
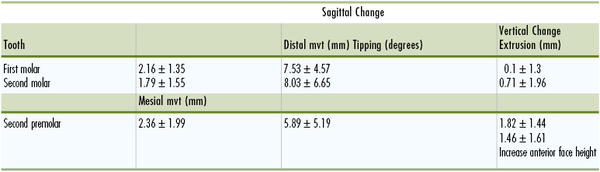
Although the Jones jig appliance can distalize maxillary first molars effectively, it has negative effects on the anchor unit.44,45 Compared to the headgear, however, it has the advantage of accelerated distal molar movement within a short time span.45 Upon completion of distalization, proper anchorage must be used to maintain the molar relationship. Suitable anterior retraction mechanics must be used to achieve this goal. The use of full palatal coverage combined with short Class II elastics to reinforce posterior anchorage could possibly minimize the reciprocal anchorage loss of the molar anchor units during anterior segment retraction. An option that should be considered is nighttime headgear wear, which can be tolerated, especially by the young patient.
Intermaxillary Class II Malocclusion Correction Appliances
Several intermaxillary fixed noncompliant appliances have been proposed and used over the last two decades.6,12,13,41,42,46–48 The advantage of these appliances is that they allow forward displacement of the mandible and a distal force on the maxillary teeth as well as an anterior force on the mandibular dentition. The net result of these three force vectors is correction of a Class II malocclusion. The common disadvantages of intermaxillary appliances are undesirable steepening of the occlusal plane with concomitant flaring of the lower incisors and distal tipping along with extrusion of the maxillary incisors.
Herbst Appliance
The Herbst appliance was developed in the early 1900s and reintroduced by Pancherz46,47 in the mid-1970s. Pancherz showed that a 6-month Herbst treatment in prepeak pubertal patients with a Class II, Division 1 malocclusion resulted in a Class I occlusion relationship. However, he reported that improvement in occlusion was equally due to skeletal and dentoalveolar changes: a Class II molar correction averaging 6.7-mm resulted from a 2.2-mm increase in mandibular length, a 1.8-mm mesial movement of mandibular incisors, and a 2.8-mm distal movement of maxillary molars.
Pancherz and Hägg48 found that sagittal growth at the condyle in patients treated with the Herbst appliance at the peak in pubertal growth was twice that observed in patients treated 3 years before or 3 years after the peak. Other studies49,50 have shown that greater percentages of molar and overjet correction were dentoalveolar in nature in postpubertal patients with greater lower incisor flaring.
Jasper Jumper
Fixed intermaxillary appliances such as the Jasper jumper incorporate active pushing force on the maxillary molars and mandibular dentition. In a clinical study Rankin51 reported greater dentoalveolar effects than skeletal effects. The Class II correction was obtained from mesial movement of lower molars and a significant flaring of the lower incisors. Jasper and McNamara42 concluded that the skeletal and dental components of Class II correction were approximately equal, whereas Weiland and Bantleon41 attributed only 38% of molar correction to skeletal changes. The majority of the studies on this appliance have shown that Class II correction is attributed to a slight increase in mandibular length, a significant posterior movement of the maxillary posterior segments, and proclination of the lower incisors.52,53
Summary
Headgear is perhaps the most useful appliance for maxillary molar distalization if used in the early treatment of Class II malocclusions. Kim et al.5 have shown that the occlusion established early during the growth phase is most likely to be maintained throughout life. Based on this and the premise that children are more compliant before adolescence, the headgear becomes a versatile appliance for treatment of Class II malocclusions. Its effect is twofold: (1) distal movement of the maxillary molars and (2) an orthopedic effect on the maxilla that restrains growth.
Both extraoral and intraoral inter-arch appliances require patient compliance, which may sometimes pose difficulty. Intermaxillary appliances that use the mandibular arch as anchorage may have protrusive effects on the mandibular teeth. All investigations that have evaluated intraoral arch noncompliance appliances for molar distalization have come to surprisingly similar conclusions on the behavior of both the distal segment and the anterior anchor unit. The intramaxillary arch appliances, which have gained in popularity because they do not require patient compliance to distalize molars, show loss of anchorage whereby the premolars move mesially with concomitant protrusion of the maxillary incisors. This suggests that no matter which intraoral appliance is used, it behooves the clinician to avoid round tripping in retraction of maxillary anterior teeth.
It is necessary that the molars are held back with some other form of appliance upon completion of distalization. The use of a Nance palatal arch or TPAs has proven not to resist the anchorage loss during the subsequent retraction of the anterior segment.
References
1. Kloehn SJ. Orthodontics: force or persuasion. Angle Orthod. 1953;23:56–66.
2. Ricketts RM, Bench RW, Gugino CF, Hilgers JJ, Schulhof RJ. Bioprogressive Therapy. Rocky Mountain Orthodontics: Denver, CO; 1979.
3. Cetlin NM, Ten Hoeve A. Nonextraction treatment. J Clin Orthod. 1983;17:396–413.
4. Macho GA. Cephalometric and craniometric age changes in adult humans. Ann Hum Biol. 1986;14:49–61.
5. Kim YE, Nanda RS, Sinha PK. Transition of molar relationships in different skeletal growth patterns. Am J Orthod Dentofacial Orthop. 2002;121:280–290.
6. Campbell E. A prospective clinical trial and mechanical analysis of a push type fixed intermaxillary Class II correction appliance [master's thesis]. University of Connecticut: Storrs, CT; 2003.
7. Kalra V. The K-loop distalizing appliance. J Clin Orthod. 1995;29:298–301.
8. Kingsley NW. Treatise on Oral Deformities. Appleton & Co: New York, NY; 1880.
9. Angle EH. Treatment of Malocclusion of the Teeth. SS White Dental Manufacturing Co: Philadelphia, PA; 1907.
10. Oppenheim A. Biologic orthodontic therapy and reality. Angle Orthod. 1936;6:69–79.
11. Rabbie ABM, Leung FYC, Chayanupatkul A, Hägg U. The correlation between neovascularization and bone formation in the condyle during forward mandibular positioning. Angle Orthod. 2002;72:431–438.
12. Voudouris JC, Woodside DG, Altuna G, Kuftinec MM, Angelopoulos G, Bourque PJ. Condyle–fossa modifications and muscle interactions during Herbst treatment, part 1: new technological methods. Am J Orthod Dentofacial Orthop. 2003;123:604–613.
13. Voudouris JC, Woodside DG, Altuna G, et al. Condyle–fossa modifications and muscle interactions during Herbst treatment, part 2: results and conclusions. Am J Orthod Dentofacial Orthop. 2003;124:13–29.
14. Haack DC, Weinstein S. The mechanics of centric and eccentric cervical traction. Am J Orthod. 1958;44:346–357.
15. Hershey GH, Houghton CW, Burstone CJ. Unilateral face-bows: a theoretical analysis. Am J Orthod. 1981;79:229–249.
16. Contasti GI, Legan HL. Biomechanic guidelines for headgear application. J Clin Orthod. 1982;16:308–312.
17. Wilson MD. Vertical control of maxillary molar position with a palatal appliance [thesis]. Health Sciences Center, University of Oklahoma: Oklahoma City, OK; 1996.
18. DeBerardinis M, Stretesky T, Sinha PK, Nanda RS. Evaluation of the vertical holding appliance in treatment of high-angle patients. Am J Orthod Dentofacial Orthop. 2000;117:700–705.
19. Nanda RS, Chawla JM. Variability of leeway space in Lucknow children. Ind Dental J. 1973;45:99–108.
20. Villalobos FJ, Sinha PK, Nanda RS. Longitudinal assessment of vertical and sagittal control in the mandibular arch by the mandibular fixed lingual arch. Am J Orthod Dentofacial Orthop. 2000;118:366–370.
21. Chiba Y, Motoyoshi M, Namura S. Tongue pressure on loop of transpalatal arch during deglutition. Am J Orthod Dentofacial Orthop. 2003;123:29–34.
22. Hubbard GW. A cephalometric evaluation of non-extraction cervical headgear treatment in Class II malocclusion [thesis]. Health Sciences Center, University of Oklahoma: Oklahoma City, OK; 1992.
23. Hubbard GW, Nanda RS, Currier GF. A cephalometric evaluation of non-extraction cervical headgear treatment in Class II malocclusion. Angle Orthod. 1994;60:359–370.
24. Wilson WL. Variations of labiolingual therapy in Class II cases. Am J Orthod. 1955;41:852–871.
25. Muse DS, Fillman MJ, Emmerson WJ, Mitchell RD. Molar and incisor changes with Wilson rapid molar distalization. Am J Orthod Dentofacial Orthop. 1993;104:556–565.
26. Harnick DJ. Case report: Class II correction using a modified Wilson bimetric distalizing arch and maxillary second molar extraction. Angle Orthod. 1998;68:275–280.
27. Ücem TT, Yüksel S, Okay C, Gülsen A. Effects of a three-dimensional bimetric maxillary distalizing arch. Eur J Orthod. 2000;22:293–298.
28. Hilgers JJ. The pendulum appliance for Class II non-compliance. J Clin Orthod. 1992;26:706–714.
29. Ghosh J, Nanda RS. Evaluation of an intraoral maxillary molar distalization technique. Am J Orthod Dentofacial Orthop. 1996;110:639–646.
30. Bussick TJ, McNamara JA Jr. Dentoalveolar and skeletal changes associated with the pendulum appliance. Am J Orthod Dentofacial Orthop. 2000;117:333–343.
31. Wong AMK, Rabie ABM, Hägg U. The use of pendulum appliance in the treatment of Class II malocclusion. Br Dent J. 1999;187:367–370.
32. Scuzzo G, Pisani F, Takemoto K. Modified molar distalization with a modified pendulum appliance. J Clin Orthod. 1999;33:645–650.
33. Scuzzo G, Takemoto K, Pisani F, Della VS. The modified pendulum appliance with removable arms. J Clin Orthod. 2000;34:244–246.
34. Byloff FK, Kärcher H, Clar E, Stoff F. An implant to eliminate anchorage loss during molar distalization: a case report involving the Graz implant-supported pendulum. Int J Adult Orthodon Orthognath Surg. 2000;15:129–137.
35. Carano A, Testa M. The distal jet for upper molar distalization. J Clin Orthod. 1996;30:374–380.
36. Bowman SJ. Modifications of the distal jet. J Clin Orthod. 1998;32:549–556.
37. Quick AN, Harris AMP. Molar distalization with a modified distal jet appliance. J Clin Orthod. 2000;34:419–423.
38. Bowman SJ. Class II combination therapy (distal jet and jasper jumpers): a case report. J Orthod. 2000;27:213–218.
39. Patel A. Analysis of the distal jet appliance for maxillary molar distalization [thesis]. Health Sciences Center, University of Oklahoma: Oklahoma City, OK; 1999.
40. Ngantung V, Nanda RS. Posttreatment evaluation of the distal jet appliance. Am J Orthod Dentofacial Orthop. 2001;120:178–185.
41. Weiland FJ, Bantleon H. Treatment of Class II malocclusions with the Jasper Jumper appliance—a preliminary report. Am J Orthod Dentofacial Orthop. 1995;108:341–350.
42. Jasper JJ, McNamara JA. The correction of interarch malocclusions using a fixed force module. Am J Orthod Dentofacial Orthop. 1995;108:641–650.
43. Jones RD, White MJ. Rapid Class II molar correction with an open-coil jig. J Clin Orthod. 1992;26:661–664.
44. Brickman CD, Sinha PK, Nanda RS. Evaluation of the Jones jig appliance for distal molar movement. Am J Orthod Dentofacial Orthop. 2000;118:526–534.
45. Haydar S, Üner O. Comparison of Jones jig molar distalization with extraoral traction. Am J Orthod Dentofacial Orthop. 2000;117:49–53.
46. Pancherz H. Treatment of Class II malocclusions by jumping the bite with the Herbst appliance. Acta Odotol Scand. 1980;38:187–200.
47. Pancherz H. The mechanism of Class II correction in Herbst appliance treatment: a cephalometric investigation. Am J Orthod. 1982;82:104–113.
48. Pancherz H, Hägg U. Dentofacial orthopedics in relation to chronologic age, growth period and skeletal development: an analysis of 72 male patients with Class II division 1 malocclusion treated with Herbst appliance. Eur J Orthod. 1988;10:169–176.
49. Croft RS, Buschang PH, English JD, Meyer R. A cephalometric and tomographic evaluation of Herbst treatment in the mixed dentition. Am J Orthod Dentofacial Orthop. 1999;116:435–443.
50. Konik M, Pancherz H, Hansen K. The mechanism of Class II correction in late Herbst treatment. Am J Orthod Dentofacial Orthop. 1997;112:87–91.
51. Rankin T. Correction of Class II malocclusions with a fixed functional appliance [thesis]. University of Connecticut: Storrs, CT; 1990.
52. Cash RG. Adult non-extraction treatment with Jasper Jumper. J Clin Orthod. 1991;25:443.
53. Cope JB. Quantitative evaluation of craniofacial changes with Jasper Jumper therapy. Angle Orthod. 1994;64:113.