Biomechanical Aspects of a Modified Protraction Headgear
Ravindra Nanda
A routine dilemma in the treatment of children with developing Class III malocclusions is the choice of treatment strategy and whether early intervention will be successful in the long-term. Early treatment decisions should be based on several considerations, including genetics and family history; severity of the problem; whether the problem is diagnosed in the midface, mandible, or both; the age of the patient; patient compliance; and growth status of the patient.
The prevalence of children with Class III malocclusion in the United States is relatively small compared to Japan, Korea, and Taiwan. Two studies evaluating the incisor relationship in children have reported an anterior crossbite incidence of 0.8% to 1.0%.1,2 One study reported a Class III molar relationship incidence of 3.8% in high school children.3 However, a Class III malocclusion in a child deserves special attention due to the esthetic, occlusion, function, and psychosocial concerns it raises.
Treatment of developing Class III patients is often based on the orthodontist's expectations of treatment. The parents should be fully informed about the variability of results that can be expected. It is likely wishful thinking to aim to always convert a Class III growth pattern to a Class I growth pattern. The reality is that treatment results range from 100% success to no change at all in the long-term. The degree of success is based on the etiology of the Class III pattern, severity of malocclusion, age and growth status, choice of appliance used, and degree of patient cooperation. Other short-term goals should not be overlooked (i.e., to provide young Class III patients with a functioning occlusion, reduction in severity, and some esthetic improvement during their formative years).
Rationale for Using Protraction Headgear
Delaire et al.4–8 are credited with introducing the concept of protraction headgear to treat Class III malocclusions. Nanda introduced a modified protraction headgear in 1980,9 based on biomechanical concepts.
The rationale for protraction headgear is to apply heavy forces on the midface in order to advance the maxilla anteriorly. In patients with a normal sized mandible and retrusive maxilla, forward displacement of the maxilla is conceptually good. Several studies in the past 3 decades have shown that 25% to 41% of Class III problems in children are primarily the result of a retrognathic maxilla.10–12
The efficacy of protraction headgear is also supported by several studies in primates in the 1970s and 1980s.13–17 These studies, using cephalometrics and histological techniques, showed that treatment with an anterior force on the maxilla is capable of causing disassociation of sutural articulations by a resorption and apposition process at the sutural interfaces. Our own experience has also shown that the direction of midface protraction can be altered by changing the direction and point of delivery of the force.
In recent years noteworthy clinical studies have been reported regarding the use of protraction headgear.18–25 The majority of these studies show an anterior movement of the maxillary dentition, a significant extrusion of the upper molars, anterior displacement of the maxillary dentition, 1- to 3-mm anterior displacement of the maxilla, and a significant rotation of the mandible downward and backward.
A conventional protraction headgear, as described by Delaire et al.,4–8 and its variations use elastics from the molars (or other points at the occlusal plane level) to the facial mask. The interlabial gap and lips limit the ability to change the point of force application to attain predictable movement of the maxilla in the anterior direction.
Nanda9 introduced a modified protraction headgear in 1980, which allowed changes in the direction of force and point of force application on the maxilla as well as the chin. The study showed that use of a modified protraction headgear for 4 to 8 months can displace the maxilla 1- to 3-mm and maxillary dentition 1- to 4-mm. These changes were accompanied by remodeling at the B point, lingual tipping of the mandibular incisors, and downward rotation of the mandible. The cumulative effect of these changes was the correction of the Class III malocclusion. This chapter describes the biomechanical aspects of this headgear, which allows modification of forces in Class III patients to achieve the desired changes, such as in long face and short face Class III patients.
Components of Modified Protraction Headgear
There are two main components of a protraction headgear: intraoral setup and extraoral setup.
Intraoral Components
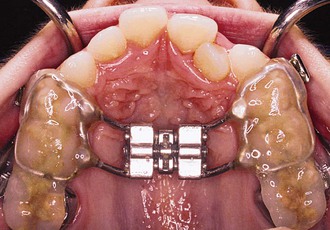
The protraction headgear force is applied via elastics to teeth or other devices supported by teeth and/or the palate. The primary aim is to transmit the force to the midface sutural interfaces. To achieve this, it is important to stabilize the maxilla as one unit (Fig. 16-1). In the primary dentition, it is advisable to use a cemented acrylic occlusal bite block or a removable acrylic plate with occlusal coverage (see Chapter 12). In patients with the mixed dentition and early permanent dentition, a removable acrylic plate (Fig. 16-2) should be used, supported by bands with headgear tubes on the molars or a rigid archwire with a palatal arch. Probably the best stabilization in patients with maxillary first molars is provided by a fixed rapid palatal expansion (RPE) device (Fig. 16-3). We prefer a Hyrax type of nonbonded device, as bonded RPEs (Fig. 16-4) interfere with the primary exfoliating teeth or teeth in the eruptive phase. Studies have also indicated that a simultaneous sutural expansion with an RPE at the start of protraction headgear treatment facilitates the anterior movement of the maxilla.19,20,26,27
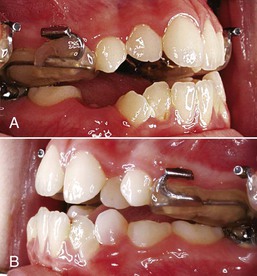
Figure 16-1 A, Left and (B) right lateral views of an intraoral stabilization appliance. An acrylic bite block includes a heavy archwire to which a headgear tube is soldered. The bite block provides disocclusion to facilitate forward displacement of the maxilla and is cemented to posterior maxillary teeth.

Figure 16-2 Occlusal view of a removable intraoral stabilization appliance. The acrylic plate has a clasp that fits on a molar tube of a cemented band. This plate must be worn when the protraction appliance is in use.

Extraoral Components
The extraoral components (Fig. 16-5) of a modified protraction headgear have two parts. The first is a facemask and the second is an intraoral-to-extraoral connecting force device that uses a modified headgear bow instead of intraoral elastics.

Figure 16-5 Complete modified protraction headgear device. It includes a facemask, a modified inner bow of a headgear, and elastics.
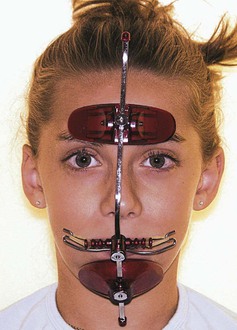
Commonly used facemasks have chin and forehead support connected by a heavy metal arch that has a horizontal bar for attachment of a force module. The forehead and chin supports are adjustable. The horizontal bar also must be adjustable vertically to vary the point of force attachment (Figs. 16-6 and 16-7).

Figure 16-6 Lateral view of a patient with the appliance shown in Figure 16-5 in place. The outer bow of the headgear is attached to the center bar of the facemask. The point of attachment on the mask can be moved up or down and the outer bow can be similarly positioned to achieve the desirable line of force.
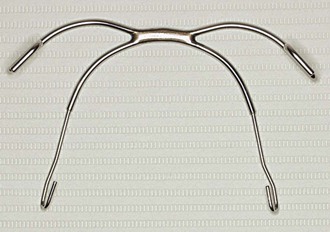
A conventional headgear bow with a standard outer and inner bow without loops can be easily converted into a modified bow for use with the facemask. It is important that the molar band has a headgear tube. In cemented acrylic stabilization devices, a headgear tube can be embedded in acrylic.
To construct a reverse headgear bow (Fig. 16-8), a U-shaped horizontal bend is made in such a way that it can be inserted into the molar tubes from the distal side. Anteriorly, the bow should clear the incisors and should be between the upper and lower lips. The outer bow is modified to make a hook in the premolar area in such a way that elastics can be attached to the horizontal bar of the facemask. The vertical position of the outer bow is adjusted to deliver the necessary force for a predictable maxillary displacement.
Protraction Headgear Force System
The following four components of force systems are important for proper adjustments of the protraction headgear.
Magnitude of Force
Hickory and Nanda28 showed in an in vitro study of 2-day-old rat cranial sutures that very small forces (0.2 to 0.6 g) applied with wire springs are capable of generating cellular activity along with an increase in the suture width. In human studies, the force values used for protraction of the maxilla have ranged from 200 to 800 g. Most of the studies give no rationale for the magnitude of the force selected and in clinical practice the force used is often based on anecdotal experience.
Indeed, there have been no prospective studies to determine the optimal force to protract the maxilla. However, based on clinical experience, studies in the literature, and sutural morphology changes related to age progression, certain observations regarding the desirable magnitude of force can be made.
The sutural articulations in children are simple; interdigitations interlock more with age. A clear example is the midpalatal suture. The suture remains patent long after growth is complete but it becomes difficult to open with an RPE after the age of 15 to 16 years due to the complex interlocking of sutures. Conversely, in adolescents, midpalatal suture opening is very simple and can be accomplished with minimal tipping of the posterior teeth. A protraction force on the maxilla needs “disarticulation” at numerous sutures (Fig. 16-9), most notably zygomaticomaxillary, pterygopalatine, and nasomaxillary sutures of the midface. With age, these sutures become not only more mechanically intertwined, but also more tortuous in their orientation. Also, for the maxilla to advance forward in each affected suture, numerous areas of resorption and apposition must take place due to their tortuous nature, quite unlike the midpalatal suture.
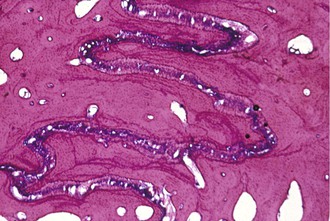
Figure 16-9 Histological photograph of an area of zygomaticomaxillary suture of a Macaca nemestrina monkey subjected to an anterior protraction force. Note the tortuous nature of the suture with areas of stress and strain and resting lines.
Thus the sutural anatomy and age of the patient play a major role in determining the amount of force needed to bring the maxilla forward with protraction forces. For preadolescent patients (5 to 8 years), a force of 200 to 250 g on each side is adequate and for early adolescent patients (8 to 11 years), a force of 300 to 450 g on each side may be desirable. In late adolescent patients (12 years and up), higher forces (450 to 600 g) can be used but, in our experience, protraction of the midface in the latter group is minimal. It is advisable to start with lower force values that can be increased if needed, especially in late adolescent patients.
Direction and Point of Force Application
Direction of the applied force is one of the most important force components for anterior displacement of the maxilla. Nanda17 varied the point of force application in primates and showed that by changing the line of force on the midface, the center of rotation of the maxilla could be altered. Later, Nanda and Hickory16 speculated, based on different centers of rotation created by varying the line of protraction force, that the center of resistance of the midface is probably 5- to 10-mm below the orbitale on the zygomatic bone. Later, Tanne et al.29,30 reported that the center of resistance of the maxilla was located between the root tip of the maxilla first and second premolars. Miki31 agreed with the previous two authors but added that, in the vertical direction, the center of resistance of the midface was between the orbitale and the distal root apex of the first maxillary molars. Hata et al.32 and Lee et al.33 studied the effects of changing the level of force application on dried skulls and confirmed the findings of Nanda17 in primates. They reported that a line of force 5-mm above the palatal plane and 15-mm above the occlusal plane did not result in counterclockwise movement of the maxilla and dentition.
Keles et al.34 studied the effects of varying the force direction on maxillary orthopedic protraction in two groups of patients. The first group received protraction headgear with a force applied by intraoral elastics and the second group received a force applied with a modified protraction headgear as described above.9 The authors reported that in the first group the maxilla rotated counterclockwise (Fig. 16-10), resulting in downward and backward rotation of the mandible, while in the second group an anterior translation of the maxilla with no to minimal mandibular rotation occurred. This important study showed that predictable changes can be achieved in the direction of maxillary advancement with desired or without undesirable mandibular changes.
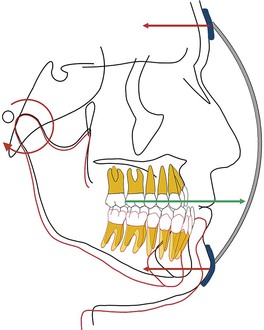
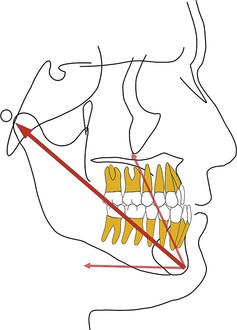
Figure 16-10 Force diagram of a protraction headgear device using intraoral elastics to deliver force. Note the clockwise moment on the midface and dentition resulting in a downward and backward rotation of the mandible.
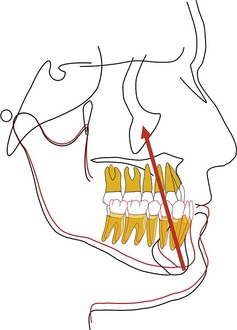
By changing the point of force attachment on the facemask or outer bow of the headgear, the vertical dimension of the face can be very nicely controlled. This is especially important in Class III patients with a long vertical dimension and a steep mandibular plane. Similarly, in Class III patients with a flat mandibular plane and a deep bite, a force below the level of the occlusal plane may be more desirable to rotate the mandible downward and backward (see Fig. 16-10). A line of force closer to the center of resistance of the midface will deliver a translatory force (Fig. 16-11) and a line of force closer to the occlusal plane has a rotational force (Fig. 16-12).
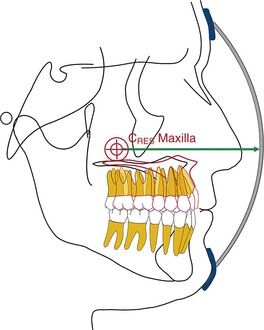
Figure 16-11 Schematic representation of a line of force through the center of resistance (CRES) of the maxilla, which will result in a translatory movement of the maxilla. The precise location of the CRES of the midfacial bones is difficult to locate but most studies point to the area 5- to 10-mm below the orbitale.
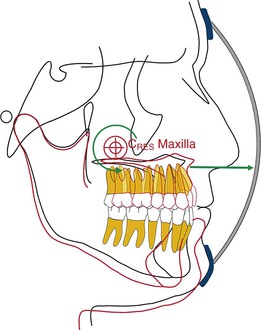
Figure 16-12 Force diagram showing the nature of the maxillary and mandibular change when the point of force application is at the level of the root apices of the maxillary teeth. CRES, Center of resistance.
The force delivered by the protraction facemask on the chin is almost a “forgotten” force and is very rarely mentioned in the literature. An anterior force on the midface applies equal and opposite force on the forehead and chin (see Fig. 16-10). The direction of the force on the chin is distal and almost in a straight line, which can also cause a rotation of the mandible downward and backward. In Class III long faced patients, a vertical pull chin cap (Fig. 16-13) can be added to minimize the undesirable forces on the chin. A chin cap is especially desirable in Class III patients with a long vertical dimension and open-bite tendency (Fig. 16-14).
Duration of Force
The majority of clinical studies recommend use of a protraction headgear for anywhere from 3 to 12 months. Patient compliance beyond 6 months is difficult. Also, the older the patient, the less cooperative he or she will be. In our clinic, use of a protraction headgear is stopped after 6 months. In some cases, if necessary after an observation period, patients are asked to use the headgear again for 3 to 4 months.
The daily wear time also depends on the age of the patient. In preadolescent patients, 10 to 12 hours of use per day is sufficient. In adolescent patients, it may be necessary to increase the wear time from 12 to 16 hours per day. The latter group may have problems with compliance.
Force Constancy
The force is applied with elastics from the outer bow of the headgear to the facemask. The elastic force should be measured at the beginning to determine the desired force level. Patients should be instructed to use fresh elastics as much as possible.
 Case Reports 1 and 2
Case Reports 1 and 2
Two patient examples are presented. The first patient is unique because a decision was made to extract four premolars after protraction headgear use (Fig. 16-15). Clinical photographs are shown for the second patient 6 years after protraction (Fig. 16-16). In both patients a modified protraction headgear was used and the point of attachment and line of force were changed at various times during the protraction period.
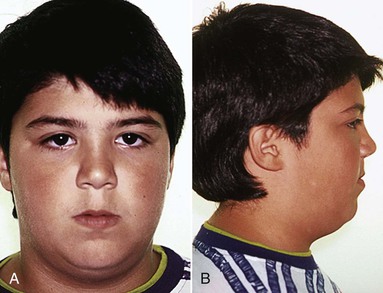
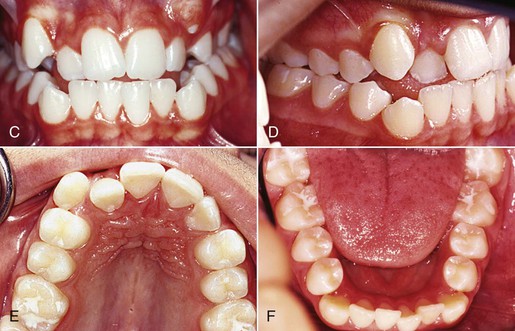
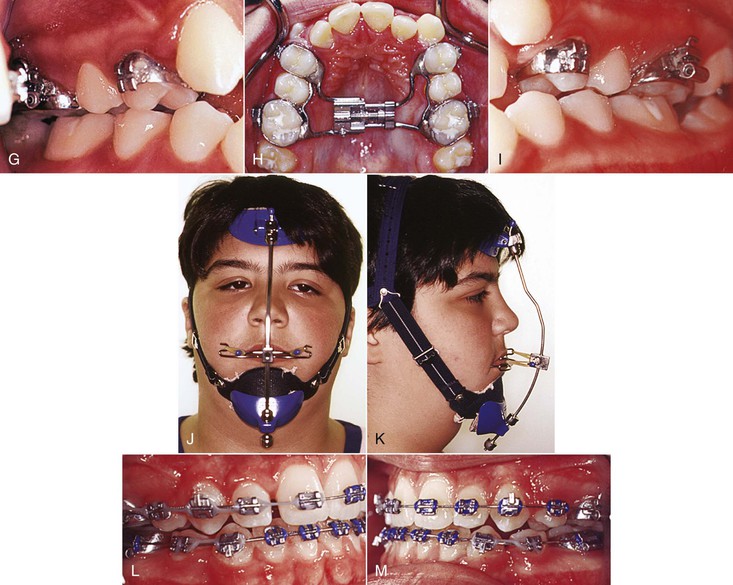
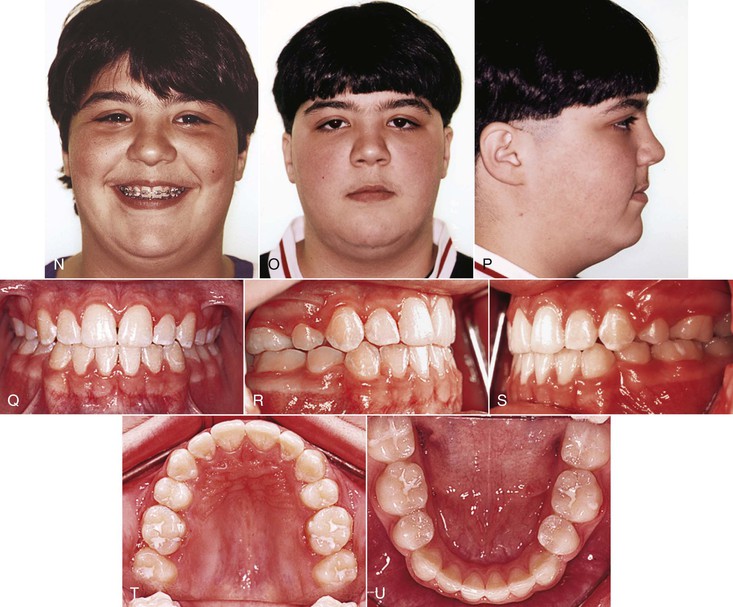
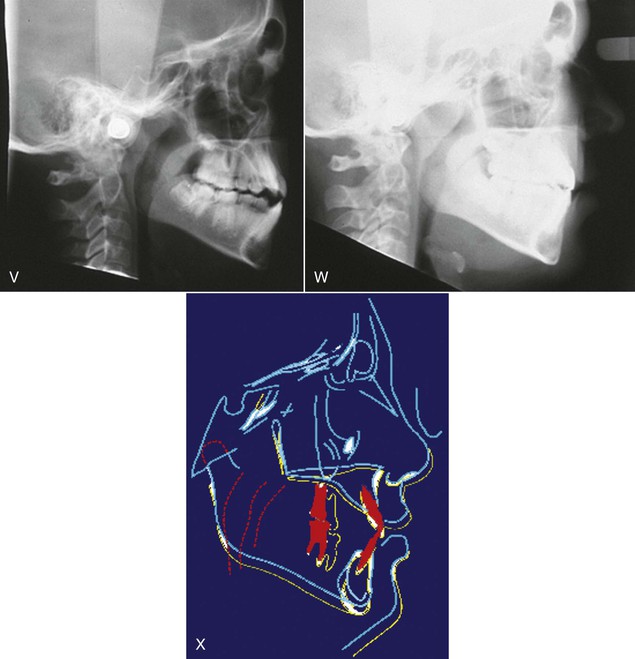
Figure 16-15 A–F, Frontal and lateral facial and intraoral views of an adolescent patient determined to have a developing Class III malocclusion after a careful examination of dental, facial, and family history findings and a cephalometric analysis. C and D, Edge-to-edge anterior bite and skeletal maxillary constriction. E and F, Intraoral view of upper and lower arches. G–I, Intraoral view showing a rapid palatal expansion (RPE) appliance at the end of the maxillary expansion. J and K, Frontal and lateral extraoral views with the protraction headgear in place. The chin cap component is added during the active RPE phase to prevent any extrusion of the maxillary posterior teeth. L and M, Lateral intraoral views and (N) frontal view with smile after extraction of the four first premolars and completion of the space closure. Protraction headgear was used for 6 months prior to the extractions. O–U, Facial and intraoral views at the end of the treatment. V, Before and (W) after cephalograms and (X) superimposition tracings showing cumulative changes over a 3-year treatment period.
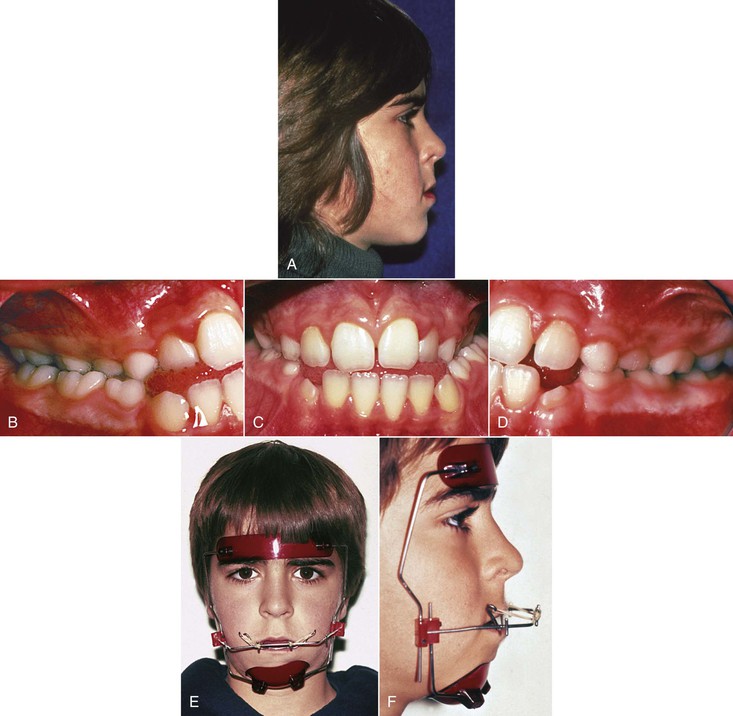
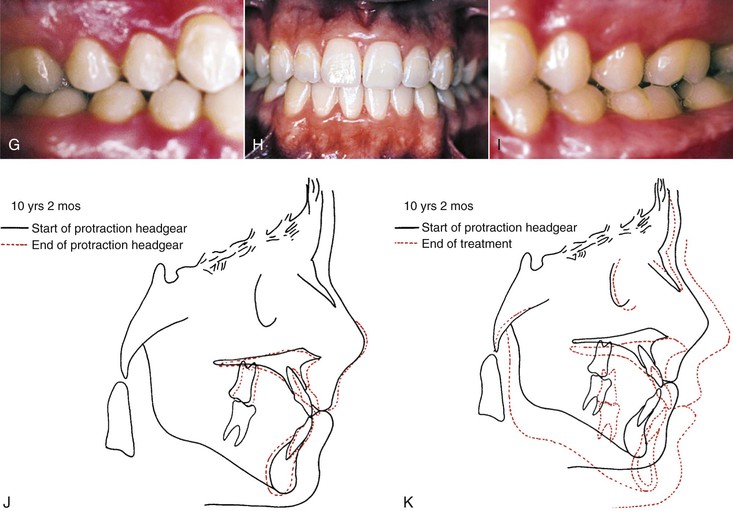
Figure 16-16 A–D, Extraoral and intraoral views of a developing Class III malocclusion in an early adolescent patient. E and F, Extraoral frontal and lateral views of the protraction headgear appliance in place. Note that the line of force in this patient is at the level of the root apices of the maxillary teeth. The line of force was adjusted at various times during the 6-month protraction headgear application to achieve the desired results. G–I, Intraoral views of the dentition 6 years following the application of the protraction headgear and 3 years into the retention period. J, Cephalometric superimposition tracings of the patient at the end of the protraction headgear period. K, Six years after the end of protraction. Note the amount of maxillary and mandibular growth.
References
1. Kelly JE, Sanchez M, Van Kirk LE. An Assessment of the Occlusion of the Teeth of Children. [DHEW Publication No (HRA) 74-1612] National Center for Health Statistics: Washington, DC; 1973.
2. Proffit WR, Fields HW, Moray LJ. Prevalence of malocclusion and orthodontic treatment need in the United States: estimates from the N-HANES III survey. Int J Adult Orthod Orthogn Surg. 1998;13:97–106.
3. Mills LF. Epidemiologic studies of occlusion IV: the prevalence of malocclusion in a population of 1,455 school children. J Dent Res. 1966;45:332–336.
4. Delaire J. Confection du masque orthopedique. Rev Stomat Paris. 1971;72:579–584.
5. Delaire J. La croissance maxillaire. Trans Eur Orthod Soc. 1971;81–102.
6. Delaire J. L’articulation fronto-maxillaire: bases theoretiques et principles generaux d’application de forces extra-orales postero-anterieures sur masque orthopedique. Rev Stomat Paris. 1976;77:921–930.
7. Delaire J, Verdon P, Lumineau JP, Cherga-Negrea A, Talmant J, Boisson M. Note de tecnique. Rev Stomatol. 1972;73:633–642.
8. Delaire VJ, Verdon P, Floor J. Moglichkeiten und Grenzen Extraoraler Kratie in Postereo-anterior Richtung unter Verwandung der Orthopadischen Maske. Forsch Keiferorthop. 1978;39:27–45.
9. Nanda R. Biomechanical and clinical considerations of a protraction headgear. Am J Orthod. 1980;78:125–139.
10. Dietrich UC. Morphological variability of skeletal Class III relationships as revealed by cephalometric analysis. Trans Eur Orthod Soc. 1970;46:131–140.
11. Guyer EC, Ellis E, McNamara JA Jr, Behrents RG. Components of Class III malocclusion in juveniles and adolescents. Angle Orthod. 1986;56:7–30.
12. Williams S, Andersen CE. The morphology of the potential Class III skeletal pattern in the growing child. Am J Orthod. 1986;89:302–311.
13. Dellinger EL. A preliminary study of anterior maxillary displacement. Am J Orthod. 1973;63:509–516.
14. Jackson GW, Kokich VG, Shapiro PA. Experimental and postexperimental response to anteriorly directed extraoral force in young Macaca nemestrina. Am J Orthod. 1979;75:318–333.
15. Kambara T. Dentofacial changes produced by extraoral forward force in the Macaca irus. Am J Orthod. 1977;71:249–277.
16. Nanda R, Hickory W. Zygomaticomaxillary suture adaptations incident to anteriorly-directed forces in rhesus monkeys. Angle Orthod. 1984;54:199–210.
17. Nanda R. Protraction of maxilla in rhesus monkeys by controlled extraoral forces. Am J Orthod. 1978;74:121–141.
18. Baccetti T, Franchi L, McNamara JA Jr. Treatment and post-treatment craniofacial changes following rapid maxillary expansion and facial mask therapy. Am J Orthod Dentofacial Orthop. 2000;118:404–411.
19. Baccetti T, McGill JS, Franchi L, McNamara JA Jr, Tollaro I. Skeletal effects of early treatment of Class III malocclusion with maxillary expansion and face-mask therapy. Am J Orthod Dentofacial Orthop. 1998;113:333–343.
20. MacDonald KE, Kapust AJ, Turley PK. Cephalometric changes after correction of Class III malocclusion with maxillary expansion/facemask therapy. Am J Orthod Dentofacial Orthop. 1999;116:13–24.
21. McGill JS, McNamara JA Jr. Treatment and post-treatment effects of rapid maxillary expansion and facial mask therapy. [Monograph 36, Craniofacial Growth Series] McNamara JA Jr. Growth Modification: What Works, What Doesn't and Why. Center for Human Growth and Development, University of Michigan: Ann Arbor, MI; 1999.
22. Ngan P, Hägg U, Yiu C, Merwin D, Wei SH. Treatment response to maxillary expansion and protraction. Eur J Orthod. 1996;18:151–168.
23. Ngan P, Yiu C, Hu A, Hägg U, Wei SH, Gunel E. Cephalometric and occlusal changes following maxillary expansion and protraction. Eur J Orthod. 1998;20:237–254.
24. Pangrazio-Kulbersh V, Berger J, Kersten G. Effects of protraction mechanics on the midface. Am J Orthod Dentofacial Orthop. 1998;114:484–491.
25. Turley PK. Orthopedic correction of Class III malocclusion with palatal expansion and custom protraction headgear. J Clin Orthod. 1988;22:314–325.
26. Ngan P, Hägg U, Yiu C, Wei H. Treatment response and long-term dentofacial adaptations to maxillary expansion and protraction. Semin Orthod. 1997;3:255–264.
27. Shanker S, Ngan P, Wade D, et al. Cephalometric A point changes during and after maxillary protraction and expansion. Am J Orthod Dentofacial Orthop. 1996;110:423–430.
28. Hickory WB, Nanda R. Effect of tensile force magnitude on release of cranial suture cells into S phase. Am J Orthod Dentofacial Orthop. 1987;91:328–334.
29. Tanne K, Hiraga J, Kakiuchi K, Yamagata Y, Sakuda M. Biomechanical effect of anteriorly directed extraoral forces on the craniofacial complex: a study using the finite element method. Am J Orthod Dentofacial Orthop. 1989;95:200–207.
30. Tanne K, Sakuda M. Biomechanical and clinical changes of the craniofacial complex from orthopedic maxillary protraction. Angle Orthod. 1991;61:145–152.
31. Miki M. An experimental research on the directional of the complex by means of the external force: two dimensional analysis on the sagittal plane of the craniofacial skeleton. J Tokyo Dent Coll. 1979;79:1563–1597.
32. Hata S, Itoh T, Nakagawa M, et al. Biomechanical effects of maxillary protraction on the craniofacial complex. Am J Orthod. 1987;91:305–311.
33. Lee K, Ryu Y, Park Y, Rudolph D. A study of holographic interferometry on the initial reaction of maxillofacial complex during protraction. Am J Orthod. 1997;111:623–632.
34. Keles A, Erverdi N, Sezen S. Bodily distalization of molars with absolute anchorage. Angle Orthod. 2003;73:471–482.