Evidence-Based Assessment

Ellen K. is a 23-year-old, white, unemployed woman who entered a substance abuse treatment program because of numerous drug-related driving offenses (Fig. 1-1).

1-1
After Ellen’s admission, the examiner collected a health history and performed a complete physical examination. The actual preliminary list of significant findings looked like this:
• High school academic record strong (A−/B+) in first 3 years, grades fell senior year but did graduate
• Alcohol abuse, started age 16, heavy daily usage × 3 years prior to admission (PTA), last drink 4 days PTA
• Smoked 2 packs per day (PPD) × 2 years, prior use 1 PPD × 4 years
• Elevated blood pressure (BP); 142/100 mm Hg at end of examination today
• Diminished breath sounds, with moderate expiratory wheeze and scattered rhonchi at both bases
• Grade ii/vi systolic heart murmur, left lower sternal border
• Resolving hematoma, 2 to 3 cm, right (R) infraorbital ridge
• Missing R lower first molar, gums receding on lower incisors, multiple dark spots on all teeth
• Well-healed scar, 28 cm long × 2 cm wide, R lower leg, with R leg 3 cm shorter than left (L), sequela of auto accident age 12
• Altered nutrition—omits breakfast, daily intake has no fruits, no vegetables, eats meals at fast-food restaurants most days
• Oral contraceptives for birth control × 3 years, last pelvic examination 1 year PTA
• Unemployed × 6 months, previous work as cashier, bartender
• History of physically abusive relationship with boyfriend, today has orbital hematoma as a result of being hit; states, “It’s OK, I probably deserved it.”
• History of sexual abuse by father when Ellen was 12 to 16 years of age
• Relationships—estranged from parents, no close women friends, only significant relationship is with boyfriend of 2 years whom Ellen describes as physically abusive and alcoholic
The examiner analyzed and interpreted all the data; clustered the information, sorting out which data to refer and which to treat; and identified the diagnoses. It is interesting to note how many significant findings are derived from data the examiner collected. Not only physical data but also cognitive, psychosocial, and behavioral data are significant for an analysis of Ellen’s health state. Also, the findings are interesting when considered from a life-cycle perspective; that is, Ellen is a young adult who normally should be concerned with the developmental tasks of emancipation from parents, building an independent lifestyle, establishing a vocation, making friends, forming an intimate bond with another, and establishing a social group.
A body of clinical evidence has validated the importance of using the assessment techniques in Ellen’s case. For example, measuring BP screens for hypertension and early intervention here wards off heart attack and stroke. Listening to breath sounds screens (in Ellen’s case) for asthma, which is compounded by her smoking. Listening to heart sounds yields Ellen’s heart murmur, which could be “innocent” or a sign of a structural abnormality in a heart valve—further examination will tell. The physical examination is not just a rote formality. Its parts are determined by the best clinical evidence available and documented in the professional literature.
Assessment—Point of Entry in an Ongoing Process
Assessment is the collection of data about the individual’s health state. Throughout this text, you will be studying the techniques of collecting and analyzing subjective data (i.e., what the person says about himself or herself during history taking) and objective data (i.e., what you as the health professional observe by inspecting, percussing, palpating, and auscultating during the physical examination). Together with the patient’s record and laboratory studies, these elements form the database.
From the database, you make a clinical judgment or diagnosis about the individual’s health state or response to actual or risk health problems and life processes, as well as diagnoses about higher levels of wellness. Thus the purpose of assessment is to make a judgment or diagnosis.
An organized assessment is the starting point of diagnostic reasoning. Because all health care diagnoses, decisions, and treatments are based on the data you gather during assessment, it is paramount that your assessment be factual and complete.
Diagnostic Reasoning
The step from data collection to diagnosis can be a difficult one. Most beginning examiners perform well in gathering the data, given adequate practice, but then treat all the data as being equally important. This makes decision making slow and labored.
Diagnostic reasoning is the process of analyzing health data and drawing conclusions to identify diagnoses. Novice examiners most often use a diagnostic process involving hypothesis forming and deductive reasoning. This hypothetico-deductive process has four major components: (1) attending to initially available cues; (2) formulating diagnostic hypotheses; (3) gathering data relative to the tentative hypotheses; and (4) evaluating each hypothesis with the new data collected, thus arriving at a final diagnosis. A cue is a piece of information, a sign or symptom, or a piece of laboratory data. A hypothesis is a tentative explanation for a cue or a set of cues that can be used as a basis for further investigation.
For example, consider Ellen K., the case study presented at the beginning of this chapter. Ellen presents with a number of initial cues, one of which is the resolving hematoma under her eye. (1) You can recognize this cue even before history taking begins. Is it significant? (2) Ellen says she ran into a door, although she mumbles as she speaks and avoids eye contact. At this point, you formulate a hypothesis of trauma. (3) During the history and physical examination, you gather data to support or reject the tentative hypothesis. (4) You synthesize the new data collected, which support the hypothesis of trauma but eliminate the accidental cause. The final diagnoses are resolving right orbital contusion and risk for trauma.
Once you complete data collection, develop a preliminary list of significant signs and symptoms and all patient health needs. This is less formal in structure than your final list of diagnoses will be and is in no particular order. (Such a list for Ellen is found on p. 1.)
Cluster or group together the assessment data that appear to be causal or associated. For example, with a person in acute pain, associated data are rapid heart rate and anxiety. Organizing the data into meaningful clusters is slow at first; experienced examiners cluster data more rapidly because they recall proven results of earlier patient situations and recognize the same patterns in the new clinical situation.9
Validate the data you collect to make sure they are accurate. As you validate your information, look for gaps in data collection. Be sure to find the missing pieces, because identifying missing information is an essential critical-thinking skill. How you validate your data depends on experience. If you are unsure of the blood pressure, validate it by repeating it yourself. Eliminate any extraneous variables that could influence BP results, such as recent activity or anxiety over admission. If you have less experience analyzing breath sounds or heart murmurs, ask an expert to listen. Even with years of clinical experience, some signs always require validation (e.g., a breast lump).
Critical Thinking and the Diagnostic Process
The standards of practice in nursing, traditionally termed the nursing process, include six phases: assessment, diagnosis, outcome identification, planning, implementation, and evaluation.2 This is a dynamic, interactive process; in today’s complex clinical setting, practitioners move back and forth within the steps (Fig. 1-2).
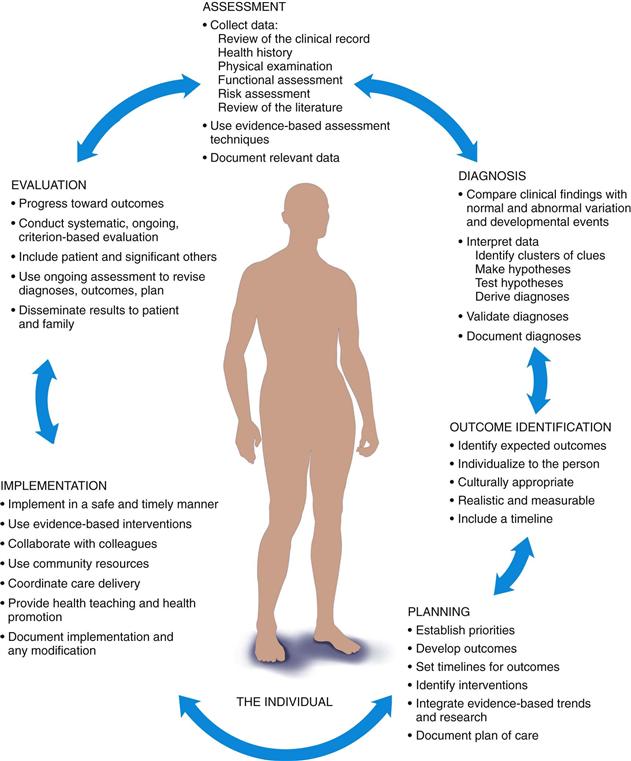
1-2
Although the nursing process is a problem-solving approach, the way in which we apply the process depends on our level and time of experience. The novice has no experience with a specified patient population and uses rules to guide performance. It takes time, perhaps 2 to 3 years in similar clinical situations to achieve competency, in which you see actions in the context of arching goals or daily plans for patients. With more time and experience, the proficient nurse understands a patient situation as a whole rather than as a list of tasks. At this level, you can see long-term goals for the patient and how today’s interventions apply to the point you want the patient to be in, say, 6 weeks. Finally, it seems that expert nurses vault over the steps and arrive at a clinical judgment in one leap. The expert has an intuitive grasp of a clinical situation and zeroes in on the accurate solution.4
Functioning at the level of expert in clinical judgment includes using intuition—that is, knowledge received as a whole. Intuition is characterized by immediate recognition of patterns—expert practitioners learn to attend to a pattern of assessment data and act without consciously labeling it. Whereas the beginner operates more from a set of defined, structured rules, the expert practitioner uses intuitive links, has the ability to see salient issues in a patient situation, and knows instant therapeutic responses.5 The expert has a storehouse of experience about which interventions have been successful in the past.
For example, compare the actions of the nonexpert and the expert nurse in the following situation of a young man with Pneumocystis jiroveci (P. carinii) pneumonia:
He was banging the siderails, making sounds, and pointing to his endotracheal tube. He was diaphoretic, gasping, and frantic. The nurse put her hand on his arm and tried to ascertain whether he had a sore throat from the tube. While she was away from the bedside retrieving an analgesic, the expert nurse strolled by, hesitated, listened, went to the man’s bedside, re-inflated the endotracheal cuff, and accepted the patient’s look of gratitude because he was able to breathe again. The nonexpert nurse was distressed that she had misread the situation. The expert reviewed the signs of a leaky cuff with the nonexpert and pointed out that banging the siderails and panic help differentiate acute respiratory distress from pain.11
The method of moving from novice to becoming an expert practitioner is through the use of critical thinking. We all start as novices, when we need the familiarity of clear-cut rules to guide actions. Critical thinking is the means by which we learn to assess and modify, if indicated, before acting.
Critical thinking is required for sound diagnostic reasoning and clinical judgment. During your career, you will need to sort through vast amounts of data and information in order to make the sound judgments to manage patient care. These data will be dynamic, unpredictable, and ever changing. There will not be any one protocol you can memorize that will apply to every situation.
The following critical-thinking skills are organized in a logical progression of the ways the skills might be used in the nursing process.1 Although each skill here is described separately, they are not used that way in the clinical area. Rather than a step-by-step linear process, critical thinking is a multidimensional thinking process. With experience, you will be able to apply these skills in a rapid, dynamic, and interactive way. For now, follow Ellen’s case study through the steps.
1. Identifying assumptions. That is, recognize that you could take information for granted or see it as fact when actually there is no evidence for it. Ask yourself, What am I taking for granted here? For example, in Ellen’s situation, you might have assumptions of a “typical profile” of a person with alcohol abuse, based on your past experience or exposure to media coverage. However, drug abuse affects people of all ages and from all walks of life; the facts of Ellen’s situation are unique.
2. Identifying an organized and comprehensive approach to assessment. This depends on the patient’s priority needs and your personal or institutional preference. Ellen has many problems, but at her time of admission, she is not acutely physically ill. Thus you may use any organized format for assessment that is feasible for you: a head-to-toe approach, a body systems approach (e.g., cardiovascular, gastrointestinal), a regional area (e.g., pelvic examination), or the use of a preprinted assessment form developed by the hospital or clinic.
3. Validation, or checking the accuracy and reliability of data. For example, in addictions treatment, a clinician will corroborate data with a family member in order to verify the accuracy of Ellen’s history. In Ellen’s particular case, her significant others are absent or nonsupportive and the corroborative interview may need to be with a social worker.
4. Distinguishing normal from abnormal when identifying signs and symptoms. Spotting abnormal signs and symptoms leads to problem identification. At first it is difficult to discriminate abnormal signs and symptoms versus what is expected for the patient’s age, gender, culture, and lifestyle. However, your ease will grow with study, practice, and experience. Increased BP, wheezing, and heart murmur are among the many abnormal findings in Ellen’s case.
5. Making inferences or hypotheses. This involves interpreting the data and deriving a correct conclusion about the health status. This presents a challenge for the beginning examiner, because it needs a baseline amount of knowledge and experience. Is Ellen’s increased BP caused by the stress of admission or a chronic condition? Is the heart murmur innocent or caused by heart valve pathology?
6. Clustering related cues, which will help you see relationships among the data. For example, heavy alcohol use, social consequences of alcohol use, academic consequences, and occupational consequences are a clustering of cues that suggest a maladaptive pattern of alcohol use.
7. Distinguishing relevant from irrelevant. A complete history and physical examination furnish a vast amount of data. Look at the clusters of data, and consider which data are important for a health problem or a health promotion need. This skill is also a challenge for beginning examiners and one area where a clinical mentor can be invaluable.
8. Recognizing inconsistencies. When Ellen gives the explanation that she ran into a door (subjective data), it is at odds with the location of the infraorbital hematoma (objective data). With this kind of conflicting information, you can investigate and further clarify the situation.
9. Identifying patterns. This helps fill in the whole picture and discover missing pieces of information. You need to know usual function of the heart, characteristics of innocent murmurs, and risk factors for abnormal or pathologic murmurs in order to decide if the systolic murmur is a problem for Ellen.
10. Identifying missing information, gaps in data, or a need for more data to make a diagnosis. Ellen will need more interviewing regarding any increasing tolerance to alcohol, any withdrawal signs or symptoms, and laboratory data regarding liver enzymes and blood count in order to name a diagnosis.
11. Promoting health by identifying risk factors. This applies to generally healthy people and concerns disease prevention and health promotion. To accomplish this skill, you need to identify and manage known risk factors for the individual’s age-group and cultural status. This will drive your wellness diagnosis. For example, counseling for injury prevention is an important intervention for Ellen because motor vehicle and other unintentional injuries are a leading cause of death for this age-group.
12. Diagnosing actual and potential (risk) problems from the assessment data. A full list of diagnoses (both medical and nursing) is derived from Ellen K.’s health history and physical examination and is found in Chapter 27. The biomedical focus is the diagnosis and treatment of the specific agents or pathogens that cause disease. Assessment factors are a list of biophysical symptoms and signs. The person is certified as healthy when these symptoms and signs have been eliminated. When disease does exist, medical diagnoses are worded to identify and explain the cause of disease.
Nursing diagnoses are clinical judgments about a person’s response to an actual or potential health state. The most recently approved North American Nursing Diagnosis Association (NANDA) 2009-2011 list includes (1) actual diagnoses, existing problems that are amenable to independent nursing interventions; (2) risk diagnoses, potential problems that an individual does not currently have but is particularly vulnerable to developing; and (3) wellness diagnoses, which focus on strengths and reflect an individual’s transition to a higher level of wellness. Throughout this book, appropriate diagnoses from this list are presented and developed as they pertain to related content in each chapter. In Chapter 27, “The Complete Health Assessment,” the list of findings for Ellen K. is analyzed and rewritten as diagnoses.
Regarding Ellen’s case study, the medical diagnosis is used to evaluate the etiology (cause) of disease. The nursing diagnosis is used to evaluate the response of the whole person to actual or potential health problems. For example, both the admitting nurse and later the physician auscultate Ellen’s lung sounds and determine that they are diminished and that wheezing is present. This is both a medical and a nursing clinical problem. The physician listens to diagnose the cause of the abnormal sounds (in this case, asthma) and to order specific drug treatment. The nurse listens to detect abnormal sounds early, to monitor Ellen’s response to treatment, and to initiate supportive measures and teaching; for example, the nurse may teach Ellen which behavioral measures may help her quit smoking and may recommend that Ellen initiate a walking program.
The medical and nursing diagnoses should not be seen as isolated from each other. It makes sense that the medical diagnosis of asthma be reflected in the nursing diagnoses, as interpreted by the nurse’s knowledge of the person’s response to asthma. In this book, common nursing diagnoses are presented along with medical diagnoses to illustrate common abnormalities. Please observe how these two types of diagnoses are interrelated.
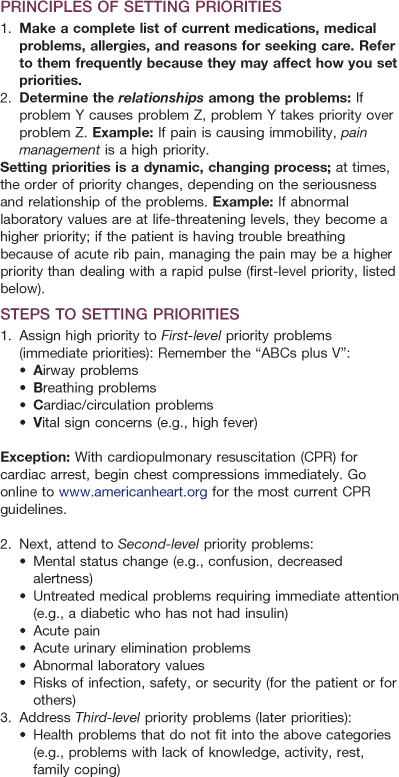
13. Setting priorities when there is more than one diagnosis. In the hospitalized, acute care setting, the initial problems are usually related to the reason for admission. However, the acuity of illness often determines the order of priorities of the person’s problems (Table 1-1).
For example, first-level priority problems are those that are emergent, life threatening, and immediate, such as establishing an airway or supporting breathing.
Second-level priority problems are those that are next in urgency—those requiring your prompt intervention to forestall further deterioration, for example, mental status change, acute pain, acute urinary elimination problems, untreated medical problems, abnormal laboratory values, risks of infection, or risk to safety or security. Ellen has abnormal physical signs that fit in the category of untreated medical problems. For example, Ellen’s adventitious breath sounds are a cue to further assess respiratory status to determine the final diagnosis. Ellen’s mildly elevated blood pressure needs monitoring also.
Third-level priority problems are those that are important to the patient’s health but can be addressed after more urgent health problems are addressed. In Ellen’s case, the data indicating diagnoses of Deficient Knowledge, Dysfunctional Family Processes, and Chronic Low Self-Esteem fit in this category. Interventions to treat these problems are more long-term, and the response to treatment is expected to take more time.
Collaborative problems are those in which the approach to treatment involves multiple disciplines. Collaborative problems are certain physiologic complications in which nurses have the primary responsibility to diagnose the onset and monitor the changes in status.7 For example, the data regarding alcohol abuse represent a collaborative problem. With this problem, the sudden withdrawal of alcohol has profound implications on the central nervous and cardiovascular systems. During detoxification, Ellen’s response to the rebound effects of these systems is managed.
14. Identifying patient-centered expected outcomes. What specific, measurable results will you expect that will show an improvement in the person’s problem after treatment? The outcome statement should include a specific time frame. For example: After 5 days, Ellen will demonstrate how to manage balanced nutrition by keeping a food diary and by stating which food groups are present/absent in her diet.
15. Determining specific interventions that will achieve your outcomes. These interventions aim to prevent, manage, or resolve health problems. This is the health care plan. For specific interventions, state who should perform the intervention, when and how often, and the method used.
16. Evaluating and correcting thinking. Look at the expected outcomes, and apply them for evaluation. Do the stated outcomes match the individual’s actual progress? Then, analyze whether your interventions were successful or not. Continually think, “What could I be doing differently or better?”
17. Determining a comprehensive plan and evaluating and updating the plan. Record the revised plan of care and keep it up-to-date. Communicate the plan to the multidisciplinary team. Be aware that this is a legal document and that accurate recording is important for evaluation, insurance reimbursement, and research.
Evidence-Based Assessment
Does honey help burn wounds heal more quickly? Is St. John’s wort effective in relieving the symptoms of major depression? Does male circumcision reduce the risk of transmitting human immunodeficiency virus (HIV) in heterosexual men? Can magnesium sulfate reduce cerebral palsy risk in premature infants? Can infusing hearts with stem cells help heal tissue damage after a heart attack?
Health care is a rapidly changing field. The amount of medical and nursing information available today has skyrocketed. Current efforts of cost containment result in a hospital population composed of people who have increased acuity and an earlier discharge than in the past. Clinical research studies are continuously pushing the field forward. Keeping up with these advances and translating them into practice are very challenging. Budget cuts, staff shortages, and increasing patient acuity mean that the clinician has little time to grab a lunch break, let alone browse the most recent journal articles for advances in a clinical specialty.
However, all patients deserve to be treated with the most current best-practice techniques. It is this conviction that led to the development of evidence-based practice (EBP). In 1972, a British epidemiologist and early proponent of EBP, Archie Cochrane, identified a pressing need for systematic reviews of randomized clinical trials. In a landmark case, Dr. Cochrane noted multiple clinical trials published between 1972 and 1981 showing that the use of corticosteroids to treat women in premature labor reduced the incidence of infant mortality. A short course of corticosteroid stimulates fetal lung development, thus preventing respiratory distress syndrome, a serious and common complication of premature birth. Yet these findings had not been implemented into daily practice and thousands of low-birth-weight premature infants were needlessly dying. Following a systematic review of the evidence in 1989, obstetricians were finally aware that the corticosteroid treatment was so effective. Corticosteroid treatment has since been shown to reduce the risk of infant mortality by 30% to 50%.8
EBP is more than the use of best-practice techniques to treat patients. “EBP is a systematic approach to practice that emphasizes the use of best evidence in combination with the clinician’s experience, as well as the patient preferences and values, to make decisions about care and treatment”13 (Fig. 1-3). This definition is comprehensive and holistic. Note how clinical decision making depends on all four factors: the best evidence from a critical review of research literature; the patient’s own preferences; the clinician’s own experience and expertise; and finally, physical examination and assessment. Assessment skills must be practiced with hands-on experience and refined to a high level.
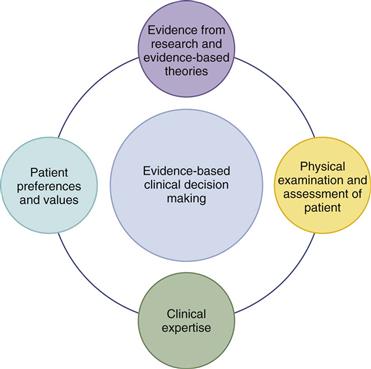
1-3
Although assessment skills are foundational to EBP, it is important to question tradition when no compelling research evidence exists to support it. Some time-honored assessment techniques have dropped out of the examination repertoire because clinical evidence has shown them to be less than useful. For example, the traditional practice of auscultating bowel sounds was found to not be the best indicator of returning gastrointestinal (GI) motility in patients having abdominal surgery.14 This research team first reviewed earlier studies suggesting that early postoperative bowel sounds probably do not represent the return of normal GI motility and therefore listening to the abdomen is not useful in this situation. Research did show the primary markers for returning GI motility after abdominal surgery to be the return of flatus and the first postoperative bowel movement. The Madsen team instituted a new practice protocol and monitored patient outcomes to check if discontinuing the auscultation of bowel sounds was detrimental to abdominal surgery patients. Detrimental outcomes did not occur; the new practice guideline was shown to be safe for patients’ recovery and a better allocation of staff time.
Despite the advantages to patients who receive care based on EBP, it often takes up to 17 years for research findings to be implemented into practice.3 This troubling gap has led researchers to examine closely the barriers to EBP, both as individual practitioners and as organizations. As individuals, nurses lack research skills in evaluating quality of research studies, are isolated from other colleagues knowledgeable in research, and lack confidence to implement change.10 More significant barriers are the organizational characteristics of health care settings. Nurses lack time to go to the library to read research; health care institutions have inadequate library research holdings; and organizational support for EBP is lacking when nurses wish to implement changes in patient care.10 Fostering a culture of EBP at the undergraduate and graduate levels is one way in which health care educators are attempting to make evidence-based care the “gold standard” of practice. Students of medicine and nursing are now taught how to filter through the wealth of scientific data and critique their findings. They are learning to discern which interventions would best serve their individual patients. Facilitating support for EBP at the organizational level includes time to go to the library; teaching to conduct electronic searches; journal club meetings; establishing nursing research committees; linking staff with university researchers; and ensuring adequate research journals and preprocessed evidence resources available in the library.10 “Without the ability to deliver EBP within a context of caring that embraces compassion, cultural sensitivity, and respect for patients and their families, healthcare would fall painfully short of its ultimate goal of providing safe, effective, and holistic care that meets the bio/psycho/social needs of its consumers.”16
Collecting Four Types of Data
Every examiner needs to establish four different types of databases depending on the clinical situation: complete, focused or problem-centered, follow-up, and emergency.
1 Complete (Total Health) Database
This includes a complete health history and a full physical examination. It describes the current and past health state and forms a baseline against which all future changes can be measured. It yields the first diagnoses.
In primary care, the complete database is collected in a primary care setting, such as a pediatric or family practice clinic, independent or group private practice, college health service, women’s health care agency, visiting nurse agency, or community health agency. When you work in these settings, you are the first health professional to see the patient and have primary responsibility for monitoring the person’s health care. This is the opportunity to build and strengthen your relationship with the patient. For the well person, this database must describe the person’s health state, perception of health, strengths or assets such as health maintenance behaviors, individual coping patterns, support systems, current developmental tasks, and any risk factors or lifestyle changes. For the ill person, the database also includes a description of the person’s health problems, perception of illness, and response to the problems.
For well and ill people, the complete database must screen for pathology as well as determine the ways people respond to that pathology or to any health problem. You must screen for pathology because you are the first, and often the only, health professional to see the patient. You will screen for pathology in order to refer the patient to another professional, to help the patient make decisions, and to perform appropriate treatments. But this database also notes the human responses to health problems. This factor is important because it provides additional information about the person that leads to nursing diagnoses.
In acute hospital care, the complete database also is gathered after admission to the hospital. In the hospital, data related specifically to pathology may be collected by the admitting physician. You will collect additional information on the patient’s perception of illness, functional ability or patterns of living, activities of daily living, health maintenance behaviors, response to health problems, coping patterns, interaction patterns, and health goals. This approach completes the database from which the nursing diagnoses are made.
2 Focused or Problem-Centered Database
This is for a limited or short-term problem. Here, you collect a “mini” database, smaller in scope and more targeted than the complete database. It concerns mainly one problem, one cue complex, or one body system. It is used in all settings—hospital, primary care, or long-term care. For example, 2 days after surgery, a hospitalized person suddenly has a congested cough, shortness of breath, and fatigue. The history and examination focus primarily on the respiratory and cardiovascular systems. Or, in an outpatient clinic, a person presents with a rash. The history and examination follow the direction of this presenting concern, such as whether the rash had an acute or chronic onset, was associated with a fever, and was localized or generalized. History and examination must include a clear description of the rash.
3 Follow-Up Database
The status of any identified problems should be evaluated at regular and appropriate intervals. What change has occurred? Is the problem getting better or worse? What coping strategies are used? This type of database is used in all settings to follow up short-term or chronic health problems.
4 Emergency Database
This calls for a rapid collection of the data, often compiled concurrently with lifesaving measures. Diagnosis must be swift and sure. For example, in a hospital emergency department, a person is brought in with suspected substance overdose. The first history questions are “What did you take?,” “How much did you take?,” and “When?” The person is questioned simultaneously while his or her airway, breathing, circulation, level of consciousness, and disability are being assessed. Clearly, the emergency database requires more rapid collection of data than the episodic database.
Expanding the Concept of Health
Assessment is the collection of data about an individual’s health state. A clear idea of health is important because this determines which assessment data should be collected. In general, the list of data that must be collected has lengthened as our concept of health has broadened.
Consideration of the whole person is the essence of holistic health. Holistic health views the mind, body, and spirit as interdependent and functioning as a whole within the environment. Health depends on all these factors working together. The basis of disease is multifaceted, originating both from within the person and from the external environment. Thus the treatment of disease requires the services of numerous providers. Nursing includes many aspects of the holistic model—the interaction of the mind and body, the oneness and unity of the individual. Both the individual human and the external environment are open systems, dynamic and continually changing and adapting to each other. Each person is responsible for his or her own personal health state and an active participant in health care. Health promotion and disease prevention form the core of nursing practice.
In a holistic model, assessment factors are expanded to include such things as culture and values, family and social roles, self-care behaviors, job-related stress, developmental tasks, and failures and frustrations of life. All are significant to health.
Health promotion and disease prevention now round out our concept of health. Guidelines to prevention emphasize the link between health and personal behavior. The report of the U.S. Preventive Services Task Force19 asserts that the great majority of deaths among Americans younger than 65 years are preventable. Prevention can be achieved through counseling from primary care providers designed to change people’s unhealthy behaviors related to smoking, alcohol and other drug use, lack of exercise, poor nutrition, injuries, and sexually transmitted infections. This is a wider, more dynamic concept of health. Health promotion is a set of positive acts we can take. In this model, the focus of the health professional is on teaching and helping the consumer choose a healthier lifestyle.
The frequency interval of assessment varies with the person’s illness and wellness needs. Most ill people seek care because of pain or some abnormal signs and symptoms they have noticed. This prompts an assessment—gathering a complete, a focused, or an emergency database (Fig. 1-4). In addition, risk assessment and preventive services can be delivered in this context, once the presenting concerns are addressed

1-4
But for the well person, opinions are inconsistent about assessment intervals. The term annual checkup is vague. What does it constitute? Is it necessary or cost-effective? How can primary care clinicians deliver preventive services to persons with no signs and symptoms of illness? Routine health checkups are an excellent opportunity to deliver preventive services. Although routine health checkups could induce unnecessary costs and promote non-recommended services, advocates justify well-person visits because of delivery of some recommended preventive services and reduction of patient worry.6
The Guide to Clinical Preventive Services is a positive approach to health assessment and risk reduction.19 The Guide is updated annually and is accessible online or in print. It presents evidence-based, gold standard recommendations on screening, counseling, and preventive topics and includes clinical considerations for each topic. These services include screening factors to gather during the history, age-specific items for physical examination and laboratory procedures, counseling topics, and immunizations. This approach moves away from an annual physical ritual and toward rational and varying periodicity. Health education and counseling are highlighted as the means to deliver health promotion and disease prevention.
For example, the guide to examination for Ellen K. (23-year-old female, nonpregnant, sexually active, tobacco user) would be recommended to include the following services for preventive health care:
1. Screening history for dietary intake, physical activity, tobacco/alcohol/drug use, and sexual practices
2. Physical examination for height and weight, blood pressure, and screening for cervical cancer, chlamydia, HIV, and other sexually transmitted infections
3. Counseling for tobacco use and interventions and for alcohol misuse and behavioral intervention
5. Healthy diet counseling including lipid disorder screening and obesity screening
6. Chemoprophylaxis to include multivitamin with folic acid (females capable of or planning pregnancy)
7. Type 2 diabetes mellitus screening for those with sustained BP over 135/80 mm Hg
Obviously, Ellen’s individual health problems demand immediate intervention and preclude a strict adherence to this preventive list. Indeed, many of Ellen’s findings are seen as “red flags” based on predictable risk factors from this list. Ellen will need a complete history, physical examination, and laboratory studies.
 Culture and Genetics
Culture and Genetics
In a holistic model of health care, assessment factors must include culture. An introduction to cross-cultural concepts follows in Chapter 2. These concepts are developed throughout the text as they relate to specific chapters.
Metaphors such as melting pot, mosaic, and salad bowl have been used to describe the cultural diversity that characterizes the United States. According to the U.S. Census Bureau, close to 50% of the population of the United States will consist of people from diverse racial, ethnic, and cultural groups by the year 2050. Emerging minority is a term that has been used to classify the populations that are rapidly becoming a combined numerical majority.17
The population of the United States surpassed 310 million people in the autumn of 2010; about 1 in 8 people was an immigrant, and about 1 in 3 U.S. residents was part of a group other than single-race non-Hispanic white according to national estimates by race, Hispanic origin, and age released by the Census Bureau. The nation’s emerging majority population totaled 98 million, or 33%, of the country’s total population. Hispanics are the largest and fastest growing group.
If current demographic trends continue, the following population diversity is expected in the United States in the twenty-first century: Hispanics, 24.3%; Blacks, 13.2%; Asian/Pacific Islander, 8.9%; and American Indian, 0.8%.18 Hispanic and Asian populations are expected to double between now and 2050. It is expected that by 2040, the white, European majority will be a numerical minority population.
In the beginning of the twenty-first century, there is a steady flow of immigrants and refugees into the United States. Because the United States is sometimes perceived as the center of advanced health care and technology, foreign nationals who return home after treatment have been inflating the census reports at many U.S. hospitals, with the more popular types of U.S. interventions being cardiovascular, neurologic, and cancer treatments. For example, 35% of kidney transplant recipients at some U.S. hospitals have come from other countries. At the same time, U.S. health care providers go abroad to work in a wide variety of health care settings in the international community. Medical and nursing teams volunteer to provide free medical and surgical care in developing countries (Fig. 1-5). International interchanges are increasing among nurses and physicians, making attention to the cultural aspects of health and illness an even greater priority.
1-5
During your professional career, you may be expected to assess short-term foreign visitors, international university faculty, students from abroad studying in U.S. high schools and universities, family members of foreign diplomats, immigrants, refugees, members of more than 106 different ethnic groups, and American Indians from 510 federally recognized tribes. A serious conceptual problem exists in that nurses and physicians are expected to know, understand, and meet the health needs of people from culturally diverse backgrounds without any formal preparation for doing so.
The inclusion of CULTURE in health assessment is important to gather data that are accurate and meaningful and to intervene with culturally sensitive and appropriate care. Members of some cultural groups are demanding culturally relevant health care that incorporates their specific beliefs and practices. An increasing expectation exists among members of certain cultural groups that health care providers will respect their “cultural health rights,” an expectation that frequently conflicts with the unicultural Western biomedical world view taught in U.S. educational programs that prepare nurses and other health care providers. “Cultural malpractice” may soon become a recognized phenomenon.
Given the multicultural composition of the United States and the projected increase in the number of individuals from diverse cultural backgrounds anticipated in the future, a concern for the cultural beliefs and practices of people is becoming increasingly important.
Bibliography
1. Alfaro-LeFevre R. Critical thinking and clinical judgment: a practical approach. 4th ed. St. Louis: Saunders; 2009.
2. American Nurses Association. Nursing scope and standards of performance and standards of clinical practice. Washington, DC: American Nurses Publishing; 2004.
3. Balas EA, Boren SA. Managing clinical knowledge for health care improvements. In: Bemmel J, McCray AT, eds. Yearbook of medical informatics 2000. Stuttgart, Germany: Schattauer; 2000.
4. Benner P, Tanner CA, Chesla CA. Expertise in nursing practice. New York: Springer; 1996.
5. Benner P, Tanner CA, Chesla CA. Becoming an expert nurse. American Journal of Nursing. 1997;97 16BBB-16DDD.
6. Boulware LE, Marinopoulos S, Phillips KA. Systematic review: The value of the periodic health evaluation. Annals Internal Medicine. 2007;146(4):289–300.
7. Carpenito-Moyet L. Nursing diagnosis: application to clinical practice. 10th ed. Philadelphia: Lippincott Williams & Wilkins; 2004.
8. Cochrane Collaboration. Accessed May 10, 2009, from www.cochrane.org; 2009.
9. Coderre S, Mandin H, Harasym PH, et al. Diagnostic reasoning strategies and diagnostic success. Medical Education. 2003;37(8):695–703.
10. DiCenso A, Guyatt G, Ciliska D. Evidence-based nursing: A guide to clinical practice. St. Louis: Mosby; 2005.
11. Hanneman SK. Advancing nursing practice with a unit-based clinical expert. Image. 1996;28(4):331–337.
12. Hunter A, Denman-Vitale S, Garzon L. Global infections: Recognition, management and prevention. Nurse Practitioner. 2007;32(2):34–41.
13. Leufer TC. Evidence-based practice: Improving patient outcomes. Nursing Standard. 2009;23(32):35–39.
14. Madsen D, Sebolt T, Cullen L, et al. Listening to bowel sounds: An evidence-based practice project. American Journal of Nursing. 2005;105(12):40–50.
15. McKenna HP, Ashton S, Keeney S. Barriers to evidence-based practice in primary care. Journal of Advanced Nursing. 2004;45(2):178–189.
16. Melnyk BM, Fineout-Overholt E. Evidence-based practice in nursing & healthcare. Philadelphia: Lippincott Williams & Wilkins; 2005.
16a. Melnyk BM, Fineout-Overholt E, Stillwell SB, et al. The seven steps of evidence-based practice. American Journal of Nursing. 2010;110(1):51–53.
17. Spector RE. Cultural diversity in health and illness. Upper Saddle River, NJ: Prentice Hall; 2004.
17a. Stillwell SB, Fineout-Overholt E, Melnyk BM, et al. Asking the clinical question: A key step in evidence-based practice. American Journal of Nursing. 2010;110(3):58–61.
17b. Throckmorton T, Windle PE. Evidence-based case management practice Part 1: The systemic review. Professional Case Management. 2009;14(2):76–81.
18. U.S. Bureau of the Census. General population characteristics. Washington, DC: U.S. Government Printing Office; 2000; Website www.census.gov; 2000.
19. U.S. Preventive Services Task Force (USPSTF). Guide to clinical preventive services, 2009. Accessed August 17, 2010, from www.ahrq.gov/clinic/prevenix.htm; 2009.