Mental Status Assessment
Components of the Mental Status Examination
Thought Processes and Perceptions
Supplemental Mental Status Examination
Summary Checklist: Mental Status Assessment

http://evolve.elsevier.com/Jarvis/
• Bedside Assessment Summary Checklist
• Physical Examination Summary Checklist
Structure and Function
Defining Mental Status
Mental status is a person’s emotional (feeling) and cognitive (knowing) function. Optimal functioning aims toward simultaneous life satisfaction in work, in caring relationships, and within the self. Mental health is relative and ongoing. Everyone has “good” days and “bad” days. Usually, mental status strikes a balance, allowing the person to function socially and occupationally.
The stress surrounding a traumatic life event (death of a loved one, serious illness) tips the balance, causing transient dysfunction. This is an expected response to a trauma. Mental status assessment during a traumatic life event can identify remaining strengths and can help the individual mobilize resources and use coping skills.
A mental disorder is apparent when a person’s response is much greater than the expected reaction to a traumatic life event. A mental disorder is defined as a significant behavioral or psychological pattern that is associated with distress (a painful symptom) or disability (impaired functioning) and has a significant risk of pain, disability, or death or a loss of freedom.2 Mental disorders include organic disorders (due to brain disease of known specific organic cause [e.g., delirium, dementia, alcohol and drug intoxication and withdrawal]) and psychiatric mental illness (in which an organic etiology has not yet been established [e.g., anxiety disorder or schizophrenia]). Mental status assessment documents a dysfunction and determines how that dysfunction affects self-care in everyday life.
Mental status cannot be scrutinized directly like the characteristics of skin or heart sounds. Its functioning is inferred through assessment of an individual’s behaviors:
Consciousness: Being aware of one’s own existence, feelings, and thoughts and aware of the environment. This is the most elementary of mental status functions.
Language: Using the voice to communicate one’s thoughts and feelings. This is a basic tool of humans, and its loss has a heavy social impact on the individual.
Mood and affect: Both of these elements deal with the prevailing feelings; affect is a temporary expression of feelings or state of mind, and mood is more durable, a prolonged display of feelings that color the whole emotional life.
Orientation: The awareness of the objective world in relation to the self.
Attention: The power of concentration, the ability to focus on one specific thing without being distracted by many environmental stimuli.
Memory: The ability to lay down and store experiences and perceptions for later recall. Recent memory evokes day-to-day events; remote memory brings up years’ worth of experiences.
Abstract reasoning: Pondering a deeper meaning beyond the concrete and literal.
Thought process: The way a person thinks, the logical train of thought.
Thought content: What the person thinks—specific ideas, beliefs, the use of words.
Perceptions: An awareness of objects through the five senses.
 Developmental Competence
Developmental Competence
Infants and Children
Emotional and cognitive functioning mature progressively from simple reflex behavior into complex logical and abstract thought. It is difficult to separate and trace the development of just one aspect of mental status. All aspects are interdependent. For example, consciousness is rudimentary at birth because the cerebral cortex is not yet developed; the infant cannot distinguish the self from the mother’s body. Consciousness gradually develops along with language so that by 18 to 24 months, the child learns that he or she is separate from objects in the environment and has words to express this. We also can trace language development: from the differentiated crying at 4 weeks, the cooing at 6 weeks, through one-word sentences at 1 year to multi-word sentences at 2 years. Yet the concept of language as a social tool of communication occurs around 4 to 5 years of age, coincident with the child’s readiness to play cooperatively with other children.
Attention gradually increases in span through preschool years so that by school age, most children are able to sit and concentrate on their work for a period of time. Some children are late in developing concentration. School readiness coincides with the development of the thought process; around age 7 years, thinking becomes more logical and systematic and the child is able to reason and understand. Abstract thinking, the ability to consider a hypothetical situation, usually develops between ages 12 and 15 years, although a few adolescents never achieve it.
The Aging Adult
The aging process leaves the parameters of mental status mostly intact. There is no decrease in general knowledge and little or no loss in vocabulary. Response time is slower than in youth; it takes a bit longer for the brain to process information and react to it. Thus performance on timed intelligence tests may be lower for the aging person—not because intelligence has declined, but because it takes longer to respond to the questions. The slower response time affects new learning; if a new presentation is rapidly paced, the older person does not have time to respond to it.4
Recent memory, which requires some processing (e.g., medication instructions, 24-hour diet recall, names of new acquaintances), is somewhat decreased with aging. Remote memory is not affected.
Age-related changes in sensory perception can affect mental status. For example, vision loss (as detailed inChapter 14) may result in apathy, social isolation, and depression. Hearing changes are common in older adults (see the discussion of presbycusis inChapter 15). Age-related hearing loss involves high-frequency sounds. Consonants are high-frequency sounds, so older people who have difficulty hearing them have problems with normal conversation. This problem produces frustration, suspicion, and social isolation and makes the person look confused.
The era of older adulthood contains more potential for loss than do earlier eras, such as loss of loved ones, loss of job status and prestige, loss of income, and loss of an energetic and resilient body. Also, living with chronic diseases (heart failure, cancer, diabetes, osteoporosis) includes the fear of loss of life itself. The grief and despair surrounding these losses can affect mental status. These losses can result in disorientation, disability, or depression.
Components of the Mental Status Examination
The full mental status examination is a systematic check of emotional and cognitive functioning. The steps described here, however, rarely need to be taken in their entirety. Usually, you can assess mental status through the context of the health history interview. During that time, keep in mind the four main headings of mental status assessment:
Integrating the mental status examination into the health history interview is sufficient for most people. You will collect ample data to be able to assess mental health strengths and coping skills and to screen for any dysfunction.
It is necessary to perform a full mental status examination when you discover any abnormality in affect or behavior, and in the following situations:
• Patients whose initial brief screening suggests an anxiety disorder or depression.
• Family members concerned about a person’s behavioral changes, such as memory loss, inappropriate social interaction.
• Brain lesions (trauma, tumor, brain attack [also known as cerebrovascular accident or stroke]). A mental status assessment documents any emotional or cognitive change associated with the lesion. Not recognizing these changes hinders care planning and creates problems with social readjustment.
• Aphasia (the impairment of language ability secondary to brain damage). A mental status examination assesses language dysfunction as well as any emotional problems associated with it, such as depression or agitation.
• Symptoms of psychiatric mental illness, especially with acute onset.
In every mental status examination, note these factors from the health history that could affect your interpretation of the findings:
• Any known illnesses or health problems, such as alcoholism or chronic renal disease.
• Current medications whose side effects may cause confusion or depression.
• The usual educational and behavioral level—note that factor as the normal baseline, and do not expect performance on the mental status examination to exceed it.
• Responses to personal history questions, indicating current stress, social interaction patterns, sleep habits, drug and alcohol use.
In the following examination, the sequence of steps forms a hierarchy in which the most basic functions (consciousness, language) are assessed first. The first steps must be accurately assessed to ensure validity for the steps to follow. That is, if consciousness is clouded, then the person cannot be expected to have full attention and to cooperate with new learning. Or, if language is impaired, subsequent assessment of new learning or abstract reasoning (anything that requires language functioning) can give erroneous conclusions.
Objective Data
| EQUIPMENT NEEDED | |
| (Occasionally) Pencil, paper, reading material |

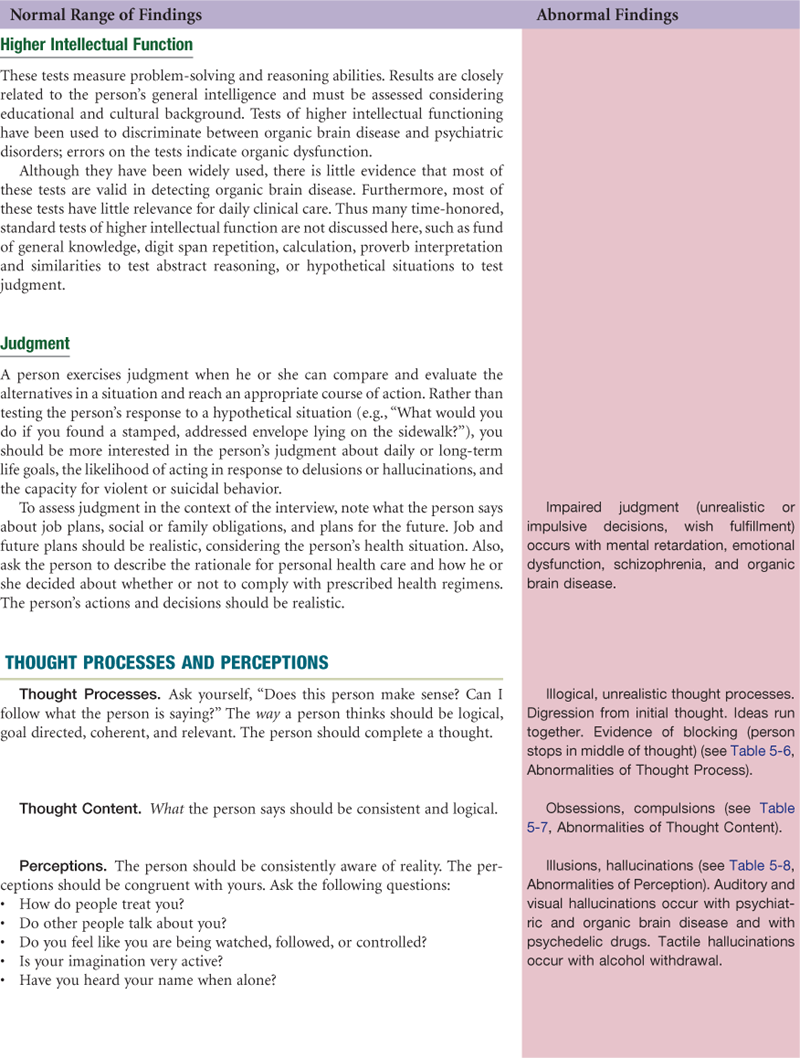
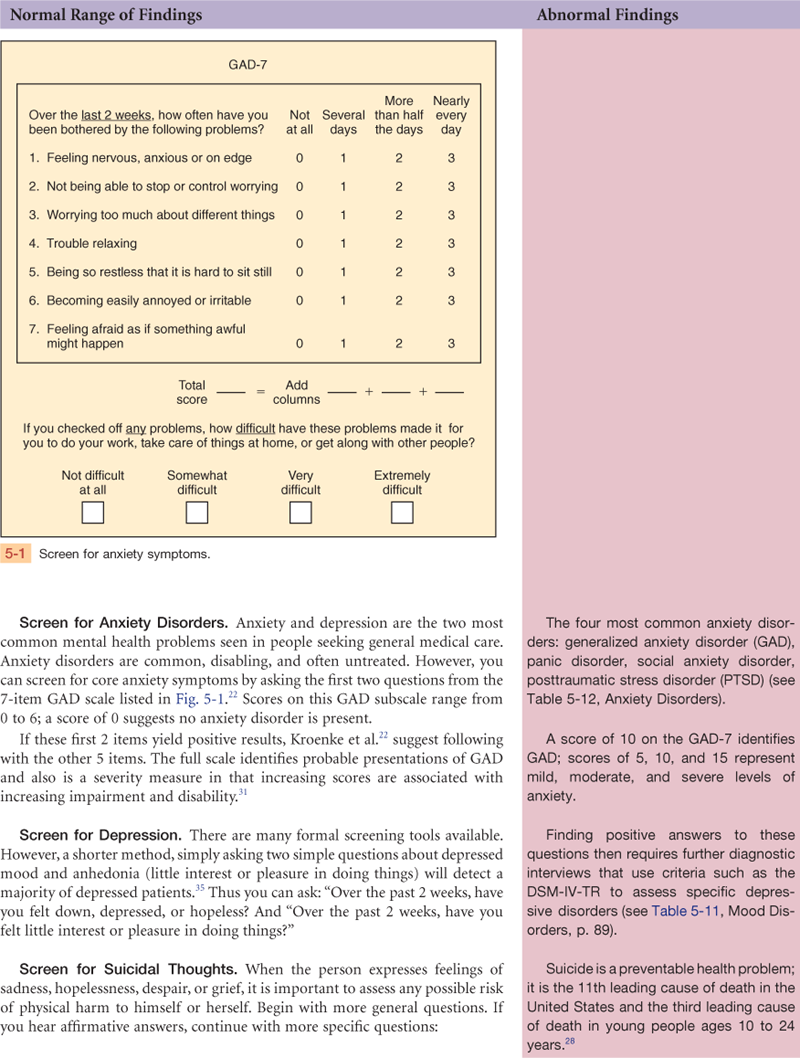
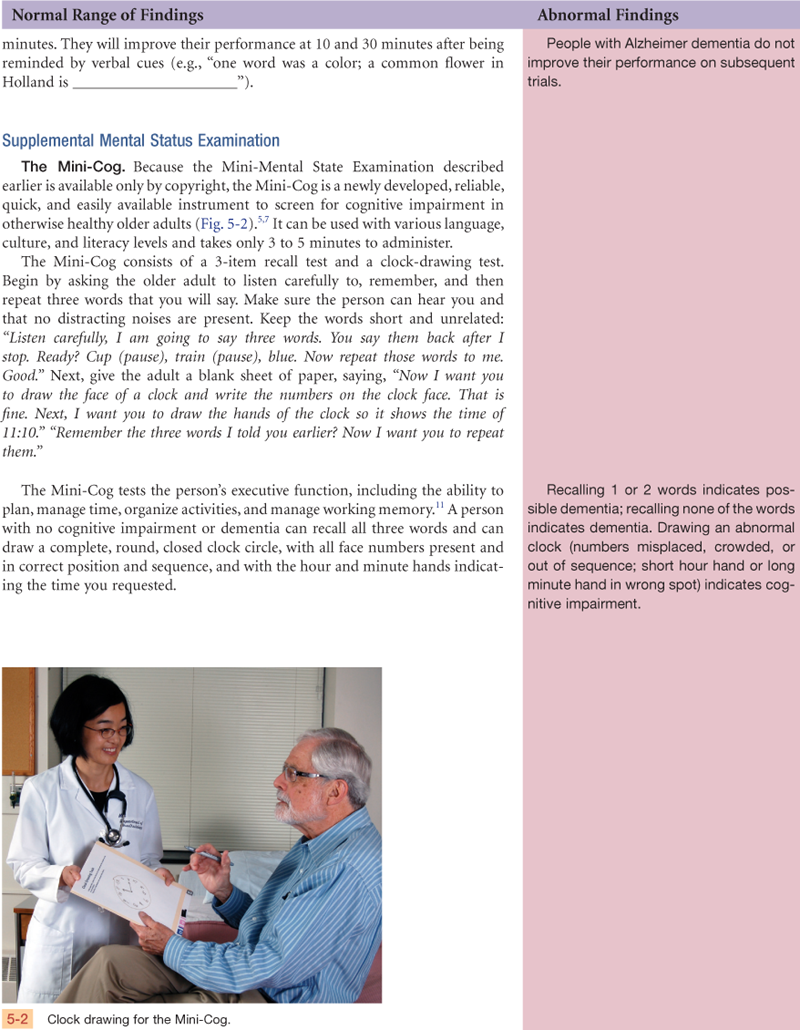
Table 5-1
Sample Items from the Mini-Mental State Examination (MMSE)
ORIENTATION TO TIME
“What is the date?”
REGISTRATION
“Listen carefully, I am going to say three words. You say them back after I stop.
Ready? Here they are …
HOUSE (pause), CAR (pause), LAKE (pause). Now repeat those words back to me.”
(Repeat up to five times, but score only the first trial.)
NAMING
“What is this?” (Point to a pencil or pen.)
READING
“Please read this and do what it says.” (Show examinee the words on the stimulus forms.)
CLOSE YOUR EYES
Reproduced by special permission of the Publisher, Psychological Assessment Resources, Inc., 16204 North Florida Avenue, Lutz, Florida 33549, from the Mini-Mental State Examination, by Marshal Folstein and Susan Folstein, Copyright 1975, 1998, 2001 by Mini Mental LLC, Inc. Published 2001 by Psychological Assessment Resources, Inc. Further reproduction is prohibited without permission of PAR, Inc. The MMSE can be purchased from PAR, Inc. by calling (813) 968-3003.
 Documentation and Critical Thinking
Documentation and Critical Thinking
Sample Charting
Appearance: Person’s posture is erect, with no involuntary body movements. Dress and grooming are appropriate for season and setting.
Behavior: Person is alert, with appropriate facial expression and with fluent, understandable speech. Affect and verbal responses are appropriate.
Cognitive functions: Oriented to time, person, place. Able to attend cooperatively with examiner. Recent and remote memory intact. Can recall four unrelated words at 5-, 10-, and 30-minute testing intervals. Future plans include returning to home and to local university once individual therapy is established and medication is adjusted.
Thought processes: Perceptions and thought processes are logical and coherent. No suicide ideation.
Score on Mini-Mental State Examination is 28.
Focused Assessment: Clinical Case Study
Lola P. is a 79-year-old married, white woman, with a recent hospitalization for evaluation of increasing memory loss, confusion, and socially inappropriate behavior. Her family reports that Mrs. P.’s hygiene and grooming have decreased; she eats very little and has lost weight, does not sleep through the night, has angry emotional outbursts that are unlike her former demeanor, and does not recognize her younger grandchildren. Her husband reports that she has drifted away from the stove while cooking, allowing food to burn on the stovetop. He has found her wandering through the house in the middle of the night, unsure of where she was. She used to “talk on the phone for hours” but now he has to push her into conversations. During this hospitalization, Mrs. P. has undergone a series of medical tests, including a negative lumbar puncture test, normal electroencephalogram (EEG), and a benign head computed tomography (CT) scan. Her physician now suggests a diagnosis of Alzheimer dementia.
Appearance: Sitting quietly, somewhat slumped, picking on loose threads on her dress. Hooded, zippered sweatshirt top worn over dress. Hair is gathered in loose ponytail with stray wisps. No makeup.
Behavior: Awake and gazing at hands and lap. Expression is flat and vacant. Will make eye contact when called by name, although gaze quickly shifts back to lap. Speech is a bit slow but articulate; some trouble with word choice.
Cognitive functions: Oriented to person and place. Can state the season but not the day of the week or the year. Is not able to repeat the correct sequence of complex directions involving lifting and shifting glass of water to the other hand. Scores a one-word recall on the Four Unrelated Words Test. Cannot tell examiner how she would plan a grocery shopping trip.
Thought processes: Experiences blocking in train of thought. Thought content is logical. Acts cranky and suspicious with family members. No suicide ideation.
Mini-Mental State Examination score is 17 and shows poor recall ability and marked difficulty with serial 7s.
Assessment
Chronic confusion
Impaired social interaction
Impaired memory
Wandering
Abnormal Findings
TABLE 5-3
Adapted from Strub, R.L., Black, F.W. (2000). Mental status examination in neurology (4th ed.). Philadelphia: Davis, with permission.
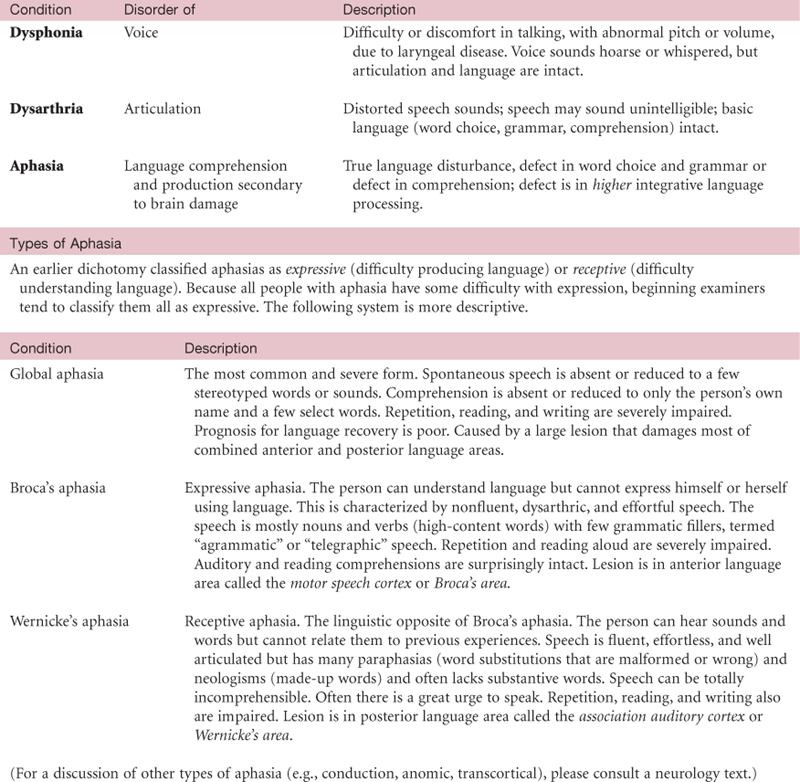
TABLE 5-5
Abnormalities of Mood and Affect
| Type of Mood or Affect | Definition | Clinical Example |
| Flat affect (blunted affect) | Lack of emotional response; no expression of feelings; voice monotonous and face immobile | Topic varies, expression does not |
| Depression | Sad, gloomy, dejected; symptoms may occur with rainy weather, after a holiday, or with an illness; if the situation is temporary, symptoms fade quickly | “I’ve got the blues.” |
| Depersonalization (lack of ego boundaries) | Loss of identity, feels estranged, perplexed about own identity and meaning of existence | “I don’t feel real.” “I feel like I’m not really here.” |
| Elation | Joy and optimism, overconfidence, increased motor activity, not necessarily pathologic | “I’m feeling very happy.” |
| Euphoria | Excessive well-being, unusually cheerful or elated, which is inappropriate considering physical and mental condition, implies a pathologic mood | “I am high.” “I feel like I’m flying.” “I feel on top of the world.” |
| Anxiety | Worried, uneasy, apprehensive from the anticipation of a danger whose source is unknown | “I feel nervous and high strung.” “I worry all the time.” “I can’t seem to make up my mind.” |
| Fear | Worried, uneasy, apprehensive; external danger is known and identified | Fear of flying in airplanes |
| Irritability | Annoyed, easily provoked, impatient | Person internalizes a feeling of tension, and a seemingly mild stimulus “sets him (or her) off” |
| Rage | Furious, loss of control | Person has expressed violent behavior toward self or others |
| Ambivalence | The existence of opposing emotions toward an idea, object, person | A person feels love and hate toward another at the same time |
| Lability | Rapid shift of emotions | Person expresses euphoric, tearful, angry feelings in rapid succession |
| Inappropriate affect | Affect clearly discordant with the content of the person’s speech | Laughs while discussing admission for liver biopsy |
Abnormal Findings for Advanced Practice
TABLE 5-6
Abnormalities of Thought Process
| Type of Process | Definition | Clinical Example |
| Blocking | Sudden interruption in train of thought, unable to complete sentence, seems related to strong emotion | “Forgot what I was going to say.” |
| Confabulation | Fabricates events to fill in memory gaps | Gives detailed description of his long walk around the hospital although you know Mr. J. remained in his room all afternoon. |
| Neologism | Coining a new word; invented word has no real meaning except for the person; may condense several words | “I’ll have to turn on my thinkilator.” |
| Circumlocution | Round-about expression, substituting a phrase when cannot think of name of object | Says “the thing you open the door with” instead of “key.” |
| Circumstantiality | Talks with excessive and unnecessary detail, delays reaching point; sentences have a meaningful connection but are irrelevant (this occurs normally in some people) | “When was my surgery? Well I was 28, I was living with my aunt, she’s the one with psoriasis, she had it bad that year because of the heat, the heat was worse then than it was the summer of ‘92, …“ |
| Loosening associations | Shifting from one topic to an unrelated topic; person seems unaware that topics are unconnected | “My boss is angry with me and it wasn’t even my fault. (pause) I saw that movie too, Lassie. I felt really bad about it. But she kept trying to land the airplane and she never knew what was going on.” |
| Flight of ideas | Abrupt change, rapid skipping from topic to topic, practically continuous flow of accelerated speech; topics usually have recognizable associations or are plays on words | “Take this pill? The pill is blue. I feel blue. (sings) She wore blue velvet.” |
| Word salad | Incoherent mixture of words, phrases, and sentences; illogical, disconnected, includes neologisms | “Beauty, red-based five, pigeon, the street corner, sort of.” |
| Perseveration | Persistent repeating of verbal or motor response, even with varied stimuli | “I’m going to lock the door, lock the door. I walk every day and I lock the door. I usually take the dog and I lock the door.” |
| Echolalia | Imitation, repeats others’ words or phrases, often with a mumbling, mocking, or mechanical tone | Nurse: “I want you to take your pill.” Patient (mocking): “Take your pill. Take your pill.” |
| Clanging | Word choice based on sound, not meaning, includes nonsense rhymes and puns | “My feet are cold. Cold, bold, told. The bell tolled for me.” |
TABLE 5-7
Abnormalities of Thought Content
| Type of Content | Definition | Clinical Example |
| Phobia | Strong, persistent, irrational fear of an object or situation; feels driven to avoid it | Cats, dogs, heights, enclosed spaces |
| Hypochondriasis | Morbid worrying about his or her own health, feels sick with no actual basis for that assumption | Preoccupied with the fear of having cancer; any symptom or physical sign means cancer |
| Obsession | Unwanted, persistent thoughts or impulses; logic will not purge them from consciousness; experienced as intrusive and senseless | Violence (parent having repeated impulse to kill a loved child); contamination (becoming infected by shaking hands) |
| Compulsion | Unwanted repetitive, purposeful act; driven to do it; behavior thought to neutralize or prevent discomfort or some dreaded event | Handwashing, counting, checking and rechecking, touching |
| Delusions | Firm, fixed, false beliefs; irrational; person clings to delusion despite objective evidence to contrary | Grandiose—person believes he or she is God; famous, historical, or sports figure; or other well-known person Persecution—“They are out to get me.” |
TABLE 5-8
| Type of Perception | Definition | Clinical Example |
| Hallucination | Sensory perceptions for which there are no external stimuli; may strike any sense: visual, auditory, tactile, olfactory, gustatory | Visual: seeing an image (ghost) of a person who is not there; auditory: hearing voices or music |
| Illusion | Misperception of an actual existing stimulus, by any sense | Folds of bed sheets appear to be animated |
TABLE 5-9
Schizophrenia*
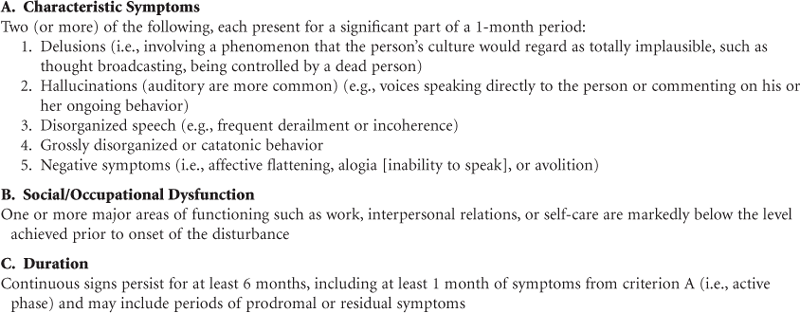
*These diagnostic categories are meant to be illustrative, not inclusive. Please see the original source or a psychiatry textbook for further categories and schizophrenia subtypes, such as paranoid type, catatonic type, disorganized type.
Adapted from the American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders (4th ed.). Washington, DC: The Association. Reprinted with permission from the American Psychiatric Association.
TABLE 5-10
Delirium, Dementia, and Amnestic Disorders*
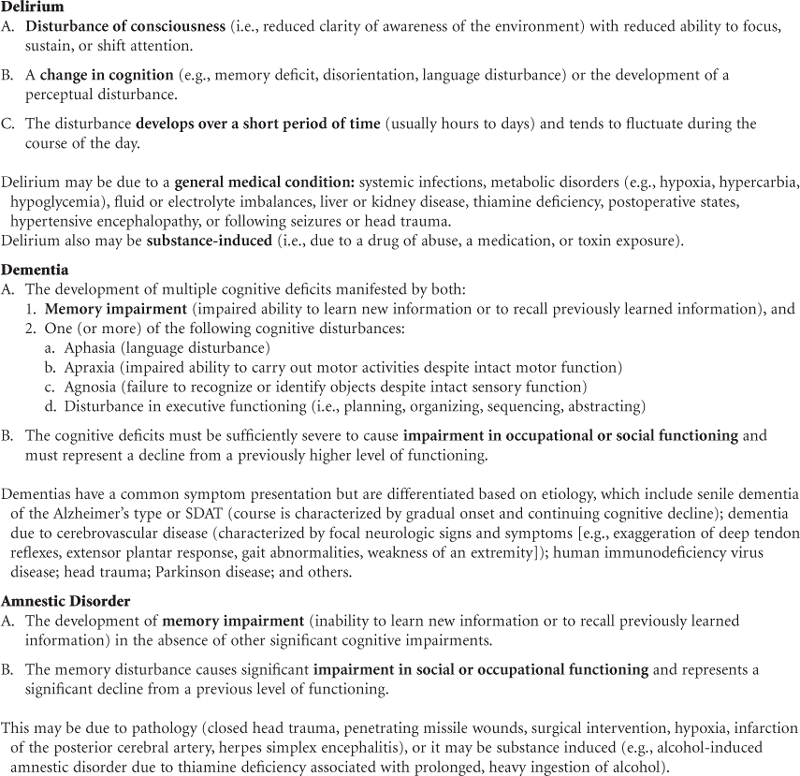
*The terms organic mental disorder and organic brain syndrome are no longer used for these disorders. These diagnostic categories are meant to be illustrative, not inclusive. Please refer to the original source for additional details and for further categories.
Adapted from the American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders (4th ed.). Washington, DC: The Association. Reprinted with permission from the American Psychiatric Association.
TABLE 5-11
Mood Disorders*
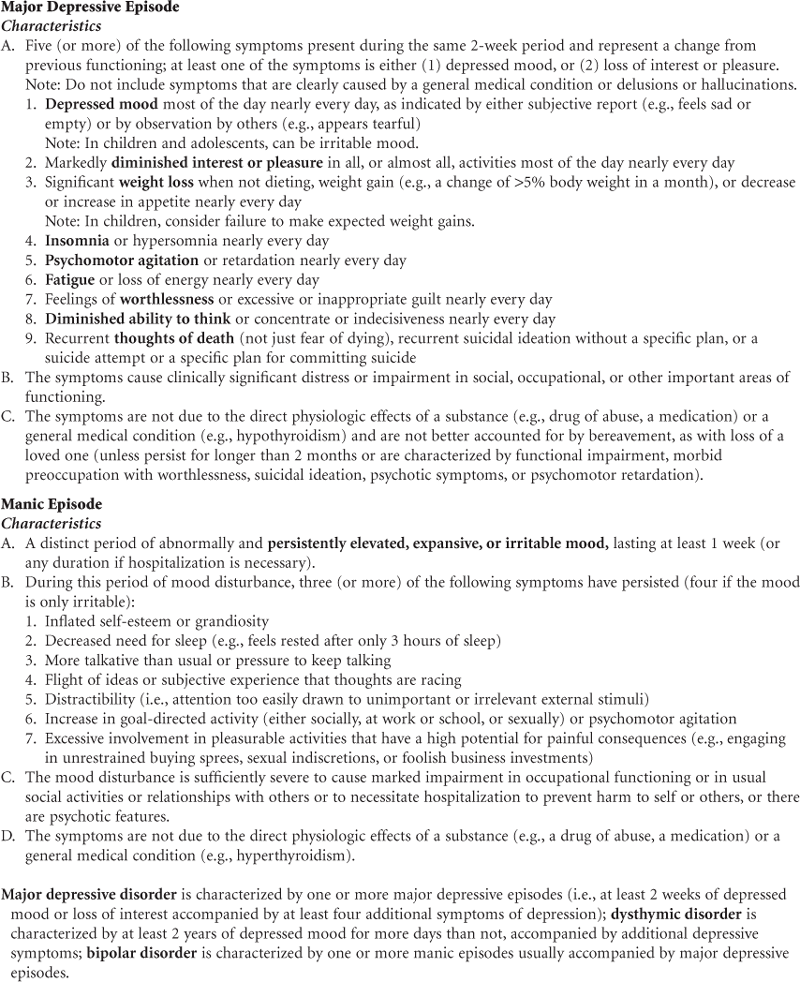
*These diagnostic categories are meant to be illustrative, not inclusive. Please see the original source or a psychiatry textbook for further categories, such as personality disorders or somatoform disorders.
Adapted from the American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders (4th ed.). Washington, DC: The Association. Reprinted with permission from the American Psychiatric Association.
TABLE 5-12
Anxiety Disorders*
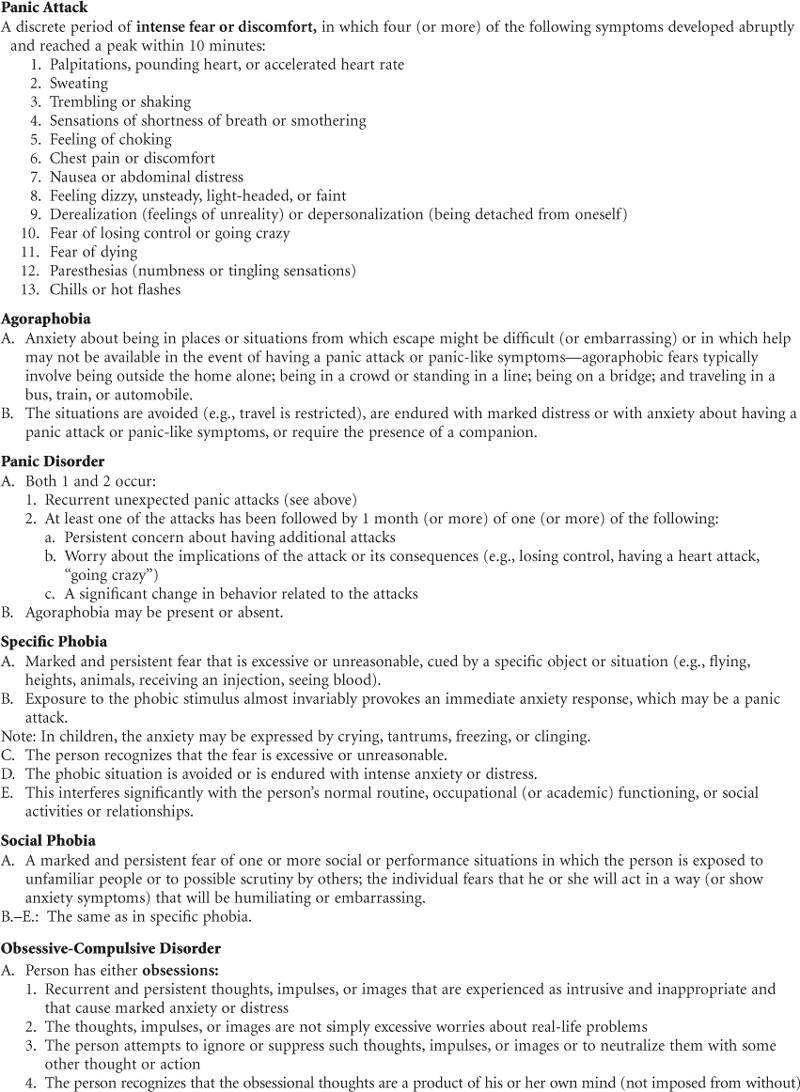
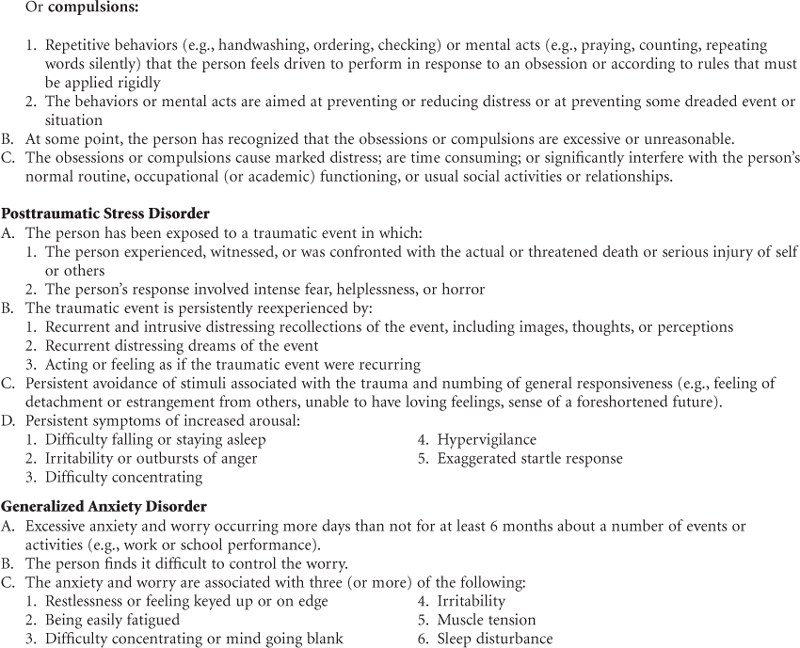
*These diagnostic categories are meant to be illustrative, not inclusive. Please see the original source or a psychiatry textbook for further details and categories of anxiety disorders.
Adapted from the American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders (4th ed.). Washington, DC: The Association. Reprinted with permission from the American Psychiatric Association.
Summary Checklist: Mental Status Assessment
 For a PDA-downloadable version, go to http://evolve.elsevier.com/Jarvis/.
For a PDA-downloadable version, go to http://evolve.elsevier.com/Jarvis/.
Bibliography
1. Adelman AM, Daly MP. Initial evaluation of the patient with suspected dementia. American Family Physician. 2005;71(9):1745–1750.
1a. Alverzo JP. A review of the literature on orientation as an indicator of level of consciousness. Journal of Nursing Scholarship. 2006;38(2):159–164.
2. American Psychiatric Association. Diagnostic and statistical manual of mental disorders. Text Revision 4th ed. Washington, DC: The Association; 2000.
3. Beatty GE. Shedding light on Alzheimer’s. Nurse Practitioner. 2006;31(9):32–45.
4. Birren JE, Schaie KW, eds. Handbook of the psychology of aging. 6th ed. San Diego: Academic Press; 2006.
5. Borson S, Scanlan JM, Watanabe J, et al. Improving identification of cognitive impairment in primary care. International Journal of Geriatric Psychiatry. 2006;21(4):349–355.
6. Bradway C, Hirschman KB. Working with families of hospitalized older adults with dementia. American Journal of Nursing. 2008;108(10):52–61.
7. Brodaty H, Low LF, Gibson L, et al. What is the best dementia screening instrument for general practitioners to use? American Journal of Geriatric Psychiatry. 2006;14(5):391–400.
8. Centers for Disease Control and Prevention. Suicide facts at a glance. Website www.cdc.gov/ncipc/dvp/suicide/SuicideDataSheet.pdf.
9. De Nisco S, Tiago C, Kravitz C. Evaluation and treatment of pediatric ADHD. Nurse Practitioner. 2005;30(8):14–25.
10. Depaulo Jr JR, Folstein MF. Psychiatric disturbances in neurological patients: Detection, recognition and hospital course. Annals of Neurology. 1978;4(3):225–228.
11. Doerflinger DMC. The Mini-Cog. American Journal of Nursing. 2007;107(12):62–72.
12. Fick DM, Mion LC. Delirium superimposed on dementia. American Journal of Nursing. 2008;108(1):52–61.
12a. Fisher D, Valente S. Evaluating and managing insomnia. Nurse Practitioner. 2009;34(8):21–26.
13. Folstein MF, Folstein SE, McHugh PR. “Mini-Mental State”: A practical method for grading the cognitive state of patients for the clinician. Journal of Psychiatric Research. 1975;12:189–198.
14. Forrest J, Willis L, Holm K, et al. Recognizing quiet delirium. American Journal of Nursing. 2007;107(4):35–39.
15. Fricchione G. Generalized anxiety disorder. New England Journal of Medicine. 2004;351(7):675–676.
16. Garand L, Mitchell AM, Dietrick A, et al. Suicide in older adults: Nursing assessment of suicide risk. Issues in Mental Health Nursing. 2006;29(4):355–370.
17. Gary FA. Stigma: barrier to mental health care among ethnic minorities. Issues in Mental Health Nursing. 2005;26(10):979–999.
18. Gill JM, Saligan LN. Don’t let SAD get you down this season. Nurse Practitioner. 2008;33(12):22–26.
18a. Gill J, Saligan LN, Henderson WA, et al. PTSD—Know the warning signs. Nurse Practitioner. 2009;34(7):30–37.
19. Greenberg SA. The geriatric depression scale: Short form. American Journal of Nursing. 2007;107(10):60–70.
20. Guess KF. Posttraumatic stress disorder. Nurse Practitioner. 2006;31(3):26–35.
21. Holcomb SS. Identification and treatment of depression. Nurse Practitioner. 2006;31(12):42–44.
21a. Inouye SK. Delirium in older persons. New England Journal of Medicine. 2006;354(11):1157–1165.
22. Kroenke K, Spitzer RL, Williams JB, et al. Anxiety disorders in primary care: Prevalence, impairment, comorbidity, and detection. Annals of Internal Medicine. 2007;146(5):317–325.
23. Lemiengre J, Nelis T, Jooston E, et al. Detection of delirium by bedside nurses using the confusion assessment method. Journal of the American Geriatrics Society. 2006;54(4):685–689.
24. Lumby B. Guide schizophrenia patients to better physical health. Nurse Practitioner. 2007;32(7):30–38.
25. Maslow K, Mezey M. Recognition of dementia in hospitalized older adults. American Journal of Nursing. 2008;108(1):40–50.
26. McCravy S, Johnson A, Wetsel MA, et al. Speak the language of autism. Nurse Practitioner. 2010;35(4):26–33.
27. Mynatt S, Cunningham P. Unraveling anxiety and depression. Nurse Practitioner. 2007;32(8):28–37.
28. National Institute of Mental Health. Suicide in the U.S.: statistics and prevention. Website www.nimh.nih.gov/health/publications/suicide-in-the-us-statistics-and-prevention.shtml.
29. Rabins PV. Research update: Mild cognitive impairment (MCI)—definition, diagnosis, and treatment possibilities. Advanced Studies in Medicine. 2004;4(6):290–296.
30. Roux SL, Overcash J. Scratching the surface: Addressing self-harm in adolescents. Nurse Practitioner. 2008;33(6):30–36.
31. Spitzer RL, Kroenke K, Williams JBW, et al. A brief measure for assessing generalized anxiety disorder. Archives of Internal Medicine. 2006;166(10):1092–1097.
32. Stanton K. Communicating with ED patients who have chronic mental illness. American Journal of Nursing. 2007;107(2):61–65.
33. Strub RL, Black FW. Mental status examination in neurology. 4th ed. Philadelphia: Davis; 2000.
34. Thayer KM, Bruce ML. Recognition and management of major depression. Nurse Pract. 2006;31(5):12–25.
35. U.S. Preventive Services Task Force. Screening for depression in adults: recommendations and rationale. Agency for Healthcare Research and Quality. Website www.ahrq.gov/clinic/3rduspstf/depression/depressrr.htm.
36. U.S. Preventive Services Task Force. Screening for suicide risk in adults: recommendations and rationale. Agency for Healthcare Research and Quality. Website www.ahrq.gov/clinic/3rduspstf/suicide/suiciderr.htm.
36a. Valente S. Suicide risk in elderly patients. Nurse Practitioner. 2008;33(8):34–40.
37. Waszynski CM. Detecting delirium. American Journal of Nursing. 2007;107(12):50–60.
38. Weber K. Asperger’s syndrome: From hiding to thriving. Nurse Practitioner. 2008;33(7):14–22.