Domestic Violence Assessment
Outline
Intimate Partner Violence Defined
Child Abuse and Neglect Defined
Elder Abuse and Neglect Defined
Assessing for Intimate Partner Violence
Assessing for Elder and Vulnerable Person Abuse and Neglect
Screening for Child Abuse and Neglect
Assessing for Risk of Homicide
When She Says “No” to the AAS but There Are Other IPV Health Indicators

Intimate partner violence, child abuse, and elder abuse are important health problems that health care professionals must recognize and assess. The Joint Commission (formerly known as JCAHO) requires that all health care settings have policies and procedures to assess, document, and make referrals for all kinds of family violence, including child abuse. All of the major nursing and medical organizations such as the American Nurses Association (ANA) and the American Medical Association (AMA) have policy statements recognizing the need for health care professionals to assess family violence.
Intimate Partner Violence Defined
The Centers for Disease Control and Prevention (CDC) definition for intimate partner violence (IPV) will be used throughout this chapter. The definition identifies two types of IPV46:
• Physical and/or sexual violence (use of physical force) or threat of such violence
• Psychological/emotional abuse and/or coercive tactics when there has been prior physical and/or sexual violence between persons who are spouses or nonmarital partners (dating, boyfriend/girlfriend) or former spouses or nonmarital partners
Child Abuse and Neglect Defined
Child abuse and neglect are defined at both the federal and state levels. The Child Abuse and Prevention Treatment Act (CAPTA) dictates the minimum standards that must be incorporated into the state statutes. Most of the state statutes incorporate the following definitions:
• Neglect is failure to provide for a child’s basic needs (physical, educational, medical, and emotional).
• Physical abuse is physical injury due to punching, beating, kicking, biting, burning, shaking, or otherwise harming a child. Even if the parent or caregiver did not intend to harm the child, such acts are considered abuse when done purposefully.
• Sexual abuse includes fondling a child’s genitals, incest, penetration, rape, sodomy, indecent exposure, and commercial exploitation through prostitution or the production of pornographic materials.
• Emotional abuse is any pattern of behavior that harms a child’s emotional development or sense of self-worth. It includes frequent belittling, rejection, threats, and withholding of love and support.
Elder Abuse and Neglect Defined
Almost every state has some form of mandatory reporting of abused older adults and other vulnerable patients (the developmentally disabled and the mentally ill). You need to be familiar with specific state reporting requirements in your state of practice. Those who work in communities that border two states will need to be informed about mandatory reporting statutes in both states. In some communities, the reporting mechanism is established county by county, while some states have a statewide hotline. As mandatory reporters of abuse, you need only have suspicion that elder abuse and/or neglect may have occurred in order to generate a call to the authorities. Many nurses, physicians, and social workers are erroneously under the assumption that they must have proof of abuse before calling the hotline. Although exact definitions of elder abuse and neglect vary from state to state, the AMA has developed a generic list of definitions that are clinically useful (Table 7-1).5 The National Research Council defines elder abuse as8:
1. Intentional actions that cause harm or create a serious risk of harm (whether or not harm is intended) to a vulnerable elder by a caregiver or person who stands in a trust relationship to the elder
or
2. Failure by a caregiver to satisfy the elder’s basic needs or to protect the elder from harm
TABLE 7-1
AMA Definitions for Elder Abuse and Neglect
| Physical abuse | Violent acts that result or could result in injury, pain, impairment, and/or disease |
| Physical neglect | Failure of the family member and/or caregiver to provide basic goods and/or services such as food, shelter, health care, and medications |
| Psychological abuse | Behaviors that result in mental anguish |
| Psychological neglect | Failing to provide basic social stimulation |
| Financial abuse | Intentional misuse of the elderly person’s financial/material resources without the informed consent of the person |
| Financial neglect | Failure to use the assets of the elderly person to provide services needed by the elderly person |
Adapted from Arvanis, S. C., Adelman, R. D., Breckman, R., et al. (1993). Diagnostic and treatment guidelines on elder abuse and neglect. Archives of Family Medicine, 2(4), 371-388.
Health Effects of Violence
Although estimates vary, approximately 1 million women in the United States report being physically and/or sexually assaulted by an intimate partner annually.56 Lifetime estimates of intimate violence vary from 5% to 51%,56 with the most usual range between 25% and 35%. Women are significantly more likely to be physically or sexually assaulted by a current or former intimate partner than by an acquaintance, family member, friend, or stranger.45,56 As high as these figures are, it is commonly accepted that they (particularly crime data) represent underestimates of the true incidence and prevalence of IPV.
In 2007, 794,000 children in the Unites States were determined by Child Protective Services to have been maltreated. Of these children, approximately 59% were neglected, 11% were physically abused, 8% were sexually abused, 8% were emotionally or psychologically abused, and fewer than 1% were medically neglected.57 Although a number of children are injured by non-related caregivers, approximately 80% of children are injured by a parent or parents. Approximately 1760 children were confirmed to have died from maltreatment. Young children account for most of these deaths. Over 75% of the deaths due to child maltreatment were in children younger than 4 years. In deaths due to child maltreatment, nearly 70% were caused by one or both parents.57
Aside from minor differences, the reporting laws across the United States are essentially the same. As in cases of elder abuse, only a reasonable suspicion that a child has been maltreated is needed in order to make a report to the appropriate authorities. Waiting until a conclusive diagnosis of abuse is made can put children at risk of further abuse and injury.
A persuasive body of knowledge accumulated in the past decade has established that violent experiences have significant effects on women’s health. The most obvious health care problem for abused women is injury. Cutaneous injuries can be caused by blunt, squeezing, and/or sharp mechanisms of injury.52 Blunt-force injury is the most common form of intimate partner violence, with being struck by a hand (closed fist or slap) the most common mechanism of blunt-force trauma.51 When blunt injuries cause the skin to tear, the wound is best described as a laceration.50-52 When a sharp instrument (knife, razor, scalpel, glass) slices through the tissue, the wound is best described as a cut or incision.50-52 Strangulation (often referred to by patient as “being choked”) can be caused by the manual compression of the neck by any body part (usually hands) or by tightening a cordlike object around the neck (ligature compression).50,52,55 Many of the mechanisms of injury just mentioned have particular patterns that can be recognized.6,50-52
In many controlled investigations of women in a variety of health care settings, abused women also have been found to have significantly more chronic health problems, including significantly more neurologic, gastrointestinal, and gynecologic symptoms and chronic pain.9,12,39 Abused women have also been shown to visit health care professionals more often than women not battered and to incur more health care costs. In terms of mental health, abused women also have significantly more depression, suicidality, and post-traumatic stress disorder (PTSD) symptoms, as well as problems with substance abuse.59 The forced sex that accompanies physical abuse in 40% to 45% of the cases contributes to a host of reproductive health problems including chronic pelvic pain, unintended pregnancy, STIs (including HIV), and urinary tract infections.10 Abuse during pregnancy is also a significant health problem, with serious consequences for both the pregnant mother (e.g., depression, substance abuse) and infant (low birth weight, increased risk of child abuse).23,35
Although more than half of battered women say they have been injured, only 25% to 30% of abused women say they have actually sought health care for one of the injuries.47 Even so, the majority of abused women (80%) say they have been in the health care setting for some reason, either for regular checkups or for one of the long-term health problems described previously. Because many abused women are not yet ready to seek help from a shelter or from the criminal justice system, the health care system can be an extremely important early point of contact. By uncovering abuse in its early stages, it is hoped that the pattern of violence can be stopped and long-term health problems avoided or minimized.
The health effects of elder abuse are not nearly as well studied. Complications from intentional injury can range from minor pain and discomfort to life-threatening injuries.18 Bleeding from intentional trauma can cause significant changes in circulatory homeostasis, leading to marked fluctuations in blood pressure and pulse, shock, and then death. Localized infections can progress to generalized sepsis and then death in aging patients who are immunocompromised. The actual assault or the stress leading up to or following an assault can contribute to cardiac complications. All of the sexually transmitted infections and sexually related complications that are sequelae of abuse for the younger women are present in the older sexually assaulted women. In addition, postmenopausal women have more friable vaginal mucosal tissue secondary to de-estrogenation.42
Abuse of older adults often is coupled with neglect. Neglect can manifest itself with symptoms of dehydration and malnutrition. Neglect can be intentional or unintentional. Many family members or caregivers working with an aging person consciously, and with malice, withhold food, water, medication, and appropriate necessities, while often stealing the financial assets of the older, dependent person. This type of neglect is often, by definition, criminal in nature.
Other family members or caregivers working with an older person struggle with their own severe physical and cognitive health challenges. Their intentions are good; however, the older patient may experience profound unintentional neglect. Although unintentional neglect is usually not viewed as a crime, it is still reportable to adult protective service agencies. Self-neglect raises often unanswerable questions about one’s right to live autonomously versus society’s obligation to care for a person who is not able to care for herself or himself. Suspected self-neglect is also a mandatory reportable activity to adult protective services.
There are many possible long-term physical and psychological effects of child maltreatment. The immediate consequences can include a spectrum of physical injuries such as bruises, fractures, and lacerations and can involve more severe injury such as inflicted traumatic brain injury (shaken baby syndrome). More severe forms of maltreatment can lead to death or long-term disability such as mental retardation, blindness, and physical disability.
Child maltreatment can have deleterious effects on a child’s quality of life and overall poor health, which can last into adulthood.4,16 Ongoing child maltreatment can lead to changes in brain structure and chemistry, which may lead to long-term physical, psychological, emotional, social, and cognitive dysfunction.24 Childhood physical abuse is reported to be the most consistent predictor of youth violence.30 Children who are abused are 11 times more likely to be arrested for violent crime as a juvenile and 2.7 times more likely to be arrested for violent crime as an adult.19 Approximately one third of abused children will abuse their own children.43 Two out of three people in drug treatment programs report abuse as children.29
Examples of risk factors that may contribute to child maltreatment14:
• Disabilities or mental retardation in children that may increase caregiver burden
• Social isolation of families
• Parents’ lack of understanding of children’s needs and child development
• Parents’ history of domestic abuse
• Poverty and other socioeconomic disadvantages, such as unemployment
• Family disorganization, dissolution, and violence, including intimate partner violence
• Young, single, nonbiological parents
• Poor parent-child relationships and negative interactions
• Parental thoughts and emotions supporting maltreatment behaviors
• Parental stress and distress, including depression or other mental health conditions
Although there are identified risk factors for child maltreatment, a study on missed cases of abusive head trauma conducted by Jenny et al.26 found several factors significant for missed injuries. They found that missed cases of abusive head injury occurred more often in white children than children of minority races, in children with both parents living with the child, in younger children, and in children with less severe presenting symptoms.
Assessing for Intimate Partner Violence
Routine, universal assessments for intimate partner violence means asking every woman at every health care encounter if she has been abused by a husband, boyfriend, or other intimate partner or ex-partner. The majority of both abused and nonabused women say that they are in favor of routine assessments and that they believe it would assist women in getting help for the problem.3,22 Routine, universal assessment for IPV has been called for by most nursing professional organizations (e.g., ANA; American College of Nurse Midwives [ACNM]; Association of Women’s Health and Obstetrics and Neonatal Nursing [AWHONN]; Emergency Nurses Association [ENA]; International Association of Forensic Nurses [IAFN]; Nursing Network on Violence Against Women, International [NNVAWI]).33
How to Assess
The Abuse Assessment Screen (AAS) has been used in many different health care settings, has been translated into at least seven languages, and has strong support for reliability and validity.53 It has never been copyrighted, with the intention that nurses be able to revise and reformat its content to be adaptable to their own health care setting (Fig. 7-1).
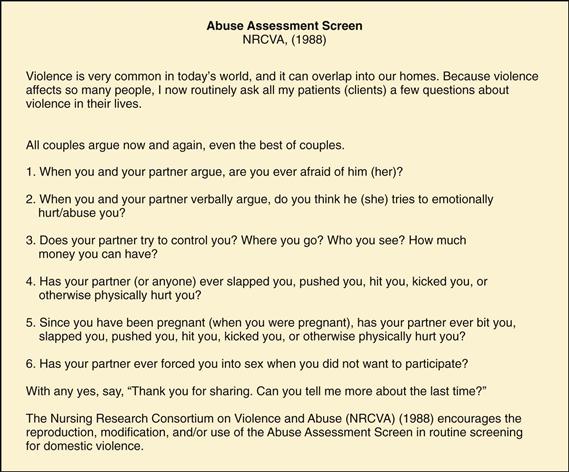
Many health care professionals precede the questions with an introduction such as: “Because domestic violence is so common in our society, we are asking all women the following questions.” or “Because domestic violence has such serious health care consequences, we are asking all of our female patients the questions that follow.” This both alerts the woman that questions about domestic violence are coming and makes sure that the woman knows she is not being singled out for these questions.
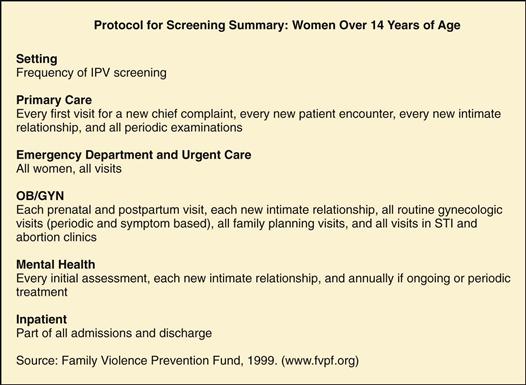
The Family Violence Prevention Fund20 has developed a protocol for the recommended frequency of screening (Fig. 7-2).
Assessment
If a woman answers “yes” to any of the AAS questions, you need to ask questions designed to assess how recent and how serious the abuse was. Asking the woman to “tell me about this abuse in your relationship” is a good way to start. Even if the woman says “yes” only to the first question and calls the abuse “only emotional” or “not that bad” or says “we just fight a lot” at first, more abuse may be revealed as you gently assess the situation. This type of assessment is often like “peeling layers of an onion,” with more violence being uncovered as the assessment continues. This is not “denial” on the woman’s part but, rather, the normal minimization that often accompanies trauma from violence.
It is appropriate for you to show that you are concerned and even distressed about the degree of violence. One message that needs to be conveyed during the assessment is that the abuse is not the woman’s fault; this can be said several times. Another important message is that you are concerned and that help is possible. Still another is that several health problems can occur because of domestic violence and that is why it is necessary to conduct a thorough assessment. In fact, in a recent survey of 265 abused women who accepted a referral to a social worker, 59% said it was because the medical provider expressed concern that their presenting health problem was related to IPV.32
Assessing for Elder and Vulnerable Person Abuse and Neglect
Routine assessment for possible elder abuse and neglect can be more complicated than assessments for IPV. Older adults can present for health care cognitively and physically intact or with multiple health, physical, and cognitive challenges. Assessing for intimate partner violence in older adults is very similar to screening for IPV among younger women if the patient is cognitively intact.27 The AAS can be a useful screen for assessing domestic violence among older women. You may modify the introductory statement as follows: “Because domestic violence has such serious health care consequences, we are asking women of all ages the following questions.”
Whereas some aging women have been in abusive relationships for decades, others are experiencing for the first time physical and sexual violence from normally nonabusive partners who themselves are afflicted with behavior-altering neurologic illness (Alzheimer disease, organic brain syndromes). An older battered woman in a long-term abusive relationship may be trying to outlive her abuser, whereas the newly abused older woman may be reluctant to disclose because of embarrassment, shame, and fears that her partner will be institutionalized.
Older adults are vulnerable to abuse from other family members and caregivers. The AMA nine-question clinically effective screen can be used with older persons who are cognitively intact (Table 7-2). Chapter 3 gives further direction for assessment.
TABLE 7-2
AMA Elder Abuse Screening Questions
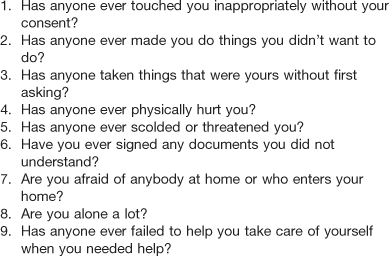
Adapted from Arvanis, S. C., Adelman, R. D., Breckman, R., et al. (1993). Diagnostic and treatment guidelines on elder abuse and neglect. Archives of Family Medicine, 2(4), 371-388.
Assessment of physical abuse and/or neglect in the cognitively challenged person is much more complicated. Physical findings that are inconsistent with the history provided by the patient, family member, or caregiver are significant red flags of possible abuse and neglect. Almost all states have some form of mandatory reporting of suspected abuse of patients ages 65 years and older. To report abuse, you need not have proof of abuse or neglect, only reasonable cause to suspect that elder abuse or neglect may have occurred.
History
It is important also to assess and document prior abuse, including prior IPV, childhood physical and sexual abuse, and prior rapes of all kinds (stranger, date, intimate partner). Cumulative trauma has been associated with more severe mental and physical health problems.59 Also important to determine is the history of traumatic injuries, because these may have an impact on the current health condition. For instance, a woman may have experienced prior episodes of head trauma and strangulation, both of which may be related to chronic but subtle neurologic symptoms and problems. Another extremely important area of history and examination in cases of IPV or elder abuse is a mental status examination, both for potential head trauma and neurologic symptoms and also for mental health problems. All survivors of violence should be given a mental status examination, with particular attention to the most frequent mental health problems associated with violence: depression, suicidality, PTSD, substance abuse, and anxiety. Chapter 5 gives direction for conducting this part of the history.
Screening for Child Abuse and Neglect
The American Academy of Pediatrics1 recommends screening for IPV as an active means to prevent child maltreatment. There is a significant co-occurrence between child abuse and IPV, and it is suggested that when exposed to both, children may have more significant long-term health effects.25 Child abuse is reported in 33% to 77% of homes where there is ongoing abuse of an adult.1 Positive responses should prompt you to involve additional members of the health care team (e.g., physician, social worker).
An important part of evaluating any child for suspected abuse is to determine the child’s age and developmental level. Could the child have suffered the injury that is being reported based on his or her developmental level? For example, the history that a 3-week-old child rolled off a bed causing injury is not yet developmentally plausible. Because you may not be able to directly observe the child’s motor and cognitive milestones during the history taking, it is important to ask thecaregivers directly. Is your child crawling, pulling to stand, or walking? What other developmental issues are currently being faced at home: for example, tantrums, potty training?
If the child is verbal, a history should be obtained away from the caregivers through open-ended questions or spontaneous statements. It is important to remember that children may have suffered significant trauma yet respond only minimally to open-ended questions.36 Keeping the questions short and using age-appropriate language and familiar words can help enrich the history taking. Children older than 11 years can generally be expected to provide a history at the level of most adults.36
The medical history is also an important part of your evaluation. Has the child had previous hospitalizations or injuries, or does he or she suffer from any chronic medical conditions? Does the child take any medication that may cause easy bruising? Does the child have a history of repeated visits to the hospital? Was there a delay in seeking care for anything other than a minor injury? Is there a history of substance abuse in the family or any financial or social stressors in the home? What are the typical methods of discipline used in the home?
Physical Examination
Important components of the physical examination of the known survivor of IPV and/or elder abuse include a complete head-to-toe visual examination, especially if the patient is receiving health services secondary to reported abuse. When the examination reveals physical findings, knowledge of basic medical forensic terminology is essential in all documentation. Table 7-3 lists the most common forensic terms with definitions. Note that the most commonly misused terms are ecchymosis and laceration. Ecchymoses are not directly related to blunt-force trauma that results in bruising, and not all open wounds should be called lacerations (only those related to splitting of tissue from blunt-force impact and/or tearing of tissue should be).
TABLE 7-3
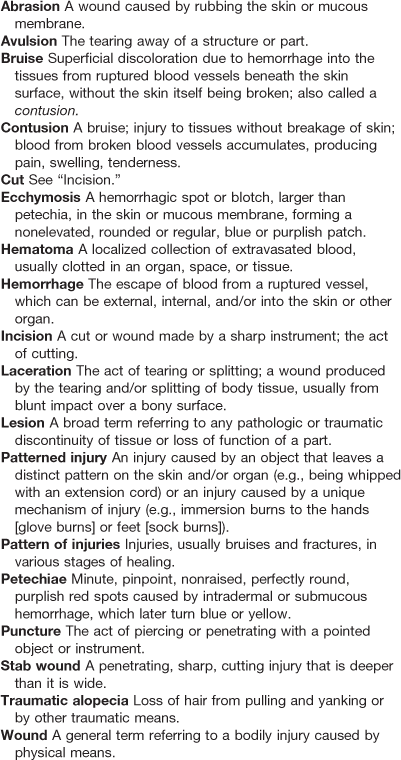
Adapted from Miller, B. F., Keane, C. B., O’Toole, M. (2005). Miller-Keane encyclopedia & dictionary of medicine, nursing, and allied health (7th ed.). Philadelphia: Saunders; Sheridan, D. J. (2001). Treating survivors of intimate partner abuse: forensic identification and documentation. In Olshaker, J. S., Jackson, M. L., Smock, W. S., editors: Forensic emergency medicine, Philadelphia: Saunders; Taber’s cyclopedic medical dictionary. (1997). Philadelphia: Davis.
Keep in mind the following guidelines when documenting the physical examination50-52:
• Bruise can be used interchangeably with contusion.
• Laceration is related to avulsion.
• Ecchymosis is related to (senile) purpura.
• Petechia is related to purpura.
• Rug burn is more accurately described as a friction abrasion.
• Incision can be used interchangeably with cut.
• Cut can be used interchangeably with sharp injury.
• Stab wounds are penetrating, deep, sharp injuries.
• Hematoma is a collection of blood that is often but not always caused by blunt-force trauma.
Many practitioners try to date bruises based on the color; however, there is no scientific evidence to support the accurate dating of injuries based on color of the contusion.28,37 Therefore trying to accurately date injuries solely by examination is forensically futile. However, some guidelines can assist in determining if the approximate age of the bruise is consistent with the history being provided by the patient and/or caregiver.
A new bruise is usually red and will often develop a purple or purple-blue appearance 12 to 36 hours after blunt-force trauma. The color of bruises (and ecchymoses) generally progresses from purple-blue to bluish green to greenish brown to brownish yellow before fading away. This process will be the same on all people; however, depending on the color of a person’s skin, the process may be more or less visible and more or less able to be photographed. In general, newer bruises will be mostly reddish purple, whereas bruises that are beginning to age will be more greenish brown or brownish yellow.37
Multiple factors can contribute to older adults bruising more readily or more severely than younger people. Medications and abnormal blood values related to medication side effects and underlying hematologic disorders can affect ease of bruising or the formation of ecchymosis. Common medications that increase risk for bruising or bleeding complications include but are not limited to the following: aspirin, ibuprofen, any of the nonsteroidal anti-inflammatory drugs, warfarin, heparin, valproic acid, prednisone, and clopidogrel. Vitamin nutritional supplements also may contribute to hematologic complications, especially if the person is already taking a blood-thinning or platelet-altering medication. Bilberry, garlic, ginger, and ginkgo are among the more common supplements linked to increased risk of bruising and/or bleeding complications.17
Any health evaluation for known or suspected elder abuse and neglect should include baseline laboratory tests, including, at a minimum, a complete blood count (CBC) with platelet level, basic blood chemistries (including blood urea nitrogen [BUN], creatinine, protein, and albumin), serum liver function tests, a coagulation panel, and a urinalysis.21
Physical Examination of Children
The forensic terminology used in documentation of IPV/elder abuse applies similarly to children. A visual inspection of the child from head to toe is important in any physical examination. Significant injuries can be hidden under clothing, diapers, socks, and long hair. The American Academy of Pediatrics2 defines significant trauma as any injury beyond temporary redness of the skin. Bruising in children is one of the most common physical findings in child abuse. Unfortunately, it can also be easily overlooked and may be a missed opportunity for intervention and prevention of further injury. Pierce et al.41 found that bruising was a missed warning sign in up to 44% of fatal and near-fatal cases of physical child abuse. Accidental bruising in healthy, active children is common, yet the presence of bruises in babies has significance in evaluating a child for abuse. Children who are not yet walking with support—”cruising”—typically should not have bruises.54 Bruising in infants who are not yet cruising, usually infants younger than 9 months, should alert you to possible abusive mechanisms to the injury or an underlying medical illness.
Once children begin to walk, bruising, particularly on the bony prominences, is common.54 Reece and Ludwig44 found that in children who were walking, 40% to 50% had bruises over the bony prominences of the front of their bodies. Sugar, Taylor, and Feldman54 found that bruising in “atypical” places such as the buttocks, hands, feet, and abdomen was exceedingly rare and should arouse concern. This is further supported by Pierce et al.,41 who found that in children younger than 4 years, bruising on the torso, ears, and neck as well as any bruising on a pre-cruising infant was significantly correlated with abuse, in absence of a compelling history. Similarly, Mosqueda et al.34 studied older adults who had accidental bruises and found that nearly 90% of their bruises were on their extremities and no accidental bruises were found on the neck, ears, genitalia, buttocks, or soles of the feet. Furthermore, any bruise that takes the shape of an object should be considered highly specific for abuse. Bruising found in non-mobile children should raise the concern for further injury, including fractures and intracranial injury.
Health care providers are often asked to estimate the ages of bruises, particularly as it relates to an inflicted injury. This should be avoided, because published evidence does not support the ability to date a bruise by color alone, either by visual assessment or photography.31
In addition to bruising, lacerations, abrasions, bite marks, and burns are commonly seen in abused children. These findings, taken into context of the child’s developmental level, history and mechanism of injury, location of injury, and social history, can help guide in determining if an injury is concerning for abuse.
Documentation
Documentation of intimate partner violence and elder abuse must include detailed, nonbiased progress notes, the use of injury maps, and photographic documentation in the health record. Examples of photographic documentation of patients of one of the authors are included in this chapter (Figs. 7-3 through 7-9*).

7-3 Patterned fingernail-like scratch abrasions to the left lateral neck from a manual strangulation mechanism of injury.

7-4 Patterned punchlike abrasion to the mid-forehead from an assailant wearing a ring with a stone; sutured laceration to the left eyebrow; sutured partial-avulsion injury to the nose, punchlike contusion to the left eye involving the sclera, and manual strangulation–related abrasion to the neck.

7-5 Newer patterned looped, cordlike contusions to the right upper posterior shoulder and left lower posterior shoulder; patterned looped, cordlike scar to the right mid-lateral back; scabbed, cordlike abrasions to the mid-back; patterned kick/stomplike heel contusion to the left mid-back; and patterned foot/kick/stomplike heel and sole bruise imprint to the upper left posterior shoulder.



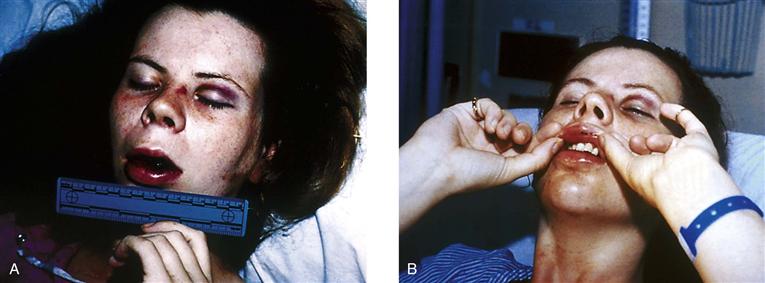
7-9 Series of two photographs to illustrate how photographs can be used to demonstrate mechanisms of injuries. A, Victim has obvious facial trauma to her left eyelid, left lateral nose, and mouth. The left lateral nose contusion was caused by the nosepiece of her glasses being forcefully pushed into her skin from a punch injury to the left eye. The patient’s glasses absorbed much of the punch force and were broken (not pictured). A second punch produced the mouth trauma. B, The force of the mouth punch caused the upper teeth to leave patterned contusions, abrasions, and minor lacerations to the oral mucosa of the upper lip.
Written documentation of histories of IPV and elder abuse need to be verbatim but within reason. It is clinically unrealistic to document verbatim every statement made by an abused patient. However, it is critical to document exceptionally poignant statements made by the victim that identify the reported perpetrator and severe threats of harm made by the reported perpetrator. Other aspects of the abuse history, including reports of past abusive incidents, can be paraphrased with the use of partial direct quotations.
When quoting or paraphrasing the history, you should not sanitize the words reportedly heard by the victim. Verbatim documentation of the reported perpetrator’s threats interlaced with curses and expletives can be extremely useful in future court proceedings. Also, be careful to use the exact terms an abused patient may use to describe sexual organs or sexually assaultive behaviors.
Photographic documentation in the medical record can be invaluable. Prior written consent to take photographs should be obtained from all cognitively intact, competent adults. Most health facilities have standardized consent to photograph forms. If a patient is unconscious or cognitively impaired, the taking of photographs without consent is generally viewed as ethically sound because it is a noninvasive, painless intervention that has high potential to help a suspected abuse victim. There are advantages and disadvantages to the different photographic systems (35-mm versus digital) commonly in use.7,50 In general, any in-focus picture of injury is better than no picture, regardless of what system is used.
When documenting the history and physical findings of child abuse and neglect, use the words the child has given to describe how his or her injury occurred. Remember that the possibility arises that the abuser may be accompanying the child. If the child is nonverbal, use statements from caregivers. It is important to know your employer/institutional protocol for obtaining a history in cases of suspected child maltreatment. Some protocols may delay a full interview until it can be done by a forensically trained interviewer.
Assessing for Risk of Homicide
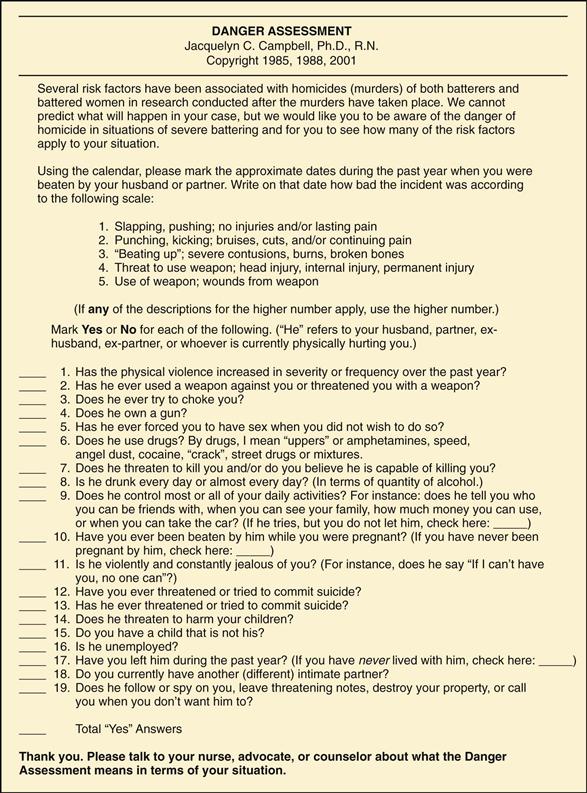
Women in this country are more often killed by a husband, boyfriend, or ex-husband than by anyone else, and about three fourths of these women had been abused by the man who subsequently killed them.13 In a multicity study of intimate partner homicide of women, 42% of the women killed had been seen somewhere in the health care system (the ED in the majority of cases but also in primary care, prenatal care, and other settings) for something in the year before she was killed.48 These encounters were missed opportunities for health care professionals to identify IPV and intervene to decrease the danger. The same study found reliability and validity support for the Danger Assessment (DA), a 19-item yes/no instrument that has been used extensively by nurses in the health care system as well as advocates in other settings with battered women13 (Fig. 7-10). The instrument starts with a calendar so that women can more accurately see for themselves how frequent and severe the violence has become over the past year. This is also an excellent assessment of frequency and severity for the health care provider. Although there are no predetermined cutoff scores on the DA, the more “yes” answers there are, the more serious the danger of the woman’s situation. In the previously described multicity study, abused women who were the victims of a homicide had an average score of 7.1 on the original 15-item DA. The DA is copyrighted, so users need to use it intact and are asked to communicate with the author if they are planning to use it in research. It can also be downloaded from www.son.jhmi.edu.
When She Says “No” to the AAS But There Are Other IPV Health Indicators
In addition to the AAS, providers need to be alert for the conditions particularly associated with IPV, including gynecologic problems (especially STIs, pelvic pain, and complaints of sexual dysfunction), chronic irritable bowel syndrome, back pain, depression, and the presenting symptoms of PTSD (especially problems sleeping and “panic” attacks or problems with “nerves”). When these problems occur, and especially when they persist, a thorough and repeated assessment for domestic violence is needed. In this case, an instrument such as the Women’s Experience with Battering (WEB)15 scale might be used in addition to the AAS, or gentle indirect queries may be used (e.g., “I am concerned about your health conditions. Is there any chance that stress at home is contributing to these problems?”).
 culture and genetics
culture and genetics
Domestic violence is a phenomenon that occurs cross-culturally.58 It may be more difficult to determine in many cultural groups. For example, the battering may be hidden, covered by clothing and heavy facial makeup, by many Chinese women. Indicators that domestic violence may be a problem include higher reported rates of alcoholism, suicide, and homicide in American Indian and other communities.
Domestic violence has a profound effect on the person, family, and community, and the roots or outcomes are seen in the following examples38:
• The reporting of serious psychological distress among persons 18 years of age and older was 3.0% for the general population, 3.0% for whites, 7.1% for American Indians, and 3.0% for African Americans.
• The heavy use of alcohol by persons 12 years of age and older for the white population was 7.5%, African Americans 4.4%, and American Indians 8.7% of the population.
• Death rates from suicide among the general male population was 10.9 per 100,000 residents, but 16.4 per 100,000 male American Indians and 9.8 per 100,000 African Americans.
• Death rates for homicide among the general male population was 9.4 per 100,000 residents, but 11.6 per 100,000 male American Indians and 36.4 per 100,000 African Americans.
Bibliography
1. American Academy of Pediatrics. The role of the pediatrician in recognizing and intervening on behalf of abused women. Pediatrics. 1998;101(6):1091–1092.
2. American Academy of Pediatrics. When inflicted skin injuries constitute child abuse. Pediatrics. 2002;110:644–645.
3. Anglin D. Diagnosis through disclosure and pattern recognition. In: Mitchell C, Anglin D, eds. Intimate partner violence: A health-based perspective. New York: Oxford University Press; 2009.
4. Arnow BA. Relationships between childhood maltreatment, adult health and psychiatric outcomes and medical utilization. The Journal of Clinical Psychiatry. 2004;65(Suppl. 12):10–15.
5. Arvanis SC, Adelman RD, Breckman R, et al. Diagnostic and treatment guidelines on elder abuse and neglect. Archives of Family Medicine. 1993;2(4):371–388.
6. Besant-Matthews PE. Blunt and sharp injuries. In: Lynch V, Duval JB, eds. Forensic nursing. St. Louis: Mosby; 2006.
7. Besant-Matthews PE, Smock WS. Forensic photography in the emergency department. In: Olshaker JS, Jackson MC, Smock WS, eds. Forensic emergency medicine. Philadelphia: Lippincott Williams & Wilkins; 2001;257–282.
8. Elder mistreatment: Abuse, neglect, and exploitation in an aging America. In: Bonnie RJ, Wallace RB, eds. Washington, DC: National Academies Press; 2003.
9. Campbell J, Jones AS, Dienemann J, et al. Intimate partner violence and physical health consequences. Archives of Internal Medicine. 2002;162:1157–1163.
10. Campbell J, Soeken K. Forced sex and intimate partner violence: Effects on women’s health. Violence Against Women. 1999;5:1017–1035.
11. Campbell J, Soeken KL. Women’s responses to battering: a test of the model. Research in Nursing & Health. 1999;22:49–58.
12. Campbell JC. Health consequences of intimate partner violence. Lancet. 2002;359(9314):1331–1336.
13. Campbell JC, et al. Risk assessment for intimate partner homicide. In: Pinard GF, Pagani L, eds. Clinical assessment of dangerousness: Empirical contributions. New York: Cambridge University Press; 2001.
14. Child Welfare Information Gateway. Common risk and protective factors. Retrieved September 8, 2007, from www.childwelfare.gov/preventing/overview/commonfactors.cfm; 2007.
15. Coker A, Smith PH, McKeown RE, et al. Frequency and correlates of intimate partner violence by type: physical, sexual, and psychological battering. American Journal of Public Health. 2000;90(4):553–559.
16. Corso PS, Edwards VJ, Fang X, et al. Health related quality of life among adults who experienced maltreatment during childhood. American Journal of Public Health. 2008;98(6):1094–1100.
17. Nursing herbal medicine handbook. In: Doyle RM, Harold C, Johnson P, eds. Springhouse: PA: Springhouse; 2001.
18. Dyer CB, Connolly MT, McFeeley P. The clinical and medical forensics of elder abuse and neglect. In: Bonnie RJ, Wallace RB, eds. Elder mistreatment: Abuse, neglect and exploitation in an aging America. Washington, DC: National Academies Press; 2003.
19. English DJ, Widom CS, Brandford C. Another look at the effects of child abuse National Institute of Justice. Journal. 2004;251:23–24.
20. Family Violence Prevention Fund. Preventing domestic violence: Clinical guidelines on routine screening. San Francisco: Author; 1999; www.fvpf.org; 1999.
21. Geroff AJ, Olshaker JS. Elder abuse. In: Olshaker JS, Jackson MC, Smock WS, eds. Forensic emergency medicine. Philadelphia: Lippincott Williams & Wilkins; 2001.
22. Glass NE, Dearwater S, Campbell JC. Intimate partner violence screening and intervention: Data from eleven Pennsylvania and California community hospital emergency departments Journal of Emergency. Nursing. 2001;27(2):141–149.
23. Goodman PE. Intimate partner violence and pregnancy. In: Mitchell C, Anglin D, eds. Intimate partner violence: A health-based perspective. New York: Oxford University Press; 2009.
24. Hagele DM. The impact of maltreatment on the developing child. North Carolina Medical Journal. 2005;66(5):356–359.
25. Herrenkohl TI, Sousa C, Tajima EA, et al. Intersection of child abuse and children’s exposure to domestic violence. Trauma, Violence & Abuse. 2008;9(2):84–99.
26. Jenny C, Hymel KP, Ritzen A, et al. Analysis of missed cases of abusive head trauma. JAMA: The Journal of the American Medical Association. 1999;281:621–626.
27. Koin D. Intimate partner violence among the elderly and people with disabilities. In: Mitchell C, Anglin D, eds. Intimate partner violence: A health-based perspective. New York: Oxford University Press; 2009.
28. Langlois NEI, Greshman GA. The aging of bruises: A review and study of the colour changes with time. Forensic Science International. 2001;50:227–238.
29. Leshner AI. NIDA probes the elusive link between child abuse and later drug use. NIDA Notes (serial online). Retrieved September 8, 2007, from www.nida.nih.gov/NIDA_Notes/NNVol13N2/DirrepVol13N2.html; 2007.
30. Maas C, Herrenkohl TI, Sousa C. Review of research on child maltreatment and violence in youth. Trauma, Violence & Abuse. 2008;9(1):56–67.
31. Maguire S, Mann MK, Sibert J, et al. Can you age bruises accurately in children? A systematic review. Archives of Disease in Childhood. 2005;90(2):187–189.
32. McCaw B, Bauer HM, Berman WH, et al. Women referred for on-site domestic violence services in a managed care organization. Women & Health. 2002;35(2/3):23–40.
33. Mitchell C, James L. Evolving health policy on intimate partner violence. In: Mitchell C, Anglin D, eds. Intimate partner violence: A health-based perspective. New York: Oxford University Press; 2009.
34. Mosqueda L, Burnight K, Liao S. The life cycle of bruises in older adults. Journal of the American Geriatrics Society. 2005;53(8):1339–1343.
35. Murphy CC, Schei B, Myhr TL, et al. Abuse: a risk factor for low birth weight? A systematic review and meta-analysis. Canadian Medical Association Journal. 2001;164(11):1567–1572.
36. Myers JE, Berliner LA, Briere J, et al. The APSAC handbook on child maltreatment. Thousand Oaks, CA: Sage Publications; 2002.
37. Nash KR, Sheridan DJ. Can one accurately date a bruise: State of the science. Journal of Forensic Nursing. 2009;5:31–37.
38. National Center for Health Statistics. Health, United States, 2005, with chartbook on trends in the health of Americans (USDHHS Publication No 2005-1232). Hyattsville, MD: Author; 2006.
39. Nicolaidis C, Liebschutz J. Chronic physical symptoms in survivors of intimate partner violence. In: Mitchell C, Anglin D, eds. Intimate partner violence: A health-based perspective. New York: Oxford University Press; 2009.
40. O’Toole MT. Miller-Keane encyclopedia and dictionary of medicine, nursing, and allied health. 7th ed. Philadelphia: Saunders; 2005.
41. Pierce MC, Kaczor K, Aldridge S, et al. Bruising characteristics discriminating physical child abuse from accidental trauma. Pediatrics. 2010;125(1):67–74.
42. Poulos C, Sheridan DJ. Genital injuries in postmenopausal women after sexual assault. Journal of Elder Abuse & Neglect. 2008;20(4):323–335.
43. Prevent Child Abuse New York. The costs of child abuse and the urgent need for prevention. Retrieved April 8, 2010, from http://preventchildabuseny.org/pdf/cancost.pdf; 2003.
44. Reece RM, Ludwig S. Child abuse: medical diagnosis and management. 2nd ed. Philadelphia: Lippincott Williams & Wilkins; 2001.
45. Rennison CM. Intimate partner violence 1993-2001 (NCJ-197838). Washington, DC: Bureau of Justice Statistics; 2003.
46. Saltzman LE, Fanslow JL, McMahon PM, et al. Intimate partner violence surveillance: uniform definitions and recommended data elements (Version 1.0). Atlanta: National Center for Injury Prevention and Control, Centers for Disease Control and Prevention; 1999.
47. Saltzman LE, Houry D. Prevalence of nonfatal and fatal intimate partner violence in the Unites States. In: Mitchell C, Anglin D, eds. Intimate partner violence: A health-based perspective. New York: Oxford University Press; 2009.
48. Sharps P, Koziol-McLain J, Campbell J, et al. Health care providers’ missed opportunities for preventing femicide. Preventive Medicine. 2001;33:373–380.
49. Sheridan DJ. Treating survivors of intimate partner abuse: forensic identification and documentation. In: Olshaker JS, Jackson MC, Smock WS, eds. Forensic emergency medicine. Philadelphia: Lippincott Williams & Wilkins; 2001.
50. Sheridan DJ. Treating survivors of intimate partner abuse: forensic identification and documentation. In: Olshaker JS, Jackson MC, Smock WS, eds. 2007) Forensic emergency medicine. 2nd ed. Philadelphia: Lippincott Williams & Wilkins; 2007.
51. Sheridan DJ, Nash KR. Acute injury patterns of intimate partner violence. Trauma, Violence & Abuse. 2007;8(3):281–289.
52. Sheridan DJ, Nash KR, Poulos CA, et al. Soft tissue and cutaneous injury patterns. In: Mitchell C, Anglin D, eds. Intimate partner violence: a health-based perspective. New York: Oxford University Press; 2009.
53. Soeken K, McFarlane J, Parker B, et al. The abuse assessment screen: a clinical instrument to measure frequency, severity, and perpetrator of abuse against women. In: Campbell JC, ed. Empowering survivors of abuse: Health care for battered women and their children. Newbury Park, CA: Sage; 1998.
54. Sugar NF, Taylor JA, Feldman KW. Bruises in infants and toddlers: Those who don’t cruise rarely bruise. Archives of Pediatrics & Adolescent Medicine. 1999;153(4):399–403.
55. Taliaferro E, Hawley D, McClane G, et al. Strangulation in intimate partner violence. In: Mitchell C, Anglin D, eds. Intimate partner violence: a health-based perspective. New York: Oxford University Press; 2009.
56. Tjaden P, Thoennes N. Full report of the prevalence, incidence, and consequences of violence against women (NCJ-183781). Washington, DC: National Institute of Justice; 2000.
57. U.S. Department of Health and Human Services, Administration on Children, Youth and Families. Child maltreatment 2007. Washington, DC: U.S. Government Printing Office; 2009; Retrieved January 26, 2010, from www.acf.hhs.gov/programs/cb/stats_research/index.htm#can; 2009.
58. Warrier S. Culture and cultural competency in addressing intimate partner violence. (2009). In: Mitchell C, Anglin D, eds. Intimate partner violence: A health-based perspective. New York: Oxford University Press; 2009.
59. Warsaw C, Brashler P, Gil J. Mental health consequence of intimate partner violence. (2009). In: Mitchell C, Anglin D, eds. Intimate partner violence: A health-based perspective. New York: Oxford University Press; 2009.