Abdomen

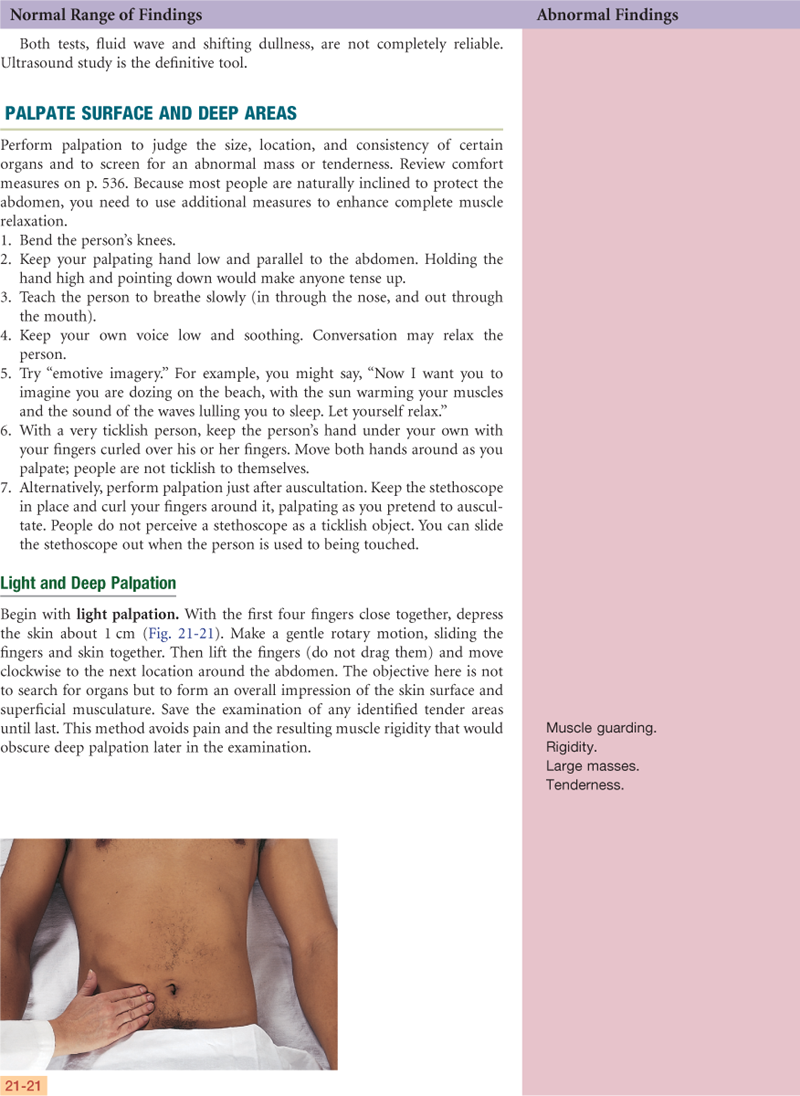
http://evolve.elsevier.com/Jarvis/
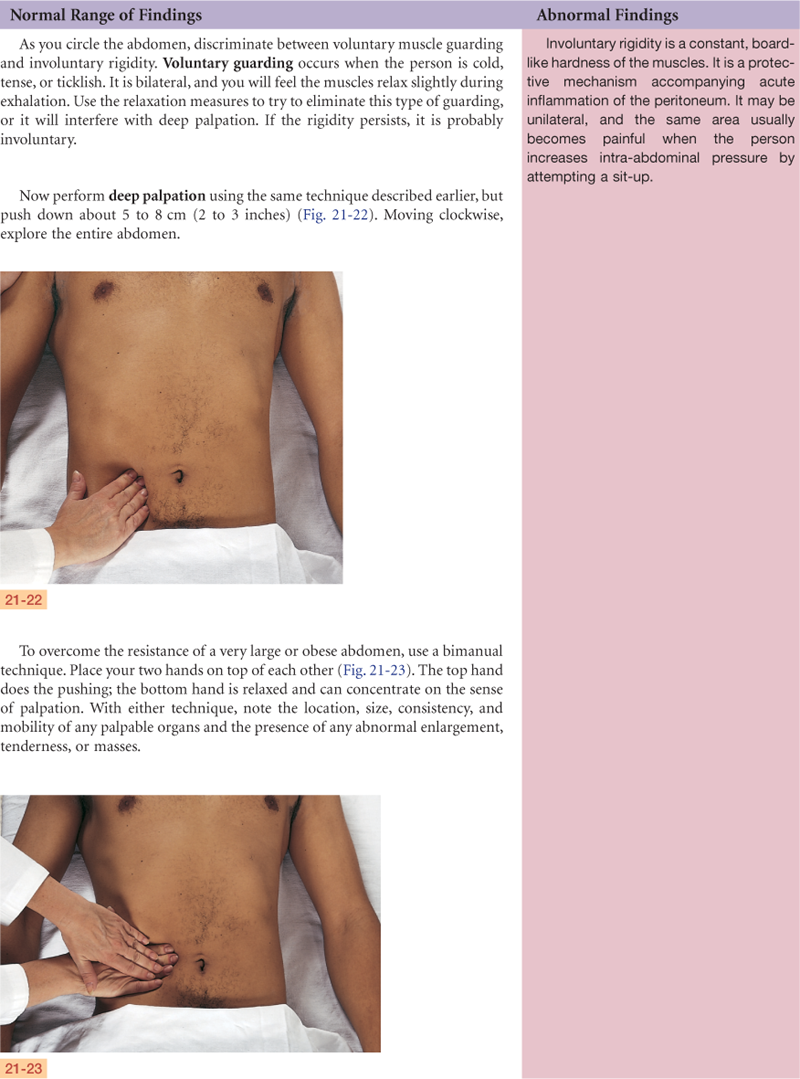
• Bedside Assessment Summary Checklist
• Physical Examination Summary Checklist
• Quick Assessment for Common Conditions
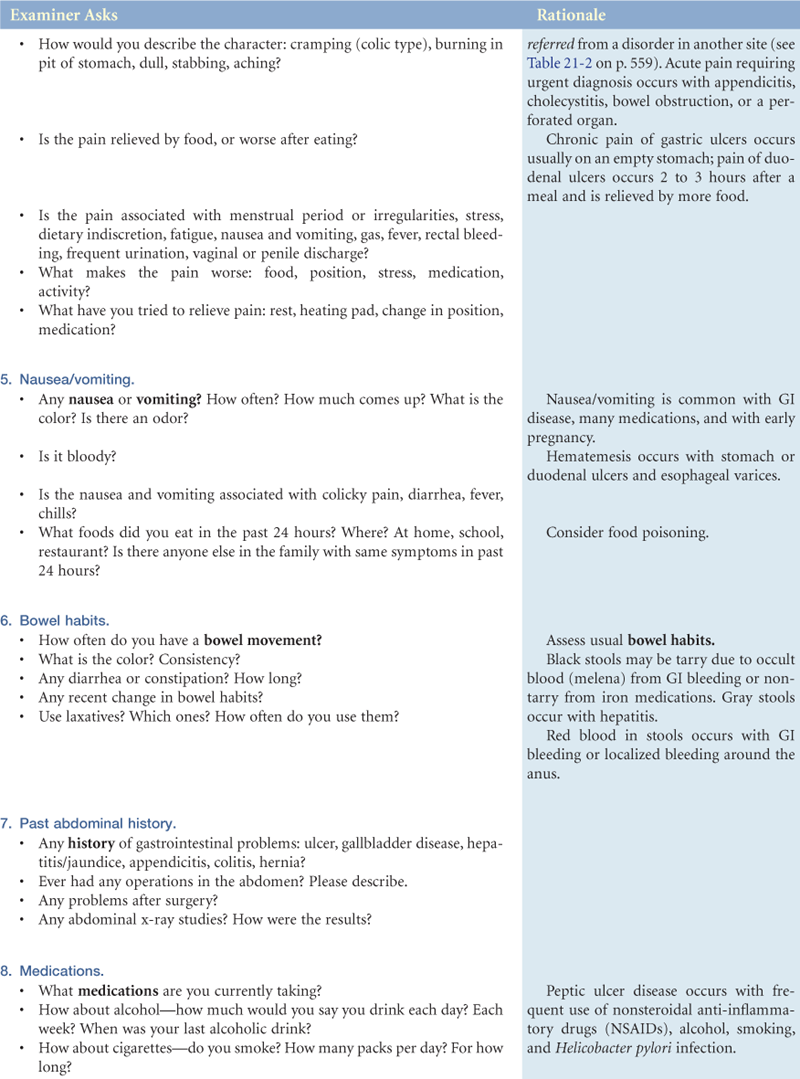
Peptic Ulcer Disease
Structure and Function
Surface Landmarks
The abdomen is a large, oval cavity extending from the diaphragm down to the brim of the pelvis. It is bordered in back by the vertebral column and paravertebral muscles and at the sides and front by the lower rib cage and abdominal muscles (Fig. 21-1). Four layers of large, flat muscles form the ventral abdominal wall. These are joined at the midline by a tendinous seam, the linea alba. One set, the rectus abdominis, forms a strip extending the length of the midline, and its edge is often palpable. The muscles protect and hold the organs in place, and they flex the vertebral column.
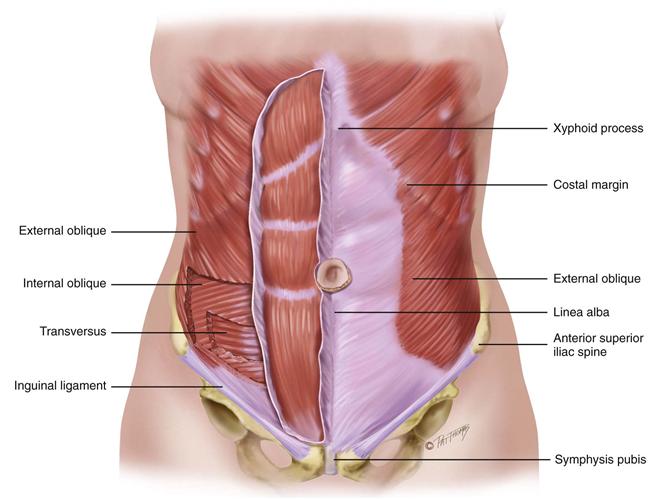
21-1 Copyright © (2006) © Pat Thomas, 2006.
Internal Anatomy
Inside the abdominal cavity, all the internal organs are called the viscera. It is important that you know the location of these organs so well that you could draw a map of them on the skin (Fig. 21-2). You must be able to visualize each organ that you listen to or palpate through the abdominal wall.
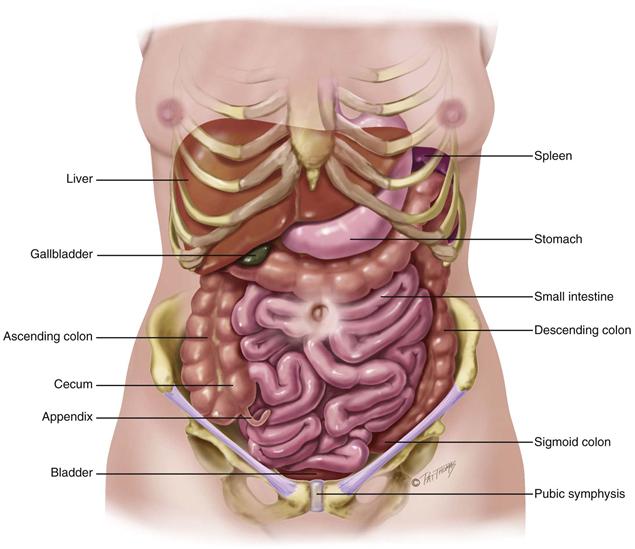
21-2 Copyright © (2006) © Pat Thomas, 2006.
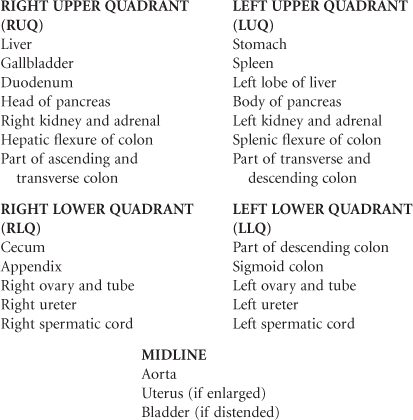
The solid viscera are those that maintain a characteristic shape (liver, pancreas, spleen, adrenal glands, kidneys, ovaries, and uterus). The liver fills most of the right upper quadrant (RUQ) and extends over to the left midclavicular line. The lower edge of the liver and the right kidney normally may be palpable. The ovaries normally are palpable only on bimanual examination during the pelvic examination.
The shape of the hollow viscera (stomach, gallbladder, small intestine, colon, and bladder) depends on the contents. They usually are not palpable, although you may feel a colon distended with feces or a bladder distended with urine. The stomach is just below the diaphragm, between the liver and spleen. The gallbladder rests under the posterior surface of the liver, just lateral to the right midclavicular line. Note that the small intestine is located in all four quadrants. It extends from the stomach’s pyloric valve to the ileocecal valve in the right lower quadrant (RLQ), where it joins the colon.
The spleen is a soft mass of lymphatic tissue on the posterolateral wall of the abdominal cavity, immediately under the diaphragm (Fig. 21-3). It lies obliquely with its long axis behind and parallel to the tenth rib, lateral to the midaxillary line. Its width extends from the ninth to the eleventh rib, about 7 cm. It is not palpable normally. If it becomes enlarged, its lower pole moves downward and toward the midline.
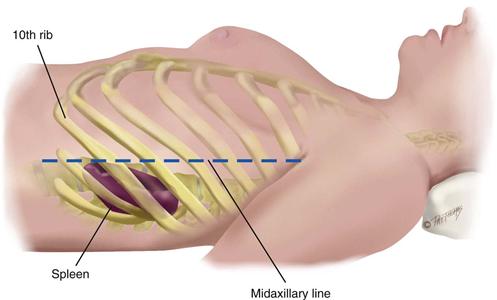
21-3 Copyright © (2006) © Pat Thomas, 2006.
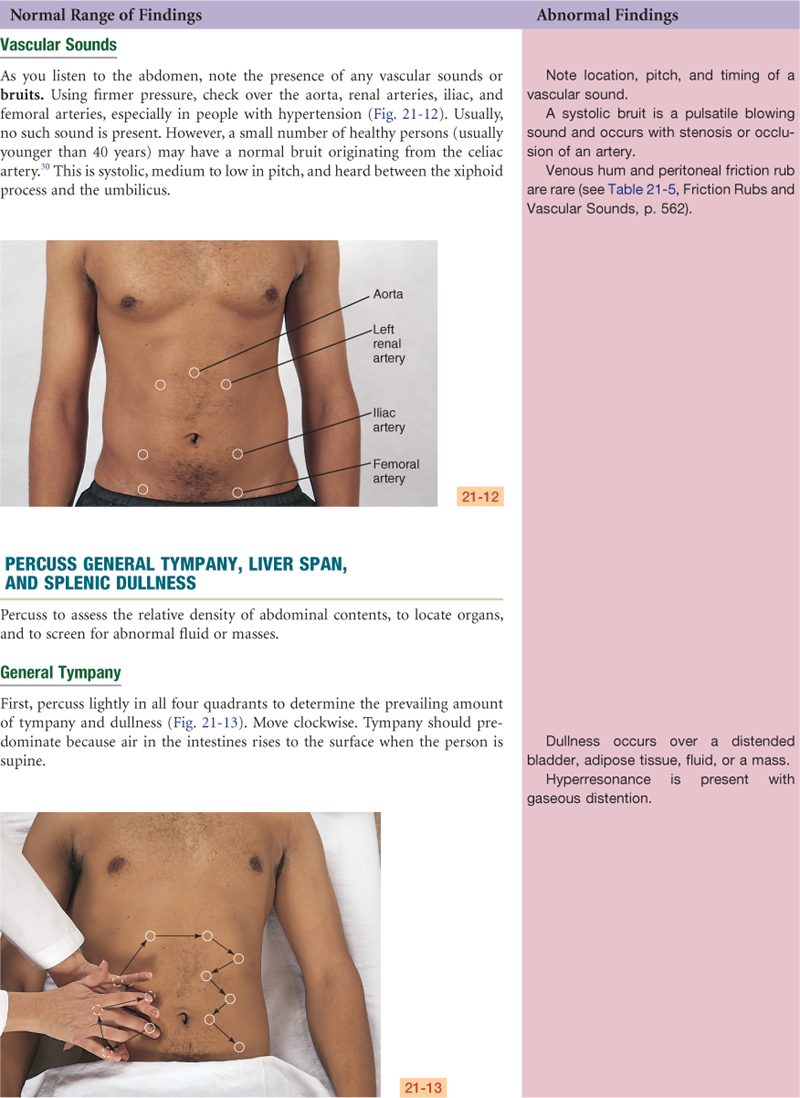
The aorta is just to the left of midline in the upper part of the abdomen (Fig. 21-4). It descends behind the peritoneum, and at 2 cm below the umbilicus, it bifurcates into the right and left common iliac arteries opposite the fourth lumbar vertebra. You can palpate the aortic pulsations easily in the upper anterior abdominal wall. The right and left iliac arteries become the femoral arteries in the groin area. Their pulsations are easily palpated as well, at a point halfway between the anterior superior iliac spine and the symphysis pubis.
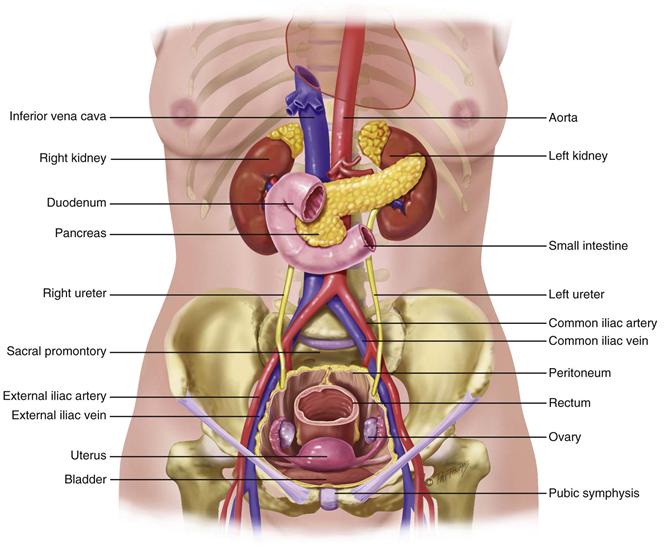
21-4 Copyright © (2006) © Pat Thomas, 2006.
The pancreas is a soft, lobulated gland located behind the stomach. It stretches obliquely across the posterior abdominal wall to the left upper quadrant.
The bean-shaped kidneys are retroperitoneal, or posterior to the abdominal contents (Fig. 21-5). They are well protected by the posterior ribs and musculature. The twelfth rib forms an angle with the vertebral column, the costovertebral angle. The left kidney lies here at the eleventh and twelfth ribs. Because of the placement of the liver, the right kidney rests 1 to 2 cm lower than the left kidney and sometimes may be palpable.
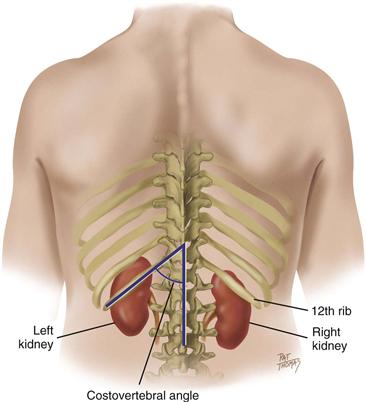
21-5
For convenience in description, the abdominal wall is divided into four quadrants by a vertical and a horizontal line bisecting the umbilicus (Fig. 21-6). (An older, more complicated scheme divided the abdomen into nine regions. Although the old system generally is not used, some regional names persist, such as epigastric for the area between the costal margins, umbilical for the area around the umbilicus, and hypogastric or suprapubic for the area above the pubic bone.)
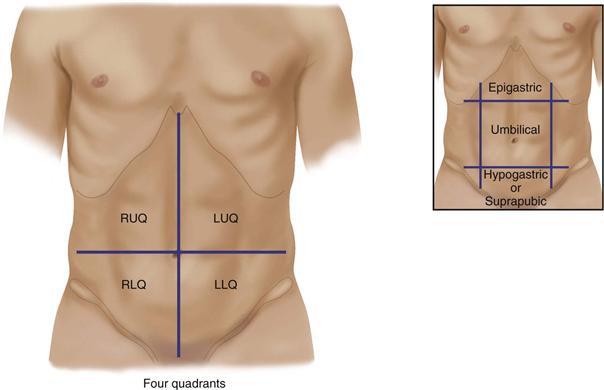
21-6
The anatomic location of the organs by quadrants is as follows:
 Developmental Competence
Developmental Competence
Infants and Children
In the newborn, the umbilical cord shows prominently on the abdomen. It contains two arteries and one vein. The liver takes up proportionately more space in the abdomen at birth than in later life. In healthy term neonates, the lower edge may be palpated 0.5 to 2.5 cm below the right costal margin. Age-related values of expected liver span are listed in the Objective Data section. The urinary bladder is located higher in the abdomen than in the adult. It lies between the symphysis and the umbilicus. Also, during early childhood, the abdominal wall is less muscular, so the organs may be easier to palpate.
The Pregnant Woman
Nausea and vomiting, or “morning sickness,” is an early sign of pregnancy for most pregnant women, starting between the first and second missed periods. The cause is unknown but may be due to hormone changes such as the production of human chorionic gonadotropin (hCG). Another symptom is “acid indigestion” or heartburn (pyrosis) caused by esophageal reflux. Gastrointestinal motility decreases, which prolongs gastric emptying time. The decreased motility causes more water to be reabsorbed from the colon, which leads to constipation. The constipation, as well as increased venous pressure in the lower pelvis, may lead to hemorrhoids.
The enlarging uterus displaces the intestines upward and posteriorly. Bowel sounds are diminished. Traditional thinking was that the appendix was displaced upward and to the right. But clinical evidence has contradicted this and have shown that pregnancy does not change the location of the appendix.19,33 Any appendicitis-related pain during pregnancy would still be felt in the right lower quadrant. Finally, skin changes on the abdomen, such as striae and linea nigra, are discussed later in this chapter on p. 537 and in Chapter 12.
The Aging Adult
Aging alters the appearance of the abdominal wall. During and after middle age, some fat accumulates in the suprapubic area in females as a result of decreased estrogen levels. Males also show some fat deposits in the abdominal area, resulting in the “big belly.” This accentuates in adults with a more sedentary lifestyle.
With further aging, adipose tissue is redistributed away from the face and extremities and to the abdomen and hips. The abdominal musculature relaxes.
Changes of aging occur in the gastrointestinal system but do not significantly affect function as long as no disease is present.
• Salivation decreases, causing a dry mouth and a decreased sense of taste (discussed in Chapter 16).
• Esophageal emptying is delayed. If an aging person is fed in the supine position, this increases risk for aspiration.
• Gastric acid secretion decreases with aging. This may cause pernicious anemia (because it interferes with vitamin B12 absorption), iron deficiency anemia, and malabsorption of calcium.
• The incidence of gallstones increases with age, occurring in 10% to 20% of middle-aged and older adults, being more common in females.
• Liver size decreases by 25% between the ages of 20 and 70 years, although most liver function remains normal. Drug metabolism by the liver is impaired, in part because by age 65, blood flow through the liver is decreased by 33%.12 Therefore the liver metabolism that is responsible for the enzymatic oxidation, reduction, and hydrolysis of drugs is substantially decreased with age. Prolonged liver metabolism causes increased side effects (e.g., older people taking benzodiazepines scored lower on functional status measures and had increased risk for hip fracture).38
• Aging persons frequently report constipation; most prevalence estimates are between 12% and 19%.18 Because there is confusion as to what defines constipation, the Rome criteria28 have been developed as standardized symptom criteria. These symptoms include reduced stool frequency (less than 3 bowel movements per week), as well as other common and troubling associated symptoms (i.e., straining, lumpy or hard stool, feeling of incomplete evacuation, feeling of anorectal blockage, use of manual maneuvers).
Common causes of constipation include decreased physical activity, inadequate intake of water, a low-fiber diet, side effects of medications (opioids, tricyclic antidepressants), irritable bowel syndrome, bowel obstruction, hypothyroidism, and inadequate toilet facilities (i.e., difficulty ambulating to the toilet may cause the person to deliberately retain the stool until it becomes hard and difficult to pass).
 Culture and genetics
Culture and genetics
Lactase is the digestive enzyme necessary for absorption of the carbohydrate lactose (milk sugar). In some racial groups, lactase activity is high at birth but declines to low levels by adulthood. These people are lactose intolerant and have abdominal pain, bloating, and flatulence when milk products are consumed. Millions of American adults have the potential for lactose-intolerance symptoms, and traditional estimated rates were that 15% of whites, 50% of Mexican Americans, and 80% of African Americans had the condition. Yet a recent study found the prevalence rates in practical life settings is significantly lower than previously estimated rates.36 When subjects were screened for symptoms following a typical serving of dairy food in the home setting, lactose-intolerance prevalence estimates were 7.72% for whites, 19.5% for African Americans, and 10% for Hispanics.36 This is clinically significant because dairy foods meet crucial nutritional requirements including calcium, magnesium, and potassium. If people perceive themselves to be lactose intolerant based on racial heritage, the lowered calcium intake may affect bone health. Health care providers should encourage low-fat or fat-free daily foods and monitor any symptoms.
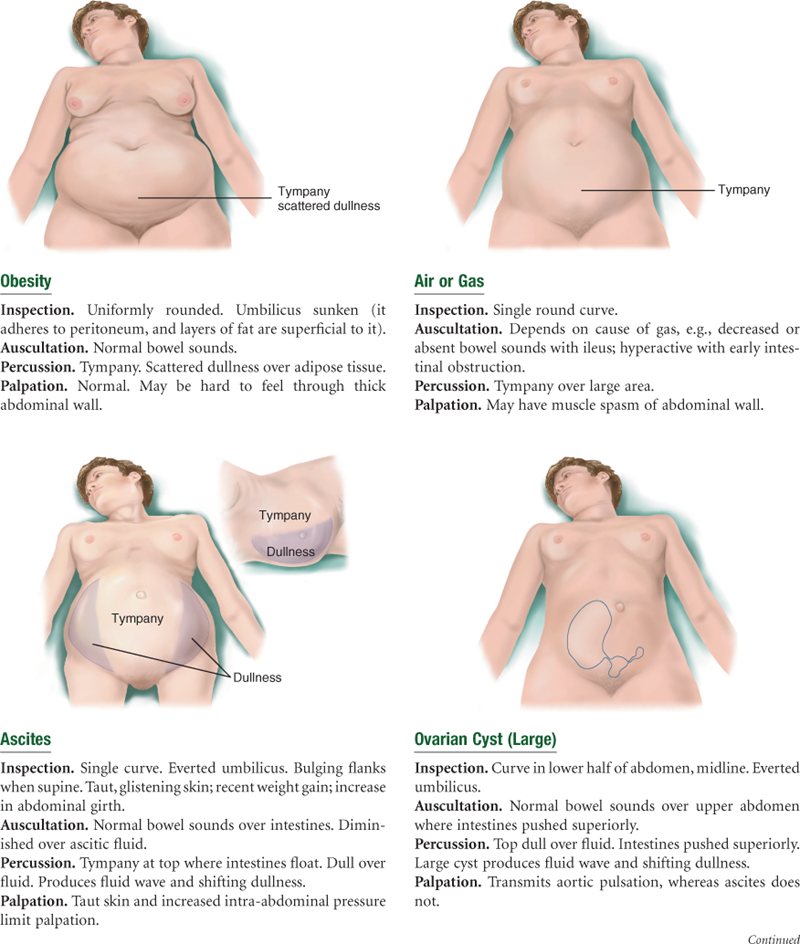
Obesity is the accumulation of excess body fat. Obesity is caused by a complex interaction of genetic predisposition, dietary intake, physical inactivity, and what is now called an “obesogenic” environment16 (one that encourages large portions of high-fat, energy-dense food). The prevalence of obesity has increased in the United States and globally. Currently, one third of American adults are obese (BMI ≥30 kg/m2), and by 2015, the estimates are that 40% or more U.S. adults will be obese.44
Data from the National Health and Nutrition Examination Survey (NHANES) show significant differences among racial/ethnic groups.37 Among children, Mexican-American boys had a greater prevalence of overweight than had white or Black boys. Mexican-American and Black girls were significantly more likely to be overweight than white girls. No differences were found in overweight rates in men of various racial groups. But in adult women, Mexican Americans and African Americans were significantly more likely to be obese than were whites.
Obesity in adults results in comorbidities of type 2 diabetes and cardiovascular disease. Obese children have an increased risk for asthma, diabetes, liver disease, cardiovascular disease, sleep apnea, and joint problems, and they risk becoming obese adults.25 Controlling the obesity epidemic will be important in containing health care costs. Do Americans view obesity as a threat in the same way they now view the dangers of smoking? A change in public awareness and public thinking to regard obesity as a “common enemy” has been proposed to garner public support.25 The areas for needed change are vast and include personal, community, and government strategies. Recommendations include the following25:
Making healthful food and beverages more widely available; providing access to healthier food by locating stores in underserved areas; and decreasing the availability of less healthful food and beverages. … discourage consumption of sugar-sweetened beverages; increased support for breastfeeding; linkages between local farms and institutions to increase fruit and vegetable consumption; shifts in agricultural policy; and improved community infrastructure to promote biking, walking, and use of public transit.

 Documentation and Critical Thinking
Documentation and Critical Thinking
Sample Charting
Subjective
States appetite is good with no recent change, no dysphagia, no food intolerance, no pain, no nausea/vomiting. Has one formed BM/day. Takes vitamins, no other prescribed or over-the-counter medication. No history of abdominal disease, injury, or surgery. Diet recall of past 24 hours listed at end of history.
Objective
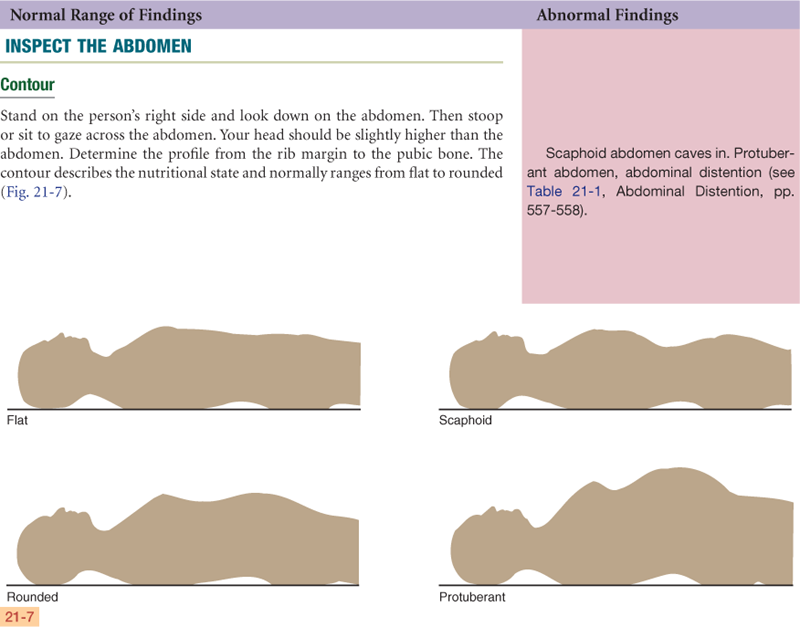
Inspection: Abdomen flat, symmetric, with no apparent masses. Skin smooth with no striae, scars, or lesions.
Auscultation: Bowel sounds present, no bruits.
Percussion: Tympany predominates in all four quadrants, liver span is 8 cm in right midclavicular line. Splenic dullness located at tenth intercostal space in left midaxillary line.
Palpation: Abdomen soft, no organomegaly, no masses, no tenderness.
Assessment
Healthy abdomen, bowel sounds present
Focused Assessment: Clinical Case Study 1
George E. is a 58-year-old unemployed divorced white male with chronic alcoholism who enters the chemical dependency treatment center.
Subjective
States past 6 months has been drinking 1 pint whiskey/day. Last alcohol use 1 week PTA, with “5 or 6” drinks that episode. Estranged from family, lives alone. Makes a few meals on hot plate. States never has appetite. Has fatigue and weakness.
Objective
Inspection: Appears older than stated age. Oriented, although verbal response time slowed. Weight loss of 12 lb in past 3 mo.
Abdomen protuberant, symmetric, no visible masses. Poor skin turgor. Dilated venous pattern over abdominal wall. Hair sparse in axillary, pubic area.
Auscultation: Bowel sounds present. No vascular sounds.
Percussion: Tympany predominates over abdomen. Liver span is 16 cm in right midclavicular line. No fluid wave. No shifting dullness.
Palpation: Soft. Liver palpable 10 cm below right costal margin, smooth and nontender. No other organomegaly or masses.
Assessment
Alcohol dependence, severe, with physiologic dependence
Imbalanced nutrition: less than body requirements R/T impaired absorption
Ineffective coping R/T effects of chronic alcoholism
Social isolation
Focused Assessment: Clinical Case Study 2
Edith J. is a 63-year-old retired homemaker with a history of lung cancer with metastasis to the liver.
Subjective
Feeling “puffy and bloated” for the past week. States unable to get comfortable. Also short of breath “all the time now.” Difficulty sleeping. “I feel like crying all the time now.”
Objective
Inspection: Weight increase of 8 lb in 1 week. Abdomen is distended with everted umbilicus and bulging flanks. Girth at umbilicus is 85 cm. Prominent dilated venous pattern present over abdomen.
Auscultation: Bowel sounds present, no vascular sounds.
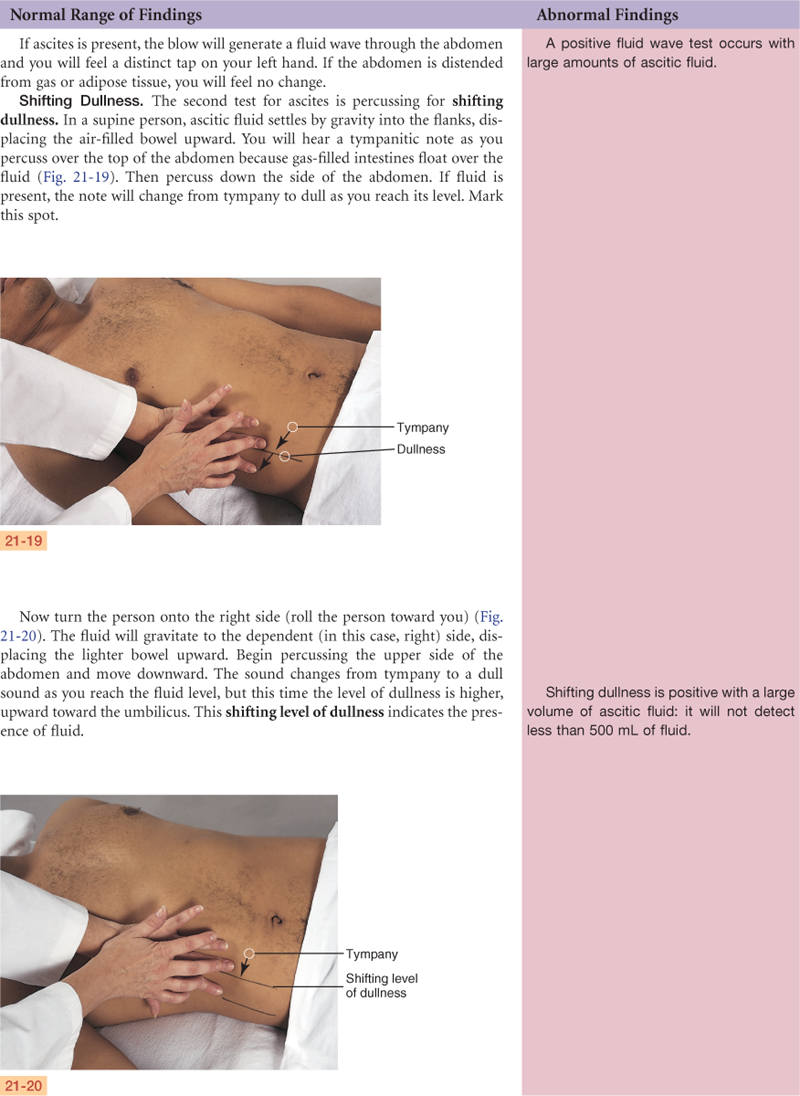
Percussion: When supine, tympany present at dome of abdomen, dullness over flanks. Shifting dullness present. Positive fluid wave present. Liver span is 12 cm in right midclavicular line.
Palpation: Abdominal wall firm, able to feel liver with deep palpation at 6 cm below right costal margin. Liver feels firm, nodular, nontender. 4+ pitting edema in both ankles.
Assessment
Ascites
Grieving
Ineffective breathing pattern R/T increased intra-abdominal pressure
Pain R/T distended abdomen
Risk for impaired skin integrity R/T ascites, edema, and faulty metabolism
Insomnia
Focused Assessment: Clinical Case Study 3
Dan G. is a 17-year-old Black male high school student who enters the emergency department with abdominal pain for 2 days.
Subjective
Two days PTA, Dan noted general abdominal pain in umbilical region. Now pain is sharp and severe, and Dan points to location in right lower quadrant. No BM for 2 days. Nausea and vomiting off and on 1 day.
Objective
Inspection: BP 112/70, Temp 38° C, pulse 116, resp 18.
Lying on side with knees drawn up under chin. Resists any movement. Face tight and occasionally grimacing. Cries out with any sudden movement.
Auscultation: No bowel sounds present. No vascular sounds.
Percussion: Tympany. Percussion over RLQ leads to tenderness.
Palpation: Abdominal wall is rigid and boardlike. Extreme tenderness to palpation in RLQ. Rebound tenderness is present in RLQ. Positive iliopsoas muscle test.
Assessment
Acute abdominal pain in RLQ
Nausea
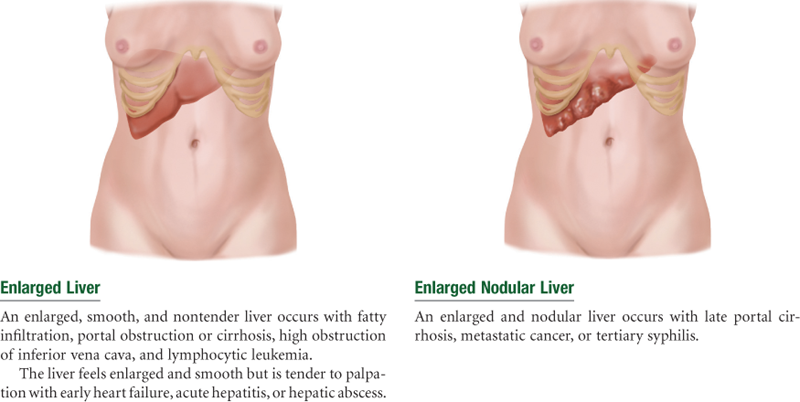
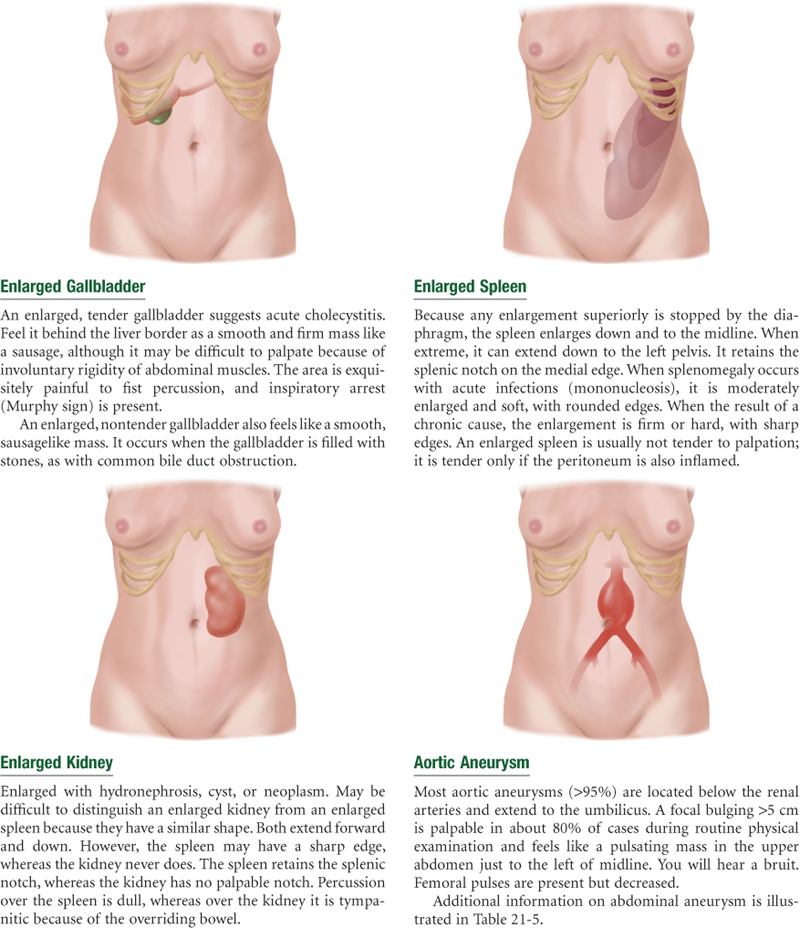
Abnormal Findings for Advanced Practice
Summary Checklist: Abdomen Examination
 For a PDA-downloadable version, go to http://evolve.elsevier.com/Jarvis/.
For a PDA-downloadable version, go to http://evolve.elsevier.com/Jarvis/.
Bibliography
1. Ambinder M. Beating obesity. The Atlantic 2010, May;:72–83.
2. Amerine E. Get optimum outcomes for acute pancreatitis patients. Nurse Practitioner. 2007;32(6):2007.
3. Anwar A. Benzodiazepines: uses, mode of action and prescribing issues. Nurse Prescribing. 2008;6(12):544–548.
4. Apovian CM. The causes, prevalence, and treatment of obesity revisited in 2009: what have we learned so far? American Journal of Clinical Nutrition. 2010;91(1):77S–279S.
5. Bartley MK. Acute abdominal pain: a diagnostic challenge. Nurse Practitioner. 2008;33(3):34–39.
6. Becker AE, Eddy KT, Perloe A. Clarifying criteria for cognitive signs and symptoms for eating disorders in DSM-V. International Journal of Eating Disorders. 2009;42(7):611–619.
7. Biro FM, Wien M. Childhood obesity and adult morbidities. American Journal of Clinical Nutrition. 2010;91:1499S–1505S.
8. Bollinger RR, Barbas AS, Bush EL, et al. Biofilms in the large bowel suggest an apparent function of the human vermiform appendix. Journal of Theoretical Biology. 2007;249:826–831.
9. Brenner ZR, Krenzer ME. Understanding acute pancreatitis. Nursing. 2010;40(1):32–38.
10. Budd GM, Falkenstein K. Bariatric surgery: putting the squeeze on obesity. Nurse Practitioner. 2009;34(7):39–46.
11. Fitzgerald MA. Nonalcoholic fatty liver disease. Nurse Practitioner. 2007;32(2):24–25.
12. Frith J, Jones D, Newton JL. Chronic liver disease in an ageing population. Age and Ageing. 2009;38(1):11–18.
13. Gujral H, Collantes RS. Understanding viral hepatitis: a guide for primary care. Nurse Practitioner. 2009;34(12):23–32.
14. Halpert AD. Importance of early diagnosis in patients with irritable bowel syndrome. Postgraduate Medicine. 2010;122(2):102–111.
15. Harmon HW. Treatment options for irritable bowel syndrome. Nurse Practitioner. 2007;32(7):39–43.
16. Heber D. An integrative view of obesity. American Journal of Clinical Nutrition. 2010;91(1):280S–283S.
17. Heitkemper M, Wolff J. Challenges in chronic constipation management. Nurse Practitioner. 2007;32(4):36–43.
18. Higgins PD, Johanson JF. Epidemiology of constipation in North America: a systematic review. American Journal of Gastroenterology. 2004;99(4):750–759.
19. Hodjati H, Kazerooni T. Location of the appendix in the gravid patient: a re-evaluation of the established concept. International Journal of Gynaecology and Obstetrics. 2003;81(3):245–247.
20. Holloway TJ. The root of the problem: an irritable bowel or an average American lifestyle? Gastrointestinal. Nursing. 2010;8(1):31–37.
21. Howland RH. Effects of aging on pharmacokinetic and pharmacodynamic drug processes. Journal of Psychosocial Nursing and Mental Health Services. 2009;47(10):15–18.
22. Jacobson BC, Somers SC, Fuchs CS, et al. Body-mass index and symptoms of gastroesophageal reflux in women. New England Journal of Medicine. 2006;354(2340-2348):2405–2408.
23. Kelso LA. Cirrhosis: caring for patients with end-stage liver failure. Nurse Practitioner. 2008;33(7):24–31.
24. King J. Infectious mononucleosis: update and considerations. Nurse Practitioner. 2009;34(11):42–45.
25. Klein JD, Dietz W. Childhood obesity: the new tobacco. Health Affairs. 2010;29(3):388–392.
26. Kortgen A, Recknagel P, Bauer M. How to assess liver function? Current Opinion in Critical Care. 2010;16(2):126–141.
27. Lawson EE, Grand RJ, Neff RK, et al. Clinical estimation of liver span in infants and children. Archives of Pediatrics & Adolescent Medicine. 1978;132:474–476.
28. Longsterth GF, Thompson WG, Chey WD, et al. Functional bowel disorders. Gastroenterology. 2006;130:1480–1491.
29. Madsen D, Sebolt T, Cullen L, et al. Listening to bowel sounds: an evidence-based practice project. American Journal of Nursing. 2005;105(12):40–50.
30. McGee S. Evidence based physical diagnosis. 2nd ed. Philadelphia: Saunders; 2007.
31. Meier P, Seitz HK. Age, alcohol metabolism and liver disease. Current Opinion in Clinical Nutrition and Metabolic Care. 2008;11(1):21–26.
32. Miller S, Alpert P. Assessment and differential diagnosis of abdominal pain. Nurse Practitioner. 2006;31:39–47.
33. Mourad J, Elliott JP, Erickson L, Lisboa L. Appendicitis in pregnancy: new information that contradicts long-held clinical beliefs. American Journal of Obstetrics and Gynecology. 2000;182(5):1027–1029.
34. Murphy MA, Colwell C, Pineda G, et al. Abdominal pain: a review of select conditions. EMS Magazine. 2010;39(1):68–74.
35. Nguyen DM, El-Serag HB. The epidemiology of obesity. Gastroenterology Clinics of North America. 2010;39(1):1–7.
36. Nicklas TA, Qu H, Hughes SO, et al. Prevalence of self-reported lactose intolerance in a multiethnic sample of adults. Nutrition Today. 2009;44(5):222–229.
37. Ogden CL, Carroll MD, Curtin LR, et al. Prevalence of overweight and obesity in the United States, 1999-2004. Journal of the American Medical Association. 2006;295(13):1549–1555.
38. Reid LD, Johnson RE, Gettman DA. Benzodiazepine exposure and functional status in older people. Journal of the American Geriatrics Society. 1998;46:71–76.
39. Riley L, Rubin M. A guide to physical examination and history taking of the abdomen. Gastroenterology Nursing. 2010;33(2):167.
40. Schiodt FV, Chung RT, Schilsky ML, et al. Outcome of acute liver failure in the elderly Liver. Transplantation. 2009;15(11):1481–1487.
41. Sheipe M. Breaking through obesity with gastric bypass surgery. Nurse Practioner. 2006;31(10):13–23.
42. Tekwani K, Sikka R. High-risk chief complaints III: abdomen and extremities. Emergency Medicine Clinics of North America. 2009;27(4):747–765.
43. Tucker WN, Saab S, Rickman LS, Mathews WC. The scratch test is unreliable for detecting the liver edge. Journal of Clinical Gastroenterology. 1997;25:410–414.
44. Wang Y, Beydoun MA. The obesity epidemic in the United States—gender, age, socioeconomic, racial/ethnic, and geographic characteristics: a systematic review and meta-regression analysis. Epidemiologic Reviews. 2007;29:6–28.
45. Zimmerman PG. Is it appendicitis? American Journal of Nursing. 2008;108(9):27–32.