The Pregnant Woman
Outline
Pregnancy and the Endocrine Placenta
Changes During Normal Pregnancy
Routine Laboratory and Radiologic Imaging Studies

http://evolve.elsevier.com/Jarvis/
• Bedside Assessment Summary Checklist
• Head-to-Toe Examination of the Pregnant Woman
• Physical Examination Summary Checklist
Structure and Function
Pregnancy and the Endocrine Placenta
The first day of the menses is day 1 of the menstrual cycle. For the first 14 days of the cycle, one or more follicles in the ovary develop and mature. One follicle grows faster than the others, and on day 14 of the menstrual cycle, this dominant follicle ruptures and ovulation occurs. If the ovum meets viable sperm, fertilization occurs somewhere in the oviduct (fallopian tube). The remaining cells in the follicle form the corpus luteum, or “yellow body,” which makes important hormones. Chief among these is progesterone, which prevents the sloughing of the endometrial wall, ensuring a rich vascular network into which the fertilized ovum will implant.
The fertilized ovum, now called the blastocyst, continues to divide, differentiate, and grow rapidly. Specialized cells in the blastocyst produce human chorionic gonadotropin (hCG), which stimulates the corpus luteum to continue making progesterone. Between days 20 and 24, the blastocyst implants into the wall of the uterus, which may cause a small amount of vaginal bleeding. A specialized layer of cells around the blastocyst becomes the placenta. The placenta starts to produce progesterone to support the pregnancy at 7 weeks and takes over this function completely from the corpus luteum at about 10 weeks.
The placenta functions as an endocrine organ and produces several hormones. These hormones help in the growth and maintenance of the fetus, and they direct changes in the woman’s body to prepare for birth and lactation. The hCG stimulates the rise in progesterone during pregnancy. Progesterone maintains the endometrium around the fetus, increases the alveoli in the breast, and keeps the uterus in a quiescent state. Estrogen stimulates the duct formation in the breasts, increases the weight of the uterus, and increases certain receptors in the uterus that are important at birth.
The average length of pregnancy is 280 days from the first day of the last menstrual period (LMP), which is equal to 40 weeks, 10 lunar months, or 9 calendar months. Note that this includes the 2 weeks when the follicle was maturing but before conception actually occurred. Pregnancy is divided into three trimesters: (1) the first 12 weeks, (2) from 13 to 27 weeks, and (3) from 28 weeks to delivery.
A woman who is pregnant for the first time is called a primigravida. After she delivers, she is called a primipara. The multigravida is a pregnant woman who has previously carried a fetus to the point of viability. She is a multipara after delivery. Any pregnant woman might be called a gravida. Commonly used terminology is G (gravida), P (para), T (term), PT (preterm deliveries), A (abortion—missed, therapeutic, voluntary), L (living children). It may be written as G5 T3 PT0 A2 L3.
Changes During Normal Pregnancy
Pregnancy is diagnosed by three types of signs and symptoms. Presumptive signs are those the woman experiences, such as amenorrhea, breast tenderness, nausea, fatigue, and increased urinary frequency. Probable signs are those detected by the examiner, such as an enlarged uterus. Positive signs of pregnancy are those that are direct evidence of the fetus, such as the auscultation of fetal heart tones (FHTs) or positive cardiac activity on ultrasound (US).
First Trimester
Conception occurs on approximately the 14th day of the menstrual cycle. The blastocyst (developing fertilized ovum) implants in the uterus 6 to 10 days after conception, sometimes accompanied by a small amount of painless bleeding, which may be interpreted as a menstrual period.14 The serum hCG becomes positive after implantation when it is first detectable in maternal serum at approximately 8 to 11 days after conception.
The following menstrual period is missed. At the time of the missed menses, hCG can be detected in the urine. Breast tingling and tenderness begin as the rising estrogen levels promote mammary growth and development of the ductal system; progesterone stimulates the alveolar system as well as the mammary growth. Chorionic somatomammotropin (also called human placental lactogen or hPL), also produced by the placenta, stimulates breast growth and exerts lactogenic properties.40 More than half of all pregnant women have nausea and vomiting. The cause is unclear but may involve the hormonal changes of pregnancy, low blood sugar, gastric overloading, slowed peristalsis, an enlarging uterus, and emotional factors. Fatigue is common and may be related to the initial fall in metabolic rate that occurs in early pregnancy.40
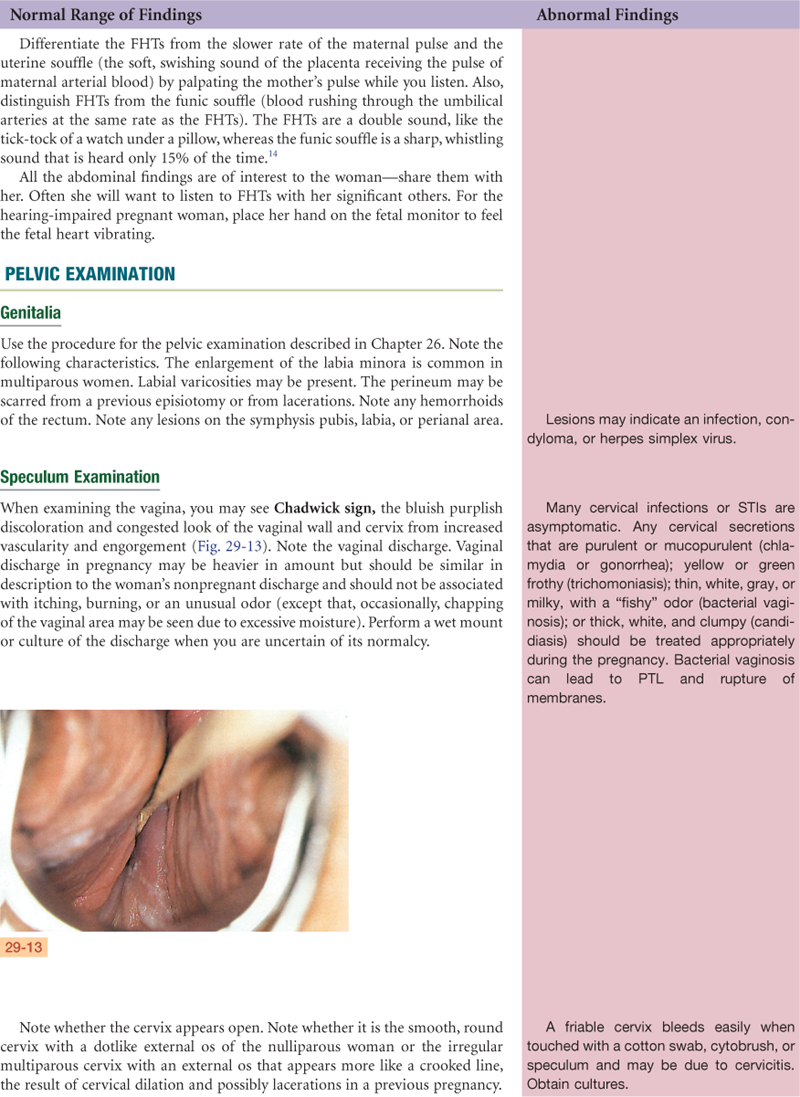
Estrogen and possibly progesterone cause hypertrophy of the uterine muscle cells, and uterine blood vessels and lymphatics enlarge. The uterus becomes globular in shape, softens, and flexes easily over the cervix (Hegar sign). This causes compression of the bladder, which results in urinary frequency. Increased vascularity, congestion, and edema cause the cervix to soften (Goodell sign) and become bluish purple (Chadwick sign).
Early first-trimester blood pressures (BPs) reflect prepregnancy values. In the 7th gestational week, BP begins to drop until mid-pregnancy as a result of falling peripheral vascular resistance. The BP gradually returns to the nonpregnant baseline by term. Systemic vascular resistance decreases from the vasodilatory effect of progesterone and prostaglandins and possibly because of the low resistance of the placental bed.13
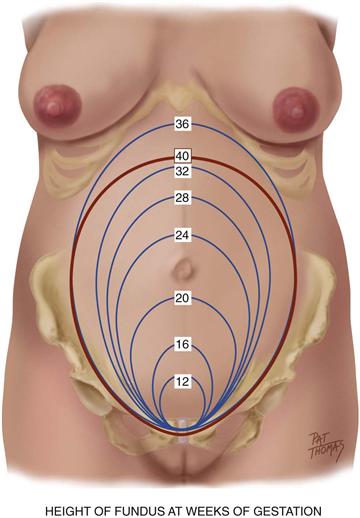
At the end of 9 weeks, the embryonic period ends and the fetal period begins, at which time major structures are present.40 FHTs can be heard by Doppler US between 9 and 12 weeks. The uterus may be palpated just above the symphysis pubis at about 12 weeks. See Fig. 29-1 for growth of the uterine fundus during the first trimester.
29-1
When the pregnancy is viable, a gestational sac should be visible on transvaginal ultrasound by 5 weeks gestation or when the maternal serum hCG level is between 1100 and 1500 mU/mL.13 When a fertilized egg develops a placenta and membranes but no embryo, this is called a blighted ovum. With this, the hCG levels will rise early on, then begin to drop, and vaginal bleeding ensues. Some women will not be aware that they were pregnant.
Second Trimester
By weeks 12 to 16, the nausea, vomiting, fatigue, and urinary frequency of the first trimester improve. The woman recognizes fetal movement (“quickening”) at approximately 18 to 20 weeks (the multigravida earlier). As breast enlargement continues, the veins of the breast enlarge and are more visible through the skin of lightly pigmented women. Colostrum, the precursor of milk, may be expressed from the nipples. Colostrum is yellow in color and contains more minerals and protein but less sugar and fat than mature milk. Colostrum also contains antibodies, which are protective for the newborn during its first days of life until mature milk production begins.14
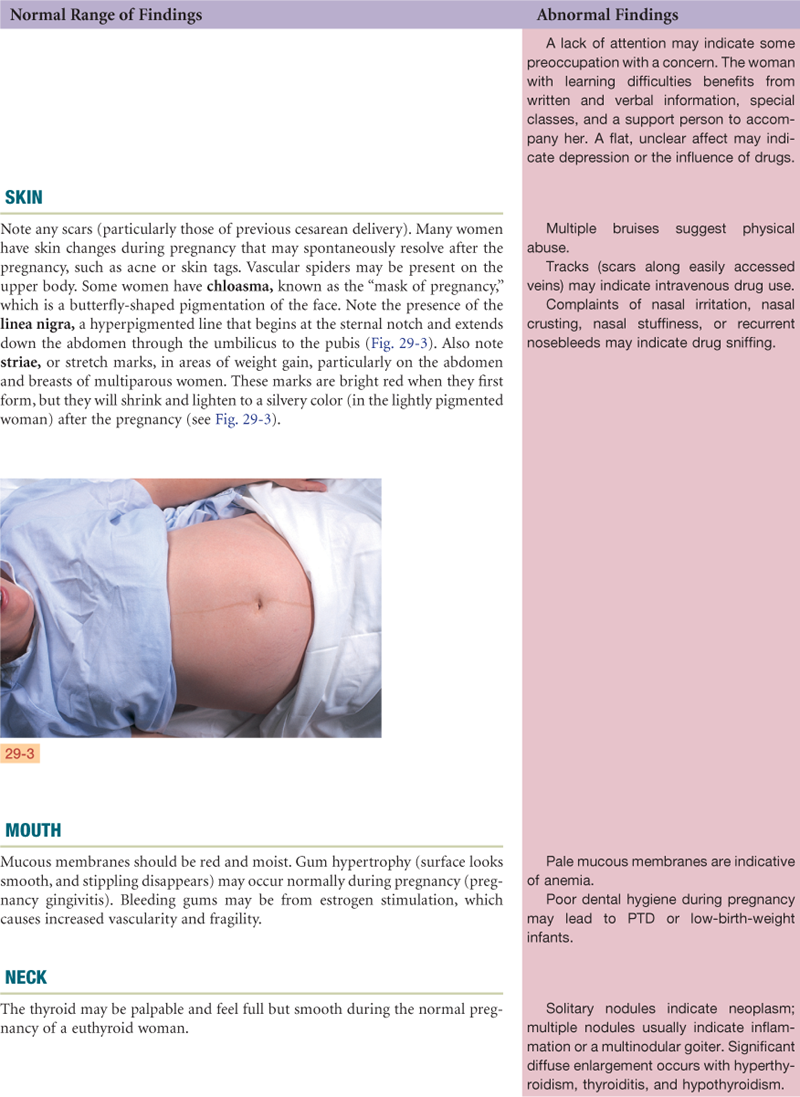
The areolae and nipples darken, it is thought, because estrogen and progesterone have a melanocyte-stimulating effect, and melanocyte-stimulating hormone levels escalate from the second month of pregnancy until delivery. For the same reason, the midline of the abdominal skin becomes pigmented and is called the linea nigra. You may note striae gravidarum (“stretch marks”) on the breast, abdomen, and areas of weight gain.
During the second trimester, systolic BP may be 2 to 8 mm Hg lower and diastolic BP 5 to 15 mm Hg lower than prepregnancy levels.14 This drop is most pronounced at 20 weeks and may cause symptoms of dizziness and faintness, particularly after rising quickly. Stomach displacement from the enlarging uterus and altered esophageal sphincter and gastric tone as a result of progesterone predispose the woman to heartburn. Intestines are also displaced by the growing uterus, and tone and motility are decreased because of the action of progesterone, often causing constipation. The gallbladder, possibly resulting from the action of progesterone on its smooth muscle, empties sluggishly and may become distended. The stasis of bile, together with the increased cholesterol saturation of pregnancy, predisposes some women to gallstone formation.
Progesterone and, to a lesser degree, estrogen cause increased respiratory effort during pregnancy by increasing tidal volume. Hemoglobin, and therefore oxygen-carrying capacity, also increases. Increased tidal volume causes a slight drop in partial pressure of arterial carbon dioxide (PaCO2), causing the woman to occasionally have dyspnea.14
With the rise of hCG in the first trimester, there is a transient decrease in thyroid-stimulating hormone (TSH) levels between 8 and 14 weeks’ gestation. Plasma iodine levels decrease, allowing a transient increase in thyroid gland size in approximately 15% of pregnant women.
Cutaneous blood flow is augmented during pregnancy, caused by decreased vascular resistance, presumably helping to dissipate heat generated by increased metabolism. Gums may hypertrophy and bleed easily. This condition is called gingivitis or epulis of pregnancy due to growth of the capillaries of the gums.14 For the same reason, nosebleeds may occur more frequently than usual. Pregnant women with periodontal disease, a chronic local oral infection, are at risk for preterm delivery.
FHTs are audible by fetoscope (as opposed to Doppler imaging) at approximately 17 to 19 weeks. The fetal outline is palpable through the abdominal wall at approximately 20 weeks. Fig. 29-1 illustrates the growth of the uterine fundus during the second trimester.
Third Trimester
Blood volume, which increased rapidly during the second trimester, peaks in the middle of the third trimester at approximately 45% greater than the prepregnancy level and plateaus thereafter. This volume is greater in multiple gestations.13 Erythrocyte mass increases by 20% to 30% (caused by an increase in erythropoiesis, mediated by progesterone, estrogen, and placental chorionic somatomammotropin). However, plasma volume increases slightly more, causing a slight hemodilution and a small drop in hematocrit. BP slowly rises again to approximately the prepregnancy level.14
Uterine enlargement causes the diaphragm to rise and the shape of the rib cage to widen at the base. Decreased space for lung expansion may cause a sense of shortness of breath. The rising diaphragm displaces the heart up and to the left. Cardiac output, stroke volume, and force of contraction are increased. The pulse rate rises 15 to 20 beats per minute.13 Because of the increase in blood volume, a functional systolic murmur, grade ii/iv or less, can be heard in more than 95% of pregnant women.13
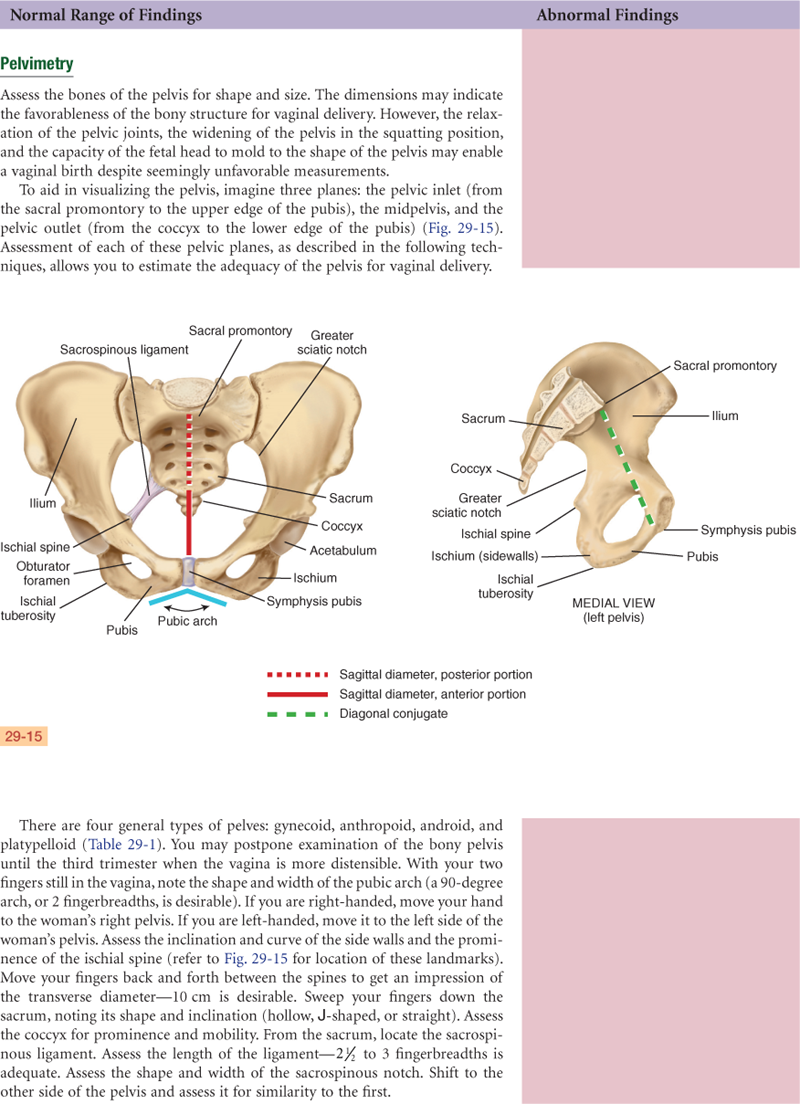
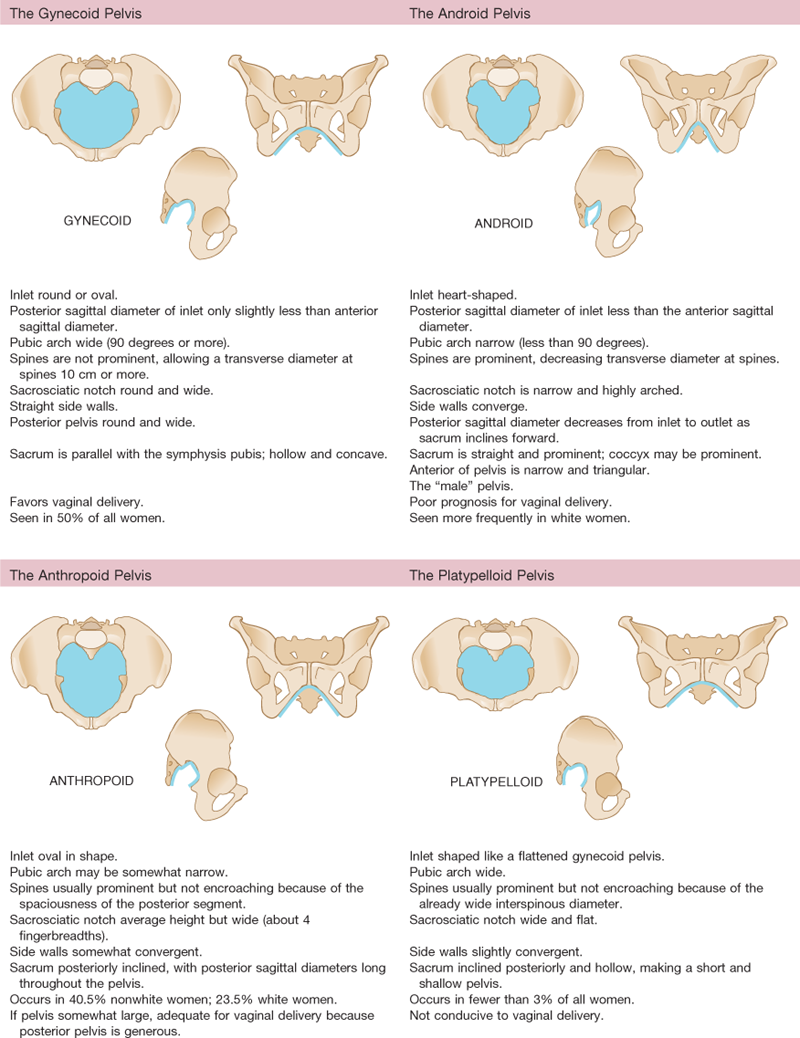
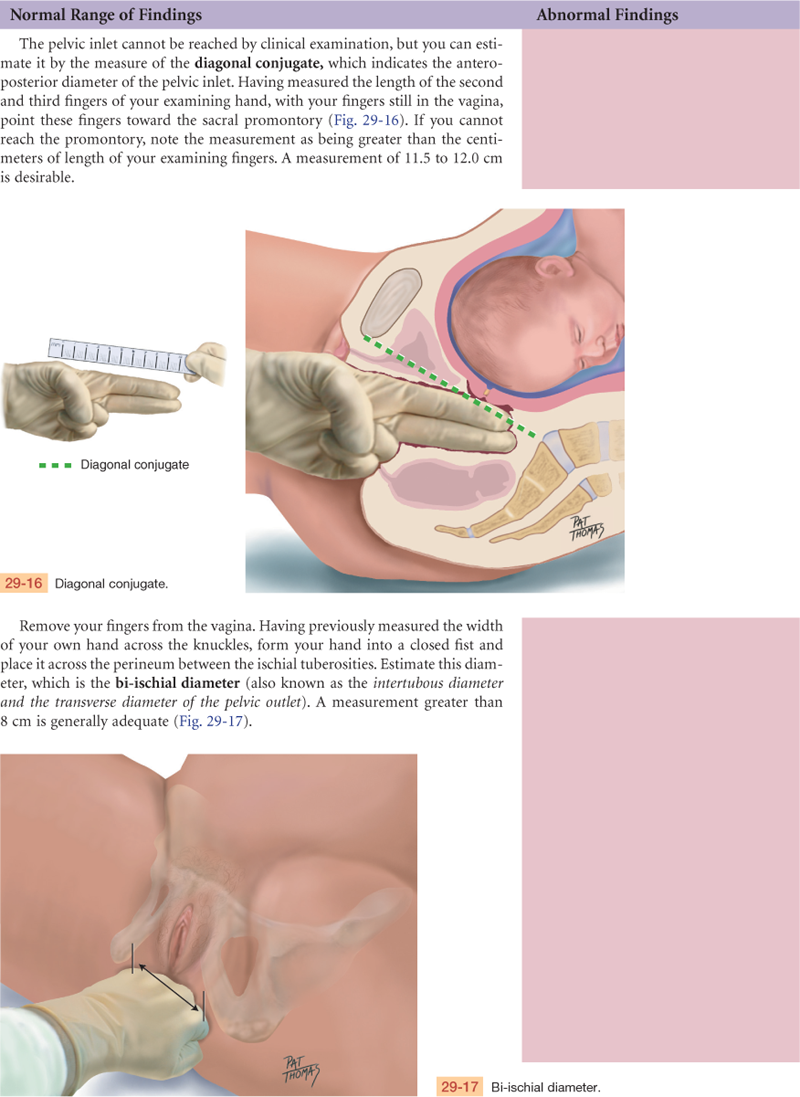
Edema of the lower extremities may occur as a result of the enlarging fetus impeding venous return and from lower colloid osmotic pressure. The edema worsens with dependency, such as prolonged standing. Varicosities, which have a familial tendency, may form or enlarge from progesterone-induced vascular relaxation. Also causing varicosities is the engorgement caused by the weight of the full uterus compressing the inferior vena cava and the vessels of the pelvic area, resulting in venous congestion in the legs, vulva, and rectum. Hemorrhoids are varicosities of the rectum that are worsened by constipation, which occurs from relaxation of the large bowel by progesterone.
Progressive lordosis (an inward curvature of the lumbar spine) occurs to compensate for the shifting center of balance caused by the anteriorly enlarging uterus, predisposing the woman to backaches. Slumping of the shoulders and anterior flexion of the neck from the increasing weight of the breasts may cause aching and numbness of the arms and hands as a result of compression of the median and ulnar nerves in the arm,40 commonly referred to as carpal tunnel syndrome.
Approximately 2 weeks before going into labor, the primigravida experiences engagement (also called “lightening” or “dropping”), when the fetal head moves down into the pelvis. Symptoms include a lower-appearing and smaller-measuring fundus, urinary frequency, increased vaginal secretions from increased pelvic congestion, and increased lung capacity. In the multigravida, the fetus may move down at any time in late pregnancy or often not until labor. The cervix, in preparation for labor, begins to thin (efface) and open (dilate). A thick mucous plug, formed in the cervix as a mechanical barrier during pregnancy, is expelled at variable times before or during labor. Between 37 and 42 weeks, the pregnancy is considered term. After 42 weeks, the pregnancy is considered postdates.
Determining Weeks of Gestation
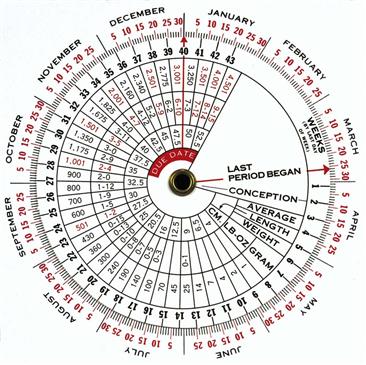
The expected date of delivery, or EDD, being 280 days from the first day of the LMP, may be calculated by using Nägele’s rule. That is, determine the first day of the last normal menstrual period (normal in timing, length, premenstrual symptoms, and amount of flow and cramping). Using the first day of the LMP, add 7 days and subtract 3 months. This date is the EDD. This date can then be used with a pregnancy wheel on which the EDD arrow is set, and then the present date will be pointing to the present week’s gestation (Fig. 29-2). The number of weeks of gestation also can be estimated by physical examination (bimanual and pelvic examination), by measurement of the maternal serum hCG, by US, and by signs such as the first perceived fetal movement.
Weight Gain in Pregnancy
The amount of weight gained by term represents a baby, amniotic fluid, placenta, increased uterine size, increased blood volume, increased extravascular fluid, maternal fat stores, and increased breast size. Weight gain during pregnancy reflects both the mother and fetus; approximately 25% of the total gain is attributed to the fetus, 11% to the placenta and amniotic fluid, and the remainder to the mother.11
The Institute of Medicine, based on the World Health Organization guidelines, recommends the following weight gain in pregnancy based on initial body mass index (BMI). Underweight (<18.5 kg/m2)—total weight gain range: 28-40 pounds; normal weight (18.5-24.9 kg/m2)—total weight gain range: 25-35 pounds; overweight (25.0-29.9 kg/m2)—total weight gain range: 15-25 pounds; obese (≥30.0 kg/m2)—total weight gain range: 11-20 pounds. For twin gestation and normal weight women—total weight gain range: 37-54 pounds; overweight—31-50 pounds; and obese—25-42 pounds.41
 Developmental Competence
Developmental Competence
Each year in the United States, almost one million teenage women, ages 15 to 19 years, become pregnant and 78% are unplanned. Many of these pregnancies pose serious medical risks for both mother and fetus, such as toxemia and low-birth-weight infants; it is unclear whether these risks are due to biologic or social factors, prolonged labor, or postpartum complications.18 Other risks for the pregnant adolescent are psychosocial. This young woman is at risk for the downward cycle of poverty beginning with an incomplete education, failure to limit family size, and continuing with failure to establish a vocation and become independent. She may be unprepared emotionally to be a mother. Her social situation may be stressful. She may not have the support of her family, her partner, or his family. Medical risks for the pregnant adolescent are generally related to poverty, inadequate nutrition, substance abuse, and sometimes sexually transmitted infections (STIs), poor health before pregnancy, and emotional and physical abuse from her partner, family, and peers.
The adolescent, for social reasons, often seeks health care later and is noncompliant with ongoing prenatal care, although early prenatal care has been shown to provide optimal management. In developing countries, maternal mortality for pregnant teenagers is a major concern because of hypertension, embolism, ectopic pregnancy, and complications from pregnancy termination where abortion is illegal.14
On the other hand, many Baby Boomers have delayed childbearing, and since the advent of assisted fertility, more women older than 35 years are now becoming pregnant. Women of “advanced maternal age” (after age 35 years) are often more prepared emotionally and financially to parent; however, they are more at risk for infertility and age-related anomalies. Fertility declines with advancing maternal age due to a decrease in the number and health of eggs to be ovulated, a decrease in ovulation, endometriosis, and early-onset menopause.
The risk for Down syndrome increases from about 1 in 1250 at age 25 to 1 in 1000 at age 30, 1 in 400 at age 35, 1 in 100 at age 40, and 1 in 30 at age 45.26a
Women ages 35 years and older or with a history of a genetic abnormality are offered genetic counseling and the options of both prenatal diagnostic screening tests. Two prenatal diagnostic options are chorionic villi sampling (CVS) performed between weeks 11 and 13 in which a small sample of chorionic villi is removed, and amniocentesis between weeks 15 and 20 in which a small amount of amniotic fluid is removed to analyze genetic makeup. Both are associated with a small risk for complications and miscarriage. Prenatal screening involves a fetal anatomy US scan and serum screening.
Carrier screening for cystic fibrosis (CF) is offered to check the inherited genetic disease affecting breathing and digestion. Both parents need to be carriers to pass the condition on to the fetus (a 25% chance [1 in 4] that the child will have CF).
Because the incidence of chronic diseases increases with age, women older than 35 years who are pregnant more often have medical complications such as diabetes, obesity, and hypertension.14 The increased incidence of hypertension causes an increase in placental abruption and preeclampsia. Hypertension, in turn, increases intrauterine growth restriction (IUGR). More women of advanced maternal age have placenta previa, placental abruption, uterine rupture, and cesarean deliveries. They have more spontaneous abortions, in part because of the increase in genetically abnormal embryos.
 Culture and genetics
Culture and genetics
Some complications of pregnancy occur more frequently in certain racial groups. Women who live in underdeveloped nations do not have the advantages of advanced technology. More than 500,000 women die in childbirth each year. According to the United Nations Populations Fund, this number remains globally high in an age in which these deaths are preventable. Of these maternal deaths, 90% occur in Africa and Asia and occur from severe bleeding, sepsis, eclampsia, obstructed labor, and unsafe abortions. Many women who survive pregnancy and childbirth may suffer a lifetime of physical and emotional complications such as vaginal/rectal fistula.39a
The Hispanic population within the United States between 1990 and 2000 grew by more than 40%. It is projected that between 2000 and 2010 that will increase by another 34%. Hispanics had the highest birth rate in 2003, with 82.2 births per 1000 teen females ages 15 to 19.32 Still there are disparities in adequate access to preventive, prenatal, and dental care with these cultural groups along with Asian/Pacific Islander and American Indian/Alaska Native population.32 Nonwhite pregnant women have an increased risk for gestational diabetes mellitus (GDM), pregnancy-induced hypertension (PIH), and preterm labor and delivery (PTL/PTD).
Pregnancy is not only a medical event but also one with profound psychological and social meaning for the woman and for her family and community. All cultures recognize pregnancy as a unique period in a woman’s life that surrounds special customs and beliefs that have been developed throughout the ages. The spiritual practices and beliefs provide her either with or without support. Understanding what role these beliefs and practices play in the woman’s pregnancy helps you acknowledge the cultural differences. Pregnancy is intensely personal and involves such charged issues as sexuality, relationships, contraception, nutritional practices, maternal weight gain, gender of the fetus, and abortion. You may begin by inquiring whether the woman or her significant others have any special requests. This communicates your intention to respect cultural differences and preferences. A continuing rapport will help enable the woman to bring up issues as they develop.
A woman’s resistance to an action or a suggestion by the clinician may represent a cultural, social, or financial issue. Such issues may also be held differently by the woman and her significant others. Examples of culturally charged issues are dietary practices, sexuality during and after pregnancy, preference for gender of care provider, preference for gender of infant, and contraceptive usage. Use your skill to understand such preferences within a cultural context and accept rather than judge the person. Whenever safe and possible, respect such wishes. This enhances the success of the birth in its psychological and social dimensions.
Subjective Data
| Examiner Asks | Rationale |
| 1. Menstrual history • When was the first day of your last menstrual period that was normal in timing, premenstrual symptoms, length, amount of flow, cramping? • Number of days in cycle? • Age at menarche? | Using Nägele’s rule, calculate the EDD with this date. With a pregnancy wheel, determine the current number of weeks of gestation. |
| 2. Gynecologic history | |
| • Ever had surgery of the cervix? Uterus? Fallopian tubes? | Cervical surgery may affect the integrity of the cervix during pregnancy and increases the risk for cervical insufficiency, preterm cervical dilation, and preterm delivery. Uterine surgery increases the risk for uterine rupture during pregnancy and labor. |
| • Any known history of or exposure to genital herpes? | Onset during pregnancy is potentially teratogenic (i.e., causing physical defects in the developing fetus), and a lesion at delivery precludes vaginal birth. |
| • Papanicolaou (Pap) tests: When was your last one? Any history of abnormal? If so, when? Have you ever had a colposcopy? Cervical biopsy? | Because more women delay childbearing, there may be an increase in diagnosing gynecologic cancers during pregnancy. Cancer is the second most common cause of maternal death in the reproductive years.19 |
| • Any history of infertility, fibroids, or uterine abnormalities? | May increase risk for ectopic pregnancy, miscarriage, PTL/PTD. |
| • Any history of gonorrhea, chlamydia, syphilis, trichomoniasis, pelvic inflammatory disease (PID)? | STIs increase the risk for premature rupture of membranes, PTL/PTD, postpartum maternal and fetal infections. |
| • Do you or does your partner have more than one sexual partner? | Increases the risk for STIs and human immunodeficiency virus (HIV) infection. |
| • Were you a preterm infant? | Patients who themselves were preterm infants are at increased risk for PTD. |
| • Have you had a mammogram, breast biopsy, breast implants, lumpectomy, or mastectomy? | Breast cancer is the most common cancer in pregnancy, affecting approximately 1 in 3000 pregnancies, occurring between the ages of 32 and 38 years.28 |
| 3. Obstetric history | |
| • Number of times pregnant? Number of term or preterm deliveries? Number of spontaneous miscarriages, elective abortions, or ectopic pregnancies? Any fetal or neonatal deaths? | An obstetric history helps provide care during the current pregnancy. |
| • In earlier pregnancies, any history of gestational hypertension, preeclampsia, eclampsia, HELLP (Hemolysis, Elevated Liver enzymes, Low Platelets) syndrome, diabetes, β-hemolytic Streptococcus infection, IUGR, congenital anomalies, premature labor, postpartum hemorrhage, or postpartum depression? | The woman who has experienced these complications in the past is at increased risk for them in subsequent pregnancies. |
| • How did you experience previous pregnancies and deliveries? | The subjective quality of previous experiences affects current pregnancy. |
| • Ever had a cesarean section? If so, what was the indication? At how many centimeters of dilation, if any, was the surgery performed? What type of uterine incision was made? (Confirming records of this surgery must be obtained.) Have you ever had a vaginal birth after a cesarean section (VBAC)? | The vertical, or “classical,” incision carries a higher risk for rupture and mandates that all subsequent deliveries be by cesarean section. The “low transverse” or horizontal incision carries a low risk, and subsequent deliveries may be vaginal. Note that the direction of the skin scar does not necessarily tell how the uterus was incised. |
| • Any history of infertility? Have you used assisted reproductive technology? | With donor eggs, the age of the egg donor is used in calculating genetic testing. |
| • Any history of preterm labor or preterm rupture of membranes? | Requires close observation during the current pregnancy. Previous PTD is associated with recurrence. |
| • Have you been told you have cervical insufficiency? Incompetency? Have you had a cervical cerclage placed in previous pregnancies? | A cervical cerclage is a stitch placed surgically to hold the cervix closed during the pregnancy and normally placed between weeks 12 and 15. |
| • Tell me the gestational ages and weights of your babies at birth. | A small infant may indicate prematurity or IUGR—complications that are repeatable. A large infant may indicate GDM (also repeatable). Conversely, birth weights of other children may indicate a “constitutional size” (e.g., the tendency of a couple to conceive smaller but normal children). Also, the woman’s pelvis has been “proven” to the weight of the largest baby born vaginally; bear this number in mind as labor begins, estimating and comparing the weight of the baby about to be born. |
| • Did you breastfeed the previously born infants? How was that experience for you? | Her experience and knowledge base will shape your teaching and support. |
| • Any history of mastitis? | A poor or painful previous experience increases breastfeeding support after this pregnancy. |
| 4. Current pregnancy. (Having calculated the current number of weeks of gestation, you can reassess the probable accuracy of that date when eliciting the following history.) | |
| • What method of contraceptive did you use most recently, and when did you discontinue it? | Recent use of birth control pills or other hormonal contraceptives causes delayed ovulation and irregular menses—consider when establishing the EDD. An intrauterine device (IUD) that is still in place requires removal; it threatens the pregnancy. Also, this opens topic of whether pregnancy was planned. |
| • Was the pregnancy planned? How do you feel about it? | Even a planned pregnancy represents loss—perhaps a loss of freedom, compromise of goals, loss of time with other children or partner. The first trimester is known as the “trimester of ambivalence,” and encouraging acceptance and expression of these feelings helps resolution. |
| • How does the baby’s father feel about the pregnancy? Other family members? | The woman may need assistance in gathering her support group. Inviting significant others to future visits affirms their importance and supports involvement. |
| • Experienced any vaginal bleeding? When? How much? What color? Accompanied by any pain? | Vaginal bleeding may indicate threatened abortion, cervicitis, or ectopic pregnancy in 1st trimester and must be investigated. |
| • Are you experiencing any nausea and/or vomiting? | Nausea and vomiting usually begin between weeks 4 and 5, peak between weeks 8 and 12, and resolve between weeks 14 and 16. Persistent and severe nausea and vomiting lead to hyperemesis. |
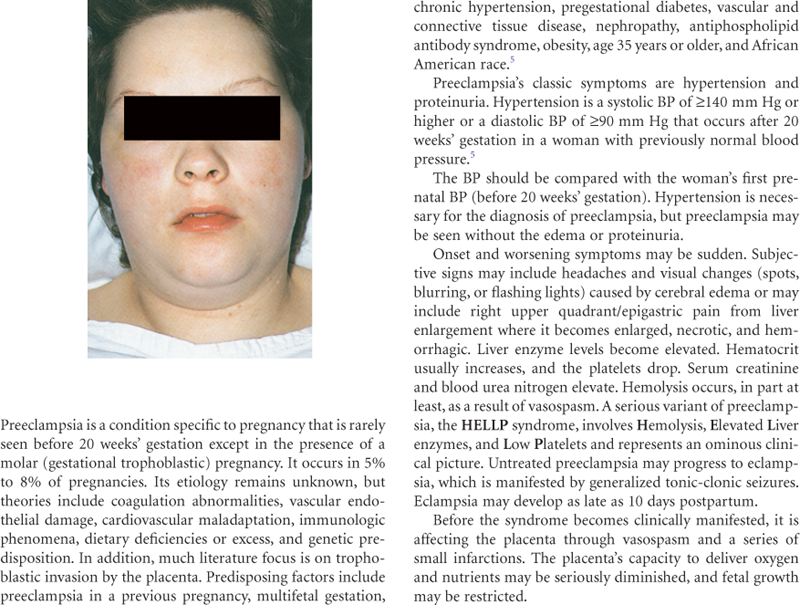
| • Experienced abdominal pain? When? Where in your abdomen? Accompanied by vaginal bleeding? | Common causes of abdominal pain in early pregnancy are spontaneous abortion, ectopic pregnancy, urinary tract infection (UTI), and round ligament discomfort. Late pregnancy causes are premature labor, placental abruption, and HELLP syndrome (see Table 29-2, Preeclampsia, p. 822). Also consider other medical and surgical causes for abdominal pain. |
| • Experienced any illnesses since being pregnant? Any recent fever(s), unexplained rash, or infections? | Helps establish any possible exposures to infectious agents. |
| • Had any x-rays? Taken any medications? | Discuss the potential effect of any teratogenic exposure. Refer for expert counseling if necessary. |
| • Experiencing any visual changes such as the new onset of blurred vision or spots before your eyes? | In the third trimester, may be a sign of preeclampsia. Evaluate for other signs and symptoms of preeclampsia (see Table 29-2). |
| • Experiencing any edema? Where and under what circumstances? | In the third trimester, differentiate the normal weight-dependent edema of pregnancy from the edema of preeclampsia. |
| • Any frequency or burning with urination? Any blood in your urine? Do you void in small amounts? Any history of UTIs, pyelonephritis, or kidney stones? | Differentiate the normal urinary frequency of the first and third trimesters from UTI, for which pregnant women are at increased risk. Confirm by urinalysis. UTIs increase the rate of PTD. |
| • Any vaginal burning or itching? Any foul-smelling or colored discharge? | To rule out vaginal infection, add cultures or a wet mount to the pelvic examination. Explain the normal increase in vaginal secretions during pregnancy. |
| • What date did you first feel the baby move? | This sign is compared with the EDD to evaluate the accuracy of that date. |
| • How does the baby move on a daily basis? | Fetal movement is an excellent indicator of fetal health. Clinicians assign women to count fetal movements starting at 28 weeks of pregnancy. |
| • Do you have cats in the home? | Explain toxoplasmosis, a teratogenic disease transmitted through cat feces. To avoid exposure, another person should empty cat litter at frequent intervals. |
| • What are your plans for breastfeeding this baby? | Arrange reading, classes, and other support for the woman who is breastfeeding for the first time or for the woman with an unsuccessful earlier experience. |
| 5. Medical history | |
| • Do you have allergies to medications or foods? If so, what type of reaction? | Prevents prescribing error. |
| • Any personal or family history of cancer? | Advanced maternal age during pregnancy increases risk for breast, ovarian, uterine, and colon cancers. |
| • Do you have a history of asthma? If yes, have you ever had an attack in which you needed a breathing tube placed? | Poor control and frequent exacerbations of asthma during pregnancy may result in maternal hypoxia and decrease in fetal oxygenation. |
| • Ever had German measles (rubella)? | This mild childhood disease is highly teratogenic, especially during the first trimester. Instruct the woman who has not had rubella to avoid small children who are ill. Check immunity status in the serum prenatal panel. The nonimmune woman will be offered immunization after delivery. |
| • Ever had chickenpox? | Rarely, varicella causes congenital anomalies. The nonimmune woman should avoid exposure. |
| • Any history of injury to the back or another weight-bearing part? | The localized and overall weight gain of pregnancy and the joint-softening property of progesterone cause lordosis and will aggravate such injuries with increasing gestational age. |
| • Have you been tested for HIV? When? What was the result? Ever had a blood transfusion? Used a needle to take street drugs? Had a sexual partner who had any HIV risk factors? | HIV screening must be offered to all pregnant women to decrease the risk for transmission of the virus across the placenta to the fetus. Breastfeeding is contraindicated for the HIV-positive mother because the virus is present in the breast milk. |
| • Do you smoke cigarettes? How many? For how many years? Ever tried to quit? Drink any alcohol? How many times per week? Use any street drugs? | Explain the danger of these substances in pregnancy. Smoking increases the risk for ectopic pregnancy, spontaneous abortion, low birth weight, prematurity, preterm premature rupture of membranes, pregnancy-induced hypertension, placental abruption, and sudden infant death syndrome. Alcohol increases the risk to the fetus for fetal alcohol syndrome (see Table 13-4). Cocaine use during pregnancy is associated with congenital anomalies, a fourfold increased risk for abruptio placentae, and the risk for fetal addiction. Narcotic-addicted infants may have developmental delays or behavioral disturbances.14 Refer to a counseling/support program and periodic toxicology screening. Refer to a smoking cessation program. |
| • Do you take any prescribed, over-the-counter, or herbal medications? | Screen all medications to establish safety during pregnancy. |
| • Do you have a regular exercise program? What type? | Regular exercise in pregnancy may reduce risk for pregnancy-induced hypertension. |
| • Has your vitamin D level been checked? | Vitamin D is essential for maternal response to the calcium demands of the fetus for growth and bone development. Maternal anorexia and malaise often are associated with vitamin D deficiency22 and should be evaluated when these symptoms occur. |
| 6. Family history | |
| • Anyone in your family have hypertension? | Increases the risk for chronic hypertension and for preeclampsia. |
| • Diabetes? If so, of juvenile or adult onset? Insulin dependent? | Increases risk for GDM. A heavy family history might prompt early screening and dietary interventions. |
| • Mental illness, including depressive, anxiety, eating, personality, and psychotic disorders? | Maternal depression is associated with low birth weight, preterm delivery, and stillbirth20 and postpartum depression. |
| • Kidney disease? | Increases risk for renal disease, hypertension, and preeclampsia. |
| • Fraternal twins? | The tendency to ovulate twice in one month is familial, increasing the incidence of twinning. |
| • Anyone in your family or in the family of the baby’s father had congenital anomalies? | Some anomalies, such as heart conditions, are familial. Offer genetic counseling if needed. |
| • Is your racial or ethnic descent Mediterranean? | Increased risk for β-thalassemia. |
| African American? | Increased risk for sickle-cell disease. |
| Ashkenazi Jewish? | Increased risk for Tay-Sachs disease. |
| Irish? | Increased risk for spinal malformations. |
| 7. Review of systems | |
| • Your weight before pregnancy? | Baseline needed to evaluate changes. |
| • Wear glasses? | A transient change in visual correction may occur during pregnancy. |
| • When did you last see the dentist? Need any dental work? | Gums may be puffy and bleed easily during pregnancy, predisposing caries. Poor dental hygiene can lead to PTD, low-birth-weight babies, and neonatal death. Dental care is an important part of prenatal care; notify the dentist that she is pregnant. |
| • Been exposed to tuberculosis (TB) or had a positive PPD skin test or chest x-ray examination? | Consider TB screening; positive result requires chest x-ray examination even in pregnancy. |
| • Any cardiovascular disease, heart disease, or disease of a heart valve? | The woman with cardiac disease is monitored carefully for signs of cardiac compromise. Blood volume increases by 40%, and the demand on the heart is significantly increased. |
| • Any anemia? What kind? When? Was it treated? How? Did it improve? | Pregnancy worsens any preexisting anemia because iron is used extensively by the fetus. Identify the need for early supplementation. Sickle-cell anemia may worsen during pregnancy, whereas sickle-cell carriers have more UTIs. Screen the latter periodically for bacteriuria. |
| • Had thrombophlebitis, pulmonary embolus (PE), or deep venous thrombosis (DVT)? Or known clotting disorder? | Pregnancy itself is a hypercoagulable state because of increases in coagulation factors. This increases the risk for phlebitis, DVTs, or PEs.14 |
| • Have you had hypertension or kidney disease? | Renal disease or chronic hypertension increases risk for preeclampsia. Know the baseline BP and renal function to evaluate any changes. |
| • Any history of hepatitis B or C? | Confirm with serum testing. Perinatal transmission occurs by exposure to infected blood and genital secretions during delivery and by cracked and bleeding nipples during feeding. |
| • Any history of thyroid disease? | Uncontrolled hyperthyroidism is associated with increased neonatal morbidity resulting from preterm birth and low birth weight. Uncontrolled hypothyroidism is related to delayed mental development in children. |
| • Any history of seizures? On any medications? | Women with epilepsy taking medications have increased incidence of stillbirths and IUGR and a 4% to 8% risk for birth defects, such as cleft lip or palate, heart abnormalities, and spina bifida.17 |
| • Have you had urinary tract infections? | The hormonal milieu of pregnancy predisposes the woman to UTIs, indicating periodic screening. Pregnancy may also mask the symptoms of UTIs. Further, a serious UTI may cause irritability of the uterus, threatening preterm labor. Educate the woman in measures to prevent UTIs. |
| • Have you had depression or any other mental illness? | This woman will be at risk for postpartum depression. Assist her to prepare a support network. Counseling may help her navigate the developmental challenges of becoming a mother. |
| • Do you feel safe in your relationship or home environment? | Violence during pregnancy is common. Questioning the safety of the woman is part of prenatal care. |
| • Are you in a relationship with someone who physically or emotionally abuses or threatens you? | Most women will not freely offer this information. You must ask these questions at the appropriate time and in a nonthreatening manner. |
| • Has anyone forced you to have sexual activities against your will? | Incest or other abuse increases risk for dysfunctional labor and cesarean delivery. |
| • Do you have diabetes? On oral hypoglycemics, insulin injection, or insulin pump? Did you have diabetes during a previous pregnancy? | Diabetes is carefully managed during pregnancy to avoid serious complications, such as a macrosomic infant and operative delivery. Consider early screening and nutritional interventions. |
| 8. Nutritional history | |
| • Do you follow a special diet? Are you vegetarian? | A special diet may have nutritional risk. Help achieve adequate nutrition within the confines of her diet. Refer for dietary counseling. |
| • Any food intolerance? | A food intolerance might affect the woman’s and fetus’s nutrition, such as lactose intolerance limiting calcium intake. |
| 9. Environment/hazards | |
| • What is your occupation? What are the physical demands of the work? Are you exposed to any strong odors, chemicals, radiation, or other harmful substances? Or potentially harmful physical contact? | Hazards? Possible teratogenic exposures? The woman who is rubella nonimmune may be advised not to continue working in a daycare center. Suitability for pregnancy? The woman whose job requires long hours of standing may be disabled early if signs of PTL occur. |
| • Do you consider your food and housing adequate? | Refer for state and federal programs to assist with food, housing, or other needs. |
| • How do you wear your seatbelt when driving? | For maternal and fetal safety, instruct the woman to place the lap belt below the uterus and to use the shoulder strap. |
| • Other questions or concerns? | Encourage the woman to write down questions between visits. |
Objective Data
| PREPARATION | EQUIPMENT NEEDED |
| The initial examination for pregnancy is often a woman’s first pelvic examination, and many women are extremely anxious. Alternatively, the woman may not know for certain whether she is pregnant, and she may be anxious about the findings. Verbally prepare the woman for what will happen during the examination before touching her. Save the pelvic examination for last—by that time, the woman will be more comfortable with your gentle, informing manner. Communicate all findings as you go along to demonstrate your respectful affirmation of her control and responsibility in her own health and health care and that of her child. Ask the woman to empty her bladder before the examination, reserving a clean-catch specimen for dipping for protein and glucose, and for urinalysis, if required. Before the examination, ask her to weigh herself on the office scale. Provide the woman with an escort or chaperone during examinations. Give the woman a gown and drape. Begin the examination with the woman sitting on the examination table, wearing the gown, her lap covered by a drape. During the breast examination, help her lie down. She remains recumbent for the abdominal and extremity examination. Use the lithotomy position for the pelvic examination (see Chapter 26). Help her to a seated position to check her BP. Recheck after the examination if BP is elevated. |
Stethoscope, BP cuff Centimeter measuring tape Fetoscope and Doppler sonometer Reflex hammer Urine collection containers Dipstix for checking urine for glucose and protein Equipment needed for pelvic examination as noted in Chapter 26. |

 Documentation and Critical Thinking
Documentation and Critical Thinking
Focused Assessment: Clinical Case Study 1
Rosa is a 27-year-old Latina woman, gravida 2 para 1, who presents with her husband and daughter for her first prenatal visit.
Subjective
Rosa is a full-time homemaker who completed 2 years of college. Last normal menstrual period (LNMP) was April 4 of this year (certain of date), with an expected date of delivery (EDD) of January 11 of next year, making her 10 weeks’ gestation today. Her obstetric history includes a normal spontaneous vaginal delivery (NSVD) 3 years ago of a viable 7 lb, 12 oz female infant after an 8-hour labor without anesthesia, with a midline episiotomy. No complications of pregnancy, delivery, or the postpartum. She breastfed her daughter, Ana, for 1 year. Present pregnancy was planned, and Rosa and her husband are pleased. Rosa is having breast tenderness and nausea on occasion, which resolves with crackers. No past medical or surgical conditions are present. She denies allergies. Family history is significant only for diet-controlled adult-onset diabetes in two maternal aunts.
Objective
General: Appears well nourished and is carefully groomed. English is second language, and Rosa is fluent.
Skin: Light tan in color, surface smooth with no lesions, small tattoo noted on left forearm.
Mouth: Good dentition and oral hygiene. Oral mucosa pink, no gum hypertrophy. Thyroid gland small and smooth.
Chest: Expansion equal, respirations effortless. Lung sounds clear bilaterally with no adventitious sounds. No CVA tenderness.
Heart: Rate 76 bpm, regular rhythm, S1 and S2 are normal, not accentuated or diminished, with soft, blowing systolic murmur Gr ii/vi at 2nd left interspace.
Breasts: Tender, without masses; with supple, everted nipples. Breast self-exam reviewed.
Abdomen: No masses, bowel sounds present. No hepatosplenomegaly. Uterus nonpalpable. No inguinal lymphadenopathy noted.
Extremities: No varicosities, redness, or edema. Homan sign negative. DTRs 2+ and equal bilaterally.
BP 110/68 mm Hg, sitting.
Pelvic: Bartholin’s, urethra, and Skene’s glands (BUS) negative for discharge. Vagina: pink, with white, creamy, non-odorous discharge. Cervix: pink, closed, multiparous, 2 cm long, firm.
Uterus: 10-week size, consistent with dates, nontender, dextrorotated. FHTs heard with Doppler, rate 140s.
Pelvis: Pubic arch wide; side walls straight, spines blunt, interspinous diameter >10 cm.
Sacrum hollow; coccyx mobile. Sacrospinous ligament 3 fingerbreadths (FBs) wide. Diagonal conjugate >12 cm, bituberous diameter >8 cm. Spacious gynecoid pelvis proven to 7 lb, 12 oz.
Assessment
Intrauterine pregnancy 10 weeks by good dates, size = dates.
Rosa and husband happy with pregnancy; she feels well.
Plan
Begin prenatal vitamins.
Prenatal blood screen and urinalysis.
HIV screening offered and accepted.
Reviewed comfort measures for nausea.
Reviewed warning signs—vaginal bleeding and abdominal pain.
Return visit in 4 weeks.
Focused Assessment: Clinical Case Study 2
Kadija is a 30-year-old Ethiopian woman, gravida 9 para 7, who presents with an interpreter and her eldest daughter for her first prenatal visit.
Subjective
Kadija is a full-time homemaker and runs a daycare facility within her home. She immigrated to the United States 5 years ago with her husband and children. Her husband is employed. She lives in a one-bedroom apartment with her family. Her last menstrual period was May 28th of this year, with an EDD of March 5th of next year, making her 11 weeks’ gestation today. She is a poor historian for her deliveries in Ethiopia other than one child “died in childbirth.” She delivered her last child vaginally, here in the United States without complications after 5 hours of labor. She is unsure of the baby’s weight. She had a female circumcision as a child. She is having nausea with occasional vomiting, has breast tenderness, and 1 week ago experienced “pink” vaginal spotting. She is unsure of her family history. Both parents are deceased as well as all but one of her seven siblings. This pregnancy is unexpected, but okay. She is concerned about transportation to her appointments since her husband works days and she does not drive.
Objective
General: Appears well nourished and is carefully groomed. English is second language, but she understands some. Daughter who is present with her mom is well groomed and speaks English.
Skin: Dark tan in color, surface smooth, Small scarring on left arm and both legs. No lesions or tattoos.
Mouth; Poor dentition. Oral mucosa pink, some gum hypertrophy. Thyroid gland small and smooth.
Chest: Expansion equal, respiration effortless. Lung sounds clear bilaterally with no adventitious sounds. No CVA tenderness.
Heart: Rate 84 bpm, regular rhythm, S1 and S2 are normal, not accentuated or diminished, with soft, blowing systolic murmur Gr ii/vi at 2nd left interspace.
Breasts: Tender, no masses, large everted nipples. No drainage present. Breast self-exam reviewed.
Abdomen: No masses, bowel sounds present in four quadrants. No hepatomegaly or splenomegaly. Uterus non-palpable. No inguinal lymphadenopathy noted. No healed incision(s) noted.
Extremities: No lower extremity varicosities, edema, or redness noted. Negative Homan sign. 1+ DTRs. BP 124/76 mm Hg.
Pelvic: Female circumcision present without infibulated scarring. Bartholin’s, urethra, and Skene’s glands (BUS) negative for discharge. Vagina pink, with white, creamy, non-odorous discharge. Cervix pink, non-friable, closed, and approximately 3 cm long and soft. Vaginal wall muscles lax. No evidence of a cystocele or rectocele.
Uterus: Approximately 11-week size and nontender. Dextrorotated. FHTs not heard with Doppler. Confirmed on ultrasound along with dating.
Pelvis: Pubic arch wide; side walls straight, spines blunt, interspinous diameter >12 cm, bituberous diameter >8 cm. Spacious, proven, gynecoid pelvis to ≈8 pounds.
Assessment
Intrauterine pregnancy at 11 weeks’ gestation by ultrasound today with positive fetal cardiac activity. Size = dates. Aware of potential language and cultural issues. Via interpreter, understands advised prenatal testing, clinic routine, and warning signs and symptoms in pregnancy. Physical examination within normal limits (WNL)
Plan
Begin prenatal vitamins.
Routine prenatal blood screening, plus check thyroid function tests, vitamin D level, Sickle cell, and thalassemia screen.
HIV and CF screening discussed, offered, and accepted.
Reviewed prenatal screening (Seq 1 and 2, US for NT). Will discuss with her husband and let us know.
Reviewed clinic routing and how to contact clinic personal after hours.
Reviewed comfort measures for nausea and vomiting. Offered medication; declined at this time.
Reviewed warning signs: vaginal bleeding, abdominal pain, pain with urination.
Return to clinic in 2 weeks if desires prenatal screening, or 4 weeks if does not.
Refer to social worker and transportation services.
Obtain records from previous pregnancy and delivery in United States.
 For a PDA-downloadable version, go to
For a PDA-downloadable version, go to