Functional Assessment of the Older Adult

http://evolve.elsevier.com/Jarvis/
• Head-to-Toe Examination of the Older Adult
The United States has a large and expanding population of older adults. The implications of the graying of America are staggering for all health care systems (Fig. 30-1). In 2006, persons 65 years of age and older represented 12.6% (over one in every eight) of the U.S. population.3 They also accounted for 38% of non-federal short-stay hospitalizations, with those ages 75 years and older totaling 24% of all inpatients.26 In 2005, older adults averaged more office visits than younger adults (7.7 visits for those ages 75 years and older vs. 3.9 visits for those 45 to 65 years of age). Older Americans also had higher out-of-pocket health care expenditures than younger Americans (12.7% of total expenditures on health care for older Americans vs. 5.7% for all other consumers).3
30-1
Older adults also make up 80% of home care visits and 90% of those in nursing homes.34 Many older Americans live with disabilities or have activity limitations, often a result of having multiple chronic conditions that may include sensory, physical, or mental impairments. Approximately 37% of older adults reported a severe disability in 2005 requiring some type of assistance.3
In 2007, 1.57 million older Americans lived in nursing homes, with 15% of these residents being ages 85 years and older. In addition, between 2% and 5% of older adults lived in senior housing and had access to at least one assistive service.
Personal caregiving can be formal (hired, paid caregivers) or informal (family, friends). In 1999, 3.7 million older Medicare enrollees received either formal or informal care and two thirds of these persons were receiving informal care only.27a In addition, aging or older adult cannot be defined only by the chronologic age of an individual as it is for Social Security (ages 65 years and older). Older adults are truly heterogeneous, and differences exist among biological, social, physical, and emotional rates of aging.69 Older age-groups are often categorized as young-old (65-74 years), middle-old (75-84 years), and old-old (85 years and older). Although the number of chronic diseases does increase with aging, it is important to remember that a substantial number of older adults both enjoy aging and report good to excellent health.60
The comprehensive assessment of an older adult requires knowledge of not only normal aging changes but also the consequences of chronic diseases, genetic makeup, and lifestyle. A comprehensive geriatric assessment is multidimensional and incorporates the physical examination as well as assessments of mental status, functional status, social and economic status, pain, and examination of the physical environment for safety concerns. Multiple disciplines may participate in this assessment, including physicians; nurses; physical, occupational, and speech therapists; social workers; case managers; nutritionists; and pharmacists. Early recognition of disabilities and treatable conditions is instrumental in preserving function and quality of life for older adults.
The normal changes of aging presented in previous chapters do not necessarily represent pathology, but with the imposition of acute and chronic illnesses, including hospitalization, an older adult may be predisposed to disability. Older adults may arrive in clinics or hospitals not only with an acute illness such as pneumonia but also with ongoing chronic “geriatric syndromes,” such as urinary incontinence, fragile skin, confusion, problems with eating or feeding, falls, and sleep disorders.46 If these syndromes are not identified early, an older adult may develop functional decline.
Normal aging changes and the development of disease may precipitate transitions from home to a variety of settings, where nursing-focused assessments are performed. Care may be provided in hospitals; in skilled nursing, long-term care, assisted living, and acute rehabilitation facilities; and in hospice, senior centers, homes, and clinics. The setting where care is provided usually determines the types of assessment and instruments used. However, the goal of the functional assessment remains the same (i.e., to identify an older adult’s strengths and any limitations) so that appropriate interventions will promote independence and prevent functional decline.
Functional Ability
Functional ability refers to one’s ability to perform activities necessary to live in modern society and can include driving, using the telephone, or performing personal tasks such as bathing and toileting. Functional ability also incorporates an older adult’s physiologic and psychological status and the physical and social environment.86 Functional status, as defined by Richmond et al.,91 is “the individuals’ actual performance of activities and tasks associated with their current life roles” and depends on motivation, sensory capacity such as vision and hearing, degree of assistance needed to accomplish the tasks, and cognition.54 For example, the effect that arthritis might have on a person’s ability to exercise may affect physical function. A condition such as Alzheimer disease may affect problem solving, safety concerns, and motivation, which in turn affect function. Lack of social support or a safe physical setting is an environmental issue that affects functional status and possibly the ability to live independently. The interaction of these components provides a snapshot of an older adult’s functional status at a given point in time.86 Functional status is not static; older adults may move continuously through varying stages of independence and disability.
The assessment of function is an important geriatric tenet to provide a baseline for continuing comparison, to predict prognosis, and to assist the practitioner with objective measures to determine efficacy of treatments. Just knowing the person’s medical diagnosis is not sufficient to predict functional abilities. Older adults may not experience the usual symptoms of an acute illness. Often a decline in functional status may herald the presence of another process such as an infection.
A functional assessment of an older adult is the basis for care planning, goal setting, and discharge planning. A functional assessment also is needed for eligibility to obtain many services such as durable medical equipment, home modifications, and inpatient or outpatient rehabilitation services. For the older adult and family, a functional assessment can identify areas for current and future planning, such as the most appropriate living situation.
A functional assessment includes three overarching domains: activities of daily living (ADLs), instrumental activities of daily living (IADLs), and mobility.86 A functional evaluation should be systematic, with attention paid to the particular needs of the person, such as the presence of pain, fatigue, shortness of breath, or memory problems. There are two approaches to use for performing a functional assessment: (1) asking individuals about their abilities to perform the tasks (using self-reports) or (2) actually observing their ability to perform the tasks. For persons with memory problems, the use of surrogate reporters (proxy reports) such as family members or caregivers may be necessary, keeping in mind that they may either overestimate or underestimate the actual abilities.
Activities of Daily Living
ADLs are those tasks necessary for self-care. Typically, ADLs measure domains of eating/feeding, bathing, grooming (the individual tasks of washing face, combing hair, shaving, cleaning teeth), dressing (lower body and upper body), toileting (bowel and bladder), walking (including propelling a wheelchair), using stairs (ascending and descending), and transferring (e.g., bed to chair). The ADL instruments are designed as either self-report, observation of tasks, or proxy/surrogate report.
The Katz Index of Independence in ADL
The Katz Index of ADL51 is based on the concept of physical disability and was intended to measure physical function in older adults and the chronically ill. It is one of the few functional assessment instruments to provide a theoretical framework for its domains of measurement,70 and it is the foundation for most of the newer functional assessment instruments.86 It is widely used in both clinical practice and research to measure performance, evaluate treatment outcomes, and predict the need for continuing supervised care.
The Index of ADL was developed as a hierarchical structure. Katz believed that physical functions were lost in the most complex activities first, then were lost in descending order, and were regained again in order of ascending complexity.70 Activities assessed are bathing, dressing, toileting, transferring from bed to chair, continence, and feeding. This instrument has been modified over the years since its development. A simplified method for scoring the instrument is to use a dichotomous rating of independence or dependence in the six activities (Fig. 30-2). One point is given for each independent item. Only those activities that can be performed without help are rated as independent.
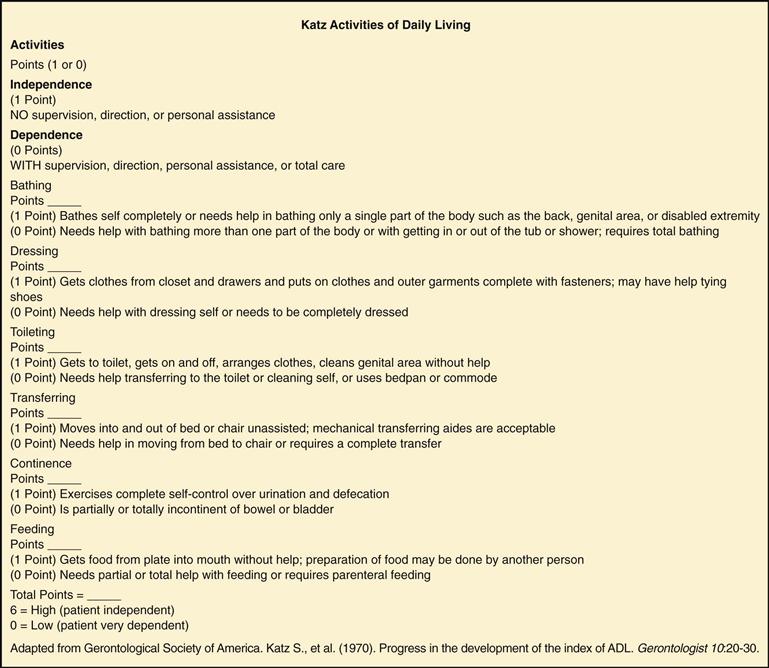
30-2
The Katz ADL is a useful instrument in many settings. The tool takes approximately 5 minutes to administer, but its use has limitations. In an outpatient setting or clinic visit, the provider cannot observe the older adult perform the activity and must rely on a self-report or surrogate report. In the hospital, nursing staff may be assisting with transferring or grooming activities and may underestimate ability for self-care. In addition, small changes in the ability to perform these activities may not be identified.
Remember that the instrument is measuring function at the current point in time and is valuable for planning specific types of assistance the older person may need. For example, a person may be unable to bathe independently on hospital discharge but can feed himself or herself and transfer to a commode safely and independently. In this case, plan for a home health aide to go twice a week to the home to assist the older adult with bathing.
Additional Activity-of-Daily-Living Instruments
Additional tools used to assess ADL ability are the Barthel Index,64 the Functional Independence Measure (FIM),39 and the Rapid Disability Rating Scale-2 (RDS-2).62,63 The Barthel Index includes definitions of each task to facilitate ease of scoring and has a more comprehensive assessment of mobility than the Katz instrument. The Barthel Index is often used to follow progress in rehabilitation settings.86
The FIM was developed by a consensus panel of physical medicine and rehabilitation staff, has been widely tested on older adults, and has a telephone, an in-person, and a proxy version of the instrument. It is more sensitive to change than the other ADL instruments but takes formal training and is more time consuming.86
The RDS-2 is completed by a family member or professional caregiver familiar with the abilities of the older adult. It is designed to measure what the person can actually do versus what he or she could do. You should conduct a training session to orient the observer to this instrument.
Instrumental Activities of Daily Living
Many IADL instruments have been developed since the 1960s, with the goal of measuring functional abilities necessary for independent community living. Typically, IADL tasks include shopping, meal preparation, housekeeping, laundry, managing finances, taking medications, and using transportation. Tasks such as yard work or home maintenance and leisure activities such as reading and other hobbies are included in some but not all IADL instruments. These instruments may have cultural and gender biases, especially in older cohorts.86 IADL instruments measure tasks (doing laundry, cooking, housework) historically done by women, and most do not address activities done primarily by men, such as home repairs and working in the yard.
Lawton Instrumental Activities of Daily Living
IADL measures were first developed by Lawton and Brody in 1969 to address higher-order components of the Katz ADL scale and to measure the more complex ADLs required for a person to adapt to the environment.86 The instrument was originally developed to determine the most suitable living situation for an older adult. The theory was that determining competence and maintenance of life skills such as shopping, cooking, and managing finances is a meaningful way to assess function because these abilities are a prerequisite for independent living. As with the Katz Index, the IADL instrument assumes a hierarchical nature of skill acquisition and loss. The Lawton IADL scale contains eight items (Fig. 30-3): use of telephone, shopping, meal preparation, housekeeping, laundry, transportation, self-medication, and management of finances. Women are scored in all eight domains, whereas men are scored in five, omitting laundry, housekeeping, and preparing food.
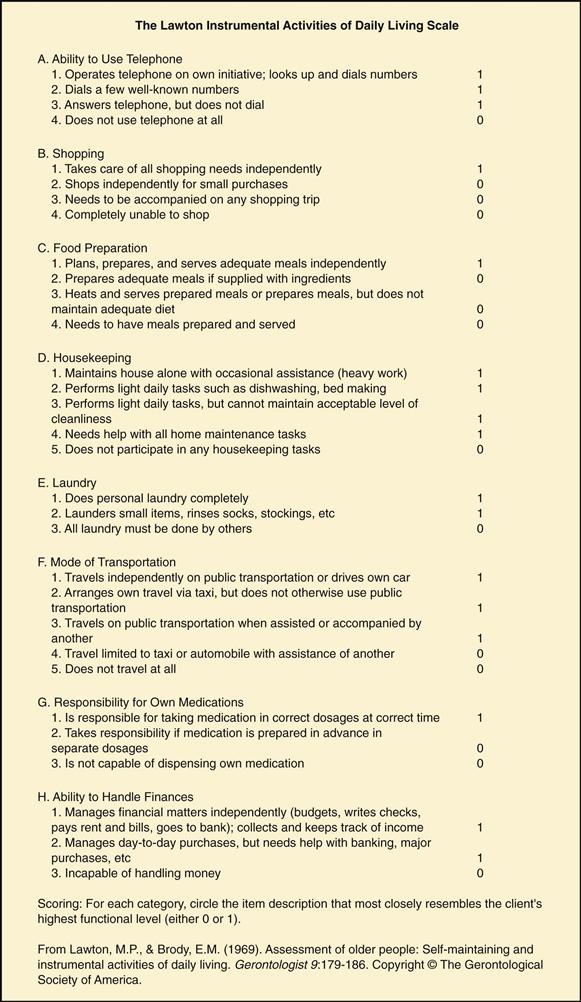
30-3
The Lawton IADL instrument is designed as a self-report measure of performance rather than ability. Direct testing is often not feasible, such as demonstrating the ability to prepare food while a hospital inpatient. Attention to the final score is less important than identifying a person’s strengths and areas where assistance is needed. The instrument is useful in acute hospital settings for discharge planning and ongoing in outpatient settings. It would not be useful for those residing in institutional settings because many of these tasks are already being managed for the resident.
Additional IADL Instruments
Other IADL instruments available are the Older Americans Resources and Services Multidimensional Functional Assessment Questionnaire-IADL (OARS-IADL)31 and the Direct Assessment of Functional Abilities (DAFA).50 The OARS-IADL assesses five areas of personal function: social, economic, mental health, physical health, and self-care capacity; it is administered either as a self-report or trained observer instrument. The questions are the same for men and women. The DAFA is a 10-item observational instrument for use with adults with dementia. It requires the person to demonstrate tasks of money management, shopping, hobbies, meal preparation, awareness, reading, and transportation.86 The obvious strength of this instrument is the direct observation versus self-reporting or proxy reporting; however, it can take up to an hour and a half to complete, so it would not be feasible to use in an acute hospital setting.
Advanced Activities of Daily Living
Advanced activities of daily living (AADLs) are activities that an older adult performs as a family member, a member of society, and community, including occupational and recreational activities.38 Various AADL instruments commonly include self-care, mobility, work (either paid or volunteer), recreational activities/hobbies, and socialization. Occupational therapists often perform assessment of AADLs. The older adult sets priorities for these activities so that interventions can be individualized.
Measuring Physical Performance
A disadvantage of many of the ADL and IADL instruments is the self-report or proxy report of functional activities. Incorporating an objective standardized measure of performance prevents overestimation or underestimation of abilities. Many of the physical performance measures also incorporate balance, gait, motor coordination, and endurance. Many of the tests are timed. Although there are clear advantages to directly observing the older adult perform the activities, there are some disadvantages. The instruments can be very time consuming, require training and special equipment, and have the possibility that the individual might fall or sustain an injury during the testing.
The Physical Performance Test (PPT)90 is appropriate for use with community-dwelling older adults. Administered by a trained observer, the test requires approximately 15 minutes to complete and assesses upper body fine motor and coarse motor activities, balance, mobility, coordination, and endurance. Activities such as eating, dressing, transferring, and stair climbing are simulated and timed.
The Performance Activities of Daily Living (PADL)56 uses a trained observer and specific props. Examples of activities tested are drinking from a cup, combing hair, shaving, lifting food with a spoon and into mouth, putting on and removing slippers, making a phone call, and turning a key in a lock. The older adult has 2 minutes to complete each task before moving on to the next one. The instrument has demonstrated high correlations with proxy reports and has a high predictive validity for future hospitalizations and mortality.86
The Get Up and Go Test67 is a reliable and valid test to quantify functional mobility. The test is quick, requires little training and no special equipment, and is appropriate to use in many settings, including hospitals and clinics. This instrument can predict a person’s ability to go outside alone safely. As the practitioner observes, the person rises from a chair, walks 10 feet, turns, walks back to the chair, and sits down. Factors to note are sitting balance, transferring from sitting to standing (e.g., does the person need to push off the armrest to rise), pace and stability of walking, ability to turn without staggering, and sitting back down in the chair. Another instrument to assess gait and balance is the Tinetti Gait and Balance Evaluation,98 a 28-point tool that is performed by trained observers and takes approximately 20 minutes to complete. Both of these instruments also provide useful information about falls risk.
Assessment of Risk for Functional Decline During Hospitalization
Losing the ability to perform ADLs and IADLs as a result of acute illness and hospitalization is common in older adults and can have significant negative consequences, including nursing home discharge and death.20,32 This functional decline is attributable to the imposition of acute illness on an aging body with diminished physiologic reserve and to limited mobility commonly experienced during a hospital admission.23 Because hospital-acquired functional decline has been noted to occur within 2 days of a hospital admission,44 it is important to identify older adults who are at greatest risk for loss of ADLs or mobility at this critical time.
One easy-to-use assessment instrument is the Hospital Admission Risk Profile (HARP)92 (Fig. 30-4). The HARP was developed based on three predictive variables for ADL loss during and after hospitalization for an acute medical illness and includes (1) older age, (2) impaired cognitive functioning, and (3) reduced IADL ability within 2 weeks before admission.92 The HARP instrument assesses patients using age, an abbreviated 21-point Folstein Mini-Mental State Exam (MMSE), and IADL preadmission status.92 The MMSE portion of the instrument consists of 10 orientation questions, registration (3 items), attention (5 items), and recall (previous 3 registration items). Depending on the score, patients are then identified as low, medium, or high risk for loss of ADLs and can be referred early for restorative interventions such as in-hospital rehabilitation, care on a geriatric unit, and multidisciplinary discharge planning.37
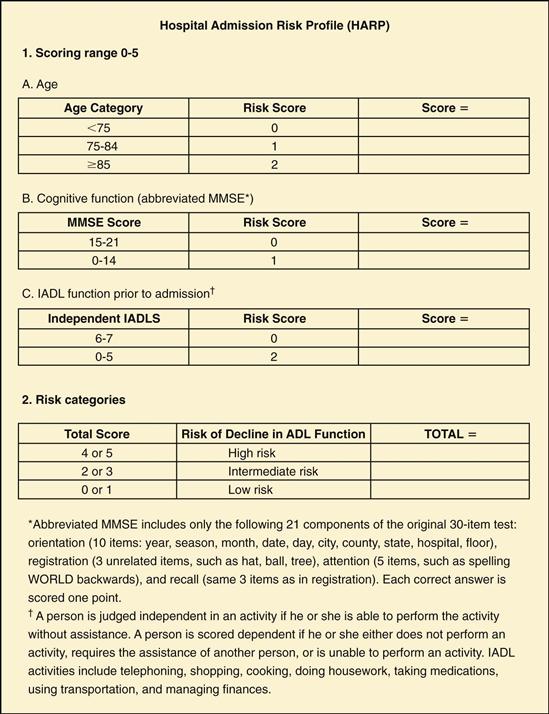
30-4
Assessment of Cognition
The assessment of cognitive status in older adults is an important part of the functional assessment. Cognitive impairment resulting from disease may be attributed by patients, families, and health care providers to normal changes with aging and can delay diagnostic workup. In general, a gradual and mild to moderate decline in short-term memory may be attributable to aging; an older adult may need more time to learn new material or a new task or may need a system for reminders. Domains of cognition included in most mental status assessments are attention, memory, orientation, language, visuospatial skills, and higher cognitive functions, such as the ability to plan and execute functioning.
Altered cognition in older adults is commonly attributed to three disorders—dementia, delirium, or depression—although other disorders, such as normal pressure hydrocephalus, also may contribute. Depressed persons often complain of memory impairment. Delirium presents as an acute change in cognition, affecting the domain of attention. Delirium is usually attributable to an acute illness, such as an infection, or a medication side effect, whereas persons with Alzheimer dementia have alterations in word finding and naming objects in addition to memory problems. These disorders commonly occur simultaneously and can complicate assessments. For example, persons with dementia are at higher risk for delirium and, in the early stages of dementia, may also be depressed.
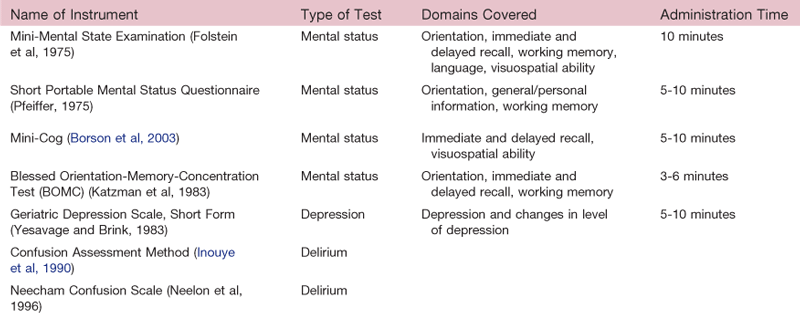
For nurses in various settings, cognitive assessments provide continuing comparisons with the individual’s baseline to detect any acute changes, such as with delirium. The assessments are not diagnostic but, rather, are for screening purposes and identify the need for a more comprehensive workup. Cognitive assessments are important for discharge planning (e.g., will the person remember to take the prescribed medications) and to assess for readiness for learning. As with screening for ADLs and IADLs, assessment of cognition helps with determining the best discharge plan. Common assessment instruments are listed in Table 30-1.
Depression and Function
Depression is common in older adults although, contrary to popular belief, it is not a normal part of aging or a natural reaction to acute illness or hospitalization. Although aging is often accompanied by loss and unwanted change, most older adults do not suffer from depression. Emotional experiences of sadness, grief, response to loss, and temporary “blue” moods are considered normal. Persistent depression that interferes significantly with ability to function is not. Fortunately, mood disorders including depression are the most common reversible psychiatric conditions in later life.
Estimates of major depression in older people living in the community range from less than 1% to about 5% but rise to 13.5% in those who require home health care and to 11.5% in hospitalized older patients.45
Functional impairment in both ADLs and IADLs has been associated with higher levels of depressive symptoms.24 Although older adults with physical impairments are at greater risk for depression, depression is not an inevitable consequence of functional impairment.
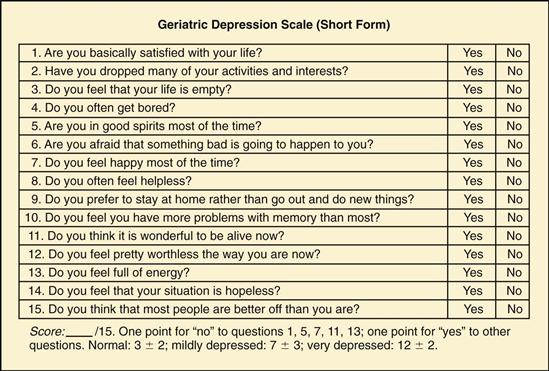
Prevention and treatment of depression may be two of the most effective targets for interventions aimed at reducing functional decline and increasing the number of years an older adult maintains independence.12,87 Therefore it is vital to screen and identify those who have depressive symptoms. Several short screening instruments have been developed and validated for depression screening in the older adult. One example of a screening tool is the Geriatric Depression Scale, Short Form (Fig. 30-5).92a,101a This basic screening tool consists of 15 yes/no questions easily used in a variety of care settings spanning from the community to acute care hospitals and long-term care settings. The Geriatric Depression Scale, Short Form can be used with both cognitively intact patients and patients who have mild to moderate cognitive impairments. Typically it takes 5 to 7 minutes to complete. Each question can equal one point. A score of 0 to 5 is considered normal; scores above 5 warrant further clinical assessment.57,92a,101a
30-5
Depression tends to be long lasting and can recur. Because of these two factors, a wait-and-see approach to treatment is not desirable and timely treatment is necessary. Common treatment options are psychotherapy, antidepressant medications, and electroconvulsive therapy.
Social Domain
The quality of life an older person experiences is closely linked to the success of social function. The social domain focuses on relationships within family, social groups, and the community and comprises multiple dimensions including the sources of formal and informal assistance available from those relationships. Knowledge of the day-to-day routines can give you baseline information and a reference point to detect functional decline during future encounters.
A comprehensive social assessment is spread over several evaluation periods. Because more than 80% of all care provided is by family members, the social assessment also addresses assessment of caregivers.14,94 By use of a multidimensional approach, potential risks such as elder mistreatment may be identified (Table 30-2).
Social networks consist of informal supports that are accessed by the older adult.74 Informal support is based on cultural beliefs regarding who should be providing care, prior relationships, and location and availability of the caregiver. Informal support includes family and close long-time friends and is usually provided free of charge. The total economic value of informal caregiving in the United States for all diseases is estimated to be at least $306 billion annually, more than twice the amount paid for nursing home care.5,75 Services provided include tasks such as shopping, bathing, feeding, and paying bills. An example of informal support is a neighbor who has daily contact with the client and shares food and company.
Formal supports include programs such as social welfare and other social service and health care delivery agencies such as home health care. Semiformal supports such as church societies, neighborhood groups, and senior centers also form an important role in social support.21,102
The availability of assistance from family or friends frequently determines whether a functionally dependent older adult remains at home or is institutionalized. Several studies conclude that the presence of a caregiver is the most important factor in the discharge plan of older adults from an acute care hospital.10 Knowing who would be available to help the person if he or she becomes ill is important to document, even for healthy older adults.
Gather your assessment of social support in a systematic manner. Several standardized assessment instruments are available to provide structured assessment. The Norbeck Social Support Questionnaire79,80 was developed to measure the multiple components of social support.* It allows the individual to rate his or her own social network and perceived social support from the network. The Norbeck Social Support Questionnaire can also be used to measure social support with caregivers. Primary caregivers (especially spouse and adult children) often face high levels of demand and limitations on personal freedom that can result in increased stress, burden, and impaired physical health.
Caregiver Assessment
Most older adults with functional impairment live in the community with the help of informal support (commonly a spouse or other family member, often a daughter). Many spousal caregivers are as frail as the person they are caring for, or many adult children are themselves older than 65 years and may be having to cope with their own chronic illnesses. Although many caregivers experience satisfaction from providing care, great mental and physical stressors may also be linked with caregiving.53,89 High levels of functional dependency place a burden on the caregiver and may result in caregiver burnout, sleep disturbances, depression, morbidity, and even increased mortality.6,83
An older person’s need for institutionalization often is better predicted from assessment of the caregiver characteristics and stress than from the severity of the patient’s illness.95 The health and well-being of the patient and caregiver are closely linked. For these reasons, part of caring for a frail older adult involves paying attention to the well-being of the caregiver. For the stressed caregiver, a health care provider may help identify programs such as caregiver support groups, respite programs, adult day care, or hired home health aides.
Assessment of Caregiver Burden
All caregivers should be screened for caregiver burden; for individuals caring for a frail, frequently cognitively impaired older adult, the demands can be overwhelming. The level of care the older adult requires may exceed caregiver ability. Caregiver burden is the perceived strain by the person who cares for an elderly, chronically ill, or disabled person. Caregiver burden is linked to the caregiver’s ability to cope and handle stress. Signs of possible caregiver burnout include multiple somatic complaints, increased stress and anxiety, social isolation, depression, and weight loss.
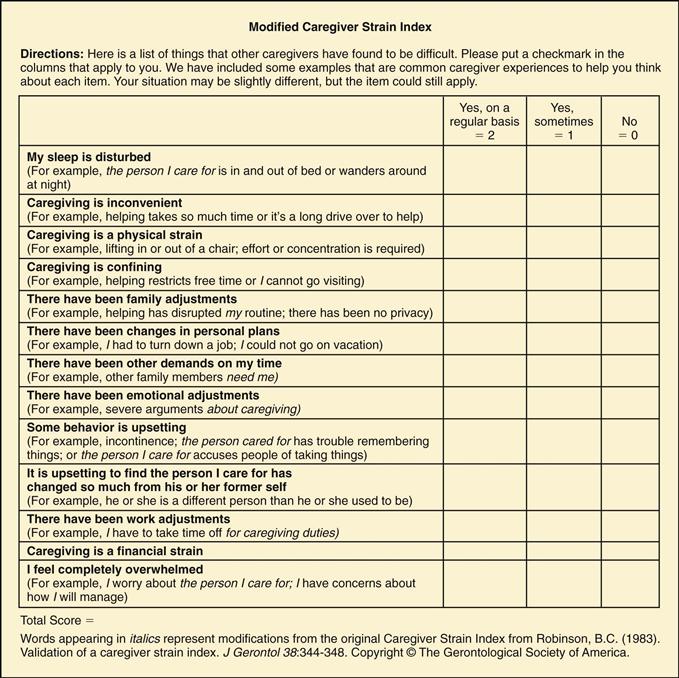
One formal screening tool is the Modified Caregiver Strain Index, which identifies caregivers of any age needing a more comprehensive assessment (Fig. 30-6). It is a brief tool with 13 questions addressing potential strain in employment, financial, physical, social, and time domains.82,97 Caregiver stress can potentially lead to elder mistreatment; therefore a thorough assessment may identify opportunities to prevent and stop elder mistreatment (see Chapter 7).
30-6
Contexts of Care
Older adults reside and enter the health care system along multiple levels or contexts of care. Nurses, as part of the health care team, care for older adults along a continuum of these contexts including acute care hospitalization, inpatient nursing facilities, in the community, and at home providing home health care. Some common threads shared by these care settings are the focus on functionally impaired older adults and optimizing the functional status and quality of life through the involvement of a team of care providers. The comprehensive functional assessment aids in determining the type and level of services an older adult may need and the most appropriate match to the needs and wants of the individual.
The location of the care setting contributes to the ability to perform a comprehensive functional assessment. It may be more difficult to perform a complete assessment in the acute care setting while the older adult is experiencing an acute illness and the length of stay may be short versus in a nursing facility where an assessment may be achieved over time. In addition, if a resident resides in the home environment, the parameters of assessment will be broader than if he or she is in an inpatient long-term living situation. For example, older adults who live at home require an assessment of the home environment and community resources available, caregiver assessment if needed, and the ability to self-perform ADLs and IADLS.
Acute Care Setting
For older adults, acute hospitalization offers the hope of relief of symptoms and treatment of illness and disease. But it also puts them at risk for adverse consequences of hospitalization including functional decline, iatrogenic complications, and subsequent discharge to a nursing facility.35,71
Researchers have found that older adults admitted to a hospital for acute illness will lose independent function in one or more ADLs.21,40,99
In the past decade, a few hospital-based models of care have emerged designed to enhance patient functioning during hospitalization and improve outcomes for older adults post-discharge. Hospitals have come to appreciate the increased risk for functional decline and adverse outcomes, and targeted interventions to prevent decline have shown to be successful. One popular model of care is the Acute Care for Elders (ACE) unit, which is a dedicated unit within a hospital setting focused toward preventing functional decline in older adults through the design of the physical environment (e.g., bright lights, flooring to help prevent falls), collaboration among interdisciplinary teams, patient-centered care, and nursing protocols for clinical care (e.g., indwelling urinary catheter removal, reduction of restraint use, early mobilization).19,84 Acute care nurses equipped with specialized knowledge and skills can have an impact on improving outcomes for the hospitalized older adult.
Community
The vast majority of older adults reside in the community, and misconceptions about nursing homes statistics are common. Fewer than 5% of older adults live in nursing homes on any given day. The percentage of those who live in a long-term care facility at any point in time increases from 1% of those ages 65 to 74 years to about 17% of those older than 85 years.3 Since the mid-1980s, the rate of nursing home residence for people older than 65 years has been declining.3 This decline can be contributed partly to the increase in assistive living facilities and popularity and availability of home health care services.
One of the goals of community-based services is to assist the older adult to remain at home. Assessment of functional status assists in determining the type of services an older adult needs to maintain independence and living at home. A low or negative result on a screening tool during assessment does not necessarily lead to the need for institutionalization. It may mean the older adult requires increased services to maintain home living. The availability of support through community services is a factor helping older adults maintain their independence and avoid institutionalization.
Home Care
Home care refers to a range of supportive social and health services provided in the home environment. Services include skilled nursing care, primary care, therapy (physical, occupational, and speech), social work, nutrition, case management, ADL assistance, and some durable medical equipment. Physical, psychosocial, and functional assessments are all part of the home care nurse’s responsibility. The home care nurse is tending not only to the illness of the older adult but also to the home safety considerations, family dynamics, and functional ability. Because of advances in health care technology, equipment is smaller and more portable. As a result, people who once were limited to hospitalization can now be treated or managed at home. In addition to cost advantages with home care versus hospitalization, older adults have been shown to recover faster when at home in familiar settings than when placed in institutions and also can avoid the risk for infection exposure.
Nursing Facilities
Nursing facilities include a broad range of services from minimal support to maximal assistance. The length of stay at nursing facilities also varies from short stays after hospitalization for rehabilitation to long-term residential living.
Assistive Living
Assistive living facilities are a popular choice for older adults and typically are considered between home care and long-term care. There is great diversity in the services provided. Most assistive living facilities provide apartment-style living, although there are some single-family dwellings that are licensed to provide care. Facilities offer homelike environments where residents have the opportunity for social interaction through group dining and activities. All provide room, meals, and housekeeping. Some offer assistance with personal care and/or support with ADLs, transportation, and recreational activities as part of an overall package; others offer services that can be added on separately.
Continuing Care Retirement Communities
The unique feature of continuing care retirement communities is that all care needs for the older adult can be met in one community, supporting the concept of aging in place. These facilities feature independent living arrangements and homes that offer a variety of social and recreational activities. But they also have assisted-living and skilled nursing level of care. In these types of communities, residents can progress through the continuum of care while residing in the same community. An older adult can enter the community at the independent level of living, and as illness and/or functional limitations occur, they can move to a higher level of support to the assisted living locations and then the skilled nursing level if needed. Some older adults may not ever leave the independent living level, whereas others may progress to skilled nursing as the need for care arises.
Maintaining Independence
Exercise
Exercise and activity are essential for health promotion and maintenance in the older adult and to assist in achieving an optimal level of functioning. A sedentary lifestyle is an important contributor to the loss in the ability to independently perform ADLs. Exercise does not prevent the process of aging, but it increases functional ability, helping to maximize the older adult’s independence.
Exercise has positive health effects in older adults, including those with impairments.43,48 The positive effects of exercise include improving cardiovascular function, postural stability, flexibility and range of motion, and strength and muscle mass; decreasing body fat; and possibly helping to reduce pain and discomfort. Because of these positive effects, fall risk and fractures may be decreased. In addition, participation in physical exercise has shown to reduce depressive symptoms and improve feelings of psychosocial well-being.42,61,72,88
The American Heart Association and the American College of Sports Medicine both provide recommendations for different types of activity and steps to implement exercise programs for those older than 65 years.78 Physical exercise is separated into four categories: aerobic, muscle strengthening, flexibility, and balance. Aerobic activity guidelines suggest a minimum of 30 minutes of moderate-intensity exercise 5 days a week or a minimum of 20 minutes of vigorous-intensity exercise 3 days a week, or a combination of both moderate and vigorous exercise. The definitions for moderate and vigorous intensity depend on the older adult’s baseline physical condition.78 Muscle strengthening includes resistance and weight training and is recommended to be performed 2 days a week. Weight training has been shown to be beneficial in the older adult for muscle strength and endurance.7 Flexibility training to maintain range of motion is recommended 2 days a week for at least 10 minutes. Balance training to improve stability is important to help prevent falls. Tai chi has been shown to improve range of motion, balance, and flexibility.7
To help with compliance, physical activities should be readily available and have minimal cost associated with participation. Because pathology, both known and undiscovered, may be present in older adults (e.g., osteoporosis), the physical activity chosen should not present excessive stress on the skeletal system. Walking is a popular mode of exercise for cardiovascular endurance, is accessible, and is associated with minimal cost. Water activities or stationary cycling may be alternative exercise modes for individuals where walking is not feasible. The American Heart Association and the American College of Sports Medicine guidelines emphasize a graduated and step-wise approach to initiating exercise.78 Developing an activity plan, particularly for older adults with chronic health conditions, may warrant clearance and input from a health care provider or referral to a specialty program (e.g., cardiac rehabilitation).
Health Care Maintenance
Functional decline and a loss of independence are not inevitable consequences of aging. Although the prevalence of chronic disease increases with age, most older people remain functionally independent. But given the presence of chronic disease among older adults, evidence-based interventions for screening and detection of health conditions and disease are important to maximize quality of life. The Agency for Healthcare Research and Quality (AHRQ) in partnership with AARP provides recommendations on daily steps to promote good health, screening tests, and medications to help in disease prevention in the publication “Staying Healthy at 50+.” It provides a guide for older adults to follow to ensure they are receiving screening appropriate for their age and health status. Multiple age-related conditions are amenable to prevention or improvement with screening and appropriate and timely intervention.
Environmental Assessment
The physical environment of the older person includes the home environment and community system and is critical to maintaining independence. Environmental hazards within the home can be a potential constraint on the older adult’s day-to-day functioning. Common environmental hazards include inadequate lighting, loose throw rugs, curled carpet edges, obstructed hallways, cords in walkways, lack of grab bars in tub and shower, and low and loose toilet seats.15,28,52 These hazards increase the risk for falls and fractures. Environmental modification can promote mobility and reduce the likelihood of the older adult’s falling.
The functional assessment should inquire about the safety of the neighborhood and ask whether older persons have transportation or transportation services available in geographic proximity to where they live (Fig. 30-7). The community needs to possess access to basic services such as food and clothing stores, pharmacists, financial institutions, health care facilities, and social service agencies. The community environment needs to provide safety conditions such as street lamps, sidewalks, and police and fire protection.15 Both the home and community environment affect the safety of the older adult.13 These are especially important for older adults dependent in IADLs and still living within the community.

30-7
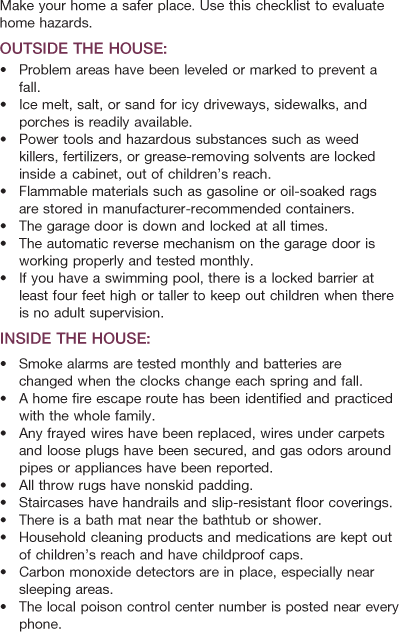
Older persons often have problems not easily detected during an office visit. A home visit can reveal challenges in the living situation, such as household and bathing hazards, social isolation, family/caregiver stress, and nutrition issues.52 For example, a walk through the kitchen can assist the health care provider in assessing the nutritional status and food preferences of the older adult. An empty refrigerator and/or kitchen cabinets may give clues to previously unrecognized functional impairment, such as dementia, mobility challenges, or a decline in the ability to perform IADLs, which would warrant further assessment. Interventions such as home health assistance, transportation, and shopping services may support the older adult to maintain community living. The U.S. Consumer Product Safety Commission website (www.cpsc.gov/CPSCPUB/PUBS/705.pdf) has a safety checklist an older person or family member can use for a self-assessment. See also Table 30-3.
Older Adult Drivers
Older adult drivers account for 15% of all licensed drivers in the United States, 8% of all traffic crash injuries, and 19% of all pedestrian fatalities.76 Safe driving requires intact cognitive functioning, sensory perception, good physical abilities (e.g., strength to turn the steering wheel and use pedals; enough range of motion to turn head and neck), alertness, and suitable reflexes.55 Early and routine attention to health care maintenance activities such as vision and hearing checks, exercise to maintain flexibility and range of motion, and workup of any cognitive abnormalities may allow the older adult to continue to drive safely for longer periods.
Driving represents independence, freedom, and control and is often a necessary part of functioning in daily life, such as getting to work or shopping for groceries. Driving also facilitates remaining connected socially with family and friends. Driving cessation can be devastating to an older adult and can lead to intensified and prolonged symptoms of depression66 and steep declines in physical functioning.27b If driving must be limited or cease altogether, it is important to establish a plan of action to enhance independence and maintain normal activity levels. This might mean accessing public transportation, carpooling, or increased involvement of family and friends for activities that require motor transportation. The decision to allow an older adult to continue driving is generally made by local state licensing agencies. Many states, either by statute or regulation, have identified mandated physician reporting obligations for conditions such as sensory impairments or neurodegenerative illnesses.
Older adults often recognize that their driving abilities have changed and adjust their driving habits accordingly, such as limiting to daytime, good weather conditions, or only local driving. However, when this is not the case, family members, friends, or health care providers may be concerned enough about the safety of the older driver and others in the community that they need to intervene. Several resources are available to assist with either self-assessment of driving skills or for use by caregivers and health care providers. One practical approach is published by The American Association of Retired Persons (AARP) and is a checklist of warning signs of when to stop driving (Table 30-4). In addition, the American Automobile Association (AAA) and AARP provide online driver self-assessment tests, and local departments of motor vehicles and area agencies on aging can provide additional resources to assist older adults and their families with ongoing assessment and planning. The National Highway Traffic Safety Administration (NHTSA) has published a brochure that outlines assessment, critical conversations, planning and evaluation, and resources for older adults, their families, or health care providers related to safe driving (www.nhtsa.dot.gov/people/injury/olddrive/UnderstandOlderDrivers/pages/Preface.html).
Table 30-4
Warning Signs for When to Stop Driving
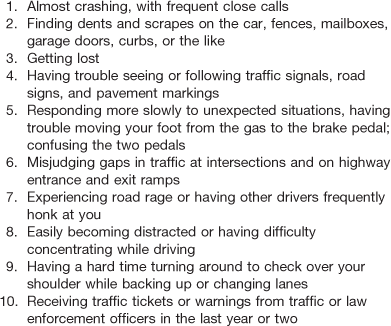
Adapted from AARP. (2010). What are the warning signs that indicate someone should begin to limit driving or to stop altogether? Retrieved January 5, 2011, from www.aarp.org/home-garden/transportation/info-05-2010/Warning_Signs_Stopping.print.html.
Sleep
Sufficient sleep is a necessary part of health. Sleep architecture does change with aging, such as more difficulty falling and staying asleep; however, significantly altered sleep patterns are not a normal part of aging, and the prevalence of insomnia is low in healthy older adults.4 Most adults of all ages need about 8 hours of sleep per night to feel alert and rested. Medical and psychiatric illnesses, such as cardiac and pulmonary disease, osteoarthritis, dementia, delirium, and depression, as well as side effects of the medications to treat these disorders (beta-blockers corticosteroids, bronchodilators, decongestants, diuretics) are contributing factors to insomnia. In addition, other causes of insomnia are intake of alcohol, nicotine, and caffeine; sleep apnea; restless leg syndrome; and circadian rhythm disturbances.4,18 Detrimental consequences of poor sleep in older adults are poor health outcomes such as obesity,81 altered physical functioning,25 falls,58 impaired cognition,81 and increased risk for death.27
Sleep is disrupted very often in the hospital; the need for tests, vital signs, and pain assessments occurs 24 hours a day. Bright lights, pagers, inability to maintain a cool environment, and staff conversation all contribute to sleep disruption. In addition, delirium, an acute and fluctuating change in mental status, is common in older hospitalized adults. Delirium contributes to disruption in sleep-wake cycles, in which patients are awake all night and difficult to keep awake during the day.
Because medications such as sedatives and hypnotics, often used to treat insomnia, have many side effects for older adults, such as falls and delirium, a nonpharmacologic approach to managing sleep in the hospital is recommended (Table 30-5). In the home, use of relaxing music; exposure to sunlight during the day; consistent bedtime routines; limiting food and drink after early evening; reduced light, noise, and room temperature; and whole-body relaxation may improve sleep.55
TABLE 30-5
Nonpharmacologic Interventions to Promote Sleep
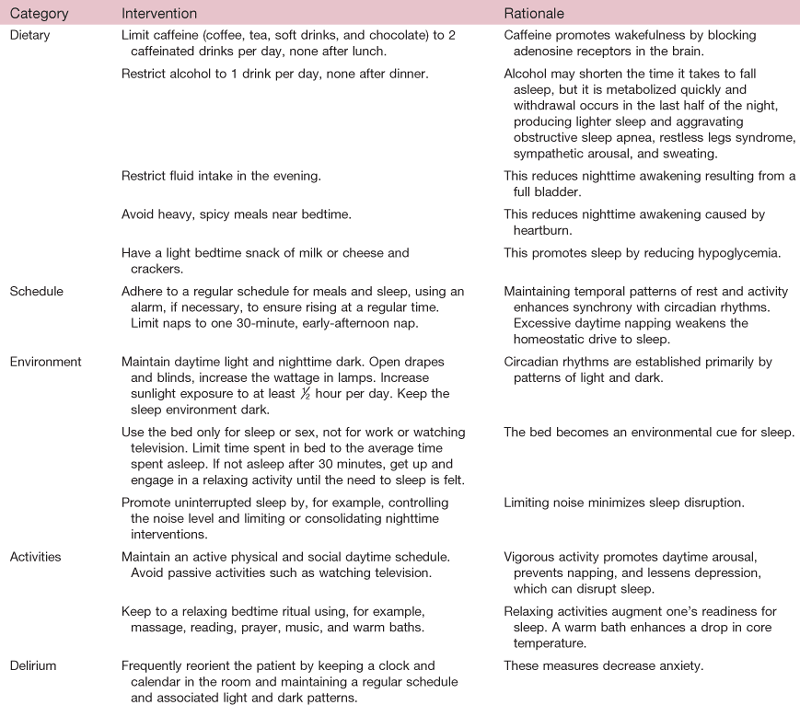
From Cole, C., & Richards, K. (2007). Sleep disruption in older adults. American Journal of Nursing, 107(5), 40-49.
One instrument useful for measurement of the quality and patterns of sleep in older adults is the Pittsburgh Sleep Quality Index (PSQI). The PSQI can be used across health care settings and can be used for initial and ongoing assessments.93
Spiritual Assessment
Spirituality provides personal answers about the meaning and purpose of one’s own life41 and how to interpret life events and regard them as “bigger than oneself.” Spiritual health may improve with age, even as physical and mental health deteriorate. The aging process is a part of one’s journey with capability for growth.8 Views on spirituality vary greatly from one adult to another and among people of the same faith or belief system. It is important to acknowledge spirituality as a powerful coping mechanism during stressful life events and illness through to the end of life.73
Spiritual assessment is highly individual and may be delayed until a provider-client relationship has been developed. Open-ended questions provide a foundation for future dialogue. A sample question posed during the initial assessment may be “Do you consider yourself to be a spiritual person?” If the person says “yes,” a follow-up question could be “How does that spirituality relate to your health or health care decisions?” Involving chaplains or clergy members when possible and appropriate can provide the older adult with support and can serve as a resource to the clinician.
Special Considerations
Assessment of the functional status of an older adult can be more time consuming than for younger adults. It may take longer for him or her to understand and process the questions and to respond. The presence of physical disabilities, anxiety, depression, pain, or fatigue may necessitate several sessions to complete the assessment (Fig. 30-8). The older adult may need assistance with clothing and may prefer that a family member be present for all or parts of the examination. For hospitalized or institutionalized older adults, consider assessing function during normal activities such as grooming, at mealtime, or during toileting.

30-8
Understand that a person with multiple medical problems may tire early and easily and that many medications have side effects that contribute to fatigue or affect the attention span. Again, assessments may need to be done incrementally, such as positioning for comfort and clustering similar tasks to prevent fatigue. Having the person use glasses or hearing aids can mitigate communication difficulties resulting from vision or hearing loss. Provide directions in written format if necessary, and have hearing amplifiers and page magnifiers available. Face the person as much as possible, speak slowly in a lower-pitched voice, and enunciate words clearly. Be prepared to use interpreters rather than family members for non–English-speaking clients.
Older adults are a heterogeneous group. You must be aware of your own attitudes and beliefs about older adults to ensure that the functional assessment is truly reflecting abilities and not the myth that functional decline is a normal outcome of aging. Demonstrating respect and interest and treating the client as an individual are imperative. Ask how the older adult would like to be addressed. Maximize communication by using terminology understandable to the person rather than using medical jargon. Including the older adult in decision making about how the interview or testing is to be done will establish rapport and promote self-esteem. Be aware of body language and behaviors, and be prepared to modify your approach. Touch can also help in establishing rapport and can reduce anxiety.
A functional assessment can be intimidating for older adults. Frustration or embarrassment may arise if some physical maneuvers cannot be performed or questions cannot be answered during cognitive testing. They may also be fearful about the consequences of functional testing, such as losing independent living or having a caregiver move into the home. Try to provide reassurance that not everyone can complete all of the tasks or answer all of the questions and that, to the extent possible, confidentiality will be honored.
Ensure adequate space if doing tests of mobility. An aging adult may need room to maneuver an assistive device. When testing mobility, stand close to him or her to prevent a fall. The environment should be well lighted with increased illumination; avoid high-gloss, shiny, slippery surfaces. Minimize extraneous noise such as those from intercoms, televisions, or high-traffic areas. Warm rooms, access to fluids, proximity to a bathroom, and privacy are important.
Cultural Considerations
Be aware that cultural influences are parts of the person’s life (review Chapter 2). Food habits and dietary beliefs may conflict with dietary recommendations made by health care providers. The response to pain, including how it is perceived, how much is considered tolerable, and the reaction to pain experienced, varies among and within different cultures. How the person interprets the symptoms, meaning, and causes of illness can be defined by his or her culture. It also plays a part in when the older adult seeks care and may influence how the illness is treated. He or she may want to try traditional/alternative practices to prevent or treat certain conditions.
Wide differences appear among individuals in every culture. Learn how the person’s culture fits together with suggested interventions. Culture also influences whether the older adult relies on family for care or the approach to decision making (i.e., involvement of family and friends), disclosure of medical information (e.g., cancer diagnosis), and end-of-life care (i.e., advance directives, resuscitation preferences, and nutrition).16,33,101
Assessing Those in Pain
If the older adult is feeling pain or discomfort, the depth of knowledge gathered through the assessments will suffer. Alleviating pain should be a priority over other aspects of the assessment. It may be necessary to administer premedication before portions of the assessment, especially if the assessment requires movement. Another strategy is to use positioning to decrease pain. Ask what position is most comfortable. Providing comfort can help maximize the information gathered. It is paramount to remember older adults with cognitive impairment do not experience less pain. This population suffers from conditions typically associated with pain (e.g., arthritis, osteoporosis, cancer, shingles) just as frequently as cognitively intact persons.
A variety of pain assessment scales are available to use in the cognitively impaired older adult population. The “gold standard” continues to be a person’s self-report. Several studies have demonstrated that those with cognitive impairment can provide self-report pain, which must be taken seriously.85
Assessing Older Adults with Altered Cognition
Cognitive impairment poses unique challenges. The older adult may not be able to actively participate in the evaluation and/or provide consistent answers. Gathering information from the older adult firsthand is always the best but is not always feasible. To ensure the collection of reliable information, one strategy is to interview the caregiver and/or family to obtain subjective assessment data. Another is to arrange opportunities to assess the person during different times of the day, when he or she may be more clear-headed. If possible, split the assessment into smaller sections at a time. Be flexible.
Adults with cognitive impairment may need questions or directions broken down into single commands, repeated word for word, with ongoing verbal cueing or a physical cue. For example, after getting the person’s attention, the interviewer might say “sit here” and pat the chair. Never assume that he or she cannot respond to questions even when there is known cognitive impairment. Using yes or no questions may prevent frustration. Be relaxed and patient because a person with dementia may mirror your emotions. If a family member or caregiver does need to provide collateral information, avoid doing this in front of the person.
Bibliography
1. AARP. Know when to limit or stop driving. Retrieved January 5, 2010, from www.aarp.org/home-garden/transportation/info-05-2010/Warning_Signs_Stopping.print.html; 2010.
2. Reference deleted in proofs.
3. Administration on Aging. Aging statistics. Retrieved August 31, 2009, from www.aoa.gov/AoARoot/Aging_Statistics/index.aspx; 2008.
4. Ancoli-Israel S. Sleep and its disorders in aging populations. Sleep Medicine. 2009;10(Suppl. 1):S7–S11 2009.
5. Arno PS, Levine C, Memmott MM. The economic value of informal caregiving. Health Affairs. 1999;18:182–188.
6. Beach SR, Schulz R, Williamson GM, et al. Risk factors for potentially harmful informal caregiver behavior. Journal of the American Geriatrics Society. 2005;53:255–261.
7. Bellew JW, Symons TB, Vandervoort AA. Geriatric fitness: effects of aging and recommendations for exercise in older adults. Cardiopulmonary Physical Therapy Journal. 2005;16(1):20–31.
8. Berggren-Thomas P, Griggs MJ. Spirituality in aging: spiritual need or spiritual journey? Journal of Gerontological Nursing. 1995;21(3):5–10.
9. Reference deleted in proofs.
10. Brown LJ, Potter JF, Foster BG. Caregiver burden should be evaluated during geriatric assessment. Journal of the American Geriatrics Society. 1990;38:455–460.
11. Buhr GT, Kuchibhatla M. Caregivers’ reasons for nursing home placement: cues for improving discussions with families prior to transition. The Gerontologist. 2006;46(1):52–61.
12. Callahan CM, Kroenke K, Counsell SR, et al. Treatment of depression improves physical functioning in older adults. Journal of the American Geriatrics Society. 2005;53:367–373.
13. Carol W. Socioeconomic and environmental influences. In: Lueckenotte AG, ed. Gerontological nursing. St. Louis: Mosby; 1996;180–191.
14. Chichin E, et al. Caregiving/mistreatment. In: Mezey M, Fulmer T, Mariano C, eds. Best nursing practices for older adults: incorporating essential gerontological content into baccalaureate nursing education and staff development. 3rd ed. New York: American Association of Colleges of Nursing Washington DC & The John A. Hartford Foundation Institute for Geriatric Nursing; 2001.
15. Chu N. Environment/home. In: Luggen AS, Travis SS, Meiner S, eds. NGNA core curriculum for gerontological advanced practice nurses. Thousand Oaks, CA: SAGE; 1998.
16. Chu NL. Culture, race, and ethnicity. In: Luggen AS, Travis SS, Meiner S, eds. NGNA core curriculum for gerontological advanced practice nurses. Thousand Oaks, CA: SAGE; 1998.
17. Cole C, Richards K. Sleep disruption in older adults. American Journal of Nursing. 2007;107(5):40–50.
18. Cooke JR, Ancoli-Israel S. Sleep and its disorders in older adults. Psychiatric Clinics of North America. 2006;29(4):177–193.
19. Counsell SR, Holder CM, Liebenauer LL, et al. Effects of a multicomponent intervention on functional outcomes and process of care in hospitalized older patients: a randomized controlled trial of acute care for elders (ACE) in a community hospital. Journal of the American Geriatrics Society. 2000;48(12):1572–1581.
20. Covinsky KE, Justice AC, Rosenthal GE, et al. Measuring prognosis and case mix in hospitalized elders: the importance of functional status. Journal of General Internal Medicine. 1997;12(4):203–208.
21. Covinsky KE, Newcomer R, Fox P, et al. Patient and caregiver characteristics associated with depression in caregivers on patients with dementia. Journal of General Internal Medicine. 2003;18(12):1006–1014.
22. Reference deleted in proofs.
23. Creditor MC. Hazards of hospitalization of the elderly. Annals of Internal Medicine. 1993;18(3):219–223.
24. Cummings SM, Neff JA, Husaini BA. Functional impairment as a predictor of depressive symptomatology: the role of race, religiosity, and social support. Health & Social Work. 2003;29(1):23–32.
25. Dam TT, Ewing S, Ancoli-Israel S, et al. Association between sleep and physical function in older men: the osteoporotic fractures in men sleep study. Journal of the American Geriatrics Society. 2008;56(9):1665–1673.
26. DeFrances CJ, Lucas CA, Buie VC, et al. 2006 National hospital discharge survey. National Health Statistics Reports. 2008;30(5):1–20.
27. Dew MA, Hoch CC, Busse DJ, et al. Healthy older adults’ sleep predicts all-cause mortality at 4 to 19 years of follow-up. Psychosomatic Medicine. 2003;65(1):63–73.
28a. Duke University and the National Institute on Aging. National Long Term Care Survey. Retrieved January 5, 2011, from http://www.nltcs.aas.duke.edu/index.htm; 1999.
28b. Edwards JD, Lunsman M, Perkins M, et al. Driving cessation and health trajectories in older adults. Journal of Gerontology: A Biological Science. 2009;64(12):1290–1295.
29a. Eliopoulis C. Gerontological nursing. 4th ed Philadelphia: Lippincott; 1997.
29b. Reference deleted in proofs.
30. Reference deleted in proofs.
31. Fillenbaum GG, Smyer MA. The development, validity, and reliability of the OARS multidimensional functional assessment questionnaire. Journal of Gerontology. 1981;36(4):428–434.
32. Fortinsky RH, Covinsky KE, Palmer RM, et al. Effects of functional status changes before and during hospitalization on nursing home admission of older adults. The Journals of Gerontology Series A, Biological Sciences and Medical Sciences. 1999;54(10):M521–M526.
33. Reference deleted in proofs.
34. GeroNurse Online. Why gerontological nursing certification? Retrieved January 5, 2011, from www.geronurseonline.com/; 2009.
35. Gillis A, MacDonald B. Deconditioning in the hospitalized elderly. Canadian Nurse. 2005;101(6):16–20.
36. Reference deleted in proofs.
37. Graf C. The hospital admission risk profile. American Journal of Nursing. 2008;108(8):62–72.
38. Guse LW. Assessment of the older adult. In: Mauk KL, ed. Gerontological nursing competencies for care. Sudbury, MA: Jones & Bartlett; 2006;265–292.
39. Hamilton BB, Granger CV, Sherwin FS, et al. A uniform national data system for medical rehabilitation. In: Fuher MJ, ed. Rehabilitation outcomes: analysis and measurement. Baltimore: Brooks; 1987.
40. Hart BD, Birkas J, Lachmann M, et al. Promoting positive outcomes for elderly persons in the hospital: prevention and risk factor modification. AACN Clinical Issues. 2002;13(1):22–33.
41. Heriot CS. Spirituality and aging. Holistic Nursing Practice. 1992;7(1):22–31.
42. Hessert MJ, Gugliucci MR, Pierce HR. Functional fitness: maintaining or improving function for elders with chronic diseases. Family Medicine. 2005;37(7):472–476.
43. Heyn P, Abreu BC, Ottenbacher KJ. The effects of exercise training on elderly persons with cognitive impairment and dementia: a meta-analysis. Archives of Physical Medicine and Rehabilitation. 2004;85(10):1694–1704.
44. Hirsch CH, Sommers L, Olsen A, et al. The natural history of functional morbidity in hospitalized patients. Journal of the American Geriatrics Society. 1990;38(12):1296–1303.
45. Hybels CF, Blazer DG. Epidemiology of late-life mental disorders. Clinics in Geriatric Medicine. 2003;19(4):663–696.
46. Inouye SK, van Dyck CH, Alessi CA, et al. Clarifying confusion: the confusion assessment method. Annals of Internal Medicine. 1990;113:941–948.
47. Reference deleted in proofs.
48. Jette AM, Keysor JJ. Disability models: implications for arthritis exercise and physical activity interventions. Arthritis and Rheumatism. 2003;49:114–120.
49. Reference deleted in proofs.
50. Karagiozis H, Gray S, Sacco J, et al. The direct assessment of functional abilities (DAFA): a comparison to an indirect measure of instrumental activities of daily living. The Gerontologist. 1998;38:113–121.
51. Katz S, Ford AB, Moskowitz RW, et al. Studies of illness in the aged: the index of ADL, a standardized measure of biological and psychosocial functioning. Journal of the American Medical Association. 1963;185:94–101.
52. Kim LC, Dyer CB. Assessment of older adults in their homes. In: Gallo JJ, ed. Handbook of geriatric assessment. 4th ed. Sudbury, MA: Jones & Bartlett; 2006.
53. Kramer B. Gain in the caregiving experience: Where are we? What next? The Gerontologist. 1997;37:218–232.
54. Kresevic DM, Mezey M. Assessment of function. In: Mezey M, ed. Geriatric nursing protocols for best practice. 2nd ed New York: Springer Publishing; 2003;31–46.
55. Krieger-Blake LS. Changes that affect independence in later life. In: Mauk KL, ed. Gerontological nursing: competencies for care. Boston: Jones & Bartlett; 2006;321–354.
56. Kuriansky JB, Gurland B. Performance test of activities of daily living. International Journal of Aging & Human Development. 1976;7:343–352.
57. Kurlowicz L, Greenberg SA. The Geriatric Depression Scale, Try this: best practices in nursing care to older adults. Issue #4. Retrieved September 1, 2009, from http://consultgerirn.org/uploads/File/trythis/try_this_4.pdf; Revised 2007.
58. Latimer HillE, Cumming RG, Lewis R, et al. Sleep disturbances and falls in older people. The Journal of Gerontology Series A, Biological Sciences and Medical Sciences. 2007;62(1):62–66.
59. Lawton MP, Brody EM. Assessment of older people: self-maintaining and instrumental activities of daily living. The Gerontologist. 1969;9:179–186.
60. Lehman CA, Poindexter A. The aging population. In: Mauk KL, ed. Gerontological nursing: competencies for care. Boston: Jones & Bartlett; 2006;29–56.
61. Lin S, Woollacott M. Postural muscle responses following changing balance threats in young, stable older, and unstable older adults. Journal of Motor Behavior. 2002;34(1):37–44.
62. Linn M. Rapid Disability Rating Scale-2 (RDRS-2). Psychopharmacology Bulletin. 1988;24:799–800.
63. Linn M, Linn B. The Rapid Disability Rating Scale-2. Journal of the American Geriatrics Society. 1982;30:378–382.
64. Mahoney FI, Barthel DW. Functional evaluation: the Barthel Index. Maryland State Medical Journal. 1965;14:61–65.
65. Reference deleted in proofs.
66. Marottoli RA, Mendes de Leon CF, Glass TA, et al. Driving cessation and increased depressive symptoms: prospective evidence from the New Haven Established Populations for Epidemiologic Studies of the Elderly (EPESE). Journal of the American Geriatrics Society. 1997;45:202–206.
67. Mathias S, Nayak US, Isaacs B. Balance in elderly patients: the “Get Up and Go” test. Archives of Physical Medicine and Rehabilitation. 1986;67:387–389.
68. Reference deleted in proofs.
69. Mauk KL. Introduction to gerontological nursing. In: Mauk KL, ed. Gerontological nursing: competencies for care. Boston: Jones & Bartlett; 2006;5–28.
70. McDowell I, Newell C. Measuring health: a guide to rating scales and questionnaires. 2nd ed New York: Oxford University Press; 1996.
71. Mezey MD, Fulmer T, Abraham I. Geriatric nursing protocols for best practice. 2nd ed. New York: Springer Publishing; 2003.
72. Milton D, Porcari JP, Foster C, et al. The effect of functional exercise training on functional fitness levels of older adults. Gundersen Lutheran Medical Journal. 2008;5(1):4–8.
73. Moore S. Spirituality. In: Luggen AS, Travis SS, Meiner S, eds. NGNA core curriculum for gerontological advanced practice nurses. Thousand Oaks, CA: SAGE; 1998.
74. Morano C, Morano B. Social assessment. In: Gallo JJ, ed. Handbook of geriatric assessment. 4th ed. Sudbury, MA: Jones & Bartlett; 2006.
75. National Family Caregivers Association (NFCA) and Family Caregiver Alliance (FCA). Prevalence, hours and economic value of family caregiving: updated state-by-state analysis of 2004 national estimates. Kensington, MD: NFCA; and San Francisco: FCA; 2006.
76. National Highway Traffic Safety Administration National Center for Statistics and Analysis. 2007 data—traffic safety facts: older adults (DOT HS 810 992). Washington, DC: National Highway Traffic Safety Administration; 2007.
77. Reference deleted in proofs.
78. Nelson ME, Rejeski J, Blair SN, et al. Physical activity and public health in older adults: recommendations from the American College of Sports Medicine and the American Heart Association. Circulation. 2007;116:1094–1105.
79. Norbeck JS, Lindsey AM, Carrieri VL. The development of an instrument to measure social support. Nursing Research. 1980;30:264–269.
80. Norbeck JS, Lindsey AM, Carrieri VL. Further development of the Norbeck Social Support Questionnaire: normative data and validity testing. Nursing Research. 1983;32:4–9.
81. Ohayon MM, Vecchierini MF. Normative sleep data, cognitive function and daily living activities in older adults in the community. Sleep. 2005;289(8):981–989.
82. Onega LL. How to try this—helping those who help others: the modified caregiver strain index. American Journal of Nursing. 2008;108(9):62–70.
83. O’Rourke N, Tuokko H. The psychological and physical costs of caregiving: the Canadian Study of Health and Aging. Journal of Applied Gerontology. 2000;19:389–404.
84. Palmer RM, Counsell SR, Landefeld SC. Acute care for elders unit: practical considerations for optimizing health outcomes. Disease Management and Health Outcomes. 2003;11(8):507–517.
85. Pautex S, Gold G. Assessing pain intensity in older adults. Geriatrics & Aging. 2006;9:399–402.
86. Pearson V. Assessment of function. In: Kane R, Kane R, eds. Assessing older persons: measures, meaning and practical applications. New York: Oxford University Press; 2000;17–48.
87. Penninx BW, Deeg DJ, van Eijk JT, et al. Changes in depression and physical decline in older adults: a longitudinal perspective. Journal of Affective Disorders. 2000;61:1–12.
88. Penninx BW, Rejeski WJ, Pandya J, et al. Exercise and depressive symptoms: a comparison of aerobic and resistance exercise effects on emotional and physical function in older persons with high and low depressive symptomatology. The Journal of Gerontology Series B, Psychological Sciences and Social Sciences. 2002;57:P124–P132.
89. Pinquart M, Sorensen S. Correlates of physical health of informal caregivers: a meta-analysis. The Journal of Gerontology Series B, Psychological Sciences and Social Sciences. 2007;62(2):126–137.
92. Reuben DB, et al. Geriatrics at your fingertips. New York: The American Geriatrics Society; 2009.
90. Reuben DB, Siu AL. An objective measure of physical function of elderly outpatients: the physical performance test. Journal of the American Geriatrics Society. 1990;38(10):1105–1112.
91. Richmond T, Tang ST, Tulman L, et al. Measuring function. In: Frank-Stromberg M, Olsen SJ, eds. Instruments for clinical health-care research. 3rd ed Sudbury, MA: Jones & Bartlett; 2004.
92. Sager MA, Rudberg MA, Jalaluddin M, et al. Hospital admission risk profile (HARP): identifying older patients at risk for functional decline following acute medical illness and hospitalization. Journal of the American Geriatrics Society. 1996;44(3):251–257.
96. Sheikh JI, Yesavage JA. Geriatric depression scale: Recent evidence and development of a shorter version. Clinical Gerontology. 1986;5:165–172.
93. Smyth CA. Evaluating sleep quality in older adults. The American Journal of Nursing. 2008;108(5):42–51.
94. Stone R, Cafferate GL, Sangl J. Caregivers of the frail elderly: a national profile. The Gerontologist. 1987;27:616–626.
95. Reference deleted in proofs.
96. Sullivan MT. The modified caregiver strain index (CSI), Try this: best practices in nursing care to older adults. Issue # 14. Retrieved January 5, 2011 from http://consultgerirn.org/uploads/File/trythis/try_this_14.pdf; Revised 2007.
97. Thornton M, Travis SS. Analysis of the reliability of the modified caregiver strain index. The Journals of Gerontology Series B, Psychological Sciences and Social Sciences. 2003;58B(2):127–132.
98. Tinetti ME. Performance-oriented assessment of mobility problems on elderly patients. Journal of the American Geriatrics Society. 1986;34:119–126.
99. Tucker D, Molsberger SC, Clark A. Walking for wellness: a collaborative program to maintain mobility in hospitalized older adults. Geriatric Nursing. 2004;25(4):242–245.
100. Reference deleted in proofs.
101. Welch A. Cultural influences. In: Lueckenotte AG, ed. Gerontological nursing. St. Louis: Mosby; 1996.
106. Yesavage JA, Brink TL, Rose TL, et al. Development and validation of a geriatric depression rating scale: a preliminary report. Journal of Psychiatric Research. 1983;17:27.
102. Zarit S, Pearlin L. Family caregiving: integrating informal and formal systems for care. In: Zarit S, Pearlin L, Schaie K, eds. Caregiving systems: informal and formal helpers. Hillsdale, NJ: L. Erlbaum Associates; 1993;303–316.
*Norbeck Social Support Questionnaire is available online at http://evolve.elsevier.com/Jarvis.