29 ASTHMATIC ATTACK: WHAT TO LOOK FOR
| Acute asthma: | A disorder characterised by paroxysmal narrowing of the bronchi. The bronchoconstriction causes wheezing, shortness of breath and a tight feeling in the chest. |
CXR FINDINGS IN ACUTE ASTHMA
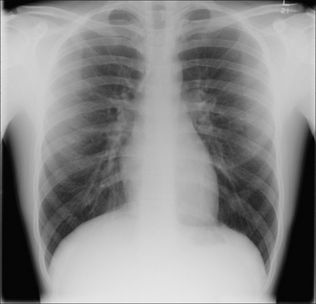
In 95% of patients the CXR is normal. In a few patients the lungs demonstrate hyperinflation—i.e. generalised hyperlucency (increased blackening) with the domes of the diaphragm unusually low.
IS A CXR NECESSARY?1-4

WHEN IS A CXR USEFUL?

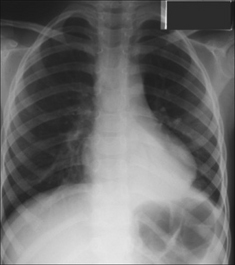
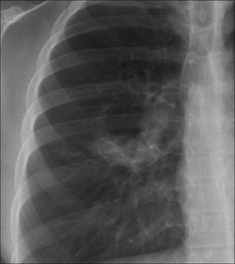
Figure 29.2 Acute asthma. Unexplained clinical deterioration. Collapse of the left lower lobe due to a mucus plug in the bronchus.
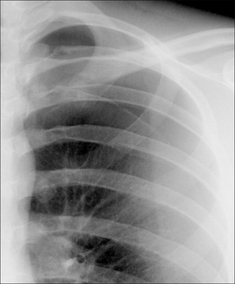
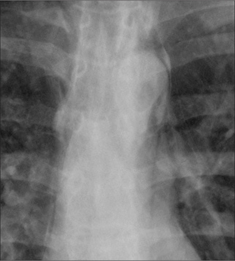
Figure 29.4 Acute asthma. Pleuritic chest pain. Extensive mediastinal emphysema. The process causing the emphysema is explained on pp. 123–124.
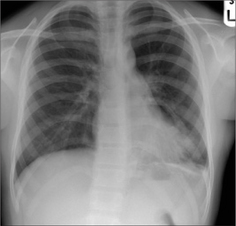
Figure 29.5 Acute asthma. Unexpected clinical deterioration. Left-sided shadowing effaces the heart border. Pneumonia. The consolidation—pneumonia—is situated in a lingular segment of the left upper lobe.
AN INTERESTING CONDITION—ABPA4,7
ABPA = allergic bronchopulmonary aspergillosis
Aetiology/pathology
A rare cause of asthma. Spores of the fungus Aspergillus fumigatus are inhaled. A hypersensitivity reaction is induced. The bronchi contain hyphae and the walls of the large bronchi become damaged resulting in proximal bronchiectasis; the upper lobes are especially affected.
Clinical features
Asthma unresponsive to conventional treatment. Blood eosinophilia. Immediate skin reaction to Aspergillus.
The CXR
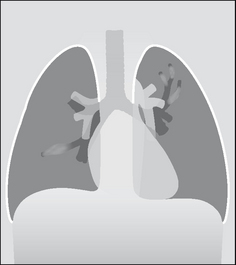
Recognition of the classical CXR appearances resulting from ABPA may be the first signal that the patient does not have simple asthma. If the proximal bronchi become dilated and filled with mucus this causes a CXR appearance which is referred to as the toothpaste shadow, or a finger-in-glove appearance (Figs 29.6 and 29.7). Pulmonary densities, representing areas of acute eosinophilic infiltration of the alveoli4 also occur. These shadows often come and go—they flit—sometimes spontaneously, sometimes in response to steroid treatment.
1. Findley LJ, Sahn SA. The value of chest roentgenograms in acute asthma in adults. Chest. 1981;80:535-536.
2. Dawson KP, Capaldi N. The chest X-ray and childhood acute asthma. Aust Clin Rev. 1993;13:153-156.
3. Tsai TW, Gallagher EJ, Lombardi G, et al. Guidelines for the selective ordering of admission chest radiography in adult obstructive airway disease. Ann Emerg Med. 1993;22:1854-1958.
4. Lynch DA. Imaging of asthma and allergic bronchopulmonary mycosis. Radiol Clin North Am. 1998;36:129-142.
5. Mecoy RJ. When a wheeze is not asthma. Aust Fam Physician. 1993;22:941-945.
6. Scott PM, Glover GW. All that wheezes is not asthma. Br J Clin Pract. 1995;49:43-44.
7. Patterson R, Greenberger PA, Radin RC, et al. Allergic bronchopulmonary aspergillosis: staging as an aid to management. Ann Intern Med. 1982;96:286-291.