32 BLUNT TRAUMA: WHAT TO LOOK FOR
Following an injury to the thorax, a CXR is usually the baseline radiographic examination.
A normal CXR will often provide considerable clinical reassurance.
Deciding that the CXR is normal depends on an informed and accurate assessment of the image.
MVA: motor vehicle accident (USA) RTA: road traffic accident (UK)
QUESTION 1—ARE THERE ANY FRACTURES?
MINOR THORACIC TRAUMA
There is no indication for a routine CXR in the majority of these patients. Demonstration of a simple rib fracture on a radiograph will not affect treatment. The only indication for a CXR is to exclude a pneumothorax in a patient in whom the pain or other symptoms raise this possibility. Oblique views of the ribs are not indicated.
MAJOR THORACIC TRAUMA1-6
Particular sites need special attention (Figs 32.1-32.3).
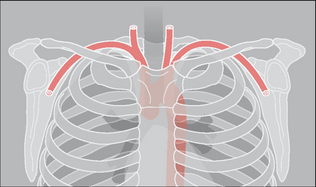
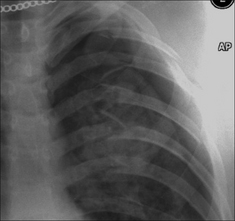
Figure 32.1 There is a close relationship between the subclavian artery and the posterior aspect of the first rib and the clavicle. The first rib is very strong. If an injury causes a fracture of this rib then it should be assumed that a very powerful blow has been sustained.
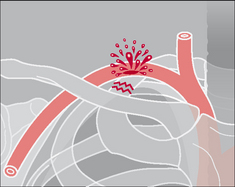
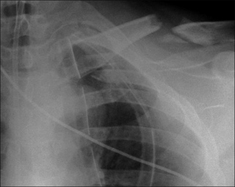
Figure 32.3 RTA. Fractures of the left clavicle, third rib, and scapula. Clearly, a very violent force had occurred. The priority: clinical assessment to rule out a vascular injury.
Double check ribs 1–3, the clavicles, and the scapulae7,8
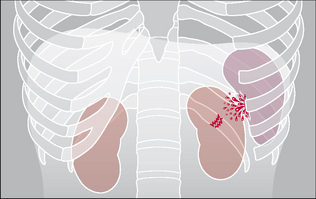
Double check ribs11–12
A fracture of either of these floating ribs may cause a laceration to the liver, spleen, or kidney (Fig. 32.4). Look very carefully because this area of the radiograph is often underexposed.
Look for a flail segment
 A flail segment is clinically important because it may cause paradoxical movement of the adjacent lung, which can adversely affect gas exchange. This effect varies between patients. Mechanical ventilation may be required. A flail segment is defined as two fractures in each of two or more adjacent ribs. It may also:
A flail segment is clinically important because it may cause paradoxical movement of the adjacent lung, which can adversely affect gas exchange. This effect varies between patients. Mechanical ventilation may be required. A flail segment is defined as two fractures in each of two or more adjacent ribs. It may also:
 Result from a fracture involving the sternum and/or a fracture extending across the midline to involve the opposite ribs. Involve the costal cartilages on each side of the midline. When this occurs the abnormal segment will not be recognised on a CXR because cartilaginous fractures are not visible on a radiograph (Fig. 32.6).
Result from a fracture involving the sternum and/or a fracture extending across the midline to involve the opposite ribs. Involve the costal cartilages on each side of the midline. When this occurs the abnormal segment will not be recognised on a CXR because cartilaginous fractures are not visible on a radiograph (Fig. 32.6).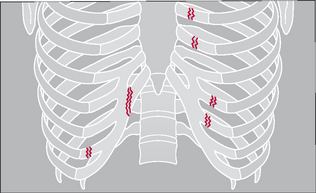
Assess the sternum carefully
Clinical suspicion of a possible fracture of the sternum must be relayed to the radiographer (technologist) because diagnosis normally requires an additional lateral (cross-table) radiograph.
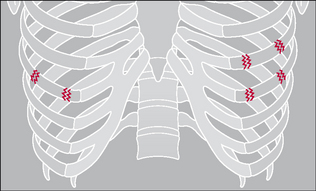
Figure 32.5 The rib fractures on the right side do not indicate a flail segment. On the left side there are two fractures in each of two adjacent ribs: a flail segment is present.
Sternoclavicular dislocations rarely cause an important soft tissue injury, but a sternal fracture always raises the possibility of an injury to the myocardium.
QUESTION 2—IS THERE A PNEUMOTHORAX?
Following violent trauma the CXR is obtained with the patient lying on a trolley or examination couch. A large pneumothorax will be obvious. Smaller pneumothoraces are more difficult to detect on a supine CXR. Recognising a small pneumothorax is important—particularly if the patient is to be treated with positive pressure ventilation.
The features indicating a pneumothorax on a supine CXR are described in Chapter 7, pp. 97–100.

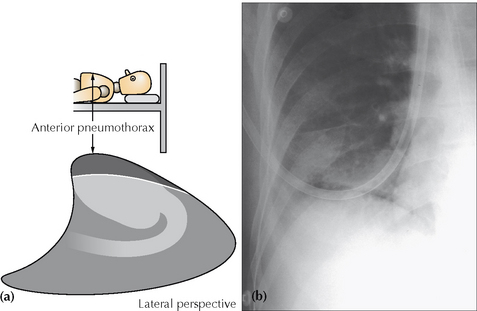
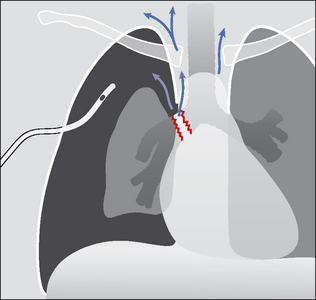
Figure 32.8 Pneumothorax. When the injured patient is lying supine, air in the pleural space collects at the highest point—i.e. anteriorly (a). On the frontal CXR the visceral pleural line may not be evident. The diagnosis will need to be made by scrutinising the areas around the dome of the diaphragm and adjacent to the lateral border of the heart (b). The black line outlining the diaphragm indicates a pneumothorax: see p. 97 for a detailed description.
QUESTION 3—IS THERE A PNEUMOMEDIASTINUM?
The CXR appearances of a pneumomediastinum are described in Chapter 8, pp. 123–127. If serial CXRs show a persistent severe pneumomediastinum (+/– pneumothorax) then consider whether there is an unrecognised tracheobronchial rupture (p. 366) or an unrecognised oesophageal rupture.

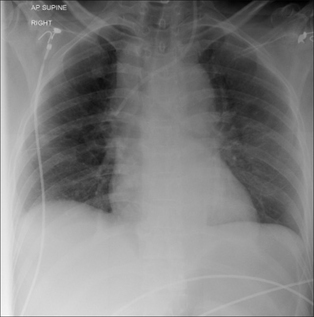
Figure 32.9 Male. Age 56. Intoxicated and fell over. Supine CXR. Multiple rib fractures. Air outlines the descending aorta; it has also dissected outside the pleura and appears as a black line along the surface of the right dome of the diaphragm. This is an extensive pneumomediastinum. Several mechanisms could explain the presence of this mediastinal air—e.g. a traumatic pneumothorax or a tear through the trachea, bronchus or oesophagus. In this patient the air had arisen from a tear of the lung parenchyma with subsequent dissection through the interstitial tissues, thence to the hilum, and out into the mediastinum.
QUESTION 4—IS THERE AN AORTIC RUPTURE?
CXR APPEARANCE
In most cases of aortic rupture the mediastinum or aortic contour will appear widened. The following CXR features are very suggestive of an aortic injury2,3,10,11:
Major arterial injury
A completely normal mediastinal contour on the sitting-up CXR will exclude the diagnosis of a major arterial injury2. The following signs are of modest value in hinting at a definite arterial injury. Their importance lies in alerting the physician that a major abnormality might, just possibly, have occurred…but their positive predictive value is low2.
Mediastinal widening
Mediastinal widening is not necessarily bad news. In approximately 80% of trauma patients with true mediastinal widening—this is not due to aortic rupture. The widening is due to bleeding from small arteries and small veins.
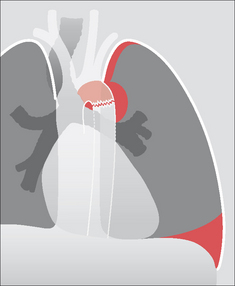
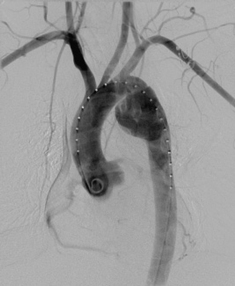
Figure 32.10 Deceleration injury. Aortic rupture at the isthmus. The haematoma has widened the mediastinum, extended over the apex of the left lung, and it has also displaced the trachea to the right. Some blood has leaked into the left pleural space.
QUESTION 5—IS THERE A TRACHEO-BRONCHIAL RUPTURE?
These injuries result from very violent trauma—usually a deceleration force applied to the anterior chest wall. An injury to the great vessels or an intracranial injury are recognised associations of tracheal or bronchial rupture.
CXR features4,12 suggesting a tear of a main airway (transection or rupture):
QUESTION 6—IS THERE LUNG CONTUSION?
Contusion is very common following a violent injury. It appears as an area of consolidation, similar in appearance to lobar pneumonia.
QUESTION 7—IS THERE AN INJURY TO THE HEART?
The sternum and thoracic spine protect the heart and pericardium from non-penetrating injuries. The demonstration of anterior rib fractures or a sternal fracture should always raise the possibility—not the probability—of a myocardial injury. The CXR is usually unhelpful in excluding the possibility of pericardial or myocardial damage. Echocardiography provides a much more sensitive evaluation.
QUESTION 8—IS THE DIAPHRAGM NORMAL?14-17
Rupture of a dome of the diaphragm occurs in approximately 5% of cases of severe thoracic trauma14,16. A rupture is more common with blunt trauma than with a penetrating injury. The mechanism of injury is usually a sudden rise of intra-abdominal pressure from violent compression to the abdomen or lower thorax1.
A rupture may affect either dome. The left dome is more commonly involved14—in the ratio of 4:1. A few cases are bilateral. In 50% or more of cases herniation of abdominal viscera through the rupture is delayed14. Delay may be two or more years after the injury and results from a small tear subsequently increasing in size.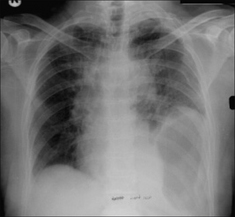
Figure 32.17 Male. Age 35. RTA. Widened mediastinum (due to a haematoma from ruptured veins). Multiple rib fractures. Seemingly high left dome of the diaphragm with the stomach gas bubble also unusually high. Diaphragmatic rupture with herniation of part of the stomach into the thorax.
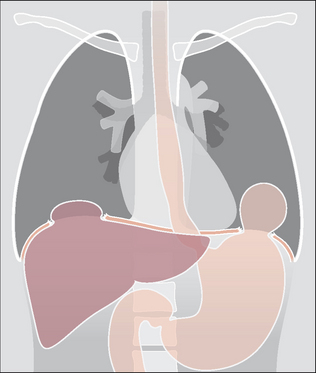
Figure 32.18 Rupture of both the right and left domes of the diaphragm. The diaphragm is injured in approximately 5% of severe thoracic injuries14,16 and 22% of all thoraco-abdominal injuries3. Some 33% of these injuries are diagnosed three years after the trauma…sometimes because the abnormal CXR features were previously overlooked3. The most common site of injury is at the apex of the left dome.
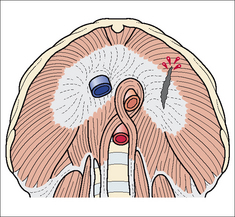
Figure 32.16 The diaphragm viewed from below. Sagittal rupture through the central tendon and muscular part of the left dome from an antero-posterior compressive force. The tendon has a relatively poor blood supply and when ruptured it heals slowly and less effectively than the surrounding muscle.
1. Schnyder P, Wintermark M. Radiology of Blunt Trauma of the Chest. Berlin: Springer-Verlag, 2000.
2. Mirvis SE, Templeton PA. Imaging in acute thoracic trauma. Semin Roentgenol. 1992;27:184-210.
3. Besson A, Saegesser F. A colour atlas of chest trauma and associated injuries. London: Wolfe Medical Publications, 1982.
4. Collins J, Stern EJ. Chest Radiology: The Essentials. Philadelphia, PA: Lippincott, Williams and Wilkins, 1999.
5. Groskin SA. Selected topics in chest trauma. Radiology. 1992;183:605-617.
6. Goodman LR, Putman CE. The SICU chest radiograph after massive blunt trauma. Radiol Clin North Am. 1981;19:111-123.
7. Woodring JH, Fried AM, Hatfield DR, et al. Fractures of first and second ribs. Predictive value for arterial and bronchial injury. AJR. 1982;138:211-215.
8. Gupta A, Jamshidi M, Rubin JR. Traumatic first rib fracture: is angiography necessary? A review of 730 cases. Cardiovasc Surg. 1997;5:48-53.
9. Ontell FK, Moore EH, Shepard JA, et al. The costal cartilages in health and disease. Radiographics. 1997;17:571-577.
10. Cowley RA, Turney SZ, Hankins JR, et al. Rupture of thoracic aorta caused by blunt trauma: a fifteen year experience. J Thorac and Cardiovasc Surg. 1990;100:652-660.
11. Mirvis SE, Bidwell JK, Buddemeyer EU, et al. Value of chest radiography in excluding traumatic aortic rupture. Radiology. 1987;163:487-493.
12. Kelly JP, Webb WR, Moulder PV, et al. Management of airway trauma. (1) Tracheobronchial injuries. Ann Thorac Surg. 1985;40:551-555.
13. Greene R. Lung alterations in thoracic trauma. J Thorac Imaging. 1987;2:1-11.
14. Eren S, Kantarci M, Okur A. Imaging of diaphragmatic rupture after trauma. Clin Radiol. 2006;61:467-477.
15. Iochum S, Ludig T, Walter F, et al. Imaging of diaphragmatic injury: a diagnostic challenge? Radiographics. 2002;22:103-116.
16. Nursal TZ, Ugurlu M, Kologlu M, et al. Traumatic diaphragmatic hernias; a report of 26 cases. Hernia. 2001;5:25-29.
17. Gelman R, Mirvis SE, Gens D. Diaphragm rupture due to blunt trauma: sensitivity of chest radiographs. AJR. 1991;156:51-57.
18. Chan O, Wilson A, Walsh M. ABC of emergency radiology: major trauma. BMJ. 2005;330:1136-1138.