Chapter 523 Renal Tubular Acidosis
Renal tubular acidosis (RTA) is a disease state characterized by a normal anion gap (hyperchloremic) metabolic acidosis in the setting of normal or near-normal glomerular filtration rate. There are 4 main types: proximal (type II) RTA, classic distal (type I) RTA, hyperkalemic (type IV) RTA, and combined proximal and distal (type III). Proximal RTA results from impaired bicarbonate reabsorption and distal RTA from failure to secrete acid. Either of these defects may be inherited and persistent from birth or acquired, as is seen more commonly in clinical practice.
Normal Urinary Acidification
Kidneys contribute to acid-base balance by reabsorption of filtered bicarbonate (HCO3−) and excretion of hydrogen ion (H+) produced every day. Hydrogen ion secretion from tubule cells into the lumen is key in the reabsorption of HCO3−, formation of titratable acidity (H+ bound to buffers such as HPO42−), and formation of ammonium ions (NH4+). Because loss of filtered HCO3− is equivalent to addition of H+ to the body, all filtered bicarbonate should be absorbed before dietary H+ can be excreted. About 90% of filtered bicarbonate is absorbed in the proximal tubule and the remaining 10% in the distal segments, mostly thick ascending limb and outer medullary collecting tubule (CT) (Fig. 523-1). In the proximal tubule and thick ascending limb of the loop of Henle (TAL) H+ from water is secreted by the Na+-H+ exchanger on the luminal membrane. H+ combines with filtered bicarbonate resulting in the formation of H2CO3, which splits into water and CO2 in the presence of carbonic anhydrase (CA) IV. CO2 diffuses freely back into the cell, combines with OH− (from H2O) to form HCO3− in the presence of CA II, and returns to systemic circulation via the Na+-3HCO3− cotransporter situated at the basolateral membrane of the cell. In the CT, H+ is secreted into lumen by H+ATPase (adenosine triphosphatase) and H-CO3− is returned to systemic circulation by HCO3–-Cl− exchanger located on the basolateral membrane. The H+ secreted proximally and distally in excess of the filtered HCO3− is excreted in the urine either as titratable acid or as NH4+.
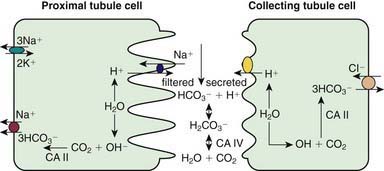
Figure 523-1 Major cellular luminal events in acid-base regulation in the proximal and the collecting tubule cells. In the proximal tubule, H+, split from H2O, is secreted into the lumen via Na+/H+ exchanger, and HCO3−, formed by combination of OH− (split from H2O) with CO2 in the presence of carbonic anhydrase (CA) II, is returned to the systemic circulation by a Na+-3HCO3− cotransporter. Similarly, in the collecting tubule, H+ is secreted into the lumen by an active H+-ATPase (adenosine triphosphatase), and HCO3− is returned to the systemic circulation via a HCO3−-Cl− exchanger. H+ secreted into the lumen combines with filtered HCO3− to form carbonic acid (H2CO3) and then CO2 and H2O in the presence of CA IV, which can be passively reabsorbed.
(Modified from Rose BD, Post TW: Clinical physiology of acid-base and electrolyte disorders, ed 5, New York, 2001, McGraw-Hill.)
523.1 Proximal (Type II) Renal Tubular Acidosis
Rajasree Sreedharan and Ellis D. Avner
Pathogenesis
Proximal RTA can be inherited and persistent from birth or occur as a transient phenomenon during infancy. Although rare, it may be primary and isolated. Proximal RTA usually occurs as a component of global proximal tubular dysfunction or Fanconi syndrome, which is characterized by low molecular weight proteinuria, glycosuria, phosphaturia, aminoaciduria, and proximal RTA. The causes of proximal RTA and Fanconi syndrome are outlined in Table 523-1. Many of these causes are inherited disorders. In addition to cystinosis and Lowe syndrome, autosomal recessive and dominant pRTA are addressed further in this section. Other inherited forms of Fanconi syndrome include galactosemia (Chapter 81.2), hereditary fructose intolerance (Chapter 81.3), tyrosinemia (Chapter 79.2), and Wilson disease (Chapter 349.2). Dent disease, or X-linked nephrolithiasis, is discussed in Chapter 525.3. In children, an important form of secondary Fanconi syndrome is exposure to ifosfamide, a component of many treatment regimens for Wilms tumor and other solid tumors.
Table 523-1 COMMON CAUSES OF RENAL TUBULAR ACIDOSIS
PROXIMAL RENAL TUBULAR ACIDOSIS
Primary
Secondary
DISTAL RENAL TUBULAR ACIDOSIS
Primary
Secondary
HYPERKALEMIC RENAL TUBULAR ACIDOSIS
Primary
Secondary
Autosomal Recessive Disease
Isolated autosomal recessive pRTA is caused by mutations in the gene encoding the sodium bicarbonate cotransporter NBC1. It manifests with ocular abnormalities (band keratopathy, cataracts, and glaucoma, often leading to blindness), short stature, enamel defects of the teeth, intellectual impairment, and occasionally basal ganglia calcification along with pRTA. Autosomal dominant pattern of inheritance has been identified in a single pedigree with nine members presenting with hyperchloremic metabolic acidosis, normal ability to acidify urine, normal renal function, and growth retardation.
Cystinosis
Cystinosis is a systemic disease caused by a defect in the metabolism of cystine, which results in accumulation of cystine crystals in most of the major organs of the body, notably the kidney, liver, eye, and brain. It occurs at an incidence of 1 : 100,000-1 : 200,000. In certain populations, such as French Canadians, the incidence is much higher. At least 3 clinical patterns have been described. Young children with the most severe form of the disease (infantile or nephropathic cystinosis) present in the first 2yr of life with severe tubular dysfunction and growth failure. If the disease is not treated, the children develop end-stage renal disease by the end of their 1st decade. A milder form of the disease manifests in adolescents and is characterized by less-severe tubular abnormalities and a slower progression to renal failure. A benign adult form with no renal involvement also exists.
Cystinosis is caused by mutations in the CTNS gene, which encodes a novel protein, cystinosin. Cystinosin is thought to be an H+-driven lysosomal cystine transporter. Genotype-phenotype studies demonstrate that patients with severe nephropathic cystinosis carry mutations that lead to complete loss of cystinosin function. Patients with milder clinical disease have mutations that lead to expression of partially functional protein. Patients with nephropathic cystinosis present with clinical manifestations reflecting their pronounced tubular dysfunction and Fanconi syndrome, including polyuria and polydipsia, growth failure, and rickets. Fever, caused by dehydration or diminished sweat production, is common. Patients are typically fair skinned and blond because of diminished pigmentation. Ocular presentations include photophobia, retinopathy, and impaired visual acuity. Patients also can develop hypothyroidism, hepatosplenomegaly, and delayed sexual maturation. With progressive tubulointerstitial fibrosis, renal insufficiency is invariant.
The diagnosis of cystinosis is suggested by the detection of cystine crystals in the cornea and confirmed by measurement of increased leukocyte cystine content. Prenatal testing is available for at-risk families.
Treatment of cystinosis is directed at correcting the metabolic abnormalities associated with Fanconi syndrome or chronic renal failure. In addition, specific therapy is available with cysteamine, which binds to cystine and converts it to cysteine. This facilitates lysosomal transport and decreases tissue cystine. Oral cysteamine does not achieve adequate levels in ocular tissues, so additional therapy with cysteamine eyedrops is required. Early initiation of the drug can prevent or delay deterioration of renal function. Patients with growth failure that does not improve with cysteamine might benefit from treatment with growth hormone. Kidney transplantation is a viable option in patients with renal failure. With prolonged survival, additional complications may become evident, including central nervous system abnormalities, muscle weakness, swallowing dysfunction, and pancreatic insufficiency. It is unclear whether long-term cysteamine therapy decreases these complications.
Lowe Syndrome
Lowe syndrome (oculocerebrorenal syndrome of Lowe) is a rare X-linked disorder characterized by congenital cataracts, mental retardation, and Fanconi syndrome. The disease is caused by mutations in the OCRL1 gene, which encodes the phosphatidylinositol polyphosphate 5-phosphatase protein. The abnormalities seen in Lowe syndrome are thought to be due to abnormal transport of vesicles within the Golgi apparatus. Kidneys show nonspecific tubulointerstitial changes. Thickening of glomerular basement membrane and changes in proximal tubule mitochondria are also seen.
Patients with Lowe syndrome typically present in infancy with cataracts, progressive growth failure, hypotonia, and Fanconi syndrome. Significant proteinuria is common. Blindness and renal insufficiency often develop. Characteristic behavioral abnormalities are also seen, including tantrums, stubbornness, stereotypy (repetitive behaviors), and obsessions. There is no specific therapy for the renal disease or neurologic deficits. Cataract removal is generally required.
Clinical Manifestations of Proximal RTA and Fanconi Syndrome
Patients with isolated, sporadic, or inherited proximal RTA present with growth failure in the 1st year of life. Additional symptoms can include polyuria, dehydration (due to sodium loss), anorexia, vomiting, constipation, and hypotonia. Patients with primary Fanconi syndrome have additional symptoms, secondary to phosphate wasting, such as rickets. Those with systemic diseases present with additional signs and symptoms specific to their underlying disease. A non–anion gap metabolic acidosis is present. Urinalysis in patients with isolated proximal RTA is generally unremarkable. The urine pH is acidic (<5.5) because distal acidification mechanisms are intact in these patients. Urinary indices in patients with Fanconi syndrome demonstrate varying degrees of phosphaturia, aminoaciduria, glycosuria, uricosuria, and elevated urinary sodium or potassium. Depending on the nature of the underlying disorder, laboratory evidence of chronic renal insufficiency, including elevated serum creatinine, may be present.
523.2 Distal (Type I) Renal Tubular Acidosis
Rajasree Sreedharan and Ellis D. Avner
Pathogenesis
As with proximal RTA, distal RTA can be sporadic or inherited. It can also occur as a complication of inherited or acquired diseases of the distal tubules. Primary or secondary causes of distal RTA can result in damaged or impaired functioning of one or more transporters or proteins involved in the acidification process, including the H+/ATPase, the HCO3−/Cl− anion exchangers, or the components of the aldosterone pathway. Because of impaired hydrogen ion excretion, urine pH cannot be reduced to <5.5, despite the presence of severe metabolic acidosis. Loss of sodium bicarbonate distally, owing to lack of H+ to bind to in the tubular lumen (see Fig. 523-1), results in increased chloride absorption and hyperchloremia. Inability to secrete H+ is compensated by increased K+ secretion distally, leading to hypokalemia. Hypercalciuria is usually present and can lead to nephrocalcinosis or nephrolithiasis. Chronic metabolic acidosis also impairs urinary citrate excretion. Hypocitraturia further increases the risk of calcium deposition in the tubules. Bone disease is common, resulting from mobilization of organic components from bone to serve as buffers to chronic acidosis.
Clinical Manifestations
Distal RTA shares features with those of proximal RTA, including non–anion gap metabolic acidosis and growth failure. However, distinguishing features of distal RTA include nephrocalcinosis and hypercalciuria. The phosphate and massive bicarbonate wasting characteristic of proximal RTA is generally absent.
Causes of primary and secondary distal RTA are listed in Table 523-1. Although inherited forms are rare, 3 specific inherited forms of distal RTA have been identified, including an autosomal recessive form associated with sensorineural deafness.
Medullary sponge kidney is a relatively rare sporadic disorder in children, although not uncommon in adults. It is characterized by cystic dilatation of the terminal portions of the collecting ducts as they enter the renal pyramids. Ultrasonographically, patients often have medullary nephrocalcinosis. Although patients with this condition typically maintain normal renal function through adulthood, complications include nephrolithiasis, pyelonephritis, hyposthenuria (inability to concentrate urine), and distal RTA. Associations of medullary sponge kidney with Beckwith-Wiedemann syndrome or hemihypertrophy have been reported.
523.3 Hyperkalemic (Type IV) Renal Tubular Acidosis
Rajasree Sreedharan and Ellis D. Avner
Pathogenesis
Type IV RTA occurs as the result of impaired aldosterone production (hypoaldosteronism) or impaired renal responsiveness to aldosterone (pseudohypoaldosteronism). Acidosis results because aldosterone has a direct effect on the H+/ATPase responsible for hydrogen secretion. In addition, aldosterone is a potent stimulant for potassium secretion in the collecting tubule; consequently, lack of aldosterone results in hyperkalemia. This further affects acid-base status by inhibiting ammoniagenesis and, thus, H+ excretion. Aldosterone deficiency typically occurs as a result of adrenal gland disorders such as Addison disease or some forms of congenital adrenal hyperplasia. In children, aldosterone unresponsiveness is a more common cause of type IV RTA. This can occur transiently, during an episode of acute pyelonephritis or acute urinary obstruction, or chronically, particularly in infants and children with a history of obstructive uropathy. The latter patients can have significant hyperkalemia, even in instances when renal function is normal or only mildly impaired. Rare examples of inherited forms of type IV RTA have been identified.
Clinical Manifestations
Patients with type IV RTA, like those with type I and II RTA, can present with growth failure in the first few years of life. Polyuria and dehydration (from salt wasting) are common. Rarely, patients (especially those with pseudohypoaldosteronism type 1) present with life-threatening hyperkalemia. Patients with obstructive uropathies can present acutely with signs and symptoms of pyelonephritis, such as fever, vomiting, and foul-smelling urine. Laboratory tests reveal a hyperkalemic non–anion gap metabolic acidosis. Urine may be alkaline or acidic. Elevated urinary sodium levels with inappropriately low urinary potassium levels reflect the absence of aldosterone effect.
Diagnostic Approach
The first step in the evaluation of a patient with suspected RTA is to confirm the presence of a normal anion gap metabolic acidosis, identify electrolyte abnormalities, assess renal function, and rule out other causes of bicarbonate loss such as diarrhea (Chapter 52). Metabolic acidosis associated with diarrheal dehydration is extremely common, and acidosis generally improves with correction of volume depletion. Patients with protracted diarrhea can deplete their total-body bicarbonate stores and can have persistent acidosis despite apparent restoration of volume status. In instances where a patient has a recent history of severe diarrhea, full evaluation for RTA should be delayed for several days to permit adequate time for reconstitution of total-body bicarbonate stores. If acidosis persists beyond a few days in this setting, additional studies are indicated.
Serum electrolytes, blood urea nitrogen, calcium, phosphorus, creatinine, and pH should be obtained by venous puncture. Traumatic blood draws (such as heel stick specimens), small volumes of blood in “adult-size” specimen collection tubes, or prolonged specimen transport time at room temperature can lead to falsely low bicarbonate levels, often in association with an elevated serum potassium value. True hyperkalemic acidosis is consistent with type IV RTA, whereas the finding of normal or low potassium suggests type I or II. The blood anion gap should be calculated using the formula [Na+] − [Cl− + HCO3−]. Values of <12 demonstrate the absence of an anion gap. Values of >20 are highly suggestive of the presence of an anion gap. If such an anion gap is found, then other diagnoses (lactic acidosis, inborn errors of metabolism, ingested toxins) should be investigated. If tachypnea is noted, evaluation of an arterial blood gas might help to rule out the possibility of a mixed acid-base disorder primarily involving respiratory and metabolic components. A detailed history, with particular attention to growth and development, recent or recurrent diarrheal illnesses, and family history of mental retardation, failure to thrive, end-stage renal disease, infant deaths, or miscarriages is essential. Physical examination should determine growth parameters and volume status as well as the presence of any dysmorphic features suggesting an underlying syndrome.
Once the presence of a non–anion gap metabolic acidosis is confirmed, urine pH can help distinguish distal from proximal causes. A urine pH <5.5 in the presence of acidosis suggests proximal RTA, whereas patients with distal RTA typically have a urine pH >6.0. The urine anion gap ([urine Na+ + urine K+] − urine Cl−) is sometimes calculated to confirm the diagnosis of distal RTA. A positive gap suggests a deficiency of ammoniagenesis and, thus, the possibility of a distal RTA. A negative gap is consistent with proximal tubule bicarbonate wasting (gastrointestinal bicarbonate wasting). A urinalysis should also be obtained to determine the presence of glycosuria, proteinuria, or hematuria, suggesting more global tubular damage or dysfunction. Random or 24-hr urine calcium and creatinine measurements will identify hypercalciuria. Renal ultrasonography should be performed to identify underlying structural abnormalities such as obstructive uropathies as well as to determine the presence of nephrocalcinosis (Fig. 523-2).

Treatment and Prognosis
The mainstay of therapy in all forms of RTA is bicarbonate replacement. Patients with proximal RTA often require large quantities of bicarbonate, up to 20 mEq/kg/24 hr in the form of sodium bicarbonate or sodium citrate solution (Bicitra or Shohl’s solution). The base requirement for distal RTAs is generally in the range of 2-4 mEq/kg/24 hr, although patients’ requirements can vary. Patients with Fanconi syndrome usually require phosphate supplementation. Patients with distal RTA should be monitored for the development of hypercalciuria. Those with symptomatic hypercalciuria (recurrent episodes of gross hematuria), nephrocalcinosis, or nephrolithiasis can require thiazide diuretics to decrease urine calcium excretion. Patients with type IV RTA can require chronic treatment for hyperkalemia with sodium-potassium exchange resin (Kayexalate).
Prognosis depends to a large part on the nature of any underlying disease. Patients with treated isolated proximal or distal RTA generally demonstrate improvement in growth, provided serum bicarbonate levels can be maintained in the normal range. Patients with systemic illness and Fanconi syndrome can have ongoing morbidity with growth failure, rickets, and signs and symptoms related to their underlying disease.
523.4 Rickets Associated with Renal Tubular Acidosis
Rickets may be present in primary RTA, particularly in type II or proximal RTA. Hypophosphatemia and phosphaturia are common in the renal tubular acidoses, which are also characterized by hyperchloremic metabolic acidosis, various degrees of bicarbonaturia, and, often, hypercalciuria and hyperkaluria. Bone demineralization without overt rickets usually is detected in type I and distal RTA. This metabolic bone disease may be characterized by bone pain, growth retardation, osteopenia, and, occasionally, pathologic fractures. Although acute metabolic acidosis in vitamin D–deficient animals can impair the conversion of 25-hydroxyvitamin D (25[OH]D) to 1,25-dihydroxyvitamin D (1,25[OH]2D), resulting in reduced levels of this active metabolite, the circulating levels of 1,25(OH)2D in patients with either type of RTA are normal. If patients with RTA have chronic renal insufficiency, serum 1,25(OH)2D levels are reduced in relation to the degree of renal impairment.
Bone demineralization in distal RTA probably relates to dissolution of bone because the calcium carbonate in bone serves as a buffer against the metabolic acidosis due to the hydrogen ions retained by patients with RTA.
Administration of sufficient bicarbonate to reverse acidosis reverses bone dissolution and the hypercalciuria that is common in distal RTA. Proximal RTA is treated with both bicarbonate and oral phosphate supplements to heal rickets. Doses of phosphate similar to those used in familial hypophosphatemia or Fanconi syndrome may be indicated. Vitamin D is required to offset the secondary hyperparathyroidism that complicates oral phosphate therapy. Following therapy, growth in patients with type II (proximal) RTA is greater than in patients with primary Fanconi syndrome.
Alper SL. Genetic diseases of acid-base transporters. Annu Rev Physiol. 2002;64:899-923.
Chan JCM, Scheinman JI, Roth KS. Renal tubular acidosis. Pediatr Rev. 2001;22:277-286.
Fry AC, Karet FE. Inherited renal acidoses. Physiology. 2007;22:202-211.
Fulop M, Mackay M. Renal tubular acidosis, Sjögren syndrome, and bone disease. Arch Intern Med. 2004;164:905-909.
Gahl WA. Cystinosis. In: Avner ED, Harmon WE, Niaudet P, et al, editors. Pediatric nephrology. ed 6. Heidelberg, Germany: Springer-Verlag; 2009:1019-1038.
Gahl WA. Early oral cysteamine therapy for nephropathic cystinosis. Eur J Pediatr. 2003;162(Suppl 1):S38-S41.
Hsu SY, Tsai IJ, Tsau YK. Comparison of growth in primary Fanconi syndrome and proximal renal tubular acidosis. Pediatr Nephrol. 2005;20:460.
Igarashi T. Fanconi syndrome. In: Avner ED, Harmon WE, Niaudet P, et al, editors. Pediatric nephrology. ed 6. Heidelberg, Germany: Springer-Verlag; 2009:1039-1068.
Izzedine H, Launay-Vacher V, Isnard-Bagnis C, et al. Drug-induced Fanconi’s syndrome. Am J Kidney Dis. 2003;41:292-309.
Kalatzis V, Antignac C. New aspects of the pathogenesis of cystinosis. Pediatr Nephrol. 2003;18:207-215.
Magen D, Berger L, Coady MJ, et al. A loss-of-function mutation in NaPi-IIa and renal Fanconi’s syndrome. N Engl J Med. 2010;362(12):1102-1108.
Nicoletta JA, Schwartz GJ. Distal renal tubular acidosis. Curr Opin Pediatr. 2004;16:194-198.
Pongchaiyakul C, Domrongkitchaiporn S, Stichantrakul W, et al. Incomplete renal tubular acidosis and bone mineral density: a population survey in a area of endemic renal tubular acidosis. Nephrol Dial Transplant. 2004:3029-3033.
Prie D, Friedlander G. Genetic disorders of renal phosphate transport. N Engl J Med. 2010;362:2399-2409.
Quigley R. Renal tubular acidosis. In: Avner ED, Harmon WE, Niaudet P, et al, editors. Pediatric nephrology. ed 6. Heidelberg, Germany: Springer-Verlag; 2009:979-1004.
Rodriguez-Soriano J. New insights into the pathogenesis of renal tubular acidosis—from functional to molecular studies. Pediatr Nephrol. 2000;14:1121-1136.
Rose BD, Post TW. Regulation of acid-base balance. In Clinical physiology of acid-base and electrolyte disorders, ed 5, New York: McGraw-Hill; 2001:325-371.
Wappner RS. Lowe syndrome. In GeneClinics: Clinical Genetic Information Resource (database online), http://www.geneclinics.org/.
Wuhl E, Haffner D, Offner G, et al. Long-term treatment with growth hormone in short children with nephropathic cystinosis. J Pediatr. 2001;138:880-887.