Chapter 666 The Foot and Toes
The foot may be divided into the forefoot (toes and metatarsals), the midfoot (cuneiforms, navicular, cuboid), and the hindfoot (talus and calcaneus). Although the tibiotalar joint (ankle) provides plantar flexion and dorsiflexion, the subtalar joint (between the talus and calcaneus) is oriented obliquely, providing inversion and eversion. Inversion represents a combination of plantar flexion and varus, and eversion involves dorsiflexion and valgus. The subtalar joint is especially important for walking on uneven surfaces. The talonavicular and calcaneocuboid joints connect the midfoot with the hindfoot.
Abnormalities affecting the osseous and articular structures of the foot may be congenital, developmental, neuromuscular, or inflammatory. Problems with the foot and/or toes may be associated with a host of connective tissue diseases and syndromes such as overuse syndromes, which are commonly observed in young athletes. Symptoms can include pain and abnormal shoe wear; cosmetic concerns are common.
666.1 Metatarsus Adductus
Metatarsus adductus is common in newborns and involves adduction of the forefoot relative to the hindfoot. When the forefoot is supinated and adducted, the deformity is termed metatarsus varus (Fig. 666-1). The most common cause is intrauterine molding, where the deformity is bilateral in 50% of cases. As with other intrauterine positional foot deformities, a careful hip examination should always be performed.

Clinical Manifestations
The forefoot is adducted (occasionally supinated), whereas the midfoot and hindfoot are normal. The lateral border of the foot is convex, and the base of the 5th metatarsal appears prominent. Range of motion at the ankle and subtalar joints is normal. Both the magnitude and the degree of flexibility should be documented. When the foot is viewed from the plantar surface, a line through the midpoint of (and parallel to) the heel should normally extend through the 2nd toe. Flexibility is assessed by stabilizing the hindfoot and midfoot in a neutral position with one hand and applying pressure over the 1st metatarsal head with the other. In the walking child with an uncorrected metatarsus adductus deformity, an in-toe gait and abnormal shoe wear can occur. A subset of patients also have a dynamic adduction deformity of the great toe (hallux varus), which is often most noticeable during ambulation. This usually improves spontaneously and does not require treatment.
Radiographic Evaluation
Radiographs are not performed routinely, but an anteroposterior (AP) and lateral weight-bearing or simulated weight-bearing radiographs are indicated in toddlers or older children with residual deformities. The AP radiographs demonstrate adduction of the metatarsals at the tarsometatarsal articulation and an increased intermetatarsal angle between the 1st and 2nd metatarsals.
Treatment
The treatment of metatarsus adductus is based on the rigidity of the deformity; most children respond to nonoperative treatment. Deformities that are flexible and overcorrect into abduction with passive manipulation may be observed. The feet that correct just to a neutral position can benefit from stretching exercises and retention in a slightly overcorrected position by a splint or reverse-last shoes. These are worn full time (22 hr/day), and the condition is re-evaluated in 4-6 wk. If improvement occurs, treatment can be continued. If there is no improvement, serial plaster casts should be considered. When stretching a foot with metatarsus adductus, care should be taken to maintain the hindfoot in neutral to slight varus alignment to avoid creating hindfoot valgus. Feet that cannot be corrected to a neutral position might benefit from serial casting; the best results are obtained when treatment is started before 8 mo of age. In addition to stretching the soft tissues, the goal is to alter physeal growth and stimulate remodeling, resulting in permanent correction. Once flexibility and alignment are restored, orthoses or corrective shoes are generally recommended for an additional period. A dynamic hallux varus usually improves spontaneously, and no active treatment is required.
Surgical treatment may be considered in the small subset of patients with symptomatic residual deformities that have not responded to previous treatment. Surgery is generally delayed until children are 4-6 yr of age. Cosmesis is often a concern, and pain and/or the inability to wear certain types of shoes occasionally leads patients to consider surgery. Options for surgical treatment include either soft-tissue release or osteotomy. An osteotomy (midfoot or multiple metatarsals) is most likely to result in permanent restoration of alignment.
666.2 Calcaneovalgus Feet
Harish S. Hosalkar, David A. Spiegel, and Richard S. Davidson
The calcaneovalgus foot is common in the newborn (30-50% of newborns have a mild version) and is secondary to in utero positioning. Excessive dorsiflexion and eversion are observed in the hindfoot, and the forefoot may be abducted. An associated external tibial torsion may be present.
Clinical Manifestations
The infant typically presents with the foot dorsiflexed and everted, and occasionally the dorsum is in contact with the anterolateral surface of the lower leg. Plantar flexion and inversion are often restricted. As with other intrauterine positional deformities, a careful hip examination should be performed; if there is any concern, hip ultrasonography should be considered. The calcaneovalgus foot may be confused with a congenital vertical talus and is rarely associated with a posteromedial bow of the tibia. A calcaneovalgus deformity may also be seen in older patients, typically those with a neuromuscular imbalance involving weakness or paralysis of the gastrocnemius-soleus complex (polio, myelomeningocele).
Radiographic Evaluation
Radiographs are usually not required, but they should be ordered if the deformity fails to correct spontaneously or with early treatment. AP and lateral radiographs, with a lateral radiograph of the foot in maximal plantar flexion, might help distinguish calcaneovalgus from a vertical talus. If a posteromedial bow of the tibia is suspected, anteroposterior and lateral radiographs of the tibia and fibula are necessary.
Treatment
Mild cases of calcaneovalgus foot, in which full passive range of motion is present at birth, require no active treatment. These usually resolve within the 1st weeks of life. A gentle stretching program, focusing on plantar flexion and inversion, is recommended for cases with some restriction in motion. For cases with a greater restriction in mobility, serial casts may be considered to restore motion and alignment. Casting is rarely required in the treatment of calcaneovalgus feet. The management for cases associated with a posteromedial bow of the tibia is similar.
666.3 Talipes Equinovarus (Clubfoot)
Talipes equinovarus (also known as clubfoot) describes a deformity involving malalignment of the calcaneotalar-navicular complex. Components of this deformity may be best understood using the mnemonic CAVE (cavus, adductus, varus, equinus). Although this is predominantly a hindfoot deformity, there are plantar flexion (cavus) of the 1st ray and adduction of the forefoot/midfoot on the hindfoot. The hindfoot is in varus and equinus. The clubfoot deformity may be positional, congenital, or associated with a variety of underlying diagnoses (neuromuscular or syndromic).
The positional clubfoot is a normal foot that has been held in a deformed position in utero and is found to be flexible on examination in the newborn nursery. The congenital clubfoot involves a spectrum of severity, while clubfoot associated with neuromuscular diagnoses or syndromes are typically rigid and more difficult to treat. Clubfoot is extremely common in patients with myelodysplasia and arthrogryposis (Chapter 674).
Congenital clubfoot is seen in approximately 1/1,000 births. Although numerous theories have been proposed, the etiology is multifactorial and likely involves the effects of environmental factors in a genetically susceptible host. The risk is approximately 1 in 4 when both a parent and one sibling have clubfeet. It occurs more commonly in males (2 : 1) and is bilateral in 50% of cases. The pathoanatomy involves both abnormal tarsal morphology (plantar and medial deviation of the head and neck of the talus) and abnormal relationships between the tarsal bones in all three planes, as well as associated contracture of the soft tissues on the plantar and medial aspects of the foot.
Clinical Manifestations
A complete physical examination should be performed to rule out coexisting musculoskeletal and neuromuscular problems. The spine should be inspected for signs of occult dysraphism. Examination of the infant clubfoot demonstrates forefoot cavus and adductus and hindfoot varus and equinus (Fig. 666-2). The degree of flexibility varies, and all patients exhibit calf atrophy. Both internal tibial torsion and leg-length discrepancy (shortening of the ipsilateral extremity) are observed in a subset of cases.

Radiographic Evaluation
Anteroposterior and lateral radiographs are recommended, often with the foot held in the maximally corrected position. Multiple radiographic measurements can be made to describe malalignment between the tarsal bones. The navicular bone does not ossify until 3-6 yr of age, so the focus of radiographic interpretation is the relationships between segments of the foot. A common radiographic finding is “parallelism” between lines drawn through the axis of the talus and the calcaneus on the lateral radiograph, indicating hindfoot varus. Many clinicians believe that radiographs are not required in the evaluation and treatment of clubfoot in infancy and reserve these studies for older children with persistent or recurrent deformities.
Treatment
Nonoperative treatment is initiated in all infants and should be started as soon as possible following birth. Techniques have included taping and strapping, manipulation and serial casting, and functional treatment. Historically, a significant percentage of patients treated by manipulation and casting required a surgical release, which was usually performed between 3 and 12 mo of age. Although many feet remain well aligned after surgical releases, a significant percentage of patients have required additional surgery for recurrent or residual deformities. Stiffness remains a concern at long-term follow-up. Pain is uncommon in childhood and adolescence, but symptoms can appear during adulthood. These concerns have led to considerable interest in less-invasive methods for treating the deformity.
The Ponseti method of clubfoot treatment involves a specific technique for manipulation and serial casting and may be best described as minimally invasive rather than nonoperative. The order of correction follows the mnemonic CAVE. Weekly cast changes are performed, and 5 to 10 casts are typically required. The most difficult deformity to correct is the hindfoot equinus, for which ~90% of patients require an outpatient percutaneous tenotomy of the heel cord. Following the tenotomy, a long leg cast with the foot in maximal abduction (70 degrees) and dorsiflexion is worn for 3 wk; the patient then begins a bracing program. An abduction brace is worn full time for 3 mo and then at nighttime for 3-5 yr. A subset of patients require transfer of the tibialis anterior tendon to the middle cuneiform for recurrence. Although most patients require some form of surgery, the procedures are minimal in comparison with a surgical release, which requires capsulotomy of the major joints (and lengthening of the muscles) to reposition the joints in space. The results of the Ponseti method are excellent at up to 40 yr of follow-up. Compliance with the splinting program is essential; recurrence is common if the brace is not worn as recommended. Functional treatment, or the French method, involves daily manipulations (supervised by a physical therapist) and splinting with elastic tape, as well as continuous passive motion (machine required) while the baby sleeps. Although the early results are promising, the method is labor intensive, and it remains unclear whether the technique will achieve greater popularity in the USA. These minimally invasive methods are most successful when treatment is begun at birth or during the first few months of life.
Surgical realignment has a definite role in the management of clubfeet, especially in the minority of congenital clubfeet that have failed nonoperative or minimally invasive methods, and for the neuromuscular and syndromic clubfeet that are characteristically rigid. In such cases, nonoperative methods such as the Ponseti technique are potentially of value in decreasing the magnitude of surgery required. Common surgical approaches include a release of the involved joints (realign the tarsal bones), a lengthening of the shortened posteromedial musculotendinous units, and usually pinning of the foot in the corrected position. The specific procedure is tailored to the unique characteristics of each deformity. For older children with untreated clubfeet or those in whom a recurrence or residual deformity is observed, bony procedures (osteotomies) may be required in addition to soft-tissue surgery. Triple arthrodesis is reserved as salvage for painful, deformed feet in adolescents and adults.
Alvarado DM, Aferol H, McCall K, et al. Familial isolated clubfoot is associated with recurrent chromosome 17q23.1q23.2 microduplications containing TBX4. Am J Hum Genetics. 2010;87:154-160.
Bridgens J, Kiely N. Current management of clubfoot (congenital talipes equinovarus). BMJ. 2010;340:308-312.
Canto MJ, Cano S, Palau J, et al. Prenatal diagnosis of clubfoot in low-risk populations: associated anomalies and long-term outcome. Prenatal Diag. 2008;28:343-346.
Chang CH, Kumar SJ, Riddle EC, et al. Macrodactyly of the foot. J Bone Joint Surg Am. 2002;84:1189-1194.
Dobbs MB, Gurnett CA. Update on clubfoot: etiology and treatment. Clin Orthop Relat Res. 2009;467:1146-1153.
Herzenberg JE, Radler C, Bor N. Ponseti versus traditional methods of casting for idiopathic clubfoot. J Pediatr Orthop. 2002;22:517-521.
Ippolito E, Fraracci L, Farsetti P, et al. The influence of treatment on the pathology of clubfoot. CT study at maturity. J Bone Joint Surg Br. 2004;86:574-580.
Morcuende JA, Dolan LR, Dietz FR, et al. Radical reduction in the rate of extensive corrective surgery for clubfeet using the Ponseti method. Pediatrics. 2004;113:376-380.
Noonan KJ, Richards BS. Nonsurgical management of idiopathic clubfoot. J Am Acad Orthop Surg. 2003;11:392-402.
Offerdal K, Jebens N, Blaas HGK, et al. Prenatal ultrasound detection of talipes equinovarus in a non-selected population of 49 314 deliveries in Norway. Ultrasound Obstet Gynecol. 2007;30:838-844.
Paton RW, Choudry Q. Neonatal foot deformities and their relationship to developmental dysplasia of the hip. J Bone Joint Surg Br. 2009;91:B655-B658.
Roye DPJr, Roye BD. Idiopathic congenital talipes equinovarus. J Am Acad Orthop Surg. 2002;10:239-248.
Sankar WN, Weiss J, Skaggs DL. Orthopaedic conditions in the newborn. J Am Acad Orthop Surg. 2009;17:112-122.
Steinman S, Richards BS, Faulks S, et al. A comparison of two nonoperative methods of idiopathic clubfoot correction: the Ponseti method and the French functional (physiotherapy) method. Surgical technique. Bone Joint Surg Am. 2009;91(Suppl 2):299-312.
666.4 Congenital Vertical Talus
Congenital vertical talus is an uncommon foot deformity in which the midfoot is dorsally dislocated on the hindfoot. Approximately 40% are associated with an underlying neuromuscular condition or a syndrome (Table 666-1); although the remaining 60% had been thought to be idiopathic, there is increasing evidence that some of these may be related to single gene defects. Neurologic causes include myelodysplasia, tethered cord, and sacral agenesis. Other associated conditions include arthrogryposis, Larsen syndrome, and chromosomal abnormalities (trisomy 13-15, 19). Depending on the age at diagnosis, the differential diagnosis might include a calcaneovalgus foot, oblique talus (talonavicular joint reduces passively), flexible flatfoot with a tight Achilles tendon, and tarsal coalition.
Table 666-1 ETIOLOGIES OF CONGENITAL VERTICAL TALUS
CENTRAL NERVOUS SYSTEM AND SPINAL CORD
MUSCLE
CHROMOSOMAL ABNORMALITY
KNOWN GENETIC SYNDROMES
From Alaee F, Boehm S, Dobbs M: A new approach to the treatment of congenital vertical talus, J Child Orthop 1:165–174, 2007.
Clinical Manifestations
Congenital vertical talus has also been described as a rocker-bottom foot (Fig. 666-3) or a Persian slipper foot. The plantar surface of the foot is convex, and the talar head is prominent along the medial border of the midfoot. The fore part of the foot is dorsiflexed (dorsally dislocated on the hindfoot) and abducted relative to the hindfoot, and the hindfoot is in equinus and valgus. There is an associated contracture of the anterolateral (tibialis anterior, toe extensors) and the posterior (Achilles tendon, peroneals) soft tissues. The deformity is typically rigid. A thorough physical examination is required to identify any coexisting neurologic and/or musculoskeletal abnormalities.

Radiographic Evaluation
AP, lateral, and maximal plantar flexion radiographs should be obtained when the diagnosis is suspected. The plantar flexion view helps to determine whether the dorsal subluxation or dislocation of the midfoot on the hindfoot can be reduced passively. Although the navicular does not ossify until 3-6 yr of age, the relationship between the talus and the 1st metatarsal may be evaluated.
Treatment
The initial management consists of serial manipulation and casting, which is started shortly after birth. Initially, an attempt is made to reduce the dorsal dislocation of the forefoot and midfoot on the hindfoot. Once this has been achieved, attention can be directed toward stretching the hindfoot contracture. These deformities are typically rigid, and surgical intervention is required in the majority of cases. In such cases, casting helps to stretch out the contracted soft tissues. Surgery is generally performed between 6 and 12 mo of age; a soft-tissue release is performed as a one- or two-stage procedure. One component involves release and lengthening of the contracted anterior soft tissues in concert with an open reduction of the talonavicular joint, and the other involves a posterior release with lengthening of the contracted musculotendinous units. Fixation with Kirschner wires is commonly performed to maintain alignment. Postoperatively, casting is employed for a variable period; patients often use an orthosis for extended periods, depending on the underlying diagnosis. Salvage options for recurrent or residual deformities in older children include a subtalar or triple arthrodesis.
Alaee F, Boehm S, Dobbs MB. A new approach to the treatment of congenital vertical talus. J Child Orthop. 2007:1165-1174.
Mazzocca AD, Thomson JD, Deluca PA, et al. Comparison of the posterior approach versus the dorsal approach in the treatment of congenital vertical talus. J Pediatr Orthop. 2001;21:212-217.
666.5 Hypermobile Pes Planus (Flexible Flatfeet)
Pes planus (also know as flatfoot) is a common diagnosis, with a prevalence of up to 23%, depending on the diagnostic criteria. Three types of flatfeet may be identified: a flexible flatfoot, a flexible flatfoot with a contracture of the Achilles tendon, and a rigid flatfoot. Flatfoot describes a change in foot shape, and there are several abnormalities in alignment between the tarsal bones. There is eversion of the subtalar complex. The hindfoot is aligned in valgus, and there is midfoot sag at the naviculocuneiform and/or the talonavicular joint. The forefoot is abducted relative to the hindfoot, and the head of the talus is uncovered and prominent along the plantar and medial border of the midfoot and hindfoot. Hypermobile or flexible pes planus is a common source of concern for parents, but these children are rarely symptomatic. Pes planus is common in neonates and toddlers and is associated with physiologic ligamentous laxity. Improvement may be seen when the longitudinal arch develops between 5 and 10 yr of age. Pes planus is less common in societies where shoes are not worn during infancy and childhood. A flexible-sole shoe is recommended. Flexible flatfeet persisting into adolescence and adulthood are usually associated with familial ligamentous laxity and can be identified in other family members.
Clinical Manifestations
Patients typically have a normal longitudinal arch when examined in a non–weight-bearing position, but the arch disappears when standing. The hindfoot collapses into valgus, and the midfoot sag becomes evident. Generalized ligamentous laxity is commonly observed. Range of motion should be assessed at both the subtalar and the ankle joints and will be normal in patients with a flexible flatfoot. When assessing range of motion at the ankle, the foot should always be inverted while testing dorsiflexion. If the foot is neutral or everted, spurious dorsiflexion can occur through the midfoot, masking a contracture of the Achilles tendon. If subtalar motion is restricted, then the foot is not hypermobile or flexible, and other diagnoses such as tarsal coalition and juvenile rheumatoid arthritis must be considered. On occasion, there is tenderness and/or callus formation under the talar head medially. The shoes should be assessed as well and can have evidence of excessive wear along the medial border.
Radiographic Evaluation
Routine radiographs of asymptomatic flexible flatfeet are usually not indicated. Weight-bearing radiographs (AP and lateral) are required to assess the deformity. On the AP radiograph, there is widening of the angle between the longitudinal axis of the talus and the calcaneus, indicating excessive heel valgus. The lateral view shows distortion of the normal straight-line relationship between the long axis of the talus and the 1st metatarsal, with a sag either of the talonavicular or naviculocuneiform joint, resulting in flattening of the normal medial longitudinal arch (Fig. 666-4).

Treatment
The natural history of the flexible pes planus remains unknown, and there is little evidence to suggest that this condition results in long-term problems or disability. Thus, treatment is reserved for the small subset of patients who develop symptoms.
Patients with hindfoot pain or those with abnormal shoe wear might benefit from an orthosis, such as a medial arch support. Severe cases, often associated with an underlying connective tissue disorder such as Ehlers-Danlos syndrome or Down syndrome, might benefit from a custom orthosis such as the UCBL (University of California Biomechanics Laboratory) to better control the hindfoot and prevent collapse of the arch. Although an orthosis can relieve symptoms, there is no evidence for any permanent change in the shape of the foot or alignment of the tarsal bones.
Patients with a flexible flatfoot and a tight Achilles tendon should be treated by stretching exercises, and on occasion, the muscle needs to be lengthened surgically. For the few patients with persistent pain, surgical treatment may be considered.
There has been considerable interest in a lateral column lengthening, which addresses all components of the deformity. The procedure involves an osteotomy of the calcaneus, and a trapezoidal bone graft is placed. A lengthening of the Achilles tendon is required, and a plantar flexion osteotomy of the medial cuneiform is often performed. This procedure preserves the mobility of the hindfoot joints, in contrast to a subtalar or triple arthrodesis. A hindfoot arthrodesis can correct the deformity adequately, but the stress transfer to neighboring joints can result in late-onset, painful degenerative changes. Another option is to insert a spacer into the sinus tarsi to block eversion at the subtalar joint. These procedures may be complicated by synovitis or loosening of the implant.
Evans AM. The flat-footed child—to treat or not to treat: what is the clinician to do? J Am Podiatr Med Assoc. 2008;98:386-393.
Giannini BS, Ceccarelli F, Benedetti MG, et al. Surgical treatment of flexible flatfeet in children: a four-year follow-up study. J Bone Joint Surg Am. 2001;83:78-79.
Lin CJ, Lai KA, Kuan TS, et al. Correlating factors and clinical significance of flexible flatfeet in preschool children. J Pediatr Orthop. 2001;21:378-382.
666.6 Tarsal Coalition
Harish S. Hosalkar, David A. Spiegel, and Richard S. Davidson
Tarsal coalition (also known as peroneal spastic flatfoot) results from a congenital failure of segmentation of the primitive mesenchyme, leading to the union of two or more tarsal bones. The condition is characterized by a painful, rigid flatfoot deformity and peroneal (lateral calf) muscle spasm but without true spasticity. Any condition that alters the normal gliding and rotatory motion of the subtalar joint can produce the clinical appearance of a tarsal coalition. Thus, congenital malformations, arthritis or inflammatory disorders, infection, neoplasms, and trauma are possible causes.
The most common tarsal coalitions occur at the medial talocalcaneal (subtalar) facet and between the calcaneus and navicular (calcaneonavicular). Coalitions can be fibrous, cartilaginous, or osseous. Tarsal coalition occurs in approximately 1% of the general population and appears to be inherited as an autosomal dominant trait with nearly full penetrance. Approximately 60% of calcaneonavicular and 50% of medial facet talocalcaneal coalitions are bilateral.
Clinical Manifestations
Approximately 25% of patients become symptomatic, typically during the 2nd decade of life. Although the flatfoot and a decrease in subtalar motion might have been present since early childhood, the onset of symptoms can correlate with the additional restriction in motion that occurs as a cartilaginous bar ossifies. The timing of ossification varies between the talonavicular (3-5 yr of age), the calcaneonavicular (8-12 yr), and the talocalcaneal (12-16 yr) coalitions. Hindfoot pain is commonly observed, especially in the region of the sinus tarsi and also under the head of the talus. Symptoms are activity related and are often increased with running or prolonged walking, especially on uneven surfaces. There may be tenderness over the site of the coalition and/or pain with testing of subtalar motion. The clinical appearance of a flatfoot is seen in both the weight-bearing and non–weight-bearing positions. There is a restriction in subtalar motion.
Radiographic Evaluation
AP and lateral weight-bearing radiographs and an oblique radiograph of the foot should be obtained (Table 666-2). A calcaneonavicular coalition will be seen best on the oblique radiograph. The lateral radiograph might show elongation of the anterior process of the calcaneus, known as the anteater sign. A talocalcaneal coalition may be seen on a Harris (axial) view of the heel. On the lateral radiograph, there may be narrowing of the posterior facet of the subtalar joint, or a C-shaped line along the medial outline of the talar dome and the inferior outline of the sustentaculum tali (C sign). Beaking of the anterior aspect of the talus on the lateral view is common and results from an alteration in the distribution of stress. This finding does not imply the presence of degenerative arthritis. Irregularity in the subchondral bony surfaces may be seen in patients with a cartilaginous coalition, in contrast to a well-formed bony bridge in those with an osseous coalition.
Table 666-2 RADIOGRAPHIC SECONDARY SIGNS ASSOCIATED WITH TARSAL CONDITIONS
From Slovis TL, editor: Caffey’s pediatric diagnostic imaging, ed 11, vol 2, Philadelphia, 2008, Mosby, p 2604.
A fibrous coalition might require additional imaging studies to diagnose. Plain films may be diagnostic, but a CT scan is the imaging modality of choice when a coalition is suspected (Fig. 666-5). In addition to securing the diagnosis, this study helps to define the degree of joint involvement in patients with a talocalcaneal coalition. Coalitions are uncommon, but >1 tarsal coalition may be observed in the same patient.

Treatment
The treatment of symptomatic tarsal coalitions varies according to the type and extent of coalition, the age of the patient, and the presence and magnitude of symptoms. Treatment is required only for symptomatic coalitions, and the initial management consists of activity restriction and nonsteroidal anti-inflammatory medications, with or without a shoe insert. Immobilization in a short leg walking cast for 4-6 wk may be required in patients with more-pronounced symptoms.
For patients with chronic pain despite an adequate trial of nonoperative therapy, surgical treatment should be considered, and options include resection of the coalition, osteotomy, or arthrodesis. For the calcaneonavicular coalition, resection and interposition of the extensor digitorum brevis muscle have been successful. The surgical treatment of talocalcaneal coalitions is based on the degree of joint involvement, as defined by CT. For patients with <50% of the joint involved, resection of the coalition with interposition of fat or a split portion of the flexor hallucis tendon may be considered. For those with extensive involvement of the joint and/or degenerative changes, a triple arthrodesis may be the best option. The role of osteotomy in the management of tarsal coalition is currently under investigation.
666.7 Cavus Feet
Harish S. Hosalkar, David A. Spiegel, and Richard S. Davidson
Cavus is a deformity involving plantar flexion of the forefoot or midfoot on the hindfoot and can involve the entire forepart of the foot or just the medial column. The result is an elevation of the longitudinal arch (Fig. 666-6), and a deformity of the hindfoot often develops to compensate for the primary forefoot abnormality. Familial cavus can occur, but most patients with this deformity have an underlying neuromuscular etiology. The initial goal is to rule out (and treat) any underlying causes. These diagnoses can relate to abnormalities of the spinal cord (occult dysraphism, tethered cord, poliomyelitis, myelodysplasia, Friedrich ataxia) and peripheral nerves (hereditary motor and sensory neuropathies such as Charcot-Marie-Tooth disease, Dejerine-Sottas disease, Refsum disease). A unilateral cavus foot is most likely to result from an occult intraspinal anomaly, and bilateral involvement usually suggests an underlying nerve or muscle disease. Cavus is commonly observed in association with a hindfoot deformity. In cavovarus, which is the most common deformity in patients with the hereditary motor and sensory neuropathies, progressive weakness and muscle imbalance result in plantar flexion of the 1st ray or medial column. For the foot to land flat, the hindfoot must roll into varus. With equinocavus, the hindfoot is in equinus; in calcaneocavus (usually seen in polio or myelodysplasia), the hindfoot is in calcaneus (excessive dorsiflexion).

Treatment
The 1st step involves identifying any underlying diagnosis, because this knowledge helps to determine the specific management. With mild deformities, stretching of the plantar fascia and exercises to strengthen weakened muscles can help to delay progression. An ankle-foot orthosis may be necessary to stabilize the foot and improve ambulation.
Surgical treatment is indicated for progressive or symptomatic deformities that have failed to respond to nonoperative measures. The specific procedures recommended depend on the degree of deformity and the underlying diagnosis. In the case of a progressive neuromuscular condition, recurrence of deformity is commonly observed, and additional procedures may be required to maintain a plantigrade foot. Families should be counseled in detail regarding the disease process and the expected gains from the surgery. The goal of surgery is to restore motion and alignment and to improve muscle balance. For milder deformities, a soft-tissue release of the plantar fascia, often combined with a tendon transfer, might suffice. For patients with a fixed bony deformity of the forefoot and midfoot and/or the hindfoot, one or more osteotomies may be required for realignment. A triple arthrodesis (calcaneocuboid, talonavicular, and subtalar) may be required for severe or recurrent deformities in older patients.
666.8 Osteochondroses and Apophysitis
Harish S. Hosalkar, David A. Spiegel, and Richard S. Davidson
Osteochondroses are acquired focal disorders of ossification involving epiphyses, apophyses, and other epiphyseal equivalents. Idiopathic avascular necrosis is rarely observed in the tarsal navicular (Köhler disease) or the 2nd or 3rd metatarsal head (Freiberg infraction). Köhler disease (Fig. 666-7) typically appears in children around age 5 or 6 yr and is 3-fold more common in boys than girls. Freiberg infraction is more common in girls and typically occur between ages 8 and 17 yr. Thess are generally self-limited conditions that commonly result in activity-related pain, which can at times be disabling. The treatment is based on the degree of symptoms and commonly includes restriction of activity. For patients with Köhler disease, a short leg cast (6-8 wk) can provide significant relief. Patients with Freiberg infraction can benefit from a period of casting and/or shoe modifications such as a rocker-bottom sole, a stiff-soled shoe, or a metatarsal bar. Degenerative changes occasionally occur following the gradual healing process, and surgical intervention is required in a subset of cases. Procedures have included joint debridement, bone grafting, redirectional osteotomy, subtotal or complete excision of the metatarsal head, and joint replacement.

Figure 666-7 Köhler disease. Anteroposterior radiograph of a 7 yr old boy who presented with fever, pain, and swelling of the midfoot. The left foot reveals a small, fragmented, sclerotic navicular (arrow).
(From Slovis TL, editor: Caffey’s pediatric diagnostic imaging, ed 11, vol 2, Philadelphia, 2008, Mosby.)
Apophysitis represents inflammation at the insertion of a muscle group from repetitive tensile loading and is most commonly observed during periods of rapid growth. These stresses result in microfractures at the fibrocartilaginous insertion site, associated with inflammation. Calcaneal apophysitis (Sever disease) is the most common cause of heel pain in children; treatment includes activity modification, nonsteroidal anti-inflammatory medications, heel cord stretching exercises, and heel cushions or arch supports. Iselin disease represents an apophysitis at the 5th metatarsal base (peroneus brevis) and is less common. Radiographs should be considered when the symptoms are unilateral or with a failure to respond to treatment.
666.9 Puncture Wounds of the Foot
Harish S. Hosalkar, David A. Spiegel, and Richard S. Davidson
Most puncture wound injuries to the foot may be adequately managed in the emergency department. Treatment involves a thorough irrigation and a tetanus booster, if appropriate; many clinicians recommend antibiotics. Using this approach, most children heal without a complication. A subset of patients develop cellulitis, most often due to Staphylococcus aureus (Chapter 174), and require intravenous antibiotics with or without surgical drainage. Deep infection is uncommon and may be associated with septic arthritis, osteochondritis, or osteomyelitis. The most common organisms are S. aureus and Pseudomonas (Chapter 197); the treatment involves a thorough surgical debridement followed by a short (10-14 days) course of systemic antibiotics. Plain radiographs demonstrate any metallic fragments, but ultrasonography may be necessary to identify glass or wooden objects. Routine exploration and removal of foreign bodies is not required, but it may be necessary when symptoms are present, with recurrences, or when an infection is suspected. Pain and/or gait disturbance is more likely with superficial objects under the plantar surface of the foot. One special situation occurs when a puncture wound from a nail comes through an old sneaker. There is a high risk of a pseudomonal infection, and thorough irrigation and debridement under general anesthesia followed by systemic antibiotics for 10-14 days should be considered.
666.10 Toe Deformities
Juvenile Hallux Valgus (Bunion)
Juvenile hallux valgus is 10-fold more common in girls and is typically associated with familial ligamentous laxity, and a positive family history is common. The etiology is multifactorial, and important factors include genetic factors, ligamentous laxity, pes planus, wearing shoes with a narrow toe box, and occasionally spasticity (cerebral palsy).
Clinical Manifestations
There is prominence of the 1st metatarsophalangeal (MTP) joint and often erythema from chronic irritation. The great toe is in valgus and is usually pronated, and there is splaying of the forefoot. Pes planus, with or without an associated heel cord contracture, is also observed commonly. Cosmesis is perhaps the most common concern, and some patients have pain in the region of the 1st MTP joint and/or difficulty with shoe wear.
Radiographic Evaluation
Weight-bearing AP and lateral radiographs of the feet are obtained. On the AP view, common measurements include the angular relationships between the 1st and 2nd metatarsals (intermetatarsal angle, <10 degrees is normal) and between the 1st metatarsal and the proximal phalanx (hallux valgus angle, <25 degrees is normal) (Fig. 666-8). The orientation of the 1st metatarsal-medial cuneiform joint is also documented. On the lateral radiograph, the angular relationship between the talus and the 1st metatarsal helps to identify a midfoot break associated with pes planus. Radiographs are more helpful in surgical planning than in establishing the diagnosis.

Treatment
Conservative management of adolescent bunions consists primarily of shoe modifications. It is important that footwear accommodate the width of the forefoot. Patients should avoid wearing shoes with a narrow toe box and/or a high heel. Shoe modifications such as a soft upper, bunion last, or heel cup may also be recommended. In the presence of a pes planus, an orthotic to restore the medial longitudinal arch may be beneficial. Stretching exercises are recommended to treat contracture of the Achilles tendon. The value of night splinting remains to be determined.
Surgical treatment is reserved for patients with persistent and disabling pain who have failed a course of nonoperative therapy. Surgery is not advised purely for cosmesis. Surgery is usually delayed until skeletal maturity to decrease the risk of recurrence. Radiographs are essential in preoperative planning to assess both the magnitude of deformity (hallux valgus angle, intermetatarsal angle, distal metatarsal articular angle) and associated features such as obliquity of the 1st metatarsal-medial cuneiform joint. Surgical treatment often involves a soft-tissue release and/or rebalancing procedure at the 1st MTP joint, and a single or double osteotomy of the 1st metatarsal to decrease foot width and realign the joints along the medial column of the forefoot. An arthrodesis of the 1st MTP joint may be indicated in patients with spasticity in order to prevent recurrence.
Curly Toes
A curly toe is caused by contracture of the flexor digitorum longus, and there is flexion at the MTP and the interphalangeal (IP) joints associated with medial deviation of the toe. The toe usually lies underneath its neighbor, and the 4th and 5th toes are most commonly involved. The deformity rarely causes symptoms, and active treatment (stretching, splinting, or taping) is not required. Most cases improve over time, and a subset resolve completely. For the rare case in which there is chronic pain or skin irritation, release of the flexor digitorum longus muscle at the distal interphalangeal joint may be considered.
Overlapping 5th Toe
Congenital digitus minimus varus, or varus 5th toe, involves dorsiflexion and adduction of the 5th toe. The 5th toe typically overlaps the 4th. There is also a rotatory deformity of the toe, and the nail tends to point outward. The deformity is usually bilateral and might have a genetic basis. Symptoms are frequent and involve pain over the dorsum of the toe from shoe wear.
Nonoperative treatment has not been successful. For symptomatic patients, several different options for reconstruction have been described. Common features include releasing the contracted extensor tendon and the MTP joint capsule (dorsal, dorsomedial, or complete). A partial removal of the proximal phalanx and creation of a syndactyly between the 4th and 5th toes has been performed in conjunction with the release as well.
Polydactyly
Polydactyly is the most common congenital toe deformity and is seen in approximately 2/1,000 births and is bilateral in 50% of cases. Polydactyly may be preaxial (great toe) or postaxial (5th toe), and occasionally one of the central toes is duplicated. Associated anomalies are found in approximately 10% of the preaxial and 20% of postaxial polydactyly. One third of patients also have polydactyly of the hand. Conditions that may be associated with polydactyly include Ellis-van Creveld (chondroectodermal dysplasia), longitudinal deficiency of the tibia, and Down syndrome. The extra digit may be either rudimentary or well formed, and plain radiographs of the foot help to define the anatomy and evaluate any coexisting bony anomalies.
Treatment is indicated for cosmesis and to allow fitting with standard shoes. This involves surgical removal of the extra digit, and the procedure is generally performed between 9 and 12 mo of age. Rudimentary digits may be surgically excised earlier but should not be “tied off.”
Syndactyly
Syndactyly involves webbing of the toes, which may be incomplete or complete (extends to the tip of the toes), and the toenails may be confluent. There is often a positive family history, and the 3rd and 4th toes are involved most commonly. Symptoms are extremely rare, and cosmetic concerns are uncommon. Treatment is only required for patients in whom there is an associated polydactyly (Fig. 666-9). In such cases, the border digit is excised, and the extra skin facilitates coverage of the wound. If the syndactyly does not involve the extra toe, then it can be observed. A complex syndactyly may be seen in patients with Apert syndrome.

Hammer Toe
A hammer toe involves flexion at the proximal IP (PIP) joint with or without the distal IP (DIP) joint, and the MTP joint may be hyperextended. This deformity may be distinguished from a curly toe by the absence of rotation. The 2nd toe is most commonly involved, and a painful callus can develop over the dorsum of the toe where it rubs on the shoe. Nonoperative therapy is rarely successful, and surgery is recommended for symptomatic cases. A release of the flexor tendons suffices in the majority of cases. Some authors have recommended a transfer of the flexor tendon to the extensor tendon. For severe cases with significant rigidity, especially in older patients, a partial or complete resection of the proximal phalanx and a PIP fusion may be required.
Mallet Toe
Mallet toe involves a flexion contracture at the DIP joint and results from congenital shortening of the flexor digitorum longus tendon. Patients can develop a painful callus on the plantar surface of the tuft. Because nonoperative therapy is usually unsuccessful, surgery is required for patients with chronic symptoms. For flexible deformities in younger children, release of the flexor digitorum longus tendon is recommended. For stiffer deformities in older patients, resection of the head of the middle phalanx, or arthrodesis of the DIP joint, may be considered.
Claw Toe
A claw toe deformity involves hyperextension at the MTP joint and flexion at both the PIP and DIP joints, often associated with dorsal subluxation of the MTP joint. The majority are associated with an underlying neurologic disorder such as Charcot-Marie-Tooth disease. The etiology is usually muscle imbalance, and the extensor tendons are recruited to substitute for weakening of the tibialis anterior muscle. If treatment is elected, surgery is required. Transfer of the extensor digitorum (or hallucis) tendon to the metatarsal neck is commonly performed along with a dorsal capsulotomy of the MTP joint and fusion of the fusion of the PIP joint (IP joint of the great toe).
Annular Bands
Bands of amniotic tissue associated with amniotic disruption syndrome (early amniotic rupture sequence, congenital constriction band syndrome, annular band syndrome) can become entwined along the extremities, resulting in a spectrum of problems from in utero amputation (Fig. 666-10) to a constriction ring along a digit (Fig. 666-11) (Chapter 102). These rings, if deep enough, can impair arterial or venous blood flow. Concerns regarding tissue viability are less common, but swelling from impairment in venous return is often a great problem. The treatment of annular bands usually involves observation; however, circumferential release of the band may be required emergently if arterial inflow is obstructed or electively to relieve venous congestion.


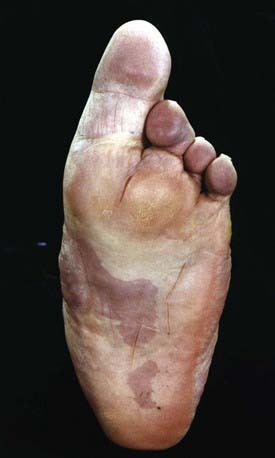
Macrodactyly
Macrodactyly represents an enlargement of the toes and can occur as an isolated problem or in association with a variety of other conditions such as Proteus syndrome (Fig. 666-12), neurofibromatosis, tuberous sclerosis, and Klippel-Trenaunay-Weber syndrome. This condition results from a deregulation of growth, and there is hyperplasia of one or more of the underlying tissues (osseous, nervous, lymphatic, vascular, fibrofatty). Macrodactyly of the toes may be seen in isolation (localized gigantism) or with enlargement of the entire foot. In addition to cosmetic concerns, patients might have difficulty wearing standard shoes.
The treatment is observation, if possible. This is a difficult condition to treat surgically, and complications are common. For involvement of a single toe, the best option may be a resection of the ray (including the metatarsal). For greater degrees of involvement, debulking of the various tissues is required. Often, a growth arrest of the underlying osseous structures is performed. Stiffness and wound problems are common. The rate of recurrence is high, and more than one debulking may be required. Patients may elect to have an amputation if the process cannot be controlled by less extensive procedures.
Subungual Exostosis
A subungual exostosis is a mass of normal bone tissue that projects out from the dorsal and medial surface of a toe, under the nail. The etiology is unknown but might relate to minor repetitive trauma. The great toe is involved most often. Patients present with discomfort, and the toenail may be elevated. The lesion may be demonstrated on plain radiographs and histologically involves normal bone with a fibrocartilaginous cap. The treatment for symptomatic lesions is excision, and the recurrence rate is in the range of 10%.
Ingrown Toenail
Ingrown toenails are relatively common in infants and young children and usually involve the medial or lateral border of the great toe. Symptoms include chronic irritation and discomfort; more advanced stages include drainage, infection, and granulations tissue. If conservative measures including shoe modifications, warm soaks, and appropriate nail trimming fail to control the symptoms, then surgical removal of a portion of the nail should be considered. Several surgical approaches are available, including avulsion of the ingrowing nail or avulsion with removal of the underlying germinal matrix. Chemical matrixectomy using NaOH is an alternative to surgery.
Coughlin MJ. Lesser toe abnormalities. Instr Course Lect. 2003;52:421-444.
Lokiec F, Ezra E, Krasin D, et al. A simple and efficient surgical technique for subungual exostosis. J Pediatr Orthop. 2001;21:76-79.
Yang G, Yanchar NL, Lo AY, et al. Treatment of ingrown toenails in the pediatric population. J Pediatr Surg. 2008;43(5):931-935.
666.11 Painful Foot
Harish S. Hosalkar, David A. Spiegel, and Richard S. Davidson
A differential diagnosis for foot pain in different age ranges is shown in Table 666-3. In addition to the history and physical examination, plain radiographs are most helpful in establishing the diagnosis. Occasionally, more sophisticated imaging modalities are required.
666.12 Shoes
In toddlers and children, a shoe with a flexible sole is recommended. This recommendation is in part based on studies suggesting that the development of the longitudinal arch seems to be best in societies where shoes are not worn. With increased participation of children in sports on hard surfaces, well-cushioned, shock-absorbing shoes are helpful in the child and adolescent athlete to decrease the chances of developing an overuse syndrome. In small shoes, cushioning elements are often oversized. During school age the child’s connective tissue gains stability. Cushioning for the school-age child must strike a balance between adequate cushioning and the growing child’s need for adequate mechanical stimuli to help the muscles and bones develop. Connective tissue strength and joint flexibility reach adult levels by the age of 15 yr. Otherwise, shoe modifications are generally reserved for abnormalities in alignment between segments of the foot or symptoms from an underlying condition. Numerous modifications are available.