Chapter 667 Torsional and Angular Deformities
667.1 Normal Limb Development
An understanding of normal limb development is essential for pediatricians to recognize pathologic conditions during routine and targeted exams. During the 7th wk of intrauterine life, the lower limb rotates medially to bring the great toe toward the midline. The hip joint forms by the 11th wk; the proximal femur and acetabulum continue to develop until physeal closure in adolescence. At birth, the femoral neck is rotated forward approximately 40 degrees. This forward rotation is referred to as anteversion (the angle between the axis of the femoral neck and the transcondylar axis). The increased anteversion increases the internal rotation of the hip. Femoral anteversion decreases to 15-20 degrees by 8-10 yr of age. The second source of limb rotation is found in the tibia. Infants can have 30 degrees of medial rotation of the tibia, and by maturity the rotation is between 5 degrees of medial rotation and 15 degrees of lateral rotation (Fig. 667-1). Excessive medial rotation of tibia is referred to as medial tibial torsion. The tibial torsion is the angular difference between the axis of the knee and the transmalleolar axis. The medial or lateral rotation beyond ±2 standard deviations (SDs) from the mean is considered abnormal rotation.
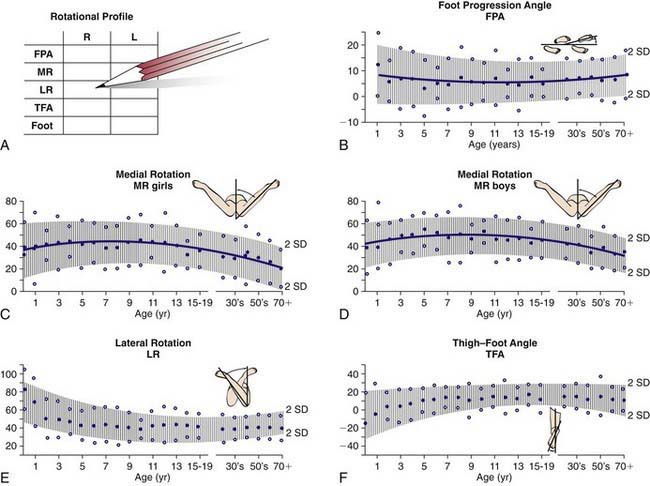
Figure 667-1 A-F, The rotational profile from birth to maturity is depicted graphically. All graphs include 2 standard deviations from the mean for the foot progression angle (FPA) for femoral medial rotation (MR) and lateral rotation (LR) (for boys and girls), and the thigh-foot angle (TFA).
(From Morrissey RT, Weinstein SL, editors: Lovell and Winter’s pediatric orthopaedics, ed 3, Philadelphia, 1990, Lippincott Williams & Wilkins.)
Limb rotation is also found in the foot. The abnormalities could be excessive adduction or abduction. Torsional deformity may be simple, involving a single segment, or complex, involving multiple segments. Complex deformities may be additive (internal tibial torsion and internal femoral torsion are additive) or compensatory (external tibial torsion and internal femoral torsion are compensatory).
The normal tibiofemoral angle at birth is 10-15 degrees of physiologic varus. The alignment changes to 0 degrees by 18 mo, and physiologic valgus up to 12 degrees is reached in between 3 and 4 yr of age. The normal valgus of 7 degrees is achieved by 5-8 yr of age (Fig. 667-2). Persistence of varus beyond 2 yr of age may be pathologic. Overall, 95% of developmental physiologic genu varum and genu valgum cases resolve with growth. Persistent genu valgum or valgus into adolescence is considered pathologic and deserves further evaluation.
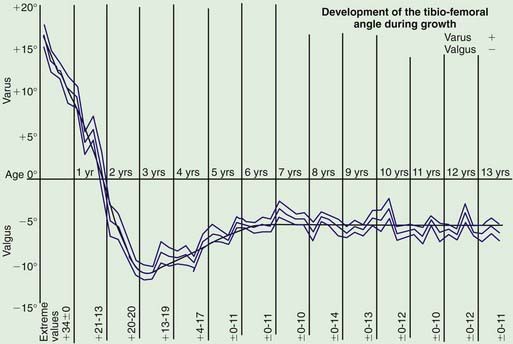
Figure 667-2 The normal coronal alignment of the knee plotted for age.
(From Salenius P, Vanka E: The development of the tibiofemoral angle in children. J Bone Joint Surg Am 57:259–261, 1975.)
Arazi M, Ogun TC, Memik R. Normal development of the tibiofemoral angle in children: a clinical study of 590 normal subjects from 3 to 17 years of age. J Pediatr Orthop. 2001;21:264-267.
Cahuzac JP, Vardon D, Sales de Gauzy J. Development of the clinical tibiofemoral angle in normal adolescents: a study of 427 normal subjects from 10 to 16 years of age. J Bone Joint Surg Br. 1995;77:729-732.
Heath CH, Staheli LT. Normal limits of knee angle in white children—genu varum and genu valgum. J Pediatr Orthop. 1993;13:259-262.
Salenius P, Vankka E. The development of the tibiofemoral angle in children. J Bone Joint Surg Am. 1975;57:259-261.
667.2 Evaluation
In evaluation of concerns relating to the limb, the pediatrician should obtain a history of the onset, progression, functional limitations, previous treatment, evidence of neuromuscular disorder, and any significant family history.
The examination should assess the exact torsional profile and include (1) foot progression angle, (2) femoral anteversion, (3) tibial version with thigh-foot angle, and (4) assessment of foot adduction and abduction.
Foot Progression Angle
Limb position during gait is expressed as the foot progression angle (FPA) and represents the angular difference between the axis of the foot with the direction in which the child is walking. Its value is usually estimated by asking the child to walk in the clinic hallway (Fig. 667-3). Inward rotation of the foot is assigned a negative value, and outward rotation is designated with positive value. The normal FPA in children and adolescents is 10 degrees (range, −3 to 20 degrees). The FPA serves only to define whether there is an in-toeing or out-toeing gait.
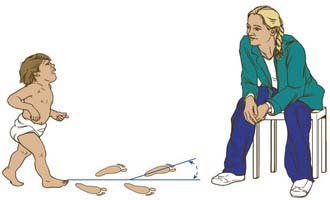
Figure 667-3 Foot progression angle. The long axis of the foot is compared with the direction in which the child is walking. If the long axis of the foot is directed outward, the angle is positive. If the foot is directed inward, the angle is negative and indicates in-toeing.
(From Thompson GH: Gait disturbances. In Kliegman RM, editor: Practical strategies in pediatric diagnosis and therapy. Philadelphia, 2004, Saunders.)
Femoral Anteversion
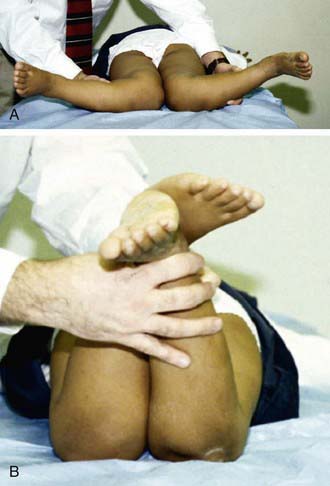
Measuring the hip rotation with the child in prone position, the hip in neutral flexion or extension, thighs together, and the knees flexed 90 degrees indirectly assesses the anteversion (Fig. 667-4). Both hips are assessed at the same time. As the lower leg is rotated ipsilaterally, this produces internal rotation of the hip, whereas contralateral rotation produces external rotation. Excessive anteversion increases internal rotation, and, retroversion increases the external rotation.
Tibial Rotation
Tibial rotation is measured using the transmalleolar angle (TMA). The TMA is the angle between the longitudinal axis of the thigh with a line perpendicular to the axis of the medial and lateral malleolus (Fig. 667-5). In the absence of foot deformity, the thigh foot angle (TFA) is preferred (Fig. 667-6). It is measured with the child lying prone. The angle is formed between the longitudinal axis of the thigh and the longitudinal axis of the foot. It measures the tibial and hindfoot rotational status. Inward rotation is assigned a negative value, and outward rotation is designated a positive value. Inward rotation indicates internal tibial torsion, whereas outward rotation represents external tibial torsion. Infants have a mean angle of −5 degrees (range, −35 to 40 degrees) as a consequence of normal in utero position. In mid-childhood through adult life, the mean TFA is 10 degrees (range, −5 to 30 degrees).
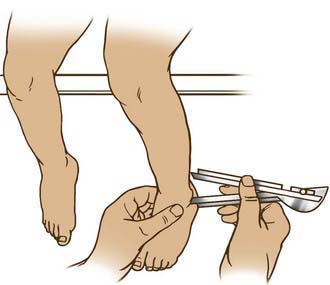
Figure 667-5 The transmalleolar angle is measured with the patient sitting at the edge of the table and the distal femoral condyles aligned with the side of the table. The angle between a line through the medial and lateral malleoli and edge of the table should be approximately 30 degrees external.
(From Bleck EE: Orthopaedic management in cerebral palsy, London, 1987, MacKeith Press, p 55.)

Foot Shape and Position
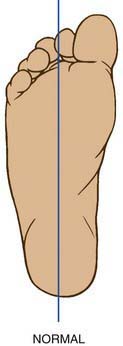
The foot is observed for any deformities in prone and standing position. The heel bisector line (HBL) is used to evaluate the foot adduction and abduction deformities. The HBL is a line that divides the heel in two equal halves along the longitudinal axis (Fig. 667-7). It normally extends to the 2nd toe. When the HBL points medial to the 2nd toe, the forefoot is abducted, and when the HBL is lateral to the 2nd toe, the forefoot is adducted.
It is also important to screen every affected child for associated hip dysplasia and neuromuscular problems (cerebral palsy).
Ruwe PA, Gage JR, Ozonoff MB, et al. Clinical determination of femoral anteversion: a comparison of established techniques. J Bone Joint Surg Am. 1992;74:820-830.
Thompson GH. Gait disturbances. In: Kliegman RM, editor. Practical strategies in pediatric diagnosis and therapy. ed 2. Philadelphia: WB Saunders; 2003:823-843.
667.3 Torsional Deformities
Internal Femoral Torsion
In-toeing gait most commonly results from excessive femoral anteversion. It occurs more commonly in girls than boys (2 : 1) in children 3-6 yr of age. The etiology of femoral torsion is controversial. Some believe that it is congenital and a result of persistent infantile femoral anteversion, whereas others believe it is acquired secondary to abnormal sitting habits. Some children are in habit of sitting in a W position or sleeping prone. On examination, most children with this condition have generalized ligamentous laxity. Gait examination reveals that entire leg is inwardly rotated. Internal hip rotation is increased beyond 70 degrees, and consequently the external rotation is restricted to 10-20 degrees. The patellas are pointing inward when the foot is straight, and compensatory external rotation of the tibia is demonstrated.
Diagnosis is made clinically on examination; CT can provide objective measurements but is rarely indicated. The treatment is predominantly observation and correction of abnormal sitting habits. The torsion usually corrects with growth by 8-10 yr of age. Persistent deformity, unacceptable cosmesis, functional impairment, anteversion >45 degrees, and no external rotation beyond neutral are some of the indications for operative intervention. Surgery involves derotation osteotomy of the femur.
Internal Tibial Torsion
Medial tibial torsion manifests with in-toeing gait and is commonly associated with congenital metatarsus varus, genu valgum, or femoral anteversion. This condition is usually seen during the 2nd yr of life. Normally at birth, the medial malleolus lies behind the lateral malleolus, but by adulthood, it is reversed, with the tibia in 15 degrees of external rotation. The treatment is essentially observation and reassurance, because spontaneous resolution with normal growth and development can be anticipated. Significant improvement usually does not occur until the child begins to pull to stand and walk independently. Thereafter, correction can be seen as early as 4 yr of age and in some children by 8-10 yr of age. Persistent deformity with functional impairment is treated with supramalleolar osteotomy.
External Femoral Torsion
External femoral torsion can follow a slipped capital femoral epiphysis (SCFE); there is a low threshold to perform radiographs of the hips in children >10 yr of age. Femoral retrotorsion, when of idiopathic origin, is usually bilateral. The disorder is associated with an out-toeing gait and increased incidence of degenerative arthritis. The clinical examination of external femoral torsion shows excessive hip external rotation and limitation of internal rotation. The hip will externally rotate up to 70-90 degrees, whereas internal rotation is only 0-20 degrees. If SCFE is detected, it is treated surgically. Occasionally, persistent femoral retroversion after SCFE can produce functional impairment such as a severe out-toeing gait and difficulty opposing one’s knees in the sitting position. The latter can be disabling to adolescent girls. Should this occur, a derotation osteotomy might be necessary.
External Tibial Torsion
Lateral tibial torsion is less common than medial rotation and is often associated with a calcaneovalgus foot. It can be compensatory to persistent femoral anteversion and idiopathic or secondary to a tight iliotibial band. The natural growth rotates the tibia externally, and hence external tibial torsion can become worse with time. Clinically, the patella faces outward when the foot is straight. The TFA and the TMA are increased. There may be associated patellofemoral instability with knee pain. Though some correction can occur with growth, extremely symptomatic children need supramalleolar osteotomy, which is usually done by 10-12 yr of age.
Metatarsus Adductus
Metatarsus adductus (Chapter 666.01) manifests with forefoot adduction and inversion of all metatarsals. Ten to 15% are associated with hip dysplasia. The prognosis is good, because the majority get better with nonoperative intervention. The feet, which are flexible and correctable up to neutral, are treated with stretching exercises. Those that are not completely correctable are treated with serial casting. Rigid deformities, which are not correctable by stretching, are treated with medial capsulotomy of the 1st metatarsal cuneiform joint and soft-tissue release by 2 yr of age. Osteotomies of the base of the metatarsal are usually done after 6 yr of age.
667.4 Coronal Plane Deformities
Genu varum and genu valgum are common pediatric deformities of the knee. The age-appropriate normal values for knee angle are presented in Figure 667-2. Tibial bowing is common during the 1st year, bowlegs are common during the 2nd year, and knock-knees are most prominent between 3 and 4 yr of age.
Genu Varum
Physiologic bowleg is a common torsional combination that is secondary to normal in utero positioning (Fig. 667-8). Spontaneous resolution with normal growth and development can be anticipated. Persistence of varus beyond 2 yr of age may be pathologic. The different causes are metabolic bone disease (vitamin D deficiency, rickets, hypophosphatasia), asymmetric growth arrest (trauma, infection, tumor, Blount), bone dysplasia (dwarfism, metaphyseal dysplasia), and congenital and neuromuscular disorders (Table 667-1). It is prudent to differentiate physiologic bowing from Blount disease (Table 667-2). Physiologic bowing should also be differentiated from rickets and skeletal dysplasia. Rickets has classic bone changes with trumpeting widening and fraying of the metaphysis and widening of the physis (Chapter 48).

Figure 667-8 A, In recumbent position, tibia and femora are bowed but the legs do not appear bowed. B, In erect position during weight bearing and with ankles in apposition, the legs are bowed.
(From Slovis TL, editor: Caffey’s pediatric diagnostic imaging, ed 11, Philadelphia, 2008, Mosby.)
Table 667-1 CLASSIFICATION OF GENU VARUM (BOWLEGS)
PHYSIOLOGIC
ASYMMETRIC GROWTH
METABOLIC DISORDERS
SKELETAL DYSPLASIA
Modified from Thompson GH: Angular deformities of the lower extremities. In Chapman MW, editor: Operative orthopedics, ed 2, Philadelphia, 1993, JB Lippincott, pp 3131–3164.
Table 667-2 DIFFERENTIATION OF LEG BOWING
| PHYSIOLOGIC BOWING | BLOUNT DISEASE |
|---|---|
| Gentle and symmetric deformity | Asymmetric, abrupt, and sharp angulation |
| Metaphyseal-diaphyseal angle <11 degrees | Metaphyseal-diaphyseal angle >11 degrees |
| Normal appearance of the proximal tibial growth plate | Medial sloping of the epiphysis Widening of the physis Fragmentation of the metaphysis |
| No significant lateral thrust | Significant lateral thrust |
Tibia Vara
Idiopathic tibia vara, or Blount disease, is a developmental deformity resulting from abnormal endochondral ossification of the medial aspect of the proximal tibial physis leading to varus angulation and medial rotation of the tibia (Fig. 667-9). The incidence is greater in African-Americans and in toddlers who are overweight, have an affected family member, or started walking early in life. It has been classified into three types depending on the age at onset: infantile (1-3 yr), juvenile (4-10 yr), and adolescent (11 yr or older). The juvenile and adolescent forms are commonly combined as late-onset tibia vara. The exact cause of tibia vara remains unknown.

Figure 667-9 Clinical photograph (A) and standing anteroposterior radiograph (B) of a 5 yr old girl with bilateral early-onset Blount disease.
(From Sabharwal S: Blount disease, J Bone Joint Surg Am 91:1758–1776, 2009.)
The infantile form of tibia vara is the most common; its characteristics include predominance in black girls, approximately 80% bilateral involvement, a prominent medial metaphyseal beak, internal tibial torsion, and leg-length discrepancy (LLD). The characteristics of the juvenile and adolescent forms (late onset) include predominance in black boys, normal or greater than normal height, approximately 50% bilateral involvement, slowly progressive genu varum deformity, pain rather than deformity as the primary initial complaint, no palpable proximal medial metaphyseal beak, minimal internal tibial torsion, mild medial collateral ligament laxity, and mild lower extremity length discrepancy. The infantile group has the greatest potential for progression.
An anteroposterior standing radiograph of both lower extremities with patellas facing forward and a lateral radiograph of the involved extremity should be obtained (Fig. 667-10). Weight-bearing radiographs are preferred and allow maximal presentation of the clinical deformity. The metaphyseal-diaphyseal angle can be measured and is useful in distinguishing between physiologic genu varum and early tibia vara (Fig. 667-11). Langenskiöld has six stages on radiographs (Fig. 667-12). The differentiation is based on fragmentation of the epiphysis, beaking of the medial tibial epiphysis, depression of the medial tibial plateau, and formation of a bony bar. Occasionally, CT with three-dimensional reconstructions, or MRI, may be necessary to assess the meniscus, the articular surface of the proximal tibia including the posteromedial slope, or the integrity of the proximal tibial physis.

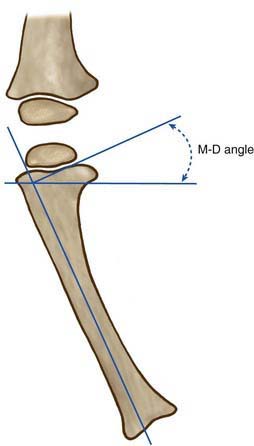
Figure 667-11 Metaphyseal-diaphyseal (M-D) angle. Draw a line on the radiograph through the proximal tibial physis. Draw another line along the lateral tibial cortex. Last, draw a line perpendicular to the shaft line as demonstrated in the diagram.
(From Morrissey RT, Weinstein SL, editors: Lovell and Winter’s pediatric orthopaedics, ed 3, Philadelphia, 1990, Lippincott Williams & Wilkins.)
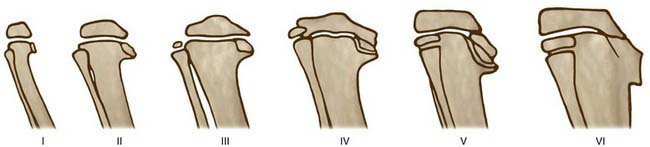
Figure 667-12 Depiction of the stages of infantile Blount disease.
(From Langeskiöld A: Tibia vara [osteochondrosis deformans tibiae]: a survey of 23 cases, Acta Chir Scand 103:1, 1952.)
Management is based on the stage of the disease, the age of the child, and nature of presentation (primary or recurrent deformity). In children younger than 3 yr and Langenskiöld stage <3, bracing is effective and can prevent progression in 50% of these children. A maximal trial of 1 yr of orthotic management is recommended. If complete correction is not obtained after 1 yr or if progression occurs during this time, a corrective osteotomy may be indicated. Surgical treatment is also indicated in children >4 yr of age, those at Langenskiöld stage >3, and those with severe deformities. A proximal tibial valgus osteotomy and associated fibular diaphyseal osteotomy are usually the procedures of choice. In late-onset tibia vara, correction is also necessary to restore the mechanical axis of the knee. Hemiplateau elevation with correction of posteromedial slope has also been established as a treatment modality in relapsed cases.
Genu Valgum (Knock-Knees)
The normal valgus is achieved by 4 yr of age. Variation up to 15 degrees of valgus is possible until 6 yr of age, and thus physiologic valgus has a good chance of correction until this age. The intermalleolar distance with the knees approximated is normally <2 cm, and in a severe valgus deformity it could measure >10 cm. Pathologic conditions leading to valgus are metabolic bone disease (rickets, renal osteodystrophy), skeletal dysplasia, posttraumatic physeal arrest, tumors, and infection. The increased valgus at the knee causes lateral deviation of the mechanical axis with stretching of the medial aspect of the knee leading to knee pain. Deformities >15 degrees and occurring after 6 yr of age are unlikely to correct with growth and require surgical management. In the skeletally immature, medial tibial epiphyseal hemiepiphysiodesis or stapling (guided growth) is attempted for correction. In the skeletally mature, osteotomy is necessary at the center of rotation of angulation and is usually situated in the distal femur. Long-length anteroposterior radiographs of the leg in a weight-bearing stance are necessary for preoperative planning.
Cheema JI, Grissom LE, Harcke HT. Radiographic characteristics of lower-extremity bowing in children. Radiographics. 2003;23(4):871-880.
Davids JR, Blackhurst DW, Allen BLJr. Radiographic evaluation of bowed legs in children. J Pediatr Orthop. 2001;21:257-263.
Do TT. Clinical and radiographic evaluation of bowlegs. Curr Opin Pediatr. 2001;13:42-46.
Doyle BS, Volk G, Smith CI. Infantile Blount’s disease: long-term follow-up of surgically treated patients at skeletal maturity. J Pediatr Orthop. 1996;16:469-476.
Feldman MD, Schoenecker PL. Use of metaphyseal-diaphyseal angle in the evaluation of bowed legs. J Bone Joint Surg Am. 1993;75:1602-1609.
Henderson RC, Kemp GJ, Greene WB. Adolescent tibia vara: alternatives for operative treatment. J Bone Joint Surg Am. 1992;74:342-350.
Henderson RC, Kemp GJ, Hayes PRL. Prevalence of late-onset tibia vara. J Pediatr Orthop. 1993;13:255-258.
Johnston CEII. Infantile tibia vara. Clin Orthop. 1990;255:13-23.
Sabharwal S. Blount disease. J Bone Joint Surg Am. 2009;91:1758-1776.
Stevens PM, Maguire M, Dales MD, et al. Physeal stapling for idiopathic genu valgum. J Pediatr Orthop. 1999;19:645-649.
Thompson GH. Angular deformities of the lower extremities in children. In: Chapman MW, editor. Operative orthopedics. ed 3. Philadelphia: JB Lippincott; 2001:4287-4335.
667.5 Congenital Angular Deformities of the Tibia and Fibula
Posteromedial Tibial Bowing
Congenital posteromedial bowing is typically associated with a calcaneovalgus foot and rarely with secondary valgus of the tibia, although the exact cause is unknown. Early operative intervention is not indicated because this bowing generally corrects with growth. However, despite the correction of angulation, there is residual shortening in the tibia and fibula. The mean growth inhibition is 12-13% (range, 5-27%). The mean leg-length-discrepancy (LLD) at maturity is 4 cm (range, 3-7 cm). The diagnosis of bowing is confirmed on radiographs, which show the posteromedial angulation without any other osseous abnormalities. The calcaneovalgus deformity of the foot improves with stretching or modified shoe wear and occasionally ankle-foot orthosis. Predicted LLD <4 cm is managed with age-appropriate epiphysiodesis of the normal leg. LLD >4 cm is managed with combination of contralateral epiphysiodesis and ipsilateral lengthening. A corrective osteotomy for distal valgus may be required and can be done in the same setting while correcting LLD.
Anteromedial Tibial Bowing (Postaxial Hemimelia)
Fibular hemimelia is the most common cause of anteromedial bowing of the tibia. The fibular deficiency can occur with complete absence of fibula or a partial development both proximally and distally. It is associated with deformities of femur, knee, tibia, ankle, and foot. The femur is short and has lateral condylar hypoplasia, causing patellar instability and genu valgum deformity. The tibia has anteromedial bowing with reduced growth potential. The keys for management are the ankle stability and foot deformities. The ankle resembles a ball-and-socket joint with lateral instability. The foot deformities are characterized by the absence of lateral digits, equinocavovarus foot, and tarsal coalition.
Various surgical options have been described, and the treatment is tailored to the patient’s needs and parents’ acceptance. A severely deformed foot could be best managed with Syme or Boyd amputation, with prosthesis as early as 1 yr of age. In the salvageable foot, LLD can be treated with contralateral leg epiphysiodesis or ipsilateral limb lengthening.
Anterolateral Tibial Bowing
Anterolateral tibial bowing is associated with congenital pseudarthrosis of tibia. Fifty percent of the patients have neurofibromatosis, but only 10% of the neurofibromatosis patients have this lesion. The pseudarthrosis or site of nonunion is typically situated at the middle third and distal third of the tibia. Boyd has classified it in increasing severity depending on the presence of cystic and dysplastic changes. The treatment for this condition has been very frustrating, with poor results. Bracing has been recommended to prevent fracture early in the course; however, it has not been successful. Numerous surgical interventions have been attempted to achieve union such as single- and dual-onlay grafting with rigid internal fixation, intramedullary pinning with or without bone grafting, and an Ilizarov device. With the advent of microsurgery, live fibular grafts have been used with varying results. Due to the poor chances of successful union and considerable LLD, a below-knee amputation with early rehabilitation may be preferred. It is important not to attempt any osteotomy for correction of the tibial bowing.
Tibial Longitudinal Deficiency
Tibial longitudinal deficiency follows an autosomal dominant inheritance pattern and has been divided into four types depending on the deficient part of the tibia. The other associated anomalies are foot deformities, hip dysplasia, and symphalangism of the hand. The treatment revolves around presence of proximal tibial anlage and a functional quadriceps mechanism. In type Ia deformity, the proximal tibial anlage is absent and knee disarticulation with prosthesis is recommended. In types Ib and II, the tibial anlage is present and the management consists of an early Syme amputation, followed later by synostosis of the fibula with the tibia, and a below-knee prosthesis. Type III is rare and the principal management is with Syme amputation and a prosthesis. Type IV deformity is associated with ankle diastasis, which requires stabilization of the ankle and correction of LLD at a later stage.
Wallach DM, Davidson RS. Pediatric lower limb disorders. In: Dormans JP, editor. Core knowledge in orthopaedics: pediatric orthopaedics. Philadelphia: Mosby; 2005:197-223.
Wallach DM, Davidson RS. Pediatric lower limb disorders. In: Dormans JP, editor. Pediatric orthopaedics and sports medicine: the requisites in pediatrics. Philadelphia: Mosby; 2005:246-272.