Chapter 48 Rickets and Hypervitaminosis D
Rickets
Bone consists of a protein matrix called osteoid and a mineral phase, principally composed of calcium and phosphate, mostly in the form of hydroxyapatite. Osteomalacia is present when there is inadequate mineralization of bone osteoid and occurs in children and adults. Rickets is a disease of growing bone that is due to unmineralized matrix at the growth plates and occurs in children only before fusion of the epiphyses. Because growth plate cartilage and osteoid continue to expand but mineralization is inadequate, the growth plate thickens. There is also an increase in the circumference of the growth plate and the metaphysis, increasing bone width at the location of the growth plates and causing some of the classic clinical manifestations, such as widening of the wrists and ankles. There is a general softening of the bones that causes them to bend easily when subject to forces such as weight bearing or muscle pull. This softening leads to a variety of bone deformities.
Rickets is principally due to vitamin D deficiency (Table 48-1) and was rampant in northern Europe and the USA during the early years of the 20th century. Although this problem was largely corrected through public health measures that provided children with adequate vitamin D, rickets remains a persistent problem in developed countries, with many cases still secondary to preventable nutritional vitamin D deficiency It remains a significant problem in developing countries as well, with some community-based and general hospital-based surveys among children in Africa finding the prevalence of rickets exceeds 10%. UNICEF has estimated that up to 25% of children in China have some evidence of rickets.

Etiology
There are many causes of rickets (Table 48-2), including vitamin D disorders, calcium deficiency, phosphorous deficiency, and distal renal tubular acidosis.
Clinical Manifestations
Most manifestations of rickets are due to skeletal changes (Table 48-3). Craniotabes is a softening of the cranial bones and can be detected by applying pressure at the occiput or over the parietal bones. The sensation is similar to the feel of pressing into a Ping-Pong ball and then releasing. Craniotabes may also be secondary to osteogenesis imperfecta, hydrocephalus, and syphilis. It is a normal finding in many newborns, especially near the suture lines, but it typically disappears within a few months of birth. Widening of the costochondral junctions results in a rachitic rosary, which feels like the beads of a rosary as the examiner’s fingers move along the costochondral junctions from rib to rib (Fig. 48-1). Growth plate widening is also responsible for the enlargement at the wrists and ankles. The horizontal depression along the lower anterior chest known as Harrison groove occurs from pulling of the softened ribs by the diaphragm during inspiration (Fig. 48-2). Softening of the ribs also impairs air movement and predisposes patients to atelectasis and pneumonia.
Table 48-3 CLINICAL FEATURES OF RICKETS
GENERAL
HEAD
CHEST
BACK
EXTREMITIES
HYPOCALCEMIC SYMPTOMS†
* These features are most commonly associated with the vitamin D deficiency disorders.
† These symptoms develop only in children with disorders that produce hypocalcemia (see Table 48-4).


There is some variation in the clinical presentation of rickets based on the etiology. Changes in the lower extremities tend to be the dominant feature in X-linked hypophosphatemic rickets. Symptoms secondary to hypocalcemia occur only in those forms of rickets associated with decreased serum calcium (Table 48-4).
The chief complaint in a child with rickets is quite variable. Many children present because of skeletal deformities, whereas others have difficulty walking owing to a combination of deformity and weakness. Other common presenting complaints include failure to thrive and symptomatic hypocalcemia (Chapter 565).
Radiology
Rachitic changes are most easily visualized on posteroanterior radiographs of the wrist, although characteristic rachitic changes can be seen at other growth plates (Figs. 48-3 and 48-4). Decreased calcification leads to thickening of the growth plate. The edge of the metaphysis loses its sharp border, which is described as fraying. The edge of the metaphysis changes from a convex or flat surface to a more concave surface. This change to a concave surface is termed cupping and is most easily seen at the distal ends of the radius, ulna, and fibula. There is widening of the distal end of the metaphysis, corresponding to the clinical observation of thickened wrists and ankles as well as the rachitic rosary. Other radiologic features include coarse trabeculation of the diaphysis and generalized rarefaction.


Diagnosis
Most cases of rickets are diagnosed based on the presence of classic radiographic abnormalities. The diagnosis is supported by physical examination findings (see Table 48-3) and a history and laboratory test results that are consistent with a specific etiology.
Clinical Evaluation
Because the majority of children with rickets have a nutritional deficiency, the initial evaluation should focus on a dietary history, emphasizing intake of vitamin D and calcium. Most children in industrialized nations receive vitamin D from formula, fortified milk, or vitamin supplements. Along with the amount, the exact composition of the formula or milk is pertinent, because rickets has occurred in children given products that are called milk (soy milk) but are deficient in vitamin D and/or minerals.
Cutaneous synthesis mediated by sunlight exposure is an important source of vitamin D. It is important to ask about time spent outside, sunscreen use, and clothing, especially if there may be a cultural reason for increased covering of the skin. Because winter sunlight is ineffective at stimulating cutaneous synthesis of vitamin D, the season is an additional consideration. Children with increased skin pigmentation are at increased risk for vitamin D deficiency because of decreased cutaneous synthesis.
The presence of maternal risk factors for nutritional vitamin D deficiency, including diet and sun exposure, is an important consideration when a neonate or young infant has rachitic findings, especially if the infant is breast-fed. Determining a child’s intake of dairy products, the main dietary source of calcium, provides a general sense of calcium intake. High dietary fiber can interfere with calcium absorption.
The child’s medication use is relevant, because certain medications such as the anticonvulsants phenobarbital and phenytoin increase degradation of vitamin D, and aluminum-containing antacids interfere with the absorption of phosphate.
Malabsorption of vitamin D is suggested by a history of liver or intestinal disease. Undiagnosed liver or intestinal disease should be suspected if the child has gastrointestinal (GI) symptoms, although occasionally rickets is the presenting complaint. Fat malabsorption is often associated with diarrhea or oily stools, and there may be signs or symptoms suggesting deficiencies of other fat-soluble vitamins (A, E, and K; Chapters 45, 49, and 50).
A history of renal disease (proteinuria, hematuria, urinary tract infections) is an additional significant consideration, given the importance of chronic renal failure as a cause of rickets. Polyuria can occur in children with chronic renal failure or Fanconi syndrome.
Children with rickets might have a history of dental caries, poor growth, delayed walking, waddling gait, pneumonia, and hypocalcemic symptoms.
The family history is critical, given the large number of genetic causes of rickets, although most of these causes are rare. Along with bone disease, it is important to inquire about leg deformities, difficulties with walking, or unexplained short stature, because some parents may be unaware of their diagnosis. Undiagnosed disease in the mother is not unusual in X-linked hypophosphatemia. A history of a unexplained sibling death during infancy may be present in the child with cystinosis, the most common cause of Fanconi syndrome in children.
The physical examination focuses on detecting manifestations of rickets (see Table 48-3). It is important to observe the child’s gait, auscultate the lungs to detect atelectasis or pneumonia, and plot the patient’s growth. Alopecia suggests vitamin D-dependent rickets type 2.
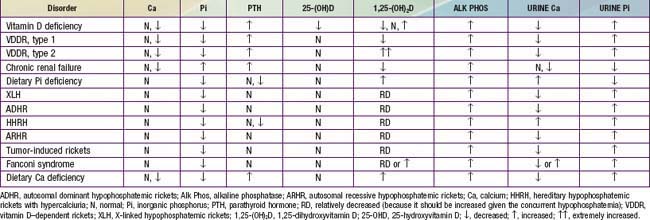
The initial laboratory tests in a child with rickets should include serum calcium, phosphorus, alkaline phosphatase, parathyroid hormone (PTH), 25-hydroxyvitamin D, 1,25-dihydroxyvitamin D3, creatinine, and electrolytes (see Table 48-4 for interpretation). Urinalysis is useful for detecting the glycosuria and aminoaciduria (positive dipstick for protein) seen with Fanconi syndrome. Evaluation of urinary excretion of calcium (24 hr collection for calcium or calcium:creatinine ratio) is helpful if hereditary hypophosphatemic rickets with hypercalciuria or Fanconi syndrome is suspected. Direct measurement of other fat-soluble vitamins (A, E, and K) or indirect assessment of deficiency (prothrombin time for vitamin K deficiency) is appropriate if malabsorption is a consideration.
Vitamin D Disorders
Vitamin D Physiology
Vitamin D can be synthesized in skin epithelial cells and therefore technically is not a vitamin. Cutaneous synthesis is normally the most important source of vitamin D and depends on the conversion of 7-dehydrochlesterol to vitamin D3 (3-cholecalciferol) by ultraviolet B radiation from the sun. The efficiency of this process is decreased by melanin; hence, more sun exposure is necessary for vitamin D synthesis in people with increased skin pigmentation. Measures to decrease sun exposure, such as covering the skin with clothing or applying sunscreen, also decrease vitamin D synthesis. Children who spend less time outside have reduced vitamin D synthesis. The winter sun away from the equator is ineffective at mediating vitamin D synthesis.
There are few natural dietary sources of vitamin D. Fish liver oils have a high vitamin D content. Other good dietary sources include fatty fish and egg yolks. Most children in industrialized countries receive vitamin D via fortified foods, especially formula and milk (both of which contain 400 IU/L) and some breakfast cereals and breads. Supplemental vitamin D may be vitamin D2 (which comes from plants or yeast) or vitamin D. Breast milk has a low vitamin D content, approximately 12-60 IU/L.
Vitamin D is transported bound to vitamin D–binding protein to the liver, where 25-hydroxlase converts vitamin D into 25-hydroxyvitamin D (25-D), the most abundant circulating form of vitamin D. Because there is little regulation of this liver hydroxylation step, measurement of 25-D is the standard method for determining a patient’s vitamin D status. The final step in activation occurs in the kidney, where 1α-hydroxylase adds a second hydroxyl group, resulting in 1,25-dihydroxyvitamin D (1,25-D). The 1α-hydroxylase is upregulated by PTH and hypophosphatemia; hyperphosphatemia and 1,25-D inhibit this enzyme. Most 1,25-D circulates bound to vitamin D–binding protein.
1,25-D acts by binding to an intracellular receptor, and the complex affects gene expression by interacting with vitamin D–response elements. In the intestine, this binding results in a marked increase in calcium absorption, which is highly dependent on 1,25-D. There is also an increase in phosphorus absorption, but this effect is less significant because most dietary phosphorus absorption is vitamin D independent. 1,25-D also has direct effects on bone, including mediating resorption. 1,25-D directly suppresses PTH secretion by the parathyroid gland, thus completing a negative feedback loop. PTH secretion is also suppressed by the increase in serum calcium mediated by 1,25-D. 1,25-D inhibits its own synthesis in the kidney and increases the synthesis of inactive metabolites.
Nutritional Vitamin D Deficiency
Vitamin D deficiency remains the most common cause of rickets globally and is prevalent, even in industrialized countries. Because vitamin D can be obtained from dietary sources or from cutaneous synthesis, most patients in industrialized countries have a combination of risk factors that lead to vitamin D deficiency.
Etiology
Vitamin D deficiency most commonly occurs in infancy due to a combination of poor intake and inadequate cutaneous synthesis. Transplacental transport of vitamin D, mostly 25-D, typically provides enough vitamin D for the 1st 2 mo of life unless there is severe maternal vitamin D deficiency. Infants who receive formula receive adequate vitamin D, even without cutaneous synthesis. Because of the low vitamin D content of breast milk, breast-fed infants rely on cutaneous synthesis or vitamin supplements. Cutaneous synthesis can be limited due to the ineffectiveness of the winter sun in stimulating vitamin D synthesis; avoidance of sunlight due to concerns about cancer, neighborhood safety, or cultural practices; and decreased cutaneous synthesis because of increased skin pigmentation.
The effect of skin pigmentation explains why most cases of nutritional rickets in the USA and northern Europe occur in breast-fed children of African descent or other dark-pigmented populations. The additional impact of the winter sun is supported by the fact that such infants more commonly present in the late winter or spring. In some groups, complete covering of infants or the practice of not taking infants outside has a significant role, explaining the occurrence of rickets in infants living in areas of abundant sunshine, such as the Middle East. Because the mothers of some infants can have the same risk factors, decreased maternal vitamin D can also contribute, both by leading to reduced vitamin D content in breast milk and by lessening transplacental delivery of vitamin D. Rickets caused by vitamin D deficiency can also be secondary to unconventional dietary practices, such as vegan diets that use unfortified soy milk or rice milk.
Clinical Manifestations
The clinical features are typical of rickets (see Table 48-3), with a significant minority presenting with symptoms of hypocalcemia; prolonged laryngospasm is occasionally fatal. These children have an increased risk of pneumonia and muscle weakness leading to a delay in motor development.
Laboratory Findings
Table 48-4 summarizes the principal laboratory findings. Hypocalcemia is a variable finding due to the actions of the elevated PTH to increase the serum calcium concentration. The hypophosphatemia is due to PTH-induced renal losses of phosphate, combined with a decrease in intestinal absorption.
The wide variation in 1,25-D levels (low, normal, or high) is secondary to the upregulation of renal 1α-hydroxylase due to concomitant hypophosphatemia and hyperparathyroidism. Because serum levels of 1,25-D are much lower than the levels of 25-D, even with low levels of 25-D there is still often enough 25-D present to act as a precursor for 1,25-D synthesis in the presence of an upregulated 1α-hydroxylase. The level of 1,25-D is only low when there is severe vitamin D deficiency.
Some patients have a metabolic acidosis secondary to PTH-induced renal bicarbonate wasting. There may also be generalized aminoaciduria.
Diagnosis and Differential Diagnosis
The diagnosis of nutritional vitamin D deficiency is based on the combination of a history of poor vitamin D intake and risk factors for decreased cutaneous synthesis, radiographic changes consistent with rickets, and typical laboratory findings (see Table 48-4). A normal PTH level almost never occurs with vitamin D deficiency and suggests a primary phosphate disorder.
Treatment
Children with nutritional vitamin D deficiency should receive vitamin D and adequate nutritional intake of calcium and phosphorus. There are 2 strategies for administration of vitamin D. With stoss therapy, 300,000-600,000 IU of vitamin D are administered orally or intramuscularly as 2-4 doses over 1 day. Because the doses are observed, stoss therapy is ideal in situations where adherence to therapy is questionable. The alternative is daily, high-dose vitamin D, with doses ranging from 2,000-5,000 IU/day over 4-6 wk. Either strategy should be followed by daily vitamin D intake of 400 IU/day if <1 yr old or 600 IU/day if >1 yr, typically given as a multivitamin. It is important to ensure that children receive adequate dietary calcium and phosphorus; this dietary intake is usually provided by milk, formula, and other dairy products.
Children who have symptomatic hypocalcemia might need intravenous calcium acutely, followed by oral calcium supplements, which typically can be tapered over 2-6 wk in children who receive adequate dietary calcium. Transient use of intravenous or oral 1,25-D (calcitriol) is often helpful in reversing hypocalcemia in the acute phase by providing active vitamin D during the delay as supplemental vitamin D is converted to active vitamin D. Calcitriol doses are typically 0.05 µg/kg/day. Intravenous calcium is initially given as an acute bolus for symptomatic hypocalcemia (20 mg/kg of calcium chloride or 100 mg/kg of calcium gluconate). Some patients require a continuous intravenous calcium drip, titrated to maintain the desired serum calcium level. These patients should transition to enteral calcium, and most infants require approximately 1,000 mg of elemental calcium.
Prognosis
Most children have an excellent response to treatment, with radiologic healing occurring within a few months. Laboratory test results should also normalize rapidly. Many of the bone malformations improve dramatically, but children with severe disease can have permanent deformities and short stature. Rarely, patients benefit from orthopedic intervention for leg deformities, although this is generally not done until the metabolic bone disease has healed, there is clear evidence that the deformity will not self-resolve, and the deformity is causing functional problems.
Congenital Vitamin D Deficiency
Congenital rickets is quite rare in industrialized countries and occurs when there is severe maternal vitamin D deficiency during pregnancy. Maternal risk factors include poor dietary intake of vitamin D, lack of adequate sun exposure, and closely spaced pregnancies. These newborns can have symptomatic hypocalcemia, intrauterine growth retardation, and decreased bone ossification, along with classic rachitic changes. More subtle maternal vitamin D deficiency can have an adverse effect on neonatal bone density and birthweight, cause a defect in dental enamel, and predispose infants to neonatal hypocalcemic tetany. Treatment of congenital rickets includes vitamin D supplementation and adequate intake of calcium and phosphorus. Use of prenatal vitamins containing vitamin D prevents this entity.
Secondary Vitamin D Deficiency
Etiology
Along with inadequate intake, vitamin D deficiency can develop due to inadequate absorption, decreased hydroxylation in the liver, and increased degradation. Because vitamin D is fat-soluble, its absorption may be decreased in patients with a variety of liver and GI diseases, including cholestatic liver disease, defects in bile acid metabolism, cystic fibrosis and other causes of pancreatic dysfunction, celiac disease, and Crohn disease. Malabsorption of vitamin D can also occur with intestinal lymphangiectasia and after intestinal resection.
Severe liver disease, which is usually also associated with malabsorption, can cause a decrease in 25-D formation due to insufficient enzyme activity. Because of the large reserve of 25-hydroxlase activity in the liver, vitamin D deficiency due to liver disease usually requires a loss of >90% of liver function. A variety of medications increase the degradation of vitamin D by inducing the cytochrome P450 (CYP) system. Rickets due to vitamin D deficiency can develop in children receiving anticonvulsants such as phenobarbital or phenytoin or antituberculosis medications such as isoniazid or rifampin.
Treatment
Treatment of vitamin D deficiency due to malabsorption requires high doses of vitamin D. Because of its better absorption, 25-D (25-50 µg/day or 5-7 µg/kg/day) is superior to vitamin D3. The dose is adjusted based on monitoring of serum levels of 25-D. Alternatively, patients may be treated with 1,25-D, which also is better absorbed in the presence of fat malabsorption, or with parenteral vitamin D. Children with rickets due to increased degradation of vitamin D by the CYP system require the same acute therapy as indicated for nutritional deficiency (discussed earlier), followed by long-term administration of high doses of vitamin D (e.g., 1,000 IU/day), with dosing titrated based on serum levels of 25-D. Some patients require as much as 4,000 IU/day.
Vitamin D–Dependent Rickets, Type 1
Children with vitamin D–dependent rickets type 1, an autosomal recessive disorder, have mutations in the gene encoding renal 1α-hydroxylase, preventing conversion of 25-D into 1,25-D. These patients normally present during the 1st 2 yr of life and can have any of the classic features of rickets (see Table 48-3), including symptomatic hypocalcemia. They have normal levels of 25-D but low levels of 1,25-D (see Table 48-4). Occasionally, 1,25-D levels are at the lower limit of normal, inappropriately low given the high PTH and low serum phosphorus levels, both of which should increase the activity of renal 1α-hydroxylase and cause elevated levels of 1,25-D. As in nutritional vitamin D deficiency, renal tubular dysfunction can cause a metabolic acidosis and generalized aminoaciduria.
Treatment
These patients respond to long-term treatment with 1,25-D (calcitriol). Initial doses are 0.25-2 µg/day, and lower doses are used once the rickets has healed. Especially during initial therapy, it is important to ensure adequate intake of calcium. The dose of calcitriol is adjusted to maintain a low-normal serum calcium level, a normal serum phosphorus level, and a high-normal serum PTH level. Targeting a low-normal calcium concentration and a high-normal PTH level avoids excessive dosing of calcitriol, which can cause hypercalciuria and nephrocalcinosis. Hence, patient monitoring includes periodic assessment of urinary calcium excretion, with a target of <4 mg/kg/day.
Vitamin D–Dependent Rickets, Type 2
Patients with vitamin D–dependent rickets type 2 have mutations in the gene encoding the vitamin D receptor, preventing a normal physiologic response to 1,25-D. Levels of 1,25-D are extremely elevated in this autosomal recessive disorder (see Table 48-4). Most patients present during infancy, although rickets in less severely affected patients might not be diagnosed until adulthood. Less-severe disease is associated with a partially functional vitamin D receptor. Approximately 50-70% of children have alopecia, which tends to be associated with a more severe form of the disease and can range from alopecia areata to alopecia totalis. Epidermal cysts are a less common manifestation.
Treatment
Some patients respond to extremely high doses of vitamin D2, 25-D or 1,25-D, especially patients without alopecia. This response is due to a partially functional vitamin D receptor. All patients with this disorder should be given a 3-6 mo trial of high-dose vitamin D and oral calcium. The initial dose of 1,25-D should be 2 µg/day, but some patients require doses as high as 50-60 µg/day. Calcium doses are 1,000-3,000 mg/day. Patients who do not respond to high-dose vitamin D may be treated with long-term intravenous calcium, with possible transition to very high dose oral calcium supplements. Treatment of patients who do not respond to vitamin D is difficult.
Chronic Renal Failure (Chapter 529.2)
With chronic renal failure, there is decreased activity of 1α-hydroxylase in the kidney, leading to diminished production of 1,25-D. In chronic renal failure, unlike the other causes of vitamin D deficiency, patients have hyperphosphatemia as a result of decreased renal excretion (see Table 48-4).
Treatment
Therapy requires the use of a form of vitamin D that can act without 1-hydroxylation by the kidney (calcitriol), which both permits adequate absorption of calcium and directly suppresses the parathyroid gland. Because hyperphosphatemia is a stimulus for PTH secretion, normalization of the serum phosphorus level via a combination of dietary phosphorus restriction and the use of oral phosphate binders is as important as the use of activated vitamin D.
Calcium Deficiency
Pathophysiology
Rickets secondary to inadequate dietary calcium is a significant problem in some countries in Africa, although there are cases in other regions of the world, including industrialized countries. Because breast milk and formula are excellent sources of calcium, this form of rickets develops after children have been weaned from breast milk or formula and is more likely to occur in children who are weaned early. Rickets develops because the diet has low calcium content, typically <200 mg/day. There is little intake of dairy products or other sources of calcium. In addition, because of reliance on grains and green leafy vegetables, the diet may be high in phytate, oxalate, and phosphate, which decrease absorption of dietary calcium. In industrialized countries, rickets due to calcium deficiency can occur in children who consume an unconventional diet. Examples include children with milk allergy who have low dietary calcium and children who transition from formula or breast milk to juice, soda, or a calcium-poor soy drink, without an alternative source of dietary calcium.
This type of rickets can develop in children who receive intravenous nutrition without adequate calcium. Malabsorption of calcium can occur in celiac disease, intestinal abetalipoproteinemia, and after small bowel resection. There may be concurrent malabsorption of vitamin D.
Clinical Manifestations
Children have the classic signs and symptoms of rickets (see Table 48-3). Presentation can occur during infancy or early childhood, although some cases are diagnosed in teenagers. Because calcium deficiency occurs after the cessation of breast-feeding, it tends to occur later than the nutritional vitamin D deficiency that is associated with breast-feeding. In Nigeria, nutritional vitamin D deficiency is most common at 4-15 mo of age, whereas calcium-deficiency rickets typically occurs at 15-25 mo of age.
Diagnosis
Laboratory findings include increased levels of alkaline phosphatase, PTH, and 1,25-D (see Table 48-4). Calcium levels may be normal or low, although symptomatic hypocalcemia is uncommon. There is decreased urinary excretion of calcium, and serum phosphorus levels may be low due to renal wasting of phosphate from secondary hyperparathyroidism, which can also cause aminoaciduria. In some children, there is coexisting nutritional vitamin D deficiency, with low 25-D levels.
Treatment
Treatment focuses on providing adequate calcium, typically as a dietary supplement (doses of 700 [1-3 yr age], 1,000 [4-8 yr age], 1,300 [9-18 yr age] mg/day of elemental calcium are effective). Vitamin D supplementation is necessary if there is concurrent vitamin D deficiency (discussed earlier). Prevention strategies include discouraging early cessation of breast-feeding and increasing dietary sources of calcium. In countries such as Kenya, where many children have diets high in cereal with negligible intake of cow’s milk, school-based milk programs have been effective in reducing the prevalence of rickets.
Phosphorous Deficiency
Inadequate Intake
With the exception of starvation or severe anorexia, it is almost impossible to have a diet that is deficient in phosphorus, because phosphorus is present in most foods. Decreased phosphorus absorption can occur in diseases associated with malabsorption (celiac disease, cystic fibrosis, cholestatic liver disease), but if rickets develops, the primary problem is usually malabsorption of vitamin D and/or calcium.
Isolated malabsorption of phosphorus occurs in patients with long-term use of aluminum-containing antacids. These compounds are very effective at chelating phosphate in the GI tract, leading to decreased absorption. This decreased absorption results in hypophosphatemia with secondary osteomalacia in adults and rickets in children. This entity responds to discontinuation of the antacid and short-term phosphorus supplementation.
Phosphatonin
Phosphatonin is a humoral mediator that decreases renal tubular reabsorption of phosphate and therefore decreases serum phosphorus. Phosphatonin also decreases the activity of renal 1α-hydroxylase, resulting in a decrease in the production of 1,25-D. Fibroblast growth factor–23 (FGF-23) is the most well characterized phosphatonin, but there are a number of other putative phosphatonins (discussed later). Increased levels of phosphatonin cause many of the phosphate-wasting diseases (see Table 48-2).
X-Linked Hypophosphatemic Rickets
Among the genetic disorders causing rickets due to hypophosphatemia, X-linked hypophosphatemic rickets (XLH) is the most common, with a prevalence of 1/20,000. The defective gene is on the X chromosome, but female carriers are affected, so it is an X-linked dominant disorder.
Pathophysiology
The defective gene is called PHEX because it is a PHosphate-regulating gene with homology to Endopeptidases on the X chromosome. The product of this gene appears to have an indirect role in inactivating the phosphatonin FGF-23. Mutations in the PHEX gene lead to increased levels of FGF-23. Because the actions of FGF-23 include inhibition of phosphate reabsorption in the proximal tubule, phosphate excretion is increased. FGF-23 also inhibits renal 1α-hydroxylase, leading to decreased production of 1,25-D.
Clinical Manifestations
These patients have rickets, but abnormalities of the lower extremities and poor growth are the dominant features. Delayed dentition and tooth abscesses are also common. Some patients have hypophosphatemia and short stature without clinically evident bone disease.
Laboratory Findings
Patients have high renal excretion of phosphate, hypophosphatemia, and increased alkaline phosphatase; PTH and serum calcium levels are normal (see Table 48-4). Hypophosphatemia normally upregulates renal 1α-hydroxylase and should lead to an increase in 1,25-D, but these patients have low or inappropriately normal levels of 1,25-D.
Treatment
Patients respond well to a combination of oral phosphorus and 1,25-D (calcitriol). The daily need for phosphorus supplementation is 1-3 g of elemental phosphorus divided into 4-5 doses. Frequent dosing helps to prevent prolonged decrements in serum phosphorus because there is a rapid decline after each dose. In addition, frequent dosing decreases diarrhea, a complication of high-dose oral phosphorus. Calcitrol is administered 30-70 ng/kg/day divided into 2 doses.
Complications of treatment occur when there is not an adequate balance between phosphorus supplementation and calcitriol. Excess phosphorus, by decreasing enteral calcium absorption, leads to secondary hyperparathyroidism, with worsening of the bone lesions. In contrast, excess calcitriol causes hypercalciuria and nephrocalcinosis and can even cause hypercalcemia. Hence, laboratory monitoring of treatment includes serum calcium, phosphorus, alkaline phosphatase, PTH, and urinary calcium, as well as periodic renal ultrasounds to evaluate patients for nephrocalcinosis. Because of variation in the serum phosphorus level and the importance of avoiding excessive phosphorus dosing, normalization of alkaline phosphatase levels is a more useful method of assessing the therapeutic response than measuring serum phosphorus. For children with significant short stature, growth hormone is an effective option. Children with severe deformities might need osteotomies, but these procedures should be done only when treatment has led to resolution of the bone disease.
Prognosis
The response to therapy is usually good, although frequent dosing can lead to problems with compliance. Girls generally have less severe disease than boys, probably due to the X-linked inheritance. Short stature can persist despite healing of the rickets. Adults generally do well with less aggressive treatment, and some receive calcitriol alone. Adults with bone pain or other symptoms improve with oral phosphorus supplementation and calcitriol.
Autosomal Dominant Hypophosphatemic Rickets
Autosomal dominant hypophosphatemic rickets (ADHR) is much less common than XLH. There is incomplete penetrance and variable age of onset. Patients with ADHR have a mutation in the gene encoding FGF-23. The mutation prevents degradation of FGF-23 by proteases, leading to increased levels of this phosphatonin. The actions of FGF-23 include decreased reabsorption of phosphate in the renal proximal tubule, which results in hypophosphatemia, and inhibition of the 1α-hydroxylase in the kidney, causing a decrease in 1,25-D synthesis.
In ADHR, as in XLH, abnormal laboratory findings are hypophosphatemia, an elevated alkaline phosphatase level, and a low or inappropriately normal 1,25-D level (see Table 48-4). Treatment is similar to the approach used in XLH.
Autosomal Recessive Hypophosphatemic Rickets
Autosomal recessive hypophosphatemic rickets is an extremely rare disorder due to mutations in the gene encoding dentin matrix protein 1, which results in elevated levels of FGF-23, leading to renal phosphate wasting, hypophosphatemia, and low or inappropriately normal levels of 1.,25-D. Treatment is similar to the approach used in XLH.
Hereditary Hypophosphatemic Rickets with Hypercalciuria
Hereditary hypophosphatemic rickets with hypercalciuria (HHRH) is a rare disorder that is mainly described in the Middle East.
Pathophysiology
This autosomal recessive disorder is due to mutations in the gene for a sodium-phosphate cotransporter in the proximal tubule. The renal phosphate leak causes hypophosphatemia, which then stimulates production of 1,25-D. The high level of 1,25-D increases intestinal absorption of calcium, suppressing PTH. Hypercalciuria ensues due to the high absorption of calcium and the low level of PTH, which normally decreases renal excretion of calcium.
Clinical Manifestations
The dominant symptoms are rachitic leg abnormalities (see Table 48-3), muscle weakness, and bone pain. Patients can have short stature, with a disproportionate decrease in the length of the lower extremities. The severity of the disease varies, and some family members have no evidence of rickets but have kidney stones secondary to hypercalciuria.
Laboratory Findings
Laboratory findings include hypophosphatemia, renal phosphate wasting, elevated serum alkaline phosphatase levels, and elevated 1,25-D levels. PTH levels are low (see Table 48-4).
Treatment
Therapy relies on oral phosphorus replacement (1-2.5 g/day of elemental phosphorus in 5 divided oral doses). Treatment of the hypophosphatemia decreases serum levels of 1,25-D and corrects the hypercalciuria. The response to therapy is usually excellent, with resolution of pain, weakness, and radiographic evidence of rickets.
Overproduction of Phosphatonin
Tumor-induced osteomalacia is more common in adults than in children, where it can produce classic rachitic findings. Most tumors are mesenchymal in origin and are usually benign, small, and located in bone. These tumors secrete a number of different putative phosphatonins (FGF-23, frizzled-related protein 4, and matrix extracellular phosphoglycoprotein); different tumors secrete different phosphatonins or combinations of phosphatonins. These phosphatonins produce a biochemical phenotype that is similar to XLH, including urinary phosphate wasting, hypophosphatemia, elevated alkaline phosphatase levels, and low or inappropriately normal 1,25-D levels (see Table 48-4). Curative treatment is excision of the tumor. If the tumor cannot be removed, treatment is identical to that used for XLH.
Renal phosphate wasting leading to hypophosphatemia and rickets (or osteomalacia in adults) is a potential complication in McCune-Albright syndrome, an entity that includes the triad of polyostotic fibrous dysplasia, hyperpigmented macules, and polyendocrinopathy (Chapter 556.6). Affected patients have inappropriately low levels of 1,25-D and elevated levels of alkaline phosphatase. The renal phosphate wasting and inhibition of 1,25-D synthesis are related to the polyostotic fibrous dysplasia. Patients have elevated levels of the phosphatonin FGF-23, presumably produced by the dysplastic bone. Hypophosphatemic rickets can also occur in children with isolated polyostotic fibrous dysplasia. Although it is rarely possible, removal of the abnormal bone can cure this disorder in children with McCune-Albright syndrome. Most patients receive the same treatment as children with XLH. Bisphosphonate treatment decreases the pain and fracture risk associated with the bone lesions.
Rickets is an unusual complication of epidermal nevus syndrome (Chapter 643). Patients have hypophosphatemic rickets due to renal phosphate wasting and also have an inappropriately normal or low level of 1,25-D due to excessive production of FGF-23. The timing of presentation with rickets varies from infancy to early adolescence. Resolution of hypophosphatemia and rickets has occurred after excision of the epidermal nevi in some patients but not in others. In most cases, the skin lesions are too extensive to be removed, necessitating treatment with phosphorus supplementation and 1,25-D. Rickets due to phosphate wasting is an extremely rare complication in children with neurofibromatosis (Chapter 589.1), again presumably due to the production of a phosphatonin.
Fanconi Syndrome
Fanconi syndrome is secondary to generalized dysfunction of the renal proximal tubule (Chapter 523.1). There are renal losses of phosphate, amino acids, bicarbonate, glucose, urate, and other molecules that are normally reabsorbed in the proximal tubule. Some patients have partial dysfunction, with less generalized losses. The most clinically relevant consequences are hypophosphatemia due to phosphate losses and proximal renal tubular acidosis due to bicarbonate losses. Patients have rickets as a result of hypophosphatemia, with exacerbation from the chronic metabolic acidosis, which causes bone dissolution. Failure to thrive is a consequence of both rickets and renal tubular acidosis. Treatment is dictated by the etiology (Chapters 523.1 and 523.4).
Dent Disease (Chapter 525.3)
Dent disease is an X-linked disorder usually caused by mutations in the gene encoding a chloride channel that is expressed in the kidney. Some patients have mutations in the OCRL 1 gene, which can also cause Lowe syndrome (Chapter 523.1). Affected males have variable manifestations, including hematuria, nephrolithiasis, nephrocalcinosis, rickets, and chronic renal failure. Almost all patients have low molecular weight proteinuria and hypercalciuria. Other, less universal abnormalities are aminoaciduria, glycosuria, hypophosphatemia, and hypokalemia. Rickets occurs in approximately 25% of patients, and it responds to oral phosphorus supplements. Some patients also need 1,25-D, but this treatment should be used cautiously because it can worsen the hypercalciuria.
Rickets of Prematurity (Chapter 100)
Rickets in very low birthweight infants has become a significant problem, as the survival rate for this group of infants has increased.
Pathogenesis
The transfer of calcium and phosphorus from mother to fetus occurs throughout pregnancy, but 80% occurs during the 3rd trimester. Premature birth interrupts this process, with rickets developing when the premature infant does not have an adequate supply of calcium and phosphorus to support mineralization of the growing skeleton.
Most cases of rickets of prematurity occur in infants with a birthweight <1,000 g. It is more likely to develop in infants with lower birthweight and younger gestational age. Rickets occurs because unsupplemented breast milk and standard infant formula do not contain enough calcium and phosphorus to supply the needs of the premature infant. Other risk factors include cholestatic jaundice, a complicated neonatal course, prolonged use of parenteral nutrition, the use of soy formula, and medications such as diuretics and corticosteroids.
Clinical Manifestations
Rickets of prematurity occurs 1-4 mo after birth. Infants can have nontraumatic fractures, especially of the legs, arms, and ribs. Most fractures are not suspected clinically. Because fractures and softening of the ribs lead to decreased chest compliance, some infants have respiratory distress due to atelectasis and poor ventilation. This rachitic respiratory distress usually develops >5 wk after birth, distinguishing it from the early-onset respiratory disease of premature infants. These infants have poor linear growth, with negative effects on growth persisting beyond 1 yr of age. An additional long-term effect is enamel hypoplasia. Poor bone mineralization can contribute to dolichocephaly. There may be classic rachitic findings, such as frontal bossing, rachitic rosary, craniotabes, and widened wrists and ankles (see Table 48-3). Most infants with rickets of prematurity have no clinical manifestations, and the diagnosis is based on radiographic and laboratory findings.
Laboratory Findings
Due to inadequate intake, the serum phosphorus level is low or low-normal in rickets of prematurity. The renal response is appropriate, with conservation of phosphate leading to a low urine phosphate level; the tubular reabsorption of phosphate is >95%. Most patients have normal levels of 25-D, unless there has been inadequate intake or poor absorption (discussed earlier). The hypophosphatemia stimulates renal 1α-hydroxylase, so levels of 1,25-D are high or high-normal. These high levels can contribute to bone demineralization, because 1,25-D stimulates bone resorption. Serum levels of calcium are low, normal, or high, and patients often have hypercalciuria. Elevated serum calcium levels and hypercalciuria are secondary to increased intestinal absorption and bone dissolution due to elevation of 1,25-D levels and the inability to deposit calcium in bone because of an inadequate phosphorus supply. The hypercalciuria indicates that phosphorus is the limiting nutrient for bone mineralization, although increased provision of phosphorus alone often cannot correct the mineralization defect; increased calcium is also necessary. Hence, there is an inadequate supply of calcium and phosphorus, but the deficiency in phosphorus is greater.
Alkaline phosphatase levels are often elevated, but some affected infants have normal levels. In some instances, normal alkaline phosphatase levels may be secondary to resolution of the bone demineralization because of an adequate mineral supply despite the continued presence of radiologic changes, which take longer to resolve. However, alkaline phosphatase levels may be normal despite active disease. No single blood test is 100% sensitive for the diagnosis of rickets. The diagnosis should be suspected in infants with an alkaline phosphatase level that is >5-6 times the upper limit of normal for adults (unless there is concomitant liver disease) or a phosphorus level <5.6 mg/dL. The diagnosis is confirmed by radiologic evidence of rickets, which is best seen on films of the wrists and ankles. Films of the arms and legs might reveal fractures. The rachitic rosary may be visible on chest x-ray. Unfortunately, x-rays cannot show early demineralization of bone because changes are not evident until there is >20-30% reduction in the bone mineral content.
Diagnosis
Because many premature infants have no overt clinical manifestations of rickets, screening tests are recommended. These tests should include weekly measurements of calcium, phosphorus, and alkaline phosphatase. Periodic measurement of the serum bicarbonate concentration is also important, because metabolic acidosis causes dissolution of bone. At least 1 screening x-ray for rickets at 6-8 wk of age is appropriate in infants who are at high risk for rickets; additional films may be indicated in very high risk infants.
Prevention
Provision of adequate amounts of calcium, phosphorus, and vitamin D significantly decreases the risk of rickets of prematurity. Parenteral nutrition is often necessary initially in very premature infants. In the past, adequate parenteral calcium and phosphorus delivery was difficult because of limits secondary to insolubility of these ions when their concentrations were increased. Current amino acid preparations allow higher concentrations of calcium and phosphate, decreasing the risk of rickets. Early transition to enteral feedings is also helpful. These infants should receive either human milk fortified with calcium and phosphorus or preterm infant formula, which has higher concentrations of calcium and phosphorus than standard formula. Soy formula should be avoided because there is decreased bioavailability of calcium and phosphorus. Increased mineral feedings should continue until the infant weighs 3-3.5 kg. These infants should also receive approximately 400 IU/day of vitamin D via formula and vitamin supplements.
Treatment
Therapy for rickets of prematurity focuses on ensuring adequate delivery of calcium, phosphorus, and vitamin D. If mineral delivery has been good and there is no evidence of healing, then it is important to screen for vitamin D deficiency by measuring serum 25-D. Measurement of PTH, 1,25-D, and urinary calcium and phosphorus may be helpful in some cases.
Distal Renal Tubular Acidosis (Chapter 523)
Distal renal tubular acidosis usually manifests with failure to thrive. Patients have a metabolic acidosis with an inability to acidify the urine appropriately. Hypercalciuria and nephrocalcinosis are typically present. There are many possible etiologies, including autosomal recessive and autosomal dominant forms. Rickets is variable, and it responds to alkali therapy (see Fig. 48-4).
Hypervitaminosis D
Etiology
Hypervitaminosis D is secondary to excessive intake of vitamin D. It can occur with long-term high intake or with a substantial, acute ingestion (see Table 48-1). Most cases are secondary to misuse of prescribed or over-the-counter vitamin D supplements, but other cases have been secondary to accidental overfortification of milk, contamination of table sugar, and inadvertent use of vitamin D supplements as cooking oil. The recommended upper limits for long-term vitamin D intake are 1,000 IU for children <1 year old and 2,000 IU for older children and adults. Hypervitaminosis D can also result from excessive intake of synthetic vitamin D analogs (25-D, 1,25-D). Vitamin D intoxication is never secondary to excessive exposure to sunlight, probably because ultraviolet irradiation can transform vitamin D3 and its precursor into inactive metabolites.
Pathogenesis
Although vitamin D increases intestinal absorption of calcium, the dominant mechanism of the hypercalcemia is excessive bone resorption.
Clinical Manifestations
The signs and symptoms of vitamin D intoxication are secondary to hypercalcemia. GI manifestations include nausea, vomiting, poor feeding, constipation, abdominal pain, and pancreatitis. Possible cardiac findings are hypertension, decreased Q-T interval, and arrhythmias. The central nervous system effects of hypercalcemia include lethargy, hypotonia, confusion, disorientation, depression, psychosis, hallucinations, and coma. Hypercalcemia impairs renal concentrating mechanisms, which can lead to polyuria, dehydration, and hypernatremia. Hypercalcemia can also lead to acute renal failure, nephrolithiasis, and nephrocalcinosis, which can result in chronic renal insufficiency. Deaths are usually associated with arrhythmias or dehydration.
Laboratory Findings
The classic findings in vitamin D intoxication are hypercalcemia and extremely elevated levels of 25-D (>150 ng/mL). Hyperphosphatemia is also common. PTH levels are appropriately decreased owing to hypercalcemia. Hypercalciuria is universally present and can lead to nephrocalcinosis, which is visible on renal ultrasound. Hypercalcemia and nephrocalcinosis can lead to renal insufficiency.
Surprisingly, levels of 1,25-D are usually normal. This may be due to downregulation of renal 1α-hydroxylase by the combination of low PTH, hyperphosphatemia, and a direct effect of 1,25-D. There is evidence indicating that the level of free 1,25-D may be high, owing to displacement from vitamin D–binding proteins by 25-D. Nephrocalcinosis is often visible on ultrasound or CT scan. Anemia is sometimes present; the mechanism is unknown.
Diagnosis and Differential Diagnosis
The diagnosis is based on the presence of hypercalcemia and an elevated serum 25-D level, although children with excess intake of 1,25-D or another synthetic vitamin D preparation have normal levels of 25-D. With careful sleuthing, there is usually a history of excess intake of vitamin D, although in some situations (overfortification of milk by a dairy) the patient and family may be unaware.
The differential diagnosis of vitamin D intoxication focuses on other causes of hypercalcemia. Hyperparathyroidism produces hypophosphatemia, whereas vitamin D intoxication usually causes hyperphosphatemia. Williams syndrome is often suggested by phenotypic features and accompanying cardiac disease. Subcutaneous fat necrosis is a common cause of hypercalcemia in young infants; skin findings are usually present. The hypercalcemia of familial benign hypocalciuric hypercalcemia is mild, asymptomatic, and associated with hypocalciuria. Hypercalcemia of malignancy is an important consideration. High intake of calcium can also cause hypercalcemia, especially in the presence of renal insufficiency. Questioning about calcium intake should be part of the history in a patient with hypercalcemia. Occasionally, patients are intentionally taking high doses of calcium and vitamin D.
Treatment
The treatment of vitamin D intoxication focuses on control of hypercalcemia. Many patients with hypercalcemia are dehydrated as a result of polyuria from nephrogenic diabetes insipidus, poor oral intake, and vomiting. Rehydration lowers the serum calcium level via dilution and corrects prerenal azotemia. The resultant increased urine output increases urinary calcium excretion. Urinary calcium excretion is also increased by high urinary sodium excretion. The mainstay of the initial treatment is aggressive therapy with normal saline, often in conjunction with a loop diuretic to further increase calcium excretion.
Normal saline, with or without a loop diuretic, is often adequate for treating mild or moderate hypercalcemia. More significant hypercalcemia usually requires other therapies. Glucocorticoids decrease intestinal absorption of calcium by blocking the action of 1,25-D. There is also a decrease in the levels of 25-D and 1,25-D. The usual dosage of prednisone is 1-2 mg/kg/24 hr.
Calcitonin, which lowers calcium by inhibiting bone resorption, is a useful adjunct, but its effect is usually not dramatic. There is an excellent response to intravenous or oral bisphosphonates in vitamin D intoxication. Bisphosphonates inhibit bone resorption through their effects on osteoclasts. Hemodialysis using a low or 0 dialysate calcium can rapidly lower serum calcium in patients with severe hypercalcemia that is refractory to other measures.
Along with controlling hypercalcemia, it is imperative to eliminate the source of excess vitamin D. Additional sources of vitamin D such as multivitamins and fortified foods should be eliminated or reduced. Avoidance of sun exposure, including the use of sunscreen, is prudent. The patient should also restrict calcium intake.
Abrams SA. Dietary guidelines for calcium and vitamin D: a new era. Pediatrics. 2011;127(3):566-568.
Ariceta G, Langman CB. Growth in X-linked hypophosphatemic rickets. Eur J Pediatr. 2007;166:303-309.
Cole CR, Grant FK, Tangpricha V, et al. 25-hydroxyvitamin D status of healthy, low-income, minority children in Atlanta, Georgia. Pediatrics. 2010;125:633-639.
DiMeglio LA. Bisphosphonate therapy for fibrous dysplasia. Pediatr Endocrinol Rev Suppl. 2007;4:440-445.
Doneray H, Ozkan B, Caner I, et al. Intragastric alendronate therapy in two infants with vitamin D intoxication: a new method. Clin Toxicol (Phila). 2008;46:300-302.
Dong Y, Pollock N, Stallman-Jorgensen IS, et al. Low 25-hydroxyvitamin D levels in adolescents: race, season, adiposity, physical activity, and fitness. Pediatrics. 2010;125:1104-1111.
Feng JQ, Ward LM, Liu S, et al. Loss of DMP1 causes rickets and osteomalacia and identifies a role for osteocytes in mineral metabolism. Nat Genet. 2006;38:1310-1315.
Garabedian M. Regulation of phosphate homeostasis in infants, children, and adolescents, and the role of phosphatonins in this process. Curr Opin Pediatr. 2007;19:488-491.
Greer FR. Defining vitamin D deficiency in children: beyond 25-OH vitamin D serum concentrations. Pediatrics. 2009;124:1471-1473.
Grey V, Atkinson S, Drury D, et al. Prevalence of low bone mass and deficiencies of vitamins D and K in pediatric patients with cystic fibrosis from 3 Canadian centers. Pediatrics. 2008;122:1014-1020.
Iyer P, Diamond FBJr. Shedding light on hypovitaminosis D and rickets. Adv Pediatr. 2007;54:115-133.
Kumar J, Muntner P, Kaskel FJ, et al. Prevalence and associations of 25-hydroxyvitamin D deficiency in US children: NHANES 2001–2004. Pediatrics. 2009;124:e362-e370.
Lerch C, Meissner T: Interventions for the prevention of nutritional rickets in term born children, Cochrane Database Sys Rev (4):CD006164, 2007.
Misra M, Pacaud D, Petryk A, et al. Vitamin D deficiency in children and its management: review of current knowledge and recommendations. Pediatrics. 2008;122:398-417.
Nguyen M, Boutignon H, Mallet E, et al. Infantile hypercalcemia and hypercalciuria: new insights into a vitamin D-dependent mechanism and response to ketoconazole treatment. J Pediatr. 2010;157:296-302.
Pearce SHS, Cheetham TD. Diagnosis and management of vitamin D deficiency. BMJ. 2010;340:142-146.
Perrine CG, Sharma AJ, Jefferds MED, et al. Adherence to vitamin D recommendations among US infants. Pediatrics. 2010;125:627-632.
Pettifor JM. What’s new in hypophosphataemic rickets? Eur J Pediatr. 2008;167:493-499.
Rosen CJ. Vitamin D insufficiency. N Engl J Med. 2011;364(3):248-254.
Ross AC, Manson JE, Abrams SA, et al. The 2011 report on dietary reference intakes for calcium and vitamin D from the Institute of Medicine: what clinicians need to know. J Clin Endocrinol Metab. 2011;96(1):53-58.
Sahota O. Reducing the risk of fractures with calcium and vitamin D. BMJ. 2010;340:109-110.
Saintonge S, Bang H, Gerber LM. Implications of a new definition of vitamin D deficiency in a multiracial us adolescent population: The National Health and Nutrition Examination Survey III. Pediatrics. 2009;123:797-803.
Shaikh A, Berndt T, Kumar R. Regulation of phosphate homeostasis by the phosphatonins and other novel mediators. Pediatr Nephrol. 2008;23:1203-1210.
Shaw N. Vitamin D and bone health in children. BMJ. 2011;342:239-240.
Shellhaas RA, Barks AK, Joshi SM. Prevalence and risk factors for vitamin D insufficiency among children with epilepsy. Pediatr Neurol. 2010;42:422-426.
Wagner CL, Greer FR, American Academy of Pediatrics Section on Breastfeeding; American Academy of Pediatrics Committee on Nutrition. Prevention of rickets and vitamin D deficiency in infants, children, and adolescents. Pediatrics. 2008;122(5):1142-1152.
Winzenberg T, Powell S, Shaw KA, et al. Effects of vitamin D supplementation on bone density in healty children: systematic review and meta-analysis. BMJ. 2011;342:267.