TEMPORAL AND INFRATEMPORAL FOSSAE
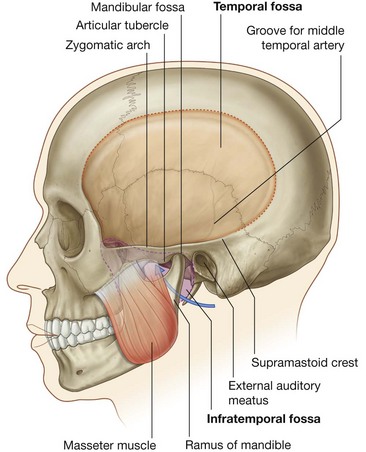
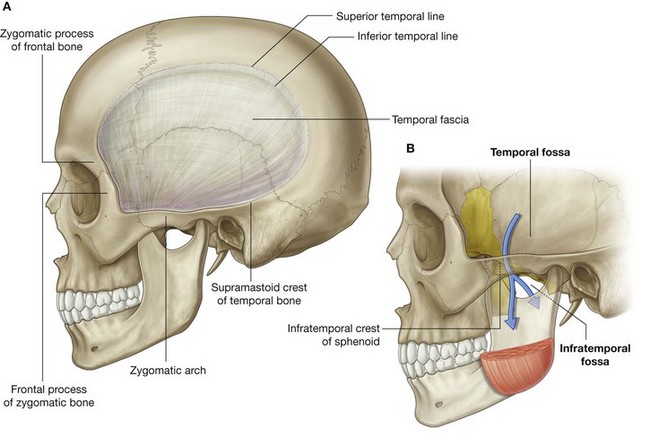
The temporal and infratemporal fossae are interconnected spaces on the lateral side of the head (Fig. 8.126). Their boundaries are formed by bone and soft tissues.
The temporal fossa is superior to the infratemporal fossa, above the zygomatic arch, and communicates with the infratemporal fossa below through the gap between the zygomatic arch and the more medial surface of the skull.
The infratemporal fossa is a wedge-shaped space deep to the masseter muscle and the underlying ramus of mandible. Structures that travel between the cranial cavity, neck, pteryatine fossa, floor of the oral cavity, floor of the orbit, temporal fossa, and superficial regions of the head pass through it.
Of the four muscles of mastication (masseter, temporalis, medial pterygoid, and lateral pterygoid) that move the lower jaw at the temporomandibular joint, one (masseter) is lateral to the infratemporal fossa, two (medial and lateral pterygoid) are in the infratemporal fossa, and one fills the temporal fossa.
Bony framework
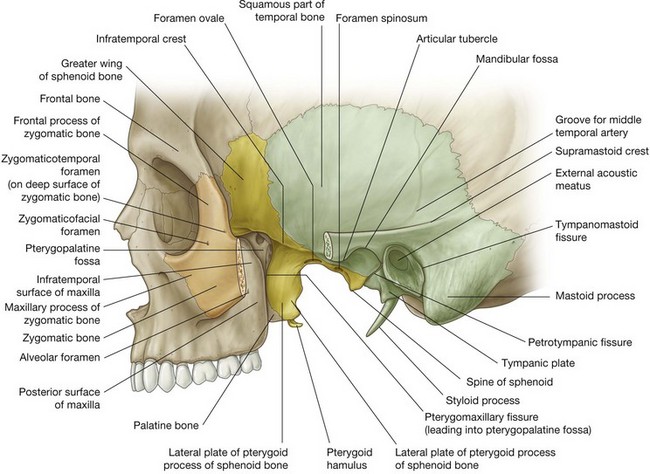
Bones that contribute significantly to the boundaries of the temporal and infratemporal fossae include the temporal, zygomatic, and sphenoid bones, and the maxilla and mandible (Fig. 8.127 and Fig. 8.128).
Parts of the frontal and parietal bones are also involved.
Temporal bone
The squamous part of the temporal bone forms part of the bony framework of the temporal and infratemporal fossae.
The tympanic part of the temporal bone forms the posteromedial corner of the roof of the infratemporal fossa, and also articulates with the head of mandible to form the temporomandibular joint.
The lateral surface of the squamous part of the temporal bone is marked by two surface features on the medial wall of the temporal fossa:

a transversely oriented
supramastoid crest, which extends posteriorly from the base of the zygomatic process and marks the posteroinferior border of the temporal fossa;
a vertically oriented
groove for middle temporal artery, a branch of the superficial temporal artery.
Two features that participate in forming the temporomandibular joint on the inferior aspect of the root of the zygomatic process are the articular tubercle and the mandibular fossa. Both are elongate from medial to lateral. Posterior to the mandibular fossa is the external auditory meatus. The tympanic part of the temporal bone is a flat concave plate of bone that curves inferiorly from the back of the mandibular fossa and forms part of the wall of the external auditory meatus.
When viewed from inferiorly, there is a distinct tympanosquamous fissure between the tympanic and squamous parts of the temporal bone. Medially, a small slip of bone from the petrous part of the temporal bone insinuates itself into the fissure and forms a petrotympanic fissure between it and the tympanic part (Fig. 8.127).
The chorda tympani nerve exits the skull and enters the infratemporal fossa through the medial end of the petrotympanic fissure.
Sphenoid bone
The parts of the sphenoid bone that form part of the bony framework of the infratemporal fossa are the lateral plate of the pterygoid process and the greater wing (Fig. 8.127). The greater wing also forms part of the medial wall of the temporal fossa.
The greater wings extend one on each side from the body of sphenoid. They project laterally from the body and curve superiorly. The inferior and lateral surfaces form the roof of the infratemporal fossa and the medial wall of the temporal fossa, respectively.
The sharply angled boundary between the lateral and inferior surfaces of the greater wing is the infratemporal crest (Fig. 8.127).
Two apertures (the foramen ovale and the foramen spinosum) pass through the base of the greater wing and allow the mandibular nerve [V3] and the middle meningeal artery, respectively, to pass between the middle cranial fossa and infratemporal fossa. In addition, one or more small sphenoidal emissary foramina penetrate the base of the greater wing anteromedial to the foramen ovale and allow emissary veins to pass between the pterygoid plexus of veins in the infratemporal fossa and the cavernous sinus in the middle cranial fossa.
Projecting vertically downward from the greater wing immediately medial to the foramen spinosum is the irregularly shaped spine of sphenoid, which is the attachment site for the cranial end of the sphenomandibular ligament.
The lateral plate of the pterygoid process is a vertically oriented sheet of bone that projects posterolaterally from the pterygoid process (Fig. 8.127). Its lateral and medial surfaces provide attachment for the lateral and medial pterygoid muscles, respectively.
Maxilla
The posterior surface of the maxilla contributes to the anterior wall of the infratemporal fossa (Fig. 8.127). This surface is marked by a foramen for the posterior superior alveolar nerve and vessels. The superior margin forms the inferior border of the inferior orbital fissure.
Zygomatic bone
The zygomatic bone is a quadrangular-shaped bone that forms the palpable bony prominence of the cheek:
a
maxillary process extends anteromedially to articulate with the zygomatic process of the maxilla;
a
frontal process extends superiorly to articulate with the zygomatic process of the frontal bone;
a
temporal process extends posteriorly to articulate with the zygomatic process of the temporal bone to complete the zygomatic arch.
A small zygomaticofacial foramen on the lateral surface of the zygomatic bone transmits the zygomaticofacial nerve and vessels onto the cheek.
A thin plate of bone extends posteromedially from the frontal process and contributes to the lateral wall of the orbit on one side and the anterior wall of the temporal fossa on the other. A zygomaticotemporal foramen on the temporal fossa surface of the plate where it attaches to the frontal process is for the zygomaticotemporal nerve.
Ramus of mandible
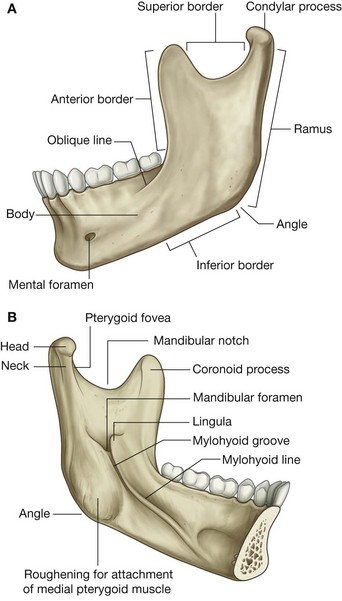
The ramus of mandible is quadrangular in shape and has medial and lateral surfaces and condylar and coronoid processes (Fig. 8.128).
The lateral surface of the ramus of mandible is generally smooth except for the presence of a few obliquely oriented ridges. Most of the lateral surface provides attachment for the masseter muscle.
The posterior and inferior borders of the ramus intersect to form the angle of mandible, while the superior border is notched to form the mandibular notch. The anterior border is sharp and is continuous below with the oblique line on the body of mandible.
The coronoid process extends superiorly from the junction of the anterior and superior borders of the ramus. It is a flat, triangular process that provides attachment for temporalis muscle.
The condylar process extends superiorly from the posterior and superior borders of the ramus. It consists of:
the
head of mandible, which is expanded medially and participates in forming the temporomandibular joint; and
the
neck of mandible, which bears a shallow depression (the
pterygoid fovea) on its anterior surface for attachment of the lateral pterygoid muscle.
The medial surface of the ramus of mandible is the lateral wall of the infratemporal fossa (Fig. 8.128B). Its most distinctive feature is the mandibular foramen, which is the superior opening of the mandibular canal. The inferior alveolar nerve and vessels pass through this foramen.
Immediately anterosuperior to the mandibular foramen is a triangular elevation (the lingula) for attachment of the mandibular end of the sphenomandibular ligament.
An elongate groove (the mylohyoid groove) extends anteroinferiorly from the mandibular foramen. The nerve to mylohyoid is in this groove.
Posteroinferior to the mylohyoid groove and mandibular foramen, the medial surface of the ramus of mandible is roughened for attachment of the medial pterygoid muscle.
Temporomandibular joints
The temporomandibular joints, one on each side, allow opening and closing of the mouth and complex chewing or side-to-side movements of the lower jaw.
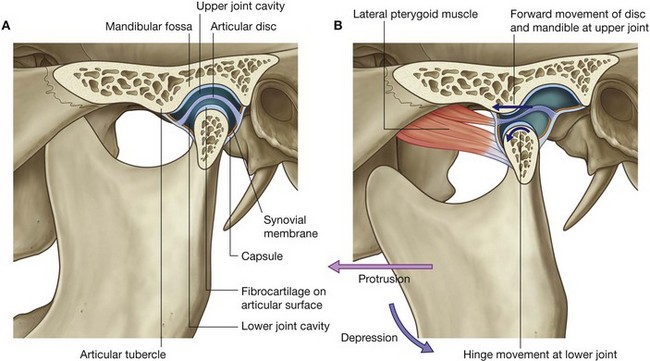
Each joint is synovial and is formed between the head of mandible and the articular fossa and articular tubercle of the temporal bone (Fig. 8.129A).
Unlike most other synovial joints where the articular surfaces of the bones are covered by a layer of hyaline cartilage, those of the temporomandibular joint are covered by fibrocartilage. In addition, the joint is completely divided by a fibrous articular disc into two parts:
the lower part of the joint allows mainly the hinge-like depression and elevation of the mandible;
the upper part of the joint allows the head of the mandible to translocate forward (protrusion) onto the articular tubercle and backward (retraction) into the mandibular fossa.
Opening the mouth involves both depression and protrusion (Fig. 8.129B).
The forward or protrusive movement allows greater depression of the mandible by preventing backward movement of the angle of mandible into structures in the neck.
Joint capsule
The synovial membrane of the joint capsule lines all nonarticular surfaces of the upper and lower compartments of the joint and is attached to the margins of the articular disc.
The fibrous membrane of the joint capsule encloses the temporomandibular joint complex and is attached:
above along the anterior margin of the articular tubercle;
laterally and medially along the margins of the articular fossa;
posteriorly to the region of the tympanosquamous suture; and
below around the upper part of the neck of mandible.
The articular disc attaches around its periphery to the inner aspect of the fibrous membrane.
Extracapsular ligaments
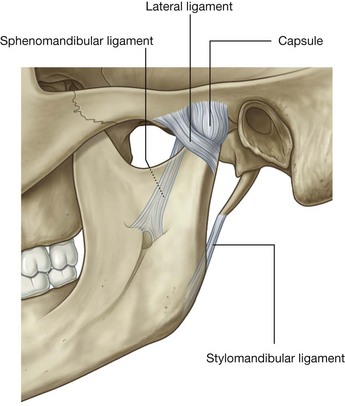
Three extracapsular ligaments are associated with the temporomandibular joint—the lateral, sphenomandibular, and the stylomandibular ligaments (Fig. 8.130):
the
lateral ligament is closest to the joint, just lateral to the capsule, and runs diagonally backward from the margin of the articular tubercle to the neck of the mandible;
the
sphenomandibular ligament is medial to the temporomandibular joint, runs from the spine of the sphenoid bone at the base of the skull to the lingula on the medial side of the ramus of mandible;
the
stylomandibular ligament passes from the styloid process of the temporal bone to the posterior margin and angle of mandible.
Movements of the mandible
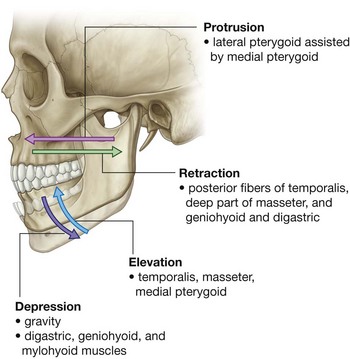
A chewing or grinding motion occurs when the movements at the temporomandibular joint on one side are coordinated with a reciprocal set of movements at the joint on the other side. Movements of the mandible include depression, elevation, protrusion, and retraction (Fig. 8.131):
depression is generated by the digastric, geniohyoid, and mylohyoid muscles on both sides, is normally assisted by gravity and, because it involves forward movement of the head of mandible onto the articular tubercle, the lateral pterygoid muscles are also involved;
elevation is a very powerful movement generated by the temporalis, masseter, and medial pterygoid muscles and also involves movement of the head of mandible into the mandibular fossa;
protraction is mainly achieved by the lateral pterygoid muscle, with some assistance by the medial pterygoid;
retraction is carried out by the geniohyoid and digastric muscles, and by the posterior and deep fibers of the temporalis and masseter muscles, respectively.
Except for the geniohyoid muscle, which is innervated by the C1 spinal nerve, all muscles that move the temporomandibular joints are innervated by the mandibular nerve [V3] by branches that originate in the infratemporal fossa.
Masseter muscle
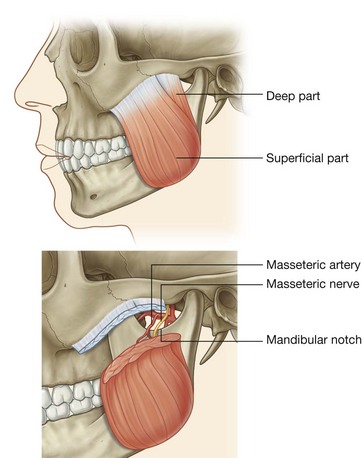
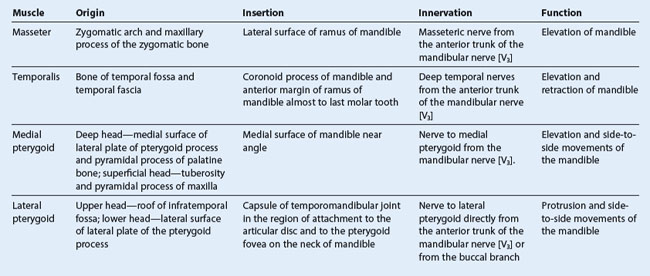
The masseter muscle is a powerful muscle of mastication that elevates the mandible (Fig. 8.132 and Table 8.11). It overlies the lateral surface of the ramus of mandible.
The masseter muscle is quadrangular in shape and is anchored above to the zygomatic arch and below to most of the lateral surface of the ramus of mandible.
The more superficial part of the masseter originates from the maxillary process of the zygomatic bone and the anterior two-thirds of the zygomatic process of the maxilla. It inserts into the angle of mandible and related posterior part of the lateral surface of the ramus of mandible.
The deep part of the masseter originates from the medial aspect of the zygomatic arch and the posterior part of its inferior margin and inserts into the central and upper part of the ramus of mandible as high as the coronoid process.
The masseter is innervated by the masseteric nerve from the mandibular nerve [V3] and supplied with blood by the masseteric artery from the maxillary artery.
The masseteric nerve and artery originate in the infratemporal fossa and pass laterally over the margin of the mandibular notch to enter the deep surface of the masseter muscle.
Temporal fossa
The temporal fossa is a narrow fan-shaped space that covers the lateral surface of the skull (Fig. 8.133A):
its upper margin is defined by a pair of temporal lines that arch across the skull from the zygomatic process of the frontal bone to the supramastoid crest of the temporal bone;
it is limited laterally by the
temporal fascia, which is a tough, fan-shaped aponeurosis overlying the temporalis muscle and attached by its outer margin to the superior temporal line and by its inferior margin to the zygomatic arch;
anteriorly, it is limited by the posterior surface of the frontal process of the zygomatic bone and the posterior surface of the zygomatic process of the frontal bone, which separate the temporal fossa behind from the orbit in front;
its inferior margin is marked by the zygomatic arch laterally and by the infratemporal crest of the greater wing of the sphenoid medially (
Fig. 8.133B)—between these two features, the floor of the temporal fossa is open medially to the infratemporal fossa and laterally to the region containing the masseter muscle.
Contents
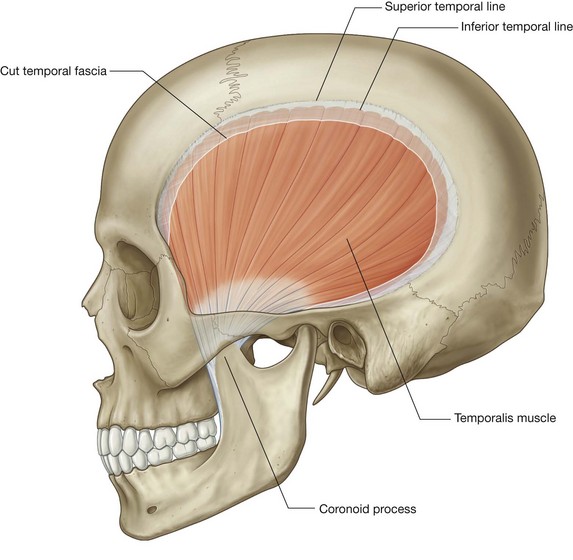
The major structure in the temporal fossa is the temporalis muscle.
Also passing through the fossa is the zygomaticotemporal branch of the maxillary nerve [V2], which enters the region through the zygomaticotemporal foramen on the temporal fossa surface of the zygomatic bone.
Temporalis muscle
The temporalis muscle is a large, fan-shaped muscle that fills much of the temporal fossa (Fig. 8.134). It originates from the bony surfaces of the fossa superiorly to the inferior temporal line and is attached laterally to the surface of the temporal fascia. The more anterior fibers are oriented vertically while the more posterior fibers are oriented horizontally. The fibers converge inferiorly to form a tendon, which passes between the zygomatic arch and the infratemporal crest of the greater wing of the sphenoid to insert on the coronoid process of the mandible.
The temporalis muscle attaches down the anterior surface of the coronoid process and along the related margin of the ramus of mandible, almost to the last molar tooth.
The temporalis is a powerful elevator of the mandible. Because this movement involves posterior translocation of the head of mandible from the articular tubercle of the temporal bone and back into the mandibular fossa, the temporalis also retracts the mandible or pulls it posteriorly. In addition, the temporalis participates in side-to-side movements of the mandible.
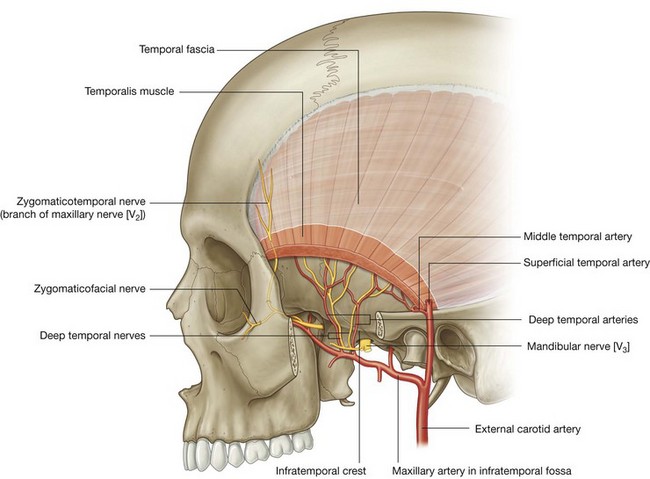
The temporalis is innervated by deep temporal nerves that originate from the mandibular nerve [V3] in the infratemporal fossa and then pass into the temporal fossa.
Blood supply of the temporalis is by deep temporal arteries, which travel with the nerves, and the middle temporal artery, which penetrates the temporal fascia at the posterior end of the zygomatic arch.
Deep temporal nerves
The deep temporal nerves, usually two in number, originate from the anterior trunk of the mandibular nerve [V3] in the infratemporal fossa (Fig. 8.135). They pass superiorly and around the infratemporal crest of the greater wing of the sphenoid to enter the temporal fossa deep to the temporalis muscle, and supply the temporalis muscle.
Zygomaticotemporal nerve
The zygomaticotemporal nerve is a branch of the zygomatic nerve (see Fig. 8.81, p. 884). The zygomatic nerve is a branch of the maxillary nerve [V2], which originates in the pteryatine fossa and passes into the orbit.
The zygomaticotemporal nerve enters the temporal fossa through one or more small foramina on the temporal fossa surface of the zygomatic bone.
Branches of the zygomaticotemporal nerve pass superiorly between the bone and the temporalis muscle to penetrate the temporal fascia and supply the skin of the temple (Fig. 8.135).
Deep temporal arteries
Normally two in number, these vessels originate from the maxillary artery in the infratemporal fossa and travel with the deep temporal nerves around the infratemporal crest of the greater wing of the sphenoid to supply the temporalis muscle (Fig. 8.135). They anastomose with branches of the middle temporal artery.
Middle temporal artery
The middle temporal artery originates from the superficial temporal artery just superior to the root of the zygomatic arch between this structure and the external ear (Fig. 8.135). It penetrates the temporalis fascia, passes under the margin of the temporalis muscle, and travels superiorly on the deep surface of the temporalis muscle.
The middle temporal artery supplies the temporalis and anastomoses with branches of the deep temporal arteries.
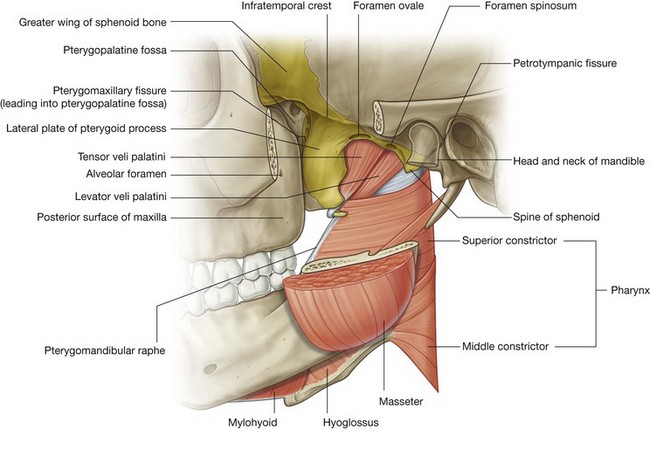
Infratemporal fossa
The wedge-shaped infratemporal fossa is inferior to the temporal fossa and between the ramus of mandible laterally and the wall of the pharynx medially. It has a roof, a lateral wall, and a medial wall, and is open to the neck posteroinferiorly (Fig. 8.136):
the
roof is formed by the inferior surfaces of the greater wing of the sphenoid and the temporal bone, contains the foramen spinosum, foramen ovale, and the petrotympanic fissure, and lateral to the infratemporal crest of the greater wing of the sphenoid, is open superiorly to the temporal fossa;
the
lateral wall is the medial surface of the ramus of mandible, which contains the opening to the mandibular canal;
the
medial wall is formed anteriorly by the lateral plate of the pterygoid process and more posteriorly by the pharynx and by two muscles of the soft palate (tensor and levator veli palatini muscles), and contains the pterygomaxillary fissure anteriorly, which allows structures to pass between the infratemporal and pteryatine fossae;
the
anterior wall is formed by part of the posterior surface of the maxilla, contains the alveolar foramen, and the upper part opens as the inferior orbital fissure into the orbit.
Contents
Major contents of the infratemporal fossa include the sphenomandibular ligament, medial and lateral pterygoid muscles (Table 8.11), the maxillary artery, the mandibular nerve [V3], branches of the facial nerve [VII] and the glossopharyngeal nerve [IX], and the pterygoid plexus of veins.
Sphenomandibular ligament
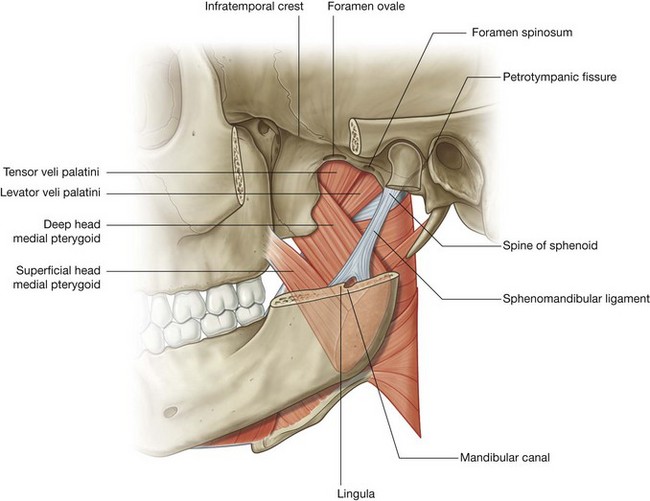
The sphenomandibular ligament is an extracapsular ligament of the temporomandibular joint. It is attached superiorly to the spine of the sphenoid bone and expands inferiorly to attach to the lingula of the mandible and the posterior margin of the mandibular foramen (Fig. 8.137).
Medial pterygoid
The medial pterygoid muscle is quadrangular in shape and has deep and superficial heads (Fig. 8.137):
the
deep head is attached above to the medial surface of the lateral plate of the pterygoid process and the associated surface of the pyramidal process of the palatine bone, and descends obliquely downward, medial to the sphenomandibular ligament, to attach to the roughened medial surface of the ramus of mandible near the angle of mandible;
the
superficial head originates from the tuberosity of the maxilla and adjacent pyramidal process of the palatine bone and joins with the deep head to insert on the mandible.
The medial pterygoid mainly elevates the mandible. Because it passes obliquely backward to insert into the mandible, it also assists the lateral pterygoid muscle in protruding the lower jaw.
The medial pterygoid is innervated by the nerve to medial pterygoid from the mandibular nerve [V3].
Lateral pterygoid
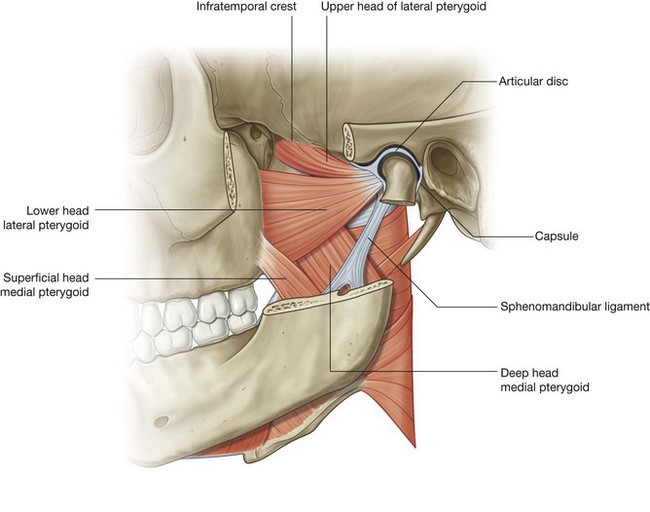
The lateral pterygoid is a thick triangular muscle and like the medial pterygoid muscle has two heads (Fig. 8.138):
the
upper head originates from the roof of the infratemporal fossa (inferior surface of the greater wing of the sphenoid and the infratemporal crest) lateral to the foramen ovale and foramen spinosum;
the
lower head is larger than the upper head and originates from the lateral surface of the lateral plate of the pterygoid process, and the inferior part insinuates itself between the cranial attachments of the two heads of the medial pterygoid.
The fibers from both heads of the lateral pterygoid muscle converge to insert into the pterygoid fovea of the neck of mandible and into the capsule of the temporomandibular joint in the region where the capsule is attached internally to the articular disc.
Unlike the medial pterygoid muscle whose fibers tend to be oriented vertically, those of the lateral pterygoid are oriented almost horizontally. As a result, when the lateral pterygoid contracts it pulls the articular disc and head of mandible forward onto the articular tubercle and is therefore the major protruder of the lower jaw.
The lateral pterygoid is innervated by the nerve to lateral pterygoid from the mandibular nerve [V3].
When the lateral and medial pterygoids contract on only one side, the chin moves to the opposite side. When opposite movements at the two temporomandibular joints are coordinated, a chewing movement results.
Mandibular nerve [V3]
The mandibular nerve [V3] is the largest of the three divisions of the trigeminal nerve [V].
Unlike the ophthalmic [V1] and maxillary [V2] nerves, which are purely sensory, the mandibular nerve [V3] is both motor and sensory.
In addition to carrying general sensation from the teeth and gingivae of the mandible, the anterior two-thirds of the tongue, mucosa on the floor of the oral cavity, the lower lip, skin over the temple and lower face, and part of the cranial dura mater, the mandibular nerve [V3] also carries motor innervation to most of the muscles that move the mandible, one of the muscles (tensor tympani) in the middle ear, and one of the muscles of the soft palate (tensor veli palatini).
All branches of the mandibular nerve [V3] originate in the infratemporal fossa.
Like the ophthalmic [V1] and maxillary [V2] nerves, the sensory part of the mandibular nerve [V3] originates from the trigeminal ganglion in the middle cranial fossa (Fig. 8.138):
the sensory part of the mandibular nerve [V
3] drops vertically through the foramen ovale and enters the infratemporal fossa between the tensor veli palatini muscle and the upper head of the lateral pterygoid muscle;
the small motor root of the trigeminal nerve [V] passes medial to the trigeminal ganglion in the cranial cavity, then passes through the foramen ovale and immediately joins the sensory part of the mandibular nerve [V
3].
Branches
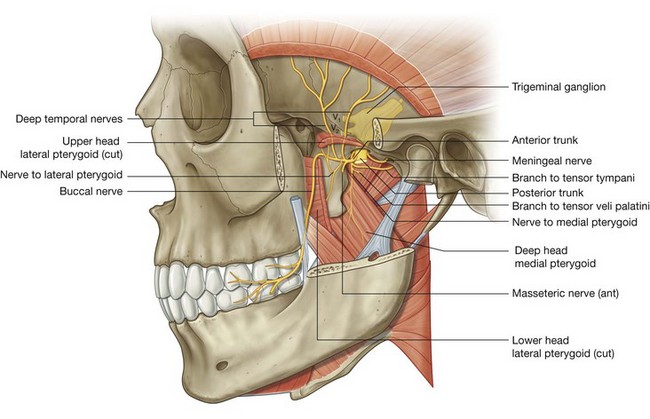
Soon after the sensory and motor roots join, the mandibular nerve [V3] gives rise to a small meningeal branch and to the nerve to medial pterygoid, and then divides into anterior and posterior trunks (Fig. 8.139):
branches from the anterior trunk are the buccal, masseteric, and deep temporal nerves, and the nerve to lateral pterygoid, all of which, except the buccal nerve (which is predominantly sensory) are motor nerves;
branches from the posterior trunk are the auriculotemporal, lingual, and inferior alveolar nerves, all of which, except a small nerve (nerve to mylohyoid) that branches from the inferior alveolar nerve, are sensory nerves.
Meningeal branch
The meningeal branch originates from the medial side of the mandibular nerve [V3] and ascends to leave the infratemporal fossa with the middle meningeal artery and re-enter the cranial cavity through the foramen spinosum (Fig. 8.139). It is sensory for the dura mater, mainly of the middle cranial fossa, and also supplies the mastoid cells that communicate with the middle ear.
Nerve to medial pterygoid
The nerve to medial pterygoid also originates medially from the mandibular nerve [V3] (Fig. 8.139). It descends to enter and supply the deep surface of the medial pterygoid muscle. Near its origin from the mandibular nerve [V3], it has two small branches:
one of these supplies the tensor veli palatini;
the other ascends to supply the tensor tympani muscle, which occupies a small bony canal above and parallel to the pharyngotympanic tube in the temporal bone.
Buccal nerve
The buccal nerve is a branch of the anterior trunk of the mandibular nerve [V3] (Fig. 8.139). It is predominantly a sensory nerve, but may also carry the motor innervation to the lateral pterygoid muscle and to part of the temporalis muscle.
The buccal nerve passes laterally between the upper and lower heads of lateral pterygoid and then descends around the anterior margin of the insertion of temporalis muscle to the anterior margin of the ramus of mandible, often slipping through the tendon of temporalis. It continues into the cheek lateral to the buccinator muscle to supply general sensory nerves to the adjacent skin and oral mucosa and the buccal gingivae of the lower molars.
Masseteric nerve
The masseteric nerve is a branch of the anterior trunk of the mandibular nerve [V3] (Figs. 8.132 and 8.139). It passes laterally over the lateral pterygoid muscle and through the mandibular notch to penetrate and supply the masseter muscle.
Deep temporal nerves
The deep temporal nerves, usually two in number, originate from the anterior trunk of the mandibular nerve [V3] (Fig. 8.139). They pass laterally above the lateral pterygoid muscle and curve around the infratemporal crest to ascend in the temporal fossa and supply the temporalis muscle from its deep surface.
Nerve to lateral pterygoid
The nerve to lateral pterygoid may originate directly as a branch from the anterior trunk of the mandibular nerve [V3] or from its buccal branch (Fig. 8.139). From its origin, it passes directly into the deep surface of the lateral pterygoid muscle.
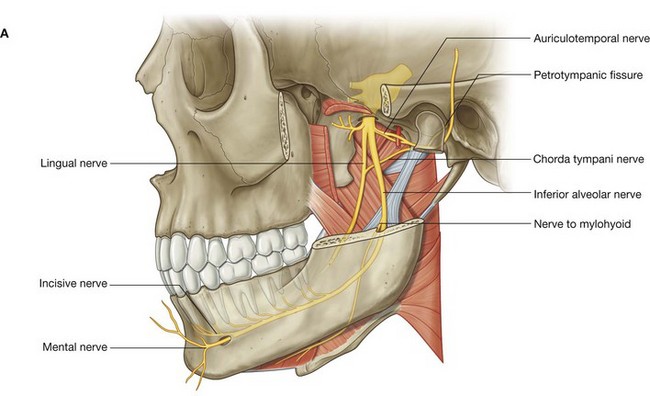
Auriculotemporal nerve
The auriculotemporal nerve is the first branch of the posterior division of the mandibular nerve [V3] and originates as two roots, which pass posteriorly around the middle meningeal artery ascending from the maxillary artery to the foramen spinosum (Fig. 8.140).
The auriculotemporal nerve passes first between the tensor veli palatini muscle and the upper head of lateral pterygoid muscle, and then between the sphenomandibular ligament and the neck of mandible. It curves laterally around the neck of mandible and then ascends deep to the parotid gland between the temporomandibular joint and ear.
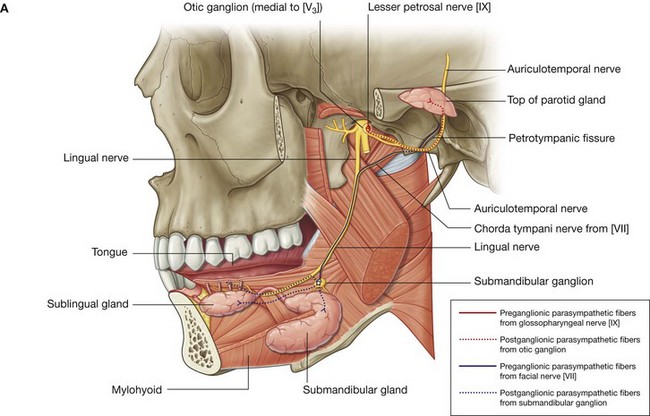
The terminal branches of the auriculotemporal nerve carry general sensation from skin over a large area of the temple. In addition, the auriculotemporal nerve contributes to sensory innervation of the external ear, the external auditory meatus, tympanic membrane, and temporomandibular joint. It also delivers postganglionic parasympathetic nerves from the glossopharyngeal nerve [IX] to the parotid gland.
Lingual nerve
The lingual nerve is a major sensory branch of the posterior trunk of the mandibular nerve [V3] (Fig. 8.140). It carries general sensation from the anterior two-thirds of the tongue, oral mucosa on the floor of the oral cavity, and lingual gingivae associated with the lower teeth.
The lingual nerve is joined high in the infratemporal fossa by the chorda tympani branch of the facial nerve [VII], which carries:
taste from the anterior two-thirds of the tongue; and
parasympathetic fibers to all salivary glands below the level of the oral fissure.
The lingual nerve first descends between the tensor veli palatini muscle and the lateral pterygoid muscle, where it is joined by the chorda tympani nerve, and then descends across the lateral surface of the medial pterygoid muscle to enter the oral cavity.
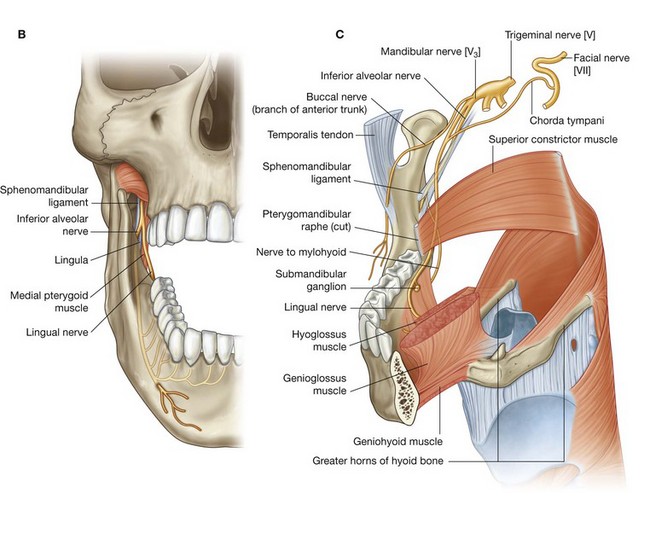
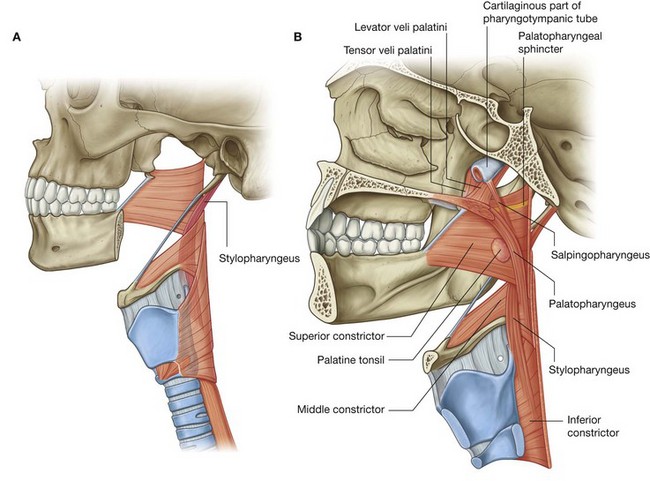
The lingual nerve enters the oral cavity between the posterior attachment of the mylohyoid muscle to the mylohyoid line and the attachment of the superior constrictor of the pharynx to the pterygomandibular raphe. As the lingual nerve enters the floor of the oral cavity, it is in a shallow groove on the medial surface of the mandible immediately inferior to the last molar tooth. In this position, it is palpable through the oral mucosa and in danger when operating on the molar teeth and gingivae.
The lingual nerve passes into the tongue on the lateral surface of the hyoglossus muscle where it is attached to the submandibular ganglion (see p. 936), which contains the secondary cell bodies for the parasympathetic nerves of the chorda tympani nerve carried from the infratemporal fossa into the floor of the oral cavity on the lingual nerve.
Inferior alveolar nerve
The inferior alveolar nerve, like the lingual nerve, is a major sensory branch of the posterior trunk of the mandibular nerve [V3] (Fig. 8.140). In addition to innervating all lower teeth and much of the associated gingivae, it also supplies the mucosa and skin of the lower lip and skin of the chin. It has one motor branch, which innervates the mylohyoid muscle and the anterior belly of the digastric muscle.
The inferior alveolar nerve originates deep to the lateral pterygoid muscle from the posterior trunk of the mandibular nerve [V3] in association with the lingual nerve. It descends on the lateral surface of the medial pterygoid muscle, passes between the sphenomandibular ligament and the ramus of mandible, and then enters the mandibular canal through the mandibular foramen. Just before entering the mandibular foramen, it gives origin to the nerve to mylohyoid, which lies in the mylohyoid groove inferior to the foramen and continues anteriorly below the floor of the oral cavity to innervate the mylohyoid muscle and the anterior belly of the digastric muscle.
The inferior alveolar nerve passes anteriorly within the mandibular canal of the lower jaw. The mandibular canal and its contents are inferior to the roots of the molar teeth, and the roots can sometimes curve around the canal making extraction of these teeth difficult.
The inferior alveolar nerve supplies branches to the three molar teeth and the second premolar tooth and associated labial gingivae, and then divides into its two terminal branches:
the
incisive nerve, which continues in the mandibular canal to supply the first premolar, incisor, and canine teeth, and related gingivae.
the
mental nerve, which exits the mandible through the mental foramen and supplies the lower lip and chin.
The mental nerve is palpable and sometimes visible through the oral mucosa adjacent to the roots of the premolar teeth.
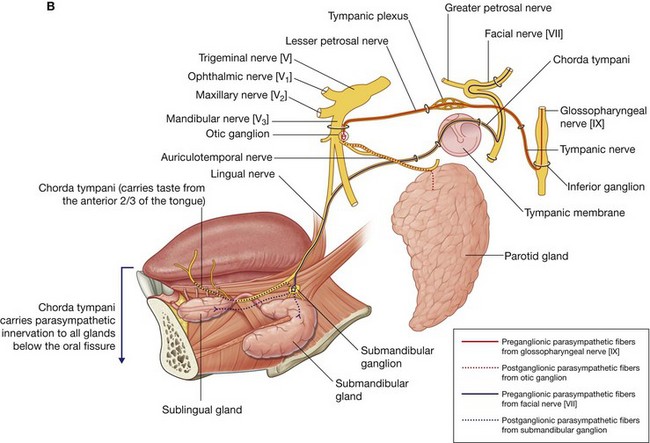
Chorda tympani and the lesser petrosal nerve
Branches of two cranial nerves join branches of the mandibular nerve [V3] in the infratemporal fossa (Fig. 8.141). These are the chorda tympani branch of the facial nerve [VII] and the lesser petrosal nerve, a branch of the tympanic plexus in the middle ear, which had its origin from a branch of the glossopharyngeal nerve [IX] (see Fig. 8.111, p. 907).
Chorda tympani
The chorda tympani (Fig. 8.141) carries taste from the anterior two-thirds of the tongue and parasympathetic innervation to all salivary glands below the level of the oral fissure.
The chorda tympani originates from the facial nerve [VII] within the temporal bone and in association with the mastoid wall of the middle ear, passes anteriorly through a small canal, and enters the lateral aspect of the middle ear. As it continues anterosuperiorly across the middle ear, it is separated from the tympanic membrane by the handle of malleus. It leaves the middle ear through the medial end of the petrotympanic fissure, enters the infratemporal fossa, descends medial to the spine of the sphenoid and then to the lateral pterygoid muscle, and joins the lingual nerve.
Preganglionic parasympathetic fibers carried in the chorda tympani synapse with postganglionic parasympathetic fibers in the submandibular ganglion, which “hangs off” the lingual nerve in the floor of the oral cavity.
Postganglionic parasympathetic fibers leave the submandibular ganglion and either:
re-enter the lingual nerve to travel with its terminal branches to reach target tissues; or
pass directly from the submandibular ganglion into glands.
The taste (SA) fibers do not pass through the ganglion and are distributed with terminal branches of the lingual nerve.
In the clinic
Lingual nerve injury
A lingual nerve injury proximal to where the chorda tympani joins it in the infratemporal fossa will produce loss of general sensation from the anterior two-thirds of the tongue, oral mucosa, gingivae, the lower lip, and the chin.
If a lingual nerve lesion is distal to the site where it is joined by the chorda tympani, secretion from the salivary glands below the oral fissure and taste from the anterior two-thirds of the tongue will also be lost.
Lesser petrosal nerve
The lesser petrosal nerve carries mainly parasympathetic fibers destined for the parotid gland (Fig. 8.141). The preganglionic parasympathetic fibers are located in the glossopharyngeal nerve [IX] as it exits the jugular foramen at the base of the skull. Branching from the glossopharyngeal nerve [IX] either within or immediately outside the jugular foramen is the tympanic nerve.
The tympanic nerve re-enters the temporal bone through a small foramen on the ridge of bone separating the jugular foramen from the carotid canal and ascends through a small bony canal (inferior tympanic canaliculus) to the promontory located on the labyrinthine (medial) wall of the middle ear. Here it participates in the formation of the tympanic plexus. The lesser petrosal nerve is a branch of this plexus.
The lesser petrosal nerve contains mainly preganglionic parasympathetic fibers. It leaves the middle ear and enters the middle cranial fossa through a small opening on the anterior surface of the petrous part of the temporal bone just lateral and inferior to the opening for the greater petrosal nerve, a branch of the facial nerve [VII]. The lesser petrosal nerve then passes medially and descends through the foramen ovale with the mandibular nerve [V3].
In the infratemporal fossa, the preganglionic parasympathetic fibers synapse with cell bodies of postganglionic parasympathetic fibers in the otic ganglion located on the medial side of the mandibular nerve [V3] around the origin of the nerve to medial pterygoid. Postganglionic parasympathetic fibers leave the otic ganglion and join the auriculotemporal nerve, which carries them to the parotid gland.
In the clinic
Dental anesthesia
Anesthesia of the inferior alveolar nerve is widely practiced by most dentists. The inferior alveolar nerve is one of the largest branches of the mandibular nerve [V3], carries the sensory branches from the teeth and mandible, and receives sensory information from the skin over the mandible.
The inferior alveolar nerve passes into the mandibular canal and runs within the medullary cavity of the mandible, piercing the anterior aspect of the mandible through the mental foramen.
Dental procedures require perineuronal infiltration of the inferior alveolar nerve by local anesthetic. To anesthetize this nerve the needle is placed lateral to the anterior arch of the fauces (palatoglossal arch) in the oral cavity and is advanced along the medial border around the inferior third of the body of mandible so that anesthetic can be deposited in this region.
It is also possible to anesthetize the infra-orbital, mental, incisive, and buccal nerves, depending on where the anesthesia is needed.
Maxillary artery
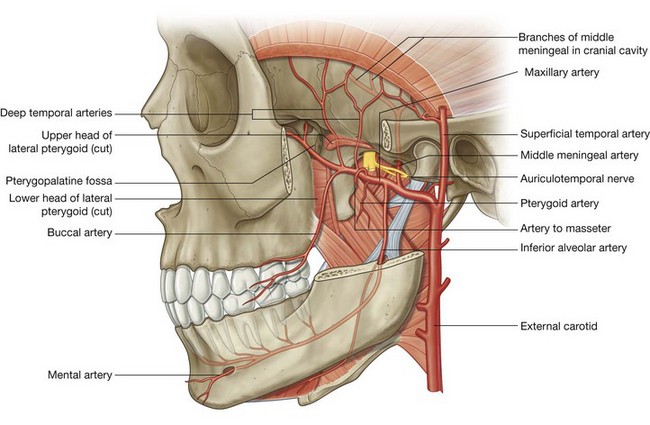
The maxillary artery is the largest branch of the external carotid artery in the neck and is a major source of blood supply for the nasal cavity, the lateral wall and roof of the oral cavity, all teeth, and the dura mater in the cranial cavity. It passes through and supplies the infratemporal fossa and then enters the pteryatine fossa, where it gives origin to terminal branches (Fig. 8.142).
The maxillary artery originates within the substance of the parotid gland and then passes forward, between the neck of mandible and sphenomandibular ligament, into the infratemporal fossa. It ascends obliquely through the infratemporal fossa to enter the pteryatine fossa by passing through the pterygomaxillary fissure. This part of the vessel may pass either lateral or medial to the lower head of lateral pterygoid. If it passes medial to the lower head, the maxillary artery then loops laterally between the upper and lower heads of lateral pterygoid to access the pterygomaxillary fissure.
Branches
Branches of the maxillary artery are as follows:
the first part of the maxillary artery (the part between the neck of mandible and the sphenomandibular ligament) gives origin to two major branches (the middle meningeal and inferior alveolar arteries) and a number of smaller branches (deep auricular, anterior tympanic, and accessory meningeal);
the second part of the maxillary artery (the part related to the lateral pterygoid muscle) gives origin to deep temporal, masseteric, buccal, and pterygoid branches, which course with branches of the mandibular nerve [V
3];
the third part of the maxillary artery is in the pteryatine fossa (see p. 946).
Middle meningeal artery
The middle meningeal artery ascends vertically from the maxillary artery and passes through the foramen spinosum to enter the cranial cavity (Fig. 8.142). In the infratemporal fossa, it passes superiorly between the sphenomandibular ligament on the medial side and the lateral pterygoid muscle on the lateral side. Just inferior to the foramen spinosum, it passes between the two roots of the auriculotemporal nerve at their origin from the mandibular nerve [V3].
The middle meningeal artery is the largest of the meningeal vessels and supplies much of the dura mater, bone, and related bone marrow of the cranial cavity walls.
Within the cranial cavity, the middle meningeal artery and its branches travel in the periosteal (outer) layer of dura mater, which is tightly adherent to the bony walls. As major branches of the middle meningeal artery pass superiorly up the walls of the cranial cavity, they can be damaged by lateral blows to the head. When the vessels are torn, the leaking blood, which is under arterial pressure, slowly separates the dura mater from its attachment to the bone, resulting in an extradural hematoma.
Inferior alveolar artery
The inferior alveolar artery descends from the maxillary artery to enter the mandibular foramen and canal with the inferior alveolar nerve (Fig. 8.142). It is distributed with the inferior alveolar nerve and supplies all lower teeth, and contributes to the supply of the buccal gingivae, chin, and lower lip.
Before entering the mandible, the inferior alveolar artery gives origin to a small mylohyoid branch, which accompanies the nerve to mylohyoid.
Deep auricular, anterior tympanic, and accessory meningeal arteries
The deep auricular, anterior tympanic, and accessory meningeal arteries are small branches from the first part of the maxillary artery and contribute to the blood supply of the external acoustic meatus, deep surface of the tympanic membrane, and cranial dura mater, respectively.
The accessory meningeal branch also contributes small branches to surrounding muscles in the infratemporal fossa before ascending through the foramen ovale into the cranial cavity to supply dura mater.
Branches from the second part
Deep temporal arteries, usually two in number, originate from the second part of the maxillary artery and travel with the deep temporal nerves to supply the temporalis muscle in the temporal fossa (Fig. 8.142).
Numerous pterygoid arteries also originate from the second part of the maxillary artery and supply the pterygoid muscles.
The masseteric artery, also from the second part of the maxillary artery, accompanies the masseteric nerve laterally through the mandibular notch to supply the masseter muscle.
The buccal artery is distributed with the buccal nerve and supplies skin, muscle, and oral mucosa of the cheek.
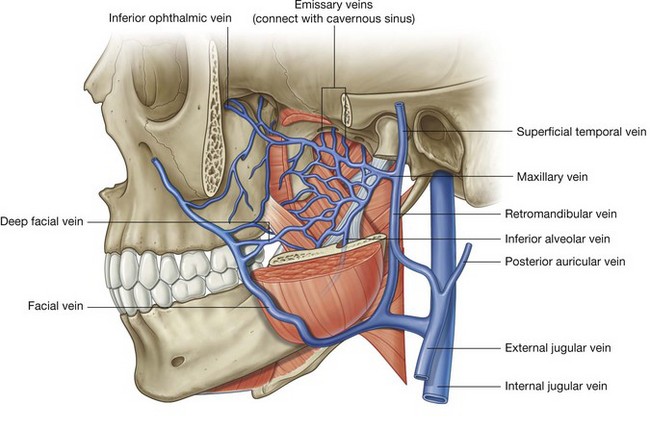
Pterygoid plexus
The pterygoid plexus is a network of veins between the medial and lateral pterygoid muscles, and between the lateral pterygoid and temporalis muscles (Fig. 8.143).
Veins that drain regions supplied by arteries branching from the maxillary artery in the infratemporal fossa and pteryatine fossa connect with the pterygoid plexus. These tributary veins include those that drain the nasal cavity, roof and lateral wall of the oral cavity, all teeth, muscles of the infratemporal fossa, paranasal sinuses, and nasopharynx. In addition, the inferior ophthalmic vein from the orbit can drain through the inferior orbital fissure into the pterygoid plexus.
Significantly, small emissary veins often connect the pterygoid plexus in the infratemporal fossa to the cavernous sinus in the cranial cavity. These emissary veins, which pass through the foramen ovale, through the cartilage that fills the foramen lacerum, and through a small sphenoidal foramen on the medial side of the lateral plate of the pterygoid process at the base of the skull, are a route by which infections can spread into the cranial cavity from structures, such as the teeth, that are drained by the pterygoid plexus. Also, because there are no valves in veins of the head and neck, anesthetic inadvertently injected under pressure into veins of the pterygoid plexus can backflow into tissues or into the cranial cavity.
The pterygoid plexus connects:
posteriorly, via a short maxillary vein, with the retromandibular vein in the neck; and
anteriorly, via a deep facial vein, with the facial vein on the face.
PTERYATINE FOSSA
The pteryatine fossa is an inverted teardrop-shaped space between bones on the lateral side of the skull immediately posterior to the maxilla (Fig. 8.144).
Although small in size, the pteryatine fossa communicates via fissures and foramina in its walls with the:
middle cranial fossa;
infratemporal fossa;
floor of the orbit;
lateral wall of the nasal cavity;
oropharynx; and
roof of the oral cavity.
Because of its strategic location, the pteryatine fossa is a major site of distribution for the maxillary nerve [V2] and for the terminal part of the maxillary artery. It also contains the pteryatine ganglion where preganglionic parasympathetic fibers originating in the facial nerve [VII] synapse with postganglionic parasympathetic fibers and these fibers, along with sympathetic fibers originating from the T1 spinal cord level join branches of the maxillary nerve [V2].
All the upper teeth receive their innervation and blood supply from the maxillary nerve [V2] and the terminal part of the maxillary artery, respectively, that pass through the pteryatine fossa.
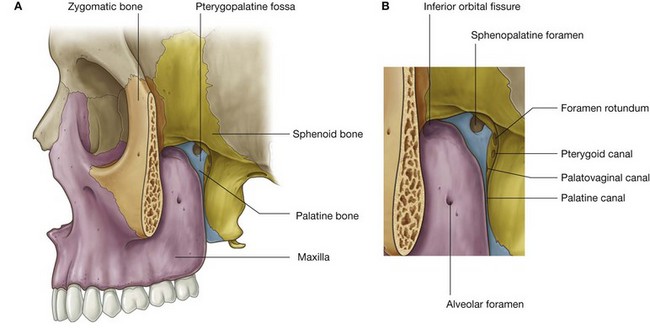
Skeletal framework
The walls of the pteryatine fossa are formed by parts of the palatine, maxilla, and sphenoid bones (Fig. 8.144):
the anterior wall is formed by the posterior surface of the maxilla;
the medial wall is formed by the lateral surface of the palatine bone;
the posterior wall and roof are formed by parts of the sphenoid bone.
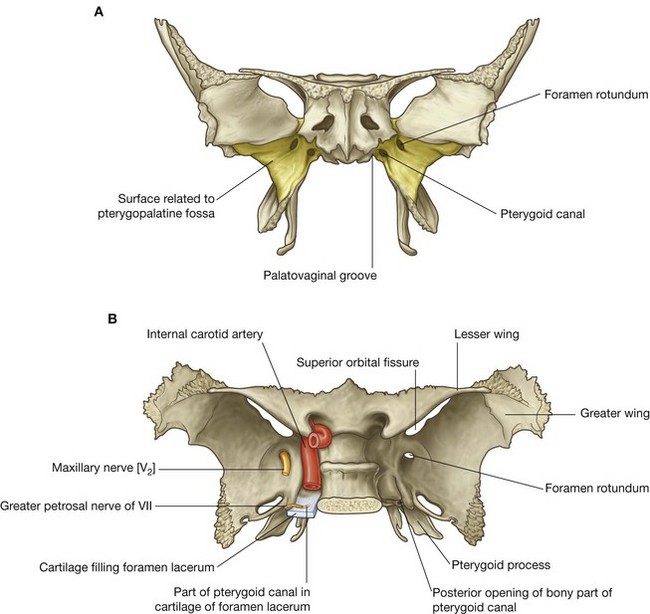
Sphenoid bone
The part of the sphenoid bone that contributes to the formation of the pteryatine fossa is the anterosuperior surface of the pterygoid process (Fig. 8.145). Opening onto this surface are two large foramina:
the maxillary nerve [V
2] passes through the most lateral and superior of these—
the foramen rotundum—which communicates posteriorly with the middle cranial fossa (
Fig. 8.145B);
the greater petrosal nerve from the facial nerve [VII] and sympathetic fibers from the internal carotid plexus join to form the nerve of the pterygoid canal that passes forward into the pteryatine fossa through the more medial and inferior foramen—
the anterior opening of the pterygoid canal.
Pterygoid canal
The pterygoid canal is a bony canal opening onto the posterior surface of the pterygoid process and then continuing superomedially for a short distance in the cartilage that fills the foramen lacerum and surrounding the posterior opening of the pterygoid canal. The pterygoid canal opens into the middle cranial fossa just anteroinferior to the internal carotid artery as the vessel enters the cranial cavity through the carotid canal (Fig. 8.145B).
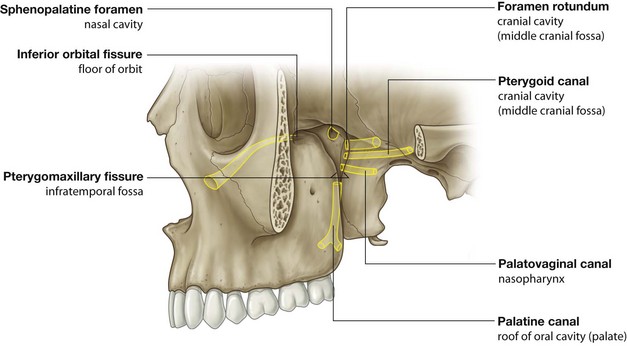
Gateways
Seven foramina and fissures provide apertures through which structures enter and leave the pteryatine fossa (Fig. 8.146):
the foramen rotundum and pterygoid canal communicate with the middle cranial fossa and open onto the posterior wall;
a small
palatovaginal canal opens onto the posterior wall and leads to the nasopharynx;
the palatine canal leads to the roof of the oral cavity (hard palate) and opens inferiorly;
the sphenopalatine foramen opens onto the lateral wall of the nasal cavity and is in the medial wall;
the lateral aspect of the pteryatine fossa is continuous with the infratemporal fossa via a large gap (the
pterygomaxillary fissure) between the posterior surface of the maxilla and pterygoid process of the sphenoid bone;
the superior aspect of the anterior wall of the fossa opens into the floor of the orbit via the inferior orbital fissure.
Contents
The maxillary nerve [V2] and terminal part of the maxillary artery enter and branch within the pteryatine fossa. In addition, the nerve of the pterygoid canal enters the fossa carrying:
preganglionic parasympathetic fibers from the greater petrosal branch of the facial nerve [VII]; and
postganglionic sympathetic fibers from the deep petrosal branch of the carotid plexus.
The preganglionic parasympathetic fibers synapse in the pteryatine ganglion and both the sympathetic and postganglionic parasympathetic fibers pass with branches of the maxillary nerve [V2] out of the fossa and into adjacent regions.
In addition to nerves and arteries, veins and lymphatics also pass through the pteryatine fossa.
Maxillary nerve [V2]
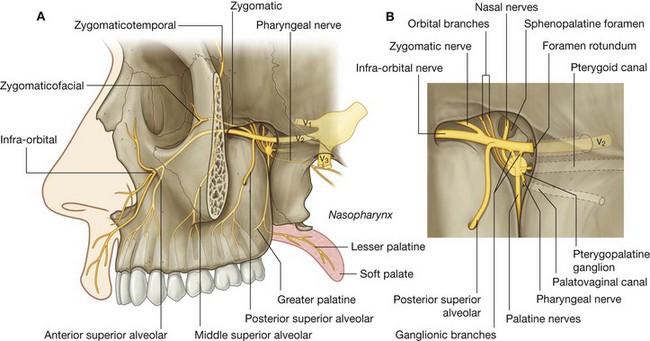
The maxillary nerve [V2] is purely sensory. It originates from the trigeminal ganglion in the cranial cavity, exits the middle cranial fossa, and enters the pteryatine fossa through the foramen rotundum (Fig. 8.147). It passes anteriorly through the fossa and exits as the infra-orbital nerve through the inferior orbital fissure.
While passing through the pteryatine fossa, the maxillary nerve [V2] gives rise to the zygomatic nerve, the posterior superior alveolar nerve, and two ganglionic branches. The two ganglionic branches originate from its inferior surface and pass through the pteryatine ganglion.
Postganglionic parasympathetic fibers, arising in the pteryatine ganglion, join the general sensory branches of the maxillary nerve [V2] in the pteryatine ganglion, as do postganglionic sympathetic fibers from the carotid plexus, and the three types of fibers leave the ganglion as orbital, palatine, nasal, and pharyngeal branches.
Branches
Orbital branches.
The orbital branches are small and pass through the inferior orbital fissure to contribute to the supply of the orbital wall and of the sphenoidal and ethmoidal sinuses.
Greater and lesser palatine nerves.
The greater and lesser palatine nerves (Fig. 8.147) pass inferiorly from the pteryatine ganglion, enter and pass through the palatine canal, and enter the oral surface of the palate through the greater and lesser palatine foramina.
The greater palatine nerve passes forward on the roof of the oral cavity to innervate mucosa and glands of the hard palate and the adjacent gingiva, almost as far forward as the incisor teeth.
In the palatine canal, the greater palatine nerve gives origin to posterior inferior nasal nerves, which pass medially through small foramina in the perpendicular plate of the palatine bone and contribute to the innervation of the lateral nasal wall.
After passing through the lesser palatine foramen, the lesser palatine nerve passes posteriorly to supply the soft palate.
Nasal nerves.
The nasal nerves (Fig. 8.147), approximately seven in number, pass medially through the sphenopalatine foramen to enter the nasal cavity. Most pass anteriorly to supply the lateral wall of the nasal cavity, while others pass across the roof to supply the medial wall.
One of the nerves passing across the roof to supply the medial wall of the nasal cavity (the nasopalatine nerve) is the largest of the nasal nerves and passes anteriorly down the nasal septum, through the incisive canal and fossa in the hard palate to enter the roof of the oral cavity and supply mucosa, gingiva, and glands adjacent to the incisor teeth.
Pharyngeal nerve.
The pharyngeal nerve passes posteriorly from the pteryatine ganglion, and leaves the fossa through the palatovaginal canal, which it then exits to supply the mucosa and glands of the nasopharynx.
Zygomatic nerve.
The zygomatic nerve (Fig. 8.147) originates directly from the maxillary nerve [V2] in the pteryatine fossa, which it leaves to enter the orbit through the inferior orbital fissure. It passes forward on the lateral orbital wall and divides into zygomaticotemporal and zygomaticofacial branches:
the
zygomaticotemporal branch continues forward at the base of the lateral orbital wall, passes through a small bony canal in the zygomatic bone to enter the temporal fossa through a small foramen in the lateral orbital margin on the posterior surface of the frontal process of the zygomatic bone, and passes superficially to supply skin over the temple;
the
zygomaticofacial branch also passes forward at the base of the lateral orbital wall, leaves through a small bony canal, in the orbital margin, which opens via multiple small foramina on the anterolateral surface of the zygomatic bone, and its branches supply the adjacent skin.
Posterior superior alveolar nerve.
The posterior superior alveolar nerve (Fig. 8.147) originates from the maxillary nerve [V2] in the pteryatine fossa and passes laterally out of the fossa through the pterygomaxillary fissure to enter the infratemporal fossa. It continues laterally and inferiorly to enter the posterior surface of the maxilla through a small alveolar foramen approximately midway between the last molar tooth and the inferior orbital fissure. It then passes inferiorly just deep to the mucosa of the maxillary sinus to join the superior dental plexus.
The posterior superior alveolar nerve supplies the molar teeth and adjacent buccal gingivae, and contributes to the supply of the maxillary sinus.
Infra-orbital nerve.
The infra-orbital nerve (Fig. 8.147) is the anterior continuation of the maxillary nerve [V2] that leaves the pteryatine fossa through the inferior orbital fissure. It lies first in the infra-orbital groove in the floor of the orbit and then continues forward in the infra-orbital canal.
While in the infra-orbital groove and canal, the infra-orbital nerve gives origin to middle and anterior superior alveolar nerves, respectively, which ultimately join the superior alveolar plexus to supply the upper teeth:
the middle superior alveolar nerve also supplies the maxillary sinus;
the anterior superior alveolar nerve also gives origin to a small nasal branch, which passes medially through the lateral wall of the nasal cavity to supply parts of the areas of the nasal floor and walls.
The infra-orbital nerve exits the infra-orbital canal through the infra-orbital foramen inferior to the orbital margin and divides into nasal, palpebral, and superior labial branches:
nasal branches supply skin over the lateral aspect of the external nose and part of the nasal septum;
palpebral branches supply skin of the lower eyelid;
superior labial branches supply skin over the cheek and upper lip, and the related oral mucosa.
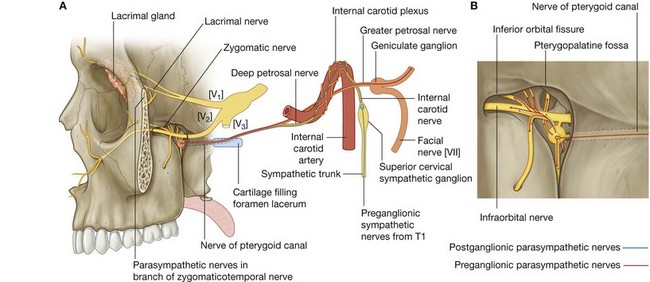
Nerve of the pterygoid canal and the pteryatine ganglion
The nerve of the pterygoid canal (Fig. 8.148) is formed in the middle cranial fossa by the union of:
the greater petrosal nerve (a branch of the facial nerve [VII]); and
the deep petrosal nerve (a branch of the internal carotid plexus).
The nerve of the pterygoid canal passes into the pteryatine fossa and joins the pteryatine ganglion. It carries mainly preganglionic parasympathetic and postganglionic sympathetic fibers.
Greater petrosal nerve
The greater petrosal nerve, which originates from the geniculate ganglion of the facial nerve [VII] in the temporal bone, exits the temporal bone through a small canal that opens via a fissure onto the anterior surface of the petrous part of the temporal bone. It passes anteromedially along the posterior margin of the middle cranial fossa and then under the internal carotid artery to reach the superior surface of the cartilage filling the foramen lacerum.
As the greater petrosal nerve passes under the internal carotid artery, it is joined by the deep petrosal nerve to form the nerve of the pterygoid canal.
The greater petrosal nerve carries parasympathetic innervation to all glands above the oral fissure, including:
mucous glands in the nasal cavity;
salivary glands in the upper half of the oral cavity; and
the lacrimal gland in the orbit.
The greater petrosal nerve also carries some taste (SA) fibers from the soft palate in the lesser palatine nerve.
Deep petrosal nerve
The deep petrosal nerve is formed by postganglionic sympathetic fibers that originate in the superior cervical sympathetic ganglion in the neck and leave the ganglion as the internal carotid nerve.
Preganglionic fibers that synapse in the ganglion are from the T1 spinal nerve.
The internal carotid nerve forms the internal carotid plexus around the internal carotid artery as the internal carotid artery passes through the skull and into the cranial cavity. Some of the fibers from the internal carotid plexus converge to form the deep petrosal nerve, which leaves the internal carotid plexus in the middle cranial fossa and joins the greater petrosal branch of the facial nerve [VII].
The deep petrosal nerve carries postganglionic sympathetic fibers destined mainly for blood vessels.
Pteryatine ganglion
The nerve of the pterygoid canal enters the superior surface of the cartilage that fills the foramen lacerum and passes anteriorly through the cartilage to enter the pterygoid canal in the root of the pterygoid process of the sphenoid bone. It passes through the canal and into the pteryatine fossa where it joins the pteryatine ganglion formed around the branches of the maxillary nerve [V2] (Fig. 8.148).
The pteryatine ganglion is the largest of the four parasympathetic ganglia in the head and is formed by the cell bodies of the postganglionic neurons associated with preganglionic parasympathetic fibers of the facial nerve [VII] carried by the greater petrosal nerve and the nerve of the pterygoid canal.
The postganglionic parasympathetic fibers that originate in the pteryatine ganglion, together with postganglionic sympathetic fibers passing through the ganglion, join fibers from the ganglionic branches of the maxillary nerve [V2] to form orbital, palatine, nasal, and pharyngeal branches, which leave the ganglion.
Other postganglionic parasympathetic and sympathetic fibers pass superiorly through the ganglionic branches of the maxillary nerve [V2] to enter the main trunk of the maxillary nerve and be distributed with the zygomatic, posterior superior alveolar, and infra-orbital nerves. Of these, the postganglionic parasympathetic and sympathetic fibers that pass into the orbit with the zygomatic nerve are particularly important because they ultimately innervate the lacrimal gland.
Innervation of the lacrimal gland
Approximately midway along the orbital wall, the postganglionic parasympathetic and sympathetic fibers leave the zygomaticotemporal branch of the zygomatic nerve and form a special autonomic nerve, which travels up the lateral orbital wall to join the lacrimal nerve (Fig. 8.148 and Fig. 8.81).
The lacrimal nerve is a major general sensory branch of the ophthalmic nerve [V1], which passes forward in the orbit at the margin between the lateral wall and roof.
The postganglionic parasympathetic and sympathetic fibers pass with the lacrimal nerve to the lacrimal gland.
A lesion anywhere along the course of parasympathetic fibers that leave the brain as part of the facial nerve [VII] and are ultimately carried to the lacrimal gland along branches of the ophthalmic nerve [V1] results in “dry eye” and can eventually lead to loss of vision in the affected eye.
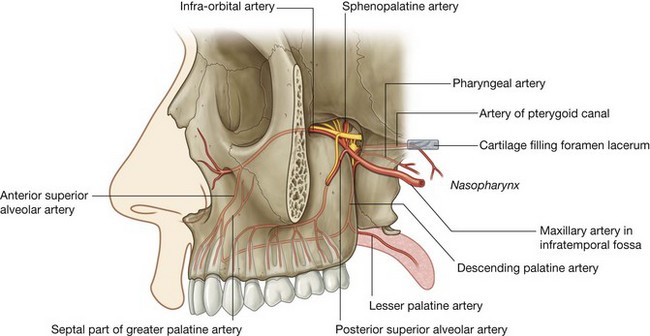
Maxillary artery
The maxillary artery is a major branch of the external carotid artery in the neck. It originates adjacent to the neck of mandible, passes forward through the infratemporal fossa, and then enters the pteryatine fossa through the pterygomaxillary fissure (Fig. 8.149).
The part of the maxillary artery in the pteryatine fossa (the third part) is anterior to the pteryatine ganglion and gives origin to branches that accompany branches of the maxillary nerve [V2] and the pteryatine ganglion.
Branches of the maxillary artery include the posterior superior alveolar, infra-orbital, greater palatine, pharyngeal, and sphenopalatine arteries, and the artery of the pterygoid canal. Collectively, these branches supply much of the nasal cavity, the roof of the oral cavity, and all upper teeth. In addition, they contribute to the blood supply of the sinuses, oropharynx, and floor of the orbit.
Branches
Posterior superior alveolar artery.
The posterior superior alveolar artery originates from the maxillary artery as it passes through the pterygomaxillary fissure. It meets the posterior superior alveolar nerve, accompanies it through the alveolar foramen on the infratemporal surface of the maxilla, and supplies the molar and premolar teeth, adjacent gingiva, and the maxillary sinus.
Infra-orbital artery.
The infra-orbital artery passes forward with the infra-orbital nerve and leaves the pteryatine fossa through the inferior orbital fissure. With the infra-orbital nerve, it lies in the infra-orbital groove and infra-orbital canal, and emerges through the infra-orbital foramen to supply parts of the face.
Within the infra-orbital canal, the infra-orbital artery gives origin to:
branches that contribute to the blood supply of structures near the floor of the orbit—the inferior rectus and inferior oblique muscles, and the lacrimal sac; and
anterior superior alveolar arteries, which supply the incisor and canine teeth and the maxillary sinus.
Greater palatine artery.
The greater palatine artery passes inferiorly with the palatine nerves into the palatine canal. It gives origin to a lesser palatine branch, which passes through the lesser palatine foramen to supply the soft palate, and then continues through the greater palatine foramen to supply the hard palate. The latter vessel passes forward on the inferior surface of the palate to enter the incisive fossa and pass superiorly through the incisive canal to supply the anterior aspect of the septal wall of the nasal cavity.
Pharyngeal branch.
The pharyngeal branch of the maxillary artery travels posteriorly and leaves the pteryatine fossa through the palatovaginal canal with the pharyngeal nerve. It supplies the posterior aspect of the roof of the nasal cavity, the sphenoidal sinus, and the pharyngotympanic tube.
Sphenopalatine artery.
The sphenopalatine artery is the terminal branch of the maxillary artery. It leaves the pteryatine fossa medially through the sphenopalatine foramen and accompanies the nasal nerves, giving off:
posterior lateral nasal arteries, which supply the lateral wall of the nasal cavity and contribute to the supply of the paranasal sinuses; and
posterior septal branches, which travel medially across the roof to supply the nasal septum—the largest of these branches passes anteriorly down the septum to anastomose with the end of the greater palatine artery.
Artery of pterygoid canal.
The artery of pterygoid canal passes posteriorly into the pterygoid canal. It supplies surrounding tissues and terminates, after passing inferiorly through cartilage filling the foramen lacerum, in the mucosa of the nasopharynx.
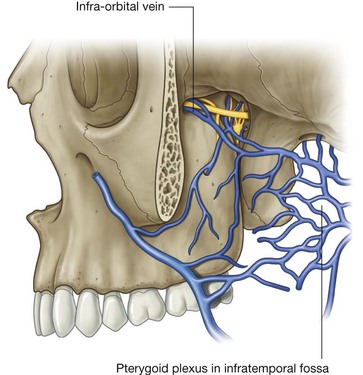
Veins
Veins that drain areas supplied by branches of the terminal part of the maxillary artery generally travel with these branches back into the pteryatine fossa.
The veins coalesce in the pteryatine fossa and then pass laterally through the pterygomaxillary fissure to join the pterygoid plexus of veins in the infratemporal fossa (Fig. 8.150).
The infra-orbital vein, which drains the inferior aspect of the orbit, may pass directly into the infratemporal fossa through the lateral aspect of the inferior orbital fissure, so bypassing the pteryatine fossa.
NECK
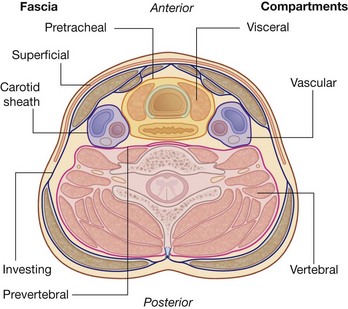
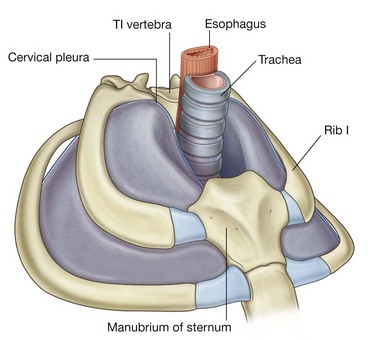
The neck is a tube providing continuity from the head to the trunk. It extends anteriorly from the lower border of the mandible to the upper surface of the manubrium of sternum, and posteriorly from the superior nuchal line on the occipital bone of the skull to the intervertebral disc between the CVII and TI vertebrae. Within the tube, four compartments provide longitudinal organization (Fig. 8.151):
the visceral compartment is anterior and contains parts of the digestive and respiratory systems, and several endocrine glands;
the vertebral compartment is posterior and contains the cervical vertebrae, spinal cord, cervical nerves, and muscles associated with the vertebral column;
the two vascular compartments, one on each side, are lateral and contain the major blood vessels and the vagus nerve [X].
All these compartments are contained within unique layers of cervical fascia.
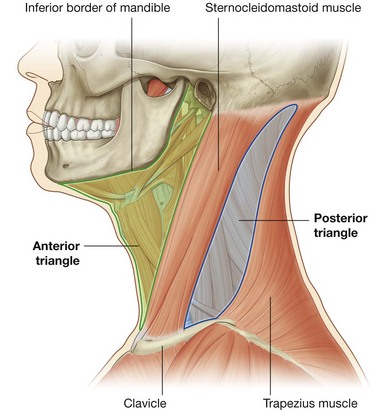
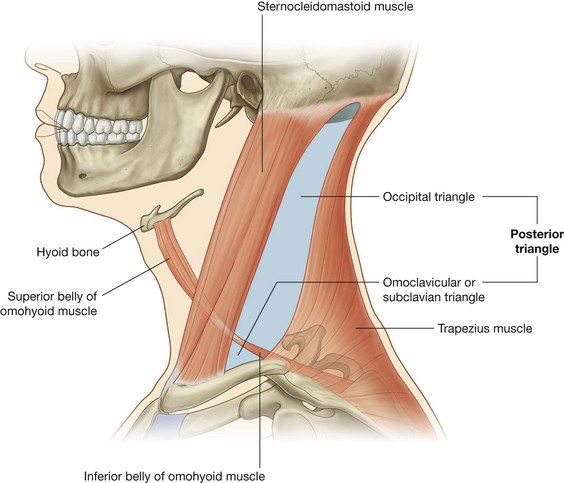
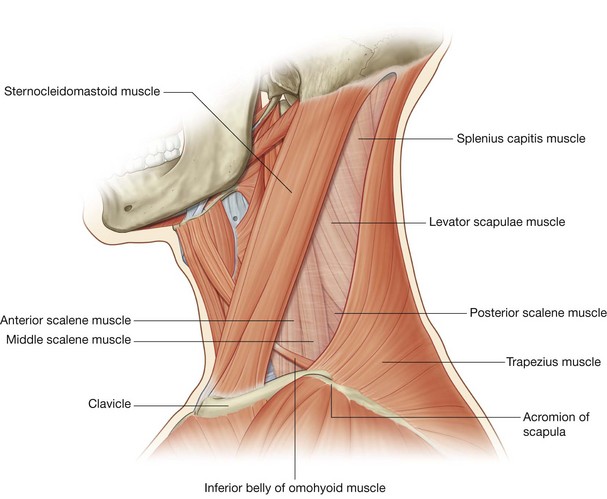
For descriptive purposes the neck is divided into anterior and posterior triangles (Fig. 8.152):
the boundaries of the
anterior triangle are the anterior border of the sternocleidomastoid muscle, the inferior border of the mandible, and the midline of the neck;
the boundaries of the
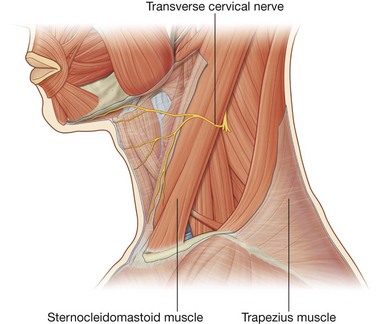
posterior triangle are the posterior border of the sternocleidomastoid muscle, the anterior border of the trapezius muscle, and the middle one-third of the clavicle.
Fascia
The fascia of the neck has a number of unique features.
The superficial fascia in the neck contains a thin sheet of muscle (the platysma), which begins in the superficial fascia of the thorax, runs upward to attach to the mandible and blend with the muscles on the face, is innervated by the cervical branch of the facial nerve [VII], and is only found in this location.
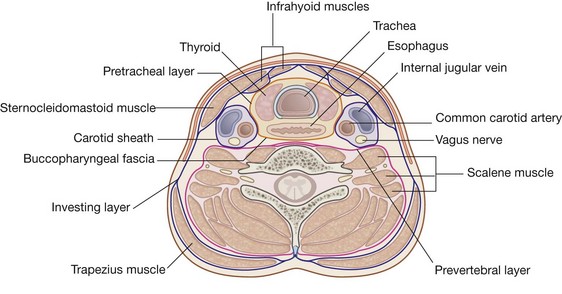
Deep to the superficial fascia, the deep cervical fascia is organized into several distinct layers (Fig. 8.151). These include:
an investing layer, which surrounds all structures in the neck;
the prevertebral layer, which surrounds the vertebral column and the deep muscles associated with the back;
the pretracheal layer, which encloses the viscera of the neck; and
the carotid sheaths, which receive a contribution from the other three fascial layers and surround the two major neurovascular bundles on either side of the neck.
Investing layer
The investing layer completely surrounds the neck (Fig. 8.153).
Attaching posteriorly to the ligamentum nuchae and the spinous process of the CVII vertebra, this fascial layer splits as it passes forward to enclose the trapezius muscle, reunites into a single layer as it forms the roof of the posterior triangle, splits again to surround the sternocleidomastoid muscle, and reunites again to join its twin from the other side.
Anteriorly, the investing fascia surrounds the infrahyoid muscles.
The investing fascia is attached:
superiorly to the external occipital protuberance and the superior nuchal line;
laterally to the mastoid process and zygomatic arch; and
inferiorly to the spine of the scapula, the acromion, the clavicle, and the manubrium of sternum.
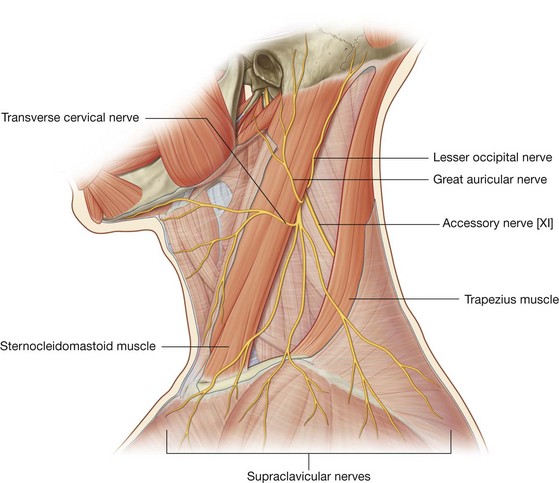
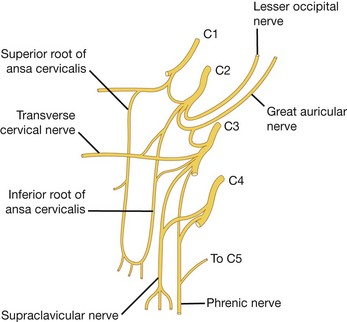
The external and anterior jugular veins, and the lesser occipital, great auricular, transverse cervical, and supraclavicular nerves, all branches of the cervical plexus, pierce the investing fascia.
Prevertebral layer
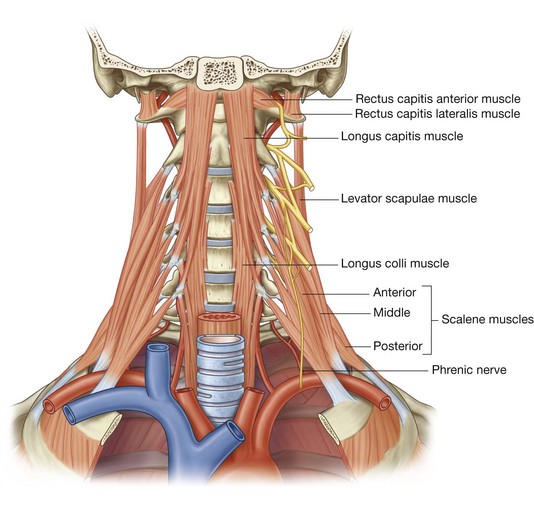
The prevertebral layer is a cylindrical layer of fascia that surrounds the vertebral column and the muscles associated with it (Fig. 8.153). Muscles in this group include the prevertebral muscles, the anterior, middle, and posterior scalene muscles, and the deep muscles of the back.
The prevertebral fascia is attached posteriorly along the length of the ligamentum nuchae, and superiorly forms a continuous circular line attaching to the base of the skull. This circle begins:
anteriorly as the fascia attaches to the basilar part of the occipital bone, the area of the jugular foramen, and the carotid canal;
continues laterally, attaching to the mastoid process; and
continues posteriorly along the superior nuchal line ending at the external occipital protuberance, where it associates with its partner from the opposite side.
Anteriorly, the prevertebral fascia is attached to the anterior surfaces of the transverse processes and bodies of vertebrae CI to CVII.
The prevertebral fascia passing between the attachment points on the transverse processes is unique. In this location, it splits into two layers, creating a longitudinal fascial space containing loose connective tissue that extends from the base of the skull through the thorax (Figs. 8.153 and 8.154).
There is one additional specialization of the prevertebral fascia in the lower region of the neck. The prevertebral fascia in an anterolateral position extends from the anterior and middle scalene muscles to surround the brachial plexus and subclavian artery as these structures pass into the axilla. This fascial extension is the axillary sheath.
Pretracheal layer
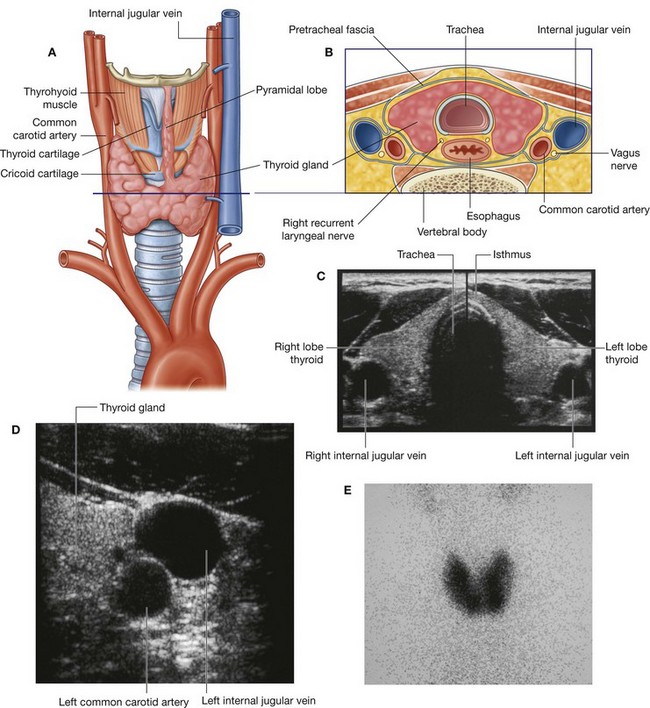
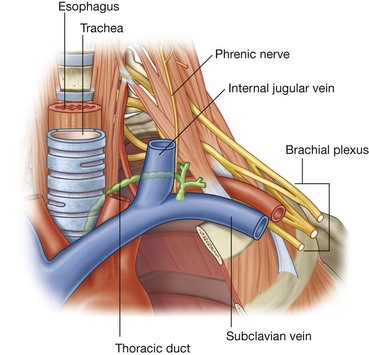
The pretracheal layer consists of a collection of fascias that surround the trachea, esophagus, and thyroid gland (Fig. 8.153). Anteriorly, it consists of a pretracheal fascia that crosses the neck, just posterior to the infrahyoid muscles, and covers the trachea and the thyroid gland. The pretracheal fascia begins superiorly at the hyoid bone and ends inferiorly in the upper thoracic cavity. Laterally, this fascia continues and covers the thyroid gland and the esophagus.
Posteriorly, the pretracheal layer is referred to as the buccopharyngeal fascia and separates the pharynx and the esophagus from the prevertebral layer (Fig. 8.154).
The buccopharyngeal fascia begins superiorly at the base of the skull and ends inferiorly in the thoracic cavity.
Carotid sheath
Each carotid sheath is a column of fascia that surrounds the common carotid artery, the internal carotid artery, the internal jugular vein, and the vagus nerve as these structures pass through the neck (Fig. 8.153).
It receives contributions from the investing, prevertebral, and pretracheal layers, though the extent of each component’s contribution varies.
Fascial compartments
The arrangement of the various layers of cervical fascia organizes the neck into four longitudinal compartments (Fig. 8.151):
the first compartment is the largest, includes the other three, and consists of the area surrounded by the investing layer;
the second compartment consists of the vertebral column, the deep muscles associated with this structure, and is the area contained within the prevertebral layer;
the third compartment (the visceral compartment) contains the pharynx, the trachea, the esophagus, and the thyroid gland, which are surrounded by the pretracheal layer;
finally, there is a compartment (the carotid sheath) consisting of the neurovascular structures that pass from the base of the skull to the thoracic cavity, and the sheath enclosing these structures receives contributions from the other cervical fascias.
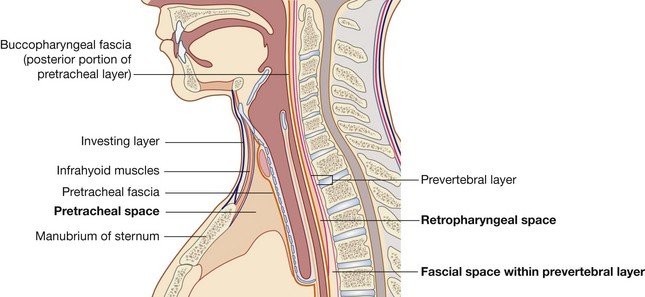
Fascial spaces
Between the fascial layers in the neck are spaces that may provide a conduit for the spread of infections from the neck to the mediastinum.
Three spaces could be involved in this process (Fig. 8.154):
the first is the
pretracheal space between the investing layer of cervical fascia (covering the posterior surface of the infrahyoid muscles) and the pretracheal fascia (covering the anterior surface of the trachea and the thyroid gland), which passes between the neck and the anterior part of the superior mediastinum;
the second is the
retropharyngeal space between the buccopharyngeal fascia (on the posterior surface of the pharynx and esophagus) and the prevertebral fascia (on the anterior surface of the transverse processes and bodies of the cervical vertebrae), which extends from the base of the skull to the upper part of the posterior mediastinum;
the
third space is within the prevertebral layer covering the anterior surface of the transverse processes and bodies of the cervical vertebrae. This layer splits into two laminae to create a fascial space that begins at the base of the skull and extends through the posterior mediastinum to the diaphragm.
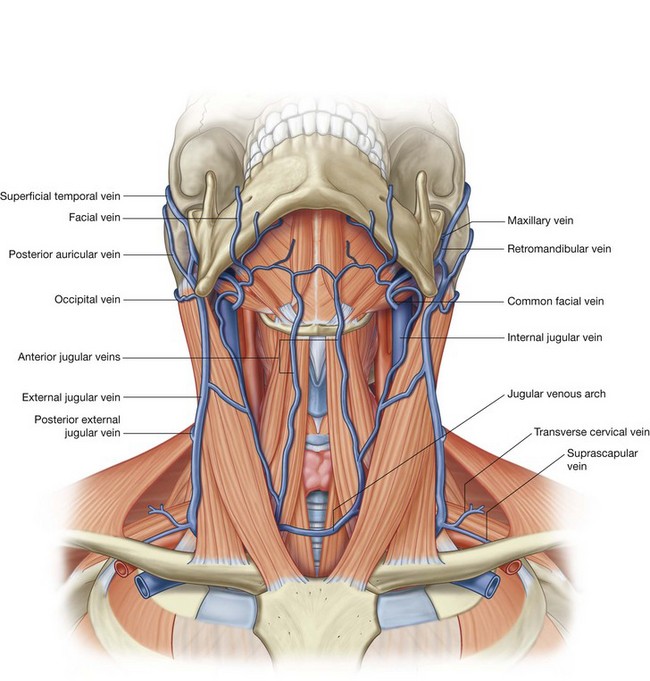
Superficial venous drainage
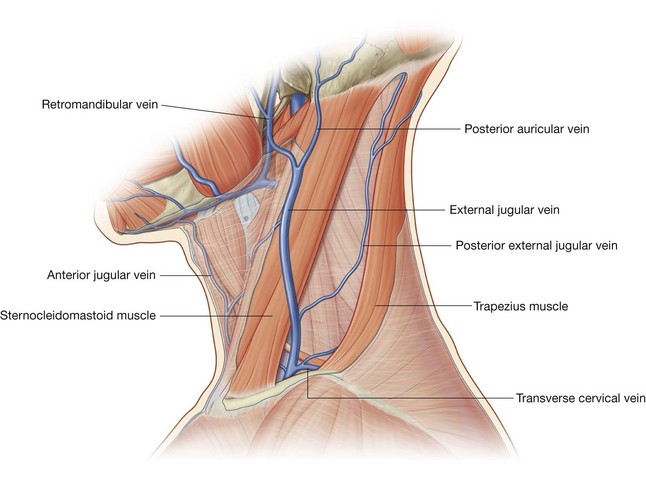
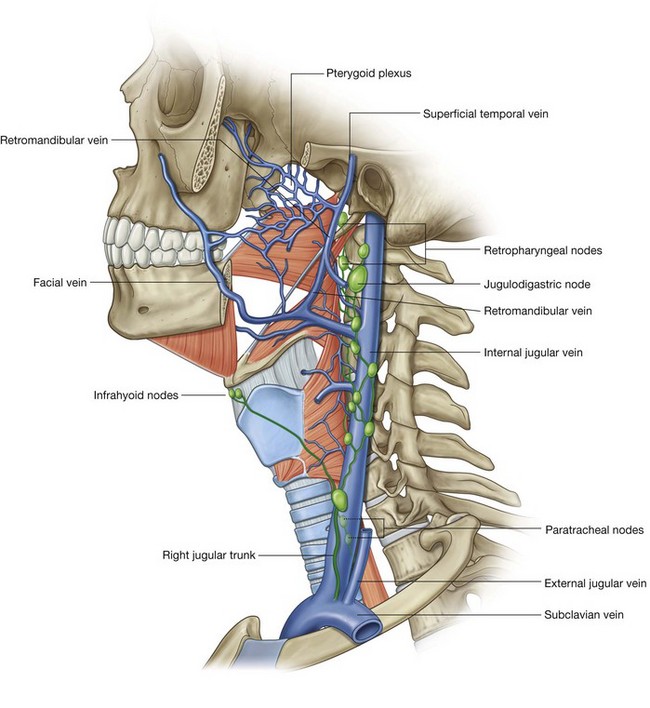
The external jugular and anterior jugular veins are the primary venous channels for superficial venous drainage of the neck (Fig. 8.155).
External jugular veins
The external jugular vein is formed posterior to the angle of mandible as the posterior auricular vein and the retromandibular vein join:
the posterior auricular vein drains the scalp behind and above the ear;
the retromandibular vein is formed when the
superficial temporal and
maxillary veins join in the substance of the parotid gland and descends to the angle of mandible where it divides into an anterior and a posterior division (
Fig. 8.155)—the posterior division joins the posterior auricular vein to form the external jugular vein, the anterior division joins the
facial vein, to form the common facial vein, which passes deep and becomes a tributary to the internal jugular vein.
Once formed, the external jugular vein passes straight down the neck in the superficial fascia and is superficial to the sternocleidomastoid muscle throughout its course, crossing it diagonally as it descends.
Reaching the lower part of the neck, just superior to the clavicle and immediately posterior to the sternocleidomastoid muscle, the external jugular vein pierces the investing layer of cervical fascia, passes deep to the clavicle, and enters the subclavian vein.
Tributaries received by the external jugular vein along its course include the posterior external jugular vein (draining superficial areas of the back of the neck) and the transverse cervical and suprascapular veins (draining the posterior scapular region).
Anterior jugular veins
The anterior jugular veins, although variable and inconsistent, are usually described as draining the anterior aspect of the neck (Fig. 8.155). These paired venous channels, which begin as small veins, come together at or just superior to the hyoid bone. Once formed, each anterior jugular vein descends on either side of the midline of the neck.
Inferiorly, near the medial attachment of the sternocleidomastoid muscle, each anterior jugular vein pierces the investing layer of cervical fascia to enter the subclavian vein. Occasionally, the anterior jugular vein may enter the external jugular vein immediately before the external jugular vein enters the subclavian vein.
Often, the right and left anterior jugular veins communicate with each other, being connected by a jugular venous arch in the area of the suprasternal notch.
In the clinic
Fascial planes of the head and neck
The neck contains a series of compartments, which are bound by tight fascia. All these compartments are within the overall investing layer of cervical fascia. From a clinical perspective the importance of these compartments is that infection tends to spread within compartments or within the spaces between the various fascial layers. For example, if infection arises in the pretracheal space it may spread inferiorly into the superior mediastinum and lie anterior to the pericardium.
In the clinic
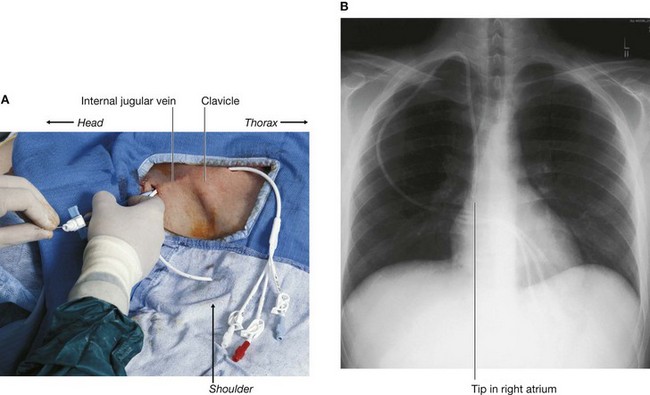
Central venous access
In most instances, access to peripheral veins of the arm and the leg will suffice for administering intravenous drugs and fluids and for obtaining blood for analysis. In certain circumstances it is necessary to place larger-bore catheters in the central veins, for example for dialysis, parenteral nutrition, or the administration of drugs that have a tendency to produce phlebitis.
“Blind puncture” of the subclavian and jugular veins to obtain central venous access used to be standard practice. However, subclavian vein puncture is not without complications. As the subclavian vein passes inferiorly, posterior to the clavicle, it passes over the apex of the lung. Any misplacement of a needle into or through this structure may puncture the apical pleura, producing a pneumothorax. Inadvertent arterial puncture and vein laceration may also produce a hemopneumothorax.
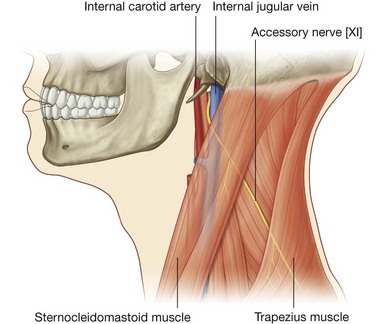
A puncture of the internal jugular vein (Fig. 8.156) carries fewer risks, but local hematoma and damage to the carotid artery are again important complications.
Current practice is to identify major vessels using ultrasound and to obtain central venous access under direct vision to avoid any significant complication.
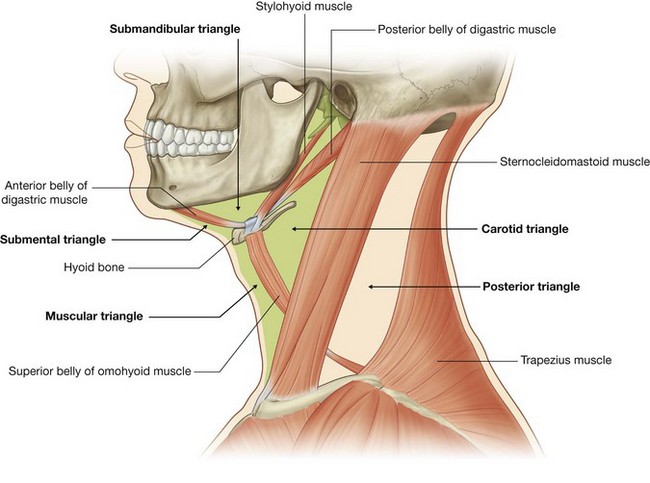
Anterior triangle of the neck
The anterior triangle of the neck is outlined by the anterior border of the sternocleidomastoid muscle laterally, the inferior border of the mandible superiorly, and the midline of the neck medially (Fig. 8.157). It is further subdivided into several smaller triangles as follows:
the
submandibular triangle is outlined by the inferior border of the mandible superiorly and the anterior and posterior bellies of the digastric muscle inferiorly;
the
submental triangle is outlined by the hyoid bone inferiorly, the anterior belly of the digastric muscle laterally, and the midline;
the
muscular triangle is outlined by the hyoid bone superiorly, the superior belly of the omohyoid muscle, and the anterior border of the sternocleidomastoid muscle laterally, and the midline;
the
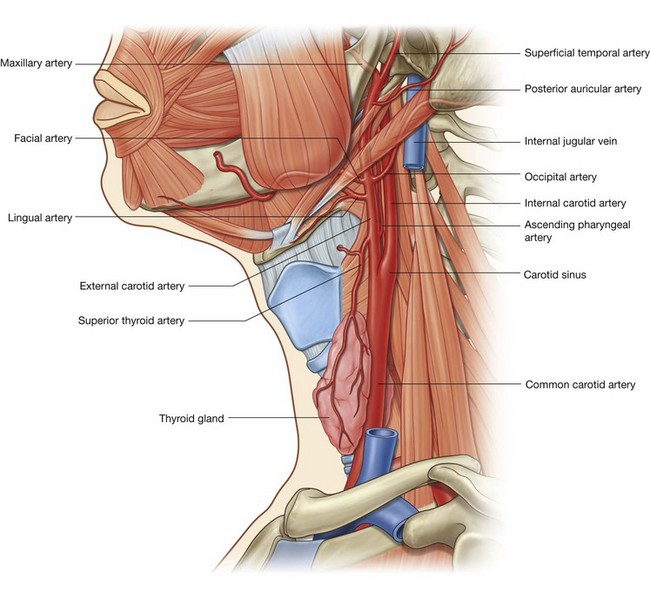
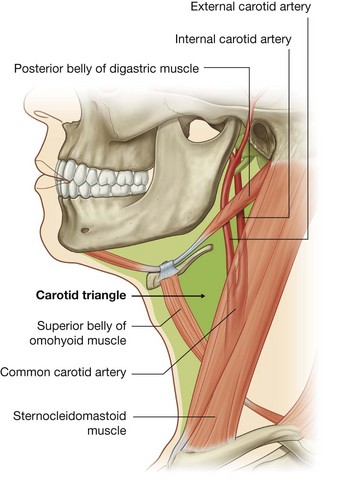
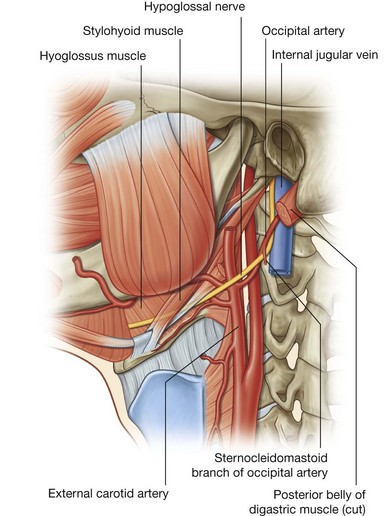
carotid triangle is outlined by the superior belly of the omohyoid muscle anteroinferiorly, the stylohyoid muscle and posterior belly of the digastric superiorly, and the anterior border of the sternocleidomastoid muscle posteriorly.
Each of these triangles contains numerous structures that can be identified as being within a specific triangle, passing into a specific triangle from outside the area, originating in one triangle and passing to another triangle, or passing through several triangles while passing through the region.
A discussion of the anterior triangle of the neck must therefore combine a systemic approach, describing the muscles, vessels, and nerves in the area, with a regional approach, describing the contents of each triangle.
Muscles
The muscles in the anterior triangle of the neck (Table 8.12) can be grouped according to their location relative to the hyoid bone:
muscles superior to the hyoid are classified as
suprahyoid muscles and include the stylohyoid, digastric, mylohyoid, and geniohyoid;
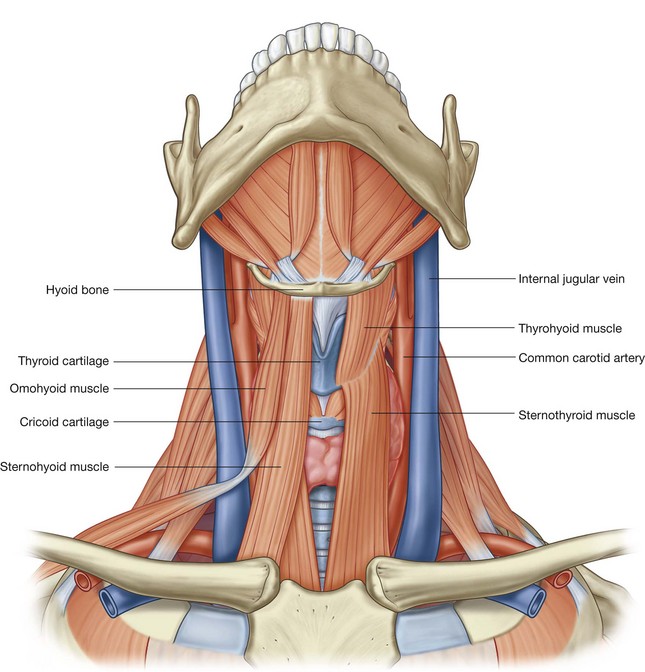
muscles inferior to the hyoid are
infrahyoid muscles and include the omohyoid, sternohyoid, thyrohyoid, and sternothyroid.
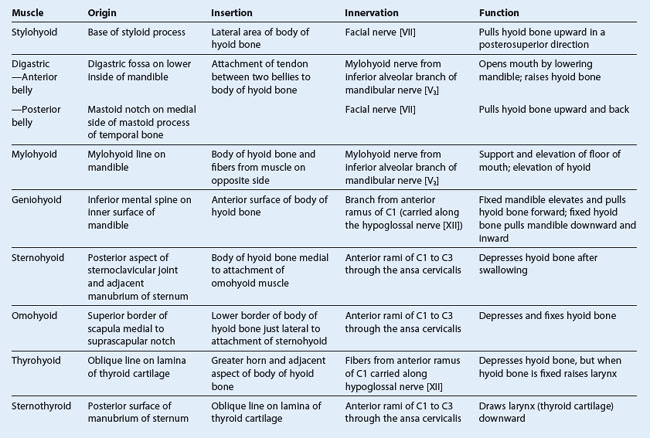
Suprahyoid muscles
The four pairs of suprahyoid muscles are in the submental and submandibular triangles (Fig. 8.157). They pass in a superior direction from the hyoid bone to the skull or mandible and raise the hyoid, as occurs during swallowing.
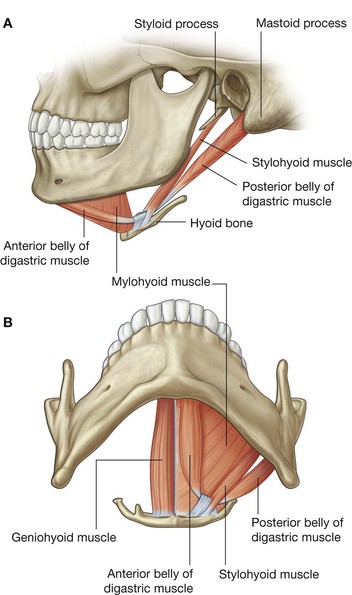
Stylohyoid
The stylohyoid muscle arises from the base of the styloid process and passes anteroinferiorly to attach to the lateral area of the body of the hyoid bone (Fig. 8.158). During swallowing it pulls the hyoid bone posterosuperiorly and it is innervated by the facial nerve [VII].
Digastric
The digastric muscle has two bellies connected by a tendon, which attaches to the body of the hyoid bone (Fig. 8.158):
the
posterior belly arises from the mastoid notch on the medial side of the mastoid process of the temporal bone;
the
anterior belly arises from the digastric fossa on the lower inside of the mandible.
The tendon between the two bellies, which is attached to the body of the hyoid bone, is the point of insertion of both bellies. Because of this arrangement, the muscle has multiple actions depending on which bone is fixed:
when the mandible is fixed, the digastric muscle raises the hyoid bone;
when the hyoid bone is fixed, the digastric muscle opens the mouth by lowering the mandible.
Innervation of the digastric muscle is from two different cranial nerves.
The innervation of the posterior belly of the digastric muscle is by the facial nerve [VII], whereas the anterior belly of the muscle is innervated by the mandibular division [V3] of the trigeminal nerve [V].
Mylohyoid
The mylohyoid muscle is superior to the anterior belly of the digastric and, with its partner from the opposite side, forms the floor of the mouth (Fig. 8.158). It originates from the mylohyoid line on the medial surface of the body of the mandible and inserts into the hyoid bone and also blends with the mylohyoid muscle from the opposite side.
This mylohyoid muscle supports and elevates the floor of the mouth and elevates the hyoid bone. It is innervated by the mandibular division [V3] of the trigeminal nerve [V].
Geniohyoid
The geniohyoid muscle is the final muscle in the suprahyoid group (Fig. 8.158). A narrow muscle, it is superior to the medial part of each mylohyoid muscle. The muscles from each side are next to each other in the midline.
The geniohyoid arises from the inferior mental spine of the mandible and passes backward and downward to insert on the body of the hyoid bone.
It has two functions depending on which bone is fixed:
fixation of the mandible elevates and pulls the hyoid bone forward;
fixation of the hyoid bone pulls the mandible downward and inward.
The geniohyoid is innervated by a branch from the anterior ramus of C1 carried along the hypoglossal nerve [XII].
Infrahyoid muscles
The four infrahyoid muscles are in the muscular triangle (Fig. 8.157). They attach the hyoid bone to inferior structures and depress the hyoid bone. They also provide a stable point of attachment for the suprahyoid muscles. Because of their appearance, they are sometimes referred to as the “strap muscles.”
Sternohyoid
The sternohyoid muscle is a long, thin muscle originating from the posterior aspect of the sternoclavicular joint and adjacent manubrium of sternum (Fig. 8.159). It ascends to insert onto the body of the hyoid bone. It depresses the hyoid bone and is innervated by the anterior rami of C1 to C3 through the ansa cervicalis.
Omohyoid
Lateral to the sternohyoid muscle is the omohyoid muscle (Fig. 8.159). This muscle consists of two bellies with an intermediate tendon in both the posterior and anterior triangles of the neck:
the
inferior belly begins on the superior border of the scapula, medial to the suprascapular notch, and passes forward and upward across the posterior triangle ending at the intermediate tendon;
the
superior belly begins at the intermediate tendon and ascends to attach to the body of the hyoid bone just lateral to the attachment of the sternohyoid;
the intermediate tendon is attached to the clavicle, near its medial end, by a fascial sling.
The omohyoid depresses and fixes the hyoid bone. It is innervated by the anterior rami of C1 to C3 through the ansa cervicalis.
Thyrohyoid
The thyrohyoid muscle is deep to the superior parts of the omohyoid and sternohyoid (Fig. 8.159). Originating at the oblique line on the lamina of the thyroid cartilage it passes upward to insert into the greater horn and adjacent aspect of the body of the hyoid bone.
The thyrohyoid muscle has variable functions depending on which bone is fixed. Generally, it depresses the hyoid, but when the hyoid is fixed it raises the larynx (e.g., when high notes are sung). It is innervated by fibers from the anterior ramus of C1 that travel with the hypoglossal nerve [XII].
Sternothyroid
Lying beneath the sternohyoid and in continuity with the thyrohyoid, the sternothyroid is the last muscle in the infrahyoid group (Fig. 8.159). It arises from the posterior surface of the manubrium of sternum and passes upward to attach to the oblique line on the lamina of the thyroid cartilage.
The sternothyroid muscle draws the larynx (thyroid cartilage) downward and is innervated by the anterior rami of C1 to C3 through the ansa cervicalis.
Vessels
Passing through the anterior triangle of the neck are the common carotid arteries and their branches, the external and internal carotid arteries. These vessels supply all structures of the head and neck.
Associated with this arterial system are the internal jugular vein and its tributaries. These vessels receive blood from all structures of the head and neck.
Carotid system
Common carotid arteries
The common carotid arteries are the beginning of the carotid system (Fig. 8.160):
the
right common carotid artery originates from the brachiocephalic trunk immediately posterior to the right sternoclavicular joint and is entirely in the neck throughout its course;
the
left common carotid artery begins in the thorax as a direct branch of the arch of the aorta and passes superiorly to enter the neck near the left sternoclavicular joint.
Both right and left common carotid arteries ascend through the neck, just lateral to the trachea and esophagus, within a fascial compartment (the carotid sheath). They give off no branches as they pass through the neck.
Near the superior edge of the thyroid cartilage each common carotid artery divides into its two terminal branches—the external and internal carotid arteries (Fig. 8.161).
The superior part of each common carotid artery and its division into external and internal carotid arteries occurs in the carotid triangle (Fig. 8.162), which is a subdivision of the anterior triangle of the neck (see Fig. 8.157).
At the bifurcation, the common carotid artery and the beginning of the internal carotid artery are dilated. This dilation is the carotid sinus and contains receptors that monitor changes in blood pressure and are innervated by a branch of the glossopharyngeal nerve [IX].
Another accumulation of receptors in the area of the bifurcation is responsible for detecting changes in blood chemistry, primarily oxygen content. This is the carotid body and is innervated by branches from both the glossopharyngeal [IX] and vagus [X] nerves.
Internal carotid arteries
After its origin, the internal carotid artery ascends toward the base of the skull (Fig. 8.161). It gives off no branches in the neck and enters the cranial cavity through the carotid canal in the petrous part of the temporal bone.
The internal carotid arteries supply the cerebral hemispheres, the eyes and the contents of the orbits, and the forehead.
External carotid arteries
The external carotid arteries begin giving off branches immediately after the bifurcation of the common carotid arteries (Fig. 8.161 and Table 8.13) as follows:
the
superior thyroid artery is the first branch, arises from the anterior surface near or at the bifurcation, and passes in a downward and forward direction to reach the superior pole of the thyroid gland;
the
ascending pharyngeal artery is the second and smallest branch—it arises from the posterior aspect of the external carotid artery and ascends between the internal carotid artery and the pharynx;
the
lingual artery arises from the anterior surface of the external carotid artery just above the superior thyroid artery at the level of the hyoid bone, passes deep to the hypoglossal nerve [XII], and passes between the middle constrictor and hyoglossus muscles;
the
facial artery is the third anterior branch of the external carotid artery, arises just above the lingual artery, passes deep to the stylohyoid and posterior belly of the digastric muscles, continues deep between the submandibular gland and mandible, and emerges over the edge of the mandible just anterior to the masseter muscle, to enter the face;
the
occipital artery arises from the posterior surface of the external carotid artery, near the level of origin of the facial artery, passes upward and posteriorly deep to the posterior belly of the digastric muscle, and emerges on the posterior aspect of the scalp;
the
posterior auricular artery is a small branch arising from the posterior surface of the external carotid artery, and passes upward and posteriorly;
the
superficial temporal artery is one of the terminal branches and appears as an upward continuation of the external carotid artery—beginning posterior to the neck of mandible, it passes anterior to the ear, crosses the zygomatic process of the temporal bone, and above this point divides into anterior and posterior branches;
the
maxillary artery is the larger of the two terminal branches of the external carotid artery—arising posterior to the neck of mandible, it passes through the parotid gland, continues medial to the neck of mandible and into the infratemporal fossa, and continues through this area into the pteryatine fossa.
Table 8.13 Branches of the external carotid artery
| Branch |
Supplies |
| Superior thyroid artery |
Thyrohyoid muscle, internal structures of the larynx, sternocleidomastoid and cricothyroid muscles, thyroid gland |
| Ascending pharyngeal artery |
Pharyngeal constrictors and stylopharyngeus muscle, palate, tonsil, pharyngotympanic tube, meninges in posterior cranial fossa |
| Lingual artery |
Muscles of the tongue, palatine tonsil, soft palate, epiglottis, floor of mouth, sublingual gland |
| Facial artery |
All structures in the face from the inferior border of the mandible anterior to the masseter muscle to the medial corner of the eye, the soft palate, palatine tonsil, pharyngotympanic tube, submandibular gland |
| Occipital artery |
Sternocleidomastoid muscle, meninges in posterior cranial fossa, mastoid cells, deep muscles of the back, posterior scalp |
| Posterior auricular artery |
Parotid gland and nearby muscles, external ear and scalp posterior to ear, middle and inner ear structures |
| Superficial temporal artery |
Parotid gland and duct, masseter muscle, lateral face, anterior part of external ear, temporalis muscle, parietal and temporal fossae |
| Maxillary artery |
External acoustic meatus, lateral and medial surface of tympanic membrane, temporomandibular joint, dura mater on lateral wall of skull and inner table of cranial bones, trigeminal ganglion and dura in vicinity, mylohyoid muscle, mandibular teeth, skin on chin, temporalis muscle, outer table of bones of skull in temporal fossa, structures in infratemporal fossa, maxillary sinus, upper teeth and gingivae, infra-orbital skin, palate, roof of pharynx, nasal cavity |
Veins
Collecting blood from the skull, brain, superficial face, and parts of the neck, the internal jugular vein begins as a dilated continuation of the sigmoid sinus, which is a dural venous sinus. This initial dilated part is referred to as the superior bulb of jugular vein and receives another dural venous sinus (the inferior petrosal sinus) soon after it is formed. It exits the skull through the jugular foramen associated with the glossopharyngeal [IX], vagus [X], and accessory [XI] nerves, and enters the carotid sheath.
The internal jugular vein traverses the neck within the carotid sheath, initially posterior to the internal carotid artery, but passes to a more lateral position farther down. It remains lateral to the common carotid artery through the rest of the neck with the vagus nerve [X] posterior and partially between the two vessels.
The paired internal jugular veins join with the subclavian veins posterior to the sternal end of the clavicle to form the right and left brachiocephalic veins (Fig. 8.160).
Tributaries to each internal jugular vein include the inferior petrosal sinus, and the facial, lingual, pharyngeal, occipital, superior thyroid, and middle thyroid veins.
In the clinic
Jugular venous pulse
The jugular venous pulse is an important clinical sign that enables the physician to assess the venous pressure and waveform and is a reflection of the functioning of the right side of the heart.
Nerves
Numerous cranial and peripheral nerves:
pass through the anterior triangle of the neck as they continue to their final destination;
send branches to structures in or forming boundaries of the anterior triangle of the neck; and
while in the anterior triangle of the neck, send branches to nearby structures.
The cranial nerves in these categories include the facial [VII], glossopharyngeal [IX], vagus [X], accessory [XI], and hypoglossal [XII].
Branches of spinal nerves in these categories include the transverse cervical nerve from the cervical plexus and the upper and lower roots of the ansa cervicalis.
Facial nerve [VII]
After emerging from the stylomastoid foramen, the facial nerve [VII] gives off branches that innervate two muscles associated with the anterior triangle of the neck:
the posterior belly of the digastric;
stylohyoid.
The facial nerve [VII] also innervates platysma muscle that overlies the anterior triangle and part of the posterior triangle of the neck.
Glossopharyngeal nerve [IX]
The glossopharyngeal nerve [IX] leaves the cranial cavity through the jugular foramen. It begins its descent between the internal carotid artery and the internal jugular vein, lying deep to the styloid process and the muscles associated with the styloid process. As the glossopharyngeal nerve [IX] completes its descent, it passes forward between the internal and external carotid arteries, and curves around the lateral border of the stylopharyngeus muscle (Fig. 8.163). At this point, it continues in an anterior direction, deep to the hyoglossus muscle, to reach the base of the tongue and the area of the palatine tonsil.
As the glossopharyngeal nerve [IX] passes through the area of the anterior triangle of the neck it innervates the stylopharyngeus muscle, sends a branch to the carotid
sinus, and supplies sensory branches to the pharynx.
Vagus nerve [X]
The vagus nerve [X] exits the cranial cavity through the jugular foramen between the glossopharyngeal [IX] and accessory [XI] nerves.
Outside the skull the vagus nerve [X] enters the carotid sheath and descends through the neck enclosed in this structure medial to the internal jugular vein and posterior to the internal carotid and common carotid arteries (Fig. 8.164).
Branches of the vagus nerve [X] as it passes through the anterior triangle of the neck include a motor branch to the pharynx, a branch to the carotid body, the superior laryngeal nerve (which divides into external and internal laryngeal branches), and possibly a cardiac branch.
Accessory nerve [XI]
The accessory nerve [XI] is the most posterior of the three cranial nerves exiting the cranial cavity through the jugular foramen. It begins its descent medial to the internal jugular vein, emerging from between the internal jugular vein and internal carotid artery to cross the lateral surface of the internal jugular vein as it passes downward and backward to disappear either into or beneath the anterior border of the sternocleidomastoid muscle (Fig. 8.165).
The accessory nerve gives off no branches as it passes through the anterior triangle of the neck.
Hypoglossal nerve [XII]
The hypoglossal nerve [XII] leaves the cranial cavity through the hypoglossal canal and is medial to the internal jugular vein and internal carotid artery immediately outside the skull. As it descends, it passes outward between the internal jugular vein and internal carotid artery (Fig. 8.166). At this point it passes forward, hooking around the occipital artery, across the lateral surfaces of the internal and external carotid arteries and the lingual artery, and then continues deep to the posterior belly of the digastric and stylohyoid muscles. It passes over the surface of the hyoglossus muscle and disappears deep to the mylohyoid muscle.
The hypoglossal nerve [XII], which supplies the tongue, does not give off any branches as it passes through the anterior triangle of the neck.
Transverse cervical nerve
The transverse cervical nerve is a branch of the cervical plexus arising from the anterior rami of cervical nerves C2 and C3. It emerges from beneath the posterior border of the sternocleidomastoid muscle, near the middle of the muscle, and loops around the sternocleidomastoid to cross its anterior surface in a transverse direction (Fig. 8.167). It continues across the neck and provides cutaneous innervation to this area.
Ansa cervicalis
The ansa cervicalis is a loop of nerve fibers from cervical nerves C1 to C3 that innervate the “strap muscles” in the anterior triangle of the neck (Fig. 8.168). It begins as branches from the cervical nerve C1 join the hypoglossal nerve [XII] soon after it leaves the skull.
As the hypoglossal nerve [XII] completes its descent and begins to pass forward across the internal and external carotid arteries, some of the cervical nerve fibers leave it and descend between the internal jugular vein and the internal, and then common, carotid arteries. These nerve fibers are the superior root of the ansa cervicalis and innervate the superior belly of the omohyoid muscle, and the upper parts of the sternohyoid and sternothyroid muscles.
Completing the loop is a direct branch from the cervical plexus containing nerve fibers from the second and third cervical nerves C2 and C3 (Fig. 8.168). This is the inferior root of the ansa cervicalis. It descends either medial or lateral to the internal jugular vein before turning medially to join the superior root. At this location, the ansa cervicalis gives off branches that innervate the inferior belly of the omohyoid, and the lower parts of the sternohyoid and sternothyroid muscles.
Thyroid and parathyroid glands
The thyroid and parathyroid glands are endocrine glands positioned anteriorly in the neck.
Both glands begin as pharyngeal outgrowths that migrate caudally to their final position as development continues.
The thyroid gland is a large, unpaired gland, while the parathyroid glands, usually four in number, are small and are on the posterior surface of the thyroid gland.
Thyroid gland
The thyroid gland is anterior in the neck below and lateral to the thyroid cartilage (Fig. 8.169). It consists of two lateral lobes (which cover the anterolateral surfaces of the trachea, the cricoid cartilage, and the lower part of the thyroid cartilage) with an isthmus that connects the lateral lobes and crosses the anterior surfaces of the second and third tracheal cartilages.
Lying deep to the sternohyoid, sternothyroid, and omohyoid muscles, the thyroid gland is in the visceral compartment of the neck. This compartment also includes the pharynx, trachea, and esophagus and is surrounded by the pretracheal layers of fascia.
The thyroid gland arises as a median outgrowth from the floor of the pharynx near the base of the tongue. The foramen cecum of the tongue indicates the site of origin and the thyroglossal duct marks the path of migration of the thyroid gland to its final adult location. The thyroglossal duct usually disappears early in development, but remnants may persist as a cyst or as a connection to the foramen cecum (i.e., a fistula).
There may also be functional thyroid gland:
associated with the tongue (a lingual thyroid);
anywhere along the path of migration of the thyroid gland; or
extending upward from the gland along the path of the thyroglossal duct (a pyramidal lobe).
Arterial supply
Two major arteries supply the thyroid gland.
Superior thyroid artery.
The superior thyroid artery is the first branch of the external carotid artery (Fig. 8.170). It descends, passing along the lateral margin of the thyrohyoid muscle, to reach the superior pole of the lateral lobe of the gland where it divides into anterior and posterior glandular branches:
the
anterior glandular branch passes along the superior border of the thyroid gland and anastomoses with its twin from the opposite side across the isthmus;
the
posterior glandular branch passes to the posterior side of the gland and may anastomose with the inferior thyroid artery (
Fig. 8.171).
Inferior thyroid artery.
The inferior thyroid artery is a branch of the thyrocervical trunk, which arises from the first part of the subclavian artery (Figs. 8.170 and 8.171). It ascends along the medial edge of the anterior scalene muscle, passes posteriorly to the carotid sheath, and reaches the inferior pole of the lateral lobe of the thyroid gland.
At the thyroid gland the inferior thyroid artery divides into an:
inferior branch, which supplies the lower part of the thyroid gland and anastomoses with the posterior branch of the superior thyroid artery; and
an ascending branch, which supplies the parathyroid glands.
Occasionally, a small thyroid ima artery arises from the brachiocephalic trunk or the arch of the aorta and ascends on the anterior surface of the trachea to supply the thyroid gland.
Venous and lymphatic drainage
Three veins drain the thyroid gland (Fig. 8.170):
the
superior thyroid vein primarily drains the area supplied by the superior thyroid artery;
the
middle and
inferior thyroid veins drain the rest of the thyroid gland.
The superior and middle thyroid veins drain into the internal jugular vein, and the inferior thyroid veins empty into the right and left brachiocephalic veins, respectively.
Lymphatic drainage of the thyroid gland is to nodes beside the trachea (paratracheal nodes) and to deep cervical nodes inferior to the omohyoid muscle along the internal jugular vein.
Recurrent laryngeal nerves
The thyroid gland is closely related to the recurrent laryngeal nerves. After branching from the vagus nerve [X] and looping around the subclavian artery on the right and the arch of the aorta on the left, the recurrent laryngeal nerves ascend in a groove between the trachea and esophagus (Fig. 8.171). They pass deep to the posteromedial surface of the lateral lobes of the thyroid gland and enter the larynx by passing deep to the lower margin of the inferior constrictor of the pharynx.
Together with branches of the inferior thyroid arteries, the recurrent laryngeal nerves are clearly related to, and may pass through ligaments, one on each side, that bind the thyroid gland to the trachea and to the cricoid cartilage of the larynx. These relationships need to be considered when surgically removing or manipulating the thyroid gland.
Parathyroid glands
The parathyroid glands are two pairs of small, ovoid, yellowish structures on the deep surface of the lateral lobes of the thyroid gland. They are designated as the superior and inferior parathyroid glands (Fig. 8.171). However, their position is quite variable and they may be anywhere from the carotid bifurcation superiorly to the mediastinum inferiorly.
Derived from the third (the inferior parathyroid glands) and fourth (the superior parathyroid glands) pharyngeal pouches, these paired structures migrate to their final adult position and are named accordingly.
The arteries supplying the parathyroid glands are the inferior thyroid arteries, and venous and lymphatic drainage follows that described for the thyroid gland.
In the clinic
Thyroid gland
The thyroid gland develops from a small region of tissue near the base of the tongue. This tissue descends as the thyroglossal duct from the foramen cecum in the posterior aspect of the tongue to pass adjacent to the anterior aspect of the middle of the hyoid bone. The thyroid tissue continues to migrate inferiorly and eventually comes to rest at the anterior aspect of the trachea in the root of the neck.
Consequently, the migration of thyroid tissue may be arrested anywhere along the embryological descent of the gland. Ectopic thyroid tissue is relatively rare. More frequently seen is the cystic change that arises from the thyroglossal duct. The usual symptom of a thyroglossal duct cyst is a midline mass. Ultrasound easily demonstrates its nature and position, and treatment is by surgical excision. The whole of the duct as well as a small part of the anterior aspect of the hyoid bone must be excised to prevent recurrence.
In the clinic
Thyroidectomy
A thyroidectomy is a relatively common surgical procedure. In most cases it involves excision of part or most of the thyroid gland, leaving some gland behind. This surgical procedure is usually carried out for benign diseases, such as multinodular goiter. However, thyroid carcinoma, albeit rare, is also an indication for thyroidectomy.
Given the location of the thyroid gland, there is a possibility of damaging other structures when carrying out a thyroidectomy, namely the parathyroid glands (which may be excised en masse with the thyroid gland), the recurrent laryngeal nerve, the sympathetic trunk, and rarely, the nerves of the carotid sheath.
In the clinic
Thyroid gland pathology
Thyroid gland pathology is extremely complex. In essence, thyroid gland pathology should be assessed from two points of view. First, the thyroid gland may be diffusely or focally enlarged, for which there are numerous causes. Second, the thyroid gland may undersecrete or oversecrete the hormone thyroxine.
One of the commonest disorders of the thyroid gland is a multinodular goiter, which is a diffuse irregular enlargement of the thyroid gland with areas of thyroid hypertrophy and colloid cyst formation. Most patients are euthyroid (i.e., have normal serum thyroxine levels). The typical symptom is a diffuse mass in the neck, which may be managed medically or may need surgical excision if the mass is large enough to affect the patient’s life or cause respiratory problems.
Isolated nodules in the thyroid gland may be a dominant nodule in a multinodular gland or possibly an isolated tumor of the thyroid gland. Isolated tumors may or may not secrete thyroxine depending on their cellular morphology. Treatment is usually by excision.
Immunological diseases may affect the thyroid gland and may overstimulate it to produce excessive thyroxine. These diseases may be associated with other extrathyroid manifestations, which include exophthalmos, pretibial myxedema, and nail changes. Other causes of diffuse thyroid stimulation include viral thyroiditis. Some diseases may cause atrophy of the thyroid gland, leading to undersecretion of thyroxine (myxedema).
Location of structures in different regions of the anterior triangle of the neck
The regional location of major structures in the anterior triangle of the neck is summarized in Table 8.14. Structures can be identified as being within a specific subdivision, passing into a specific subdivision from outside the area, originating in one subdivision and passing to another subdivision, or passing through several subdivisions while traversing the region.
Table 8.14 Subdivisions of the anterior triangle of the neck—a regional approach
| Subdivision |
Boundaries |
Contents |
| Submental triangle (unpaired) |
Mandibular symphysis; anterior belly of digastric muscle; body of hyoid bone |
Submental lymph nodes; tributaries forming the anterior jugular vein |
| Submandibular triangle (paired) |
Lower border of mandible; anterior belly of digastric muscle; posterior belly of digastric muscle |
Submandibular gland; submandibular lymph nodes; hypoglossal nerve [XII]; mylohyoid nerve; facial artery and vein |
| Carotid triangle (paired) |
Posterior belly of digastric muscle; superior belly of omohyoid muscle; anterior border of sternocleidomastoid muscle |
Tributaries to common facial vein; cervical branch of facial nerve [VII]; common carotid artery; external and internal carotid arteries; superior thyroid; ascending pharyngeal; lingual, facial, and occipital arteries; internal jugular vein; vagus [X], accessory [XI], and hypoglossal [XII] nerves; superior and inferior roots of ansa cervicalis; transverse cervical nerve |
| Muscular triangle (paired) |
Midline of neck; superior belly of omohyoid muscle; anterior border of sternocleidomastoid muscle |
Sternohyoid, omohyoid, sternohyoid, and thyrohyoid muscles; thyroid and parathyroid glands; pharynx |
Posterior triangle of the neck
The posterior triangle of the neck is on the lateral aspect of the neck in direct continuity with the upper limb. It is bordered:
anteriorly by the posterior edge of the sternocleidomastoid muscle;
posteriorly by the anterior edge of the trapezius muscle;
basally by the middle one-third of the clavicle; and
apically by the occipital bone just posterior to the mastoid process where the attachments of the trapezius and sternocleidomastoid come together (
Fig. 8.172).
The roof of the posterior triangle consists of an investing layer of cervical fascia that surrounds the sternocleidomastoid and trapezius muscles as it passes through the region.
The muscular floor of the posterior triangle is covered by the prevertebral layer of cervical fascia; and from superior to inferior consists of the splenius capitis, levator scapulae, and the posterior, middle, and anterior scalene muscles.
Muscles
Numerous muscles participate in forming the borders and floor of the posterior triangle of the neck (Table 8.15).
In addition, the omohyoid muscle passes across the inferior part of the posterior triangle before disappearing under the sternocleidomastoid muscle and emerging in the anterior triangle (Fig. 8.173). It is enclosed in the investing layer of cervical fascia and crosses the posterior triangle from lateral to medial as it continues in a superior direction. It originates on the superior border of the scapula, just medial to the scapular notch and eventually inserts into the inferior border of the body of the hyoid bone. It has two bellies connected by a tendon, which is anchored by a fascial sling to the clavicle:
the
superior belly is in the anterior triangle;
the
inferior belly crosses the posterior triangle, subdividing it into a small,
omoclavicular or subclavian triangle inferiorly and a much larger
occipital triangle superiorly.
The omohyoid is innervated by branches of the ansa cervicalis (anterior rami from C1 to C3) and it depresses the hyoid bone.
Vessels
External jugular vein
One of the most superficial structures passing through the posterior triangle of the neck is the external jugular vein (Fig. 8.174). This large vein forms near the angle of mandible, when the posterior branch of the retromandibular and posterior auricular veins join, and descends through the neck in the superficial fascia.
After crossing the sternocleidomastoid muscle, the external jugular vein enters the posterior triangle and continues its vertical descent.
In the lower part of the posterior triangle, the external jugular vein pierces the investing layer of cervical fascia and ends in the subclavian vein.
Tributaries to the external jugular vein while it traverses the posterior triangle of the neck include the transverse cervical, suprascapular, and anterior jugular veins.
Subclavian artery and its branches
Several arteries are found within the boundaries of the posterior triangle of the neck. The largest is the third part of the subclavian artery as it crosses the base of the posterior triangle (Fig. 8.175).
The first part of the subclavian artery ascends to the medial border of the anterior scalene muscle from either the brachiocephalic trunk on the right side or directly from the arch of the aorta on the left side. It has numerous branches.
The second part of the subclavian artery passes laterally between the anterior and middle scalene muscles, and one branch may arise from it.
The third part of the subclavian artery emerges from between the anterior and middle scalene muscles to cross the base of the posterior triangle (Fig. 8.175). It extends from the lateral border of the anterior scalene muscle to the lateral border of rib I where it becomes the axillary artery and continues into the upper limb.
A single branch (the dorsal scapular artery) may arise from the third part of the subclavian artery. This branch passes posterolaterally to reach the superior angle of the scapula where it descends along the medial border of the scapula posterior to the rhomboid muscles.
Transverse cervical and suprascapular arteries
Two other small arteries also cross the base of the posterior triangle. These are the transverse cervical and the suprascapular arteries (Fig. 8.175). They are both branches of the thyrocervical trunk, which arises from the first part of the subclavian artery.
After branching from the thyrocervical trunk, the transverse cervical artery passes laterally and slightly posteriorly across the base of the posterior triangle anterior to the anterior scalene muscle and the brachial plexus. Reaching the deep surface of the trapezius muscle, it divides into superficial and deep branches:
the
superficial branch continues on the deep surface of the trapezius muscle;
the
deep branch continues on the deep surface of the rhomboid muscles near the medial border of the scapula.
The suprascapular artery, also a branch of the thyrocervical trunk, passes laterally, in a slightly downward direction across the lowest part of the posterior triangle, and ends up posterior to the clavicle (Fig. 8.175). Approaching the scapula, it passes over the superior transverse scapular ligament and distributes branches to muscles on the posterior surface of the scapula.
Veins
Veins accompany all the arteries described previously.
The subclavian vein is a continuation of the axillary vein and begins at the lateral border of rib I. As it crosses the base of the posterior triangle, the external jugular, and, possibly, the suprascapular and transverse cervical veins enter it (Fig. 8.175). It ends by joining with the internal jugular vein to form the brachiocephalic vein near the sternoclavicular joint. In the posterior triangle it is anterior to, and slightly lower than, the subclavian artery and passes anterior to the anterior scalene muscle.
Transverse cervical and suprascapular veins travel with each of the similarly named arteries. These veins become tributaries to either the external jugular vein or the initial part of the subclavian vein.
Nerves
A variety of nerves pass through or are within the posterior triangle. These include the accessory nerve [XI], branches of the cervical plexus, components forming the brachial plexus, and branches of the brachial plexus.
Accessory nerve
The accessory nerve [XI] exits the cranial cavity through the jugular foramen. It descends through the neck in a posterior direction, to reach the anterior border of the sternocleidomastoid muscle. Passing either deep to or through and innervating the sternocleidomastoid muscle, the accessory nerve [XI] continues to descend and enters the posterior triangle (Fig. 8.176). It crosses the posterior triangle, still in an obliquely downward direction, within the investing layer of cervical fascia as this fascia crosses between the sternocleidomastoid and trapezius muscles. When the accessory nerve [XI] reaches the anterior border of the trapezius muscle, it continues on the deep surface of the trapezius and innervates it.
The superficial location of the accessory nerve as it crosses the posterior triangle makes it susceptible to injury.
Cervical plexus
The cervical plexus is formed by the anterior rami of cervical nerves C2 to C4, and possibly a contribution from the anterior ramus of cervical nerve C1 (Fig. 8.177).
The cervical plexus forms in the substance of the muscles making up the floor of the posterior triangle within the prevertebral layer of cervical fascia, and consists of:
muscular (or deep) branches;
cutaneous (or superficial) branches.
The cutaneous branches are visible in the posterior triangle emerging from beneath the posterior border of the sternocleidomastoid muscle.
Muscular branches
Muscular (deep) branches of the cervical plexus distribute to several groups of muscles. A major branch is the phrenic nerve, which supplies the diaphragm with both sensory and motor innervation (Fig. 8.177). It arises from the anterior rami of cervical nerves C3 to C5. Hooking around the upper lateral border of the anterior scalene muscle, the nerve continues inferiorly across the anterior surface of the anterior scalene within the prevertebral fascia to enter the thorax (Fig. 8.175). As the nerve descends in the neck, it is “pinned” to the anterior scalene muscle by the transverse cervical and suprascapular arteries.
Several muscular branches of the cervical plexus supply prevertebral and lateral vertebral muscles, including the rectus capitis anterior, rectus capitis lateralis, longus colli, and longus capitis (Fig. 8.178 and Table 8.16).
The cervical plexus also contributes to the formation of the superior and inferior roots of the ansa cervicalis (Fig. 8.177). This loop of nerves receives contributions from the anterior rami of the cervical nerves C1 to C3 and innervates the infrahyoid muscles.
Cutaneous branches
Cutaneous (superficial) branches of the cervical plexus are visible in the posterior triangle as they pass outward from the posterior border of the sternocleidomastoid muscle (Figs. 8.176 and 8.177):
the
lesser occipital nerve consists of contributions from cervical nerve C2 (
Fig. 8.177), ascends along the posterior border of the sternocleidomastoid muscle, and distributes to the skin of the neck and scalp posterior to the ear;
the
great auricular nerve consists of branches from cervical nerves C2 and C3, emerges from the posterior border of the sternocleidomastoid muscle, and ascends across the muscle to the base of the ear, supplying the skin of the parotid region, the ear, and the mastoid area;
the
transverse cervical nerve consists of branches from the cervical nerves C2 and C3, passes around the midpart of the sternocleidomastoid muscle, and continues horizontally across the muscle to supply the lateral and anterior parts of the neck;
the
supraclavicular nerves are a group of cutaneous nerves from cervical nerves C3 and C4 that, after emerging from beneath the posterior border of the sternocleidomastoid muscle, descend and supply the skin over the clavicle and shoulder as far inferiorly as rib II.
Brachial plexus
The brachial plexus forms from the anterior rami of cervical nerves C5 to C8 and thoracic nerve T1. The contributions of each of these nerves, which are between the anterior and middle scalene muscles, are the roots of the brachial plexus. As the roots emerge from between these muscles, they form the next component of the brachial plexus (the trunks) as follows:
the anterior rami of C5 and C6 form the upper trunk;
the anterior ramus of C7 forms the middle trunk;
the anterior rami of C8 and T1 form the lower trunk.
The trunks cross the base of the posterior triangle (Fig. 8.175). Several branches of the brachial plexus may be visible in the posterior triangle (see Fig. 7.52). These include the:
dorsal scapular nerve to the rhomboid muscles;
long thoracic nerve to the serratus anterior muscle;
nerve to the subclavius muscle; and
suprascapular nerve to the supraspinatus and infraspinatus muscles.
Root of the neck
The root of the neck (Fig. 8.179) is the area immediately superior to the superior thoracic aperture and axillary inlets. It is bounded by:
the top of the manubrium of sternum and superior margin of the clavicle anteriorly; and
the top of the thoracic vertebra TI and the superior margin of the scapula to the coracoid process posteriorly.
It contains structures passing between the neck, thorax, and upper limb. There is also an extension of the thoracic cavity projecting into the root of the neck. This consists of an upward projection of the pleural cavity, on both sides, and includes the cervical part of the parietal pleura (cupula), and the apical part of the superior lobe of each lung.
Anteriorly, the pleural cavity extends above the top of the manubrium of sternum and superior border of rib I, while posteriorly, due to the downward slope of the superior thoracic aperture the pleural cavity remains below the top of vertebra TI.
Vessels
Subclavian arteries
The subclavian arteries on both sides arch upward out of the thorax to enter the root of the neck (Fig. 8.180).
The right subclavian artery begins posterior to the sternoclavicular joint as one of two terminal branches of the brachiocephalic trunk. It arches superiorly and laterally to pass anterior to the extension of the pleural cavity in the root of the neck and posterior to the anterior scalene muscle. Continuing laterally across rib I, it becomes the axillary artery as it crosses its lateral border.
The left subclavian artery begins lower in the thorax than the right subclavian artery as a direct branch of the arch of the aorta. Lying posterior to the left common carotid artery and lateral to the trachea, it ascends and arches laterally, passing anterior to the extension of the pleural cavity and posterior to the anterior scalene muscle. It continues laterally over rib I, and becomes the axillary artery as it crosses the lateral border of rib I.
Both subclavian arteries are divided into three parts by the anterior scalene muscle (Fig. 8.180):
the first part extends from the origin of the artery to the anterior scalene muscle;
the second part is the part of the artery posterior to the anterior scalene muscle;
the third part is the part lateral to the anterior scalene muscle before the artery reaches the lateral border of rib I.
All branches from the right and left subclavian arteries arise from the first part of the artery, except in the case of one branch (the costocervical trunk) on the right side (Fig. 8.180). The branches include the vertebral artery, the thyrocervical trunk, the internal thoracic artery, and the costocervical trunk.
Vertebral artery
The vertebral artery is the first branch of the subclavian artery as it enters the root of the neck (Fig. 8.180). A large branch, arising from the first part of the subclavian artery medial to the anterior scalene muscle, it ascends and enters the foramen in the transverse process of vertebra CVI. Continuing to pass superiorly, the vertebral artery passes through the foramina of vertebrae CV to CI. At the superior border of vertebra CI, the artery turns medially and crosses the posterior arch of vertebra CI. From here it passes through the foramen magnum to enter the posterior cranial fossa.
Thyrocervical trunk
The second branch of the subclavian artery is the thyrocervical trunk (Fig. 8.180). It arises from the first part of the subclavian artery medial to the anterior scalene muscle, and divides into three branches—the inferior thyroid, the transverse cervical, and the suprascapular arteries.
Inferior thyroid artery.
The inferior thyroid artery (Fig. 8.180) is the superior continuation of the thyrocervical trunk. It ascends, anterior to the anterior scalene muscle, and eventually turns medially, crossing posterior to the carotid sheath and its contents and anterior to the vertebral artery. Reaching the posterior surface of the thyroid gland it supplies the thyroid gland.
When the inferior thyroid artery turns medially, it gives off an important branch (the ascending cervical artery), which continues to ascend on the anterior surface of the prevertebral muscles, supplying these muscles and sending branches to the spinal cord.
Transverse cervical artery.
The middle branch of the thyrocervical trunk is the transverse cervical artery (Fig. 8.180). This branch passes laterally, across the anterior surface of the anterior scalene muscle and the phrenic nerve, and enters and crosses the base of the posterior triangle of the neck. It continues to the deep surface of the trapezius muscle, where it divides into superficial and deep branches:
the
superficial branch continues on the deep surface of the trapezius muscle;
the
deep branch continues on the deep surface of the rhomboid muscles near the medial border of the scapula.
Suprascapular artery.
The lowest branch of the thyrocervical trunk is the suprascapular artery (Fig. 8.180). This branch passes laterally, crossing anterior to the anterior scalene muscle, the phrenic nerve, the third part of the subclavian artery, and the trunks of the brachial plexus. At the superior border of the scapula, it crosses over the superior transverse scapular ligament and enters the supraspinatus fossa.
Internal thoracic artery
The third branch of the subclavian artery is the internal thoracic artery (Fig. 8.180). This artery branches from the inferior edge of the subclavian artery and descends.
It passes posterior to the clavicle and the large veins in the region and anterior to the pleural cavity. It enters the thoracic cavity posterior to the ribs and anterior to the transversus thoracis muscle and continues to descend giving off numerous branches.
Costocervical trunk
The final branch of the subclavian artery in the root of the neck is the costocervical trunk (Fig. 8.180). It arises in a slightly different position, depending on the side:
on the left, it arises from the first part of the subclavian artery, just medial to the anterior scalene muscle;
on the right, it arises from the second part of the subclavian artery.
On both sides, the costocervical trunk ascends and passes posteriorly over the dome of the pleural cavity and continues in a posterior direction behind the anterior scalene muscle. Eventually it divides into two branches—the deep cervical and the supreme intercostal arteries:
the
deep cervical artery ascends in the back of the neck and anastomoses with the descending branch of the occipital artery;
the
supreme intercostal artery descends anterior to rib I and divides to form the posterior intercostal arteries for the first two intercostal spaces.
Veins
Numerous veins pass through the root of the neck. Small veins accompany each of the arteries described above, and large veins form major drainage channels.
The subclavian veins begin at the lateral margin of rib I as continuations of the axillary veins. Passing medially on each side, just anterior to the anterior scalene muscles, each subclavian vein is joined by the internal jugular vein to form the brachiocephalic veins.
The only tributary to the subclavian veins are the external jugular veins.
The veins accompanying the numerous arteries in this region empty into other veins.
Nerves
Several nerves and components of the nervous system pass through the root of the neck.
Phrenic nerves
The phrenic nerves are branches of the cervical plexus and arise on each side as contributions from the anterior rami of cervical nerves C3 to C5 come together. Passing around the upper lateral border of each anterior scalene muscle, the phrenic nerves continue inferiorly across the anterior surface of each anterior scalene muscle within the prevertebral layer of cervical fascia (Fig. 8.181). Leaving the lower edge of the anterior scalene muscle each phrenic nerve passes between the subclavian vein and artery to enter the thorax and continue to the diaphragm.
Vagus nerves [X]
The vagus nerves [X] descend through the neck within the carotid sheath, posterior to and just between the common carotid artery and the internal jugular vein.
In the lower part of the neck, the vagus nerves [X] give off cardiac branches, which continue downward and medially, passing posterior to the subclavian arteries to disappear into the thorax.
In the root of the neck, each vagus nerve [X] passes anterior to the subclavian artery and posterior to the subclavian vein as it enters the thorax (Fig. 8.181).
Recurrent laryngeal nerves
The right and left recurrent laryngeal nerves are visible as they originate in (the right recurrent laryngeal nerve), or pass through (the left recurrent laryngeal nerve), the root of the neck.
The right recurrent laryngeal nerve is a branch of the right vagus nerve [X] as it reaches the lower edge of the first part of the subclavian artery in the root of the neck (Fig. 8.181). It passes around the subclavian artery and upward and medially in a groove between the trachea and the esophagus as it heads to the larynx.
The left recurrent laryngeal nerve is a branch of the left vagus nerve [X] as it crosses the arch of the aorta in the superior mediastinum. It passes below and behind the arch of the aorta and ascends beside the trachea to the larynx.
Sympathetic nervous system
Various components of the sympathetic nervous system are visible as they pass through the root of the neck. These include:
the cervical part of the sympathetic trunk;
the ganglia associated with the cervical part of the sympathetic trunk; and
cardiac nerves branching from the cervical part of the sympathetic trunk (
Fig. 8.182).
The sympathetic trunks are two parallel cords that run from the base of the skull to the coccyx. Along the way they are punctuated by ganglia, which are collections of neuronal cell bodies outside the CNS.
Cervical part of the sympathetic trunk
The cervical part of the sympathetic trunk is anterior to the longus colli and longus capitis muscles, and posterior to the common carotid artery in the carotid sheath and the internal carotid artery. It is connected to each cervical spinal nerve by a gray ramus communicans (Fig. 8.183). There are no white rami communicantes in the cervical region.
Ganglia
Three ganglia are usually described along the course of the sympathetic trunk in the cervical region, and in these ganglia ascending preganglionic sympathetic fibers from the upper thoracic spinal cord levels synapse with postganglionic sympathetic fibers. The postganglionic sympathetic fibers are distributed in branches from these ganglia.
Superior cervical ganglion.
A very large superior cervical ganglion in the area of cervical vertebrae CI and CII marks the superior extent of the sympathetic trunk (Figs. 8.182 and 8.183). Its branches pass to:
the internal carotid and external carotid arteries, forming plexuses around these vessels;
cervical spinal nerves C1 to C4 through gray rami communicantes;
the pharynx; and
the heart as
superior cardiac nerves.
Middle cervical ganglion.
A second ganglion inferior to the superior cervical ganglion along the course of the sympathetic trunk (the middle cervical ganglion) is encountered at about the level of cervical vertebra CVI (Figs. 8.182 and 8.183). Branches from this ganglion pass to:
cervical spinal nerves C5 and C6 through gray rami communicantes; and
the heart as
middle cardiac nerves.
Inferior cervical ganglion
At the lower end of the cervical part of the sympathetic trunk is another ganglion (the inferior cervical ganglion), which becomes very large when it combines with the first thoracic ganglion and forms the cervicothoracic ganglion (stellate ganglion). The inferior cervical ganglion (Figs. 8.182 and 8.183) is anterior to the neck of rib I and the transverse process of cervical vertebra CVII, and posterior to the first part of the subclavian artery and the origin of the vertebral artery.
Branches from this ganglion pass to:
spinal nerves C7 to T1 through gray rami communicantes;
the vertebral artery, forming a plexus associated with this vessel; and
the heart as
inferior cardiac nerves.
This ganglion may also receive white rami communicantes from thoracic spinal nerve T1, and occasionally, from T2.
Lymphatics
Thoracic duct
The thoracic duct is a major lymphatic channel that begins in the abdomen, passes superiorly through the thorax, and ends in the venous channels in the neck. It passes through the lower thoracic cavity in the midline with:
the thoracic aorta on the left;
the azygos vein on the right; and
the esophagus anteriorly.
At about the level of thoracic vertebra TV the thoracic duct passes to the left and continues to ascend just to the left of the esophagus. It passes through the superior mediastinum and enters the root of the neck to the left of the esophagus (Fig. 8.184). Arching laterally, it passes posterior to the carotid sheath and turns inferiorly in front of the thyrocervical trunk, the phrenic nerve, and the vertebral artery.
The thoracic duct terminates in the junction between the left internal jugular and the left subclavian veins. Near its junction with the venous system it is joined by:
the
left jugular trunk, which drains lymph from the left side of the head and neck;
the
left subclavian trunk, which drains lymph from the left upper limb; and
occasionally, the
left bronchomediastinal trunk, which drains lymph from the left half of the thoracic structures (
Fig. 8.185).
A similar confluence of three lymphatic trunks occurs on the right side of the body. Emptying into the junction between the right internal jugular and right subclavian veins are:
the
right jugular trunk from the head and neck;
the
right subclavian trunk from the right upper limb; and
occasionally, the
right bronchomediastinal trunk carrying lymph from the structures in the right half of the thoracic cavity and the right upper intercostal spaces.
There is variability in how these trunks enter the veins. They may combine into a single right lymphatic duct to enter the venous system or enter as three separate trunks.
Lymphatics of the neck
A description of the organization of the lymphatic system in the neck becomes a summary of the lymphatic system in the head and neck. It is impossible to separate the two regions. The components of this system include superficial nodes around the head, superficial cervical nodes along the external jugular vein, and deep cervical nodes forming a chain along the internal jugular vein (Fig. 8.186).
The basic pattern of drainage is for superficial lymphatic vessels to drain to the superficial nodes. Some of these drain to the superficial cervical nodes on their way to the deep cervical nodes and others drain directly to the deep cervical nodes.
Superficial lymph nodes
Five groups of superficial lymph nodes form a ring around the head and are primarily responsible for the lymphatic drainage of the face and scalp. Their pattern of drainage is very similar to the area of distribution of the arteries near their location.
Beginning posteriorly these groups (Fig. 8.186) are:
occipital nodes near the attachment of the trapezius muscle to the skull and associated with the occipital artery—lymphatic drainage is from the posterior scalp and neck;
mastoid nodes (
retroauricular/posterior auricular nodes) posterior to the ear near the attachment of the sternocleidomastoid muscle and associated with the posterior auricular artery—lymphatic drainage is from the posterolateral half of the scalp;
pre-auricular and parotid nodes anterior to the ear and associated with the superficial temporal and transverse facial arteries—lymphatic drainage is from the anterior surface of the auricle, the anterolateral scalp, the upper half of the face, the eyelids, and the cheeks;
submandibular nodes inferior to the body of mandible and associated with the facial artery—lymphatic drainage is from structures along the path of the facial artery as high as the forehead, as well as the gingivae, the teeth, and the tongue;
submental nodes inferior and posterior to the chin—lymphatic drainage is from the center part of the lower lip, the chin, the floor of the mouth, the tip of the tongue, and the lower incisor teeth.
Lymphatic flow from these superficial lymph nodes passes in several directions:
drainage from the occipital and mastoid nodes passes to the superficial cervical nodes along the external jugular vein;
drainage from the pre-auricular and parotid nodes, the submandibular nodes, and the submental nodes passes to the deep cervical nodes.
Superficial cervical lymph nodes
The superficial cervical nodes are a collection of lymph nodes along the external jugular vein on the superficial surface of the sternocleidomastoid muscle (Fig. 8.186). They primarily receive lymphatic drainage from the posterior and posterolateral regions of the scalp through the occipital and mastoid nodes, and send lymphatic vessels in the direction of the deep cervical nodes.
Deep cervical lymph nodes
The deep cervical nodes are a collection of lymph nodes that form a chain along the internal jugular vein (Fig. 8.186). They are divided into upper and lower groups where the intermediate tendon of the omohyoid muscle crosses the common carotid artery and the internal jugular vein.
The most superior node in the upper deep cervical group is the jugulodigastric node (Fig. 8.186). This large node is where the posterior belly of the digastric muscle crosses the internal jugular vein and receives lymphatic drainage from the tonsils and tonsillar region.
Another large node, usually associated with the lower deep cervical group because it is at or just inferior to the intermediate tendon of the omohyoid muscle, is the jugulo-omohyoid node (Fig. 8.186). This node receives lymphatic drainage from the tongue.
The deep cervical nodes eventually receive all lymphatic drainage from the head and neck either directly or through regional groups of nodes.
From the deep cervical nodes, lymphatic vessels form the right and left jugular trunks, which empty into the right lymphatic duct on the right side or the thoracic duct on the left side.
In the clinic
Clinical lymphatic drainage of the head and neck
Enlargement of the neck lymph nodes (cervical lymphadenopathy) is a common manifestation of disease processes that occur in the head and neck. It is also a common manifestation of diffuse diseases of the body, which include lymphoma, sarcoidosis, and certain types of viral infection such as glandular fever and human immunodeficiency virus (HIV) infection.
Evaluation of cervical lymph nodes is extremely important in determining the nature and etiology of the primary disease process that has produced nodal enlargement.
Clinical evaluation includes a general health assessment, particularly relating to symptoms from the head and neck. Examination of the nodes themselves often gives the clinician a clue as to the nature of the pathological process.
Soft, tender, and inflamed lymph nodes suggest an acute inflammatory process, which is most likely to be infective.
Firm multinodular large-volume rubbery nodes often suggest a diagnosis of lymphoma.
Examination should also include careful assessment of other nodal regions, including the supraclavicular fossae, the axillae, the retroperitoneum, and the inguinal regions.
Further examination may include digestive tract endoscopy, chest radiography, and body CT scanning.
Most cervical lymph nodes are easily palpable and suitable for biopsy to establish a tissue diagnosis. Biopsy can be performed using ultrasound for guidance and good samples of lymph nodes may be obtained.
The lymphatic drainage of the neck is somewhat complex, clinically. A relatively simple “level” system of nodal enlargement has been designed that is extremely helpful in evaluating lymph node spread of primary head and neck tumors. Once the number of levels of nodes are determined, and the size of the lymph nodes, the best mode of treatment can be instituted. This may include surgery, radiotherapy, and chemotherapy. The lymph node level also enables a prognosis to be made. The levels are as follows:
Level 1—from the midline of the submental triangle up to the level of the submandibular gland.
Level 2—from the skull base to the level of the hyoid bone anteriorly from the posterior border of the sternocleidomastoid muscle.
Level 3—the inferior aspect of the hyoid bone to the bottom cricoid arch and anterior to the posterior border of the sternocleidomastoid up to the midline.
Level 4—from the inferior aspect of the cricoid to the top of the manubrium of sternum and anterior to the posterior border of the sternocleidomastoid muscle.
Level 5—posterior to sternocleidomastoid muscle and anterior to the trapezius muscle above the level of the clavicle.
Level 6—below the hyoid bone and above the jugular (sternal) notch in the midline.
Level 7—below the level of the jugular (sternal) notch.
PHARYNX
The pharynx is a musculofascial half-cylinder that links the oral and nasal cavities in the head to the larynx and esophagus in the neck (Fig. 8.187). The pharyngeal cavity is a common pathway for air and food.
The pharynx is attached above to the base of the skull and is continuous below, approximately at the level of vertebra CVI, with the top of the esophagus. The walls of the pharynx are attached anteriorly to the margins of the nasal cavities, oral cavity, and larynx. Based on these anterior relationships the pharynx is subdivided into three regions, the nasopharynx, oropharynx, and laryngopharynx:
the posterior apertures (choanae) of the nasal cavities open into the nasopharynx;
the posterior opening of the oral cavity (oropharyngeal isthmus) opens into the oropharynx;
the superior aperture of the larynx (laryngeal inlet) opens into the laryngopharynx.
In addition to these openings, the pharyngeal cavity is related anteriorly to the posterior one-third of the tongue and to the posterior aspect of the larynx. The pharyngotympanic tubes open into the lateral walls of the nasopharynx.
Lingual, pharyngeal, and palatine tonsils are on the deep surface of the pharyngeal walls.
The pharynx is separated from the posteriorly positioned vertebral column by a thin retropharyngeal space containing loose connective tissue.
Although the soft palate is generally considered as part of the roof of the oral cavity, it is also related to the pharynx. The soft palate is attached to the posterior margin of the hard palate and is a type of “flutter valve” that can:
swing up (elevate) to close the pharyngeal isthmus, and seal off the nasopharynx from the oropharynx;
swing down (depress) to close the oropharyngeal isthmus and seal off the oral cavity from the oropharynx.
Skeletal framework
The superior and anterior margins of the pharyngeal wall are attached to bone and cartilage, and to ligaments. The two sides of the pharyngeal wall are welded together posteriorly in the midline by a vertically oriented cord-like ligament (the pharyngeal raphe). This connective tissue structure descends from the pharyngeal tubercle on the base of the skull to the level of cervical vertebra CVI where the raphe blends with connective tissue in the posterior wall of the esophagus.
There is an irregular C-shaped line of pharyngeal wall attachment on the base of the skull (Fig. 8.188). The open part of the C faces the nasal cavities. Each arm of the C begins at the posterior margin of the medial plate of the pterygoid process of the sphenoid bone, just inferior to the cartilaginous part of the pharyngotympanic tube. The line crosses inferior to the pharyngotympanic tube and then passes onto the petrous part of the temporal bone where it is just medial to the roughening for the attachment of one of the muscles (levator veli palatini) of the soft palate. From here, the line swings medially onto the occipital bone and joins the line from the other side at a prominent elevation of bone in the midline (the pharyngeal tubercle).
Anterior vertical line of attachment for the lateral pharyngeal walls
The vertical line of attachment for the lateral pharyngeal walls to structures related to the nasal and oral cavities and larynx is discontinuous and in three parts (Fig. 8.189).
First part
On each side, the anterior line of attachment of the lateral pharyngeal wall begins superiorly on the posterior edge of the medial pterygoid plate of the sphenoid bone just inferior to where the pharyngotympanic tube lies against this plate. It continues inferiorly along the edge of the medial plate of the pterygoid process and onto the pterygoid hamulus. From this point, the line descends along the pterygomandibular raphe to the mandible where this part of the line terminates.
The pterygomandibular raphe is a linear cord-like connective tissue ligament that spans the distance between the tip of the pterygoid hamulus and a triangular roughening immediately posterior to the third molar on the mandible. It joins a muscle of the lateral pharyngeal wall (superior constrictor) with a muscle of the lateral wall of the oral cavity (buccinator).
Second part
The second part of the line of attachment of the lateral pharyngeal wall is related to the hyoid bone. It begins on the lower aspect of the stylohyoid ligament, which connects the tip of the styloid process of the temporal bone to the lesser horn of the hyoid bone. The line continues onto the lesser horn and then turns and runs posteriorly along the entire upper surface of the greater horn of the hyoid where it terminates.
Third part
The most inferior and third part of the line of attachment of the lateral pharyngeal wall begins superiorly on the superior tubercle of the thyroid cartilage, and descends along the oblique line to the inferior tubercle.
From the inferior tubercle, the line of attachment continues over the cricothyroid muscle along a tendinous thickening of fascia to the cricoid cartilage where it terminates.
Pharyngeal wall
The pharyngeal wall is formed by skeletal muscles and by fascia. Gaps between the muscles are reinforced by the fascia and provide routes for structures to pass through the wall.
Muscles
The muscles of the pharynx are organized into two groups based on the orientation of muscle fibers.
The constrictor muscles have fibers oriented in a circular direction relative to the pharyngeal wall, whereas the longitudinal muscles have fibers oriented vertically.
Constrictor muscles
The three constrictor muscles on each side are major contributors to the structure of the pharyngeal wall (Fig. 8.190 and Table 8.17) and their names indicate their position—superior, middle, and inferior constrictor muscles. Posteriorly, the muscles from each side are joined together by the pharyngeal raphe. Anteriorly, these muscles attach to bones and ligaments related to the lateral margins of the nasal and oral cavities and the larynx.
The constrictor muscles overlap each other in a fashion resembling the walls of three flower pots stacked one on the other. The inferior constrictors overlap the lower margins of the middle constrictors and, in the same way, the middle constrictors overlap the superior constrictors.
Collectively, the muscles constrict or narrow the pharyngeal cavity.
When the constrictor muscles contract sequentially from top to bottom, as in swallowing, they move a bolus of food through the pharynx and into the esophagus.
All of the constrictors are innervated by the pharyngeal branch of the vagus nerve [X].
Superior constrictors
The superior constrictor muscles together bracket the upper part of the pharyngeal cavity (Fig. 8.190).
Each muscle is attached anteriorly to the pterygoid hamulus, pterygomandibular raphe, and adjacent bone of the mandible. From these attachments, the muscle fans out posteriorly and joins with its partner muscle from the other side at the pharyngeal raphe.
A special band of muscle (the palatopharyngeal sphincter) originates from the anterolateral surface of the soft palate and circles the inner aspect of the pharyngeal wall, blending with the inner aspect of the superior constrictor.
When the superior constrictor constricts during swallowing, it forms a prominent ridge on the deep aspect of the pharyngeal wall that catches the margin of the elevated soft palate, which then seals closed the pharyngeal isthmus between the nasopharynx and oropharynx.
Middle constrictors
The middle constrictor muscles are attached to the lower aspect of the stylohyoid ligament, the lesser horn of the hyoid bone, and the entire upper surface of the greater horn of the hyoid (Fig. 8.190).
Like the superior constrictors, the middle constrictor muscles fan out posteriorly and attach to the pharyngeal raphe.
The posterior part of the middle constrictors overlaps the superior constrictors.
Inferior constrictors
The inferior constrictor muscles attach anteriorly to the oblique line of the thyroid cartilage, the cricoid cartilage, and a ligament that spans between these two attachments to cartilage and crosses the cricothyroid muscle (Fig. 8.190).
Like the other constrictor muscles, the inferior constrictor muscles spread out posteriorly and attach to the pharyngeal raphe.
The posterior part of the inferior constrictors overlaps the middle constrictors. Inferiorly, the muscle fibers blend with and attach into the wall of the esophagus.
The parts of the inferior constrictors attached to the cricoid cartilage bracket the narrowest part of the pharyngeal cavity.
Longitudinal muscles
The three longitudinal muscles of the pharyngeal wall (Fig. 8.191 and Table 8.18) are named according to their origins—stylopharyngeus from the styloid process of the temporal bone, salpingopharyngeus from the cartilaginous part of the pharyngotympanic tube (salpinx is Greek for “tube”), and palatopharyngeus from the soft palate. From their sites of origin, these muscles descend and attach into the pharyngeal wall.
The longitudinal muscles elevate the pharyngeal wall, or during swallowing, pull the pharyngeal wall up and over a bolus of food being moved through the pharynx and into the esophagus.
Stylopharyngeus
The cylindrical stylopharyngeus muscle (Fig. 8.191A) originates from the base of the medial surface of the styloid process of the temporal bone, descends between the superior and middle constrictor muscles to fan out on, and blend with, the deep surface of the pharyngeal wall. It is innervated by the glossopharyngeal nerve [IX].
Salpingopharyngeus
Salpingopharyngeus (Fig. 8.191B) is a small muscle originating from the inferior aspect of the pharyngotympanic tube, descending on, and blending into the deep surface of the pharyngeal wall. It is innervated by the vagus nerve [X].
Palatopharyngeus
Palatopharyngeus (Fig. 8.191B), in addition to being a muscle of the pharynx, is also a muscle of the soft palate (see p. 1048). It is attached to the upper surface of the palatine aponeurosis, and passes posteriorly and inferiorly to blend with the deep surface of the pharyngeal wall.
Palatopharyngeus forms an important fold in the overlying mucosa (the palatopharyngeal arch). This arch is visible through the oral cavity and is a landmark for finding the palatine tonsil, which is immediately anterior to it on the oropharyngeal wall.
In addition to elevating the pharynx, the palatopharyngeus participates in closing the oropharyngeal isthmus by depressing the palate and moving the palatopharyngeal fold toward the midline.
Palatopharyngeus is innervated by the vagus nerve [X].
Fascia
The pharyngeal fascia is separated into two layers, which sandwich the pharyngeal muscles between them:
a thin layer (
buccopharyngeal fascia) coats the outside of the muscular part of the wall and is a component of the pretracheal layer of cervical fascia (see pg. 950);
a much thicker layer (
pharyngobasilar fascia) lines the inner surface.
The fascia reinforces the pharyngeal wall where muscle is deficient. This is particularly evident above the level of the superior constrictor where the pharyngeal wall is formed almost entirely of fascia (Fig. 8.191). This part of the wall is reinforced externally by muscles of the soft palate (tensor and levator veli palatini).
Gaps in the pharyngeal wall and structures passing through them
Gaps between muscles of the pharyngeal wall provide important routes for muscles and neurovascular tissues (Fig. 8.192).
Above the margin of superior constrictor, the pharyngeal wall is deficient in muscle and completed by pharyngeal fascia.
The tensor and levator veli palatini muscles of the soft palate initially descend from the base of the skull and are lateral to the pharyngeal fascia. In this position, they reinforce the pharyngeal wall:
levator veli palatini passes through the pharyngeal fascia inferior to the pharyngotympanic tube and enters the soft palate;
the tendon of tensor veli palatini turns medially around the pterygoid hamulus and passes through the origin of the buccinator muscle to enter the soft palate.
One of the largest and most important apertures in the pharyngeal wall is between the superior and middle constrictor muscles of the pharynx and the posterior border of the mylohyoid muscle, which forms the floor of the mouth (Fig. 8.192). This triangular-shaped gap not only enables stylopharyngeus to slip into the pharyngeal wall, but also allows muscles, nerves, and vessels to pass between regions lateral to the pharyngeal wall and the oral cavity, particularly to the tongue.
The gap between the middle and inferior constrictor muscles allows the internal laryngeal vessels and nerve access to the aperture in the thyrohyoid membrane to enter the larynx.
The recurrent laryngeal nerves and accompanying inferior laryngeal vessels enter the larynx posterior to the inferior horn of the thyroid cartilage deep to the inferior margin of the inferior constrictor muscle.
Nasopharynx
The nasopharynx is behind the posterior apertures (choanae) of the nasal cavities and above the level of the soft palate (Fig. 8.193). Its ceiling is formed by the sloping base of the skull and consists of the posterior part of the body of the sphenoid bone and the basal part of the occipital bone. The ceiling and lateral walls of the nasopharynx form a domed vault at the top of the pharyngeal cavity that is always open.
The cavity of the nasopharynx is continuous below with the cavity of the oropharynx at the pharyngeal isthmus. The position of the pharyngeal isthmus is marked on the pharyngeal wall by a mucosal fold caused by the underlying palatopharyngeal sphincter, which is part of the superior constrictor muscle.
Elevation of the soft palate and constriction of the palatopharyngeal sphincter closes the pharyngeal isthmus during swallowing and separates the nasopharynx from the oropharynx.
There is a large collection of lymphoid tissue (the pharyngeal tonsil) in the mucosa covering the roof of the nasopharynx. Enlargement of this tonsil, known then as adenoids, can occlude the nasopharynx so that breathing is only possible through the oral cavity.
The most prominent features on each lateral wall of the nasopharynx are:
the pharyngeal opening of the pharyngotympanic tube; and
mucosal elevations and folds covering the end of the pharyngotympanic tube and the adjacent muscles.
The opening of the pharyngotympanic tube is posterior to and slightly above the level of the hard palate, and lateral to the top of the soft palate.
Because the pharyngotympanic tube projects into the nasopharynx from a posterolateral direction, its posterior rim forms an elevation or bulge on the pharyngeal wall. Posterior to this tubal elevation (torus tubarius) is a deep recess (pharyngeal recess).
Mucosal folds related to the pharyngotympanic tube include:
the small vertical
salpingopharyngeal fold, which descends from the tubal elevation and overlies salpingopharyngeus muscle; and
a broad fold or elevation (
torus levatorius) that appears to emerge from just under the opening of the pharyngotympanic tube, continues medially onto the upper surface of the soft palate, and overlies the levator veli palatini muscle.
Oropharynx
The oropharynx is posterior to the oral cavity, inferior to the level of the soft palate, and superior to the upper margin of the epiglottis (Fig. 8.193). The palatoglossal folds (arches), one on each side, that cover the palatoglossal muscles, mark the boundary between the oral cavity and the oropharynx. The arched opening between the two folds is the oropharyngeal isthmus. Just posterior and medial to these folds are another pair of folds (arches), the palatopharyngeal folds, one on each side, that overlie the palatopharyngeus muscles.
The anterior wall of the oropharynx inferior to the oropharyngeal isthmus is formed by the upper part of the posterior one-third or pharyngeal part of the tongue. Large collections of lymphoid tissue (the lingual tonsil) are in the mucosa covering this part of the tongue.
The palatine tonsils are on the lateral walls of the oropharynx. On each side, there is a large ovoid collection of lymphoid tissue in the mucosa lining the superior constrictor muscle and between the palatoglossal and palatopharyngeal arches. The palatine tonsils are visible through the oral cavity just posterior to the palatoglossal folds.
When holding liquid or solids in the oral cavity, the oropharyngeal isthmus is closed by depression of the soft palate, elevation of the back of the tongue, and movement toward the midline of the palatoglossal and palatopharyngeal folds. This allows a person to breathe while chewing or manipulating material in the oral cavity.
On swallowing, the oropharyngeal isthmus is opened, the palate is elevated, the laryngeal cavity is closed, and the food or liquid is directed into the esophagus. A person cannot breathe and swallow at the same time because the airway is closed at two sites, the pharyngeal isthmus and the larynx.
Laryngopharynx
The laryngopharynx extends from the superior margin of the epiglottis to the top of the esophagus at the level of vertebra CVI (Fig. 8.193).
The laryngeal inlet opens into the anterior wall of the laryngopharynx. Inferior to the laryngeal inlet, the anterior wall consists of the posterior aspect of the larynx.
The cavity of the laryngopharynx is related anteriorly to a pair of mucosal pouches (valleculae), one on each side of the midline, between the base of the tongue and epiglottis. The valleculae are depressions formed between a midline mucosal fold and two lateral folds that connect the tongue to the epiglottis.
There is another pair of mucosal recesses (piriform fossae) between the central part of the larynx and the more lateral lamina of the thyroid cartilage. The piriform fossae form channels that direct solids and liquids from the oral cavity around the raised laryngeal inlet and into the esophagus.
Tonsils
Collections of lymphoid tissue in the mucosa of the pharynx surrounding the openings of the nasal and oral cavities are part of the body’s defense system. The largest of these collections form distinct masses (tonsils). Tonsils occur mainly in three areas (Fig. 8.193):
the pharyngeal tonsil, known as adenoids when enlarged, is in the midline on the roof of the nasopharynx;
the palatine tonsils are on each side of the oropharynx between the palatoglossal and palatopharyngeal arches just posterior to the oropharyngeal isthmus; (The palatine tonsils are visible through the open mouth of a patient when the tongue is depressed.)
the lingual tonsil refers collectively to numerous lymphoid nodules on the posterior one-third of the tongue.
Small lymphoid nodules also occur in the pharyngotympanic tube near its opening into the nasopharynx, and on the upper surface of the soft palate.
Vessels
Arteries
Numerous vessels supply the pharyngeal wall (Fig. 8.194).
Arteries that supply upper parts of the pharynx include:
the ascending pharyngeal artery;
the ascending palatine and tonsillar branches of the facial artery; and
numerous branches of the maxillary and the lingual arteries.
All these vessels are from the external carotid artery.
Arteries that supply the lower parts of the pharynx include pharyngeal branches from the inferior thyroid artery, which originates from the thyrocervical trunk of the subclavian artery.
The major blood supply to the palatine tonsil is from the tonsillar branch of the facial artery, which penetrates the superior constrictor muscle.
Veins
Veins of the pharynx form a plexus, which drains superiorly into the pterygoid plexus in the infratemporal fossa, and inferiorly into the facial and internal jugular veins (Fig. 8.195).
Lymphatics
Lymphatic vessels from the pharynx drain into the deep cervical nodes and include retropharyngeal (between nasopharynx and vertebral column), paratracheal, and infrahyoid nodes (Fig. 8.195).
The palatine tonsils drain through the pharyngeal wall into the jugulodigastric nodes in the region where the facial vein drains into the internal jugular vein (and inferior to the posterior belly of the digastric muscle).
Nerves
Motor and most sensory innervation (except for the nasal region) of the pharynx is mainly through branches of the vagus [X] and glossopharyngeal [IX] nerves, which form a plexus in the outer fascia of the pharyngeal wall (Fig. 8.196).
The pharyngeal plexus is formed by:
the pharyngeal branch of the vagus nerve [X];
branches from the
external laryngeal nerve from the
superior laryngeal branch of the vagus nerve [X]; and
pharyngeal branches of the glossopharyngeal nerve [IX].
The pharyngeal branch of the vagus nerve [X] originates from the upper part of its inferior ganglion above the origin of the superior laryngeal nerve and is the major motor nerve of the pharynx.
All muscles of the pharynx are innervated by the vagus nerve [X] mainly through the pharyngeal plexus, except for the stylopharyngeus, which is innervated directly by a branch of the glossopharyngeal nerve [IX].
Each subdivision of the pharynx has a different sensory innervation:
the nasopharynx is innervated by a pharyngeal branch of the maxillary nerve [V
2] that originates in the pteryatine fossa and passes through the palatovaginal canal in the sphenoid bone to reach the roof of the pharynx;
the oropharynx is innervated by the glossopharyngeal nerve [IX] via the pharyngeal plexus;
the laryngopharynx is innervated by the vagus nerve [X] via the internal branch of the superior laryngeal artery.
Glossopharyngeal nerve [IX]
The glossopharyngeal nerve [IX] is related to the pharynx throughout most of its course outside the cranial cavity.
After exiting the skull through the jugular foramen, the glossopharyngeal nerve [IX] descends on the posterior surface of the stylopharyngeus muscle, passes onto the lateral surface of the stylopharyngeus, and then passes anteriorly through the gap between the superior and middle constrictors to eventually reach the posterior aspect of the tongue.
As the glossopharyngeal nerve [IX] passes under the free edge of superior constrictor, it is just inferior to the palatine tonsil lying on the deep surface of the superior constrictor.
Pharyngeal branches to the pharyngeal plexus and a motor branch to the stylopharyngeus muscle are among branches that originate from the glossopharyngeal nerve [IX] in the neck.
Because sensory innervation of the oropharynx is by the glossopharyngeal nerve [IX], this nerve carries sensory innervation from the palatine tonsil and is also the afferent limb of the gag reflex.