The Child with a Communicable Disease
1 Define each key term listed.
2 Interpret the detection and prevention of common childhood communicable diseases.
3 Discuss the characteristics of common childhood communicable diseases.
4 Discuss three principles involved in standard and transmission-based precautions used to prevent the transmission of communicable diseases in children.
5 Discuss national and international immunization programs.
6 Describe the nurse’s role in the immunization of children.
7 Demonstrate a teaching plan for preventing sexually transmitted infections (STIs) in an adolescent.
8 Formulate a nursing care plan for a child with acquired immunodeficiency syndrome (AIDS).
 , p. 731)
, p. 731) , p. 731)
, p. 731) , p. 731)
, p. 731) , p. 734)
, p. 734) , p. 731)
, p. 731) , p. 734)
, p. 734) , p. 732)
, p. 732) , p. 731)
, p. 731) , p. 734)
, p. 734) , p. 731)
, p. 731) , p. 734)
, p. 734) , p. 731)
, p. 731) , p. 734)
, p. 734) , p. 731)
, p. 731) , p. 734)
, p. 734) http://evolve.elsevier.com/Leifer
http://evolve.elsevier.com/Leifer
There have been only a few brief periods in history when infectious disease did not dominate the attention of health care professionals. Despite immunization, sanitation, antimicrobial drugs, and other controls, the world continues to face infectious agents such as human immunodeficiency virus (HIV), hepatitis, tuberculosis, and sexually transmitted infections (STIs). Despite our knowledge of immunizations, some children still suffer from common communicable diseases. Antimicrobial drug-resistant organisms are increasing in number and virulence, and immunocompromised patients are threatened by nonpathogenic organisms. Prevention and control are key factors in managing infectious disease.
 Health Promotion
Health Promotion
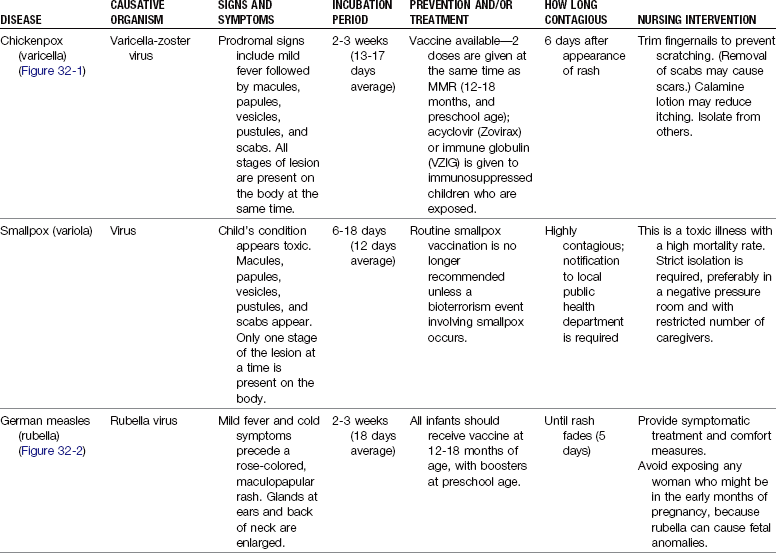
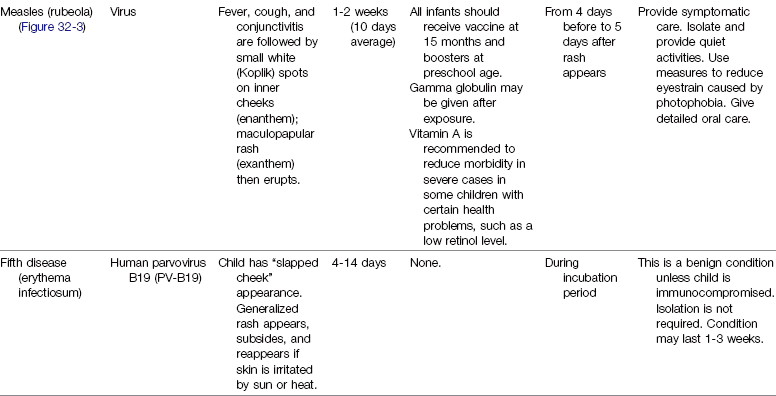
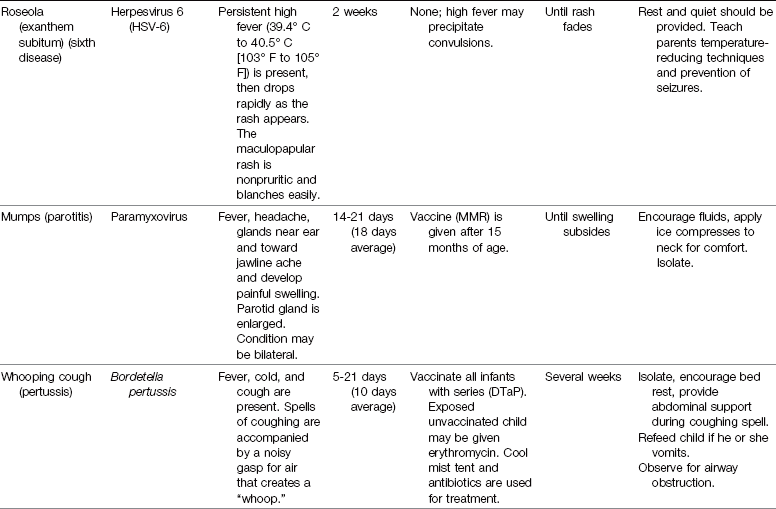
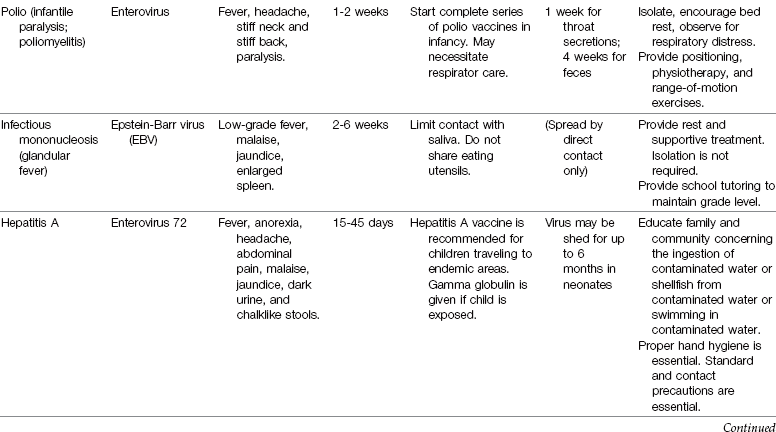
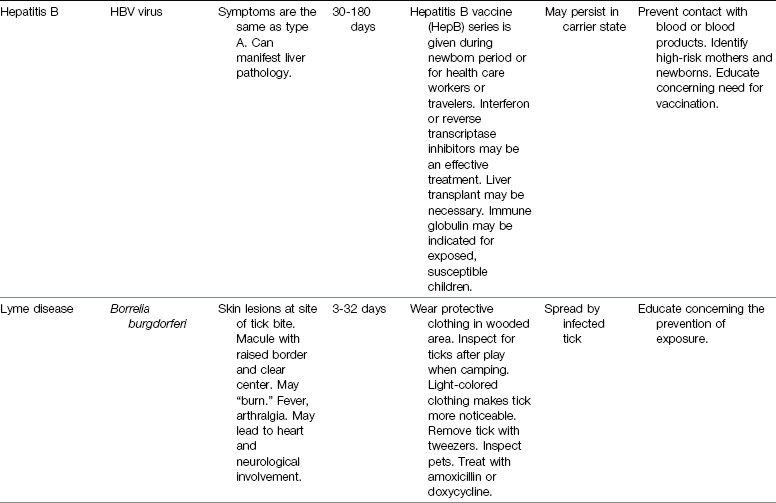
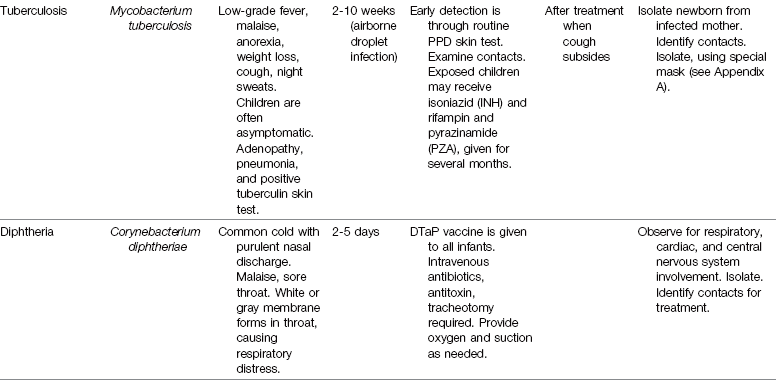
Communicable Diseases of Childhood

DTaP, Diphtheria-tetanus–acellular pertussis vaccine; MMR, measles-mumps-rubella vaccine; PPD, purified protein derivative; VZIG, varicella-zoster immune globulin.
Note: DTaP is given to infants and children up to age 10; Tdap (tetanus-diphtheria–acellular pertussis vaccine) is given to children age 11 and older.



Common Childhood Communicable Diseases
The incidence of common childhood communicable diseases has dramatically decreased as immunological agents have been developed. Diseases such as smallpox have declined to a point worldwide that routine immunizations are no longer recommended. (A brief review of smallpox is presented in this chapter because the nurse must be able to identify a smallpox lesion and promptly isolate the patient and arrange for immediate follow-up care to prevent an outbreak of this deadly illness.) Providing all children with the appropriate immunizations is the health care challenge of today. Air travel is commonplace, and rapid transmission of contagious diseases from around the world makes alert assessment by the nurse and all health care workers essential.
Review of Terms
A communicable disease is one that can be transmitted, directly or indirectly, from one person to another. Organisms that cause disease are called pathogens.
The incubation period is the time between the invasion by the pathogen and the onset of clinical symptoms. The prodromal period refers to the initial stage of a disease: the interval between the earliest symptoms and the appearance of a typical rash or fever. Children are often contagious during this time, but because the symptoms are not specific they may attend preschool or another group program and spread the disease. A fomite is any inanimate material that absorbs and transmits infection. A vector is an insect or animal that carries and spreads a disease. A pandemic is a worldwide high incidence of a communicable disease. An epidemic is a sudden increase of a communicable disease in a localized area. Endemic refers to a continuous incidence of a communicable disease expected in a localized area.
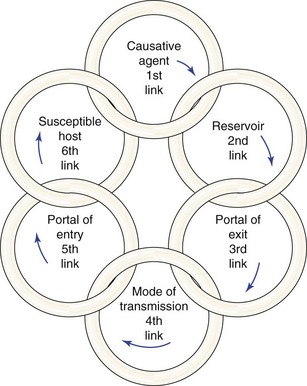
Body substance refers to moist secretions or parts of the body that can contain microorganisms. Emesis, saliva, sputum, semen, urine, feces, and blood are examples of body substances. Body substance precautions indicate the need to wear disposable protective gloves and/or garments when coming in contact with these body substances. A portal of entry is a route by which the organisms enter the body (e.g., a cut in the skin). A portal of exit is the route by which the organisms exit the body (e.g., feces or urine). A reservoir for infection is a place that supports the growth of organisms (e.g., standing, stagnant water). The chain of infection refers to the way in which organisms spread and infect the individual (Figure 32-4). Standard precautions are found in Appendix A. Careful hand hygiene is basic and essential to prevent the spread of infection.
Host Resistance
Many factors contribute to the virulence of an infectious disease. The age, sex, and genetic makeup of the child have a bearing on the degree of resistance. The nutritional status of the person, as well as physical and emotional health, is also important. The efficiency of the blood-forming organs and of the immune systems affects resistance. Important factors in host resistance to disease include the following:
• Intact skin and mucous membranes: A break in the skin can be a portal of entry for an organism that can cause illness.
• Phagocytes in the blood attack and destroy organisms.
• The functioning immune system in the body responds to fight infection. Some factors in this immune response include interferon, T cells, B cells, and antibodies. Vaccinations assist the body to manufacture antibodies that can help the child to resist infections.
The child who has an underlying condition such as diabetes, cystic fibrosis, burns, or sickle cell disease may be more susceptible to certain organisms. Children with HIV or acquired immunodeficiency syndrome (AIDS) or cancer and children receiving steroid or immunosuppressive drugs often have depressed immune systems. This makes them very susceptible to opportunistic infections (an opportunistic infection is caused by organisms normally found in the environment that the immune-suppressed individual cannot resist or fight). An infection acquired in a health care facility during hospitalization is termed a health care–associated infection.
Types of Immunity
Immunity is natural or acquired resistance to infection. In natural immunity, resistance is inborn. Some races apparently have a greater natural immunity to certain diseases than others. Immunity also varies from person to person. If two persons are exposed to the same disease, one may become very ill and the other may show no evidence of the disease.
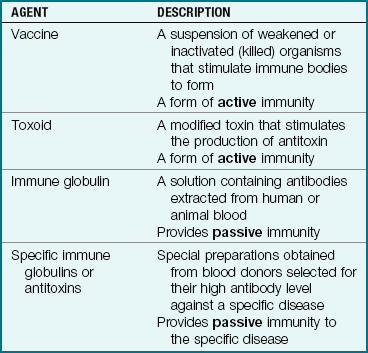
Acquired immunity is not the result of inherited factors but is gained as a result of having the disease or is artificially acquired by receiving vaccines or immune serums. Vaccines contain live attenuated (weakened) or dead organisms that are not strong enough to cause the disease but stimulate the body to develop an immune reaction and antibodies. When the person produces his or her own immunity, it is called active immunity.
If a person is exposed and needs immediate protection from a specific infectious disease, antibodies can be obtained in immune serums; most are from animals, but some are from humans. For example, tetanus serum (used to prevent lockjaw) is procured from the horse, but gamma globulin, which is rich in antibodies, is obtained from human blood. This type of immunity, known as passive immunity, acts immediately but does not last as long as immunity actively produced by the body. Passive immunity provides the antibody. It does not stimulate the system to produce its own antibodies.
A carrier is a person who is capable of spreading a disease but does not show evidence of it. Typhoid fever is an example of a disease spread by a carrier.
Transmission of Infection
Infection can be transmitted from one person to another by direct or indirect means. Direct transmission involves contact with the person who is infected (the body fluids of that person, such as nasal discharge or an open lesion). Indirect transmission involves contact with objects that have been contaminated by the infected person. These objects are called fomites. Bedrails, intravenous (IV) pumps, overbed tables, door handles, used tissues, countertops, and toys are examples of fomites. For example, the respiratory syncytial virus (RSV) lives on dry soap for several hours. Therefore picking up soap used by a person infected with RSV transmits the organism. This is one of the reasons why use of liquid soap is advocated. The chain of infection transmission is shown in Figure 32-4. Preventing the spread of infection depends on breaking the chain.
Various tests are available to determine whether an individual has been exposed to a particular disease, such as the Mantoux intradermal purified protein derivative (PPD) skin test or a blood serum test called the QuantiFERON-TB Gold test, for tuberculosis. The Schick test for diphtheria and the Dick test for scarlet fever have been replaced by serum DNA-PCR (DNA polymerase chain reaction) testing.
Medical Asepsis, Standard Precautions, and Transmission-Based Precautions
The purpose of medical aseptic techniques used with all patients is to prevent the spread of infection from one person to another. A person or object is considered contaminated if he, she, or it has touched the infected patient or any equipment or fomite that has come in contact with the patient or his or her bodily fluids.
Articles that have come in direct contact with the patient must be disinfected before they can be used by others. When something is disinfected, the microorganisms in or on it are killed by physical or chemical means. The autoclave, which uses steam under pressure, is considered effective in killing most microbes when the article is adequately exposed and sterilized for the proper length of time.
All children suspected of having a communicable disease who are admitted to the hospital are placed on both standard and transmission-based precautions until a definite diagnosis is established. A private room or negative-pressure room (prevents air from flowing out of the room when the door is opened) may be assigned. (See Appendix A for specific transmission-based precautions and the practices required.)
Disposable items are used when a child is placed on transmission-based precautions; these include tissues, suction catheters, thermometers, suture sets, nursing bottles, and blood pressure cuffs. They are disposed of according to hospital protocol.
The nurse must understand the importance of protecting himself or herself and others from a contagious patient. This is accomplished by specific precautions, called standard precautions. The Centers for Disease Control and Prevention (CDC) recommend standard precautions be used on all patients; these involve, at minimum, hand hygiene and the use of disposable gloves. In addition to these precautions, transmission-based precautions are designed according to the method of spread of infection, such as airborne infection isolation (AII), contact, and droplet (see Appendix A).
Airborne infection isolation precautions are used for patients with conditions such as tuberculosis, varicella (chickenpox), and rubeola (measles). Small airborne particles floating in the air can be inhaled any place in the room. The use of negative-pressure rooms and respirator masks (e.g., N95 particulate masks) are required upon entering the room. The respirator masks are removed upon exiting the room.
Contact precautions are used when the condition causes organisms to be transmitted via skin-to-skin contact or through indirect touch of a contaminated fomite. Gloves and a cover gown are worn for close contact with patients with RSV, patients with hepatitis A who are incontinent, patients with contagious skin diseases such as impetigo, and patients with wound infections. It is important to note that some diseases may have more than one mode of spread and therefore necessitate more than one precaution technique.
Droplet precautions are used with diseases such as pertussis and influenza. When the patient coughs or sneezes, the droplets can contaminate an area 3 feet around the patient. Beyond the 3-foot radius, a mask and gown are not usually necessary.
Standard precautions are discussed in Appendix A along with the protocols for the use of masks, gowns, gloves, and other protective equipment. Personal protective equipment (PPE) should be worn when anticipating the risk of exposure to blood, body fluids, or other potentially infectious materials.
 Safety Alert!
Safety Alert!
Disposable gloves should be worn whenever touching something that is moist and not yours.
Protective Environment Isolation
Protective environment isolation precautions (previously called reverse isolation) are used for patients who are not communicable but have a lowered resistance and are highly susceptible to infection. This simple procedure reduces the incidence of health care–associated infections. The patient is placed in a private room with the door closed. It is recommended that all persons wear a gown, a mask, and gloves when attending the child. Both the child and family need adequate explanations concerning the protective environment precautions.
Hand Hygiene
The nurse must perform hand hygiene on his or her hands between patients and after removing gloves. Hospital-approved antibacterial soaps and lotions are used. The use of hot water, instead of warm water, can irritate skin and may promote the development of resistant strains of microorganisms. Self-contained liquid soap dispensers are preferable to bar soap, which can harbor organisms. Alcohol-based hand sanitizers can be used as long as the hands are not visibly soiled. Artificial fingernails, including tips, wraps, and nail jewelry are not permitted in patient care areas. Refer to hospital infection prevention and control policies. Caregivers with skin lesions on exposed areas of their bodies should not provide direct patient care until the lesions are completely cleared.
Safety Alert!
Alcohol-based hand sanitizers should not be used when caring for a patient diagnosed with Clostridium difficile diarrhea, because this organism is spore forming and resistant to alcohols. Soap and water must be used after every contact.
 Nursing Tip
Nursing Tip
Teaching children and their families to wash their hands before meals and after using the toilet, blowing their noses, sneezing, or handling soiled objects is important to minimize the spread of infection and promote healthy living. Making hand hygiene fun for children can motivate them to wash appropriately for a minimum of 15 seconds.
Family Education
Education of family members must be ongoing. Factors to be emphasized include the necessity for immunization of children, proper storage of food (particularly perishables), use of pasteurized milk, proper cooking of meats, cleanliness in food preparation, and proper hand hygiene. The nurse must review the ways in which infectious diseases are spread. Children must be taught to avoid using community hand towels. Other modes of transmission, such as crowded living conditions, insects, rodents, and sandboxes, may also be discussed.
Rashes
Many infectious diseases begin with a rash. Rashes tend to be itchy (pruritic) and uncomfortable. Symptomatic care is provided by prescribing acetaminophen (Tylenol) and diphenhydramine (Benadryl) or topical lotions. Rashes can be described as follows (see Box 30-1):
• Erythema: Diffused reddened area on the skin
• Macule: Circular reddened area on the skin
• Papule: Circular reddened area on the skin that is elevated
• Vesicle: Circular reddened area on the skin that is elevated and contains fluid
• Pustule: Circular reddened area on the skin that is elevated and contains pus
• Scab: Dried pustule that is covered with a crust
• Pathognomonic: Term used to describe a lesion or symptom that is characteristic of a specific illness (e.g., Koplik spots are pathognomonic for measles)
Safety Alert!
Apply lotions to open lesions sparingly to prevent absorption that could lead to drug toxicity.
Worldwide travel makes it a priority for the nurse to be able to communicate with patients in different languages concerning signs and symptoms that may indicate the presence of a communicable disease. Appendix F is an example of a multilingual list of common symptoms related to communicable diseases that can be used by health care personnel.
Worldwide Immunization Programs
In Healthy People 2020, the United States Public Health Service made immunizing 95% of all children in the United States against childhood communicable diseases a goal to achieve by the year 2020. In 2009, only 75% of children covered by health maintenance organizations (HMOs) in the United States were up to date in their immunizations by 2 years of age, and 1% to 3% of children across the United States were excused from immunization for religious or philosophical reasons (Sharts-Hopko, 2009). Some reasons for the current low vaccination rate include a knowledge deficit in parents, a lack of accessibility to vaccination clinics, the cost of vaccinating children, a fear of adverse reactions, misunderstandings about contraindications, failure to track or follow up on immunization records, and failure to understand the current immunization guidelines.
Federally funded programs to provide vaccines and to educate are already in place. The effort of the World Health Organization (WHO) and the United Nations Children’s Fund (UNICEF) has resulted in dramatic declines in vaccine-preventable illnesses worldwide, especially in developing countries. New vaccines are developed and assessed for routine use in endemic areas.
Table 32-1 presents types of immunization agents. The influenza vaccine, the pneumococcal vaccine, the varicella vaccine, and RSV immune globulin (RespiGam) are available for children. Vaccines for cholera and yellow fever are available for families traveling to endemic areas. The CDC provides advice concerning vaccinations needed for persons traveling to various parts of the world.
The Nurse’s Role
Worldwide immunization practices have eliminated smallpox as a threat. However, nurses must remain alert to signs and symptoms of communicable diseases, including smallpox. The threat of bioterrorism increases the risk of these and other diseases reemerging. Measles is rarely seen in developed countries. Current vaccinations against varicella, hepatitis, influenza (for children 6 months of age and older or high-risk children), and pneumonia (for children over 2 years of age) are available, and the challenge is to make them accessible. The nurse is a vital link in educating parents about the need for immunizations. The U.S. Public Health Service has forms listing the benefits and risks of immunizations that are available to aid in parent education. Parental consent is required before a child is vaccinated, and appropriate vaccine information statements (VISs) should be provided and reviewed with the parents before administration of the vaccine.
Vaccines
In newborn infants, the presence of passively acquired immunity from the mother may inhibit the infant’s natural immune response to vaccines. Therefore, routine immunizations are not started until 2 months of age, unless a high risk of infection exists. Because hepatitis B is a continuing problem in the United States, the immunization series for hepatitis B is often started before the newborn is discharged to the home.
Most antibodies cannot reach intracellular sites of infection but can prevent spread from the site of entry into the body to a target organ. For that reason, vaccinations prevent the disease, but most cannot be used to treat the disease once cellular penetration of the organism has occurred. For some diseases postexposure immunization is recommended; immune globulins are most often the choice.
Multiple doses of a vaccine at predetermined intervals may be needed to achieve an immunity status. The nurse can educate parents and school personnel about immunization schedules and should assess the immunization status of each child at every clinic visit (Figure 32-5).

FIGURE 32-5 The “hug” restraining position for administration of vaccinations. Note that the arms are restrained by the mother and that the child’s legs are restrained between the mother’s knees. The mother comforts the child during the procedure and may breastfeed after the procedure. The site for intramuscular injections in infants is the thigh, and the nurse wears a protective glove. The use of aerosol sprays or EMLA cream may reduce the pain of multiple injections in infants and children.
Routes of Administration
The correct route of administration is important to achieve immunization. The oral, subcutaneous, and intramuscular routes are used for various vaccines. The route of administration of a vaccine influences the response of the infant. The recommended route must be used to obtain optimum response. For example, the administration of hepatitis B vaccine into the buttock will not result in the same optimal level of immunity as administration of the vaccine into the deltoid muscle (Mandell et al., 2005).
Storage and Handling
Correct storage of vaccines is essential to ensure their potency. The nurse should check the label to determine what type of refrigeration is needed. Proper storage and handling of vaccines ensures that potency is maintained. Improper temperatures can reduce the potency of the vaccine, and there are often no visible signs of these changes. Vaccines should not be stored in the doors of refrigerators or freezers, near the cold air vents in the refrigerator, or in storage bins; and they must be placed in the center of shelves to allow free flow of air around the vaccines. Most vaccines are stored inside the refrigerator at 1.6° C to 7.7° C (35° F to 46° F). Varicella vaccine (Varivax) and live attenuated influenza virus (LAIV) are very fragile. The varicella and LAIV must be stored in the freezer at −15° C (5° F) or lower and used within 30 minutes of reconstitution. The vaccines cannot be refrozen after they have been thawed. Inactivated vaccines can be harmed if frozen, and live vaccines are harmed by heat and light. This information is especially important to know when participating in outdoor mass immunization programs. In clinic or office settings, the refrigerator temperatures must be documented at the beginning and the end of each work day, and the records must be kept on file for at least 3 years. Refrigerator-freezers with automatic defrost cycles are not appropriate for vaccine storage because temperatures may not be held stable as required (Mandell et al., 2005).
Emergency Preparedness
Most parts of the United States are threatened at times by sudden and unexpected power outages caused by storms, earthquakes, and other events. To minimize the potential for vaccine loss, preventive steps should be taken in preparation for such an emergency. These steps include keeping several bottles of water and cold packs in the freezer to help maintain the temperature of the vaccines if power is disrupted.
Allergies and Adverse Responses
Allergies: Children who have a history of allergy to neomycin should notify the health care provider before receiving the inactivated poliovirus vaccine (IPV), the measles-mumps-rubella vaccine (MMR), the varicella vaccine and some influenza vaccines (Fluvirin). An allergy to eggs should also be reported before receiving MMR, varicella, or influenza vaccines. Epinephrine should be available in the unit where vaccines are administered, and the child should be observed for a minimum of 20 minutes before he or she leaves the area.
A serious allergy to baker’s yeast should be reported to the health care provider before recombinant hepatitis B immunization is administered (Mandell et al., 2005). The influenza vaccine should be given with caution to persons who are allergic to eggs. Varicella vaccine, if not given on the same day as MMR, must be given no less than 28 days later. A tuberculin test should not be given within 6 weeks of receiving an MMR or varicella immunization, because the results will not be accurate.
Mercury Toxicity: Thimerosal is a mercury-containing preservative used in some vaccines, and there is some concern over the rise of mercury toxicity in children. The American Academy of Pediatrics (AAP) recommends that Comvax, a thimerosal-free hepatitis B vaccine, be used within 12 hours after birth for all high-risk newborn infants born in the United States (Mandell et al., 2005). The pneumococcal vaccine (Prevnar) does not contain thimerosal and is effective in preventing common childhood pneumonia and otitis media. The U.S. Food and Drug Administration (FDA) is urging the elimination of mercury in vaccines and medical equipment, such as thermometers and blood-pressure machines. Parents should be counseled about reducing exposures to other sources of mercury.
Adverse Reactions: On some occasions vaccines may elicit a hypersensitivity response or may block the body’s immune defenses. Rotavirus is a live, attenuated oral vaccine recommended by the AAP to be given in a three-dose schedule (RV-5) or a two-dose schedule (RV-1) depending on the type of vaccine used. The vaccine is not recommended for immunocompromised children or children with latex allergy because the RV-1 applicator contains latex. The vaccine is given between 2 and 6 months of age with at least a 1-month interval between doses. All doses should be administered by 8 months of age (AAP, 2009a). If vomiting occurs after an oral dose, the dose should not be repeated.
The hepatitis A vaccine is not licensed to be used before 2 years of age (Mandell et al., 2005). Serious adverse events occurring within a designated time after vaccination should be reported to the national Vaccine Adverse Events Reporting System (VAERS) (www.vaers.hhs.gov) or by calling 800-822-7967. The National Childhood Vaccine Injury Act of 1986 contains a provision for compensation in some cases of specific vaccine injuries. All patients should be directly observed for 15 to 20 minutes after receiving an immunization (Bruhn & Tillett, 2009), and appropriate equipment for the treatment of anaphylaxis should be immediately available.
Refusal of Vaccination
When a parent refuses immunizations for a child the nurse should listen carefully for the reason and offer appropriate education. Some vaccines contain heavy metals, antibiotics, and animal products (Grabenstein, 2009). Animal products contained in a vaccine may present a problem for parents with specific cultural beliefs. The nurse should be culturally sensitive and offer education concerning the values of the vaccine as well as options. Detailed information concerning contents of vaccines can be obtained online (see Online Resources at the end of the chapter).
Nursing Responsibilities in Vaccine Administration
The nurse must be aware of when the vaccines are due to be administered, the immunization history of the child, which vaccines can be given together, contraindications, the route of administration, and the proper equipment needed. Epinephrine should be on hand for emergencies, and the child should remain in the clinic under observation for at least 20 minutes.
Reducing pain at the site of injection, especially when multiple injections are required, should be considered. The use of vapocoolant sprays or EMLA cream is effective. Using the proper technique of injection of vaccines is important. The Haemophilus influenzae type b (Hib) vaccine must be given in a separate syringe from other vaccines given at the same clinic visit. The varicella vaccine is given subcutaneously, whereas the diphtheria-tetanus–acellular pertussis (DTaP) vaccine causes significant tissue irritation if given subcutaneously, and careful intramuscular (IM) technique is essential. Combination vaccines have been developed that reduce the number of injections required at each clinic visit.
The recommended immunization program in the United States is approved by the CDC and the AAP (Box 32-1). Advances in the field of immunology may change recommendations for existing policies and cause new policies to be developed (see the sites listed in Online Resources for updates). Alternative methods of vaccine delivery are being developed, including use of the intranasal route and transdermal techniques (Sharts-Hopko, 2009).
Before a vaccine is given to a child, the nurse should provide a vaccine information statement (VIS) to the parent, discuss the vaccine, and obtain consent. VISs are printed in several different languages and can easily be obtained online (see Online Resources).
Immunization Schedule for Children: Informed consent concerning the potential risks and the documentation of immunization are essential. Parents should have copies of their child’s immunization records. The immunization program for children in the United States is described in Figure 32-6.
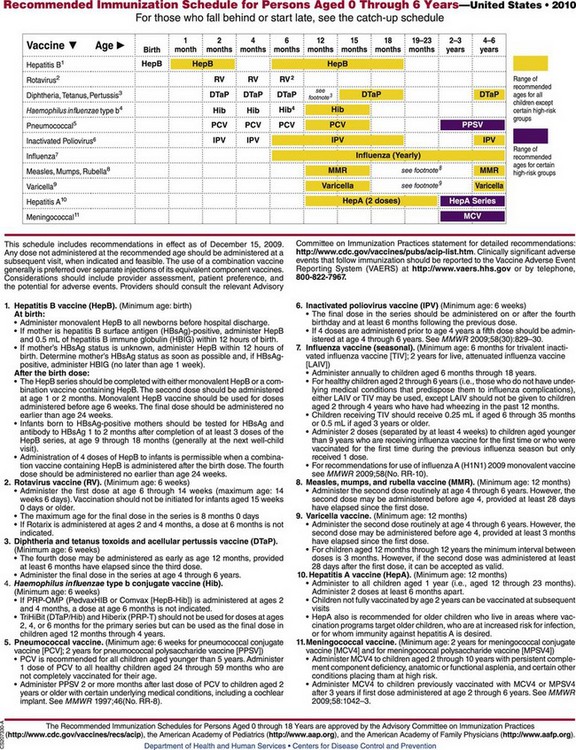
FIGURE 32-6 Immunization schedule for infants and children in the United States. Hib is given intramuscularly. MMR and IPV are given subcutaneously. DTaP/Tdap, Diphtheria toxoids, pertussis, and tetanus and tetanus-diphtheria–acellular pertussis vaccine; HepB, hepatitis B vaccine; Hep, hepatitis; Hib, Haemophilus influenzae type b vaccine; IPV, inactivated poliovirus vaccine; MMR, measles-mumps-rubella vaccine.
Contraindications to live virus vaccine administration may include the following:
• Immunocompromised state (necessitates individual evaluation by the health care provider)
• Immunocompromised caregiver in the home (necessitates individual evaluation by the health care provider)
• Corticosteroid therapy (necessitates individual evaluation)
• History of high fever (40.5° C [105° F]) after previous vaccinations
A subcutaneous injection should be administered with a  inch, 23- to 25-gauge needle; an IM injection should be administered with a 1- to
inch, 23- to 25-gauge needle; an IM injection should be administered with a 1- to  , 22- to 25-gauge needle; and an intradermal injection should be administered with a
, 22- to 25-gauge needle; and an intradermal injection should be administered with a  to
to  inch, 25- to 27-gauge needle with the bevel up and parallel to the volar surface of the forearm.
inch, 25- to 27-gauge needle with the bevel up and parallel to the volar surface of the forearm.
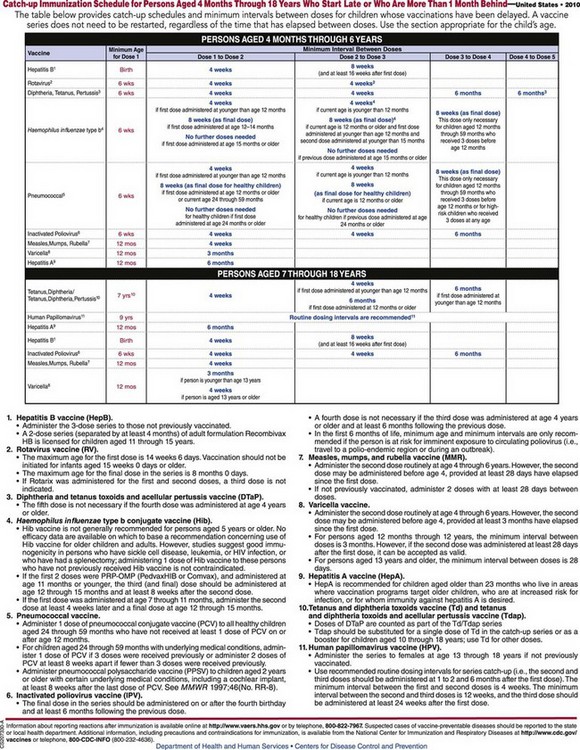
Children from 4 months to 18 years of age who start the immunization process late or are more than 1 month behind should adhere to the catch-up schedule (Figure 32-7).
The Future of Immunotherapy
Research concerning the development of new vaccines and the refinement of established vaccines continues at an amazing pace. The use of transgenic plants for oral administration of bacterial and viral antigens would enable low-cost, effective distribution. Research in the field of transcutaneous immunization involves the application of an antigen with an adjuvant to the intact skin. Recombinant DNA technology and the use of adjuvants are being developed for rheumatic fever and malaria. Alum is an adjuvant currently used in the vaccine against hepatitis B to increase its effectiveness. RNA and DNA viruses are being developed for use as carriers (vectors) of other antigens. Forms of bacterial DNA are also being developed as carriers of antigens. A “gene gun” that blasts the vaccine through intact skin is also in the development stage. The techniques in research may hold promise for developing effective vaccines against influenza A virus, HIV type 1 (HIV-1), malaria organisms, and the Ebola virus. A catalogue of genes that code for viruses and potential immunogens is being studied.
The most exciting development in immunology is the use of immunotherapy for noncommunicable diseases. An example would be the mucosal administration of myelin in multiple sclerosis and a type 2 collagen for rheumatic arthritis. The possibility of preventing specific types of cancer has been recognized, and the challenge of developing tumor antigens that lyse tumor cells is also a clear possibility. In Alzheimer’s disease the formation of neurotoxic plaques in the brain causes the loss of mental function. Early immunization with amyloid B may prevent or lyse the plaque formation and prevent the devastating problems of this disease.
The use of immunotherapy for autoimmune diseases is promising. The greatest achievement of the twentieth century was the eradication of smallpox and the development of many safe vaccines for children. Perhaps the achievement of the twenty-first century will be the development of immunotherapy for noncommunicable diseases such as Alzheimer’s disease and cancer.
Bioterrorism and the Pediatric Patient
A New Type of Childhood Trauma
Physiological Effects
Children are generally more vulnerable to biological warfare, because their immune systems are not fully developed. They are also closer to the ground, so heavy particles from an aerosol-propelled agent may reach them in higher doses than a taller adult. All new drugs are tested on adults as they are being developed, and it sometimes takes many years to determine safety for the pediatric patient. Therefore a new drug that is developed to treat a bioterror or chemical agent may in reality be more harmful than beneficial to the pediatric patient. The large head and body surface area in relation to weight and the low body fat content makes the child more vulnerable to develop hypothermia, which can be life threatening in the pediatric age-group. Therefore the routine “hazmat” decontamination procedure of stripping and total body washing may not be suitable for the pediatric patient.
The thin skin of the pediatric patient may make dermal chemicals, such as mustard gas, more dangerous to children than adults. A relatively small blood volume makes children more susceptible to fluid losses caused by cholera or other gastrointestinal toxins. Smallpox vaccine cannot be given to pregnant women, and other vaccines, such as anthrax, may not be useful for children. Gas masks are often not available in pediatric sizes, and the national disaster medical system protocol may not make provisions for pediatric beds.
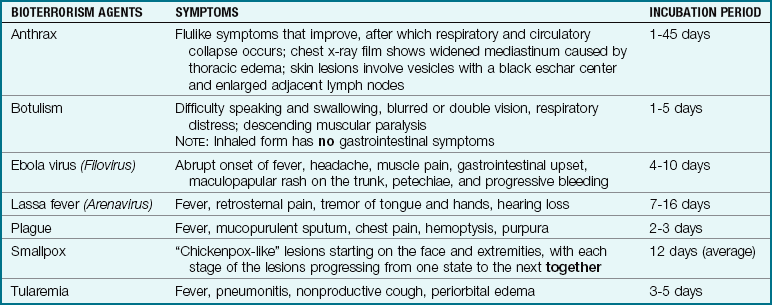
Table 32-2 lists common diseases (and their symptoms) that are spread through bioterrorism. Chemical agents that may be used in a terrorist attack may include pulmonary agents such as chlorine, cyanide agents such as sulfur mustard, nerve agents such as sarin, or incapacitating agents such as the military glycolate anticholinergic compound coded BZ by the North Atlantic Treaty Organization (NATO). The local health department’s bioterrorism branch should be contacted concerning the management of victims.
Psychological Effects
Terrorist acts in the form of chemical warfare or physical assaults such as bombings can be brought into the home via television from remote locations in the United States, thus violating a child’s personal feeling of safety. Children listen to television and to their trusted adults expressing fears, perhaps lose loved ones or friends, and may play out their own fears with toys, in art, or through altered behavior.
The Nurse’s Role
Emergency Preparedness: The nurse can assist families to prepare for natural disasters, such as hurricanes or floods, or manmade disasters, such as bioterrorist attacks or bombings. The American Medical Association (AMA) office guidelines for preparing a family and community disaster plan state that the family should keep several days’ supply of food, water, pet food, warm clothing, blankets, copies of vital documents, and toiletries on hand. A battery-powered radio and extra medications, eyeglasses, and basic first aid supplies are also essential. Disaster drills held on a regular schedule should include emergency plans, exit strategies, and out-of-state family contact phone numbers or email addresses. Children should be taught the importance of keeping personal identification with them at all times (perhaps an ID bracelet for infants or small children) and how to call for help when needed (see Online Resources).
Initial Observation: Although the ABCs of emergency triage for adults apply to children, a pediatric quick examination includes the following:
• Airway: Assess for blockage or obstruction that may be present
• Breathing (respiratory effort): Tachypnea may indicate shock, whereas retractions may indicate a lung problem
• Circulation: Circulatory problems causing cyanosis, pallor, mottling, capillary refill time (CFT) more than 2 seconds
• Mental status: Alert, awareness of surroundings, interacts
The initial examination of a patient after suspected exposure to a biological agent may be delayed between exposure and the development of symptoms (incubation period). Tentative triage categories for victims of bioterrorist attacks may include immediate (requiring prompt intervention), delayed (care can wait for a short time), minimal (only outpatient care is required), and expectant (moribund victims unlikely to survive lifesaving measures) (Armstrong, 2002).
A heightened awareness by health care professionals plays a critical role in facilitating early recognition of the release of a biological agent as a weapon. The health care professional must immediately notify the infection prevention and control department of the hospital, which will work with hospital administration and the local health department. The CDC in Atlanta will be notified of the suspected or confirmed event by the state health department. It is very important that the reporting chain of command be followed. A 24-hour local health department contact number is available to the health care professional.
The Pediatric Patient in a Disaster Setting
The pediatric patient has a proportionately larger body surface area and thinner skin than an adult. Children may also suffer increased pulmonary problems from the same exposure as adults. Children are closer to the ground and may be more readily exposed to vaporized agents of terror. The immature blood-brain barrier and increased central nervous system (CNS) receptor sensitivity may increase susceptibility of children to the effects of nerve agents. Vascular access may be difficult in the pediatric patient, and dosage calculations for varied kilogram weights increases the challenge for safe medical therapy for this population. Pediatric autoinjectors of low-dose atropine and pralidoxime are available for treatment of children with severe clinical symptoms after nerve agent exposure. Drs. Jim Broselow and Bob Luten have developed a color-coding system to reduce medication errors in children. Their systems includes a water-resistant “Pediatric Antidotes for Chemical Warfare tape,” which measures the child’s length to determine weight and color zones that correlate to safe dosages of specific emergency drugs commonly used in bioterrorism attacks. This tape is used as a guide in emergency care in the field or hospital emergency rooms.
Sexually Transmitted Infections
Sexually transmitted infection (STI) is the general name given to infections spread through direct sexual activity. This term replaces the terms sexually transmitted disease and venereal disease. STIs can be transmitted by a pregnant woman to her unborn child and cause serious problems in the fetus such as blindness, birth defects, or death (Table 32-3). The occurrence of an STI in a prepubertal patient should always prompt investigation into the possibility of sexual abuse.
Table 32-3
Nursing Care to Prevent and Treat Sexually Transmitted Infections
| Nursing Goals |
| CONCERN | NURSING INTERVENTIONS |
| Children under 12 years of age | Provide age-appropriate instruction concerning sexuality; also explore expected patterns that might occur before next visit. |
| Puberty and adolescence | Review structure and function of reproductive systems; review personal hygiene; discuss values and decision making, possible sexual behavior and consequences, and prevention of pregnancy and sexually transmitted infections (STIs). |
| Self-concept: anticipate evidence of fear, embarrassment, anger, and decreased self-esteem upon suspicion of infection | Create nonjudgmental atmosphere; listen, assess level of knowledge, observe nonverbal behavior, establish confidentiality; provide privacy when assisting with pelvic or genital examination; provide appropriate draping of patient; realize anger is often a mask for depression, grief—do not take personally. |
| Skin and hair | It is not uncommon to see skin rashes, “crabs” (pubic lice), or scabies (mites). |
| Sexual partners | Determine sexual preference; investigate and direct to treatment; persons at particular risk are those who have multiple sexual partners, are homosexuals, are with new partners, or have history of prior STI. |
| Sexual intercourse | Encourage patient to abstain during treatment; use condom to prevent reinfection. |
| Medication | Encourage patient to take all of prescribed medication; if taking tetracycline, advise to take 1 hour before or 2 hours after meals (on empty stomach); avoid dairy products, antacids, iron, and sunlight. |
| Compliance with treatment | Stress importance of follow-up and routine annual Papanicolaou (Pap) smears. |
| Sequelae | Discuss the possible complications of specific disorders such as birth defects and infertility. |
Nursing Care and Responsibilities
Regardless of the medical professional’s feelings about the changes in society and sexual permissiveness, the consequences of these changes must be recognized and managed. Nurses who wish to help adolescents with STIs must create an environment in which the adolescent feels safe and at ease. Adolescents need emotional support, which the nurse can provide through listening and maintaining a nonjudgmental attitude.
The nurse approaches the patient with sensitivity and recognizes that the adolescent is embarrassed and in need of privacy, especially during examinations. Girls are often afraid and always nervous about a pelvic examination. This is true even when their outward manner may seem otherwise. Careful explanations are needed. The patient is draped appropriately, and the nurse remains during the examination to provide reassurance. The findings are discussed with the patient, and questions are encouraged. Most adolescents need to be drawn out and do not readily ask questions, even when they do not understand.
The requirement to report sexual contacts is an emotionally charged topic that often prevents patients from seeking help. The person who is assured of confidentiality and who has been treated in a dignified manner is more apt to cooperate. Girls who are sexually active must be taught to take responsibility for their own health. Young people must be made aware of the fact that sex with only one partner does not eliminate the risk because this partner may have had contact with others; the partner needs to have had only one sexual experience with one infected person to transmit disease.
The nurse assesses the person’s level of knowledge and provides information at an understandable level. Many young people have little knowledge of their body and their developing sexuality. Others have mild to deep-seated emotional problems that must be addressed. They may be using sex to escape from reality, to express hostility or rebellion, or to call attention to themselves. They may be involved in relationships they no longer desire and therefore need help in formulating positive attitudes toward themselves. They also need help understanding their behavior and that of others. In particular, adolescents must learn that they are responsible for their own actions if they choose to be sexually active. Prevention of STIs is discussed in Chapter 11.
HIV/AIDS in Children
Pediatric HIV/AIDS is a worldwide public health problem with a devastating outcome. Children usually acquire the HIV infection through the following:
• Contact with an infected mother at birth (approximately 90% of cases in infants)
• Sexual contact with an infected person
• Use of contaminated needles or contact with infected blood
Educating the public about the role of unprotected sex and intravenous drug abuse in increasing the risk of HIV infection is a public health challenge. The recommended HIV counseling and testing for pregnant women and the highly active antiretroviral therapy (HAART) has played an important role in preventing perinatal transmission (Cibulka, 2006).
AIDS is caused by a retrovirus known as HIV-1 that attacks lymphocytes (the white blood cells that protect against disease). It appears to cause an imbalance between the helper T cells (CD4+) that support the immune system and the suppressor T cells that shut it down. In a person not infected with HIV, the number of CD4+ cells remains constant over time. In an HIV-infected person, the number of CD4+ cells drops as months and years go by. The CD4+ cell count is a measure of the damage to the immune system caused by HIV and of the body’s ability to fight infection. A physician uses the CD4+ cell count to help determine the best medical treatments for the individual.
A series of terms for this disorder have been developed, but the disease is now classified along a continuum of categories by the CDC:
• Asymptomatic infection. This refers to a latent period. Individuals in this category have positive antibody tests, indicating exposure to the virus, but they are not ill.
• Symptomatic HIV infection. Many individuals have this earlier and milder condition (compared with AIDS). This was formerly referred to as AIDS-related complex (ARC).
• AIDS. This refers to the most advanced involvement, which includes the finding of HIV antibodies in the patient’s blood, the presence of complicating opportunistic infections, and other criteria.
Children do not get AIDS from casual relationships at schools and medical facilities or through family living. The virus is infectious but not highly contagious, and the circumstances for acquiring it are specific, as previously indicated. Improved attention to hygiene practices in response to this disease can only be applauded.
Because passive transmission of antibodies from the mother occurs, infants are born with antibodies that crossed the placenta. Some infants’ systems become clear of antibodies in about 15 months, whereas other infants eventually experience the infection. Because of the transference of antibodies, the standard enzyme-linked immunosorbent assay (ELISA) and Western blot tests used to diagnose HIV infection in older children and adults are less reliable until the child is at least 15 months of age.
Manifestations
Criteria for the disease in children have been outlined by the CDC. Initial symptoms in infancy are vague and include failure to thrive, lymphadenopathy (enlarged lymph glands), chronic sinusitis, and nonresponse to the treatment of infections. The patient becomes subject to overwhelming infection. Opportunistic infections such as oral thrush, Pneumocystis jiroveci (formerly called Pneumocystis carinii) pneumonia, herpes viruses, and cytomegalovirus take advantage of the body’s depressed immune system. Kaposi’s sarcoma, a rare type of skin cancer, appears to be less common in children than in adults. Serious bacterial infections such as meningitis, impetigo, and urinary tract problems are reported in children. In general, the symptoms of HIV infection develop more rapidly in infants, and this may be attributed to the infant’s immature immune system.
Treatment and Nursing Care
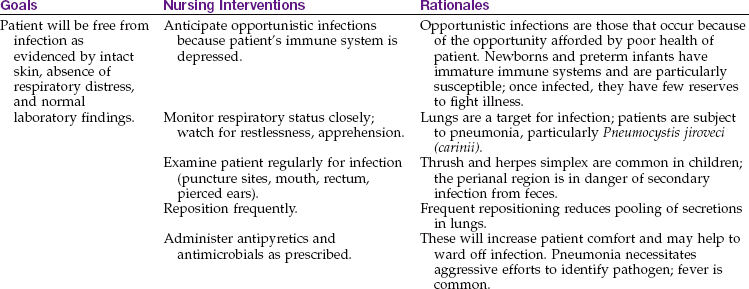
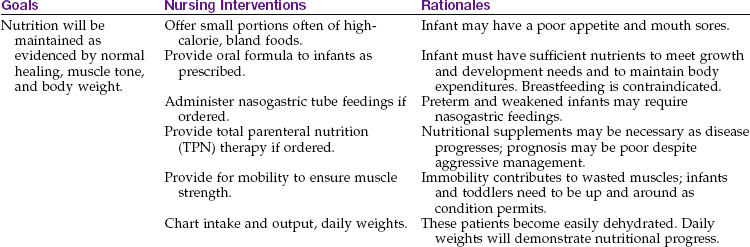
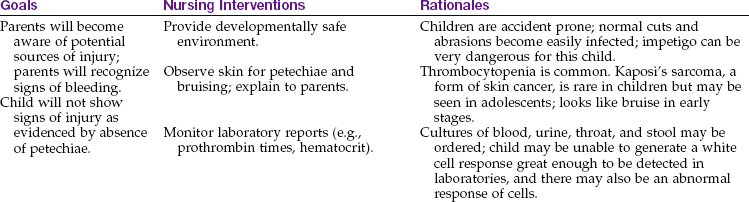
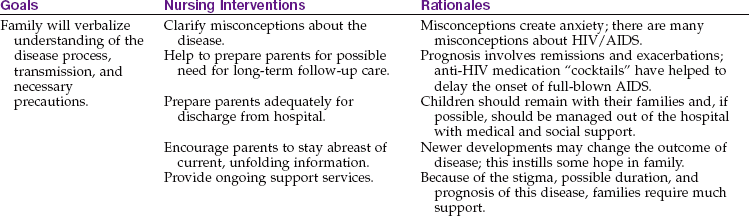
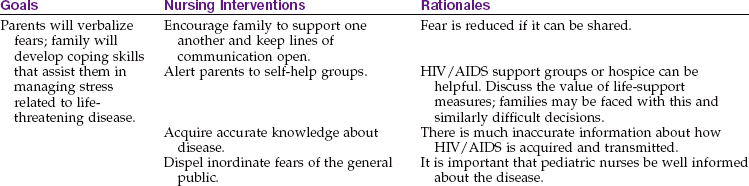
The goals of care are to slow the growth of the virus, prevent opportunistic infections, and provide adequate nutrition and supportive therapy. Assessment and care of the child with HIV/AIDS are critically important. Education concerning long-term compliance with prescribed antiviral drugs and supportive care to promote growth and development are essential. The CD4+ and lymphocyte counts are normally high in infancy and decline to adult levels when a child is approximately 6 years old. Nursing Care Plan 32-1 provides selected nursing diagnoses and interventions for a newborn or infant with HIV/AIDS.
32-1  Nursing Care Plan
Nursing Care Plan
The Infant with HIV
An infant boy, who is positive for human immunodeficiency virus (HIV), has been admitted with an upper respiratory infection; his mother is rooming in.

Fear (parents and patient) related to loss of normal life or possible death
1. A new mother has been diagnosed with AIDS and is rooming-in with her infant in the pediatric unit. The mother states she wants to breastfeed her infant because she feels well enough. Her CD4+ levels are high. She states she wants herself and the infant to adhere to normal routine practices like other healthy newborns. What nursing response is appropriate?
Psychological support for these children is paramount. Sensory stimulation and touching are especially important for infants. The effects of isolation can be physically and emotionally devastating to the developing child. Many infants are abandoned, outlive their mothers, or must live in foster care. Unique programs such as Children’s AIDS Program (CAP) provide a homelike respite care environment and day care. The goal of the program is to help families living with HIV/AIDS infection to stay together.
The nurse anticipates interventions related to the care of the child with a life-threatening disease. Efforts to support families in crisis are particularly pertinent. Often the extended family must take over. Many families have few financial resources and are exhausted from the child’s frequent hospitalizations and physical care. They need to be introduced to such agencies as social service, financial aid, HIV/AIDS and grief support groups, home health, nutritional programs such as Women, Infants, and Children (WIC), and hospice.
Several medications are used to manage HIV/AIDS in children. A fungal infection caused by P. jiroveci may be the first opportunistic infection to affect the pediatric patient. Prophylactic medications are available. The nurse should be alert for central nervous system involvement such as motor deficits or a failure to achieve developmental milestones. RSV, pneumonia, renal failure, and gastrointestinal malfunction often plague the child with HIV/AIDS.
Children with HIV/AIDS should be assessed for the need to update routine immunizations. Tuberculosis testing is done routinely and as needed. Several antiviral drugs are being tested in children. Early diagnosis and treatment can improve the quality and length of life for many children.
Prevention
Prevention is the core of education related to HIV/AIDS. Education of adolescents should include methods of transmission, hazards of IV and illicit drug use, and safe sex practices. The strict use of standard precautions when caring for all patients is essential, especially when handling blood and other body fluids. The health education curriculum in elementary school for students and staff should include information concerning HIV/AIDS prevention. Nurses should encourage high-risk adolescents to undergo counseling and testing with the hope of modifying risky behaviors.
Get Ready for the NCLEX® Examination!
Key Points
• Standard precautions are techniques recommended by the CDC to prevent the transmission of communicable diseases.
• Body substance refers to moist secretions of the body that can contain microorganisms.
• An opportunistic infection is caused by organisms normally found in the environment that the immunosuppressed child cannot fight.
• Immunization programs in the United States provide active immunity for children.
• Proper hand hygiene is the basic essential factor in preventing the transmission of infection.
• Proper storage of vaccines and appropriate routes of administration are essential to ensure the potency of the vaccine.
• Education of parents about the need for immunizations against common childhood communicable diseases is a primary nursing responsibility.
• It is the responsibility of the nurse to know when the immunizations are due, the immunization history of the child, contraindications, routes of administration, and which vaccines can be given together. The child should be observed for untoward reactions for at least 20 minutes following immunization.
• Koplik spots are white spots on the mucous membrane of the oral cavity that occur before a skin rash and are indicative of measles (rubeola) infection.
• In chickenpox (varicella), all stages of the skin lesions are present on the skin at the same time.
• A child with German measles (rubella) should not be cared for by a woman in the early months of pregnancy because the virus can cause fetal anomalies.
• In children with roseola, a persistently high fever suddenly drops as the rash erupts.
• Gamma globulin offers passive immunity for exposed children who are immunosuppressed.
• The AMA offers guidelines to help families to prepare for community disasters.
• Listening skills and a nonjudgmental attitude are essential when caring for adolescents with sexually transmitted infections (STIs).
• Children acquire the HIV/AIDS infection by contact with an infected mother at birth, sexual contact with an infected person, or use of contaminated needles during drug use.
• The long-term nursing goals in the care for a child with AIDS are to promote compliance for long-term drug therapy and to provide support to maintain optimum growth and development.
Additional Learning Resources
 Go to your Study Guide for additional learning activities to help you master this chapter content.
Go to your Study Guide for additional learning activities to help you master this chapter content.
Go to your Evolve website (http://evolve.elsevier.com/Leifer) for the following FREE learning resources:
• Answer Guidelines for Critical Thinking Questions
• Answers and Rationales for Review Questions for the NCLEX® Examination
• Glossary with English and Spanish pronunciations
• Interactive Review Questions for the NCLEX® Examination
• Patient Teaching Plans in English and Spanish
 Online Resources
Online Resources• Advisory Committee on Immunization Practices (ACIP): www.cdc.gov/vaccines/recs/acip/default.htm
• Broselow-Luten System: www.colorcodingkids.com/index.html
• Child health statistics: www.childstats.gov
• National Immunization Program: www.cdc.gov/vaccines/
• Public health emergency preparedness and response: www.bt.cdc.gov; http://pediatrics.aappublications.org/cgi/content/abstract/117/2/560
• Smallpox vaccine recommendations: www.cdc.gov/mmwr/preview/mmwrhtml/rr5010a1.htm
• Specific group vaccine schedules: www.cdc.gov/vaccines/spec-grps/default.htm
• Vaccine Adverse Events Reporting Service: www.vaers.hhs.gov
• Vaccine information statements (VISs): www.cdc.gov/vaccines/pubs/vis
Review Questions for the NCLEX® Examination
1. The nurse is caring for a newborn with HIV/AIDS. What is the priority goal?
2. An adolescent diagnosed with AIDS asks about the mode of transmission for the illness. An accurate response is that it was most likely through:
1. casual contact with a friend who is HIV-positive.
2. a latent response to an inherited predisposition.
3. use of a contaminated toilet seat.
4. contact with contaminated body substance through sex or intravenous needle use.
3. When providing play therapy for a child with a communicable disease who is in an isolation room, what would be one priority principle or rationale for toy selection?
1. The toy should be selected from the hospital playroom.
4. A parent brings a 4-month-old infant to the clinic for the second in the routine immunization series. The nurse should prepare for administration of which immunizations?