The Child with a Skin Condition
1 Define each key term listed.
2 Recall the differences between the skin of the infant and that of the adult.
3 Identify common congenital skin lesions and infections.
4 Describe two topical agents used to treat acne.
5 Summarize the nursing care for a child who has infantile eczema. State the rationale for each nursing measure.
6 Discuss the nursing care of various microbial infections of the skin.
7 Discuss the prevention and care of pediculosis and scabies.
8 Differentiate among first-, second-, and third-degree burns: the anatomical structures involved, the appearance, the level of sensation, and the first aid required.
9 List five objectives of the nurse caring for the burned child.
10 Describe how the response of the child with burns differs from that of the adult.
11 Identify the principles of topical therapy.
12 Differentiate four types of topical medication.
13 Examine the emergency treatment of three types of burns.
14 Discuss the prevention and treatment of sunburn and frostbite.
 , p. 695)
, p. 695) , p. 699)
, p. 699) , p. 704)
, p. 704) , p. 707)
, p. 707) , p. 694)
, p. 694) , p. 704)
, p. 704) , p. 704)
, p. 704) , p. 694)
, p. 694) , p. 691)
, p. 691) , p. 696)
, p. 696) , p. 703)
, p. 703) , p. 690)
, p. 690) , p. 704)
, p. 704) , p. 704)
, p. 704) , p. 704)
, p. 704) , p. 704)
, p. 704) , p. 691)
, p. 691)
 , p. 698)
, p. 698) , p. 691)
, p. 691) , p. 700)
, p. 700) , p. 692)
, p. 692) , p. 691)
, p. 691) , p. 691)
, p. 691) , p. 691)
, p. 691) , p. 704)
, p. 704) http://evolve.elsevier.com/Leifer
http://evolve.elsevier.com/Leifer
Skin Development and Functions
The main function of the skin is protection. It acts as the body’s first line of defense against disease. It prevents the passage of harmful physical and chemical agents and prevents the loss of water and electrolytes. It also has a great capacity to regenerate and repair itself. The skin and the structures derived from it, such as hair and fingernails, are known as the integumentary system. Figure 30-1 depicts these structures and how they differ in the developing child and in the adult.
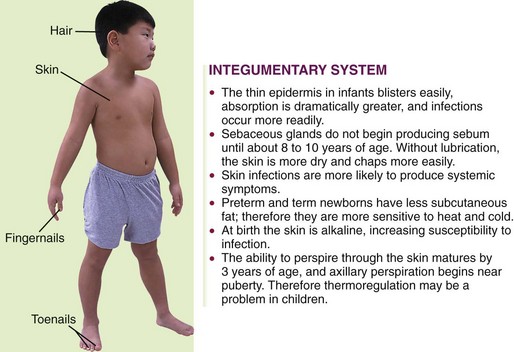
FIGURE 30-1 Summary of some integumentary system differences between the child and the adult. The integumentary system consists of the skin and the structures derived from it. This system protects the body, helps to regulate body temperature, and receives stimuli such as pressure, pain, and temperature.
Maintaining skin integrity is important to self-esteem and therefore has both a psychological and a physiological component. This is particularly evident in patients with facial disfiguration. Four basic skin sensations—pain, temperature, touch, and pressure—are felt by the skin in conjunction with the nervous system. The skin also secretes sebum, which helps to protect and maintain its texture. The outer surface of the skin is acidic, with a pH of 4.5 to 6.5 to protect the skin from pathological bacteria, which thrive in an alkaline environment.
The skin is composed of two layers: the epidermis (derived from the ectoderm) and the dermis (derived from the mesoderm). Vernix caseosa, a cheeselike substance, covers the fetus until birth. This protects the fetal skin from maceration as the fetus floats in its watery home. The fetal skin is at first so transparent that blood vessels are clearly visible. Downy lanugo hair begins to develop at about 13 to 16 weeks, especially on the head. At 21 to 24 weeks the skin is reddish and wrinkled, with little subcutaneous fat. Adipose tissue forms during later weeks. At birth the subcutaneous glands are well developed, and the skin is pink and smooth and has a polished look. It is thinner than the skin of an adult.
Skin Disorders and Variations
Certain skin conditions in children may be associated with age, as in the case of milia in infants and acne in adolescents. A skin condition may be a manifestation of a systemic disease, such as chickenpox. Some lesions, such as strawberry nevi and mongolian spots, are congenital. Other skin lesions, such as those seen in rubella and fifth disease, are self-limited and do not necessitate treatment.
There are great individual differences in skin texture, color, pH, and moisture. Skin color is an important diagnostic criterion in cases of liver disease, heart conditions, and child abuse and for overall assessment. Complete blood counts and serum electrolyte levels are helpful in diagnosing skin conditions. Skin tests are used in diagnosing allergies. The purified protein derivative (PPD) test is useful in screening for tuberculosis. Skin scrapings are used for microscopic examination. The Wood’s light is an instrument used to diagnose certain skin conditions. It reflects a particular color according to the organism present.
Hair condition is important to observe. Hair is inspected for color, texture, quality, distribution, and elasticity. Hair may become dry and brittle and may lack luster owing to inadequate nutrition. Hair may begin to fall out or even change color during illness or the ingestion of certain medications.
Skin conditions may be acute or chronic. The nurse should describe the lesions with regard to size, color, configuration (e.g., butterfly rash), presence of pain or itching, distribution (e.g., arms, legs, behind ears), and whether the rash is general or local. Hives, a general rash that appears abruptly, is often an allergic or medication reaction. The condition of the skin around the lesions is also significant, as is the skin turgor. Managing itching is a key component in preventing secondary infection from scratching. Dressings and ointments are applied as prescribed. Preventing infections is a consideration in open wounds. Mongolian spots and physiological jaundice are covered in Chapters 12 and 14. The communicable diseases are discussed in Chapter 32.
Many childhood infectious diseases, such as measles, German measles, and chickenpox, involve the presence of an exanthem (a skin rash). Box 30-1 identifies terms used to describe some conditions of the skin that the nurse may witness. Some rashes begin as one lesion and evolve into others. For example, the sequence of chickenpox rash is macule to papule, to vesicle, and then to crust. A stye is an infection of the sebaceous gland of the eyelash (Figure 30-2).
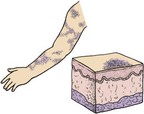
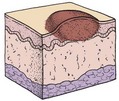
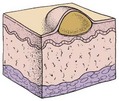
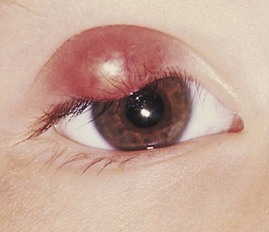
FIGURE 30-2 A stye, or hordeolum, is an inflammation of the sebaceous gland of the eyelid commonly seen in infants and children.
Congenital Lesions
The strawberry nevus (Figure 30-3) is a common hemangioma (consists of dilated capillaries in the dermal space) that may not become apparent for a few weeks after birth. Although it is harmless and usually disappears without treatment, it is disturbing to parents, especially when it appears on the head or face. At first it is flat, but it gradually becomes raised. The lesion is bright red, elevated, and sharply demarcated. The lesions gradually blanch, with 60% disappearing spontaneously by 5 years of age and 90% disappearing by 9 years of age. Laser treatment or excision may be considered if the area becomes ulcerated. Parents are often quizzed about the growth by insensitive persons and may be advised of various unorthodox treatments. The nurse offers support and reassurance to parents and corrects misinformation. After laser surgery, the skin may appear black for 7 to 10 days. Salicylates should be avoided, and sun exposure should be minimized.

Port-Wine Nevus
Port-wine nevi (Figure 30-4) are present at birth and are caused by dilated dermal capillaries. The lesions are flat, sharply demarcated, and purple to pink. The lesion darkens as the child gets older. If the area is small, cosmetics may disguise the lesion. If the area is large, laser surgery may be indicated.

Skin Manifestations of Illness
• Café au lait macules occur in 10% to 20% of people and are light brown, oval patches on the skin. Multiple café au lait macules are associated with neurofibromatosis (a chromosomal abnormality) and tuberous sclerosis.
• Hypopigmented macules are whitish oval- or leaf-shaped macules. Multiple hypopigmented macules are associated with tuberous sclerosis.
• Butterfly rash over the nose and cheeks can be associated with photosensitivity and may be associated with systemic lupus erythematosus (SLE).
• Scaling skin eruption around the mouth in a horseshoe-like distribution, around the chin and cheeks or as a perianal rash and involving papules and scales, is associated with zinc deficiency in infants. It also is associated with diarrhea and failure to thrive.
• Vascular birth marks such as hemangioma resemble a bruise that changes in appearance over the years. Hemangiomas around the chin may be associated with airway problems, and those appearing around the lumbar region may be associated with spinal problems.
Infections
Pathophysiology: Miliaria (prickly heat) refers to a rash caused by excess body heat and moisture (Figure 30-5). There is a retention of sweat in the sweat glands, which have become blocked or inflamed. Rupture or leakage into the skin causes the inflamed response. It appears suddenly as tiny, pinhead-sized, reddened papules with occasional clear vesicles. It may be accompanied by pruritus (itching). It is seen in infants during hot weather or in newborns that sleep in overheated rooms. It often occurs in the diaper area or in the folds of the skin where moisture accumulates. Plastic enclosures on diapers hold in body warmth that results in a rash. This harmless condition may be reversed by removing extra clothing, bathing, skin care, and frequent diaper changes.

Intertrigo
Pathophysiology: Intertrigo (in, “into,” and terere, “to rub”) is the medical term for chafing. It is a dermatitis that occurs in the folds of the skin (Figure 30-6). The patches are red and moist and are usually located along the neck and in the inguinal and gluteal folds. This condition is aggravated by urine, feces, heat, and moisture. Obese children are more prone to intertrigo. Prevention consists of keeping the affected areas clean and dry. The child is allowed to be out of diapers to expose the area to air and light. Maceration of the skin can lead to secondary infections.

Seborrheic Dermatitis
Pathophysiology: Seborrheic dermatitis (cradle cap) is an inflammation of the skin that involves the sebaceous glands (Figure 30-7). It is characterized by thick, yellow, oily, adherent, crustlike scales on the scalp and the forehead. The skin beneath the patches may be red (erythematous). Less often it may involve the eyelids, the external ear, and the inguinal area. Secondary bacterial and yeast infections may occur. It is seen in newborns, in infants, and at puberty. In newborns it is commonly known as “cradle cap.” It is seen in infants with sensitive skin, even when the head and hair are washed frequently. Seborrhea resembles eczema, but it usually does not itch and there is a negative family history. In adolescence it is more localized and is usually confined to the scalp. A condition resembling seborrheic dermatitis is common in children and adolescents infected with the human immunodeficiency virus (HIV).

Treatment: Treatment consists of shampooing the hair on a regular basis. Scales that are particularly stubborn in newborns may be softened by applying baby oil to the head the evening before and shampooing in the morning. The scalp is rinsed well. A soft brush is helpful in removing loose particles from the hair. The nurse teaches the parent how to shampoo an infant’s head using the football hold (see Figure 22-4). A dandruff-control shampoo is used for adolescents. Medications such as sulfur, salicylic acid, or hydrocortisone may be prescribed. Topical antifungal agents effective against Pityrosporum have also been suggested. The response to therapy is usually rapid.
Diaper Dermatitis
Pathophysiology: Diaper dermatitis (diaper rash) is a commonly seen condition that results from prolonged contact of the skin to a mixture of urine and feces. The urine increases the pH of the skin, resulting in increased sensitivity to fecal enzymes. If the skin remains moist inside the soiled diaper, the skin may become more likely to develop a Candida albicans infection. The rash of simple diaper dermatitis may appear as an erythema (redness); however, a beefy red rash in the diaper area may be indicative of a Candida (thrush) infection and necessitates prompt treatment (Figure 30-8). Disposable diapers contain a super-absorbent gel material that helps maintain normal skin pH and therefore reduces the occurrence of diaper dermatitis.

Treatment and Nursing Care: It is easier to prevent diaper rash than to cure it. This is accomplished by frequent diaper changes to limit the skin’s exposure to moisture. The diaper is periodically removed to expose the skin to light and air. With each diaper change, the perineal area is gently and thoroughly cleansed (preferably with warm water) and gently dried. After bowel movements, the area is cleansed with mild soap and water. The skin folds are thoroughly washed, rinsed, and dried. A cloth, non–alcohol-containing wipe or a cosmetic pad may be used to remove feces from the skin. Some common over-the-counter ointments for prevention of diaper dermatitis include ointments with the active ingredients of vitamins A and D and lanolin, and other products containing 10% zinc oxide. Products with a higher percentage of zinc oxide are protective but hard to wash off. Aggressive scrubbing of the skin should be avoided. Mineral oil can aid in removing sticky ointments. The use of corticosteroid ointments in an occluded diaper area should be avoided since skin absorption can cause systemic complications (Eichenfeld et al., 2008).
Acne Vulgaris
Pathophysiology: Acne is an inflammation of the sebaceous glands and hair follicles in the skin (Figure 30-9). Because of hormonal influence, the sebaceous glands enlarge at puberty and secrete increased amounts of a fatty substance called sebum. Genetic factors and stress are also thought to play a part. The course of acne may be brief or prolonged (lasting 10 years or longer). Premenstrual acne in girls is not uncommon. The principal lesions include comedones, papules, and nodulocystic growths.

FIGURE 30-9 Acne. Acne is the most common skin problem of adolescence. An increase in sebaceous gland activity creates increased oiliness. Open comedones (blackheads) and closed comedones (whiteheads) are common. Severe acne includes papules and nodules. The lesions appear on the face, chest, back, and shoulders.
A comedo (plural, comedones) is a plug of keratin, sebum, or bacteria. Keratin is a protein substance and is the main constituent of epidermis and hair. There are two types of comedones: open and closed. In the open comedo, or blackhead, the surface is darkened by melanin. Closed comedones, or whiteheads, are responsible for the inflammatory process of acne. With continued buildup, the walls of the follicle rupture, releasing their irritating contents into the surrounding skin. A pustule may appear when this develops near the exterior. This process occurs no matter how carefully the teenager washes because surface bacteria are not involved in the pathogenesis. Acne is usually seen on the chin, the cheeks, and the forehead. It can also develop on the chest, the upper back, and the shoulders. It usually is more severe in winter.
Treatment: The basic treatment of acne has changed considerably over the past few years. It is no longer thought that certain foods trigger the condition; therefore the restriction of chocolate, peanuts, and cola drinks is unwarranted. A regular, well-balanced diet is encouraged. Patients who are not taking tetracycline or vitamin A benefit from sunshine. General hygienic measures of cleanliness, rest, and the avoidance of emotional stress may help to prevent exacerbations.
Routine skin cleansing is indicated, and greasy hair and cosmetic preparations should be avoided. Excessive cleansing of the skin can irritate and chap the tissues. Squeezing pimples ruptures intact lesions and causes local inflammation. The topical preparations recommended include benzoyl peroxide gels or lotions that dry and peel the skin and suppress fatty acid growth. Tretinoin acid (Retin-A) helps eliminate keratinous plugs. Vitamin A can increase sensitivity to the sun, so precautions should be taken when it is used. Tetracycline, erythromycin, doxycycline (Vibramycin), or minocycline (Minocin) may be given in conjunction with topical medications in more serious cases. Monilial vaginitis is a secondary complication sometimes seen when these drugs are used, and this should be explained to the unsuspecting adolescent girl.
Isotretinoin (Accutane) is given to patients with severe pustulocystic acne who have been unable to benefit from other types of treatment. It has many side effects; thus the patient must be carefully monitored with liver studies and lipid levels. It is not prescribed during pregnancy or to those at risk for pregnancy because of the possibilities of fetal deformity. Planing of the skin to minimize scarring (dermabrasion) is done selectively, because it is not always successful. Oral contraceptives (OCs) such as Ortho Tri-Cyclen (norgestimate and ethinyl estradiol) may also be given because sebum production is controlled by androgens, and these OCs reduce androgen levels.
Acne is distressing to the adolescent, particularly when the face is extensively involved. Sometimes even a minimal problem is seen as disastrous when it happens before an important event. The self-conscious young person feels different and embarrassed. The nurse who is attuned to the feelings of individuals can provide understanding support. Although the adolescent is educated to assume responsibility for the regimen, including the parents helps to prevent conflict surrounding it. Drug-induced acne can occur in children taking long-term steroids, phenobarbital, phenytoin, lithium, vitamin B12, or medications containing iodides or bromides.
 Nursing Tip
Nursing TipHerpes Simplex Type I
Pathophysiology: Herpes simplex type I, a viral infection, is commonly known as a cold sore or fever blister. It may begin with a feeling of tingling, itching, or burning on the lip. Vesicles and crusts form (Figure 30-10). Spontaneous healing occurs in about 8 to 10 days. Communicability is highest early in the formation and is spread by direct contact. Recurrence is common because the virus lies dormant in the body until it is activated by stress, sun exposure, menstruation, fever, and other causes. Patients must become familiar with their own personal triggers. Herpes can be serious in newborns and in the patients who are immunocompromised.

Treatment and Nursing Care: Topical acyclovir may reduce viral shedding and hasten healing. In the hospital, ointments are applied with gloved hands. Contact and protective environment precautions should be followed (see Appendix A). Patients are instructed not to pick at lesions, because this may produce spreading to other sites. They should not share lipstick and should avoid kissing while lesions are active. Sensitivity to the self-conscious adolescent who has a cold sore is important. Genital herpes caused by the herpes virus type II and spread by sexual contact is discussed in Chapter 11 and Table 11-1. The distinction between the two types has become less clear because of an increase in the practice of oral-genital sex.
Infantile Eczema
Pathophysiology: Infantile eczema, or atopic dermatitis, is an inflammation of genetically hypersensitive skin (Figure 30-11). The pathophysiology is characterized by local vasodilation in affected areas. This progresses to spongiosis, or the breakdown of dermal cells and the formation of intradermal vesicles. Chronic scratching produces weeping and results in lichenification, or coarsening, of the skin folds. The exact cause of this condition is difficult to pinpoint because it is thought to be caused mainly by allergy. Infantile eczema is rarely seen in breastfed infants until they begin to eat additional food. It seems to follow a definite familial history of allergies; emotional factors are often involved.

FIGURE 30-11 Infantile eczema (atopic dermatitis) is characterized by erythematous papules and vesicles with weeping, oozing, and crusts on the face and body. Severe itching is common. There is often a family history of allergy.
Eczema is actually a symptom rather than a disorder. It indicates that the infant is oversensitive to certain substances called allergens, which enter the body via the digestive tract (food), by inhalation (dust, pollen), by direct contact (wool, soap, strong sunlight), or by injections (insect bites, vaccines). Some children develop the triad of atopic dermatitis, asthma, and hay fever.
Manifestations: Although infantile eczema can occur at any age, it is more common during the first 2 years. The pruritic lesions form vesicles that weep and develop a dry crust. They are more severe on the face but may occur on the entire body, particularly in the skin folds. Eczema is worse in the winter than in the summer and has periods of temporary remission.
The infant scratches because the itching is constant, and he or she is irritable and unable to sleep. The lesions become easily infected by bacterial or viral agents. Infants and children with eczema should not be exposed to adults with cold sores because they may develop a systemic reaction with high fever and multiple vesicles on the eczematous skin. Eczema may flare up after immunization. Laboratory studies may show an increase in immunoglobulin E (IgE) and eosinophil levels.
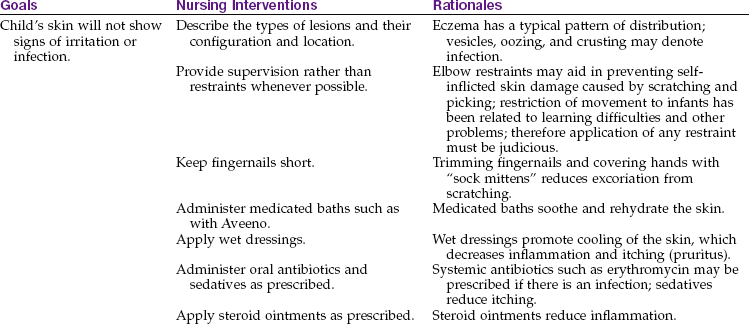
Treatment and Nursing Care: Treatment of the child with infantile eczema is aimed at relieving pruritus (itching), hydrating the skin, relieving inflammation, and preventing infection. An emollient bath is sometimes ordered for its soothing effect on the skin. Oatmeal and a mixture of cornstarch and baking soda are examples of emollients prescribed. The infant’s hair is washed with a soap substitute rather than a shampoo. Some dermatologists think that bathing should be kept to a minimum. The physician may suggest that a bath oil such as Alpha Keri Therapeutic Bath Oil be used as the lesions begin to heal. This prevents the skin from becoming too dry. To be correctly used, bath oils should be added after the patient has soaked for a while and the skin is hydrated. In this way, moisture is sealed rather than excluded, as it is when oil is added before the patient gets into the tub.
Whenever possible, patients are treated at home because of the danger of infection in the hospital. When soap is used, a mild, nonperfumed soap such as Dove or Neutrogena is used. Glycerin-based lubricants are preferred over lanolin, which may be an irritant to an infant who is allergic to wool (Perry et al., 2010). Aquaphor and Eucerin are lotions that can be used to enhance skin hydration.
Corticosteroids may be administered systemically or locally. Antibiotics are needed if infection is present. Medication to help relieve itching is ordered for the patient. A child who is uncomfortable and unable to sleep may receive sedation.
The nurse plays a vital role in the treatment of patients with skin problems (Nursing Care Plan 30-1). The nurse should assess the family’s ability to cope with the care of this child at home. Techniques of home bathing or application of soaks combined with quiet playtime enhances family coping. Control of itching is essential. Ointments are applied with a gloved hand to minimize contact with the skin. The fingernails of the child are kept short, and cotton gloves or socks can be used to prevent scratching. Appropriate dress is advised, as is using cotton fabric and avoiding wool and stuffed animals because of their allergy potential. Clothes should be laundered using mild soaps, avoiding products that contain fragrances or harsh chemicals. Parents should be taught the principles of general hygiene to prevent secondary infection of the open skin lesions. A hypoallergenic formula and a plan to identify possible food allergens are explained to parents. When a food allergen is the cause of eczema, stopping the food results in a clearing of the skin; however, restarting the food after a time may cause an anaphylactic reaction. The types of topical medications are listed in Table 30-1.
30-1  Nursing Care Plan
Nursing Care Plan
The Child with Eczema
An 18-month-old child is brought to the clinic by his parents. The child has many open lesions on the skin and is diagnosed with eczema.
Risk for imbalanced nutrition, less than body requirements related to irritability, sensitivity to certain foods
Deficient parental knowledge related to nature of disorder

1. Parents bring their child to the clinic. This child has a history of long-term asthma and eczema. The child is dressed in a wool jacket and is eating from a bag of peanuts. The mother states she has been using a lanolin lotion for dry skin that her friend gave her, but the child’s skin lesions have only become worse. What teaching interventions by the nurse would be appropriate?
Table 30-1
| TYPE | DEFINITION |
| Cream | A water-based emulsion of oil in water that is nongreasy for use on weeping lesions |
| Ointment | An oil-based emulsion of water in oil that is clear and greasy; used on dry skin; does not rub off easily |
| Lotion | A suspension of powder in water that should be shaken well before using; may be drying; often used on scalp lesions |
| Aerosol spray | Suspension of medication in an alcohol base; alcohol evaporates, leaving medication on the skin; effective for hairy areas |
| Gel | A clear, semisolid emulsion; liquefies when applied to skin |
| Bath oils | Bath oils are not used in pediatrics because they lubricate the sides of the tub, causing falls and injuries; the value of the treatment must be weighed against the risks involved; colloidal oatmeal baths may be soothing |
Parent teaching concerning topical therapy: Skin lesions can be pruritic (itchy), scaling, weeping, or crusted. Most skin lesions cause psychological stress, which should be addressed for both the parents and the child with the skin lesion. Prevention of secondary infection is essential, and the nurse should help the parent to understand the signs of inflammation or infection. When topical medication is applied, the lesions may change in form or color as they heal. Parents should be advised of changes to expect and when to seek follow-up advice. The nurse should teach parents the principles and techniques of applying topical medication:
• Absorption is best when an ointment is applied after a warm bath.
• Medication should be applied by stroking in the direction of hair growth. (Circular or rubbing motions can inflame hair follicles.)
• Teach how much ointment to apply (e.g., pea-sized bead).
• The use of elbow restraints can prevent an infant from scratching while allowing freedom of movement.
• Do not use topical steroids when a viral infection is present.
Over-the-counter skin products: Parents should be guided in the use of over-the-counter products that affect skin health. Simple ointments such as petrolatum, A + D, and zinc oxide are helpful only if they are washed off completely between diaper changes. Frequent diaper changes are essential. High-absorbency disposable diapers decrease wetness of the skin and may help to prevent diaper dermatitis. Home-laundered diapers are not subject to high temperatures, and soaps often contain fragrances that may be irritating. Commercially prepared wipes sometimes contain perfumes and can leave the skin moist; warm water and a mild soap are less irritating. If paper towels are used, prints should be avoided because the color dyes can be irritating to the skin. Cortisone creams should be avoided because cortisone may temporarily clear the rash but does not resolve the underlying cause that will prevent recurrence.
Staphylococcal Infection
Pathophysiology: The genus of bacteria called Staphylococcus comprises common bacteria that are found in dust and on the skin. Under normal conditions, they do not present a problem to the healthy body’s defenses. Skin infections may occur if the number of organisms increases in preterm infants and newborns, whose general resistance is low. An abscess may form, and infection may enter the bloodstream. This condition is called septicemia. Pneumonia, osteomyelitis, or meningitis may result. Primary infection of the newborn may develop in the umbilicus or circumcision wound. It may occur while the newborn is in the hospital or after discharge. This infection spreads readily from one infant to another. Small pustules on the newborn must be reported immediately.
Treatment and Nursing Care: Antibiotics effective against the appropriate strain of Staphylococcus are administered. Ointments may be locally applied.
In past years the staphylococci that invaded the body developed resistance to the drugs in current use. Methicillin-resistant Staphylococcus aureus (MRSA) infections are resistant to certain antibiotics and are handled under strict contact isolation precautions. The use of disposable individual equipment for patients and aseptic techniques can decrease health care–associated spread of infection.
Scalded skin syndrome is caused by S. aureus. The lesions begin with a mild erythema with sandpaper texture; vesicles appear and rupture and peeling occurs, exposing a bright red surface. The skin looks as though it has been scalded, and child abuse is often suspected. Intravenous (IV) antibiotics, strict isolation, and prevention of secondary infection are priorities. Maintaining warmth and fluid-electrolyte balance are also important in the plan of care. Healing usually takes place without scarring.
Impetigo
Pathophysiology: Impetigo is an infectious disease of the skin caused by staphylococci or by group-A beta-hemolytic streptococci. It results when the organism comes in contact with a break in the skin, such as an insect bite. The bullous form seen primarily in infants is usually staphylococcal, whereas nonbullous types, more commonly seen in children and young adults, can harbor either organism. The newborn is susceptible to this infection because resistance to skin bacteria is low. Impetigo tends to spread from one area of skin to another and is contagious.
Manifestations: The first symptoms of a bullous lesion are red papules (Figure 30-12). These eventually become small vesicles or pustules surrounded by a reddened area. When the blister breaks, the surface beneath is raw and weeping. The lesions may occur anywhere but are most often found around the nose and mouth and in moist areas of the body, such as the creases of the neck, the axilla, and the groin. A crust may form in older children, and scratching may cause further infection.

Treatment and Nursing Care: Systemic antibiotics are administered either orally or parenterally. Parents are instructed to wash the lesions 3 or 4 times daily to remove crusts. Ointments such as mupirocin (Bactroban) may be prescribed for topical application. Prevention of the disease by treating small cuts promptly is important. The prognosis with proper treatment is good. Nursing care consists primarily of preventing this disease.
Education of parents includes reminding them of the necessity for prompt attention to minor cuts and bites. In diagnosed cases, compliance with the treatment regimen is needed to prevent the spread of infection to other children and family members. If the diagnosis is made in the newborn nursery, the infant is isolated to prevent other newborns from becoming infected. Nephritis may occur as a complication of beta-hemolytic streptococcal infections.
Fungal Infections
Pathophysiology: Fungal infections are caused by several closely related fungi that have a preference for invading the stratum corneum, the hair, and the nails. The word tinea comes from the Latin “worm.” The common name for this infection is ringworm. Fungi are larger than bacteria. Some fungi may be transmitted from person to person and others from animal to person. The name denotes the part of the body involved.
Tinea capitis: Tinea capitis (“ringworm of the scalp”) is seen in school-age children. It is characterized by patches of alopecia (hair loss). The hair loses pigment and may break off. The papules become pustules, which progress to red scales. There are areas of circular balding.
Diagnosis is made by history and appearance. Some strains of tinea capitis glow green under a Wood’s light. This condition is treated with griseofulvin (Fulvicin, Grisactin), which is administered by mouth. It is given with or after meals to avoid gastrointestinal irritation and increase absorption. Suspensions should be well shaken. Parents are instructed to continue therapy as long as ordered and not to miss a dose. Exposure to the sun is avoided. Treatment may be necessary for 8 to 12 weeks. Children may go to school but are warned not to exchange hats, combs, or other personal items. Selenium sulfide shampoos are also used. This infection can be stubborn and may take several weeks to clear.
Tinea corporis: Tinea corporis (“ringworm of the skin”) is evident as an oval scaly inflamed ring with a clear center. It is seen on the face, neck, arms, and hands (Figure 30-13). It can be transmitted by infected pets. Treatment consists of local application of an antifungal preparation such as haloprogin twice daily for 2 to 4 weeks. More severe cases may necessitate treatment with oral griseofulvin.

Tinea pedis: Tinea pedis refers to athlete’s foot. Lesions are located between the toes, on the instep, and on the soles. There is accompanying pruritus. It occurs more often in preadolescents and adolescents. It is diagnosed by direct microscopic scrapings of the lesions. Treatment consists of topical therapy with an antifungal preparation. Oral griseofulvin therapy may also be given. Adolescents are cautioned to avoid alcohol consumption when taking this medicine because it may produce tachycardia and flushing.
Because this condition is aggravated by heat and moisture, the feet must be carefully dried, especially between the toes. Clean socks are worn. Shoes need to be well ventilated. Plastic shoes that retain heat are avoided. Recurrences are common.
Tinea cruris: Tinea cruris (“thigh”) affects the groin area and is commonly referred to as “jock itch.” It occurs on the inner aspects of the thighs and scrotum. The initial lesion is small, raised, and scaly. It spreads, and tiny vesicles occur at the margins of the rash. Local application of tolnaftate liquid (Tinactin, Aftate) or powder is effective. Spray solutions may cause stinging. General hygiene should be stressed.
Pediculosis
The infestation of humans by lice is termed pediculosis. There are three types: pediculosis capitis (head lice), pediculosis corporis (body lice), and pediculosis pubis (crabs or pubic lice). The various types usually remain in the part of the body designated by their name. They are transmitted from person to person or by contact with contaminated articles. Their survival depends on the blood they extract from the infected person. Severe itching in the affected area is the main symptom. In all cases, treatment is aimed at ridding the patient of the parasite, treating the excoriated skin, and preventing the infestation of others. The most common form seen in children is head lice (Figure 30-14).

Pathophysiology: Pediculosis capitis, which is commonly known as head lice, affects the scalp and hair. The louse lays eggs (nits) that attach to the hair and hatch within 3 or 4 days. Head lice are more common in girls than in boys because of hair length and the tendency to share combs and hair ornaments. The parasite may be acquired from hats, combs, or hairbrushes. It is easily transferred from one child to another and is seen most often in the school-age child and in preschool children who attend day care centers.
Manifestations: Children with pediculosis capitis suffer from severe itching of the scalp. They scratch their heads frequently and often cause further irritation. The hair becomes matted. Pustules and excoriations may be seen about the face. Nurses admitting patients to pediatric units should be on the alert for head lice. In particular, the nurse inspects the hairline at the back of the neck and about the ears. Crusts, pediculi, nits, and dirt may cause matting of the hair and a foul odor. When the condition is discovered, it is handled with discretion so as not to embarrass the child or parents.
Treatment and nursing care: Treatment is directed toward killing the lice, getting rid of the nits, and managing any infections of the face and scalp. Family members and playmates of the child should be examined and treated as necessary. Shampoos such as Nix are commonly used. Retreatment may be necessary in 1 week to 10 days. Lindane (Kwell) has also been used; however, it has more reported neurotoxic side effects (consult package insert).
If the eyebrows and eyelashes are involved, a thick coating of petroleum jelly (Vaseline) may be applied, followed by removal of the remaining nits. Nits on the head are removed by combing the hair with a fine-toothed comb dipped in a 1 : 1 solution of white vinegar and water. The hair is then washed. In some cases, recovery is hastened by cutting the hair. Transmission-based contact isolation precautions should be followed.
Children should be cautioned against swapping caps, head scarves, and combs. Parents are instructed to inspect the child’s head regularly. Parents are encouraged to report infestations to the school nurse, because widespread outbreaks are periodically encountered.
Scabies
Pathophysiology: Scabies is a parasitic infection caused by the itch mite, Sarcoptes scabiei. It is seen worldwide. It is caused by the adult female mite, who burrows under the skin and lays eggs. The mite has a round body and four pairs of legs and is visible by microscopic examination. A characteristic burrow is sometimes seen under the skin, particularly between the fingers. Burrows contain the eggs and feces of the mite. Itching is intense, especially at night. A vesiculopustular lesion can occur in children.
Scabies may occur anywhere on the body but is seldom seen on the face. It thrives in moist body folds, but in young children the lesions may appear on the head, the palms, and the soles of the feet. It is spread by close personal contact, including sexual relations. It is rarely transmitted by fomites because the isolated mite dies within 2 to 3 days (see Chapter 32).
Treatment and Nursing Care: Treatment consists of the application of permethrin (Elimite). It can be used for children older than 2 months of age. Parents are instructed to follow the directions carefully. All family members, baby-sitters, and close associates require treatment. Transmission-based contact isolation precautions are followed (see Appendix A).
Injuries
Pathophysiology: Burns often occur during childhood. They are the leading cause of accidental death in the home for children between 1 and 4 years of age. Sometimes burns are a result of child abuse and neglect. The two times of day during which burns are most likely to occur are the early morning hours before parents awaken and after school. There are several types of burns:
• Thermal: due to fire or a scalding vapor or liquid
• Chemical: due to a corrosive powder or liquid
• Electrical: due to electrical current passing through the body
Burns can involve the skin or mucous membranes. When a child is burned by fire near the face, the flames may be inhaled, causing a burn of the mucous membrane lining the airway. Assessing for resulting edema and respiratory distress is a priority. When a formula or food is heated in the microwave oven, “hot spots” occur that can cause burns to the mucous membranes lining the mouth.
The differences in responses of children to a burn are as follows:
• The child’s skin is thinner than that of the adult, leading to a more serious depth of burn with lower temperatures and shorter exposure than with adults.
• The large body surface area of the child results in greater fluid, electrolyte, and heat loss.
• Immature response systems in young children can cause shock and heart failure.
• The increased basal metabolic rate (BMR) of a child results in increased protein and calorie needs.
• Less muscle and fat in the body results in protein and caloric deficiencies when oral intake is limited.
• The skin is more elastic in children, causing pulling on the scarring areas and resulting in formation of a larger scar.
• The immature immune system predisposes the child to developing infections that complicate burn treatment.
• The prolonged immobilization and treatment required for burns adversely affects growth and development.
 Safety Alert!
Safety Alert!Classification: The severity of a burn depends on the area, extent, and depth of involvement. The size of the burn is calculated as a percentage of total body surface area (TBSA). Age-related charts are used for children, because their body proportions differ from those of adults and a standard (rule of nines) cannot be applied (Figure 30-15). The terms partial thickness and full thickness describe the extent of destruction of the skin. In partial-thickness burns, only some of the skin layers are damaged. Full-thickness burns are deeper and more extensive and may necessitate skin grafting. The classification of and first aid treatment for burns are summarized in Table 30-2. One can survive a rather extensive superficial burn, whereas a deep burn involving a smaller surface area can threaten the patient’s life. Table 30-3 discusses children’s response to burn injuries.
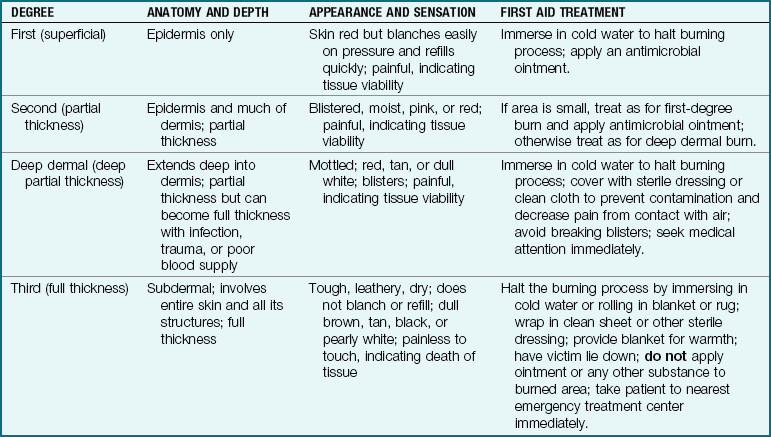
Table 30-3
Response to Burn Injury in Children*
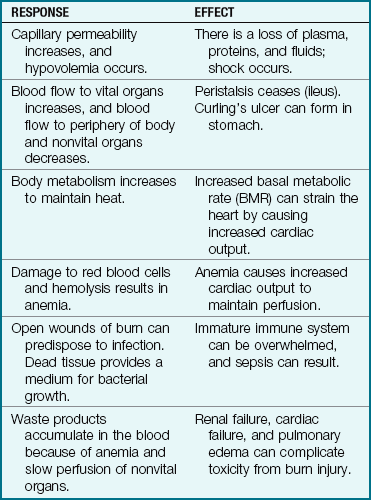
*Thermal injuries produce both local and systemic effects.
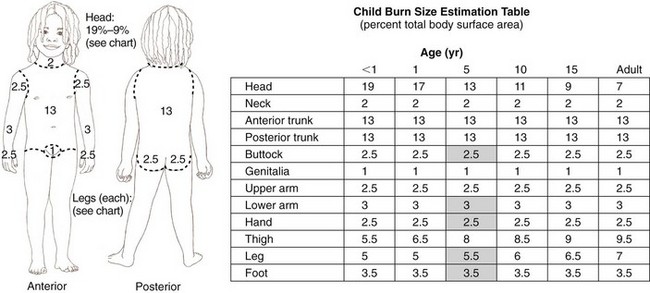
FIGURE 30-15 Body surface area (BSA) charts. This chart is used to determine the developmentally related percentage of body surface area burned. The percent of BSA involved is the basis for determining the fluid and nutritional needs of the burned child. In children younger than 3 years of age, the “rule of nines” assigns the infant’s head as 18% of total BSA (TBSA) and the lower extremities as 14% TBSA, with 9% assigned to each arm and  to the hands or palms. This chart is also referred to as the Lund Bower chart.
to the hands or palms. This chart is also referred to as the Lund Bower chart.
Burns can also be complicated by fractures, soft tissue injury, or preexisting conditions such as diabetes, obesity, epilepsy, and heart or renal disease. Moderate burns are considered to be (1) partial-thickness burns involving 15% to 30% of body surface, or (2) full-thickness burns involving less than 10% of body surface. Major burns are (1) partial-thickness types involving 30% or more of body surface or (2) full-thickness burns involving 10% or more of body surface. Partial-thickness and full-thickness burns must be regarded as open wounds that have the added danger of infection. The “6 Cs” of burn care include clothing, cooling, cleaning, chemoprophylaxis, covering, and comforting or pain relief (Herndon, 2007). Burn treatment can be given in an outpatient clinic, in a general hospital, or at a specialized burn center.
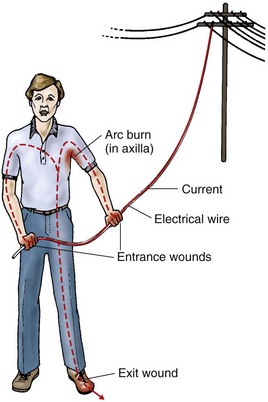
Care of electrical burns: When electricity is the cause of the injury, the child should be assessed for entry and exit lesions that may appear as a small erythematous area. The locations of the entry and exit wounds indicate the path of electricity through the body (Figure 30-16). Muscle damage can occur, and if the electrical current passes through the heart, cardiac muscle damage can result. Deep muscle damage can cause renal impairment from myoglobinuria. The child should be observed closely for responses with electrocardiography (ECG) monitors, the recording of vital signs, and assessment of cardiac enzymes before discharge.
Emergency care: Community education programs emphasize the response to a child with a burn injury. The school nurse plays a major role in the education process, as follows:
• Stop the burning process. Stop, drop, and roll is the sequence of care. Rolling the child in a blanket smothers the flames. A caustic powder should be brushed off before water is used to wash the area; this prevents spreading the caustic substance and enlarging the area of contact. Electricity should be turned off before touching a child who has been electrocuted.
• Evaluate the injury. Check the “ABCs” (airway, breathing, circulation) of the victim. Cardiopulmonary resuscitation (CPR) is initiated as appropriate. Minor burns can be treated; major burns should be assessed by a physician.
• Cover the burn. The burned area should be covered with a clean cloth to minimize contact with air, reduce pain, minimize hypothermia, and prevent contamination of the wound. Burned clothing and jewelry should be removed, because metal retains heat and continues the burn injury.
• Transport to a hospital. Do not give any fluids by mouth, because peristalsis may have diminished in response to the burn injury. If available, IV fluids and oxygen should be administered and the child comforted and reassured.
Care of minor thermal burns: Minor burns are treated at home and followed with clinic visits until healing is complete. The wound is cleansed and an antimicrobial ointment applied with a loose dressing. Blisters are not disturbed unless it was a chemical burn. Dressings are changed as prescribed, and the parent is advised to report any sign of infection. The status of tetanus immunization is reviewed and updated as needed. Pain relief is administered as needed. The wound of a minor burn is usually completely healed within 20 days. Evaluation of scarring and effect on range of motion (ROM) will determine future follow-up needs.
Care of major burns: The immediate treatment of shock in cases of severe burns is handled by the physician, nurse, and respiratory therapist and other specialists in the emergency department or, in some instances, the operating room. Priorities include establishing an airway in patients with facial burns or smoke inhalation, instituting IV lines, and assessing burn wounds and other, perhaps initially unrecognized, injuries. At times, some of these procedures are carried out simultaneously.
Establishing an airway: Cyanosis, singed nasal hairs, charred lips, and stridor are indications that flames may have been inhaled. An endotracheal tube is inserted to maintain an adequate airway, although this is not required for all patients. This permits the delivery of humidified air with oxygen, easy removal of secretions from respiratory passages, and use of a pressure ventilator if needed. Sedation is administered with caution to prevent further respiratory inhibition.
If eschar (eschara, “scab”) from burns on the trunk inhibits respirations, an incision called an escharotomy is made to prevent the restriction of chest movement. Blood gas levels, including level of carbon monoxide, are ascertained. The child is placed on sterile sheets. Attendants wear a face mask, sterile gown, and gloves.
IV infusions are begun to prevent intravascular dehydration and electrolyte imbalance. Ringer’s lactate solution is often used initially. Albumin or plasma may be used when capillary permeability is restored (within 24 to 48 hours).
Laboratory studies include hematocrit and sodium chloride, potassium, carbon dioxide, blood urea nitrogen, creatinine, and serum protein levels. Blood typing and cross-matching are performed. Fluid therapy requires close monitoring throughout hospitalization. To determine urine volume and characteristics, a urinary catheter is inserted and an intake and output record is maintained.
The loss of fluid causes renal vasoconstriction, leading to depressed glomerular filtration and oliguria. Acute renal failure can develop without adequate therapy. Urine output is observed hourly. It varies considerably, but on the average 20 to 30 mL/hr for patients older than age 2 years is considered adequate during the resuscitative stage. The patient’s weight is recorded and used as baseline data for determining adequacy of ongoing treatment.
A nasogastric tube is inserted and is attached to low wall suction. This empties the stomach and prevents complications such as gastric dilation, vomiting, and paralytic ileus (intestinal muscle paralysis). The patient has nothing by mouth for the first 24 hours. Sporadic bleeding as a result of Curling’s ulcer (stress ulcer) is not uncommon in patients with severe burns; the administration of IV antacids such as cimetidine has helped to reduce its incidence.
Wound care: Cleaning a burn wound can be painful, and measures for pain relief should be taken. Chlorhexidine (Hibiclens) and povidone-iodine (Betadine) can inhibit the healing process and are not advised for use on open burn wounds. Mild soap and water with thorough rinsing is preferred. Residual crusts can be removed with mineral oil or daily applications of Polysporin (polymixin and bacitracin) topical cream. The black eschar of necrotic tissue can be debrided via whirlpool. Yellow eschar is not removed.
Immediate care of the wound itself includes cleansing and debridement (removal of dried crusts) of necrotic tissue. The loss of skin increases the threat of infection, and fluid loss caused by evaporation can be significant. The immune system is depressed. Strict asepsis is maintained, and the wound site is treated in accordance with the physician’s instruction. A tetanus immunization history is obtained, and tetanus prophylaxis is administered as required. Low doses of antibiotics may be prescribed to prevent streptococcal infection.
A semiopen method of burn dressing may be used, although exposure methods may be useful on accessible areas such as the face. The wound is covered by a few layers of sterile gauze that has been saturated with antibacterial ointment or cream. The gauze is held in place by elastic netting (Figure 30-17). When the wound is being dressed, no two burn surfaces should touch. A sterile blanket may be used to prevent chilling. The wound is cleansed by tub baths, or in many cases, whirlpool baths are used to soften necrotic areas and debride the wound. Surgical debridement is done when needed to cleanse the wound and prepare the new granulation tissue for grafting. The use of ointments such as Sulfamylon or Silvadene may be prescribed. A biological dressing or a synthetic dressing may be used to prevent fluid loss and promote healing. The burn area is closed and resurfaced by grafting.
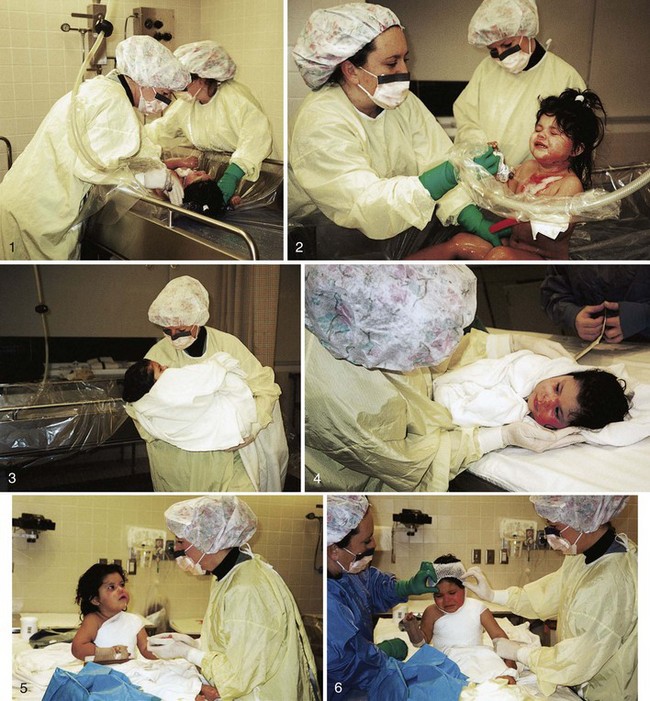
FIGURE 30-17 Collage of burn dressing change. This child is having her burn dressings changed and is undergoing whirlpool bath debridement. She is gently dried with sterile towels, and a pressure dressing is reapplied. (Photos courtesy Pat Spier, RN-C.)
Skin grafts: Temporary grafts are used during the acute stage of recovery. They protect the wound from infection and reduce fluid loss but are eventually rejected by the body. Temporary grafts include homografts (usually tissue from disease-free cadavers) and heterografts (tissues obtained from different species). Heterografts are also referred to as xenografts (xeno, “foreign,” and graft, “slice of skin”).
Many grafts are derived from pigskin, which is available commercially either fresh or frozen; these biological dressings are often used in children and are called porcine xenografts. They are particularly useful in partial-thickness or deep dermal burns and have greatly improved burn management. Deep dermal wounds may be preceded by tangential (merely touching) excision, which is a surgical technique of removing burned eschar with a dermatome. Thin layers are shaved down to the live tissues, and temporary porcine grafts are applied.
There are two types of permanent grafts: autografts and isografts. An autograft (auto, “self”) is healthy tissue obtained from another part of the patient’s body. An isograft (iso, “equal”) is obtained from the patient’s identical twin or genotype. Permanent grafts are done during the rehabilitative stage of the patient’s illness to improve appearance and function. The site from which the tissue has been removed is called the donor area.
Advances in grafting techniques have improved the overall prognosis in burn patients and have helped to minimize scarring. A split-thickness skin graft can be prepared with the use of a dermatome. For extensive burns, it is sometimes difficult to find enough intact skin for use. Special methods such as the Tanner mesh graft may be used. In this method a strip of split-thickness skin is run through a special cutting machine that makes multiple slits; this expands the skin to provide more coverage, in some cases as much as 9 times the original area of the skin. The graft is sutured in place to maintain tension.
The “postage stamp” graft consists of small pieces of donor skin placed on the granulation tissue. Spaces between grafts allow for drainage and healing. Full-cover grafts are sheets of skin placed intact over the wound. These are cosmetically more effective than patch and mesh grafts but are not always available. The donor site is covered with xenograft or fine mesh gauze; it heals in about 2 weeks. Newly grafted areas are covered with sterile dressings. Every effort is made to prevent bleeding and infection. The areas surrounding the wound are observed for edema and impaired circulation.
Biological dressings: Biological dressings can be applied to a noninfected burn wound within 6 hours of the injury and will peel off as the wound heals. Dressing changes are not necessary. The dressings are made from neonatal foreskin fibroblast cells combined in a nylon mesh that is sterile and frozen for storage. Once thawed, they cannot be refrozen. The dressings, Biobrane or TransCyte with bismuth-impregnated petrolatum gauze, contain human or pigskin products, and hypersensitivity should be considered before use. Elastic dressings may be used for a short time to hold it in contact with the wound, or a splint may be placed to immobilize an involved joint. TransCyte is transparent, so outer dressings can be removed to assess the wound. The dressing should be covered with a plastic bag before daily baths or showers are taken. The dressing may change color as the wound heals.
Posthealing care: After basic healing has occurred, a nonperfumed moisturizer cream such as Eucerin or Nivea, or cocoa butter, may be recommended to maintain skin moisture. Ointments containing lanolin are not advised. Sun block should be used to prevent hyperpigmentation of the newly healed skin. It may take 2 years for complete healing to occur. Systemic antihistamines such as diphenhydramine (Benadryl) or hydroxyzine (Atarax) may be prescribed to control itching. Bicarbonate of soda baths are soothing.
Nursing Care of the Burned Child: Children who have suffered extensive burns and survive the early dangers face a long period of hospitalization and require specialized care. The various aspects of nursing care differ with the age of the patient, the area of the burn, and the type of treatment used. Box 30-2 lists topical agents used in treating burn patients.
Protective isolation (expanded precautions) is instituted. All instruments that come in contact with the wound must be sterile. Ointments are applied with a sterile gloved hand or sterile tongue depressor. Care must be taken to prevent injury to granulation tissue. If the wound is to be covered, a layer of fine mesh gauze is secured with sterile fluffs, followed by Kling bandages and a stockinette or elastic tubular netting.
The nurse immediately reports signs of infection: elevations of temperature, pulse, and respiration; restlessness and confusion; pain; purulent drainage; and an odor emanating from the wound dressing. A careful description of the wound in the nurse’s notes facilitates daily comparison and determination of progress. All infection must be cleared before skin grafting can be performed.
The nurse remains alert for signs of fluid overload, in particular, behavioral changes and altered sensorium. Although initially restricted to prevent nausea and vomiting, oral fluids are necessary during the convalescent stages to prevent kidney damage and to maintain body fluid requirements. The nurse must use ingenuity to persuade the child to take sufficient amounts of fluids. An accurate record of intake and output of fluids is kept.
The demands on the metabolism as it deals with this trauma are increased, and more calories are spent as water evaporates from the wound site. Frequent feedings of foods high in calories, protein, and iron are therefore necessary. A high-protein diet—a normal diet with added amounts of meat, milk, eggs, fish, or poultry—is usually prescribed. Iron therapy may be initiated if anemia begins to develop. Eggnogs are nourishing between-meals drinks for burn patients with such needs. Small amounts are offered frequently. Vitamins A, B, and C and zinc sulfate are given to hasten healing and to stimulate the appetite. Gavage feedings may be necessary. Accurate daily records of foods consumed, calorie count, and patient’s weight will help to determine the nutritional status.
The nurse bears in mind that other, unaffected parts of the body need exercise and proper positioning to prevent painful contractures. The child’s position is changed every 2 to 4 hours unless contraindicated. A footboard is used to prevent foot drop. Support should be given by means of pillows, sandbags, and rolled towels as necessary.
The physical therapist attends to the child regularly for exercise and to keep the joints limber and healthy. The child begins to ambulate as soon as possible. Self-help activities and mobility are encouraged. Pressure splints or elasticized garments help to reduce scar tissue and are sometimes worn for months after discharge.
Emotional support: A burn injury is taxing to the child and parents. It requires long periods of hospitalization and frequent readmissions. The accident itself is terrifying for the child but is made even worse if caused by disobedience. Nurses encourage children to express their feelings. Analgesics are administered before painful procedures. The long-term patient requires diversions of various types. School tutors are requested, and contact is maintained with peers through cards or e-mail.
Nurses give constant support to the parents, who usually feel guilty if the child was injured in an accident. Nurses indicate by their manner that they do not blame the parents for what has happened. Preparation for discharge begins early. The multidisciplinary health care team includes the physician, the nurse, the school nurse, the schoolteacher, the physiotherapist, and the psychologist. Instructions are given regarding wound care, diet, exercise, and rest. Return appointments are made, and referral agencies are contacted. Methods to improve the physical appearance of the patient are discussed. The importance of burn prevention cannot be overemphasized. Figure 30-18 shows the difference in appearance of a scald burn wound from an accidental spill and a scald wound that was inflicted (child abuse).

Sunburn
Sunburn is a common skin injury caused by overexposure to the sun, especially at midday. Sunburn can be a minor epidermal burn or a more serious partial-thickness burn with blistering. Goals of treatment include stopping sun exposure, treating inflammation, and rehydrating the skin. Immersion in a tepid water bath (36.7° C [98° F]) for 15 to 20 minutes is the initial treatment. A bland oil-in-water moisturizing lotion can be applied. Education is the key to preventing sunburn. Covering the skin with clothing, wearing a hat, and using sun screen liberally is recommended. Two types of products are available. Topical sunscreen partially absorbs ultraviolet (UV) light, and sunblocks reflect sunlight. Zinc oxide and titanium dioxide are effective sunblocks. Sunscreens have a sun protection factor (SPF) rating to evaluate effectiveness at blocking the sun’s rays. If individuals normally burn in sun exposure after 10 minutes, use of an SPF 15 sunscreen will allow 10 × 15, or 150, minutes of sun exposure before burning occurs. Sunscreens with para-aminobenzoic acid (PABA) are very effective, but some children are sensitive or can have an allergic reaction. Sunscreens are not recommended for infants under 6 months of age. Small infants should be physically protected from excessive sun exposure.
Frostbite
Frostbite is the result of the freezing of a body part. Chilblain is a cold injury with erythema and the formation of vesicles and ulcerative lesions that occur as a result of vasoconstriction. Education to prevent cold injury is essential for those living in or visiting cold climates. School nurses play a vital role in educating parents and children. Adequate layered clothing, including hats and gloves (wool over cotton), is preferred.
In exposure to extreme cold, warmth is lost in the periphery of the body before the core temperature drops, and the extremities can suffer considerable damage before the onset of potentially fatal hypothermia. Therefore, in extreme cases of exposure to freezing temperatures, the head and the torso should be warmed before the extremities to ensure survival with minimal consequences. Frostbitten extremities appear pale and hard and are without sensation. Dry clothing should be applied and muscle activity encouraged. Blankets or sleeping bags are initially used to start rewarming. Warm, moist oxygen; warming blankets; and warming baths of 37.8° C to 42.2° C (100° F to 108° F) are used. A deep purple flush appears with the return of sensation, which is accompanied by extreme pain. Pain relief and monitoring of vital signs are essential. Blistering and ulcers can occur and are treated with whirlpool soaks. Skin damage is similar to that incurred with burns. Frostbite can result in necrosis (death) of tissue and may necessitate amputation of the extremity.
Get Ready for the NCLEX® Examination!
Key Points
• The skin is the body’s first line of defense against disease.
• Certain skin conditions are symptoms of systemic disease.
• Common skin problems in infants are diaper dermatitis, seborrheic dermatitis, and atopic dermatitis (eczema).
• A strawberry nevus is an example of a hemangioma.
• Pediculosis is the term for lice. Lice may occur on the head, body, or pubic area.
• Tinea pedis, or athlete’s foot, is prevented by drying the feet well, particularly between the toes, and wearing well-ventilated footwear.
• A severe burn can cause a loss of function in two of the most important properties of the skin: the ability to protect against infection and the ability to prevent the loss of body fluid.
• Electrical burns carry the risk of thrombosis and tissue damage in other parts of the body.
• The severity of a burn depends on the area, extent, and depth of involvement.
• Preventing infection is an important nursing intervention for patients with burns or any skin lesion.
• A sunburn can be a minor epidural burn or a partial-thickness burn with blisters.
• Topical sunscreens partially absorb the sun’s UV rays and have ratings to evaluate the effectiveness of blocking these rays. Sun blockers reflect sunlight.
• Frostbite can cause tissue damage similar to burns.
• Absorption of a topical hydrating medication is best when applied after a warm bath.
• Types of burns include thermal, electrical, chemical, and radiation.
Additional Learning Resources
 Go to your Study Guide for additional learning activities to help you master this chapter content.
Go to your Study Guide for additional learning activities to help you master this chapter content.
Go to your Evolve website (http://evolve.elsevier.com/Leifer) for the following FREE learning resources:
• Answer Guidelines for Critical Thinking Questions
• Answers and Rationales for Review Questions for the NCLEX® Examination
• Glossary with English and Spanish pronunciations
• Interactive Review Questions for the NCLEX® Examination
 Online Resources
Online Resources• American Academy of Dermatology: www.aad.org/index.html
• Burn awareness and prevention: www.shrinershq.org/Hospitals/BurnAwareness
Review Questions for the NCLEX® Examination
1. Why is pain relief important in the burn patient?
2. What would be contraindicated in a patient with infantile eczema?
1. Wrapping the infant in a wool blanket
2. Covering hands with cotton mittens
3. What is a characteristic sign of third-degree burns?
4. What is contained in an emollient bath often prescribed for children with eczema?
5. The cause of infantile eczema may be the basis of a teaching plan for the child’s parent. Infantile eczema is most likely caused by: