The Nurse’s Role in Women’s Health Care
1 Define each key term listed.
2 Explain aspects of preventive health care for women.
3 Describe each menstrual disorder and its care.
4 Explain each gynecological infection in terms of cause, transmission, treatment, and care.
5 Describe the various methods of birth control, including side effects and contraindications of each.
6 Describe how to use natural family planning methods for contraception or infertility management.
7 Describe possible causes and treatment of infertility.
8 Explain the changes that occur during the perimenopausal period and after menopause.
9 Explain the medical and nursing care of women who are nearing or have completed menopause.
10 Discuss the medical and nursing care of women with pelvic floor dysfunction or problems related to benign growths in the reproductive tract.
11 Describe the nursing care and treatment of a woman with leiomyoma.
 , p. 251)
, p. 251) , p. 272)
, p. 272) , p. 266)
, p. 266) , p. 251)
, p. 251) , p. 252)
, p. 252) , p. 252)
, p. 252) , p. 276)
, p. 276) , p. 272)
, p. 272) , p. 251)
, p. 251) , p. 251)
, p. 251) , p. 251)
, p. 251) , p. 269)
, p. 269) , p. 272)
, p. 272) , p. 259)
, p. 259) http://evolve.elsevier.com/Leifer
http://evolve.elsevier.com/Leifer
Today women from all ethnic backgrounds choose to be active participants in their health care and therefore need information about their bodies, health promotion, self-care techniques, and choices concerning treatment options. Culturally competent communication is the key to empowering the woman to feel confident about her ability to care for herself and her family. In some cultures, women ask when they want to know; in other cultures, women wait to be told what to do. To be an effective teacher about health behaviors, the nurse must understand the cultural needs, past experiences, and individual goals of the patient. The nurse offers support, knowledge, and caring behaviors that help the woman cope with screening tests or problems.
Goals of Healthy People 2020
Some Healthy People 2020 (U.S. Department of Health and Human Services [USDHHS), 2010) goals and strategies related to women’s health include the following:
• Increasing the number of women over the age of 40 who have mammograms to help curb the rise in breast cancer
• Increasing the number of women over the age of 18 who have Papanicolaou (Pap) tests to reduce the number of deaths from cervical cancer
• Reducing the occurrence of vertebral fractures in older women with osteoporosis
• Reducing the occurrence of sexually transmitted infections (STIs [formerly known as sexually transmitted diseases—STDs])
Achievement of these goals requires preventive care, screening, and increased accessibility to health care.
Preventive Health Care for Women
The goal of preventive health care, or health maintenance, is the prevention or early identification of disease. The value of preventive health care is that some disabling conditions can be prevented or their severity lessened by specific measures, such as altering the diet or detecting the disorder early and at a more treatable stage. Preventive care for women may include disorders with these characteristics:
• Exclusive to women, such as cervical cancer
• Dominant in women, such as breast cancer or osteoporosis
• Prevalent in the general population, such as hypertension or colorectal cancers
This chapter will focus on those disorders that are exclusive to or dominant in women. Much of preventive health care involves screening tests. These tests are not diagnostic but can identify whether additional testing is needed. Examples of screening tests that are common in women’s health care include mammography to identify breast cancer and Pap tests for cervical cancer.
 Nursing Tip
Nursing Tip
Encouraging women to practice preventive health care can help prevent some disorders or identify them early, when they are the most treatable.
Breast Care
Three approaches are needed for early detection of breast cancer:
The nurse’s role is to educate women about the benefit of all three examinations and techniques of self-examination. The reader should consult a medical-surgical text for additional information about the diagnosis and treatment of breast cancer.
Nursing Tip
Preventive care for breast health involves self-examination, professional examinations, and mammography at the appropriate ages.
Breast Self-Examination
Breast self-examination (BSE) should be performed by all women after age 20 years at about the same time each month. The best time for BSE is 1 week after the beginning of the menstrual period. If she is not menstruating, the woman may choose any day that is easy for her to remember, such as the first day of each month. Skill 11-1 describes how to teach a woman to perform BSE.
Skill 11-1 How to Perform Breast Self-Examination








To learn to know how the breasts feel and detect any changes
Note: Perform breast self-examination monthly. If you are menstruating, do the examination 1 week after the beginning of your period because your breasts are less tender at this time. If you are not menstruating, choose any day that you can easily remember, such as the first day of each month. Examine your breasts three ways: before a mirror, lying down, and in the shower.
1. Inspect your breasts in four steps:
2. At each step, note any change in the shape or appearance of your breasts.
3. Note skin or nipple changes such as dimpling of the skin.

1. Place a small pillow under your right shoulder and put your right hand under your head while you examine your right breast with your left hand.
2. Use the sensitive pads of your fingers to press gently into the breast tissue.

2. Use your soapy fingers to feel the breast tissue in the same systematic pattern described under “Lying Down.”

Contact the American Cancer Society at 1-800-ACS-2345, or visit the website at www.cancer.org.
The chief value of BSE is that a woman learns how her own breasts feel. This is particularly valuable if she has fibrocystic breast changes, in which there are often many lumps that may change with hormonal fluctuations. The woman who knows her own breasts is more likely to notice when something is different about them.
Professional Breast Examination
BSE is a supplement to, rather than a substitute for, regular professional examinations. Although the woman who does regular BSE knows what is usual for her own breasts, professionals have the training and experience to identify suspicious breast masses. It is part of every annual gynecological examination and is done more frequently for women who have a high risk for breast cancer. It is recommended at yearly intervals for all women over age 20 years. The professional examination is similar to that for BSE.
Mammography
Mammography uses very-low-dose x-rays to visualize the breast tissue. It can detect breast tumors very early—long before the woman or a professional can feel them. The breast is compressed firmly between two plates, which is briefly uncomfortable. Scheduling the mammogram after a menstrual period reduces the discomfort because the breasts are less tender at that time. The American Cancer Society (2007) currently recommends a mammogram every 1 to 2 years for all women age 40 years or over. Women at higher risk for breast cancer may begin mammography earlier.
Vulvar Self-Examination
Women over 18 years of age (or younger, if sexually active) should perform a monthly examination of the external genitalia to identify lesions or masses that may indicate infection or malignancy. The woman should use a hand mirror in a good light to systematically inspect and palpate her vulva and mons pubis for any new growths of any type, any painful or inflamed areas, ulcers, sores, or changes in skin color. She should report any abnormalities to her health care provider.
Pelvic Examination
The pelvic examination should be scheduled between menstrual periods, and the woman should not douche or have sexual intercourse for at least 48 hours before the examination to avoid altering the Pap test. The purpose of the pelvic examination is to identify conditions such as tumors, abnormal discharge, infections, or unusual pain.
The health care provider first checks the external genitalia to identify signs or problems similar to those noted in vulvar self-examination. Next, a speculum is inserted to visualize the woman’s cervix and vagina for inflammation, discharge, or lesions. The speculum is warmed and lubricated with warm water only. A Pap test is obtained to screen for changes in the vaginal and cervical tissues that may be precancerous. The current American Cancer Society recommendations (2009) for the Pap test are as follows:
• Yearly for all women age 18 years or older or whenever they become sexually active (whichever comes first)
• After three or more normal examinations, the Pap test may be performed less frequently at the health care provider’s discretion
After the Pap test is obtained, the health care provider will perform an internal, or bimanual, examination to evaluate the internal organs. The index and middle fingers of one hand are inserted into the vagina and the other hand is placed on the abdomen to permit palpation of the cervix, uterus, and ovaries between the fingers. After the internal examination, a single lubricated finger is inserted into the rectum to identify hemorrhoids or other lesions. A test for fecal occult blood may be done at this time (see a medical-surgical text for details).
Menstrual Disorders
Menstrual cycle disorders can cause many women distress. The nursing role in each depends on the disorder’s cause and treatment. Common nursing roles involve explaining any recommended treatments (e.g., medications) and caring for the woman before and after procedures. The nurse also provides emotional support to the patient.
Amenorrhea
Amenorrhea is the absence of menstruation. It is normal before menarche, during pregnancy, and after menopause. Amenorrhea that is not normal may fall into one of two categories:
1. Primary: failure to menstruate by age 16 years; failure to menstruate by age 14 years if she has not developed any secondary sex characteristics
2. Secondary: cessation of menstruation for at least three cycles or 6 months in a woman who previously had an established pattern of menstruation
Treatment of amenorrhea begins with a thorough history, physical examination, and laboratory examinations to identify the cause. Pregnancy testing is done for any sexually active woman.
The specific treatment depends on the cause that is identified. For example, women who are very thin or have a low percentage of body fat may have amenorrhea because fat is necessary for estrogen production. This group of women may include athletes but may also include patients who have eating disorders such as anorexia or bulimia. Therapy for their eating disorder may result in the resumption of normal periods. Other treatments are aimed at correcting the cause, which may be an endocrine imbalance.
Abnormal Uterine Bleeding
Abnormal uterine bleeding is (1) too frequent, (2) too long in duration, or (3) excessive in amount. Metrorrhagia is uterine bleeding that is usually normal in amount but occurs at irregular intervals. Menorrhagia refers to menstrual bleeding that is excessive in amount. The average woman loses about 35 mL of blood during normal menstruation. Blood loss greater than 80 mL/month is considered excessive and often results in anemia. Common causes for any type of abnormal bleeding include the following:
• Pregnancy complications, such as an unidentified pregnancy that is ending in spontaneous abortion
• Lesions of the vagina, cervix, or uterus (benign or malignant)
• Breakthrough bleeding (BTB) that may occur in the woman taking oral contraceptives
• Endocrine disorders such as hypothyroidism
• Failure to ovulate or respond appropriately to hormones secreted with ovulation (dysfunctional uterine bleeding)
Treatment of abnormal uterine bleeding depends on the identified cause. Pregnancy complications and benign or malignant lesions are treated appropriately. BTB may be relieved by a change in the oral contraceptive used. Abnormal hormone secretion is treated with the appropriate medications. Surgical dilation and evacuation (D&E [formerly known as dilation and curettage, or D&C]) may serve to remove intrauterine growths or aid in diagnosis. Hysterectomy may be done for some disorders if the woman does not want other children. A newer technique, laser ablation, can permanently remove the abnormally bleeding uterine lining without a hysterectomy. Menorrhagia can be treated with mefenamic acid (a nonsteroidal antiinflammatory drug, or NSAID) or tranexamic acid (an antifibrinolytic) if hormone therapy is contraindicated.
Menstrual Cycle Pain
Mittelschmerz (“middle pain”) is pain that many women experience around ovulation, near the middle of their menstrual cycle. Mild analgesics are usually sufficient to relieve this discomfort. The nurse can teach the woman that this discomfort, although annoying, is harmless.
Dysmenorrhea
Dysmenorrhea, painful menses or “cramps,” affects many women. It occurs soon after the onset of menses and is spasmodic in nature. Discomfort is in the lower abdomen and may radiate to the lower back or down the legs. Some women also have diarrhea, nausea, and vomiting. It is most common in young women who have not been pregnant (nulliparas).
There are two types of dysmenorrhea: primary, in which there is no evidence of pelvic abnormality, and secondary, in which a pathological condition is identifiable. Primary dysmenorrhea is a leading cause of short-term recurrent school absenteeism in adolescent girls in the United States. Characteristics include the following:
• Onset is shortly after menarche with heavy menstrual flow.
• Pain starts no more than a few hours before menstruation starts and lasts no more than 72 hours.
• Pelvic examination results are normal.
• Secondary dysmenorrhea most commonly results from endometriosis, the use of an intrauterine device (IUD) to prevent pregnancy, pelvic inflammatory disease, uterine polyps, or ovarian cysts. Treatment involves identifying and treating the cause.
Vasopressins and prostaglandins from the endometrium (uterine lining) play an important role in dysmenorrhea. Some women produce excessive amounts of prostaglandins from the endometrium, and these substances are potent stimulants of painful uterine contractions. Three treatments may provide relief:
1. Prostaglandin-inhibitor drugs, such as ibuprofen (Motrin, Advil) or naproxen (Naprosyn, Anaprox) (Prostaglandin inhibitors are most effective if taken before the onset of menstruation and cramps.)
2. Heat application to the lower abdomen or back
3. Oral contraceptives, which reduce the amount of endometrium built up each month and therefore reduce prostaglandin secretion
Low-fat and vegetarian diets reduce serum estrogen levels and can relieve menstrual pain in some women. Vitamins B and E, and the high level of omega-3 fatty acids in vegetarian diets influence prostaglandin metabolism and may have effects similar to antiinflammatory agents (French, 2005).
Endometriosis
Endometriosis is the presence of tissue that resembles endometrium outside the uterus. This tissue responds to hormonal stimulation just as the uterine lining does. The lesions may cause pain, pressure, and inflammation to adjacent organs as they build up and slough during menstrual cycles.
Endometriosis causes pain in many women that is either sharp or dull. It is more constant than the spasmodic pain of dysmenorrhea. Dyspareunia (painful sexual intercourse) may be present. Endometriosis appears to cause infertility in some women.
Treatment of endometriosis may be either medical or surgical. Medications such as danazol and agonists of gonadotropin-releasing hormone (GnRH) may be given via nasal spray to reduce the buildup of tissue by inducing an artificial menopause. The woman may have hot flashes and vaginal dryness, similar to symptoms occurring at natural menopause. She is also at increased risk for other problems that occur after menopause, such as osteoporosis and serum lipid changes. Surgical treatment includes the following:
Premenstrual Dysphoric Disorder
Formerly called premenstrual syndrome (PMS), premenstrual dysphoric disorder (PMDD) is associated with abnormal serotonin response to normal changes in the estrogen levels during the menstrual cycle. The following symptom criteria (which are used to diagnose PMDD) occur between ovulation and the onset of menstruation, begin to improve between the menstruation and ovulation phase, and are not present in the week after the menstrual period. Five or more of the following symptoms usually occur regularly:
• Anxiety, tension, feeling “on edge”
• Increased sensitivity to rejection
• Decreased interest in usual activities
• Change in appetite—food cravings
• Physical symptoms such as breast tenderness, bloating, weight gain, headaches
Treatment includes prescribing calcium, magnesium, and vitamin B6 (helps convert tryptophan to serotonin) and a diet rich in complex carbohydrates and fiber (to lengthen effects of the carbohydrate meal). Stress management and exercise are also advised. Medical management includes oral contraceptives (low-estrogen, progestin-dominant), diuretics during the luteal phase of the menstrual cycle (between ovulation and onset of menstruation), and NSAIDs to prevent headaches.
Serotonin reuptake inhibitors such as fluoxetine (Sarafem) may also be prescribed for negative behavior. Medroxyprogesterone (Depo-Provera) may be indicated to inhibit ovulation and thus control estrogen levels. Patient education concerning maintenance of a monthly calendar of symptoms, stress management, and dietary guidance are important nursing responsibilities. Although eating chocolate has been shown to elevate depressed moods, excessive consumption should be avoided.
The Normal Vagina
At birth the infant’s vaginal epithelium is controlled by estrogen from the mother and is rich in glycogen, with a low pH of 3.7 to 6.3. When the maternal estrogen effect decreases, the vaginal epithelium atrophies and contains little glycogen. The pH rises to 7. Estrogen influence returns at puberty, and glycogen increases. The interaction of glycogen and estrogen in the vaginal epithelium results in the growth of lactobacilli, which have bacteriostatic action. The pH falls to 3.5 to 4.5. The types of bacteria found in the vagina vary with the pH of the vagina. Factors that change the normal flora of the vagina and predispose to vaginal infection include the following:
• Antibiotics: Encourage yeast overgrowth
• Sexual intercourse: Raises pH to 7 or higher for 8 hours after coitus
• Uncontrolled diabetes mellitus: Increases glucose that promotes organism growth
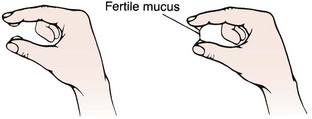
The normally acidic pH for the vagina is the first line of defense against vaginal infections. Normal vaginal secretions are made up of creamy white epithelial cells and mucus from the cervix, Skene’s glands, and Bartholin’s glands. The secretions prevent dryness and infection. Immediately after menstruation the mucus is thin, but as ovulation approaches, the estrogen level increases; at ovulation, the mucus is clear and slippery and can be stretched without breaking (spinnbarkeit) (see Figure 11-2). After ovulation the mucus is cloudy and sticky. At menopause, lowered estrogen causes vaginal dryness and the pH may change, predisposing the woman to vaginal discomfort and infections. Other factors can alter the pH of the vagina temporarily and include the following:
 Health Promotion
Health Promotion
Preventing Vaginal Infections
By promoting vaginal health, nurses can enhance the quality of life for the women they counsel. The promotion of vaginal health includes wearing cotton underwear, avoiding tight-fitting nylon or spandex pants, wiping front to back after toileting, and frequent handwashing. A healthy lifestyle with a high-fiber, low-fat diet, and exercise strengthens the immune system and can prevent many infections. Douching increases the risk for vaginal infections. Women should not douche or use internal feminine hygiene products without first consulting with their health care provider.
Gynecological Infections
Vaginal infections are the most common reason for women to seek health care. Nurses play a key role in educating women concerning vaginal health and the prevention of sexually transmitted infections. Identifying high-risk behavior and providing nonjudgmental, sensitive counseling and education should be part of every physical checkup. Safe sex practices, the reduction of the number of partners, and avoiding the exchange of body fluids are part of primary prevention of STIs. Community-based education in schools and churches is also important in primary prevention.
There are three classes of gynecological infections:
Toxic Shock Syndrome
Toxic shock syndrome (TSS) is a rare and potentially fatal disorder. It is caused by strains of Staphylococcus aureus that produce toxins that can cause shock, coagulation defects, and tissue damage if they enter the bloodstream. TSS is associated with the trapping of bacteria within the reproductive tract for a prolonged time. Factors that increase the risk of TSS include the use of high-absorbency tampons and the use of a diaphragm or cervical cap for contraception. Signs and symptoms of TSS include the following:
• Generalized rash that resembles sunburn
• Skin peeling from the palms and soles 1 to 2 weeks after the illness
The incidence of TSS has decreased, but nurses continue to play a role in prevention. The nurse’s role is primarily one of education. The following teaching points should be included:
Sexually Transmitted Infections
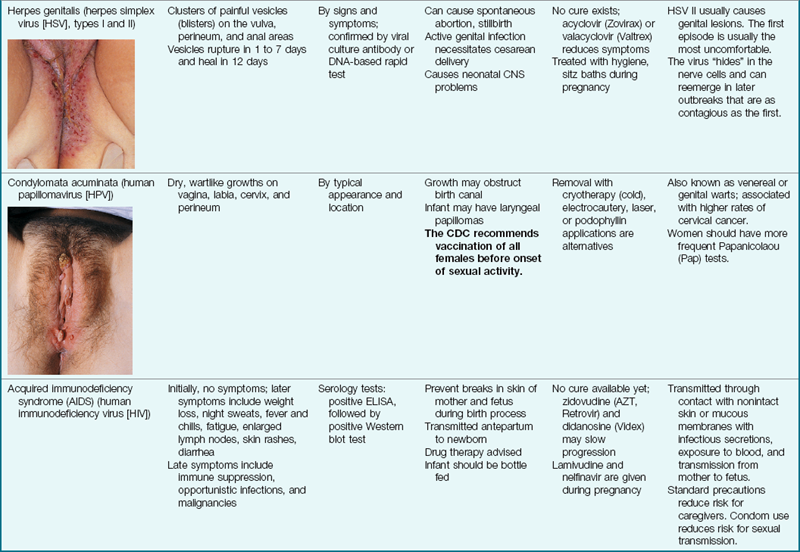
STIs are those that can be spread by sexual contact, although several of these have other modes of transmission as well. It is important that all sexual contacts, even those who are asymptomatic, be completely treated to eradicate the infection. Table 11-1 gives specific information about STIs that the nurse may encounter. Certain STIs must be reported to the health department.
Table 11-1
Sexually Transmitted Infections
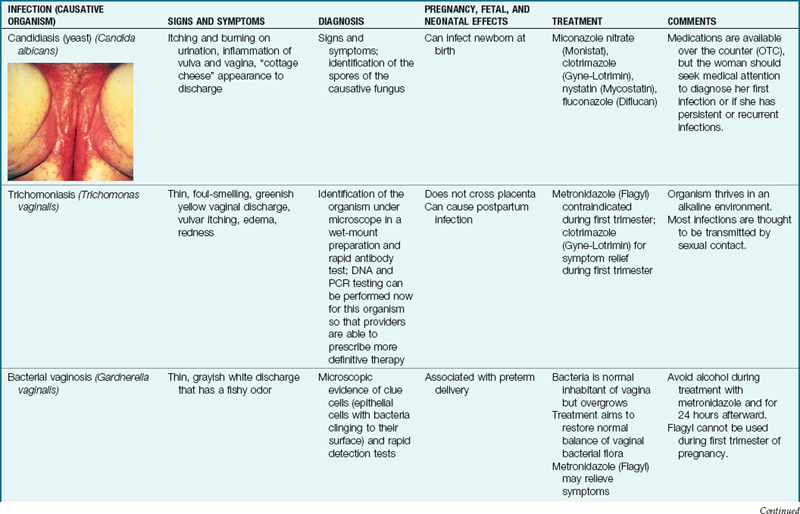
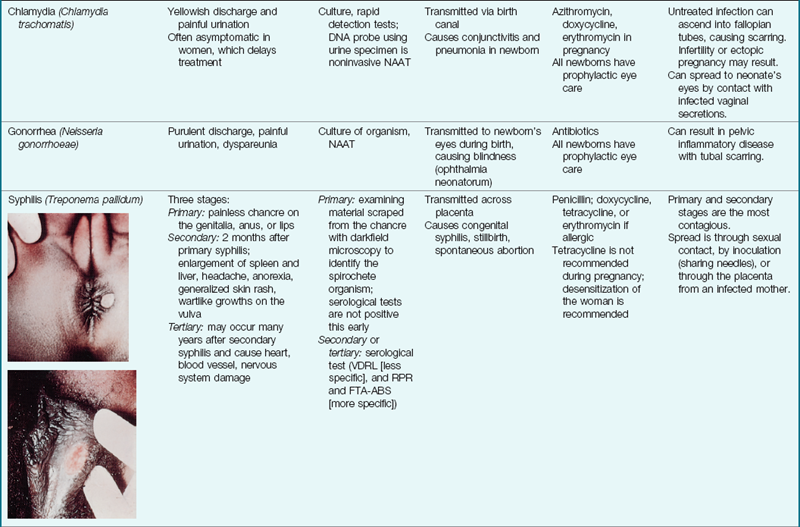
CNS, Central nervous system; ELISA, enzyme-linked immunosorbent assay; FTA-ABS, fluorescent treponemal antibody absorption; NAAT, nucleic acid amplification test; RPR, rapid plasma reagin; VDRL, Venereal Disease Research Laboratory.
Nursing care related to STIs primarily focuses on patient education to prevent spread of these infections, including the following:
• Teaching signs and symptoms that should be reported to the health care provider
• Teaching measures to prevent spread of infection, such as use of a condom
• Explaining treatment measures
• Emphasizing the importance of completing treatment and follow-up and of treating all partners to eliminate the spread of infection
The incidence of STIs has increased over the past few decades. Teaching STI prevention to women across the life span is important because some viral STIs remain in the body for life and can have long-term complications. The most common viral STI is human papillomavirus (HPV), with more than 100 variations. HPV types 16 and 18 are associated with serious cervical cancer, and women who are immunocompromised are at the greatest risk. The use of condoms may not protect the woman if the male’s lesion is on the scrotum or inguinal folds. It may take 3 to 6 months after infection to develop visible warts. Treatment includes cryotherapy, laser vaporization, electrodiathermy, and electrofulguration with a loop electrode excision procedure. Topical agents are used, such as podofilox (Condylox), imiquimod (Aldara), and bichloroacetic acid (BCA). Lidocaine cream may be used 20 minutes before painful treatments. 5-Fluorouracil (5-FU) is no longer used for this condition because of serious side effects.
Herpes simplex virus II (HSV II) is another example of a viral STI that is recurrent and incurable. HSV infection during pregnancy can have serious consequences for the newborn.
Hepatitis B can be sexually transmitted if sexual practices include anal-oral sexual contact, digital rectal sexual intercourse, or multiple sex partners. Symptoms are nonspecific and include malaise, anorexia, nausea, and fatigue. Liver failure can develop. Hepatitis B vaccine can prevent the disease, and immunoglobulin can be given if known exposure has occurred.
Chlamydia trachomatis is the most common bacterial STI in the United States (Centers for Disease Control and Prevention [CDC], 2008). Treatment tends to be delayed because infection is often asymptomatic.
Gonorrhea (GC) is the second most common reportable infectious disease in the United States and a major cause of pelvic inflammatory disease (PID). The occurrence of gonorrhea in 2007 declined except for an increase of 1.8% in the black population. Casual sex in the 15- to 19-year age-group and sex associated with drug use are the highest-risk practices for GC infection (CDC, 2008). Several nucleic acid amplification tests are now available to detect chlamydia, GC, and trichomonas with a simple noninvasive urine sample, with results available in a few hours. Fluoroquinolones are no longer recommended for treatment of GC infections (CDC, 2008).
The rate of syphilis reached an all time low in 2000. However, over the past 7 years the rate has been increasing. Between 2006 and 2007, a 15.2% increase in the diagnosis of syphilis has been noted (CDC, 2008). Untreated syphilis is a risk factor in the spread of human immunodeficiency virus (HIV) infection and also leads to central nervous system (CNS), musculoskeletal, and heart complications. Most newborns of mothers infected with syphilis will have congenital syphilis or die. An external chancre is a characteristic first sign and resolves within 6 weeks without treatment; however, the disease spreads internally. A rash also occurs and resolves, and then the latent period of syphilis occurs and progresses to tertiary syphilis. Aortic aneurysms, dementia, and death can occur.
The number of women infected with HIV worldwide is staggering. Patient education plays a key role in prevention, quality of life, and compassionate and knowledgeable referral. Early diagnosis, access to care, medications, and safe sex practices are improving outcomes and decreasing occurrence. Universal HIV screening at pregnancy is a goal of the National Academy of Sciences Institute of Medicine, because many women do not realize they are infected in the early stages. Education for prevention is essential. Nurses may be less likely to consider the older age-group at risk and may miss opportunities for early detection and education for prevention. Sexual contact and intravenous (IV) drug use are the most common risk behaviors for HIV infection.
Prevention of disease is the key role of the nurse. The nurse must develop strategies, use initiatives, and contact adolescents in the community setting, schools, and churches. Teaching all age-groups healthy behaviors such as abstinence, safe sex practices, and discussion of STI prevention is essential. Improving access to care and early detection is also important. The CDC offers various free programs that are available over the Internet and can be used by nurses and teachers in the community to teach STI prevention.
Pelvic Inflammatory Disease
Pelvic inflammatory disease (PID) is an infection of the upper reproductive tract. Asymptomatic STIs are a common cause of PID. The cervix, uterine cavity, fallopian tubes, and pelvic cavity are often involved. Infertility may be the result.
The woman’s symptoms vary according to the area affected. Fever, pelvic pain, abnormal vaginal discharge, nausea and anorexia, and irregular vaginal bleeding are common. When examined, the abdomen and pelvic organs are often very tender. Laboratory tests identify common general signs of infection, such as elevated leukocytes and an elevated sedimentation rate. Cultures of the cervical canal are done to identify the infecting organism. Urinalysis is usually done to identify infection of the urinary tract.
Treatment may be administered on an inpatient or outpatient basis depending on the severity of the infection. Antibiotics are begun promptly to treat the infection. A change in antibiotic(s) is made if culture and sensitivity testing indicates that another one would be more effective.
Douching results in changes in the vaginal flora and predisposes the woman to the development of PID, bacterial vaginosis, and ectopic pregnancies. However, many women practice regular douching in the belief that it is cleansing. The nurse can play an important role in educating the woman to prevent PID. A diagnosis of PID is reportable to the local health department in many states.
Family Planning
Contraception (birth control) may be part of the nurse’s responsibility in family-planning clinics, in physician or nurse-midwife practices, or on the postpartum or gynecology units of an acute care hospital. In addition, family members and friends may turn to the nurse as a resource person who can answer their questions about contraception. The nurse can play a part in helping couples choose and correctly use contraceptive methods that enable them to have children who are both wanted and well timed. The nurse’s role in family planning includes the following:
• Answering general questions about contraceptive methods
• Explaining different methods that are available, including accurate information about their advantages and disadvantages
• Teaching the correct use of the method or methods of contraception that the patient chooses
A couple’s choice of contraception often changes as needs change. Factors that influence the choice of a contraceptive include the following:
• Health status, including risk for STI
• Impact of an unplanned pregnancy on the woman or family
• Convenience and degree of spontaneity that is important to the couple
• Degree of comfort the partners have with touching their bodies
Contraception does not always prevent pregnancy. An important consideration for patients is how likely the method is to fail. A contraceptive technique may fail because the method is ineffective or the user is using the method inappropriately. The following two Healthy People 2020 (USDHHS, 2010) goals are relevant to the provision of family planning services:
Natural Family Planning
Natural family planning, also called fertility awareness, involves learning to identify the signs and symptoms associated with ovulation. The couple either abstains from intercourse or uses a barrier method during the period that is presumed to be fertile. The ovum is viable up to 24 hours after ovulation, and sperm are viable for 48 to 72 hours in the fallopian tube, although most die within 24 hours.
Natural family planning methods are acceptable to most religions. They require no administration of systemic hormones or insertion of devices. They are not only reversible but also can actually be used to increase the odds of achieving pregnancy when the couple desires a child.
Natural family planning requires extensive assessment and charting of all the changes in the menstrual cycle. The woman must be highly motivated to track the many factors that identify ovulation. Both partners must be willing to abstain from intercourse for much of the woman’s cycle if the method is used to prevent pregnancy. They must also be willing to accept the relatively high failure rate of 20%. Most women use a combination of the following four methods for predicting when they are fertile to increase the predictive value over that of each method on its own.
Basal Body Temperature
The basal body temperature (BBT) is taken upon awakening and before any activity (Figure 11-1). This technique is based on the fact that the basal temperature rises very slightly at ovulation (about 0.2° C [0.4° F]) and remains higher in the last half of the cycle. Unfortunately, BBT is better at identifying that ovulation has already occurred rather than predicting when it is about to occur. The most important time point to identify in attempting conception or contraception is the day before ovulation, rather than the day of ovulation (Fehring et al., 2008).
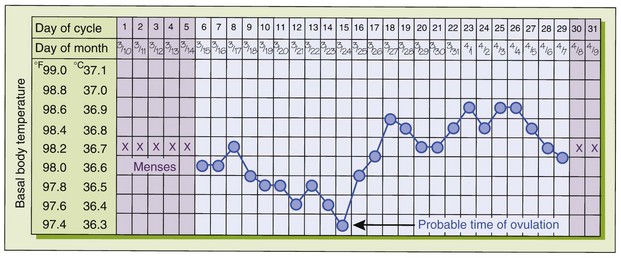
FIGURE 11-1 Basal body temperature chart. By taking and recording her temperature, the woman can determine the probable time of ovulation.
A basal thermometer is calibrated in tenths of a degree or uses an electronic digital format to detect these tiny changes. The woman charts each day’s temperature to identify her temperature pattern. A rise in the BBT for the last 14 days of the cycle means that ovulation has probably occurred. Some electronic models have a memory to retain each day’s temperature and display the pattern on a small screen.
Many factors can interfere with the accuracy of the BBT in predicting ovulation. Poor sleep, illness, jet lag, sleeping late, alcohol intake the evening before, or sleeping under an electric blanket or on a heated waterbed can make the BBT unreliable.
Cervical Mucus
The cervical mucus method of predicting ovulation is also called the Billings method. The character and amount of cervical mucus changes during the menstrual cycle since estrogen and progesterone influence the mucus-secreting glands of the cervix. Immediately after menstruation, the cervical mucus is sticky, thick, and white. As ovulation nears, the mucus increases and becomes thin, slippery, and clear to aid the passage of sperm into the cervix. The slippery mucus can be stretched 6 cm or more and has the consistency of egg white (Figure 11-2). The stretching characteristic of the mucus is called spinnbarkeit. After ovulation the mucus again becomes thicker. Factors that interfere with the accuracy of cervical mucus assessment include the use of antihistamines, vaginal infections, contraceptive foams or jellies, sexual arousal, and recent coitus. The noticeable changes in vaginal mucous before ovulation can aid in natural family planning and fertility awareness (Zinaman, 2009).
Calendar, or Rhythm, Method
The woman charts her menstrual cycles on a calendar for several months. If they are regular, she may be able to predict ovulation. The rhythm method is based on the fact that ovulation usually occurs about 14 days before the next menstrual period. This would be about halfway through a 28-day cycle, but would be on day 16 of a 30-day cycle.
Marquette Method
The Marquette method of natural family planning incorporates the use of an electronic hormonal fertility monitor that tracks changing of levels of a urinary metabolite of estrogen and luteinizing hormone (LH). It can be used in combination with other traditional methods such as BBT and cervical mucus to identify a 6-day fertile window that can be used to plan or help prevent pregnancy (Fehring, 2008).
Temporary Contraception
Reversible contraception is defined as the temporary prevention of fertility.
Abstinence
Abstinence is 100% effective in preventing pregnancy and STIs, including infection with HIV; however, most couples believe that their sexual relationship adds to the quality of life. Therefore abstinence is rarely an option the couple will consider. Most religious groups support abstinence among unmarried people and adolescents.
Hormonal Contraceptives
Hormonal contraceptives have one or more of the following contraceptive effects:
• Make the cervical mucus thick and resistant to sperm penetration
• Make the uterine endometrium less hospitable if a fertilized ovum does arrive
Hormonal contraceptives do not protect either partner from STIs, including HIV infection.
Oral Contraceptives (“The Pill”): Oral contraceptives (OCs) are a popular, highly effective, and reversible method of birth control (Figure 11-3). They contain either combined hormones (estrogen and progestin) or progestin alone (“minipill”).

FIGURE 11-3 Contraceptives. This photo shows common types of contraceptives: condoms, diaphragms, oral contraceptives, transdermal patch, and parenteral contraceptives.
Oral contraceptives require a prescription. The woman’s history is obtained, and she will have a physical examination, including breast and pelvic examinations and a Pap test. She should have a yearly physical examination, Pap test, breast examination, and blood pressure check. See Treatment Options on p. 273 regarding the use of oral contraceptives for treating menopause and menstrual irregularities.
Monthly contraception: Combination OCs are available in 21- or 28-pill packs. If the woman has a 21-pill pack, she takes one pill each day at the same time for 21 days, and then stops for 7 days. The woman who has a 28-day pack takes a pill each day; the last seven pills of the pack are inert but help her maintain the habit of taking the pill each day. Menstruation occurs during the 7-day period when either no pills or inert pills are ingested.
Some pills are multiphasic in that their estrogen and progestin content changes during the cycle to mimic natural hormonal activity. If the woman takes multiphasic pills, it is very important that she take each pill in order. Taking the pills at the same time each day is important, regardless of the type of OC, to maintain a stable blood level of the hormones.
It is most important that the medication-free interval not be extended beyond 7 days. Taking the first pill of the cycle on time is most critical in preventing accidental pregnancies.
Extended-dose contraception: Extended-dose contraception is also known as induced amenorrhea. Research has shown that there are no specific health benefits to monthly menstruation (Fontenot & Harris, 2008). Ethinyl-estradiol and norethindrone (Loestrin 24 Fe) contains 24 days of active hormone and 4 days of ferrous fumarate tablets instead of placebo pills. Drospirenone and ethinyl-estradiol (YAZ) also provides a 24-day regimen. Ethinyl-estradiol and levonorgestrel 30/150 (Seasonale) is an extended-cycle oral contraceptive. The woman takes the active hormone for 84 days and then the hormone-free placebo for 7 days, resulting in a menstrual period once every 3 months. There has been no evidence of adverse effects noted with the extended-dose regimen, and its failure rate is 0.9% compared to 1.3% with conventional (monthly) administration (Fontenot & Harris, 2008). Levonorgestrel and ethinyl-estradiol 90/20 (Lybrel), a continuous low-dose OC, was approved by the U.S. Food and Drug Administration (FDA) in 2007. There are no planned withdrawal bleeds, but some women report spotting or breakthrough bleeding about 3 days/month.
Benefits: OCs have a failure rate of 1.3% for combined pills and 0.5% for minipills. They reduce the risk for ovarian and endometrial cancer. Their effect on the risk for breast and cervical cancer risks is not yet definitively established. Women tend to have less cramping and lighter periods (and therefore less anemia) when taking OCs. OCs may improve premenstrual symptoms for some women. In some formulations, iron and folic acid supplementation has been added to the OC pill.
Side effects and contraindications: Common side effects of OCs include nausea, headache, breast tenderness, weight gain, and spotting between periods or amenorrhea. These effects generally decrease within a few months and are seen less frequently with low-dose OCs.
Women with the following disorders should not take OCs or should take them with caution:
• Thromboembolic disorders (blood clots)
• Cerebrovascular accident or heart disease
• Estrogen-dependent cancer or breast cancer
• A smoking pattern of more than 15 cigarettes a day for women older than age 35 years (the pill is safe for women over age 35 years if they do not smoke)
 Safety Alert
Safety Alert
Smoking increases the chance of experiencing complications related to oral contraceptives, particularly in women over age 35 years.
The first episode of menstrual bleeding after an abortion is usually preceded by ovulation, and therefore contraception should begin immediately to prevent pregnancy. However, after a term delivery there is a high risk of thromboembolism; therefore, the contraceptive is usually started 4 weeks postpartum.
The use of combination OCs also decreases breast milk production, and OC use is therefore contraindicated in the breastfeeding woman until lactation is well established. Women who breastfeed at least 10 times per day usually do not ovulate for 10 weeks postpartum, but breastfeeding is not a reliable method of contraception. Progestin-only OCs (minipill) may be used until menstruation returns in women who breastfeed regularly.
The newer extended-dose oral contraceptive, YAZ, has been used successfully to minimize the bloating, fluid retention, and symptoms of PMDD usually associated with oral contraceptives. Serum potassium levels should be monitored for women who take this medication with other medications known to increase serum potassium levels.
Some medications decrease the effectiveness of OCs, including the following:
 Memory Jogger
Memory JoggerNursing care: The woman needs thorough teaching if the pill is to be a satisfactory contraceptive for her. Teaching should be done in her own language, and supplemented by generous written materials if she can read. Teaching points should include the following:
• How to take the specific drug
• What to do if a dose is missed or if she decides to stop using it and does not want to become pregnant
• Common side effects and signs and symptoms that should be promptly reported
• Backup contraceptive methods, such as barrier methods (discussed later in this chapter)
• Supplemental barrier methods of contraception to use in addition to OCs, which also reduce the risk of STIs (including HIV infection)
Hormone Implants: Etonogestrel implant (Implanon), approved by the FDA in 2006, is a single-rod system that involves the placement of one implant under the skin of the upper, nondominant, arm that provides contraception for 3 years and does not affect bone mineral density (Fontenot & Harris, 2008). Implanon can be used during lactation, and when it is discontinued, the woman will have a rapid return to fertility. Intradermal implants can be removed in the outpatient clinic with the use of a local anesthetic.
Medroxyprogesterone acetate (Depo-SubQ Provera 104): Medroxyprogesterone acetate (Depo-SubQ Provera 104) is an injectable form of slow-release progestin. Its contraceptive action is similar to that of the minipill and hormone implant. It provides 3 months of highly effective contraception; therefore, it must be administered every 3 months. Fertility returns about 1 year after stopping the medication (Hacker, Gambone, & Hobel, 2010).
The injection is given subcutaneously within 5 days of the menstrual period. If given later than 5 days after the menstrual period, the woman should use another form of contraception as well, because ovulation may have already occurred. The breastfeeding woman usually starts hormone injections 6 weeks after birth, and the nonlactating woman may start 5 days after delivery. Depo-SubQ Provera 104 may result in decreased bone density and is not recommended for long-term use by teens; however, the decreased bone density is reversible (Fontenot & Harris, 2008).
Side effects and contraindications: The side effects and contraindications of hormone injections are similar to those of OCs and hormone implants. Menstrual irregularities, breakthrough bleeding, and amenorrhea are common complaints and are often the reason why women stop taking the drug.
Nursing care: The woman should be taught about the side effects and problems to report. It should be emphasized that she must return for continued injections if she wants to maintain a constant level of hormone and thus prevent pregnancy. A backup contraceptive method should be taught for use if she decides to stop the injections or is delayed in returning for subsequent injections. Women with seizure disorders can use this method of contraception without fear of interaction with their antiseizure medication. Women with coagulation problems or sickle cell anemia benefit from this type of contraception, which suppresses ovulation and reduces blood loss (Fontenot & Harris, 2008).
Intrauterine Devices: Intrauterine devices (IUDs) are a reversible method of birth control that requires a prescription and a health care provider to insert it. They are effective (98% or greater) and reversible, and no specific actions are required related to intercourse. The ParaGard is a small, T-shaped, copper-containing plastic device that is effective for 10 years. Other devices, such as Mirena, carry a sleeve on one segment that contains a reservoir of progesterone or levonorgestrel that is diffused into the uterus each day. The action is local in the uterine cavity, and blood levels do not increase. The levonorgestrel type of IUD (LNG-IUS) must be replaced every 5 years. The LNG-IUS is also used to control menorrhagia. The main mechanism of contraceptive action of a copper IUD is the production of a sterile inflammatory reaction that is spermicidal and toxic to the blastocyte. Copper impedes sperm transport and viability in the cervical mucus. On removal of the IUD, fertility rapidly returns. The IUD does not protect against STIs.
Side effects and contraindications: Cramping and bleeding are likely to occur with insertion. Insertion should not be done during menses. Increased menstruation and dysmenorrhea may occur and are common reasons why a woman decides to have the IUD removed. The woman who has heavier periods may need iron supplementation.
Nursing care: The woman is taught about side effects and how to take iron supplements if they are prescribed. The woman will need to feel for the fine plastic strings (tail) that are connected to the IUD to verify that it is in place. She should check the tail weekly for the first 4 weeks after insertion, then monthly. The woman is taught to report if she cannot feel the tail that protrudes into the vagina, or if it is longer or shorter than previously. The nurse can teach her the signs of infection (fever, pain, change in vaginal discharge) and the signs of ectopic pregnancy (see Chapter 5) that should be promptly reported.
Transdermal Patch: Ortho-Evra is a transdermal adhesive patch containing hormones (norelgestromin ethinyl-estradiol) that is applied to the skin once a week for 3 weeks, followed by a 1-week patch-free interval to allow for menstruation to occur. It provides effective contraception similar to oral contraceptives. The hormones contained in the Ortho-Evra patch are metabolized differently in the body than those contained in the oral pill and therefore may provide a higher hormone level than the label indicates. Studies concerning the effects on the health of the woman are ongoing (Ortho-McNeil-Janssen, 2009). The FDA warns that counterfeit contraceptive patches that may provide little or no protection against pregnancy have been sold on foreign websites.
Vaginal Ring: A flexible, one-size vaginal ring (NuvaRing) that releases estrogen and progestin locally instead of systemically has been approved for contraceptive use in the United States. The ring is worn in the vagina for 3 weeks and removed for 1 week to allow for withdrawal bleeding (Fontenot & Harris, 2008).
Barrier Methods
Barrier methods work by blocking the entrance of semen into the woman’s cervix. Spermicides (sperm-killing chemicals) play a part in some of these methods. They help the woman avoid the use of systemic hormones. Some barrier methods offer some protection against STIs by providing a barrier to contact.
Some barrier methods must be applied just before intercourse (condoms, spermicidal foams, and suppositories), whereas others can be inserted several hours earlier (diaphragm, cervical cap). Spermicidal foams and suppositories are messy and may drip from the vagina. These methods are not suitable for people who are uncomfortable touching their bodies. They are often used as a backup method of contraception.
Barrier methods are inexpensive per use. The diaphragm and cervical cap require a fitting and prescription, which adds to their initial cost. Other barrier methods are over-the-counter purchases. These methods are often chosen as backup methods or when the woman is lactating, or if she cannot tolerate OCs or an IUD.
Sponge: The Today sponge is a one-size, single use, non-prescription barrier sponge contraceptive that works by absorbing the semen and providing a barrier to the cervix and a spermicide. It has been approved for use in the United States.
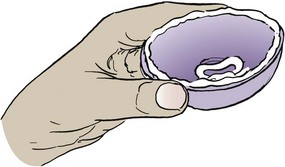
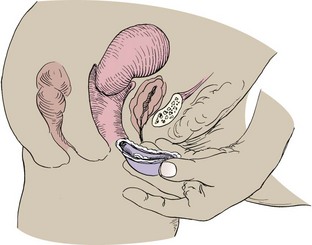
Diaphragm and Cervical Cap: Diaphragms and cervical caps are rubber domes that fit over the cervix and are used with spermicides to kill sperm that pass the mechanical barrier (Skill 11-2). The diaphragm and cervical cap are fitted by a health care provider. The woman must learn how to insert and remove the diaphragm or cervical cap and to verify proper placement. User misplacement, especially of the small cervical cap, is a common reason for unintended pregnancy.
Skill 11-2 How to Use a Diaphragm
To learn to use a diaphragm for contraception
Note: A diaphragm can be inserted up to 4 hours before intercourse. Skill of insertion and removal increases with practice.
1. Apply spermicidal cream or gel inside at center and around the rim of the diaphragm. This aids the insertion and offers a more complete seal.
2. Hold diaphragm between your thumb and finger and compress diaphragm. Use fingers of other hand to spread the labia (lips of the vagina).
3. Begin to insert diaphragm into vagina with spermicide toward the cervix. Squatting or placing one foot on a chair makes insertion (and removal) easier.
4. Insert diaphragm into vagina. Direct it inward and downward behind and below the cervix.
5. Tuck the front of the rim of diaphragm behind the pubic bone.
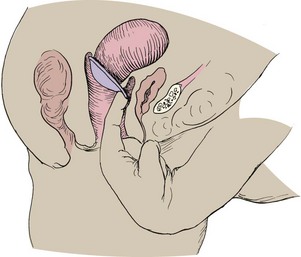
6. Feel your cervix through the center of the diaphragm.
7. Leave diaphragm in place at least 6 hours after intercourse.
8. To remove diaphragm, assume squatting position and bear down. Hook a finger over the top rim to break suction, and pull diaphragm down and out.
9. Wash diaphragm with mild soap and dry well after each use.
10. Dust diaphragm with cornstarch. Scented talc or baby powder can weaken the rubber.
11. Inspect it occasionally for small holes by holding it up to light.
The woman should check either device for weak spots or pinholes before insertion by holding it up to the light. Spermicidal jelly or cream is applied to the ring and the center of the diaphragm before inserting it and positioning it over the cervix. It may be inserted several hours before intercourse and should remain in place for at least 6 hours after intercourse, but not more than 24 hours to prevent pressure on local tissue. More spermicidal jelly or cream must be inserted into the vagina if the couple repeats coitus within 6 hours. The diaphragm must be refitted after each birth or a weight change of 10 pounds or more. The cap must be refitted yearly and after birth, abortion, or surgery.
The FemCAP is a latex-free cap that fits over the cervix and must be fitted, prescribed, and initially inserted by a health care provider. Spermicide can be added to the dome of the cap. Lea’s shield, a silicone reusable shield, is used with a spermicide and has been FDA approved since 2002.
Side effects and contraindications: Women who have an allergy to rubber or spermicides are not good candidates for the diaphragm or cervical cap. Pressure on the bladder may increase the risk of urinary tract infection.
Nursing care: The health care provider who fits the device will provide much of the teaching on insertion, verification of placement, and removal. The nurse often reinforces the teaching, especially about the use and reapplication of spermicide for repeat intercourse. The nurse should teach the woman about signs of uterine infection (pain, foul-smelling drainage, or fever) and of sensitivity to the product (irritation or itching). The woman also should be taught to report signs and symptoms of urinary tract infection: fever, pain or burning with urination, urgency, or urinary frequency.
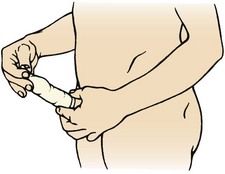
Male Condom: Male condoms are sheaths of thin latex, polyurethane, or natural membrane (“skins”) worn on the penis during intercourse. Condoms collect semen before, during, and after ejaculation. They come in various styles, such as ribbed, lubricated, and colored, and with or without spermicide. They are single-use, low-cost items that are widely available from vending machines, drugstores, and family planning clinics. Latex condoms provide some protection from STIs, including HIV. Natural membrane condoms do not prevent the passage of viruses, including HIV. See Skill 11-3 for the correct use of the condom.
Skill 11-3 How to Use the Male Condom
1. Use a new condom each time you have intercourse.
2. Check the expiration date on packages, because condoms deteriorate over time.
3. Apply the condom before you have any contact with the woman’s vagina, because there are sperm in the secretions before you ejaculate.
4. Squeeze the air from the tip when placing the condom over the end of your penis. Leave a half inch of space at the tip to allow sperm to collect and to prevent breakage.

5. Hold the tip while you unroll the condom over the erect penis.
6. Do not use petroleum jelly, grease, or oil as lubricants because they can cause the condom to burst. Instead, use a water-soluble lubricant such as K-Y Jelly.
7. Hold on to the condom at the base of the penis to prevent spillage as you withdraw from the vagina.

8. Remove the condom carefully to be sure that no semen spills from it.
9. Place the condom in the trash or in some safe disposal.

To prevent condom breakage, water-soluble lubricants should be used if the condom or vagina is dry. Unlike other, oil-based lubricants, water-soluble lubricants do not damage the latex or cause breakage. The penis should be withdrawn from the vagina immediately if the man feels that the condom is breaking or becoming dislodged. The condom is removed and a new one applied. Condoms are not reused because even a pinhole can lead to pregnancy or permit the entry of viruses, including HIV. The condom package should be checked for expiration date.
The nurse should educate patients to prevent common condom mistakes, including the following:
• Allowing the penis to lose erection while still in the vagina
• Opening the condom package with the teeth or a sharp object, which can tear the condom
• Unrolling the condom before applying it to the penis
• Using of out-of-date condoms (condoms with spermicide last for 2 years; others, 5 years)
• Using baby oil, cold cream, vegetable oil, or petroleum jelly to lubricate the condom
• Storing condoms in the wallet (heat destroys spermicide)
• Not leaving space between the tip of the penis and the condom to provide a reservoir for ejaculate
Female Condom: Female condoms are essentially used for the same purpose as male condoms—to prevent pregnancy and to protect the woman from HIV and other STIs (Figure 11-4). Two styles of female condoms are currently available:
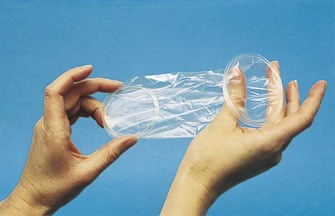
1. Two flexible rings, one that fits into the vagina and one that remains outside, connected by a polyurethane sheath
2. A bikini-panty style that has a pouch that fits inside the vagina
In 2005, a latex-free nitrile condom was introduced with a soft sponge rather than a firm ring to hold it in place (Kaplan, 2008a).
Female condoms are prelubricated, single-use items available over the counter. They give the woman control over her exposure to infections without having to rely on the cooperation of her partner. Its failure rate in pregnancy prevention is 5%. Many women find it unattractive.
Spermicides: Spermicidal foam, cream, jelly, film, and suppository capsules are over-the-counter contraceptives. They are inserted into the vagina before intercourse to neutralize vaginal secretions, destroy sperm, and block entrance to the uterus. Each product has specific directions for use. Vaginal films and suppositories must melt before they are effective, which takes about 15 minutes. Most spermicides are effective for no more than 1 hour. Reapplication is needed for repeated coitus. The woman should not douche for at least 6 to 8 hours after intercourse.
Adolescents often choose this type of contraception because it is inexpensive and easy to obtain. Teenagers should be taught that products labeled “for personal hygiene use” do not have contraceptive action. Spermicides have an actual failure rate of 21%. The use of a condom with the spermicide increases the contraceptive effectiveness.
Emergency Contraception
The “morning after” pill is a method of preventing pregnancy after unprotected sexual intercourse. It can be used if contraceptives fail (such as a condom that tears), in cases of rape, or in other situations as needed.
A larger-than-normal dose of oral contraceptive can be taken no later than 72 hours after unprotected sex, and a second dose is repeated 12 hours later.
Plan B emergency contraception is a progestin-only package that contains two tablets that are to be taken 12 hours apart. The pills can be taken up to 72 hours after unprotected sexual intercourse. This pill is specifically designed for emergency contraception and is available without prescription to women over 18 years of age. Legislation is pending to have this product available without prescription to 17-year-olds as well. Emergency contraceptives using medicines containing estrogen was not as well tolerated, and estrogen is known to increase cardiovascular risk; therefore, the Plan B progestin-only package is in use today.
A new emergency contraceptive, uliprisal (ella), has been approved by the FDA. It prevents pregnancy by prolonging ovulation and can be taken within 5 days of unprotected sex.
Unreliable Contraceptive Methods
Withdrawal, or coitus interruptus, is withdrawal of the penis before ejaculation. It demands more self-control than most men can achieve. Preejaculatory secretions often contain sperm that can fertilize an ovum.
Douching
Douching after intercourse is not a form of birth control and may actually transport sperm farther into the birth canal.
Breastfeeding
Breastfeeding inhibits ovulation in many women as long as the infant receives at least 10 feedings in 24 hours because the prolactin secreted to stimulate milk production also inhibits ovulation. If the woman supplements with formula or when the infant begins taking solids, milk intake (and thus prolactin secretion) falls. Ovulation is then likely, and pregnancy can occur. Remember that ovulation precedes menstruation—pregnancy can occur before the first menstrual period after birth.
Permanent Contraception
Sterilization is a permanent method of birth control that is almost 100% effective in preventing pregnancy. Although the procedures may be reversed in some cases, reversal is expensive and not always successful. Therefore patients should think carefully about this decision and consider it permanent.
Advantages: The advantages of sterilization relate to the fact that the person can consider the risk of pregnancy to be near zero. Minimal anxiety about becoming pregnant may help the individual to enjoy the sexual relationship more.
Disadvantages: A major disadvantage of sterilization is the same as its primary advantage: permanence. Divorce, marriage, death of a child, or a change in attitude toward having children may make the person regret his or her decision. The procedures require surgery, and although the risks are small, they are the same as for other surgical procedures: hemorrhage, infection, injury to other organs, and anesthesia complications.
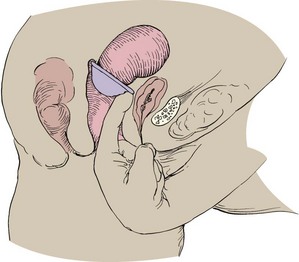
Male Sterilization: Male sterilization, or vasectomy, is performed by making a cut in each side of the scrotum and cutting each vas deferens, the tube through which the sperm travel (Figure 11-5, A). Because sperm are already present in the system distal to the area of ligation, sterility is not immediate. Another method of birth control must be used until all sperm have left the system, usually about 1 month. The man should return to his physician for analysis of his semen to verify that it no longer contains sperm. Men need information about the anatomy and physiology of their sex organs. They need reassurance that they will still have erections and ejaculations and that intercourse will remain pleasurable.
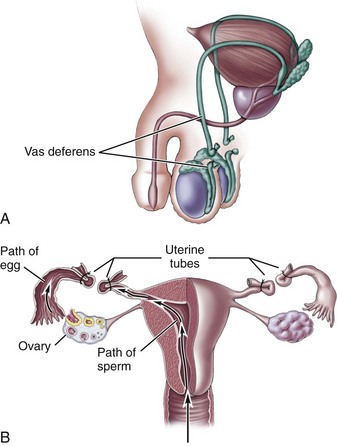
FIGURE 11-5 Surgical methods of birth control. A, Vasectomy, the cutting and ligation (tying off) of the vas deferens. B, Tubal ligation, the ligation of the fallopian tubes.
The surgery takes about 20 minutes and is performed on an outpatient basis with a local anesthetic. There is some pain, bruising, and swelling after the surgery. Rest, a mild analgesic, and the application of an ice pack are comfort measures. As in other surgeries, the man should report the following:
Tubal ligation: Tubal ligation involves blocking or ligating the fallopian tubes. It can be accomplished by using electrocautery or clips. Tubal ligation is easy to perform during the immediate postpartum period because the fundus, to which the tubes are attached, is large and near the surface. Three methods may be used:
1. A minilaparotomy, nicknamed “Band-Aid surgery,” uses an incision near the umbilicus in the immediate postpartum period or just above the symphysis pubis at other times. The surgeon makes a tiny incision, brings each tube through it, and ligates and cuts the tube.
2. Laparoscopic surgery is similar, but the tubes are identified and ligated through a lighted tube called a laparoscope (Figure 11-5, B).
3. The traditional approach is performed during other abdominal surgery, usually a cesarean birth.
The discomfort after the minilaparotomy or laparoscopy is usually easily relieved with oral analgesia. Some women experience nausea from the anesthesia. Even though this is not considered major surgery, the woman requires 1 or 2 days to recuperate. She should report signs of bleeding or infection, as with the male vasectomy.
Hysteroscopic sterilization: A hysteroscope can be placed through the vagina into the cervix. Saline distends the uterus and an Essure microinsert is placed into the fallopian tubes. A benign inflammation occurs that results in permanent closure of the fallopian tubes within 3 months. This type of procedure helps the woman avoid hospitalization, anesthesia, and abdominal scarring. Contraceptives must be used for 3 months until tubal fibrosis occurs. A hysterosalpingogram can confirm closure of the tubes (Theroux, 2008).
Infertility
Infertility is the inability to conceive when desired. The strict definition of infertility is that a couple who has regular, unprotected sexual intercourse for 1 year cannot conceive. Infertility is primary if conception has never occurred and secondary when there have been one or more pregnancies before the infertility. The definition is usually expanded to couples who conceive but repeatedly lose a pregnancy.
More couples are seeking help for infertility for many reasons, including the following:
• Couples are delaying childbearing until their mid- to late 30s, when a natural decline in fertility occurs.
• New treatments may cause couples to reconsider their acceptance of childlessness and initiate or resume infertility therapy.
Social and Psychological Implications
The role of parent is one that most people expect to assume at some time. Because parenting is such an expected and necessary part of society, infertility has implications that go far beyond the physical.
Assumption of Fertility
Most couples assume they are fertile and work hard to prevent pregnancy as they pursue educational or career goals. They expect to conceive in a few months at the most when they do decide to have a child. They enjoy being with parents and expectant parents and often begin making preparations for living space and supplies that an infant will need. As months pass and the woman’s period comes each month, the couple becomes less certain that they will become parents themselves. Once-joyful occasions, such as baby showers, become melancholy or anxiety-provoking events. The potential grandparents may think their children are waiting too long to start a family or may even believe they are selfish, if they do not realize that the younger couple is trying to conceive.
Psychological Reactions
Shock: Shock is often a couple’s first reaction to infertility. Their reactions vary based on how easily the infertility is alleviated, their personalities and self-images, and their relationship.
Guilt: The partner who has the identified problem may feel guilty because he or she is depriving the other one of children. Either partner may regret past choices that now affect their fertility, such as sexual practices that resulted in infections that scarred the fallopian tubes.
Isolation: Infertile couples often feel different from those who have no problem conceiving. They may isolate themselves from these people to avoid emotional pain. In doing so, they may also isolate themselves from sources of support.
Depression: Infertility challenges one’s sense of control and self-image. The couple may experience a roller coaster of hope alternating with despair as the woman has her period each month. They may become judgmental and angry with others.
Stress on the Relationship: Either or both partners may feel unlovable because their self-esteem has been shaken. A man often finds it difficult to perform sexually “on demand” for semen specimens or at specific times each month. Their sexual relationship may take on a clinical air rather than one of love and support.
Cultural and Religious Considerations
In many cultures, fertility (or the lack thereof) is considered strictly a female problem. It may be closely linked to the woman’s social status. The stigma of infertility can lead to divorce and rejection from family and society. To choose treatment for infertility may go against the couple’s societal norms, particularly if the male must be treated to achieve pregnancy.
Religious norms influence what tests and treatments a couple is willing to pursue. Surrogate parenting, in vitro fertilization, or other techniques may not be acceptable in terms of the couple’s personal or religious beliefs. Conflict can arise if a potentially successful therapy is acceptable to one member of the couple but not to the other.
Factors Affecting Infertility
Many factors that cause infertility are unknown. Some couples may have a problem that makes it unlikely that they would conceive, yet they have several children. Others have no identified problem but still cannot conceive.
Male Factors
Abnormal Sperm: To produce a pregnancy, the man must deposit a sufficient number of normal sperm near the cervix, and the sperm must be protected from the acidic vaginal secretions until they enter the cervix. The sperm must be able to swim purposefully to the waiting ovum. A man may have a sperm count that is too low to achieve fertilization. He may have a sufficient number of sperm, but too many of these are dead or abnormally formed. Sperm are continuously formed, and many factors can affect their formation. Some factors that can interfere with normal sperm formation and function include the following:
Abnormal Erections: Anything that impairs nervous system function or blood flow to the penis can interfere with erections. Some drugs, notably antihypertensives, reduce or shorten the duration of erections.
Abnormal Ejaculation: Some drugs and nervous system disorders may cause retrograde ejaculation, in which semen is released into the bladder rather than from the penis. Hypospadias (urethral opening on the underside of the penis rather than the tip) causes semen to be deposited closer to the vaginal outlet rather than near the cervix.
Abnormal Seminal Fluid: Seminal fluid carries the sperm into the vagina, but only sperm enter the cervix to fertilize the ovum. Semen coagulates immediately after ejaculation, and then liquefies within 30 minutes to allow sperm to swim toward the cervix. Sperm will be trapped or will not survive if the seminal fluid remains thick or if its composition does not protect the sperm from the vaginal secretions.
Female Factors
A woman’s fertility depends on regular production of normal ova, having an open path from the ovary to the uterus, and having a uterine endometrium that supports the pregnancy.
Disorders of Ovulation: Normal ovulation depends on a balanced and precisely timed interaction between the hypothalamus, the pituitary, and the ovary (see Chapter 2). If the hypothalamus and/or pituitary do not properly stimulate the ovary, ovulation will not occur. Conversely, the ovary may not respond despite normal hormonal stimulation. Chemotherapeutic drugs for cancer, excessive alcohol intake, and smoking can interfere with ovulation. Sometimes ovulation does not occur because the woman is entering the climacteric early.
Abnormal Fallopian Tubes: Infections such as chlamydia and gonorrhea can cause scarring and adhesions of the fallopian tubes that block them. Adhesions may also occur because of endometriosis, pelvic surgery, appendicitis, peritonitis, or ovarian cysts. If the tubal obstruction allows the smaller sperm to pass but is too narrow for the resulting fertilized ovum, ectopic tubal pregnancy may occur (see Chapter 5). The same conditions may cause abnormal transport of the ovum through the tube.
Abnormal Uterus, Cervix, or Ovaries: Congenital abnormalities of the reproductive tract or uterine myomas (benign uterine muscle tumors) may interfere with normal implantation of the ovum, or they may result in repeated spontaneous abortion or early preterm labor. Women with polycystic ovaries have abnormalities of ovulation and menstruation that accompany the hormonal dysfunction associated with this disorder.
Hormone Abnormalities: In addition to interfering with ovulation, abnormal hormone stimulation can interfere with proper development of the uterine lining, resulting in an inability to conceive or in repeated spontaneous abortions. Abnormalities in the amount or timing of any hormone necessary for endometrial buildup, ovum development and release, or support of the conceptus can result in infertility.
Other Factors That May Influence Fertility
Coital Frequency: Intercourse more than three times per week is best for conception. The window of opportunity to conceive opens 2 days before ovulation and closes 1 day after ovulation.
Cigarette Smoking: Cigarette smoking of more than 15 cigarettes per day suppresses the function of the immune system, leading to an early loss of reproductive function. Nicotine has an effect on tubal motility, resulting in an increased risk of ectopic pregnancies.
Exercise, Diet, and Weight: Excessive exercise and weight loss may be linked to decreased fertility. A low-calorie vegetarian diet is associated with a short luteal phase, and excessive weight loss may influence the release of gonadotropins. Ovarian dysfunction is common in obese women, especially those who gain weight rapidly. However, weight is thought to be a cofactor of infertility rather than a direct cause.
Emotional Factors: Emotional factors do not cause infertility, but many infertile couples experience stress and anxiety and require emotional understanding. A strong support system is helpful in the decision to start or stop fertility treatments.
Medical Problems: Pelvic adhesions can obstruct the fallopian tube and cause infertility. Adhesions can result from abdominal and/or pelvic surgery, Crohn’s disease, ulcerative colitis, or celiac disease. PID and STIs are also associated with infertility.
Drugs and Chemicals: Pollutants in the environment and medications or chemicals ingested may influence fertility. Chemotherapeutic agents used in the treatment of cancer are related to infertility. Research is ongoing concerning the protective effect of suppressing ovarian function or storing ova during chemotherapeutic treatments. Recreational drugs such as marijuana and cocaine pose an increased risk for infertility. Cocaine use in men has been shown to affect the motility of sperm and contribute to infertility of the couple. Antihistamines can decrease vaginal lubrication, antihypertensives can decrease erectile ability, barbiturates can inhibit the release of gonadotropin, and NSAIDs can block egg release. The use of cimetidine, monoamine oxidase (MAO)-inhibitor antidepressants, and lithium are also thought to alter male reproduction. Reprotox is a center that maintains a database of reproductive effects of industrial chemicals. This database can be found at www.reprotox.org/Default.aspx and requires membership to access.
Evaluation of Infertility
Both members of a couple are evaluated for infertility. The evaluation begins with a thorough history and physical examination to identify evidence of other conditions that may also be affecting their fertility. Testing proceeds from the simple to the complex; however, it may be accelerated in the older woman because of her natural decline in fertility with age.
Male Testing
A semen analysis is the first male test performed. Semen is best collected by masturbation; if this is not an option, semen can be collected in a condom that does not contain spermicide. Endocrine tests identify the presence of hormonal stimulation that is necessary for sperm formation. Ultrasonography can identify anatomical abnormalities. Testicular biopsy is an invasive procedure to obtain a sample of testicular tissue for analysis.
Female Testing
The methods for predicting ovulation discussed in the section on natural family planning can also be used to evaluate infertility. Ultrasonography is used to assess the structure of reproductive organs, to identify the maturation and release of the ovum, and to ensure proper timing for other tests, such as the postcoital test. Ultrasonography is also used to identify multifetal pregnancies. The postcoital test is done 6 to 12 hours after intercourse to evaluate the action of sperm within the woman’s cervical mucus at the time of ovulation. Endocrine tests evaluate the hormone stimulation of ovulation and the buildup of the uterine lining to prepare for pregnancy. More invasive tests are sometimes required. The hysterosalpingogram is an x-ray study using contrast medium to evaluate the structure of the reproductive organs. An endometrial biopsy is done to obtain a sample of uterine lining to assess its response to hormones. Hysteroscopy and laparoscopy use an endoscope (instrument that allows visual inspection of internal organs) to examine the uterine interior and the pelvic organs.
Therapy for Infertility
The specific therapy depends on what cause, if any, was identified by testing.
Medications
Medications may be given to the man to improve semen quality or to the woman to induce ovulation, prepare the uterine endometrium for pregnancy, or support the pregnancy once it is established. Several drugs are given in combination with another drug to mimic natural function. Medications are continued for six to nine cycles for optimum outcome. Some of the drugs that may be prescribed include the following:
• Bromocriptine (Parlodel) (pergolide mesylate and dopamine agonists CV205-502 are newer drugs showing promise): Corrects excess prolactin secretion by the pituitary, which would interfere with implantation of the fertilized ovum
• Clomiphene (Clomid): Induces ovulation; may be used with human chorionic gonadotropin (hCG)
• Gonadotropin-releasing hormone (GnRH, Lutrepulse): Stimulates production of other hormones that, in turn, stimulate ovulation in the female and production of testosterone and sperm in the male (may be administered via intravenous [IV] pump worn on the waist)
• Leuprolide (Lupron): Reduces endometriosis
• Menotropins (Pergonal): Stimulates ovulation and sperm production
• Nafarelin (Synarel): Reduces endometriosis
• Progesterone: Promotes implantation of the fertilized ovum
• Urofollitropin (Fertinex): Stimulates ovulation
Medications given to induce ovulation also increase the risk of multifetal gestations. Although most of these multiple gestations are twins, higher multiples present a much higher risk for maternal, fetal, and neonatal complications. The parents of high multiples may need to make a decision about which, if any, of their fetuses to abort so that the others have a better chance of achieving maturity. This situation presents a difficult ethical situation for both parents and professionals.
Surgical Procedures
Surgery may be used to correct anatomical abnormalities such as varicocele, adhesions, or tubal obstruction.
Therapeutic Insemination
Once called “artificial insemination,” therapeutic insemination may use the male partner’s sperm or sperm from an anonymous donor. Therapeutic insemination also may be used by a woman who wants to bear a child biologically on her own. If sperm are placed directly in the uterus, they are washed and concentrated to improve their chances of fertilizing an ovum. Donors are screened for genetic defects, infections, and high-risk behaviors. Donor sperm is held frozen for 6 months to reduce the risk of transmitting a disease that was not apparent at the initial screening. Reputable centers limit the number of times a man may donate his sperm to reduce the chance of inadvertent consanguinity (blood relationship) between his offspring when they grow up.
Surrogate Parenting
A surrogate mother may donate the use of her uterus only, with the sperm and ovum coming from the infertile couple who have a problem carrying a pregnancy. Or, she may be inseminated with the male partner’s sperm, thus supplying both her genetic and her gestational components. Surrogate mothering cannot be anonymous, and the birth mother inevitably forms bonds with the fetus during the months of pregnancy.
Advanced Reproductive Techniques
Advanced reproductive technologies give new hope to couples who may have once considered their infertility to be irreversible (Table 11-2). However, some of the newest techniques are still considered experimental and thus are not covered by insurance.
Table 11-2
Summary of Assisted Reproductive Therapies (ARTs)
| THERAPY | DESCRIPTION |
| Therapeutic insemination | Donor sperm are placed in the uterus or fallopian tube; sperm may be the partner’s or a donor’s. |
| In vitro fertilization (IVF) | After inducing ovulation, ova are recovered by laparoscopy or transvaginal aspiration under sonography; they are then fertilized with sperm from the partner or a donor in the laboratory and 2 days later are transferred to the uterus. |
| Gamete intrafallopian transfer (GIFT) | Oocytes are retrieved into a catheter that contains prepared sperm; up to two ova are injected into each fallopian tube, where fertilization occurs. The woman must have at least one open tube. |
| Tubal embryo transfer (TET), also called zygote intrafallopian transfer (ZIFT) | Ova are fertilized as in IVF but are transferred to the fallopian tube as soon as fertilization occurs. The resulting embryos enter the uterus normally for implantation. |
| Donor oocyte | Multiple ova are retrieved from a woman. They are fertilized and placed in the prepared uterus of the infertile woman. |
| Surrogate mother | A woman allows her ova to be inseminated by the partner or another donor. She then carries the fetus and agrees to relinquish the infant after birth. |
| Gestational surrogate | The infertile couple undergoes IVF, but the resulting embryos are placed in the prepared uterus of a woman who has agreed to carry the fetus for them. The woman does not donate any of her genetic components. |
| Intracytoplasmic sperm injection (ICSI) | Sperm are inserted directly into ova. |
Bypassing Obstacles to Conception: The following techniques place intact sperm and ova together to allow fertilization. Each begins with ovulation induction by medications to obtain several ova and thus improve the likelihood of a successful pregnancy.
• In vitro fertilization (IVF): Several ova are obtained and mixed with the partner’s or a donor’s semen. Up to four resulting embryos are then returned to the uterus 2 days later.
• Gamete intrafallopian transfer (GIFT): Ova are obtained and mixed with sperm. The gametes are placed in the fallopian tubes, where fertilization and entry into the uterus occur normally.
• Tubal embryo transfer (TET), also called zygote intrafallopian transfer (ZIFT). The ova are fertilized outside the woman’s body and returned to the fallopian tube at an earlier stage than with IVF.
In general, GIFT and TET have a higher pregnancy rate than IVF. These techniques can result in a multifetal pregnancy. Rarely do all ova or embryos returned to the uterus actually implant.
Microsurgical Techniques: The surgical care of the infertile woman has been revolutionized by the development of laser and microsurgical techniques for male and female infertility. A surgeon can “operate” on the ovum itself to inject a sperm into it (intracytoplasmic sperm injection [ICSI]). The fertilized ovum is placed into the uterus, as with IVF.
Outcomes of Infertility Therapy
Three outcomes are possible after infertility therapy:
1. Achievement of a “take-home” infant
2. Unsuccessful therapy resulting in a decision about adoption
Becoming pregnant changes the couple’s anxiety but does not eliminate it. Because of past disappointments, they may be reluctant to invest emotionally in the pregnancy. They may delay preparations for birth because they expect to be disappointed again or fear that something will go wrong. Even when their infant is born, they may have unrealistic expectations of themselves as parents after all the difficulties in achieving pregnancy.
Couples who decide to pursue adoption must consider their preferences and the realities of the adoption “market.” Most couples prefer to adopt an infant of the same race, but that child may not be available. Some couples fear that they will have a biological child after adoption and wonder if they can love the two children equally.
When a pregnancy is lost after treatment, the couple may feel optimism mixed with sadness. On one hand, they proved that they could conceive. On the other hand, they did not get an infant.
Legal and Ethical Factors in Assisted Reproduction
Noncoital reproduction brings with it many legal and ethical issues. In most cases, assisted reproductive techniques (ARTs) are used to assist infertile couples. However, this technique can also be used by a couple to avoid known genetic anomalies carried by one partner. Donors and surrogates involve third parties, and their emotional bonds and legal rights must be considered. Homosexual couples or single parents can create a child through surrogacy, and a changed family structure evolves.
Parental rights are a legal challenge. It is now possible for a child to have five parents: a sperm donor, an egg donor, a gestational surrogate, and the parents who will rear the child. The right to bear a child is protected by the United States Constitution; the government cannot usually interfere. The nontraditional family is therefore entitled to constitutional protection.
Cloning one’s lost child is now a possibility. The fate of a frozen embryo when the parents divorced has been challenged in court. The sale of frozen embryos has a growing impact on our legal system. Federally funded research on fetal tissue can effect future research and development. State laws can also prevent funding of private research. The problems of insurance coverage and access to care are also highly debated issues.
Nursing Care Related to Infertility Treatment
Much of the nursing role involves supporting the couple as they undergo diagnosis and make decisions concerning treatment. The nurse must use tactful therapeutic communication to help each member of the couple discuss their feelings. Partners are encouraged to accept their feelings. The normality of feelings that seem out of place (such as ambivalence about a pregnancy after working so hard to achieve it) is reinforced. The couple is helped to identify ways to communicate with each other and to discuss available options that empower them with control.
The couple’s sense of control should be increased as much as possible. Their positive coping skills are reinforced, and more constructive alternatives to poor coping are explored. They may benefit from relaxation techniques, support groups, and other stress-management methods. Support groups can also reduce their sense of isolation. The couple should be helped to explore their options at each decision point. Only the person(s) involved can make the decision, but the nurse can help them to explore their feelings.
Menopause
The definition of menopause according to the World Health Organization (WHO) is the cessation of menstrual periods for a 12-month period because of changes in estrogen production. The climacteric (change of life) is also known as the perimenopausal period, which extends for 2 to 8 years before menstruation ceases. The last menstrual period occurs at approximately 51 years of age (Boston Women’s Health Book Collective, 2008). In the 2- to 8-year period before this time, the ova slowly degenerate and menstrual cycles are often anovulatory and irregular. Estrogen production by the ovaries decreases. Pregnancy can occur during the climacteric, and the woman should be encouraged to continue any birth control that she has used in the past. Decreasing estrogen in the woman increases her risk for osteoporosis, arteriosclerosis, and increases in cholesterol levels in the blood. Menopause may be induced at any age by surgery, pelvic irradiation, or extreme stress.
Physical Changes
The decrease in estrogen specifically causes the following:
• Changes in the menstrual cycle
• Vasomotor instability (hot flashes)
• Decreased moisture and elasticity of vagina that can cause dyspareunia (painful intercourse)
Other symptoms such as mood swings and irritability are also experienced. Hot flashes are a well-known phenomenon. The woman suddenly feels a burning or hot sensation of her skin followed by perspiration. Hot flashes often occur during the night, and some women have several sleep interruptions because of them. They are more likely to occur when menopause is artificial, such as through oophorectomy (removal of the ovaries), rather than when it occurs naturally. The woman may also notice chills, palpitations, dizziness, and tingling of the skin as part of the vasomotor instability.
The reproductive organs are estrogen dependent, leading to changes as the estrogen level declines. The uterus shrinks, and the ovaries atrophy. The sacral ligaments relax, and pelvic muscles weaken, which can result in pelvic floor dysfunction. The cervix becomes pale and shrinks. The vagina becomes shorter, narrower, and less elastic. There is less lubrication. Some women notice a change in libido (sexual desire) at this time. Coitus may be uncomfortable because of vaginal dryness. Urinary incontinence may be a problem since the muscles controlling urine flow atrophy. The breasts atrophy.
Loss of estrogen secretion also means an end to its protective effect on the woman’s cardiovascular and skeletal systems. Estrogen increases the amount of high-density lipoproteins, which carry cholesterol from body cells to the liver for excretion. The incidence of heart disease rises dramatically after menopause because low-density lipoproteins, which carry cholesterol into body cells (including blood vessels), increase.
Estrogen assists the deposition of calcium in the bones to strengthen them. Loss of bone mass accelerates as estrogen levels fall, resulting in osteoporosis. Osteoporosis is a leading cause of vertebral, hip, and other fractures in postmenopausal women because the bones become very fragile. Both males and females lose bone mass as they age. Females, who have a lower bone mass to begin with because they are smaller, lose more in proportion to the total amount as they age. In addition, they live longer than males, and the loss continues longer. Therefore problems such as hip fractures related to age affect many more women than men. The bones may be so fragile that a fracture occurs and causes a fall, rather than the fracture being the result of a fall.
Psychological and Cultural Variations
Women from different cultures have different experiences of menopause. How the society views aging, the role of the female, and femininity itself has a bearing. In countries in which age is revered, menopause is practically a “nonevent.” In the United States, with its emphasis on youth, sex appeal, and physical beauty, menopause can threaten the woman’s feelings of health and self-worth. A positive aspect of menopause is that it is a time of liberation from monthly periods, cramps, and the fear of unwanted pregnancy. It can be the beginning of a satisfying postreproductive life.
Treatment Options
Culture, finances, and access to health care are factors that must be considered. Partnership-building communication with the health care team can help the woman cope with lifestyle changes that may be necessary to maintain health. Exercise, an increase in the dietary intake of calcium and magnesium, and a high-fiber, low-fat diet rich in antioxidants are essential.
In the past, hormone replacement therapy (HRT) was advocated for most women to treat menopausal symptoms that interfered with activities of daily living and for its protective effect on the cardiovascular and skeletal systems. However, in 2002 a large study (Women’s Health Initiative [WHI]) was stopped because evidence indicated the women had increased occurrence of heart attack or stroke, breast cancer, and thrombophlebitis. The risks were thought to outweigh the benefits of HRT. The U.S. Preventive Services Task Force (USPSTF), the American College of Obstetricians and Gynecologists (ACOG), the American Heart Association, the North American Menopause Society, and the Canadian Task Force on preventive health care all recommend against the use of hormone replacement therapy for the prevention of chronic diseases in postmenopausal women.
Today, HRT decisions are based on the individual patient, with the benefits and risks clearly identified. Nurses should counsel their patients taking HRT to have regular follow-up care and report any signs of complications, such as headache, vision changes, signs of thrombophlebitis, or cardiac symptoms (Hacker et al., 2010).
Contraindications for HRT include estrogen-dependent breast cancer, endometrial cancer, thromboembolic disease, a history of malignant melanoma, chronic liver disease, severe hypertriglyceridemia, gallbladder disease, and seizure disorders. Although women who are BRCA-1 gene carriers have a 60% to 80% chance of developing breast cancer, prophylactic oophorectomy before menopause lowers the risk of cancer. The use of postmenopausal HRT after oophorectomy HRT is not contraindicated in women with BRCA-1 mutations (Eisen, Lubinski, Gronwald, et al., 2008). Annual breast examinations and regular self-breast assessments are advised for women undergoing HRT.
Complementary and Alternative Therapies
The use of over-the-counter complementary therapy during menopause has become very popular. Some examples include the following:
• Yam root contains natural progesterone in the form of diosgenin but does not provide a proven progesterone effect; it has oral and topical forms.
• Ginseng may help relieve menopausal symptoms such as hot flashes and headaches.
• Soy products contain phytoestrogens and are thought to reduce problems such as hot flashes and help convert vitamin D into calcitonin.
• Vitamin E is thought to stabilize estrogen levels.
• Black cohosh, marketed as Remifemin, is thought to reduce luteinizing hormone.
• Calcium and vitamin D supplements are recommended for women who cannot spend at least 30 minutes a day in the sun.
Homeopathy, acupuncture, and relaxation techniques can also be helpful. See Chapter 34 for more information concerning complementary and alternative medicine (CAM) therapies. Excessive caffeine intake and alcohol ingestion may increase calcium excretion, and smoking further decreases estrogen utilization; thus they should be avoided.
Therapy for Osteoporosis
Osteoporosis occurs when the loss of calcium from the bones is faster than its deposition in the bones. Signs of osteoporosis include a loss of height, the development of a “dowager’s hump” (a dorsal kyphosis and cervical lordosis), curvature of the upper spine, and increased susceptibility to hip and spinal fractures. Calcium intake from food sources such as dairy products, dark green leafy vegetables, soybeans, and wheat bread and/or calcium supplements can prevent complications of osteoporosis. Weight-bearing exercises such as walking, hiking, stair climbing, and dancing are advisable. High-impact exercises should be avoided. Bone mineral density (BMD) testing is recommended for postmenopausal women over 65 years of age to assess risk for osteoporosis. Alendronate (Fosamax) may be prescribed. Esophageal and gastric irritation are common side effects of alendronate, and the woman should be instructed to drink 8 ounces of plain water and sit upright for 30 minutes after taking the drug and before eating a meal. Raloxifene (Evista) acts like estrogen to prevent bone loss but does not cause adverse side effects. Parathyroid hormones and calcitonin show promise in future treatment.
Nursing Care of the Menopausal Woman
Nursing Care Plan 11-1 offers further nursing interventions in addition to those discussed here. The woman’s knowledge of the changes surrounding menopause is assessed. If she is near the age for the climacteric to begin, any symptoms are identified. Treatments or tests that the woman will have, such as bone density studies, are clarified. The nurse must determine the woman’s understanding of the risks and benefits of HRT when helping her to decide about the therapy, with written information given to reinforce verbal teaching.
11-1  Nursing Care Plan
Nursing Care Plan
The Woman Experiencing Perimenopausal Symptoms
A 49-year-old woman tells the nurse that she is experiencing a lot of discomfort relating to her beginning menopause. She states she is having hot flashes and does not enjoy having sex anymore, among other “embarrassing” symptoms.
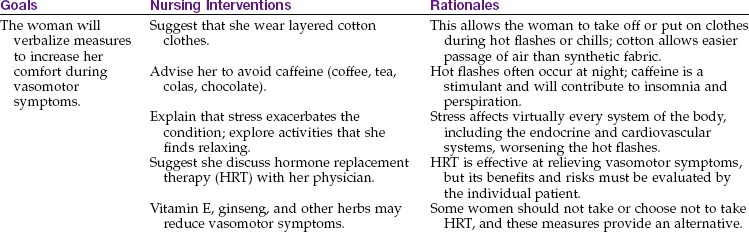
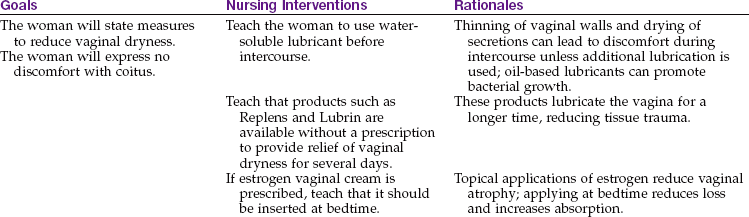
Stress urinary incontinence and infection related to genital atrophy
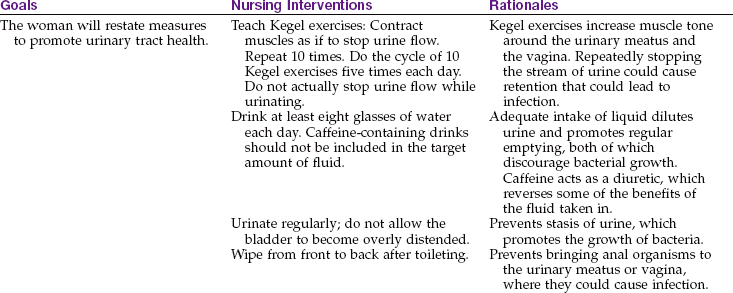
1. A woman, age 49 years, requests help in controlling her anxiety level. She reports hot flashes, night sweats, sleep pattern disturbances, and mood swings. She is afraid her husband will leave her and wants medication to “calm her down.” Based on her age and history, what is the best response of the nurse?
The woman is taught what signs and symptoms she should report, such as vaginal bleeding that recurs after the cessation of menstrual periods. She should also report signs of vaginal irritation or signs of urinary tract infection because these are more common with atrophy of vaginal tissues.
The woman is also taught how to take prescribed medications properly. For example, the nurse must teach her that calcium is best absorbed if she also takes vitamin D. Taking foods or other medications before allowing at least 30 minutes (preferably 1 hour) for alendronate to be absorbed will negate the benefit of that dose. Lying down after taking alendronate can cause severe esophageal irritation.
The woman should be informed of medication-related side effects to report. She should contact her health care provider if she has headaches, visual disturbances, signs of thrombophlebitis, heaviness in her legs, chest pain, or breast lumps, because these symptoms may indicate adverse side effects associated with HRT. Basic education concerning the use of CAM therapies and their side effects (see Chapter 34) and interactions should be included in the teaching plan.
The woman should be taught about the value of weight-bearing exercise in slowing bone loss. She must be helped to identify suitable exercises that she enjoys and cautioned about the high-impact ones that she should avoid. Because even minor falls can result in disabling fractures in women who have osteoporosis, the nurse should teach the woman ways to make her environment safer. Safety needs may be as simple as making sure there are adequate lights with handy switches and that loose cords and obstructions are secured outside of walking paths. Nonskid bath and shower floors and convenient grab bars reduce the risk of falls when bathing.
The nurse should identify the woman’s perception of her menopausal status with consideration of cultural factors, sexuality concerns, access to care, and use of self-medication. Teaching the woman about available support groups in the community and the physiology of menopause can increase compliance with preventive health measures.
Pelvic Floor Dysfunction
Pelvic floor dysfunction occurs when the muscles, ligaments, and fascia that support the pelvic organs are damaged or weakened. The dysfunction may occur as a result of childbirth injury but often does not become obvious until the perimenopausal period. There are two classifications of pelvic floor dysfunction that often occur together:
Vaginal Wall Prolapse
The vaginal wall may prolapse in either the anterior or posterior wall or in both walls.
Cystocele
A cystocele occurs when the anterior vaginal wall becomes too weak to support the bladder that contains urine. Stress incontinence may result and cause the woman to lose urine when there is a sudden increase in intraabdominal pressure, such as with laughing, coughing, or sneezing.
Rectocele
A rectocele occurs when the posterior vaginal wall becomes weakened. When the woman strains to defecate, feces are pushed against the weakened wall rather than being directed toward the rectal sphincter for elimination. The woman may use digital pressure against her posterior vaginal wall to facilitate defecation.
Uterine Prolapse
A uterine prolapse occurs when the ligaments that support the uterus and vagina are weakened. The uterus sags downward in the vagina. It is more likely to occur in the woman who has had several vaginal births or one who had large infants. Symptoms of uterine prolapse include pelvic fullness, a dragging sensation, pelvic pressure, fatigue, and a low backache. In addition, the woman will often have symptoms characteristic of vaginal wall prolapse.
Management of Pelvic Floor Dysfunction
Medical management of pelvic floor dysfunction depends on several factors, such as age, physical condition, sexual activity, and extent of the problem. Surgical correction gives the most definitive relief. The vaginal wall(s) may be repaired, and a vaginal hysterectomy is often done for uterine prolapse. The two surgeries are often combined. If the woman cannot have surgery, a pessary (a device to support the pelvic structures) may be inserted into her vagina. Contraindications to the use of a pessary include pelvic infections, PID, and latex allergy. Careful hygiene and follow-up care are essential when a pessary is inserted to prevent complications such as ulcerations or infections.
Nursing Care of the Woman with Pelvic Floor Dysfunction
Kegel exercises can help to strengthen the pubococcygeal muscle, a major support for the urethra, vagina, and rectum. The woman should contract her muscles as if stopping the flow of urine. She should not actually do the exercise while urinating. She should repeat the contraction 10 times and perform this cycle five times each day. The woman should continue Kegel exercises for the rest of her life to maintain pelvic muscle tone.
To reduce some of the low back and pelvic discomforts associated with pelvic relaxation, the woman can be taught to lie down with her feet elevated. Assuming the knee-chest position for a few minutes may also help. Measures to prevent constipation, such as adequate fluid and fiber intake, reduce hard feces that would put further pressure on a rectocele.
Urinary Incontinence
Urinary incontinence is an uncontrollable leakage of urine from the bladder. Stress incontinence is leakage caused by a sudden increase in intraabdominal pressure (as occurs with sneezing or coughing). Urge incontinence is the inability to control the urge to urinate because of an overactive bladder. Urinary incontinence in women is often related to genital trauma during childbirth and is most common in multiparous women. It can be worsened by drugs such as antidepressants, diuretics, caffeine, anticholinergics, alcohol, beta-blockers, and angiotensin-converting enzyme (ACE) inhibitors.
Treatment and Nursing Care
The nurse can teach the woman how to do Kegel exercises, which can be enhanced by the use of vaginal weights to strengthen the pelvic floor muscles. Electrical muscle stimulation (TENS) may also be prescribed. Medications used for an overactive bladder include oxybutynin (Ditropan XL), tolterodine (Detrol), imipramine (Tofranil), dicyclomine (Bentyl), and hyoscyamine (Cystospaz).
Surgical procedures for stress incontinence include injection of collagen into periurethral tissue. Extracorporeal magnetic innervation is a noninvasive stimulation of muscles that has shown promise in both stress incontinence and overactive bladder. Intraurethral occlusive plugs, valved catheters that act as an artificial urinary sphincter control, are rapidly replacing absorbent pads and surgical intervention.
Other Female Reproductive Tract Disorders
A woman may have other reproductive tract disorders during her life. An overview of some common benign ones is presented in the following sections. A medical-surgical text should be consulted for more information about these and information about malignant female reproductive tract disorders.
Uterine Fibroids
Uterine fibroids are also known as leiomyomas, myomas, and myofibromas. Uterine fibroids are benign growths of uterine muscle cells and are a very common gynecological condition. They grow under the influence of estrogen, and they are thus most prominent during the childbearing years and often atrophy after menopause. Nulliparity and obesity are risk factors, whereas oral contraceptives reduce the risk of forming fibroids. Many women have no problems with fibroids, but they sometimes cause irregular bleeding, pressure on the bladder, pelvic pressure, dysmenorrhea, and menorrhagia with blood loss exceeding 200 mL/month.
Treatment
Uterine fibroids that are asymptomatic are observed and periodically reevaluated. If the woman is symptomatic, there are surgical and nonsurgical options. Surgical interventions include hysteroscopic myomectomy, where the fibroid is removed with a hysteroscope rather than a surgical incision, but this is not an option for large or multiple lesions. A hysterectomy (removal of the entire uterus) can be performed if the woman is past her childbearing years. Medical treatment before surgery improves outcome. A laparoscopic myomectomy, the surgical removal of fibroids, preserves fertility. Myolysis is the laser or electrosurgical destruction of fibroids, and it also preserves fertility.
Uterine fibroid embolization is a nonsurgical technique of treating uterine fibroids that involves fewer physiological effects than drug therapy, fewer psychological effects than surgery, and a faster recovery time. The nurse should help the woman understand her options in relation to her childbearing goals. Some women feel sexual functioning is related to having a uterus, and the nurse can help clarify misconceptions and reduce anxieties. The preoperative and postoperative care is similar to that for any abdominal surgery (a medical-surgical text should be consulted).
Ovarian Cysts
A follicular ovarian cyst may develop if the follicle fails to rupture and release its ovum during the menstrual cycle. This type of cyst usually regresses with the next menstrual cycle. A lutein cyst may occur when the corpus luteum that develops after ovulation fails to regress. The lutein cyst is more likely to cause pain. An ovarian cyst that ruptures or becomes twisted and infarcted as its blood supply is cut off can cause pelvic pain and tenderness.
Diagnosis is by transvaginal ultrasound examination. A laparoscopy may aid in diagnosing and differentiating the ovarian cyst pain from that caused by endometriosis. Laparotomy may be required to remove the cyst.
Cultural Aspects of Pain Control
Pain is considered the fifth vital sign for nurses to assess on a regular basis. Culture and ethnicity may have an impact on the accuracy of pain assessment. Asian women may understand a vertical pain score because they read downward rather than left to right (see Chapter 21 for pain rating scales). Descriptive words for pain can imply intensity, such as “aches” versus “hurt.” In general, any pain score above 5 on a scale of 0 to 10 can interfere with activities of daily living and requires nursing intervention.
Ethnicity can affect drug metabolism so that a dose that is effective for one ethnic group may not be the same in others. Drug research often uses white males as subjects.
Diet can affect drug absorption. For example, griseofulvin requires fat in the diet for adequate absorption. Malnutrition can interfere with the absorption and excretion of medications. Smoking is known to have an impact on the metabolism of some drugs.
CAM therapy can affect the action of prescribed drugs. For example, ginseng alters metabolism and therefore affects the absorption and elimination of drugs (see Chapter 34 for details of CAM therapy). Patients should be asked what type of self-care they use for chronic pain. Many patients report using CAM therapy in addition to prescribed drugs. Some women suffer in silence with pain that is not relieved by prescribed medication, believing nothing more can be done. These women need guidance and counseling. Pain clinics may be available in some hospitals. Members of some cultural groups will not report embarrassing side effects, such as diarrhea, and may stop taking the medication because of these side effects. Careful, sensitive questioning by the nurse is essential because this information may not be volunteered.
Understanding pain, its symptoms, and its causes as well as the influence of culture, ethnicity, diet, and CAM therapy on pain relief is essential if nurses are to provide comprehensive care to their patients.
Get Ready for the NCLEX® Examination
Key Points
• Preventive care is cost-effective because health problems can be caught early and treated.
• Teaching a woman breast care can reduce her risk of death from breast cancer.
• Several self-help measures can relieve some symptoms of premenstrual syndrome.
• Prevention of toxic shock syndrome involves not allowing microorganisms the time to grow in the woman’s reproductive tract.
• Sexually transmitted infections (STIs) must be adequately treated in all sexual contacts to stop the transmission and to prevent resistance to antibiotics.
• Contraception is an individual choice. The nurse must avoid incorporating personal preferences when educating patients about contraceptive methods.
• Contraceptive choices include temporary contraception, such as barrier methods or hormones, or permanent contraception, such as hysteroscopic sterilization or vasectomy.
• Emergency contraception, Plan B, is a progestin-only medication taken in two doses 12 hours apart within 72-hours of unprotected sexual intercourse.
• Fertility awareness methods can be used both to prevent pregnancy and to increase the chance of achieving it.
• Except for abstinence, condoms (male and female) offer the best protection from STIs, including HIV.
• Nursing care of infertile couples includes helping them to evaluate their options at different phases during evaluation and treatment.
• Common menopausal symptoms, such as hot flashes and vaginal dryness, stem from the cessation of ovulation and the decrease in hormonal activity, particularly that of estrogen and progesterone.
• Prevention of disabling osteoporosis begins with adequate calcium and vitamin D intake during youth to achieve maximum bone mass. Reducing risk for osteoporosis after menopause is best accomplished by adequate calcium and vitamin D intake combined with exercise.
• Alternative therapies for hormone replacement are available for women who cannot take estrogen (see Chapter 34).
• Pain is considered a fifth vital sign and should be assessed with cultural sensitivity.
Additional Learning Resources
 Go to your Study Guide for additional learning activities to help you master this chapter content.
Go to your Study Guide for additional learning activities to help you master this chapter content.
Go to your Evolve website (http://evolve.elsevier.com/Leifer) for the following FREE learning resources:
• Answer Guidelines for Critical Thinking Questions
• Answers and Rationales for Review Questions for the NCLEX® Examination
• Glossary with English and Spanish pronunciations
• Interactive Review Questions for the NCLEX® Examination
• Patient Teaching Plans in English and Spanish
 Online Resources
Online Resources• American Congress of Obstetricians and Gynecologists (ACOG): www.ACOG.org
• Managing contraception: www.managingcontraception.com
• Marquette Method: www.marquette.edu/efficacy.php; http://nursing.slu.edu/ncfe/index.html
• Menopause: www.menopause.org/psht08.pdf
• National Osteoporosis Foundation: www.nof.org
• National Women’s Health Information Center: www.4women.gov
• Planned Parenthood: www.plannedparenthood.org
• Prevention and early detection of cervical cancer: www.cancer.org/docroot/CRI/content/CRI_2_6x_cervical_cancer_prevention_and_early_detection_8.asp?sitearea=PED
• Reproductive toxicology database: www.reprotox.org
• Today sponge: www.todaysponge.com
Review Questions for the NCLEX® Examination
1. Choose the correct teaching for breast self-examination (BSE):
1. Monthly BSE eliminates the need for a professional examination until after age 40 years.
2. BSE should be done 1 week after the beginning of each menstrual period.
3. Dry fingers make it easier to feel very small lumps that are just under the skin.
2. The women’s health nurse practitioner recommends ibuprofen to relieve a patient’s menstrual cramps. The nurse should teach her to take the drug:
1. with a full glass of water and wait 30 minutes before taking any food.
2. on a full stomach, but only if her cramps seem to be getting more severe.
3. three times per day for 1 week before she expects her period to begin.
4. with food, just before her period begins or soon after it begins.
3. What is a reliable temporary (reversible) birth control method?
4. To relieve or reduce symptoms of premenstrual dysphoric syndrome, what should the nurse recommend that the woman do?
5. Patient teaching to prevent osteoporosis in the menopausal woman should include: