Visual Perception
2 Describe the typical development of visual-perceptual skills.
3 Identify factors that contribute to typical or atypical development of visual perception.
4 Explain the effects of visual-perceptual problems on occupations and life activities such as activities of daily living, education, work, play, leisure, and social participation.
5 Describe models and theories that may be used in structuring intervention plans for children who have problems with visual-perceptual skills.
6 Identify assessments and methods useful in the evaluation of visual-perceptual skills in children.
7 Describe intervention strategies for assisting children in improving or compensating for problems with visual-perceptual skills.
8 Give case examples, including principles of evaluation and intervention.
Some consider vision to be the most influential sense in humans.15 There is little argument that vision is the dominant sense in human perception of the external world; it helps the individual to monitor what is happening in the environment outside the body. Because of the complexity of the visual system, it is difficult to imagine the impact of a visual-perceptual deficit on daily living. Functional problems that may result include difficulties with eating, dressing, reading, writing, locating objects, driving, and many other activities necessary for engagement in an occupation.
Given that occupational therapists focus on individuals’ participation in activities of daily living (ADLs), education, work, play, leisure, and social activities, the focus on the client factor of visual perception and its effects on performance skills, including literacy, can be critical. Literacy is embedded within all areas of occupational performance,141 from ADLs (reading recipes) and education (taking notes in class) to social participation (reading bus schedules). The reauthorization of both the Individuals with Disabilities Education Act (IDEA, 2004) and the No Child Left Behind Act (NCLB, 2001) addresses the need to better address literacy for children in public schools. Part C of the reauthorized IDEA requires that preliteracy be addressed in the very young child. For children of any age, occupational therapists can support literacy in many ways, including providing services to improve visual perception.
Although visual perception is a major intervention emphasis of occupational therapists working with children, it is one of the least understood areas of evaluation and treatment. The information presented in this chapter reflects current knowledge of visual perception that relates to evaluation of and intervention for children. The information in this area continues to evolve as research confirms or disproves explanatory models of the visual-perceptual system.
DEFINITIONS
Visual perception is defined as the total process responsible for the reception (sensory functions) and cognition (specific mental functions) of visual stimuli. The sensory function or visual-receptive component is the process of extracting and organizing information from the environment, and the specific mental functions that constitute the visual-cognitive component provide the capacity to organize, structure, and interpret visual stimuli, giving meaning to what is seen.102 Together these two components enable a person to understand what he or she sees, and both are necessary for functional vision. Visual-perceptual skills include the recognition and identification of shapes, objects, colors, and other qualities. Visual perception allows a person to make accurate judgments on the size, configuration, and spatial relationships of objects. The visual-receptive components are described in the Occupational Therapy Practice Framework: Domain and Process, 2nd Edition, under client factors of sensory functions and pain, and the visual-cognitive components are described under specific mental functions.2
THE VISUAL SYSTEM
Hearing and vision are the distant senses that allow a person to understand what is happening in the environment outside his or her body or in extrapersonal space. These sense organs transmit information to the brain, the primary function of which is to receive information from the world for processing and coding. The visual sensory stimuli are then integrated with other sensory input and associated with past experiences. Approximately 70% of the sensory receptors in humans are allocated to vision. The eye, oculomotor muscles and pathways, optic nerve, optic tract, occipital cortex, and associative areas of the cerebral cortex (parietal and temporal lobes) are all included in this process. It is imperative that occupational therapists gain an understanding of the neurophysiologic interactions in the central nervous system (CNS) so that they can effectively evaluate and treat children with problems in the visual system. This discussion begins with the sensory receptor, the eye.
Anatomy of the Eye
A basic understanding of the anatomy and physiology of the eye aids comprehension of its influence on perception (Figure 12-1). The eye functions to transmit light to the retina, on which it focuses images of the environment. The eye is shaped to refract light rays such that the most sensitive part of the retina receives rays at a convergent point. The cornea covers the front of the eye and is part of the outermost layer of the eyeball. It plays a significant part in the focusing or bending of light rays that enter the eye. Behind the cornea is the aqueous humor, a clear fluid; the pressure of this fluid helps both to maintain the shape of the cornea and to focus light rays. The colored part of the eye, the iris, with its center hole, the pupil, is directly behind the cornea. The iris controls the amount of light entering the eye by increasing or decreasing the size of the pupil. The light then progresses through the crystalline lens, which does the fine focusing for near or far vision, and through a jelly-like substance called the vitreous humor.
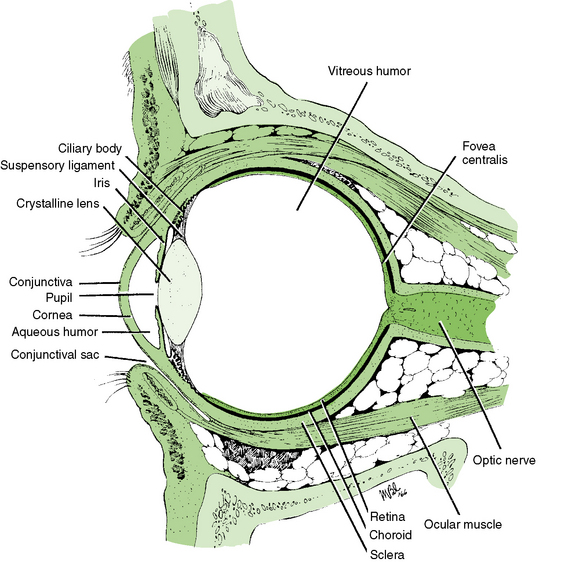
FIGURE 12-1 Cross-section of the eye. From Ingalls, A. J., & Salerno, M. C. [1983]. Maternal and child health nursing [5th ed.]. St. Louis: Mosby.
The eye has three layers: the sclera, the choroid, and the retina. The sclera, which is fibrous and elastic, helps hold the rest of the eye structure in place; the choroid is composed primarily of blood vessels that nourish the eye; and the retina is the innermost layer. The retinal layer is composed of receptor nerve cells that contain a chemical activated by light. The retina has three types of receptor cells: cones, which are used for color perception and visual acuity; rods, which are used for night and peripheral vision; and pupillary cells, which control opening (dilation) and closing (constriction) of the pupil.
The fovea centralis, which is located in the retina, is the point of sharpest and clearest vision. It is most responsive to daylight and must receive a certain amount of light before it transmits the signal to the optic nerve. The retina responds to spatial differences in the intensity of light stimulation, especially at contrasting border areas, and provides basic information about light and dark areas. Light stimulates the visual receptor cells in the retina, causing electrochemical changes that trigger an electrical impulse to flow to the optic nerve. The optic nerve (cranial nerve II) transmits the visual sensory messages to the brain for processing. This information travels to the brain in a special way. Fibers from the nasal half of each retina divide, and half of the fibers cross to the contralateral side of the brain. Fibers from the outer half of each retina do not divide; therefore, they carry visual information ipsilaterally. Thus visual information from either the left or right visual field enters the opposite portion of each retina and then travels to the same hemisphere of the brain. This organization means that even with the loss of vision in one eye, information is transmitted to both hemispheres of the brain. It also means that damage in the region of the left or right occipital cortex can cause a loss of vision, referred to as a field cut, in the opposite visual field.72
The optic nerve leads from the back of the eye to the lateral geniculate nucleus in the optic thalamus. It is here that binocular information is received and integrated at a basic level, which may contribute to crude depth perception. Information then passes from the two lateral geniculate bodies of the thalamus to the visual cortex in the occipital lobe (area 17). From the occipital cortex the refined visual information is sent in two directions via visual area 18 or 19.109,110 Some impulses flow upward to the posterior parietal lobe, where visual-spatial processing occurs, focusing on the location of objects and their relationships to objects in space. This pathway is referred to as the dorsal stream. The magnocellular channel is dominant in the dorsal stream; this channel is associated with motion and depth detection, stereoscopic vision, and interpretation of spatial organization.69 Other impulses flow downward to the inferior temporal lobe, where visual object processing takes place. Information sent here is analyzed for the specific details of color, form, and size needed for accurate object identification; the focus is on pattern recognition and detail and on remembrance of the qualities of objects. This is referred to as the ventral stream. The parvocellular channel is dominant in the ventral stream; this channel is thought to be important for color perception and for detailed analysis of the shape and surface properties of objects.82
Visual-Receptive Functions
The oculomotor system enables the reception of visual stimuli (visual-receptive process). The visual-receptive components include visual fixation, pursuit and saccadic eye movements, acuity, accommodation, binocular fusion and stereopsis, and convergence and divergence. Visual fixation on a stationary object is a prerequisite skill for other oculomotor responses, such as shifting the gaze between objects (scanning) or tracking. Each eye is moved by the coordinated actions of the six extraocular muscles. These are innervated by cranial nerves III, IV, and VI (oculomotor, trochlear, and abducens nerves). The oculomotor nuclei are responsible for automatic conjugate eye movements (lateral, vertical, and convergence). They also help regulate the position of the eyes in relation to the position of the head. The nuclei receive most of their information from the superior colliculus.
Two types of eye movements are used to gather information from the environment: pursuit eye movements, or tracking, and saccadic eye movements, or scanning. Visual pursuit, or tracking, involves continued fixation on a moving object so that the image is maintained continuously on the fovea. The smooth pursuit system is characterized by slow, smooth movements. Tracking may occur with the eyes and head moving together or with the eyes moving independently of the head. Saccadic eye movements, or scanning, are defined as a rapid change of fixation from one point in the visual field to another. A saccade may be voluntary, as when localizing a quickly displaced stimulus or when reading, or it may be involuntary, as during the fast phases of vestibular nystagmus. A saccadic movement is precise, although the presence of a slight overshoot or undershoot is normal.
In addition to voluntary control of eye movements, the vestibulo-ocular pathways control conjugate eye movements reflexively in response to head movement and position in space. These pathways enable the eyes to remain fixed on a stationary object while the head and body move.
In addition to the tasks of visual fixation, pursuit movements, and saccadic movements, other visual-receptive components include the following:
• Acuity: The capacity to discriminate the fine details of objects in the visual field. A visual acuity measurement of 20/20 means that a person can perceive as small an object as an average person can perceive at 20 feet.
• Accommodation: The ability of each eye to compensate for a blurred image. Accommodation refers to the process used to obtain clear vision (i.e., to focus on an object at varying distances). This occurs when the internal ocular muscle (the ciliary muscle) contracts and causes a change in the crystalline lens of the eye to adjust for objects at different distances. Focusing must take place efficiently at all distances, and the eyes must be able to make the transition from focusing at near point (a book or a piece of paper) to far point (the teacher and the blackboard) and vice versa. It should take only a split second for this process of accommodation to occur.
• Binocular fusion: The ability mentally to combine the images from the two eyes into a single percept. There are two prerequisites for binocular fusion. First, the two eyes must be aligned on the object of regard; this is called motor fusion, and it requires coordination of the six extraocular muscles of each eye and precision between the two eyes. Second, the size and clarity of the two images must be compatible; this is known as sensory fusion. Only when these two prerequisites have been met can the brain combine what the two eyes see into a single percept.
• Stereopsis: Binocular depth perception or three-dimensional vision.
• Convergence and divergence: The ability of both eyes to turn inward toward the medial plane and outward from the medial plane.
For a more detailed description of the function of these components, see the textbook by Gentile.57
Visual-Cognitive Functions
Interpretation of the visual stimulus is a mental process involving cognition, which gives meaning to the visual stimulus (visual-cognitive process). The visual-cognitive components are visual attention, visual memory, visual discrimination, and visual imagery.
Visual Attention
Visual attention involves the selection of visual input. It also provides an appropriate time frame through which visual information is passed by the eye to the primary visual cortex of the brain, where visual-perceptual processing can occur. Voluntary eye movements of localization, fixation, ocular pursuit, and gaze shift lay the foundation for optimal functioning of visual attention.71 The following are the four components of visual attention:
• Alertness: Reflects the natural state of arousal. Alerting is the transition from an awake to the attentive and ready state needed for active learning and adaptive behavior.
• Selective attention: The ability to choose relevant visual information while ignoring less relevant information; it is conscious, focused attention.
• Visual vigilance: The conscious mental effort to concentrate and persist at a visual task. This skill is exhibited when a child plays diligently with a toy or writes a letter.
• Divided, or shared, attention: The ability to respond to two or more simultaneous tasks. This skill is exhibited when a child is engaged in one task that is automatic while visually monitoring another task.
Visual Memory
Visual memory involves the integration of visual information with previous experiences. Long-term memory, the permanent storehouse, has expansive capacity. In contrast, short-term memory can hold a limited number of unrelated bits of information for approximately 30 seconds.
Visual Discrimination
Visual discrimination is the ability to detect features of stimuli for recognition, matching, and categorization. Recognition is the ability to note key features of a stimulus and relate them to memory; matching is the ability to note the similarities among visual stimuli; and categorization is the ability mentally to determine a quality or category by which similarities or differences can be noted. These three abilities require the capability both to note similarities and differences among forms and symbols with increasing complexity and to relate these findings to information previously stored in long-term memory.
Visual-perceptual abilities aid the manipulation of a visual stimulus for visual discrimination.144 Because visual perception has not been consistently defined, resources on visual perception use different terms and categories to define the same visual-perceptual skills. At times this contributes to confusion, because different disciplines may define the same terms differently.
It is also important to note that a distinction exists between object (form) vision (ventral stream) and spatial vision (dorsal stream).67,84 Object vision is implicated in the visual identification of objects by color, texture, shape, and size (i.e., what things are). Spatial vision, which is concerned with the visual location of objects in space (i.e., where things are), responds to motor information and seems to be integral to egocentric localization during visuomotor tasks.72 As discussed earlier, these two classes of function are mediated by separate neural systems. The cortical tracts for both object vision and spatial vision are projected to the primary visual cortex, but the object vision pathway goes to the temporal lobe and the spatial vision pathway goes to the inferior parietal lobe. These anatomic divisions have been verified repeatedly. However, researchers have emphasized differences in how these two areas use visual information.63,64 Visual information about object characteristics permits the formation of long-term perceptual representations that support object identification and visual learning. Spatial vision provides information about the location of object qualities that are needed to guide action, such as adjusting the hand during reach to the size and orientation of an object.
Based on studies done with individuals who had acquired brain damage, these two functions have been shown to be independent.98,100 That is, disturbances of object recognition can occur without spatial disability, and spatial disability can occur with normal object perception.46 Following are definitions of the object (form) and spatial-perceptual skills, although they are not entirely separate entities.
Object (Form) Perception: Form discrimination and processing involves multiple visual areas in the brain. It is thought that form perception is accomplished by two processes with two separate systems carrying different aspects of form information.67 The first system, the abstract visual form system (AVF) is thought to perform abstract processing to recognize types of forms. The AVF system is used when the visual form information should be processed and stored in an abstract, nonspecific manner. For example, when a child is scanning the gym supply cabinet for a soccer ball, he is attempting to find a ball but not a specific ball. The second system, specific visual form (SVF) system, provides specific processing to distinguish different instances of a type of form. The SVF system processes input in a manner that produces specific output representations that distinguish different instances of the same type of form—for example, the child searching for his soccer ball among those of his teammates after practice is over.
• Form constancy: The recognition of forms and objects as the same in various environments, positions, and sizes. Form constancy helps a person develop stability and consistency in the visual world. It enables the person to recognize objects despite differences in orientation or detail. Form constancy enables a person to make assumptions regarding the size of an object even though visual stimuli may vary under different circumstances. The visual image of an object in the distance is much smaller than the image of the same object at close range, yet the person knows that the actual sizes are equivalent. For example, a school-aged child can identify the letter A whether it is typed, written in manuscript, written in cursive, written in upper or lower case letters, or italicized.
• Visual closure: The identification of forms or objects from incomplete presentations. This enables the person quickly to recognize objects, shapes, and forms by mentally completing the image or by matching it to information previously stored in memory. This allows the person to make assumptions regarding what the object is without having to see the complete presentation. For example, a child working at his or her desk is able to distinguish a pencil from a pen, even when both are partly hidden under some papers.
• Figure-ground recognition: The differentiation between foreground or background forms and objects. It is the ability to separate essential data from distracting surrounding information and the ability to attend to one aspect of a visual field while perceiving it in relation to the rest of the field. It is the ability to visually attend to what is important. For example, a child is able visually to find a favorite toy in a box filled with toys, scissors in a cluttered drawer, his or her mother in a crowded room, or a shirtsleeve on a monochromatic shirt.
Spatial Perception: There are two types of spatial relations: categorical spatial relations (above-below, right-left, on-off) and coordinate spatial relations (specify locations in a way that can be used for precise movements).130
• Position in space/visual spatial orientation: The determination of the spatial relationship of figures and objects to oneself or other forms and objects. This provides the awareness of an object’s position in relation to the observer or the perception of the direction in which it is turned. This perceptual ability is important to understanding directional language concepts such as in, out, up, down, in front of, behind, between, left, and right. In addition, position in space perception provides the ability to differentiate among letters and sequences of letters in a word or in a sentence. For example, the child knows how to place letters equal spaces apart and touching the line; he or she is able to recognize letters that extend below the line, such as p, g, q, or y. Another aspect of spatial perception, now referred to as object-focused spatial abilities, focuses on the spatial relations of objects irrespective of the individual.154 This includes skills evaluated by many formal assessments; however, poor performance on a formal test may or may not be linked to functional behavior.
• Depth perception: The determination of the relative distance between objects, figures, or landmarks and the observer and changes in planes of surfaces. This perceptual ability provides an awareness of how far away something is, and it also helps people move in space (e.g., walking down stairs, catching a ball, pouring water into a glass, parking a car). Depth perception is the third dimension beyond the two-dimensional image in the retina.123 Binocular vision, along with monocular cues such as texture, shading and linear perspective, all contribute to perception of three-dimensional shape and distance. Visual acuity and ocular alignment must also be adequate. The parietal lobe has been associated with depth perception.
• Topographic orientation: The determination of the location of objects and settings and the route to the location. Wayfinding depends on a cognitive map of the environment. These maps include information about the destination, spatial information, instructions for execution of travel plans, recognition of places, keeping track of where one is while moving about, and anticipation of features. These are important means of monitoring one’s movement from place to place.46 In addition, the images a person sees must be recognized if he or she is to make sense of what is viewed and if the individual is to find his or her way around.46 For example, the child is able to leave the classroom for a drink of water from the water fountain down the hall and then return to his or her desk.
Visual Imagery
Another important component in visual cognition is visual imagery, or visualization. Visual imagery refers to the ability to “picture” people, ideas, and objects in the mind’s eye even when the objects are not physically present. Developmentally, the child is first able to picture objects that make certain sounds and those that are familiar by taste or smell. The ability to picture what words say while reading is the next step. For example, the child can imagine the character of a book based on the written description. This level of visual-verbal matching provides the foundation for reading comprehension and spelling.
Motor and Process Skills
Client factors may affect performance skills that in turn may affect activities and occupations. Motor skills of posture, mobility, and coordination may be affected by poor visual skills. For example, in the area of mobility, research has shown the importance of vision in the development of proprioception of the hand prior to the onset of reaching in newborn infants.33 This can explain why young babies spend much time visually examining their hands. By 5 to 7 months, infants, in preparation for reaching, may use the current sight of the object’s orientation, or the memory of it, to orient the hand for grasping; sight of the hand has no effect on hand orientation at this point.96 If problems occur in visual memory affecting the memory of the hand, the hand may not be properly oriented during reach, and this affects coordination.
Process skills of knowledge, temporal organization, organization of space and objects, and adaptation all can be affected by visual perception. Children who have acquired damage to the white matter around the lateral ventricles or damage to the posterior parietal lobes can find it difficult to use vision to guide their body movements.47 For example, a floor boundary between carpet and linoleum can be difficult to cross because it looks the same as a step. Black-and-white tiled floors can be frightening to walk across. At a curb, the foot may be lifted to the wrong height, too early, or too late, and walking down stairs without a banister is difficult and dangerous.
Developmental Framework for Intervention
Warren presented a developmental framework based on a bottom-up approach to evaluation and treatment.157 Using the work of Moore,62 Warren suggested that with knowledge of where the deficit is located in the visual system, the therapist could design appropriate evaluation and treatment strategies to remediate basic problems and improve perceptual function.157 To apply this approach, the occupational therapist must have an understanding of the visual system, including both the visual-receptive and visual-cognitive components. Although Warren’s model was presented as a developmental framework for evaluation and treatment of visual-perceptual dysfunction in adults with acquired brain injuries, it is useful as a model for children with visual-perceptual deficits. A hierarchy of visual-perceptual skill development in the central nervous system is presented in Figure 12-2. The definitions of components of each level are provided in the following list and are used in later descriptions of intervention.
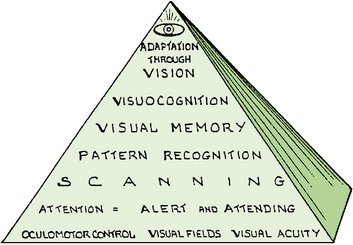
FIGURE 12-2 Hierarchy of visual-perceptual skills development. From Warren, M. [1993]. A hierarchical model for evaluation and treatment of visual perceptual dysfunction in adult acquired brain injury. I. American Journal of Occupational Therapy, 47, 42-54.
1. Primary visual skills form the foundation of all visual functions.
• Oculomotor control provides efficient eye movements that ensure that the scan path is accomplished.
• Visual fields register the complete visual scene.
• Visual acuity ensures that the visual information sent to the CNS is accurate.
2. Visual attention. The thoroughness of the scan path depends on visual attention.
3. Scanning. Pattern recognition depends on organized, thorough scanning of the visual environment. The retina must record all the detail of the scene systematically through the use of a scan path.
4. Pattern recognition. The ability to store information in memory requires pattern detection and recognition. This is the identification of the salient features of an object.
• Configural aspects (shape, contour, and general features)
• Specific features of an object (details of color, shading, and texture)
5. Visual memory. Mental manipulation of visual information needed for visual cognition requires the ability either to retain the information in memory for immediate recall or to store for later retrieval.
6. Visual cognition. This is the ability to mentally manipulate visual information and integrate it with other sensory information to solve problems, formulate plans, and make decisions.
Warren’s model provides a framework for assessing vision alone, without consideration of the other sensory systems. When visual-perceptual problems relate to sensory integration (SI) dysfunction, models based on SI theories can guide evaluation and intervention.20 These models consider organization of multisensory systems and the influence of vision as it integrates with other sensory systems.
Vision can be viewed as a dynamic blending of sensory information in which new visual and motor input are combined with previously stored data and then used to guide a reaction. Research demonstrates an expansive interconnectivity of sensory systems.143 Studies of brain activity confirm that when an individual is using the visual system, many areas of the brain are activated. Evidence of full brain activity during visualization supports the concept that vision should be viewed in the totality of all sensory systems.
DEVELOPMENTAL SEQUENCE
As with other areas of development, the development of visual-receptive process and abilities takes place according to a prescribed timetable, which begins in the womb. By gestational week 24, gross anatomic structures are in place, and the visual pathway is complete. Between gestational weeks 24 and 40, the visual system, particularly the retina and visual cortex, undergoes extensive maturation, differentiation, and remodeling.62 As early as the fifth gestational month, eye movements are produced by vestibular influences.43 At birth the infant has rudimentary visual fixation ability and brief reflexive tracking ability. The visual system at this age is relatively immature compared with other sensory systems, and considerable development occurs over the next 6 months.62
Toward the end of the second month, accommodation, convergence, and oculomotor subsystems are established.15 Stereopsis is evident at about 2 months of age; it does not appear to depend on visual recognition and does not need to be taught.160 Maximum accommodation is reached at 5 years of age, and the child should be able to sustain this skill effort for protracted periods at a fixed distance.
Controlled tracking skills progress in a developmental pattern from horizontal eye movements to eye movements in vertical, diagonal, and circular directions. By kindergarten a child should be able to move the eyes with smooth control and coordination in all directions. This can be demonstrated by asking the child to follow with the eyes a moving object located 8 to 12 inches from the child’s face. If the child moves the head as a unit along with the eyes, this skill is still developing. Visual acuity is best at 18 years of age and tends to decline thereafter.
Visual-Cognitive Functions
Vision enables infants to acquire information from multiple locations at a range of distances and is a means for infants to organize information received from their other senses.142 By coordinating visual and auditory input, infants accumulate information as they explore places, events, and individuals in the physical and social environments.137 Some visual-cognitive capacities are present at birth, whereas other higher-level visual-cognitive abilities are not fully developed until adolescence. This development occurs through perceptual learning, the process of extracting information from the environment. Perceptual learning increases with experience and practice and through stimulation from the environment.
Object (Form) Vision
Long before infants can manipulate objects or move around space, they have well-developed visual-perceptual abilities, including pattern recognition, form constancy, and depth perception. Infants as young as 1 week of age show a differential response to patterns, with complex designs and human faces receiving more attention than simple circles and triangles. The infant learns to attend to relevant aspects of visual stimuli, to make discriminations, and to interpret available cues according to experiences. Babies can organize visual information in at least three ways. Perception of brightness emerges first by 2 months of age. By 4 months, most infants can group objects by shape and proximity.49
Visual perception develops as the child matures, with most developmental changes taking place by 9 years of age. However, children vary in the rate at which they acquire perceptual abilities, in their effective use of these capacities, and in the versatility and comfort with which they apply these functions.89
The child first learns to recognize an object based on its general appearance and not by specific details. As the child learns to classify objects into categories and types, it becomes apparent that he or she is able to extract the features that make the object part of that category.108 For example, the child learns to categorize cars as certain types or to classify animals according to their species. Williams estimated the developmental ages when primary visual-perceptual skills develop (Table 12-1).161
TABLE 12-1
Developmental Ages for Emergence of Visual-Perceptual Skills

Modified from Williams, H. (1983). Perceptual and motor development. Englewood Cliffs, NJ: Prentice Hall.
Bouska and colleagues described three areas in which a child demonstrates increasing ability to discriminate visually.15 These areas include (1) the ability to recognize and distinguish specific distinctive features (e.g., that b and d are different because of one feature); (2) the ability to observe invariant relationships in events that occur repeatedly over time (e.g., a favorite toy is the same even when distance makes it appear smaller); and (3) the ability to find a hierarchy of pattern or structure, allowing the processing of the largest unit possible for adaptive use during a particular task (e.g., a map is scanned globally for the shape of a country, but subordinate features are scanned for the route of a river).59 These skills are important for learning to read and write. Justice and Ezell described emergent literacy as comprising two broad yet highly interrelated domains of knowledge: written language awareness and phonologic awareness.79 Written language awareness, also referred to as print awareness,135 describes children’s knowledge of the forms and functions of printed language (e.g., distinctive features of alphabet letters, storybook conventions, environmental signs).
The child’s first perceptions of the world develop primarily from tactile, kinesthetic, and vestibular input. As these three basic senses become integrated with the higher level senses, vision and audition gradually become dominant. Young children or beginning readers tend to prefer learning through their tactile and kinesthetic senses and have lower preferences for visual and auditory learning.26 At 6 or 7 years of age, most children appear to prefer kinesthetic, tactile, visual, and auditory learning, in that order. They learn easily through their sense of touch and whole-body movement and have difficulty learning through listening activities. The predominant reading style of primary grade children and struggling readers is global, tactile, and kinesthetic.26 Global reading methods (i.e., recorded stories, shared reading) start with a modeled story, practice words from the story, and teach phonics skills. This differs from analytic reading methods (e.g., phonics) that teach sounds letters make, then practice words containing the sounds taught, and proceed to stories. Tactile learners recall what they touch, are often doodlers, and learn better when they can touch or manipulate objects (such as a reading game). Kinesthetic learners recall what they experience and learn when engaged in physical activity (e.g., acting in plays, floor games, building models).27
Research shows that struggling readers prefer and do better in classrooms that allow for movement, have some comfortable seating and varied lighting, and enable students to work with relevant ease in different groupings.44 Research indicates that when the student’s environmental preferences are met, they are more likely to associate reading with pleasure, to read for longer periods, and overall read at higher levels.44 Generally, boys are less auditory and verbal and remain kinesthetic longer than girls. Around third grade most children become highly visual, and not until fifth grade do many children learn well through their auditory sense. However, it is important to remember that reading style strengths and preferences develop at different times and rates.26
In the young child, visual discrimination of forms precedes by years the visual-motor ability to copy forms. Throughout elementary school, the child assimilates more internal detail of figures and develops greater ability to understand, recall, and recreate such configurations. Children begin to use simultaneous and sequential data to develop strategies, and cognitive or learning styles begin to emerge. In addition, children learn best through their dominant sensory input channel. About 40% of school-age children remember visually presented information, whereas only 20% to 30% recall what is heard.25
Information processing in the visual-perceptual–motor domain has been identified as one of the major factors that predict readiness for the first grade. There is evidence that the child who enters school with delayed perceptual development may not catch up with his or her peers in academic achievement.52 Of the children who have difficulty reading in first grade, 88% have difficulty reading at the end of fourth grade.78 Adequate perceptual discrimination is considered necessary for the development of the literacy skills of reading and writing.86,136 An important aspect of developing early literacy is termed alphabetics. This includes phonemic and phonologic awareness, letter recognition, print awareness, and phonics. Letter recognition/identification, defined as knowing the names of the letters of the alphabet, supports reading acquisition. Measures of the ability to name letters have been shown to be predictors of reading development, especially when letter naming is taught in conjunction with other beginning reading skills. Print awareness refers to knowledge or concepts about print, such as the following: (1) print carries a message; (2) there are conventions of print such as directionality (left to right, top to bottom), differences between letters and words, distinctions between upper and lower case, punctuation; and (3) books have some common characteristics (e.g. author, title, front/back). It has been shown that print awareness supports reading acquisition (e.g., decoding). Occupational therapists are not primarily responsible for teaching students to read or write but may address many of the performance skills to support student literacy outcomes.8
Children gradually develop the abilities to attend to, integrate, sort, and retrieve increasingly larger chunks of visual data. These stimuli from the environment usually arrive for processing either in a simultaneous array or in a specific serial order.89 An example of simultaneous processing involves observing and later trying to recall what someone wore.
Sequential processing involves the integration of separate elements into groups, where the elements have a specific arrangement in time with each element leads only to one other. Sequential processing enables the child to perceive an ordered series of events.60 An example of sequential processing is the visual information provided in the written instructions for assembling a plastic model. An effective learner in the classroom needs to be able to evaluate, retain, process, and produce both simultaneous and sequential packages of information or action. In addition, children must learn to analyze and synthesize material containing more detail at a faster rate.
In adolescence, perceptual skills are enhanced by their interrelationship with expanding cognitive skill. Thus the adolescent can imagine, create, and construct complex visual forms. The adolescent is able to manipulate visual information mentally to solve increasingly complex problems, formulate plans, and make decisions. Of the children who are poor readers at the end of third grade, 75% remain poor readers in high school.131 Teenager rites of passage such as obtaining a driver’s license or independent dating may be challenging or impossible for an individual with severe visual-perceptual deficits.
Spatial Vision
In the developmental process of organizing space, the child first acquires a concept of vertical dimensions, followed by a concept of horizontal dimensions. Oblique and diagonal dimensions are more complex, and perception of these spatial coordinates matures later. A 3- to 4-year-old child can discriminate vertical lines from horizontal ones, but children are unable to distinguish oblique lines until about 6 years of age.37 The ability to discriminate between mirror- or reverse-image numbers and letters, such as b and d, and p and q, does not mature in some children until around 7 years of age.75
The child develops an understanding of left and right from the internal awareness that his or her body has two sides140; this understanding of left and right, called laterality, proceeds in stages. A child’s awareness of his or her own body is generally established by 6 or 7 years of age. Before 7 years of age, a child is not yet ready to handle spatial concepts on a strictly visual basis. The child must relate them to his or her own body.
Around the eighth year the child begins to project laterality concepts outside himself or herself. The child then develops directionality, or the understanding of an external object’s position in space in relation to himself or herself. This allows the child to handle spatial phenomena almost exclusively in a visual manner. By sensing a difference between body sides, the child becomes aware that figures and objects also have a right and a left. The child “feels” this visually.
Directionality is thought to be important in the visual discrimination of letters and numbers for both reading and writing. The child first learns these concepts in relation to himself or herself and then transfers them to symbols and words.
Role of Vision in Social Development
The importance of vision in facilitating infants’ participation in social interactions has been widely recognized.99 Facial expressions are an important way to communicate emotions.76 Infants respond to attentive, social initiations from their parents by visually focusing on their parents’ eyes, smiling, and occasionally shifting gaze to scan their parents’ faces and the environment. Mutual gaze between parents and infants facilitates emotional attachment. Adults’ facial expressions appear to be the major driving force during social interactions with infants younger than 6 months. Infants discriminate between happy and sad facial expressions by 3 months of age. Toward the end of the first year an infant can shift attention from one person to another person, or to an object of mutual interest in joint attention paradigms.42 Social imitation then shifts from simple reactions to another person’s facial expressions to imitations of another person’s actions with objects. Toddlers will imitate a peer’s action on an object, but only when identical objects are available.
VISUAL-PERCEPTUAL PROBLEMS
The importance of good vision for classroom work cannot be overemphasized. More than 50% of a student’s time is spent working at near-point visual tasks such as reading and writing. Another 20% is spent on tasks that require the student to shift focus from distance to near and near to distance, such as copying from the board. For more than 70% of the day, therefore, tremendous stress is put on the visual system.115 Many students with visual dysfunction may have difficulty meeting the behavioral demands of sitting still, sustaining attention, and completing their work. Academic instruction in the first years places great demand on the child’s visual processing skills, with emphasis on recognition, matching, and recall. In early elementary grades, periods of sustained near work are infrequent, and visual stimuli (letters) are relatively large and widely spaced.
Visual efficiency becomes a more significant need in later elementary grades, middle school, and high school. Letters and text become smaller and more closely spaced and reading requires more comprehension effort for extended periods of time. Students visually attend for sustained periods of near work.102
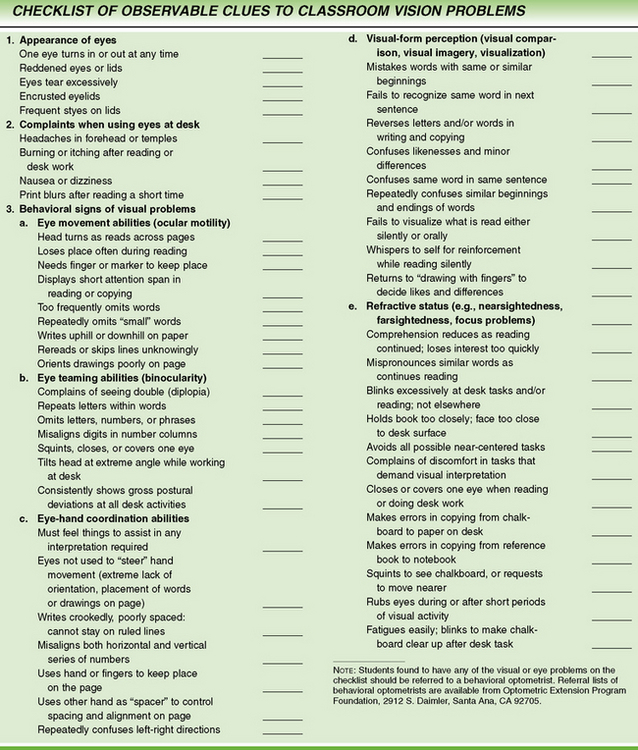
Learning-related vision problems represent deficits in two broad visual system components: visual efficiency and visual information processing.13 Figure 12-3 presents a sample list of behaviors noted in children with specific visual problems.102 In addition, individuals with functional vision problems may exhibit56:
• Difficulty completing school tasks in a timely manner
• Adaptation of the visual system through the development of a refractive error to perform near-centered visual tasks
• Distraction or inattention as a secondary problem, thus decreasing the opportunity for practice and learning
Impairment of oculomotor control can occur through disruption of cranial nerve function or disruption of central neural control. The pattern of oculomotor dysfunction depends on the areas of the brain that have been injured and the nature of the injury.88 Oculomotor problems can limit the ability to control and direct gaze. In addition, when large amounts of energy must be used on the motor components of vision, little energy may be left for visual-cognitive processing.72 Warren157 and Scheiman125 present detailed descriptions of oculomotor deficits and other deficits seen in visual-receptive components.
At least 20% of students with learning disabilities have been found to have prominent visual information–processing problems. The prevalence of visual efficiency problems in children with learning disabilities is thought to be in the 15% to 20% range.126 Accommodative disorders have been reported in 60% to 80% of individuals with visual efficiency problems; accommodative insufficiency is the most prevalent type.102 Convergence insufficiency is the most common convergence anomaly.
Refractive Errors
A child who is nearsighted has blurred distant vision but generally experiences clarity at near point. The child who is farsighted frequently has clear distant and near vision but has to exert extra effort to maintain clear vision at near point. The child with astigmatism experiences blurred vision at distance and near, with the degree of loss of clarity depending on the severity of the astigmatism. Measures of visual acuity alone do not predict how well children interpret visual information.72 Other determinants include the ability to see objects in low-contrast lighting conditions, the ability of the eye to adapt to different lighting conditions, visual field problems, accommodation, and other oculomotor functions.72,74
If accommodation takes longer than previously described, words appear blurry and the child tends to lose his or her place, missing important information and understanding. When accommodation for near objects is poor, presbyopia exists; this individual is described as farsighted.
If the conditions of motor fusion and sensory fusion have not been met, allowing binocular fusion to occur (this process was described previously), single binocular vision is at best difficult and at worst impossible. If one eye overtly turns in, out, up, or down because of muscular imbalance, the condition is known as strabismus, sometimes referred to as a crossed or wandering eye. This can result in double vision or mental suppression of one of the images. This, in turn, can affect the development of visual perception. Some children have surgery to correct an eye turn. Although this intervention can correct the eye cosmetically, it does not always result in binocular vision.
Another type of binocular dysfunction is called phoria. Phoria refers to a tendency for one eye to turn slightly in, out, up, or down, but overt misalignment of the two eyes is absent. Phoria requires the child to expend additional mechanical effort to maintain motor fusion of the two eyes, whether focusing near or far. The extra effort frequently detracts from the child’s ability to process and interpret the meaning of what he or she sees.
Visual-Cognitive Functions
The integrity of the attention system is considered to be a prerequisite for higher cognitive functions. To review, visual attention is composed of alertness, selective attention, vigilance, and shared attention. If the child’s state of alertness or arousal is impaired, the child may demonstrate behaviors of overattentiveness, underattentiveness, or poor sustained attention.144 Children who are overattentive may be compelled to respond to visual stimuli around them rather than attend to the task at hand, may be easily distracted by visual stimuli, and may demonstrate continual visual searching behaviors. Children who are underattentive may have difficulty orienting to visual stimuli, may habituate quickly to a visual stimulus, and may fatigue easily. At this level a child may refrain from attending to a familiar stimulus. A child with poor sustained attention may demonstrate a high activity level and may be easily distracted.
Selective attention is the next level of visual attention, and a child with difficulty in this area demonstrates a reduced ability to focus on a visual target. The child may have difficulty screening out unimportant or irrelevant information and may focus on or may be distracted by irrelevant stimuli. A child with difficulty in selective attention is easily confused. The child may focus on unnecessary tasks or information and therefore not obtain the specific information needed for the task. Selective attention is critical for encoding information into memory and successfully executing goal-directed behavior.
A child with reduced vigilance skills shows reduced persistence on a visual task and poor or cursory examination of visual stimuli. The child cannot maintain visual attention. The more complex the visual structure of an object, the lengthier the process of visual analysis and the greater the vigilance skills needed. Impaired sustained attention is associated with error awareness95 as well as with working memory to hold and manipulate information.133 A child with deficits in shared attention can focus well only on one task at a time. He or she may be easily confused or distracted if required to share visual attention between two tasks.
Enns and Cameron suggested that visual inattention is the result of an inability to select the features that differentiate objects in a visual array.48 The child cannot see, recognize, or isolate the salient features and therefore does not know where to focus visual attention. Luria suggested that problems of visual recognition represent a breakdown of the active feature by feature analysis necessary for interpretation of a visual image.92 The current psychological literature focuses on such constructs as mental resource, automaticity, and stimulus selection.3 The research focuses on the attention demands that numerous competing stimuli make on individuals with a limited capacity to process those stimuli and on the fact that these exteroceptive stimuli can be processed either with awareness (i.e., effortful processing) or automatically (i.e., effortless processing).
Memory
The child with visual memory deficits has poor or reduced ability to recognize or retrieve visual information and to store visual information in short- or long-term memory. The child may fail to attend adequately, may fail to allow for storage of visual information, or may show a prolonged response time. The child may demonstrate the inability to recognize or match visual stimuli presented previously because he or she has not stored this information in memory, or the child may be unable to retrieve it from memory.144 The child may have good memory for life experiences but not for factual material and may fail to relate information to prior knowledge. He or she may demonstrate inconsistent recall abilities and poor ability to use mnemonic strategies for storage.
Visual sequential memory problems are seen when the child has difficulty recalling the exact sequence of letters, numbers, symbols, or objects. Visual spatial memory deficits are seen when the child has difficulty recalling the spatial location of a previously seen stimulus and is unable to identify or reproduce it.
Visual Discrimination
The child with poor discrimination abilities may demonstrate impaired ability to recognize, match, and categorize. Ulman proposed that a finite set of visual operations, or routines, are performed to extract shape properties and spatial relationships.152 Usually an individual recognizes an object by orienting to its top or bottom. A child with poor matching skills may demonstrate difficulty matching the same shape presented in a different spatial orientation or may confuse similar shapes. A child with poor matching skills also may have difficulty recognizing form in a complex field.
Object (Form) Vision: Children with form constancy problems may have difficulty recognizing forms and objects when they are presented in different sizes or different orientations in space or when differences in detail exist. This interferes with the child’s ability to organize and classify perceptual experiences for meaningful cognitive operations.106 This may result in difficulty recognizing letters or words in different styles of print or in making the transition from printed to cursive letters.
A child with a visual closure deficit may be unable to identify a form or object if an incomplete presentation is made; the child therefore would always need to see the complete object to identify it. For example, a child would have difficulty reading a sign if the letters were partly occluded by tree branches.
The child with figure-ground problems may not be able to pick out a specific toy from a shelf. He or she also may have difficulty sorting and organizing personal belongings. The child may overattend to details and miss the big picture or may overlook details and miss the important information. Children with figure-ground problems may have difficulty attending to a word on a printed page because they cannot block out other words around it. The child with figure-ground difficulties may not have good visual search strategies. Marr suggested that control of the direction of gaze is a prerequisite for efficiency of visual search.93 Cohen described the following visual search strategies34:
1. The viewer looks for specific visual information and makes crude distinctions between figure and ground by isolating one figure from another.
2. The viewer determines which figures are most meaningful (the process stops here when recognition is immediate).
3. When recognition is not immediate, the viewer makes a hypothesis about the visual information received and directs attention to selected items to test the hypothesis.
Rogow and Rathwill found that good readers more frequently proceeded from the left to the right and from the top down to find “hidden figures” than did poor readers.117 Good readers were also more flexible in their approach; they rotated the page as needed and were not content until they found as many hidden figures as possible. The good readers also were less distressed by ambiguity, and they understood that pictures could be viewed in different ways.
Spatial Vision: A child with position in space difficulty has trouble discriminating among objects because of their placement in space. These children also have difficulty planning their actions in relation to objects around them and may show delayed gross motor skills. They may show letter reversals in writing or reading past 8 years of age and may show confusion regarding the sequence of letters or numbers in a word or math problem (e.g., was/saw). Writing and spacing letters and words on paper may be a problem. The children may show difficulty understanding directional language such as in, out, on, under, next to, up, down, and in front of. They may show inconsistent directional attack when reading.
Decreased depth perception can affect the child’s ability to walk through spaces and to catch a ball. The child may be unable to determine visually when the surface plane has changed and may have difficulty with steps and curbs. Transference of visual-spatial notations across two visual planes can make copying from the blackboard difficult. Faulty interpretation of the spatial relationships can contribute to a problem with sorting and organizing personal belongings. The child may show confusion in right and left.
A child who has diminished topographic orientation may be easily lost and unable to find his or her way from one location to the next. The child may also demonstrate difficulty determining the location of objects and settings and may not recognize the images that help people find their way around the environment.46 The child may be unable to walk from home to school without getting lost.
Diagnoses with Problems in Visual Perception
When children with disabling conditions have visual problems, the effects of the visual impairments can be tremendous. Numerous studies have found a high frequency of vision problems among individuals with disabilities.32 Severe refractive errors are common among children with developmental problems,117 and impaired visual attention can have a pervasive negative influence on the functional behavior of these children. Often considered distractible, these children may be able to locate objects but have difficulty sustaining eye contact or recognizing objects visually.117
Retinopathy of prematurity (ROP) is the single most cited cause of blindness in preterm infants. However, the number of infants with ROP has declined in past 25 years because of changes in medical interventions for premature infants.136 Cortical visual impairment also occurs in preterm infants and is generally associated with severe CNS damage, such as periventricular leukomalacia. Other visual disorders common in preterm children include lenses that are too thick, poor visual acuity, astigmatism, extreme myopia, strabismus, amblyopia, and anisometropia (unequal refraction of the eyes).5 These children also have difficulty processing visual information. Scores for visual attention, pattern discrimination, visual recognition, memory, and visual-motor integration are lower than those for full-term infants.29,120,132 Studies of older children suggest that these problems often persist.117
Children with developmental disabilities commonly have a coexisting diagnosis of blindness or other visual impairment. These children also may have sensory integrative deficits that further complicate their functional abilities.119
Children with cerebral palsy (CP) frequently have been identified as a group with visual-perceptual deficits.17,21 Children with CP often have a strabismus, oculomotor problems, convergence insufficiencies, or nystagmus. These problems may also limit the ability to control and direct visual gaze.117
Early research indicated that the degree of perceptual impairment in individuals with CP was related to the type and severity of the motor impairment.10 In a comparison study, children with CP scored significantly lower on a motor-free test of visual perception than typical children.96 These findings supported earlier studies that showed that a group of children with spastic quadriplegia demonstrated the greatest problems in visual perception. Children with left hemiplegia scored significantly lower than control children on motor-free visual tests, but children with right hemiplegia did not.21
In children with language delay, poorly developed visual perception may contribute to the language difficulties. For example, language moves from the general to the specific. Young children call every animal with four legs a dog. Eventually they are able to discriminate visually between dogs and lions, and the vocabulary follows the visual-perceptual lead. Next, they can tell Dalmatians from Dachshunds, but they are unable to recognize that both are dogs. Finally, the ability to categorize and generalize emerges somewhere between 7 and 9 years of age. In addition, the child who has visual-spatial perception deficits may show difficulty understanding directional language, such as in, on, under, and next to.
Visual-perceptual problems are found more frequently in individuals who have significantly higher verbal scores than performance scores on intelligence testing. Not all children with learning disabilities have visual-perceptual problems.70 A recent study suggests that early brain damage can give rise to specific visual-perceptual deficits, independent of, although occurring in association with, selective impairment in nonverbal intelligence.138
Children with learning disabilities may have difficulty filtering out irrelevant environmental stimuli and therefore have erratic visual attention skills. Children who have difficulty interpreting and using visual information effectively are described as having visual-perceptual problems because they have not acquired adequate visual-perceptual skills despite having normal vision.144 Children with developmental coordination disorder (DCD) obtained significantly lower scores compared with typically developing children on a motor-free test of visual perception.147 Although group differences were statistically significant, some of the children with DCD did not have general visual-perceptual dysfunction.
Dyslexia is best understood as a neurocognitive deficit that is specifically related to reading and spelling processes. Dyslexia can occur for two different reasons. One cause is that the reader has difficulty decoding words (single word identification) and encoding words (spelling).132 A second reason for dyslexia is that the reader makes a significant number of letter reversals (b – d), letter transpositions in words when reading or writing (sign – sing) or has right-left confusion.66
Daniels and Ryley studied the incidence of visual-perceptual and visual-motor deficits in children with psychiatric disorders.39 In their study, deficits in visual-motor skills occurred far more frequently than deficits in visual-perceptual skills. When visual-perceptual problems occurred, they did so in conjunction with visual-motor skill problems.
Some children with autism have demonstrated poor oculomotor function.121 Children with autism often do not appear to focus their vision directly on what they are doing.103 A possible explanation is that they use peripheral vision to the exclusion of focal vision. One study found that children with autism spend the same amount of time inspecting socially oriented pictures, have the same total number of fixations, and have scan path lengths similar to those of typically developing children.153 These results do not support the generally held notion that children with autism have a specific problem in processing socially loaded visual stimuli. The study authors suggested that the often-reported abnormal use of gaze in everyday life is not related to the nature of the visual stimuli, but that other factors, such as social interaction, may play a role.
Effects of Visual-Perceptual Problems on Performance Skills and Occupations
The effects of visual-perceptual problems may be subtle. However, when the child is asked to perform a visual-perceptual task, he or she may be slow or unable to perform it. Because visual-perceptual dysfunction affects the child’s ability to use tools and to relate materials to one another,4 bilateral manipulative skills are affected to a greater degree than the child’s basic prehension patterns indicate. The child with visual-perceptual deficits may show problems with cutting, coloring, constructing with blocks or other construction toys, doing puzzles, using fasteners, and tying shoes. Visual perception deficits also can influence children’s areas of occupation, such as activities of daily living (ADLs), education, work, play, leisure, and social participation.
Children with visual-perceptual problems may demonstrate difficulty with ADLs. In grooming, the child may have difficulty obtaining the necessary supplies and using a brush and comb and mirror to comb and style the hair. Applying toothpaste to the toothbrush may be difficult for the child. Using fasteners; donning and doffing clothing, prostheses, and orthoses; tying shoes; and matching clothes may present problems. Skilled use of handwriting, telephones, computers, and communication devices may present difficulty for the child with visual-cognitive problems. Instrumental ADLs, such as home management, may present problems. For example, the child may have trouble sorting and folding clothes. Community mobility may be difficult because the child is unable to locate objects and find his or her way. In play, the child may demonstrate difficulty with playing games and sports, drawing and coloring, cutting with scissors, pasting, constructing, and doing puzzles.
Classroom assignments may present problems for the child with visual-perceptual problems. He or she may have difficulty with educational activities such as reading, spelling, handwriting, and math. The educational problems seen in the school-aged child are considered in some detail next. Visual processing deficits are considered developmental. With maturation and experience the performance of the child with deficits improves, but the rate of maturation of skill continues to lag.
Problems in Reading
The role of phonologic processing deficits in the understanding of reading disability is significant.146 These deficits are manifested in the failure to use or properly understand phonologic information when processing written or oral language. This is seen in the inadequacy of phonemic awareness, the poor understanding of sound-symbol correspondence rules, and the improper storage and retrieval of phonologic information. Deficits in short- and long-term memory can also affect comprehension.
At least a subgroup of children with reading problems confuses orientation and visual recognition of letters.161 The characteristics of printed (written) information make reading possible; these include a word’s graphic configuration, orthography (order of letters), phonology (sounds represented), and semantics (meaning). The child benefits from these multiple simultaneous cues in reading. If the child has difficulty with one characteristic, he or she can rely on perception of the other characteristics to extract the meaning. In early reading, children first encounter the visual configuration (graphics) and orthographics of a printed word. The child then must break the written word into its component phonemes (phonology), hold them in active working memory, and synthesize and blend the phonemes to form recognizable words (semantics). Visual word recognition seems to involve a subphonemic level of processing.91 After practice, this step is accomplished and the word then can be dealt with as a gestalt or in its entirety rather than letter by letter and added to the child’s growing sight vocabulary. Sight vocabulary consists of words that are instantly recognized as gestalts. As the child’s reliance on sight vocabulary increases, decoding takes less time and automaticity develops, which allows the child to begin to concentrate on comprehension and retention.
Understanding sentences requires adding two more variables, context (word order) and syntax (grammatical construction), to the skills previously discussed.90 For reading paragraphs, chapters, and texts, it is assumed that decoding is automatic. A hierarchy can be assumed such that any developmental dysfunctions that impair decoding or sentence comprehension impede text reading.
The segmenting of written words in early reading calls for a variety of skills. First, children must be able to recognize individual letter symbols. This requires visual attention, visual memory, and visual discrimination. Two aspects of word reading are important for comprehension: accuracy and speed. The more attentional resources are consumed by lower level process (i.e., word identification), the fewer resources are available for comprehension.
Letter knowledge contributes significantly to reading and should be measured in preschool, kindergarten, and first grade. The prerequisite skills of letter naming and phonemic awareness should be assessed early in kindergarten.
Visual-perceptual attributes are different from the capacity to assimilate visual detail. The child may be diagnosed as having visual-perceptual problems when he or she is limited in attending to or extracting data presented simultaneously. In this instance the child does not have difficulty with the specific perceptual content but with the amount of information that must be simultaneously perceived to understand the whole.
Children with visual discrimination deficits may not be able to recognize symbols and therefore may be slow to master the alphabet and numbers. Their relatively weak grasp of constancy of forms may make visual discrimination an inefficient process. Some children cannot readily discern the differences between visually similar symbols. Confusion between the letters p, q, and g and between a and o, as well as letter reversals, may result, such as the notorious differentiation between b and d. A meta-analysis was conducted using 161 studies to examine the relationship between visual-perceptual skills and reading achievement.83 The findings suggest that visual perception is an important correlate of reading achievement and should be included in the complex of factors predicting it. Visual discrimination abilities (form perception and spatial perception) are somewhat less important at advanced stages of the learning-to-read process than they are during the initial stages of reading acquisition.16
Confusion over the directionality and other spatial characteristics of a word may result in weak registration in visual memory, again possibly causing significant delays in the consolidation of a sight vocabulary. Even frequently encountered words need to be analyzed anew each time they appear. A child with visual-spatial deficits has difficulty with map reading and interpretation of instructional graphics such as charts and diagrams. Graphic representations require the child to integrate, extract the most salient elements from, condense, and organize the large amount of stimuli presented at once. Again, the child may not have difficulty with the perceptual content, but the amount of information to be assimilated simultaneously is more than the child can integrate and remember.90
Memory deficits affect reading in a number of ways. Children with visual memory problems may be unable to remember the visual shape of letters and words. Such children may also demonstrate an inability to associate these shapes with letters, sounds, and words.65 Children with weaknesses of visual-verbal associative memory have difficulty establishing easily retrievable or recognizable sound-symbol associations. They are unable to associate the sound, visual configuration, or meaning of the word with what is seen or heard. Children who have difficulty with active working memory also may have difficulty holding one aspect of the reading process in suspension while pursuing another component. This ability is closely related to perceptual span, or the ability to recall the beginning of the sentence while reading the end of it. The child must take a second look at the beginning of a sentence after reading the end of it.
With severe dysfunction, recognition of words may be impaired,90 which interferes with the acquisition of sight vocabulary. Problems with visual perception might be suspected in a child who appears to be better at understanding what was read than at actually decoding the words. This child has good language abilities but some trouble processing written words.
According to Raymond and Sorensen, children with dyslexia have been shown to have normal detection but abnormal integration of visual-motion perception.111 The authors suggest that perhaps a collection of inefficient information-processing mechanisms produces the characteristic symptoms of dyslexia.
Problems in Spelling
Research by Giles and Terrel does not support the hypothesis that proficient spelling is mediated by visual memory.60 They suggest that spelling skills may depend on be visual recognition or visual imagery ability. Children with impaired processing of simultaneous visual stimuli may have difficulty with spelling. Their inability to visualize words may result from indistinct or distorted initial visual registration. Such children who have strong sound-symbol association may spell the word phonetically (e.g., lite for light) yet incorrectly.
Problems in Handwriting and Visual Motor Integration
Handwriting requires the ability to integrate the visual image of letters or shapes with the appropriate motor response. Handwriting difficulties affect between 10% to 30% of school-age children. Visual-cognitive abilities may affect writing in a variety of situations. Children with problems in attention may have difficulty with correct letter formation, spelling and the mechanics of grammar, punctuation, and capitalization. They also have difficulty formulating a sequential flow of ideas necessary for written communication. For a child to write spontaneously, he or she must be able to revisualize letters and words without visual cues. A child with visual memory problems may have difficulty recalling the shape and formation of letters and numbers. Other problems seen in the child with poor visual memory include mixing small and capital letters in a sentence, writing the same letter many different ways on the same page, and being unable to print the alphabet from memory. In addition, legibility may be poor, and the child may need a model to write.
Visual discrimination problems may also affect the child’s handwriting. The child with poor form constancy does not recognize errors in his or her own handwriting. The child may be unable to recognize letters or words in different prints and therefore may have difficulty copying from a different type of print to handwriting. The child may also show poor recognition of letters or numbers in different environments, positions, or sizes. If the child is unable to discriminate a letter, he or she may have difficulty forming it. A child with visual-closure difficulty always needs to see the complete presentation of what he or she is to copy. A child with figure-ground problems may have difficulty copying because he or she is unable to determine what is to be written; the child therefore may omit important segments or may be slower than peers in producing written products.
Visual-spatial problems can affect a child’s handwriting in many ways. The child may reverse letters such as m, w, b, d, s, c, and z and numbers such as 2, 3, 5, 6, 7, and 9. If the child is unable to discriminate left from right, he or she may have difficulty with left–to-right progression in writing words and sentences. The child may overspace or underspace between words and letters and may have trouble keeping within the margins. The most common spatial errors in handwriting involve incorrect and inconsistent spacing between writing units, and variability in orientation of major letter features when the letter is written repeatedly.155 When a child has a spatial disability, he or she may be unable to relate one part of a letter to another part and may demonstrate poor shaping or closure of individual letters or a lack of uniformity in orientation and letter size.163 The child may have difficulty placing letters on a line and adapting letter sizes to the space provided on the paper or worksheet. Pilot studies have begun to explore the relationship between visual-cognitive skills and handwriting.164 Tseng and Cermak found that visual perception shows little relationship to handwriting, whereas kinesthesia, visual-motor integration, and motor planning appear to be more closely related to it.148 Further research is necessary to better understand the role of visual perception in handwriting.
Failure on visual-motor tests may be caused by underlying visual-cognitive deficits, including visual discrimination, poor fine motor ability, or inability to integrate visual-cognitive and motor processes, or by a combination of these disabilities. Therefore, careful analysis is necessary to determine the underlying problem. Tseng and Murray examined the relationship of perceptual-motor measures to legibility of handwriting in Chinese school-age children.149 They found visual-motor integration to be the best predictor of handwriting. Weil and Cunningham-Amundson studied the relationship between visual-motor integration skills and the ability to copy letters legibly in kindergarten students.159 A moderate correlation was found between students’ visual-motor skills and their ability to copy letters legibly. The researchers found that as students’ scores on the Developmental Test of Visual-Motor Integration (VMI) increased, so did scores on the Scale of Children’s Readiness in PrinTing (SCRIPT). Also, students who were able to copy the first nine forms on the VMI were found to perform better on the SCRIPT. Daly, Kelley, and Krauss partly replicated the Weil and Cunningham-Amundson study and found a strong positive relationship between kindergarten students’ performance on the VMI and their ability to copy letter forms legibly.38 They suggest that students are ready for formal handwriting instruction once they have the ability to copy the first nine forms on the VMI.
Extensive research on the relationship between visual-motor integration and handwriting skills has been completed. Studies of handwriting remediation suggest that intervention is effective. There is some evidence that handwriting difficulties do not resolve without intervention.51
Problems in Mathematics
Poor visual-perceptual ability is significantly related to poor achievement in mathematics, even when controlling for verbal cognitive ability. Therefore, visual perceptual ability, and particularly visual memory, should be considered to be among the skills significantly related to mathematics achievement.85 Consequently, visual-perceptual ability, and particularly visual memory skill, should be assessed in children with poor achievement in mathematics. The child with visual-perceptual problems can have difficulty aligning columns for calculation, and answers therefore are incorrect because of alignment problems and not calculation skills. Worksheets with many rows and columns of math problems may be disorienting to children with figure-ground problems. Children with poor visual memory may have difficulty using a calculator. Visual memory difficulties also may present problems when addition and subtraction problems require multiple steps. Geometry, because of its spatial characteristics, is very difficult for the child with visual-spatial perception problems. Recognition, discrimination, and comparison of object form and space are part of the foundation of higher-level mathematic skills. The visual imagery required to match and compare forms and shapes is difficult for students with visual-perceptual problems, which interfere with their ability to learn these underlying skills.
A longitudinal investigation that studied the relationship of sensory integrative development to achievement found that sensory integrative factors, particularly praxis, were strongly related to arithmetic achievement.102 This relationship was found at younger ages (6 to 8 years), and the strength of the association declined with age (10 to 12 years).
EVALUATION METHODS
Evaluation of visual-perceptual functions requires the therapist to consider the entire process of vision and examine the relationship of visual function to behavior and performance.129 Visual-receptive and visual-cognitive components may represent different issues in a child’s school performance. Problems can and do exist in either area, with differing effects on the learning process. However, visual-receptive components can influence the information obtained for visual-cognitive analysis. Because receptive and cognitive components are important in the visual processing of information, assessment of each child should be conducted using an interdisciplinary approach, recognizing that the interplay of visual-receptive abilities, visual-cognitive skills, and school success is different for each child.
Reports generated by other educational or medical specialists often provide standardized measures of performance. Securing this information often eliminates the need for the occupational therapist to spend time administering additional visual-motor or visual-perceptual tests that yield the same information. This information also can help the occupational therapist select alternative measures that yield different data that could further help in understanding a child’s problem. An interview with the teacher or classroom observation should be a major component of the assessment process. For example, information on visual stimulation in the classroom, which could affect the child’s attention and focus, should be determined. The therapist might also determine whether most visual work for copying is done at near point or far point. The child’s parents also should be interviewed, and they should be included as part of the team in the diagnosis and treatment of the child.
Through the interdisciplinary approach, the occupational therapist’s findings can be integrated with those of the reading specialist, psychologist, speech-language pathologist, parent, and classroom teacher. By combining test results and analysis of the child’s performance, the team members ascertain the nature of the interaction of the disability with the activity. A vision specialist, such as an ophthalmologist or an optometrist, may be needed to assess visual-receptive dysfunction and to remediate the condition.
Evaluation of Visual-Receptive Functions
Evaluation should begin by focusing on the integrity of the visual-receptive processes, including visual fields, visual acuity, and oculomotor control.158 In children who have deficits in these foundational skills, insufficient or inaccurate information about the location and features of objects is sent to the CNS, and the quality of their learning through the visual sense is severely affected. Warren suggested that what sometimes appear to be visual-cognitive deficits are actually visual-receptive problems, which may include oculomotor disturbances.156 Therefore, visual-receptive and visual-cognitive deficits may be misdiagnosed. The occupational therapist should be familiar with visual screening, because evaluation of vision and oculomotor skills assists in the assessment and analysis of their influence on visual perception and functional performance.144
Visual screening consists of basic tests administered to determine which children are at risk for inadequate visual functions.15,72 The purpose of the screening is to determine which children should be referred for a complete diagnostic visual evaluation. Therefore, the purpose of screening the visual-receptive system is to determine how efficient the eyes are in acquiring visual information for further visual-cognitive interpretation. The checklist presented in Figure 12-3 can alert the therapist to visual symptoms commonly found in children who demonstrate poor visual performance.
Perimetry (computerized measurement of visual field by systematically showing lights of differing brightness and size in the peripheral visual field), confrontation, and careful observation of the child as he or she performs daily activities provide useful information about field integrity.165 For example, missing or misreading the beginning or end of words or numbers may indicate a central field deficit.
The child’s refractive status, which is the clinical measurement of the eye, should be determined. A school nurse or vision specialist usually performs this test. The refractive status reflects whether the student is nearsighted (myopic), farsighted (hyperopic), or has astigmatism. Several methods can be used to determine a child’s refractive status. One method, the Snellen test, is used to screen children at school or in the physician’s office. However, it measures only eyesight (visual acuity) at 20 feet. This figure, expressed commonly as 20/20 for normal vision, has little predictive value for how well a child uses his or her vision. It is estimated that the Snellen Test detects fewer than 5% of visual problems.129 When a child passes this screening, he or she may be told that the existing vision is fine. However, it is only the eyesight at 20 feet that is fine.
Some schools and clinics use a Telebinocular or similar instrument in vision screening. This device provides information on clarity or visual acuity at both near and far distances, as well as information on depth perception and binocularity (two-eyed coordination). Warren suggested that the Contrast Sensitivity Test is best for measuring acuity.158 A pediatric version of this test is available (Vistech Consultants, Dayton, Ohio).
The occupational therapist may observe oculomotor dysfunction in the child. The screening test should answer several questions, including the following73,165:
1. Do the eyes work together? How well?
2. Where is visual control most efficient and effective? Least efficient and effective?
3. What types of eye movements are quick and accurate? Which are not?
4. Does the child move his head excessively when reading? Skip lines when reading?
Screening tools that can be used by occupational therapists are presented in Table 12-2.
TABLE 12-2
| Test | Authors | Description |
| Visual Screening | Bouska, Kauffman, & Marcus (1990)15 | Comprehensive screening test of distance and near vision, convergence near point, horizontal pursuits, distant and near fixations, and stereoscopic visual skills to identify children who should be referred to a qualified vision specialist for a complete diagnostic visual evaluation. |
| Sensorimotor Performance Analysis | Richter & Montgomery (1991)* | Assessment of visual tracking, visual avoidance, visual processing, and hand-eye coordination during gross and fine motor tasks. |
| Pediatric Clinical Vision Screening for Occupational Therapists | Scheiman (1991)† | A test that screens accommodation, binocular vision, and ocular motility. |
| Clinical Observations of Infants | Ciner, Macks, & Schanel-Klitsch (1991)32 | Description methods for testing vision in early intervention programs. |
*Richter, E., & Montgomery, P. (1991). The sensorimotor performance analysis. Hugo, MN: PDP Products.
†Scheiman, M. (1991). Pediatric clinical vision screening for occupational therapists. Philadelphia: Pennysylvania College of Optometry.
In addition, the child’s ocular health should be evaluated. The presence of a disease or other pathologic condition, such as glaucoma, cataracts, or deterioration of the nerves or any part of the eye, must be ruled out. An interview with the family regarding significant visual history helps identify any conditions that may be associated with visual limitations. This information can also be obtained from a review of the child’s records and from consultation with other professionals involved in direct care of the child (e.g., teacher or physician).
When visual problems are detected in screening, the child may be referred to a vision specialist such as an optometrist. The specialist can help determine whether the child has a visual problem that might be causing or contributing to school difficulties. The therapist then will be able to understand the effect those deficits have on function and can devise intervention strategies by designing and selecting appropriate activities that are within the child’s visual capacity.15
Evaluation of Visual-Cognitive Functions
Clinical evaluation and observation may be the occupational therapist’s most useful assessment methods. The therapist should observe the child for difficulty selecting, storing, retrieving, or classifying visual information. Observations may include visual search strategies used during visual-perceptual tasks (e.g., outside borders to inside), how the child approaches the task, how the child processes and interprets visual information, the child’s flexibility in analyzing visual information, methods used for storage and retrieval of visual information, the amount of stress associated with visual activities, and whether the child fatigues easily during visual tasks. The therapist should analyze the tasks observed carefully to determine what visual skills are needed and to identify the areas in which the child has difficulty.
Tsurumi and Todd have applied task analysis to the nonmotor tests of visual perception.150 This information greatly assists the therapist in analyzing the results of these tests. Currently, the best method for evaluating visual attention in children is informal observation during occupational performance tasks. Standardized assessments that may be used include the following:
• Bruininks-Oseretsky Test of Motor Proficiency (2nd Ed.) (BOT-2)19: An individually administered, standardized test for individuals 4 through 21 years of age. The test measures a wide array of motor skills. The eight subtests include fine motor precision, fine motor integration, manual dexterity, bilateral coordination, balance, running speed and agility, upper-limb coordination, and strength. This test has been the most widely used standardized measure of motor proficiency and has good reliability and validity.
• Test of Visual Analysis Skills122: An untimed, individually administered, criterion-referenced test for children 5 to 8 years of age. The child is asked to copy simple to complex geometric patterns. The purpose of the assessment is to determine if the child is competent at or in need of remediation for perception of the visual relationships necessary for integrating letter and word shapes. Reliability and validity of this test indicate that the psychometric properties are adequate.
Visual-Spatial Tests
• Jordan Left-Right Reversal Test, revised77: An untimed, standardized test for children 5 to 12 years of age that can be administered individually or to a group. It is used to detect visual reversals of letters, numbers, and words, and the test manual includes remediation exercises for reversal problems. The test takes about 20 minutes to administer and score and has good test-retest reliability and criterion-related validity.
Visual-Perceptual Tests
• Test of Visual-Perceptual Skills (Non-Motor), Third Edition (TVPS-R)94: A norm-referenced test for children 4 to 18 years of age that can be administered individually or to a small group. The subtests include visual discrimination, visual memory, visual-spatial relationships, form constancy, visual-sequential memory, visual figure-ground and visual closure. The test uses black and white designs as stimuli for perceptual tasks, and responses are made vocally or by pointing.
• Developmental Test of Visual Perception, Second Edition (DTVP-2)68: A norm-referenced test for children 4 to 10 years of age that is unbiased relative to race, gender, and handedness. The eight subtests include hand-eye coordination, copying, spatial relationships, position in space, figure-ground competence, visual closure, visual-motor speed, and form constancy. This test has been shown to have strong normative data and good reliability and validity.
• Componential Assessment of Visual Perception (CAVP)113: A computer-assisted evaluation tool that was designed as a process-based approach to the evaluation of visual-perceptual functioning in children and adults with neurologic disorders. Promising clinical usefulness has been reported in terms of utility, ease of use, format, and appeal.112
• Motor-Free Visual Perception Test, Third Edition (MVPT-3)35: A norm-referenced test that is quick and easy to administer. Scoring requires adding the number of correct choice responses. This test has a high test-retest reliability and internal validity. Also, criterion validity is determined relative to academic performance.
• Test of Pictures, Forms, Letters, Numbers, Spatial Orientation, and Sequencing Skills54: A norm-referenced test for children 5 to 9 years of age that can be administered individually or to a group. The test, which has seven subtests, measures the ability to perceive forms, letters, and numbers in the correct direction and to perceive words with letters in the correct sequence.
Visual-Motor Integration Tests
• Wide Range Assessment of Visual Motor Abilities (WRAVMA)1: A norm-referenced, standardized test for children 3 to 17 years of age. Assesses and compares visual-spatial skills through the matching subtest, fine motor skills through the pegboard subtest and integrated visual-motor skills through the drawing subtest. Each subtest requires 4 to 10 minutes and offers easy administration and sound psychometric properties.
• The Developmental Test of Visual-Motor Integration, 5th Edition, Revised (VMI)6: This test assesses three subtest areas for individuals 2 to 19 years of age and has strong content, concurrent and construct validity.
These tests can be used to evaluate how the child is processing, organizing, and using visual-cognitive information. Care should be taken in interpreting and reporting test results because it is not always clear what visual-perceptual tests are measuring. Because of the complexity of the tests, it is certain that they tap different kinds and levels of function, including language abilities.
The effectiveness of any treatment method is largely determined by how the child is diagnosed; therefore, careful analysis of test results and observations is important. Burtner et al. provided a critical review of seven norm-referenced, standardized tests of visual-perceptual skills frequently administered by pediatric therapists.22 Each assessment tool was critically appraised for its purpose, clinical utility, test construction, standardization reliability, and validity. Discussion focused on the usefulness of these assessment tools for describing, evaluating, and predicting visual-perceptual functioning in children.
INTERVENTION
The theoretical approaches that guide evaluation and treatment of visual-perceptual skills can be categorized as developmental, neurophysiologic, or compensatory. The developmental model devised by Warren,157,158 described in a previous section, is based on the concept that higher level skills evolve from integration of lower level skills and are subsequently affected by disruption of lower level skills. Skill levels in the hierarchy function as a single entity and provide a unified structure for visual perception. As pictured in Figure 12-2, oculomotor control, visual field, and acuity form the foundational skills, followed by visual attention, scanning, pattern recognition or detection, memory, and visual cognition. Identification and remediation of deficits in lower level skills permit integration of higher-level skills. Occupational therapists who follow this model need to evaluate lower level skills before proceeding to higher level skills to determine where the deficit is in the visual hierarchy and to design appropriate evaluation and intervention strategies.
The neurophysiologic approaches address the maturation of the human nervous system and the link to human performance. These approaches help create environmental accommodations to sensory hypersensitivity and visual distractibility. They also promote organization of movement around a goal, reinforcing the sensory feedback from that movement. Neurophysiologic approaches emphasize the importance of postural stability for oculomotor efficiency. The role of visual perception as part of sensory integration and the way the child perceives his or her environment are discussed in Chapter 11. The neurophysiologic approaches focus on improving visual-receptive and visual-cognitive components to enhance a child’s occupational performance.
Learning theories and behavioral approaches emphasize a child’s development of visual analysis skills. The therapist provides the child with a systematic method for identifying the pertinent, concrete features of spatially organized patterns, thereby enabling the child to recognize how new information relates to previously acquired knowledge on the basis of similar and different attributes. Because the child learns to generalize to dissimilar tasks, that improvement in visual-perceptual skills leads to increased levels of occupational performance.
In compensatory approaches, classroom materials or instructional methods are modified to accommodate the child’s limitations. The environment can also be altered or adapted. The therapist may work with the classroom teacher on behalf of the child to provide necessary supports. Adaptation and compensation techniques can include reducing classroom visual distractions, providing visual stimuli to direct attention and guide response, and modifying the input and output of computer programs. In daily living skills, adaptations to increase grooming, dressing, eating, and communication skills can be made. In play situations, toys can be made more accessible, and in work activities, adaptations can be made to promote copying, writing, and organizational skills. Box 12-1 outlines compensatory instruction guidelines.
Perceptual training programs use learning theories to remediate deficits or prerequisite skills and have been implemented in the public schools for more than 2 decades. Occupational therapists generally use activities from these approaches in combination with neurophysiologic and compensatory approaches.
Optometry and occupational therapy have common goals related to the effects of vision on performance.72,125 When a visual dysfunction is identified, sometimes only environmental modifications (e.g., changes in lighting, desk height, or surface tilt) are needed to alleviate the problem. In many cases, glasses (lens therapy) are prescribed to reduce the stress of close work or to correct refractive errors. In other cases, optometric vision therapy may be prescribed by an optometrist and carried out collaboratively with an occupational therapist. Through vision therapy, optometrists provide structured visual experiences to enhance basic skills and perception. Vision training is well supported by evidence but should be performed only under supervision of an optometrist. Collaboration between the occupational therapist and the optometrist is supported by case studies and clinical judgment.
Intervention Strategies
For a child of any age, an important treatment strategy is education regarding the problem the child is experiencing.150 The occupational therapist can help interpret the functional implications of the vision problem for the child and his or her parents, caregivers, and teachers. At times this can be the most helpful intervention for the child. This section presents intervention suggestions according to age groups. However, activities should be analyzed and then selected according to the child’s needs rather than according to his or her age group.
These activities illustrate both the developmental and compensatory approaches. Often activities combine approaches. For example, when classroom materials are adapted so that the print is larger and less visual information is presented (compensatory approach), the child might be better able to use visual-perceptual skills, with resulting improvement in those skills (developmental approach). For each age group, the focus of intervention is occupation in natural environments. The aim of occupational therapy intervention is to reduce activity limitations and enhance participation in everyday activities.145
Infants
Glass presented a protocol for working with preterm infants in a neonatal intensive care unit (NICU).62 Dim lighting allows the newborn to spontaneously open his or her eyes. Stimulation of the body senses (e.g., tactile-vestibular stimulation) can influence the development of distance sense (e.g., visual), which matures later.120,151 On the basis of research of neonatal vision, Glass suggested ways to use the human face as the infant’s first source of visual stimulation. The intensity, amplitude, and distance of the stimulus depend on whether the intent is to arouse or quiet the infant. Glass also recommended beginning with softer, simpler forms and three-dimensional objects and varying the stimuli based on whether the intent is to soothe or arouse the infant. Mobiles hung over cribs should be placed approximately 2 feet above the infant and slightly to one side. This allows for selective attention by the infant. In addition, Glass suggested that black and white patterns be reserved for full-term infants who are visually impaired and unable to attend to a face or toy.62 Once a visual response is elicited with the high-contrast pattern, a shift to a pattern with less contrast should be made. Recent studies suggest that 3- to 5-month-old infants may be attracted to toys that reflect light or flash light congruently with a sound.107 At the age of 4½ months, the preference for the familiar precedes the preference for novel as infants examine visual stimuli.116 This presentation of stimuli is important in the formation of memory representations.
Preschool and Kindergarten
Occupational therapists can help preschool and kindergarten teachers organize the classroom activities to help children develop the readiness skills needed for visual perception. Teachers should understand the increased need for a multisensory approach with young children who are struggling with shape, letter, and number recognition. For example, the child might benefit from tactile input to learn shapes, letters, and numbers. By using letters with textures, the child has additional sensory experiences on which he or she can rely when visual skills are diminished. Children should be encouraged to feel shapes, letters, and words through their hands and bodies. Letters can be formed with clay, sandpaper, beads, or chocolate pudding (Figure 12-4). Studies have shown that the incorporation of visuo-haptic and haptic exploration of letters in reading training programs facilitates 5-year-old children’s understanding of the alphabet.41

All preschool, kindergarten, and primary classes should include frequent activities that develop body-in-space concepts to improve spatial perception. Even with a range of levels of understanding among young students, group activities, such as Statue, shadow dancing, and Simon Says, can reinforce body-in-space comprehension. Children benefit from watching and imitating one another. The therapist may pair children so that one can model for the other in an obstacle course or other gross motor activity. Appendix 12-A on the Evolve website lists publications describing activities for both classroom teachers and therapists.
Shared storybook reading has been found to provide a particularly useful context within which to promote at-risk preschoolers’ emergent literacy knowledge.80 Further study has shown placing that emphasis on the print concepts by talking about and by pointing to the print increases visual attention to it. Children attended to print significantly more often when being read a storybook with large narrative print, relatively few words per page, and multiple instances of print embedded within the illustrations.81
Studies of handwriting suggest that no significant difference in letter writing legibility exists between kindergartners who use paper with lines and those who use paper without lines.38,159 The study investigators suggest that teachers allow kindergarten children to experiment with various types of writing paper when initially learning proper letter formation.
Elementary School
Therapy should begin at the level of the visual hierarchy where the child is experiencing difficulty. If the child is experiencing difficulty with visual-receptive skills, cooperative efforts between the occupational therapist and the optometrist may be helpful. The school-based occupational therapist’s objectives for improving visual-receptive skills (as these appear on student’s individualized education program) are to support the child’s academic goals and appropriate curricular outcomes.
Organizing the Environment: Visual perception affects a child’s view of the entire learning environment. Visually distracting and competing information can be problematic to the child who has not yet fully developed his or her skills. The child may require that the classroom be less “busy” visually to allow him or her to focus on learning. Limiting a distractible child’s peripheral vision by using a carrel is often helpful (Figure 12-5). In addition, the level of illumination needs to be monitored, and glare must be controlled.
The child needs a stable postural base that allows his or her eyes to work together. Children often sit at ill-fitting furniture, which can compound their problems. The occupational therapist can help the teacher properly position the child. The therapist can add bolsters to seat backs, put blocks under the child’s feet, or provide the child with a slant board if any of these materials will help the child use vision more efficiently or increase productivity. The therapist can also stress the importance of encouraging different positions for visual activity. Figure 12-6 shows such alternative positions as prone, “television position” for sitting, and side-lying for visual-perceptual activities such as reading. Each position should place the child in good alignment and should offer adequate postural support.
Children may benefit from color-coded worksheets to help them attend to what visually goes together. However, children with color vision problems may have difficulty with educational materials that are color coded, particularly when the colors are pastel or muddy. Therefore, it is important to differentiate an actual visual color deficit from a problem either with color naming or with color identification.32
Christenson and Rascho proposed strategies to assist the elderly in topographic orientation, and these can be adapted for children.30 The authors found that use of landmarks and signage can enhance wayfinding skills and topographic orientation. They recommend the use of pictures or signs that are realistic and simple and that have high color contrast. For example, a simple, graphic depiction of a lunch tray with food could be used for the cafeteria door.
Visual Attention: With a sensory processing approach, general sensory stimulation or inhibition may be provided during or before visually oriented activities to improve visual attending skills. If the child is overaroused, the therapist can diminish sensory input to calm him or her; if the child is underaroused, the therapist selects alerting activities to increase the level of arousal.
For the child with impaired visual attention, the therapist addresses goals using varied activities and time segments that are achievable. The therapist identifies activities that are intrinsically motivating to the child because these help maintain the child’s attention. The therapist should plan activities together with the child and use as many novel activities as possible. Most challenging to the therapist is adapting or modifying task activities while maintaining a playful learning environment for the child. For example, the therapist may have many activities focusing on the same visual-perceptual problem, and he or she changes activities frequently, depending on the child’s sustained attention to the task. The therapist also gradually increases the amount of sustained attention needed to complete the task. Elimination of extraneous environmental stimuli is helpful at each level of visual attention.
The occupational therapist can be a consultant to the classroom teacher suggesting ways to improve the child’s attention to learning in the classroom. For instance, the therapist can provide activities during a classroom session and then leave further suggestions for activities that the teacher can implement during the week. Specific components of attention could be addressed in a hierarchical manner so that intervention tasks gradually place greater demands on attention (e.g., progressing from sustained attention to divided attention).
Visual attention skills are enhanced by activities that are developmentally appropriate and visually and tactilely stimulating. Manual activities such as drawing or manipulating clay encourage the eyes to view the movements involved.117 In addition, the hand helps educate the eye about object qualities such as weight, volume, and texture and helps direct the eye to the object.117 Simultaneous hand and eye movements construct internal representations of objects and improve object recognition.
Activities to compensate for limitations in attention include (1) placing a black mat that is larger than the worksheet underneath it to increase high contrast, thereby assisting visual attention to the worksheet; (2) drawing lines to group materials; and (3) reorganizing worksheets.144 Visual stimuli on a worksheet or in a book can be reduced by covering the entire page except the activity on which the student is working or by using a mask that uncovers one line at a time (Figure 12-7). Reducing competing sensory input in both the auditory and visual modalities can be helpful for some students with poor visual attention. For example, headphones can be worn when working on a visual task. Good lighting and use of pastel-colored paper helps reduce glare. Encouraging children to search for high-interest photographs or pictures can help increase visual attention skills.117 Where’s Waldo? and similar books are highly motivating and encourage children to develop search strategies and visual attention.
Other suggestions include cueing the child to important visual information by using a finger to point, a marker to underline, or therapist verbalization to help the child maintain visual attention. For example, children tend to look at a picture when it is named. The therapist can use large, colorful pictures combined with rhyming chants to encourage attention to the pictures.117 Visual work should be presented when the student’s energy is highest and not when he or she is fatigued.117 Strategy training can be used to control distractibility, impulsivity, or a tendency to lose track or to overfocus.145 Intervention strategies may include the following50:
• Attending to the whole situation before attending to parts
• Monitoring the tendency to become distracted
• Searching the whole scene before responding
• Devising time-pressure management strategies50
Visual Memory: Children with visual memory problems need consistent experiences; the therapist therefore should consult with the parents and teachers so that this consistency can be maintained at home and in the classroom. There is no evidence that repetitive practice of word lists or objects generalizes to other material.31 Instead, memory strategies may help with encoding or with the retrieval of memory. Grouping information in ways that provide retrieval cues can help a child remember interrelated data.127 Several strategies may be helpful. Chunking is organizing information into smaller units, or chunks. This can be done by cutting up worksheets and presenting one unit or task at a time. Maintenance rehearsal (repetition) helps the child hold information in his or her short-term memory but seems to have no effect on long-term storage. An example of this strategy would be repeating a phone number until the number is dialed. Elaborative rehearsal is a strategy by which new information is consciously related to knowledge already stored in long-term memory. By the time a child is 8 years of age, he or she can rehearse more than one item at a time and can rehearse information together as a set to remember. Children can also relate ideas to more than one other idea.
Mnemonic devices are memory-directed tactics that help transform or organize information to enhance its retrievability through use of language cues such as songs, rhymes, and acronyms. Gibson suggested that memory is composed primarily of distinctive features (what makes something different).58 If the child has good visualization, this can be used as a memory strategy for encoding information. Occupational therapists can help the child determine differences in visual stimuli to promote storage in memory. Playing games such as Concentration, copying a sequence after viewing it for a few seconds, or remembering what was removed from a tray of several items can be enjoyable ways to increase visual memory (Case Study 12-1). The therapist first provides the student with short, simple tasks that he or she can complete quickly and successfully; gradually, as the student accomplishes tasks, the therapist increases their length and complexity.
 CASE STUDY 12-1
CASE STUDY 12-1When Todd was a 9-year-old student in the third grade, most of his day was spent in the regular third grade classroom, where he functioned at grade level in all areas of academics except reading. Todd received daily resource room instruction in this area. This instruction consisted of copying, worksheet completion, and drill and repetition techniques and did not include opportunities for manipulative activities.
An occupational therapy evaluation indicated that Todd’s perceptual skills were delayed about 2 years, with weaknesses noted in visual-spatial relations, figure-ground perception, and visual sequential memory. From interviewing the teacher, the therapist learned that Todd was not moving from learning to read to reading to learn. His decoding was not automatic; therefore, he was spending considerable time figuring out what the words were rather than comprehending what he was reading. He also reported that his eyes tired easily while reading. Good eye movements were needed to sustain reading for longer periods. Because of poor spatial abilities, Todd had difficulty discerning differences in visually similar symbols and had difficulty with words that differed only by sequence (three and there) or spatial orientation (dad and bad). The third grade reading books had more print per page and fewer illustrations to give cues. Too many words on the page made it difficult for Todd because of his poor figure-ground abilities. He demonstrated an inability to recall the exact order of words, poor sight vocabulary, and poor spelling caused by poor visual sequential memory.
The therapist referred Todd for optometric evaluation because of his reported visual fatigue during reading tasks. Planning together with Todd, the therapist and the teacher developed strategies to assist him in increasing his visual memory. Initially, short visual memory tasks were used, and gradually the length of tasks was increased. This was done using visual memory games (such as Concentration) and activities on the computer. In addition, visual discrimination tasks were started, beginning with simple forms and moving to forms that were more complex.
In consultation with the teacher, the therapist recommended reducing the amount of print per page and masking what was not immediately needed when this could not be done. Phonics approaches to word recognition were recommended (see Table 12-3), as were using verbal mediation to decode words.
External strategies and aids can also be used, such as notebooks, hand-held computers, and tape recorders, to name a few. Also, tasks and environments can be rearranged so that they are less demanding on memory.143 Examples include labeling drawers with the contents inside them, making cue cards with directions for tasks, and posting signs to help the child find his or her classroom. Emotional memory has been shown to be the strongest kind of memory. When students are deeply interested and emotionally involved in what they are reading, they are more likely to comprehend and learn from it.23
Visual Discrimination: The therapist must use task analysis to design an intervention program. Remediation should follow an orderly design15 so that the child can make sense of each performance. By analyzing the continuum of a task, the therapist can grade the activity from simple to complex to allow success while challenging the child’s visual abilities.11 Intervention strategies should aim to help children recognize and attend to the identifying features by teaching them to use their vision to locate objects and then to use object features as well as other cues to form identification hypotheses.127 Teaching children to scan or search pictures visually instructs the child in the value of looking for and finding meaning. With high-interest materials the therapist can teach the child to look from top to bottom and left to right.117 Using pictures from magazines, the therapist removes an important part of a picture and asks the student to identify what part is missing. Drawing, painting, and other art and craft activities encourage exploration and manipulation of visual forms. As the child moves from awareness to attention and then to selection, he or she becomes better able to discriminate between the important and unimportant features of the environment.
Occupational therapists can assist teachers in reorganizing the child’s worksheets. Color-coding different problems may assist the child in visually attending to the correct section. Worksheets can also be cut up and reorganized to match the child’s visual needs. It is important gradually to phase out the restructuring of the worksheets so that the child can eventually use the sheets as they are presented in the workbooks.
When a child has problems copying from the chalkboard, the occupational therapist may recommend that the chalkboard be regularly cleaned in an effort to reduce clutter and provide high contrast for chalk marks. Notations on chalkboards, bulletin boards, or overhead transparencies should be color coded, well spaced, and uncluttered. These practices can reduce figure-ground problems. The therapist may also suggest that the teacher reduce use of the chalkboard by having the children copy from one paper to another with both papers in the same plane. A teacher may be encouraged to try bean bag games in which the targets are placed at approximately the same distance from the child’s eyes as the chalkboard so that a student can practice focusing and fixating the eyes near and far in play.
Reducing the amount of print on a page (less print, fewer math problems) and providing mathematical problems on graph paper with numbers in columns in the 1s, 10s, and 100s places help students with figure-ground difficulties. Masking the part of the worksheet not being worked on can help the child focus on one problem at a time. Cooper proposed a theoretic model for the implementation of color contrast to enhance visual ability in the older adult.36 Principles of color contrast and the ways in which color contrast can be achieved by varying hue, brightness, or color saturation, of an object in relation to its environment are the foundation of the method of intervention. This helps a child identify the relevant information, such as the classroom materials and supplies.
Decoding Problems in Reading: Children who have difficulty distinguishing between similar visual symbols may benefit from a multisensory approach. This includes tracing the shapes and letters, hearing them, saying them, and then feeling them, allowing a number of routes of processing to help supplement weak visual-perceptual processing. Thus the child sees it, hears it, traces it, and writes it. Eating letters is an activity children love; alphabet cereal, gelatin jigglers, and cookies in the shape of letters can be served for snacks. Children can trace the letters with frosting from tubes onto cookies and with catsup from packets.
For children with word recognition difficulty, the initial emphasis should be on recognition rather than retrieval. The child can be given a choice of visually similar words to complete sentences that have single words missing. In addition, using word families (ball, call, and tall) to increase sight vocabulary enhances word recognition skills. Phonic approaches may also be the best reading instruction method for children with poor word recognition. Textbooks recorded on CDs can be ordered from local and state libraries from the American Printing House for the Blind (1839 Frankfurt Ave., P.O. Box 6085, Frankfurt, KY 40206). The student can hear and read the textbook at the same time, which provides input through two sensory modalities.
If the child has strong verbal skills, verbal mediation (talking through printed words) should be stressed, and the child could be encouraged to describe what he or she sees to retain the information. A strategy that may assist a child who reverses letters in words is to follow along the printed lines with a finger. This technique helps stress reading the letters in the correct sequence. Reading material rich in pictorial content (e.g., comic books), pictures with captions and cartoons, and computer software designed to enhance sight vocabulary can strengthen these associations. Verbal instruction to guide and support the child’s nonverbal problem-solving processes and direct verbal training on a spatial task have been shown to be an effective treatment strategy for children with nonverbal learning difficulties.53
Several studies support the use of colored filters to improve reading skills.14,128 Color overlays have been used for children with difficulty reading due to visual fatigue and visual perceptual distortions that are reported as movement of the print (jumping, fading, disappearing, blurring), merging of the print and background, and patterns within the print. Research suggests that they may be a beneficial tool to use when children have reading difficulties. Blaskey et al. investigated the effectiveness of Irlen (colored) filters for improving comfort and reading performance and for determining whether traditional optometric intervention would be effective in relieving the symptoms commonly reported by people seeking help through the use of Irlen filters.12 Results revealed that subjects in both treatment groups showed improvement in vision functioning. Although the subjects in the Irlen filter group did not show any significant gains in reading rate, work recognition in context, or comprehension, they did report increased comfort in vision when reading.
The What Works Clearinghouse collects, reviews, and reports on studies of education programs, products, practices, and policies in selected topic areas, using a set of standards based on scientifically valid criteria. Programs in early childhood education including print awareness and beginning reading are reviewed. The site can be accessed at http://www.w-w-c.org or http://www.whatworks.ed.gov.
Visualization: The development of visualization techniques, or visual imagery, may be delayed. Like all skills, this proceeds from the concrete to the abstract. Therapists can start by helping students picture something that they can touch or feel. Using a grab bag with toys or objects inside that the child identifies without vision is a good way to do this.
As material becomes less concrete, more visual skills are drawn into play. A student might be asked to visualize something that he or she has done. The occupational therapist can facilitate the child’s thinking by reminding him or her to consider various factors, such as color, brightness, size, sounds, temperature, space, movement, smells, and tastes. The hope is that once the child practices verbally, he or she will generalize the visualization process to reading.7
Children with poor visualization may have difficulty spelling and may need to learn spelling rules thoroughly. They may also demonstrate reading comprehension problems. In addition, they may have difficulty forming letters because they are unable to visualize them. This would become evident when the child writes from dictation. Sometimes the child can visualize a letter from the sound, but it is reversed or missing parts.
Learning Styles: All students have a preferred learning style.24,26 When a student is taught through his or her preferred style, the child can learn with less effort and remember better.44,114 Figure 12-8 shows diagnostic learning styles. All students need to be taught through their strongest senses and then reinforced through their next strongest sense.
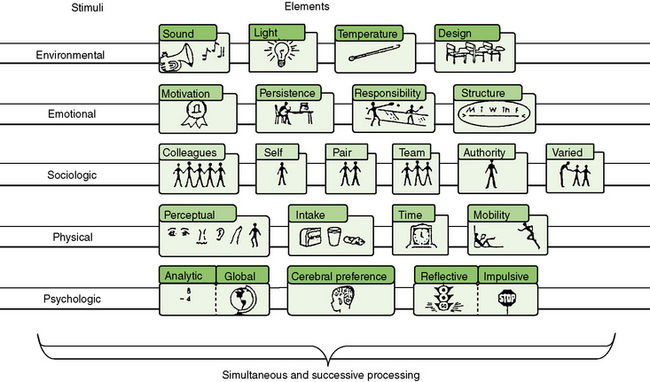
FIGURE 12-8 Diagnostic learning styles. Courtesy Rita Dunn, EdD, St. John’s University, Jamaica, NY.
Auditory learners recall at least 75% of what is discussed or heard in a normal 40- to 45-minute period. Visual learners remember what they see and can retrieve details and events by concentrating on the things that they have seen. Tactual and kinesthetic learners assimilate best by touching, manipulating, and handling objects. They remember more easily when they write, doodle, draw, or move their fingers. It is best to introduce material to them through art activities, baking, cooking, building, making, interviewing, and acting experiences. If a child has weaknesses in visual processing, it is more difficult for him or her to learn through the visual sense. This child may learn more effectively through the kinesthetic and tactile senses. Box 12-2 presents suggestions for kinesthetic learning.
Occupational therapists can greatly assist teachers by helping to determine a child’s perceptual strengths and weaknesses so that an appropriate reading program can be matched to the child’s preferred perceptual modality. Once the child is in first grade, it is important to determine what reading program the teacher is using. Table 12-3 matches reading methods to perceptual strengths and weaknesses and global and analytic styles.
TABLE 12-3
Matching Reading Methods to Perceptual Strengths
| Reading Method | Description | Reading Style Requirements |
| Phonics | Isolated letter sounds or letter clusters are taught sequentially and blended to form words. | Auditory and analytic strengths |
| Linguistic | Patterns of letters are taught and combined to form words. | Auditory and analytic strengths |
| Orton-Gillingham | Consists of phonics and tactile stimulation in the form of writing and tracing activities. | Auditory and analytic strengths combined with visual weaknesses |
| Whole word | Before reading a story, new words are presented on flash cards and in sentences, with accompanying pictures. | Visual and global strengths |
| Language-experience | Students read stories that they have written. | Visual, tactile, and global strengths |
| Fernald | Language-experience method, plus student traces over new words with index finger of writing hand. | Tactile and global strengths combined with visual weaknesses |
| Choral reading | Groups read a text in unison. | Visual and global strengths |
| Recorded book | Students listen two or three times to brief recordings of books, visually track the words, then read the selection aloud. | Visual and global strengths |
From Carbo, M. (2007). Becoming a great teacher of reading: Achieving high rapid reading gains with powerful differentiated strategies. Thousand Oaks, CA: Corwin Press.
In addition to perceptual strengths, the therapist must keep in mind the child’s preferred manner of approaching new material. For instance, global learners require an overall comprehension first and then can attend to the details. Analytic learners piece details together to form an understanding.
Visual-Motor Integration: To review, the therapist should first focus on the underlying visual-receptive functions and then focus on the visual-cognitive functions. This should proceed in the sequence of visual attention, visual memory, visual discrimination, and specific visual discrimination skills. A multisensory approach to handwriting may be helpful to a child with visual-cognitive problems. Working with the eyes closed can be effective in reducing the influence of increased effort that vision can create and in lessening the visual distractions. Keeping the eyes closed can also improve the awareness of the kinesthetic feedback from letter formation.
The therapist should be aware of which handwriting approach is used in the classroom. The child whose preferred learning style is based on an auditory system can be assisted in learning handwriting through use of a talking pen. Handwriting programs that appear easier for children with visual-cognitive problems include Loops and Other Groups9 and Handwriting Without Tears.101 Olsen described strategies to help children correct or avoid reversals. During handwriting lessons, the child should proofread his or her own work and circle the best-formed letters. Chapter 19 has comprehensive information on developing handwriting skills.
Children with visual-spatial problems often choose random starting points, which can confuse the writing task from the onset. Concrete cues must be used to teach abstract handwriting concepts. For example, colored lines on the paper or paper with raised lines can be helpful for the child who has difficulty knowing where to place the letters on the page. In addition, green lines drawn to symbolize go on the left side of the paper and red lines to symbolize stop on the right side may help a child know which direction to write his or her letters and words. Upright orientation of the writing surface may also lessen directional confusion of letter formation (up means up and down means down) versus orientation at a desk on a horizontal surface, where up means away from oneself and down means toward oneself.127
Directional cues can be paired with verbal cues for the child who commonly reverses letters and numbers. These cognitive cues rely on visual images for distinguishing letters and include the following:
1. With palms facing the chest and thumbs up, the student makes two fists. The left hand will form a b and the right hand will form a d.
2. Lower case b is like B, only without the top loop.
3. To make a lower case d, remember that c comes first, then add a line to make a d.
The therapist can develop cue cards for the student to keep at his or her desk with common reversals. Lee has developed a frame of reference for reversal errors in handwriting based on visual-perceptual theory.87 See Box 12-3 for the postulates for change as outlined by Lee.
Children with visual-cognitive problems often overspace or underspace words. The correct space should be slightly more than the width of a single lower case letter. When a child has handwriting spacing problems, the occupational therapist may recommend using a decorated tongue depressor or a pencil to space words, or simply have the child use his or her finger as a guide. The child can also imagine a letter in the space to aid in judging the distance.
When students need additional help to stop at lines, templates with windows can be used in teaching handwriting. These templates can be made out of cardboard with three windows; one for one-line letters (a, c, e, i, m, and n), one for two-line letters (b, d, k, l, and t), and the third for three-line letters (f, g, j, p, q, z, and y). It is important to consider that visual memory is used to recognize the letters or words to be written, and motor memory starts the engram for producing the written product. Therefore it may be that motor memory, not visual memory, is the basis for the problem.
Dankert, Davies, and Gavin evaluated whether preschool children with developmental delays who received occupational therapy would demonstrate improvement in visual-motor skills.40 The children received a minimum of one individual 30-minute session and one group 30-minute session per week for one school year. Their performance was compared with that of two control groups: typically developing peers who received occupational therapy and typically developing peers who did not receive occupational therapy. The results showed that the students with developmental delays demonstrated statistically significant improvement in visual-motor skills and developed skills at a rate faster than expected compared with typically developing peers.
Computers: Many excellent educational computer programs for young children are already on the market. Software programs that are highly motivating for children of all ages are available. Living books on the computer reinforce the written word with the spoken word and assist in developing a sight-word vocabulary.
The computer can be used as a motivational device to help increase the child’s attention to the task. It also provides a means to practice skills in an independent manner. Drill and practice software record data on accuracy and the time taken to complete the drills, allowing the therapist to record the child’s progress. The therapist can adapt the computer program by changing the background colors to those that enhance the child’s visual-perceptual skills. The therapist can also enlarge the written information so that less information is present on the screen. Sands and Buchholz provide a discussion on the use of computers in reading instruction.124 Appendix 12-A on the Evolve website includes a list of computer software and hardware companies that provide current information on technologic and educational resources available for children with a variety of special needs.
Studies have shown that children’s use of computer-based activities resulted in improved performance. For example, using single-subject reversal design study, Cardona, Martinez, and Hinojosa examined five children 3 to 5 years of age who had developmental disabilities to measure the effectiveness of using a computer to increase attention to developmentally appropriate visual analysis activities.28 The results suggested that each child’s attention to task performance improved during the computer-based activities as measured by the number of off-task behaviors. Sitting tolerance and visual attention to the task did not change. All participants seemed to be interested in and motivated to engage in the computer-based activities.
More research is needed to examine a longer intervention phase and the effectiveness of computer-based intervention in natural settings such as a classroom. Authors who have studied the effects of computer games in kindergarten-age children recommend their use in improving visual-perceptual skills.104 Their findings indicate that, on the basis of required time and motivation level, computer games are more efficient than other educational programs.
Currently a considerable body of literature supports the use of virtual environment technology to train spatial behavior in the real world.45 Occupational therapists should incorporate this information into their interventions.
SUMMARY
Children with visual-perceptual problems often receive the services of occupational therapists. This chapter described a developmental approach that emphasizes methods of identifying the underlying client strengths and deficits in visual-receptive and visual-cognitive skills. The relationship of these components to various performance skills was described. Using the developmental approach, the occupational therapist helps the child increase his or her visual-perceptual skills by addressing the skill problems that appear to be limiting function. By adapting classroom materials and instruction methods, the therapist also helps the child compensate for visual-perceptual problems. Intervention often includes a combination of developmental and compensatory activities. This holistic approach enables the child with visual-perceptual problems to achieve optimal function and learning.
Little evidence exists in the occupational therapy literature regarding treatment effectiveness for visual-perceptual problems in children. See Table 12-4 for results of visual-perceptual treatment. As a profession, occupational therapy has identified that visual-perceptual problems are within its domain of practice. Further, occupational therapy practitioners, authors, and researchers have defined practice models and intervention activities to remediate visual-perceptual problems. The next step is to systematically test the effectiveness of these intervention programs.
TABLE 12-4
Evidence of Visual-Perceptual and Visual-Motor Treatment
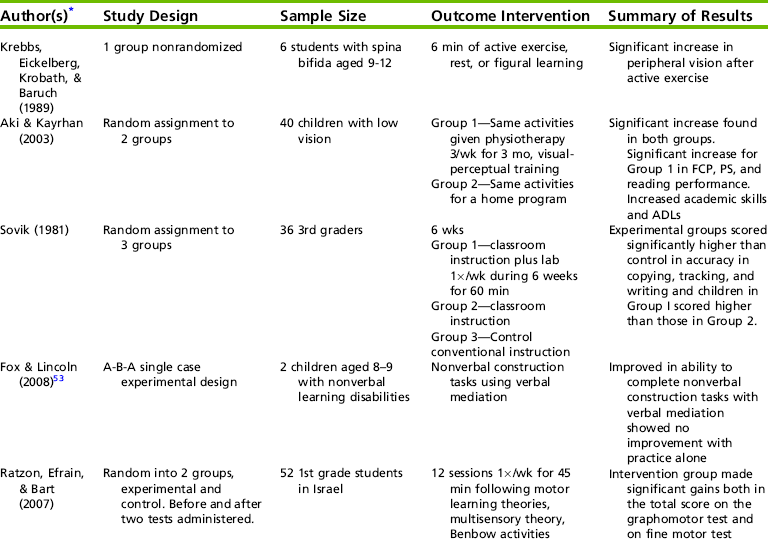
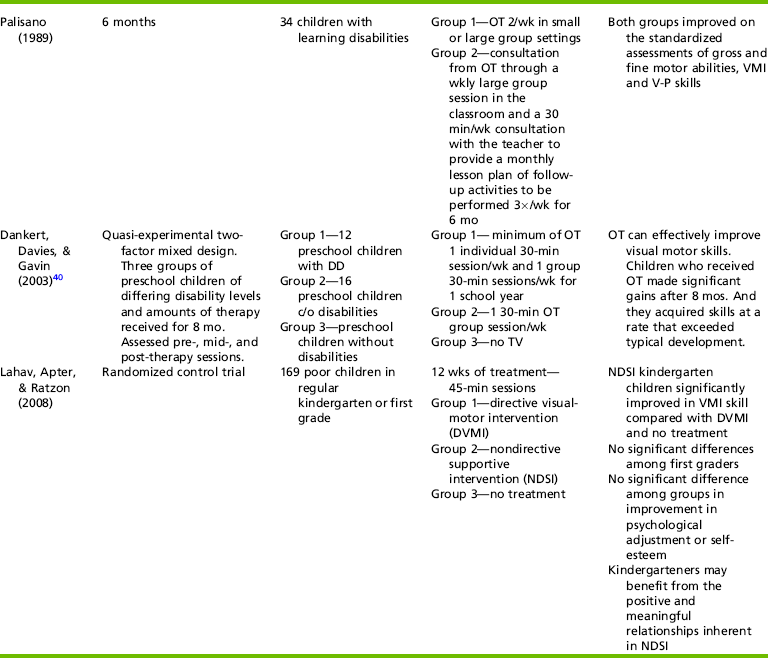
*Complete source information follows:
Aki, E., & Kayihan, H. (2003). The effect of visual perception training on reading, writing and daily living activities in children with low vision. Fizyoterapi Rehabilitasyon, 14(3), 95-99. Krebbs, P., Eickelberg, W., Krobath, H., & Barvch, I. (1989). Effects of physical exercise on peripheral vision and learning in children with spina bifida manifesta. Perceptual and Motor Skills, 68, 167-174. Lahav, O., Apter, A., & Ratzon, N. (2008). A comparison of the effects of directive visuomotor intervention versus nondirective supportive intervention in kindergarten and elementary school children. Journal of Neural Transmission, 115(8), 1231-1239. Palisano, R. J. (1989). Comparison of two methods of service delivery for students with learning disabilities. Physical and Occupational Therapy in Pediatrics, 9(3), 79-100. Ratzon, N. Z., Efraim, D., & Bart, O. (2007). A short-term graphomotor program for improving writing readiness skills of first-grade students. American Journal of Occupational Therapy, 61(4), 399-405. Sovik, N. (1981). An experimental study of individualized learning/instruction in copying, tracking, and handwriting based on feedback principles. Perceptual and Motor Skills, 53, 195-215.
REFERENCES
1. Adams, W., Sheslow, D. Wide range assessment of visual motor abilities manual. Wilmington, DE: Wide Range, Inc, 1995.
2. American Occupational Therapy Association (AOTA), Occupational therapy practice framework: Domain and process, 2nd ed. American Journal of Occupational Therapy, 2008;62:625–683.
3. Arguin, M., Cavanagh, P., Joanette, Y. Visual feature integration with an attention deficit. Brain and Cognition. 1994;24:44–56.
4. Ayres, A.J. Sensory Integration and the Child. Los Angeles: Western Psychological Services, 1979.
5. Batshaw, M.L., Pellegrino, L., Roizen, N. Children with handicaps: A medical primer, 6th ed. Baltimore: Brookes, 2007.
6. Beery, K.E., Beery, N.A. Developmental Test of Visual-Motor Integration with supplemental Developmental Tests of Visual Perception and Motor Coordination: Administration, Scoring, and Teaching Manual, 5th ed. Upper Saddle River, NJ: Pearson, 2004.
7. Bell, N. Visualizing and verbalizing for language comprehension and thinking. Paso Robles, CA: Academy of Reading Publishers, 1991.
8. Bell, B., Swinth, Y. Defining the role of occupational therapy to support literacy development. School System Special Interest Section Quarterly. 2005;12(3):1–4.
9. Benbow, M. Loops and other groups. Tucson, AZ: Therapy Skill Builders, 1990.
10. Birch, H.G. Brain damage in children: The biological and social aspects. New York: Williams & Wilkins, 1964.
11. Blanksby, B.S. Visual therapy: A theoretically based intervention program. Journal of Visual Impairment and Blindness. 1992;86:291–294.
12. Blaskey, P., Scheimen, M., Parisi, M., Ciner, E.B., Gallaway, M., Sleznick, R. The effectiveness of Irlen filters for improving reading performance: A pilot study. Journal of Learning Disabilities. 1990;23:604–612.
13. Borsting, E. Visual perception and reading. In: Garzia R., ed. Vision and reading. St. Louis: Mosby, 1996.
14. Bouldoukian, J., Wilkins, A.J., Evans, B.J.W. Randomised controlled trial of the effect of couloured overlays on the rate of reading of people with specific learning difficulties. Ophthalmic & Physiological Optics. 2002;22:55–60.
15. Bouska, M.J., Kauffman, N.A., Marcus, S.E. Disorders of the visual perception system. In Umphred D.A., Lazaro R.T., eds.: Neurological rehabilitation, 6th ed., St. Louis: Elsevier, 2006.
16. Bowers, P.G., Ishaik, G. RAN’s contributions to understanding reading disabilities. In: Swanson H.L., Harris K.R., Graham S., eds. Handbook of learning disabilities. New York: Guilford Press; 2003:140–157.
17. Breakey, A.S., Wilson, J.J., Wilson, B.C. Sensory and perceptual functions in the cerebral palsied. Journal of Nervous and Mental Diseases. 1994;158:70–77.
19. Bruininks, R.H., Bruininks, R. Bruininks-Oseretsky Test of Motor Proficiency, 2nd ed. BOT-2. Upper Saddle River, NJ: Pearson Assessment, 2005.
20. Burpee, J.D. Sensory integration and visual functions. In: Gentile M., ed. Functional visual behavior: A therapist’s guide to evaluation and treatment options. Bethesda, MD: American Occupational Therapy Association, 1997.
21. Burtner, P.A., Dukeminier, A., Ben, L., Qualls, C., Scott, K. Visual perceptual skills and related school functions in children with hemiplegic cerebral palsy. New Zealand Journal of Occupational Therapy. 2006;53(1):24–29.
22. Burtner, P.A., Wilhite, C., Bordegaray, J., Moedl, D., Roe, R.J., Savage, A.R. Critical review of visual perceptual tests frequently administered by pediatric therapists. Physical and Occupational Therapy in Pediatrics. 1997;17:39–61.
23. Caine, R.N., Caine, G., McClintic, C., Klimek, K. 12 Brain mind learning principles in action. Thousand Oaks, CA: Corwin Press, 2005.
24. Carbo, M. Reading Style Inventory (Revised). Roslyn, NY: National Reading Styles Institute, 1992.
25. Carbo, M. Reading styles times twenty. Educational Leadership. 1997;54:38–42.
26. Carbo, M. Becoming a great teacher of reading: Achieving high rapid reading gains with powerful, differentiated strategies. Thousand Oaks, CA: Corwin Press and National Association of Elementary School Principals, 2007.
27. Carbo, M. Best practices for achieving high, rapid reading gains. The Education Digest. 2008;73(7):57–61.
28. Cardona, M., Martinez, A.L., Hinojosa, J. Effectiveness of using a computer to improve attention to visual analysis activities of five preschool children with disabilities. Occupational Therapy International. 2000;7:42–56.
29. Caron, A., Caron, R. Processing of relational information as an index of infant risk. In: Friedman S., Sigman M., eds. Preterm birth and psychological development. New York: Academic Press, 1981.
30. Christenson, M.A., Rascho, B. Environmental cognition and age-related sensory change. Occupational Therapy Practice. 1989;1:28–35.
31. Cicerone, K.D. Evidence-based cognitive rehabilitation: Recommendations for clinical practice. Archives of Physical Medicine and Rehabilitation. 2000;81:1596–1615.
32. Ciner, E.B., Macks, B., Schanel-Klitsch, E. A cooperative demonstration project for early intervention vision services. Occupational Therapy Practice. 1991;3:42–56.
33. Clifton, R.K., Muir, D.W., Ashmead, D.H., Clarkson, M.G. Is visually guided reaching in early infancy a myth? Child Development. 1993;64:1099–1110.
34. Cohen, K.M. The development of strategies of visual search. In: Fisher D.F., Monty R.A., Senders J.W., eds. Eye movements: Cognition and visual perception. Hillsdale, NJ: Erlbaum, 1981.
35. Colarusso, R.P., Hammill, D.D. Motor-Free Visual Perception Test, 3rd ed. Novata, CA: Academic Therapy Publications, 2003.
36. Cooper, B.A. A model for implementing color contrast in the environment of the elderly. American Journal of Occupational Therapy. 1985;39:253–258.
37. Cratty, B.J. Perceptual and motor development in infants and children. New York: Macmillan, 1970.
38. Daly, C.J., Kelley, G.T., Krauss, A. Relationship between visual-motor integration and handwriting skills of children in kindergarten: A modified replication study. American Journal of Occupational Therapy. 2003;57:459–462.
39. Daniels, L.E., Ryley, C. Visual-perceptual and visual-motor performance in children with psychiatric disorders. Canadian Journal of Occupational Therapy. 1991;58(30):137–141.
40. Dankert, H.L., Davies, P.L., Gavin, W.J. Occupational therapy effects on visual-motor skills in preschool children. American Journal of Occupational Therapy. 2003;57:542–549.
41. de Boisferon, A.H., Bara, F., Gentaz, E., Cole, P. Preparation of young children to read: Effects of visual-haptic exploration of letters and visual perception of writing motions. L’Annee Psychologique. 2007;107:537–564.
42. D’Entremont, B., Hains, S.M.J., Muir, D.W. A demonstration of gaze following in 3-to-6 month olds. Infant Behavior and Development. 1997;20:569–572.
43. DeQuiros, J.B., Schranger, O.L. Neuropsychological fundamentals in learning disabilities. Novato, CA: Academic Therapy Publications, 1979.
44. Dunn, R., Griggs, S.A., Olson, J., Gorman, B., Beasley, M. A meta-analytic validation of the Dunn and Dunn learning styles model. Journal of Educational Research. 1995;88:353–363.
45. Durlach, N., Allen, G., Dorken, R., Garnett, R., Loomis, J., Templeman, J., et al. Virtual environments and the enhancement of spatial behavior. Presence: Teleoperators and Virtual Environments. 2000;9:593–616.
46. Dutton, G. Visual problems in children with damage to the brain. Visual Impairment Research–2002. 2002;4:113–121.
47. Dutton, G., Ballantyne, J., Boyd, G., Bradnam, M., Day, R., McCulloch, D., et al. Cortical visual dysfunction in children: A clinical study. Eye. 1996;10:302–309.
48. Enns, J.T., Cameron, S. Selective attention in young children: The relation between visual search, filtering, and priming. Journal of Experimental Child Psychology. 1987;44:38–63.
49. Farran, E.K., Cole, V.L. Perceptual grouping and distance estimates in typical and atypical development: Comparing performance across perception, drawing, and construction tasks. Brain & Cognition. 2008;68:157–165.
50. Fasotti, L., Kovacs, F., Eling, P., Brouwer, W.H. Time pressure management as a compensatory strategy training after closed head injury. Neuropsychological Rehabilitation. 2000;10:47–65.
51. Feder, K.P., Maynemer, A. Handwriting development, competency, and intervention. Developmental Medicine & Child Neurology. 2007;49:312–317.
52. Fegans, L.V., Merriwether, A. Visual discrimination of letter-like forms and its relationship to achievement over time in children with learning disabilities. Journal of Learning Disabilities. 1990;23:417–425.
53. Fox, T., Lincoln, N. Verbal mediation as a treatment strategy for children with non-verbal learning difficulties. International Journal of Therapy and Rehabilitation. 2008;15(7):315–320.
54. Gardner, M.F. Test of Pictures-Forms-Letters-Numbers-Spatial Orientation & Sequencing Skills. Burlington, CA: Psychological and Educational Publications, 1992.
56. Garzia, R. The relationship between visual efficiency problems and learning. In: Scheiman M.M., Rouse M.W., eds. Optometric management of learning-related vision problems. St. Louis: Mosby-Year Book, 1994.
57. Gentile, M. Functional visual behavior: A therapist’s guide to evaluation and treatment options. Bethesda, MD: American Occupational Therapy Association, 1997.
58. Gibson, E.J. Perceptual learning and the theory of word perception. Cognitive Psychology. 1991;2:351.
59. Gibson, E.J., Levin, H. The psychology of reading. Cambridge, MA: MIT Press, 1975.
60. Giles, D.C., Terrell, C.D. Visual sequential memory and spelling ability. Educational Psychology. 1997;17:245–253.
61. Gilfoyle, E., Grady, A., Moore, J. Children adapt, 2nd ed. Thorofare, NJ: Slack, 1990.
62. Glass, P. Development of visual function in preterm infants: Implications for early intervention. Infants and Young Children. 1993;6(1):11–20.
63. Goodale, M. Perception and action in the human visual system. In: Gazzaniga M.S., ed. The new cognitive neurosciences. 2nd ed. Cambridge, MA: MIT Press; 2000:365–377.
64. Goodale, M., Milner, L.S. Separate visual pathways for perception and action. Trends in Neuroscience. 1992;15:20–25.
65. Greene, L.J. Learning disabled and your child: A survival handbook. New York: Ballantine Books, 1987.
66. Griffin, J.R., Christensen, G.N., Wesson, M.D., Erickson, G.B. Optometric management of reading dysfunction. Boston: Butterworth-Heinemann, 1997.
67. Gulyas, B., Heywood, C.A., Popplewell, D.A., Roland, P.E., Cowey, A. A visual form discrimination from color or motion cues: Functional anatomy by positron emission tomography. Proceedings of the National Academy of Science USA. 1994;92:9965–9969.
68. Hammill, D.D., Pearson, N.A., Voress, J.K. Developmental Test of Visual Perception, 2nd ed. Austin, TX: Pro-Ed, 1993.
69. Hendry, S.H.C., Calkins, D.J. Neuronal chemistry and functional organization in the primate visual system. Trends in Neurosciences. 1998;21:244–349.
70. Hung, S.S., Fisher, A.G., Cermak, S.A. The performance of learning-disabled and normal young men on the test of visual-perceptual skills. American Journal of Occupational Therapy. 1987;41:790–797.
71. Hyvarinen, L. Assessment of visually impaired infants. Ophthalmology Clinics of North America. 1994;7:219–225.
72. Hyvarinen, L. Considerations in evaluation and treatment of the child with low vision. American Journal of Occupational Therapy. 1995;49:891–897.
73. Hyvarinen, L. Vision testing manual. La Salle, IL: Precision Vision, 1995.
74. Hyvarinen, L. Vision in children: Normal and abnormal. Medford, Ontario: Canadian Deaf, Blind and Rubella Association, 1988.
75. Ilg, F.L., Ames, L.B. School readiness. New York: Harper & Row, 1981.
76. Izard, C. Emotions and facial expressions: A perspective from differential emotions therapy. In: Russell J.A., Fernandez-Dols J.M., eds. The psychology of facial expression. New York: Cambridge University Press, 1997.
77. Jordan, B.A. Jordan Left-Right Reversal Test, 3rd ed. Los Angeles: Western Pscyhological Services, 1991.
78. Juel, C. Learning to read and write: A longitudinal study of 54 children from first through fourth grades. Journal of Educational Psychology. 1988;80:437–447.
79. Justice, L.M., Ezell, H.K. Descriptive analysis of written language awareness in children from low income households. Communication Disorders Quarterly. 2001;22:123–134.
80. Justice, L.M., Ezell, H.K. Use of storybook reading to increase print awareness in at-risk children. American Journal of Speech-Language Pathology. 2002;11:17–29.
81. Justice, L.M., Lankford, C. Preschool children’s visual attention to print during storybook reading: Pilot findings. Communication Disorders Quarterly. 2002;24(1):11–21.
82. Kandel, E.R., Schwartz, J.H., Jessell, T.M. Principles of neural science. New York: Elsevier Science, 1991.
83. Kavale, K. Meta-analysis of the relationship between visual perceptual skills and reading achievement. Journal of Learning Disabilities. 1982;15:42–51.
84. Kosslyn, S., Chabis, C.F., Marsolek, C.J., Koenig, O. Categorical versus coordinate spatial relations: Computational analyses and computer simulations. Journal of Experimental Psychology of Human Perceptual Performance. 1992;18:562–577.
85. Kulp, M., Earley, M., Mitchell, G., Timmerman, L., Frasco, C., Geiger, M., et al. Are visual perceptual skills related to mathematics ability in second through sixth grade children? Focus on Learning Problems in Mathematics, Optometry and Vision Science. 2004;80:431–436.
86. Kulp, M.T., Schmidt, P.P. Visual predictors of reading performance in kindergarten and first grade children. Optometry Vision Science. 1996;73:255–262.
87. Lee, S. A frame of reference for reversal errors in handwriting: A historical review of visual-perceptual theory. School System Special Interest Section Quarterly. 2006;13(1):1–4.
88. Leigh, R.J., Zee, D.S. Neurology of eye movements. Philadelphia: F.A. Davis, 1983.
89. Levine, M. Developmental variation and learning disorders. Cambridge, MA: Educators Publishing Service, 1987.
90. Levine, M., Hooper, S., Montgomery, J., et al. Learning disabilities: An interactive developmental paradigm. In: Lyon G.R., Gray D.B., Krasnegor N.A., Kavanagh J.F., eds. Better understanding learning disabilities: New views from research and their implications for education and public policy. Cambridge, MA: Educators Publishing Service, 1993.
91. Lukatela, G., Eaton, T., Lee, C., Turvey, M.T. Does visual word identification involve a sub-phonemic level? Cognition. 2001;78:B41–B52.
92. Luria, A. Higher cortical functions in man. New York: Basic Books, 1966.
93. Marr, D. Vision. San Francisco: Freeman, 1982.
94. Martin, N. Test of Visual Perceptual Skills, 3rd ed. Novato, CA: Academy Publishers, 2006.
95. McAvinue, L., O’Keeffe, F., McMackins, D., Robertson, I.H. Impaired sustained attention and error awareness in traumatic brain injury: Implications for sight. Neuropsychological Rehabilitation. 2005;15(5):569–587.
96. McCarty, M.E., Clifton, R.K., Ashmead, P.L., Lee, P., Goubet, N. How infants use vision for grasping objects. Child Development. 2001;72:973–987.
97. Menken, C., Cermak, S.A., Fisher, A.G. Evaluating the visual-perceptual skills of children with cerebral palsy. American Journal of Occupational Therapy. 1987;41(10):646–651.
98. Milner, A.D., Goodale, M.A. Visual pathways to perception and action. In: Hicks T.P., Molotchnikoff S., Ono T., eds. The visually responsive neuron: From basic neurophysiology to behavior. New York: Elsevier Science; 1993:317–337.
99. Muir, D.W., Nadel, J. Infant social perception. In: Slater A., ed. Perceptual development: Visual, auditory, and speech perception in infancy. East Sussex, UK: Psychology Press; 1998:247–286.
100. Necombe, F., Ratcliff, G., Disorders of spatial analysis. Boller, E., Grafman, J., eds. Handbook of neuropsychology, Vol. 2. New York: Elsevier Science, 1989.
101. Olsen, J.Z. Handwriting without tears: First grade printing teacher’s guide. Cabin John, MD: Handwriting Without Tears, 2008.
102. Optometric Extension Program Foundation. Santa Ana, CA: The Foundation, 2006.
103. Osterling, J., Dawson, G. Early recognition of children with autism: A study of first birthday videotapes. Journal of Autism and Developmental Disorders. 1994;24:247–257.
104. Parham, L.D. The relationship of sensory integrative development to achievement in elementary students: Four-year longitudinal patterns. Occupational Therapy Journal of Research. 1998;18:105–127.
105. Perov, A., Kozminsky, E. The effect of computer games practice on the development of visual perception skills in kindergarten children. Computers in the Schools. 1989;6(3/4):113–122.
106. Piaget, J. Development and learning. Ithaca, NY: Cornell University Press, 1964.
107. Pizur-Barnekow, K., Kraemer, G.W., Winters, J.M. Pilot study investigating infant vagal reactivity and visual behavior during object perception. American Journal of Occupational Therapy. 2008;62:198–205.
108. Quinn, P.C. Object and spatial categorization in young infants: “What” and “Where” in early visual perception. In: Slater A., ed. Perceptual development: Visual, auditory, and speech perception in infancy. Psychology Press, 1998.
109. Rafal, R.D., Posner, M.I. Cognitive theories of attention and the rehabilitation of attentional deficits. In: Meier M.J., Benton A.L., Diller L., eds. Neuropsychological rehabilitation. New York: Guilford Press, 1987.
110. Ratcliff, G. Perception and complex visual processes. In: Meier M.J., Benton A.L., Diller L., eds. Neuropsychological rehabilitation. New York: Guilford Press; 1987:182–201.
111. Raymond, J.E., Sorensen, R.E. Visual motion perception in children with dyslexia: Normal detection but abnormal integration. Visual Cognition. 1998;5:389–404.
112. Reid, D.T., Jutai, J. The Componential Assessment of Visual Perception manual. Toronto, Ontario: University of Toronto, Department of Occupational Therapy, 1994.
113. Reid, D.T., Jutai, J. A pilot study of perceived clinical usefulness of a new computer-based tool for assessment of visual perception in occupational therapy practice. Occupational Therapy International. 1997;4:81–98.
114. Reutzel, D.R., Smith, J.A. Accelerating struggling readers’ progress: A comparative analysis of expert opinion and current research recommendations. Reading and Writing Quarterly. 2004;20:63–89.
115. Ritty, J.M., Solan, H., Cool, S.J. Visual and sensory-motor functioning in the classroom: A preliminary report of ergonomic demands. Journal of the American Optometric Association. 1993;64(4):238–244.
116. Roder, B.J., Bushnell, E.W., Sasseville, A.M. Infant preferences for familiarity and novelty during the course of visual processing. Infancy. 2001;1(4):491–507.
117. Rogow, S.M. Visual perceptual problems of visually impaired children with developmental disabilities. Re:View. 1992;24(2):57–64.
118. Rogow, S.M., Rathwill, D. Seeing and knowing: An investigation of visual perception among children with severe visual impairments. Journal of Vision Rehabilitation. 1989;3(3):55–66.
119. Roley, S., Schneck, C. Sensory integration and the child with visual impairment and blindness. In: Smith Roley S., Blanche E., Schaff R., eds. Sensory integration and developmental disabilities. Tucson, AZ: Therapy Skill Builders, 2001.
120. Rose, S.A. Enhancing visual recognition memory in preterm infants. Developmental Psychology. 16(85), 1980.
121. Rosenhall, J., Johansson, E., Gilberg, C. Oculomotor findings in autistic children. Journal of Laryngeal Otology. 1988;102:435–439.
122. Rosner, J. Test of Visual Analysis Skills. Academic Therapy, 1999.
123. Sakata, H., Taira, M., Kusunoki, M., Murata, A., Tanaka, Y. The TINS lecture: The parietal association cortex in depth perception and visual control of hand action. Trends in Neurosciences. 1997;20(8):350–357.
124. Sands, S., Buchholz, E.S. The underutilization of computers to assist in the remediation of dyslexia. International Journal of Instructional Media. 1997;24(2):153–175.
125. Scheiman, M. Understanding and managing vision deficits: A guide for occupational therapists. Thorofare, NJ: Slack, 1997.
126. Scheiman, M., Gallaway, M., Coulter, R. Prevalence of vision and ocular disorders in a clinical pediatric population. Journal of the American Optometric Association. 1996;67:193–202.
127. Schneck, C.M. Intervention for visual perceptual problems. In: Case-Smith J., ed. Occupational therapy: Making a difference in the school system. Bethesda, MD: American Occupational Therapy Association, 1998.
128. Scholber, M., Mateer, C. Cognitive rehabilitation: An integrative neuropsychological approach. New York: Guilford Press, 2001.
129. Scott, L., McWhinnie, H., Taylor, L., Stevenson, M., Irons, P., Lewis, E., et al. Double-masked placebo-controlled trial of £9, precision spectral filters in children who use coloured overlays. Ophthalmic & Physiological Optics. 2002;14:365–370.
130. Seiderman, A.S., Marcus, S.E. 20/20 is not enough: The new world of vision. New York: Alfred A. Knopf, 1990.
131. Sergent, J. Judgments of relative position and distance on representations of spatial relations. Journal of Experimental Psychology: Human Perception and Performance. 1991;91:762–780.
132. Shaywitz, B.A. The Yale Center for the study of learning and attention: Longitudinal and neuro-biological studies. Learning Disabilities: A Multidisciplinary Journal. 1997;8:21–30.
133. Shaywitz, S.E. Dyslexia. New England Journal of Medicine. 1998;338:307–312.
134. Sigman, M., Parmelee, A. Visual preferences of four-month-old premature and full-term infants. Child Development. 1974;45:959–965.
135. Snow, C., Burns, M.S., Griffin, P. Preventing reading difficulties in young children. Washington, DC: National Academy Press, 1998.
136. Sortor, J., Kulp, M. Are the results of the Beery-Buktenica Developmental Test of Visual-Motor Integration and its subtest related to achievement test scores? Optometry and Vision Science. 2003;80:758–763.
137. Spelke, E.S., Cortelyou, A. Perceptual aspects of social knowing: Looking and listening in infancy. In: Lamb M.E., Sherrod L.R., eds. Infant social cognition: Empirical and theoretical considerations. Hillsdale, NJ: Erlbaum; 1981:61–83.
138. Stiers, P., De Cock, P., Vandenbussche, E. Separating visual perception and non-verbal intelligence in children with early brain injury. Brain and Development. 1999;21:397–406.
139. Stiles, S., Knox, R. Medical issues, treatments, and professionals. In: Holbrook M.C., ed. Children with visual impairments: A parent’s guide. Bethesda, MD: Woodbine House; 1996:21–48.
140. Suchoff, I.B. Visual-spatial development in the child, 2nd ed. New York: State University of New York, State College of Optometry, 1987.
141. Swinth, Y.L., Handley-Moore, D. Supplementary lesson 8: Handwriting, keyboarding, and literacy: What is the role of occupational therapy. In: Swinth Y.L., ed. Occupational therapy in school-based practice: Contemporary issues and trends. Bethesda, MD: American Occupational Therapy Association, 2004. [online course].
142. Teplin, S.W. Visual impairment in infants and young children. Infants and Young Children. 1995;8:18–51.
143. Thelan, D., Smith, L.B. A dynamic systems approach to the development of cognitions and action. Cambridge, MA: MIT Press, 1994.
144. Todd, V.R. Visual perceptual frame of reference: An information processing approach. In: Kramer P., Hinojosa J., eds. Frames of reference for pediatric occupational therapy. 2nd ed. Baltimore: Williams & Wilkins; 1999:205–256.
145. Toglia, J.P. Cognitive-perceptual retraining and rehabilitation. In: Crepeau E.B., Cohen E.S., Schell B.A.B., eds. Willard and Spackman’s occupational therapy. 10th ed. Philadelphia: Lippincott Williams & Wilkins; 2003:607–629.
146. Torgesen, J.K., Wagner, R.K., Rashotte, C.A. Longitudinal studies of phonological processing and reading. Journal of Learning Disabilities. 1994;27:276–286.
147. Tsai, C., Wilson, P.H., Wu, S.K. Role of visual-perceptual skills (non-motor) in children with developmental coordination disorder. Human Movement Science. 2008;27:649–664.
148. Tseng, M.H., Cermak, S.A. The influence of ergonomic factors and perceptual-motor abilities on handwriting performance. American Journal of Occupational Therapy. 1993;47:919–926.
149. Tseng, M.H., Murray, E.A. Differences in perceptual-motor measures in children with good and poor handwriting. Occupational Therapy Journal of Research. 1994;14:19–36.
150. Tsurumi, K., Todd, V. Tests of visual perception: What do they tell us? School System Special Interest Section Quarterly. 1998;5(4):1–4.
151. Turkewitz, G., Kenny, P.A. The role of developmental limitations of sensory input on sensory/perceptual organization. Developmental and Behavioral Pediatrics. 6(302), 1985.
152. Ulman, S. Visual routines. In: Pinker S., ed. Visual cognition. Cambridge: MIT Press; 1986:97–159.
153. Van der Geest, J.N., Kemner, C., Camfferman, G., Verbaten, M.N., Van Engeland, H. Looking at images with human figures: Comparison between autistic and normal children. Journal of Autism and Developmental Disorders. 2002;32(2):69–75.
154. Voyer, D., Voyer, S., Bryden, M.P. Magnitude of sex differences in spatial abilities: A meta-analysis and consideration of critical variables. Psychological Bulletin. 1995;117:250–270.
155. Wann, J., Kardirkamanathan, M. Variability in children’s handwriting: Computer diagnosis of writing difficulties. In: Wann J., Wing A., Sovik N., eds. Development of graphic skills: Research, perspectives, and educational implications. London: Academic Press; 1991:223–236.
156. Warren, M. Identification of visual scanning deficits in adults after CVA. American Journal of Occupational Therapy. 1990;44:391–399.
157. Warren, M. A hierarchical model for evaluation and treatment of visual perceptual dysfunction in adult acquired brain injury. I. American Journal of Occupational Therapy. 1993;47:42–54.
158. Warren, M. A hierarchical model for evaluation and treatment of visual perceptual dysfunction in adult acquired brain injury. II. American Journal of Occupational Therapy. 1993;47:55–66.
159. Weil, M.J., Cunningham-Amundson, S.J. Relationship between visuomotor and handwriting skills of children in kindergarten. American Journal of Occupational Therapy. 1994;48:982–988.
160. Westheimer, G., Levi, D.M. Depth attraction and repulsion of disparate foveal stimuli. Vision Research. 1987;27(8):1361–1368.
161. Williams, H. Perceptual and motor development. Englewood Cliffs, NJ: Prentice-Hall, 1983.
162. Willows, D.M., Terepocki, M. The relation of reversal errors to reading disabilities. In: Willows D.M., Kruk R.S., Corcois E., eds. Visual processes in reading and reading disabilities. Hillsdale, NJ: Erlbaum; 1993:265–286.
163. Ziviani, J. The development of graphmotor skills. In: Henderson A., Pehoski C., eds. Hand function in the child: Foundations for remediation. St. Louis: Mosby; 2006:184–193.
164. Ziviani, J., Hayes, A., Chant, D. Handwriting: A perceptual motor disturbance in children with myelomeningocele. Occupational Therapy Journal of Research. 1990;10:12–26.
165. Zoltan, B. Visual processing skills. Vision, perception, & cognition, 4th ed. Thorofare; NJ: Slack, 2007.