Influencing Participation Through Assistive Technology
1 Define and articulate the purposes of assistive devices and services and their relevance to the practice of occupational therapy.
2 Understand legal mandates regarding assistive technology service delivery.
3 Identify guiding frameworks/models that influence decisions about assistive technology.
4 Recognize and participate in a collaborative team approach for providing assistive technology services.
5 Describe application of assistive technology to enhance or improve childhood occupations across practice settings.
6 Apply a child and family-centered approach to evaluation, selection, and implementation of assistive technology.
7 Recognize cultural differences and their impact on acceptance of assistive technologies.
8 Recognize the continuum and interrelationship between no-tech and high-tech solutions.
9 Understand and apply evidence-based practices throughout the service delivery process.
“Not every child has an equal talent or an equal ability or equal motivation; but children have the equal right to develop their talent, their ability, and their motivation.”
INTRODUCTION
Assistive technology (AT) has been an important tool since the origins of the occupational therapy profession, as well as throughout its history, to improve function and participation. Traditionally, therapists have used different types of adaptive equipment, such as reachers, buttonhooks, and pencil grips, to promote functional independence in their clients. However, within the past 10 to 15 years, with the rapid technological advances in society, specifically with the introduction of the microprocessor chip, occupational therapists have increasingly used a wide range of electronic devices, from simple switches to complex robotics, to support meaningful occupational engagement. Stoller described AT as “special devices or structural changes that promote a sense of self-competence, the further acquisition of developmental skills into occupational behaviors, and/or an improved balance of time spent between the occupational roles in an individual’s life as determined by the individual’s goals and interests and the external demands of the environment” (p. 6).100
“Occupational therapy practitioners’ understanding of their clients’ daily occupational needs, abilities, and contexts make them ideal collaborators in the design, development, and clinical application of new or customized technological devices” (p. 678).3 Assistive technologies may unlock human potential and optimize human performance throughout the life span and across contexts, and allow individuals to assume or regain valued life roles. The selection of the “right tool for the job” bridges the gap between what people want to do and what they can do to participate in activities that are meaningful and life sustaining. Assistive technologies can serve a variety of needs and can be part of the educational and/or rehabilitative process depending on the environment in which services are provided. Congress has enacted a variety of legislation designed to support the procurement and use of AT for individuals with disabilities. This expansion in the use of AT opens new doors, creates opportunities, and enables individuals with disabilities to realize functional goals that were previously unattainable. Although the materials, structure, and form of devices used continue to change over time, the primary emphasis of AT across the lifespan continues to be on functional outcomes for AT users above all other considerations.28 With the influx of technology into the daily lives of all individuals comes the increased responsibility for occupational therapists to keep abreast of current trends so that the tools they recommend and implement can produce the best outcomes for the clients they serve.
Influencing Childrens’ Growth and Development with Assistive Technology
Children have an “inborn drive to discover and learn” (p. 1)19 that motivates them to understand the world around them, strive for independence, establish a sense of self, and connect socially with others. When a disabling condition is present, children may have difficulty with accessing play, learning, or self-care activities. Burkhart offered four “secrets” to support children’s successful engagement: (1) create motivating activities, (2) develop opportunities for active participation, (3) present information and materials using multiple modalities, and (4) use authentic learning scenarios in natural contexts.19 Research indicates that AT can be instrumental in helping young children with disabilities learn valuable life skills such as social skills, including sharing and taking turns, communication skills, attending, fine and gross motor skills, self-confidence, and independence.7,54,76,105,107 As children grow, they may use technology to develop independence in many activities of daily living (ADLs) and instrumental activities of daily living (IADLs), complete school assignments, develop prevocational and vocational skills, increase opportunities for social participation, and play games or participate in leisure activities. The use of AT can create exciting opportunities for children to explore, interact, and function in their environments.
For children with disabilities, introducing the appropriate types of technology systems as early as possible may enable the child to participate in important learning situations that otherwise, because of his or her disabilities, may not be possible. For more than 20 years, researchers and clinicians have documented and discussed the unique opportunities that all types of AT offer for teaching and for advancing the life choices of children with disabilities.9,10,33,43,54,61,85,101,105
Because technology is constantly changing, this chapter presents problem-solving strategies, principles, and frameworks for decision making versus in-depth descriptions of specific devices or systems. The frameworks and guidelines for decision making that are presented should not be viewed as limiting strategies. Rather, they are meant to be a starting point. Each practitioner needs to adjust the concepts given the individual needs of the client and family, teaming issues, availability of resources, and many other factors unique to each situation.
Definition and Legal Aspects of Assistive Technology
AT comprises a broad range of devices, services, strategies, and practices used to address functional problems encountered by individuals who have disabilities.28 Assistive technology is legally defined by Public Law (PL) 108-364 The Assistive Technology Act of 1998, as amended: “any item, piece of equipment or product system whether acquired commercially off the shelf, modified, or customized that is used to increase, maintain or improve functional capabilities of individuals with disabilities.”
PL 108-364 further defines an AT service as any service that directly assists an individual with a disability in the selection, acquisition, or use of an AT device. The law includes several clarifications to enhance the definition of AT service: (1) evaluating needs and skills for AT; (2) acquiring assistive technologies; (3) selecting, designing, repairing, and fabricating AT; (4) coordinating services with other therapies; and (5) training both individuals with disabilities and those working with them to use the technologies effectively.
In a similar manner, the Individuals with Disabilities Education Improvement Act (IDEA) (PL 108-446) defines both AT devices and services as a means of providing a free and appropriate public education (FAPE). IDEA 2004 requires that individualized education program (IEP) and individualized family service plan (IFSP) teams consider a child’s need for AT devices and services at least annually during the development of the IEP/IFSP. Additional information regarding other legislation related to AT can be found in Table 20-1.
TABLE 20-1
Other Legislation Related to Assistive Technology
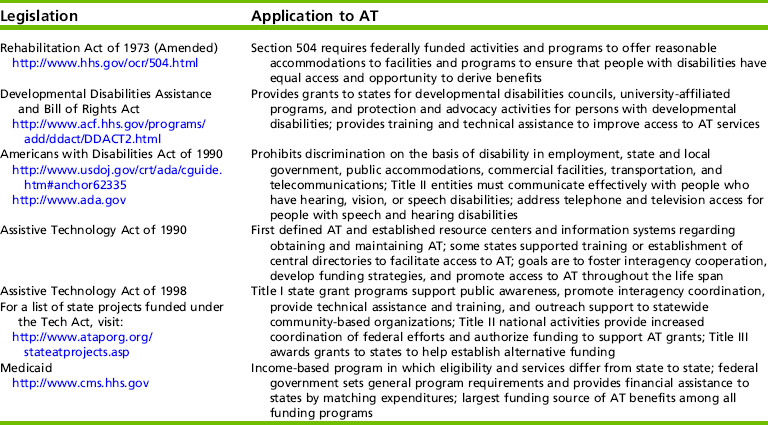
From Cook, A., & Polgar, J. (2008). Cook & Hussey’s assistive technologies: principles and practice (3rd ed.). St. Louis: Elsevier.
In this chapter, assistive technology is used as a broad term that encompasses devices ranging from low technology to high technology. Low-tech devices (e.g., pencil-and-paper communication boards and built-up foam handles) are inexpensive, simple to make, and easy to obtain. High-tech devices (e.g., wheelchairs, augmentative communication devices, and computers) are generally expensive, more difficult to make, and more difficult to obtain. Mid-tech devices fall somewhere in between and may consist of hand-made or commercially available items.
This chapter discusses general information regarding the use of AT with children, followed by specific examples of application. Other chapters in this text specifically address the other areas of AT (see Chapters 16 and 21). Many of the principles and decision-making strategies discussed in this chapter can be generalized to all areas of AT.
Models for Assistive Technology Assessment and Decision Making
“When matching person and technology, you become an investigator, a detective. You find out what the different alternatives are within the constraints.”
—From Living in the State of Stuck: How Technology Impacts the Lives of People with Disabilities
The occupational therapy practitioner uses a variety of theories and practice models to guide the occupational therapy process (evaluation, intervention, and outcome monitoring). Practice models specifically related to AT help occupational therapists make decisions regarding its use and facilitate the integration of AT within the practice of occupational therapy.
Assessment tools and models to guide AT evaluation and service delivery have been developed by a number of professionals.7,16,28,91,109,113 Each of these models provides a framework for evaluating needs, making decisions, and implementing intervention. Using a model for service delivery helps to ensure that the evaluation process is systematic and complete. Three models are highlighted in this chapter.
The Human Activity Assistive Technology (HAAT) model,28 the Student Environment Task Tool (SETT) framework,113 and the Matching Person and Technology (MPT) assessment process90 follow the person-environment-occupation (PEO) model65 and emphasize an occupation-based approach to AT practice. These models provide frameworks for decision making regarding the selection, implementation, and evaluation of AT.28
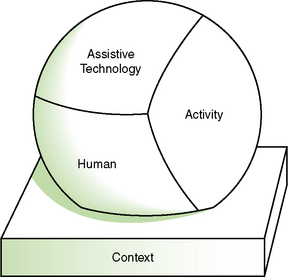
Human Activity Assistive Technology
The HAAT model (Figure 20-1) is a dynamic and interactive model in which three factors—the human, activity, and AT—form a collective whole that is then placed within the context of participation.28 The human component includes physical, cognitive, and emotional elements. Activities are synonymous with occupations (e.g., self-care, productivity, leisure), and AT refers to a device and/or service. The context is strongly emphasized as a determining factor for outcomes.28
Student Environment Task Tool
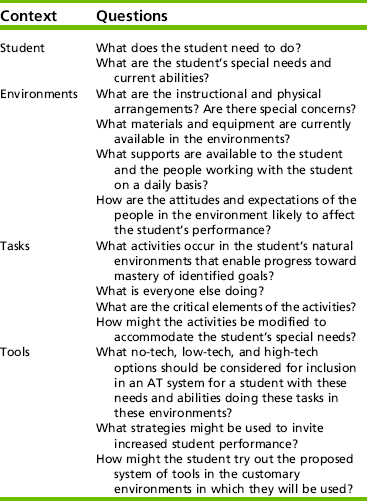
A framework developed specifically for school settings is referred to as the SETT framework: student, environment, task, and tools. This framework is designed to support good decision making that promotes collaboration, communication, sharing of knowledge and perspectives, flexibility, and ongoing processes among educational team members.113 It supports a student’s participation in curricular and extracurricular activities throughout the school day. SETT includes a series of questions that are designed to guide discussion, evaluation, and intervention. Teams may choose to use a few or all of the questions, depending on the needs of the student. Table 20-2 outlines the SETT questions. Many of these questions are consistent with the type of information that an occupational therapist gathers as part of the occupational profile and occupational performance analysis, and they appear applicable to a variety of settings.
Matching Person and Technology
The MPT model and assessment process are designed to help individualize the process of matching each person with the most appropriate AT. This model and process consider three factors: milieu (i.e., characteristics of the environment and psychosocial setting in which the person uses the technology), personality (i.e., personality, temperament, and preferences), and technology (i.e., functions and features).90
Child- and Family-Centered Approach
The social context of AT use can be considered the most influential and important, because it is often the social environment, including the attitude of others, that creates a disability more than the physical barriers in the environment.28 Any person (e.g., parent, sibling, teacher) who interacts with an individual using AT, either directly or indirectly, is considered part of the social context. The simple presence of a disability can be socially stigmatizing, and the introduction of AT can add additional burden, particularly when individuals within the social environment do not support use of the technology. It is important to recognize key individuals who provide assistance to the child using AT across environments (e.g., home, school, work), because technology use is facilitated when assistance is received from consistent individuals.
Each person’s unique culture influences the manner in which he or she interacts with others and the importance of participation and engagement in various activities and life roles.28 Some cultures do not value the independence that AT provides individuals with disabilities, or an AT device may be abandoned if it replaces an important life function of another family member. For example, the grandmother who views communicating for a child with cerebral palsy as one of her roles may resist the child’s use of an augmentative communication system. Cultural factors must be considered in providing AT devices and services. Box 20-1 summarizes some sociocultural factors that the therapist may need to consider when evaluating, designing, and selecting AT systems for children.
Abandonment
We are fascinated with technology. We expect it to make a difference in our lives, and particularly in education. We see its effects as beneficial. We look for it to change and improve what has come before. We await technological improvements in our lives, from better toaster ovens to improved, more efficient schools… (p. 3).57
Despite the many promises of technology, one third or more of individuals discontinue their use of their AT device.90 Abandonment can mean the device is no longer needed, but more often it signifies a mismatch between the user and the device. When a device fails to live up to its promise of potential, freedom, and independence, disillusionment with the idea of AT may result. Failure to take into consideration the user’s preferences, ideas and desires for an AT device is a primary reason for abandonment.77,90 Users of AT, their families, and/or educational staff may have high expectations for an AT device and can be devastated when expectations are not fully met with far-reaching results.
Learned Helplessness and Self-Determination
Psychologist Norris Hansell theorized that there are seven essential and interrelated attachments necessary to create a sense of connectedness and quality of life.49 These include having the supports necessary for existence (food, water, air, information); identity; connection with other persons; connection to groups; connection to a social role; money and purchasing power; and a system of meaning, each implying reciprocity with others. When this reciprocity is thrown off balance by internal or external circumstances, a sense of isolation, helplessness, and hopelessness can occur. “Human beings can be proactive and engaged, or, alternatively, passive and alienated, largely as a function of the social conditions in which they develop and function” (p. 68).88 Ryan and Deci determined the needs for competence, relatedness, and autonomy as essential for social development and personal well-being.88 AT can build bridges or create additional barriers between the user and the environment in which he or she wishes to participate.
Children with disabilities can become passive and unmotivated because of a lack of learning opportunities or a lack of independent control over their environment. This can result in decreased interest in or skills to interact with the environment.35 When children perceive that they have little control over outcomes within their environments, the phenomenon of learned helplessness can result. Learned helplessness is a secondary disability and is the belief that one cannot exert personal control over outcomes experienced when interacting with the environment.1,69 Children with learned helplessness exhibit low self-esteem, directly affecting how they interact and perform functional skills. They usually demonstrate a lack of initiation and an inability to cope with the events around them. In addition, when opportunities for integrating basic cognitive and perceptual skills are missed in early childhood, these children do not develop a foundation for learning higher-level concepts. Strategies and adaptations that allow these children the maximum amount of independence possible as early as possible decrease the chance for them to learn that they have no control over their environment.
The opposite of learned helplessness is self-determination. Self-determination is defined as “acting as the primary causal agent in one’s life and making choices and decisions regarding one’s quality of life free from undue external influence or interference” (p. 24).110 Self-determination is an umbrella term that encompasses several common concepts used in describing children’s personal, social, and skill development. These concepts include self-efficacy (outcome and efficacy expectations), self-esteem, and self-advocacy. Efficacy expectations are personal beliefs regarding one’s capability to realize a desired behavior in a specific context (judgment of what one can do with the skills one has). Outcome expectations are personal beliefs about whether a particular behavior will lead to a particular consequence (being able to determine if one’s goals are realistic). Self-esteem is the belief that one has in oneself, or self-respect. Self-advocacy refers to an individual’s being able to speak for him or herself, make decisions for him or herself, and know what his or her rights are, particularly when those rights have been violated or diminished. The individual is able to take ownership of his or her needs, rather than expecting someone else to take responsibility for them because he or she has a disability.104,110 Appreciating and being able to function with a sense of interdependence are also crucial parts of self-determination.
Self-determination is a set of skills that can be taught and learned. Key characteristics and components include autonomy, self-awareness, choice making (i.e., often children with disabilities are not given the opportunities to make effective choices), decision making, problem solving, goal setting and attainment, internal locus of control, positive attributions of efficacy and outcome expectations, and self-knowledge.110 With the increased emphasis on transition services and preparing children for life skills beyond school, occupational therapists should promote the development of self-determination for children of all ages. This includes ensuring that services develop skills of interdependence and independence, addressing the participation and productivity of children, recognizing that self-determination can mean different things to different people, and recognizing that self-determination is a quality-of-life issue that can be addressed across settings, environments, and opportunities. AT devices can help with the development, practice, and effective use of self-determining behaviors for children with disabilities.
SETTING THE STAGE FOR ASSISTIVE TECHNOLOGY SERVICE PROVISION
“The institutional context refers to larger organizations within a society that are responsible for policies, decision-making processes, and procedures” (p. 43).28 The International Classification of Function, Disability, and Health (ICF) categorizes economic, legal, and political components as services, systems, and policies. This institutional overlay has major implications for both the acquisition and use of AT, with regards to funding, legislation related to environmental and community access, as well as standards that govern product design, function, and safety standards.28
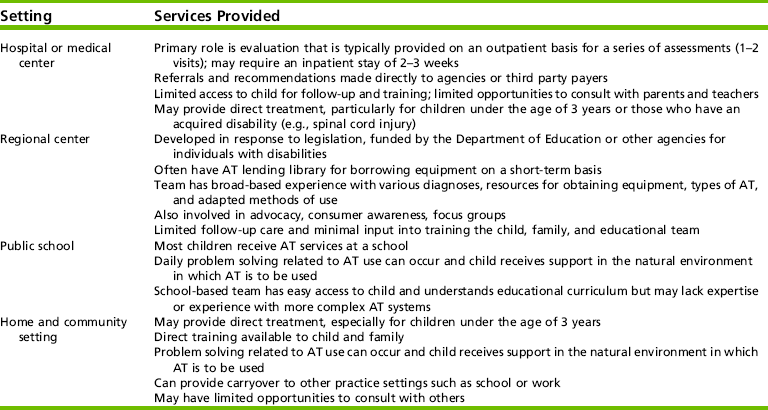
Differences in practice settings in which occupational therapy practitioners who use AT may be employed are outlined in Table 20-3. The role of the OT practitioner in each of these settings is governed by a combination of professional scope of practice, the expertise of other members of the team, and the agency or funding source.
Occupational Therapy Process and Assistive Technology in the Schools
According to the most recent statistics published by the U.S. Department of Education, Office of Special Education Programs, as required under the IDEA, an estimated 7.1 million children from birth to 21 years of age receive special education services.108 Most children who need AT receive those services in school. AT devices and services are provided if necessary for a child to receive FAPE in the least restrictive environment (LRE). The need for AT must be considered, at least annually, for all children who receive services under IDEA. When AT is a necessary part of the student’s program, then the school district is responsible to make sure that it is available to the child. It is not uncommon for the expertise of an occupational therapy practitioner to be requested when the team is considering AT for a student. Guides and models for considering AT for students in special education are available online (see Appendix 20-A on the Evolve website for Internet resources).
Baush, Ault, and Hasselbring indicated that appropriate AT devices and services can help a student improve, increase, or maintain performance to perform or develop functional skills (e.g., self-help, mobility, or communication), access curriculum (e.g., multimedia presentations or books on tape), become a more efficient learner (e.g., pencil grips and raised lined paper to improve writing legibility), or compensate for lack of skills (e.g., word prediction software to assist with spelling or reduce keystrokes).8 The roles and responsibilities of IEP team members, including the occupational therapist, providing AT services within a school setting are listed in Box 20-2.
The Transdisciplinary Team
The provision of AT services occurs across disciplines, and the training and experience of the service providers has not been widely studied112 (Research Note 20-1) and the profession of “assistive technologist” does not exist.95 Professionals specialize in AT on the basis of personal interest and self-study. Several universities offer certificate programs and advanced degrees in AT. In addition, the Rehabilitation Engineering and Technological Society of North America (RESNA) has established a mechanism for verifying a minimum level of competence for individuals serving as AT providers through an examination process that provides credentialing for persons working as assistive technology practitioners (ATPs). The ATP usually has a background in a rehabilitation discipline such as occupational therapy, physical therapy, speech-language pathology, or engineering.
 RESEARCH NOTE 20-1
RESEARCH NOTE 20-1
The training of providers working with children who need AT devices or services has not kept pace with the variety and complexity of AT devices available. This article reports on a survey of pediatric occupational therapists who responded to questions about their training needs in the area of AT and delivering AT services. A large number of respondents reported less-than-adequate training in policies governing AT services and the organization and function of the service delivery system. Therapists reported a need and interest for accessible and affordable training in the areas of funding of technology and services; collaborating with families and other service providers; and accessing reliable, knowledgeable vendors.
• Policy and practice context for providing AT services has become more complex, and practitioners are faced with, or unaware of, new and more sophisticated devices that might promote more opportunities for meaningful participation in their clients with disabilities.
• A majority of pediatric occupational therapists in this national sample rated their preparation in the area of AT as being less than adequate, and rated their confidence in terms of delivering AT and AT services as low.
• Training in identification of funding sources and use of high-tech devices is among the most pressing training needs.
Long, T. M., Woolverton, M., Perry, D. F., & Thomas, M.J. (2007). Training needs of pediatric occupational therapistsin assistive technology. American Journal of OccupationalTherapy, 61, 345–354.
As with many other specialty areas in pediatrics, the successful implementation of AT requires a cohesive and effective team that emphasizes shared vision and ownership. The team’s input is critical to making decisions regarding AT because devices are used across the child’s environments and address multiple performance goals that cross professional boundaries. Decisions that the transdisciplinary professional team and the family make together are most likely to meet the multifaceted needs of the child. The child and the family are considered members of the team in all forms of service delivery.
The specific members of the team may be different in various situations depending on the type of device being introduced to the child, the expertise of the individuals involved, and the specific setting. For example, in a clinical setting, the team may include the child and family, occupational therapist, physical therapist, speech-language pathologist, doctor, nurse, rehabilitation engineer, and social worker. In school-based practice, the team may include the child and family, occupational therapist, physical therapist, speech-language pathologist, educator, administrator, and psychologist.
In some settings, occupational therapy assistants and aides provide some of the AT services. Assistants are particularly helpful in training a child to use a system once the therapist has set up and established the program. Assistants and aides may also be involved in practicing use of the device with the child and helping others use the systems. Therapists working in AT service delivery must determine which activities are appropriate to delegate and which activities are specialized and require the training and skills of a therapist.
Assistive Technology Evaluation and Intervention: A Dynamic Process
The occupational therapist has a key role on the AT evaluation team. The unique perspective on occupation and engagement in meaningful activities that the occupational therapist offers the team is helpful in determining needs, problem-solving potential solutions, and evaluating outcomes. The assessment of client satisfaction has been one of the key factors in determining the effective implementation and usefulness of AT in the lives of individuals with disabilities.30,31,90,92,104
In addition to evaluation and intervention services, AT services may also include device procurement, training, skill acquisition, monitoring, and other services that support and enable the child’s participation in home, school, and community activities. Because of the complexity of many AT systems, specifically those that are high-tech, the therapist needs a systematic procedure for follow-up and adjustments to help ensure the viability of the system over time. These steps of the process are dynamic rather than linear and sequential. For example, intervention may begin by addressing prerequisite skills for AT use before completing the AT evaluation and procuring a specific device. Once a system has been chosen and purchased, evaluation, monitoring, and decision-making processes continue throughout intervention.
Evaluation
When evaluating AT needs, the occupational therapist closely examines the child’s abilities and difficulties, demands of the environment and task, and the child’s goals. The first step of the evaluation is to identify key activities that the child or family needs or wants him or her to do. The Canadian Occupational Performance Measure is a useful tool to assist with the identification of client-centered goals and the importance of the goals.64 The importance that an individual assigns to an activity helps predict whether he or she will accept technology that enables participation in that activity.98
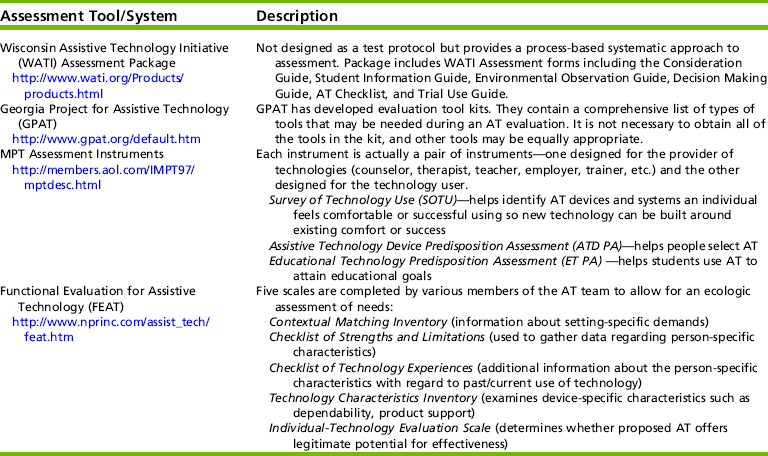
A number of inventories, checklists, and processes have been developed to assist with evaluation.95 When an evaluation is requested, observation should occur in the student’s natural environment, which might include home, school (e.g., classroom, playground, lunchroom, bathroom, extracurricular areas), and community settings (e.g., work settings or other relevant locations). All the factors that are traditionally considered when conducting an occupational therapy evaluation, including frequency or duration needed to complete an activity, have a direct relationship to potential AT recommendations (Box 20-3). During the evaluation, it is important that any existing technology used by the child and its effectiveness in the customary environment be documented. A complete occupational therapy evaluation may or may not be a component of the AT process depending on the practice setting in which it occurs. Formal and informal assessments that may be used during the evaluation process are described in Table 20-4.
The AT evaluation may be completed by the team who will also provide the intervention (e.g., fitting and training of the device) or a team that has been formed specifically for the purpose of completing AT evaluations. Many hospitals, clinics, and some community agencies and schools have a designated AT team because of the complexity of many AT systems. The occupational therapist who does not work with AT on a regular basis may have difficulty maintaining expertise on all the systems and devices available because of the number of devices and the rapid development of new systems. When separate teams are responsible for evaluation and intervention, ideally these teams collaborate to make decisions and recommendations.
In addition to a comprehensive evaluation, a trial period with different types of AT is needed to achieve a good match between the AT device or system and the child and family. The trial period may be one of the most important aspects of the AT evaluation. These trials can help prevent the costly procurement of an incorrect device. The cost of AT includes not only the purchase of the device but also the ongoing expenses for maintenance, upgrades to the system, and repairs. Questions that the therapist should address throughout assessment and intervention in relationship to cost include the following105:
• What financial resources are available to the family?
• When the AT device is in need of repair, does the family have access to services?
• Does the AT device significantly increase the child’s level of independence and function?
• Can the AT device be adapted to enable higher levels of function as the child grows and matures?
• Can a less complex device meet the same needs just as well?
The team discusses these issues and others unique to each family in deciding whether the system is a reasonable and appropriate investment for the family that will result in increasing the child’s functional independence. The team should present the child and family with objective and realistic information regarding investment in and use of AT.
Given a complete description of the options and alternatives, the family and the team make the final decision as to what AT is implemented and how it is incorporated into the child’s program. Box 20-4 presents 11 criteria, developed by more than 700 AT consumers, that the team should use to evaluate different AT devices. In summary, AT evaluations should be conducted (1) as part of an ongoing process linked to educational and/or therapeutic planning, (2) by a team within the natural setting where the child needs to engage in his or her occupations, (3) with trials with potential AT devices, and (4) with meaningful follow-through involving all team members.83
Decision Making
Occupational therapy practitioners use problem-solving and clinical reasoning skills throughout the process of procurement, implementation, and follow-up with AT. Problem solving should involve defining the situation or problem, determining the short- and long-term goals, and brainstorming potential processes to reach the determined goals. The therapist is often tempted to define the situation or problem and immediately jump to a possible technology for fixing the problem. However, if the therapist does not consider the short- and long-term goals before discussing potential solutions, the strategies implemented may not have a long-term benefit for the child. Many tools are available to support problem solving and decision making.
In addition to the assessment tools described in Table 20-4, The Council for Exceptional Children Technology and Media Division (TAM) website (http://www.tamcec.org/publications/index.htm) offers several tools, including an AT Consideration Wheel (Figure 20-2) that can help school teams consider a wide range of options, and a series of “fans” with user guides that feature technology devices on each blade, along with resources for locating the devices. Ablenet, a software company, has a CD-ROM available that provides information about low-tech devices and the use of simple communication aids for children with disabilities (http://www.ablenet.com). Finally, new information that supports effective decision making for children with disabilities is continually being added to the National Center for Technology Innovation (NCTI) website (http://www.nationaltechcenter.org). Because of the rapid changes with technology in our society, practitioners working in this area of practice need to develop a strategy for keeping current with best practices related to effective decision making.
FIGURE 20-2 AT products available from the Technology and Media (TAM) Division of the Council for Exceptional Children, Reston, VA. Photo courtesy Judith Schoonover.
When working with children of any age, the team, including the occupational therapist, should consider short- and long-term goals in terms of what the child’s needs are at present, 1 year later, 3 to 5 years later, and 7 to 10 years later. This can be difficult in working with young children, but the information can facilitate decision making, especially in addressing AT needs. In working with an adolescent, the focus becomes a successful transition plan, independence in the community, and participation in work roles. The procurement and use of the AT can be a critical part of a successful transition into future life roles for an adolescent.18,63,99 The team should revisit and rewrite goals systematically as the child grows and matures, as contexts change, as child and family needs and desires change, and if the child’s medical condition changes.
Lahm and Sizemore interviewed AT teams to identify factors that influenced decision making in selecting AT.62 Important factors included client goals, environmental demands, family/client demands, and client diagnosis. Funding was considered but was lower in importance. Because an awareness of environmental demands was another important factor, evaluations should include strategies for gathering information about the environmental demands (e.g., phone interviews) to facilitate the best decision making.
Device Procurement
It can take up to several months to procure an AT device. When funding issues stall the process, members of the team may be involved in writing letters of justification to insurance companies and other third-party payers. Careful documentation during the trial periods with different devices can help with this process. Documentation can include videos or pictures of the child using the system that demonstrates how the system helps improve his or her function.
Once the system has arrived, the team works to put the system together, test the system, and begin training. Some companies provide vendors that can help with the process, and others have videos that come with the system. However, it is not uncommon for a system to be delivered with minimal instructions. This can be daunting to the family if the system is delivered directly to the home and family members and other support providers are unsure how to use it. Comprehensive intervention and education are needed to help the child and family incorporate the device into their daily lives.
Funding
Occupational therapy practitioners working in the area of AT are often involved in helping procure the appropriate devices. In particular, they often provide the documentation used in applying for funding. Funding can come from various sources, including Medicaid, grants, private insurance, nonprofit agencies such as United Cerebral Palsy, private foundations, schools, and individual payment. In some states, funds are available through the Department of Developmental Disabilities, the Department of Health, or the Department of Social Services to help purchase AT devices. As students enter high school and begin the transition to work and career sites, the state’s vocational rehabilitation agency may also assist with the funding of devices. In addition, there are some alternative sources of funding that the team may want to consider.21 These include community service organizations, equipment loan programs, used and recycled equipment, and technical assistance projects. Often these alternative sources can take additional time and effort to research and contact. However, when a family or system has limited resources, pursuing creative funding options can result in the successful procurement of a device. When families cannot afford new devices or secure funding, they may explore AT reuse programs such as the Pass It On Center coordinated by the U.S. Department of Education’s Office of Special Education and Rehabilitative Services (OSERS), because these programs often do not have eligibility requirements.75 Occupational therapists should learn about the different funding options available within their state and region to contribute to the team’s effort to obtain funding for AT devices.
Funding of AT in school districts often raises unique issues. The school district is the payer of last resort, but it is ultimately responsible for AT devices that the child needs to learn in the school environment.21,106 Public or private insurance can be applied to obtain AT devices and services when they are determined to be medically necessary.96 The use of these funds must be voluntary on the part of the parents and with their written consent. School districts can also work with community service organizations or associations (e.g., the Muscular Dystrophy Association) to purchase AT devices or pay for services. If the AT device is purchased with the parents’ funds or insurance, then the device belongs to the child and the child’s family. However, if the school district purchases the device, then the school district owns the device.74,109
Often the occupational therapist writes or assists with writing a letter of justification to support the funding of an AT device. Strong supporting documentation that clearly demonstrates the necessity of the device to strengthen the child’s engagement in occupation is an important part of the process. This documentation is based on the evaluation data gathered by the team and takes into consideration the language and priorities of the funding agency.21 If the letter is written to a health insurance agency, then medical necessity must be emphasized; if it is directed to an education-related funding source, then it must address the child’s ability to access and participate in educational programming. Requests to vocational agencies must address employment potential and skills.21,93,109 Other key elements in the letter may include information about the child, the device, the evaluation procedures including results of any trials conducted, and the environment(s) in which it will be used; how the child will benefit from the device; alternative or potential outcomes of not being provided the device; supporting photos or measurements; and information about the cost of the device and other options considered.
Implementation of AT Services
An AT implementation plan should include: person(s) responsible, conditions of use, frequency of use, and duration of use. The team considers all of the tasks and contexts in which the AT will be used. Thus, for example, if a student requires a voice output communication system, it should be readily available at all times throughout his day (e.g., at lunch or recess to socialize, during instruction to ask or answer questions, during independent work to indicate needs and wants, and at home to interact with his/her family).
The introduction of an AT device, especially a complex device, can change the focus of a child’s program. Time must be spent on training and practice within the child’s natural environments (i.e., school, home) as the family and professionals make efforts to integrate use of the device into the child’s everyday activities. Thus, the development of skills needed to use the device often becomes the focus of intervention. Involvement by every member of the team encourages skill generalization to various settings and situations of the child. When staff are encouraged to work as a team and time provided for them to communicate, the effectiveness of AT is likely to increase.16 The AT devices should be readily accessible; if the device or strategy takes longer than 60 seconds to access and set up, it is less likely to be used. Examples of forms used to document an implementation plan (e.g., the NATRI Assistive Technology Implementation Plan and the QIAT Plan for Evaluation of Effectiveness of AT Use) can be accessed at the Evolve website.
Education Tech Points: A Framework for Assistive Technology Planning, as developed by Gayle Bowser and Penny Reed, identifies key points to assist educational teams in making decisions regarding the use of AT services and facilitates identifying resources that can be written into the child’s IEP.16 These points are beneficial for AT teams to consider regardless of the practice setting. Implementation and periodic review of the plan will help avoid the potential abandonment of recommended AT devices and services. Considerations related to AT implementation and day-to-day operations may include the following16:
Measuring Progress and Outcomes
Not only does good AT decision making require an eye on the future, but evaluating the outcomes of AT takes a long-term commitment32 to ensure that it continues to support the child’s engagement and participation in purposeful activities. Often it is difficult to operationalize and define global outcomes specific to AT.44 The goal of outcome measurement is to determine the efficacy and utility of AT devices and implications for abandonment. It is important that occupational therapists as members of AT teams select appropriate outcome measures to help determine whether devices and services have the intended effect.
Data collection is critical to evaluating AT’s success. The team should be involved in a collaborative discussion regarding how data will be collected. Data collection should be simple and straightforward enough for all team members including family members to understand and complete with ease. Often, there are various ways to measure effectiveness or differing ideas on what the desired response or outcome of the child should be. For example, when designing a data sheet for switch use, one needs to consider which part of the body will be used to activate the switch, how much wait time will be allowed before a prompt is given, the type of prompt to be given (e.g., visual, verbal, hand-over-hand,), and how to define objectively what constitutes success for the given task (e.g., single switch activation, activation or deactivation of an electronic device, holding a switch for a specified amount of time). The occupational therapist can guide the team in a discussion of how to measure the child’s performance.95
Data collected over time can support the continued use of AT devices already in place or justify the need for follow-up evaluation. Often data are collected on targeted goals and objectives and are dependent upon the service settings in which the device is used. Possible factors to measure include changes in the child’s performance or level of function, change in level of participation, how often the device is used and under what circumstances, overall consumer satisfaction, goal achievement, quality of life, and cost analysis/savings. Table 20-5 outlines a number of assessments that may be used to evaluate outcome measures for AT.5
TABLE 20-5
Assistive Technology (AT) Outcome Measures
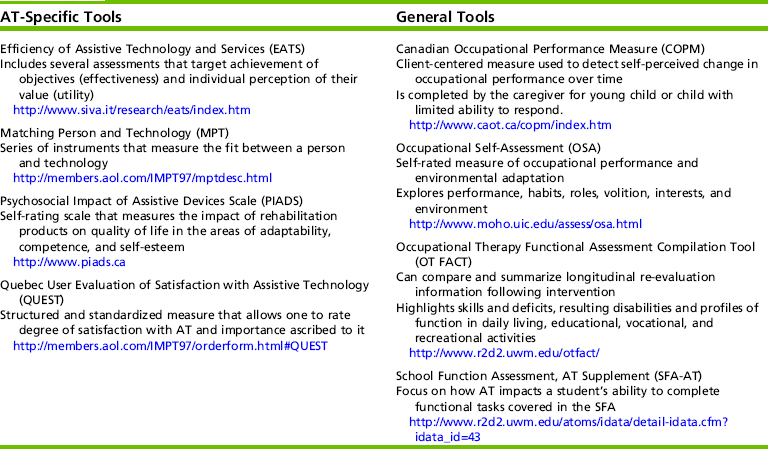
From Argabrite Grove, R., Broeder, K., Gitlow, L., Goodrich, B., Levan, P., Moser, C., et al. (2007, April). Assistive technology in the schools: From start to finish. Pre-Conference Institute at AOTA’s Annual Conference & Expo, St. Louis, MO.
Often, once the child and family have a basic understanding of the AT system and begin to use it independently, the occupational therapist may discharge the child from direct services. However, discharge from a regular routine of intervention should include a follow-up plan. The therapist can perform follow-up in several ways, from a telephone call to an extended clinic visit or simple review and analysis of data collected. The type of follow-up and when it should occur depends on the complexity of the system and the skills of the child, family, and other professionals working with the child. A predetermined schedule for follow-up (e.g., at intervals of 6 months or less or sometimes 1 year or more) is a component of effective service delivery. Problems and delays in service can be prevented with planned periodic review.16
In addition to outcomes for individual users of AT, instruments are available to assist AT teams in conducting quality assurance studies for the services that they provide. Quality Indicators for Assistive Technology (QIATs)80 and the School Profile of Assistive Technology Services81 are both used in school settings to support the development and delivery of AT services. Use of these indicators as guidelines can support outcomes for the child, the family, the classroom, and the system.
UNIVERSAL DESIGN AND ACCESS
Because it encompasses such a broad spectrum of services, the definition of AT is elusive. Perhaps because of this elusive nature, some therapists fail to recognize that the familiar tools in their “toolboxes” are really AT devices (Figure 20-3). Therapists working with children with special needs, their families, and educators often create, individualize, or adapt devices to enable independent participation for students with physical, communication, or developmental challenges to learning.100

FIGURE 20-3 Examples of readily available, universally designed low-tech tools. Photo courtesy Judith Schoonover.
Professionals and consumers have a common misconception that AT is complicated and expensive. Often, simple low-tech solutions are overlooked. Mistrett found that given a range of low- to high-tech solutions, families generally choose to use low-tech solutions more often, perhaps because their appearance is more like typically found toys and materials, and calls less attention to the disability.72 Assistive technology can be viewed as a barrier rather than a bridge, or “just one more thing to do,” unless it is intuitive and its value is revealed in everyday successes. Special educator and AT consultant Judith Sweeney suggests that the best way to facilitate acceptance of AT is the EASY way: Economy of cost and time; Additional (or Adapted) use of familiar tools; tool selection based on Standards that are already a part of what must be taught; and ownership, telling the student and teacher “the tool is Yours.”103 Sweeney recognizes that it is imperative for the entire team to accept and promote use of the tools for students to be successful in their occupations.
AT can help to level the playing field for children with disabilities, enhancing physical, instructional, and social inclusion opportunities.
Access
Providing physical access to homes and schools may include both devices and services.56 Modifications to buildings, rooms, and other facilities allow children with physical or sensory impairments to navigate both inside and outside of buildings using curb cuts, ramps, and door openers; labeling of key areas with pictures, text, and Braille; the provision of accommodations for individuals of varying sizes; or those who use wheelchairs to access restrooms, water fountains, pay phones, or elevators. Occupational therapy practitioners are trained to identify ways to improve performance and safety in the natural context to arrange resources, and to modify the environment to decrease or eliminate barriers.
Bus modifications for entry and exit and safe and appropriate seating can help with transportation to and from school and school-related activities including field trips, sports, and recreation. Within the building, doors, walkways, handles, light switches, and stairs can be modified to provide equal access to all students. Outside the building, seating and playground modifications can allow or enhance safe mobility and participation in recreational activities.45
Universal access has become an important concept that guides school and clinic purchase of new technology, particularly new computer systems. Most schools and clinics have established guidelines for ensuring universal access as they update and expand their computer systems. When all children, including those with disabilities, have equal access to technology, costly modifications for individuals can be avoided. Often the complexity of AT is not considered when general technology is purchased, so that computers do not support some of the software programs or adaptive peripherals needed by children with disabilities. A team of professionals, consumers, technology developers, and standards organizations must plan together to ensure that technology is accessible to all.
Universal Design
Ronald Mace, founder and program director of The Center for Universal Design,24 was an internationally known architect and visionary who used the term universal design to describe the concept of making all products and the built environment physically pleasing and usable to the greatest extent possible by everyone, regardless of their age, ability, or status in life. Mace used a wheelchair for mobility purposes, and his work relating to accessible design was instrumental in the passage of national legislation prohibiting discrimination against people with disabilities, the Fair Housing Amendments Act of 1988, and The Americans with Disabilities Act of 1990. The principles of universal design are outlined in Box 20-5.
According to The Center for Universal Design, “the intent of UD is to simplify life for everyone by making products, communications, and the built environment more usable by as many people as possible at little or no extra cost.”24 Universal design is a proactive approach that can eliminate many barriers, but does not replace the need for individualized AT. Although typical furnishings, toys, and instructional materials found in homes and classrooms may meet the needs of many, items that are “easier to handle, larger, less slippery, color coded or in some ways more inviting and functional” (p. 5)82 may be required for others.
Positioning and Ergonomics
Positioning and ergonomics conceptually include the physical positioning of the child for comfort, function, and work; location of the child within the environment; and location of supports in relationship to the child. A child’s positioning should never be static in nature. Seating, positioning, and mobility devices are often the foundation for successful use of all other AT, and they may be used to improve body stability, provide proximal trunk and head support, allow for exploration of the environment, and reduce localized skin pressure.78 The right seating and positioning equipment allow users to interact with their environment and perform tasks that are meaningful and life sustaining. “A task performance position is one that the person must be able to assume and maintain and in which the person can move” (p. 3).55
The environment cannot and should not come to the child; the child should be able to enter into and interact within the environment. One size does not fit all (Figure 20-4). With any population, there are variances in physical size and stature, and access methods can make it a challenge to provide adjustability to fit everyone comfortably. Computer use is rapidly becoming the rule (and the computer the tool of choice) rather than the exception in home, work, and school environments. Ergonomic working arrangements allow users to work in neutral, relaxed positions that consider energy conservation, which is important to maximize productivity for all users while protecting health and minimizing the risk of injury. Productivity is the result of a comfortable marriage of the user and the tool.

FIGURE 20-4 One size does not fit all. It is important to adjust learning environments to promote health and productivity. Photo courtesy Judith Schoonover.
As technology becomes a more important part of children’s lives at home and school, so does the need to pay attention to the health aspects of using computers. Proactive approaches to ergonomics programs should be embraced, particularly with regards to prolonged computer usage. American children typically spend between one and three hours a day at a computer, putting them at high risk for wrist, neck, and back problems.29 If children, or those advocating on their behalf, learn at an early age how to adjust a workstation, they will make similar adjustments later in life. These habits and skills can be established as early as the preschool years. Many schools have chosen not to include ergonomics programs because of the costs often associated with implementation. Box 20-6 outlines some minor changes that have minimal or no costs associated with them.
PARTICIPATION: SUPPORTING LIFE SKILLS WITH ASSISTIVE TECHNOLOGY
Often, occupational therapy practitioners work with very young children or children with significant disabilities. Although prerequisite skills may be necessary for successful use of certain devices, many children use a range of AT to address life skills such as communication, mobility, self-help, play and leisure, and work.114 For these children, low technology, such as the use of simple switches and cause and effect toys/appliances or software, may be the AT system of choice. Therapists may use these devices to help a child learn cause and effect or to build foundational skills for future AT systems. For some children with significant disabilities, simple devices that provide sensory input (e.g., fans, vibrators, music, lights) may be more motivating than some of the cause-effect toys or software (Figure 20-5). These devices can be hooked into an electronic aid to daily living (EADL) and then a switch can be used to turn them on and off. The EADL can run electronically operated toys or appliances and has functions that allow the child control of how the switch is used (e.g., a timer can be used so the child has to hit the switch every 30 seconds).
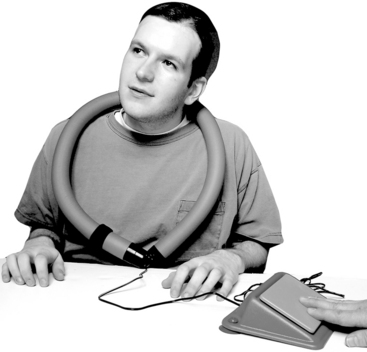
FIGURE 20-5 An example of a vibrating snake attached to a switch as a means to provide independent control of sensory input. Photo courtesy Enabling Devices; http://enablingdevices.com.
Often, low-tech solutions are controlled through a single switch. Typically, a touch switch that requires a press and release is used (Figure 20-6, A). However, for some children, this type of switch may not be motivating, or the student may not have the physical skills needed to access the switch. Figure 20-6, B, shows an example of a switch that helps a student learn cause-effect relationships. Some children may not have the physical skills to press or pull against resistance. These children may use a switch that is activated through a light touch (Figure 20-7, A). Switches can be mounted so that the position can be easily adjusted to improve access for a student (Figure 20-7, B). Although this switch requires minimal controlled movement, its cognitive demand is greater than that for the switches pictured. The touch-free switch may be too abstract for students with low cognitive skills.26

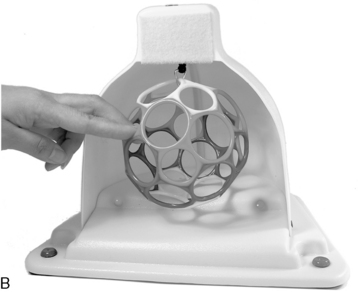
FIGURE 20-6 A, An example of a touch switch: the jelly bean switch. B, An example of a switch that is activated by pulling on the multicolored ball. A, Photo courtesy Enabling Devices, B, Photo courtesy Ablenet; http://www.ablenetinc.com.
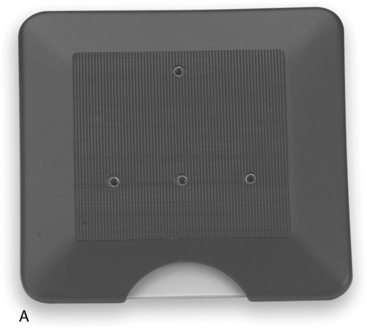

FIGURE 20-7 A, The Sensitrac flat pad switch. Switch is activated by a simple touch. B, The Sensitrac flat pad switch can be easily positioned for a child to access. Photos courtesy Ablenet.
Through the use of low-tech tools, switches, and simple cause-effect activities, children with disabilities can participate in a variety of learning activities at home and in the classroom. Figure 20-8, A, shows an example of how a child with a disability can participate in a water play activity through a switch toy. Figure 20-8, B, shows how a child can participate in a gardening activity, and Figure 20-8, C, illustrates how a student with a disability can play a game with his peers. Switches may allow partial participation, in which the student uses a switch to complete one step of the task. For example in Figure 20-8, B, the student pressed the switch to turn on the Water-Pik; then another student used the Water-Pik to water the flowers.



FIGURE 20-8 A, The child uses the switch to play with the water toy. B, The child uses the switches to participate in a gardening activity with her peers. C, The child uses the switch to turn on the Bed Bugs game. A and C, Photo courtesy Ablenet; B, Photo courtesy Enabling Devices.
Alternative and Augmentative Communication
If all my possessions were taken from me with one exception, I would choose to keep the power of communication, for by it I would soon regain all the rest.
Verbal communication is an inherent function of human beings and lends quality and detail to our social interactions with one another. Communication is not designed to be a solitary activity, because the purpose of communication is to exchange and share information with another individual. Children with disabilities may present with a range of performance levels related to receptive and expressive language. It is important that we consider the continuum of AT options available to support communication at any level. As stated by the National Joint Committee for the Communications of Persons with Severe Disabilities, “all persons, regardless of the extent or severity of their disabilities, have a basic right to affect, through communication, the conditions of their own existence.”73 In addition to this basic right, the committee has outlined specific communication rights that should be ensured during all daily communication acts with persons with disabilities (Box 20-7).
Alternative and augmentative communication (AAC) is defined as communication that does not require speech and that can be individualized to the unique needs of the child. An AAC system uses a combination of all the methods of communication available to a child. This can include “any residual speech, vocalizations, gestures, and communicative behaviors in addition to specific communication strategies and communication aids” (p. 7).34 The overall purpose of AAC is to enable the transmission of a message to another individual. According to Beukelman and Miranda, even students with severe disabilities can benefit from AAC use.11 Research indicates that individuals with complex communication needs who do not gain successful access to AAC are at high risk for abuse, crime, unemployment, and limited social networks.17,27
AAC interventions, much like other AT tools, should be dynamic and include not only the individual child, but also his/her primary communication partners. Beyond the obvious function of self-expression, AAC can help to support the development of language, emerging literacy skills, enhance participation in educational settings, facilitate friendships, and support interactions with family members and people in the greater community.28 When one family member relies on AAC, it always has an impact on the entire family unit.47 For this reason, it is imperative to use a collaborative approach when evaluating and implementing AAC supports. Various members of the team will bring different levels of expertise to share: child and parents will have the best knowledge of daily communication needs and routines, teachers will have knowledge related to literacy and instruction, speech-language pathologists are experts in language development, and occupational and physical therapists provide services related to positioning, accessing, and physically using the AAC system.
Attitude and acceptance of AAC play a role in its impact on the quality and function of interactions. AAC systems must be designed with layout and components that match the desires, preferences, abilities, skills, and environmental contexts of the child. Many parents are fearful that AAC will interfere with speech development, when in fact it has been found to enhance it.14 A family-centered approach should be used when AAC is integrated into the child’s daily experiences and interactions, to ensure caregiver support of its use.68
Communicative interaction has four purposes67: expression of wants and needs, information transfer, social closeness, and social etiquette. It is important for practitioners to also be aware of the three types of AAC communicators36: emergent communicators who have no reliable method of symbolic expression, context-dependent communicators who do have symbolic communication but are limited to specific contexts because they are only intelligible to familiar partners or may have insufficient vocabulary, and independent communicators who can communicate with anyone on any topic. Research indicates that children who use AAC are most frequently identified as “responders,” whereas typically developing peers consistently act as the “initiators” of communication.25 These classifications can serve as a foundation for identifying and establishing an AAC system in conjunction with the use of strategies that facilitate communication (Box 20-8).
AAC devices can be viewed on at least two continua, including no-tech to high-tech systems and aided or unaided communication methods. Depending on their age, contexts, and skills, children may use a combination to aided and unaided communication and a combination of low- and high-tech devices. Unaided or body-based communication is no-tech and consists of vocalizations, gestures, facial expressions, sign language, pantomime, eye gaze, and/or pointing. All people use some combination of unaided communication. Children with disabilities often use gestures, facial expressions, and body language as allowed by their functional skills.
Aided communication systems are distinguished as either nonelectronic or electronic communication aids and require the child to be able to use a symbol system.28 Nonelectronic aids are considered low-tech and include communication boards or books, picture-based systems, or paper and pencil. Picture-based systems are used increasingly with children in preschool, children with severe disabilities, and children with autism (Figure 20-9). Some children may find it easier to use visual-based systems of communication and to process content delivered using such systems. Visual representation such as objects, photographs, realistic drawings, line drawings, and written words can be used to increase understanding, communication, and social connectedness, and can take many forms depending on the environment and the circumstances under which they are used. Visual bridges52 can be designed to assist students to communicate about themselves using a combination of written words, objects, photos, computer-generated picture symbols, clip art, or other visual cues. Visual bridges can also be used during reading and writing activities. Emergent readers benefit from graphics paired with text to reinforce the meaning of print. Visual supports can be used during the development of schedules, augmentative communication systems, games, sequencing, and academics.

For individuals who have difficulty understanding two-dimensional visual representation systems such as photos, drawings, and graphics, Bloomfield suggests the use of True Object-Based Icons (TOBIs).15 TOBIs are any drawing, picture, or photo cut out in the actual shape or outline of the item they represent, thus providing visual information to the communicator (Figure 20-10). Tangible symbols are another example of providing symbolic representation of language, allowing communicators to relate to objects and experiences beyond their immediate context. Tangible symbols87 are two- and three-dimensional manipulatives that can be objects, parts of an object, or an associated object that conveys meaningful information to the user or represents their communicative intent. For example, a small bit of chain might indicate time to swing, or a circle formed from a pipe cleaner may indicate “morning circle” (Figure 20-11).
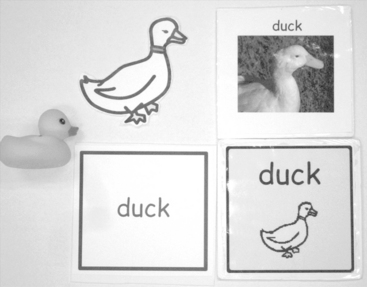
FIGURE 20-10 Multiple means of representation clockwise from left: an object, a TOBI, a photo, a picture symbol, and a word. Photo courtesy of Judith Schoonover.
Electronic communication aids or devices are generally considered more high-tech and may include speech generating devices, talking frames, cell phones, or computers. Speech-generating devices may produce digitized or synthesized speech output.28 Digitized speech records a person’s actual voice and allows flexibility in selecting a child, male, or female voice; however, it requires a lot of memory for storage and is limited to only what is recorded and stored. Synthesized speech is generated electronically but has the advantage of text-to-speech capabilities. The intelligibility of synthesized speech can vary depending on the type of system.
For children with severe disabilities or young children, several different types of simple AAC devices can be used. One example can be seen in Figure 20-12, A. This device has a recorded message that is activated each time the user presses the switch (Figure 20-12, B). Another simple AAC device that is good for individuals who are ambulatory is shown in Figure 20-12, C; it is worn like a watch and can have several prerecorded messages. The messages are easy to change, and symbols can be used to help the user remember the messages (Figure 20-12, D). Devices like those in Figure 20-12, E, are good for children who may eventually use more high-tech AAC.




FIGURE 20-12 AAC devices. A, BigMac communication device. B, Using the BigMac to participate in circle time. C, Talk Trac communication device. D, Using the Talk Trac and Step-by-Step communication devices to go shopping. E, Supertalker. Photos courtesy Ablenet.
High-tech electronic communication aids generally are either computer-based systems or dedicated systems. Computer-based systems are often considered for children who are using or will be using some sort of computer-assistive technology in addition to a communication system. Computer-based systems are made up of computers that can perform as a communication system through the use of specialized software and other modifications, but can also carry out other functions such as environmental control. Ideally, computer-based systems should be able to be mounted on wheelchairs or easily portable in some other manner. Dedicated systems operate primarily as electronic communication aids (Figure 20-13) with hardware and software features specifically designed for communication purposes. These systems are available in various sizes and weights and provide auditory, visual, or printed output. All electronic communication devices are programmed with individualized overlays. The board’s overlays can indicate as few as 2 and as many as 128 choices to the child.
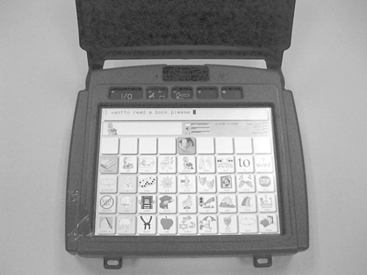
FIGURE 20-13 Example of a dedicated, dynamic display augmentative and alternative communication device. Photo courtesy of Judith Schoonover.
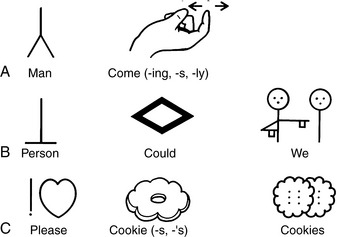
A number of factors must be considered in designing a high-tech AAC system, the first of which is to assess the child’s symbolic representation.12 What type of symbol will the child be able to use? Receptive understanding of functional objects, visual matching, and spelling and literacy skills related to word recognition are all cognitive skills that will help define the symbol system that is necessary. Examples of symbol systems include real objects, photographs, pictographs, Blissymbols (featuring grammar and syntax categorization by parts of language), and traditional orthography (use of letters and words). Examples of Blissymbols, Rebus, and PicSyms can be seen in Figure 20-14.
The control interface or manner in which a child interacts to provide input to the device may include use of a keyboard; single, dual, or multiple switch arrays; and joystick, mouse, or other alternative pointing devices.28 A child may make selections either directly by pointing or touching, or he or she may use an indirect method such as auditory or visual scanning, directed scanning, or coded access. To allow a child to communicate faster than the rate of keying in text, encoding (or symbol) systems are used. This language uses sequenced multiple-meaning icons to retrieve words, phrases, or sentences. Like word prediction, many communication systems come with message prediction. Some of the more advanced systems can learn the communication “style” of the user and begin to predict with greater accuracy.
In addition to the input method, AAC devices use two visual display types (screens). A dynamic communication display offers thousands of graphics (some that are electronically animated) and text options. The display changes (using the same message-formation process that produces natural speech) based on the choices of the user. They are often accessed via a touch screen; however, alternatives are available. Dynamic displays, such as the one in Figure 20-13, are helpful for children who may have difficulties with memory, but they do require a high level of visual attention, constant decision making, and the need for mastery of object permanence. Visual scene displays offer “hot spots” that are contextually embedded within graphics that provide more meaningful and individualized interactive displays (Figure 20-15). Drager38 made a comparison of visual scene displays and more traditional grid layouts used by typically developing 2½-year-old children during communicative tasks during a birthday party. Findings indicated that performance was better using the visual scene display.
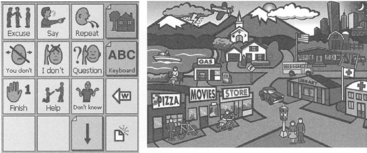
FIGURE 20-15 Visual scene display versus grid. From Blackstone, S. [2004]. Visual scene displays. Augmentative Communications News, 16, 1-5.
Once a device has been obtained, programming of the device and training of the child and all communication partners are essential for success. Collaborative efforts should be taken to identify vocabulary that includes conversational messages (greetings, information sharing, and requests), core vocabulary (for literate or preliterate children to encourage language and cognitive development), and fringe vocabulary (unique to the individual child’s activities, preferences, family, environments, favorite expressions, etc.).28 Vocabulary needs will vary by context, communication mode, and individual characteristics.13 Beukelman and Mirenda have developed core vocabulary and high-frequency word lists for a variety of settings and age groups, which can be found at http://aac.unl.edu/vbstudy. The child should be taught specific functions of communication such as requesting; rejecting/protesting; gaining attention; engaging in greetings, farewells, and other social niceties; commenting; achieving social closeness; asking for information; and confirming/denying.37 Communication competence67 should be the targeted outcome for any child using an AAC system (Box 20-9).
As with all other AT, communication systems are constantly being upgraded and changed. Continuing education courses and additional training can familiarize therapists with the terminology, communication strategies, and available hardware and software. AAC can help equalize opportunities for children to interact with peers, siblings and family members, and adults within relevant environments (e.g., school staff).
Computers
Use of personal computers by individuals of all ages is becoming more prevalent in school, home, and work settings. The computer is a flexible, motivating, and powerful instructional tool that can facilitate individualized teaching and learning. Computers with or without specialized software provide children with multiple means of communicating, playing, exploring, self-expression, interacting with the environment, learning cause and effect, and completing school and work-related tasks with greater degrees of independence. Most children with and without disabilities have had some exposure to a computer system by the time they enter school. At home, the computer might be used for recreation, entertainment, communication, work, and study. Social connections with others can be formed through e-mail, instant messaging, and social networking sites. For example, some adolescents with disabilities describe social networks and friendships that they have been able to develop using the computer, Internet access, and appropriate software programs.104
Swinth and colleagues found that children as young as 6 months of age could access a switch to play a simple cause-effect game on the computer.106 A computer can motivate children to learn and develop a large repertoire of skills. It provides simulations of experiences that children with motor disabilities cannot otherwise experience. The computer is also infinitely patient with drill and practice and can provide the repetition needed for some children to learn. An almost endless variety of software programs, input devices, and output devices are available to customize computers to meet the individual needs of each child.4 Young children can be introduced to a progression of systems that follows their developmental and functional needs. For a child who is born with a disability, success using simple systems precedes the use of more complex systems. Table 20-6 outlines benefits of computer use for children.
TABLE 20-6
Benefits of Computers for Young Children
Burkhart, L. J. Effective use of computers with young children. Available at http://www.lburkhart.com/handcomp.html
At school, children typically use word processing programs, the Internet, e-mail, and virtual classrooms in some aspect of their education. Software programs for children and adults cover most academic subjects as well as recreational and competitive activities. For example, math software and Internet sites include features such as virtual manipulatives or drills; creative writing software has recording features, sound, graphics, and animations; keyboarding software teaches typing as software and website designers continue to add features that make their products and sites accessible to a growing range of people and abilities.
For all children, the judicious use of computers and software can help develop literacy or strengthen skills through the use of games, screen readers, and online books. “Virtual field trips” allow students to visit and explore environments that might otherwise be inaccessible, and computer simulations can provide preparation for social situations, academic tasks, prevocational training, and driver education. For children who are unable to recognize print in traditional formats, modifications to access the same text as that for their peers can decrease their dependence on the support of others in the environment to read or write for them. Often the computer is a magnet for children who have difficulty engaging in traditional classroom activities. When, as a result of motor, emotional, or attentional difficulties, children are challenged to produce art products or written work, the computer can assist in generating digital artwork or text that is neat and uniform in appearance. Producing more accurate, legible, or attractive work can increase self-esteem and self-expression and decrease frustration. The multimedia features of the computer can support learning rules, turn taking, and social skills.94 As with any tool, the user must be aware of its features and trained in its applications and maintenance to receive full benefits. Competencies that school-based occupational therapists should possess include the ability to operate major computing systems used in public schools and troubleshoot system problems, establish networks using telecommunications systems, operate general application programs, apply teacher utility tools, and provide computer-based instruction.48
To successfully access a computer system, the user must be able to provide input into the system, receive output (or information) from the computer, and process that information to use it in a functional, meaningful manner. Various types of computers (e.g., Macintosh or personal computer [PC]) are available in the home, school, clinical, and work settings. Before recommending the purchase of software programs or adapted access devices, the memory and technology of the system must be evaluated to determine its compatibility with the program. Now, many software programs are both PC and Mac compatible. For example, alternative keyboards can be used on either machine without significant reconfiguration. However, because certain hardware and access devices remain specific to either the PC or the Mac, therapists should attend to these specifications.
Input
In considering different input systems, the “least change” principle should be applied. This means that a standard keyboard and standard workstation with some modifications are preferred over an expanded keyboard or other type of input device if the child can use them (Figure 20-16), exemplifying the concept of least restrictive environment (Table 20-7).
TABLE 20-7
Problem Solving for Computer Access (Starting with a Standard Computer Workstation)
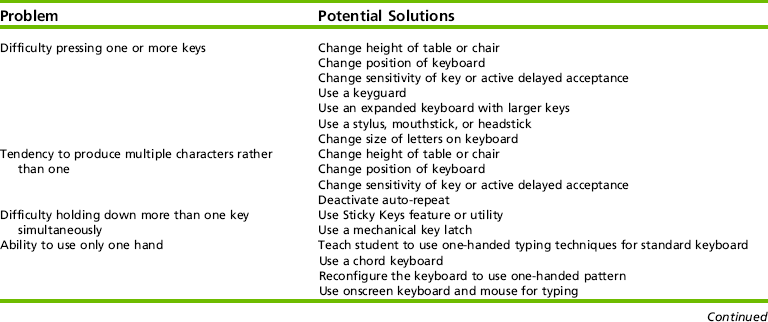
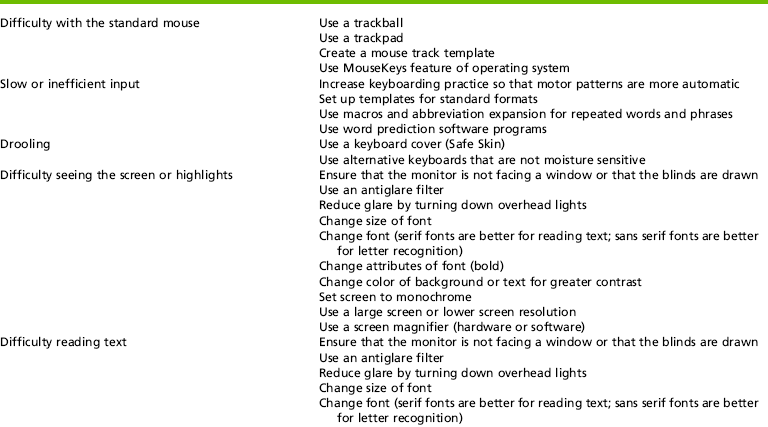
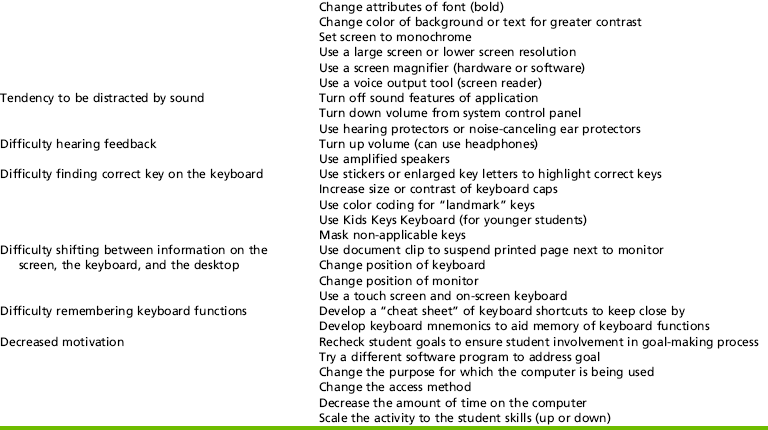
Swinth, Y. L., & Anson, D. (1998). Alternatives to handwriting: Keyboarding and text-generation techniques for schools. In J. Case-Smith (Ed.), AOTA self-paced clinical course: Occupational therapy: Making a difference in school system practice. Rockville, MD: AOTA.
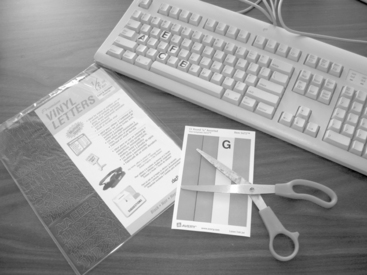
FIGURE 20-16 Example of low-tech keyboard modifications including color-coding and enlarging letters on keys. Photo courtesy Judith Schoonover.
For some children, using an ergonomic keyboard rather than a standard keyboard will increase their proficiency on the computer. For a child with slight tremors, disabling the auto-repeat function, or using a keyguard (plastic covers for the keyboard with a single hole) may enable independent use of the standard system (Figure 20-17). Software programs are available to redefine the keyboard versus using the standard QWERTY keyboard that comes with most computers. One commonly used keyboard offers as one of its keyboard layouts a color-coded alphabetic layout for younger children or children with cognitive delays who cannot find letters using the QWERTY layout. Switches, adapted keyboards, and voice recognition systems offer alternative means for computer access to children with limited movement.

FIGURE 20-17 An example of a keyguard for an alternative keyboard. Keyguards also are available for standard keyboards. Photo courtesy IntelliTools, Petaluma, CA.
Alternate input systems come with their own software programs or a combination of unique hardware and software adaptations. Some alternate input systems allow for direct selection (the user selects letters, words, or phrases by touching or pointing to the desired key), and others allow indirect selection (an intermediate step is used when sending a command to the computer). Direct selection offers more choices to the child, requires less cognitive skill than indirect selection, and should be the first type of system considered. An example of direct selection is an expanded keyboard; indirect selection includes using letter scanning or Morse code and a switch. Various scanning methods are available including row-column scanning, step scanning, and automatic scanning. The method that the therapist chooses depends on the skills of the child using the system. In row-column scanning, the computer will scan down rows. Once the user selects the row in which the letter, number, or word resides, then the computer scans across the columns. In automatic scanning, the computer scans through all the choices at a predetermined rate.
Switches: Switches allow access to the computer with a single movement. Many of the switches that can be used to access low-tech solutions (see Figures 20-6 and 20-7) can also be used to access the computer. Many of the more complex switch systems use indirect selection. In considering a switch-driven system, consideration should be given to the motoric and cognitive requirements of the system.26 For example, a child who is able to accurately and reliably hit a switch at 9 months of age does not have the cognitive skills to understand the concept of scanning. In addition, research suggests that the placement of the switch (e.g., a head switch versus a switch that is struck with the hand) may have a cognitive component that affects a child’s accuracy.46 A single (or dual) switch can be used to run systems such as Morse code and scanning. Morse code is faster than scanning, but requires the user to learn a new language.
Alternate Keyboards: Alternate keyboards include programmable membrane keyboards, miniature keyboards, chord keyboards, and onscreen keyboards. Each type of alternate keyboard varies in size, layout, and complexity. Membrane keyboards assist the child with decreased fine-motor control or cognitive delays to successfully make choices on the computer and allow for customization of overlays, and it provides voice output. Programmable keyboards (Figure 20-18) allow use of customized overlays and can be set up with “hotkeys” to allow the child to enter numbers, words, and phrases by hitting one key. Changing the overlay, software program, and customization setup is relatively simple, making it easy to create new activities that align with the classroom curriculum or the current interests of the child. Miniature keyboards are smaller than the standard keyboard. Miniature keyboards are typically lightweight and designed to be used by children with limited range of motion or poor endurance. Chord keyboards, like miniature keyboards, are designed to minimize finger travel. Use of these keyboards, similar to playing the piano, requires multiple simultaneous keystrokes to type letters and phrases. Onscreen keyboards (virtual keyboards) are software programs that provide the image of a standard or modified keyboard on the computer screen. The user can access these “keys” via different input systems such as a mouse, touch screen, trackball, joystick, or eye-gaze system.
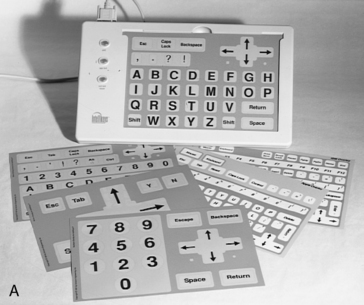

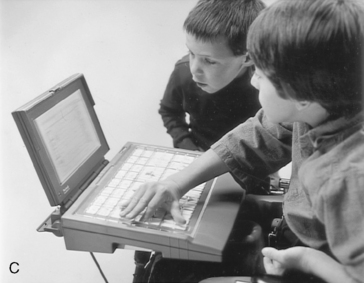
FIGURE 20-18 Examples of alternate keyboards. A, IntelliKeys with alphabet overlay. B, KeyLargo and overlay examples. C, KeyLargo used with a powerbook. A, Photo courtesy Don Johnston, Inc., Wauconda, IL; B and C, Courtesy IntelliTools, Petaluma, CA. Note: KeyLargo is now available from Infogrip http://www.infogrip.com.
Mouse Emulators: Mouse emulators are hardware or software systems with output that the computer reads like a standard mouse. Various devices are available that simulate mouse movement and/or clicking by using head and body movement to perform those operations. The continuum of mouse emulators included using the arrow keys on a standard keyboard, touch pads, trackballs, and head pointers. Interactive whiteboards and touch windows can also be considered mouse emulators. Using these systems, the child activates the computer by touching the interactive whiteboard, or the touch window that fits like a window over a computer monitor screen.
Voice Recognition: Voice (or speech) recognition systems, in which the computer recognizes and translates voice sounds into text or commands, can be an option for individuals with severe motoric limitations. The user must have fair-to-good articulation to successfully operate a voice recognition system, and typically understand basic editing and grammar commands. The child speaks into a microphone to enter text, control the mouse, and execute computer commands. Voice recognition systems generally are not used with children under 12 years of age because of the complexity of the system. These systems can be isolating to use as they often pick up ambient noise in the background and may require the user to work outside of the classroom.
Other Input Systems: Other types of input systems used with children include eye-gaze systems, Braille, TouchFree Switch, and a Tongue Touch Keypad. Eye-gaze systems require the child to visually focus on a desired position on the computer monitor. An optic light on the computer “reads” where the child gazes and makes the appropriate selection. To word process, eye-gaze systems use onscreen keyboards and other systems. Several programs allow a child who is blind or who has a significant visual impairment to input into the computer using Braille. The Touch Free Switch operates via a camera on top of the computer and is activated by a predetermined movement by the child. The Tongue Touch Keypad has nine tongue-activated keys that the child activates. Once the user activates the keys, a signal is sent to an interface box connected to the computer.
Output Systems and Information Processing
Output is the product or outcome that is produced when using a computer. Just like input, computer output can also accommodate the needs of individuals with disabilities. Information (output) from the computer is displayed visually on the monitor or printed from the printer. For a child with a visual impairment, perceptual impairment, or cognitive impairment, adaptations to the monitor may need to be considered. Some printers provide Braille output, and several software programs provide voice output. Some of these programs read text, whereas others provide output regarding all the functions of the computer. Voice output systems can help support learning and computer use and exploration for students with learning disabilities, cognitive delays, autism, and visual impairments.
The computer’s output and the child’s successful processing of information are often closely related. If children with disabilities cannot successfully process and use the information received from the computer in a meaningful and functional manner, they will not use the system over time. With the increased screen resolution and the complexity of graphics now available in computers, some children with visual-perceptual difficulties find the visual information they receive distracting or overwhelming. For example, a child who has poor figure-ground skills may have difficulty with graphics that are cluttered and complex.
Software
Careful decisions must be made to find programs that match children’s interests and skills. With the burgeoning number of software programs available, from simple to highly complex, many children with disabilities can use common software programs that are available to everyone. Often software programs require that the user make specific, discrete responses to visual, auditory, or tactile stimuli. The child must be able to attend briefly and have the interest and motivation to activate a toy or a computer purposefully. Computer activities and programs, including public domain software, can be used to teach basic skills, such as object permanence, sustained attention, and cause-effect relationships. Other computer programs teach skills in discrimination, matching, and directionality. The occupational therapist can determine whether and how the software customizes the video and audio display to meet students’ individualized needs.
With all the different input and output methods and software programs available, computers offer many ways to help children develop functional independence in life roles. Children can have opportunities to use computers throughout their school years and into their work settings; they can also use computers as environmental control devices and for play and leisure exploration.
Electronic Aids for Daily Living
Originally, EADLs were known as environmental control units. These are systems that allow a child to control appliances in the environment. EADLs allow the child to interact with and manipulate one or more electronic appliances, such as a television, radio, CD player, lights, telephone, or fan. This can be accomplished using voice activation, switch access, a computer interface, or adaptations such as X-10 units (transmitters and receivers) that use a communications “language,” allowing compatible products to interact with each other using the existing electrical wiring. The EADL should meet the child’s primary needs, as well as any long-range goals. The system should also be fairly easy to assemble, learn to use, and maintain. As mentioned previously, EADLs can be integrated into a child’s computer system. They also can be stand-alone systems. Some of these systems have discrete control interface (an electronic device is either turned on or off, such as lights, fans, or a television set), and others are capable of continuous control interface (devices that operate in successively greater or smaller degrees of control). Lowering and raising the volume on a television and dimming a light are examples of continuous control. A common EADL setup used with children is shown in Figure 20-19. Many EADL options are available for a variety of settings.
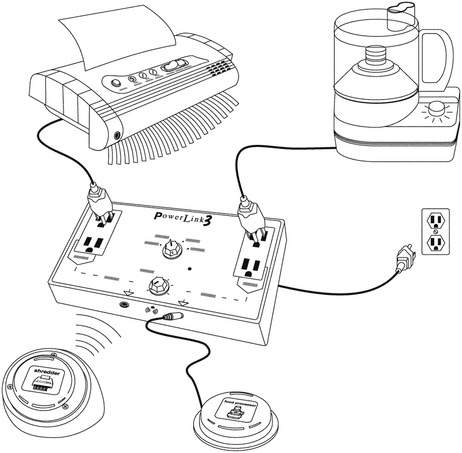
CHANGING THE LANDSCAPE IN EDUCATION: PLANNING FOR EVERY STUDENT IN THE 21st CENTURY
One aspect of universal access that is gaining increased attention in the schools is universal design for learning.86 School administrators have placed increased emphasis on the development and implementation of a universally designed curriculum that allows all children equal opportunity to learn and demonstrate what they have learned. AT and accessible software are important elements of a universally designed curriculum.51 Universal design for learning (UDL) involves developing and improving learning environments where all children are included. A UDL framework provides multiple means of (1) representation, to give learners various ways of acquiring information and knowledge; (2) expression, to provide learners alternatives for demonstrating what they know; and (3) engagement, to tap into learners’ interests, offer appropriate challenges, and increase motivation.53
Instructional Technology
Sometimes students with disabilities require technology that is helpful or sometimes used by students without disabilities. For example, most classrooms have tools like calculators and word processors. Students with disabilities might need to use calculators or word processors, or use them with modifications to participate in math or writing activities. This need redefines common classroom tools as AT that may be a required service in the IEP; therefore, it is important to consider how important the tool is to the student’s learning and participation.
Schools use many kinds of instructional technology, providing software in most academic areas and for students of all ages. Some examples include literacy software for children to develop letter-to-sound correspondence, math software for drill and practice of math facts, keyboarding software, and content-area software to reinforce concepts of science and social studies. Student assignments may include copying or producing written work using a word processor, research using the Internet, and email. A computer, computer-based device, or software program may be AT if it provides specific input or output that a user needs to access needed information. Features in software applications including adjustable user settings and alternate keyboard access can help reduce barriers and positively influence participation. Occupational therapy practitioners who are aware of the accessibility needs of their clients can advocate for the purchase of accessible instructional software. The National Center on Accessible Information Technology in Education promotes the use of electronic and information technology for individuals with disabilities in educational institutions at all academic levels, and features a searchable database of questions and answers regarding accessible educational and instructional technology on its website (http://www.washington.edu/accessit/). Features to consider in evaluating accessibility of instructional software are outlined in Box 20-10.
Assistive Technology for Literacy Skills
The primary goals of IDEA 2004 and the No Child Left Behind Act (NCLB) of 2001 are improving student achievement and providing students with disabilities access to the general education curriculum; however, providing access does not guarantee increased participation, especially for children who have reading and writing difficulties.23 Literacy skills include the complicated processes of reading, writing, and spelling as forms of communication; reading is the communication process of constructing meaning from written text, and writing is the communication process of composing meaningful text.
Literacy is more than learning to read, write and spell proficiently. It is learning to enjoy words and stories when someone else is reading to the child. It is learning to love books and all the worlds that can be opened by books. It is a way of achieving social closeness through sharing literacy experiences with friends or classmates. It is finding out about the way things are in places we have never visited or in places that have never existed. If we understand that literacy is all of these things and more we can also understand that everyone can achieve some degree of literacy if given opportunities and exposure (p. 3).70
Literacy begins with the recognition that words correspond to speech and that words are made up of sound. Repeated exposure to literacy experiences such as looking at books, exposure to signage, and writing demonstrates the importance of words. We live in a world that requires literacy. Traditional print such as books and newspapers, as well as information and communication technology including word processors, presentation software, the Internet, and e-mail, is used to relay information. In a text-based society, nonreaders are at risk for difficulties with managing information, and reduction in academic skill acquisition, societal integration, and quality of life. Limited literacy skills also affect the likelihood of successful competitive or supported employment.60
Children who struggle with learning to read and write need to be supported by individuals who can accurately assess their strengths and weaknesses, select, and apply AT tools and strategies effectively. AT can help children with disabilities in language acquisition. They can learn that words are something to pay attention to. They can learn about the world around them by simply listening to stories. Most important, they can increase their opportunities for social closeness. Koenig and Holbrook define functional literacy as “the application of literacy skills and the use of a variety of literacy tools to accomplish daily tasks in the home school, community, and work setting” (p. 265).59 A multitude of software, word processors, text readers, and electronic books are available on the Internet to support children’s literacy. An essential element related to the effectiveness of technology in supporting literacy is its interactive quality, which allows children to get involved with the content as they manipulate the media.42 Literacy software programs interact with children, similar to a parent’s reading to children and involving them in the book by turning the pages, looking at pictures, and asking questions. Technology allows children to control the process and “hook” their interest. Koenig reiterates the importance of starting early with children “regardless of the severity” of their disability.58 All individuals can benefit from these experiences, although the benefits realized by each child will be different.
The National Center for Technology Innovation (NCTI) website (http://www.techmatrix.org/) serves as a database of published research and commercial products that are reviewed for universal design features that support student literacy. This site reviews products for features such as text-to-speech capabilities, in-line dictionary support, customizable views, and progress monitoring options, and allows the searcher to create a customized matrix by subject and/or type of learning support.
Reading Skills
Children most at risk for reading difficulties are those with less verbal skill, phonologic awareness, letter knowledge, and familiarity with the basic purposes of and mechanisms for reading.20 Research on early reading development emphasizes the pairing of written words and sounds for helping children’s decoding skills. For children with physical, visual, communication, or cognitive delays, traditional books may restrict their ability to interact with and access books. One of the methods that can be used to provide successful literacy experiences is through adapting books. Adapted books provide print access that follows the Universal Design for Learning (UDL) framework. Adaptations can include making books easier to use (turning pages or holding) and text easier to read (simplified, changed) and remember. The original story or subject is maintained, but may contain modified language, clear visual representations, and manageable page layouts to increase the potential for participation. Adapted books can be used by themselves, or with AT ranging from low-tech homemade devices to switches, voice output communication aides, Braille and large print materials, sign language, or adapted props.
Copyright laws allow the creation and use of books in an alternate format solely for the purpose of making the book accessible to persons with disabilities; however, it is important to review copyright laws and how they pertain to each situation in which an adapted book is being contemplated. A copy of the original book is required when using an adapted book. Books can be adapted to provide physical access to text by creating space between pages with page “fluffers” (foam, weather stripping, sponges, giant paper clips, clothespins), using book holders for stabilization (recipe book holders, card holders, acrylic display frames, easels), or by reproducing them so that they can be listened to or viewed with technology (Figure 20-20). Accommodations for print difficulties include change in font size and color, magnification, contrast, audio output, tactile display, icon-enhanced text, scaffolded information, and multimedia. Electronic books combine reading, writing, listening, and speaking and provide a multisensory approach with related pictures, sound, and video, and appeal to different learning styles. Through the appropriate provision and support, technology can allow children to control their own learning.

FIGURE 20-20 Example of an adapted book with tactile and rebus symbol support. Photo courtesy Judith Schoonover.
The ability to read is essential for many daily life activities and participation in varied environments at home, school, work, and in the community. Reading contributes to play and leisure, academics and world knowledge, communication and social awareness, following directions and schedules, shopping and meal preparation, and work-related tasks. When the ability to read print text is affected by visual, visual motor, visual processing, decoding, tracking, attentional, or cognitive difficulties, AT can provide alternatives to traditional print text. For example, Edyburn proposed a process of scaffolding digital text to meet the varied reading and cognitive needs of children by reducing the amount of text, as well as adding additional visual cues in the form of pictures or symbols. He used the term cognitive rescaling to describe “a process of altering the cognitive difficulty of information” (p. 10).40 Other accommodations for print disabilities include the use of commercially available talking photo albums, specific reading software, e-text, audio recordings, screen readers, and multimedia.
Assistive Technology for Writing
The act of writing not only requires motor and sensory skills but also includes cognitive processes in the form of recognizable language and vocabulary, generation of ideas, organization of ideas, expression of ideas, and use of correct grammar, punctuation, and spelling. With handwriting as the most common reason for referrals to occupational therapy in school-based practice, practitioners are well aware that writing skills can be enhanced with no-tech or low-tech aids and devices. Simple adaptations, like smooth-writing pens that are comfortable to hold or adapted paper, can make the difference between needing physical assistance and working independently. Universally designed tools, such as a pen, become AT when needed to achieve targeted goals. Service delivery in the natural context, using tools that are intuitive, may mean borrowing or adapting tools that already exist in the classroom.
For individuals who may have motor difficulties that affect the ability to write for function, alternatives for written production should be explored such as the use of a keyboard and mouse (or alternative mouse) or a portable word processor or notebook computer. Beyond the physical components, writing can be conceptualized as a cognitive process that includes the following steps: prewriting/brainstorming ideas, drafting/composing and organizing initial ideas, editing, and, finally, publishing the final product.28
Standard word processing and multimedia software, often available in the classroom, features sizable and colored fonts, line spacing options, spell and grammar checking, opportunities for outlining and highlighting, use of tables to organize information, use of macros and abbreviation expansion, general accessibility features, and incorporation of multiple media to represent ideas. More specifically, concept-mapping software allows the user to conceptualize information graphically using a combination of pictures and/or text. It is helpful for planning, organizing, and drafting and frequently offers templates for getting started (Figure 20-21).
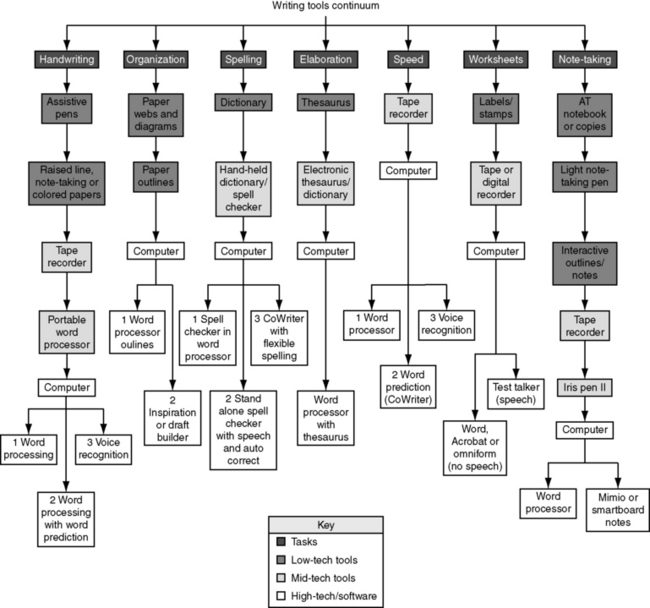
FIGURE 20-21 Writing tools continuum created with graphic organizer software by Judi Sweeney, Onion Mountain Technology (http://www.onionmountaintech.com). Figure courtesy Judith Schoonover.
Other software products allow the child to complete a written assignment with visual and/or auditory feedback. Word prediction and word completion can reduce the number of keystrokes necessary and as a result may increase overall speed.28 After a child types in the first few letters of a word, the program will attempt to predict whole words and presents a list of choices for the child to scan and select (Figure 20-22). Many word prediction programs include customizable dictionaries that suggest alternative word selections, which can facilitate improvement in the quality of a child’s written work. These features are beneficial to support spelling for children who have good word recognition skills. Spell-checking programs have proved to be helpful editing tools, specifically when integrated into a word processing program; however, grammar checkers have not.66 Other options may include use of a traditional or electronic dictionary or thesaurus for children who have word retrieval deficits.
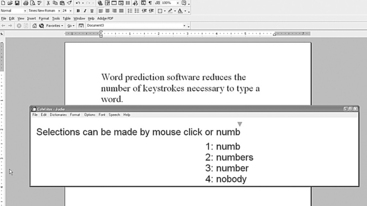
In combination with visual supports, some children benefit from the use of auditory feedback. Text-to-speech software converts printed digital text to synthetic speech. This feature is available in a number of software applications, free Internet downloads, and on recent versions of Windows and Macintosh operating systems. Synthesized text-to-speech screen readers support drafting and editing, which can help a child more readily detect errors because the text is read out loud. They also reduce the visual load for individuals with visual processing deficits, and are a valuable alternative for auditory learners. Users with print disabilities can also access contents of web pages, e-mail, e-books, or printed documents scanned with optical character recognition (OCR) software and converted to digital text. Pairing print with digital speech output is available in a number of applications. The age and gender of the “voice,” reading rate, dynamic highlighting, and color of font and background can be manipulated to address the individual needs or preferences of the user.
Conversely, some children require speech-to-text (or voice recognition) options that allow them to dictate thoughts and commands to a program that produces written text for them. Speech input technology responds to the human voice by producing text or executing verbally dictated commands to navigate through computer applications.28 Speech-to-text software was initially envisioned as a business tool, but has been found to be an effective strategy to support children’s learning. Speech recognition presents words through speech, so to produce accurate dictation, the user must have appropriate oral mechanisms.50 The process results in a multisensory written language experience. Voice quality, pitch, volume, and articulation have a direct impact on the quality of the product generated, as well as set-up and positioning of the user. In addition to specific dictation software products, recent versions of Windows and Macintosh operating systems include speech recognition features. A substantial training component is required to use this type of technology, and the environmental context in which it is used must be examined closely. Speech input can be accomplished by dictating to another individual or a tape recorder as a less costly alternative. This allows individuals with intelligible speech to express themselves, even when writing is problematic for attentional, motoric, or cognitive reasons.
Assistive Technology for Math
Mathematics is a part of typical school curriculum and is considered a functional life skill. Mathematical concepts include sorting, numbers, differences in attributes (color, shape, size), patterns, counting, sequence, graphing, and numeration. Ideally, a combination of individualized instructional strategies and numerous opportunities to use and manipulate concrete objects to count, sort, compare, and combine is used to reinforce concepts of same/different and greater than/less than/equal to. Children with sensory, cognitive, or physical disabilities may need additional support (e.g., grippers, nonskid materials) or alternatives to hands-on manipulation such as “virtual manipulation” (http://nlvm.usu.edu/en/NAV/vlibrary.html) to allow active participation in math exploration.6
Children with visual processing or visual motor deficits affecting their ability to see likenesses and differences in shape and form, difficulties with copying and writing, physical limitations, or cognitive challenges can benefit from a wide array of AT supports when instructional strategies, curriculum modifications, use of manipulatives, flashcards, and repetition are not enough. Math difficulties may affect future financial management skills, with resultant decrease in independence. To determine whether a child needs AT in the area of mathematics, the IEP team should consider whether the child is able to effectively participate in math instruction and complete math requirements of the curriculum or work setting without the use of aids/devices. If not, then a determination must be made regarding which tools would most effectively reduce barriers to accessing the curriculum.
Common classroom math tools such as rulers, compasses, protractors, and calculators can be modified to make them easier to handle or keep in place. Low-tech math solutions may include use of a customized number line; TouchMath® (a multisensory teaching approach that links manipulation with memorization of math facts), enlarged or masked math worksheets; graph or grid paper for aligning problems; alternatives for responding such as math stamps for drawing graphs, clocks, and number lines; and use of simple calculators (Figure 20-23). Providing alternative visual representation of math problems with graphics can increase the child’s understanding.
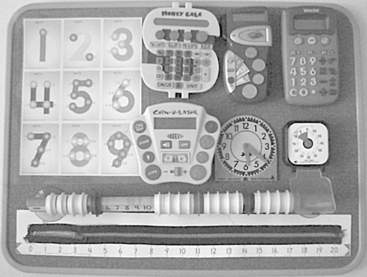
FIGURE 20-23 Examples of no-tech, low-tech math supports including TouchMath®, number lines and counters, coin calculators, a calculator with enlarged buttons, a Time Timer, and a standard Judy Clock math manipulative. Photo courtesy Judith Schoonover.
A calculator is an electronic, mechanical, or onscreen device for the performance of mathematical computations. Calculators accept keypad input and display results on a readout screen, paper tape, or computer screen. Calculators speed up calculation time, provide feedback and an alternate way to “write” numbers, and may improve accuracy. Calculators come in many sizes with features such as big number buttons and large keypads, and range in operational capacity from simple to complex. Handheld calculators can help a learner who has problems writing numbers in the correct order; talking calculators vocalize data and resulting computations through speech synthesis; special-feature calculators allow the user to select options to speak and simultaneously display numbers, functions, entire equations, and results; on-screen computer calculator programs offer features such as speech synthesis, and some allow the user to adjust the display including size and color of the keys and numbers. Specialized calculators use realistic money bill and coin buttons to count money or teach the value of different coins. Children can practice addition and subtraction with coin denominations. Individualizing the calculator for the user’s unique needs may include providing tactile cues, enlarging or masking buttons, stabilizing or angling the calculator to improve access, using a colored filter over the display to change contrast between the numbers and the background, or providing a tool to access the buttons.
Access software or electronic math worksheets provide the opportunity to engage in the same curriculum as for typical peers by using a different platform to enter answers.84 For example, instead of pencil and paper, a computer and a peripheral device such as a joystick, touch screen, interactive whiteboard, or alternate keyboard are used to record responses. These software programs help the user organize, align, and work through math problems using the computer. Numbers that appear onscreen can also be read aloud with a speech synthesizer. Microsoft Excel provides a computer equivalent to a paper ledger, with extensive graphing capabilities. Grids comprise columns and rows (intersections called cells). Each cell may contain labels, data, or formulas (mathematical equations that do all the work). Interactive math websites are available on the Internet. Textbook manufacturers may provide digital copies of textbooks on CD-ROM and most maintain websites with additional teaching resources and information.
Assistive Technology and Transition
Transition planning is essential to pave the way to successful change. Transitions are an inevitable part of life, yet the passages from preschool to elementary school, elementary school to high school, and high school into early adulthood can result in a loss of continuity. For an individual with disabilities, transitions can be especially challenging if the supports that provide access to participation are not available or prove unsuitable in the new environment. Critical information, as well as competencies, can be lost if positioning, teaching methodologies, and information regarding specialized technology are not passed along from one stage and setting to the next. IDEA mandates the provision of both AT services and transition services for students with disabilities. When a student with a disability requires AT to accomplish one or more functional skills, the use of that AT must be included in effective transition planning. Transition plans for AT users address the ways the student’s use of devices and services are transferred from one setting to another. AT transition involves people from different classrooms, programs, buildings, or agencies working together to ensure continuity. Self-determination, advocacy, and implementation are critical issues for transition planning. Although the involvement of occupational therapy is important during the student’s transition into adulthood, only 16% of all occupational therapists (compared with 29% who work in school settings) provide transition services for students ages 13 to 21.2
In addition to ensuring that AT devices and support services accompany students during transitions, service providers should assist clients and their families in becoming responsible users of AT. As Wehmeyer asserted, if students with disabilities are to actually achieve greater control over their lives, then it is important to provide (1) opportunities to exert control and make choices; (2) supports and accommodations needed; and (3) opportunities to learn new skills to increase participation.111 The goal of self-management and independent use should begin the first time a child uses AT, steering him or her onto a path of optimal independence as an adult. Competencies should be developed in the area for which the AT device was chosen (e.g., communication, writing) as well as in how to use and care for the device, when to use it, and the social implications and responsibilities of using the device.22 Development of self-determination skills to ensure that AT becomes an integrated part of typical routines will aid in successful transitions from home to school and from school to the community.22
For individuals beginning or ending their public school education, transition planning is included in legal mandates. Explicit documentation is needed during all transitions to ensure the individual transitioning has the support needed. Documentation can take the form of text, photos, and videos. For students who require AT devices or services to receive FAPE, transition plans should contain a statement of needed AT devices and services, and indicate agency responsibilities and linkages, if appropriate. The child should be allowed to take an AT device home or to other environments if it is necessary for FAPE. Various agencies may be involved, and the decision regarding who is responsible for providing the AT services needed for successful postgraduation activities should be determined in advance by the transition team.
Involvement of occupational therapy practitioners during the transition process assists the youth in the development of work, community, and independent living skills. Working as a member of the transition team, the occupational therapy practitioner may access and address student-related factors, including social, sensory, motor, and perceptual abilities; task-related factors, such as analysis of physical and perceptual requirements of the task; and environmental factors, such as analysis of noise level, clutter in the environment, and accessibility of work or living space. The QIAT Consortium has identified areas of best practice for AT transition79 (Box 20-11), and although their guidelines focus mainly on the late high school transition to postsecondary and work placement, they serve as a reminder of the goals of the transition process and help identify key elements that need to be addressed in a transition plan.
Evidence-Based Practice and Assistive Technology
Although there is research available documenting the benefits and limitations of many AT devices,39,41,89,102 AT outcome measurement and trials of AT services are limited. Because of the ever-changing nature of this field, the complexity of the devices, and the need for individualized decisions, it is difficult to build a large evidence base in this area of practice that is consistent with the available technology.41 Some AT companies are adding research information regarding their products and AT outcomes to their websites. Whenever possible, AT research should guide and support decision making and provide further foundational knowledge about AT devices and services. When evidence is not available, occupational therapy practitioners working in this area must engage in data-based decision making with each client to document whether the use of the device results in increased participation across environments. Occupational therapists should be good consumers of AT research and should also measure and document AT outcomes as part of best practice services.
SUMMARY
Childhood is a time when children undergo continuous developmental changes and expand on skills that will eventually lead to functional abilities. Assistive technologies can diminish the impact of disabilities and allow children improved alternatives to participate.72 Children who use AT at an early age have the advantage of developing with AT and using it to their benefit throughout their lives. Occupational therapy practitioners who work with children and youth should become familiar with the continuum of AT options (Table 20-8) and are ideally suited to evaluate and determine an appropriate match of AT tools to the child. The combination of occupational therapy and AT services together can promote success across all areas of occupation in which a child engages.78
TABLE 20-8
Continuum of Assistive Technology Devices
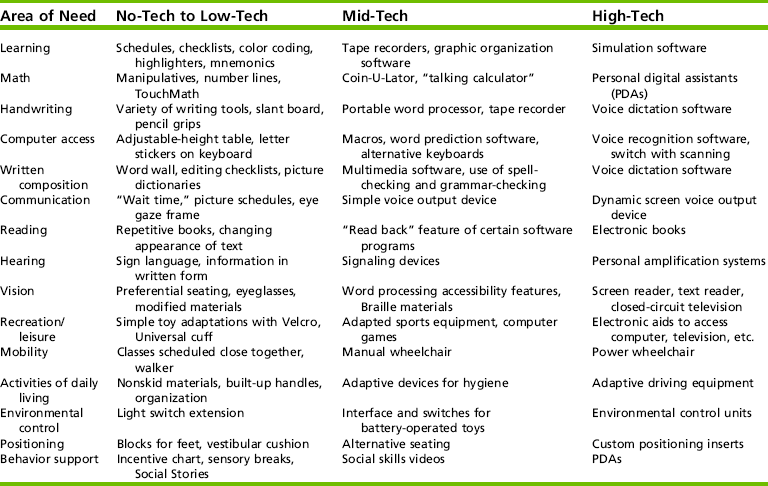
From Schoonover, J., Levan, P., & Argabrite Grove, R. (2006). Occupational therapy and assistive technology in school-based practice: Supporting participation. OT Practice, 11(1), CE1-CE8.
To successfully blend the use of AT into occupational therapy practice, it is necessary to embrace a holistic approach of AT as both a device and a service. Considering the hopes and dreams of a child, his or her family, and the physical and social climate, occupational therapy practitioners can ensure that AT is matched appropriately to the child. Best-practice interventions should include AT and are dependent on the practitioner’s ability to not only articulate what a child needs, but to also remain knowledgeable of current technologies, document the impact of interventions, collaborate with other team members, and influence decision making about participation across environmental contexts. The challenge is to increase collaborative practices, insist on opportunities for professional development, advocate for the provision of appropriate AT, and continue to define the role of occupational therapy in the provision of AT.
Various resources on the Internet can help occupational therapy practitioners stay current with all the changes in AT. Recent advances in AT allow many devices to grow and expand with the child during the developmental years and into adolescence and adulthood as they undergo transition into higher education and community work experiences. With the current pace of progress and research, future AT will offer greater ease of use, wider application, assistance in additional areas of function, and more availability as a result of lower costs (Case Study 20-1). The responsibility of those who implement AT intervention is to provide a health-promoting balance between occupational roles and activities consistent with the individual’s valued goals and interests, as well as the demands of society.100 The direct connection between occupational therapy and AT allows us to unlock human potential and optimize human performance through the promotion of participation in activities that are personally meaningful, relevant, and life sustaining.
 CASE STUDY 20-1 AT Problem Solving
CASE STUDY 20-1 AT Problem Solving
Jeremy is a 2-year-old with Down syndrome. His family wants to provide every opportunity for him to develop cognitive skills. They plan for him to attend regular education classrooms as he gets older. They were recently at a conference and heard about computers as tools for supporting learning and educational performance for some children with Down syndrome. They asked the early intervention team to recommend a computer system and software to use with Jeremy. What would you recommend?
Linnea is a third-grade student with spinal muscular atrophy. She is fully included in her neighborhood school with support from related services as needed. Recently, she has been complaining to her parents and therapists that her hand gets tired when writing and that her handwriting looks “sloppy.” Her teacher also has noticed that she seems irritable and lacks concentration during class. Linnea, her family, and her therapists have discussed using computers for written communication in the past, but Linnea and her family have always been reluctant to explore this at length because she does not want to “look different.” Linnea has had experience with computers since kindergarten. Her class goes to the computer lab three times a week, and she began learning basic keyboarding skills in second grade. Her classroom has two computers that students use for drill, practice, and special projects. How would you address Linnea’s handwriting problems?
Margy is 17 years old and has cognitive impairments and attention deficit–hyperactivity disorder (ADHD). During her last individualized transition plan (ITP), her family expressed the desire for Margy to get a job in the family carpet cleaning business. Margy enjoys greeting people, and others enjoy her bubbly and outgoing personality, so her dad and mom felt it would be good if she could work with the receptionist in the front office of their business. Her dad felt that she should have more responsibility than simply greeting customers. He said that Margy has always enjoyed working on the computer and recommended that she learn data entry on the computer to make productive use of her down time when she was not talking with a customer. The team agreed that this could be a reasonable expectation for Margy and worked to develop a plan to reach this goal. Describe a plan that evidences multidisciplinary input.
REFERENCES
1. Abramson, L.Y., Seligman, M.E.P., Teasdale, J.D. Learned helplessness in humans: Critique and reformation. Journal of Abnormal Psychology. 1978;87:49–74.
2. American Occupational Therapy Association. AOTA 2000 member compensation survey. Bethesda, MD: Author, 2000.
3. American Occupational Therapy Association. Assistive technology within occupational therapy practice. American Journal of Occupational Therapy. 2004;58:678–680.
4. Anson, D.K. Alternative computer access: A guide to selection. Philadelphia: F.A. Davis, 1997.
5. Argabrite Grove, R., Broeder, K., Gitlow, L., Goodrich, B., Levan, P., Moser, C., et al. Assistive technology in the schools: From start to finish. St. Louis, MO: Pre-Conference Institute at AOTA’s Annual Conference & Expo, 2007.
6. Assistive Technology Training Online (ATTO) Project. Retrieved October 2006, from http://atto.buffalo.edu/registered/ATBasics/Curriculum/Math/printmodule.php.
7. Bain, B.K., Leger, D. Assistive technology: An interdisciplinary approach. New York: Churchill Livingstone, 1997.
8. Baush, M.E., Ault, M.J., Hasselbring, T.S. Assistive technology planner: From IEP consideration to classroom implementation. Lexington, KY: National Assistive Technology Research Institute, 2006.
9. Behrmann, M.M. A brighter future for early learning through high tech. The Pointer. 1984;28:23–26.
10. Behrmann, M.M., Jones, J.K., Wilds, M.L. Technology intervention for very young children with disabilities. Infants and Young Children. 1989;1:66–77.
11. Beukelman, D.R., Mirenda, P. Augmentative and alternative communication: Management of severe communication disorders in children and adults. Baltimore: Brookes, 1992.
12. Beukelman, D.R., Mirenda, P. Augmentative and alternative communication: Management of severe communication disorders in children and adults, 3rd ed. Baltimore: Brookes, 2005.
13. Beukelman, D.R., McGinnis, J., Morrow, D. Vocabulary selection in augmentative and alternative communication. Augmentative and Alternative Communication. 1991;7:171–185.
14. Blackstone, S. False beliefs, widely held. Augmentative Communication News. 2006;3:1–6.
15. Bloomfield, B.C. Icon to, I Can: A visual bridge to independence. TEACCH International Conference, Chapel Hill, NC, May 23–24, 2000.
16. Bowser, G., Reed, P. Education TECH points: A framework for assistive technology planning. Winchester, OR: Coalition for Assistive Technology in Oregon, 1998.
17. Bryen, D.N., Cohen, K., Carey, A. Augmentative communication employment training and supports: Some employment outcomes. Journal of Rehabilitation. 2004;70:10–18.
18. Burgstahler, S. The role of technology in preparing youth with disabilities for postsecondary education and employment. Journal of Special Education Technology. 2003;18:7–20.
19. Burkhart, L. Getting past learned helplessness for children who face severe challenges: Four secrets for success, 2002. Retrieved October 9, 2006, from, http://www.lburkhart.com.
20. Burns, M.S., Griffin, P., Snow, C.E. Starting out right: A guide to promoting children’s reading success, Washington, DC, National Academy Press, 1999. Available online:, http://www.nap.edu/html/sor/.
21. Carlson, S.J., Clarke, C.D., Harden, B., Karr, S., Rosenberg, G.G., Swinth, Y.L., et al. Assistive technology and IDEA: Effective practices for related services personnel. Rockville, MD: American Speech-Language-Hearing Association (ASHA), 2003.
22. Castellani, J., Bowser, G. Transition planning: Assistive technology supports and services. In Technology in Action, 2. Arlington, VA: Center for Technology in Education, Johns Hopkins University, and Technology and Media Division of the Council for Exceptional Children; 2006.
23. Castellani, J., Jetts, T. Using technology to provide access to the general education curriculum-techniques to try. In: Wilbarger C., ed. Technology and media for accessing the curriculum: Instructional support for students with disabilities. Arlington, VA: Technology and Media Division (TAM) Council for Exceptional Children, 2005.
24. Center for Universal Design About universal design, 1997. Retrieved August 30, 2008, from, http://design.ncsu.edu/cud/about_ud/about_ud.htm.
25. Clarke, M., Kirton, A. Patterns of interaction between children with physical disabilities using augmentative and alternative communication systems and their peers. Child Language Teaching and Therapy. 2003;19:135–151.
26. Cole, J., Swinth, Y.L. Comparison of the touch-free switch to a physical switch, children’s abilities and preferences: A pilot study. Journal of Special Education Technology. 2004;19(2):19–30.
27. Collier, B. When I grow up…Supporting youth who use augmentative communication for adulthood. Proceedings of the 2005 Alberta rehabilitation and assistive technology consortium conference. Edmonton, Canada, 2005. Retrieved August 2008 from, http://www.acrat.ca.
28. Cook, A., Polgar, J. Cook & Hussey’s Assistive technologies: Principles and practice, 3rd ed. St. Louis: Elsevier, 2008.
29. Cornell University, Computers in schools are putting elementary schoolchildren at risk for posture problems, says Cornell study. Science Daily 1999. Retrieved August 2008 from, http://www.sciencedaily.com/releases/1999/02/990202071806.htm.
30. Demers, L., Weiss-Lambrou, R., Ska, B. The Quebec user evaluation of satisfaction with assistive technology (QUEST 2.0): An overview and recent progress. Technology and Disability. 2002;14:101–105.
31. Demers, L., Wessels, R.D., Weiss-Lambrou, R., Ska, B., De Witte, L.P. An international content validation of the Quebec user evaluation of satisfaction with assistive technology (QUEST). Occupational Therapy International. 1999;6:159–175.
32. DeRuyter, F. Evaluating outcomes in assistive technology: Do we understand the commitment? Assistive Technology. 1995;7:3–16.
33. Dickey, R., Shealey, S.H. Using technology to control the environment. American Journal of Occupational Therapy. 1987;41:717–721.
34. Doster, S., Politano, P. Augmentative and alternative communication. In: Hammel J., ed. AOTA self-paced clinical course: Technology and occupational therapy: A link to function. Rockville, MD: AOTA, 1996.
35. Douglas, J., Reeson, B., Ryan, M. Computer microtechnology for a severely disabled preschool child. Child Care: Health and Development. 1988;14:93–104.
36. Dowden, P., Cook, A.M. Choosing effective selection techniques for beginning communicators. In: Reichle J., Beukelman D., Light J., eds. Exemplary practices for beginning communicators. Baltimore: Brookes; 2002:101–124.
37. Downing, J. Teaching communication skills to students with severe disabilities, 2nd ed. Baltimore: Brookes, 2005.
38. Drager, K. Light technologies with different system layouts and language organizations. Journal of Speech, Language, and Hearing Research. 2003;46:289–312.
39. Edyburn, D.L. 1999 in review: A synthesis of the special education technology literature. Journal of Special Education. 2000;15:7–18.
40. Edyburn, D.L. Cognitive rescaling strategies. Closing the Gap. 2002;21:1–4.
41. Edyburn, D.L., Assistive technology and evidence-based practice. ConnSENSE Bulletin 2003. Retrieved March 2008, from, http://www.connsensebulletin.com.
42. Farmer, L., Turn on to reading through technology. Library Talk, Sept./Oct., 1998:16–17.
43. Foulds, R.A. Applications of microcomputers in the education of the physically disabled child. Exceptional Children. 1982;49:143–162.
44. Gelderblom, G.J., deWitte, L.P. The assessment of assistive technology outcomes, effects and costs. Technology and Disability. 2002;14:91–94.
45. George, C.L., Schaff, J.I., Jeffs, T.L. Physical access in today’s schools: Empowerment through assistive technology. In: Edyburn D., Higgins K., Boone R., eds. The handbook of special education technology. Whitefish Bay, WI: Knowledge by Design, 2005.
46. Glickman, L., Deitz, J., Anson, D., Stewart, K. Effect of switch control site on computer skills of infants and toddlers. American Journal of Occupational Therapy. 1996;50:545–553.
47. Goldbart, J., Marshall, J. Pushes and pulls” on the parents of children who use AAC. Augmentative and Alternative Communication. 2004;20:194–208.
48. Hammel, J., Niehues, A. Integrating general and assistive technology into school-based practice: Process and information resources. In: Case-Smith J., ed. Occupational therapy: Making a difference in school system practice. Rockville, MD: AOTA, 1998.
49. Hansell, N. The person-in-distress: On the biosocial mechanisms of adaptation. New York: Behavioral Sciences Press, 1974.
50. Higgins, E.L., Raskind, M.H. Speaking to read: the effects of continuous vs. discrete speech recognition systems on the reading and spelling of children with learning disabilities. Journal of Special Education Technology. 2000;15:19–30.
51. Hitchcock, C., Stahl, S., Assistive technology, universal design, universal design for learning: improved learning opportunities. Journal of Special Education Technology 2003;18:45–52. IDEA Practices. (2004). Retrieved August 2008 from, http://www.ideapractices.org.
52. Hodgdon, L.A. Visual strategies for improving communication, Volume I: Practical supports for school and home. Troy, MI: QuirkRoberts Publishing, 1995.
53. Jackson, R. Curriculum access for students with low-incidence disabilities: The promise of universal design for learning, Wakefield, MA, National Center on Accessing the General Curriculum, 2005. Retrieved August 2008 from, http://www.cast.org/publications/ncac/ncac_lowinc.html.
54. Judge, S.L. Computer applications in programs for young children with disabilities: Current status and future directions. Journal of Special Education Technology. 2001;16(1):29–40.
55. Kangas, K.M. The task performance position: providing seating for accurate access to assistive technology. Physical Disabilities Special Interest Section Quarterly. 2000;23(September):1–3.
56. Kelker, K., Holt, R. Family guide to assistive technology. Cambridge, MA: Brookline Books, 2000.
57. Kerr, S.T. Technology and the future of schooling: Ninety-fifth yearbook of the national society for the study of education, part II. Chicago, IL: University of Chicago Press, 1996.
58. Koenig, A.J. A framework for understanding the literacy of individuals with visual impairments. Journal of Visual Impairment and Blindness. 1992;86:277–284.
59. Koenig, A.J., Holbrook, M.C., Literacy skills. Koenig, A.J., Holbrook, M.C., eds. Foundations of education: Instructional strategies for teaching children and youth with visual impairments, New York, American Foundation for the Blind, 2000;Vol. 2:265–329.
60. Koppenhaver, D.A., Evans, D., Yoder, D.E. Childhood reading and writing experiences of literate adults with severe speech and motor impairments. Augmentative and Alternative Communication. 1991;7:20–33.
61. Lahm, E.A. Technology with low incidence populations: Promoting access and learning. Reston, VA: The Council for Exceptional Children, 1989.
62. Lahm, E.A., Sizemore, L. Factors that influence assistive technology decision-making. Journal of Special Education Technology. 2002;17(1):15–26.
63. Lamb, P. The role of the vocational rehabilitation counselor in procuring technology to facilitate success in postsecondary education for youth with disabilities. Journal of Special Education Technology. 2003;18(4):53–63.
64. Law, M., Baptiste, S., Carswell, A., McColl, M.A., Polatajko, H., Pollock, N. Canadian Occupational Performance Measure, 4th ed. Toronto, ON: Canadian Association of Occupational Therapy Inc, 2005.
65. Law, M., Cooper, B., Strong, S., Stewart, D., Rigby, P., Letts, L. The person-environment-occupation model: A transactive approach to occupational performance. Canadian Journal of Occupational Therapy. 1996;63:9–23.
66. Lewis, R. Classroom technology for students with learning disabilities. In: Edyburn D., Higgins K., Boone R., eds. Handbook of special education technology research and practice. Whitefish Bay, WI: Knowledge by Design, 2005.
67. Light, J. Toward a definition of communicative competence for individuals using augmentative and alternative communication systems. Augmentative and Alternative Communication. 1989;5:137–144.
68. Light, J.C., Drager, K. Improving the design of augmentative and alternative technologies for young children. Assistive Technology. 2002;14:17–32.
69. Maier, S.F., Seligman, M.E. Learned helplessness: Theory and evidence. Journal of Experimental Psychology: General. 1976;105:3–46.
70. Mirenda, P. Bonding the uncertain mosaic. Augmentative and Alternative Communication. 1993;9:3–9.
72. Mistrett, S. Assistive technology helps young children with disabilities participate in daily activities. In: Wilbarger C., ed. Technology and media for accessing the curriculum: Instructional support for students with disabilities. Arlington, VA: Technology and Media Division (TAM), 2005.
73. National Joint Committee for the Communication Needs of Persons with Severe Disabilities. Guidelines for meeting the communication needs of persons with severe disabilities. ASHA. 1992;34(March):1–8.
74. Neighborhood Legal Services, Inc Funding of assistive technology: The public school’s special education system as a funding source: The cutting edge, 2003. Retrieved October 10, 2008, from, http://www.nls.org.
75. Office of Special Education and Rehabilitative Services, U.S. Department of Education. Reuse your assistive technology. Retrieved July 2008 from, http://www.ed.gov/print/programs/atsg/at-reuse.html.
76. Parette, H.P., VanBiervliet, A. A prospective inquiry into technology needs and practices of school-aged children with disabilities. Journal of Special Education Technology. 1990;10:198–206.
77. Phillips, B., Zhao, H. Predictors of assistive technology abandonment. Assistive Technology. 1993;5:36–45.
78. Post, K.M., Hartmann, K., Gitlow, L., Rakoski, D. AOTA’s Centennial Vision for the future: How can technology help? Technology Special Interest Section Quarterly. 2008;18(March):1–4.
79. QIAT Consortium AT in transition, 2007. Retrieved June 2008 from, http://natri.uky.edu/assoc_projects/qiat/documents/6%20QIAT%20QIs%20Transition.doc.
80. QIAT Consortium Quality indicators for assistive technology services, 2007. Retrieved August 2008 from, http://natri.uky.edu/assoc_projects/qiat/.
81. Reed, P. School profile of assistive technology services, 2000. Retrieved August 2008 from, http://www.wati.org/AT_Services/schoolprofile.html.
82. Reed, P. Designing environments for successful kids. Oshkosh, WI: Wisconsin Assistive Technology Initiative, 2003.
83. Reed, P. The WATI assessment package, 2004. Retrieved October 2005 from, http://www.wati.org/Materials/pdf/wati%20assessment.pdf.
84. Richardson, C., Technology supports for math. T/TAC Linklines 2001. (November/December). Retrieved July 2009 from, http://web.wm.edu/ttac/articles/assistivetech/mathsupports.html.
85. Robinson, L.M. Designing computer intervention for very young handicapped children. Journal of the Division for Early Childhood. 1986;103:209–213.
86. Rose, D.H., Meyer, A. Teaching every student in the digital age: Universal design for learning. Alexandria, VA: Association for Supervision and Curriculum Development, 2002.
87. Rowland, C., Schweigert, P. Tangible symbol systems: Making the right to communicate a reality for individuals with sever disabilities, 2nd ed. Portland, OR: OHSU Design to Learn Projects, 2000.
88. Ryan, R., Deci, E. Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. American Psychologist. 2000;55:68–78.
89. Scherer, M.J. Outcomes of assistive technology use on quality of life. Disability and Rehabilitation. 1996;18:439–448.
90. Scherer, M.J. Living in the state of stuck: How technology impacts the lives of people with disabilities. Cambridge, MA: Brookline Books, 2000.
91. Scherer, M.J., Craddock, G. Matching person & technology (MPT) assessment process. Technology and Disability. 2002;14:125–131.
92. Scherer, M.J., Lane, J.P. Assessing consumer profiles of “ideal” assistive technologies in ten categories: An integration of quantitative and qualitative methods. Disability and Rehabilitation. 1997;19:528–535.
93. Schmeler, M.R., Strategies in documenting the need for assistive technology: An analysis of documentation procedures. AOTA Technology Special Interest Section Quarterly, Bethesda, MD, American Occupational Therapy Association, 1997;Vol. 7:.
94. Schoonover, J., Feist, C. Using computers to design accessible learning environments. AOTA. School System Special Interest Section Quarterly. 2007;14(March):1–4.
95. Schoonover, J., Levan, P., Argabrite Grove, R. Occupational therapy and assistive technology in school-based practice: supporting participation. OT Practice. 2006;11:CE1–CE8.
96. Sibert, R.I. Financing assistive technology: An overview of public funding sources. AOTA Technology Special Interest Section Newsletter. 1997;7:1–4.
98. Spencer, J. Alternative meanings of assistive technology. In: Gray D.B., Quatrano L.A., Lieberman M.L., eds. Designing and using assistive technology: The human perspective. Baltimore, MD: Brookes, 1998.
99. Stodden, R.A., Conway, M.A., Chang, K.B.T. Findings from the study of transition, technology and postsecondary supports for youth with disabilities: Implications for secondary school educators. Journal of Special Education Technology. 2003;18(4):29–43.
100. Stoller, L.C. Low-tech assistive devices: A handbook for the school setting. Framingham, MA: Therapro, Inc, 1998.
101. Sullivan, M.W., Lewis, M. Assistive technology for the very young: Creating responsive environments. Infants and Young Children. 2000;12(4):34–52.
102. Swanson, H.L. Instructional components that predict treatment outcomes for students with learning disabilities: Support for a combined strategy and direct instruction model. Learning Disabilities Research and Practice. 1999;14:129–140.
103. Sweeney, J. Getting assistive technology into the mainstream the EASY way. Closing the Gap. 2007;25:1–4.
104. Swinth, Y.L. The meaning of assistive technology in the lives of high school students and their families. Seattle, WA: University of Washington, 1997. [Unpublished doctoral dissertation].
105. Swinth, Y.L. Assistive technology in early intervention: Theory and practice. In Case-Smith J., ed.: Pediatric occupational therapy and early intervention, 2nd ed., Woburn, MA: Butterworth-Heinemann, 1998.
106. Swinth, Y.L., Anson, D. Alternatives to handwriting: Keyboarding and text-generation techniques for schools. In: Case-Smith J., ed. AOTA self-paced clinical course: Occupational therapy: Making a difference in school system practice. Rockville, MD: American Occupational Therapy Association, 1998.
107. Todis, M., Walker, H.M. User perspectives on assistive technology in educational settings. Focus on Exceptional Children. 1993;46(3):1–16.
108. U.S. Department of Education, Office of Special Education Programs, Data Analysis System Children with disabilities receiving special education under Part B of the Individuals with Disabilities Education Act, 2006. Retrieved July 2008 from, https://www.ideadata.org/tables30th/ar_1-1.xls.
109. Washington Assistive Technology Alliance [WATA] Paying for the assistive technology you need: A consumer guide to funding sources in Washington State, 1999. Retrieved November 2003 from, http://uwctds.washington.edu/resources/legal/funding%20manual/index.htm.
110. Wehmeyer, M.L. Self-determination as an educational outcome: Why is it important to children, youth, and adults with disabilities? In: Sands D.J., Wehmeyer M.L., eds. Self-determination across the life span: Independence and choice for people with disabilities. Baltimore: Brookes; 1996:17–36.
111. Wehmeyer, M.L., Promoting the self-determination of students with severe disabilities. ERIC Digest 2002. Retrieved June 2008 from, http://eric.ed.gov/ERICDocs/data/ericdocs2sql/content_storage_01/0000019b/80/29/d2/46.pdf.
112. Weintraub, H., Bacon, C., Wilcox, M., AT and young children: Confidence, experience and education of early intervention providers. Research Brief, Tots n Tech Research Institute, 2004;Vol. 1. Retrieved February 2008 from, http://tnt.asu.edu.
113. Zabala, J.S. 2002 update of the SETT framework, 2002. Retrieved September 2003 from (University of Kentucky), http://sweb.uky.edu/~jszabala/JoySETT.html.
114. Zabala, J. 10 Things everyone needs to know about assistive technology in schools in 2006. Orlando, FL: Presented at the national conference of the Assistive Technology Industry Association (ATIA), 2007.